The human body has numerous musculoskeletal muscles that allow the host to do various movements without pain or discomfort. Each muscle group has tendons, muscles, ligaments, and connective tissues surrounding the skeletal joint and protecting the skeletal structure. Each muscle group in the body allows different functions, from turning the neck from side to side to enabling the legs to provide motion when walking. Now naturally, the body ages over time, which can lead to muscle weakness in the muscle groups and affect the connective tissues, or various disruptors can develop in a healthy body that can also affect the muscles and connective tissues. Fortunately, the multiple muscle groups and connective tissues are affected by overlapping risk profiles. In that case, there are many treatments and techniques that many pain specialists utilize to restore the body and relieve pain-like symptoms associated with musculoskeletal disorders. Today’s article examines connective tissues, how conditions can affect the connective tissues, and how the MET technique stretches or strengthens the body’s connective tissue. We provide information about our patients to certified medical providers that offer available therapy techniques like MET (muscle energy techniques) for individuals dealing with chronic conditions associated with disorders affecting the body’s connective tissues that can correlate and develop with overlapping pain profiles. We encourage each patient appropriately by referring them to our associated medical providers based on their diagnosis results. We accept that education is a spectacular way when asking our providers the most crucial questions at the patient’s acknowledgment. Dr. Alex Jimenez, D.C., assesses this information as an educational service. Disclaimer
What Are Connective Tissues?
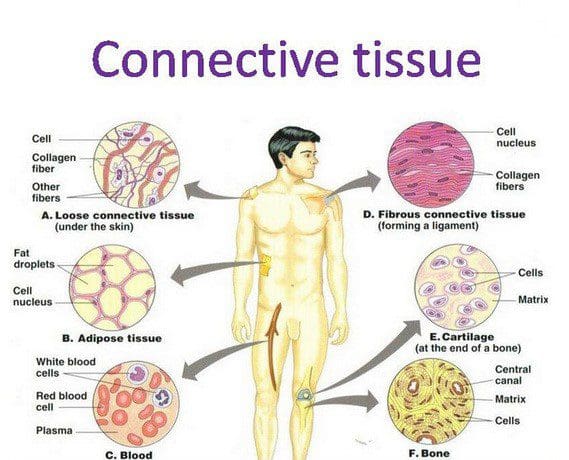
The human body is a multiplex machine that is composed of many tissues that surround the skeletal joints and vital organs with the basic functions that the body produces. Research studies reveal that, as the name has implied, connective tissues in the body refer to the several different body tissues that connect and support the other tissues by binding them to the body. Now there are three different categories that connective tissue can be broken down into:
Loose connective tissue
Dense connective tissue
Specialized connective tissues
These three different connective tissue categories have functions that allow the body to perform properly and provide support to the rest of the musculoskeletal system. The dense connective tissues make up the body’s tendons and ligaments that move the hands and feet while having a higher collagen fiber density. The loose connective tissues help keep the vital organs in place. And finally, the specialized connective tissues are composed of adipose tissues, cartilage, lymphoid tissues, etc. When the body begins to age naturally or is dealing with issues affecting the connective tissues, it can develop musculoskeletal disorders associated with the connective tissue.
Disorders Affecting The Connective Tissues
Have you been experiencing muscle pain or weakness in your body? Do your hands or feet feel tired? Or do you feel stiffness and pain in your joints? Many pain-like symptoms are associated with musculoskeletal disorders affecting the body’s connective tissues. As stated earlier, when the body begins to age naturally, the various muscles in the body can develop into musculoskeletal disorders associated with the connective tissues. Aging can affect connective tissue function as the cartilage from the specialized connective tissues has less elasticity and changes the proteoglycan both quantitatively and qualitatively, according to the book, “Clinical Applications of Neuromuscular Techniques,” written by Leon Chaitow, N.D., D.O., and Judith Walker DeLany, L.M.T. Additional research studies have revealed that environmental factors associated with the body’s immune system can affect the connective tissues. This is known as connective tissue disorder, and it can be comprised of numerous conditions that can affect the immune system and cause overlapping symptoms in the musculoskeletal system. This includes some of the following:
Inflammation in the joints causes them to lock up
Muscle weakness where myofascial entrapment affects the muscle fibers
Fatigue
Vitamin deficiency
An Introduction To MET- Video
Have you been feeling stiffness in your muscles or joints? Does it hurt when you are bending over and lifting heavy objects? Or are you feeling tired constantly? When the body deals with these issues, it can affect more than the muscles and connective tissues. This can lead to symptoms of stiffness and aches in the joints while restricting the range of motion to the muscles. When this happens to the body, many pain specialists utilize MET (muscle energy technique) and relieve those symptoms. Studies reveal that MET is a manual treatment for soft tissue, helping mobilize the joints and stretch tight muscles and fascia to improve circulation to the connective tissues and drain the lymphatic system. The video above introduces how MET is used on the body.
The MET Technique On Connective Tissues
Research studies reveal that since the muscles and joints are being held together by connective tissues, using the MET technique allows pain specialists to stretch the muscles and joints to release tension and other symptoms associated with pain. When pain specialists use the MET technique on the body, it can help strengthen the weaker muscles while paying attention to how short the muscles are affecting the body. While the MET technique can help support the muscles with combined physical therapy, it can help stretch the tight muscles and overworked connective tissues. This allows the body to be restored and get back to normal. Many pain specialists like chiropractic care allow the MET technique to stretch the trapped connective tissues and free the body’s structures to correct postural imbalances.
Conclusion
The body’s connective tissues support each muscle, organ, and skeletal structure. When issues affect the body, the various muscle groups, and connective tissues start to develop overlapping symptoms associated with pain. When pain-like symptoms affect the body, many people will go to a pain specialist and be treated using the MET technique to restore the muscles and body and return to normal.
References
Chaitow, Leon, and Judith Walker DeLany. Clinical Applications of Neuromuscular Techniques. Churchill Livingstone, 2003.
Kamrani, Payvand, et al. “Anatomy, Connective Tissue.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 24 Jan. 2022, https://www.ncbi.nlm.nih.gov/books/NBK538534/.
Page, Phil. “Current Concepts in Muscle Stretching for Exercise and Rehabilitation.” International Journal of Sports Physical Therapy, U.S. National Library of Medicine, Feb. 2012, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3273886/.
Rao, Vijay, and Simon Bowman. “Latest Advances in Connective Tissue Disorders.” Therapeutic Advances in Musculoskeletal Disease, U.S. National Library of Medicine, Aug. 2013, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3728978/.
Thomas, Ewan, et al. “The Efficacy of Muscle Energy Techniques in Symptomatic and Asymptomatic Subjects: A Systematic Review.” Chiropractic & Manual Therapies, U.S. National Library of Medicine, 27 Aug. 2019, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6710873/.
Every day, the body is in constant rest or active motion when needed, from working to exercising and getting adequate rest to repeat the cycle. However, as the body is in this dynamic/rest motion, unintentionally, many individuals will be hunched forward, causing their posture to be slouched for long periods. To that point, it can cause the surrounding neck, shoulder, and back muscles to be pulled and overly stretched, causing pain when the individual gets out of the reclined position. When a person is constantly being hunched over, the action alone could lead to poor posture, which can cause misalignment to the spine and be associated with many chronic conditions that affect their way of life. Fortunately, various treatments can help alleviate poor posture and its associated symptoms. Today’s article examines what defines good posture, the influences that can affect body posture, and how treatment techniques like MET (muscle energy technique) can help improve posture. We mention our patients to certified medical providers that provide available therapy treatments like MET (muscle energy techniques) for individuals suffering from chronic conditions associated with poor posture that can correlate with overlapping risk profiles. We encourage each patient when it is appropriate by referring them to associated medical providers based on their diagnosis or needs. We understand and accept that education is a marvelous way when asking our providers crucial questions at the patient’s request and acknowledgment. Dr. Alex Jimenez, D.C., uses this information as an educational service. Disclaimer
What Defines Good Posture?
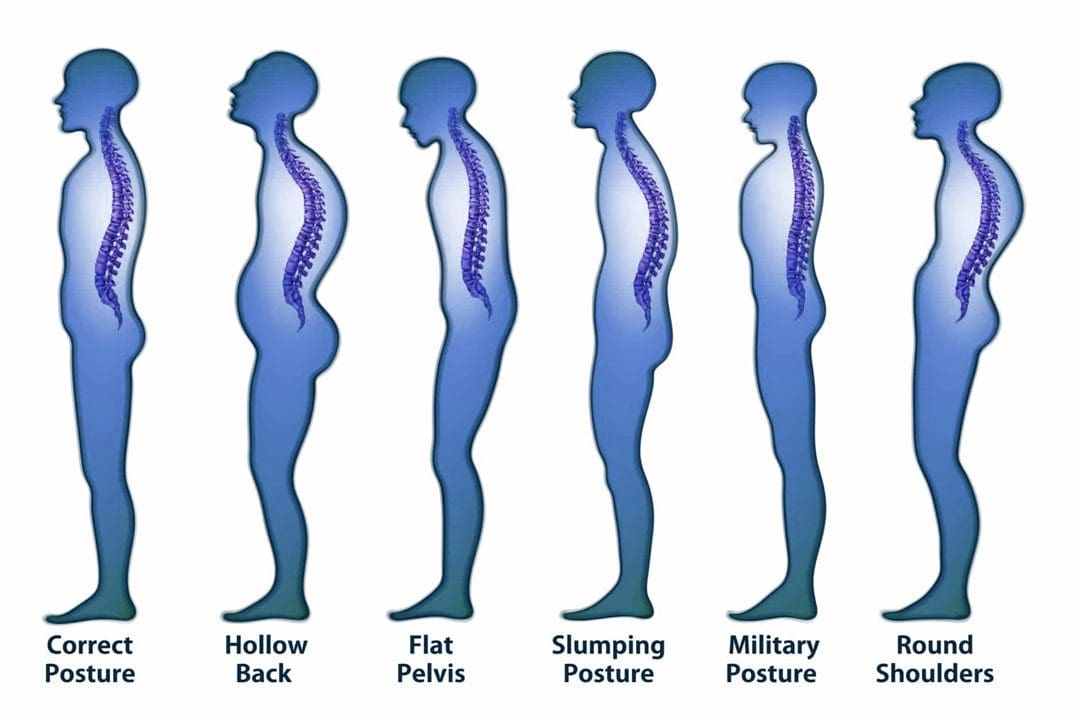
Have you been experiencing referred pain in your neck, shoulders, or lower back? Do you feel pain when stretching after being hunched over throughout the day? Or have you noticed that your neck is slanted, which causes your head to poke in front of your shoulders? Many of these issues are correlated with poor posture. Many of us have heard the saying from our parents, “Stand up straight!” And this is a reminder that having good posture correlates with good spinal health. The book, “Clinical Applications of Neuromuscular Techniques,” written by Leon Chaitow, N.D., D.O, and Judith Walker DeLany, L.M.T, mentions that posture is used to describe the static state of the spine. There are two different types of posture: static and dynamic. Static posture is when the body is in motion, while dynamic posture is when the body is resting. So good posture allows the spine to naturally curve with minimal pain affecting the cervical, thoracic, and lumbar regions.
Influences That Affect Body Posture
As stated early, many of us unintentionally hunch our bodies over time. This is one of the issues as we constantly look down on our phones, and as we get older, it can affect our ability to balance ourselves. Research studies reveal that improper posture can affect static and dynamic balance as we age. This means that when we are constantly hunched over as older adults, we are more prone to the risk of falling and causing long-term disability to our bodies. Additional research studies also mentioned that chronic conditions like forward head posture (which correlates to constantly looking down at the phone) could cause a persistent and abnormal contraction of the neck and shoulder muscles to become dysfunctional. To that point, it can cause pressure on the muscles, fascia, and nerves in the cervical-thoracic regions of the body. When bad posture affects the body over time, it can develop into musculoskeletal disorders if not treated immediately.
5 Way To Improve Posture- Video
Have you felt muscle strain on your neck, shoulders, and back? Have you felt relief when you stretch after being hunched over? Do you feel unstable when walking? These issues could be correlated with your posture if you have been experiencing these issues. When it comes to the body, it is important to make sure that maintaining good posture is not just to please your parents but to have a healthy spine. When we are constantly hunched over, it can cause the muscles and connective tissues to have gravitational strain and shorten the length of the muscles. However, realizing that you have poor posture early on can be treated. The video above shows the five best ways to improve your posture and how to strengthen the back, neck, and shoulder muscles from developing chronic conditions. Exercise alone can not be the only solution; combining it with chiropractic therapy allows the body to be fully restored with various techniques to reduce pain-like symptoms.
How The Met Technique Helps Improve Posture
So how would chiropractic care help with improving posture? Many chiropractors use techniques like MET (muscle energy technique) and spinal manipulation to help restore the body to realignment. Studies reveal that the combinations of MET and stretching can help lengthen the short muscles and restore range of motion to the body. Chiropractors use their hands and various tools to help realign the spine from subluxation and return the body to normal while freeing the tense muscles. Chiropractic care decreases the body’s risk of back injuries while reducing wear and tear on the muscles and joints, contributing to poor posture.
Conclusion
Overall, it is important to maintain good posture to prevent unwanted chronic issues from causing pain-like symptoms to the body. Recognizing the problems contributing to poor posture, treatment, and exercise can help stretch and strengthen the back muscles from hunching over. Maintaining good posture allows the body to be pain-free and prevents many unwanted symptoms from developing.
References
Chaitow, Leon, and Judith Walker DeLany. Clinical Applications of Neuromuscular Techniques. Churchill Livingstone, 2003.
Cohen, Rajal G, et al. “Lighten up! Postural Instructions Affect Static and Dynamic Balance in Healthy Older Adults.” Innovation in Aging, U.S. National Library of Medicine, 24 Mar. 2020, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7092748/.
Lee, Joon-Hee. “Effects of Forward Head Posture on Static and Dynamic Balance Control.” Journal of Physical Therapy Science, U.S. National Library of Medicine, Jan. 2016, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4756019/.
Phadke, Apoorva, et al. “Effect of Muscle Energy Technique and Static Stretching on Pain and Functional Disability in Patients with Mechanical Neck Pain: A Randomized Controlled Trial.” Hong Kong Physiotherapy Journal : Official Publication of the Hong Kong Physiotherapy Association Limited = Wu Li Chih Liao, U.S. National Library of Medicine, 14 Apr. 2016, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6385145/.
Prolonged standing can cause the pelvis to push backward, increasing the curve of the lower back/lumbar region. This increased pressure on the soft tissues surrounding the spine causes the lower back muscles to tighten and/or spasm, resulting in discomfort in the joints and nerves. Weakened core muscles and unhealthy posture/postural syndrome are the most common causes, but injury, aging, congenital malformations, or a disease/condition can also contribute to the symptoms. Injury Medical Chiropractic and Functional Medicine Clinic has a top team of professional therapists to evaluate the problem, diagnose the cause/s accurately, and develop a customized treatment and rehabilitation plan.
Prolonged Standing Back Discomfort
Back Structure
The lower back is one of the most used areas of the spine, moving around and bending during a normal day. When the body stands, the spine naturally curves both in and outwards.
The inward curve, called lordosis, curves towards the front of the body at the lower back and neck regions.
The outward curve, called kyphosis, curves towards the back of the body at the chest.
When bending over while standing, the five lumbar vertebrae of the lower back change position and shift from lordosis to kyphosis when bent completely.
When standing up from bending, the lumbar vertebrae change position again and return to the lordosis position.
Causes
The facet joints allow movement between each spine level. The standing spinal curvature can increase contact between the facet joints. As the body ages, the facet joints and discs begin to wear out, which can cause the discs and facet joints to become inflamed. Prolonged standing during normal daily activity combined with inflammation in these joints can aggravate the inflammation and cause symptoms. Regular routines and habits may contribute to low back discomfort during prolonged standing. These include:
Sleeping on a sinking or unsupportive mattress.
Practicing unhealthy postures that cause imbalances with proper weight distribution.
Not wearing proper footwear and/or supportive orthotics forces the lower spine into increased curvature and can compress the facet joints.
Not getting enough physical activity that strengthens the core.
Chiropractors are experts on the musculoskeletal system. They will:
Listen to the patient about symptoms, medical history, and occupation.
A physical examination of muscle tone, strength, and range of motion.
Therapeutic massage, electric muscle stimulation, and ultrasound therapy can help reduce muscle inflammation and increase circulation to injured soft tissues.
Chiropractic adjustments will reset joints, removing pressure from the surrounding muscles and nerves.
Targeted therapeutic strength training is recommended for core and leg muscles to improve hip flexibility.
Non-surgical decompression or traction, either with a machine or suspension, can reverse the pressure in spinal discs.
Standing Lower Back Relief Exercises
References
Hasegawa, Tetsuya, et al. “Association of low back load with low back pain during static standing.” PloS one vol. 13,12 e0208877. 18 Dec. 2018, doi:10.1371/journal.pone.0208877
Jo, Hoon, et al. “Negative Impacts of Prolonged Standing at Work on Musculoskeletal Symptoms and Physical Fatigue: The Fifth Korean Working Conditions Survey.” Yonsei medical journal vol. 62,6 (2021): 510-519. doi:10.3349/ymj.2021.62.6.510
Ognibene GT, Torres W, von Eyben R, Horst KC. Impact of a sit-stand workstation on chronic low back pain: randomized trial results. J Occup Environ Med. 2016;58(3):287-293. Abstract. https://www.ncbi.nlm.nih.gov/pubmed/26735316. Accessed March 2, 2017.
Parry, Sharon P et al. “Workplace interventions for increasing standing or walking for decreasing musculoskeletal symptoms in sedentary workers.” The Cochrane database of systematic reviews vol. 2019,11 CD012487. November 17, 2019, doi:10.1002/14651858.CD012487.pub2
Rodríguez-Romero, Beatriz, et al. “Thirty Minutes Identified as the Threshold for Development of Pain in Low Back and Feet Regions, and Predictors of Pain Intensity During 1-h Laboratory-Based Standing in Office Workers.” International journal of environmental research and public health vol. 19,4 2221. February 16, 2022, doi:10.3390/ijerph19042221
Smith, Michelle D et al. “The Influence of Using a Footstool during a Prolonged Standing Task on Low Back Pain in Office Workers.” International journal of environmental research and public health vol. 16,8 1405. April 18. 2019, doi:10.3390/ijerph16081405
When everyday factors affect how many of us function, our back muscles begin to suffer. The back muscles in the cervical, thoracic, and lumbar section surround the spine and spinal cord, which helps the body stay upright and promotes good posture. The muscles allow the upper portions of the body to bend down and twist without pain while providing stability to the lower parts of the body. However, when the body ages or everyday activities cause issues, it can develop low back pain associated with weak back muscles. There are many ways to prevent these issues from escalating with various hyperextension exercises for low back pain. This 2-part series examines how low back pain affects the body and how different hyperextension exercises can help strengthen the back. Part 1 examines how hyperextension affects the body and how it is associated with low back pain. We mention our patients to certified medical providers that provide available therapy treatments for individuals suffering from chronic low back pain. We encourage each patient when it is appropriate by referring them to associated medical providers based on their diagnosis or needs. We understand and accept that education is a marvelous way when asking our providers’ crucial questions at the patient’s request and acknowledgment. Dr. Jimenez, D.C., makes use of this information as an educational service. Disclaimer
Low Back Pain Affecting The Body
Have you been dealing with aches and pains when bending down? Do you feel stiffness in your torso when twisting? Or have you experienced limited mobility in your hips? Many of these symptoms correlate with low back pain. Studies reveal that back pain is one of the most common issues in the emergency room. Low back pain is associated with many factors that put pressure on the various muscles in the back and can lead to underlying conditions that can cause symptoms to make the body dysfunctional. Additional studies have revealed that chronic low back pain can have influenced overlapping risk profiles, which include:
Stress
Dietary habits
Lifting heavy objects
Musculoskeletal disorders
When these factors affect the back, many individuals will be in constant pain and take medication to relieve their pain. However, medicine can only go so far as it only masks the pain, but there are other ways to reduce low back pain and help strengthen the various muscles surrounding the low back.
An Overview Of Hyperextension (Part 2)
Biomedical physiologist Alex Jimenez explains how there are a couple of different variations that you can do to prevent low back pain. The first one is the elbows in front. The second one is the elbows in front while pointing them forward and keeping them pointed forward throughout the entire movement. The third one is the hands behind the head. And then the fourth variation is putting weight behind your back once you work up to this level. And then using that weight to put more stress on a pivot point. You can also hold the weight to your chest, but putting it behind your head gives you a further pivot point or a further point on the fulcrum, which are your hips putting more stress on your spinal rectors. The repetitions and frequency should be performed at the beginning of most workouts, before or after your abdominal exercises on leg days. You can use this exercise as a warmup before deadlifting or squatting. I’ll remember you don’t have to go as much weight or as many reps when you’re doing this on leg days. So we recommend starting with four sets of 20 reps and slowly working up to four sets of 40 reps. This seems like a lot, but it will be beneficial in the end.
Various Hyperextension Exercises For The Back
When it comes to low back pain, the various muscles are weak, which can lead to multiple symptoms affecting a person’s mobility. Luckily making small changes in a daily structure, like incorporating exercises that target the back, can be beneficial. Studies reveal that exercises targeting the back muscles can help strengthen the targeted muscles to have mobility and stability in the back. As a bonus, exercises combined with chiropractic treatments can help restore the body and allow the spine to be realigned. When it comes to back exercises, hyperextension exercises can help prevent low back symptoms from reoccurring and strengthen weak back muscles. Here are some of the various hyperextension exercises that benefit the back.
Reverse Flys
There are different variations of how to do reverse flys. You can pick a moderate or lightweight dumbbell or a resistance band. This exercise is great for the upper back muscles and rear deltoids.
Sit in a chair where the dumbbells are in front of you. *For resistance bands, make sure the bands are under your feet.
Pick up the dumbbells/resistance bands with the palms of your hands and bend forward.
Squeeze the shoulder blades together, lift the arms to shoulder level with slightly bent elbows, and lower them.
Repeat for three sets of 12 reps and rest in between.
Hip Thrust
Different variations to this exercise can help with the posterior muscles in the lower back. You can use barbells, dumbbells, resistance bands, or your body weight to strengthen your core back muscles.
Lean against a bench with the knees bent and the feet flat on the floor.
Rest the shoulder blades on the bench for support and have the weight placed near your core.
Raise your body slightly by pushing your heels down to the floor and walking out slowly beyond your knees.
Push through your heels to have your hips at shoulder level, hold for a second, and lower your hips back down.
Repeat for three sets of 12 reps and rest in between.
Supermans
This exercise has two different variations and makes you aware of your back muscles. This exercise helps improve muscle mobility in all three sections of the back.
Lay on the mat face down with your arms in front and your legs straight.
Keep the head in a neutral position and raise both the arms and legs off the mat. This allows the body to be in a banana shape in a comfortable position. *If you want more challenge, lift the opposite arms and legs simultaneously.
Hold for a couple of seconds for the upper and lower back and hamstrings to maintain their positions.
Lower down with control.
Repeat for three sets of 12 reps and rest in between.
Fire Hydrants
This exercise helps the lower back and glute muscles reduce the effects of low back pain and make it more challenging to use a resistance band.
Be in a cat/cow position on your mat, allowing the wrist to be aligned under the shoulders and the knees to be aligned under the hips.
Maintain a neutral spine while engaging the core.
Squeeze the glutes and lift your right leg off the mat, keeping the knee at 90 degrees. *The hips should be the only ones moving to keep the core and pelvis stable.
Lower the right leg down with control.
Repeat for three sets of 12 reps and rest before repeating the motion on the left leg.
Conclusion
All in all, having low back pain doesn’t mean your life is over. Incorporating hyperextension exercises as part of your daily routine can help strengthen your back muscles and ensure that you won’t have reoccurring symptoms from low back pain. Making these small changes can lead to beneficial results in the long run for your health and wellness journey.
References
Allegri, Massimo, et al. “Mechanisms of Low Back Pain: A Guide for Diagnosis and Therapy.” F1000Research, U.S. National Library of Medicine, 28 June 2016, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4926733/.
Casiano, Vincent E, et al. “Back Pain – Statpearls – NCBI Bookshelf.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 4 Sept. 2022, https://www.ncbi.nlm.nih.gov/books/NBK538173/.
Koes, B W, et al. “Diagnosis and Treatment of Low Back Pain.” BMJ (Clinical Research Ed.), U.S. National Library of Medicine, 17 June 2006, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1479671/.
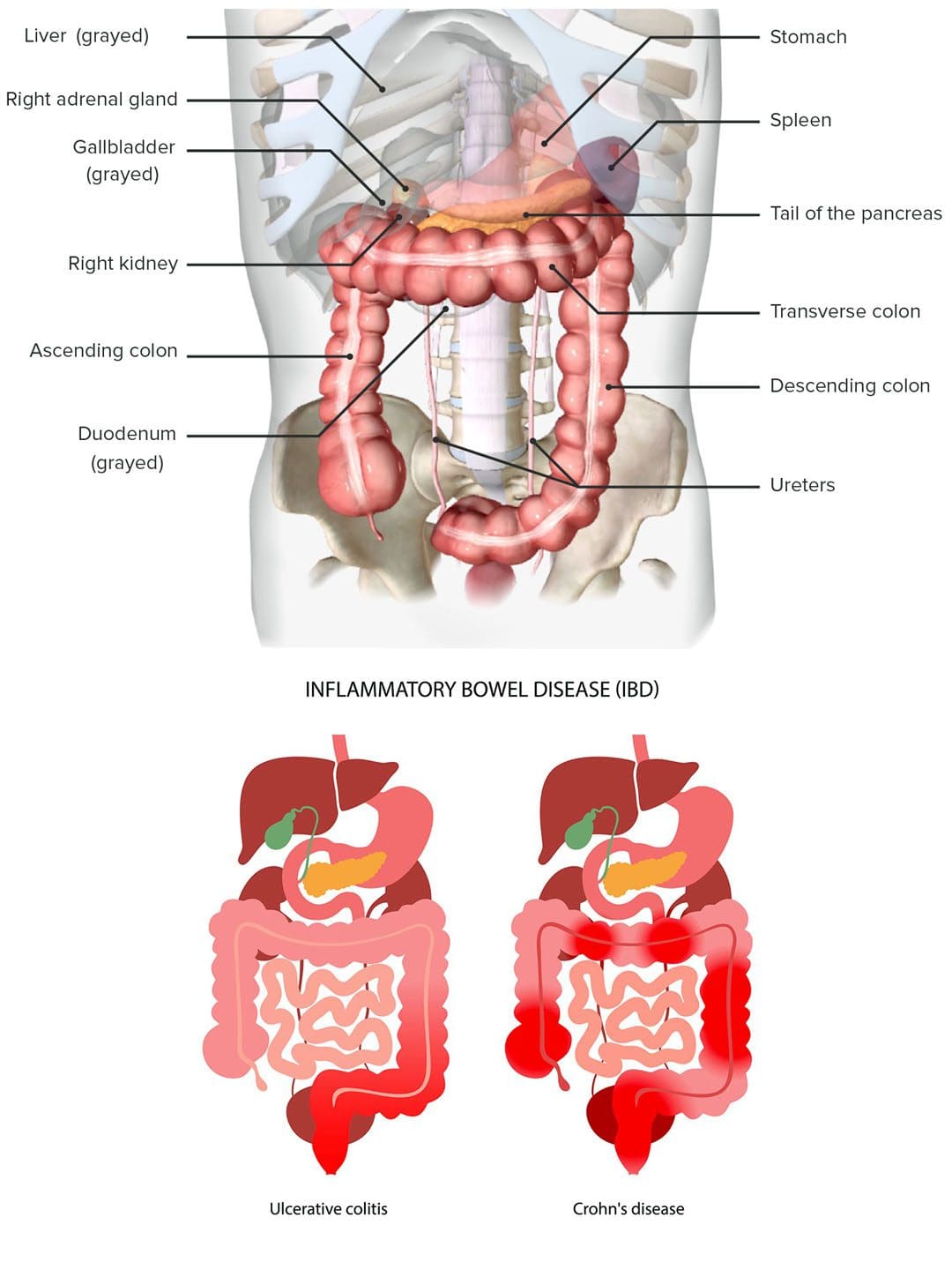
Inflammatory bowel disease, or IBD, causes inflammation of the digestive tract lining, which often involves the deeper layers. Gastrointestinal or GI problems of the stomach and intestines often include diarrhea, weight loss, rectal bleeding, fatigue, and back pain. The inflammation can reach the spine’s joints, causing stiffness, discomfort, and pain symptoms. Injury Medical Chiropractic and Functional Medicine Clinic can help manage symptoms and guide individuals on treatment options.
IBD Back Pain
IBD is a set of conditions associated with chronic or intermittent inflammation of the gastrointestinal tract. It includes Crohn’s disease – CD and ulcerative colitis – UC. Although there are genetic components that predispose individuals to IBD, environmental factors appear to contribute the most. Research shows that IBD is likely related to disturbances in the gut’s flora, which include:
Other environmental factors associated with IBD include the long-term use of birth control pills and nonsteroidal anti-inflammatory drugs/NSAIDs. Research theorizes that as the gut becomes inflamed, its normal integrity and structure become compromised and begin to leak out, causing an immune system overreaction response. This can cause non-gastrointestinal symptoms that include:
IBD can cause low back pain as the IBD can inflame the spine’s joints, especially the sacrum, as well as cause abdominal cramps and rectal sensations that radiate to the low back area. However, irritation, inflammation, or infection of any central, abdominal, or pelvic organs can cause low back pain.
Diagnosis
Diagnosis requires a physical examination of the colon – a sigmoidoscopy or a colonoscopy is used.
Both procedures take a biopsy of the intestinal tissues, which is studied to determine the extent and degree of inflammation.
Depending on the circumstances, an X-ray could be used to show the depth or extent of the condition.
Chiropractic Management
A chiropractor can help individuals decrease or completely alleviate musculoskeletal symptoms by realigning the spine and pelvis and massaging, releasing, and relaxing the muscles, which increases circulation and soothes inflammation. The reason why chiropractic care can effectively treat IBD is its ability to stabilize the internal systems. When the central nervous system and immune system communicate and function properly, this prevents the immune system from attacking the body’s tissue cells, preventing inflammation. The chiropractic whole-body approach can also help with recommendations regarding lifestyle changes and nutritional anti-inflammatory modifications.
Ulcerative Colitis
References
Centers for Disease Control and Prevention. “What Is Inflammatory Bowel Disease (IBD)?” 2022, https://www.cdc.gov/ibd/what-is-IBD.htm
Danese S, Fiocchi C. Etiopathogenesis of inflammatory bowel diseases. World J Gastroenterol. 2006;12(30):4807-4812. doi:10.3748/wjg.v12.i30.4807
Limsrivilai, Julajak et al. “Systemic Inflammatory Responses in Ulcerative Colitis Patients and Clostridium difficile Infection.” Digestive diseases and sciences vol. 63,7 (2018): 1801-1810. doi:10.1007/s10620-018-5044-1
van Erp, S J et al. “classifying Back Pain and Peripheral Joint Complaints in Inflammatory Bowel Disease Patients: A Prospective Longitudinal Follow-up Study.” Journal of Crohn’s & colitis vol. 10,2 (2016): 166-75. doi:10.1093/ecco-jcc/jjv195
Zeitz, Jonas, et al. “Pain in IBD Patients: Very Frequent and Frequently Insufficiently Taken into Account.” PloS one vol. 11,6 e0156666. 22 Jun. 2016, doi:10.1371/journal.pone.0156666
The lumbar region of the spine has various muscles and nerve roots that work together with the lower body extremities, like the hips, buttocks, legs, knees, and feet, for mobility and walking function. The various muscles in the buttock region include the gluteal muscles. They have a casual relationship with the hip muscles as they work together for hip mobility and erect good posture in the body. These various muscles and nerves also supply sensory-motor function for the legs to be mobile and provide hip mobility. The piriformis is one of the muscles assisting in the hips and buttock region. When this muscle becomes overused, it can cause mobility issues in the legs and affect a person’s ability to walk. Today’s article looks at the piriformis muscle, how trigger points are associated with piriformis syndrome, and how to manage piriformis syndrome associated with trigger points. We refer patients to certified providers who incorporate multiple methods in the lower body extremities, like sciatic pain and piriformis syndrome treatments related to trigger points, to aid individuals dealing with pain symptoms along the piriformis muscle. We encourage and appreciate patients by referring them to associated medical providers based on their diagnosis, especially when it is appropriate. We understand that education is an excellent solution to asking our providers complex questions at the patient’s request. Dr. Jimenez, D.C., utilizes this information as an educational service only. Disclaimer
What Is The Piriformis Muscle?
Have you been having issues walking from one place to another? Do you feel muscle tightness in your hips or buttock region? Or are you experiencing radiating pain traveling to your knees and feet? These pain symptoms are correlated with trigger points affecting the piriformis muscle. The piriformis is a flat, pear-shaped muscle, one of the six short rotator muscle groups in the gluteal region of the hips and thighs. The rotator muscle groups consist of the following:
Gemelli
Quadratus Femoris
Obturator Internus
Obturator Externus
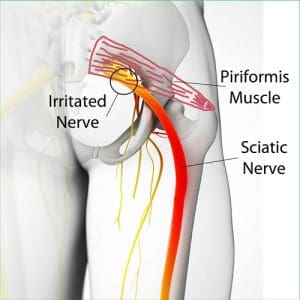
This muscle is parallel to the posterior margins of the gluteus medius and deep into the gluteus maximus. This muscle is very important to the body as it provides lower-body movement by stabilizing the hip joint and can lift and rotate the thighs away from the body. The piriformis muscle also surrounds the sciatic nerve, as this long nerve runs deep beneath the piriformis and enters the gluteal region of the rear. When the piriformis muscle becomes overused or suffers from associated traumatic factors, it can aggravate the sciatic nerve and even develop tiny nodules known as trigger points, causing mobility issues.
Trigger Points Associated With Piriformis Syndrome
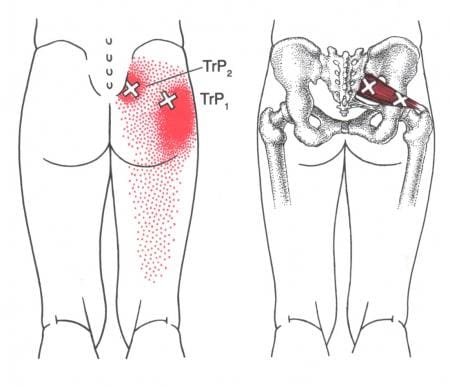
When abnormal factors affect the piriformis muscles, they can develop into trigger points associated with piriformis syndrome and cause issues in the pelvic and hip regions of the body. According to Dr. Janet G. Travell, M.D., “Myofascial Pain and Dysfunction,” trigger points can be activated when repetitive strain affects the piriformis muscle and causes symptoms of muscle weakness and pain in the hips. This causes overlapping issues in the surrounding muscles and the sciatic nerve, making diagnosing tricky for trigger points. Studies reveal that trigger points associated with piriformis syndrome may potentially cause muscle spasms or an inflammatory process to irritate the sciatic nerve that may be presented as identical to lumbar disk syndrome without neurological findings. Trigger points associated with piriformis syndrome may mimic chronic issues like fibromyalgia. Even though trigger points are tricky to pinpoint in a thorough examination, there are various ways to reduce the pain and prevent trigger points from affecting the piriformis muscle causing sciatic nerve pain.
Trigger Point Of The Week: Piriformis Muscle- Video
Have you been dealing with sciatic nerve pain? Have you found it difficult to walk for a short period? Or are you dealing with muscle tenderness or soreness in your buttock or hips? People experiencing these symptoms could be dealing with piriformis syndrome associated with trigger points. The piriformis is a small, fan-shaped muscle, one of the six short rotator muscle groups that help with hip and thigh mobility through stabilization. The piriformis muscles also surround the sciatic nerve and can succumb to injuries. When traumatic forces affect the hips and thighs, the piriformis muscle develops nodules known as trigger points, causing the muscle to irritate the sciatic nerve and cause pain in the legs. The video above shows where the piriformis muscle is located and how trigger points can mimic sciatic nerve pain in the leg without neurological findings. Studies reveal that trigger points could be a rare anatomical variation that can correlate with piriformis syndrome associated with sciatica. However, there is some good news, as there are ways to manage piriformis syndrome associated with trigger points.
Managing Piriformis Syndrome Associated With Trigger Points
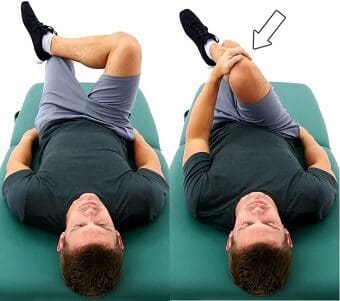
Various techniques can help manage piriformis syndrome associated with trigger points to relieve the piriformis muscle. Studies reveal that Kinesio tape on the piriformis muscle can help reduce pain and improve many individuals’ hip joint range of motion. Other techniques like stretching or deep tissue massage can help loosen up the stiff muscles and relieve trigger points from forming on the piriformis. For sciatica pain associated with trigger points along the piriformis muscle, decompression therapy can help the piriformis muscle lay off pressure on the sciatic nerve and reduce aggravated pain. These techniques can help improve hip joint mobility and increase the range of motion to the hips and lower extremities.
Conclusion
The piriformis is a small muscle that provides hip and thigh mobility. This small muscle surrounds the sciatic nerve, which helps give motor function to the legs. When traumatic factors affect the piriformis muscle, it can develop trigger points and cause sciatic pain in the hips. This causes mobility issues and pain around the hips. Various treatments are provided to help reduce the trigger points along the piriformis muscle and reduce sciatic nerve pain from causing more problems to the hips and legs mobility.
References
Chang, Carol, et al. “Anatomy, Bony Pelvis and Lower Limb, Piriformis Muscle.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 3 Oct. 2022, https://www.ncbi.nlm.nih.gov/books/NBK519497/.
Pfeifer, T, and W F Fitz. “[The Piriformis Syndrome].” Zeitschrift Fur Orthopadie Und Ihre Grenzgebiete, U.S. National Library of Medicine, 1989, https://pubmed.ncbi.nlm.nih.gov/2618150/.
R;, Hashemirad F;Karimi N;Keshavarz. “The Effect of Kinesio Taping Technique on Trigger Points of the Piriformis Muscle.” Journal of Bodywork and Movement Therapies, U.S. National Library of Medicine, 8 Feb. 2016, https://pubmed.ncbi.nlm.nih.gov/27814861/.
Ro, Tae Hoon, and Lance Edmonds. “Diagnosis and Management of Piriformis Syndrome: A Rare Anatomic Variant Analyzed by Magnetic Resonance Imaging.” Journal of Clinical Imaging Science, Medknow Publications & Media Pvt Ltd, 21 Feb. 2018, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5843966/.
Travell, J. G., et al. Myofascial Pain and Dysfunction: The Trigger Point Manual: Vol. 2:the Lower Extremities. Williams & Wilkins, 1999.
The buttock and the lower back have a casual relationship to the body, as the lower back has various muscles and nerves surrounding the spinal column. In contrast, the buttock region has multiple muscles and the sciatic nerve to keep the body upright. The sciatic nerve travels from the lumbar region of the spine across the gluteus muscles and down to the legs. The gluteus muscles include the Maximus, medius, and minimus, and they work with the sciatic nerve regarding good posture. When normal or traumatic factors begin to affect the body, like sciatica or poor posture, it can lead to developing trigger points associated with the gluteus minimus affecting the sciatic nerve. Today’s article examines the gluteus minimus, how trigger points mimic sciatic pain on the gluteus minimus, and various treatments to relieve sciatic nerve pain. We refer patients to certified providers who incorporate multiple methods in the lower body extremities, like sciatic pain treatments related to trigger points, to aid individuals dealing with pain symptoms along the gluteus medius muscles associated with sciatica. We encourage and appreciate patients by referring them to associated medical providers based on their diagnosis, especially when it is appropriate. We understand that education is an excellent solution to asking our providers complex questions at the patient’s request. Dr. Jimenez, D.C., utilizes this information as an educational service only. Disclaimer
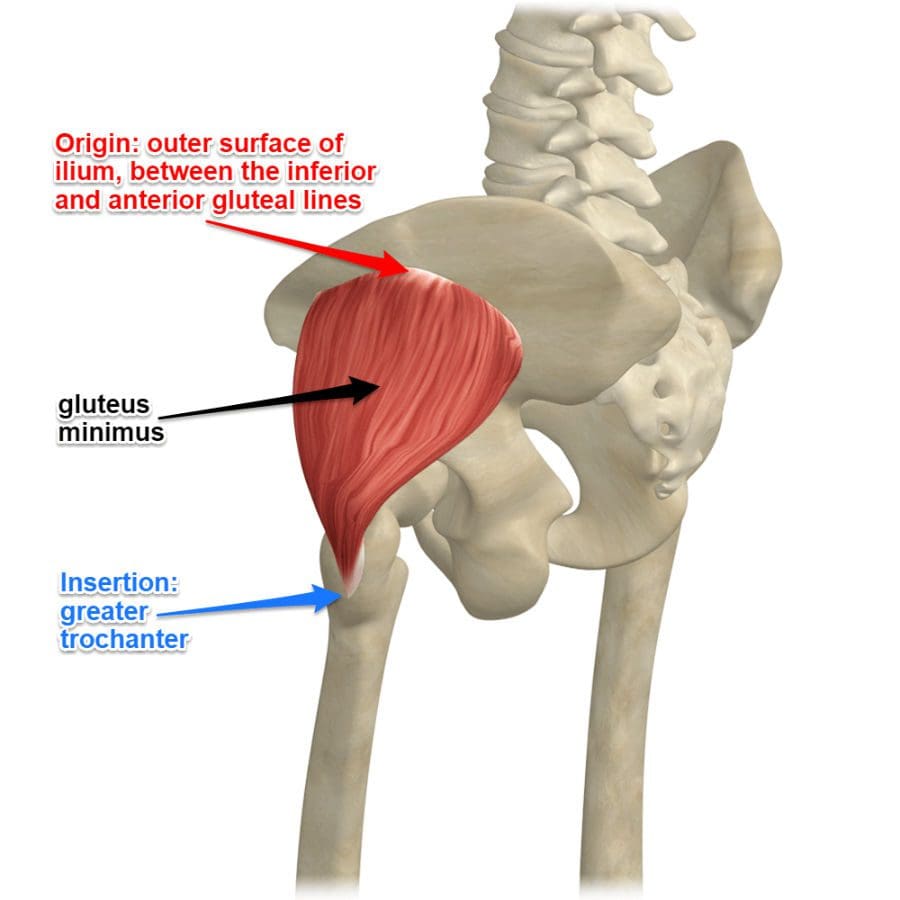
What Is The Gluteus Minimus?
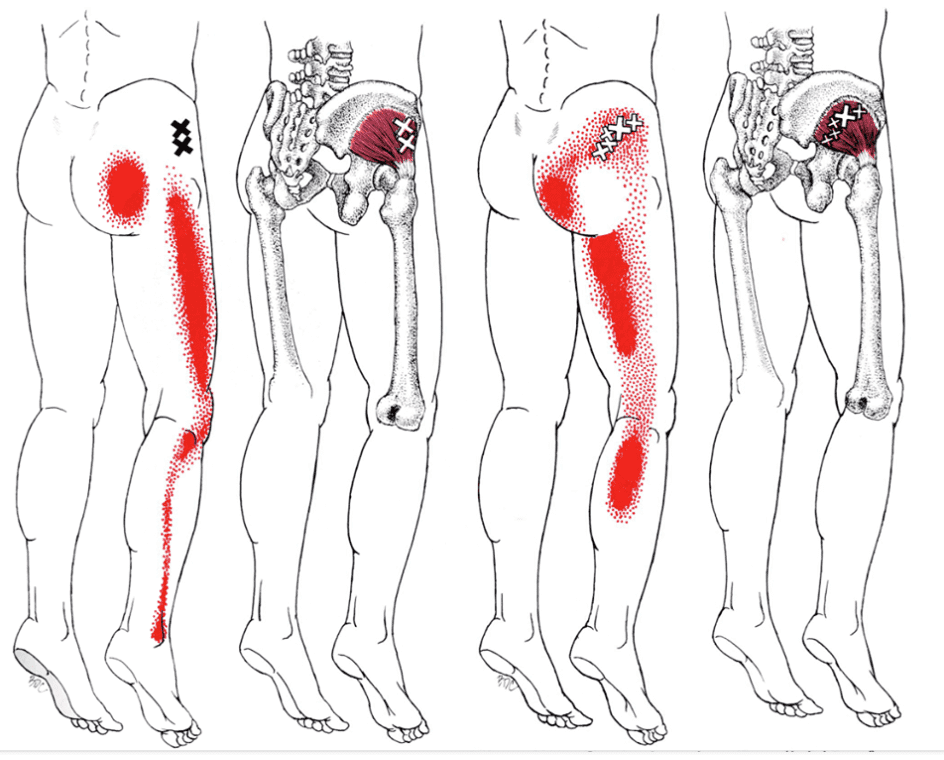
Have you been experiencing radiating pain traveling down to your leg? Do you have difficulty walking or sitting down? Do you feel tenderness or referred pain near your buttock region? Some of the issues correlate with trigger points affecting the gluteus minimus, causing pain in the sciatic nerve. As the smallest muscle in the gluteal region of the buttock, the gluteus minimus shares similar characteristics to the gluteus medius while being located beneath the medius muscle. One of the primary functions of the gluteus minimus is that it predominantly acts as a hip stabilizer and abductor. The nerves from the gluteal muscles include the sciatic nerve, which is on top of the gluteus muscles and the other nerves help supply the muscles to function in the posterior region of the body. Studies reveal that the structural integrity of the gluteus minimus muscles is the key to the lateral hip muscle, which contributes to pelvic stability and lower extremity function. However, when issues affect the gluteal muscles’ posterior region could trigger point pain mimicking sciatica.
How Trigger Points Mimic Sciatic Pain On The Gluteus Minimus?
When the lower body extremities begin to suffer from multiple issues that cause the individual to have mobility dysfunction, various factors could correlate to the dysfunction. When the gluteus minimus muscles have been overused or been through a traumatic experience, they can develop trigger points along the muscle fibers and even cause nerve entrapment along the sciatic nerve. Trigger points along the gluteus minimus can mimic sciatic nerve pain down to the back or even the side of the legs that causes excruciating and deep pain in the posterior region. Studies reveal that pain in the buttock region is a deep gluteal syndrome caused by non-discogenic pain that causes sciatic nerve entrapment.
The book, “Myofascial Pain and Dysfunction,” written by Dr. Janet G. Travell, M.D., states that many patients with active trigger points located in their gluteus minimus would complain about hip pain that could cause them to limp-walk when they are going to places. The pain caused by the active trigger points can make it difficult to stand up from a seated position due to the painful movements. The associated pain that the trigger points are causing to the gluteus minimus can be constant and excruciating; even small stretches can not alleviate the pain. The book also mentioned that trigger points could cause referred pain to the gluteus minimus that can cause various somato-visceral issues to the hips, legs, and knees if the pain worsens.
Sciatic Type Pain: Gluteus Minimus Trigger Points- Video
Are you dealing with pain in your hips, low back, and legs? Do you find it difficult to walk or stand up constantly? Or are you experiencing sciatic nerve pain that is radiating down your leg? All these pain-like symptoms are associated with trigger points along the gluteus minimus affecting the sciatic nerve. The gluteus minimus is the smallest of the gluteal muscles with the same function as the gluteus medius and predominately acts as the hip’s stabilizer and abductor. When the gluteus minimus muscles have been overused from traumatic events or normal factors, they can develop trigger points in the muscle fibers, entrap the sciatic nerve and irritate the nerve causing sciatica. The video above explain where the gluteus minimus is located and pinpoints where the trigger points are in the muscle fibers. Trigger points along the gluteus minimus can mimic sciatica by causing referred pain to travel down the leg. This can cause the individual to be unable to walk or even stand up due to the excruciating pain that they are in. Luckily, trigger points are treatable even though they are tricky to diagnose.
Various Treatments To Release Sciatic Nerve Pain
Even though trigger points along the gluteus minimus are tricky to diagnose, they are treatable through various treatments to alleviate the pain that the person is experiencing and can reduce sciatic nerve pain from causing more issues in the legs. Studies reveal that the effectiveness of active soft tissue release and trigger point block treatments combined can release entrapped nerves from the gluteus minimus and reduce low back and sciatic pain from the lower extremities. Now the treatments alone can only do so much to the individual, as many doctors tell their patients to take corrective actions or techniques to reduce the chances of trigger points from forming again on the gluteus minimus. Techniques like glute stretches, ischemic compressions, or using a foam roller can break the myofascial triggers from the gluteus minimus muscles and reduce the pain in the glutes and legs. This will help bring mobility back to the lower extremities.
Conclusion
As the smallest muscle in the body’s gluteal region, the gluteus minimus is the lower body’s predominant hip stabilizer and abductor. The gluteus minimus contributes to pelvic stability and lower extremity functionality that can be overused and can develop trigger points associated with sciatica. Trigger points along the gluteus minimus can cause referred pain to the legs and lower back while mimicking sciatic nerve pain. Thankfully various treatments and techniques can help reduce the chances of trigger points forming along the gluteus minimus and release nerve entrapment from the aggravated muscles pressing on the sciatic nerve, bringing back lower extremity mobility to the body.
References
Greco, Anthony J, and Renato C Vilella. “Anatomy, Bony Pelvis and Lower Limb, Gluteus Minimus Muscle.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 29 May 2022, https://www.ncbi.nlm.nih.gov/books/NBK556144/.
Kameda, Masahiro, and Hideyuki Tanimae. “Effectiveness of Active Soft Tissue Release and Trigger Point Block for the Diagnosis and Treatment of Low Back and Leg Pain of Predominantly Gluteus Medius Origin: A Report of 115 Cases.” Journal of Physical Therapy Science, The Society of Physical Therapy Science, Feb. 2019, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6382483/.
Martin, Hal David, et al. “Deep Gluteal Syndrome.” Journal of Hip Preservation Surgery, Oxford University Press, July 2015, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4718497/.
Travell, J. G., et al. Myofascial Pain and Dysfunction: The Trigger Point Manual: Vol. 2:the Lower Extremities. Williams & Wilkins, 1999.
Whiler, Lisa, et al. “Gluteus Medius and Minimus Muscle Structure, Strength, and Function in Healthy Adults: Brief Report.” Physiotherapy Canada. Physiotherapie Canada, University of Toronto Press, 2017, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5963550/.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine











 IBD Back Pain
IBD Back Pain