James Hill, father and teacher to two older sons and a younger daughter called Madison Hill, belong to an athletic family. Madison began participating in several sports because she had been a young woman, but she consequently experienced numerous sports injuries. Luckily, James Hill and his daughter Madison Hill went to go to Dr. Alex Jimenez and he has tremendously helped her recover after every injury she experiences. Collectively, they’ve learned to trust in chiropractic care, particularly following Dr. Alex Jimenez’s innovative treatment techniques and procedures. Mr. Hill expresses his gratitude in addition to how far Dr. Alex Jimenez’s understanding in sports injury therapy has greatly enlarged his general comprehension of the human body’s healing process. After Madison suffered a recent ankle sprain, she was instantly reassured by Dr. Alex Jimenez regarding how much faster she’d return-to-play during chiropractic care. James Hill and Madison Hill highly recommend Dr. Alex Jimenez as the non-surgical selection for volleyball sports injuries, among others..
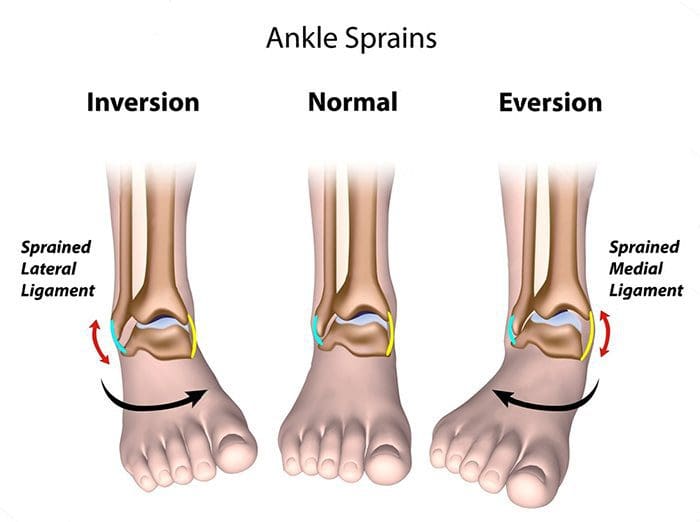
Chiropractor Ankle Sprain Treatment
Every year, millions of young athletes engage in high school sports. However, once an injury occurs, it might develop into an issue that might result in them having to discontinue their particular sport or physical activity if not treated properly. The pressure to continue participating in the sport or physical activity may cause young athletes not to follow proper recovery guidelines, which might subsequently result in more injury with long-term consequences. Sports injuries among young athletes fall into two key categories: overuse injuries and acute injuries. Both kinds include injuries to the soft tissues and bones. Whether an injury is acute or due to overuse, a young athlete who develops a symptom which impacts their athletic performance should be diagnosed appropriately by a health care professional. Sports accidents which are untreated can lead to permanent disability. Many high school sports injuries can be avoided through appropriate instruction and conditioning.
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
If you have enjoyed this video and/or we have helped you in any way please feel free to subscribe and recommend�us.
Difficulty making eye contact, gestures and words at the same time
Little imitation of others
No longer uses words they used to use
Uses another person�s hand as a tool
Social Interaction
Difficulty making eye contact
Lack of joyful expression
Lack of responsiveness to name
Does not try to show you things they�re interested in
Repetitive Behaviors & Restricted Interests
Unusual way of moving their hands, fingers or body
Develops rituals, such as lining up objects or repeating things
Focuses on unusual objects
Excessive interest in a particular object or activity which interferes with social interaction
Unusual sensory interests
Under or over reaction to sensory input
ASD Diagnostic Criteria (DSM-5)
Persistent deficits in social communication and social interaction across multiple contexts, as manifested by the following, currently or by history (examples are illustrative, not exhaustive; see text):
Deficits in social-emotional reciprocity, ranging, for example, from abnormal social approach and failure of normal back-and-forth conversation; to reduced sharing of interests, emotions, or affect; to failure to initiate or respond to social interactions.
Deficits in nonverbal communicative behaviors used for social interaction, ranging, for example, from poorly integrated verbal and nonverbal communication; to abnormalities in eye contact and body language or deficits in understanding and use of gestures; to a total lack of facial expressions and nonverbal communication.
Deficits in developing, maintaining, and understand relationships, ranging, for example, from difficulties adjusting behavior to suit various social contexts; to difficulties in sharing imaginative play or in making friends; to absence of interest in peers.
ASD Diagnostic Criteria
Restricted, repetitive patterns of behavior, interests, or activities, as manifested by at least two of the following, currently or by history (examples are illustrative, not exhaustive; see text):
Stereotyped or repetitive motor movements, use of objects, or speech (e.g., simple motor stereotypes, lining up toys or flipping objects, echolalia, idiosyncratic phrases).
Insistence on sameness, inflexible adherence to routines, or ritualized patterns of verbal or nonverbal behavior (e.g., extreme distress at small changes, difficulties with transitions, rigid thinking patterns, greeting rituals, need to take same route or eat same food every day).
Highly restricted, fixated interests that are abnormal in intensity or focus (e.g., strong attachment to or preoccupation with unusual objects, excessively circumscribed or perseverative interests).
Hyper – or Hyporeactivity to sensory input or unusual interest in sensory aspects of the environment (e.g. apparent indifference to pain/temperature, adverse response to specific sounds or textures, excessive smelling or touching of objects, visual fascination with lights or movement).
ASD Diagnostic Criteria
Symptoms must be present in the early developmental period (but may not become fully manifest until social demands exceed limited capacities, or may be masked by learned strategies in later life).
Symptoms cause clinically significant impairment in social, occupational, or other important areas of current functioning.
These disturbances are not better explained by intellectual disability (intellectual developmental disorder) or global developmental delay. Intellectual disability and autism spectrum disorder frequently co-occur; to make comorbid diagnoses of autism spectrum disorder and intellectual disability, social communication should be below that expected for general developmental level.
ASD Diagnostic Criteria (ICD- 10)
A. Abnormal or impaired development is evident before the age of 3 years in at least one of the following areas:
Receptive or expressive language as used in social communication;
The development of selective social attachments or of reciprocal social interaction;
Functional or symbolic play.
B. A total of at least six symptoms from (1), (2) and (3) must be present, with at least two from (1) and at least one from each of (2) and (3)
1. Qualitative impairment in social interaction are manifest in at least two of the following areas:
a. failure adequately to use eye-to-eye gaze, facial expression, body postures, and gestures to regulate social interaction;
b. failure to develop (in a manner appropriate to mental age, and despite ample opportunities) peer relationships that involve a mutual sharing of interests, activities and emotions;
c. lack of socio-emotional reciprocity as shown by an impaired or deviant response to other people�s emotions; or lack of modulation of behavior according to
social context; or a weak integration of social, emotional, and communicative behaviors;
d. lack of spontaneous seeking to share enjoyment, interests, or achievements with other people (e.g. a lack of showing, bringing, or pointing out to other people objects of interest to the individual).
2. Qualitative abnormalities in communication as manifest in at least one of the following areas:
a. delay in or total lack of, development of spoken language that is not accompanied by an attempt to compensate through the use of gestures or mime as an alternative mode of communication (often preceded by a lack of communicative babbling);
b. relative failure to initiate or sustain conversational interchange (at whatever level of language skill is present), in which there is reciprocal responsiveness to the communications of the other person;
c. stereotyped and repetitive use of language or idiosyncratic use of words or phrases;
d. lack of varied spontaneous make-believe play or (when young) social imitative play
3. Restricted, repetitive, and stereotyped patterns of behavior, interests, and activities are manifested in at least one of the following:
a. An encompassing preoccupation with one or more stereotyped and restricted patterns of interest that are abnormal in content or focus; or one or more interests that are abnormal in their intensity and circumscribed nature though not in their content or focus;
b. Apparently compulsive adherence to specific, nonfunctional routines or rituals;
c. Stereotyped and repetitive motor mannerisms that involve either hand or finger flapping or twisting or complex whole body movements;
d. Preoccupations with part-objects of non-functional elements of play materials (such as their oder, the feel of their surface, or the noise or vibration they
generate).
C. The clinical picture is not attributable to the other varieties of pervasive developmental disorders; specific development disorder of receptive language (F80.2) with secondary socio-emotional problems, reactive attachment disorder (F94.1) or disinhibited attachment disorder (F94.2); mental retardation (F70-F72) with some associated emotional or behavioral disorders; schizophrenia (F20.-) of unusually early onset; and Rett�s Syndrome (F84.12).
Asperger�s Syndrome Diagnostic Criteria (ICD-10)
A. Qualitative impairment in social interaction, as manifested by at least two of the following:
marked impairments in the use of multiple nonverbal behaviors such as eye-to-eye gaze, facial expression, body postures, and gestures to regulate social interaction.
failure to develop peer relationships appropriate to developmental level.
a lack of spontaneous seeking to share enjoyment, interests, or achievements with other people (e.g. by a lack of showing, bringing, or pointing out objects of interest to other people).
lack of social or emotional reciprocity.
B. Restricted repetitive and stereotyped patterns of behavior, interests, and activities, as manifested by at least one of the following:
encompassing preoccupation with one or more stereotyped and restricted patterns of interest that is abnormal either in intensity or focus.
apparently inflexible adherence to specific, nonfunctional routines or rituals.
stereotyped and repetitive motor mannerisms (e.g., hand or finger flapping or twisting, or complex whole-body movements).
persistent preoccupation with parts of objects.
C. The disturbance causes clinically significant impairment in social, occupational, or other important areas of functioning
D. There is no clinically significant general delay in language (e.g., single words used by age 2 years, communicative phrases used by age 3 years).
E. There is no clinically significant delay in cognitive development or in the development of age-appropriate self- help skills, adaptive behavior (other than social interaction), and curiosity about the environment in childhood.
F. Criteria are not met for another specific Pervasive Developmental Disorder or Schizophrenia.
Attention-Deficit/Hyperactivity Disorder (ADHD)
Inattention – gets off task easily
Hyperactivity – seems to move about constantly
Impulsivity – makes hasty actions that occur in the moment without first thinking about them
ADHD Risk Factors
Genetics
Cigarette smoking, alcohol use, or drug use during pregnancy
Exposure to environmental toxins during pregnancy
Exposure to environmental toxins, such as high levels of lead, at a young age
Somatic signs including sleep disturbances, enuresis or urinary frequency
*The onset of PANS may start with infectious agents other than strep. It also includes onset from environmental triggers or immune dysfunction
Pediatric Autoimmune Disorders Associated With Streptococcus
(PANDAS)
Presence of significant obsessions, compulsions and/or tics
Abrupt onset of symptoms or a relapsing-remitting course of symptom severity
Pre-pubertal onset
Association with streptococcal infection
Association with other neuropsychiatric symptoms (including any of the PANS �accompanying� symptoms)
PANS/PANDAS Tests
Swab/Strep culture
Blood tests for strep
Strep ASO
Anti-DNase B Titer
Streptozyme
Test for other infectious agents
MRI preferred but PET can be used if necessary
EEG
False Negatives
Not all children who have strep have elevated labs
Only 54% of children with strep showed a significant increase in ASO.
Only 45% showed an increase in anti�DNase B.
Only 63% showed an increase in either ASO and/or anti�DNase B.
Treatment Of PANS/PANDAS
Antibiotics
IVIG
Plasmaphoresis
Anti-Inflammatory protocols
Steroid medications
Omega-3’s
NSAIDS
Probiotics
Injury Medical Clinic: Chiropractor (Recommended)
Sources
�Attention Deficit Hyperactivity Disorder.� National Institute of Mental Health, U.S. Department of Health and Human Services, www.nimh.nih.gov/health/topics/attention-deficit-hyperactivity-disorder-adhd/index.shtml.
Autism Navigator, www.autismnavigator.com/.
�Autism Spectrum Disorder (ASD).� Centers for Disease Control and Prevention, Centers for Disease Control and Prevention, 29 May 2018, www.cdc.gov/ncbddd/autism/index.html.
�Introduction to Autism.� Interactive Autism Network, iancommunity.org/introduction-autism.
Shet, Anita, et al. �Immune Response to Group A Streptococcal C5a Peptidase in Children: Implications for Vaccine Development.� The Journal of Infectious Diseases, vol. 188, no. 6, 2003, pp. 809�817., doi:10.1086/377700.
�What Is PANDAS?� PANDAS Network, www.pandasnetwork.org/understanding-pandaspans/what-is-pandas/.
Unfortunately, there are no stretches for� Root canals or Kidney stones. But there are stretches for Piriformis syndrome.
These ailments are painful and no fun! Piriformis syndrome�is especially a pain, in the butt, no pun intended.
Seriously, people suffering from Piriformis syndrome have frequent and sometimes severe pain and numbness through the buttocks and down their legs. This occurs when the Piriformis muscle spasms. When this happens, it�can end up also aggravating the sciatic nerve, which compounds the pain with tingling and numbness.
The Piriformis�is a short, small�muscle deep inside our hips, and helps rotate our legs both outward and inward. Because of its proximity to the sciatic nerve, this little body part can cause big problems, and hinder our ability to run, or even walk, through our daily activities with ease.
Fortunately, there are a variety of exercises that help stretch and relax the Piriformis muscle, giving sufferers much-needed relief from the pain and numbness it causes. If you are dealing with Piriformis syndrome, try these stretches to get yourself back on your feet and moving, pain-free.
Stretches
The “Knee Up” Stretch
Lie on the floor, use a mat or thick rug for comfort, on your back. Stretch both legs out, with your arms to your sides.�Bend one of your legs at the knee and use your hand to pull it toward the opposite shoulder Hold for ten to thirty seconds.�Straighten out that leg, and then do the same motion with the opposite leg and shoulder.
The “Cross Arm” Stretch
Arrange yourself in a sitting position. The bottoms of your feet should be touching each other, with your arms crossed and your hands resting on the opposite leg. Push both knees down toward the floor until you feel the stretch inside your thighs. Hold the position for a count of 30, then relax for a few seconds and repeat up to five more times.
The “Standing” Stretch
This is a handy exercise you can do in the bathroom at work, in a hotel, or anywhere that you would rather not lie on the floor.
Begin in a standing position with both feet flat on the floor, with your feet a shoulder-length apart.��Don’t lock your knees, and keep your back straight.�Lift one knee up and grasp it with both hands. Make sure you keep the knee parallel to the corresponding hip. Use your hands to pull your knee toward the opposite shoulder until you feel a pull along the side of your buttocks. Hold up to one minute, or as long as you can balance. Repeat the action with the other leg. Try to do it three times for each leg.
The “Sit and Bend” Stretch
This is another convenient�exercise that doesn’t require getting on the floor. Choose a solid, straight-backed chair that doesn’t roll,�sit, and bring one leg across the other, resting your ankle on your other leg. Slowly lean forward until you feel a pull along the crossed leg. Hold for up to 30 seconds. Repeat with the other leg, stretching each side 3 times.
Remember that consistency is key. Perform these exercises at least once a day, every day, until your pain and numbness is gone.
These four simple exercises�help you make great strides in recovering from Piriformis syndrome. However, if you perform these for several days and still have pain, or experience pain while attempting the stretches, it is a good idea to make an appointment with a professional chiropractor. He or she will be able to evaluate your condition and offer a comprehensive treatment plan to treat the Piriformis so it doesn’t get worse, or cause additional issues with your sciatic nerve.
You try to stand up from a seated position and feel a stab of pain in your lower back. It may even shoot through your hip, buttock, or down the back of your thigh. The pain may even get worse then you walk uphill or sit for a long period of time. While these symptoms could mean a pinched nerve, lumbar disc herniation, hip bursitis, or degenerative hip disease, it could also be sacroiliac joint dysfunction.
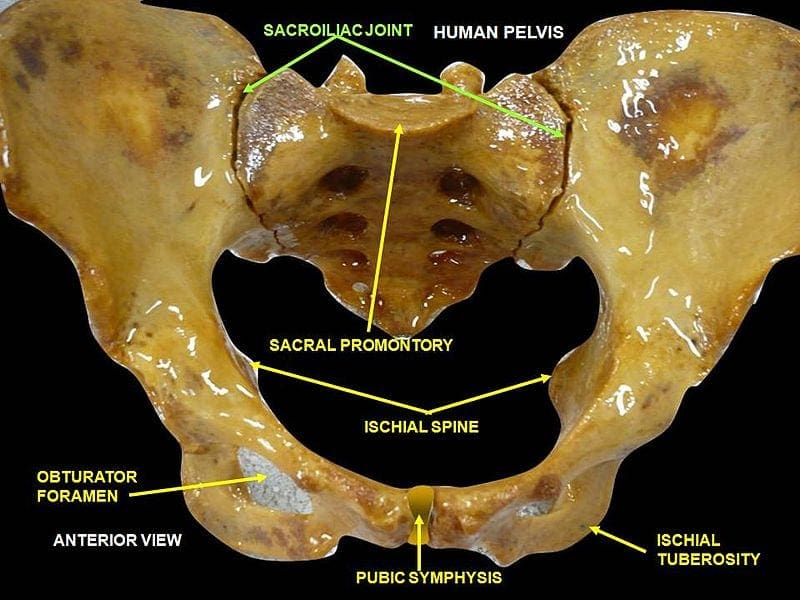
What Is Sacroiliac Joint Dysfunction?
The sacroiliac (SI) joint is located in the pelvis. It is very strong as it is a weight bearing joint connecting the pelvis to the sacrum. It is surrounded by tough ligaments that reinforce it, providing added support.
There is an SI joint located on each side of the sacrum and they work together, moving as a single unit to act as a shock absorber for the spine and for transmitting force of the upper body. Just like any other joint in the body, the SI joint can be injured or diseased, causing it to become unstable and inflamed, causing pain and limited mobility.
What Causes SI Joint Inflammation?
While doctors have not established how the pain is generated, it is believed that it is due to a change in the normal motion of the joint. This could occur due to:
Hypermobility (Instability or Too Much Movement) � This can cause the pain to reside in the lower back. It can also be felt in the hip or both the hip and lower back and may even radiate into the groin.
Hypomobility (Fixation or Too Little Movement) � This can cause the pain to reside in the lower back or buttocks and may radiate down one leg, usually in the back of the thigh. It usually doesn�t reach the knee, but sometimes can even reach the ankle and foot. In this way, the condition mimics sciatica.
Sacroiliac joint dysfunction typically affects women who are young or middle aged. Older women and men are rarely affected although it does happen.
What Are Treatment Options For Sacroiliac Joint Pain?
When SI joint pain is initially diagnosed the treatment is usually fairly conservative. Medication, physical therapy, and injections are used by doctors for pain management.
NSAIDs and other similar medications decrease inflammation and reduce pain, while physical therapy can readjust the SI joint in cases where it is dislocated or immobilized. It also includes exercises that stabilize the joint for pain management over the long term.
Steroid injections directly into the sacroiliac joint can help with the reduction of inflammation and pain while making physical therapy more effective. When steroid injections are effective but the effects are temporary there is another non-surgical treatment that is sometimes used called RFA, or radiofrequency ablation.
In cases where the conservative methods do not achieve the desired results there are surgical options that provide pain reduction and stabilization on a more permanent scale. SI fusion involves fusing the joint, providing relief.
However, there is a treatment option that is non-invasive, doesn�t involve steroids or medications that could have harmful side effects � chiropractic.
Spinal manipulation � This is the traditional chiropractic adjustment that is also known as high-velocity, low-amplitude (HVLA) thrust.
Spinal mobilization � This is a less forceful, gentle chiropractic adjustment also known as low-velocity, low-amplitude thrust.
Chiropractic is proven to be an effective, non-invasive, gentle method for relieving the pain and inflammation of SI joint dysfunction. No medication, no surgery, just relief.
So if you�ve been suffering from sacroiliac joint dysfunction, give us a call! Our Doctor of Chiropractic is here to help!
Injury Medical Clinic: Sciatica Treatments & Recoveries
Bobby Gomez describes how each visit with Dr. Alex Jimenez and to PUSH Fitness with Daniel Alvarado has resulted in great improvements in the stability of his shoulders as well as in the placement of his hips. Although Bobby Gomez’s recovery has been progressing gradually, he discusses the tremendous changes he has experienced mentally, emotionally and physically. Bobby Gomez highly recommends Dr. Alex Jimenez as the non-surgical choice for neck and back pain, as well as shoulder and hip pain.
Shoulder Pain Treatment
Cerebral palsy (commonly known as CP) affects ordinary motion in various areas of the human body and has many degrees of severity. CP causes problems with posture, gait, muscle tone and coordination of movement. Some children with CP have coexisting conditions, such as eyesight and hearing impairment. These disorders are brought on by brain damage and aren’t a direct result of cerebral palsy. Cerebral palsy does not affect life expectancy. Based on the way in which the condition is handled, motor abilities can improve or decrease over time. While severity and symptoms vary, most individuals with this condition go on to direct a rich, fulfilling life.
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
If you have enjoyed this video and/or we have helped you in any way please feel free to subscribe and share us.
Chiropractic is a very effective treatment for back pain, but what many patients don�t realize is that they can stretch to make it even better. By employing simple stretches, a chiropractic patient can improve his or her range of motion and increase flexibility. These are some great stretches that you can do at just about any fitness level.
Stretch
Knee To Chest
Lie on a firm, flat surface for this exercise. You can place a mat or towel underneath you to make it a little more comfortable. If you aren�t able to flatten your back right away, fold a small towel and place it under the small of your back to provide a little support.
Lie on your back, knees bent so that your feet are flat on the floor.
Press your lower back into the floor.
While keeping your left foot on the floor, inhale, bringing your right knee to your chest, pulling gently just until you feel a stretch. Hold it for 20 to 30 seconds. You can also keep your left leg straight if that is more comfortable. Make sure you keep your back pressed to the floor.
Exhale, releasing your right knee and return to the starting position.
Repeat the movement with the left leg.
Repeat this stretch 3 to 5 times with each leg.
Child�s Pose
This gives you a very nice stretch all through your back. If you are unable to get on your knees or if you can�t sit on your knees, you can do this while standing.
Hold onto the back of a chair and bend forward. Don�t pull and don�t rest put all of your weight on the chair, just let your body fall gently forward with your neck relaxed and your head drooping. Take baby steps backward until you feel a good stretch, then hold it while breathing normally for 20 to 30 seconds. Walk your feet back in a bit to keep your balance and stand. Repeat 4 or 5 times.
Get on your hands and knees, keeping your knees a little wider than your hips. Turn your toes inward so that they touch.
Bend your knees, pushing your hips back over your heels. Get to a comfortable sitting position.
Slowly slide your arms out in front of you, rounding out your back as you exhale. Keep your neck relaxed so that your head falls forward. Allow yourself to feel the stretch throughout your back.
Hold for 20 to 30 seconds then return to the sitting position.
Repeat the movement 4 or 5 times, keeping your movements slow, fluid, and deliberate.
Cat � Camel
If you can�t get on your knees, stand in front of a chair and place your hands on the seat. Position your feet about where your knees would be if you were on your hands and knees. Relax your neck, allowing your head to droop. Complete steps 2 through 5.
Get on your hands and knees, back straight, your hands shoulder width apart, and your knees slightly apart. Relax your neck so that your head droops. Breathe normally.
Exhale as you round your back up toward the ceiling. Press until you feel a good stretch all along your back. Hold for about 20 to 30 seconds.
Return to the starting position, keeping your back straight.
Inhale as you sway your back, pushing your stomach toward the floor. Tilt your pelvis to get a maximum stretch. Hold for 20 to 30 seconds.
Running Shoes: Feet are important. By the time the typical American reaches the age of 50, they will have walked 75,000 miles.
Runners put even more miles on their feet, and stress. Your feet are your foundation. A problem with your feet can throw your entire body out of balance. That is why when it comes to running shoes, it is important to find the right type. This guide will help you find the running shoes that are right for you.
Running Shoes
Before You Shop
Know the type of runner you are.
Different types of running require different features in shoes.
Some questions to consider:
Do you run or jog?
What surface do you run on � asphalt, treadmill, or trails?
A larger person will not move and run the same way a thin, wiry person does. An overweight person will put more stress on their feet � and shoes.
Know your running style.
The way you run, the motion of your stride and how your foot strikes the ground has great bearing on the type of running shoe you need. When your foot comes in contact with the ground, what hits first? Does the inside of your forefoot hit first? The center of your heel? The outside of your heel? Where your foot first hits is where you really want the cushion.
Know what injuries you may have sustained from running.
Plantar fasciitis, shin splints, tendonitis, and blisters are a few common injuries can be reversed or improved when you wear running shoes that fit properly.
Know the type of arch you have.
Whether you supinate (foot rolls to the outside) or pronate (foot rolls to the inside) is determined, at least in part, by the shape of your arch. While supinators are rare, quite a few people over pronate. This can be the source of injuries due to overuse.
When You Shop
Give it the 360-degree test.
When people try on shoes they typically check for fit in the toe box, but look no further than that. When you try on running shoes, you do need to make sure you have adequate space in the toe box, but you also need to check that your entire foot fits on the shoe�s platform.
Give your foot enough space.
The upper should have enough room but should not be loose. It shouldn�t squeeze your foot either though. It should fit well with no pinching or binding.
Shop later in the day.
Throughout the day your feet swell. When you run they also swell so when you shop for shoes, going when your feet are the largest will help ensure that you get the most accurate and more comfortable fit possible.
Bring your old running shoes along when you shop.
Having your old shoes with you when you shop will help the sales person determine what kind of running shoe you need. They can look at the wear on the shoe to see your running patterns and help you find a shoe that works best for you.
Get your foot measured.
As you age your feet actually change; they can expand or flatten. Don�t every assume your shoe size, get your foot measured every time. A comfortable fit is dependent upon wearing the right size shoe. You also need to keep in mind that shoe sizes may differ from brand to brand.
Dress for the run.
When you are shopping for a new pair of running shoes, dress as you would when you run. Don�t show up wearing flip flops or when you are dressed for the office. Definitely don�t show up without socks.
Forget the latest trend or what�s fashionable; think functionality.
There are plenty of sharp looking shoes, but that doesn�t mean they are the right running shoe for you. Go for fit and functionality first and fashion second.
Take them for a test drive.
Once you have settled on a pair or two, try them both on and try them out. Many stores that specialize in running shoes have a treadmill or area where runners can try their shoes. That is the only way you can tell for shoe if the shoe is right for you.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine