Introduction: My Personal Commitment to the Medico-Legal World—Bridging the Gap Between Clinical Science and Courtroom Proof
By Dr. Alex Jimenez, DC, APRN, FNP-BC | Board-Certified Nurse Practitioner & Chiropractor
Injury Medical Clinic PA, El Paso, Texas
The answer to the crucial question of whether the injury can be conclusively proven, dated, and causally connected to the traumatic event frequently determines the outcome of the high-stakes world of personal injury litigation.
My life’s work at Injury Medical Clinic PA is dedicated to answering this question with an unassailable “Yes.” I have spent decades developing a diagnostic and documentation protocol that transcends the limitations of standard clinical practice. For me, a patient is not just a set of symptoms; they are a complex medico-legal case requiring forensic-level analysis. I recognized early on that El Paso attorneys needed more than a standard radiologist’s report or a simple chiropractor’s diagnosis—they needed a comprehensive, integrated expert who could seamlessly bridge advanced musculoskeletal biomechanics (my foundation as a Chiropractic Physician, DC) with the rigorous standards of comprehensive medical management and documentation (my expertise as a Board-Certified Nurse Practitioner, APRN, FNP-BC).
This unique duality is the engine of our practice. I am not just treating the patient; I am building the legal case. My goal for every personal injury client referred to me is to deliver definitive diagnostic proof that withstands the most rigorous cross-examination, establishes clear causality using objective biomechanical markers, and determines a scientifically validated timeline for the injury—what I call injury dating.
This lengthy post serves as my own, in-depth guide to legal counsel, shedding light on the extent of my involvement in the evaluation of injuries. I meticulously examine the procedures that I use to assess patient cases. These procedures are indispensable for determining the root cause of an illness and for shedding light on the actual degree of disability and impairment that has resulted from traumatic events. I take great pride in my role as a professional in that I am committed to the idea that when a clinical case is brought before a jury, the attorneys representing the plaintiff have complete confidence in the credibility and scientific basis of the expert testimony that I provide.
Dr. Alex Jimenez, DC, APRN, FNP-BC
I will deeply discuss, from my personal experience:
The Diagnostic Imperative: My sophisticated capability to personally stage and interpret complex Magnetic Resonance Imaging (MRI) findings, distinguishing acute trauma from pre-existing conditions using forensic principles.
Causality and Timing: My systematic, proprietary methodology for establishing causality and determining the precise timing (injury dating) of trauma using advanced biomechanical and physiological markers like Modic changes and Wolff’s Law.
The Dual-Licensed Advantage: The justification and profound benefit of treatment and testimony provided by me, a dual-licensed professional, within the El Paso legal community.
Expert Credibility: How attorneys frequently utilize my expert testimony as the credible, objective voice regarding injury dating, impairment, and functional loss, ensuring my documented assessments and evaluations meet the stringent Daubert Standard.
1.0 The Diagnostic Imperative: Personally Staging and Interpreting Complex MRI Findings—Going Beyond the Radiologist’s Report
In my experience, the Magnetic Resonance Imaging (MRI) scan is the single most crucial piece of objective evidence in spinal injury litigation. However, I’ve found that a standard radiologist report often focuses primarily on morphology—describing what is seen—but fails to provide the critical context of causality and chronicity necessary for a successful legal claim.
At Injury Medical Clinic PA, I do not simply accept the outside read; I forensically interpret the physiological, mechanical, and temporal signatures embedded within the MRI data myself. I personally review every single slice and sequence because my ultimate testimony depends on my deep understanding of the images.
1.1 Meeting the Daubert Standard: My Personal Protocols for Scientific Admissibility
In the medico-legal domain, any scientific evidence I present, especially complex imaging findings, must adhere to the Daubert Standard. This requires my expert testimony to be grounded in the methods and procedures of science and supported by appropriate validation (Spinal Diagnostics, n.d.). My entire documentation protocol is built around this necessity.
I personally ensure my findings are admissible by:
Employing Validated Methodology: I utilize diagnostic criteria and staging methods that are thoroughly established in peer-reviewed orthopedic and radiological literature, such as the classification of disc pathology and the chronology of vertebral changes (Wang et al., 2017).
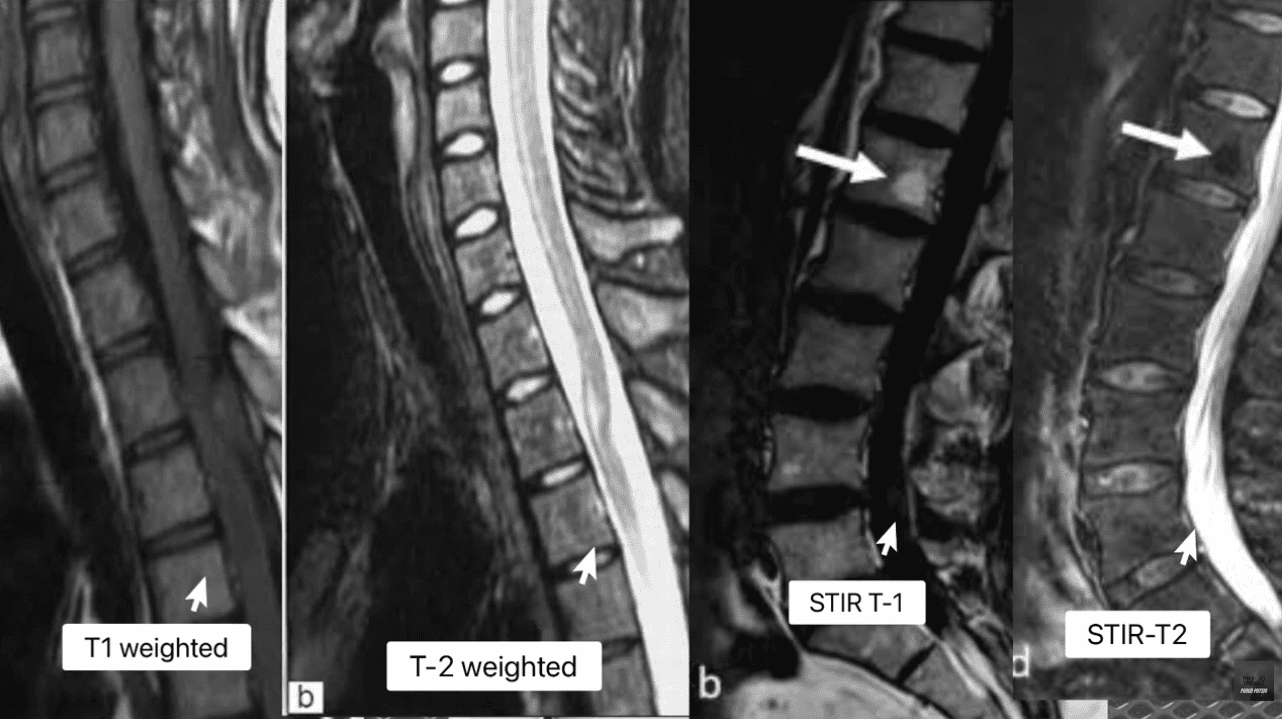
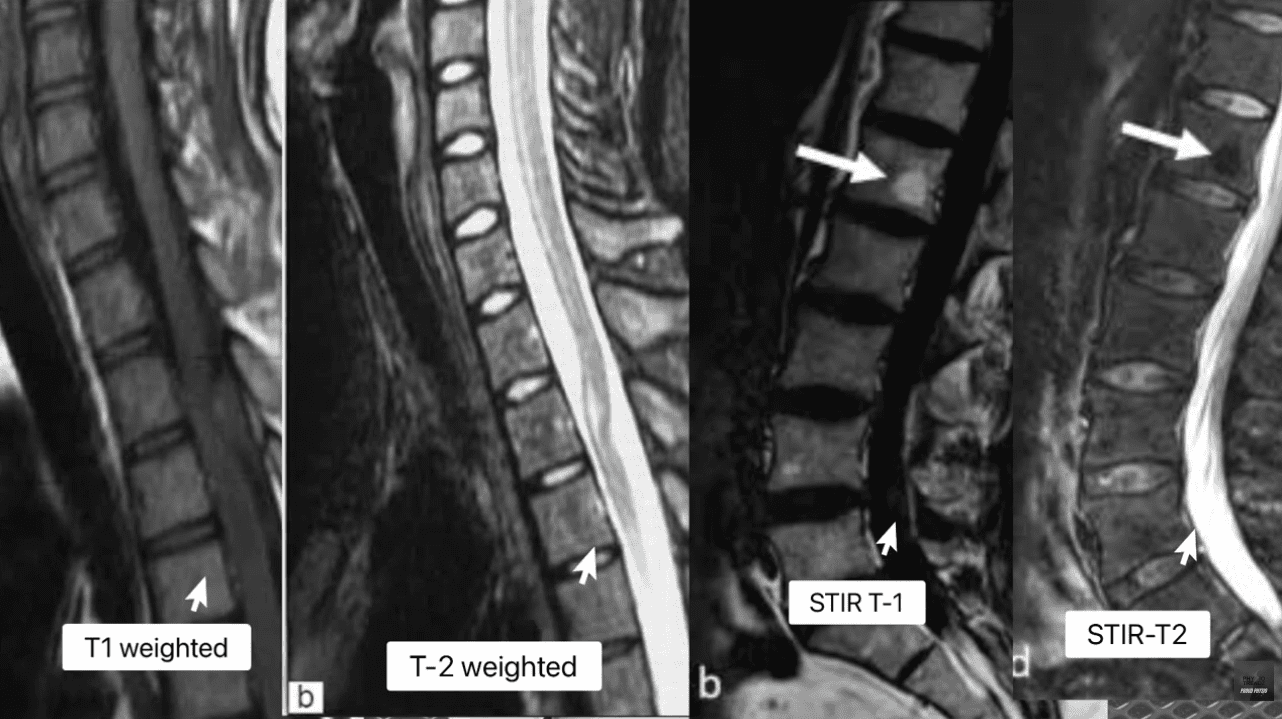
Focusing on Objectivity: My reports meticulously cite the specific MRI pulse sequences (T1, T2, STIR) and image numbers where the pathology is visualized, allowing opposing counsel and the court to verify the data. This objectivity mirrors the rigor seen in advanced quantitative neuroimaging tools like NeuroQuant®, which are successfully used to meet the Daubert standard in TBI cases (National Institutes of Health, 2022).
Simplifying Complex Science: When I testify, my goal is to translate complex terms into easily digestible concepts for the jury. I do not just state a Modic 1 change is present; I explain why it’s a marker of acute trauma, making the science reliable and understandable. This is a crucial skill that attorneys rely on me for.
1.2 Decoding the Spinal Pathologies: My Forensic Review of T1, T2, and STIR Sequences
My method for forensic MRI interpretation depends on a nuanced understanding of various pulse sequences and their physiological meaning (Advanced MRI Interpretation, n.d.). I meticulously review the T1-weighted, T2-weighted, and Short Tau Inversion Recovery (STIR) sequences because they tell different stories about the underlying tissue pathology.
MRI Staging Acute Vs Chronic Injuries
MRI Sequence
Primary Signal (Bright)
Primary Signal (Dark)
Pathological Significance
T1-Weighted
Fat (Marrow), Contrast (Gadolinium)
Water (Edema, CSF), Cortical Bone
Anatomy: Excellent for visualizing fatty infiltration (chronic muscle atrophy, Modic 2) and overall anatomical structure.
T2-Weighted
Water (Edema, CSF), Degenerated Disc
Fat (Marron), Cortical Bone
Pathology: Crucial for identifying water, making it the primary sequence for acute inflammation, disc herniation (fluid), and spinal cord changes.
STIR (Fat-Suppressed)
Water (Edema, CSF, Inflammation)
Fat (Marrow)
Acuity: The definitive sequence for acute trauma. By suppressing fat signal, any remaining bright signal is unequivocally edema, confirming acute inflammation in bone or soft tissue.
The presence of edema (abnormal fluid accumulation) in the bone marrow or soft tissues surrounding the spine is, in my professional opinion, the most powerful, objective indicator of acute trauma. This edema is the body’s immediate inflammatory response to injury and provides the temporal signature required for my precise injury dating.
1.3 Injury Dating: My Systematic Methodology for Establishing a Timeline of Trauma
The ability to accurately date an injury—to definitively state that a spinal pathology is new or acute, rather than chronic and pre-existing—is, without question, the cornerstone of a successful personal injury claim. My clinic utilizes physiological and biomechanical principles to establish this timeline with forensic precision.
1.3.1 Modic Changes: The Gold Standard for Vertebral Endplate Chronology
Modic changes are alterations in the vertebral body endplates and adjacent bone marrow, visible on MRI, that reflect different stages of pathological response. I rely on them heavily because they provide an objective and scientifically validated marker for estimating the age of an injury (Wang et al., 2017; Spinal Diagnostics, n.d.).
Determining Age of Injury Via MRI Staging
Modic Type 1 (MC1) – The Acute Signature: MC1 represents the acute inflammatory stage characterized by bone marrow edema. When I see this, I know I’m looking at an injury that is active and recent.
My Staging: I stage this based on the specific signal patterns: Dark on T1 and Bright on T2/STIR (Spinal Diagnostics, n.d.). The persistent bright signal on STIR is the definitive confirmation of active, acute inflammation.
My Testimony: I explain to attorneys that MC1 changes typically resolve or transition to the fatty Type 2 changes within approximately 6 to 8 weeks (Spinal Diagnostics, n.d.). Therefore, the presence of MC1 is a powerful, objective sign of recent trauma, often correlating directly with the patient’s reported high pain scores (Jensen et al., 2024). When a defense expert attempts to argue degeneration, my documentation of MC1 provides the irrefutable evidence of a specific, new acute event.
Modic Type 2 (MC2) – The Chronic Transition: MC2 represents the replacement of normal bone marrow with fatty tissue (Wang et al., 2017). This is a marker of a more subacute or chronic condition.
My Staging: I stage this based on the characteristic Bright on T1/T2 but crucially, Dark on STIR (fat-suppressed) sequence (Spinal Diagnostics, n.d.).
My Testimony: I use MC2 to show pre-existing degeneration, which ironically, strengthens my credibility. By acknowledging a chronic condition at one level (MC2) while simultaneously proving an acute injury at another (MC1), I demonstrate objectivity and isolate the liability to the new, acute trauma.
1.3.2 Wolff’s Law and My Chronological Interpretation of Bone Spurs
Further reinforcing my injury dating is my application of Wolff’s Law, a fundamental biomechanical principle that bone tissue adapts to the loads placed upon it (Spinal Diagnostics, n.d.). Chronic instability leads to the formation of osteophytes (bone spurs) as the body attempts to stabilize the segment through the piezoelectric effect (Spinal Diagnostics, n.d.).
The Biomechanical Timeline: I rely on scientific research confirming that it takes approximately six months for a bone spur to become radiographically visible or significant (Spinal Diagnostics, n.d.).
My Medico-Legal Implication: When I review a patient’s initial X-rays or CT scans following an MVA, and I find a complete absence of chronic osteophyte formation in the affected segment (e.g., C5-C6), yet the MRI shows an acute disc herniation, I have created an unassailable timeline. The absence of the six-month marker (the bone spur) provides strong supporting evidence that the soft-tissue injury is acute and causally related to the recent collision.
1.4 The Crucial Differential Diagnosis: My Approach to Acute Trauma vs. Chronic Degeneration
Distinguishing new trauma from old, asymptomatic degeneration is essential for proving the extent of damage. I use specific MRI markers to draw this clear line, transforming a murky diagnosis into legal certainty.
Many accident victims have some degree of pre-existing, asymptomatic degeneration. The defense always targets this reality. My expertise lies in identifying and quantifying the acute-on-chronic injury (Spinal Diagnostics, n.d.).
The tell-tale radiological sign I look for is the clear observation of newly extruded disc material extending beyond the border of a mature, pre-existing osteophyte (Spinal Diagnostics, n.d.). The osteophyte, being a chronic boney change, acts as an anatomical baseline for pre-injury status. Any disc material that has been forcefully extruded beyond this chronic bony landmark is, by definition, new trauma and directly quantifiable aggravation. I personally measure this new extrusion and document its displacement in my reports.
1.4.2 The Vacuum Disc Phenomenon: The Irrefutable Marker of Old Pathology
I use the Vacuum Disc Phenomenon as another definitive marker of a chronic, old condition. This finding—nitrogen gas (a distinct signal void, appearing black) within the center of the disc on all MRI sequences (T1, T2, and STIR)—is a reliable sign of old, irreversible degenerative changes and instability (Spinal Diagnostics, n.d.; Advanced MRI Interpretation, n.d.).
When I find a vacuum disc at one level, I include it in my report. This establishes my objectivity, allowing me to state confidently that while one level is chronic, the adjacent, non-vacuum level that displays Modic 1 changes is acute and causally related to the MVA. This approach prevents the defense from collapsing the entire spine into a single, pre-existing condition.
1.5 Analysis of Complex Non-Disc Spinal Pathologies: The Hidden Injuries
Beyond disc herniation, I specialize in the advanced interpretation of other complex spinal pathologies frequently misunderstood or missed by general practitioners, yet vital for proving injury.
1.5.1 The Spinal Epidural Venous Plexus (Batson’s Plexus): Dural Tenting
The Spinal Epidural Venous Plexus (Batson’s Plexus) is a valveless network highly susceptible to sudden pressure changes (Advanced MRI Interpretation, n.d.). In court, I must distinguish between normal physiological changes and pathological ones.
My Differential Diagnosis: Trauma can cause a physiological venous dilation because a disc extrusion can push on the thecal sac—a phenomenon known as dural tenting. This must be carefully distinguished from a pathological Epidural Varix (a symptomatic dilation that causes neural compression) (Advanced MRI Interpretation, n.d.). I rely on sequences like contrast-enhanced MRI (when medically necessary) and non-contrast flow-sensitive sequences to confirm the difference. Incorrectly diagnosing normal venous dilation as a compressive pathology can undermine an entire claim, and my careful distinction preserves my credibility.
1.5.2 Post-Traumatic Muscle Changes: Fatty Infiltration of the Multifidus
The deep lumbar muscles, particularly the multifidus, are essential stabilizers. I have seen time and again how pain-induced inhibition leads to rapid structural changes in this muscle.
My Injury Dating and Causality: This muscle transformation begins to appear on imaging as early as 2 to 12 weeks post-injury (Spinal Diagnostics, n.d.; Central Ohio Spine and Joint, n.d.). Fatty infiltration (visible as a bright signal on T1-weighted images) is highly associated with chronic pain and instability. The degree of infiltration is a crucial prognostic indicator, correlating negatively with functional improvement (Xu et al., 2024). The presence and severity of multifidus fatty infiltration provide powerful objective evidence of chronic functional impairment and instability directly resulting from the traumatic event. I use this finding to prove permanent injury to the core stabilizing system, which is critical for future medical damages.
2.0 Establishing Causality: My Biomechanical and Legal Framework
The defense is designed to argue that a plaintiff’s pain is due to aging or unrelated issues. My documentation provides the scientific and legal rebuttals necessary to establish clear causation—a process I personally manage from the moment the patient walks through my door.
2.1 The “Eggshell Plaintiff” Doctrine: My Documentation Strategy
A foundational principle in personal injury law is the “Eggshell Plaintiff” Rule: a defendant must take the victim as they find them (Cornell Law School, n.d.). This means the defendant is fully liable for the plaintiff’s injuries, even if those injuries are more severe than they would have been in an average person due to an existing, pre-disposed condition (Rafi Law Firm, n.d.).
My Personal Role: Successfully applying this doctrine in court requires meticulous documentation, which I provide by:
Defining the Baseline: Precisely evaluating the pre-accident state (using the Vacuum Disc, Modic 2/3, and chronic osteophyte timelines). I acknowledge the pre-existing state without minimizing the new trauma.
Quantifying the Acute Change: Using Modic Type 1 and Acute-on-Chronic findings to objectively demonstrate the new, causally related injury (Spinal Diagnostics, n.d.).
Proving Exacerbation: Establishing that the traumatic event (MVA) directly aggravated the pre-existing condition, resulting in new symptoms, functional loss, and permanent impairment. My reports meticulously connect the mechanism of injury to the exacerbation, ensuring the court grasps the full scope of liability.
2.2 The Biomechanical Signatures of Soft Tissue and Ligamentous Injury (Whiplash)
Soft tissue injuries, or whiplash-associated disorders (WAD), are commonly challenged as subjective. My examination protocol goes beyond standard range of motion checks to confirm structural injury.
Occult Ligamentous Injury: I utilize the MRI’s fluid-sensitive sequences (STIR) to search for occult tears and sprains. I look for the hyperintense (bright) signal in the interspinous and supraspinous ligaments (Spinal Diagnostics, n.d.), which represents edema and tearing. This finding transforms a subjective “sprain/strain” into an objective, structural instability.
Facet Capsular Edema: The facet joints are often injured during MVA hyperflexion/hyperextension. I meticulously look for capsular edema or effusion (bright signal around the joint) on T2/STIR images. This is a highly specific finding for acute trauma to the joint capsule, which often correlates to localized, severe pain.
The Biomechanical Correlation: I thoroughly document the mechanism of injury (e.g., rear-end collision, specific speed data if available) and link the vector of force to the specific pathology found (e.g., a rear-end vector causing anterior compression and posterior ligamentous tearing) (NCBI, 2023). This correlation is crucial in court to overcome defense arguments that the forces were insufficient to cause the documented injury.
3.0 The Dual-Licensed Advantage: My DC & APRN/FNP-BC Model in El Paso
The most compelling aspect of the Injury Medical Clinic PA model, and the primary reason for my success in the medico-legal field, is my unique qualification as a dual-licensed professional. The integration of the Doctor of Chiropractic (DC) and the Advanced Practice Registered Nurse/Family Nurse Practitioner (APRN/FNP-BC) licenses creates a holistic, comprehensive, and legally powerful care model that is unmatched in the El Paso area.
3.1 Comprehensive Care Models: My Integrated Approach
I bring together the best of both worlds, creating a single source of expertise that satisfies both the clinical and legal standards of care:
My Role as a Chiropractic Physician (DC): I provide unparalleled expertise in spinal biomechanics, functional assessment, manual therapy, and the non-surgical management of complex musculoskeletal injuries. The DC perspective is critical for evaluating the long-term functional impairment caused by disc, facet, and ligament pathology.
My Role as a Nurse Practitioner (APRN/FNP-BC): I provide the essential medical framework, including the ability to prescribe medication (e.g., muscle relaxants, neuropathic agents), order and manage advanced diagnostic testing (e.g., specific, medically-prescribed MRI protocols, nerve conduction studies), manage co-morbidities, and, most crucially, write comprehensive, authoritative medical-legal reports and provide expert testimony that carries the weight of a board-certified medical professional, satisfying the standard medical scrutiny of the court.
This integration ensures the patient receives optimal physical rehabilitation alongside rigorous medical documentation, all under one practice. My reports are medical documents authored by an APRN/FNP-BC, while the therapeutic details reflect the specialized biomechanical insight of a DC. This synergy is invaluable to attorneys.
3.2 Justification for Dual-Licensed Intervention: Case Archetypes in My Practice
I manage these three case archetypes every day, and they demonstrate why my dual-licensed approach is often medically and legally necessary:
Case Archetype
Clinical Presentation in My Clinic
My Dual-Licensed Treatment Rationale
Medico-Legal Value in My Reports
Type 1: Complex Cervical WAD with Radiculopathy.
Patient presents with neck pain, headaches, and confirmed numbness/tingling in the arm. MRI shows a C5-C6 disc bulge impinging on the nerve root.
My DC Expertise: Focus on specific spinal mobilization to reduce segmental dysfunction and restore cervical curve stability. My APRN Expertise: Prescribe gabapentin or NSAIDs for nerve pain, order Electromyography/Nerve Conduction Velocity (EMG/NCV) studies, and administer facet or trigger point injections if necessary (Mayo Clinic, 2024).
Causality: The combined finding of clinical radiculopathy (confirmed by NCV—a medical test I ordered) and the biomechanical trauma (my DC diagnosis) is documented under a single, authoritative medical record (my APRN report). I can objectively testify to the severity of the neurological deficit.
Type 2: Acute Lumbar Disc Extrusion with Failed Conservative Care.
Patient suffers acute L5-S1 disc extrusion causing severe, debilitating sciatica that is not responding to basic care.
My DC Expertise: Implement specialized non-surgical spinal decompression protocols and advanced core stabilization exercises. My APRN Expertise: Medically evaluate the patient’s pain using objective outcome measures (Oswestry Disability Index), rule out Red Flags (Cauda Equina), manage opioid/non-opioid medication, and critically, document the failure of conservative care, which justifies the trajectory toward advanced interventions or surgical consultation.
Damages & Prognosis: My comprehensive documentation of conservative care failure establishes the persistent, debilitating nature of the injury. This robust history is essential for the attorney to justify the valuation of both past and high-value future medical costs in front of a jury.
Type 3: Acute-on-Chronic Spinal Instability.
Patient has pre-existing, asymptomatic spinal stenosis (Modic Type 2 changes), but the MVA results in new symptoms and a new Modic Type 1 change at the adjacent level.
My DC Expertise: Focus on restoring segmental stability to the traumatized level while protecting the degenerated level. My APRN Expertise: Personally interpret the complex MRI (Modic 1 vs. Modic 2) to clearly delineate the acute injury (liability) from the pre-existing condition (eggshell) (Spinal Diagnostics, n.d.).
Defeating the Defense: My precise diagnostic report legally isolates the acute trauma (Modic 1) from the chronic degeneration (Modic 2/Vacuum Disc), providing the attorney with clear, objective evidence to apply the Eggshell Plaintiff doctrine and secure recovery for the aggravation and new injury.
4.0 My Credible Expert Witness Testimony: Illuminating Disability and Driving Monetary Recoveries
My ultimate function for the legal community is to serve as the credible, objective voice that clarifies the patient’s impairment for the jury. My testimony is built upon the synthesis of advanced clinical diagnostics and established medico-legal principles that I personally adhere to.
4.1 The Credibility Foundation: My Daubert-Compliant Testimony
Attorneys frequently utilize my expertise because my methodology is rooted in the scientific method, ensuring my opinions are admissible under the Daubert Standard. My expert testimony is not merely anecdotal; it is a direct presentation of verifiable scientific data:
Measurable Markers: When I testify, I don’t just state an opinion. I point to the imaging and explain that the Modic Type 1 change is not random, but an established scientific finding with a specific 6-8 week timeline, proving the freshness of the bone trauma (Wang et al., 2017). I use analogies, like comparing the Modic 1 change to a fresh bruise on the bone, which makes the complex science undeniable to a layperson jury.
Biomechanically Sound Conclusions: I personally explain how the physics of the impact (the vector, the forces) translates into the specific, demonstrable injury, such as the mechanism by which a sudden flexion-extension event causes an annular tear (Paredes et al., 2023). This link between physics and physiology is critical for proving causation.
The Power of the Dual Role: When I stand before the court, my opinion integrates the highest standard of musculoskeletal diagnosis (DC) with the authority of advanced medical management (APRN). I am uniquely positioned to counter both the defense’s biomechanics expert and their medical expert.
4.2 My Method for Translating Pathology into Permanent Impairment and Disability
The value of a personal injury case is directly linked to the demonstrability and permanency of the injury. My detailed reports translate abstract medical findings into tangible, compelling evidence of long-term disability for the jury.
4.2.1 Quantifying Functional Loss: From Imaging to Activities of Daily Living (ADLs)
I shift the focus from what the injury looks like on an MRI to how it permanently impairs the patient’s life:
Multifidus Fatty Infiltration: I explain to the jury that the increased bright signal on the patient’s T1 MRI is not simply “fat,” but the objective, measurable sign of a permanent loss of spinal stability (Central Ohio Spine and Joint, n.d.). I elaborate that the muscle is no longer functional, leading to chronic instability, increased risk of re-injury, and an inability to perform basic ADLs like prolonged sitting, standing, or lifting—directly correlating to a lower quality of life and permanent functional loss.
Irreversible Cord Damage (Myelomalacia): If I identify Myelomalacia (softening, necrosis, and scarring of the spinal cord tissue) on a T2 image (hyperintensity within the cord), I use this to establish a definitive, catastrophic, permanent neurological injury (Spinal Diagnostics, n.d.). This finding is irreversible and dictates a life of permanent neurological deficits, which is irrefutable evidence of severe disability that warrants significant monetary recovery.
4.2.2 Linking Causality to Prognosis and Future Medical Costs
My reports connect the initial traumatic event to the long-term cost of care. This is vital for the attorney’s calculation of future medical damages.
Permanent Impairment Rating (PIR): I use objective prognostic indicators—such as the severity of multifidus infiltration (Xu et al., 2024), the persistence of Modic 1 changes, or the presence of irreversible ligament instability—to generate a scientifically grounded Permanent Impairment Rating (PIR) using the AMA Guides to the Evaluation of Permanent Impairment.
Future Medical Requirements: The report then outlines the need for future care (e.g., ongoing chiropractic maintenance, periodic APRN follow-ups, medication management, or potential injections/surgical consultations) directly necessitated by the MVA. This robust justification of future needs is critical for maximizing the final settlement or jury award.
By establishing causation, chronicity, and prognosis through my rigorous, peer-reviewed methodology, I provide the unassailable evidence necessary to maximize the plaintiff’s recovery and to position legal counsel to confidently present even the most complex clinical cases before a jury. My role is to ensure that the injury is not only treated effectively but also documented exhaustively, establishing Injury Medical Clinic PA as the premier clinic for injuries resulting from accidents in the El Paso area.
National Institutes of Health (NIH). (2022). Updated Review of the Evidence Supporting the Medical and Legal Use of NeuroQuant® and NeuroGage® in Patients With Traumatic Brain Injury. PMC – PubMed Central. https://pmc.ncbi.nlm.nih.gov/articles/PMC9027332/
Individuals with the autoimmune disease lupus may be more sensitive to sun exposure. Are there ways to help protect the skin?
Lupus Sun Exposure
Lupus is an autoimmune disease in which the body mistakenly attacks the joints, muscles, and skin. Around 5 million individuals worldwide, and 1.5 million in the United States, have been diagnosed with lupus. The disease is most common in early to mid-adulthood, and 90% develop in women. (Lupus Foundation of America, 2021) For some, the symptoms manifest as joint swelling or muscle soreness. Skin rashes, mottling or red or purple marbled skin, and sun sensitivity are common lupus symptoms. (Medline Plus, 2024) While exposure to UV radiation from natural and artificial light can be damaging to everyone, minimal exposures can cause a flare-up for those with chronic lupus.
Certain medications can impact individual sensitivity to the sun and UV radiation.
Sun Exposure
Lupus can increase photosensitivity or immune system reaction to the sun’s rays. This symptom affects 40% and 70% of individuals with lupus. (Lupus Foundation of America, 2021) UV radiation damages cells and alters DNA. However, the damage can be more severe in those with lupus because their cells are more sensitive, and damaged cells are removed from the body more slowly, which can cause an attack on the immune system. (Lupus Foundation of America, 2021)
Symptoms
UV light and certain artificial light sources can trigger reactions in those with lupus. These reactions can happen immediately or develop weeks later and include: (Lupus Foundation of America, 2013)
Rashes or skin lesions that appear after sun exposure can come and go within hours or days, or they can last for months. (Lupus Foundation of America, 2013) UV light can also cause a lupus flare-up of symptoms, including fatigue, joint pain, tingling, and numbness. (Lupus Foundation of America, 2021)
Protection
Protecting the skin from UV radiation is recommended for everyone, but it is especially important for individuals with photosensitivity from lupus. Some strategies to protect the skin include.
Sunscreen
Applying sunscreen to the skin provides a chemical or physical barrier to UV radiation. (MD Anderson, 2024) Most commercial sunscreens offer a combination of protection:
Physical Barriers
These include minerals like titanium dioxide or zinc oxide.
The finely ground minerals lay on top of the skin’s surface and reflect UV rays away.
Chemical Absorbers
These offer a thin, protective film that absorbs UV rays before they can penetrate the skin.
Proper sunscreen application is crucial, regardless of which type is chosen. The recommended application is to apply a palmful of sunscreen every two hours or more often if it gets wet or sweaty. Look for sunscreens that offer broad-spectrum protection against:
Ultraviolet A (UVA) rays
Ultraviolet B (UVB) rays
A sun protection factor (SPF) of at least 30 is recommended.
Most clothing offers protection against UV radiation.
Individuals can purchase clothing or hats with UV-blocking properties or washing products for their clothes to increase their level of UV protection. (American Cancer Society, 2024)
Sunglasses are also important against UV radiation, eye damage, and other problems.
Utilize Shade Areas
In the summer, the sun is strongest in most locations between 10 a.m. and 4 p.m. UV rays can pass through windows, and the body is exposed to UV radiation on cloudy days (American Cancer Society, 2024). Avoiding sunlight or other strong sources of UV radiation will help protect the skin. Staying indoors or in shaded areas is the best choice during these hours.
Seeing a Healthcare Provider
Lupus treatment varies and changes over time. Individuals with lupus schedule regular appointments with their healthcare provider to review treatment and symptoms, especially after sun exposure. Avoiding sun exposure by seeking shade and wearing sunscreen and protective clothing can help reduce the chances of experiencing a flare-up. Some cases of photosensitivity are mild, while others can require more intense treatments to avoid larger flare-ups.
Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop a personalized care plan for each patient through an integrated approach to treating injuries and chronic pain syndromes, improving flexibility, mobility, and agility programs to relieve pain and help return to normal and optimal function. If other treatments are needed, Dr. Jimenez has teamed up with top surgeons, clinical specialists, medical researchers, and rehabilitation providers to provide the most effective treatments.
Unlocking Pain Relief
References
Medline Plus. (2024). Lupus. Retrieved from https://medlineplus.gov/lupus.html
Lupus Foundation of America. (2021). Lupus facts and statistics. https://www.lupus.org/resources/lupus-facts-and-statistics
U.S. Environmental Protection Agency. (2024). Health effects of UV radiation. Retrieved from https://www.epa.gov/sunsafety/health-effects-uv-radiation
Centers for Disease Control and Prevention. (2024). UV radiation. Retrieved from https://www.cdc.gov/radiation-health/features/uv-radiation.html?CDC_AAref_Val=https://www.cdc.gov/nceh/features/uv-radiation-safety/index.html
Lupus Foundation of America. (2021). UV exposure: What you need to know. https://www.lupus.org/resources/uv-exposure-what-you-need-to-know
Lupus Foundation of America. (2013). Research on photosensitivity among people with lupus. https://www.lupus.org/resources/research-on-photosensitivity-among-people-with-lupus
MD Anderson Center. (2024). How does sunscreen work? https://www.mdanderson.org/cancerwise/how-does-sunscreen-work.h00-159698334.html
Skin Cancer Foundation. (2020). Ask the expert: Does sunscreen stay effective after its expiration date? https://www.skincancer.org/blog/ask-the-expert-does-a-sunscreen-stay-effective-after-its-expiration-date/
American Cancer Society. (2024). How do I protect myself from ultraviolet (UV) rays? https://www.cancer.org/cancer/risk-prevention/sun-and-uv/uv-protection.html
When muscle pains and aches present from health conditions, work, exercise, housework, etc., many individuals turn to topical sprays, creams, ointments, and gels to bring relief. Can magnesium spray be beneficial in the fight against neuromusculoskeletal pain?
Magnesium Spray
Magnesium spray is a liquid form of magnesium applied externally to the skin that has been marketed to promote muscle relaxation, improve sleep, and manage migraines. However, studies of its effectiveness have had mixed results. Some studies have shown that topical use can:
Improve chronic muscle and joint pain. Example: fibromyalgia.
Decrease the frequency and severity of nerve pain symptoms. Example: peripheral neuropathy.
Reduce the incidence and severity of an intubation-related sore throat after surgery.
Further studies of various groups are necessary to clarify the optimal dose for each condition and to determine how topical magnesium affects magnesium blood levels.
What is It?
Magnesium is a mineral that has an important role in many of the body’s processes and is essential for the following (Gröber U. et al., 2017)
Nerve transmission
Muscle contraction
Blood pressure regulation
Blood sugar regulation
Protein production
DNA and RNA production
Currently, there is no recommended dosage for topical magnesium use. However, some major health institutions have established a recommended daily amount taken by mouth. Listed are the recommended daily magnesium intake based on age and other factors. (National Institutes of Health Office of Dietary Supplements, 2022)
14 to 18 years old: 410 mg for males, 360 mg for females and when lactating, and 400 mg when pregnant.
19 to 30 years old: 400 mg for males, 310 mg for females and when lactating, and 350 mg when pregnant.
31 to 50 years old: 420 mg for males, 320 mg for females and when lactating, and 360 mg when pregnant.
51 years old and above: 420 mg for males and 320 mg for females.
Although self-care is appropriate for minor injuries or exercise, individuals are encouraged to see their healthcare provider for severe musculoskeletal pain symptoms.
Benefits
Though taking oral magnesium supplements is common, there is limited research on using magnesium on the skin to improve magnesium levels. Studies comparing the absorption of magnesium taken by mouth with the spray applied to the skin require further research. However, some studies look at the localized effect of magnesium spray on improving a sore throat after surgery and nerve, muscle, and joint pain.
Intubation-Related Sore Throat
Topical magnesium reduced the severity of sore throat after surgery in individuals undergoing tracheal intubation compared to a placebo. (Kuriyama, A. et al., 2019) However, further studies are necessary to clarify the optimal dose.
Nerve Pain
Peripheral neuropathy is nerve damage that causes a tingling and numbing sensation in the arms or legs. In a study of individuals with chronic kidney disease, the daily application of magnesium sprays to limbs affected by peripheral neuropathy for twelve weeks decreased the frequency and severity of nerve pain symptoms. However, one limitation was that it was performed mostly in females. (Athavale, A. et al., 2023)
Chronic Muscle and Joint Pain
A small study assessed whether applying magnesium to the skin could improve the quality of life of female participants with fibromyalgia – a chronic condition that causes muscle and joint pain, fatigue, and other symptoms. The study found that four sprays of magnesium chloride applied twice daily to the upper and lower limbs for four weeks could benefit those with fibromyalgia. However, further research with larger studies is needed to confirm the results. (Engen D. J. et al., 2015)
Does The Spray Increase Overall Magnesium Levels?
Magnesium is transported into cells through magnesium transporters. The outer layer of the skin does not contain these transporters, so absorption occurs in the small areas of the sweat glands and hair follicles. (Gröber U. et al., 2017) One study suggested that applying magnesium to the skin can help with magnesium deficiency within four to six weeks, compared to four to 12 months in the case of oral magnesium supplementation. However, there is minimal research on topical magnesium and its impact on magnesium levels. Another study suggested that 56 mg of magnesium cream applied daily on the skin for 14 days had no statistically significant effect on magnesium blood levels. Although the results were statistically insignificant, a clinically relevant increase in magnesium blood levels was observed. (Kass, L. et al., 2017) Because it remains unclear if magnesium absorption via the skin is more effective than by mouth, further studies are necessary to confirm the amount of magnesium absorbed into the skin.
Using The Spray
In one study, a magnesium chloride solution was poured into a spray bottle and applied as follows (Engen D. J. et al., 2015)
The solution was sprayed into the palm and applied evenly on the affected area.
There is a four-hour wait time between spray dose applications.
Individuals should wait at least one hour after application before showering or washing the product off.
Leave the product on the skin throughout the day and wash it off before bed.
Rinse the solution off with water if the skin becomes irritated.
Avoid applying to open wounds.
Precautions
Avoid magnesium chloride sprays if you are allergic to them or their components. If you have a severe allergic reaction, such as itching, hives, or shortness of breath, seek immediate medical attention. Topically applied magnesium solution has no known side effects other than skin irritation. (Engen D. J. et al., 2015)
Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop a personalized treatment plan through an integrated approach to treating injuries and chronic pain syndromes, improving flexibility, mobility, and agility programs to relieve pain and help individuals return to optimal function. If other treatments are needed, Dr. Jimenez has teamed up with top surgeons, clinical specialists, medical researchers, and rehabilitation providers to provide the most effective treatments.
Why Choose Chiropractic?
References
Gröber, U., Werner, T., Vormann, J., & Kisters, K. (2017). Myth or Reality-Transdermal Magnesium?. Nutrients, 9(8), 813. https://doi.org/10.3390/nu9080813
National Institutes of Health Office of Dietary Supplements. (2022). Magnesium. Retrieved from https://ods.od.nih.gov/factsheets/Magnesium-HealthProfessional/#h2
Kuriyama, A., Maeda, H., & Sun, R. (2019). Topical application of magnesium to prevent intubation-related sore throat in adult surgical patients: a systematic review and meta-analysis. Application topique de magnésium pour prévenir les maux de gorge liés à l’intubation chez les patients chirurgicaux adultes: revue systématique et méta-analyse. Canadian journal of anaesthesia = Journal canadien d’anesthesie, 66(9), 1082–1094. https://doi.org/10.1007/s12630-019-01396-7
Athavale, A., Miles, N., Pais, R., Snelling, P., & Chadban, S. J. (2023). Transdermal Magnesium for the Treatment of Peripheral Neuropathy in Chronic Kidney Disease: A Single-Arm, Open-Label Pilot Study. Journal of palliative medicine, 26(12), 1654–1661. https://doi.org/10.1089/jpm.2023.0229
Engen, D. J., McAllister, S. J., Whipple, M. O., Cha, S. S., Dion, L. J., Vincent, A., Bauer, B. A., & Wahner-Roedler, D. L. (2015). Effects of transdermal magnesium chloride on quality of life for patients with fibromyalgia: a feasibility study. Journal of integrative medicine, 13(5), 306–313. https://doi.org/10.1016/S2095-4964(15)60195-9
Kass, L., Rosanoff, A., Tanner, A., Sullivan, K., McAuley, W., & Plesset, M. (2017). Effect of transdermal magnesium cream on serum and urinary magnesium levels in humans: A pilot study. PloS one, 12(4), e0174817. https://doi.org/10.1371/journal.pone.0174817
How do healthcare professionals in a chiropractic clinic provide a clinical approach to preventing medical errors for individuals in pain?
Introduction
Medical errors resulted in 44,000–98,000 hospitalized American deaths annually, and many more caused catastrophic injuries. (Kohn et al., 2000) This was more than the number of people who died annually from AIDS, breast cancer, and auto accidents at the time. According to later research, the actual number of deaths may be closer to 400,000, placing medical errors as the third most common cause of death in the US. Frequently, these mistakes are not the product of medical professionals who are inherently bad; rather, they are the outcome of systemic issues with the health care system, such as inconsistent provider practice patterns, disjointed insurance networks, underutilization or absence of safety protocols, and uncoordinated care. Today’s article looks at the clinical approach to preventing a medical error in a clinical setting. We discuss associated medical providers specializing in various pretreatments to aid individuals suffering from chronic issues. We also guide our patients by allowing them to ask their associated medical providers very important and intricate questions. Dr. Alex Jimenez, DC, only utilizes this information as an educational service. Disclaimer
Defining Medical Errors
Determining what medical error is the most crucial step in any conversation about preventing medical errors. You might assume this is a very easy chore, but that is only until you delve into the vast array of terminology utilized. Many terms are used synonymously (sometimes mistakenly) since some terminology is interchangeable, and occasionally, the meaning of a term depends on the specialty being discussed.
Even though the healthcare sector stated that patient safety and eliminating or reducing medical errors were priorities, Grober and Bohnen noted as recently as 2005 that they had fallen short in one crucial area: determining the definition of “perhaps the most fundamental question… What is a medical error? A medical error is a failure to complete a planned action in a medical setting. (Grober & Bohnen, 2005) However, none of the terms that one would often identify expressly with a medical error—patients, healthcare, or any other element—are mentioned in this description. Despite this, the definition offers a solid framework for further development. As you can see, that specific definition consists of two parts:
An execution error: A failure to complete a planned action as intended.
A planning error: is a technique that, even with perfect execution, does not produce the desired results.
The concepts of faults of execution and planning errors are insufficient if we are to define a medical error adequately. These may occur anywhere, not only at a medical establishment. The component of medical management must be added. This brings up the idea of unfavorable occurrences, known as adverse events. The most common definition of an adverse event is unintentional harm to patients brought about by medical therapy rather than their underlying disease. This definition has gained international acceptance in one way or another. For example, in Australia, the term incidents are defined as in which harm resulted in a person receiving health care. These consist of infections, injury-causing falls, and issues with prescription drugs and medical equipment. Certain unfavorable occurrences might be avoidable.
Common Types of Medical Errors
The only issue with this notion is that not all negative things happen accidentally or intentionally. Because the patient may ultimately benefit, an expected but tolerated adverse event may occur. During chemotherapy, nausea and hair loss are two examples. In this instance, refusing the recommended treatment would be the only sensible approach to prevent the unpleasant consequence. We thus arrive at the concept of preventable and non-preventable adverse occurrences as we further refine our definition. It isn’t easy to categorize a choice to tolerate one impact when it is determined that a favorable effect will occur simultaneously. But purpose alone isn’t necessarily an excuse. (Patient Safety Network, 2016, para.3) Another example of a planned mistake would be a right foot amputation due to a tumor on the left hand, which would be accepting a known and predicted unfavorable event in the hopes of a beneficial consequence where none has ever arisen before. There is no evidence to support the anticipation of a positive outcome.
Medical errors that cause harm to the patient are typically the focus of our research. Nonetheless, medical mistakes can and do occur when a patient is not harmed. The occurrence of near misses could provide invaluable data when planning how to reduce medical errors in a healthcare facility. Still, the frequency of these events compared to the frequency clinicians report them needs to be investigated. Near misses are medical errors that could have caused harm but did not to the patient, even if the patient is doing well. (Martinez et al., 2017) Why would you acknowledge something that could potentially result in legal action? Consider the scenario where a nurse, for whatever reason, had just been looking at photographs of different medications and was about to provide a medication. Maybe something lingers in her memory, and she decides that’s not how a specific medication looks. Upon checking, she found that the incorrect medicines had been administered. After checking all the paperwork, she fixes the mistake and gives the patient the right prescription. Would it be possible to avoid an error in the future if the administration record included photographs of the proper medication? It is easy to forget that there was a mistake and a chance for harm. That fact remains true regardless of whether we were fortunate enough to find it in time or suffer any negative consequences.
Errors of Outcomes & Process
We need complete data to develop solutions that improve patient safety and decrease medical errors. At the very least, when the patient is in a medical facility, everything that can be done to prevent harm and put them in danger should be reported. Many doctors have determined that using the phrases errors and adverse events was more comprehensive and suitable after reviewing mistakes and adverse events in health care and discussing their strengths and weaknesses in 2003. This combined definition would increase data gathering, including mistakes, close calls, near misses, andactive and latent errors. Additionally, the term adverse events includes terms that usually imply patient harm, such as medical injury and iatrogenic injury. The only thing that remains is determining whether a review board is a suitable body to handle the separation of preventable and non-preventable adverse events.
A sentinel event is an occurrence where reporting to the Joint Commission is required. The Joint Commission states that a sentinel event is an unexpected occurrence involving a serious physical or psychological injury. (“Sentinel Events,” 2004, p.35) There isn’t a choice, as it needs to be documented. Most healthcare facilities, however, do keep their records outlining sentinel incidents and what to do in the event of one to guarantee that the Joint Commission standards are met. This is one of those situations when it’s better to be safe than sorry. Since “serious” is a relative concept, there may be some wriggle room when defending a coworker or an employer. On the other hand, reporting a sentinel event incorrectly is better than failing to report a sentinel event. Failing to disclose can have serious consequences, including career termination.
When considering medical errors, people frequently make the mistake of focusing just on prescription errors. Medication errors are undoubtedly frequent and involve many of the same procedural flaws as other medical errors. Breakdowns in communication, mistakes made during prescription or dispensing, and many other things are possible. But we would be gravely misjudging the issue if we assumed that drug errors are the only cause of harm to a patient. One major challenge in classifying the different medical errors is determining whether to classify the error based on the procedure involved or the consequence. It is acceptable to examine those classifications here, given numerous attempts have been made to develop working definitions that incorporate both the process and the outcome, many of which are based on Lucian Leape’s work from the 1990s.
Enhance Your Lifestyle Today- Video
Analyzing & Preventing Medical Errors
Operative and nonoperative were the two main categories of adverse events that Leape and his colleagues distinguished in this study. (Leape et al., 1991) Operative problems included wound infections, surgical failures, non-technical issues, late complications, and technical difficulties. Nonoperative: headings such as medication-related, misdiagnosed, mistreated, procedure-related, fall, fracture, postpartum, anesthesia-related, neonatal, and a catch-all heading of the system were included under this category of adverse occurrences. Leape also classified errors by pointing out the point of process breakdown. He also categorized these into five headings, which include:
System
Performance
Drug Treatment
Diagnostic
Preventative
Many process faults fall under more than one topic, yet they all help to pinpoint the exact cause of the issue. If more than one physician was engaged in determining the precise areas that need improvement, then additional questioning might be required.
Technically, a medical error can be made by any staff member at a hospital. It is not limited to medical professionals like physicians and nurses. An administrator may unlatch a door, or a cleaning crew member could leave a chemical within a child’s grasp. What matters more than the identity of the perpetrator of the mistake is the reason behind it. What before it? And how can we make sure that doesn’t occur again? After gathering all the above data and much more, it’s time to figure out how to prevent similar errors. As for sentinel events, the Joint Commission has mandated since 1997 that all of these incidents undergo a procedure called Root Cause Analysis (RCA). However, using this procedure for incidents that need to be reported to outside parties would need to be corrected.
What Is A Root Cause Analysis?
RCAs “captured the details as well as the big picture perspective.” They make evaluating systems easier, analyzing whether remedial action is necessary, and tracking trends. (Williams, 2001) What precisely is an RCA, though? By examining the events that led to the error, an RCA can focus on events and processes rather than reviewing or placing blame on specific people. (AHRQ,2017) This is why it is so crucial. An RCA frequently makes use of a tool called the Five Whys. This is the process of continuously asking yourself “why” after you believe you have determined the cause of an issue.
The reason it’s called the “five whys” is because, while five is an excellent starting point, you should always question why until you identify the underlying cause of the problem. Asking why repeatedly could reveal many process faults at different stages, but you should keep asking why about every aspect of the issue until you run out of other things that could be adjusted to provide a desirable result. However, different tools besides this one can be utilized in a root cause investigation. Numerous others exist. RCAs must be multidisciplinary and consistent and involve all parties involved in the error to avoid misunderstandings or inaccurate reporting of occurrences.
Conclusion
Medical errors in healthcare institutions are frequent and mostly unreported events that seriously threaten patients’ health. Up to a quarter of a million individuals are thought to pass away each year as a result of medical blunders. These statistics are unacceptable in a time when patient safety is supposedly the top priority, but not much is being done to alter practices. If medical errors are accurately defined and the root cause of the problem is found without assigning blame to specific staff members, this is unnecessary. Essential changes can be made when fundamental causes of system or process faults are correctly identified. A consistent, multidisciplinary approach to root cause analysis that uses frameworks like the five whys to delve down until all issues and defects are revealed is a helpful tool. Although it is now necessary for the wake of sentinel events, the Root Cause Analysis may and should be applied to all mistake causes, including near misses.
Kohn, L. T., Corrigan, J., Donaldson, M. S., & Institute of Medicine (U.S.). Committee on Quality of Health Care in America. (2000). To err is human : building a safer health system. National Academy Press. http://books.nap.edu/books/0309068371/html/index.html
Leape, L. L., Brennan, T. A., Laird, N., Lawthers, A. G., Localio, A. R., Barnes, B. A., Hebert, L., Newhouse, J. P., Weiler, P. C., & Hiatt, H. (1991). The nature of adverse events in hospitalized patients. Results of the Harvard Medical Practice Study II. N Engl J Med, 324(6), 377-384. https://doi.org/10.1056/NEJM199102073240605
Martinez, W., Lehmann, L. S., Hu, Y. Y., Desai, S. P., & Shapiro, J. (2017). Processes for Identifying and Reviewing Adverse Events and Near Misses at an Academic Medical Center. Jt Comm J Qual Patient Saf, 43(1), 5-15. https://doi.org/10.1016/j.jcjq.2016.11.001
Nowadays, individuals trying to avoid surgery have more therapy options. Can regenerative medicine help treat neuromusculoskeletal injuries?
Regenerative Medicine
Regenerative medicine utilizes the body’s raw cells and is used in cancer treatment and to reduce the risk of infections. (American Cancer Society. 2020) Researchers are looking for other ways to use these cells in medical therapies.
What are These Cells
Stem cells are unspecialized cells that can develop into any cell and in certain cases renew themselves an unlimited number of times. (National Institutes of Health. 2016)
Regenerative cell therapy uses these cells as a treatment for a disease or condition.
Regenerative cells are given to individuals to replace cells that have been destroyed or have died.
In the case of cancer, they may be used to help the body regain the ability to produce regenerative cells after treatment. (American Cancer Society. 2020)
For individuals with multiple myeloma and certain types of leukemia, regenerative cell therapy is used to eliminate cancer cells.
The therapy is called graft-versus-tumor effect/GvT, where a donor’s white blood cells/WBCs are used to eliminate the cancerous tumor. (American Cancer Society. 2020)
What They Can Treat
This is a new treatment that is still going through research. The Food and Drug Administration has only approved it for certain cancers and conditions that affect the blood and immune system. (Centers for Disease Control and Prevention. 2019) Regenerative cell therapy is FDA-approved to treat: (National Cancer Institute. 2015)
Leukemia
Lymphoma
Multiple myeloma
Neuroblastoma
It is also used to decrease the risk of infection after regenerative cell transplantation in individuals with blood cancers. (U.S. Food & Drug Administration. 2023)
Researchers are studying how these cells can treat other conditions. Clinical trials are analyzing how to use the therapy for neurodegenerative diseases like:
During regenerative cell therapy, the cells are given through an intravenous line. The three places where blood-forming cells can be obtained are bone marrow, the umbilical cord, and blood. Transplants can include: (American Cancer Society. 2020)
Autologous
The cells are taken from the individual who will be receiving the therapy.
Allogeneic
The cells are donated by another individual.
Syngeneic
The cells come from an identical twin, if there is one.
Safety
The therapy has shown to provide benefits but there are risks.
One risk is known as graft-versus-host disease – GVHD.
It occurs in one-third to half of allogeneic recipients.
This is where the body does not recognize the donor’s white blood cells and attacks them causing problems and symptoms throughout the body.
To treat GVHD medications are given to suppress the immune system to stop attacking the donor cells. (American Cancer Society. 2020)
The future of regenerative cell therapy is promising. Research is ongoing to find out how these cells can treat conditions and find new ways to treat and cure diseases.
Regenerative medicine has been researched for over twenty years for conditions like macular degeneration, glaucoma, stroke, and Alzheimer’s disease. (National Institutes of Health. 2022) This therapy is a new medical treatment that could be used in future therapies as part of a multidisciplinary approach to neuromusculoskeletal injuries and conditions.
Stretching Objective: The body needs to be flexible to maintain a full range of motion. Stretching keeps the muscles supple, strong, and healthy; without it, the muscles shorten and become stiff and tight. Then, when the muscles are needed, they are weak and unable to extend fully. This increases the risk of joint pain, strains, injuries, and muscle damage. For example, sitting in a chair for a long time results in tight glute muscles and hamstrings, which leads to back discomfort symptoms and inhibits walking. Injury Medical Chiropractic and Functional Medicine Clinic can help individuals develop a personalized stretching program to maintain smooth mobility, flexibility, and function.
Stretching Objective
Benefits
The body needs to be flexible to maintain mobility, balance, and independence. The benefits of regularly stretching include:
When the muscles are stretched, so are the muscle spindles. The spindle records the change in length and speed and transmits the signals through the spinal cord, which conveys the information. This triggers the stretch reflex, which tries to resist the change by causing the stretched muscle to contract. Muscle spindle function helps maintain muscle tone and protects the body from injury. One of the reasons for holding a stretch for a specific amount of time is because, as the muscle stays in a stretched position, the spindle acclimates to the new condition and reduces its resistance signaling, gradually training the stretch receptors to allow greater lengthening of the muscles.
Chiropractic Stretch Training
However, stretching once won’t generate maximum flexibility. Tight muscles may have taken months or years to develop; therefore, it will take time to achieve flexibility and must be continually worked on to maintain it. Chiropractors and physical therapists are body movement experts and can assess individual muscle strength and develop a customized stretching program.
Muscle Spindle Activation
References
Bhattacharyya, Kalyan B. “The stretch reflex and the contributions of C David Marsden.” Annals of Indian Academy of Neurology vol. 20,1 (2017): 1-4. doi:10.4103/0972-2327.199906
Behm, David G et al. “Acute effects of muscle stretching on physical performance, range of motion, and injury incidence in healthy active individuals: a systematic review.” Applied physiology, nutrition, and metabolism = Physiologie applique, nutrition et metabolism vol. 41,1 (2016): 1-11. doi:10.1139/apnm-2015-0235
Berg, K. Stretching fundamentals. In: Prescriptive Stretching. 2nd ed. Kindle edition. Human Kinetics; 2020.
da Costa, Bruno R, and Edgar Ramos Vieira. “Stretching to reduce work-related musculoskeletal disorders: a systematic review.” Journal of rehabilitation medicine vol. 40,5 (2008): 321-8. doi:10.2340/16501977-0204
Page, Phil. “Current concepts in muscle stretching for exercise and rehabilitation.” International journal of sports physical therapy vol. 7,1 (2012): 109-19.
Witvrouw, Erik, et al. “Stretching and injury prevention: an obscure relationship.” Sports medicine (Auckland, N.Z.) vol. 34,7 (2004): 443-9. doi:10.2165/00007256-200434070-00003
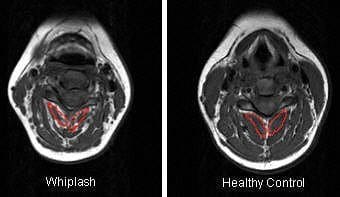
Studies on the effectiveness of chiropractic care for patients afflicted with pain secondary to whiplash injury are emerging. In 1996, Woodward et al. published a study on the efficacy of chiropractic treatment of whiplash injuries.
In 1994, Gargan and Bannister published a paper on the recovery rate of patients and found that when patients were still symptomatic after three months, there was almost a 90% chance they would remain injured. The study’s authors were from the Department of Orthopedic Surgery in Bristol, England. No conventional treatment was shown to be effective in these based chronic whiplash injury patients. However, high success rates have been found by whiplash injury patients through chiropractic care in recovering these types of patients.
Whiplash Treatment Study Results
In the Woodward study, 93 percent of the 28 patients studied retrospectively were found to have a statistically significant improvement following chiropractic care. Chiropractic care in this study consisted of PNF, spinal manipulation, and cryotherapy. Most of the 28 patients had prior therapy with NSAIDs collars and physiotherapy. The average length of time before when the patients began chiropractic care was 15.5 months post-MVA (range of 3-44 months).
This study documented what most DCs experience in clinical practice: chiropractic care is effective for individuals hurt in a motor vehicle accident. Symptoms ranging from headaches to back pain, neck pain, interscapular pain, and extremity pain related to paresthesias all responded to quality chiropractic care.
Normal & Whiplash X-Rays
Whiplash MRI Findings
The literature has also suggested cervical disc injuries aren’t uncommon after a whiplash injury. In a study published on chiropractic care for disk herniations, it was demonstrated that patients improve clinically and that repeated MRI imaging often shows decreased size or resolution of the disk herniation. Of the 28 patients studied and followed, many had disc herniations that reacted well to chiropractic care.
In a recent retrospective study by Khan et al., published in the Journal of Orthopedic Medicine, on whiplash-injured patients concerning cervical pain and dysfunction, patients were stratified into groups based on levels of a good outcome to chiropractic care:
Group I: Patients with neck pain only and restricted neck ROM. Patients had a “coat hangar” distribution of pain with no neurologic deficits; 72 percent had a fantastic outcome.
Group II: Patients with neurological symptoms or signs and limited spinal ROM. Patients had numbness, tingling, and paresthesias in the extremity.
Group III: Patients had severe neck pain with full neck ROM and bizarre pain distributions from the extremities. These patients often described chest pain, nausea, vomiting, blackouts, and dysfunction.
The results of the study showed that in class I, 36/50 patients (72%) reacted well to chiropractic care: in group II, 30/32 patients (94 percent) responded well to chiropractic care; and in group III, only 3/11 instances (27%) responded well to chiropractic care. There was a significant difference in outcomes between the three groups.
This study provides new evidence that chiropractic care is effective for whiplash-injured patients. However, the study didn’t consider patients with back injuries, extremity injuries, and TMJ injuries. It did not identify which patients had disc injuries, radiculopathy, and concussive brain injury (most likely group III patients). These types of patients respond better to a model of chiropractic care in combination with multidisciplinary providers.
These studies show what most DCs have already experienced, that the doctor of chiropractic should be the principal care provider in these cases. It’s a common opinion that in cases like group III patients, care should be multidisciplinary to achieve the best possible outcome in difficult scenarios.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please ask Dr. Jimenez or contact us at 915-850-0900.By Dr. Alex Jimenez
Additional Topics: Automobile Accident Injuries
Whiplash, among other automobile accident injuries, is frequently reported by victims of an auto collision, regardless of the severity and grade of the accident. Whiplash is generally the result of an abrupt, back-and-forth jolt of the head and neck in any direction. The sheer force of an impact can cause damage or injury to the cervical spine and the rest of the spine. Fortunately, a variety of treatments are available to treat automobile accident injuries.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine









 Stretching Objective
Stretching Objective