Health coaches are becoming more and more crucial as modern and naturopathic medicine continues to improve. More than ever, the healthcare field is progressing at high speeds and professionals do not always have the time available that some patients desire. Here is where health coaches get involved. Basically, the position of a health coach was produced to fulfill the emptiness in several doctor offices. Many physicians contribute but don’t have the time or tools to help each individual and assist in constructing healthy habits on a day to day basis. But, health coaches are available to be a supportive mentor who guides and assists patients in making healthy lifestyle changes. Many patients who seek assistance to change their lifestyle are those afflicted by some kind of chronic pain, headaches, or joint swelling.
In the previous weeks, we have defined and explained what a health coach is and what they really do, as well as the first four steps a health coach might take with a patient. Throughout this article, the fifth and sixth steps will be broken down and analyzed.
Need a refresher? No problem!
Health Coaching in El Paso: Part 1 can be found by clicking�here
Health Coaching in El Paso: Part 2 can be found by clicking�here
Health coaching in El Paso: Part 3 can be found by clicking�here
Step 5: Visualizing Your Best Self
�
This step is extremely crucial. The reason being, without a vision of where an individual wants to be, they can easily get lost on their way to achieving a goal. A vision statement is not intended to be a specific sentence, but rather a loose description of what / who the patient is trying to become.
In order to create this statement, a health coach will work with the patient to clearly identify their skills, interests, and strengths. These are oftentimes similar to the items listed on the values sheet the patient filled out while the health coach was working with them back in�step 1. Other times, the health coach will assist the patient with their vision statement by asking things like:
What are you naturally good at?
What have you always wanted to see, do, or create?
What would help you feel more fulfilled?
In addition to these questions,� the health coach might encourage the individual by steering the conversation in a way that is related to their best self. With the help from a health coach, the patient can reflect and describe their best self as well as the emotions connected to their best self (thinking, feeling, and doing). A coach will also provide critical thinking questions related to a patient’s best self such as:
How do you know you’re there?
How do you know you’re not there?
How can you remember to be your best self and not slip back into the old ways of being?
Step 6: Creating A Plan For Resiliency
It is simply human nature that all people react to stressful situations differently.� However, one thing that is guaranteed is people will need a plan to get back on track. Undergoing life changes is not a simple task, but having a plan is.�An approach for building resilience must be tailored to the specific individual. A health coach will ensure the individuals that falling off track is natural, but how you get back on track is what counts. It starts with reflecting, seeking support, and making a plan to move forward.
When a patient is placed in a stressful situation, it is key they take a moment to recognize the situation and think about how they are feeling. During the moment, it may be difficult but with practice, reflection, and help from a health coach, the process becomes easier.
The best tips when it comes to addressing resiliency are to develop connections, set daily intentions, reflect on experiences, practice self-care, and be proactive.
A health coach may encourage a journal to help patients celebrate small victories and take responsibility for their own happiness. In addition to this, there are other resources available the patients may utilize such as books, self-help support groups, and asking themselves, “What do I typically find helpful in a stressful situation?”.
By utilizing a health coach and implementing these 6 steps into one’s life, the benefits are unbelievable. Identifying values, determining goals, building a plan for action, tracking progress and results, visualizing the best self, and creating a plan for resiliency will help individuals reach their health goals better than before.
By working with a health coach and remembering these exercises, individuals are extremely likely to be successful. Not only do they have someone for accountability, but they are learning ways to become more independent and thoughtful when it comes to their health. A positive community offers support that many individuals need to thrive. Naturopathic medicine and functional approaches are becoming more recognized for their ability to work on a variety of individuals. Take advantage of all the resources around that are there to help you.�– Kenna Vaughn, Senior Health Coach�
All information and resources for this post came from an Integrative Practioner article titled, “A Six-Step Approach To Health And Wellness Coaching: A Toolkit for Practice Implementation” and can be found by clicking�here; as well as listed below in the proper bibliography.
*The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at�915-850-0900.
Miller, W. and Rose, G. (1991). Motivational Interviewing: Preparing People to Change Addictive Behavior. Guilford Publications.
Pecoraro, Wendy. �A Six-Step Approach to Health and Wellness Coaching: A Toolkit for Practice Implementation.��Official Media Integrative Practitioner, 17 Oct. 2019, www.integrativepractitioner.com/resources/e-books/a-six-step-approach-to-health-and-wellness-coaching-a-toolkit-for-practice-implementation.
Trzeciak, S. and Mazzarelli, A. (2019). Compassionomics. Studer Group.
If you are experiencing any of these situations, why not try a HIIT workout to relieve these symptoms.
Everyone can agree that they do not have enough time to exercise. When asked why people will not work out, one of the reasons is that due to their hectic lifestyle, the lack of time comes out on top of it all. The U.S. Department of Health and Human Services recommends that adults should get between 150 and 300 minutes per of moderate-intensity. There is a way to cut that time commitment in half by opting for high-intensity workouts instead. With high-intensity interval training or HIIT, it is one of the proven ways to reap all the benefits of exercise in less time. Research shows that spending less time doing HIIT may even be better than spending more time doing less intense exercises for individuals.
What is HIIT?
High-intensity interval training or HIIT alternates explosive bursts of full-throttle efforts with periods of recovery. It can either be rest or a lower-intensity exercise. In many fitness centers and gyms, HIIT workouts often include both cardio and resistance training; however, HIIT workouts can be done as a strictly cardio routine.
During intense burst in a HIIT workout, a person is working out at around 80 percent of their max heart rate for 15 seconds to a few minutes. Between each of those periods, a person is either slowing down or resting completely to let their heart rate come back down to around 50 percent.
A person can calculate different target heart rates by using an online calculator. During a workout, a person can wear a heart rate monitor to keep track on much they are exerting themselves. For a lower-tech option, Denver-based certified personal trainer Lindsay Kelly recommends the “talk test.” The way the “talk test” is when a person is doing their target intensity heart rate like sprinting; for example, it should be hard to speak more than two words without taking a breath. Then when they are in the recovery period, the reverse factor is real.
Why HIIT Works
HIIT is so effective because it allows a person to exercise at a higher intensity for such a short period. The exertion gets the heart working and the blood pumping better than any moderate-intensity exercise can bring with their prolonged periods of rest.
The Importance of Rest
While a person might not realize it, the rest periods are built into the HIIT workout and are a critical part of the routine. They force the body to adjust to a very different state of activity, which is excellent for cardiovascular conditioning.
Feel The Afterburn
Another benefit of a HIIT workout is that even after a person is finished with their HIIT workout, it keeps on working for them. Research shows that when individuals keep on burning calories after their HIIT workout at a higher than they would after a continuous exertion workout. It is commonly known as the “afterburn effect,” and it helps people extend the benefits of their efforts.
The Benefits of HIIT
Researchers have been studying HIIT extensively, and the results are precise: HIIT workouts are better than continuous exercise when it comes to improving health in a variety of ways. One of the health benefits of a HIIT workout is that it improves cardiorespiratory fitness, which is the health of the heart and breathing. This matters to a person who is trying to get in as much exercise as possible with little time because cardiorespiratory fitness is a primary factor in the risk of diseases and death. Studies have shown that HIIT workouts can increase cardiorespiratory fitness at twice the rate of continuous exercises.
The health benefits of HIIT does not stop there, as other research studies have shown that HIIT can help with the following areas of the body.
Endurance
By improving cardiorespiratory fitness, HIIT can improve a person’s stamina. What it does is that it enhances the body’s ability to consume and use oxygen. One study has compared a regular endurance training to HIIT by looking at how they affect maximal oxygen consumption known as VO2max. The research found out that HIIT was superior to endurance training by improving VO2max in healthy young to middle-aged adults. Once a person starts to build their endurance, they can increase the length or the intensity of the HIIT working periods and enjoy the significant health benefits it provides.
Heart Health
One of the significant contributors to cardiovascular disease and death is high blood pressure, and one of the best ways to keep it in check is through regular exercise. The traditional recommendation for blood pressure modulating has been to exercise at moderate intensity for at least 30 minutes on most or all day so that way high blood pressure will not transform into hypertension. Several studies have suggested that HIIT may be an even better option, and one study shows that while both continuous exercise and HIIT helps with blood pressure control, HIIT is the only workout to help reduce arterial stiffness. Arterial stiffness is a predictor of cardiovascular disease in people with high blood pressure.
Brain Function
When a person feels that that mental clarity after a good workout, it is not their imagination. The brain and mental health benefits of exercise are well documented. Research shows that HIIT helps explicitly improve the cognitive function, including short-term memory, verbal memory, attention, and processing speed in the brain. HIIT also increases the amount of oxygen that the brain gets from the blood.
Diabetes Management
Since exercise is an essential part of diabetes management, research shows that HIIT may be a wise exercise choice for anyone who has type 2 diabetes. Studies have shown that HIIT workouts can improve endothelial function, insulin sensitivity, glucose control, and other health effects of diabetes that are better than continuous exercise.
Conclusion
HIIT workouts are perfect for anyone who does not have enough time out of their busy schedule. With the alternating burst of exercises and periods of recovery, HIIT workouts are beneficial to anyone with a short amount of time to complete them. HIIT includes both cardio and resistance training and works with the entire body. Some products are excellent in countering the metabolic effects of temporary stress and supporting the body�s system.
The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
References:
Chobanian, Aram V., et al. �Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure.� AHA Journals, 1 Dec. 2003, www.ahajournals.org/doi/full/10.1161/01.hyp.0000107251.49515.c2.
Council on Sports, HHS Office. �Physical Activity Guidelines for Americans.� HHS.gov, US Department of Health and Human Services, 1 Feb. 2019, www.hhs.gov/fitness/be-active/physical-activity-guidelines-for-americans/index.html.
Dupuy, Oliver, et al. �Effect of Interval Training on Cognitive Functioning and Cerebral Oxygenation in Obese Patients: A Pilot Study.� Latest TOC RSS, Medical Journals Limited, 1 Nov. 2014, www.ingentaconnect.com/content/mjl/sreh/2014/00000046/00000010/art00016.
Francois, Monique E, and Jonathan P Little. �Effectiveness and Safety of High-Intensity Interval Training in Patients with Type 2 Diabetes.� Diabetes Spectrum: a Publication of the American Diabetes Association, American Diabetes Association, Jan. 2015, www.ncbi.nlm.nih.gov/pmc/articles/PMC4334091/.
Gillen, Jenna B., and Martin J. Gibala. �Is High-Intensity Interval Training a Time-Efficient Exercise Strategy to Improve Health and Fitness?� Applied Physiology, Nutrition, and Metabolism, 27 Sept. 2013, www.nrcresearchpress.com/doi/10.1139/apnm-2013-0187#.XdQT5y2ZP1J.
Guimar�es, Guilherme Veiga, et al. �Effects of Continuous vs. Interval Exercise Training on Blood Pressure and Arterial Stiffness in Treated Hypertension.� Hypertension Research: Official Journal of the Japanese Society of Hypertension, U.S. National Library of Medicine, June 2010, www.ncbi.nlm.nih.gov/pubmed/20379194.
Milanovi?, Zoran, et al. �Effectiveness of High-Intensity Interval Training (HIT) and Continuous Endurance Training for VO2max Improvements: A Systematic Review and Meta-Analysis of Controlled Trials.� SpringerLink, Springer International Publishing, 5 Aug. 2015, link.springer.com/article/10.1007/s40279-015-0365-0.
Pescatello, Linda S, et al. �American College of Sports Medicine Position Stand. Exercise and Hypertension.� Medicine and Science in Sports and Exercise, U.S. National Library of Medicine, Mar. 2004, www.ncbi.nlm.nih.gov/pubmed/15076798.
Unknown, Unknown. “Is High-Intensity Interval Training Right for You?” Fullscript, 12 Nov. 2019, fullscript.com/blog/high-intensity-interval-training.
Weston, Kassia S, et al. �High-Intensity Interval Training in Patients with Lifestyle-Induced Cardiometabolic Disease: a Systematic Review and Meta-Analysis.� British Journal of Sports Medicine, BMJ Publishing Group Ltd and British Association of Sport and Exercise Medicine, 1 Aug. 2014, bjsm.bmj.com/content/48/16/1227.short.
Q: Dr. Jimenez, I read one of your articles about physical therapy and spinal stenosis exercises that focus on stretches for relieving pain. I was wondering if it was also possible to do aerobic exercise with a spinal condition and can you recommend a safe cardiovascular program?
I’m a 65-year-old with spinal stenosis, and I want to stay in shape. I try to ride a stationary bike for 20 minutes at least 2 times a week, but with my low back pain, I don’t always finish the workout.
How else can I stay in shape
A: I do recommend aerobic exercise for everyone, but especially for people with spinal conditions.
Aerobic exercise increases the blood flow to the body’s tissues, and people with high levels of cardiovascular fitness generally do better dealing with spinal problems.
However, before anyone with a spine condition or any medical condition for that matter, starts a wellness and fitness program, they should check with their primary caregiver, to clear the individual as fit to exercise.
Example: Someone with cardiovascular (heart problems) can have restrictions when it comes to certain types of exercise.
A physical exam will make sure your body is ready for exercise.
Physiotherapist assisting a senior woman with exercise ball at a chiropractic rehabilitation clinic
Low-impact aerobic exercise is recommended�
Walking
Swimming
These are excellent examples of low-impact aerobic exercise. They increase heart rate and are easy on the body.
Riding a stationary bike is another recommended form of low-impact aerobic exercise.
It can be tiring, but if recommended by a caregiver/therapist, then realize they did so for a reason/s to get you healthy.
By biking, you are building up endurance, and that is exactly what you want, as it speeds up recovery.
Walking is a great exercise for spinal conditions. It is low-impact, and you can control the pace to fit your needs.��
Daily walks after lunch or after getting home are a great way to exercise.
If exercise does begin to increase back pain or another type of pain, tell your caregiver or physical therapist right away.
The phrase, no pain, no gain does not apply when there are spinal conditions. So do not try to push through the pain or think that the hurt is good.
Also, do not try to do take on too much right away. Even if you feel good, follow the fitness plan.
But if you want to mix it up, discuss with your chiropractor/physical therapist if adding walking and swimming to the plan will be beneficial, as well.
It can be tempting to not exercise with a spinal condition. But remember that if there is no movement at all, you could make the pain worse. Knowing what your body can handle and sticking to a workable schedule, these healthy steps will relieve you and help with your low back pain.
Chiropractic Care Sports Injury Rehabilitation El Paso, TX
Daniel Alvarado, the owner of Push-as-RX Fitness, discusses how he carries out his PUSHasRx Functional Fitness Workouts personal injury rehabilitation and athletic training program as a part of Dr. Alex Jimenez’s chiropractic rehabilitation plan.
Physical therapy (PT), also referred to as physiotherapy, is one of the allied health professions which, by utilizing mechanical force and motions (bio-mechanics or kinesiology), manual therapy, exercise therapy, and electrotherapy, remediates impairments and promotes mobility and purpose.
Physical therapy is used to enhance a patient’s quality of life through:
Examination
Diagnosis
Prognosis
Physical intervention
NCBI Resources
Exercise is an essential part of good health. It can help with weight loss and plays a crucial role in preventing many chronic health conditions like hypertension, diabetes, and heart disease. Regular exercise has also been shown to help with depression and anxiety. It is what nature intended; as humans, we are supposed to be active. The more active you are, the better you will look and feel � and the healthier you will be.
Increase in sports-related fractures among young and active people
Any type of bone fracture, especially when the spine is involved, comes with the most common and debilitating symptom is severe pain.
Managing pain correctly is vital to the proper healing of a fractured bone.
Unfortunately, the common treatments prescribed to manage fracture pain can cause significant side effects, especially when used beyond the short-term or acute phase of pain.
Bone fractures cannot be always be avoided, but when it comes to osteoporosis, everyone can take steps to help minimize the risk of developing the condition.
How to Prevent Osteoporosis and Bone Fracture
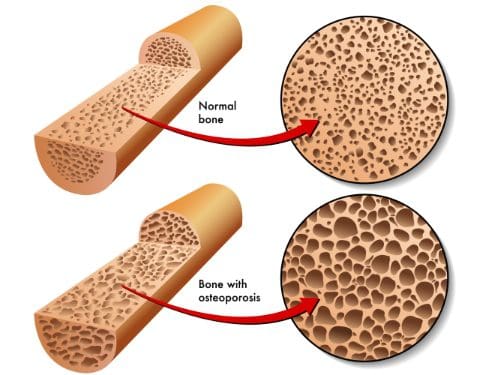
First, understand that osteoporosis is not a normal part of the aging process.
It is an irreversible and degenerative disease that causes bones to become porous over time.
Prevention should begin as early as possible, as this will benefit an individual later in life.
It’s never too late to begin taking steps!
Protecting the bones begins with the most important thing and that is diet.
Most individuals’ diet does not fill the recommended daily values of calcium and Vitamin D.
Both are essential for strong bone health and density.
Diet must be well-balanced with an abundance of:
Green leafy vegetables
Fruit
Dairy sources high in calcium:
Milk
Yogurt
Cheese
However, vitamin D is typically highest in sources of wild-caught fatty fish like salmon and tuna.
Regular exercise is the next important step to help reduce the risk and keep bones strong.
Do exercises that are both:
Weight-bearing (high/low-impact aerobics or walking/jogging)
Muscle-strengthening (weightlifting and exercise bands)
Yoga and Pilates can also help to improve:
Strength
Balance
Flexibility
These are essential in the prevention of bone fractures from falls.
Engage in exercise that you enjoy, this way you will stick with it on a regular basis.
Try for two to three sessions a week if you�re beginning and try to work up to five.
While diet and exercise are extremely important to prevent osteoporosis, there are some areas that should be removed from the lifestyle or limited.
Smoking
Alcohol
These chemicals in bothcigarettes and heavy alcohol consumption are known to be significant contributors to bone loss.
Injury Medical & Chiropractic Clinic offers not only chiropractic treatment, but exercise, and diet programs set up by professional life/health coaches that are customized to each patient. Set up an appointment today, we can help!
Chronic Body Pain Treatment El Paso, TX Chiropractor
Aracely Norte suffered a slip-and-fall accident which tremendously limited her ability to work, affecting her quality of life. Due to the chronic pain she experienced, Aracely had difficulty engaging in her regular, everyday responsibilities. After her lawyer recommended Dr. Alex Jimenez, chiropractor, Aracely found the relief she was looking for.
Chronic pain is a common issue that can occur due to a variety of reasons, including injuries and underlying conditions, however, chiropractic care can help eliminate chronic pain symptoms from the source.
NCBI Resources
As with most conditions, prevention is the most�effective treatment. If you have a family history or fall under any of the risk factors, there are things you can do to minimize the effects or prevent the conditions completely.
Your chiropractor can talk to you about lifestyle changes, exercise, and�diet�as well as supplements that you can take. Chiropractic adjustments can also be effective for many patients with osteopenia and osteoporosis as long as the chosen technique is a low force technique like Activator.
The percentage of individuals that are affected by fatigue, headaches, and overall pain is continuously growing. For the most part, these symptoms can all be linked back to a hormone imbalance. Hormone imbalances are more common than individuals realize and can affect people of all ages. Originally, hormone testing was completed through a blood draw (serum testing). However, as science is improving, there are now better, more functional ways of testing.��
As more and more studies are done, it is becoming more clear that salivary testing is superior to serum (blood) testing for hormones. There are two forms in which hormones exist in the human body, free (5%) and protein-bound (95%). Due to the protein-bound hormones being bound, they become too large to pass through into the salivary glands. This meaning that they are not bio-available and can not be delivered to the receptors in the tissues of the body.� The unbound hormones, or free hormones, are the relevant hormones that are found in the saliva. Considering the fact that free hormones are not as abundant, the hormone levels found in saliva are significantly less than those found in serum. However, many patients who are treated with serum hormone results are often overdosed because of the lack of correlation between bio-availability.
Labrix by Doctor’s Data
Similar to the D.U.T.C.H�hormone testing previously discussed, this company Labrix offers a variety of hormone testing as well.
Neurotransmitters:
NeuroBasic: ideal for monitoring therapeutic interventions of neurotransmitter imbalances previously tested or when symptoms are indicating an imbalance. This test measures Serotonin, Dopamine, Epinephrine, Norepinephrine, Glutamate, Glycine, Histamine, and Phenethylamine
Comprehensive Neurotransmitter: best when a comprehensive look at neurotransmitter secretion and metabolism of markers is needed. This test measures Serotonin, GABA, Dopamine, Norepinephrine, Epinephrine, Glutamate, Glycine, Histamine, and Phenethylamineand DOPAC, 3-MT, Normetanephrine, Metanephrine, 5-HIAA, Tryptamine, Tyrosine, Tyramine, and Taurine.
NeuroHormones:�
NeuroHormone Complete Plus:� provides insight on how the HPA axis function may be contributing to patients’ symptoms, such as mood swings, fatigue, and pain. In addition, this test is ideal for those who are at risk for breast cancer, PCOS, or a strong family history of autoimmune disease.�This test is recommended for women only.� This test measures�Estrone, Estradiol, Estriol, Progesterone, Testosterone, DHEA, Cortisol x 4, Serotonin, GABA, Dopamine, Epinephrine, Norepinephrine, Glutamate, Glycine, Histamine, Phenethylamine
NeuroHormone Complete: useful for patients (men or women) who are experiencing any type of mood disorder, addiction, fatigue, chronic illness, confusion, weight issues, low libido, PMS, or chronic pain. This test measures Estradiol, Progesterone, Testosterone, DHEA, Cortisol x 4, Serotonin, GABA, Dopamine, Epinephrine, Norepinephrine, Glutamate, Glycine, Histamine, Phenethylamine.�
NeuroAdrenal: Included in this test is a full diurnal cortisol pattern, DHEA, and 6 primary neurotransmitters to help those with symptoms such as depression, anxiety, addiction, chronic illness, and low libido. This test measures DHEA, Cortisol x 4, Serotonin, GABA, Dopamine, Epinephrine, Norepinephrine, Glutamate, Glycine, Histamine, Phenethylamine
Salivary Hormone:�
Comprehensive Plus: provides an assessment of breast cancer risk. This test is a considerationfor women only who have an increased risk for developing breast cancer, other hormonally sensitive cancers, PCOS or a family history of autoimmune disease. This test measures estrone, estriol, and Estrogen Quotient.
Women’s Helth and breast Profile: includes two risk assessment ratios, the Estrogen Quotient and the Pg/E2 ratio
Comprehensive Hormone: �assessment of hormonal status and endocrine function and includes estradiol, progesterone, testosterone, DHEA and four cortisols. This profile is useful with male and female patients because it looks at the full diurnal cortisol pattern; it is especially important in patients who are experiencing the full diurnal pattern ( weight gain, high blood sugar, elevated lipids, chronic fatigue)
Short Comprehensive: useful in men and women whose primary symptoms are related to sex hormone imbalances (elevated or depressed E2, P or T)
Basic Hormone: a basic evaluation of the sex hormones and a brief glimpse at the adrenal function with the AM cortisol level. Best for men who are experiencing decreased libido, erectile dysfunction, loss os stamina, decreased mental sharpness and metabolic syndrome. Best for women who are experiencing hot flashes, anxiety, night sweats, breast tenderness, irritability, forgetfulness, and acne.�
Comprehensive Adrenal Function: provides insight into the body�s stress response. This test measures sIgA
Adrenal Function: comprehensive view of adrenal function, DHEA, and cortisol levels. This is best for people who are fatigued, nervous, weak, crave sugar, have headaches, irritability, and depression
Diurnal Cortisol: Similar to the test above but for patients who do not need DHEA testing
Melatonin: Provides a snapshot of the sleep/wake cycle during a one day period
Salivary Hormone + CAR :
CAR: has the capability to test all the same markers as above but adds Cortisol Awakening Response “CAR” to all of them.�
For more information regarding testing and hormones tested, please visitlabrix.com��
LABRIX BASIC BOX CONTENTS:
Upon opening every box (no matter the labrix test) the patient will see a requisition form, a billable stamp, and a FedEx envelope. Under these two items, a styrofoam box (insulated cooler) with the imprint “doctorsdata.com” will be present. Once the patient lifts the lid off of the styrofoam box, they will see two more pieces of paper.� The first being a list of symptoms (patient survey) on a white sheet of paper that the patient is to fill out and place back in the styrofoam box and the second a small instruction manual.
Neurotransmitter Tests Breakdown
For the Neurotransmitter Tests, the patient is provided with the basic kit described above. The only sample type required for the neurotransmitter tests is urine.
The contents of the styrofoam box include a small plastic cup, a clear plastic bag consisting of a white tube, a dropper, an absorbent pad, and a Lab-Brix ice pack. The first step is to freeze the ice-pack and keep it frozen until ready to ship.�
In order for this test to have proper results, the patient should collect their sample with their first or second-morning urine upon waking. Then, select on the requisition form which urine ( first or second ) the sample was collected from. It is also important to note on the requisition form what time the patient woke and what time the sample was collected. The urine sample should be collected midstream. Patients will collect their sample in the plastic cup provided, not directly in the tube. Next, the patients will use the dropper provided to transfer 10 ml of the sample from the cup into the tube. Ensure the lid is screwed on tightly and gently rock the tube back and forth for 3-5 seconds to mix the urine with the preservative. The patients will then wrap the absorbent pad around the tube (not inside the tube), and place the sample tube back in the plastic bag. The bag is then to be placed in the freezer for 4-6 hours, and is to be kept frozen until ready to ship!�
Neurotransmitter + Hormone Tests Breakdown
The Neurotransmitter + Hormone analysis tests consist of urine and saliva samples. This basic test kit includes everything above. However, upon opening this styrofoam box the patient will find two plastic bags. The first being a plain plastic clear bag with a dropper, white test tube, and absorbent pad. The second plastic bag is a biohazard bag that has multiple colors on the outside and consists of 4 clear small straws, an absorbent pad, and 4 small saliva collection tubes of various colors.�
The urine sample is instructed to be taken the same way as the neurotransmitter test.
The patient should collect their sample with their first or second-morning urine upon waking. Then, select on the requisition form which urine ( first or second ) the sample was collected from. (Remember, the individual is� to note on the requisition form time they woke and what time the sample was collected). Patients will collect their sample mid-stream in the plastic cup provided, not directly in the tube. Next, use the dropper provided to transfer 10 ml of the sample from the cup into the tube. Be sure to check that the lid is screwed on tightly and gently rock the tube back and forth for 3-5 seconds to mix the urine with the preservative. The patients will then wrap the absorbent pad around the tube (not inside the tube), and place the sample tube back in the plastic bag. The bag is then to be placed in the freezer for 4-6 hours, and is to be kept frozen until ready to ship!��
The salivary collection has a few more steps considering it is 4 samples rather than one. The timing for the salivary testing is critical, so timers are encouraged. As the patient wakes up, a timer should be set for 30 minutes later. This is when the first salivary sample (the pink tube) is to be collected. Before this test, the patient should not eat, drink, brush or floss. The second collection (green tube) is to be taken right before lunch, around noon. The third (orange tube), is to be collected in the evening before dinner, and the final collection (blue tube) before bed at night.�
For all salivary collections, each tube needs to be 3/4 of the way full. The straws provided are the patient’s choice to be used. As soon as the tube is 3/4 of the way full, snap the saliva lid tightly, put into the bag in which it came, and freeze for 4-6 hours, until ready to ship. Patients are to record the date and times of the saliva collections on the bag and requisition form.�
Salivary Hormone
Considering the salivary hormone testing is done using 4 saliva samples, the instructions are the same as the saliva collection in the test mentioned above. However, to review them again,�the timing for the salivary testing is critical, so timers are highly encouraged.
As the patient wakes up, a timer should be set for 30 minutes later. This is when the first salivary sample (the pink tube) is to be collected. Before this test, the patient is not to eat, drink, brush or floss. For the second collection (green tube), it should be collected right before lunch, around noon. The third (orange tube), is to be obtained in the evening before dinner, and the final sample (blue tube) before bed at night.�
For all salivary collections, each tube needs to be 3/4 of the way full. The straws provided are to be used at the patient’s discretion. As soon as the tube is 3/4 of the way full, snap the saliva lid tightly, put into the bag in which it came, and freeze for 4-6 hours, until ready to ship. Patients are to record the date and times of the saliva collections on the bag and requisition form.�
Salivary Hormone + CAR Breakdown
Aside from the basic components, the styrofoam box includes 6 colored salvia collection tubes, 6 straws, and an absorbent pad. The tests that fall under this category require 6 samples throughout the day. It is important to remember to write down the time the samples were collected as well as the time when the patient first woke up. The first sample (yellow tube) is to be taken as soon as the patient is awake but has not gotten out of bed. In order to accomplish this properly, it is best the patient sets the tube next to their bed the night before. This makes it easy to collect first thing in the morning. It is very important that the patient sets an alarm for 30 minutes after they wake up ( second test, pink tube)and for 1 hour after they wake up (third test, lavender tube). These tests are all to be done prior to eating breakfast, brushing and flossing teeth. The fourth collection (green tube) is to be taken before lunch and the fifth (orange tube) before dinner. The sixth and final sample (blue tube) is to be collected at least one hour after dinner. Just as the other saliva samples mentioned above, these tubes are to be filled 3/4 of the way, tightly closed, placed back in the bag they came in and frozen for 4-6 hours, or until they are ready to ship.
SHIPPING INSTRUCTIONS FOR ALL TESTS:
Shipping should be done Monday-Friday as this will ensure the sample will be delivered to the lab on time. Make sure all paperwork is filled out properly and place contents back in the styrofoam box in the following order:�
sealed plastic bag with frozen specimen tubes
frozen ice pack�
requisition form, symptom sheet, and payment (if applicable)�
Next, place the lid back on the box and place the entire styrofoam box in the cardboard collection kit. Close the cardboard box and place it inside the FedEx shipping envelope provided. The patient will then write their name and address on the Billable Stamp and tear off the customer receipt for their records. Then, place on the FedEx envelope. The final step is to schedule a pick-up. In order to do this, the patient will call the FedEx toll-Free number at 1-800-463-3339 and select “schedule a pickup”. This MUST be a scheduled pick up from an address and NOT a dropbox.�
* It is important to note that patients should avoid eating avocados, eggplant, tomatoes, bananas, melons, pineapples, plums, nuts, nut butter, wine, cheese and chocolate 48 hours before and during the testing period as these could impact the results.
* Patients should keep in mind that strenuous exercise, alcohol, coffee, tea, tobacco or any other product containing nicotine is to be avoided 24 hours before and during the collection period.
Labrix is a great company that allows patients a noninvasive way to have their hormone levels checked. Almost every patient who walks in the door can benefit from this test. I highly recommend this test because hormone levels can change based on age, PMS symptoms, fatigue, blood sugar issues, or stress! These results are accurate and have a decently quick turn around time. Gaining insight and taking control of your body is now easier than ever. – Kenna Vaughn, Senior Health Coach
The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or chronic disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
*All information and photos/video content for this article are directly sourced from labrix. Please see labrix for more information and credit.
The discs that cushion the vertebrae are made up of a tough outer layer and a softer inner layer. When the outer layer is damaged and the inner layer comes out into the spine, it is referred to as�disc herniation.
Often the symptoms of a herniated disc include back pain, as the inner layer of the disc puts pressure on nerves in the spine. A herniated disc can impact the sciatic nerve, leading to sciatica.
If you know that your sciatica was caused by a herniated disc then try these exercises and stretches to help reduce back and leg pain.
Exercises that help relieve sciatica from a herniated disc
If your spine specialist or chiropractor informed you that a herniated disc is what caused the pain also known as lumbar radiculopathy they may recommend� three sciatica exercises:
Prone on elbows into Press-up
Upper back extension
Opposite arm and leg extension
These stretches can help provide relief when the root cause of sciatica from herniated or bulging disc.
Prone Elbows/Press-Up
This exercise is to ease sciatica from herniated disc pain and pressure in the lumbar spine/low back.
How to:
Lay on stomach
Slowly push up until rested on forearms
Beginners hold for 30 seconds
Once strength is gained and you feel comfortable then hold for 3 to 5 minutes
Gently lower to the floor
Repeat 10 times
Once comfortable holding for 5 minutes then perform an extended arms version, which is like push-ups raising your arms to the point where your elbows lock
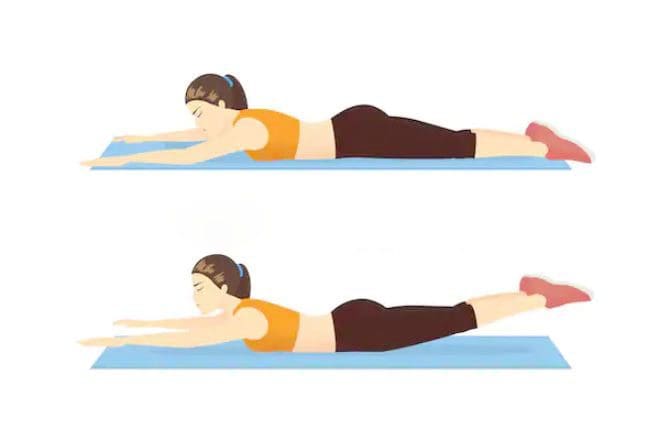
Upper Back Extension
This exercise is to strengthen and stabilize the low back muscles.
How to:
Lay on your stomach with a small pillow or rolled towel under your hips
Rest your arms at your sides
Slowly lift your upper body up off the floor, contracting your low back muscles as you rise
Hold the lifted position for 3 seconds
Slowly lower your body to the ground
Repeat 10 times
Throughout this exercise, keep movements fluid and controlled.
Opposite Arm and Leg Extension
This exercise is to stabilize your spine and strengthen your low back, hamstring and gluteus muscles.
How to:
Lay on your stomach with a small pillow or rolled towel under your abdomen
Extend both arms in front of you
Contract your abdominal muscles as you slowly lift both your right arm and left leg
Hold for 3 seconds. Lower your leg and arm down
Repeat with your left arm and right leg
Hold for 3 seconds
Repeat the exercise 5 to 10 times on each side
As you alternate the lifts, make sure to keep abdominal muscles contracted to get the full benefit.
How do these exercises relieve sciatica from herniated disc
These exercises and stretches are designed to move the pain from the leg and into the low back.
This is centralization/localization.
This is a good thing, as the goal is to get the pain centralized and back at the source.
When the leg pain goes away, it means the pressure on the sciatic nerve and related nerves has been removed.
If sciatic pain stretches down to the foot, you will feel these exercises, meaning that the pain and electrical sensations will move through the ankle and knee. Which means you’re doing it correctly.
This does not mean that the pain is immediately going to centralize to the low back, it does take time because you are trying to stretch and straighten out this long nerve.
But you will notice sciatica pain does not go as far down the leg.
Therefore�these exercises need to be done consistently and be made a part of your routine.
What to know before exercising
Before starting these stretches, consider three recommendations:
Get a doctor�s approval
A spine specialist should clear you to perform these stretches and exercises before you start.
While these exercises are safe, get a doctor�s permission before starting physical activity.
Know the cause so your exercise program helps and not makes the condition worse
Sciatica from herniated disc means a different type of exercise than sciatica caused by piriformis syndrome.
Knowing this information will help you choose an exercise plan that provides maximum relief.
Don�t push too hard
Don’t aggravate sciatica, listen to your body and go slow.
Experience any pain or symptoms:
Weakness
Tingling
Numbness
Contact a spine specialist immediately!
Sciatic nerve pain caused by a herniated or bulging disc is a common problem.
But incorporating these exercises and stretches can provide sustained relief.
The sciatic nerve is a large nerve that travels from the lower back down both of the legs and into the feet. When pressure is placed on the nerve, such as from a herniated disc, it can lead to the symptoms commonly referred to as sciatica.
The sciatic nerve can be impacted by a number of different things, including injury and degenerative diseases.
Difference Foot Orthotics Make to *REDUCE FOOT PAIN* & Correct Posture | El Paso, TX (2019)
Custom made foot orthotics can help control foot motion and posture. Healthcare professionals prescribe custom foot orthotics to help patients focus on their foot posture and mobility control. Research studies have ascertained that using custom foot orthotics for posture and mobility control can help fix excessive foot pronation and supination to prevent a variety of foot health problems. The subsequent video describes how custom foot orthotics will help control foot posture and mobility to improve health and wellness.
NCBI Resources
Sciatica is a common back ailment that affects approximately 1 in 10 adults in the United States. It is most prevalent in people between the ages of 25 and 45. Sciatica is characterized by a shooting pain that originates in the lower back and travels down through the hip, buttock, and back of the leg.
The pain can be so severe that it inhibits mobility and can prevent people from working, taking care of their homes, or just enjoying their life. Traditionally, doctors have treated the condition with medications and some invasive therapies, but chiropractic treatments have been found to be extremely effective in alleviating the pain and curing the condition.
Children are not born with a fully developed microbiome, and a baby’s diet has a large impact on the foundation set for a healthy guts future (Biotics Education Team, 1).� Setting up a child to have healthy gut flora from early stages can help them:
In the TEDDY study published in Nature Medicine, it shows that a child’s microbiome goes through 3 transitional phases:
Developmental phase (3�14 months)
Transitional phase (15�30 months)
Stable phase (31�46 months)(Stewart et al., 3)
Throughout the developmental stage, those with a higher breastfeeding rate were associated with increased levels of Bifidobacterium.� “However, once the infants were weaned, there was a rapid loss of the�Bifidobacterium spp.,�and a quick turnover occurred in the microbiome, which featured a higher population of bacteria within the�Firmicutes�phylaphase (Biotics Education Team, 1)”.� Once infants begin to wean off milk, it is helpful to start providing them with probiotic powders.
Prebiotics are the dietary fiber that the live organisms in the probiotics need to eat in order to flourish.
Some foods that include prebiotics are:
Vegetables
Fruits
Legumes
It is great to start toddlers on prebiotics and probiotics because it can help them to continue to have a healthy gut. A healthy gut can help prevent many issues that adults face later on in life (Veereman-Wauters, 4) Having a healthy gut can help to protect the gut from harmful bacteria and fungi, it can aid in sending signals to the immune system, regulate inflammation, create a supportive barrier in the cell lining of the colon and reduce the risk of cancer (Lewis, 2)�
Probiotics are safe for most children and can reduce the risk of upper respiratory tract infections and well as helping to reduce their risk of allergies. It is beneficial to have toddlers on probiotics and prebiotics so they do not develop a “leaky gut”. By starting children on probiotics and prebiotics young, it can aid their overall health for life.
ProbioMax� for Toddlers
Prebiotic and Probiotic Support for Toddlers*
�Overall, it is best to start building the child’s microbiota through the maternal diet in pregnancy, expose them to environments, and talk with their pediatrician about starting them on probiotics. It’s better to start young and build a healthy foundation than to be diagnosed in their 20’s with leaky gut from something that could have been prevented. – Insight from Kenna Vaughn, Health Coach�
NCBI Resources:
Our knowledge of microbiota is rapidly developing and changing. A relatively young field, the science of gut bacteria has been quickly taken up by industry. Most drugstores sell probiotics in some form or another, and yogurt and other fermented foods are frequently hailed as healthy for the gut because they contain live bacteria. Probiotics are food or supplements that contain living microbes intended to support or improve your microbiome’s health. If your favorite yogurt contains �live and active cultures,� you are getting a dose of probiotics along with your breakfast. These microbes are thought to bolster or replace the bacteria communities in the gut of people.
�Cites:
Biotics Education Team. �Impact of Diet on Baby’s Microbiome.� Biotics Research Blog, blog.bioticsresearch.com/impact-of-diet-on-babys-microbiome.
Lewis, Sarah. �Probiotics and Prebiotics: What’s the Difference?� Healthline, Healthline Media, 3 June 2017, www.healthline.com/nutrition/probiotics-and-prebiotics.
Stewart, Christopher J., et al. �Temporal Development of the Gut Microbiome in Early Childhood from the TEDDY Study.� Nature News, Nature Publishing Group, 24 Oct. 2018, www.nature.com/articles/s41586-018-0617-x.
Veereman-Wauters, Gigi. �Application of Prebiotics in Infant Foods.� The British Journal of Nutrition, U.S. National Library of Medicine, Apr. 2005, www.ncbi.nlm.nih.gov/pubmed/15877896.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine