Athletes both recreational and fully competitive can be impacted by injuries to the muscles and ligaments around the hip.
These injuries interfere with performance levels and sometimes end participation completely.
�Excessive pronation along with shoes with poor shock absorption has been found to be an underlying cause for various leg/hip injuries.
Custom made Orthotics improve the biomechanics of the feet and reduce the extent of pronation helping to prevent sport-related leg/foot injuries.
Over Foot Pronation
Research has determined that athletes with more foot pronation have a higher probability of sustaining a leg injury, including iliotibial band syndrome that comes from excessive tightness of the hip muscles.
People involved in sports or recreational activities lower their likelihood of developing traumatic and overuse hip injuries through chiropractic treatment and using custom foot orthotics.
The amount of pronation during standing and while running at a standard speed is determined by measuring the angles of the footprints.
Athletes with more pronation have a higher likelihood of an overuse injury.
Standing (static) and running (dynamic) prints show the amount of pronation and is a predictor of developing an overuse injury.
Athletic performance and injury prevention involve regularly checking the alignment of patients� feet in the standing position.
Hip Injuries & The Hamstring
Many hip injuries develop from poor biomechanics and improper movement, especially when running.
Smooth muscle coordination provides balance and support for the pelvis and is needed for optimum sports performance.
This includes:
Hamstring muscles
Hip abductor muscles
Tensor fascia lata or the iliotibial band
When there is an issue with the feet and ankles, abnormal motion like over-rotating the entire leg is the perfect set-up for pulls, sprains, and strains.
50% of standing consists of heel strike and maximum pronation.
The hamstring muscles function to control the knee and ankle when the heel strikes and absorb the impact.
The theory behind orthotic support is that orthotics help the hamstrings control the position of the calcaneus and knee, so there is less stress on the hip and pelvis.
Hip Injuries & Over-Pronation
Orthotics can correct excessive pronation and treatment of hip problems. These are some of the problems/pathologies that can develop.
These conditions develop in athletes who push their body’s to the limit going for optimal performances.
Conclusion
Overpronation and poor shock absorption contribute to leg injuries � from:
Foot
Lower leg
Knee
Thigh
Hip
These conditions can be prevented with custom-made orthotics.
Foot biomechanics evaluation is a must
To avoid hip injuries, athletes need regular evaluations of foot alignment and function
Wear well-designed and solid-constructed shoes
Chiropractors can prevent arch breakdown and foot problems with custom orthotics, and also treat numerous injuries to the lower extremities, especially the hips.
Excessive Foot Pronation can Affect *FOOT POSTURE & MOBILITY* | El Paso, TX (2019)
The following video discusses how excessive foot pronation can ultimately affect foot posture and mobility. Several factors can affect foot posture and mobility, such as excessive foot pronation. Excessive foot pronation is most prevalent among the general population, therefore, it is considered to be one of the most common factors for abnormal foot posture and mobility, which can lead to a variety of health issues like overuse injuries. Excessive foot pronation and even supination can ultimately affect overall health and wellness.
Hip Labrum tears in athletes can occur from a single event or recurring trauma. Running may cause labrum tears due to the labrum being utilized more for weight-bearing and taking excess forces while at the end-range motion of the leg. Sporting activities are probable causes, specifically those that require frequent hip rotation or pivoting to a loaded femur as in ballet or hockey. Constant hip rotation places increased strain on the capsular tissue and harm to the iliofemoral ligament. This subsequently causes hip instability putting increased stress on the labrum and causing a hip labrum tear.
What’s Afoot
Chiropractic�seeks to find the cause of the conditions it is used to treat, including pain, instead of just treating symptoms. Because of this, the chiropractor will work to find the cause of the pain, in this case, overpronation and overpronation, and correct it � or the effects of the condition � in addition to treating the back pain.
Overpronation and oversupination can cause a variety of injuries and conditions that affect not only the feet and ankles, but also the knees,�hips, and back as well. Some of the more common injuries and conditions include:
Flat feet or posterior tibial tendon dysfunction
Ankle Sprains
Achilles tendinitis
Arch pain
Plantar fasciitis
Corns
Shin splints
Heel pain
Tight calves
Calluses
Knee pain
Patellar tendonitis
Tight hip flexors
Back pain
Sciatica
Herniated disks
NCBI Resources
Muscle imbalances in the hip, such as tight hip flexors, can cause low back pain � or at least contribute to it. When the hip flexor muscles are too tight, it causes what is known as an anterior pelvic tilt.�Hip flexors�can become too tight if the person sits for extended periods of time or engages in activities like cycling and jogging. A chiropractor can guide you through exercises that will help release the tight muscles and stop the micro spams that occur as a result.
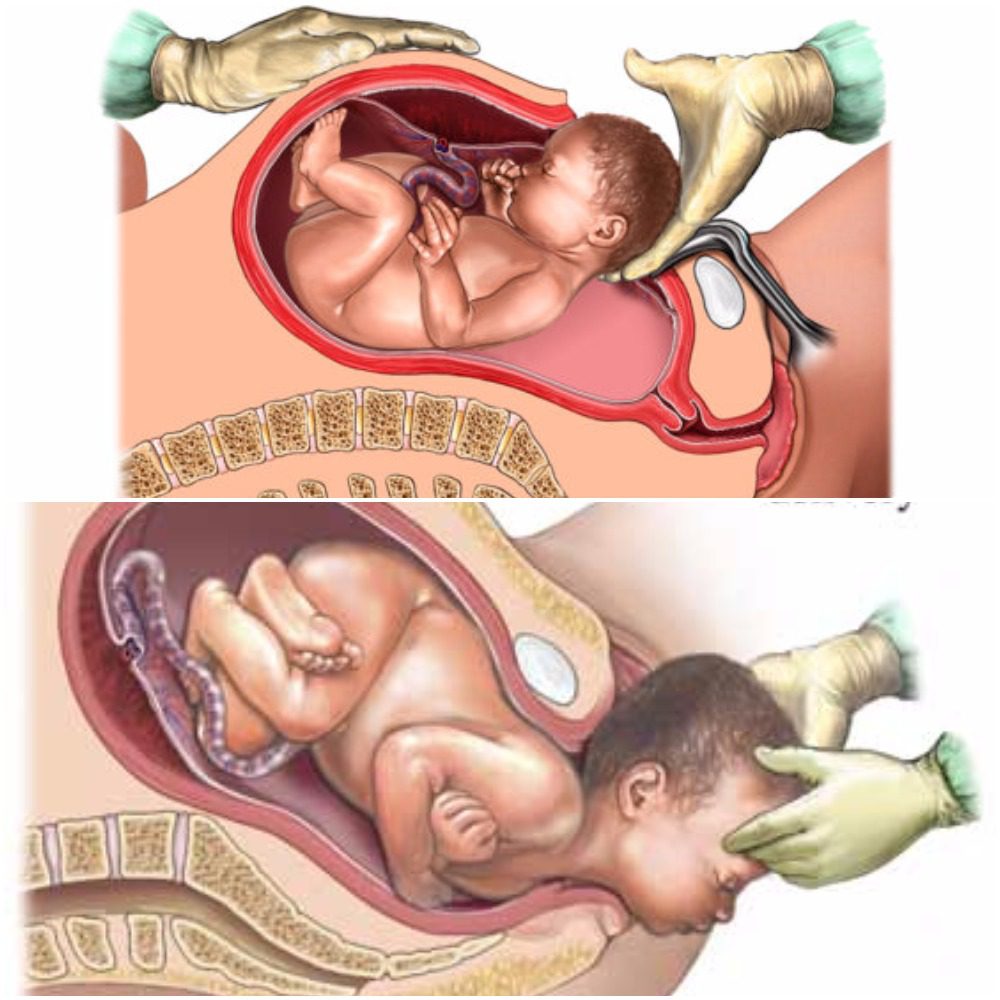
As humans, we depend on microbiomes to stay alive. Microbiomes are essential in fighting off germs and maintaining health. The development of microbiomes begins in utero where the microbes have been isolated to the placenta, fetal membranes, amniotic fluid, and umbilical cord blood, but are mainly transferred from mother to child during birth in a process referred to as “seeding” (1,2). “Seeding”� occurs as the child passes through the mothers vaginal canal and becomes coated in her microbiome. In addition to this, small amounts of microbiomes get transferred to the child as the mother breastfeeds. This early introduction from mother to infant serves as an inoculation process with long term health outcomes for the newborn (2). With the number of cesarean births being higher this decade than in the past, you may find yourself asking, “How does a cesarean birth affect my child’s microbiomes?”
Vaginal
With vaginal births still being the most common way of delivery (68%), these children are seen to have overall better health throughout their lifetime than those born via cesarian (2). Vaginal birth is the most effective way to spread the microbiomes to the child’s skin, but studies have found that microbiomes do differ between ethnic groups. Microbiomes are made up of multiple bacterias and specifically, women with a higher pH have a smaller community of protective biomes. It has also been seen that the gut microbiota in pregnant women with gestational diabetes, tend to have an increased abundance of disease-associated microbes (2). That being said, the pH and mothers gut microbes play a significant role in the types of microbiomes that get transferred to their child.
Cesarean
There are generally two ways a child ends up being born via cesarean, labor ending in a cesarean, or a planned cesarean with no labor attempted. Children who are born via cesarean with labor attempted first, have a slightly higher number of microbiomes due to the vaginal fluids exposed to them during labor than that born elective cesarean. The most effective way a mother can transfer microbiomes to their newborn via cesarean is to “incubate” a cloth for 1 hour in their vaginal canal. When the infant is born,� the doctors rub the child’s mouth, eyes, and skin with the cloth that was previously incubated within minutes after birth (2). This process ensures that the child will have microbiomes more closely related to those born vaginally. Children born elective cesarean without using the incubation method, show fewer gut microbiomes related to their mother, but rather have more skin and oral microbes, and bacteria due to the operating room (2).
Children who are born via cesarean, whether labor was attempted first or not, are more likely to develop immune-related disorders such as asthma, allergies,� inflammatory bowel disease, and obesity (2). This is directly linked to not being “seeded” by the mother. Furthermore, adults who were born via cesarean contain a fecal microbiota that is drastically different than adults who were born vaginally (2).
The purpose of the female reproductive system is to reproduce and birth. Therefore, the best route will always be vaginal if it is safe for baby and mom. This being said, a cesarean is not a bad way to bring a child into the world. The child will just face more skin irritability and have a greater risk of developing health issues due to not receiving the same microbiomes as a child born vaginally. – Kenna Vaughn, Health Coach Insight
References:
(1) Aagaard, Kjersti, et al. �The Placenta Harbors a Unique Microbiome.� Science Translational Medicine, U.S. National Library of Medicine, 21 May 2014, www.ncbi.nlm.nih.gov/pmc/articles/PMC4929217.
(2) Dunn, Alexis B, et al. �The Maternal Infant Microbiome: Considerations for Labor and Birth.� MCN. The American Journal of Maternal Child Nursing, U.S. National Library of Medicine, 2017, www.ncbi.nlm.nih.gov/pmc/articles/PMC5648605/.
As people grow into adults, maintaining normal flexibility gets to be much more challenging and losing flexibility can result in a lot of pain to the musculoskeletal system.
Unfortunately, many of us do not retain flexibility throughout the day, even when attempting to be active. Many jobs are largely sedentary, and even leisure activities keep us stuck in one place. In order to remain functional, joints and muscles need to be used, which means they need to be properly stretched without being overworked. The balance is often very delicate, fortunately, chiropractic adjustments increase flexibility.
Chiropractic’s Role in Flexibility
Most adults are not concerned with being able to twist like a pretzel, however, they do want to be able to maneuver through daily life without a lot of pain. One of the main things accomplished in most chiropractic visits is that the chiropractor will look for misalignments in the spine and seek to correct them with a combination of chiropractic adjustments and exercises.
Adjustments
When the spine is misaligned it can affect many different areas of the body including flexibility. Someone who is not flexible will have a limited range of motion (ROM) and treatments are designed to improve this and restore natural posture.
But being flexible is about more than moving better. When the body is stiff, even simple movement results in pain because it is blocked by the misalignment. When this is adjusted/corrected, blood flow improves and the process of improving flexibility becomes less taxing.
Nutrition
There is more to a chiropractor’s day than correcting misalignments in the spine. Chiropractic is holistic in nature and in order to be truly successful, it relies on the patient to be a cooperative participant in treatment. Giving nutritional advice is a big part of this.
While advice can vary from patient to patient, generally, when a person struggling with flexibility adds protein and fatty acids into their diet it can help joints and muscles to be properly nourished. People should also monitor their intake of processed and pre-packaged foods as these can contribute to inflammation.
Training Exercises
Because of many factors in our lives, as well as the effects of aging, people’s range of motion inevitably decreases as time goes by, especially if nothing is purposefully done to maintain it. Flexibility exercises are commonly strongly suggested by chiropractors as they strive to help their patients with range of motion (ROM) and flexibility issues.
In many cases, such as those where someone is suffering from tendinitis or bursitis, the truly therapeutic exercises are resistive exercises. These, however, are limited, unless a higher level of flexibility is achieved.
Flexibility programs are implemented in order to make a given joint have a wider level of extensibility, which may be achieved by either traditional static stretching or Proprioceptive Neuromuscular Facilitation (PNF) techniques, which incorporates a slow reversal hold.
Working with a chiropractor on a regular basis for help in gaining flexibility can help assure that a patient moves forward at an appropriate pace that is in line with their age and fitness level. This will help them achieve a higher level of success in their chosen sport or similar activity, and/or become more productive in their daily lives while experiencing less pain.
*FIX BAD POSTURE* with Custom Orthotics | El Paso, TX (2019)
Proper Posture
Your spine does more than keep your body upright: it�s the brain that communicates to the rest of the body. Posture even affects your emotional well-being, including self-confidence!
Poor posture takes a serious toll on health. Here are a few of the negative results:
Muscle soreness
Subluxations
Blood vessel constriction
Nerve constriction
As the years go by the problems worsen, which results
Maintaining proper posture involves sitting, standing, and lying down properly. Here is an excerpt from the American Chiropractic Association website on how to:
Sit the right way
Keep your feet on the floor or on a footrest, if they can’t reach the floor
Don’t cross your legs. Your ankles should be in front of your knees
Keep a small gap between the back of your knees and the front of your seat.
Your knees should be at or below the level of your hips.
Bear your weight primarily on the balls of your feet.
Keep your knees slightly bent.
Keep your feet about shoulder-width apart.
Let your arms hang naturally down the sides of the body.
Lie down the right way
Find the mattress that is right for you. While a firm mattress is generally recommended, some people find that softer mattresses reduce their back pain. Go with your comfort
Sleep with a pillow. Special pillows can help with postural problems resulting from a poor sleeping position
Avoid sleeping on your stomach
Healthy Feet Equals A Healthy Spine
The feet are complex structures which function�to provide protection and support to the body in relation to the spine and head posture. The feet are essential towards balancing the body�s entire weight, allowing it to walk, run, stand, and, jump. Consequently, foot complications may cause severe issues throughout the spine, hips, knees, and ankles if left untreated.
Gait & Chronic Postural Pain
Chiropractic care can be effective for treating injuries or conditions such as plantar fasciitis, Achilles tendonitis, and ankle sprains, among others. Foot health is essential towards establishing the body�s proper support and balance, together with a proper spinal posture. In the presence of foot complications, chiropractic treatment can be used to achieve long-lasting health.
NCBI Resources
Flexibility is a critical component of keeping your body fit and healthy. Research shows that people who are more flexible are better able to reach their�optimum fitness level. It can also help to prevent injury and reduce your risk of conditions like arthritis and other�chronic diseases.�They also have a better range of motion and mobility as they age.
Golfer�s elbow is a condition that affects far more than those that golf regularly. According to Dynamic Chiropractic, golfer�s elbow can affect violinists, construction workers, tennis players, bikers and more. It’s more an expression similar to tennis elbow.
Anyone who overuses the elbow can find themselves with pain inside the forearm and elbow, pain that is unlikely to go away without treatment.
While medication and surgery can be options for treatment, chiropractic provides a non-invasive, effective way to relieve golfer�s elbow without the side-effects that come with surgery and medications.
What is it?
The joint and muscles on the inside of your elbow are activated during so many activities�pretty much every time you squeeze, grip or throw something, you use them. Even when you are doing less athletic activities like texting or typing at a keyboard, you are activating the muscles, tendons, and ligaments surrounding your elbow. It is not surprising that they can be overused, especially during work activities or leisure activities that you love so much you play all the time.
Golfer�s elbow is considered an overuse injury�an injury caused by using one or more parts of the body so much that they cannot recover quickly enough. Inflammation becomes constant, scar tissue can develop and pain becomes a regular problem.
How Chiropractic Helps Golfer�s Elbow
Chiropractic care is ideal for the treatment of golfer�s elbow. For some sufferers, coming to the chiropractor is the first and obvious choice. For others, going to the doctor is the first place they start.
Once they find that prescription medications are not alleviating the problem, they may be presented with the idea of surgery. Most people are hesitant to go through surgery if they do not have to, which is understandable. They reach out to a chiropractor because they are looking for an alternative that will help them heal without the pain and uncertainty that surgery brings.
At the chiropractor, you will find non-invasive, drug-free treatments that work to return your range of motion, reduce inflammation and break up the scar tissue in the soft tissues surrounding your elbow joint.
Chiropractic Treatment
Once you visit a chiropractor you will be given a careful, thorough physical examination to determine the nature of your problem and its cause. With golfer�s elbow, the problem is fairly obvious, so your chiropractor will focus on understanding exactly what your golfer�s elbow consists of�including your level of pain, your range of motion and the effects it is having on your day-to-day movement.
Some of the ways chiropractic can treat golfer�s elbow include:
Break Scar Tissue Up
Scar tissue keeps your muscles from operating correctly and causes pain. Chiropractors have methods for breaking up scar tissue to return normal muscle function, including active release.
Returns Mobility
Joint manipulation from your chiropractor is designed to make your joints move properly. The chiropractor will gently move your elbow back and forth to realign it and to ensure that it goes as far as it should go, and no further.
Reduces Inflammation
Inflammation is what causes much of the pain you are experiencing in your elbow. Joint adjustments and breaking up scar tissue are excellent ways to reduce inflammation. As the inflammation reduces the body can heal more easily and the pain will lessen.
We Can Get You the Help You Need
As you know, golfer�s elbow can be painful and make it difficult to do the things you need to do. Let us help you get some relief. Please contact our office today to schedule an appointment with our chiropractic team.
As you move into your senior years, you may expect some discomfort and loss of mobility. Aging is hard on the body. But it is important to understand that there are things you can do to feel better. Regular exercise, a healthy diet, and chiropractic care can all make your senior years active and thriving.
How Chiropractic Can Make Your Senior Years Fantastic
The benefits of chiropractic for seniors can be considerable, including:
1. Takes away the pain.
If you are experiencing pain due to spinal or joint issues, chiropractic can help. Chiropractic care focuses on providing pain relief without the need for prescription medications or surgery.
Research has demonstrated the effectiveness of chiropractic for pain relief. In fact, one study showed that chiropractic was considerably more effective than prescribed medications. Unfortunately, many seniors assume that their pain is here to stay when it may be reduced or eliminated through regular chiropractic care.
2. Improves balance.
Seniors who are suffering from balance and coordination issues often have problems with the cervical spine, the technical term for the neck. When degenerative disc disease or other injuries disrupt the function of the mechanoreceptors located in the neck responsible for sending to the brain important information related to balance, then problems with balance can result.
Chiropractic adjustments and other related therapies are quite effective in treating neck injuries and degenerative disc disease. Regular adjustments from your chiropractor may be enough to help you get your balance back.
3. Improves mobility.
Injuries and aging can lead to a loss of range of motion, both in the spine and in the extremities. Fortunately, chiropractic care is designed to help you regain range of motion.
Your chiropractor has a variety of treatment methods to heal existing injuries while also improving range of motion. It may take several treatments to achieve the results you want, but a few visits to the chiropractor are well worth the increased range of motion you will enjoy.
4. Wear and tear on the joints are reduced.
The spine and joints need to be aligned to minimize wear on discs, bones, and other tissues. When you go for an extended period of time with a misaligned spine, it will increase the rate that your joints wear down.
One of the major benefits of chiropractic care is the way it keeps your whole body in alignment. As long as alignment is maintained, wear is minimized. Of course, alignment is lost in day-to-day life, but you can get it back by revisiting the chiropractor.
When you visit your chiropractor, he or she will ask you several questions and listen to your story to better understand the challenges you are dealing with. Once the chiropractor understands your situation, he or she will design an overall treatment plan designed to help you be as healthy as possible. Seniors that get regular chiropractic care often say they feel much better than they did before, which allows them to do more of the things they love to do.
The information herein is not intended to replace a one-on-one relationship with a qualified healthcare professional or licensed physician and is not medical advice. We encourage you to make your own health care decisions based on your research and partnership with a qualified health care professional. Our information scope is limited to chiropractic, musculoskeletal, physical medicines, wellness, sensitive health issues, functional medicine articles, topics, and discussions. We provide and present clinical collaboration with specialists from a wide array of disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the injuries or disorders of the musculoskeletal system. Our videos, posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate to and support, directly or indirectly, our clinical scope of practice.* Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We provide copies of supporting research studies available to regulatory boards and the public upon request.
We understand that we cover matters that require an additional explanation of how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
According to the American Chiropractic Association (ACA), approximately 31 million Americans deal with some form of low back pain. Fortunately, there are steps you can take to lessen the pain you are experiencing. Taking care of yourself � including maintaining a healthy weight and regular exercise � can help prevent back pain. And when you do experience back pain, chiropractic treatment and stretching can often ease your symptoms.
Prepare for Stretching
Before we get to the stretching, we recommend preparing for your stretching session so you can stretch comfortably and safely. Tips for stretching include:
Ease into it. Stretching should be done gently and smoothly, traveling from stationary to a position slowly and carefully. Avoid bouncing, which can tear muscles.
Stretching should not hurt. You should not feel significant pain when you stretch. As you move into your stretch, listen to your body and stop before you start to feel pain. Stretching should feel good, not painful.
Wear comfortable clothing. Wear loose clothing that will allow you the full range of motion.
Choose an area to stretch that is flat and clean. Choose an area that will be comfortable and well-suited for your activity.
Use padding when necessary. If you are going to be stretching on a hard surface, a little padding can make things much more comfortable.
Hold each stretch 15-30 seconds, and repeat at least 2 times. Holding a stretch lets the muscles elongate, and repeating the stretch improves your results. Repeat the stretch four times for maximum benefit.
Modify to fit your needs. Everyone must work within their limitations. When you try a stretch and you find it is not working for you, try to modify it to suit your needs. You can find modifications to most popular stretches online.
Three Stretches that Are Great For Back Pain
1. Children’s Pose
The name Child�s Pose comes from yoga, where this stretch is often used to begin each session of stretching. Child�s Pose is so popular because it is gentle and effective, and just about anyone can do it.
To do Child�s Pose, get down on your hands and knees. To begin with, place your knees slightly wider than hip-width. Flatten the tops of your feet to the floor, toes pointing behind you. Slowly move your hips back over your feet. Once you have rested your buttocks on your ankles, stretch your arms out in front of you. Feel your lower back stretch out as you hold the pose.
2. Knees/Chest
Lying on your back, use your hands to pull your knees up to your chest, rounding out your back in the process. You can interlace your fingers to hold your knees in position. If you like, hug your knees more tightly to your chest and rock left to right. To enhance the stretch, slowly bring your chin towards your chest.
3. Spine Twist
Lying on your back, stick each hand out to the side of your body to create a T shape. Bring the right knee up to your chest while keeping the left leg straight on the floor. Use your left hand to gently pull your knee higher, then pull the knee across your body to the left. Try to keep your right shoulder on the floor. Repeat on the left side.
Contact For Customized Stretches
If you are suffering from back pain, please schedule an appointment to meet with our chiropractic team. We can help design a custom stretching plan to help you ease your back pain.
El Paso Back Clinic Chiropractor Personal Injury Attorney Recommended
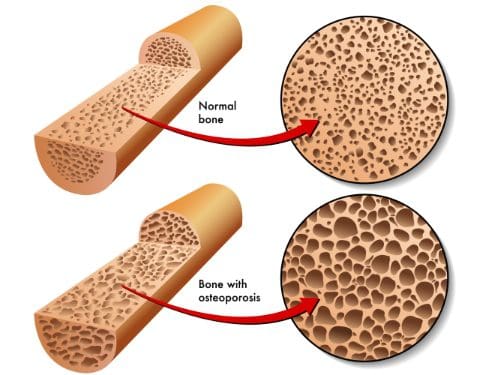
Osteopenia and osteoporosis, two very similar conditions, that are defined as decreased bone density, but osteopenia is far less. However, it is still a problem due to an increase of breaking a bone because of bone fragility.
Symptoms
Osteopenia usually doesn’t cause symptoms unless a bone is broken. However, some patients who present with osteopenia complain of dull back pain.
Symptoms associated with osteoporosis include the following:
Back pain, caused by a fractured or collapsed vertebra
Loss of height over time
A stooped posture
A bone fracture that occurs much more easily than expected
The causes and those at risk?
Women (primarily small-boned Caucasian and Asian) are most at risk for both conditions, primarily those who are age 65 or older as well as women who are postmenopausal. However, men can also be affected.
Anyone who meets any of the criteria for being at risk for either of the bone conditions should be evaluated. Often, catching the conditions early can make a significant difference in the effects that they have on the body and in some cases, can even be arrested so that they don�t progress.
Some of the common causes of both conditions include:
Lifestyle habits
Smoking
Insufficient calcium
Sedentary lifestyle
Excessive alcohol consumption
Vitamin D deficiency
Carbonated beverages
Medical Situations
Bulimia, anorexia, and other eating disorders
Estrogen deficiency in women
Certain hormone imbalances
Overactive thyroid
Certain treatments including radiation and chemotherapy
Low testosterone in men
Medications including anti-seizure, hydrocortisone, and steroids
Health issues
Tumors
Cystic fibrosis
Crohn�s disease
Digestive issues
It should also be noted that certain types of diets, particularly those that advocate extremely low fat, or no fat can also cause problems. Vitamin D is necessary for calcium absorption in the body, but vitamin D is a fat-soluble vitamin meaning the body requires some fat in order to make use of it. When there is inadequate fat, the vitamin cannot be absorbed and in turn, calcium cannot be absorbed.
A family history of osteopenia, osteoporosis, or low bone mass can increase a person risk by 50% to 85%.
A Diagnosis
Bone mineral density (BMD) tests are used to diagnose both osteopenia and osteoporosis by measuring the calcium levels in bone. This type of test can also provide an estimate of how much at risk a person is for bone fractures.
This test is painless and non-invasive. It is usually performed on the heel, shin bone, wrist, spine, finger, or hip.
Two common types of these tests are radiographs, a standard diagnostic tool for osteopenia, and Dual Energy X-ray Absorptiometry (DEXA). A DEXA scan is essentially a low energy x-ray so patients are not exposed to as much radiation as they would be if they had a regular x-ray. The results are attained by comparing the score (measurements were taken) to scans of individuals who do not have the condition.
Once the score is measured and compared, it is assessed using a chart that identifies the level or risk:
+1.0 to -1.0 – Normal bone density
-1.0 to -2.5 – Low bone density
-2.5 or higher – At risk for osteoporosis
What Treatments Is Available?
As with most conditions, prevention is the most effective treatment. If you have a family history or fall under any of the risk factors, there are things you can do to minimize the effects or prevent the conditions completely.
Your chiropractor can talk to you about lifestyle changes, exercise, and diet as well as supplements that you can take. Chiropractic adjustments can also be effective for many patients with osteopenia and osteoporosis as long as the chosen technique is a low force technique like Activator.
Many patients find these natural treatments preferable to any medications that may be prescribed. The most important thing you should do, though, is get a bone density test if you are in an at-risk category, are a woman who is postmenopausal or age 65 or older.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine