As parents and grandparents, we first need to think about the activities that we will be doing throughout the day and consider how to protect ourselves and loved ones from falls and falling injury/s.
Around the House
Most accidents indeed happen at the house. Add that to the increasing number of people, both young and elder, that work from home. Consider the following tips.
Home
If possible, hire a professional to clean the gutters or get one of those gutter washers that you can use from the ground. Falls from the roof results in multiple injuries, and some are very serious.
Would you please not stand on a chair to change lights or clean those out-of-reach areas? Always use a reliable heavy-duty step ladder with anti-slip steps and handrails. Doctors from emergency rooms report that falls from chairs are a common case they treat.
Proper Lighting
Having the right lighting throughout the house is the best defense against tripping and falling. The stairways, hallways, and entrances are primary areas that should be adequately lit to see everything around you. The light switches should be easy to find and activate. Inexpensive nightlights should be placed anywhere you go at night, like the kitchen or bathroom. A small flashlight should also be kept nearby, possibly a keychain or next to the bed in case of an emergency or if the power goes out.
Kitchen
Falling on wood or tile kitchen floors can have a serious impact on the body. A wet slippery floor can be another cause for a fall, so clean up spills or fix a dripping refrigerator immediately. Using a no-slip floor wax rather than conventional floor wax will reduce accident probability. Keep a secondary heavy-duty step ladder with wide anti-slip steps and handrails for the kitchen.
Bathroom
The bathroom has the potential to be one of the most dangerous rooms. The slick hard floor floors from bath/shower water, along with the limited room to move around comfortably and metal towel rods, can make for a dangerous space to fall in. However, bathrooms can be made safe by the following:
Handrails/grabs can be placed along the walls and shower/bath, near the toilet and sink. Make sure that the proper height is measured.
Anti-slip bath/shower mats and anti-slip floormats can go a long way to help prevent falls. They provide traction and stability while standing and moving around.
There are some top assisted bath devices in various drug stores and home centers. They include shower seats and walk-in baths.
Raised toilet seats can be easily installed and shorten the distance needed to sit and, more importantly, get up comfortably from the toilet.
Elderly and physically challenged individuals could still need help. Make sure assistance is readily available. Elderly and physically challenged individuals could benefit by carrying an alarm or emergency contact system in case they fall or need help.
Stairways
The stairway is an area that can be another danger zone. One stairway danger is the use of canes, walkers, and walkers with wheels. These can easily get snagged on a step, or the wheels can slip and quickly travel down the stairs. Safety railing and step mats with traction nibs can help prevent slips and falls. Outdoor stairs should have non-slip tape to prevent falling.
Carpeting/Rugs
Carpeting and rugs are great for warmth, foot care, and decoration, but they can also pose a danger. Here are a few tips:
Throw rugs that are not properly anchored to the floor should be anchored or used in an area that will not pose a potential injury. These rugs can be bought with a rubber backing to prevent slippage. Stores carry non-slip backing that can be cut and used between the floor and the rug.
Carpeting needs to be smooth and not wrinkled, which can snag and cause tripping.
Bent corners should be removed and fixed to prevent unraveling or tacked down with non-slip tape.
Loose fibers need to be cut off.
Furniture
Individuals that don’t use an assisted device like a cane or walker could find navigating through the house difficult. Furniture should be arranged and organized for easy maneuverability. Electrical cords should be safely placed out of the walking path.These cords can be tacked to the floorboard, placed behind/under furniture, or stored in special cord tubes/runners. Small tables, floor lamps, and plants should not be in the walking path as well as this can cause an easy bump to fall scenario.�
Footwear
Footwear should be nice but also practical. Flat-soled shoes, high heels, not properly structured, or ill-fitting shoes can lead to slips and falls. Unsupported feet will not provide a solid foundation to help prevent a fall.
If there are foot issues, custom foot orthotics can really help stabilize balance, help the spine stay aligned, and bring relief from pain. Orthotics are designed to fit inside shoes to relieve pain from various foot conditions/issues. Non-slip and anti-slip soled shoes can also help prevent a slip and fall. With these types of shoes, care needs to be taken to avoid sticking to floor surfaces. This can contribute to stumbling and tripping. Don’t wear socks or hosiery on smooth tiled/wood floors; because there is no floor-foot traction, the potential for slipping increases.
When walking outside, if the sidewalk is slippery, walk on the grass or dirt area. Try walking in an area that does not show iciness or wetness. Cat litter or rock/sidewalk salt can provide foot traction.
Assistive Devices for Balance and Stability
If you feel unstable while walking, ask your doctor about an assisted device that includes canes and walkers. If using a cane, make sure the rubber grip tip is not worn down.
Conclusion
Here are a few tips that may help you to take a proactive approach to fall prevention. Depending on specific conditions and needs, you may want to talk to your doctor, chiropractor, physical therapist, or other health care professional. They will create a customized individual plan to help prevent falls and enjoy life.
Our clinical focus and personal goals are to help your body heal naturally, quickly, and effectively. At times, it may seem like a long path; nevertheless, with our commitment to you, it’s sure to be an exciting journey. The commitment to you in health is never to lose our deep connection to each one of our patients on this journey.
Plantar Fasciitis, Reduce Foot Pain with Custom Orthotics
NCBI Resources
Aging is hard on the body. As you move into your senior years, you may expect some discomfort and loss of mobility. But it is important to understand that there are things you can do to feel better. Regular exercise, a healthy diet, and chiropractic care can all make your senior years active and thriving.
As 2020 is off to a bustling start, New Year resolutions are in full swing! Most individuals want to make healthier choices throughout their year in 2020, whether that be exercising more, eating better, or just feeling energized. After the holidays hit, most people are left feeling fatigued,� suffering headaches, and overall discomfort.
A great way to stay on track with your goals is to keep track of them! The human body requires micronutrients and macronutrients to function. Micronutrients consist of essential vitamins and minerals. Macronutrients refer to protein, fat, and carbohydrates. Macronutrients all provide the body with energy. This energy is essential to properly repair cells as well as maintain metabolism, immunity, and growth.
Carbohydrates are the main energy system in the human body. These carbohydrates provide over 50% of the daily diet. However, not all carbohydrates are created equal. There are simple and complex carbohydrates. Simple carbohydrates are those found in glucose and fructose (examples: fruit, sugar, and milk). Complex carbohydrates are those that require the body to work a little harder to break down and contain glycogen. Glycogen is important to eat as it is a valuable source of fiber.
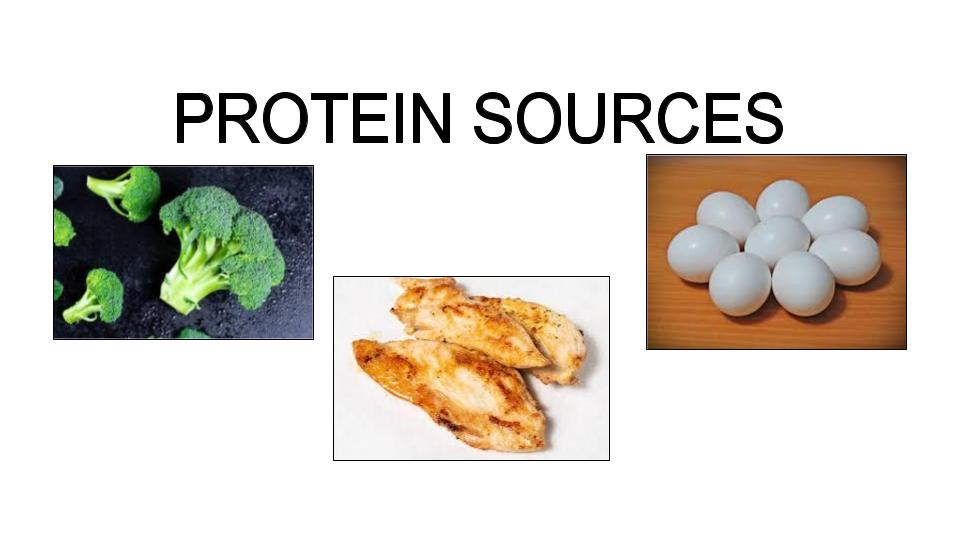
The main function of protein is to maintain and grow the body tissue. Proteins are made up of amino acids.� Amino acids are the stepping stones used for neurotransmitters, cell membranes, nucleic acids, and hormones. Protein is widely stored in the human body due to the large amount of muscle tissue the body is comprised of. Overall, there are amino acids that must be obtained through the diet to maintain optimal health. Some of these amino acids include lysine, threonine, and tryptophan.
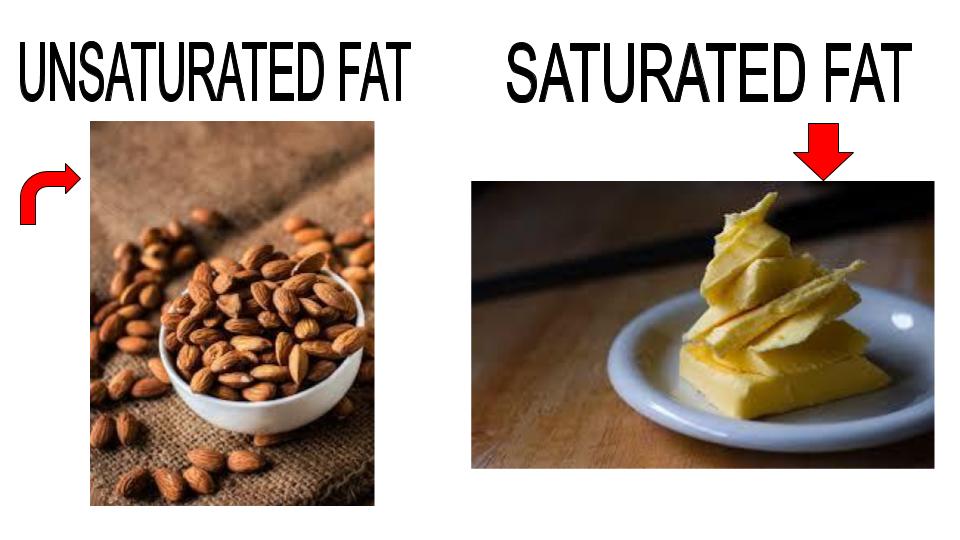
Out of all the macronutrients, dietary fats require the least amount of grams per day. Similar to carbohydrates, there are two types of fat. Saturated and unsaturated. Saturated fats can be found in butter, where unsaturated fats mainly consist of nuts and avocados. A great supplement to take for healthy fats is Omega-3 and Omega-6, also known as fish oils. Fish oils also help improve cardiovascular health and help the Body generate specialized lipid mediators.
Although each individual requires protein, fat, and carbohydrates, the optimal amount of each depends on each person as well as their body composition. Tracking macronutrients has been shown to improve weight loss and reduce inflammation.
�Tracking macros or macronutrients coupled with exercise is a great way to see results. The macronutrients each person needs depends on their body type, their goals, and their lifestyle. Health coaches such as myself can help determine what an individual’s macronutrient intake should be for weight loss results. Personally, I use the Dr. J Today app, wrist band, and scale. This app allows patients to track their food, steps, water intake, and exercise as well as provides an informative digital library. The scale directly syncs to the app, allowing me to get instant access to the weight and body composition of the patient. This scale not only measures individuals but it also measures their lean body mass, water mass, BMI, and body fat. These resources allow us to gain optimal insight and make corrections that will actually make a difference. – Kenna Vaughn, Senior Health Coach
The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.�
Physical Activity to Prevent Back Pain and Weight Gain
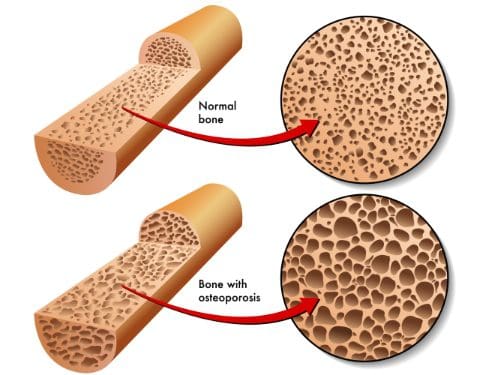
Osteoporosis
Regular physical activity will improve the body’s:
Balance
Reflexes
Coordination
This significantly reduces potential falls and injuries. Injuries from falling can be devastating for someone with osteoporosis.
Consult with your doctor before beginning any exercise program.
To help reverse bone loss, physical activity must fit the individual’s type and intensity. This will determine the appropriate exercises for your level of fitness as well as the risk of fracture.
As a way to begin walking is a great way to start a regular exercise therapy.
Walking improves bone strength because it distributes the body’s weight in a balanced manner over and over again. Bone responds best to the intensity of the walk and not the duration. Bones need to be consistently challenged as they respond by making more osteoblasts or the cellular material that fills the bone cavities. Adding these higher levels of resistance causes healthy stress to bones. This is what increases bone density.
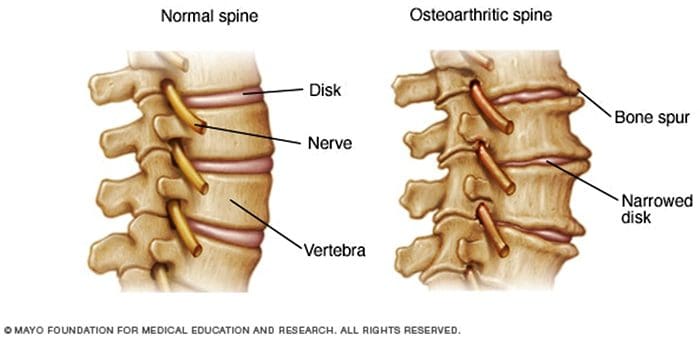
Osteoarthritis and rheumatoid arthritis are conditions that affect the flexibility of the spinal or facet joints. Flexibility, in this case, means the ability of joints to move through their normal range of motion. The amount of an individual’s range of motion is determined by how tight the muscles, tendons, and ligaments are. When muscles can stretch freely, this means the joint has better flexibility.
Low Back Pain & Possible Sciatica
To prevent low back and leg pain, the back, and hip muscles need to be flexible and strong. Individuals with poor flexibility and weak muscles in the back, pelvis, and thighs have a higher risk of increasing the curve of the lower back which can make the pelvis tilt too far forward.
Proper posture combined with flexible and strong muscles can help prevent nerve compression and pain.
Overall Health
Having healthy body composition means there needs to be more lean body mass i.e. muscle mass and less body fat. Strength training/CrossFit helps by raising the metabolic rate while lowering body fat. The increased muscle strength helps maintain correct posture and body mechanics in whatever you do.
Physical activity reduces the chance of injury while increasing physical performance like being able to climb stairs or carry groceries with much-added ease and confidence.
Exercise Suggestions
The benefits a regular exercise program offers are one of the keys to a healthier lifestyle. But take it in steps, see a health coach, physical therapist or chiropractor to help educate and guide you through an exercise treatment plan. Helpful tips:
It can take 6 to 8 weeks to see results so focus on short-term goals.
Work regular exercise into your schedule but keep important activities as a priority.
Friends and relatives can help give you support and join in the exercise.
You don’t have to do an entire workout. Instead, exercise for 10 minutes.
Consistency in physical activity is the goal. It’s not how long or hard the exercise is.
Keep a journal of your workouts and progress.
With the healthy changes made today, including diet choices and regular physical activity/exercise, your life will be one-hundred times better. This does not mean that you have to become an intense workout aficionado. Remember all that is needed is a reduction in weight of only 10%. This is what is needed to reduce the detrimental effects of being overweight.
Our clinical focus and personal goals are to help your body heal itself naturally quickly and effectively.� At times, it may seem like a long path; nevertheless, with our commitment to you, it�s sure to be an�exciting journey. The�commitment to you in health is to, never lose�our deep connection to each one of our patients on this journey.
When your body is truly healthy, you will arrive at your optimal fitness level proper physiological fitness state. �We want to help you live a new and improved lifestyle. Over the last two decades, while researching and testing methods with thousands of patients, we have learned what works effectively at decreasing pain while increasing human vitality.
*AMAZING* Custom Orthotics for Athletes | El Paso, Tx
NCBI Resources
It can be tempting to not exercise with a spinal condition. But remember that if there is no movement at all, you could make the pain worse.�Knowing what your body can handle and sticking to a workable schedule, these healthy steps will relieve you and help with your low back pain.
All individuals that participate in some form of sports or athletic training, professionals to weekend sports enthusiasts are at risk for back and neck injuries. Common injuries include strains, and sprains, pulls, and tears especially around the low back area. If left untreated these injuries can lead to chronic back pain or more severe conditions.
Although we can’t prevent all sports injuries, here are some sports tips to keep your spine healthy.
1.� Warm-Up and Stretch
Properly warming up with stretching exercises increases blood circulation and improves the flexibility of muscles and ligaments. This is not only for helping enhance athletic performance but prevents injuries by keeping the muscles/ligaments loose so if any type of collision, tear, or pull occurs the stretched muscles stay relaxed and do not tense up or contract, which helps reduce the severity of an injury. To stretch properly:
Stretch time on each part of the body is also 10-30 seconds
Stretch after the game to relieve sore or tight muscles
2. Use Proper Sport Equipment
All sports have a risk of injury. In general, the more contact there is the higher the risk of injury.
To reduce the risk of injury athletes should wear protective equipment that goes with their sport like neck rolls, shoulder, elbow and knee pads.
Well made and supportive shoes combined with custom orthotics are a must.
Other types of equipment include:
Helmet
Pads elbow, wrist, chest, knee, shins
Mouthpiece
Faceguard
Protective cup
Eye protection
3. Stay Hydrated
Injuries caused by heat occur as a result of�high temperatures, humidity and excessive/overdoing it. To avoid these serious injuries:
Drink plenty of water before, during, and after playing.
Try to avoid play or practice during extreme heat and humidity.
Wear lightweight clothing/uniform with maximum ability to allow sweat to evaporate.
Take plenty of breaks or periods of rest to allow the body to recover and recuperate.
4. Don’t Overwork/Overdo it
Repetitive Motion Disorders like tennis elbow, bursitis, and tendonitis, happen when movements e.g. swinging motions that go with the sport like tennis, bowling, golf, etc are repeated over and over and cause injury/damage to those parts of the body. To avoid overuse injury try:
Take plenty of breaks during practice and games. Do not power through it!
Use proper/correct form and techniques. If unsure then take lessons to make sure you are doing it correctly.
See a doctor if any pain or muscle fatigue, inflammation, swelling, or compression of nerve tissue present.
Cross-training can strengthen muscle groups and those areas that take the most force.
5. Stay Ready for Play with a Healthy Lifestyle
Besides sports, try to find ways to improve general health through a healthy lifestyle:
Get plenty of sleep, the body/mind needs to recover from all the activity.
Consult a doctor before beginning any new exercise program.
Staying fit, healthy and ready for play means preventing injuries from happening.� By being aware of how to prevent injuries with these basic tips, which feel free to take it further and raise the probability of avoiding back and all sports injuries.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused on treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
*BEST* Heel Spurs Treatment | El Paso, Tx (2020)
NCBI Resources
Extension sports like gymnastics, tennis, swimming, diving, football, volleyball, basketball, track and field, cricket have the most pronounced extension/rotation on the spine. With a normal extension of the lumbar spine (or backward bending), the facet joints begin to approximate each other and compress. This is a normal biomechanical movement. However, if the extension ranges are excessive, the procedures will impinge quite aggressively and damage to the cartilage surfaces within the facet joint can result.
You might not think it, but weight lifting and spine strengthening exercises can help reduce back pain. Remember the point of this type of weight lifting is not to build up the muscles like a bodybuilder but is to develop:
Core strength
Spine strength
Body strength
The muscles in the back keep the spine moving and functioning properly. When the spine or abdominal muscles are weak this creates a higher probability of a back strain or injury. Having strong, healthy spine muscles are important because they function in maintaining correct posture, which in some cases, causes chronic back pain because of poor posture.
If�only one part of the body is strengthened like the back is not enough. Therefore strengthening the rest of the body is a must. These include the body’s core and leg muscles. Total body strength will reduce back pain and can help perform regular activities, like lifting heavy objects much easier, with more confidence and with a lesser probability of injury.
Spine strengthening exercises benefits
Most important reasons are they:
Prevents future back injuries
Stabilizes the spine
Helps the spine move properly
Help maintain correct posture
Increases muscle tone
Teaches correct body mechanics
Helps build bone this is especially beneficial for those with osteoporosis or at risk of developing it
A personal trainer or sports chiropractor can help start a spine strengthening regimen. They will teach:
Simple
Specific
Strengthening
Weight lifting exercises.
A physical therapist can also develop a custom weight lifting/strength�exercise�program for optimal spine health and for reducing pain.
Most workout regimens incorporate a combination of weight lifting with actual weights/exercise machines and strengthening exercises/calisthenics with the body’s weight as the resistance for maintaining a healthy strong spine.
Here are a few weight lifting and back strengthening exercises that can help decrease and prevent back pain.
Talk to a doctor or chiropractor before beginning any exercise program. Remember to listen to your body and stop right away if there is something off.
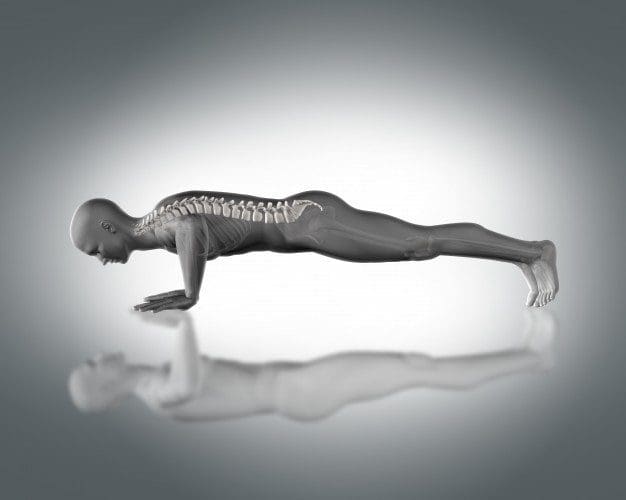
Push-ups
Push-ups help strengthen the:
Back
Chest
Arms
Core muscles
Your own body weight is the resistance.
To do this:
Position the body in a straight line from head to toe, the face looking down.
Hands should be wider than shoulder-distance apart. Walk the hands out so they are slightly higher than the shoulders
Keep the balance on toes and hands, with a straight back, lower the body to the floor by slowly bending the elbows until at a 90-degree angle.
Push up using arm upper back, and chest muscles.
Do 3 sets of 10 every day. As the strength increases do more reps.
Chest Flyes
Chest flies are excellent for building muscle in the:
Upper back
Chest
Dumbbells or a weight machine can be used for this exercise. To do this:
Lie on the floor with the knees bent and the feet flat on the ground.
Extend the arms out to either side of the body, and let them rest on the floor.
With a dumbbell in each hand, raise the dumbbells until they meet at the top at the same time, and keep a slight bend in the elbows.
Lower the hands to the ground, and repeat.
Do this exercise 15 times 3 times a week. With added strength add more reps.
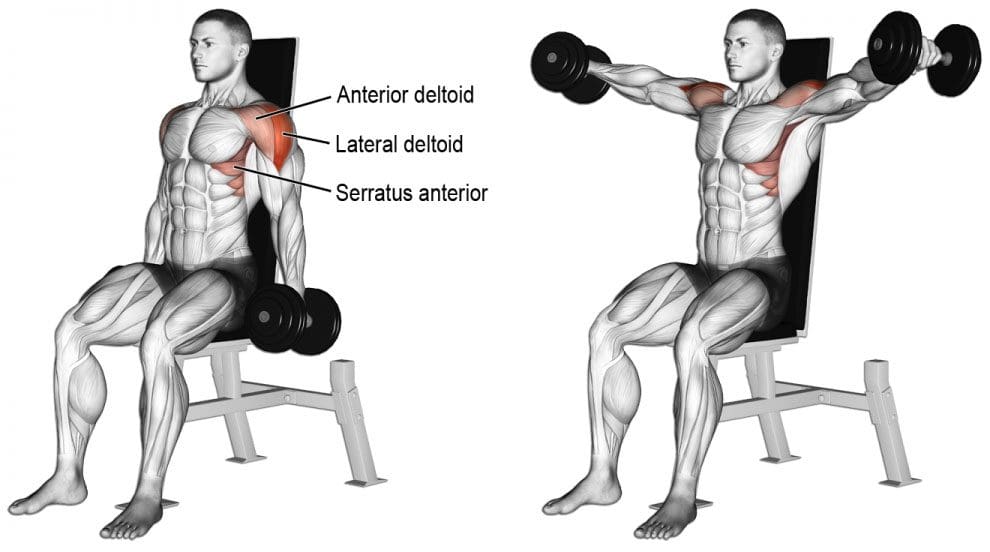
Lateral Raises
Lateral raises help strengthen the entire back. All that is needed is a set of dumbbells. To do this move:
Stand or sit with the feet equal hip-distance apart. Arms are at the side.
With a dumbbell in each hand and a slight bend in the elbows, raise the arms to the side until shoulder height. Keep the core engaged during the movement.
Once at shoulder height, slowly lower the dumbbells, and repeat.
Repeat this exercise 15 times 3 times a week. As strength increases add more reps.
These exercises should be performed slowly with a gradual build-up to more complex movements and adding more weight. Remember to breathe naturally. If you hold your breath during exercise, it can cause tension in the�muscles, which can worsen any pain or create new injuries.�Before adding weight or new spine strengthening exercises, talk to a doctor about exercising with back pain. They will let you know if there are certain movements or positions that should be avoided.
Weight lifting exercises done incorrectly can lead to more back pain and added injuries. If there is any pain while doing these exercises, stop and call a doctor, chiropractor or physical therapist right away.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused on treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
Back Pain Chiropractic Care | El Paso, Tx
NCBI Resources
It can be tempting to not exercise with a spinal condition. But remember that if there is no movement at all, you could make the pain worse. Knowing what your body can handle and sticking to a workable schedule, these healthy steps will relieve you and help with back pain.
Health coaches are becoming more and more crucial as modern and naturopathic medicine continues to improve. More than ever, the healthcare field is progressing at high speeds and professionals do not always have the time available that some patients desire. Here is where health coaches get involved. Basically, the position of a health coach was produced to fulfill the emptiness in several doctor offices. Many physicians contribute but don’t have the time or tools to help each individual and assist in constructing healthy habits on a day to day basis. But, health coaches are available to be a supportive mentor who guides and assists patients in making healthy lifestyle changes. Many patients who seek assistance to change their lifestyle are those afflicted by some kind of chronic pain, headaches, or joint swelling.
In the previous weeks, we have defined and explained what a health coach is and what they really do, as well as the first four steps a health coach might take with a patient. Throughout this article, the fifth and sixth steps will be broken down and analyzed.
Need a refresher? No problem!
Health Coaching in El Paso: Part 1 can be found by clicking�here
Health Coaching in El Paso: Part 2 can be found by clicking�here
Health coaching in El Paso: Part 3 can be found by clicking�here
Step 5: Visualizing Your Best Self
�
This step is extremely crucial. The reason being, without a vision of where an individual wants to be, they can easily get lost on their way to achieving a goal. A vision statement is not intended to be a specific sentence, but rather a loose description of what / who the patient is trying to become.
In order to create this statement, a health coach will work with the patient to clearly identify their skills, interests, and strengths. These are oftentimes similar to the items listed on the values sheet the patient filled out while the health coach was working with them back in�step 1. Other times, the health coach will assist the patient with their vision statement by asking things like:
What are you naturally good at?
What have you always wanted to see, do, or create?
What would help you feel more fulfilled?
In addition to these questions,� the health coach might encourage the individual by steering the conversation in a way that is related to their best self. With the help from a health coach, the patient can reflect and describe their best self as well as the emotions connected to their best self (thinking, feeling, and doing). A coach will also provide critical thinking questions related to a patient’s best self such as:
How do you know you’re there?
How do you know you’re not there?
How can you remember to be your best self and not slip back into the old ways of being?
Step 6: Creating A Plan For Resiliency
It is simply human nature that all people react to stressful situations differently.� However, one thing that is guaranteed is people will need a plan to get back on track. Undergoing life changes is not a simple task, but having a plan is.�An approach for building resilience must be tailored to the specific individual. A health coach will ensure the individuals that falling off track is natural, but how you get back on track is what counts. It starts with reflecting, seeking support, and making a plan to move forward.
When a patient is placed in a stressful situation, it is key they take a moment to recognize the situation and think about how they are feeling. During the moment, it may be difficult but with practice, reflection, and help from a health coach, the process becomes easier.
The best tips when it comes to addressing resiliency are to develop connections, set daily intentions, reflect on experiences, practice self-care, and be proactive.
A health coach may encourage a journal to help patients celebrate small victories and take responsibility for their own happiness. In addition to this, there are other resources available the patients may utilize such as books, self-help support groups, and asking themselves, “What do I typically find helpful in a stressful situation?”.
By utilizing a health coach and implementing these 6 steps into one’s life, the benefits are unbelievable. Identifying values, determining goals, building a plan for action, tracking progress and results, visualizing the best self, and creating a plan for resiliency will help individuals reach their health goals better than before.
By working with a health coach and remembering these exercises, individuals are extremely likely to be successful. Not only do they have someone for accountability, but they are learning ways to become more independent and thoughtful when it comes to their health. A positive community offers support that many individuals need to thrive. Naturopathic medicine and functional approaches are becoming more recognized for their ability to work on a variety of individuals. Take advantage of all the resources around that are there to help you.�– Kenna Vaughn, Senior Health Coach�
All information and resources for this post came from an Integrative Practioner article titled, “A Six-Step Approach To Health And Wellness Coaching: A Toolkit for Practice Implementation” and can be found by clicking�here; as well as listed below in the proper bibliography.
*The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at�915-850-0900.
Miller, W. and Rose, G. (1991). Motivational Interviewing: Preparing People to Change Addictive Behavior. Guilford Publications.
Pecoraro, Wendy. �A Six-Step Approach to Health and Wellness Coaching: A Toolkit for Practice Implementation.��Official Media Integrative Practitioner, 17 Oct. 2019, www.integrativepractitioner.com/resources/e-books/a-six-step-approach-to-health-and-wellness-coaching-a-toolkit-for-practice-implementation.
Trzeciak, S. and Mazzarelli, A. (2019). Compassionomics. Studer Group.
If you are experiencing any of these situations, why not try a HIIT workout to relieve these symptoms.
Everyone can agree that they do not have enough time to exercise. When asked why people will not work out, one of the reasons is that due to their hectic lifestyle, the lack of time comes out on top of it all. The U.S. Department of Health and Human Services recommends that adults should get between 150 and 300 minutes per of moderate-intensity. There is a way to cut that time commitment in half by opting for high-intensity workouts instead. With high-intensity interval training or HIIT, it is one of the proven ways to reap all the benefits of exercise in less time. Research shows that spending less time doing HIIT may even be better than spending more time doing less intense exercises for individuals.
What is HIIT?
High-intensity interval training or HIIT alternates explosive bursts of full-throttle efforts with periods of recovery. It can either be rest or a lower-intensity exercise. In many fitness centers and gyms, HIIT workouts often include both cardio and resistance training; however, HIIT workouts can be done as a strictly cardio routine.
During intense burst in a HIIT workout, a person is working out at around 80 percent of their max heart rate for 15 seconds to a few minutes. Between each of those periods, a person is either slowing down or resting completely to let their heart rate come back down to around 50 percent.
A person can calculate different target heart rates by using an online calculator. During a workout, a person can wear a heart rate monitor to keep track on much they are exerting themselves. For a lower-tech option, Denver-based certified personal trainer Lindsay Kelly recommends the “talk test.” The way the “talk test” is when a person is doing their target intensity heart rate like sprinting; for example, it should be hard to speak more than two words without taking a breath. Then when they are in the recovery period, the reverse factor is real.
Why HIIT Works
HIIT is so effective because it allows a person to exercise at a higher intensity for such a short period. The exertion gets the heart working and the blood pumping better than any moderate-intensity exercise can bring with their prolonged periods of rest.
The Importance of Rest
While a person might not realize it, the rest periods are built into the HIIT workout and are a critical part of the routine. They force the body to adjust to a very different state of activity, which is excellent for cardiovascular conditioning.
Feel The Afterburn
Another benefit of a HIIT workout is that even after a person is finished with their HIIT workout, it keeps on working for them. Research shows that when individuals keep on burning calories after their HIIT workout at a higher than they would after a continuous exertion workout. It is commonly known as the “afterburn effect,” and it helps people extend the benefits of their efforts.
The Benefits of HIIT
Researchers have been studying HIIT extensively, and the results are precise: HIIT workouts are better than continuous exercise when it comes to improving health in a variety of ways. One of the health benefits of a HIIT workout is that it improves cardiorespiratory fitness, which is the health of the heart and breathing. This matters to a person who is trying to get in as much exercise as possible with little time because cardiorespiratory fitness is a primary factor in the risk of diseases and death. Studies have shown that HIIT workouts can increase cardiorespiratory fitness at twice the rate of continuous exercises.
The health benefits of HIIT does not stop there, as other research studies have shown that HIIT can help with the following areas of the body.
Endurance
By improving cardiorespiratory fitness, HIIT can improve a person’s stamina. What it does is that it enhances the body’s ability to consume and use oxygen. One study has compared a regular endurance training to HIIT by looking at how they affect maximal oxygen consumption known as VO2max. The research found out that HIIT was superior to endurance training by improving VO2max in healthy young to middle-aged adults. Once a person starts to build their endurance, they can increase the length or the intensity of the HIIT working periods and enjoy the significant health benefits it provides.
Heart Health
One of the significant contributors to cardiovascular disease and death is high blood pressure, and one of the best ways to keep it in check is through regular exercise. The traditional recommendation for blood pressure modulating has been to exercise at moderate intensity for at least 30 minutes on most or all day so that way high blood pressure will not transform into hypertension. Several studies have suggested that HIIT may be an even better option, and one study shows that while both continuous exercise and HIIT helps with blood pressure control, HIIT is the only workout to help reduce arterial stiffness. Arterial stiffness is a predictor of cardiovascular disease in people with high blood pressure.
Brain Function
When a person feels that that mental clarity after a good workout, it is not their imagination. The brain and mental health benefits of exercise are well documented. Research shows that HIIT helps explicitly improve the cognitive function, including short-term memory, verbal memory, attention, and processing speed in the brain. HIIT also increases the amount of oxygen that the brain gets from the blood.
Diabetes Management
Since exercise is an essential part of diabetes management, research shows that HIIT may be a wise exercise choice for anyone who has type 2 diabetes. Studies have shown that HIIT workouts can improve endothelial function, insulin sensitivity, glucose control, and other health effects of diabetes that are better than continuous exercise.
Conclusion
HIIT workouts are perfect for anyone who does not have enough time out of their busy schedule. With the alternating burst of exercises and periods of recovery, HIIT workouts are beneficial to anyone with a short amount of time to complete them. HIIT includes both cardio and resistance training and works with the entire body. Some products are excellent in countering the metabolic effects of temporary stress and supporting the body�s system.
The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
References:
Chobanian, Aram V., et al. �Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure.� AHA Journals, 1 Dec. 2003, www.ahajournals.org/doi/full/10.1161/01.hyp.0000107251.49515.c2.
Council on Sports, HHS Office. �Physical Activity Guidelines for Americans.� HHS.gov, US Department of Health and Human Services, 1 Feb. 2019, www.hhs.gov/fitness/be-active/physical-activity-guidelines-for-americans/index.html.
Dupuy, Oliver, et al. �Effect of Interval Training on Cognitive Functioning and Cerebral Oxygenation in Obese Patients: A Pilot Study.� Latest TOC RSS, Medical Journals Limited, 1 Nov. 2014, www.ingentaconnect.com/content/mjl/sreh/2014/00000046/00000010/art00016.
Francois, Monique E, and Jonathan P Little. �Effectiveness and Safety of High-Intensity Interval Training in Patients with Type 2 Diabetes.� Diabetes Spectrum: a Publication of the American Diabetes Association, American Diabetes Association, Jan. 2015, www.ncbi.nlm.nih.gov/pmc/articles/PMC4334091/.
Gillen, Jenna B., and Martin J. Gibala. �Is High-Intensity Interval Training a Time-Efficient Exercise Strategy to Improve Health and Fitness?� Applied Physiology, Nutrition, and Metabolism, 27 Sept. 2013, www.nrcresearchpress.com/doi/10.1139/apnm-2013-0187#.XdQT5y2ZP1J.
Guimar�es, Guilherme Veiga, et al. �Effects of Continuous vs. Interval Exercise Training on Blood Pressure and Arterial Stiffness in Treated Hypertension.� Hypertension Research: Official Journal of the Japanese Society of Hypertension, U.S. National Library of Medicine, June 2010, www.ncbi.nlm.nih.gov/pubmed/20379194.
Milanovi?, Zoran, et al. �Effectiveness of High-Intensity Interval Training (HIT) and Continuous Endurance Training for VO2max Improvements: A Systematic Review and Meta-Analysis of Controlled Trials.� SpringerLink, Springer International Publishing, 5 Aug. 2015, link.springer.com/article/10.1007/s40279-015-0365-0.
Pescatello, Linda S, et al. �American College of Sports Medicine Position Stand. Exercise and Hypertension.� Medicine and Science in Sports and Exercise, U.S. National Library of Medicine, Mar. 2004, www.ncbi.nlm.nih.gov/pubmed/15076798.
Unknown, Unknown. “Is High-Intensity Interval Training Right for You?” Fullscript, 12 Nov. 2019, fullscript.com/blog/high-intensity-interval-training.
Weston, Kassia S, et al. �High-Intensity Interval Training in Patients with Lifestyle-Induced Cardiometabolic Disease: a Systematic Review and Meta-Analysis.� British Journal of Sports Medicine, BMJ Publishing Group Ltd and British Association of Sport and Exercise Medicine, 1 Aug. 2014, bjsm.bmj.com/content/48/16/1227.short.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine