The human body is a complex system, that requires consistent development in all areas. When it comes to weight loss being too strict can cause the body to rebel. Examples are individuals that have lost weight, then put it right back on, or get stuck in a plateau. The objective is to step off the weight loss rollercoaster and embrace weight-loss strategies that work. Here, we explore a few evidence-based weight loss strategies that focus on long-lasting success.
Improve insulin sensitivity
When consuming carbohydrates, it is broken down into sugar.
The body needs a certain amount of sugar to function. However, it is a narrow safety range. If the level gets too high for too long, cellular damage happens. The role of insulin is to guide the excess sugar/glucose into the cells. However, more individuals are experiencing high blood insulin levels, called hyperinsulinemia. Possible symptoms can include:
Sugar cravings
Unusual weight gain
Frequent hunger
Excessive hunger
Unable to concentrate
Anxiety or feelings of panic
Lack of focus
Extreme fatigue
Insulin rises because the blood sugar does. It�s dangerous to let glucose levels stay elevated, which is why more insulin gets produced to bring the blood sugar down. Given enough time constant hyperinsulinemia can result in a condition called insulin resistance, where the cells become resistant to the effects of insulin and are less effective.
Insulin sensitivity and weight loss
A high level of insulin in the blood can trigger weight gain and make losing it difficult. Results of high insulin:
Stress and stress eating could be contributing to an expanding waistline. Examples could be eating a favorite meal while barely being conscious of the process or the inability to resist a chocolate bar after a long, distressing day. Research published in the Journal of Health Psychology found that stress-related eating has a preference for calorie-dense and highly tasty foods. And when stress levels rise, food cravings rise, triggering fat gain.
Reducing stress
There are a variety of techniques that can help the mind and body relax turning off the stress response. Here are some science-based favorites:
Proper sleep means sound sleep eight hours each night. Many individuals have convinced themselves that five or six hours is enough. Unfortunately, research shows otherwise. In a study published in PLOS Medicine, researchers studied the effects of short sleep duration on hormones that lessen or increase hunger, and on body mass index or BMI. They found the participants with short sleep had reduced leptin and elevated ghrelin which increases appetite and can contribute to weight gain.
Improving sleep quality
Developing a healthy sleep routine
Have the same sleep and waking time
Time to wind down
Meditate a little before sleep
Take a warm bath 90 minutes before bed
Avoid blue light at least 90 minutes before going to sleep
Limit caffeine intake as it can negatively affect sleep even when taken six hours before sleep
Avoid/limit alcohol in the evenings
Regular physical activity can help release stress and tension, tiring the body out so sleep comes naturally
30 to 40-minute endurance sessions a week are plenty. However, for some individuals, exercising too close to bedtime can have the opposite effect. Therefore, take note of whether this would be a problem.
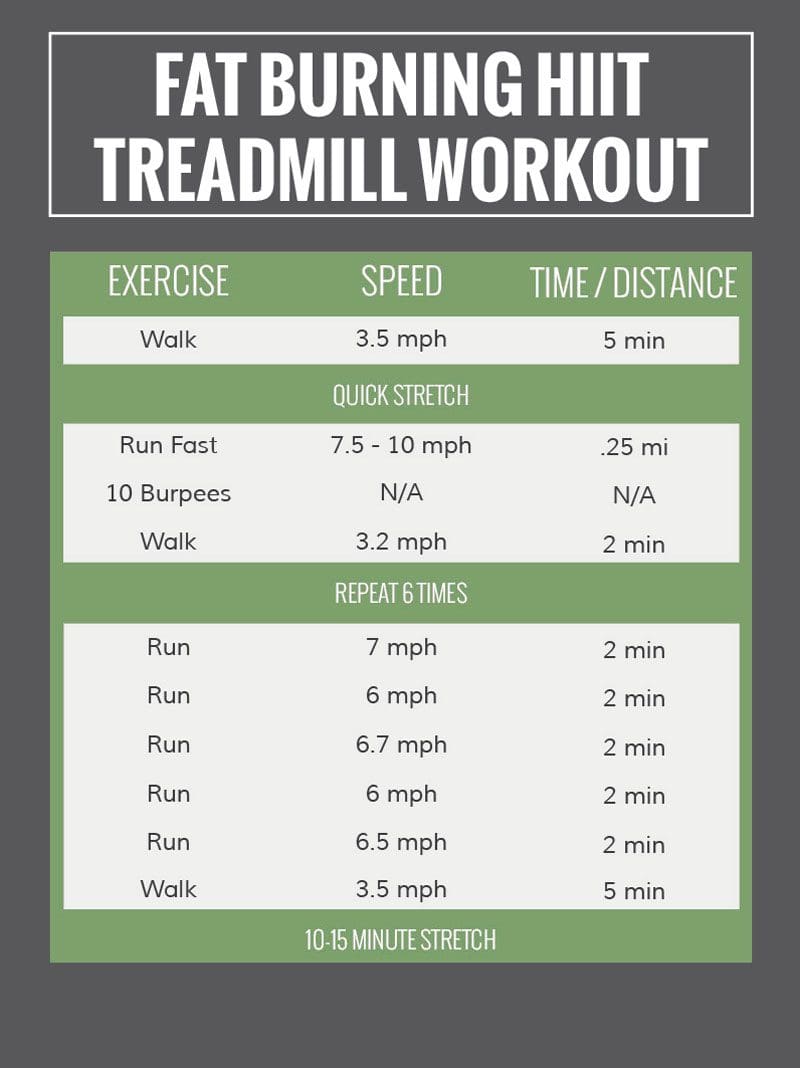
High-Intensity Interval Training
There are a variety of approaches to exercising. But there is one evidence-based approach that has been proven to:
An increased amount of muscle increases the basal metabolic rate or BMR. This increases the body’s ability to burn fat and lose weight. A loss of lean body mass lowers resting energy expenditure and increases fatigue and injury risk. For individuals trying to lose weight the metabolic decline triggered by a loss of lean body mass can cause regaining the fat previously lost. What this means is that when muscle mass drops so does metabolism along with the ability to keep the weight off.
When muscle mass increases the body can easily burn fat, making it possible to achieve and maintain a healthy weight. It�s important to remember that as the body’s muscle mass increases the body needs more energy to nourish and support this new tissue. This means that higher calories are allowed, as not having enough calories becomes counterproductive. Muscle mass increase can be achieved by:
A healthy diet will help build muscle
Strength and resistance training
Taking protein supplements
Weight loss strategies takeaway
With the right approaches, permanent weight loss is possible. Instead of deprivation, focus on science-backed approaches that work:
This will make sticking to the weight loss strategies easier and will contribute to a happy, healthy life.
Body Composition
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
References
Chao, Ariana et al. �Food cravings mediate the relationship between chronic stress and body mass index.��Journal of health psychology�vol. 20,6 (2015): 721-9. doi:10.1177/1359105315573448
Taheri, Shahrad et al. �Short sleep duration is associated with reduced leptin, elevated ghrelin, and increased body mass index.��PLoS medicine�vol. 1,3 (2004): e62. doi:10.1371/journal.pmed.0010062
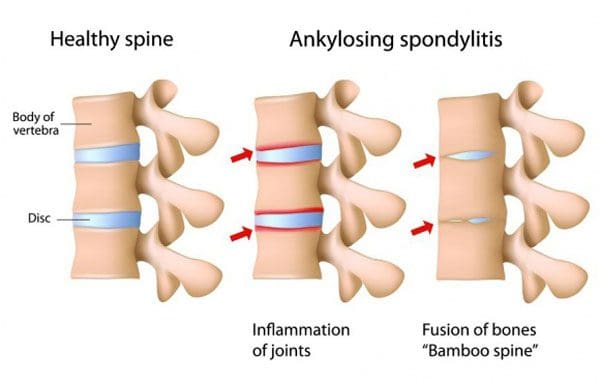
Individuals with ankylosing spondylitis have a new treatment option that was previously used for rheumatoid arthritis. It is a medication that belongs to a class known as JAK inhibitors. Ankylosing spondylitis combines joint pain with reduced mobility. Ankylosing spondylitis is different because in severe cases, the bones in the spine can fuse together, literally reducing mobility.
The disease typically begins with pain and stiffness in the back. This is usually after some time of inactivity. Symptoms start before the age of 45 and develop gradually. There is no cure for ankylosing spondylitis but there are treatments that can improve symptoms and put the condition into remission. Ankylosing spondylitis treatment is the most successful when addressed early before irreversible damage to the joints begins.
Janus Kinase Inhibitors
Janus kinase inhibitors have traditionally been used to treat:
Rheumatoid arthritis
Psoriatic arthritis
Ulcerative colitis
The medication works by decreasing the immune system�s activity. Janus kinase inhibitor drugs affect several cellular compounds that are important in the development and progression of ankylosing spondylitis. Currently, there are only three Janus kinase inhibitor medications available in the United States and FDA-approved to treat rheumatoid arthritis:
Xeljanz
Rinvoq
Olumiant
Each of the approved inhibitors targets specific enzymes
Current Ankylosing Spondylitis Treatments
Janus kinase inhibitors are not given to individuals right away. However, it could be an option if first and second-line treatments are not working. Treatments usually consist of:
First-Line Treatments
NSAIDs
Nonsteroidal anti-inflammatory medications are the most commonly used to treat ankylosing inflammation, pain, and stiffness.
Chiropractic
Chiropractic physical therapy is a major part of ankylosing spondylitis treatment keeping the spine flexible and as healthy as possible. A chiropractic/physical therapy team design and develop specific exercises to fit individual needs, which include:
Stretching and Range-of-motion exercises help maintain flexibility in the joints
Sleeping and walking posture adjustment exercises
Abdominal and spinal exercises to maintain a healthy posture
If nonsteroidal anti-inflammatory medications do not relieve symptoms, then biological medications could be prescribed. This class of medications includes:
Tumor necrosis factor blockers work by targeting cell protein that is part of the immune system, known as tumor necrosis alpha. This protein causes inflammation in the body, and the blockers suppress it.
Interleukin 17 Inhibitors
Interleukin 17 in the body’s immune system defends against infection. It uses an inflammatory response to fight infections. The IL-17 inhibitors suppress the inflammatory response and help reduce symptoms.
Other Treatment Options
Lifestyle Adjustments
Following a medical treatment plan is often combined with diet and lifestyle adjustments that are recommended to help with the condition, these include:
Most individuals with ankylosing spondylitis do not require surgery. However, a doctor could recommend surgery if there is joint damage, the hip-joint needs to be replaced, or if the pain is severe.
Inhibitor Potential
Studies are ongoing in the treatment of ankylosing spondylitis. The drug is currently in Phase 3 trials for the treatment of adults. The trial results have shown patients with active ankylosing spondylitis showed improvement in:
Fatigue
Inflammation
Back pain
The study enrolled adults with active ankylosing spondylitis who took at least two NSAIDs that were ineffective at treating symptoms. Most of the participants were men, average age of 41, and no prior usage of biologic disease-modifying antirheumatic drugs.
Janus kinase could become a standard treatment
There is still not enough research to make a prediction, but the data is promising. The inhibitors seem to be a safe option when used in a properly screened, well-matched setting that includes regular monitoring. The inhibitors appear to be effective and have the advantages of being taken orally and working fast.
Body Composition
Osteoarthritis and weight loss
Being obese has shown to be a high-risk factor for the development of osteoarthritis. This is not only from the effects of extra weight on the body’s joints but also as a result of the inflammatory effects of adipose tissue. The lower back, hips, and knees, bear the majority of the body’s weight.
An excess amount of adipose tissue on the body’s midsection and legs has been shown to negatively impact the weight-bearing joints. Promoting Lean Body Mass and encouraging weight loss lowers the risk of osteoarthritis and improves an individual’s quality of life. Exercise is regarded safe for individuals with osteoarthritis and should be incorporated to improve body composition, reduce Body Fat Mass, improve Lean Body Mass and maintain a healthy weight.
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
References
Hammitzsch A, Lorenz G, Moog P. Impact of Janus Kinase Inhibition on the Treatment of Axial Spondyloarthropathies. Frontiers in Immunology 11:2488, Oct 2020; doi 10.3389/fimmu.2020.591176.�https://www.frontiersin.org/article/10.3389/fimmu.2020.591176, accessed Jan 21, 2021.
van der Heijde D, Baraliakos X, Gensler LS, et al. Efficacy and safety of filgotinib, a selective Janus kinase 1 inhibitor, in patients with active ankylosing spondylitis (TORTUGA): results from a randomized, placebo-controlled, phase 2 trial.�Lancet.�2018 Dec 1;392(10162):2378-2387. doi: 10.1016/S0140-6736(18)32463-2. Epub 2018 Oct 22. PMID: 30360970.�https://pubmed.ncbi.nlm.nih.gov/30360970/�accessed Jan 19, 2021.
High-intensity interval training or bodybuilding? Getting to the gym, choosing a strength-training method, and figuring out which method is right for you can be frustrating and confusing. With all of the options available, there�s just no easy way to figure out which training regimen is right.
Here are two of the most popular training methods broken down. The principles behind each training method and how they influence body composition. The journey to getting healthy goes a lot smoother when knowing which training program will help reach optimal fitness goals.
Not all training programs are the same
Bodybuilding is about physical appearance. This means big muscles and low body fat which is accomplished by heavyweight training workouts. High-Intensity Interval Training/HIIT workouts focus on performing high-intensity exercises in large volume repetitions quickly to raise an individual’s heart rate, cycling between high intensity and rest. This is accomplished by using:
Light weights
Bodyweight
Cardio exercises
It�s important to understand that different training methods will affect body composition differently. Body composition is about painting an accurate picture of what�s going on in the body. The key is to break down:
What each training program looks like
What it does
How to choose the program that�s best for the individual
Gaining Lean Body Mass
Losing Fat Mass
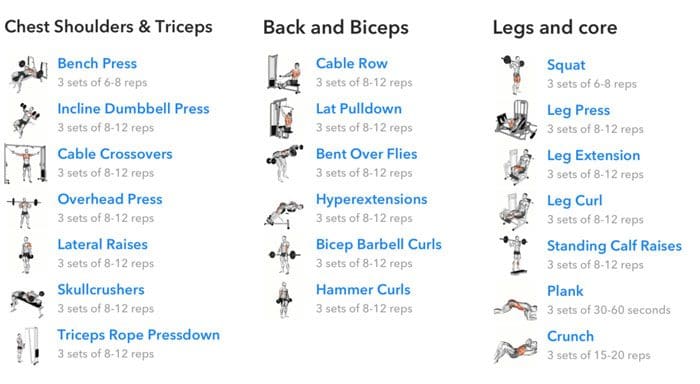
Bodybuilding
Bodybuilding at its core is about gaining muscle while minimizing body fat. Minimizing fat is a key to building a muscular-defined physique, and requires a detailed focus on protein and calorie intake. It is the emphasis on aesthetically increasing muscle size and reducing body fat. Bodybuilders focus on higher reps and lighter-weight workouts. This encourages muscle hypertrophy. Other factors in bodybuilding are:
Adequate cardio
Consistent protein intake
Calorie restrictions
These are important aspects of this type of regimen and building visually impressive musculature.
This impressive musculature is not only for looks, as it can help with fat loss as well. This is because resistance training/weight training can burn a lot of calories and lose a substantial amount of fat. A study by the Department of Exercise Science showed that 10 weeks of resistance training can reduce fat weight by 1.8kg and increase resting metabolic rate by 7%.
Body Composition
For the average person, if the focus is on building visible muscle while keeping a low body fat percentage, bodybuilding is a great choice. Ideal body composition focuses on keeping fat content to a minimum without compromise.
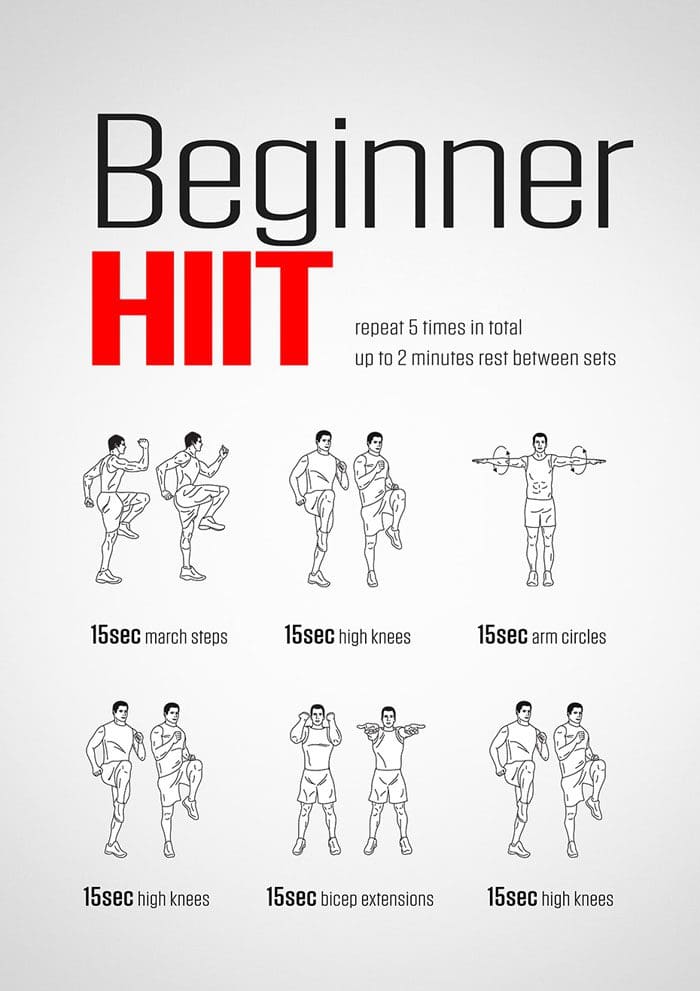
High-Intensity Interval Training/HIIT
Modern training programs like CrossFit utilize HIIT-style workouts. HIIT burns calories through workouts that significantly increase heart rate. The exercises are short, loaded with mini-breaks in between high-intensity sets designed to test cardio. The focus is on high repetitions. However, HIIT workouts are so intense that professional trainers recommend individuals only train 2-3 times a week, to avoid overstressing the body. There are bodybuilding exercises included like:
However, they are done with different goals in mind. The priority of a HIIT workout is to reduce fat, improve cardio, and developing some muscle.
Body Composition
Scientists from Ohio State University observed more than 40 subjects at all levels of cardio fitness. Over the next 10 weeks, the subjects completed a variety of HIIT workouts. The scientists realized that the individuals were developing a more capable cardio system, and their body fat percentages were dropping significantly.
If the goal is to get stronger and lose weight, then bodybuilding is the best option.
If the goal is to have stronger cardio and lose serious weight then HIIT workouts are the best option.
No matter what training program is chosen. Remember that achieving a healthy body composition that the individual feels comfortable with is the most important thing. Making positive changes and achieving optimal health is the objective. Both workout strategies can be incorporated into a regular strength training regimen. Both training methods can be challenging, but the health benefits are absolutely worth it. Contact us today to help figure out which training regimen will achieve optimal health.
InBody
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
References
Ross, Leanna M et al. �High-intensity interval training (HIIT) for patients with chronic diseases.��Journal of sport and health science�vol. 5,2 (2016): 139-144. doi:10.1016/j.jshs.2016.04.005
Westcott, Wayne L. �Resistance training is medicine: effects of strength training on health.��Current sports medicine reports�vol. 11,4 (2012): 209-16. doi:10.1249/JSR.0b013e31825dabb8
When lower back pain presents many want to retreat to the couch, bed and just lay down, but doctors, chiropractors, physical therapists, and spine specialists do not recommend this course of action. What they do recommend, other than treatment, is to engage in the easiest forms of exercise on the spine and back muscles. �
Staying sedentary is one of the worst things an individual can do to their back. When the back is aching exercise can usually help. This is because the muscles, ligaments, tendons are being stretched and not just staying still, which lets inflammation build up and swell. Moving keeps the blood flowing, allowing for broader healing and recovery.
However, back pain relief can be a challenge. Various treatment options exist because there are a variety of causes. The key is figuring out which type is best for each individual and their specific condition. An individual needs to know the cause of their type of back pain, as this determines which exercises should or should not be doing. The Pain and Therapy journal evaluated some of the best exercises for lower back pain. �
Physical Therapy Exercises
The McKenzie method can be very effective for acute disc herniation pain and sciatica. This type of exercise is to figure out if there is a specific position that helps the pain become centralized, correct any motion restrictions, and take the pressure off the region that is compressed or inflamed. Physical therapists incorporate McKenzie exercises as part of regular treatment. The strength-building moves are designed to help support the spine and consist of range-of-movement work and sustained positions. �
�
Home and Studio Workouts
Pilates is one of the easiest exercises for individuals with chronic low-back pain. Like McKenzie exercises, it utilizes sustained positions that strengthen the trunk/core muscles. The muscles are strengthened using small movements. Using the machine called a reformer, has built-in support for the spine. This is considered a low-key, muscle-toning workout that can ease chronic back pain. �
�
Water Exercise
Water exercises lessen the body’s weight, taking pressure/stress off the spine. Deep-water running with the water at shoulder-height can significantly improve low-back pain. In a study, a group of overweight/obese women worked out twice a week for an hour-long exercise session. After 12 weeks, improvements in pain intensity, personal care, sitting, standing, and sleeping were reported. �
�
Easiest Office Exercise
One of the easiest exercises is walking. It is great for the body. But the key is to walk more than usual around the office, or wherever work is. This is not about getting the heart rate up. It is about not staying in the same position for too long. When sitting and focused, an individual can stay in an uncomfortable position for some time and just push through it in an attempt to finish up the work.
Using a timer or an application that alerts every hour to get up and stretch is highly beneficial. Walk correctly to the bathroom, or just get up and walk around for a bit gets the blood pumping through the body and the muscles in motion stretching and contracting. �
�
Stabilization Exercise
Strengthening workouts can be done at home.
Stretch while standing against the wall bringing the arms up and down.
Pull the elbows down into the back, which stops the hyperactive trapezius from tensing up.
Knee to the chest motion while lying on the back
Abdominal crunches while balance on an exercise ball
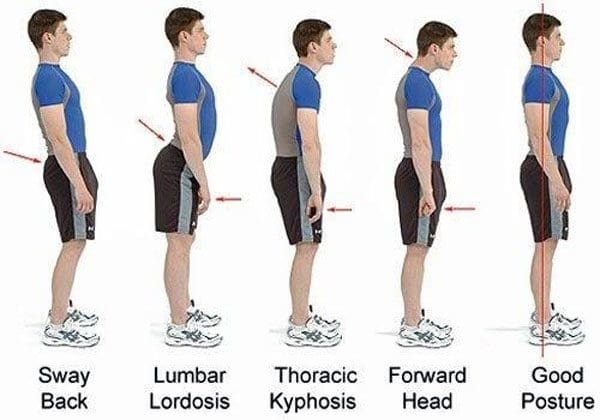
Push the head back into the headrest while driving. This helps avoid the forward head posture.
Contact a doctor, chiropractor, or physical therapist that can recommend the best stabilization exercises for the specific pain/condition. �
�
Tai Chi and Qigong
Tai Chi and Qigong are gentle exercises where an individual performs slow, controlled movements emphasizing balance and focus. Both can reduce pain, disability, and other symptoms associated with lower back pain. �
�
Body Composition Testimonial
�
Exercise After Childbirth
Physical activity for pregnant and post-birth, the American Congress of Obstetricians and Gynecologists recommends the following. The easiest exercise routines can be resumed gradually after pregnancy, once a doctor confirms it is medically safe, depending on the delivery, and the presence or absence of medical complications.
Regular aerobic exercise in lactating women has been shown to improve cardiovascular fitness without affecting milk production, composition, or infant growth.
Nursing women should consider feeding their infants before exercising in order to avoid exercise discomfort.
Nursing women also should ensure proper hydration before engaging in physical activity.
Take it slow.
�
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
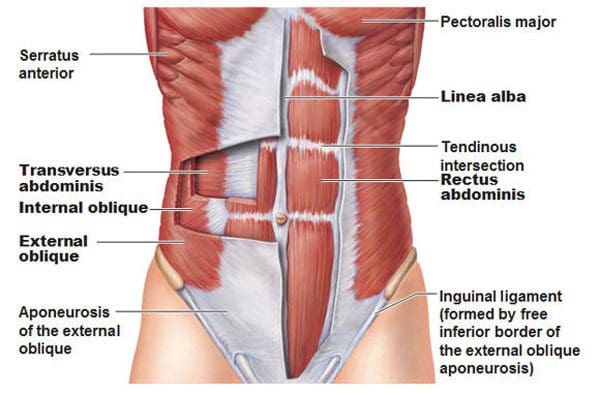
The core and the muscles involved are a group of muscles that wrap around the body’s torso. The front, back, and sides. Strengthening these muscles will improve and ultimately alleviate lower back pain. One of the main muscles that are overlooked is the transverse abdominis muscle. It is vital to a healthy core, especially if back pain is presenting. It’s known as the seatbelt muscle as it is deep in the abdomen and wraps around the waist. It has everything to do with long-term core strength and function. A properly developed transverse abdominus functions like a lumbar support belt that protects the spine. When the transverse abdominus is strong the muscle contracts to generate the correct amount of support and stability when in motion. �
�
For example, individuals that do not have low back pain engage the transverse abdominus around 30 milliseconds before moving the shoulder, while individuals that have low back pain have a delayed contraction of the transverse abdominus muscles that makes them take on awkward postures, and move in an awkward fashion contributing to back pain and continuing to weaken the core muscles. Individuals that regularly do transverse abdominus strengthening exercises greatly reduce the risk of experiencing low back pain for the first time and reduce the recurrence of those already with back pain. �
Core Muscle Anatomy
The first step to strengthening is understanding the moves and how to do them correctly with basic anatomy. Think of the core as a muscle box where the:
The body flexes and extends whenever bending forward and standing up
The body does a lateral side bend when bending the trunk to one side
The body rotates the trunk when twisting the torso
�
Muscle Weakness
The transverse abdominus tends to suffer from neglect which is one reason why it becomes weakened. This increases the risk of developing back pain. Another reason is that individuals have a weak muscle is they exercise in one-plane of movement. Not working out the core muscles in all planes of motion can contribute to back pain. For example, if an individual performs pelvic tilts, they are only moving in one plane when tilting the hips forward and back, known as flexion and extension. To achieve optimal/functional strength, the core workout needs to include side bending and twisting movements. �
Strengthening The Transverse Abdominus
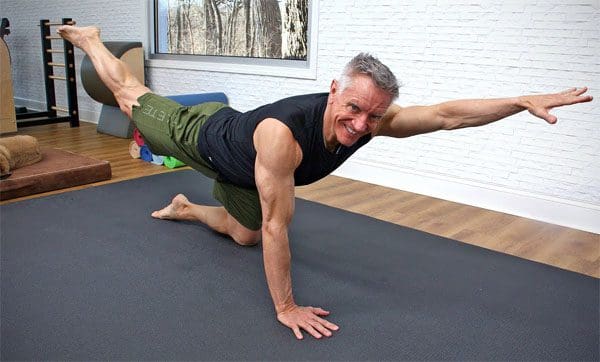
Pigeon Pose
Many individuals sit for extended amounts of time and are excessively tight along the sides and hips. The first step should be to increase the hip’s mobility before strengthening the core. If the hip muscle’s fibers become shortened, it can affect hip joint function and efficiency during core movement. The Pigeon Pose is a hip opener. How to do it:
Get on the floor with the knees and palms on the ground.
Slide the left leg back so the hip is extended, then externally rotate the right hip/turn the right leg out from the hip. Focus on positioning the right shin perpendicular to the body.
Extend the trunk so the body is upright, lifting the chest, arching the back, and looking toward the ceiling, while resting the fingertips on the floor a little forward of the hips.
Hold the pose for 30 seconds and switch sides.
This stretches the hip flexor muscles in the extended leg and the rotator and outer hip muscles in the flexed leg.
�
Pay Attention To The Engaged Muscles
Individuals can train the transverse muscles to activate faster and more effectively throughout the day by slowing down and paying attention to moving with more intent. Place the hands around the waist and engage the core to feel the muscles contracting. This will help get a feel for the movement. Once comfortable remember to engage these abdominal musclesbefore and while reaching, twisting, or lifting items. �
Pelvic Tilt
This exercise is vital for building the smaller muscles that support a healthy core. How to do it:
Lie on back with knees bent and feet on the floor.
Engage the transverse muscles and gently tilt the pelvis upward.
Return the pelvis to a neutral position.
Repeat.
Start with 3 sets of 10-12 reps.
When this is no longer challenging and can be completed without increasing back pain, advance to more challenging exercises like the bird dog, planks, or plank variations.
�
Standing Exercises
Translating core strength into functional strength and pain-free movement progresses to standing exercises that require rotation. One example is a standing lunge with rotation. How to do it:
Get into a lunge stance with the front leg flexed 90 degrees at the hip, knee, and ankle. The rear leg should be extended at the hip with the knee touching or almost touching the floor.
Twist from the waist. When comfortable doing this movement, hold weight like a dumbbell, medicine ball, or gallon jug of water in both hands, and gradually increase the weight as the muscles get stronger.
When in the process of strengthening the core, consistency is the key. Commit to a short workout every day instead of one massive workout once or twice a week. Ten minutes a day is enough to build strength, improve function, and decrease back pain. �
Improved Body Composition
Functional fitness and the ability to move about comfortably not only benefit physical wellness but also improves body composition. The aging process reduces the metabolic rate, which leads to increased body fat. Lean Body Mass gets lost from age and inactivity. Lean Body Mass contributes to the overall Basal Metabolic Rate, also known as the body’s metabolism. It is the number of calories the body needs to support essential functions. Engaging in strength training or resistance exercises will help regain the muscle loss from aging/inactivity, and can lead to an increase in lean body mass.
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
References
People who regularly engaged in TVA-strengthening exercises were less likely to experience a recurrence of low back pain:�Australian Journal of Physiotherapy�(2002), �Specific spinal exercise substantially reduces the risk of low back pain recurrence��https://www.sciencedirect.com/science/article/pii/S000495141460283X?via%3Dihub
Participating in any sports or physical activities strengthens the mind and body. But working out and engaging in these types of activities too much or without rest periods wears down the body. There is the feeling of a good workout with some sore muscles and achiness that lets you know the activity is working positively.
However, soreness can quickly lead to pain and further injury if ignored. The lower back is a common area of soreness after working out playing sports, and where muscle spasms, pulls, and pinches occur. Being able to distinguish between workout soreness and pain is critical for maintaining a healthy spine.
A constant-sore back or feelings of sharp pains is not normal. If there is a feeling of low back pain during or after a physical routine, stop and take a moment to examine the tingling, discomfort, or pain being experienced. If unsure if the soreness or pain is a cause for concern call or video conference with a chiropractor to discuss what is going on.
Physical activity and pain
Individuals participating in physical/sports activities have an increased risk of low back pain because of the consistent running, twisting, and jumping. Any of these movements place pressure on the spine along with the surrounding ligaments and muscles, which can lead to injury.
Repetitive twisting and turning, stresses the muscles around the spine, which can cause frequent muscle sprains. Running and jumping also wears down the vertebrae and discs. Impact activities can also cause injuries to the spine, nerve roots, and surrounding tissues. The most common back problems include:
Muscle sprains
Osteoarthritis
Bulging discs
Herniated discs
Sciatica
Fractures are less common but still pose a risk
Individuals should watch for achiness or stiffness that lasts longer than a few days and does not alleviate with ice or anti-inflammatory over the counter medication, or sharp pain that happens with specific movement/s, along with any pain, numbness, tingling that runs down the leg/s or to other areas should consult a medical professional.
Treatment and prevention
Maintaining the body’s health is critical. If the lower back begins to present discomfort or hurts, do not ignore it. Many will play through the pain when they should be taking a break. And ignoring any back pain could create new injuries or worsen the condition. Continued pressure on the back will worsen any strains or fractures and will hinder the body from healing properly.
Individuals tend to take on awkward/uncomfortable postures and move in awkward ways to avoid or compensate for the pain. This places added pressure in the wrong places and can cause/worsen an injury or condition. Pay attention to the pain. Try ice and heat therapy at home to see if it eases up. Using a foam roller or self-massage device can help if the back pain is muscular. However, if the pain is sharp, shooting, or does not go away, visit a chiropractor for diagnosis and treatment.
A chiropractor will conduct imaging tests and physical exams to identify the root cause. Once a diagnosis has been reached a treatment plan will be implemented through:
Massage
Stretches
Therapeutic exercises
Spinal adjustments
Health coaching
Visiting a chiropractic professional will improve the condition and strengthen the spine.
Fit Body Composition
Muscle recovery
When engaging in physical activity there is microscopic damage to the muscle cells. The stress and fatigue the body goes through during physical activity cause hormone and enzyme levels to fluctuate, increasing inflammation. This leads to:
Fat loss
Increased metabolism
Increased strength
Muscle growth
However, it happens through proper recovery. There are different types of recovery: immediate, short-term, and training.
Immediate recovery is the short time between movements. For example, when jogging, immediate recovery is the time between each stride.
Short-term is the time between sets of exercises. For example, the rest periods between exercise intervals.
Training recovery is the period between one workout session ending and the next beginning.
Research has shown that rest time is not a one size fits all. Everyone is different and therefore should consult a fitness trainer, or sports chiropractor and experiment with what feels right. For some individuals, 24 hours works. For others, it can be 48 or 72 hours to feel fully recovered. It depends on age, fitness level, physical activity intensity, diet, sleep, and more.
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
References
Smith, Jo Armour et al. �Risk Factors Associated With Low Back Pain in Golfers: A Systematic Review and Meta-analysis.��Sports health�vol. 10,6 (2018): 538-546. doi:10.1177/1941738118795425
Sedentary lifestyle prevention through chiropractic is highly recommended for seniors. With advanced age, the body’s muscles, bones, and spinal system begin to wear down and need to be maintained to retain their mobility and flexibility. Regular chiropractic adjustments are recommended as part of an active/fitness lifestyle for seniors and can help older individuals maintain optimal health.
Sedentary Lifestyle Prevention
Many seniors tend to reduce physical activity after reaching retirement age. Many individuals just want to kick back and relax. However, living too laid-back can impact overall health. A lack of exercise and physical activity can cause the muscles, cardiovascular system, and skeletal system to prematurely wear out. Living an active lifestyle will keep individuals at their best when retiring and maintain a healthy quality of life.
Pain Management
Chiropractic can help individuals realize their full potential. The chiropractic approach to achieving top health means treating the source of symptoms, and not just the symptoms. This helps maintain a high quality of life. Chiropractic sedentary prevention includes:
Adjustments
Adjustments to the body are the core of chiropractic. Adjustments are utilized to realign the spine that helps treat various nervous system-related conditions. These include subluxations, slipped discs, sciatica, nerve damage, and more. Adjustments also increase the immune system’s functionality. This is extremely beneficial for older individuals.
Nutritional Recommendations
Older individuals can benefit from a customized nutrition plan to help with any deficits in their diets. Often older individuals need more calcium to help fortify bone health. Chiropractors and health coaches can provide individuals with nutritional information needed to live a healthy life.
Exercise Program
An active lifestyle is an essential component of staying healthy. Chiropractors can provide individuals with specialized exercises that take into account their specific and specialized needs.
Physical Therapy
Physical therapy is another component of chiropractic, as it helps enhance the adjustments.
Health Coaching
Health coaching can provide individuals with the tools necessary to take charge of their health. Counseling involves exercise recommendations, nutritional advice, healthy habits development, and more depending on the individual’s abilities.
Stay Moving
A sedentary lifestyle places an older individual’s spine in a compromised position. Older individuals have an increased risk of developing detrimental spinal conditions. Overexertion happens more easily in weakened bodies. The solution is to maintain physical activity with proper support. Chiropractic is designed to improve the whole-body. If you�re looking for sedentary prevention and the latest care approaches, contact us, we’re ready to help!
Chiropractic Shoulder Pain Treatment
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
References
Hawk, Cheryl et al. �Best Practices for Chiropractic Care for Older Adults: A Systematic Review and Consensus Update.��Journal of manipulative and physiological therapeutics�vol. 40,4 (2017): 217-229. doi:10.1016/j.jmpt.2017.02.001
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine