Most people stretch and hardly pay any attention to it. Throughout the day a person may stretch upon waking or after they�ve been sitting in the same position for a while. They might do some stretches before working out or as part of physical therapy. Stretching often makes us feel better but it might be surprising to discover that it is actually beneficial to optimal body function.
As a person ages their muscles begin to tighten. This is a natural part of the aging process. However, it can cause inhibit range of motion and joint stiffness, making normal day to day activities more difficult. After certain injuries stiffness can set in, causing pain and decreased flexibility.
What many chiropractic patients may be surprised to learn is that stretching is a great complement to chiropractic care. When combined with simple stretches and low impact exercises, chiropractic patients often find that their injuries heal faster, their pain is reduced, and they simply feel better and more energetic. If that isn�t enough to convince you to incorporate stretching into your daily wellness routine, maybe these four compelling benefits will.
STRETCHING
Helps Keep The Spine Aligned
When you stretch the muscles in your chest, shoulders, and lower back it will improve your posture by helping to keep your spine in better alignment. When your muscles are not stretched properly they begin to draw up � and it usually isn�t in a uniform or symmetrical manner.
This means that muscles on one side of your spine may draw up more than the muscles on the other side. This can result in your body being pulled to that side, causing your spine to be pulled that way. Stretching prevents this from happening and when combined with consistent chiropractic care it can ensure good spinal health.
Improves Flexibility & Range Of Motion
Most people know, on some level, that stretching improves flexibility and range of motion. However, many do not act on that knowledge and they often wind up at the doctor�s office complaining of back pain. Stretching will make you more flexible which, in turn, will make you less prone to injury.
Your muscles will be able to work as effectively as possible. It is important that you don�t overdo it though. Some people take terrible risks when they stretch, thinking that if they force their bodies into certain positions or if they �bounce� to get a deeper stretch then they will be more flexible. Actually, the reverse is true. Stretching in an unsafe way such as bouncing or forcing your body far beyond its limits will result in injury including pulled muscles and muscle tearing.
Helps Relieve Stress & Detoxify The Body
When you stretch, two very significant things happen. First, your blood flow increases as blood is rushed to the muscles, your organs, and your brain. Secondly, it moves oxygen through these areas. As a result, toxins that have accumulated in your soft tissues are dispelled.
The simple stretching that relieves tension in muscles, combined with the detoxifying effect will help you feel less stressed. Stretching is a great stress management exercise, one you can do just about anywhere. You don�t need any special equipment and you can even do it right at your desk while you are working. A bonus is that you�ll feel the de-stressing effects instantly.
It relies on the body�s natural ability to heal itself by releasing the tension and easing the stiffness of the muscles in that area. The stiffer those muscles are, the more they will hurt when you try to move. By relaxing them through stretching you will find that you move much easier and with less pain.
Stretching has so many great benefits. Talk to your chiropractor about a customized stretching plan that you can do at home. You�ll love what it does for you. If you don�t have a chiropractor, give us a call at (915)850-0900. We�re here to help!
Truide Torres, office manager, developed facet syndrome from participating in gymnastics at a young age. Due to the additional stress being placed on her spine, Mrs. Torres was forced to reduce her engagement in exercise and physical activities. In order to continue being involved in fitness, Truide Torres found facet syndrome pain treatment with Dr. Alex Jimenez, D.C. in El Paso, TX. Mrs. Torres was well-informed and properly treated by Dr. Jimenez for her face syndrome and she was able to participate in her exercise and physical activities once again. Truide Torres recommends Dr. Alex Jimenez and his staff as the non-surgical choice for facet syndrome pain treatment, describing them as a caring, knowledgeable and qualified group of healthcare professionals.
Facet syndrome (also popularly known as facet joint disease, facet osteoarthritis, facet hypertrophy or aspect arthritis) is a syndrome where the facet joints (synovial diarthroses, from C2 to S1) degenerate to the purpose of causing debilitating symptoms. In conjunction with degenerative disk disease, a distinct but related illness, aspect syndrome is thought to be one of the most frequent causes of lower back pain. The signs of facet joint syndrome rely almost entirely about the location of this degenerated joint, the severity of the harm and the amount of pressure that is being put on the surrounding nerve roots. It is essential to note that the amount of pain a person experiences does not correlate well with the amount of degeneration that has occurred within the joint. A lot of men and women experience little or no pain while others, with the specific same amount of damage, experience chronic pain.
Please Recommend Us: If you have enjoyed this video and/or we have helped you in any way please feel free to recommend us. Thank You.
Migraine symptoms are painful and debilitating, often affecting the quality of life of many migraine sufferers around the globe. Although headache pain is one of the most prevalent reasons for doctor office visits each year, migraines are considered to be one of the most underdiagnosed and undertreated diseases in the medical field. Furthermore, the emotional distress caused by the unresolved physical symptoms of migraines can create a number of mental health issues which can lead to worsened symptoms.�As a result, migraine education efforts have been implemented as a part of many headache treatment options, including chiropractic care. The purpose of the following article is to demonstrate the benefits of a primary care migraine education program, known as the Mercy Migraine Management Program or MMMP, on headache impact and quality of life.
A Primary Care Migraine Education Program has Benefit on Headache Impact and Quality of Life: Results from the Mercy Migraine Management Program
Abstract
Objective: The objective of this study was to evaluate the effectiveness of the Mercy Migraine Management Program (MMMP), an educational program for physicians and patients. The primary outcome was change in headache days from baseline at 3, 6, and 12 months. Secondary outcomes were changes in migraine-related disability and quality of life, worry about headaches, self-efficacy for managing migraines, ER visits for headache, and satisfaction with headache care.
Background: Despite progress in the understanding of the pathophysiology of migraine and development of effective therapeutic agents, many practitioners and patients continue to lack the knowledge and skills to effectively manage migraine. Educational efforts have been helpful in improving the quality of care and quality of life for migraine sufferers. However, little work has been done to evaluate these changes over a longer period of time. Also, there is a paucity of published research evaluating the influence of education about migraine management on cognitive and emotional factors (e.g., self-efficacy for managing headaches, worry about headaches).
Methods: In this open-label, prospective study, 284 individuals with migraine (92% female, mean age = 41.6) participated in the MMMP, an educational and skills based program. Of the 284 who participated in the program, 228 (80%) provided data about their headache frequency, headache-related disability (as measured by the Headache Impact Test-6 (HIT-6), migraine-specific quality of life (MSQ), worry about headaches, self-efficacy for managing headaches, ER visits for headaches, and satisfaction with care at four time points over 12 months (baseline, 3 months, 6 months, 12 months).
Results: Overall, 46% (106) of subjects reported a 50% or greater reduction in headache frequency. Over 12 months, patients reported fewer headaches and improvement on the HIT-6 and MSQ (all p < .001). The improvement in headache impact and quality of life was greater among those who had more worry about their headaches at baseline. There were also significant improvements in �worry about headaches�, �self-efficacy for managing headaches�, and �satisfaction with headache care�.
Conclusion: The findings demonstrate that patients participating in the MMMP reported improvements in their headache frequency as well as the cognitive and emotional aspects of headache management. This program was especially helpful among those with high amounts of worry about their headaches at the beginning of the program. The findings from this study are impetus for further research that will more clearly, through evaluate the effects of education and skill development not only on headache but also emotional and cognitive influences.
Dr. Alex Jimenez’s Insight
Migraine headache pain is characterized as a disabling symptom which can tremendously impact an individual’s quality of life. Plus, the stress created by the worry of an imminent migraine can result in a variety of mental health issues. Many healthcare professionals and migraine sufferers lack the proper knowledge and skills on how to effectively manage migraine symptoms. Fortunately, migraine education programs, like the Mercy Migraine Management Program (MMMP), were designed to teach patients how to improve their quality of care and quality of life. Migraine education programs such as these have been demonstrated to especially benefit migraineurs with higher levels of stress. Aside from providing spinal adjustments and manual manipulations to correct the alignment of the spine, chiropractic care focuses on the treatment of the body as a whole, making sure patients are educated regarding their migraine symptoms.
Introduction
Migraine headache is a highly prevalent, painful, disabling and costly disease. The evaluation, treatment and management of migraine have been estimated to involve 5 to 9 million office visits per year to primary care physicians in the United States.[1,2] Migraine is one of the most common reason for an outpatient office visit.[3] Numerous studies have reported that patients with migraines have significantly higher pharmacy and medical claims than those without migraine.[4�7] Migraine also has high indirect costs; it has been estimated to cost US employers between 17 and 20 billion dollars annually in lost work productivity.[8,9]
Despite its prevalence and high cost, migraine remains an underdiagnosed and undertreated disease.[10�14] Given the availability of migraine-specific therapeutic agents, it is vital that physicians be able to accurately diagnose migraine. Moreover, it is important for physicians to recognize the benefits of treating migraine as a specific condition as opposed to simply �head pain�. Unfortunately recent findings concerning the accurate diagnosis and treatment of migraine suggest that most patients with migraine are not accurately diagnosed or treated.[10�12,14]
Migraine is currently conceptualized as a chronic neurologic disease characterized by intermittent episodes of acute pain.[15�17] Current guidelines for managing chronic diseases emphasize the importance of self-management.[18�22] In self-management, the emphasis is on both the patient and the provider actively treating the disease, with the patient managing the disease outside the clinical setting. Self-management (or self-care) requires that the provider afford the patient the opportunity to take the right dose of the right medication at the right time, is educated about migraine and its management, and is equipped with tools to minimize the frequency and deleterious effects of migraine attacks.
Most migraine sufferers experience some disability from headache pain and the associated symptoms of migraine.[23�26] It is often the disability emanating from migraine attacks that compromises quality of life, thus making migraine both a pain problem and a life problem. For many patients, recurrent disability combined with a lack of effective coping tools and medications that are not always effective can create uneasiness, worry and anxiety between attacks as well as when an impending attack seems imminent. This worry and anxiety may be related to low self-efficacy, a cognitive variable that involves an individual�s belief that she or he is able to successfully manage a situation.[27�29] Self-efficacy has been theorized as a potent influence of how well one manages migraines.[29�33] Recent development of new therapeutic agents and the advent of improved educational efforts have been helpful in validating migraine and improving the quality of care for migraine sufferers. However, demonstrating the overall value of a primary care based educational program for migraine is difficult. Previously published articles evaluating the benefits of migraine education have reported successful results.[34�39] However, these programs mainly involved referral of patients into a specialized clinic or educational facility for instruction from specialist practitioners or educators and followed outcomes of the patients after enrollment. Unfortunately, few communities have access to such headache specialty clinics. Accordingly, most patients rely on their primary care clinicians for educational content and counseling regarding headache care. With these concepts in mind, the Mercy Migraine Management Program (MMMP), a multi-center, targeted enrollment study was undertaken to demonstrate the overall value of a migraine educational program through a provider-group setting. Given the paucity of programs whereby the physicians and participants are provided a one-time educational program, the decision was made to evaluate whether a program of this nature was feasible and suggestive of efficacy. If so, then this would allow for further investigation using a more elegant design.
The current study was an open trial looking at the effects of the MMMP. The effect of participation in the educational program on headache frequency, headache-related quality of life, headache-related worry, self-efficacy, treatment satisfaction, and emergency room visits for headache was assessed.
Methods
Participants
The research was conducted within a 120-clinician primary care group practice caring for more than 200,000 patients (St. Johns Mercy Medical Group in St. Louis, Missouri). A total of 31 physicians and three nurse practitioners from 14 of the group�s practice sites agreed to participate. From these sites, a total of 284 patients with migraine were identified and recruited by the clinicians and agreed to participate. Among participants 92% (n = 260) were female and the mean age was 42 (SD = 12.45). In order to be eligible, patients were required to have one or more of the following: (a) ICD-9-CM code for migraine/headache diagnosis in the previous six months; (b) one or more claims for acute migraine/headache medications in the previous six months; or (c) patients with one or more ER or urgent care center visits in the previous six months coded for migraine/headache or headache NOS and at least one migraine medication. In addition, patients who presented to the primary care office for evaluation of headache were eligible for enrollment in the program if they were given an ICD-9-CM code for migraine/headache diagnosis at that time.
Procedures
Provider Education and Training
Clinicians who expressed interest in participating attended a two-hour continuing medical education program on migraine. The program covered four key concepts: (1) impact recognition diagnosis of headache (office recognition of migraine based on headache repercussions and disability rather than the characteristics of pain alone), (2) the benefits of early abortive intervention, especially with migraine-specific medications, (3) effective preventive regimens, and (4) non-pharmacologic management. The overarching goal of the program was to educate providers about how to equip the patient with tools they can use to manage their migraines on a daily basis. Participating clinicians and their staff were provided printed educational materials. A majority of the materials were developed or selected for use by the first author. These were supplemented by standardized educational materials which included: (a) Patient Centered Strategies for Effective Management of Migraine[40]; (b) The Migraineur�s Guide to Migraine[41]; and (c) Provider and Patient Tipsheets from the Migraine Matrix� education program[41], a comprehensive migraine management program for providers.
Following their participation in the educational session, physicians from the practice sites sent IRB approved notices to potentially eligible patients, identified from claims data, informing them of the study or spoke with them directly during routine office visits for headache treatment. Interested individuals who responded to the mailed invitations then came to the practice site where their migraine diagnoses were confirmed and informed consent for participation was provided, as approved by the local IRB. The subjects subsequently completed study related questionnaires. Subjects recruited at the time of an office encounter were invited to participate at the time of said visit, provided informed consent in like-manner to those described above, and completed the baseline questonnaire.
After the questionnaires were completed, the clinician provided medication or other treatment recommendations based on their knowledge attained from the educational seminar and print materials previously provided to them. No mandatory interventions were required on the part of the provider. They were to make medication and other management decisions as they saw fit for each individual participant according to their own knowledge, understanding, and preferences. They were however required to provide the educational information from the study to the individual subjects enrolled in the trial. The clinician or a member of the health care team provided the patient with the educational materials and instructed them on how to use them. The patients were encouraged to use the materials as best fit their individual situation. The materials were designed to give the patient tools to self-manage their migraines in conjunction with ongoing care from their health care team. These materials included: (a) The Migraineur�s Guide to Migraine[41]; (b) a headache diary; (c) Patient Tipsheets from the Migraine Matrix� education program[42]; (d) educational materials on diet recommendations from the National Headache Foundation; (e) written and visual instruction on how to do cervical range of motion and stretching exercises from the physical therapy department that is associated with the St John�s Mercy Medical Group; (f) biofeedback tapes developed by the Primary Care Network; and (g) Managing Your Migraine Headaches.
The patients took the materials home with instructions to be as consistent as possible with adherence to the concepts proscribed by the educational packet. After 3-months, assessments were mailed to the participants with a self-addressed stamped envelope to return. The same assessments were mailed at 6-months and 12-months post-baseline as well.
Measures
The measures below were self-administered at baseline, 3-months, 6-months, and 12-months post-baseline.
Headache Days. Individuals reported the number of days they experienced headaches over the previous 90 days. This was a primary outcome of interest.
Disability/Quality of Life
Headache Impact Test-6 (HIT-6). The HIT-6 is a six-item measure that is a reliable and valid measure assessing the impact of headache on patients� lives.[43�44] Scores for the HIT-6 are derived by summing the responses to all the items. Higher scores reflect higher levels of headache impact (i.e., poorer quality of life). This was a primary outcome of interest.
Migraine Specific Quality of life (MSQ). The MSQ is a 14-item measure designed to assess the effects of migraine on an individual�s quality of life.[45�46] There are three MSQ subscales, Emotional (MSQ-E), restrictive (MSQ-R), and preventive (MSQ-P). The MSQ has been shown to be an internally consistent, valid measure. The MSQ was not done at 3 months. This was a primary outcome of interest.
Worry about headaches. Individuals indicated the extent to which they worried about headaches disrupting their life using a 4-point scale with options of �rarely�, �sometimes�, �often�, and �almost always�. For purposes of the current study, dichotomous groups were created. Individuals who answered �rarely� or �sometimes� were labeled Low Worry. Those who answered �often� or �almost always� were labeled High Worry.
Self-efficacy for controlling headaches. Individuals indicated the extent to which they were confident in their ability to do things to help control their headaches using a 4-point scale with options of �not confident�, �a little confident�, �fairly confident�, and �very confident�. Individuals who answered �not confident� or �a little confident� were labeled Low Self-Efficacy. Those who answered �fairly confident� or �very confident� were labeled High Self-Efficacy.
Satisfaction with headache care. Individuals indicated (Yes/No) whether they were satisfied with the headache care they were receiving.
ER visits. Individuals indicated the number of times they had been to the ER for headaches during the previous 3 months. For purposes of the current study a dichotomous yes/no variable was created in order to create a percentage of individuals who had visited the ER during the previous 90 days.
Statistical Analyses
All analyses were conducted using SPSS v. 15.[47] Prior to analysis, data were checked for the fit between scale distribution and the assumptions of normality. Headache frequency violated normality assumptions and was transformed (although the transformed variables were used in the model, the original data is used in the figures for ease of understanding for the reader).
A linear random mixed model (treating subjects as random effects) was used to model the change in headache frequency at the four time points over 12 months (baseline, 3 months, 6 months, 12 months). The same was done for the HIT-6 (measured at baseline, 3-months, 6-months and 12-months) and the MSQ subscales (measured at baseline, 6-months and 12-months). In order to determine whether baseline worry and confidence influenced changes in headache and quality of life, these variables were included in the models. Although the potential existed to investigate 3-way interactions (time � worry � confidence), doing so created cells with extremely low n and thus 2-way interactions were the higher order interactions analyzed. For all comparisons, Bonferroni adjustments were made.
In order to evaluate whether there were significant changes over time for worry, efficacy, patient�s satisfaction with their headache care, or ER visits, McNemar�s test was conducted. To account for multiple comparisons, the significance level for each set of comparisons was adjusted to p<.008.
The protocol and procedures for this study were approved by the local Institutional Review Board.
Results
Headache Frequency Change Over Time
Results indicated that overall, at 3 months, 34% (n = 77/228) reported at least a 50% reduction in headache frequency from baseline. This increased to 38% (N=86) at 6 months and 46% (N=106) at 12 months.
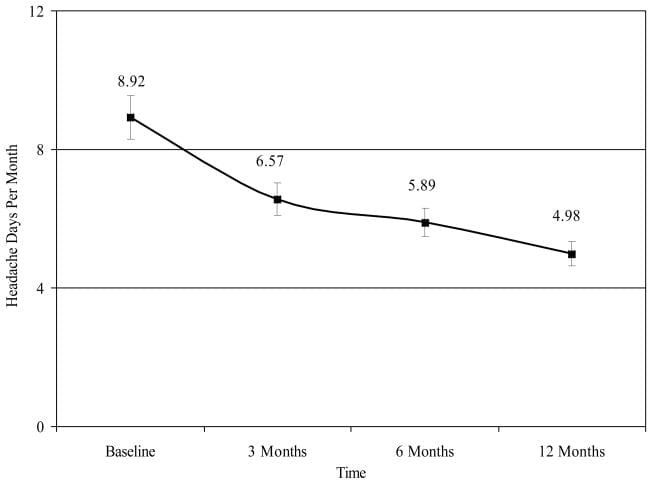
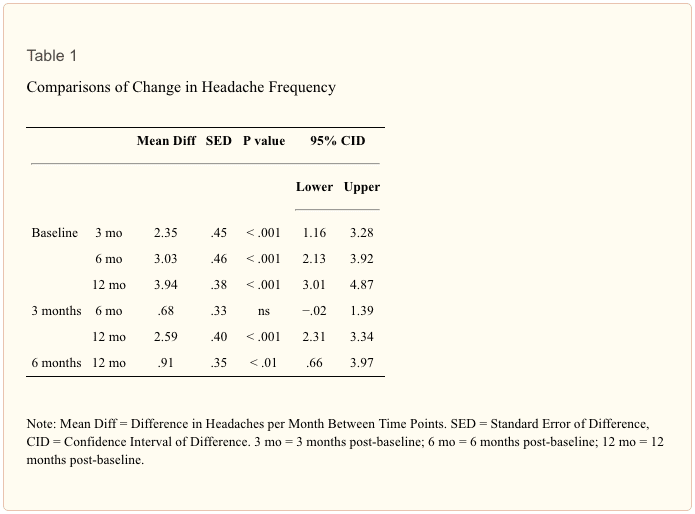
Results indicated that the main effect for reduction in headache frequency was significant (F [3, 691] = 27.89, p < .001). Figure 1 shows headache frequency per month at each time point. Table 1 shows that there was a significant reduction in headache frequency from baseline to each subsequent time point (p < .001). Also, headache frequency at month 12 was significantly lower than at month 3 and 6 (p<.001). The main effect for worry was also significant (F [1, 308] = 12.03, p < .001). Those who were labeled as having High Worry had significantly more headaches (M = 8.00, SE = .63) across the time frames than did those who were labeled as having Low Worry (M = 5.89, SE = .46) (95% CID = .62�3.68). The main effect for confidence, the time X worry interaction, and the time X confidence were all non-significant.
Figure 1: Headache days per month at baseline, 3 months, 6 months, and 12 months.
Quality of Life Disability
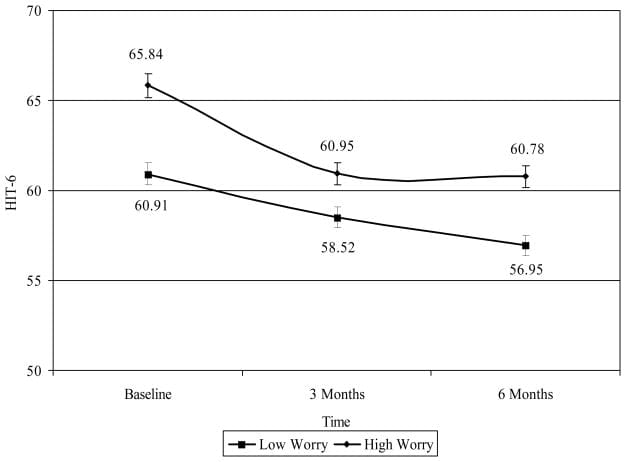
HIT-6. Results indicate that the time X worry interaction was significant (F [2, 464] = 4.54, p < .01). Figure 2 shows HIT-6 scores for each time point by level of worry. Simple effects analysis showed that the degree of reduction in headache impact was greater at 3 months among those with High Worry than among those with Low Worry. Also, those with Low Worry showed a significant reduction in headache impact comparing baseline to 3 months and 6 months, and from 3 months to 6 months, whereas those with High Worry had a significant reduction in headache impact from baseline to 3 months but not from 3 months 6 months. The main effect for confidence was significant (F [1, 292] = 4.54, p < .001) such that those with High Self-Efficacy (M = 59.60, SE = .52) had less headache impact than those with Low Self-Efficacy (M = 61.72, SD = .70) (CID = .79�3.45). Neither the time X self-efficacy or worry X self-efficacy interaction was not significant.
Figure 2: HIT-6 at each time point by worry.
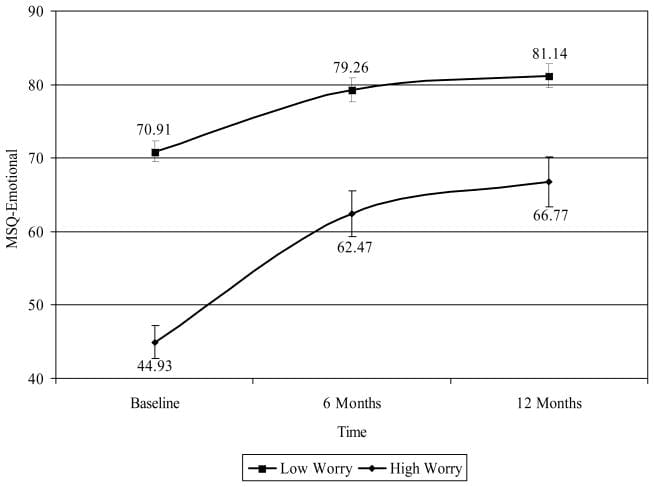
MSQ-E. Results indicate that the time X worry interaction was significant (F [2, 468] = 5.18, p < .01). Figure 3 shows MSQ-E scores for each time point by level of worry. Simple effects analysis showed that the degree of improvement in MSQ-E was greater at 3 months among those with High Worry than among those with Low Worry. The main effect for confidence was significant (F [1, 292] = 4.54, p < .001) such that those with High Self-Efficacy (M = 59.60, SD = 1.74) had better quality of life than those with Low Self-Efficacy (M = 61.72, SD = 1.87) (CID = .79�3.45). The main effect for self-efficacy, the time X self-efficacy interaction, and the worry X self-efficacy interaction were not significant.
Figure 3: MSQ-E at each time point by worry.
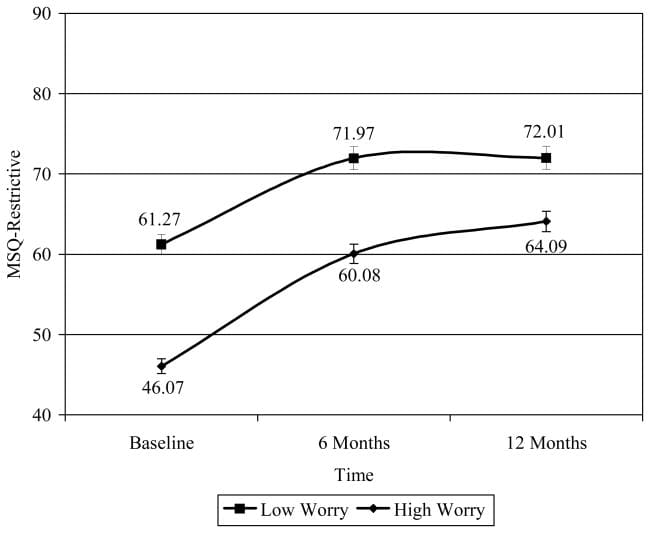
MSQ-R. Results indicate that the main effect for time was significant (F [2, 472] = 47.60, p < .001). Figure 4 shows MSQ-R for each time point by level of worry. Relative to baseline (M = 53.67, SD = 1.23), MSQ-R was significantly improved at 6 months (M = 66.02, SD = 1.35) (CID = 8.96�13.75) and at 12 months (M = 68.05, SD = 1.38) (CID = 10.34�18.42). No difference was found comparing 6 month and 12 month MSQ-R scores. The main effect for worry was significant (F [1, 281] = 34.86, p < .001) such that those with High Worry had significantly lower quality of life (M = 56.75, SD = 1.17) than those with Low Worry (M = 68.41, SD = 1.60) (CID = 7.78�15.57). The main effect for self-efficacy was significant (F [1, 281] = 7.89, p < .01) such that those with Low Self-Efficacy had significantly lower quality of life (M = 59.81, SD = 1.35) than those with Low Worry (M = 65.36, SD = 1.45) (CID = 1.67�9.44). Neither the main effect for self-efficacy or the time X confidence interaction was significant.
Figure 4: MSQ-R at each time point by worry.
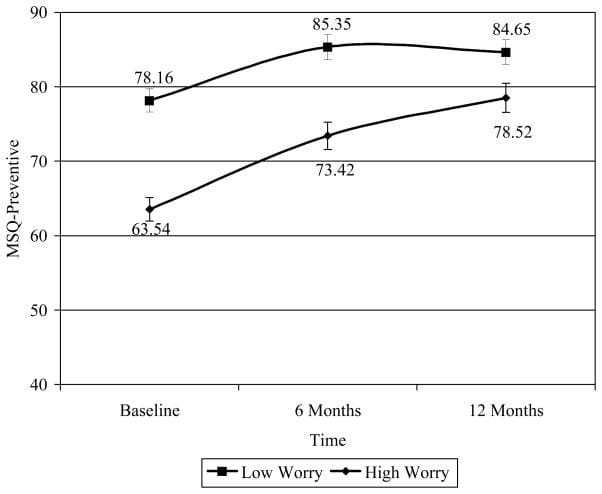
MSQ-P. Results indicate that the time X worry interaction was significant (F [2, 449] = 4.01, p < .05). Figure 5 shows MSQ-P scores for each time point by level of worry. Simple effects analysis showed that those with High Worry showed significant improvement comparing baseline to 6 months and 12 months, and from 6 month to 12 months, while those with Low Worry showed significant improvement comparing baseline to 6 months and 12 months, but no significant improvement from 6 months to 12 months. The main effect for confidence was significant (F [1, 272] = 4.11, p < .05) such that those with Low Self-Efficacy (M = 75.08, SD = 1.48) had lower quality of life than those with High Self-Efficacy (M = 79.47, SD = 1.58) (CID = .13�8.65). The time X self-efficacy interaction and the worry X self-efficacy interaction were not significant.
Figure 5: MSQ-P at each time point.
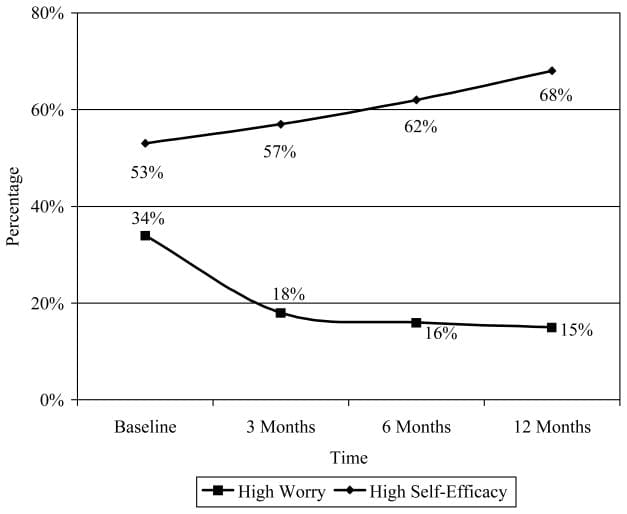
Worry about headaches. Figure 6 shows the percentage of individuals with High Worry at baseline, 3 months, 6 months, and 12 months. Results indicated that when compared to baseline, the percentage of individuals with High Worry was significantly less at 3 months (?2 [223] = 20.42, p < .001), 6 months (?2 [223] = 29.98, p < .001), and 12 months (?2 [223] = 29.82, p < .001). No other significant differences were found.
Figure 6: Percentage of individuals with high worry and high self-efficacy at each time point.
Self-Efficacy for managing headaches. Figure 6 shows the percentage of individuals with High Self-Efficacy at baseline, 3 months, 6 months, and 12 months. Results indicated that the percentage of individuals with High Self-Efficacy at 12 months was significantly more than at baseline (?2 [223] = 10.92, p < .001) and 3 months (?2 [223] = 8.02, p < .001). No other significant differences were found.
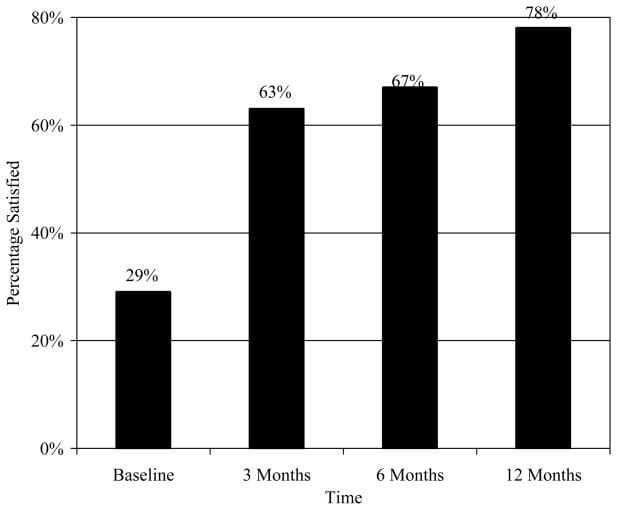
Satisfaction. Figure 7 shows the percentage of individuals who were satisfied with their headache care. Results indicated that when compared to baseline, the percentage of individuals who were satisfied with their headache care was significantly higher at 3 months (?2 [223] = 66.39, p < .001), 6 months (?2 [223] = 75.87, p < .001), and 12 months (?2 [223] = 100.99, p < .001). Also, the percentage of individuals who were satisfied with their headache care at 12 months was significantly higher than at 3 months (?2 [223] = 16.25, p < .001) and 6 months (?2 [223] = 9.80, p < .001). No other significant differences were found.
Figure 7: Satisfaction with headache care.
ER visits. Results indicated that at baseline, 8.33% (n=19) has gone to the ER for headache in the previous 3 months. Although there was a decrease in ER visits at 3 months (3.08%; n= 7), 6 months (3.95%; n = 9), and 12 months (5.26%; n = 12), these reductions were not significant.
Discussion
The primary outcome was the impact that the MMMP would have on headache frequency. Almost half (46%) of all participants reported a 50% or greater reduction in headache frequency at 12 months. It is notable that the percentage of participants experiencing a >50% reduction in headache frequency increased steadily over the 12 months, showing a lasting effect of the educational intervention. The degree of change was not significantly greater in either High Worry or Low Worry groups. However, the reduction in HIT-6 scores was significantly greater for those with High Worry compared to those with Low Worry at 3 months after baseline. In a related finding, participants with Low Self-Efficacy at baseline reported significantly greater reduction in headache impact than those with High Self-Efficacy. It is likely that this was due to participants gaining greater confidence in their own ability to manage their headaches through the education and headache management skills provided in the MMMP. This hypothesis is supported by the increasing percentage of participants with High Self-Efficacy scores and declining percentage of subjects with High Worry over the 12 month study period.
Participants reported that headache-related disability decreased and quality of life improved during the course of the study. This is an encouraging finding given that most patients seek treatment for headaches due to the disability and burden of disease. It is notable that this improvement was achieved through a low-cost, easy to administer educational program. The results also showed that patients worried less about their headaches. It has been well established among chronic pain patients that anxiety and worry about impending pain can significantly increase pain and inhibit efficacy of analgesic therapies.[48�49] To date, however, little research has looked at these phenomena among those with migraine. What research has been conducted has found that worry and anxiety appear to be a significant issue in migraine.[50�54]
It is interesting to note the interactions of worry with disability and quality of life. The focus of the current intervention was solely on education. Not enough research has been published to fully establish the importance of education in changing disease outcomes, particularly as it relates to headache pain. Perhaps the education and basic headache management skills provided in the education program equipped patients with enough knowledge and basic skills that worry and anxiety about headaches were reduced. This idea is supported by the finding that those with high worry at the beginning of the study reported the greatest amount of improvement on ratings of disability and quality of life.
The finding that satisfaction was higher serves as an encouragement that an intervention that is low cost and easy to administer can have a positive impact on patients� perception of care. There are a number of possibilities as to why this may have occurred. It could be that as a result of their education the health care providers were able to better answer patients� questions about migraine and its management. It is possible that the educational materials distributed to the patients resulted in their becoming more knowledgeable about migraine and, in turn, more satisfied with their care. It is also possible that the greater satisfaction came from having fewer headaches and headaches that were less disabling. The current study was not designed to answer these mechanistic questions, thus it is difficult to determine the influence of each of these variables on patient satisfaction. In regards to ER visits; although there was a decrease in ER visits at each time point, the percentage of individuals who had gone to the ER at baseline (8.33%) was low enough that there was little chance to see significant decline.
The results of this study imply that increased knowledge about migraine and management skills can lessen the burden of disease. This is congruent with research in other chronic disease areas (e.g., diabetes, asthma, cardiovascular disease) where providing patients with education about their disease state has been demonstrated to reduce disease burden and reduce worry and anxiety.
Although the current study is encouraging in its findings and raises the specter of future research into the disease management benefits of migraine education, there are limitations to the current study. Likely the greatest limitation to the study was the lack of a parallel condition. Not including such a condition did not allow us to evaluate the possibility that the results emanated from a positive bias or even a �self-fulfilling� outcome whereby decreases in headache were a function of participants� expectations. However, in the current study, the issue of positive bias may have been lessened by the fact the participants had no regular direct interaction with the researchers, and what interaction occurred did so at 3 or more month intervals. At the same time, with a lack of a control condition, this possibility cannot be discounted. This study was undertaken in an effort to see whether an approach that involved a one-time contact would have any impact on headache and associated outcomes. As a result, the conclusions that can be drawn from the current study are limited.
There was no formal oversight of prophylactic prescription patterns, so it is possible that the improvements seen in the participants was due to the 15% increase in the number of individuals prescribed migraine prophylaxis. However, a regression analysis was conducted to evaluate the possibility that starting migraine prophylaxis predicted improvement on the various outcomes (headache frequency, disability, quality of life, worry, satisfaction with care) at each time point. Starting migraine prophylaxis predicted a decrease in headache frequency at 3 months, but had no significant influence on any other domains at any time point. Another limitation was the lack of a parallel comparison group that did not receive the educational intervention. It is possible that the reported improvements in all these domains is a result of positive response bias. Another area of concern is that the scales and questionnaires were based on patient recall rather than diaries, allowing for recall bias. It is also possible that the physicians who participated in the educational seminar tend to have a more interactive communication approach with their patients which can have a positive influence on patient management.[50]
In summary, the purpose of the current study was to evaluate the efficacy of the MMMP which provided education about migraine and its management to health care providers and persons with migraine. In this open-label trial that utilized a linear random mixed model to evaluate change over a 12-month period, patients who participated reported fewer headaches, less disability, and improved quality of life. Also, a significant proportion of the patients reported having less worry, increased self-efficacy, and greater satisfaction with their migraine treatment. It is also worthwhile to note that the increased satisfaction, decreased worry and improved quality of life scores demonstrated in this program were achieved through a low-cost, easy to administer educational program.
Acknowledgments
The authors would like to thank Ms. Mitzi Corzine and Ms. Sally Kane at St. John�s Mercy Health Research (for managing the project), the health care providers and practices in the St. John�s Mercy Medical Group who participated, and Dr. Timothy Houle (statistical assistance). This project was funded by small unrestricted grants provided by the Primary Care Network, GlaxoSmithKline Pharmaceuticals, and Abbott Laboratories. The manuscript was prepared while the second author was funded by the National Institutes of Health (NINDS #K23NS048288).
In conclusion,�despite the fact that headache is one of the most prevalent reasons for doctor office visits each year, migraine still continues to be one of the most underdiagnosed and undertreated diseases in the medical field, impacting the overall health as wellness of migraine sufferers around the world. According to the findings of the article above, patients who participated in the Mercy Migraine Management Program, or MMMP, reported improvements in their migraine symptoms. Furthermore, migraineurs demonstrated additional improvements in a variety of other headache treatment options. Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Back Pain
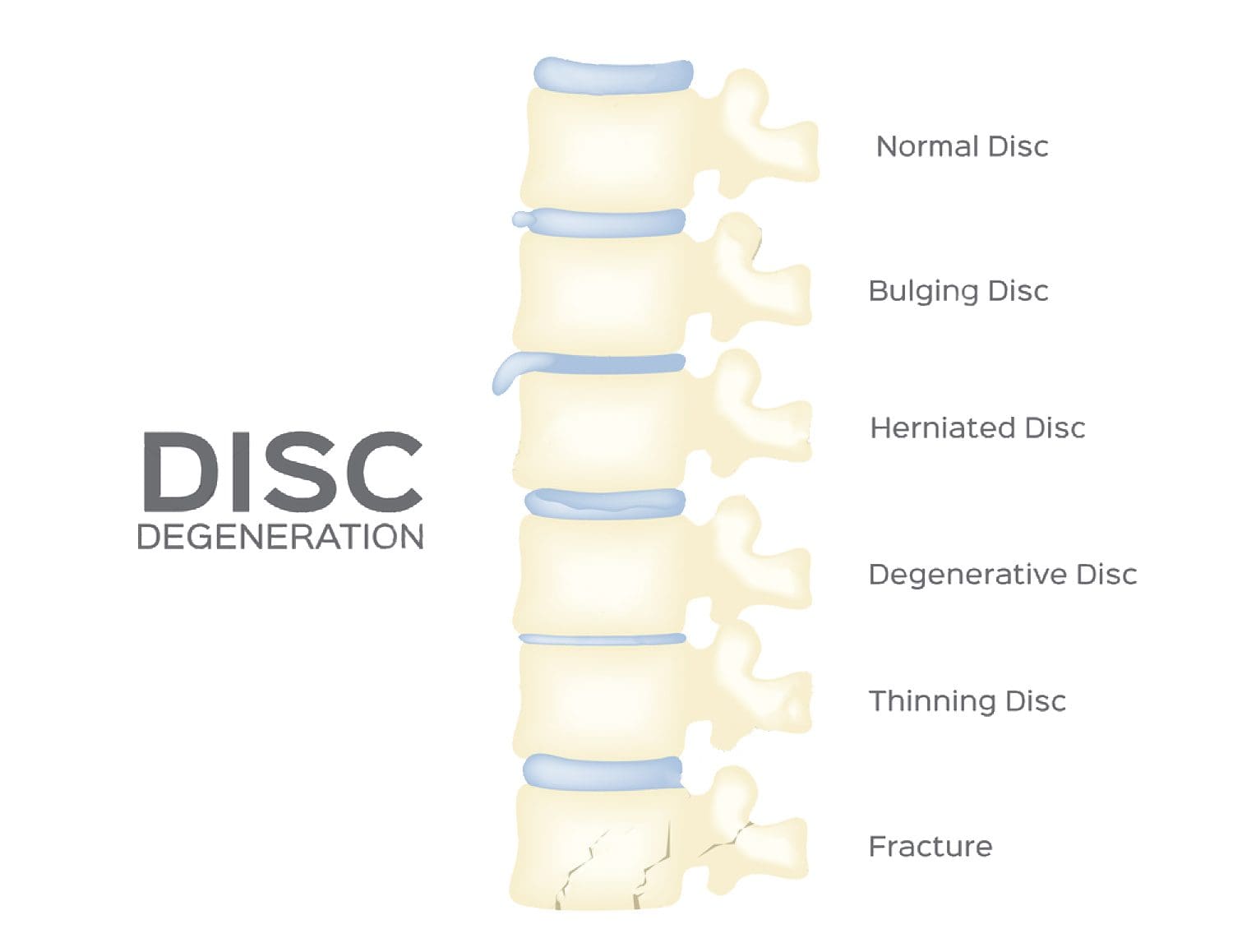
According to statistics, approximately 80% of people will experience symptoms of back pain at least once throughout their lifetimes. Back pain is a common complaint which can result due to a variety of injuries and/or conditions. Often times, the natural degeneration of the spine with age can cause back pain. Herniated discs occur when the soft, gel-like center of an intervertebral disc pushes through a tear in its surrounding, outer ring of cartilage, compressing and irritating the nerve roots. Disc herniations most commonly occur along the lower back, or lumbar spine, but they may also occur along the cervical spine, or neck. The impingement of the nerves found in the low back due to injury and/or an aggravated condition can lead to symptoms of sciatica.
1.�Gibbs TS, Fleischer AB, Jr, Feldman SR, Sam MC, O�Donovan CA. Health care utilization in patients with migraine: Demographics and patterns of care in the ambulatory setting.�Headache.�2003;43:330�335.[PubMed]
2.�Smith R. Management of chronic headache.�Can Fam Physician.�1989;35:1835�9.�[PMC free article][PubMed]
3.�Young WB, Silberstein SD.�Migraine and Other Headaches.�New York, NY: Demos Medical; 2004.
4.�Clouse JC, Osterhaus JT. Healthcare resource use and costs associated with migraine in a managed healthcare setting.�Ann Pharmacother.�1994;28:659�664.�[PubMed]
5.�Elston Lafata J, Moon C, Leotta C, Kolodner K, Poisson L, Lipton RB. The medical care utilization and costs associated with migraine headache.�J Gen Intern Med.�2004;19:1005�1012.�[PMC free article][PubMed]
6.�Pesa J, Lage MJ. The medical costs of migraine and comorbid anxiety and depression.�Headache.�2004;44:562�570.�[PubMed]
7.�Edmeads J, Mackell JA. The economic impact of migraine: An analysis of direct and indirect costs.�Headache.�2002;42:501�509.�[PubMed]
8.�Hu XH, Markson LE, Lipton RB, Stewart WF, Berger ML. Burden of migraine in the United States: disability and economic costs.�Arch Intern Med.�1999;159:813�818.�[PubMed]
9.�Stewart WF, Ricci JA, Chee E, Morganstein D, Lipton R. Lost productive time and cost due to common pain conditions in the US workforce.�JAMA.�2003;290:2443�2454.�[PubMed]
10.�Lipton RB, Stewart WF, Diamond S, Diamond ML, Reed M. Prevalence and burden of migraine in the United States: Data from the American Migraine Study II.�Headache.�2001;41:646�657.�[PubMed]
11.�Lipton RB, Stewart WF, Simon D. Medical consultation for migraine: Results from the American Migraine Study.�Headache.�1998;38:87�96.�[PubMed]
12.�Lipton RB, Diamond S, Reed M, Diamond ML, Stewart WF. Migraine diagnosis and treatment: Results from the American Migraine Study II.�Headache.�2001;41:638�645.�[PubMed]
13.�Patel NV, Bigal ME, Kolodner KB, Leotta C, Lafata JE, Lipton RB. Prevalence and impact of migraine and probable migraine in a health plan.�Neurology.�2004;63:1432�1438.�[PubMed]
14.�Diamond S, Bigal ME, Silberstein S, Loder E, Reed M, Lipton RB. Patterns of diagnosis and acute and preventive treatment for migraine in the United States: Results from the American Migraine Prevalence and Prevention Study.�Headache.�2007;47:355�363.�[PubMed]
15.�Hazard E, Munakata J, Bigal ME, Rupnow MFT, Lipton RB. The burden of migraine in the United States: Current and emerging perspectives on disease management and economic analysis.�Value Health�[PubMed]
16.�Lipton RB, Pan J. Is migraine a progressive brain disease?�JAMA.�2004;291:493�494.�[PubMed]
17.�Scher AI, Stewart WF, Ricci JA, Lipton RB. Factors associated with the onset and remission of chronic daily headache in a population-based study.�Pain.�2003;106:81�89.�[PubMed]
18.�Bodenheimer T, Lorig K, Holman H, Grumbach K. Patient self-management of chronic disease in primary care.�JAMA.�2002;288:2469�2475.�[PubMed]
19.�Chodosh J, Morton SC, Mojica W. Meta-analysis: Chronic disease self-management programs for older adults.�Ann Intern Med.�2005;143:427�438.�[PubMed]
20.�Lorig KR, Holmon H. Self-management education: history, definition, outcomes, and mechanisms.�Ann Behav Med.�2003 Aug;26(1):1�7.�[PubMed]
21.�Lorig KR, Mazonson PD, Holman HR. Evidence suggesting that health education for self-management in patients with chronic arthritis has sustained health benefits while reducing health care costs.�Arthritis Rheum.�1993;36:439�446.�[PubMed]
22.�Lorig KR, Sobel DS, Stewart AL, Brown BW, Jr, Bandura A, et al. Evidence suggesting that a chronic disease self-management program can improve health status while reducing hospitalization: A randomized trial.�Med Care.�1999;37:5�14.�[PubMed]
23.�Ferrari MD. The economic burden of migraine to society.�Pharmacoeconomics.�1998;13:667�676.[PubMed]
24.�Ford S, Calhoun A, Kahn K, Mann J, Finkel A. Predictors of disability in migraineurs referred to a tertiary clinic: Neck pain, headache characteristics, and coping behaviors.�Headache.�2008;48:523�528.[PubMed]
25.�Jelinski SE, Becker WJ, Christie SN, Giammarco R, Mackie GF, Gawel MJ, Eloff AG, Magnusson JE. Demographics and clinical features of patients referred to headache specialists.�Can J Neurol Sci.�2006;33:228�234.�[PubMed]
26.�Stewart WF, Lipton RB, Simon D. Work-related disability: results from the American Migraine study.�Cephalalgia.�1996;16:231�238.�[PubMed]
27.�Bandura A, O�Leary A, Taylor C, Gauthier J, Gossard D. Perceived self-efficacy and pain control: Opioid and nonopioid mechanisms.�J Personal Social Psychol.�1987;53:563�571.�[PubMed]
28.�Bandura A.�Self-efficacy: The Exercise of Control.�New York: W.H. Freeman and Company; 1997.
30.�Lake AI. Behavioral and nonpharmacologic treatments of headache.�Med Clin North Am.�2001;85:1055�1075.�[PubMed]
31.�Maizels M. Why should physicians care about behavioral research?�Headache.�2005;45:411�413.[PubMed]
32.�Nicholson RA, Hursey KG, Nash J. Moderators and mediators of behavioral treatment for headache.�Headache.�2005;45:513�519.�[PubMed]
33.�Penzien D, Rains J, Lipchik G, Nicholson R, Lake A, Hursey K. Future directions in behavioral headache research: Applications for an evolving health care environment.�Headache.�2005;45:526�534.[PubMed]
34.�Blumenfeld A, Tischio M. Center of excellence for headache care: Group model at Kaiser Permanente.�Headache.�2003;43:431�440.�[PubMed]
35.�Cady R, Farmer K, Beach ME, Tarrasch T. Nurse-based education: An office-based comparative model for education of migraine patients.�Headache.�2008;48:564�569.�[PubMed]
36.�Kwong WJ, Landy SH, Braverman-Panza J, Rosen JH, Hutchinson S, Burch SP. A migraine disease management program in the primary care setting: impact on patient quality of life and productivity loss.�J Clin Outcomes Manage.�2007 Jun;14(6):332�338.
37.�Maizels M, Saenz V, Wirjo J. Impact of a group-based model of disease management for headache.�Headache.�2003;43:621�627.�[PubMed]
38.�Rothrock JF, Parada VA, Sims C, Key K, Walters NS, Zweifler RM. The impact of intensive patient education on clinical outcome in a clinic-based migraine population.�Headache.�2006;46:726�731.[PubMed]
39.�Harpole L, Samsa G, Jurgelski A, et al. Headache management program improves outcome for chronic headache.�Headache.�2003;43:715�724.�[PubMed]
40.�Primary Care Network.�Patient Centered Strategies for Effective Management of Migraine.�2000.
41.�Primary Care Network.�The Migraineur�s Guide to Migraine.�1998.
42.�GlaxoSmithKline.�Migraine Matrix�.�2001.
43.�Kosinski M, Bayliss MS, Bjorner JB, et al. A six-item short-form survey for measuring headache impact: The HIT-6.�Qual Life Res.�2003;12:963�974.�[PubMed]
44.�Nachit-Ouinekh F, Dartigues JF, Henry P, et al. Use of the headache impact test (HIT-6) in general practice: Relationship with quality of life and severity.�Eur J Neurol.�2005;12:189�193.�[PubMed]
45.�Jhingran P, Osterhaus JT, Miller DW, et al. Development and validation of the Migraine-Specific Quality of Life Questionnaire.�Headache.�1998;38:295�302.�[PubMed]
46.�Jhingran P, Davis SM, LaVange LM, et al.�Migraine-Specific Quality of Life Questionnaire: Further investigation of the factor structure.�[PubMed]
47.�Statistical Packages for the Social Sciences (SPSS) [computer program]. Version 14.0.�Chicago: SPSS Inc; 2006.
48.�Asmundson GJG, Norton PJ, Norton GR. Beyond pain: The role of fear and avoidance in chronicity.�Clin Psych Rev.�1999;19:97�119.�[PubMed]
49.�McCracken LM, Gross RT. Does anxiety affect coping with chronic pain?�Clin J Pain.�1993;9:253�259.[PubMed]
50.�Bishop KL, Holm JA, Borowiak DM, Wilson BA. Perceptions of pain in women with headache: a laboratory investigation of the influence of pain-related anxiety and fear.�Headache.�2001;41:494�9.[PubMed]
51.�Lanteri-Minet M, Radat F, Chautard MH, Lucas C. Anxiety and depression associated with migraine: Influence on migraine subjects� disability and quality of life, and acute migraine management.�Pain.�2005;118:319�26.�[PubMed]
52.�Radat F, Mekies C, Geraud G, Valade D, Vives E, Lucas C. Anxiety, stress, and coping behaviours in primary care migraine patients: results of the SMILE study.�Cephalagia.�2008;28:1115�25.�[PubMed]
53.�Smith T, Nicholson R. Are changes in cognitive and emotional factors important in improving headache impact and quality of life?�Headache.�2006;46:878.
54.�White KD, Farrell AD. Anxiety and psychosocial stress as predictors of headache and abdominal pain in urban early adolescents.�J Ped Psych.�2006;31:582�96.�[PubMed]
55.�Hahn SR, Cady RK, Nelson MR. Improving healthcare professional-patient communication to promote more effective assessment of migraine impairment during and between attacks: results of the American Migraine Communication Study (AMCS) Phase II. Presented at: the Diamond Headache Clinic�s 20th Annual Practicing Physician�s Approach to the Difficult Headache Patient; February 12�15, 2007; California: Rancho Mirage;
Damaris Foreman suffered from migraines for about 23 years. After receiving traditional treatment for her migraine pain without much improvement, she was finally recommended to seek migraine pain treatment with Dr. Alex Jimenez, a chiropractor in El Paso, TX. Damaris greatly benefitted from chiropractic care and she experienced a tremendous sense of relief following her first spinal adjustment and manual manipulation. Damaris Foreman was able to confront many of her misconceptions and she learned very much about her migraine pain. Damaris describes Dr. Alex Jimenez’s migraine pain treatment as one of the best treatment she’s received and she highly recommends chiropractic care as the best non-surgical choice for improving and managing her migraines.
A migraine can be identified as a primary headache disorder characterized by recurrent headaches characterized from moderate to severe in intensity. Typically, the headaches affect one half of the head, are pulsating in nature, and can last from two to 72 hours. Associated symptoms may include nausea, vomiting, and sensitivity to light, sound, or smell. The pain may be aggravated by physical activity. Up to one-third of people who suffer from migraines experience migraine with aura: typically a brief period of visual disturbance that signals that the headache will soon happen. An aura can occur with little or no headache pain following it.
Please Recommend Us: If you have enjoyed this video and/or we have helped you in any way please feel free to recommend us. Thank You.
A primary headache is characterized as head pain caused by a headache disorder itself. The three types of primary headache disorders include, migraine, tension-type headaches and cluster headaches. Head pain is a painful and debilitating symptom that can also occur as a result of another underlying cause. A secondary headache is characterized as head pain which occurs due to an injury and/or condition. A spinal misalignment, or subluxation, along the cervical spine, or neck, is commonly associated with a variety of headache symptoms.
Cervicogenic headache is a secondary headache caused by an injury and/or condition affecting the surrounding structures of the cervical spine, or neck. Many healthcare professionals will recommend the use of drugs/medications to help improve headache, however, several alternative treatment options can be safely and effectively used to treat secondary headaches. The purpose of the following article is to demonstrate the impact of upper cervical and upper thoracic manipulation versus mobilization and exercise in patients with cervicogenic headache.
Upper Cervical and Upper Thoracic Manipulation Versus Mobilization and Exercise in Patients with Cervicogenic Headache: a Multi-Center Randomized Clinical Trial
Abstract
Background: Although commonly utilized interventions, no studies have directly compared the effectiveness of cervical and thoracic manipulation to mobilization and exercise in individuals with cervicogenic headache (CH). The purpose of this study was to compare the effects of manipulation to mobilization and exercise in individuals with CH.
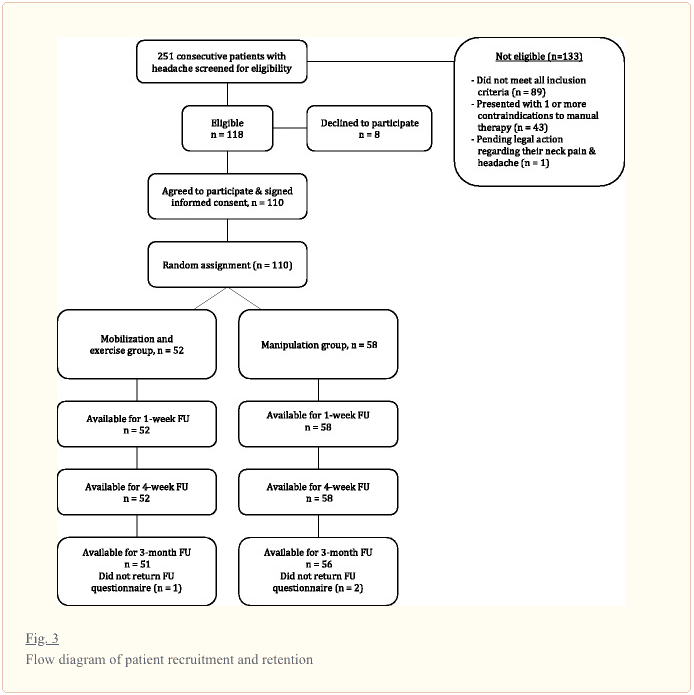
Methods: One hundred and ten participants (n?=?110) with CH were randomized to receive both cervical and thoracic manipulation (n?=?58) or mobilization and exercise (n?=?52). The primary outcome was headache intensity as measured by the Numeric Pain Rating Scale (NPRS). Secondary outcomes included headache frequency, headache duration, disability as measured by the Neck Disability Index (NDI), medication intake, and the Global Rating of Change (GRC). The treatment period was 4 weeks with follow-up assessment at 1 week, 4 weeks, and 3 months after initial treatment session. The primary aim was examined with a 2-way mixed-model analysis of variance (ANOVA), with treatment group (manipulation versus mobilization and exercise) as the between subjects variable and time (baseline, 1 week, 4 weeks and 3 months) as the within subjects variable.
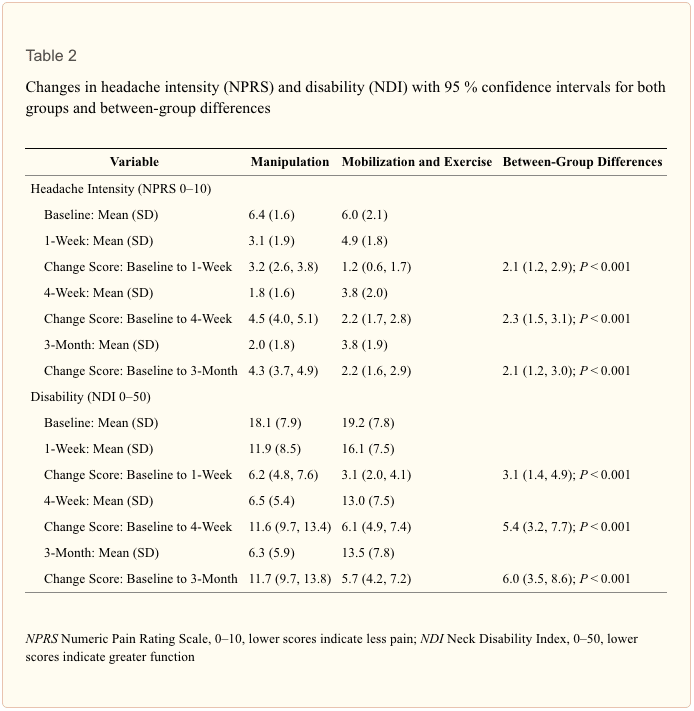
Results: The 2X4 ANOVA demonstrated that individuals with CH who received both cervical and thoracic manipulation experienced significantly greater reductions in headache intensity (p?<?0.001) and disability (p?<?0.001) than those who received mobilization and exercise at a 3-month follow-up. Individuals in the upper cervical and upper thoracic manipulation group also experienced less frequent headaches and shorter duration of headaches at each follow-up period (p?<?0.001 for all). Additionally, patient perceived improvement was significantly greater at 1 and 4-week follow-up periods in favor of the manipulation group (p?<?0.001).
Conclusions: Six to eight sessions of upper cervical and upper thoracic manipulation were shown to be more effective than mobilization and exercise in patients with CH, and the effects were maintained at 3 months.
Trial registration: NCT01580280 April 16, 2012.
Keywords:Cervicogenic headache, Spinal manipulation, Mobilization, High velocity low amplitude thrust
Dr. Alex Jimenez’s Insight
In comparison to primary headache, such as migraine, cluster headache and tension-type headache, secondary headache is characterized as head pain caused by another illness or physical issue. In the case of cervicogenic headache, the cause of head pain is due to an injury and/or condition along the cervical spine and its surrounding structures, including the vertebrae, intervertebral discs and soft tissues. In addition, many healthcare professionals believe that primary headache can be associated with health issues in the cervical spine, or neck. Cervicogenic headache treatment should target the source of the symptoms and it can vary depending on the patient. Chiropractic care utilizes spinal adjustments and manual manipulations to carefully restore the original structure and function of the spine, helping to reduce stress and pressure in order to improve cervicogenic headache symptoms, among other type of headache. Chiropractic care can also be utilized to help treat primary headaches, such as migraines.
Background
The International Classification of Headache Disorders defines cervicogenic headache (CH) as, �headache caused by a disorder of the cervical spine and its component bony, disc, and/or soft tissue elements, usually but not invariably accompanied by neck pain.� [1] (p.760) The prevalence of CH has been reported to be between 0.4 and 20 % of the headache population [2, 3], and as high as 53 % in patients with headache after whiplash injury [4]. The dominant features of CH usually include: unilaterality of head pain without side-shift, elicitation of pain with external pressure over the ipsilateral upper neck, limited cervical range of motion, and the triggering of attacks by various awkward or sustained neck movements [4, 5].
Individuals with CH are frequently treated with spinal manipulative therapy including both mobilization and manipulation [6]. Spinal mobilization consists of slow, rhythmical, oscillating techniques whereas manipulation consists of high-velocity low-amplitude thrust techniques. [7] In a recent systematic review, Bronfort and colleagues reported that spinal manipulative therapy (both mobilization and manipulation) were effective in the management of adults with CH [8]. However, they did not report if manipulation resulted in superior outcomes compared to mobilization for the management of this population.
Several studies have investigated the effect of spinal manipulation in the management of CH [9�13]. Haas et al. [10] investigated the effectiveness of cervical manipulation in subjects with CH. Jull et al. [11] demonstrated treatment efficacy for manipulative therapy and/or exercise in the management of CH. However the manipulative therapy group included manipulation and mobilization therefore it cannot be determined if the beneficial effect was a result of the manipulation, mobilization or the combination.
A few studies have examined the benefits of manipulation versus mobilization for the management of mechanical neck pain with or without exercise [14�16]. However, no studies have directly compared the effects of manipulation versus mobilization and exercise in patients with CH. Considering the purported risks of manipulation [17], it is essential to determine if manipulation results in improved outcomes compared to mobilization for the management of patients with CH. Therefore, the purpose of this randomized clinical trial was to compare the effects of manipulation versus mobilization and exercise in patients with CH. We hypothesized that patients receiving manipulation over a 4-week treatment period would experience greater reductions in headache intensity, headache frequency, headache duration, disability, and medication intake at a 3-month follow-up than patients receiving cervical and thoracic mobilization combined with exercise.
Methods
Participants
In this multi-center randomized clinical trial, consecutive patients with CH presenting to 1 of 8 outpatient physical therapy clinics from a variety of geographical locations (Arizona, Georgia, New York, Ohio, Pennsylvania, South Carolina) were recruited over a 29-month period (from April 2012 to August 2014). For patients to be eligible, they had to present with a diagnosis of CH according to the revised diagnostic criteria [5] developed by the Cervicogenic Headache International Study Group (CHISG) [5, 18, 19]. CH was classified according to the �major criteria� (not including confirmatory evidence by diagnostic anesthetic blockades) and �head pain characteristics� of the CHISG. Therefore, in order to be included in the study, patients had to exhibit all of the following criteria: (1) unilaterality of the head pain without sideshift, starting in the upper posterior neck or occipital region, eventually spreading to the oculofrontotemporal area on the symptomatic side, (2) pain triggered by neck movement and/or sustained awkward positions, (3) reduced range of motion in the cervical spine [20] (i.e., less than or equal to 32 � of right or left passive rotation on the Flexion-Rotation Test [21�23], (4) pain elicited by external pressure over at least one of the upper cervical joints (C0-3), and (5) moderate to severe, non-throbbing and non-lancinating pain. In addition, participants had to have a headache frequency of at least 1 per week for a minimum of 3 months, a minimum headache intensity pain score of two points (0�10 on the NPRS scale), a minimum disability score of 20 % or greater (i.e., 10 points or greater on the 0�50 NDI scale), and be between 18 and 65 years of age.
Patients were excluded if they exhibited other primary headaches (i.e., migraine, TTH), suffered from bilateral headaches, or exhibited any red flags (i.e., tumor, fracture, metabolic diseases, rheumatoid arthritis, osteoporosis, resting blood pressure greater than 140/90 mmHg, prolonged history of steroid use, etc.), presented with two or more positive neurologic signs consistent with nerve root compression (muscle weakness involving a major muscle group of the upper extremity, diminished upper extremity deep tendon reflex, or diminished or absent sensation to pinprick in any upper extremity dermatome), presented with a diagnosis of cervical spinal stenosis, exhibited bilateral upper extremity symptoms, had evidence of central nervous system involvement (hyperreflexia, sensory disturbances in the hand, intrinsic muscle wasting of the hands, unsteadiness during walking, nystagmus, loss of visual acuity, impaired sensation of the face, altered taste, the presence of pathological reflexes), had a history of whiplash injury within the previous 6 weeks, had prior surgery to the head or neck, had received treatment for head or neck pain from any practitioner within the previous month, had received physical therapy or chiropractic treatment for head or neck pain within the previous 3 months, or had pending legal action regarding their head or neck pain.
The most recent literature suggests that pre-manipulative cervical artery testing is unable to identify those individuals at risk of vascular complications from cervical manipulation [24, 25], and any symptoms detected during pre-manipulative testing may be unrelated to changes in blood flow in the vertebral artery [26, 27]. Hence, pre-manipulative cervical artery testing was not performed in this study; however, screening questions for cervical artery disease had to be negative [24, 28, 29]. This study was approved by the Institutional Review Board at Long Island University, Brooklyn, NY. The study was registered at www.clinicaltrials.gov with trial identifier NCT01580280. All patients were informed that they would receive either manipulation or mobilization and exercise and then provided informed consent before their enrollment in the study.
Treating Therapists
Twelve physical therapists (mean age 36.6 years, SD 5.62) participated in the delivery of treatment for patients in this study. They had an average of 10.3 (SD 5.66, range 3�20 years) years of clinical experience, and all had completed a 60 h post-graduate certification program that included practical training in manual techniques including the use of cervical and thoracic manipulation. To ensure all examination, outcome assessments, and treatment procedures were standardized, all participating physical therapists were required to study a manual of standard operating procedures and participate in a 4 h training session with the principal investigator.
Examination Procedures
All patients provided demographic information, completed the Neck Pain Medical Screening Questionnaire, and completed a number of self-report measures, followed by a standardized history and physical examination at baseline. Self-report measures included headache intensity as measured by the NPRS (0�10), the NDI (0�50), headache frequency (number of days with headache in the last week), headache duration (total hours of headache in the last week), and medication intake (number of times the patient had taken narcotic or over-the-counter pain medication in the past week).
The standardized physical examination was not limited to, but included measurements of C1-2 (atlanto-axial joint) passive right and left rotation ROM using the Flexion-Rotation Test (FRT). The inter-rater reliability for the FRT has been found to be excellent (ICC: 0.93; 95 % CI: 0.87, 0.96) [30].
Outcome Measures
The primary outcome measure used in this study was the patient�s headache intensity as measured by the NPRS. Patients were asked to indicate the average intensity of headache pain over the past week using an 11-point scale ranging from 0 (�no pain�) to 10 (�worst pain imaginable�) at baseline, 1-week, 1-month, and 3-months following the initial treatment session [31]. The NPRS is a reliable and valid instrument to assess pain intensity [32�34]. Although no data exists in patients with CH, the MCID for the NPRS has been shown to be 1.3 in patients with mechanical neck pain [32] and 1.74 in patients with a variety of chronic pain conditions [34]. Therefore, we chose to only include patients with an NPRS score of 2 points (20 %) or greater.
Secondary outcome measures included the NDI, the Global Rating of Change (GRC), headache frequency, headache duration, and medication intake. The NDI is the most widely used instrument for assessing self-rated disability in patients with neck pain [35�37]. The NDI is a self-report questionnaire with 10-items rated from 0 (no disability) to five (complete disability) [38]. The numeric responses for each item are summed for a total score ranging between 0 and 50; however, some evaluators have chosen to multiply the raw score by two, and then report the NDI on a 0�100 % scale [36, 39]. Higher scores represent increased levels of disability. The NDI has been found to possess excellent test-retest reliability, strong construct validity, strong internal consistency and good responsiveness in assessing disability in patients with mechanical neck pain [36], cervical radiculopathy [33, 40], whiplash associated disorder [38, 41, 42], and mixed non-specific neck pain [43, 44]. Although no studies have examined the psychometric properties of the NDI in patients with CH, we chose to only include patients with an NDI score of ten points (20 %) or greater, because this cut-off score captures the MCID for the NDI, which has been reported to approximate four, eight, and nine points (0�50) in patients with mixed non-specific neck pain [44], mechanical neck pain [45], and cervical radiculopathy [33], respectively. Headache frequency was measured as the number of days with headache in the last week, ranging from 0 to 7 days. Headache duration was measured as the total hours of headache in the last week, with six possible ranges: (1) 0�5 h, (2) 6�10 h, (3) 11�15 h, (4) 16�20 h, (5) 21�25 h, or (6) 26 or more hours. Medication intake was measured as the number of times the patient had taken prescription or over-the-counter analgesic or anti-inflammatory medication in the past week for their headaches, with five options: (1) not at all, (2) once a week, (3) once every couple of days, (4) once or twice a day, or (5) three or more times a day.
Patients returned for 1-week, 4-weeks, and 3-months follow-ups where the aforementioned outcome measures were again collected. In addition, at the 1-week, 4-weeks and 3-months follow-ups, patients completed a 15-point GRC question based on a scale described by Jaeschke et al. [46] to rate their own perception of improved function. The scale ranges from -7 (a very great deal worse) to zero (about the same) to +7 (a very great deal better). Intermittent descriptors of worsening or improving are assigned values from -1 to -6 and +1 to +6, respectively. The MCID for the GRC has not been specifically reported but scores of +4 and +5 have typically been indicative of moderate changes in patient status [46]. However, it should be noted that recently Schmitt and Abbott reported that the GRC might not correlate with changes in function in a population with hip and ankle injuries [47]. All outcome measures were collected by an assessor blind to group assignment.
On the initial visit patients completed all outcome measures then received the first treatment session. Patients completed 6�8 treatment sessions of either manipulation or mobilization combined with exercise over 4 weeks. Additionally, subjects were asked if they had experienced any �major� adverse events [48, 49] (stroke or permanent neurological deficits) at each follow-up period.
Randomization
Following the baseline examination, patients were randomly assigned to receive either manipulation or mobilization and exercise. Concealed allocation was performed by using a computer-generated randomized table of numbers created by an individual not involved with recruiting patients prior to the beginning of the study. Individual, sequentially numbered index cards with the random assignment were prepared for each of 8 data collection sites. The index cards were folded and placed in sealed opaque envelopes. Blinded to the baseline examination, the treating therapist opened the envelope and proceeded with treatment according to the group assignment. Patients were instructed not to discuss the particular treatment procedure received with the examining therapist. The examining therapist remained blind to the patient�s treatment group assignment at all times; however, based on the nature of the interventions it was not possible to blind patients or treating therapists.
Manipulation Group
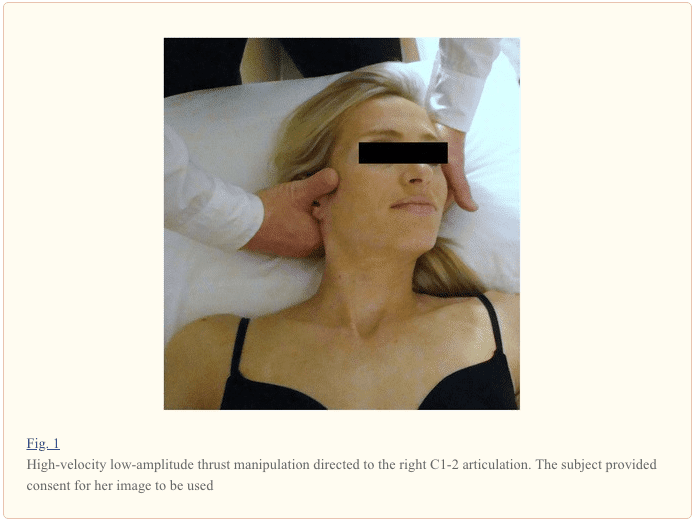
Manipulations targeting the right and left C1-2 articulations and bilateral T1-2 articulations were performed on at least one of the 6�8 treatment sessions (Figs. 1 and ?and2).2). On other treatment sessions, therapists either repeated the C1-2 and/or T1-2 manipulations or targeted other spinal articulations (i.e., C0-1, C2-3, C3-7, T2-9, ribs 1�9) using manipulation. The selection of the spinal segments to target was left to the discretion of the treating therapist and it was based on the combination of patient reports and manual examination. For both the upper cervical and upper thoracic manipulations, if no popping or cracking sound was heard on the first attempt, the therapist repositioned the patient and performed a second manipulation. A maximum of 2 attempts were performed on each patient similar to other studies [14, 50�53]. The clinicians were instructed that the manipulations are likely to be accompanied by multiple audible popping sounds [54�58]. Patients were encouraged to maintain usual activity within the limits of pain; however, mobilization and the prescription of exercises, or any use of other modalities, were not provided to this group.
The manipulation targeting C1-2 was performed with the patient in supine. For this technique, the patient�s left posterior arch of the atlas was contacted with the lateral aspect of the proximal phalanx of the therapist�s left second finger using a �cradle hold�. To localize the forces to the left C1-2 articulation, the patient was positioned using extension, a posterior-anterior (PA) shift, ipsilateral side-bend and contralateral side-shift. While maintaining this position, the therapist performed a single high-velocity, low-amplitude thrust manipulation to the left atlanto-axial joint using right rotation in an arc toward the underside eye and translation toward the table (Fig. 1). This was repeated using the same procedure but directed to the right C1-2 articulation.
The manipulation targeting T1-2 was performed with the patient in supine. For this technique, the patient held her/his arms and forearms across the chest with the elbows aligned in a superoinferior direction. The therapist contacted the transverse processes of the lower vertebrae of the target motion segment with the thenar eminence and middle phalanx of the third digit. The upper lever was localized to the target motion segment by adding rotation away and side-bend towards the therapist while the underside hand used pronation and radial deviation to achieve rotation toward and side-bend away moments, respectively. The space inferior to the xiphoid process and costochondral margin of the therapist was used as the contact point against the patient�s elbows to deliver a manipulation in an anterior to posterior direction targeting T1-2 bilaterally (Fig. 2).
Mobilization and Exercise Group
Mobilizations targeting the right and left C1-2 articulations and bilateral T1-2 articulations were performed on at least one of the 6�8 treatment sessions. On other treatment sessions, therapists either repeated the C1-2 and/or T1-2 mobilizations or targeted other spinal articulations (i.e., C0-1, C2/3, C3-7, T2-9, ribs 1�9) using mobilization. The selection of the spinal segments to target was left to the discretion of the treating therapist and it was based on the combination of patient reports and manual examination. However, in order to avoid a �contact� or �attention effect� when compared with the manipulation group, therapists were instructed to mobilize one cervical segment (i.e., right and left) and one thoracic segment or rib articulation on each treatment session.
The mobilization targeting the C1-2 articulation was performed in prone. For this technique, the therapist performed one 30 s bout of left-sided unilateral grade IV PA mobilizations to the C1-2 motion segment as described by Maitland [7]. This same procedure was repeated for one 30 s bout to the right atlanto-axial joint. In addition, and on at least one session, mobilization directed to the upper thoracic (T1-2) spine with the patient prone was performed. For this technique, the therapist performed one 30 s bout of central grade IV PA mobilizations to the T1-2 motion segment as described by Maitland [7]. Therefore, we used 180 (i.e., three 30 s bouts at approximately 2 Hz) end-range oscillations in total on each subject for the mobilization treatment. Notably, there is no high quality evidence to date to suggest that longer durations of mobilization result in greater pain reduction than shorter durations or dosages of mobilization [59, 60].
Cranio-cervical flexion exercises [11, 61�63] were performed with the patient in supine, with the knees bent and the position of the head standardized by placing the craniocervical and cervical spines in a mid-position, such that a line between the subject�s forehead and chin was horizontal, and a horizontal line from the tragus of the ear bisected the neck longitudinally. An air-filled pressure biofeedback unit (Chattanooga Group, Inc., Hixson, TN) was placed suboccipitally behind the patient�s neck and preinflated to a baseline of 20 mmHg [63]. For the staged exercises, patients were required to perform the craniocervical flexion action (�a nod of the head, similar to indicating yes�) [63] and attempt to visually target pressures of 22, 24, 26, 28, and 30 mmHg from a resting baseline of 20 mmHg and to hold the position steady for 10 s [61, 62]. The action of nodding was performed in a gentle and slow manner. A 10 s rest was allowed between trials. If the pressure deviated below the target pressure, the pressure was not held steady, substitution with the superficial flexors (sternocleidomastoid or anterior scalene) occurred, or neck retraction was noticed before the completion of the 10 s isometric hold, it was regarded as a failure [63]. The last successful target pressure was used to determine each patient�s exercise level wherein 3 sets of 10 repetitions with a 10 s isometric hold were performed. In addition to mobilizations and cranio-cervical flexion exercises, patients were required to perform 10 min of progressive resistance exercises (i.e., using Therabands� or free weights) to the muscles of the shoulder girdle during each treatment session, within their own tolerance, and specifically focusing on the lower trapezius and serratus anterior [11].
Sample Size
The sample size and power calculations were performed using online software from the MGH Biostatistics Center (Boston, MA). The calculations were based on detecting a 2-point (or 20 %) difference in the NPRS (headache intensity) at the 3 months follow-up, assuming a standard deviation of three points, a 2-tailed test, and an alpha level equal to 0.05. This generated a sample size of 49 patients per group. Allowing for a conservative dropout rate of 10 %, we planned to recruit at least 108 patients into the study. This sample size yielded greater than 90 % power to detect a statistically significant change in the NPRS scores.
Data Analysis
Descriptive statistics, including frequency counts for categorical variables and measures of central tendency and dispersion for continuous variables were calculated to summarize the data. The effects of treatment on headache intensity and disability were each examined with a 2-by-4 mixed-model analysis of variance (ANOVA), with treatment group (manipulation versus mobilization and exercise) as the between-subjects variable and time (baseline, 1 week, 4 weeks, and 3 months follow-up) as the within-subjects variable. Separate ANOVAs were performed with the NPRS (headache intensity) and NDI (disability) as the dependent variable. For each ANOVA, the hypothesis of interest was the 2-way interaction (group by time).
An independent t-test was used to determine the between group differences for the percentage change from baseline to 3-month follow-up in both headache intensity and disability. Separate Mann�Whitney U tests were performed with the headache frequency, GRC, headache duration and medication intake as the dependent variable. We performed Little�s Missing Completely at Random (MCAR) test [64] to determine if missing data points associated with dropouts were missing at random or missing for systematic reasons. Intention-to-treat analysis was performed by using Expectation-Maximization whereby missing data are computed using regression equations. Planned pairwise comparisons were performed examining the difference between baseline and follow-up periods between-groups using the Bonferroni correction at an alpha level of .05.
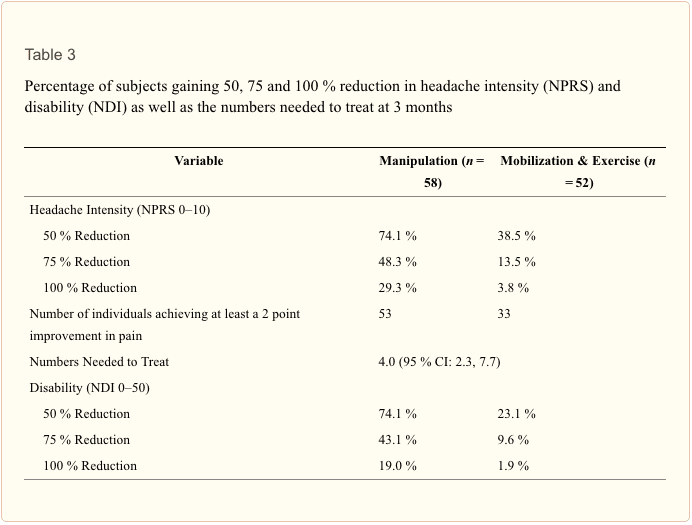
We dichotomized patients as responders at the 3-month follow-up using a cut score of 2 points improvement for headache intensity as measured by the NPRS. Numbers needed to treat (NNT) and 95 % confidence intervals (CI) were also calculated at the 3 months follow-up period using each of these definitions for a successful outcome. Data analysis was performed using SPSS 21.0.
Results
Two hundred and fifty-one patients with a primary complaint of headaches were screened for possible eligibility. The reasons for ineligibility can be found in Fig. 3, the flow diagram of patient recruitment and retention. Of the 251 patients screened, 110 patients, with a mean age of 35.16 years (SD 11.48) and a mean duration of symptoms of 4.56 years (SD 6.27), satisfied the eligibility criteria, agreed to participate, and were randomized into manipulation (n?=?58) and mobilization and exercise (n?=?52) groups. Baseline variables for each group can be found in Table 1. Twelve therapists from 8 outpatient physical therapy clinics each treated 25, 23, 20, 14, 13, 7, 6 or 2 patients, respectively; furthermore, each of the 12 therapists treated approximately an equal proportion of patients in each group. There was no significant difference (p?=?0.227) between the mean number of completed treatment sessions for the manipulation group (7.17, SD 0.96) and the mobilization and exercise group (6.90, SD 1.35). In addition, the mean number of treatment sessions that targeted the C1-2 articulation was 6.41 (SD 1.63) for the manipulation group and 6.52 (SD 2.01) for the mobilization and exercise group, and this was not significantly different (p?=?0.762). One hundred seven of the 110 patients completed all outcome measures through 3 months (97 % follow-up). Little�s Missing Completely at Random (MCAR) test was not statistically significant (p?=?0.281); therefore, we used the Expectation-Maximization imputation technique to replace missing values with predicted values for the missing 3-month outcomes.
The overall group by time interaction for the primary outcome of headache intensity was statistically significant for the NPRS (F(3,106)?=?11.196; p?<?0.001; partial eta squared?=?0.24). Between-group differences revealed that the manipulation group experienced statistically significant greater improvement in the NPRS at both the 1-week (2.1, 95 % CI: 1.2, 2.9), 4-week (2.3, 95 % CI: 1.5, 3.1) and 3-month (2.1, 95 % CI: 1.2, 3.0) follow-up periods (Table 2). In addition, an independent samples t-test revealed the between-group difference in percentage change in headache intensity (36.58 %, 95 % CI: 22.52, 50.64) from baseline to 3-month follow-up was statistically significant (t(108)?=?5.156; p?<?0.001) in favor of manipulation. See Table 3 for the percentage of subjects gaining 50, 75, and 100 % reduction in headache intensity at 3 months.
For secondary outcomes a significant group by time interaction existed for the NDI (F(3,106)?=?8.57; p?<?0.001; partial eta squared?=?0.20). At each follow-up period the manipulation group had superior outcomes in disability reduction as compared to the mobilization and exercise group. An independent samples t- test revealed the between-group mean percentage change in disability (35.56 %, 95 % CI: 24.95, 46.17) from baseline to 3 months follow-up was statistically significant (t(108)?=?6.646, p?<?0.001); indicating the manipulation group experienced a significantly greater percentage in disability reduction (Table 3).
Mann�Whitney U tests revealed that patients in the upper cervical and upper thoracic manipulation group experienced less frequent headaches at 1 week (p?<?0.001; median 2.0 versus 3.0), 4 weeks (p?<?0.001; median 1.0 versus 3.0) and 3 months (p?<?0.001; median 1.0 versus 2.5) than patients in the mobilization and exercise group. Headache duration was significantly lower at 1 week (p?=?0.005; median 2.0 versus 3.0, 4 weeks (p?<?0.001; median 1.0 versus 2.0) and 3 months (p?<?0.001; median 1.0 versus 2.0) in the manipulation group. Additionally, patient perceived improvement as measured by the GRC was significantly greater at 1 week (p?<?0.001, 4.0 versus 1.0), 4 weeks (p?<?0.001, 6.0 versus 3.0) and 3 months (p?<?0.001, 6.0 versus 3.0) than patients in the mobilization and exercise group. At 3 months, patients receiving upper cervical and upper thoracic manipulation experienced significantly (p?<?0.001) greater reductions in medication intake as compared to the mobilization and exercise group. Based on the cutoff score of 2 points on the NPRS, the NNT was 4.0 (95 % CI: 2.3, 7.7) in favor of the manipulation group at 3-month follow-up.
We did not collect any data on the occurrence of �minor� adverse events [48, 49] (transient neurological symptoms, increased stiffness, radiating pain, fatigue or other); however, no �major� adverse events [48, 49] (stroke or permanent neurological deficits) were reported for either group.
Discussion
Statement of Principal Findings
To our knowledge, this study is the first randomized clinical trial to directly compare the effectiveness of both cervical and thoracic manipulation to mobilization and exercise in patients with CH. The results suggest 6�8 sessions of manipulation over 4 weeks, directed mainly to both the upper cervical (C1-2) and upper thoracic (T1-2) spines, resulted in greater improvements in headache intensity, disability, headache frequency, headache duration, and medication intake than mobilization combined with exercises. The point estimates for between-group changes in headache intensity (2.1 points) and disability (6.0 points or 12.0 %) exceeded the reported MCIDs for both measures. Although the MCID for the NDI in patients with CH has not yet been investigated, it should however be noted that the lower bound estimate of the 95 % CI for disability (3.5 points) was slightly below (or approximated in two cases) the MCID that has been found to be 3.5 [65], 5 [66], and 7.5 [45] points in patients with mechanical neck pain, 8.5 [33] points in patients with cervical radiculopathy, and 3.5 [44] points in patients with mixed, non-specific neck pain. However, it should be recognized that both groups made clinical improvement. In addition, the NNT suggests for every four patients treated with manipulation, rather than mobilization, one additional patient achieves clinically important pain reduction at 3 months follow-up.
Strengths and Weaknesses of the Study
The inclusion of 12 treating physical therapists from 8 private clinics in 6 different geographical states enhances the overall generalizability of our findings. Although significant differences were recognized up to 3 months, it is not known if these benefits would have been sustained at long-term. In addition, we used high-velocity, low-amplitude manipulation techniques that employed bidirectional thrusts into rotation and translation simultaneously and Maitland based grade IV PA mobilization techniques; thus, we cannot be certain that these results are generalizable to other kinds of manual therapy techniques. Some might argue that the comparison group might have not received adequate intervention. We sought to balance internal and external validity so standardized treatment for both groups and provided a very explicit description of the techniques used which will also allow for replication. Furthermore, we did not measure minor adverse events and only asked about two potential major adverse events. Another limitation is that we included multiple secondary outcomes. Therapist preferences as to which technique they thought would be superior was not collected and potentially could impact the results.
Strengths and Weaknesses in Relation to Other Studies: Important Differences in Results
Jull et al. [11] demonstrated treatment efficacy for manipulative therapy and exercise in the management of CH; however, this treatment package included both mobilization and manipulation. The current study may provide evidence that the management of patients with CH should include some form of manipulation despite the fact it is often suggested that cervical manipulation should be avoided because of the risk of serious adverse events [67, 68]. Furthermore, it has been shown that individuals receiving spinal manipulation for neck pain and headaches are no more likely to experience a vertebrobasilar stroke than if they received treatment by their medical physician [69]. Additionally, after reviewing 134 case reports, Puentedura et al. concluded that with appropriate selection of patients by careful screening of red flags and contraindications, the majority of adverse events associated with cervical manipulation could have been prevented [70].
Meaning of the Study: Possible Explanations and Implications for Clinicians and Policymakers
Based on the results of the current study clinicians should consider incorporating spinal manipulation for individuals with CH. A recent systematic review found both mobilization and manipulation to be effective for the management of patients with CH but was unable to determine which technique was superior [8]. Additionally, clinical guidelines reported that manipulation, mobilization and exercise were all effective for the management of patients with CH; however, the guideline made no suggestions regarding the superiority of either technique. [71] The current results may assist authors of future systematic reviews and clinical guidelines in providing more specific recommendations about the use of spinal manipulation in this population.
Unanswered Questions and Future Research
The underlying mechanisms as to why manipulation may have resulted in greater improvements remains to be elucidated. It has been suggested that high-velocity displacement of vertebrae with impulse durations of less than 200 ms may alter afferent discharge rates [72] by stimulating mechanoreceptors and proprioceptors, thereby changing alpha motorneuron excitability levels and subsequent muscle activity [72�74]. Manipulation might also stimulate receptors in the deep paraspinal musculature, and mobilization might be more likely to facilitate receptors in the superficial muscles [75]. Biomechanical [76, 77], spinal or segmental [78, 79] and central descending inhibitory pain pathway [80�83] models are plausible explanations for the hypoalgesic effects observed following manipulation. Recently, the biomechanical effects of manipulation have been under scientific scrutiny [84], and it is plausible that the clinical benefits found in our study are associated with a neurophysiological response involving temporal sensory summation at the dorsal horn of the spinal cord [78]; however, this proposed model is currently supported only on findings from transient, experimentally induced pain in healthy subjects [85, 86], not patients with CH. Future studies should examine different manual therapy techniques with varying dosages and include a 1-year follow-up. Furthermore, future studies examining the neurophysiological effects of both manipulation and mobilization will be important for determining why there may or may not be a difference in clinical effects between these two treatments.
Conclusion
The results of the current study demonstrated that patients with CH who received cervical and thoracic manipulation experienced significantly greater reductions in headache intensity, disability, headache frequency, headache duration, and medication intake as compared to the group that received mobilization and exercise; furthermore, the effects were maintained at 3 months follow-up. Future studies should examine the effectiveness of different types and dosages of manipulation and include a long-term follow-up.
Acknowledgements
None of the authors received any funding for this study. The authors wish to thank all the participants of the study.
Footnotes
Competing interests: Dr. James Dunning is the President of the American Academy of Manipulative Therapy (AAMT). AAMT provides postgraduate training programs in spinal manipulation, spinal mobilization, dry needling, extremity manipulation, extremity mobilization, instrument-assisted soft-tissue mobilization and therapeutic exercise to licensed physical therapists, osteopaths and medical doctors. Drs. James Dunning, Raymond Butts, Thomas Perreault, and Firas Mourad are senior instructors for AAMT. The other authors declare that they have no competing interests.
Authors� contributions: JRD participated in the conception, design, data acquisition, statistical analyses and drafting of the manuscript. RB and IY participated in the design, data collection, statistical analyses and revision of the manuscript. FM participated in the design, statistical analyses, data interpretation and revision of the manuscript. MH participated in the conception, design and revision of the manuscript. CF and JC were involved in the statistical analyses, interpretation of data, and critical revision of the manuscript for important intellectual content. TS, JD, DB, and TH were involved in data collection and revision of the manuscript. All authors read and approved the final manuscript.
In conclusion,�head pain caused by secondary headache due to a health issue along the surrounding structures of the cervical spine, or neck, can cause painful and debilitating symptoms which can affect the patient’s quality of life. Spinal manipulation and mobilization can be safely and effectively utilized to help improve cervicogenic headache symptoms. Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Back Pain
According to statistics, approximately 80% of people will experience symptoms of back pain at least once throughout their lifetimes. Back pain is a common complaint which can result due to a variety of injuries and/or conditions. Often times, the natural degeneration of the spine with age can cause back pain. Herniated discs occur when the soft, gel-like center of an intervertebral disc pushes through a tear in its surrounding, outer ring of cartilage, compressing and irritating the nerve roots. Disc herniations most commonly occur along the lower back, or lumbar spine, but they may also occur along the cervical spine, or neck. The impingement of the nerves found in the low back due to injury and/or an aggravated condition can lead to symptoms of sciatica.
1.�The International Classifcation of Headache Disorders: 3rd Edition. Cephalalgia. 2013;33(9):629-808.[PubMed]
2.�Anthony M. Cervicogenic headache: prevalence and response to local steroid therapy.�Clin Exp Rheumatol.�2000;18(2 Suppl 19):S59�64.�[PubMed]
3.�Nilsson N. The prevalence of cervicogenic headache in a random population sample of 20-59 year olds.�Spine (Phila Pa 1976)�1995;20(17):1884�8. doi: 10.1097/00007632-199509000-00008.�[PubMed][Cross Ref]
4.�Bogduk N, Govind J. Cervicogenic headache: an assessment of the evidence on clinical diagnosis, invasive tests, and treatment.�Lancet Neurol.�2009;8(10):959�68. doi: 10.1016/S1474-4422(09)70209-1.[PubMed]�[Cross Ref]
5.�Sjaastad O, Fredriksen TA, Pfaffenrath V. Cervicogenic headache: diagnostic criteria. The Cervicogenic Headache International Study Group.�Headache.�1998;38(6):442�5. doi: 10.1046/j.1526-4610.1998.3806442.x.�[PubMed]�[Cross Ref]
6.�Fernandez-de-Las-Penas C, Alonso-Blanco C, Cuadrado ML, Pareja JA. Spinal manipulative therapy in the management of cervicogenic headache.�Headache.�2005;45(9):1260�3. doi: 10.1111/j.1526-4610.2005.00253_1.x.�[PubMed]�[Cross Ref]
8.�Bronfort G, Haas M, Evans R, Leininger B, Triano J. Effectiveness of manual therapies: the UK evidence report.�Chiropr Osteopat.�2010;18:3. doi: 10.1186/1746-1340-18-3.�[PMC free article]�[PubMed][Cross Ref]
9.�Haas M, Groupp E, Aickin M, Fairweather A, Ganger B, Attwood M, et al. Dose response for chiropractic care of chronic cervicogenic headache and associated neck pain: a randomized pilot study.�J Manipulative Physiol Ther.�2004;27(9):547�53. doi: 10.1016/j.jmpt.2004.10.007.�[PubMed]�[Cross Ref]
10.�Haas M, Spegman A, Peterson D, Aickin M, Vavrek D. Dose response and efficacy of spinal manipulation for chronic cervicogenic headache: a pilot randomized controlled trial.�Spine J.�2010;10(2):117�28. doi: 10.1016/j.spinee.2009.09.002.�[PMC free article]�[PubMed]�[Cross Ref]
11.�Jull G, Trott P, Potter H, Zito G, Niere K, Shirley D, et al. A randomized controlled trial of exercise and manipulative therapy for cervicogenic headache.�Spine (Phila Pa 1976)�2002;27(17):1835�43. doi: 10.1097/00007632-200209010-00004.�[PubMed]�[Cross Ref]
12.�Nilsson N. A randomized controlled trial of the effect of spinal manipulation in the treatment of cervicogenic headache.�J Manipulative Physiol Ther.�1995;18(7):435�40.�[PubMed]
13.�Nilsson N, Christensen HW, Hartvigsen J. The effect of spinal manipulation in the treatment of cervicogenic headache.�J Manipulative Physiol Ther.�1997;20(5):326�30.�[PubMed]
14.�Dunning JR, Cleland JA, Waldrop MA, Arnot CF, Young IA, Turner M, et al. Upper cervical and upper thoracic thrust manipulation versus nonthrust mobilization in patients with mechanical neck pain: a multicenter randomized clinical trial.�J Orthop Sports Phys Ther.�2012;42(1):5�18. doi: 10.2519/jospt.2012.3894.�[PubMed]�[Cross Ref]
15.�Hurwitz EL, Morgenstern H, Harber P, Kominski GF, Yu F, Adams AH. A randomized trial of chiropractic manipulation and mobilization for patients with neck pain: clinical outcomes from the UCLA neck-pain study.�Am J Public Health.�2002;92(10):1634�41. doi: 10.2105/AJPH.92.10.1634.[PMC free article]�[PubMed]�[Cross Ref]
16.�Leaver AM, Maher CG, Herbert RD, Latimer J, McAuley JH, Jull G, et al. A randomized controlled trial comparing manipulation with mobilization for recent onset neck pain.�Arch Phys Med Rehabil.�2010;91(9):1313�8. doi: 10.1016/j.apmr.2010.06.006.�[PubMed]�[Cross Ref]
17.�Wand BM, Heine PJ, O’Connell NE. Should we abandon cervical spine manipulation for mechanical neck pain? Yes.�BMJ.�2012;344:e3679. doi: 10.1136/bmj.e3679.�[PubMed]�[Cross Ref]
18.�Sjaastad O, Fredriksen TA. Cervicogenic headache: criteria, classification and epidemiology.�Clin Exp Rheumatol.�2000;18(2 Suppl 19):S3�6.�[PubMed]
19.�Vincent MB, Luna RA. Cervicogenic headache: a comparison with migraine and tension-type headache.�Cephalalgia.�1999;19(Suppl 25):11�6. doi: 10.1177/0333102499019S2503.�[PubMed][Cross Ref]
20.�Zwart JA. Neck mobility in different headache disorders.�Headache.�1997;37(1):6�11. doi: 10.1046/j.1526-4610.1997.3701006.x.�[PubMed]�[Cross Ref]
21.�Hall T, Robinson K. The flexion-rotation test and active cervical mobility–a comparative measurement study in cervicogenic headache.�Man Ther.�2004;9(4):197�202. doi: 10.1016/j.math.2004.04.004.[PubMed]�[Cross Ref]
22.�Hall TM, Briffa K, Hopper D, Robinson KW. The relationship between cervicogenic headache and impairment determined by the flexion-rotation test.�J Manipulative Physiol Ther.�2010;33(9):666�71. doi: 10.1016/j.jmpt.2010.09.002.�[PubMed]�[Cross Ref]
23.�Ogince M, Hall T, Robinson K, Blackmore AM. The diagnostic validity of the cervical flexion-rotation test in C1/2-related cervicogenic headache.�Man Ther.�2007;12(3):256�62. doi: 10.1016/j.math.2006.06.016.�[PubMed]�[Cross Ref]
24.�Hutting N, Verhagen AP, Vijverman V, Keesenberg MD, Dixon G, Scholten-Peeters GG. Diagnostic accuracy of premanipulative vertebrobasilar insufficiency tests: a systematic review.�Man Ther.�2013;18(3):177�82. doi: 10.1016/j.math.2012.09.009.�[PubMed]�[Cross Ref]
25.�Kerry R, Taylor AJ, Mitchell J, McCarthy C. Cervical arterial dysfunction and manual therapy: a critical literature review to inform professional practice.�Man Ther.�2008;13(4):278�88. doi: 10.1016/j.math.2007.10.006.�[PubMed]�[Cross Ref]
26.�Thomas LC, Rivett DA, Bateman G, Stanwell P, Levi CR. Effect of selected manual therapy interventions for mechanical neck pain on vertebral and internal carotid arterial blood flow and cerebral inflow.�Phys Ther.�2013;93(11):1563�74. doi: 10.2522/ptj.20120477.�[PubMed]�[Cross Ref]
27.�Quesnele JJ, Triano JJ, Noseworthy MD, Wells GD. Changes in vertebral artery blood flow following various head positions and cervical spine manipulation.�J Manipulative Physiol Ther.�2014;37(1):22�31. doi: 10.1016/j.jmpt.2013.07.008.�[PubMed]�[Cross Ref]
28.�Taylor AJ, Kerry R. The ‘vertebral artery test’.�Man Ther.�2005;10(4):297. doi: 10.1016/j.math.2005.02.005.�[PubMed]�[Cross Ref]
29.�Kerry R, Taylor AJ, Mitchell J, McCarthy C, Brew J. Manual therapy and cervical arterial dysfunction, directions for the future: a clinical perspective.�J Man Manip Ther.�2008;16(1):39�48. doi: 10.1179/106698108790818620.�[PMC free article]�[PubMed]�[Cross Ref]
30.�Hall TM, Robinson KW, Fujinawa O, Akasaka K, Pyne EA. Intertester reliability and diagnostic validity of the cervical flexion-rotation test.�J Manipulative Physiol Ther.�2008;31(4):293�300. doi: 10.1016/j.jmpt.2008.03.012.�[PubMed]�[Cross Ref]
31.�Jensen MP, Karoly P, Braver S. The measurement of clinical pain intensity: a comparison of six methods.�Pain.�1986;27(1):117�26. doi: 10.1016/0304-3959(86)90228-9.�[PubMed]�[Cross Ref]
32.�Cleland JA, Childs JD, Whitman JM. Psychometric properties of the Neck Disability Index and numeric pain rating scale in patients with mechanical neck pain.�Arch Phys Med Rehabil.�2008;89(1):69�74. doi: 10.1016/j.apmr.2007.08.126.�[PubMed]�[Cross Ref]
33.�Young IA, Cleland JA, Michener LA, Brown C. Reliability, construct validity, and responsiveness of the Neck Disability Index, patient-specific functional scale, and numeric pain rating scale in patients with cervical radiculopathy.�Am J Phys Med Rehabil.�2010;89(10):831�9. doi: 10.1097/PHM.0b013e3181ec98e6.�[PubMed]�[Cross Ref]
34.�Farrar JT, Young JP, Jr, LaMoreaux L, Werth JL, Poole RM. Clinical importance of changes in chronic pain intensity measured on an 11-point numerical pain rating scale.�Pain.�2001;94(2):149�58. doi: 10.1016/S0304-3959(01)00349-9.�[PubMed]�[Cross Ref]
35.�Vernon H. The Neck Disability Index: state-of-the-art, 1991-2008.�J Manipulative Physiol Ther.�2008;31(7):491�502. doi: 10.1016/j.jmpt.2008.08.006.�[PubMed]�[Cross Ref]
36.�MacDermid JC, Walton DM, Avery S, Blanchard A, Etruw E, McAlpine C, et al. Measurement properties of the Neck Disability Index: a systematic review.�J Orthop Sports Phys Ther.�2009;39(5):400�17. doi: 10.2519/jospt.2009.2930.�[PubMed]�[Cross Ref]
37.�Pietrobon R, Coeytaux RR, Carey TS, Richardson WJ, DeVellis RF. Standard scales for measurement of functional outcome for cervical pain or dysfunction: a systematic review.�Spine (Phila Pa 1976)�2002;27(5):515�22. doi: 10.1097/00007632-200203010-00012.�[PubMed]�[Cross Ref]
38.�Vernon H, Mior S. The Neck Disability Index: a study of reliability and validity.�J Manipulative Physiol Ther.�1991;14(7):409�15.�[PubMed]
39.�Vernon H. The psychometric properties of the Neck Disability Index.�Arch Phys Med Rehabil.�2008;89(7):1414�5. doi: 10.1016/j.apmr.2008.05.003.�[PubMed]�[Cross Ref]
40.�Cleland JA, Fritz JM, Whitman JM, Palmer JA. The reliability and construct validity of the Neck Disability Index and patient specific functional scale in patients with cervical radiculopathy.�Spine (Phila Pa 1976)�2006;31(5):598�602. doi: 10.1097/01.brs.0000201241.90914.22.�[PubMed]�[Cross Ref]
41.�Hoving JL, O’Leary EF, Niere KR, Green S, Buchbinder R. Validity of the neck disability index, Northwick Park neck pain questionnaire, and problem elicitation technique for measuring disability associated with whiplash-associated disorders.�Pain.�2003;102(3):273�81. doi: 10.1016/S0304-3959(02)00406-2.�[PubMed]�[Cross Ref]
42.�Miettinen T, Leino E, Airaksinen O, Lindgren KA. The possibility to use simple validated questionnaires to predict long-term health problems after whiplash injury.�Spine (Phila Pa 1976)�2004;29(3):E47�51. doi: 10.1097/01.BRS.0000106496.23202.60.�[PubMed]�[Cross Ref]
43.�McCarthy MJ, Grevitt MP, Silcocks P, Hobbs G. The reliability of the Vernon and Mior neck disability index, and its validity compared with the short form-36 health survey questionnaire.�Eur Spine J.�2007;16(12):2111�7. doi: 10.1007/s00586-007-0503-y.�[PMC free article]�[PubMed]�[Cross Ref]
44.�Pool JJ, Ostelo RW, Hoving JL, Bouter LM, de Vet HC. Minimal clinically important change of the Neck Disability Index and the Numerical Rating Scale for patients with neck pain.�Spine (Phila Pa 1976)�2007;32(26):3047�51. doi: 10.1097/BRS.0b013e31815cf75b.�[PubMed]�[Cross Ref]
45.�Young BA, Walker MJ, Strunce JB, Boyles RE, Whitman JM, Childs JD. Responsiveness of the Neck Disability Index in patients with mechanical neck disorders.�Spine J.�2009;9(10):802�8. doi: 10.1016/j.spinee.2009.06.002.�[PubMed]�[Cross Ref]
46.�Jaeschke R, Singer J, Guyatt GH. Measurement of health status. Ascertaining the minimal clinically important difference.�Control Clin Trials.�1989;10(4):407�15. doi: 10.1016/0197-2456(89)90005-6.[PubMed]�[Cross Ref]
47.�Schmitt J, Abbott JH. Global ratings of change do not accurately reflect functional change over time in clinical practice.�J Orthop Sports Phys Ther.�2015;45(2):106�11. doi: 10.2519/jospt.2015.5247.�[PubMed][Cross Ref]
48.�Carlesso L, Macdermid JC, Santaguida L. Standardization of adverse event terminology and reporting in orthopaedic physical therapy – applications to the cervical spine.�J Orthop Sports Phys Ther.�2010;40:455�63. doi: 10.2519/jospt.2010.3229.�[PubMed]�[Cross Ref]
49.�Carlesso LC, Gross AR, Santaguida PL, Burnie S, Voth S, Sadi J. Adverse events associated with the use of cervical manipulation and mobilization for the treatment of neck pain in adults: a systematic review.�Man Ther.�2010;15(5):434�44. doi: 10.1016/j.math.2010.02.006.�[PubMed]�[Cross Ref]
50.�Cleland JA, Glynn P, Whitman JM, Eberhart SL, MacDonald C, Childs JD. Short-term effects of thrust versus nonthrust mobilization/manipulation directed at the thoracic spine in patients with neck pain: a randomized clinical trial.�Phys Ther.�2007;87(4):431�40. doi: 10.2522/ptj.20060217.�[PubMed][Cross Ref]
51.�Gonzalez-Iglesias J, Fernandez-de-las-Penas C, Cleland JA, Alburquerque-Sendin F, Palomeque-del-Cerro L, Mendez-Sanchez R. Inclusion of thoracic spine thrust manipulation into an electro-therapy/thermal program for the management of patients with acute mechanical neck pain: a randomized clinical trial.�Man Ther.�2009;14(3):306�13. doi: 10.1016/j.math.2008.04.006.�[PubMed]�[Cross Ref]
52.�Gonzalez-Iglesias J, Fernandez-de-las-Penas C, Cleland JA, Gutierrez-Vega MR. Thoracic spine manipulation for the management of patients with neck pain: a randomized clinical trial.�J Orthop Sports Phys Ther.�2009;39(1):20�7. doi: 10.2519/jospt.2009.2914.�[PubMed]�[Cross Ref]
53.�Lau HM, Wing Chiu TT, Lam TH. The effectiveness of thoracic manipulation on patients with chronic mechanical neck pain – a randomized controlled trial.�Man Ther.�2011;16(2):141�7. doi: 10.1016/j.math.2010.08.003.�[PubMed]�[Cross Ref]
54.�Beffa R, Mathews R. Does the adjustment cavitate the targeted joint? An investigation into the location of cavitation sounds.�J Manipulative Physiol Ther.�2004;27(2):e2. doi: 10.1016/j.jmpt.2003.12.014.[PubMed]�[Cross Ref]
55.�Dunning J, Mourad F, Barbero M, Leoni D, Cescon C, Butts R. Bilateral and multiple cavitation sounds during upper cervical thrust manipulation.�BMC Musculoskelet Disord.�2013;14:24. doi: 10.1186/1471-2474-14-24.�[PMC free article]�[PubMed]�[Cross Ref]
56.�Reggars JW. The manipulative crack. Frequency analysis.�Australas Chiropr Osteopathy.�1996;5(2):39�44.�[PMC free article]�[PubMed]
57.�Ross JK, Bereznick DE, McGill SM. Determining cavitation location during lumbar and thoracic spinal manipulation: is spinal manipulation accurate and specific?�Spine (Phila Pa 1976)�2004;29(13):1452�7. doi: 10.1097/01.BRS.0000129024.95630.57.�[PubMed]�[Cross Ref]
58.�Evans DW, Lucas N. What is ‘manipulation’? A reappraisal.�Man Ther.�2010;15(3):286�91. doi: 10.1016/j.math.2009.12.009.�[PubMed]�[Cross Ref]
59.�Gross A, Miller J, D’Sylva J, Burnie SJ, Goldsmith CH, Graham N, et al. Manipulation or mobilisation for neck pain: a cochrane review.�Man Ther.�2010;15(4):315�33. doi: 10.1016/j.math.2010.04.002.[PubMed]�[Cross Ref]
60.�Moss P, Sluka K, Wright A. The initial effects of knee joint mobilization on osteoarthritic hyperalgesia.�Man Ther.�2007;12(2):109�18. doi: 10.1016/j.math.2006.02.009.�[PubMed]�[Cross Ref]
61.�Falla D, Bilenkij G, Jull G. Patients with chronic neck pain demonstrate altered patterns of muscle activation during performance of a functional upper limb task.�Spine (Phila Pa 1976)�2004;29(13):1436�40. doi: 10.1097/01.BRS.0000128759.02487.BF.�[PubMed]�[Cross Ref]
62.�Falla D, Jull G, Dall’Alba P, Rainoldi A, Merletti R. An electromyographic analysis of the deep cervical flexor muscles in performance of craniocervical flexion.�Phys Ther.�2003;83(10):899�906.�[PubMed]
63.�Jull G. Deep cervical flexor muscle dysfunction in whiplash.�Journal of Musculoskeletal Pain.�2000;8:143�54. doi: 10.1300/J094v08n01_12.�[Cross Ref]
64.�Rubin LH, Witkiewitz K, Andre JS, Reilly S. Methods for handling missing data in the behavioral neurosciences: Don’t throw the baby Rat out with the bath water.�J Undergrad Neurosci Educ.�2007;5(2):A71�7.�[PMC free article]�[PubMed]
65.�Jorritsma W, Dijkstra PU, de Vries GE, Geertzen JH, Reneman MF. Detecting relevant changes and responsiveness of neck pain and disability scale and Neck Disability Index.�Eur Spine J.�2012;21(12):2550�7. doi: 10.1007/s00586-012-2407-8.�[PMC free article]�[PubMed]�[Cross Ref]
66.�Stratford PW, Riddle DL, Binkley JM, Spadoni G, Westaway MD, Padfield B. Using the Neck Disability Index to make decisions concerning individual patients.�Physiother Can.�1999;51:107�12.
67.�Ernst E. Manipulation of the cervical spine: a systematic review of case reports of serious adverse events, 1995-2001.�Med J Aust.�2002;176(8):376�80.�[PubMed]
68.�Oppenheim JS, Spitzer DE, Segal DH. Nonvascular complications following spinal manipulation.�Spine J.�2005;5(6):660�6. doi: 10.1016/j.spinee.2005.08.006.�[PubMed]�[Cross Ref]
69.�Cassidy JD, Boyle E, Cote P, He Y, Hogg-Johnson S, Silver FL, et al. Risk of vertebrobasilar stroke and chiropractic care: results of a population-based case-control and case-crossover study.�Spine (Phila Pa 1976)�2008;33(4 Suppl):S176�83. doi: 10.1097/BRS.0b013e3181644600.�[PubMed]�[Cross Ref]
70.�Puentedura EJ, March J, Anders J, Perez A, Landers MR, Wallmann HW, et al. Safety of cervical spine manipulation: are adverse events preventable and are manipulations being performed appropriately? A review of 134 case reports.�J Man Manip Ther.�2012;20(2):66�74. doi: 10.1179/2042618611Y.0000000022.[PMC free article]�[PubMed]�[Cross Ref]
71.�Childs JD, Cleland JA, Elliott JM, Teyhen DS, Wainner RS, Whitman JM, et al. Neck pain: clinical practice guidelines linked to the international classification of functioning, disability, and health from the orthopedic section of the American Physical Therapy Association.�J Orthop Sports Phys Ther.�2008;38(9):A1�A34. doi: 10.2519/jospt.2008.0303.�[PubMed]�[Cross Ref]
72.�Pickar JG, Kang YM. Paraspinal muscle spindle responses to the duration of a spinal manipulation under force control.�J Manipulative Physiol Ther.�2006;29(1):22�31. doi: 10.1016/j.jmpt.2005.11.014.[PubMed]�[Cross Ref]
73.�Herzog W, Scheele D, Conway PJ. Electromyographic responses of back and limb muscles associated with spinal manipulative therapy.�Spine (Phila Pa 1976)�1999;24(2):146�52. doi: 10.1097/00007632-199901150-00012.�[PubMed]�[Cross Ref]
74.�Indahl A, Kaigle AM, Reikeras O, Holm SH. Interaction between the porcine lumbar intervertebral disc, zygapophysial joints, and paraspinal muscles.�Spine (Phila Pa 1976)�1997;22(24):2834�40. doi: 10.1097/00007632-199712150-00006.�[PubMed]�[Cross Ref]
75.�Bolton PS, Budgell BS. Spinal manipulation and spinal mobilization influence different axial sensory beds.�Med Hypotheses.�2006;66(2):258�62. doi: 10.1016/j.mehy.2005.08.054.�[PubMed]�[Cross Ref]
76.�Cassidy JD, Lopes AA, Yong-Hing K. The immediate effect of manipulation versus mobilization on pain and range of motion in the cervical spine: a randomized controlled trial.�J Manipulative Physiol Ther.�1992;15(9):570�5.�[PubMed]
77.�Martinez-Segura R, Fernandez-de-las-Penas C, Ruiz-Saez M, Lopez-Jimenez C, Rodriguez-Blanco C. Immediate effects on neck pain and active range of motion after a single cervical high-velocity low-amplitude manipulation in subjects presenting with mechanical neck pain: a randomized controlled trial.�J Manipulative Physiol Ther.�2006;29(7):511�7. doi: 10.1016/j.jmpt.2006.06.022.�[PubMed]�[Cross Ref]
78.�Bialosky JE, Bishop MD, Price DD, Robinson ME, George SZ. The mechanisms of manual therapy in the treatment of musculoskeletal pain: a comprehensive model.�Man Ther.�2009;14(5):531�8. doi: 10.1016/j.math.2008.09.001.�[PMC free article]�[PubMed]�[Cross Ref]
79.�Dunning J, Rushton A. The effects of cervical high-velocity low-amplitude thrust manipulation on resting electromyographic activity of the biceps brachii muscle.�Man Ther.�2009;14(5):508�13. doi: 10.1016/j.math.2008.09.003.�[PubMed]�[Cross Ref]
80.�Haavik-Taylor H, Murphy B. Cervical spine manipulation alters sensorimotor integration: a somatosensory evoked potential study.�Clin Neurophysiol.�2007;118(2):391�402. doi: 10.1016/j.clinph.2006.09.014.�[PubMed]�[Cross Ref]
81.�Millan M. Descending control of pain.�Prog Neurobiology.�2002;66:355�74. doi: 10.1016/S0301-0082(02)00009-6.�[PubMed]�[Cross Ref]
82.�Skyba D, Radhakrishnan R, Rohlwing J, Wright A, Sluka K. Joint manipulation reduces hyperalgesia by activation of monoamine receptors but not opioid or GABA receptors in the spinal cord.�Pain.�2003;106:159�68. doi: 10.1016/S0304-3959(03)00320-8.�[PMC free article]�[PubMed]�[Cross Ref]
83.�Zusman M. Forebrain-mediated sensitization of central pain pathways: “non-specific” pain and a new image for manual therapy.�Man Ther.�2002;7:80�8. doi: 10.1054/math.2002.0442.�[PubMed]�[Cross Ref]
84.�Bialosky JE, George SZ, Bishop MD. How spinal manipulative therapy works: why ask why?�J Orthop Sports Phys Ther.�2008;38(6):293�5. doi: 10.2519/jospt.2008.0118.�[PubMed]�[Cross Ref]
85.�Bishop MD, Beneciuk JM, George SZ. Immediate reduction in temporal sensory summation after thoracic spinal manipulation.�Spine J.�2011;11(5):440�6. doi: 10.1016/j.spinee.2011.03.001.[PMC free article]�[PubMed]�[Cross Ref]
86.�George SZ, Bishop MD, Bialosky JE, Zeppieri G, Jr, Robinson ME. Immediate effects of spinal manipulation on thermal pain sensitivity: an experimental study.�BMC Musculoskelet Disord.�2006;7:68. doi: 10.1186/1471-2474-7-68.�[PMC free article]�[PubMed]�[Cross Ref]
Truide Torres, office manager, first received chiropractic care with Dr. Alex Jimenez during her pregnancy for her lower back pain. Mrs. Torres experienced aggravating symptoms throughout the progression of her pregnancy, which led her to seek a natural treatment approach for her own health as well as that of her own baby. Once Truide Torres started chiropractic treatment with Dr. Alex Jimenez, she recovered her quality of life and was able to return to her original state of well-being. As an office manager, Truide Torres also receives regular chiropractic care for any lower back pain which may occur as a result of her job. Mrs. Truide expresses how important it is to continue her spinal maintenance and she highly recommends Dr. Alex Jimenez as the non-surgical choice for a variety of health issues.
Low back pain (LBP) is a frequent health issue involving the muscles, nerves, and bones of the spine. Pain may differ from a dull persistent pain to a sudden sharp sensation. Low back pain can be classified by length and severity (pain lasting less than 6 months), sub-chronic (6 to 12 months), or chronic (over 12 months). The status could be further categorized by the underlying cause as both bodily, non-mechanical, or referred pain. The symptoms of low back pain may generally improve in a couple weeks from the time they begin, however, some cases may require additional treatment. In the majority of episodes of lower back pain, a specific underlying cause isn’t identified or properly cared for, and healthcare professionals may attribute it to mechanical issues like joint or muscle strain.
Prenatal Yoga Exercises For Low Back Pain
Back Clinic News Extra: Migraine Pain Treatment With Chiropractic
Damaris Foreman suffered from migraines for about 23 years. After receiving traditional treatment for her migraine pain without much improvement, she was finally recommended to seek migraine pain treatment with Dr. Alex Jimenez, a chiropractor in El Paso, TX. Damaris greatly benefitted from chiropractic care and she experienced a tremendous sense of relief following her first spinal adjustment and manual manipulation. Damaris Foreman was able to confront many of her misconceptions and she learned very much about her migraine pain. Damaris describes Dr. Alex Jimenez’s migraine pain treatment as one of the best treatment she’s received and she highly recommends chiropractic care as the best non-surgical choice for improving and managing her migraines.
A migraine can be identified as a primary headache disorder characterized by recurrent headaches characterized from moderate to severe in intensity. Typically, the headaches affect one half of the head, are pulsating in nature, and can last from two to 72 hours. Associated symptoms may include nausea, vomiting, and sensitivity to light, sound, or smell. The pain may be aggravated by physical activity. Up to one-third of people who suffer from migraines experience migraine with aura: typically a brief period of visual disturbance that signals that the headache will soon happen. An aura can occur with little or no headache pain following it.
Please Recommend Us: If you have enjoyed this video and/or we have helped you in any way please feel free to recommend us. Thank You.
Diets: The statistics are sobering. The typical American diet far exceeds the daily recommended intake levels in calories from sugars and solid fats, sodium, refined grains, and saturated fat. It is also lacking in the recommended amounts of fruits, vegetables, dairy, whole grains, and oils. The result is obesity and experts project that by 2030, in the United States alone, half of all adults will be obese.
That�s when people start dieting � and that is what gets them into trouble.
Diet vs. Lifestyle Change
Bottom line, diets are temporary. There are some serious consequences that can come from dieting, especially fad or crash diets. The effects of these types of diets can also seriously impact your chiropractic care, hindering your progress.
Also, because diets are temporary, once you return to your regular eating habits the weight usually comes back.
A lifestyle change is a far better choice. It involves making smart, healthy eating choices � choices that you maintain for the rest of your life. This also impacts your chiropractic care by strengthening your body and keeping it healthy so that it is in an optimal state for healing and responds well to treatment.
Types Of Diets
There are all sorts of diets out there. Some are blatantly unhealthy but others are sneaky. They come with claims of being healthy, of being created or endorsed by doctors, or include tons of vitamin supplements but very limited food intake. It is important to be able to spot these destructive fad diets so you don�t get suckered into their hype.
Some of the most common types of fad diets include high protein, low or no carb, liquid, cabbage, grapefruit, broth or juice, and food combining. Some of these can cause serious health problems including vital organ damage. Others can cause vitamin deficiencies and dehydration. None of them can (or should) be maintained over a long period of time, much less the rest of your life.
The Dangers Of Diets
Unhealthy dieting can come with some pretty scary dangers. Because they typically omit key foods or food groups your body can become imbalanced. Some of the dangers of dieting include dehydration, fatigue, weakness, vitamin and mineral deficiency, headaches, nausea, diarrhea, constipation, mental fogginess, loss of muscle mass, organ damage, and even heart attack and stroke.
One popular diet restricts carbs, often cutting them out completely. This includes all whole grains (which have vital minerals and fiber) as well as many fruits and vegetables. The result is a diet that is mostly protein and fat.
While the dieter may lose some weight on this plan, it is at a great cost. The extremely high intake of protein which exceeds the levels that the body should have can cause liver and kidney failure. The omission of vital grains, fruits, and vegetables can lead to serious vitamin deficiencies while the increased fat intake can lead to heart attack and stroke.
If a diet eliminates any of the key foods (lean meats, whole grains, fruits, and vegetables), it advocates losing more than 2 or 3 pounds a week, or it restricts caloric intake to less than 1,200 calories a day it is potentially unhealthy and should only be done 1) under a doctor�s close supervision, and 2) on a very temporary basis.
Healthy Eating Is A Lifestyle
When you make the life changing commitment to adopt a healthy eating lifestyle you open yourself up to a world of better health, more energy, and better focus. Your body will heal faster and you will feel better.
A diet of fresh fruits and vegetables, lean meats, fresh fish, and whole grains, along with lots of water should become a way of life. It is far healthier than the temporary diets that are out there and more effective too.
If you or a loved one need additional dietary guidance, give us a call. Our Doctor of Chiropractic is here to help!
Headache pain is one of the most prevalent reasons for doctor office visits. The majority of people experience them at some point in their life and they can affect anyone, regardless of age, race and gender. The International Headache Society, or IHS, categorizes headaches as primary, when they are not caused by another injury and/or condition, or secondary, when there is an underlying cause behind them. From migraines to cluster headaches and tension headaches, people who suffer from constant head pain may find it difficult to participate in their everyday activities. Many healthcare professionals treat headache pain, however, chiropractic care has become a popular alternative treatment option for a variety of health issues. The purpose of the following article is to demonstrate evidence-based guidelines for the chiropractic treatment of adults with headache.
Evidence-Based Guidelines for the Chiropractic Treatment of Adults with Headache
Abstract
Objective: The purpose of this manuscript is to provide evidence-informed practice recommendations for the chiropractic treatment of headache in adults.
Methods: Systematic literature searches of controlled clinical trials published through August 2009 relevant to chiropractic practice were conducted using the databases MEDLINE; EMBASE; Allied and Complementary Medicine; the Cumulative Index to Nursing and Allied Health Literature; Manual, Alternative, and Natural Therapy Index System; Alt HealthWatch; Index to Chiropractic Literature; and the Cochrane Library. The number, quality, and consistency of findings were considered to assign an overall strength of evidence (strong, moderate, limited, or conflicting) and to formulate practice recommendations.
Results: Twenty-one articles met inclusion criteria and were used to develop recommendations. Evidence did not exceed a moderate level. For migraine, spinal manipulation and multimodal multidisciplinary interventions including massage are recommended for management of patients with episodic or chronic migraine. For tension-type headache, spinal manipulation cannot be recommended for the management of episodic tension-type headache. A recommendation cannot be made for or against the use of spinal manipulation for patients with chronic tension-type headache. Low-load craniocervical mobilization may be beneficial for longer term management of patients with episodic or chronic tension-type headaches. For cervicogenic headache, spinal manipulation is recommended. Joint mobilization or deep neck flexor exercises may improve symptoms. There is no consistently additive benefit of combining joint mobilization and deep neck flexor exercises for patients with cervicogenic headache. Adverse events were not addressed in most clinical trials; and if they were, there were none or they were minor.
Conclusions: Evidence suggests that chiropractic care, including spinal manipulation, improves migraine
and cervicogenic headaches. The type, frequency, dosage, and duration of treatment(s) should be based on guideline recommendations, clinical experience, and findings. Evidence for the use of spinal manipulation as an isolated intervention for patients with tension-type headache remains equivocal. (J Manipulative Physiol Ther 2011;34:274-289)
Headache, or head pain, including migraine and other types of headaches, is one of the most common types of pain reported among the general population. These may occur on one or both sides of the head, can be isolated to a specific location or they may radiate across the head from one point. While headache symptoms can vary depending on the type of head pain as well as due to the source of the health issue, headaches are considered to be a general complaint regardless of their severity and form. Headache, or head pain, may occur as a result of spinal misalignment, or subluxation, along the length of the spine. Through the use of spinal adjustments and manual manipulations, chiropractic care can safely and effectively realign the spine, reducing stress and pressure on the surrounding structures of the spine, to ultimately help improve migraine headache pain symptoms as well as overall health and wellness.
Headache is a common experience in adults. Recurring headaches negatively impact family life, social activity, and work capacity.[1,2] Worldwide, according to the World Health Organization, migraine alone is 19th among all causes of years lived with disability. Headache is third among reasons for seeking chiropractic care in North America.[3]
Accurate diagnosis is key to management and treatment, and a wide range of headache types are described in the International Classification of Headache Disorders 2 (International Headache Society [IHS]).[4] The categories are intended for clinical as well as research use. The most common headaches, tension-type and migraine, are considered primary headaches that are episodic or chronic in nature. Episodic migraine or tension-type headaches occur fewer than 15 days per month, whereas chronic headaches occur more than 15 days per month for at least 3 (migraine) or 6 months (tension-type headache).[4] Secondary headaches are attributed to underlying clinical problems in the head or neck that may also be episodic or chronic. Cervicogenic headaches are secondary headaches commonly treated by chiropractors and involve pain referred from a source in the neck and perceived in 1 or more regions of the head. The IHS recognizes cervicogenic headache as a distinct disorder,[4] and evidence that headache can be attributed to a neck disorder or lesion based on history and clinical features (history of neck trauma, mechanical exacerbation of pain, reduced cervical range of motion, and focal neck tenderness, excluding myofascial pain alone) is relevant to diagnosis but is not without controversy in the literature.[4,5] When myofascial pain alone is the cause, the patient should be managed as having tension-type headaches.[4]
Treatment modalities typically used by chiropractors to care for patients with headaches include spinal manipulation, mobilization, device-assisted spinal manipulation, education about modifiable lifestyle factors, physical therapy modalities, heat/ice, massage, advanced soft tissue therapies such as trigger point therapy, and strengthening and stretching exercises. There is a growing expectation for health professions, including chiropractic, to adopt and use research-based knowledge, taking sufficient account of the quality of available research evidence to inform clinical practice. As a result, the purpose of the Canadian Chiropractic Association (CCA) and the Canadian Federation of Chiropractic Regulatory and Educational Accrediting Boards (Federation) Clinical Practice Guidelines Project is to develop guidelines for practice based on available evidence. The purpose of this manuscript is to provide evidence-informed practice recommendations for the chiropractic treatment of headache in adults.
Methods
The Guidelines Development Committee (GDC) planned for and adapted systematic processes for literature�searching, screening, review, analysis, and interpretation. Methods are consistent with criteria proposed by the �Appraisal of Guidelines Research and Evaluation� collaboration (http://www.agreecollaboration.org). This guideline is a supportive tool for practitioners. It is not intended as a standard of care. The guideline links available published evidence to clinical practice and is only 1 component of an evidence-informed approach to patient care.
Data Sources and Searches
Systematic search and evaluation of the treatment literature were conducted using methods recommended by The Cochrane Collaboration Back Review Group[6] and Oxman and Guyatt.[7] The search strategy was developed in MEDLINE by exploring MeSH terms related to chiropractic and specific interventions and later modified for other databases. The literature search strategy was intentionally broad. Chiropractic treatment was defined as including the most common therapies used by practitioners and was not restricted to treatment modalities delivered only by chiropractors. A wide net was cast to include treatments that may be administered in chiropractic care as well as those that could also be delivered in the context of care by other health care professionals in a specific research study (Appendix A). Spinal manipulation was defined as a high-velocity low-amplitude thrust delivered to the spine. Excluded therapies included invasive analgesic or neurostimulation procedures, pharmacotherapy, injections of botulinum toxin, cognitive or behavioral therapies, and acupuncture.
Literature searches were completed from April to May 2006, updated in 2007 (phase 1), and updated again in August 2009 (phase 2). Databases searched included MEDLINE; EMBASE; Allied and Complementary Medicine; the Cumulative Index to Nursing and Allied Health Literature; Manual, Alternative, and Natural Therapy Index System; Alt HealthWatch; Index to Chiropractic Literature; and the Cochrane Library (Appendix A). Searches included articles published in English or with English abstracts. The search strategy was limited to adults (?18 years); although research studies with subject inclusion criteria encompassing a broad range of ages, such as adults and adolescents, were retrieved using the search strategy. Reference lists provided in systematic reviews (SRs) were also reviewed by the GDC to minimize relevant articles from being missed.
Evidence Selection Criteria
Search results were screened electronically, and multi-stage screening was applied (Appendix B): stage 1A (title), 1B (abstract); stage 2A (full text), 2B (full text-methodology, relevance); and stage 3 (full text-final GDC screening as clinical content experts). Duplicate citations were removed, and relevant articles were retrieved as electronic�and/or hard copies for detailed analysis. Different assessors, using the same criteria, completed the literature screens in 2007 and 2009 due to the time span between searches.
Only controlled clinical trials (CCTs); randomized, controlled trials (RCTs); and systematic reviews (SRs) were selected as the evidence base for this guideline consistent with current standards for interpreting clinical findings. The GDC did not rate observational studies, case series, or case reports because of their uncontrolled nature and probable low methodological quality vs CCTs. This approach is consistent with updated methods for SRs published by the Cochrane Back Review Group.[8] If multiple SRs were published by the same authors on a given topic, only the most recent publication was counted and used for evidence synthesis. Systematic reviews of SRs were also excluded to avoid double counting of research results.
Literature Assessment and Interpretation
Quality ratings of CCTs or RCTs included 11 criteria answered by �yes (score 1)� or �no (score 0)/do not know (score 0)� (Table 1). The GDC documented 2 additional criteria of interest: (1) researchers’ use of IHS diagnostic criteria for subject enrollment and (2) evaluation of side effects (Table 1, columns L and M). Use of IHS criteria[4] was relevant to this Clinical Practice Guideline (CPG) process to confirm diagnostic specificity within and across research studies. Studies were excluded if IHS diagnostic criteria were not applied by the researchers for subject inclusion into a study (Appendix C); and if before 2004, before cervicogenic headache was included in the IHS classification, the diagnostic criteria of the Cervicogenic Headache International Study Group[9] were not used. Side effects were reviewed as a proxy for potential risk(s) with treatment. No weighting factor(s) was applied to individual criteria, and possible quality ratings ranged from 0 to 11. Both blinding of subjects and care providers were rated in the research articles by the GDC, since these items are listed in the quality rating tool.[6] The GDC’s methods did not adapt or alter the rating tool. The rationale for this approach was that certain treatment modalities (eg, transcutaneous electrical nerve stimulation [TENS], ultrasound) and trial designs may achieve patient and/or practitioner blinding.[10] The GDC did not limit the evaluation of these benchmarks of quality if indeed they were reported in clinical studies for the treatment of headache disorders. The GDC also considered it outside their scope of expertise to modify, without validation, a widely used rating tool used to assess the clinical literature.[6] New research tools for the analysis and rating of the manual therapy literature, however, are urgently needed and are noted as an area for future research in the discussion section below.
Literature assessors were project contributors separate from the GDC and were unblinded as to study authors, institutions, and source journals. Three members of the GDC (MD, RR, and LS) corroborated quality rating methods by completing quality assessments on a random subset of 10 articles.[11-20] A high level of agreement was confirmed across quality ratings. Complete agreement on all items was achieved for 5 studies: in 10 of 11 items for 4 studies and 8 of 11 items for the 1 remaining study. All discrepancies were easily resolved through discussion and�consensus by the GDC (Table 1). Due to heterogeneity of research methods across trials, no meta-analysis or statistical pooling of trial results was done. Trials scoring more than half of the total possible rating (ie, ?6) were considered high quality. Trials scoring 0 through 5 were considered low quality. Studies with major methodological flaws or investigating specialized treatment techniques were excluded (eg, treatment not considered relevant by the GDC for the chiropractic care of patients with headache; Appendix Table 3).
Quality rating of SRs included 9 criteria answered by yes (score 1) or no (score 0)/do not know (score 0) and a qualitative response for item J �no flaws,� �minor flaws,� or �major flaws� (Table 2). Possible ratings ranged from 0 to 9. The determination of overall scientific quality of SRs with major flaws, minor flaws, or no flaws, as listed in column J (Table 2), was based on the literature raters’ answers to the previous 9 items. The following parameters were used to derive the overall scientific quality of a SR: if the no/do not know response was used, an SR was likely to have minor flaws at best. However, if �No� was used on items B, D, F, or H, the review was likely to have major flaws.[21] Systematic reviews scoring more than half of the total possible rating (ie, ?5) with no or minor flaws were rated as high quality. Systematic reviews scoring 4 or less and/or with major flaws were excluded.
Reviews were defined as systematic if they included an explicit and repeatable method for searching and analyzing the literature and if inclusion and exclusion criteria for studies were described. Methods, inclusion criteria, methods for rating study quality, characteristics of included studies, methods for synthesizing data, and results were evaluated. Raters achieved complete agreement for all rating items for 7 SRs[22-28] and for 7 of 9 items for the 2�additional SRs.[29,30] The discrepancies were deemed minor and easily resolved through GDC review and consensus (Table 2).
Developing Recommendations for Practice
The GDC interpreted the evidence relevant to chiropractic treatment of headache patients. A detailed summary of the relevant articles will be posted to the CCA/Federation Clinical Practice Guidelines Project web site.
Randomized, controlled trials and their findings were appraised to inform treatment recommendations. To assign an overall strength of evidence (strong, moderate, limited, conflicting, or no evidence),[6] the GDC considered the number, quality, and consistency of research results (Table 3). Strong evidence was considered only when multiple high-quality RCTs corroborated the findings of other researchers in other settings. Only high-quality SRs were appraised in relation to the body of evidence and to inform treatment recommendations. The GDC considered treatment modalities to have proven benefit(s) when supported by a minimum of moderate level of evidence.
Recommendations for practice were developed in collaborative working group meetings.
Results
Literature
From the literature searches, initially 6206 citations were identified. Twenty-one articles met final criteria for inclusion and were considered in developing practice recommendations (16 CCTs/RCTs[11-20,31-36] and 5 SRs[24-27,29]). Quality ratings of the included articles are provided in Tables 1 and 2. Appendix Table 3 lists articles excluded in final screening by the GDC and reason(s) for their exclusion. Absence of subject and practitioner blinding and unsatisfactory descriptions of cointerventions were commonly identified methodological limitations of the controlled trials. Headache types evaluated in these trials included migraine (Table 4), tension-type headache (Table 5), and cervicogenic headache (Table 6). Consequently, only these headache types are represented by the evidence and practice recommendations in this CPG. Evidence summaries of SRs are provided in Table 7.
Practice Recommendations: Treatment of Migraine
Spinal manipulation is recommended for the management of patients with episodic or chronic migraine with or without aura. This recommendation is based on studies that used a treatment frequency 1 to 2 times per week for 8 weeks (evidence level, moderate). One high-quality RCT,[20] 1 low-quality RCT,[17] and 1 high- quality SR[24] support the use of spinal manipulation for patients with episodic or chronic migraine (Tables 4 and 7).
Weekly massage therapy is recommended for reducing episodic migraine frequency and for improving affective symptoms potentially linked to headache pain (evidence level, moderate). One high-quality RCT[16] supports this practice recommendation (Table 4). Researchers used a 45-minute massage with focus on neuromuscular and trigger point framework of the back, shoulder, neck, and head.
Multimodal multidisciplinary care (exercise, relaxation, stress and nutritional counseling, massage therapy) is recommended for the management of patients with episodic or chronic migraine. Refer as appropriate (evidence level, moderate). One high-quality RCT[32] supports the effectiveness of multi-modal multidisciplinary intervention for migraine (Table 4). The intervention prioritizes a general management approach consisting of exercise, education, lifestyle change, and self-management.
There are insufficient clinical data to recommend for or against the use of exercise alone or exercise combined with multimodal physical therapies for the management of patients with episodic or chronic migraine (aerobic exercise, cervical range of motion [cROM], or whole body stretching). Three low-quality CCTs[13,33,34] contribute to this conclusion (Table 4).
Practice Recommendations: Tension-Type Headache
Low-load craniocervical mobilization (eg, Thera-Band, Resistive Exercise Systems; Hygenic Corporation, Akron, OH) is recommended for longer term (eg, 6 months) management of patients with episodic or�chronic tension-type headaches (evidence level, moderate). One high-quality RCT[36] showed that low-load mobilization significantly reduced symptoms of tension-type headaches for patients during the longer term (Table 5).
Spinal manipulation cannot be recommended for the management of patients with episodic tension-type headache (evidence level, moderate). There is moderate-level evidence that spinal manipulation after premanipulative soft tissue therapy provides no additional benefit for patients with tension-type headaches. One high-quality RCT[12] (Table 5) and observations reported in 4 SRs[24-27] (Table 7) suggest no benefit of spinal manipulation for patients with episodic tension-type headaches.
A recommendation cannot be made for or against the use of spinal manipulation (2 times per week for 6 weeks) for patients with chronic tension-type headache. Authors of 1 RCT[11] rated as high quality by the quality assessment tool[6] (Table 1), and summaries of this study in 2 SRs[24,26] suggest that spinal manipulation may be effective for chronic tension-type headache. However, the GDC considers the RCT[11] difficult to interpret and inconclusive (Table 5). The trial is inadequately controlled with imbalances in the number of subject-clinician encounters between study groups (eg, 12 visits for subjects in the soft tissue therapy plus spinal manipulation group vs 2 visits for subjects in the amitriptyline group). There is no way of knowing whether a comparable level of personal attention for subjects in the amitriptyline group may have impacted the study outcomes. These considerations and interpretations from 2 other SRs[25,27]contribute to this conclusion (Table 7).
There is insufficient evidence to recommend for or against the use of manual traction, connective tissue manipulation, Cyriax’s mobilization, or exercise/ physical training for patients with episodic or chronic tension-type headache. Three low-quality inconclusive studies[19,31,35] (Table 5), 1 low-quality negative RCT,[14] and 1 SR[25] contribute to this conclusion (Table 7).
Practice Recommendations: Cervicogenic Headache
Spinal manipulation is recommended for the management of patients with cervicogenic headache. This recommendation is based on 1 study that used a treatment frequency of 2 times per week for 3 weeks (evidence level, moderate). In a high-quality RCT, Nilsson et al[18] (Table 6) showed a significantly positive effect of high-velocity, low-amplitude spinal manipulation for patients with cervicogenic headache. Evidence synthesis from 2 SRs[24,29] (Table 7) supports this practice recommendation.
Joint mobilization is recommended for the management of patients with cervicogenic headache (evidence level, moderate). Jull et al[15] examined the effects of Maitland joint mobilization 8 to 12 treatments for 6 weeks in a high-quality RCT (Table 6). Mobilization followed typical clinical practice, in which the choice of low-velocity and high-velocity techniques was based on initial and progressive assessments of patients’ cervical joint dysfunction. Beneficial effects were reported for headache frequency, intensity, as well as neck pain and disability. Evidence synthesis from 2 SRs[24,29] (Table 7) supports this practice recommendation.
Deep neck flexor exercises are recommended for the management of patients with cervicogenic headache (evidence level, moderate). This recommendation is based on a study of 2 times daily for 6 weeks. There is no consistently additive benefit of combining deep neck flexor exercises and joint mobilization for cervicogenic headache. One high-quality RCT[15] (Table 6) and observations provided in 2 SRs[24,29] (Table 7) support this practice recommendation.
Safety
Practitioners select treatment modalities in conjunction with all available clinical information for a given patient. Of the 16 CCTs/RCTS[11-20,31-36] included in the body of evidence for this CPG, only 6 studies[11,12,15,20,32,36] adequately assessed or discussed patient side effects or safety parameters (Table 1, column M). Overall, reported risks were low. Three of the trials reported safety information for spinal manipulation.[11,12,20] Boline et al[11] reported that 4.3% of subjects experienced neck stiffness after initial spinal manipulation that disappeared for all cases after the first 2 weeks of treatment. Soreness or increase in headaches after spinal manipulation (n = 2) were reasons for treatment discontinuation cited by Tuchin et al.[20] No side effects were experienced by any subjects studied by Bove et al[12] using spinal manipulation for the treatment of episodic tension-type headache. Treatment trials to evaluate efficacy outcomes may not enroll adequate numbers of subjects to assess the incidence of rare adverse events. Other research methods are required to�develop a full understanding of the balance between benefits and risks.
Discussion
Spinal manipulation and other manual therapies commonly used in chiropractic have been studied in several CCTs that are heterogeneous in subject enrollment, design, and overall quality. Patient and headache types systematically represented in the evidence base are migraine, tension-type headaches, and cervicogenic headache. The primary health status outcomes reported are typically headache frequency, intensity, duration, and quality-of-life measures. The evidence is no greater than a moderate level at this time.
The evidence supports the use of spinal manipulation for the chiropractic management of patients with migraine or cervicogenic headaches but not tension-type headaches. For migraine, multidisciplinary care using weekly 45-minute massage therapy and multimodal care (exercise, relaxation, and stress and nutritional counseling) may also be effective. Alternatively, joint mobilization or deep neck flexor exercises are recommended for improving symptoms of cervicogenic headache. There appears to be no consistently additive benefit of combining joint mobilization and deep neck flexor exercises for patients with cervicogenic headache. Moderate evidence support the use of low-load craniocervical mobilization for longer term management of tension-type headaches.
Limitations
Shortcomings for this guideline include the quantity and quality of supporting evidence found during the searches. No recent adequately controlled high-quality research studies with reproducible clinical findings have been published for the chiropractic care of headache patients. Studies are needed to further our understanding of specific manual therapies in isolation or in well-controlled combinations for the treatment of migraine, tension-type headache, cervicogenic headache, or other headache types presenting to clinicians (eg, cluster, posttraumatic head- ache). Another shortcoming of this literature synthesis is the reliance on published research studies with small sample sizes (Tables 4-6), short-term treatment paradigms, and follow-up periods. Well-designed clinical trials with sufficient numbers of subjects, longer term treatments, and follow-up periods need to be funded to advance chiropractic care, and spinal manipulation in particular, for the management of patients with headache disorders. As with any literature review and clinical practice guideline, foundational information and published literature are evolving. Studies that may have informed this work may have been published after the conclusion of this study.[37-39]
Considerations for Future Research
The GDC consensus is that there is a need for further chiropractic studies with patients with headache disorders.
More high-quality clinical research is needed. Future research requires study designs using active comparators and nontreatment and/or placebo group(s) to enhance the evidence base for patient care. Patient blinding to physical interventions to manage expectancy results is needed and has been explored by researchers in chiropractic for other pain conditions.[10] The lack of systematically reported studies presents a practical challenge for generating evidence-based treatment recommendations. All future studies should be structured using systematic validated methods (eg, Consolidated Standards of Reporting Trials [CONSORT] and Transparent Reporting of Evaluations with Non-randomized Designs [TREND]).
Systematic reporting of safety data is needed in chiropractic research. All clinical trials must collect and report on potential side effects or harms even if none are observed.
Develop novel quantitative tools for evaluating manual therapy research. Blinding serves to control expectancy effects and nonspecific effects of subject-provider interactions across study groups. It is typically not possible to blind subjects and providers in efficacy studies of manual therapies. Despite inherent limitations, both blinding of subjects and care providers were rated in the research articles by the GDC, since these items are included in high-quality rating instruments.[6] Advanced research tools for analyzing and subsequent rating of the manual therapy literature are urgently needed.
To advance research on functional outcomes in the chiropractic care of headache. This guideline identified that headache studies use a variable range of measures in evaluating the effect of treatment on health outcomes. Headache frequency, intensity, and duration are the most consistently used outcomes (Tables 4-6). Serious efforts are needed to include validated patient-centered outcome measures in chiropractic research that are congruent with improvements in daily living and resumption of meaningful routines.
Cost-effectiveness. No research studies were retrieved on cost-effectiveness of spinal manipulation for the treatment of headache disorders. Future clinical trials of spinal manipulation should evaluate cost-effectiveness.
Other research methods are required to develop a full understanding of the balance between benefits and risks. This CPG does not provide a review of all chiropractic treatments. Any omissions reflect gaps in the clinical literature. The type, frequency, dosage, and duration of treatment(s) should be based on guideline recommendations, clinical experience, and knowledge of the patient until higher levels of evidence are available.
Conclusions
There is a baseline of evidence to support chiropractic care, including spinal manipulation, for the management of migraine and cervicogenic headaches. The type, frequency, dosage, and duration of treatment(s) should be based on guideline recommendations, clinical experience, and knowledge of the patient. Evidence for the use of spinal manipulation as an isolated intervention for patients with tension-type headache remains equivocal. More research is needed.
Practice guidelines link the best available evidence to good clinical practice and are only 1 component of an evidence-informed approach to providing good care. This guideline is intended to be a resource for the delivery of chiropractic care for patients with headache. It is a �living document� and subject to revision with the emergence of new data. Furthermore, it is not a substitute for a practitioner’s clinical experience and expertise. This document is not intended to serve as a standard of care. Rather, the guideline attests to the commitment of the profession to advance evidence-based practice through engaging a knowledge exchange and transfer process to support the movement of research knowledge into practice.
Practical Applications
This guideline is a resource for the delivery of chiropractic care for patients with headache.
Spinal manipulation is recommended for the management of patients with migraine or cervicogenic headaches.
Multimodal multidisciplinary interventions including massage may benefit patients with migraine.
Joint mobilization or deep neck flexor exercises may improve symptoms of cervicogenic headache.
Low-load craniocervical mobilization may improve tension-type headaches.
Acknowledgements
The authors thank the following for input on this guideline: Ron Brady, DC; Grayden Bridge, DC; H James Duncan; Wanda Lee MacPhee, DC; Keith Thomson, DC, ND; Dean Wright, DC; and Peter Waite (Members of the Clinical Practice Guidelines Task Force). The authors thank the following for assistance with the Phase I literature search assessment: Simon Dagenais, DC, PhD; and Thor Eglinton, MSc, RN. The authors thank the following for assistance with the Phase II additional literature search and evidence rating: Seema Bhatt, PhD; Mary-Doug Wright, MLS. The�authors thank Karin Sorra, PhD for assistance with literature searches, evidence rating, and editorial support.
Funding Sources and Potential Conflicts of Interest
Funding was provided by the CCA, Canadian Chiropractic Protective Association, and provincial chiropractic contributions from all provinces except British Columbia. This work was sponsored by The CCA and the Federation. No conflicts of interest were reported for this study.
In conclusion, headache is one of the most common reasons people seek medical attention. Although many healthcare professionals can treat headaches, chiropractic care is a well-known alternative treatment option frequently used to treat a variety of health issues, including several types of headaches. According to the article above, evidence suggests that chiropractic care, including spinal adjustments and manual manipulations, can improve headache and migraine. Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Back Pain
According to statistics, approximately 80% of people will experience symptoms of back pain at least once throughout their lifetimes. Back pain is a common complaint which can result due to a variety of injuries and/or conditions. Often times, the natural degeneration of the spine with age can cause back pain. Herniated discs occur when the soft, gel-like center of an intervertebral disc pushes through a tear in its surrounding, outer ring of cartilage, compressing and irritating the nerve roots. Disc herniations most commonly occur along the lower back, or lumbar spine, but they may also occur along the cervical spine, or neck. The impingement of the nerves found in the low back due to injury and/or an aggravated condition can lead to symptoms of sciatica.
1. Robbins MS, Lipton RB. The epidemiology of primary headache disorders. Semin Neurol 2010;30:107-19.
2. Stovner LJ, Andree C. Prevalence of headache in Europe: a review for the Eurolight project. J Headache Pain Aug 2010; 11:289-99.
3. Coulter ID, Hurwitz EL, Adams AH, Genovese BJ, Hays R, Shekelle PG. Patients using chiropractors in North America: who are they, and why are they in chiropractic care? Spine (Phila Pa 1976) 2002;27(3):291-6 [discussion 297-98].
4. International Headache Society. The International Classifi- cation of Headache Disorders, 2nd ed. Cephalalgia 2004;24: 9-160 (Suppl 1).
5. Bogduk N, Govind J. Cervicogenic headache: an assessment of the evidence on clinical diagnosis, invasive tests, and treatment. Lancet Neurol 2009;8:959-68.
6. van Tulder M, Furlan A, Bombardier C, Bouter L. Updated method guidelines for systematic reviews in the cochrane collaboration back review group. Spine (Phila Pa 1976) 2003; 28:1290-9.
7. Oxman AD, Guyatt GH. Validation of an index of the quality of review articles. J Clin Epidemiol 1991;44:1271-8.
8. Furlan AD, Pennick V, Bombardier C, van Tulder M. 2009 updated method guidelines for systematic reviews in the Cochrane Back Review Group. Spine (Phila Pa 1976) 2009; 34:1929-41.
9. Sjaastad O, Fredriksen TA, Pfaffenrath V. Cervicogenic headache: diagnostic criteria. The Cervicogenic Headache International Study Group. Headache 1998;38:442-5.
10. Hawk C, Long CR, Reiter R, Davis CS, Cambron JA, Evans R. Issues in planning a placebo-controlled trial of manual methods: results of a pilot study. J Altern Complement Med 2002;8:21-32.
11. Boline PD, Kassak K, Bronfort G, Nelson C, Anderson AV. Spinal manipulation vs. amitriptyline for the treatment of chronic tension-type headaches: a randomized clinical trial. J Manipulative Physiol Ther 1995;18:148-54.
12. Bove G, Nilsson N. Spinal manipulation in the treatment of episodic tension-type headache: a randomized controlled trial. JAMA 1998;280:1576-9.
13. Dittrich SM, Gunther V, Franz G, Burtscher M, Holzner B, Kopp M. Aerobic exercise with relaxation: influence on pain and psychological well-being in female migraine patients. Clin J Sport Med 2008;18:363-5.
14. Donkin RD, Parkin-Smith GF, Gomes N. Possible effect of chiropractic manipulation and combined manual traction and manipulation on tension-type headache: a pilot study. J Neuromusculoskeletal Systen 2002;10:89-97.
15. Jull G, Trott P, Potter H, et al. A randomized controlled trial of exercise and manipulative therapy for cervicogenic headache. Spine (Phila Pa 1976) 2002;27:1835-43 [discussion 1843].
16. Lawler SP, Cameron LD. A randomized, controlled trial of massage therapy as a treatment for migraine. Ann Behav Med 2006;32:50-9.
17. Nelson CF, Bronfort G, Evans R, Boline P, Goldsmith C, Anderson AV. The efficacy of spinal manipulation, amitrip- tyline and the combination of both therapies for the prophylaxis of migraine headache. J Manipulative Physiol Ther 1998;21:511-9.
18. Nilsson N, Christensen HW, Hartvigsen J. The effect of spinal manipulation in the treatment of cervicogenic headache. J Manipulative Physiol Ther 1997;20:326-30.
19. Soderberg E, Carlsson J, Stener-Victorin E. Chronic tension- type headache treated with acupuncture, physical training and relaxation training. Between-group differences. Cephalalgia 2006;26:1320-9.
20. Tuchin PJ, Pollard H, Bonello R. A randomized controlled trial of chiropractic spinal manipulative therapy for migraine. J Manipulative Physiol Ther 2000;23:91-5.
21. Chou R, Huffman LH. Nonpharmacologic therapies for acute and chronic low back pain: a review of the evidence for an American Pain Society/American College of Physicians clinical practice guideline. Ann Intern Med 2007;147: 492-504.
22. Astin JA, Ernst E. The effectiveness of spinal manipulation for the treatment of headache disorders: a systematic review of randomized clinical trials. Cephalalgia 2002;22:617-23.
23. Biondi DM. Physical treatments for headache: a structured review. Headache 2005;45:738-46.
24. Bronfort G, Nilsson N, Haas M, et al. Non-invasive physical treatments for chronic/recurrent headache. Cochrane Database Syst Rev 2004:CD001878.
25. Fernandez-de-Las-Penas C, Alonso-Blanco C, Cuadrado ML, Miangolarra JC, Barriga FJ, Pareja JA. Are manual therapies effective in reducing pain from tension-type headache?: a systematic review. Clin J Pain 2006;22:278-85.
26. Hurwitz EL, Aker PD, Adams AH, Meeker WC, Shekelle PG. Manipulation and mobilization of the cervical spine. A systematic review of the literature. Spine (Phila Pa 1976) 1996;21:1746-59.
27. Lenssinck ML, Damen L, Verhagen AP, Berger MY, Passchier J, Koes BW. The effectiveness of physiotherapy and manipulation in patients with tension-type headache: a systematic review. Pain 2004;112:381-8.
28. Vernon H, McDermaid CS, Hagino C. Systematic review of randomized clinical trials of complementary/alternative ther- apies in the treatment of tension-type and cervicogenic headache. Complement Ther Med 1999;7:142-55.
29. Fernandez-de-Las-Penas C, Alonso-Blanco C, Cuadrado ML, Pareja JA. Spinal manipulative therapy in the management of cervicogenic headache. Headache 2005;45:1260-3.
30. Maltby JK, Harrison DD, Harrison D, Betz J, Ferrantelli JR, Clum GW. Frequency and duration of chiropractic care for headaches, neck and upper back pain. J Vertebr Subluxat Res 2008;2008:1-12.
31. Demirturk F, Akarcali I, Akbayrak T, Cita I, Inan L. Results of two different manual therapy techniques in chronic tension- type headache. Pain Clin 2002;14:121-8.
32. Lemstra M, Stewart B, Olszynski WP. Effectiveness of multidisciplinary intervention in the treatment of migraine: a randomized clinical trial. Headache 2002;42:845-54.
33. Marcus DA, Scharff L, Mercer S, Turk DC. Nonpharmaco- logical treatment for migraine: incremental utility of physical therapy with relaxation and thermal biofeedback. Cephalalgia 1998;18:266-72.
34. Narin SO, Pinar L, Erbas D, Ozturk V, Idiman F. The effects of exercise and exercise-related changes in blood nitric oxide level on migraine headache. Clin Rehabil 2003;17:624-30.
35. Torelli P, Jensen R, Olesen J. Physiotherapy for tension-type headache: a controlled study. Cephalalgia 2004;24:29-36.
36. van Ettekoven H, Lucas C. Efficacy of physiotherapy
including a craniocervical training programme for tension- type headache; a randomized clinical trial. Cephalalgia 2006; 26:983-91.
37. Vavrek D, Haas M, Peterson D. Physical examination and self-reported pain outcomes from a randomized trial on chronic cervicogenic headache. J Manipulative Physiol Ther 2010;33:338-48.
38. Haas M, Aickin M, Vavrek D. A preliminary path analysis of expectancy and patient-provider encounter in an open-label randomized controlled trial of spinal manipulation for cervicogenic headache. J Manipulative Physiol Ther 2010; 33:5-13.
39. Toro-Velasco C, Arroyo-Morales M, Ferna?ndez-de-Las- Pen?as C, Cleland JA, Barrero-Herna?ndez FJ. Short-term effects of manual therapy on heart rate variability, mood state, and pressure pain sensitivity in patients with chronic tension-type headache: a pilot study. J Manipulative Physiol Ther 2009;32:527-35.
40. Allais G, De Lorenzo C, Quirico PE, et al. Non-pharmaco- logical approaches to chronic headaches: transcutaneous electrical nerve stimulation, lasertherapy and acupuncture in transformed migraine treatment. Neurol Sci 2003;24(Suppl 2): S138-42.
41. Nilsson N. A randomized controlled trial of the effect of spinal manipulation in the treatment of cervicogenic head- ache. J Manipulative Physiol Ther 1995;18:435-40.
42. Annal N, Soundappan SV, Palaniappan KMC, Chadrasekar S. Introduction of transcutaneous, low-voltage, non-pulsatile direct current (DC) therapy for migraine and chronic headaches. A comparison with transcutaneous electrical nerve stimulation (TENS). Headache Q 1992;3:434-7.
43. Nilsson N, Christensen HW, Hartvigsen J. Lasting changes in passive range motion after spinal manipulation: a randomized, blind, controlled trial. J Manipulative Physiol Ther 1996;19: 165-8.
44. Anderson RE, Seniscal C. A comparison of selected osteopathic treatment and relaxation for tension-type head- aches. Headache 2006;46:1273-80.
45. Ouseley BR, Parkin-Smith GF. Possible effects of chiropractic spinal manipulation and mobilization in the treatment of chronic tension-type headache: a pilot study. Eur J Chiropr 2002;50:3-13.
46. Fernandez-de-las-Penas C, Fernandez-Carnero J, Plaza Fernandez A, Lomas-Vega R, Miangolarra-Page JC. Dorsal manipulation in whiplash injury treatment: a randomized controlled trial. J Whiplash Related Disorders 2004;3:55-72.
47. Parker GB, Pryor DS, Tupling H. Why does migraine improve during a clinical trial? Further results from a trial of cervical manipulation for migraine. Aust N Z J Med 1980; 10:192-8.
48. Parker GB, Tupling H, Pryor DS. A controlled trial of cervical manipulation of migraine. Aust N Z J Med 1978;8:589-93.
49. Foster KA, Liskin J, Cen S, et al. The Trager approach in the treatment of chronic headache: a pilot study. Altern Ther Health Med 2004;10:40-6.
50. Haas M, Groupp E, Aickin M, et al. Dose response for chiropractic care of chronic cervicogenic headache and associated neck pain: a randomized pilot study. J Manipula- tive Physiol Ther 2004;27:547-53.
51. Sjogren T, Nissinen KJ, Jarvenpaa SK, Ojanen MT, Vanharanta H, Malkia EA. Effects of a workplace physical exercise intervention on the intensity of headache and neck and shoulder symptoms and upper extremity muscular strength of office workers: a cluster randomized controlled cross-over trial. Pain 2005;116:119-28.
52. Hanten WP, Olson SL, Hodson JL, Imler VL, Knab VM, Magee JL. The effectiveness of CV-4 and resting position techniques on subjects with tension-type headaches. J Manual Manipulative Ther 1999;7:64-70.
53. Solomon S, Elkind A, Freitag F, Gallagher RM, Moore K, Swerdlow B, et al. Safety and effectiveness of cranial electrotherapy in the treatment of tension headache. Headache 1989;29:445-50.
54. Hall T, Chan HT, Christensen L, Odenthal B, Wells C, Robinson K. Efficacy of a C1-C2 self-sustained natural apophyseal glide (SNAG) in the management of cervicogenic headache. J Orthop Sports Phys Ther 2007;37:100-7.
55. Solomon S, Guglielmo KM. Treatment of headache by transcutaneous electrical stimulation. Headache 1985;25: 12-5.
56. Hoyt WH, Shaffer F, Bard DA, Benesler ES, Blankenhorn GD, Gray JH, et al. Osteopathic manipulation in the treatment of muscle-contraction headache. J Am Osteopath Assoc 1979;78:322-5.
57. Vernon H, Jansz G, Goldsmith CH, McDermaid C. A randomized, placebo-controlled clinical trial of chiropractic and medical prophylactic treatment of adults with tension-type headache: results from a stopped trial. J Manipulative Physiol Ther 2009;32:344-51.
58. Mongini F, Ciccone G, Rota E, Ferrero L, Ugolini A, Evangelista A, et al. Effectiveness of an educational and physical programme in reducing headache, neck and shoulder pain: a workplace controlled trial. Cephalalgia 2008;28: 541-52.
59. Fernandez-de-las-Penas C, Alonso-Blanco C, San-Roman J, Miangolarra-Page JC. Methodological quality of randomized controlled trials of spinal manipulation and mobilization in tension-type headache, migraine, and cervicogenic headache. J Orthop Sports Phys Ther 2006;36:160-9.
60. Lew HL, Lin PH, Fuh JL, Wang SJ, Clark DJ, Walker WC. Characteristics and treatment of headache after traumatic brain injury: a focused review. Am J Phys Med Rehabil 2006; 85:619-27.
Chronic fatigue syndrome (CFS) is a condition that is not as straightforward as other illnesses. The symptoms can often mimic other states, including some that are pretty serious, so they must all be ruled out before a diagnosis of CFS can be determined.
This is usually not a quick process, so the patient is left dealing with troubling and often debilitating symptoms and no real answers for months or even years. By the time a patient receives a diagnosis of CFS, they are usually physically and emotionally exhausted.
Overview Of Chronic Fatigue Syndrome
According to the Centers for Disease Control (CDC), more than one million people in the United States have CFS. It is more prevalent in the U.S. than lupus, multiple sclerosis, and many types of cancer.
It is found more often in women than men; women are four times more likely to get it. While anyone of any age can get CFS, it seems to be most common in people in their 40s and 50s. Researchers have found no evidence to suggest that CFS is contagious, but they believe there may be a genetic or familial link.
Complications that can come from CFS include depression, increased absence from work, lifestyle restrictions, and inability to carry out normal daily activities like caring for children, housekeeping, or wedding functions. It can cause significant social isolation and loneliness.
Chiropractic For Chronic Fatigue Syndrome
Many people have found that chiropractic for CFS helps reduce the pain that accompanies the condition and increases injury in some patients. The chiropractor uses spinal manipulation to treat the CFS patient, allowing many symptoms associated with the disease without invasive treatments or medication.
Many CFS patients report more energy, less pain or no pain, greater flexibility, increased mobility, and reduced inflammation of joints after just a few chiropractic adjustments. Often, the patient will be recommended to attend several sessions a week for spinal adjustments and counseling on supplements and diet. All these treatments work together to relieve the symptoms, strengthen the immune system, and help the patient feel more in control of their body and condition.
Whole Patient Treatment
One of the benefits of chiropractic treatment for CFS is that it treats the whole patient, not just the symptoms. A doctor of chiropractic may recommend various chiropractic services such as spinal adjustments. Still, they will also sit with the patient and discuss that patient’s diet, daily routine, and any medications or supplements they are taking.
The chiropractor will then make dietary recommendations, including supplements that help CFS, such as:
Omega 3 fatty acids
Eiscosapentaenoic acid (EPA)
Docosahexaenoic acid (DHA)
Magnesium
Malic Acid
Linoleic Acid
Depending on the patient, they may also recommend a liver detox program and a more structured diet and exercise program.
Hope For Patients With CFS
Chiropractic care can give much-needed hope to patients with CFS. The whole patient care they receive helps not only the physical and emotional suffering as well.
The changes in diet, recommended supplements, and chiropractic treatments help the patient’s physical symptoms but also address the emotional ones, particularly depression and frustration. It is essential that patients with CFS know that there is someone who hears them, understands their difficulties, and wants to help them on every level, not just symptom control. Chiropractic care addresses all of these for optimal whole patient care.
Clinic News – Dr. Jimenez Takes A Look At Stress Management
George Lara, now retired, found relief with Dr. Alex Jimenez, back pain specialist and chiropractor, for his degenerative disk disease following two back injuries he experienced several years ago. After using drugs/medications and experiencing constant symptoms due to his DDD, Mr. Lara describes how Dr. Jimenez’s chiropractic treatment greatly helped restore his quality of life as well as promote his overall health and wellness. George Lara highly recommends Dr. Alex Jimenez as a non-surgical treatment choice for degenerative disc disease, and praises his dedication for treating his patients.
Degenerative disk disease, or DDD, refers to the natural breakdown of an intervertebral disk of the spine. Despite its title, DDD isn’t regarded as a disorder, nor is it degenerative. To the contrary, disk degeneration is frequently the consequence of ordinary daily stresses and minor accidents that cause spinal disks to slowly eliminate water in the anulus fibrosus, or even through the stiff outer layer of a disk. As water content decreases, they start to collapse. This could lead to pressure being placed on the nerves causing weakness and pain. While not necessarily symptomatic, DDD may lead to acute or chronic low back or neck pain in addition to nerve pain based on the positioning of the affected disk and the amount of strain it puts around the surrounding nerve roots.
Please Recommend Us: If you have enjoyed this video and/or we have helped you in any way please feel free to recommend us. Thank You.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine



 Please Recommend Us: If you have enjoyed this video and/or we have helped you in any way please feel free to recommend us. Thank You.
Please Recommend Us: If you have enjoyed this video and/or we have helped you in any way please feel free to recommend us. Thank You.