David Garcia is a proud father and maintenance facility worker at the Region 19 Education Services Center in El Paso, TX. However, Mr. Garcia’s daily life is often affected by his chronic lower back pain. After experiencing worsening symptoms for approximately two years, David Garcia was recommended to seek chiropractic care with Dr. Alex Jimenez by his sister, a previous patient of Dr. Jimenez. Mr. Garcia has since experienced tremendous relief from his lower back pain and he is grateful to Dr. Alex Jimenez and his staff for providing him with education regarding his health issues as well as properly caring for his injuries and/or conditions. David Garcia recommends Dr. Alex Jimenez as the non surgical choice for lower back pain.
Chiropractic Care For Lower Back Pain
Low back pain is not a specific injury or condition but rather a symptoms which may be caused by a wide variety of underlying health issues, all of varying levels of severity. The majority of low back pain does not have a clear cause but is believed to be the result of non-serious musculoskeletal problems, including sprains or strains. Obesity, smoking, weight gain during pregnancy, stress, poor physical condition, poor posture and poor sleeping positions have also been attributed to develop low back pain.A full list of possible causes includes many less common conditions. Physical causes may include osteoarthritis, degeneration of the discs between the vertebrae or a spinal disc herniation, broken vertebra(e) (such as from osteoporosis) or, rarely, an infection or tumor of the spine.
Share Free Ebook
If you have enjoyed this video and/or we have helped you in any way please feel free to subscribe and share us.
Thank You & God Bless.
Dr. Alex Jimenez DC, C.C.S.T
If you are pregnant and have back pain, you are not alone. An estimated 50 to 70 percent of women who are pregnant experience back pain, according to the American Pregnancy Association. While pregnancy and childbirth is one of the most incredible experiences a woman can have, it is also very hard on her body. There are many dramatic changes that take place during that 9 to 10 month of gestation so it is understandable that she is going to feel some aches and pains along the way.
There are a number of reasons why a pregnant woman may experience back pain including:
Natural changes to her body such as softening of ligaments and loosening of joints as her body prepares to give birth
A shift in her center of gravity as her girth increases.
Weight gain.
Position of the baby.
Her posture.
Stress, exhaustion, and worry.
Is Chiropractic Care Safe During Pregnancy?
Chiropractic care has long been held as a viable method for relieving back pain in pregnant women. Historically, midwives and other natural or alternative practitioners were the ones advocating its many benefits. This resulted in minimal data from clinical studies existing on the topic.
However, in the last decade or so, researchers have been looking closer at chiropractic and its many benefits. In one study of pregnant women and chiropractic, 94 percent of the participants experienced dramatic improvement in their pain in just 5 days.
Today many doctors and obstetricians are sending their pregnant patients to chiropractors to help them manage their back and joint pain. It is perfectly safe for both mother and baby � and both can benefit from it.
Benefits Of Chiropractic Care During Pregnancy
While chiropractic care during pregnancy can be used as a safe, non-invasive, and drug free method of pain relief, women may also enjoy other benefits which include:
A healthier, happier pregnancy.
Improved mood and less anxiety.
More mobility.
Decreased morning sickness and nausea.
Easier, faster labor and delivery.
Better flexibility.
In some cases, prevent cesarean delivery.
Improved sleep.
Faster recovery time.
Relief of pain in the back, joints, and neck.
By keeping the body in proper alignment, chiropractic care can help a woman have a healthier, happier pregnancy. She can enjoy the many benefits and experience less pain so that she can better focus on the joy of pregnancy and the wonder of bringing a new life into the world.
Why You Should Have Chiropractic Care During Pregnancy
Pregnancy brings about many changes in a woman�s body. Hormonal changes as well as physiological ones occur at rapid speeds as her body creates and maintains a perfect environment where her baby will develop and grow. These changes can cause the spine or joints to become misaligned. When this occurs, painful conditions can be created, including:
Increased curvature of the back.
Pelvic changes.
Protruding abdomen that puts pressure on the back.
Changes in posture.
Keeping the pelvis and lower back well balanced and aligned is integral to preventing lower back pain during pregnancy. What�s more, when the pelvis and spine are not in alignment, it can limit the amount of room the baby has in the womb. This condition is called intrauterine constraint. This can also inhibit the baby�s ability to get in an optimal position for delivery.
Keeping the body, including the spine, in proper alignment is vital to mobility, flexibility, and overall wellness of the body even when it is not pregnant. However, pregnancy puts specific stress on the body, creating certain needs that chiropractic care can meet. It is safe, it is effective, it is fast, and it works.
Chiropractic Clinic Extra: Stress Management Care & Treatments
Back Pain Management: Denise was involved in an auto accident which resulted in low back pain. When she realized she couldn’t sit, walk or sleep for extended periods of time without experiencing painful symptoms, Denise found chiropractic care with Dr. Alex Jimenez in El Paso, TX. Once she received treatment for her auto accident injuries, Denise experienced relief from her symptoms and she was able to perform her everyday activities once again. Thanks to the education and care Dr. Alex Jimenez provided, Denise regained her original health and wellness.
Back pain is common, with roughly nine out of ten adults experiencing it at some time in their life, and five from ten working adults developing it every year. Some estimate around 95 percent of Americans will experience back pain at some time in their lifetime. It’s by far the usual cause of chronic pain, as it is also a significant contributor of missed work and disability. In the United States alone, acute cases of lower back pain are the fifth most common reason for physician visits and causes 40 percent of missed days off work. Furthermore, it is the only leading cause of disability globally. Back pain management is possible through chiropractic treatment.�For Answers to any questions you may have please call Dr. Jimenez at 915-850-0900
Please Recommend Us: If you have enjoyed this video and/or we have helped you in any way please feel free to recommend us. Thank You.
Truide Torres, office manager, first received chiropractic care with Dr. Alex Jimenez during her pregnancy for her lower back pain. Mrs. Torres experienced aggravating symptoms throughout the progression of her pregnancy, which led her to seek a natural treatment approach for her own health as well as that of her own baby. Once Truide Torres started chiropractic treatment with Dr. Alex Jimenez, she recovered her quality of life and was able to return to her original state of well-being. As an office manager, Truide Torres also receives regular chiropractic care for any lower back pain which may occur as a result of her job. Mrs. Truide expresses how important it is to continue her spinal maintenance and she highly recommends Dr. Alex Jimenez as the non-surgical choice for a variety of health issues.
Low back pain (LBP) is a frequent health issue involving the muscles, nerves, and bones of the spine. Pain may differ from a dull persistent pain to a sudden sharp sensation. Low back pain can be classified by length and severity (pain lasting less than 6 months), sub-chronic (6 to 12 months), or chronic (over 12 months). The status could be further categorized by the underlying cause as both bodily, non-mechanical, or referred pain. The symptoms of low back pain may generally improve in a couple weeks from the time they begin, however, some cases may require additional treatment. In the majority of episodes of lower back pain, a specific underlying cause isn’t identified or properly cared for, and healthcare professionals may attribute it to mechanical issues like joint or muscle strain.
Prenatal Yoga Exercises For Low Back Pain
Back Clinic News Extra: Migraine Pain Treatment With Chiropractic
Damaris Foreman suffered from migraines for about 23 years. After receiving traditional treatment for her migraine pain without much improvement, she was finally recommended to seek migraine pain treatment with Dr. Alex Jimenez, a chiropractor in El Paso, TX. Damaris greatly benefitted from chiropractic care and she experienced a tremendous sense of relief following her first spinal adjustment and manual manipulation. Damaris Foreman was able to confront many of her misconceptions and she learned very much about her migraine pain. Damaris describes Dr. Alex Jimenez’s migraine pain treatment as one of the best treatment she’s received and she highly recommends chiropractic care as the best non-surgical choice for improving and managing her migraines.
A migraine can be identified as a primary headache disorder characterized by recurrent headaches characterized from moderate to severe in intensity. Typically, the headaches affect one half of the head, are pulsating in nature, and can last from two to 72 hours. Associated symptoms may include nausea, vomiting, and sensitivity to light, sound, or smell. The pain may be aggravated by physical activity. Up to one-third of people who suffer from migraines experience migraine with aura: typically a brief period of visual disturbance that signals that the headache will soon happen. An aura can occur with little or no headache pain following it.
Please Recommend Us: If you have enjoyed this video and/or we have helped you in any way please feel free to recommend us. Thank You.
Back pain is a daily issue for millions of Americans, with a variety of medial issues being the culprit. The results of lower back pain on the economy as a whole are far reaching, from tons of lost work time to enormous medical costs. Maignes Syndrome is estimated to be the cause of a great deal of the instances of lower back pain.
Never heard of it? Lucky you because those who are diagnosed with Maignes Syndrome suffer pain that sometimes lasts for weeks or even months, and can become quite severe. Discomfort is increased sometimes when the patient twists his torso, or lifts a heavy object.
What Is Maignes Syndrome?
Also called Thoracolumbar Junction Syndrome, Maignes Syndrome is a spinal disorder that is located in the nerves in the upper lumbar region of the back, causing pain to radiate along the nerves from the site. This spinal condition creates difficult to diagnose symptoms, since it often results in pain in a different part of the body than the actual source. It is believed this “condition exists because of the facet joint issues at the junction between the middle spine and lower spine.”. The pain from Maignes Syndrome usually shows up in the hip, lower back, or groin.
If you are experiencing lower back pain, you may suffer from Maignes Syndrome. Schedule a chiropractic visit as soon as possible, because a chiropractor benefits Maignes Syndrome sufferers in four important ways.
Chiropractors Can�
�Help Correctly Diagnose It
Unfortunately, the nature of the pain and location of the condition frequently cause Maignes Syndrome to be misdiagnosed. Sacroiliac joint pain is sometimes the diagnosis they receive, which hinders proper treatment. For this reason, the patient needs to make certain they are working with an experienced chiropractor who understands the subtle differences of the two conditions.
�Adjust The Area Where The Issue Originates
In order to minimize the symptoms of the condition, a chiropractor can administer adjustments on and around the area causing the issue, the thoracolumbar facet joints. Aligning this area correctly, and loosening the area that may have become tight from overcompensation, assists in relieving pain from Maignes Syndrome.
�Offer At Home Exercises To Help With Healing
Fortunately, there are exercises that can aid Maignes Syndrome, both in loosening the tightness of the afflicted area, and building up the surrounding muscle strength so the body can compensate for the issue. A chiropractor who understands this spinal condition can walk you through a step-by-step exercise regimen of the types of exercises that will help your body adapt to and heal from Maignes Syndrome.
�Promote Your Body’s Ability To Heal Itself
Chiropractic care is a broad-based approach to the body’s inner function and balance. Experienced chiropractors understand that all parts fit together for overall health. A patient with Maignes Syndrome benefits from chiropractic care because of this.
Your chiropractor will make a series of adjustments that help the nervous system work at optimum capacity, which promotes healing to the entire body. Attacking Maignes Syndrome directly at the site and through the body as a whole promotes faster healing and increased mobility.
Individuals with Maignes Syndrome unfortunately face an uphill battle that begins with being correctly diagnosed. The complexity of the spinal condition is the primary reason to seek a professional chiropractor’s opinion at the first sign of ongoing lower back pain. Once Maignes Syndrome is correctly pinpointed, the chiropractor will be able to design an in-house and at-home blend of treatment options to minimize your healing time and achieve a pain-free, fully functioning back.
Have you ever experienced low back pain? If you haven’t already, there’s a high probability you will present at least one case of back pain sometime during your lifetime. Back pain is one of the most prevalent spine health issues reported among the population of the United States, affecting up to 80 percent of Americans at some point in their lives. Back pain is not a specific disease, rather it is a symptom which may develop as a result of a variety of injuries and/or conditions.�Although most cases typically resolve on their own, the effective treatment of acute low back pain is essential towards preventing chronic low back pain.
Chiropractors and physical therapists frequently utilize a similar series of treatment methods, such as spinal adjustments and manual manipulations as well as massage and physical therapy, to help treat symptoms of back and low back pain. Many healthcare professionals, however, have started using the McKenzie method to manage acute back pain. The purpose of the following article is to educate patients on the effectiveness of the McKenzie method for acute non-specific low back pain.
The McKenzie Method for the Management of Acute Non-Specific Low Back Pain: Design of a Randomised Controlled Trial
Abstract
Background
Low back pain (LBP) is a major health problem. Effective treatment of acute LBP is important because it prevents patients from developing chronic LBP, the stage of LBP that requires costly and more complex treatment.
Physiotherapists commonly use a system of diagnosis and exercise prescription called the McKenzie Method to manage patients with LBP. However, there is insufficient evidence to support the use of the McKenzie Method for these patients. We have designed a randomised controlled trial to evaluate whether the addition of the McKenzie Method to general practitioner care results in better outcomes than general practitioner care alone for patients with acute LBP.
Methods/Design
This paper describes the protocol for a trial examining the effects of the McKenzie Method in the treatment of acute non-specific LBP. One hundred and forty eight participants who present to general medical practitioners with a new episode of acute non-specific LBP will be randomised to receive general practitioner care or general practitioner care plus a program of care based on the McKenzie Method. The primary outcomes are average pain during week 1, pain at week 1 and 3 and global perceived effect at week 3.
Discussion
This trial will provide the first rigorous test of the effectiveness of the McKenzie Method for acute non-specific LBP.
Background
In Australia, low back pain (LBP) is the most frequently seen musculoskeletal condition in general practice and the seventh most frequent reason for consulting a physician[1,2]. According to the Australian National Health Survey, 21% of Australians reported back pain in 2001; additionally, the Australian Bureau of Statistic’s 1998 Survey of Disability, Ageing and Carers estimated that over one million Australians suffer from some form of disability associated with back problems[1].
LBP poses an enormous economic burden to society in countries such as the USA, UK and The Netherlands[3]. In the largest state in Australia, New South Wales, back injuries account for 30% of the cost of workplace injuries, with a gross incurred cost of $229 million in 2002/03[4]. It is expected that most people with an acute episode of LBP will improve rapidly, but a proportion of patients will develop persistent lower levels of pain and disability[5,6]. Those patients with chronic complaints are responsible for most of the costs[6]. Effective treatment of acute LBP is important because it prevents patients from developing chronic LBP, the stage of LBP that requires costly and more complex treatment.
There is a growing concern about effectiveness of treatments for LBP, as reflected in the large number of systematic reviews published in the last 5 years addressing this issue. [7-12]. Despite the large amount of evidence regarding LBP management, a definitive conclusion on which is the most appropriate intervention is not yet available. A comparison of 11 international clinical practice guidelines for the management of LBP showed that the provision of advice and information, together with analgesics and NSAIDs, is the approach consistently recommended for patients with an acute episode[13]. Most guidelines do not recommend specific exercises for acute LBP because trials to date have concluded that it is not more effective than other active treatments, or than inactive or placebo treatments[8]. However, some authors have suggested that the negative results observed in trials of exercises are a consequence of applying the same exercise therapy to heterogeneous groups of patients. [14-16]. This hypothesis has some support from a recent high-quality randomised trial in which treatment based on a diagnostic classification system led to larger reductions in disability and promoted faster return to work in patients with acute LBP than the therapy recommended by the clinical guidelines[17].
In 1981, McKenzie proposed a classification system and a classification-based treatment for LBP labelled Mechanical Diagnosis and Treatment (MDT), or simply McKenzie Method[18]. Of the large number of classification schemes developed in the last 20 years [19-26], the McKenzie Method has the greatest empirical support (e.g. validity, reliability and generalisability) among the systems based on clinical features[27] and therefore seems to be the most promising classification system for implementation in clinical practice.
Physiotherapists commonly adopt the McKenzie Method for treating patients with LBP[28,29]. A survey of 293 physiotherapists in 1994 found that 85% of them perceived the McKenzie Method as moderately to very effective[28]. Nevertheless, a recent systematic review concluded that there is insufficient evidence to evaluate the effectiveness of the McKenzie Method for patients with LBP [30]. A critical concern is that most trials to date have not implemented the McKenzie Method appropriately. The most common flaw is that all trial participants are given the same intervention regardless of classification, an approach contradictory to the principles of McKenzie therapy.
The primary aim of this trial is to evaluate whether the addition of the McKenzie Method to general practitioner (GP) care results in better outcomes than GP care alone for patients with acute non-specific LBP when effect is measured in terms pain, disability, global perceived effect, and persistent symptoms.
Methods
The University of Sydney Human Research Ethics Committee granted approval for this study.
Study Sample
One hundred and forty eight participants with a new episode of acute non-specific LBP who present to GPs will be recruited for the study. A new episode of LBP will be defined as an episode of pain lasting longer than 24 hours, preceded by a period of at least one month without LBP and in which the patient did not consult a health care practitioner[31]. Participants will be screened for eligibility at their first appointment with the GP according to the inclusion and exclusion criteria.
Inclusion Criteria
To be eligible for inclusion, participants must have pain extending in an area between the twelfth rib and buttock crease (this may or may not be accompanied by leg pain); pain of at least 24 hours duration; pain of less than 6 weeks duration; and they need to be eligible for referral to private physiotherapy practice within 48 hours.
Exclusion Criteria
Participants will be excluded if they have one of the following conditions: nerve root compromise (defined as 2 positive tests out of sensation, power and reflexes for the same spinal nerve root); known or suspected serious spinal pathology; spinal surgery within the preceding 6 months; pregnancy; severe cardiovascular or metabolic disease; or inability to read and understand English.
Recruiting GPs will record the number of patients who are invited to participate, the number who decline to participate, and the number of screened patients who are ineligible and their reasons for declining participation or ineligibility. Written consent will be obtained for each participant.
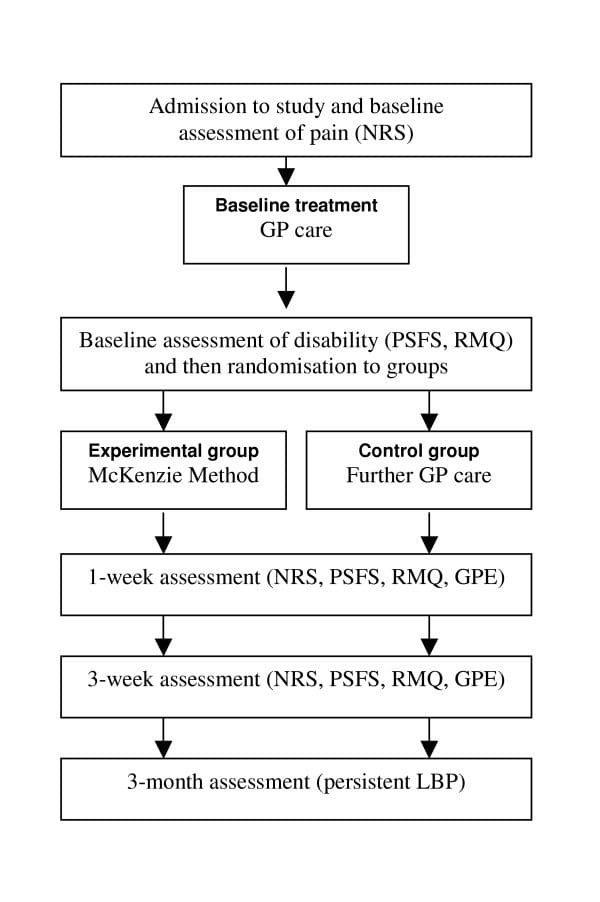
Subjects who volunteer to participate and satisfy the eligibility criteria will receive baseline treatment and then be randomly allocated to one of the study groups. To ensure equal-sized treatment groups, random permuted blocks of 4�8 participants will be used[32]. Randomisation will be stratified by Workcover compensation status. The stratified random allocation schedule will be generated by a person not otherwise involved in recruitment, assessment or treatment of subjects and the randomisation sequence will be placed in sequentially numbered, sealed envelopes. The flow of participants through the study is detailed in Figure ?1.
Figure 1: Flow of participants through the study. Legend: GP � General practitioner; NRS � Numeric pain rating scale; PSFS � Patient-specific functional scale; RMQ � Roland-Morris questionnaire; GPE � Global perceived effect; LBP � Low back pain.
Dr. Alex Jimenez’s Insight
In the management of low back pain, the attitudes, beliefs and treatment preferences of chiropractors, as well as that of physical therapists, can determine the most effective outcome measures in the care of patients with different types of spinal health issues. According to the following evidence-based research studies, the McKenzie method has been deemed to be one of the most useful treatment approaches for managing symptoms in patients with back and low back pain. Exercise and physical activity is also one of the most common treatment preferences for improving an individual’s strength, mobility and flexibility. Every healthcare professional varies in respect to their specific treatment preferences. These variations emphasize the need to identify the most effective treatment approach to guarantee proper treatment of LBP.
Outcome Measures
The McKenzie protocol is thought to promote rapid symptom improvement in patients with LBP[33,34] and this is one of the reasons that therapists choose this therapy. Therefore it is important to focus assessment on short-term outcomes. The primary outcomes will be:
Usual pain intensity over last 24 hours recorded each morning in a pain diary over the first week. Pain will be measured on a 0�10 numerical rating scale (NRS). The unit of analysis will be the mean of the 7 measures[35];
Usual pain intensity over last 24 hours (0�10 NRS) recorded at 1 and 3 weeks[35];
Global perceived effect (0�10 GPE) recorded at 3 weeks.
The secondary outcomes will be:
Global perceived effect (0�10 GPE) recorded at 1 week;
Patient-generated measure of disability (Patient-Specific Functional Scale; PSFS) recorded at 1 and 3 weeks[36];
Condition-specific measure of disability (Roland Morris Questionnaire; RMQ) recorded at 1 and 3 weeks[37];
Number of patients reporting persistent back pain at 3 months.
Following the screening consultation in which the inclusion and exclusion criteria are assessed, the GP will supervise the baseline measurement of pain. All patients will then receive an assessment booklet and a pre-paid envelope in which all other self-assessed outcome measures are to be recorded and sealed. One member of the research team will contact patients by telephone within 24 hours of the consultation with the GP in order to give explanations regarding the appropriate form of filling in the assessment booklet. At this time, other baseline outcomes will be recorded and then the patient will be randomised to study groups. The patient will be advised to keep the booklet at home, to seal it into the pre-paid envelope after the final assessment and mail the sealed envelope to the research team. To ensure the proper use of the assessment booklet and to avoid loss of data due to non-returned booklets, a blinded assessor will contact all patients by telephone 9 and 22 days after the consultation with the GP to collect patient’s answers from the 1st week and 3rd week assessments, respectively.
The procedure for obtaining outcome data will be followed for all participants, regardless of compliance with trial protocols. At 3 months, data regarding the presence of persistent (chronic) symptoms will be collected by telephone. Participants will be asked to answer the following yes-no question: “During the past 3 months have you ever been completely free of low back pain? By this I mean no low back pain at all and would this pain-free period have lasted for a whole month”. Those answering no will be considered to have persistent LBP. Information on additional treatment and the direct costs with low back pain management will also be collected at 3 months.
A secondary analysis will be performed on predictors of response to McKenzie treatment and prediction of chronicity. This will involve the measurement of participants’ expectation about the helpfulness of both treatments under investigation as well as information on the occurrence of the centralisation phenomenon. Expectation will be recorded prior to randomisation according to the procedures described by Kalauokalani et al[38].
Treatments
All participants will receive GP care as advocated by the NHMRC guideline for the management of acute musculoskeletal pain[2]. Guideline-based GP care consists of providing information on a favourable prognosis of acute LBP and advising patients to stay active, together with the prescription of paracetamol. Patients randomised to the experimental group will be referred to physiotherapy to receive the McKenzie Method. A research assistant not involved in the assessment or treatment of subjects will be responsible for the randomisation process and will contact therapists and patients to arrange the first physiotherapy session. The McKenzie treatment will be delivered by credentialed physiotherapists who will follow the treatment principles described in McKenzie’s text book[18]. All therapists will have completed the four basic courses taught by the McKenzie Institute International. To ensure the appropriate implementation of the McKenzie’s classification algorithm, a training session with a member of McKenzie’s educational program will be conducted prior to the commencement of the study. The treatment frequency will be at the discretion of the therapist with a maximum of 7 sessions over 3 weeks. We chose to restrict the McKenzie treatment to a maximum of 7 sessions based on the study of Werneke and colleagues[39], which concluded that further reductions in pain and function are not expected if favourable changes in pain location are not present until the seventh treatment visit. Treatment procedures from the McKenzie Method are summarised in the Appendix.
Participants randomised to the control group will continue their GP care as usual. All participants regardless of intervention group will be advised not to seek other treatments for their low back pain during the treatment period. Physiotherapists will be asked to withhold co-interventions during the course of the trial.
Several mechanisms will be used to ensure that the trial protocol is applied consistently. Protocol manuals will be developed and all involved researchers (GPs, physiotherapists, assessor, and statistician) will be trained to ensure that screening, assessment, random allocation and treatment procedures are conducted according to the protocol. A random sample of treatment sessions will be audited to check that treatment is being administered according to the protocol.
Data Analysis
Power was calculated based on the primary outcome measures (pain intensity and global perceived effect). A sample size of 148 participants will provide 80% power to detect a difference of 1 unit (15%) on a 0�10 pain scale (SD = 2.0) between the experimental and control groups, assuming alpha of 0.05. This allows for loss to follow-up of 15%. This sample size also allows the detection of a difference of 1.2 units (12%) on a 0�10 global perceived effect scale (SD = 2.4).
Data will be analysed by a research member blinded to group status. The primary analysis will be by intention-to-treat. In order to estimate treatment effects, between-group mean differences (95%CI) will be calculated for all outcome measures. In the primary analysis these will be calculated using linear models that include baseline values of outcome variables as covariates to maximise precision.
Discussion
We have presented the rationale and design of an RCT evaluating the effects of the McKenzie Method in the treatment of acute non-specific LBP. The results of this trial will be presented as soon as they are available.
Competing Interests
The author(s) declare that they have no competing interests.
Authors’ Contributions
LACM, CGM and RDH were responsible for the design of the study. HC was responsible for recruiting McKenzie therapists and she will also participate as a clinician in the trial. LACM and JMc will act as trial coordinators. All authors have read and approved the final manuscript.
Appendix
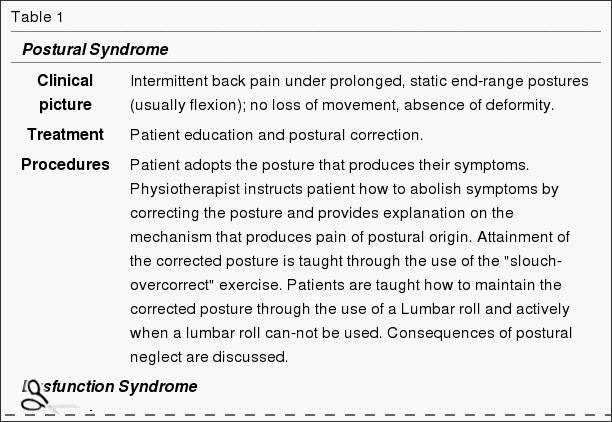
Clinical picture and treatment principles according to the McKenzie Method
This table summarises the procedures involved in the McKenzie Method (Table 1). For detailed description of all procedures and progressions, refer to McKenzie’s text book. This is particularly important for Derangement syndrome since the treatment is extremely variable and complex and the full description of procedures would not be appropriate for the purposes of this paper.
The authors thank the physiotherapists credentialed in the McKenzie Method for their participation in this project.
Managing Low Back Pain: Attitudes & Treatment Preferences of Physical Therapists & Chiropractors
Abstract
Background and Purpose:�Researchers surveyed physical therapists about their attitudes, beliefs, and treatment preferences in caring for patients with different types of low back pain problems.
Subjects and Methods: Questionnaires were mailed to all 71 therapists employed by a large health maintenance organization in western Washington and to a random sample of 331 other therapists licensed in the state of Washington.
Results: Responses were received from 293 (74%) of the therapists surveyed, and 186 of these claimed to be practicing in settings in which they treat patients who have back pain. Back pain was estimated to account for 45% of patient visits. The McKenzie method was deemed the most useful approach for managing patients with back pain, and education in body mechanics, stretching, strengthening exercises, and aerobic exercises were among the most common treatment preferences. There were significant variations among therapists in private practice, hospital-operated, and health maintenance organization settings with respect to treatment preferences, willingness to take advantage of the placebo effect, and mean number of visits for patients with back pain.
Conclusions and Discussion: These variations emphasize the need for more outcomes research to identify the most effective treatment approaches and to guide clinical practice.
In conclusion,�the effective treatment of acute low back pain is essential because it can potentially help prevent the development of chronic low back pain. A growing number of chiropractors and physical therapists, including other healthcare professionals, have utilized the McKenzie method to help manage acute non-specific low back pain in patients. According to the research study, further evidence is required to support the use of the McKenzie method for LBP, however, the outcome measures of the research study regarding the effectiveness of the McKenzie method for low back pain are promising. Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Sciatica
Sciatica is referred to as a collection of symptoms rather than a single type of injury or condition. The symptoms are characterized as radiating pain, numbness and tingling sensations from the sciatic nerve in the lower back, down the buttocks and thighs and through one or both legs and into the feet. Sciatica is commonly the result of irritation, inflammation or compression of the largest nerve in the human body, generally due to a herniated disc or bone spur.
Australian Institute of Health and Welfare . Australia’s health 2004. 1st. Camberra , AIHW; 2004.
Australian Acute Musculoskeletal Pain Guidelines Group Evidence-based management of acute musculoskeletal pain. . 2003. http://www.nhmrc.gov.au
Maetzel A, Li L. The economic burden of low back pain: a review of studies published between 1996 and 2001. Best Pract Res Clin Rheumatol. 2002;16:23�30. doi: 10.1053/berh.2001.0204. [PubMed][Cross Ref]
WorkCover Authority NSW . Statistical Bulletin. NSW Workers Compensation 2002/03. Sydney , The WorkCover Authority NSW ; 2003.
Pengel LH, Herbert RD, Maher CG, Kathryn RM. Acute low back pain: Systematic review of its prognosis. BMJ. 2003;327:1�5. [PMC free article][PubMed]
Thomas E, Silman AJ, Croft PR, Papageorgiou AC, Jayson M, Macfarlane GJ. Predicting who develops chronic low back pain in primary care: a prospective study. BMJ. 1999;318:1662�1667. [PMC free article][PubMed]
Guzm�n J, Esmail R, Karjalainen K, Malmivaara A, Irvin E, Bombardier C. Multidisciplinary rehabilitation for chronic low back pain: systematic review. BMJ. 2001;322:1511�1516. doi: 10.1136/bmj.322.7301.1511. [PMC free article][PubMed][Cross Ref]
van Tulder M, Malmivaara A, Esmail R, Koes B. Exercise therapy for low back pain. A systematic review within the framework of the Cochrane Collaboration Back Review Group. Spine. 2000;25:2784�2796. doi: 10.1097/00007632-200011010-00011. [PubMed][Cross Ref]
van Tulder M, Ostelo R, Vlaeyen JWS, Linton SJ, Morley SJ, Assendelft WJJ. Behavioral treatment for chronic low back pain. A systematic review within the framework of the Cochrane Back Review Group. Spine. 2000;25:2688�2699. doi: 10.1097/00007632-200010150-00024. [PubMed][Cross Ref]
Jellema P, van Tulder MW, van Poppel MN, Nachemson AL, Bouter LM. Lumbar supports for prevention and treatment of low back pain. A systematic review within the framework of the Cochrane Back Review Group. Spine. 2001;26:377�386. doi: 10.1097/00007632-200102150-00014. [PubMed][Cross Ref]
Ferreira ML, Ferreira PH, Latimer J, Herbert RD, Maher CG. Does spinal manipulative therapy help people with chronic low back pain? Aust J Physiother. 2002;48:277�284. [PubMed]
Pengel HM, Maher CG, Refshauge KM. Systematic review of conservative interventions for subacute low back pain. Clin Rehabil. 2002;16:811�820. doi: 10.1191/0269215502cr562oa. [PubMed][Cross Ref]
Koes BW, van Tulder MW, Ostelo R, Burton K, Waddell G. Clinical guidelines for the management of low back pain in primary care: an international comparison. Spine. 2001;26:2504�2514. doi: 10.1097/00007632-200111150-00022. [PubMed][Cross Ref]
Borkan J, Koes B, Reis S, Cherkin DC. A report from the Second International Forum for Primary Care Research on low back pain: reexamining priorities. Spine. 1998;23:1992�1996. doi: 10.1097/00007632-199809150-00016. [PubMed][Cross Ref]
Bouter LM, van Tulder MW, Koes BW. Methodologic issues in low back pain research in primary care. Spine. 1998;23:2014�2020. doi: 10.1097/00007632-199809150-00019. [PubMed][Cross Ref]
Leboeuf-Yde C, Lauritsen JM, Lauritzen T. Why has the search for causes of low back pain largely been nonconclusive? Spine. 1997;22:877�881. doi: 10.1097/00007632-199704150-00010. [PubMed][Cross Ref]
Fritz JM, Delitto A, Erhard RE. Comparison of classification-based physical therapy with therapy based on clinical practice guidelines for patients with acute low back pain. Spine. 2003;28:1363�1372. doi: 10.1097/00007632-200307010-00003. [PubMed][Cross Ref]
McKenzie R, May S. The lumbar spine. Mechanical diagnosis & therapy. 2nd. Vol. 1. Waikanae , Spinal Publications New Zealand Ltd; 2003. p. 374.
van Dillen LR, Sahrmann SA, Norton BJ, Caldwell CA, McDonnell MK, Bloom NJ. Movement system impairment-based categories for low back pain: stage 1 validation. J Orthop Sports Phys Ther. 2003;33:126�142. [PubMed]
BenDebba M, Torgerson WS, Long DM. A validated, practical classification procedure for many persistent low back pain patients. Pain. 2000;87:89�97. doi: 10.1016/S0304-3959(00)00278-5. [PubMed][Cross Ref]
Delitto A, Erhard RE, Bowling RW, DeRosa CP, Greathouse DG. A treatment-based classification approach to low back syndrome: identifying and staging patients for conservative treatment. Phys Ther. 1995;75:470�485. [PubMed]
Klapow JC, Slater MA, Patterson TL, Doctor JN, Atkinson JH, Garfin SR. An empirical evaluation of multidimensional clinical outcome in chronic low back pain patients. Pain. 1993;55:107�118. doi: 10.1016/0304-3959(93)90190-Z. [PubMed][Cross Ref]
Laslett M, van Wijmen P. Low back and referred pain: diagnosis and proposed new system of classification. N Z J Physiother. 1999;27:5�14.
Maluf KS, Sahrmann SA, van Dillen LR. Use of a classification system to guide nonsurgical management of a patient with chronic low back pain. Phys Ther. 2000;80:1097�1111. [PubMed]
Petersen T, Laslett M, Thorsen H, Manniche C, Ekdahl C, Jacobsen S. Diagnostic classification of non-specific low back pain. A new system integrating patho-anatomic and clinical categories. Physiother Theory Pract. 2003;19:213�237.
Stiefel F, deJonge P, Huyse F, al INTERMED – An assessment and classification system for case complexity: Results in patients with low back pain. Spine. 1999;24:378�384. doi: 10.1097/00007632-199902150-00017. [PubMed][Cross Ref]
McCarthy CJ, Arnall FA, Strimpakos N, Freemont A, Oldham JA. The biopsychosocial classification of non-specific low back pain: a systematic review. Phys Ther Rev. 2004;9:17�30. doi: 10.1179/108331904225003955. [Cross Ref]
Batti� MC, Cherkin DC, Dunn R, Ciol MA, Wheeler KJ. Managing low back pain: attitudes and treatment preferences of physical therapists. Phys Ther. 1994;74:219�226. [PubMed]
Li LC, Bombardier C. Physical therapy management of low back pain: An exploratory survey of therapist approaches. Phys Ther. 2001;81:1018�1028. [PubMed]
Machado LAC, de Souza MS, Ferreira PH, Ferreira ML. The McKenzie protocol for low back pain: a systematic review of the literature with a meta-analysis approach. Spine (in press) 2005. [PubMed]
de Vet HCWPD, Heymans MWMS, Dunn KMMP, Pope DPPD, van der Beek AJPD, Macfarlane GJPD, Bouter LMPD, Croft PRPD. Episodes of Low Back Pain: A Proposal for Uniform Definitions to Be Used in Research. Spine. 2002;27:2409�2416. doi: 10.1097/00007632-200211010-00016. [PubMed][Cross Ref]
Pocock SJ. Clinical trials. A practical approach. 1st. Chichester , John Wiley & Sons; 1984.
Delitto A, Cibulka MT, Erhard RE, Bowling RW, Tenhula JA. Evidence for use of an extension-mobilization category in acute low back syndrome: A prescriptive validation pilot study. Phys Ther. 1993;73:216�228. [PubMed]
Schenk RJ, Jozefczyk C, Kopf A. A randomized trial comparing interventions in patients with lumbar posterior derangement. J Manual Manip Ther. 2003;11:95�102.
Farrar J, Young J, LaMoreaux L, al Clinical importance of changes in chronic pain intensity measured on an 11-point numerical pain rating scale. Pain. 2001;94:149�158. doi: 10.1016/S0304-3959(01)00349-9. [PubMed][Cross Ref]
Stratford P, Gill C, Westaway M, Binkley J. Assessing disability and change on individual patients: a report of a patient specific measure. Physiother Can. 1995;47:258�263.
Roland M, Morris R. A study of the natural history of back pain. Part I: development of a reliable and sensitive measure of disability in low-back pain. Spine. 1983;8:141�144. [PubMed]
Kalauokalani D, Cherkin D, Sherman K, Koepsell T, R D. Lessons from a trial of acupuncture and massage for low back pain. Spine. 2001;26:1418�1424. doi: 10.1097/00007632-200107010-00005. [PubMed][Cross Ref]
Werneke M, Hart DL, Cook D. A descriptive study of the centralization phenomenon. A prospective analysis. Spine. 1999;24:676�683. doi: 10.1097/00007632-199904010-00012. [PubMed][Cross Ref]
Low back pain is a common complaint that generally goes away on its own, however, what should a person do if their LBP becomes chronic and/or persistent? How is an individual’s quality of life affected and how does their pain intensity impact their physical capacity? Is there any type of treatment which can help improve low back pain? Many different types of treatment options can be used to safely and effectively treat low back pain. The purpose of the following research study is to determine the influence of the McKenzie method and endurance exercises on low back pain. The article demonstrates evidence-based information on the improvement of the quality of life of patients with LBP after receiving the treatment protocol mentioned below.
Influence of Mckenzie Protocol and Two Modes of Endurance Exercises on Health-Related Quality of Life of Patients with Long-Term Mechanical Low Back Pain
Abstract
Introduction
Long-term Mechanical Low-Back Pain (LMLBP) negatively impacts on patients� physical capacity and quality of life. This study investigated the relationship between Health-Related Quality of Life (HRQoL) and pain intensity, and the influence of static and dynamic back extensors� endurance exercises on HRQoL in Nigerian patients with LMLBP treated with the McKenzie Protocol (MP).
Methods
A single-blind controlled trial involving 84 patients who received treatment thrice weekly for eight weeks was conducted. Participants were assigned to the MP Group (MPG), MP plus Static Back Endurance Exercise Group (MPSBEEG) or MP plus Dynamic Endurance Exercise Group (MPDBEEG) using permuted randomization. HRQoL and pain was assessed using the Short-Form (SF-36) questionnaire and Quadruple Visual Analogue Scale respectively.
Results
Sixty seven participants aged 51.8 � 7.35 years completed the study. A total drop-out rate of 20.2% was observed in the study. Within-group comparison across weeks 0-4, 4-8 and 0-8 of the study revealed significant differences in HRQoL scores (p < 0.05). Treatment Effect Scores (TES) across the groups were significantly different (p = 0.001). MPSBEEG and MPDBEEG were comparable in TES on General Health Perception (GHP) at week 4; and GHP and Physical Functioning at week 8 respectively (p > 0.05). However, MPDEEG had significantly higher TES in the other domains of the SF-36 (p = 0.001).
Conclusion
HRQoL in patients with LMLBP decreases with pain severity. Each of MP, static and dynamic back extensors endurance exercises significantly improved HRQoL in LMLBP. However, the addition of dynamic back extensors endurance exercise to MP led to greater improvement in HRQoL.
Keywords:Mckenzie protocol, endurance exercises, quality of life, back pain
Background
Low-Back Pain (LBP) is described as the constellation of symptoms of pain or discomfort originating from impairments in the structures in the low back [1�2]. LBP is one of the most common ailments afflicting mankind [3]. It is a complicated condition which affects the physiological and psychosocial aspects of the patient [4, 5]. Epidemiological reports indicate that 70 to 85% of all people have LBP at some time in their life [1, 6]. The World Health Organization predicted that the greatest increases in LBP prevalence in the next decade will be in developing nations [7]. In line with this, a systematic review by Louw et al [8] concluded that the global burden and prevalence of LBP among Africans is rising.
It is estimated that 80-90% of patients with LBP will recover within six weeks, regardless of treatment [9]. However, 5-15% of all people that have LBP will develop long-term LBP (i.e. LBP of 12 weeks and longer) [10, 11]. The patient subgroup with long-term LBP accounts for 75-90% of the socioeconomic cost of LBP [12] and over 30% of these patients with long-term LBP seek healthcare for their back complaints. Long-term LBP significantly impacts on patients� physical [13], psychological and social functioning [14] and can affect well-being and quality of life [15]. Reduced quality of life in patients with long-term LBP is associated with poor prognosis [16], intermittent or recurrent episodes of LBP [17], disability [18] and psychosocial dysfunction [19, 20].
Assessment of Health-Related Quality of Life (HRQoL) in relation to LBP has been recommended in LBP management [21, 22]. Several HRQoL instruments have been developed to assess self-perceived general health status [21, 22]. The SF-36 Health Status Questionnaire, though a generic instrument, has been recommended in the assessment of HRQoL of patients with long-term LBP [22] and it assesses eight domains such as physical functioning, role limitations due to physical problems, bodily pain, general health perceptions, vitality, social functioning, role limitation due to emotional problems and general mental health [23, 24].
Consequent to the foregoing, treatment intervention that may help improve the HRQoL of patients with long-term LBP has been advocated. Although, physiotherapy plays an important role in the management of patients with LBP, the traditional approach based on biomedical model, which is centered on the treatment of impairments and patho-physiological variables, may not fully addressed the wider range of factors including psychosocial impairments associated with long-term LBP [25, 26]. However, long-term LBP is considered to be a multi-factorial bio-psychosocial problem which has an impact on both social life [27, 28] and quality of life [29] and thus requires a multi-dimensional approach based on a bio-psychosocial model (a model that includes physical, psychological and social elements) in its assessment and treatment [30, 31].
Based on empirical recommendations from research, recent decades have witnessed tremendous advances in preventive, pharmacological and physiotherapy management for a limited number of patients with LBP especially in developed countries. However, the improvement in health outcomes observed in most Western countries over the past few decades has not been achieved in Africa [32] and therefore, the health of Africans is of global concern [8]. Compared with Australians [33], Europeans [34] and North Americans [35], the use of exercise as medicine in Africans is poor. Exercise is the central element in the physical therapy management of patients with long-term LBP [9, 36]. Exercise often does not require expensive instruments and probably the cheapest intervention and one in which the patient has some measure of direct control [37]. Nonetheless, it remains inconclusive which exercise regimen will significantly influence the quality of life of patients with long-term LBP. The McKenzie Protocol (MP) is one of the most commonly used physical therapy interventions in long-term mechanical LBP with documented effectiveness [38�41]. However, there is a dearth of studies that have investigated the influence of the MP on HRQoL in patients with long-term mechanical LBP. Therefore, this study was intended to answer the following questions: (1). Will pain intensity significantly influence HRQoL? (2) Will static and dynamic back extensors� endurance exercises significantly influence HRQoL in Nigerian patients with long-term mechanical LBP (LMLBP) treated with the MP?
Methods
Eighty four patients with LMLBP participated in this single-blind randomized trial. The participants were consecutively recruited from the physiotherapy department, Obafemi Awolowo University (OAU) Teaching Hospitals Complex and the OAU Health Centre, Ile-Ife, Nigeria. The McKenzie Institute’s Lumbar Spine Assessment Format (MILSAF) [3] was used to determine eligibility to participate in the study. Based on the MILSAF, patients who demonstrated Directional Preference (DP) for extension only were recruited to ensure homogeneity of samples. DP is described as the posture or movement that reduces or centralizes radiating pain that emanates from the spine. Exclusion criteria were red flags indicative of serious spinal pathology with signs and symptoms of nerve root compromise (with at least two of dermatomal sensory loss, myotomal muscle weakness and reduced lower limb reflexes), individuals with any obvious spinal deformity or neurological disease; pregnancy; previous spinal surgery; previous experience of static and dynamic endurance exercise and having DP for flexion, lateral or no DP. Long-term low-back pain was defined as a history of LBP of not less than 3 months [42].
Based on the sample size table by Cohen [43] with alpha level set at 0.05, degree of freedom at 2, effect size at 0.25, and power at 80, the study found a minimum sample size of 52. However, in order to accommodate for possible attrition or loss during the study, a total of 75 patients (25 per group) was included. The participants were randomly assigned to one of three treatment groups using permuted block randomization; the McKenzie Protocol (MP) Group (MPG) (n = 29), MP plus Static Back Endurance Exercise Group (MPSBEEG) (n = 27) and MP plus Dynamic Back Endurance Exercise Group (MPDBEEG) (n = 28). Sixty seven (32 males (47.8%) and 35 females (52.2%) participants completed the eight week study. Twenty five participants completed the study in MPG, 22 in MPSBEEG and 20 in MPDBEEG. A total drop-out rate of 20.2% was observed in the study. Fourteen percent of participants in MPG were lost to follow-up. Nineteen percent of the participants in MPSBEEG dropped out (out of these, 40% were lost to follow-up while 60% absconded due to improvement in their health condition). In the MPDBEEG, 28.6% of the participants dropped out (37.5% were lost to follow-up while 62.5% absconded due to improvement in their health condition).
Treatment was given thrice weekly for eight weeks and outcomes were assessed at the end of the fourth and eighth week of study. Ethics and Research Committee of the Obafemi Awolowo University Teaching Hospitals Complex and the joint University of Ibadan /University College Hospital Institutional Review Committee respectively gave approval for the study.
Instruments
A height meter calibrated from 0-200cm was used to measure the height of each participant to the nearest 0.1cm. A weighing scale was used to measure the body weight of participants in kilograms to the nearest 1.0Kg. It is calibrated from 0 – 120kg. A metronome (Wittner Metronom system Maelzel, Made in Germany) was used to set a uniform tempo for dynamic back endurance muscles endurance test, which involves repeated contraction or movements over a period of time performed synchronously to the metronome beat. Patients lay on a plinth for the MP, static and dynamic back endurance exercise respectively.
General Health Status Questionnaire – Short Form -36 (SF-36) was used to assess the quality of life of the participants. The SF-36 has been recommended in the assessment of patients with long-term LBP [24, 44, 45]. A Yoruba translated version of the Health Status Questionnaire (SF-36) was used for participants who were literate in the Yoruba language and preferred the Yoruba version. The translation was done at the department of linguistics and African languages of Obafemi Awolowo University, Ile Ife. Pearson product moment correlation coefficient (r) of 0.84 was obtained for the criterion validity of the back translation of the Yoruba version. Quadruple Visual Analogue Scale (QVAS) was used to assess pain intensity of participants. QVAS is a reliable and valid method for pain measurement [46, 47]. A Yoruba translated version of the QVAS was used for participants who were literate in the Yoruba language and prefers the Yoruba version. The translation was done at the department of linguistics and African languages of Obafemi Awolowo University, Ile Ife. Pearson product moment correlation coefficient (r) of 0.88 was obtained for the criterion validity of the back translation of the Yoruba version.
Treatment
Treatment for the different groups (MPG, MPSBEEG and MPDBEEG) comprised three phases including warm up, main exercise and cool down. Prior to treatment, the participants were instructed in details on the study procedures. This was followed by a low intensity warm-up phase of five minutes duration comprising active stretching of the upper extremities and low back and strolling at self-determined pace around the research venue. Treatment also ended with a cool-down phase comprising of the same low intensity exercise as the warm-up for about five minutes.
The McKenzie Protocol (MP) involved a course of specific lumbosacral repeated movements in extension that cause the symptoms to centralize, decrease or abolish. The determination of the direction preference for extension was followed by the main MP activities including �Extension lying prone�, �Extension In Prone� and �Extension in standing�. The MP also included a set of back care education instructions which comprised a 9 item instructional guide on standing, sitting, lifting and other activities of daily living for home exercise for all the participants (Appendix).
In addition to completing the MP (i.e., back extension exercises plus the back care education), static back extensors endurance exercise which included five different static exercises differentiated by the alteration of the positions of the upper and lower limbs with the patient in prone lying on a plinth was carried out [48]. The participants began the exercise training programme with the first exercise position, but progressed to the next exercises at their own pace when they could hold a given position for 10 seconds. On reaching the fifth progression, they continued with the fifth progression until the end of the exercise programme [48, 49]. The following were the five exercise progressions:
Participant lay in prone position with both arms by the sides of the body and lifting the head and trunk off the plinth from neutral to extension;
Participant lay in prone position with the hands interlocked at the occiput so that shoulders were abducted to 90� and the elbows flexed, and lifting the head and trunk off the plinth from neutral to extension;
Participant lay in prone position with both arms elevated forwards, and lifting the head, trunk and elevated arms off the plinth from neutral to extension;
Participant lay in prone position and lifting the head, trunk and contralateral arm and leg off the plinth from neutral to extension; and
Participant lay in prone position with both shoulders abducted and elbows flexed to 90�, and lifting the head, trunk and both legs (with knees extended) off the plinth.
If pain was aggravated during the exercise, the participant was asked to stop. If the pain diminished within 5 minutes after the exercise, he/she was asked to continue the exercise but to hold the exercise position for only 5 seconds. The participant was asked to progress to 10 seconds if there was no adverse response. Each exercise was repeated 9 times. After 10 repetitions, the participant was instructed to rest for between 30 seconds to 1 minute. Static holding time in the exercise position was gradually increased to 20 seconds to provide a greater training stimulus [50, 51]. The dosage of series of 10 repetitions was adopted from a previous protocol for participants with sub-acute LBP [52].
In addition to completing the MP, dynamic back extensors endurance exercise which included five different isokinetic exercises differentiated by the alteration of the positions of the upper and lower limbs with the patient in prone lying on a plinth was carried out. The dynamic back endurance exercise was an exact replica of the static back extensors endurance exercise protocol in terms of exercise positions, progressions and duration. However, instead of static posturing of the trunk in the prone lying position and holding the positions of the upper and lower limbs suspended in the air during all the five exercise progressions for the 10 seconds, the participant was asked to move the trunk and the suspended limbs 10 times.
If pain was aggravated during the exercise, participant was asked to stop. If the pain diminished within 5 minutes after the exercise, the participant was asked to continue the exercise but to carry out only 5 movements in the exercise position. The participant was asked to progress to 10 movements if there is no adverse response. Each exercise was repeated 9 times. After 10 repetitions, the participants were instructed to rest for between 30 seconds to 1 minute. The number of movements of the trunk in the exercise position was gradually increased to 20 seconds to provide a greater training stimulus.
In order to achieve adequate training effect based on recommendation of previous studies, a 30 to 45 minute exercise duration, thrice weekly and eight weeks exercise; and training load of 10 seconds static hold or 10 repetitions per exercise position was adopted [53, 54].
The researchers (CEM and OA) were credentialed in the McKenzie method and supervised the exercises. The researchers were blinded to the recruitment, randomization and assessment procedures which were carried out by an assistant who was blinded to the treatment protocols of the different groups. The research assistant was also credentialed in McKenzie method. The questionnaires used in this study were self- administered.
Data Analysis
Data were analyzed using descriptive of mean and standard deviation; and inferential statistics. One-way ANOVA was used to compare the participants� general characteristics and pain intensity by treatment groups. Pearson’s Product Moment Correlation Analysis was used to test the relationship between HRQoL and intensity of pain. The Kruskal Wallis test was used to compare the treatment outcomes (mean change) on HRQoL across group at week four and eight of the study respectively. Friedman’s ANOVA and Wilcoxon signed ranked tests for multiple comparisons were used to compare within group changes in across the three study time points Alpha level was set at p = 0.05. The data analyses were carried out using SPSS 13.0 version software (SPSS Inc., Chicago, Illinois, USA).
Dr. Alex Jimenez’s Insight
How can the McKenzie method improve an individual’s quality of life? With years of experience working alongside patients to help them recover from a variety of spinal health issues, I’ve seen how debilitating low back pain can be if left untreated for an increased amount of time. Although spinal adjustments and manual manipulations can efficiently help improve symptoms of low back pain, other alternative treatment options may help patients recover faster. The McKenzie method and endurance exercises are used by many healthcare professionals to safely and effectively rehabilitate patients with LBP. The results of the research study ultimately demonstrate how the treatment protocol can help improve an individual’s quality of life.
Results
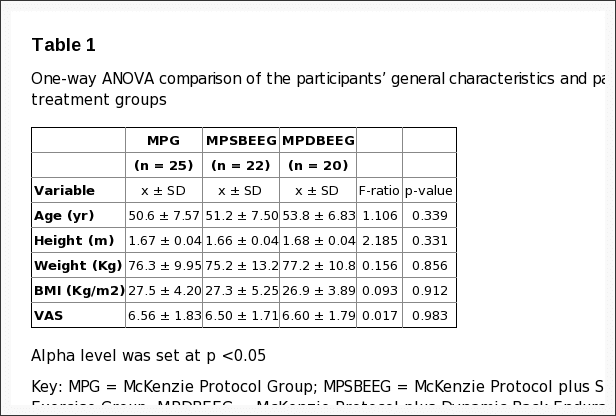
The mean age, height, weight and BMI of all the participants was 51.8 � 7.35 years, 1.66 � 0.04m, 76.2�11.2 Kg and 27.2 � 4.43 kg/m2 respectively. Comparison of the participants� general characteristics by treatment groups revealed that the participants in the different groups were comparable in their general characteristics (p > 0.05) (Table 1).
Table 1: One-way ANOVA comparison of the participants� general characteristics and pain intensity by treatment groups
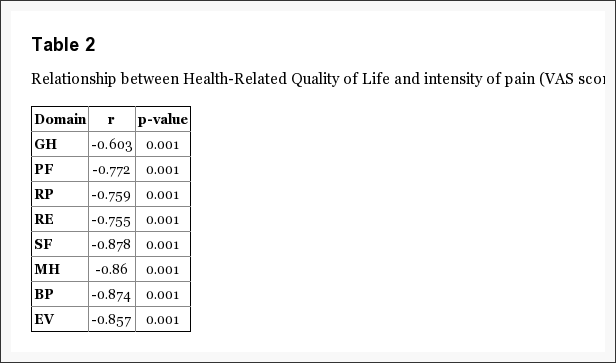
The mean pain intensity score (VAS) reported by the participants was 6.55 � 1.75. The relationship between each of the eight domains of HRQoL and intensity of pain (VAS score) is presented in Table 2.
Table 2: Relationship between Health-Related Quality of Life and intensity of pain (VAS score) (n = 67)
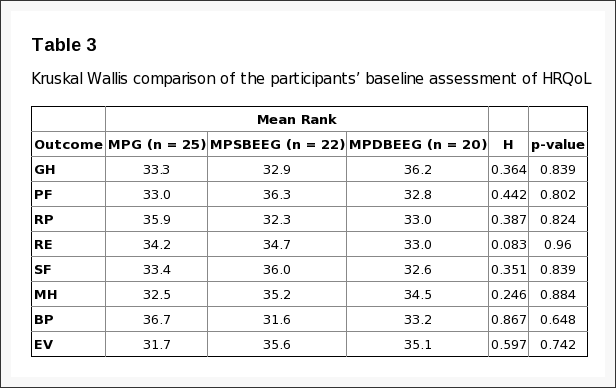
From the result, correlation co-efficient (r) ranged between-0.603 to-0.878 at p = 0.001. Table 3 shows the comparison of the participants� baseline measure of HRQoL.
Table 3: Kruskal Wallis comparison of the participants� baseline assessment of HRQoL
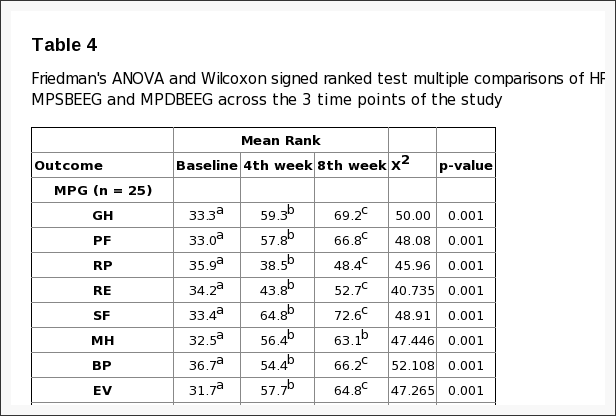
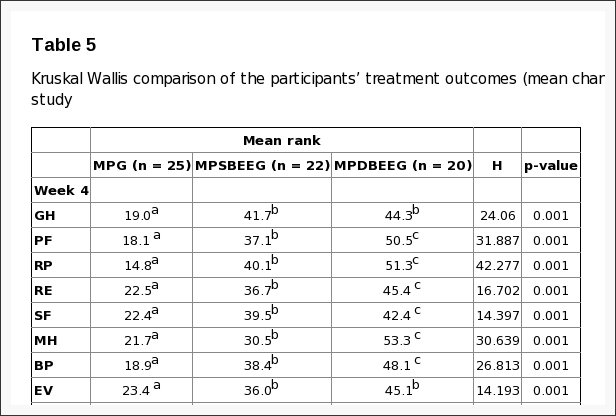
The results indicate that the participants in the different treatment groups were comparable in all the domains of HRQoL (p > 0.05). Within-group comparison of HRQoL in MPG, MPSBEEG and MPDBEEG across the 3 time points (weeks 0-4, 4-8 and 0-8) of the study showed that there were significant improvements (p < 0.05) (Table 4). Comparison of treatment outcomes (mean change score (MCS)) at week four and eight of the study are presented in Table 5. There were significant differences in SF-36 scores across the group (p > 0.05) at the end of the 4th and 8th week of the study respectively. The Tukey multiple comparisons post-hoc analysis was used to elucidate where the differences within between groups lie. The result indicated that MPSBEEG and MPDBEEG had significantly higher MCS on all domains of SF-36 compared with MPG at week four and eight respectively (p < 0.05). There was no significant difference between the MPSBEEG and MPDBEEG in the MCS of General Health Perception domain of SF-36 at week four; and on General Health Perception and Physical Functioning Domains of SF-36 at week eight respectively. However, MPDBEE had significantly higher treatment effects on other domains of HRQoL (p = 0.001).
Table 4: Friedman’s ANOVA and Wilcoxon signed ranked test multiple comparisons of HRQoL among MPG, MPSBEEG and MPDBEEG across the 3 time points of the study.
Table 5: Kruskal Wallis comparison of the participants� treatment outcomes (mean change) at week four of the study.
Discussion
This study evaluated the relationship between HRQoL and pain intensity, and the influence of static and dynamic back extensors� endurance exercises on HRQoL in Nigerian patients with LMLBP treated with the MP. The mean age of the patients in this study was 51.8 � 7.35 years. This age falls within the age bracket during which LBP is reported to be a more common problem [55]. From the result of this study, no significant difference in physical characteristics and pain intensity was found in the different treatment groups at baseline. Baseline characteristics are believed to be predictors of response to treatment in clinical trials for LBP [56]. Comparability in baseline measure in clinical trials is reported to reduce the chances of co-founders other than the intervention in predicting outcomes. Therefore, it is implied that the results obtained at different point in the course of this study could have been largely due to the effects of the various treatment regimens.
This study investigated the relationship between HRQoL and the intensity of pain. From the result, significant moderate to high inverse relationships were found between pain intensity and the different domains of HRQoL. General health perception showed the least correlation (r = -0.603; p = 0.001) while social functioning had the highest correlation with pain intensity (r = -0.878; p = 0.001). It is inferred from the study’s result that HRQoL of patients with long-term LBP decreases with severity of pain. Previous studies have reported an association between LBP and psychosocial factors [26, 57]. Specifically, significant inverse correlation has been reported between severity of pain and quality of life in patients with chronic LBP [57�59]. Pain is believed to have a profound effect on HRQoL [59] and the degree, to which the patients believe that they are disabled by it, is a powerful factor in the extent of their quality of life impairments [60]. Therefore, quality of life is an indicator of the level of endurance of people to pain [61].
Within-group comparison of each of MP, MP plus Static Back Endurance Exercise (MPSBEE) and MP plus Dynamic Back Endurance Exercise (MPDBEE) across the 3 time-points (weeks 0-4, 4-8 and 0-8) of the study revealed that each treatment regimen led to significant improvement in HRQoL. Patients in this study displayed baseline values of the SF-36 comparable to those described in other studies on chronic LBP [62]. The baseline values of all domains of the SF-36 observed in this study were lower than those of adult normative data reported by Jenkinson et al [63] leaving room for any improvement accruable to treatment regimens to be assessed. From this study, all the eight domains of the SF-36 significantly improved at the 4th and 8th week assessment. However, on the final assessment, social functioning, general health perception and bodily pain improved more than the other domains of SF-36 in the MPG. General health perception, physical functioning, social functioning, bodily pain and energy vitality improved more than the other domains of SF-36 in the MPSBEEG while general health perception, physical functioning, social functioning, bodily pain and energy vitality improved more than the other domains of SF-36 in the MPDBEEG. Role physical, role emotional and mental health were the least improved domains of the SF-36 among the treatment groups. Though significant improvements were observed in the different domains by treatment groups on final assessment, the values were still lower than the adult normative data for general health status assessed using the SF-36 questionnaire [63]. A previous study by Smeets and colleagues [64] found that active physical therapy regimen primarily designed to improve physiological aspects of LBP such as aerobic fitness level, low back muscle strength and endurance can also reduce the impact of psychosocial factors that it did not deliberately target. In view of current evidence, Hill and Fritz [57] suggest that it may not necessarily follow that a psychologist is better placed to improve treatment outcomes than a physical therapist, even when a goal of treatment is the mediation of a psychosocial factor. Hill and Fritz [57] also argue that psychosocial factors including fear of movement, anxiety, a faulty coping strategy and quality of life have a strong influence on the success of treatment for patients with back pain at a group level. Literature suggests that exercise generally has a potential benefit on psychosocial aspect of patient with long-term LBP. Long-term LBP leads to deconditioning [65] and many problems associated with deconditioning are believed to be reversible through general and specific exercise regimens [66]. Harding and Watson [66] note that improvement in overall physical function is linked with improvement in psychosocial function. Unfortunately, there is a dearth of studies on the effect of the MP and back extensors endurance exercises on HRQoL in patients with long-term mechanical LBP.
From the result of this study, comparison of the different treatment regimens indicate that MPSBEE and MPDBEE had significantly higher treatment effect on all domains of HRQoL compared with MP at week four and eight respectively. MPSBEE and MPDBEE were comparable in their effect on general health perception domain at week four; and on health perception and physical functioning domains of the HRQoL at week eight. However, MPDBEE had significantly higher treatment effects on other domains of HRQoL. Generally, exercise seems to leads to improved wellness and quality of life. Still, there does not appear to be a consensus of opinion on the most effective programme designed to maintain exercise benefits. The McKenzie method is a popular and promising classification-based treatment for LBP among physical therapists [3] in addition to delivering theoretical information in order to educate patients about their condition, so that patients are better able to understand their condition and how to change their behaviour towards an episode of LBP [67]. However, few studies have investigated the effect of the MP on HRQoL in patients with LMLBP. Udermann et al [68] found significant improvements in HRQoL measures in chronic LBP patients treated with MP but reported that the addition of resistance training for the lumbar extensors provided no additional benefit. In recent times, endurance training of the low-back extensors aimed at improving physical performance and psychosocial health in patients with LBP has increased in popularity [69, 48, 52, 70], yet their effectiveness in enhancing quality of life remains unclear [71].
The observed efficacy of the MP, MPSBEE and MPDBEE in this study could be as a result of the fact that each of the regimen contained active exercise carried out in extension positions. Active exercise can be described as functional exercise performed by the patient or client. Previous studies have shown that active exercise, irrespective of the type is more effective in the management of patients with long-term LBP than passive therapy [72, 73]. The MP utilizes a system of patient self generated force to mobilize or manipulate the spine through a series of active repeated movements or static positioning and it is based on the patient’s pain response to certain movements and postures during assessment [3]. Similarly, endurance exercises are active exercises that require static posturing or repeated movements in order to initiate overload stimuli on the musculature. The different treatment regimen in this study had movement components, either from the MP which is the baseline treatment for all the groups or from the back extensors endurance exercise protocols. It is postulated from the results of this study that the significant higher treatment outcome of MPDBEE might be due to the combined effects of movements and overload stimulus on the back extensor muscles. MPDBEE seems to contain movement ingredients, firstly, from the MP which is the baseline treatment for this group and it involved a series of active repeated movements. Secondly, the dynamic back extensors endurance exercise also involved repeated movements of the trunk and limbs in the sagittal plane. It seems that extension exercise with movement elements carried out in patterns similar to the daily tasks motions might help to improve psychosocial aspects of long-term LBP as observed in this study.
Limitations of the Study
The generalizability of the findings of this study is limited by the fact that a generic quality of life tool was employed because of the scarcity of standard HRQoL tools with documented psychometric properties specific for patients with LBP. Theoretically, specific HRQoL measures are opined to be more responsive than generic HRQL measures [74]. Like all other self-reported assessment, it is possible that the patients in this study might have given exaggerated responses or overestimated the effect of exercise on their HRQoL. Furthermore, individuals� perception of psychosocial construct such as HRQoL is believed to be influenced by subjective interpretation and cultural bias [75, 76]. The high drop-out rate observed in this study is also a potential limitation and source of bias which may limit the interpretation and generalizability of study results. Finally, the treatment outcomes of the different regimens were only measured over such a short period of time of eight weeks.
Conclusion
Health-related quality of life of patients with long-term LBP decreases with severity of pain. The McKenzie Protocol, static and dynamic back extensors endurance exercises had significant therapeutic effect on HRQoL in patients with LMLBP. However, the addition of dynamic back extensors endurance exercise to MP led to higher improvement on HRQoL. It is recommended that static or dynamic endurance exercise be combined with MP in patients with LMLBP to derive maximum improvement in general health status.
Acknowledgements
This research was funded by an African Doctoral Dissertation Research Fellowship award offered by the African Population and Health Research Center (APHRC) in partnership with the International Development Research Centre (IDRC). We would like to thank the management and clinicians of the department of physiotherapy OAUTHC, Ile-Ife, Nigeria for their support in carrying out the study. We will also like to thank all the patients who participated in this study.
Competing Interests
The authors declare no competing interests.
Authors� Contributions
All the authors have contributed in this study in ways that comply to the ICMJE authorship criteria. All the authors have read and approved the final version of the manuscript.
In conclusion,�the quality of life of patients with chronic and/or persistent low back pain improved and the pain intensity of the symptoms of LBP appeared to decrease with the use of McKenzie therapy and endurance exercises, according to the study. Furthermore, under the McKenzie treatment protocol, static and dynamic back extensor endurance exercises were recorded to significantly improve symptoms as compared to endurance exercises alone. Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Sciatica
Sciatica is referred to as a collection of symptoms rather than a single type of injury or condition. The symptoms are characterized as radiating pain, numbness and tingling sensations from the sciatic nerve in the lower back, down the buttocks and thighs and through one or both legs and into the feet. Sciatica is commonly the result of irritation, inflammation or compression of the largest nerve in the human body, generally due to a herniated disc or bone spur.
1. Waddell G. London: Churchill Livingstone; 1998. The back pain revolution.
2. Burton AK, Balague F, Cardon G, Eriksen HR, Henrotin Y, Lahad A, et al. On behalf of the COST B13 Working Group on Guidelines for Prevention in Low Back Pain. European guidelines for prevention in low back pain – November 2004. Eur Spine J. 2006;15:s136�168. [PMC free article][PubMed]
3. Mckenzie RA. Waikanae, New Zealand: Spinal Publication Limited; 1990. Treat Your Own Back. Spinal Publication. Pu.
4. Sikorski JM, Stampfer HG, Cole RM, Wheatley AE. Psychological aspects of chronic low back pain. Aust N Zeal J Surg. 1996;66(5):294�7. [PubMed]
5. Filho IT, Simmonds MJ, Protas EJ, Jones S. Back pain, physical function, and estimates of aerobic capacity: what are the relationships among methods and measures? Am J Phys Med Rehabil. 2002;81(12):913�20. [PubMed]
6. Anderson GBJ. Epidemiologic features of chronic low-back pain. Lancet. 1999;354(9178):581�585. [PubMed]
7. World Health Organization (WHO) Scientific Group on the Burden of Musculoskeletal Conditions of the Start of the New Millennium. Geneva: WHO; 2003. The burden of musculoskeletal conditions at the start of the new millennium. [PubMed]
8. Louw QA, Morris LD, Grimmer-Somers K. The prevalence of low back pain in Africa: a systematic review. BMC Musculoskelet Disord. 2007;8:105. [PMC free article][PubMed]
9. van Tulder MW, Koes BW, Bouter LM. Conservative treatment of acute and chronic nonspecific low back pain. A systematic review of randomized controlled trials of the most common interventions. Spine. 1997;22(18):2128�56. [PubMed]
10. Quittan M. Management of Back Pain. Disabil Rehabil. 2002;24(8):423�34. [PubMed]
11. Bigos SJ, McKee J, Holland JP, Holland CL, Hildebrandt J. Back pain; the uncomfortable truth-assurance and activity paradigm. Der Schmertz. 2001;15(6):430�434. [PubMed]
12. Deyo RA, Tsui-Wu YJ. Functional disability due to low-back pain: a population-based study indicating the importance of socioeconomic factors. Arthritis Rheum. 1987;30(11):1247�1253. [PubMed]
13. Coste J, Delecoeuillerie G, Cohen de Lara A, Le Parc JM, Paolaggi JB. Clinical course and prognostic factors of acute low-back pain: an inception cohort study in primary care practice. BMJ. 1994;308(6928):577�80. [PMC free article][PubMed]
14. Picavet HS, Schouten JS. Musculoskeletal pain in the Netherlands: prevalences; consequences and risk groups; the DMC 3-study. Pain. 2003;102(1-2):167�78. [PubMed]
15. Tuzun EH. Quality of life in chronic musculoskeletal pain. Best Pract Res Clin Rheumatol. 2007;21(3):567�579. [PubMed]
17. Linton SJ. A review of psychological risk factors in back and neck pain. Spine. 2000;25(9):1148�56. [PubMed]
18. Scholich SL, Hallner D, Wittenberg RH, Hasenbring MI, Rusu AC. The relationship between pain, disability, quality of life and cognitive-behavioural factors in chronic back pain. Disabil Rehabil. 2012;34(23):1993�2000. [PubMed]
19. Geisser ME, Robinson ME, Miller QL, Bade SM. Psychosocial factors and functional capacity evaluation among persons with chronic pain. J Occup Rehabil. 2003;13(4):259�76. [PubMed]
20. Lam� IE, Peters ML, Vlaeyen JW, Kleef M, Patijn J. Quality of life in chronic pain is more associated with beliefs about pain, than with pain intensity. Eur J Pain. 2005;9(1):15�24. [PubMed]
21. Deyo RA, Andersson G, Bombardier C, Cherkin DC, Keller RB, Lee CK, et al. Outcome measures for studying patients with low back pain. Spine. 1994;19(Suppl 18):2032S�6. [PubMed]
22. Bombardier C. Outcome assessments in the evaluation of treatment of spinal disorders. Spine. 2000;25(24):3100�3. [PubMed]
23. Ware JE, Snow KK, Kosinski M, Gandek B. SF-36 Health Survey – Manual and Interpretation Guide. Boston: The Health Institute; New England Medical Center. 1993;4:3.
24. Ware JE, Jr, Sherbourne CD. The MOS 36-item shortform health survey (SF-36) I. Conceptual framework and item selection. Med Care. 1992;30(6):473�483. [PubMed]
25. Main CJ, George SZ. Psychosocial Influences on Low Back Pain: Why Should You Care? Phys Ther. 2011;91(5):609�13. [PubMed]
26. Vlaeyenm JWS, Kole-Snijders AM, Boeren RG, van Eek H. Fear of movement/(re)injury in chronic low back pain and its relation to behavioral performance. Pain. 1995;62:363�372. [PubMed]
27. Gatchel RJ, Polatin PB, Mayer TG. The dominant role of psychosocial risk factors in the development of chronic low back pain disability. Spine. 1995;20(24):2702�2709. [PubMed]
28. George SZ, Joel E Bialosky, Julie M Fritz. Beliefs Acute Low Back Pain and Elevated Fear-Avoidance Physical Therapist Management of a Patient With. Phys Ther. 2004;84(6):538�549. [PubMed]
29. H�gg O, Burckhardt C, Fritzell C, Nordwall A. Quality of Life in Chronic Low Back Pain: A Comparison with Fibromyalgia and the General Population. J Muscoskel Pain. 2003;11(1):31�38.
30. Woby SR, Watson PJ, Roach NK, Urmston M. Are changes in fear-avoidance beliefs, catastrophizing, and appraisals of control, predictive of changes in chronic low back pain and disability? Eur J Pain. 2004;8(3):201�210. [PubMed]
31. Weiner BK. Spine Update – The Biopsychosocial Model and Spine Care. Spine. 2008;33(2):219�223. [PubMed]
32. Lopez A, Mathers C, Ezzati M, Jamison D, Murray J. Global and regional burden of disease and risk factors, : Systematic analysis of population health data 2001. Lancet. 2006;367(9524):1747�57. [PubMed]
33. Australian Bureau of Statistics (ABS) Canberra: ABS; 2006. Physical activity in Australia: a snapshot, 2004-05. ABS cat. no. 4835.0.55.001.
36. Hayden JA, van Tulder MW, Tomlinson G. Systematic Review: Strategies for using exercise therapy to improve outcomes in chronic low-back pain. Ann Int Med. 2005;142(9):776�785. [PubMed]
38. Cherkin DC, Deyo RA, Battla MC, Street JH, Hund M, Barlow W. A comparison of Physical therapy chiropractice manipulation or an educational booklet for the treatment of low back pain. New Eng J Med. 1998;339(15):1021�1029. [PubMed]
39. McKenzie R, May S. Mechanical diagnosis & therapy. 2nd edition. Vol. 1. Waikanae, New Zealand: Spinal Publications New Zealand Ltd.; 2003. The lumbar spine.
40. Machado LA, de Souza MS, Ferreira PH, Ferreira ML. The McKenzie method for low back pain: a systematic review of the literature with a meta-analysis approach. Spine. 2006;31:254�262. [PubMed]
41. Ayanniyi O, Lasisi OT, Adegoke BOA, Oni-Orisan MO. Management of low back pain: Attitudes and treatment preferences of physiotherapists in Nigeria. Afr J Biomed Res. 2007;10(1):41�49.
42. Mbada CE, Ayanniyi O, Ogunlade SO. Effect of static and dynamic back extensor muscles endurance exercise on pain intensity, activity limitation and participation restriction in patients with long-term mechanical low-back pain. Med Rehabil. 2011;15(3):11�20.
43. Cohen J. In Statistical Power Analyses for Behavioural Sceinces 2nd Ed Chapter 8. New Jersey: Lawrence Erlbaum Associates; 1988. The analysis of variance and covariance: Sample size tables.
44. Bronfort G, Bouter LM. Responsiveness of general health status in chronic low back pain: a comparison of the COOP charts and the SF-36. Pain. 1999;83(2):201�9. [PubMed]
45. Taylor SJ, Taylor AE, Foy MA, Fogg AJB. Responsiveness of common outcome measures for patients with low back pain. Spine. 2001;24(17):1805�1812. [PubMed]
46. Jensen MP, McFarland CA. Increasing the reliability and validity of pain intensity measurement in chronic pain patients. Pain. 1993;55(2):195�203. [PubMed]
47. Von Korff M, Deyo RA, Cherkin D, Barlow SF. Back pain in primary care: Outcomes at 1 year. Spine. 1993:55�862. [PubMed]
48. Moffroid MT, Haugh LD, Haig AJ, Henry SM, Pope MH. Endurance training of trunk extensor muscles. Phys Ther. 1993;73:10�17. [PubMed]
49. Adegoke BOA, Babatunde FO. Effect of an exercise protocol on the endurance of trunk extensor muscles: a RCT. Hong Kong Physiother J. 2007;25:2�9.
50. Petrofsky JS, Lind AR. Aging, isometric strength and endurance; and cardiovascular responses to static effort. J Appl Physiol. 1975;38(1):91�95. [PubMed]
51. Bonde-Petersen F, Mork AL, Nielsen E. Local muscle blood flow and sustained contractions of human arm and back muscles. Eur J Appl Physiol Occup Physiol. 1975;34(1):43�50. [PubMed]
52. Chok B, Lee R, Latimer J, Beng Tan S. Endurance training of the trunk extensor muscles in people with sub acute low back pain. Phys Ther. 1999;79(11):1032�1042. [PubMed]
53. Fox EL, Bowers RW, Foss ML. 4th Ed. Philadelphia: Saunders College; 1988. The physiological basis of physical education and athletics.
54. Liddle SD, Baxter GD, Gracey JH. Exercise and chronic low back pain – what works? Pain. 2004;107(1-2):176�190. [PubMed]
55. Leboeuf-Yde C, Kyvik KO. At what age does low back pain become a common problem? A study of 29;4 24 individuals aged 12-41 years. Spine. 1998;23(2):228�34. [PubMed]
56. Underwood MR, Morton V, Farrin A, UK BEAM trial team Do baseline characteristics predict response to treatment for low back pain? Secondary analysis of the UK BEAM dataset. Rheumatology. 2007;46(8):1297�1302. [PubMed]
57. Hill JC, Fritz JM. Psychosocial influences on low back pain; disability; and response to treatment. Phys Ther. 2011;91(5):712�21. [PubMed]
58. Sengul Y, Kara B, Arda MN. The relationship between health locus of control and quality of life in patients with chronic low back pain. Turk Neurosurg. 2010;20(2):180�185. [PubMed]
59. Tavafian SS, Eftekhar H, Mohammad K, Jamshidi AR, Montazeri A, Shojaeezadeh D, Ghofranipour F. Quality of Life in Women with Different Intensity of Low Back Pain. Iran J Public Health. 2005;34(2):36�39.
60. Turner JA, Jensen MP, Romano JM. Do beliefs, coping, and catastrophizing independently predict functioning in patients with chronic pain. Pain. 2000;85(1-2):115�25. [PubMed]
61. Lyons RA, Lo SV, Littlepage BNC. Comparative health status of patients with 11 common illnesses in Wales. J Epidemiol Community Health. 1994;48(4):388�390. [PMC free article][PubMed]
62. Lurie J. A review of generic health status measures in patients with low back pain. Spine. 2000;25(24):3125�9. [PubMed]
63. Jenkinson C, Coulter A, Wright L. Short form 36 (SF 36) health survey questionnaire: normative data for adults ofworking age. BMJ. 1993;306(6890):143740. [PMC free article][PubMed]
64. Smeets RJ, Vlaeyen JW, Kester AD, Knottnerus JA. Reduction of pain catastrophizing mediates the outcome of both physical and cognitive-behavioral treatment in chronic low back pain. J Pain. 2006;7:261�271. [PubMed]
65. Verbunt JA, Seelen HA, Vlaeyen JW, van de Heijden GJ, Heuts PH, Pons K, Knottnerus JA. Disuse and deconditioning in chronic low back pain: concepts and hypotheses on contributing mechanisms. Eur J Pain. 2003;7(1):9�21. [PubMed]
66. Harding VR, Watson PJ. Increasing Activity & Improving Function In Chronic Pain Management. Physiotherapy. 2000;86(12):619�630.
67. Garcia AN, Gondo FLB, Costa RA, Cyrillo FN, Silva TM, Costa LCM, Costa LOP. Effectiveness of the back school and McKenzie techniques in patients with chronic non-specific low back pain: a protocol of a randomised controlled trial. BMC Musculoskelet Disord. 2011;12:179. [PMC free article][PubMed]
68. Udermann BE, Mayer JM, Donelson RG, Graves JE, Murray SR. Combining lumbar extension training with McKenzie therapy: Effects on pain; disability; and psychosocial functioning in chronic low back pain patients. GLMJ. 2004;3(2):7�12.
69. Kovascs FM, Abraira V, Zamora J, Fernandez C. The transition from acute to subacute and chronic low back pain: A study based on determinants of quality of life and prediction of chronic disability. Spine. 2005;30:1786�1792. [PubMed]
70. Johnson OE, Adegoke BOA, Ogunlade SO. Comparison of four physiotherapy regimens in the treatment of long-term mechanical low back pain. JJPTA. 2010;13(1):9�16. [PMC free article][PubMed]
71. Shaughnessy M, Caulfield B. A pilot study to investigate the effect of lumbar stabilisation exercise training on functional ability and quality of life in patients with chronic low back pain. Int J Rehabil Res. 2004;27(4):297�301. [PubMed]
72. Kank��np�� M, Taimela S, Airaksien OJ, Hannnien O. The efficacy of active rehabilitation in chronic low back pain. Effect on pain intensity; self-experienced disability and lumbar fatigability. Spine. 1999;24(10):1034�42. [PubMed]
73. Rainville J, Hartigan C, Martinez E, Limke J, Jouve C, Finno M. Exercise as a treatment for chronic low back pain. Spine J. 2004;4(1):106�115. [PubMed]
74. Guyatt Gordon. Insights and Limitations from Health-Related Quality-of-Life Research. Gen Intern Med. 1997;12(11):720�721. [PMC free article][PubMed]
75. Kleinman A, Eisenberg L, Good B. Culture, illness and care: clinical lessons from anthropologic and cross-cultural research. Ann Intern Med. 1978;88:251�258. [PubMed]
76. Carr AJ, Higginson IJ. Are quality of life measures patient centred? BMJ. 2001;322(7298):1357�1360. [PMC free article][PubMed]
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine



 Please Recommend Us: If you have enjoyed this video and/or we have helped you in any way please feel free to recommend us. Thank You.
Please Recommend Us: If you have enjoyed this video and/or we have helped you in any way please feel free to recommend us. Thank You.