Chiropractic Care: Tracy Ludech, club director and coach of the El Paso Diggers, expresses how much of a difference the fitness program at PUSH has done for her athletes. Working cohesively and diligently together with the staff and trainers at PUSH, Tracy Ludech has witnessed tremendous improvements in her athlete’s strength, mobility and flexibility. Tracy Ludech encourages others to experience the benefits that a fitness program can have on young athletes.
Chiropractic Care Power & Rehabilitation
Physical wellness is a condition of health and well-being and, more especially, the ability to do aspects of sport, jobs and daily activities. Physical fitness is generally accomplished through proper nourishment, moderate-vigorous physical exercise, and sufficient rest. An extensive fitness program tailored to someone normally concentrates on one or more specific skills, and on medical needs like bone health. Many sources also cite psychological, social and emotional wellbeing as an significant part overall wellbeing. Physical fitness may also prevent or treat several chronic health conditions brought on by unhealthy lifestyle or aging.
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
If you have enjoyed this video and/or we have helped you in any way please feel free to subscribe and share us.
Concussions are traumatic brain injuries that affect brain function. Effects from these injuries are often temporary but can include headaches, problems with concentration, memory, balance and coordination. Concussions are usually caused by a blow to the head or violent shaking of the head and upper body. Some concussions cause loss of consciousness, but most do not. And it is possible to have a concussion and not realize it. Concussions are common in contact sports, such as football. However, most people gain a full recovery after a concussion.
Can also happen due to excessive shaking of the head or acceleration/deceleration
Mild injuries (mTBI/concussions) are the most common type of brain injury
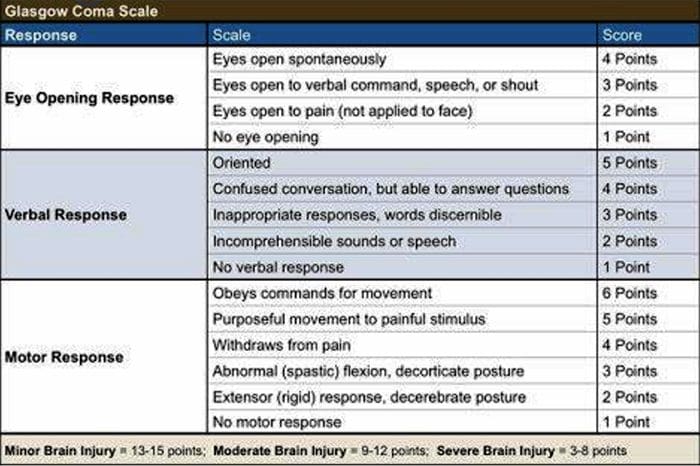
Glasgow Coma Scale
Common Causes Of Concussion
Motor vehicle collisions
Falls
Sports injuries
Assault
Accidental or intentional discharge of weapons
Impact with objects
Prevention
Prevention of concussive injuries can be paramount
Encourage Patients To Wear Helmets
Competitive sports, especially boxing, hokey, football and baseball
Horseback riding
Riding bicycles, motorcycles, ATVs, etc.
High elevation activates such as rock climbing, zip lining
Skiing, snowboarding
Encourage Patients To Wear Seatbelts
Discuss the importance of wearing seatbelts at all times in vehicles with all of your patients
Also encourage use of appropriate booster or car seats for children to ensure adequate fit and function of seat belts.
Driving Safely
Patients should never drive while under the influence of drugs, including certain medications or alcohol
Never text and drive
Make Spaces Safer For Children
Install baby gates and window latches in the home
May in areas with shock-absorbing material, such as hardwood mulch or sand
Supervise children carefully, especially when they�re near water
Prevent Falls
Clearing tripping hazards such as loose rugs, uneven flooring or walkway clutter
Using nonslip mats in the bathtub and on shower floors, and installing grab bars next to the toilet, tub and shower
Ensure appropriate footwear
Installing handrails on both sides of stairways
Improving lighting throughout the home
Balance training exercises
Balance Training
Single leg balance
Bosu ball training
Core strengthening
Brain balancing exercises
Concussion Verbiage
Concussion vs. mTBI (mild traumatic brain injury)
mTBI is the term being used more commonly in medical settings, but concussion is a more largely recognized term in the community by sports coaches, etc.
The two terms describe the same basic thing, mTBI is a better term to use in your charting
Evaluating Concussion
Remember that there does not always have to be loss of consciousness for there to be a concussion
Post-Concussion Syndrome can occur without LOC as well
Symptoms of concussion may not be immediate and could take days to develop
Monitor for 48 post head injury watching for red flags
Blurred eyesight or other vision problems, such as dilated or uneven pupils
Confusion
Dizziness
Ringing in the ears
Nausea or vomiting
Slurred speech
Delayed response to questions
Memory loss
Fatigue
Trouble concentrating
Continued or persistent memory loss
Irritability and other personality changes
Sensitivity to light and noise
Sleep problems
Mood swings, stress, anxiety or depression
Disorders of taste and smell
Mental/Behavioral Changes
Verbal outbursts
Physical outbursts
Poor judgment
Impulsive behavior
Negativity
Intolerance
Apathy
Egocentricity
Rigidity and inflexibility
Risky behavior
Lack of empathy
Lack of motivation or initiative
Depression or anxiety
Symptoms In Children
Concussions can present differently in children
Excessive crying
Loss of appetite
Loss of interest in favorite toys or activities
Sleep issues
Vomiting
Irritability
Unsteadiness while standing
Amnesia
Memory loss and failure to form new memories
Retrograde Amnesia
Inability to remember things that happened before the injury
Due to failure in recall
Anterograde Amnesia
Inability to remember things that happened after the injury
Due to failure to formulate new memories
Even short memory losses can be predictive of outcome
Amnesia may be up to 4-10 times more predictive of symptoms and cognitive deficits following concussion than is LOC (less than 1 minute)
Return To Play Progression
Baseline: No Symptoms
As the baseline step of the Return to Play Progression, the athlete needs to have completed physical and cognitive rest and not be experiencing concussion symptoms for a minimum of 48 hours. Keep in mind, the younger the athlete, the more conservative the treatment.
Step 1: Light Aerobic Activity
The Goal: Only to increase an athlete�s heart rate.
The Time: 5 to 10 minutes.
The Activities: Exercise bike, walking, or light jogging.
Absolutely no weight lifting, jumping or hard running.
Step 2: Moderate activity
The Goal: Limited body and head movement.
The Time: Reduced from typical routine.
The Activities: Moderate jogging, brief running, moderate-intensity stationary biking, and moderate-intensity weightlifting
Step 3: Heavy, non-contact activity
The Goal: More intense but non-contact
The Time: Close to typical routine
The Activities: Running, high-intensity stationary biking, the player�s regular weightlifting routine, and non- contact sport-specific drills. This stage may add some cognitive component to practice in addition to the aerobic and movement components introduced in Steps 1 and 2.
Step 4: Practice & full contact
The Goal: Reintegrate in full contact practice.
Step 5: Competition
The Goal: Return to competition.
Microglial Priming
After head trauma microglial cells are primed and can become over active
To combat this, you must mediate the inflammation cascade
Prevent repeated head trauma
Due to priming of the foam cells, response to follow-up trauma may be far more severe and damaging
What Is Post-Concussion Syndrome (PCS)?
Symptoms following head trauma or mild traumatic brain injury, that can last weeks, months or years after injury
Symptoms persist longer than expected after initial concussion
More common in women and persons of advanced age who suffer head trauma
Severity of PCS often does not correlate to severity of head injury
PCS Symptoms
Headaches
Dizziness
Fatigue
Irritability
Anxiety
Insomnia
Loss of concentration and memory
Ringing in the ears
Blurry vision
Noise and light sensitivity
Rarely, decreases in taste and smell
Concussion Associated Risk Factors
Early symptoms of headache after injury
Mental changes such as amnesia or fogginess
Fatigue
Prior history of headaches
Evaluation Of PCS
PCS is a diagnosis of exclusion
If patient presents with symptoms after head injury, and other possible causes have been ruled out => PCS
Use appropriate testing and imaging studies to rule out other causes of symptoms
Headaches In PCS
Often �tension� type headache
Treat as you would for tension headache
Reduce stress
Improve stress coping skills
MSK treatment of the cervical and thoracic regions
Constitutional hydrotherapy
Adrenal supportive/adaptogenic herbs
Can be migraine, especially in people who had pre-existing migraine conditions prior to injury
Reduce inflammatory load
Consider management with supplements and or medications
Reduce light and sound exposure if there is sensitivity
Dizziness In PCS
After head trauma, always assess for BPPV, as this is the most common type of vertigo after trauma
Dix-Hallpike maneuver to diagnose
Epley�s maneuver for treatment
Light & Sound Sensitivity
Hypersensitivity to light and sound is common in PCS and typically exacerbates other symptoms such as headache and anxiety
Management of excess mesencephalon stimulation is crucial in such cases
Sunglasses
Other light blocking glasses
Earplugs
Cotton in ears
Treatment Of PCS
Manage each symptom individually as you otherwise would
Manage CNS inflammation
Curcumin
Boswelia
Fish oil/Omega-3s � (***after r/o bleed)
Cognitive behavioral therapy
Mindfulness & relaxation training
Acupuncture
Brain balancing physical therapy exercises
Refer for psychological evaluation/treatment
Refer to mTBI specialist
mTBI Specialists
mTBI is difficult to treat and is an entire specialty both in the allopathic and complementary medicine
Primary objective is to recognize and refer for appropriate care
Pursue training in mTBI or plan to refer to TBI specialists
Sources
�A Head for the Future.� DVBIC, 4 Apr. 2017, dvbic.dcoe.mil/aheadforthefuture.
Alexander G. Reeves, A. & Swenson, R. Disorders of the Nervous System. Dartmouth, 2004.
�Heads Up to Health Care Providers.� Centers for Disease Control and Prevention, Centers for Disease Control and Prevention, 16 Feb. 2015, www.cdc.gov/headsup/providers/.
�Post-Concussion Syndrome.� Mayo Clinic, Mayo Foundation for Medical Education and Research, 28 July 2017, www.mayoclinic.org/diseases-conditions/post- concussion-syndrome/symptoms-causes/syc-20353352.
The history of chiropractic dates all the way back to 1895 when Daniel David (DD) Palmer, founder of chiropractic, did his first spinal adjustment on a janitor � restoring his hearing in the process. Palmer moved from what is now Ontario, Canada to the United States in 1865 and started practicing magnetic healing and other natural health practices in Davenport, Iowa in 1880. His interest in a more organic, less invasive approach to healing opened the door for the natural, whole body wellness that chiropractic provides.
Chiropractic
In 1895, Palmer encountered a janitor who claimed that he had lost his hearing when he moved and heard a �pop� in his back. Upon inspection, Palmer noted that the janitor had a vertebra out of place. He had the man lie on the floor, face down, while he manipulated the man�s spine, gently coaxing it into alignment. The next day the janitor claimed that he could hear again.
Two years later, after extensive research and development of the practice of what he called �chiropractic,� he opened the Palmer School of Cure where he began teaching others his techniques. After that first adjustment, word spread and this new, mysterious practice piqued the interest of the public, many who became students, including Palmer�s own son, Bartlett Joshua. Quite a few early students were practitioners of the healing arts of osteopathy and medicine. The school is still operational today as the Palmer School of Chiropractic.
The term was first coined by DD Palmer and is derived from two Greek words, the first cheir which means �hand� and praktos which means �done.� A literal translation is �done by hand� which is an apt moniker for this very hands on practice.
The first state to create laws licensing chiropractors was Kansas in 1913. By 1931, 39 states were on board, giving legal recognition to chiropractors. The last state was Louisiana in 1974.
There are more than 60,000 active licenses in the U.S. alone. Several U.S. territories, including the U.S. Virgin Islands and Puerto Rico officially recognize the practice as a legitimate health care profession. Switzerland, Japan, Australia, Great Britain, Mexico, and Canada, as well as other countries, also recognize chiropractic and have created laws to regulate it.
Over the years, chiropractic has evolved and grown beyond the sole use of spinal adjustments as treatment. Other treatments and philosophies have been developed and introduced. Research was initiated in 1975 at a conference hosted by the National Institutes of Health.
Over the years, chiropractic was not met with much acceptance by many medical associations – initially anyway. Eventually, many have come on board once that have seen chiropractic�s benefits. In 1987, the American Medical Association filed and lost an antitrust case against chiropractic. Until that time, the AMA had been boycotting the practice. That ended when they lost their case.
Chiropractic successfully changed the landscape of health care and health care practitioners. By providing a whole body approach, it has been used to treat a variety of conditions from back pain to knee injuries to colic in infants. Research backing it as a legitimate medical practice is steadily mounting. Chiropractic is proving to be beneficial for a wide variety of health ailments that extend far beyond a painful back.
As chiropractic continues to develop and grow, even more doors are opened, allowing the practice to grow and evolve. Every year researchers are finding more uses for chiropractic treatment and discovering just how beneficial it can be for a myriad of health conditions. As fast as it has grown since its discovery, it is easy to envision continued, rapid advancement in the years to come.
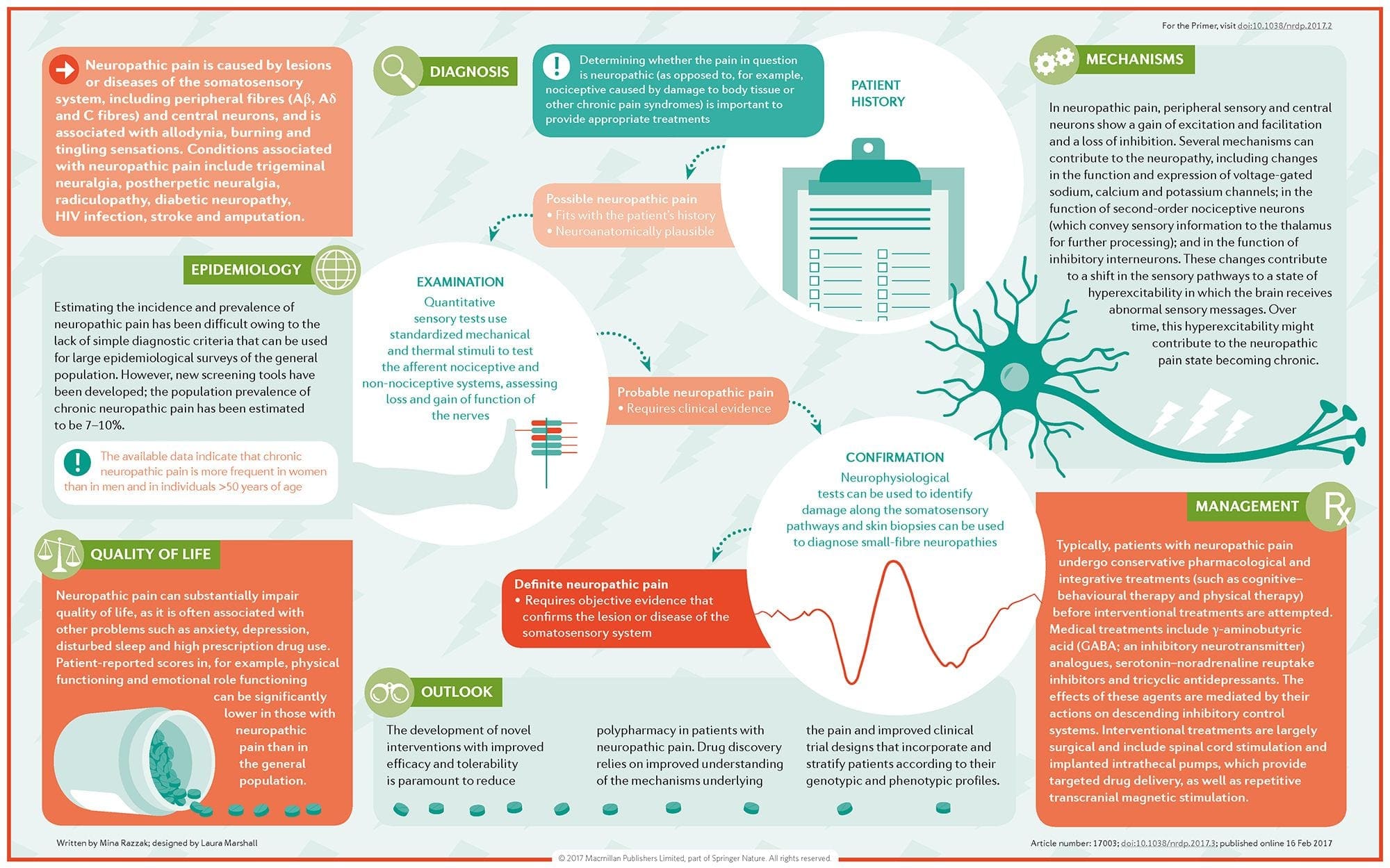
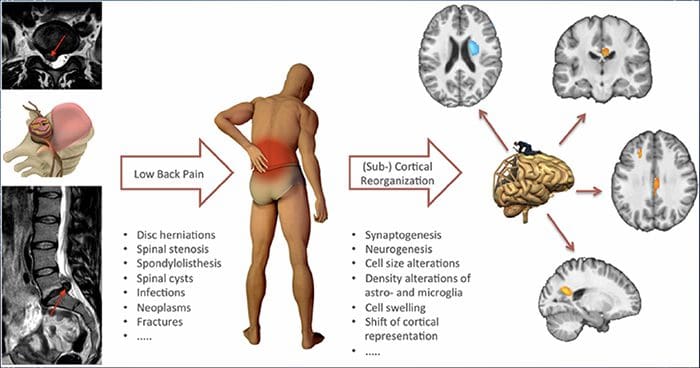
Neuropathic pain is a complex, chronic pain condition that is generally accompanied by soft tissue injury. Neuropathic pain is common in clinical practice and also poses a challenge to patients and clinicians alike. With neuropathic pain, the nerve fibers themselves may be either damaged, dysfunctional or injured. Neuropathic pain is the result of damage from trauma or disease to the peripheral or central nervous system, where the lesion may occur at any site. As a result, these damaged nerve fibers can send incorrect signals to other pain centers. The effect of a nerve fiber injury consists of a change in neural function, both at the region of the injury and also around the injury. Clinical signs of neuropathic pain normally include sensory phenomena, such as spontaneous pain, paresthesias and hyperalgesia.
Neuropathic pain, as defined by the International Association of the Study of Pain or the IASP, is pain initiated or caused by a primary lesion or dysfunction of the nervous system. It could result from damage anywhere along the neuraxis: peripheral nervous system, spinal or supraspinal nervous system. Traits that distinguish neuropathic pain from other kinds of pain include pain and sensory signs lasting beyond the recovery period. It’s characterized in humans by spontaneous pain, allodynia, or the experience of non-noxious stimulation as painful, and causalgia, or persistent burning pain. Spontaneous pain includes sensations of “pins and needles”, burning, shooting, stabbing and paroxysmal pain, or electric-shock like pain, often associated with dysesthesias and paresthesias. These sensations not only alter the patient’s sensory apparatus, but also the patient’s well-being, mood, attention and thinking. Neuropathic pain is made up of both “negative” symptoms, such as sensory loss and tingling sensations, and “positive” symptoms, such as paresthesias, spontaneous pain and increased feeling of pain.
Conditions frequently related to neuropathic pain can be classified into two major groups: pain due to damage in the central nervous system and pain because of damage to the peripheral nervous system. Cortical and sub-cortical strokes, traumatic spinal cord injuries, syringo-myelia and syringobulbia, trigeminal and glossopharyngeal neuralgias, neoplastic and other space-occupying lesions are clinical conditions that belong to the former group. Nerve compression or entrapment neuropathies, ischemic neuropathy, peripheral polyneuropathies, plexopathies, nerve root compression, post-amputation stump and phantom limb pain, postherpetic neuralgia and cancer-related neuropathies are clinical conditions that belong to the latter group.
Contents
Pathophysiology of Neuropathic Pain
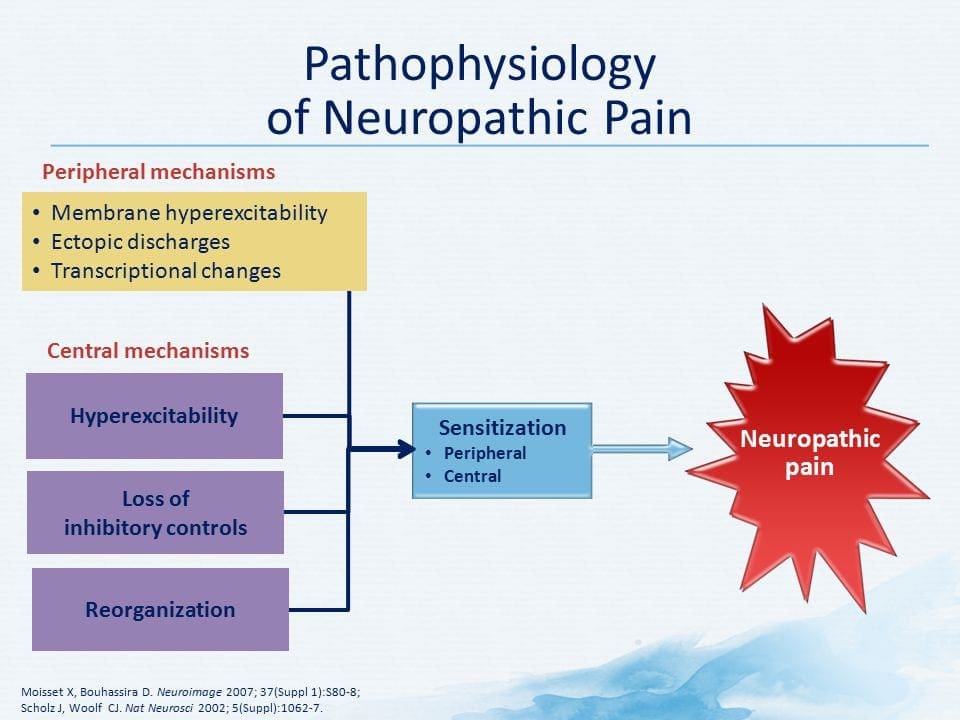
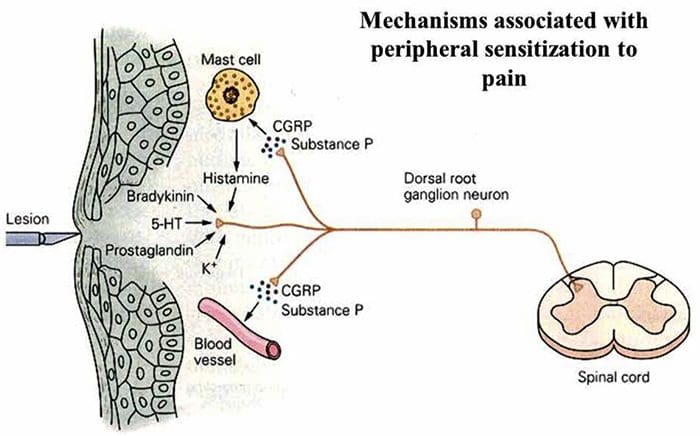
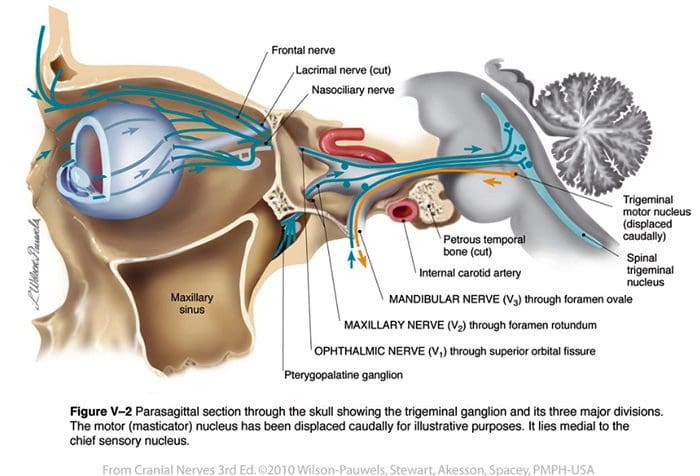
The pathophysiologic processes and concepts underlying neuropathic pain are multiple. Prior to covering these processes, a review of ordinary pain circuitry is critical. Regular pain circuitries involve activation of a nociceptor, also known as the pain receptor, in response to a painful stimulation. A wave of depolarization is delivered to the first-order neurons, together with sodium rushing in via sodium channels and potassium rushing out. Neurons end in the brain stem in the trigeminal nucleus or in the dorsal horn of the spinal cord. It is here where the sign opens voltage-gated calcium channels in the pre-synaptic terminal, allowing calcium to enter. Calcium allows glutamate, an excitatory neurotransmitter, to be released into the synaptic area. Glutamate binds to NMDA receptors on the second-order neurons, causing depolarization.
These neurons cross through the spinal cord and travel until the thalamus, where they synapse with third-order neurons. These then connect to the limbic system and cerebral cortex. There is also an inhibitory pathway that prevents pain signal transmission from the dorsal horn. Anti-nociceptive neurons originate in the brain stem and travel down the spinal cord where they synapse with short interneurons in the dorsal horn by releasing dopamine and norepinephrine. The interneurons modulate the synapse between the first-order neuron as well as the second-order neuron by releasing gamma amino butyric acid, or GABA, an inhibitory neurotransmitter. Consequently, pain cessation is the result of inhibition of synapses between first and second order neurons, while pain enhancement might be the result of suppression of inhibitory synaptic connections.
The mechanism underlying neuropathic pain, however, aren’t as clear. Several animal studies have revealed that lots of mechanisms may be involved. However, one has to remember that what applies to creatures may not always apply to people. First order neurons may increase their firing if they’re partially damaged and increase the amount of sodium channels. Ectopic discharges are a consequence of enhanced depolarization at certain sites in the fiber, resulting in spontaneous pain and movement-related pain. Inhibitory circuits might be diminished in the level of the dorsal horn or brain stem cells, as well as both, allowing pain impulses to travel unopposed.
In addition, there might be alterations in the central processing of pain when, because of chronic pain and the use of some drug and/or medications, second- and third-order neurons can create a “memory” of pain and become sensitized. There’s then heightened sensitivity of spinal neurons and reduced activation thresholds. Another theory demonstrates the concept of sympathetically-maintained neuropathic pain. This notion was demonstrated by analgesia following sympathectomy from animals and people. However, a mix of mechanics can be involved in many chronic neuropathic or mixed somatic and neuropathic pain conditions. Among those challenges in the pain field, and much more so as it pertains to neuropathic pain, is the capability to check it. There is a dual component to this: first, assessing quality, intensity and advancement; and second, correctly diagnosing neuropathic pain.
There are, however, some diagnostic tools that may assist clinicians in evaluating neuropathic pain. For starters, nerve conduction studies and sensory-evoked potentials may identify and quantify the extent of damage to sensory, but not nociceptive, pathways by monitoring neurophysiological responses to electrical stimuli. Additionally, quantitative sensory testing steps perception in reaction to external stimuli of varying intensities by applying stimulation to the skin. Mechanical sensitivity to tactile stimuli is measured with specialized tools, such as von Frey hairs, pinprick with interlocking needles, as well as vibration sensitivity together with vibrameters and thermal pain with thermodes.
It is also extremely important to perform a comprehensive neurological evaluation to identify motor, sensory and autonomic dysfunctions. Ultimately, there are numerous questionnaires used to distinguish neuropathic pain in nociceptive pain. Some of them include only interview queries (e.g., the Neuropathic Questionnaire and ID Pain), while others contain both interview questions and physical tests (e.g., the Leeds Assessment of Neuropathic Symptoms and Signs scale) and the exact novel tool, the Standardized Evaluation of Pain, which combines six interview questions and ten physiological evaluations.
Treatment Modalities for Neuropathic Pain
Pharmacological regimens aim at the mechanisms of neuropathic pain. However, both pharmacologic and non-pharmacologic treatments deliver complete or partial relief in just about half of patients. Many evidence-based testimonials suggest using mixtures of drugs and/or medications to function for as many mechanisms as possible. The majority of studies have researched mostly post-herpetic neuralgia and painful diabetic neuropathies but the results may not apply to all neuropathic pain conditions.
Antidepressants
Antidepressants increase synaptic serotonin and norepinephrine levels, thereby enhancing the effect of the descending analgesic system associated with neuropathic pain. They’ve been the mainstay of neuropathic pain therapy. Analgesic actions might be attributable to nor-adrenaline and dopamine reuptake blockade, which presumably enhance descending inhibition, NMDA-receptor antagonism and sodium-channel blockade. Tricyclic antidepressants, such as TCAs; e.g., amitriptyline, imipramine, nortriptyline and doxepine, are powerful against continuous aching or burning pain along with spontaneous pain.
Tricyclic antidepressants have been proven significantly more effective for neuropathic pain than the specific serotonin reuptake inhibitors, or SSRIs, such as fluoxetine, paroxetine, sertraline and citalopram. The reason may be that they inhibit reuptake of serotonin and nor-epinephrine, while SSRIs only inhibit serotonin reuptake. Tricyclic antidepressants can have unpleasant side effects, including nausea, confusion, cardiac conduction blocks, tachycardia and ventricular arrhythmias. They can also cause weight gain, a reduced seizure threshold and orthostatic hypotension. Tricyclics have to be used with care in the elderly, who are particularly vulnerable to their acute side effects. The drug concentration in the blood should be monitored to avoid toxicity in patients who are slow medication metabolizers.
Serotonin-norepinephrine reuptake inhibitors, or SNRIs, are a new class of antidepressants. Like TCAs, they seem to be more effective than SSRIs for treating neuropathic pain because they also inhibit reuptake of both nor-epinephrine and dopamine. Venlafaxine is as effective against debilitating polyneuropathies, such as painful diabetic neuropathy, as imipramine, in the mention of TCA, and the two are significantly greater than placebo. Like the TCAs, the SNRIs seem to confer benefits independent of their antidepressant effects. Side effects include sedation, confusion, hypertension and withdrawal syndrome.
Antiepileptic Drugs
Antiepileptic drugs can be utilized as first-line treatment especially for certain types of neuropathic pain. They act by modulating voltage-gated calcium and sodium channels, by improving the inhibitory effects of GABA and by inhibiting excitatory glutaminergic transmission. Anti-epileptic medications have not been demonstrated to be effective for acute pain. In chronic pain cases, antiepileptic drugs seem to be effective only in trigeminal neuralgia. Carbamazepine is routinely employed for this condition. Gabapentin, which functions by inhibiting calcium channel function through agonist actions at the alpha-2 delta subunit of the calcium channel, is also known to be effective for neuropathic pain. However, gabapentin acts centrally and it might cause fatigue, confusion and somnolence.
Non-Opioid Analgesics
There is a lack of strong data supporting using non-steroidal anti inflammatory medications, or NSAIDs, in the relief of neuropathic pain. This may be due to the lack of an inflammatory component in relieving pain. But they have been utilized interchangeably with opioids as adjuvants in treating cancer pain. There have been reported complications, though, especially in severely debilitated patients.
Opioid Analgesics
Opioid analgesics are a subject of much debate in relieving neuropathic pain. They act by inhibiting central ascending pain impulses. Traditionally, neuropathic pain has been previously observed to be opioid-resistant, in which opioids are more suitable methods for coronary and somatic nociceptive types of pain. Many doctors prevent using opioids to treat neuropathic pain, in large part because of concerns about drug abuse, addiction and regulatory issues. But, there are many trials that have found opioid analgesics to succeed. Oxycodone was superior to placebo for relieving pain, allodynia, improving sleep and handicap. Controlled-release opioids, according to a scheduled basis, are recommended for patients with constant pain to encourage constant levels of analgesia, prevent fluctuations in blood glucose and prevent adverse events associated with higher dosing. Most commonly, oral preparations are used because of their greater ease of use and cost-effectiveness. Trans-dermal, parenteral and rectal preparations are generally used in patients who cannot tolerate oral drugs.
Local Anesthetics
Nearby acting anesthetics are appealing because, thanks to their regional action, they have minimal side effects. They act by stabilizing sodium channels at the axons of peripheral first-order neurons. They work best if there is only partial nerve injury and excess sodium channels have collected. Topical lidocaine is the best-studied representative of the course for neuropathic pain. Specifically, the use of this 5 percent lidocaine patch for post-herpetic neuralgia has caused its approval by the FDA. The patch seems to work best when there is damaged, but maintained, peripheral nervous system nociceptor function from the involved dermatome demonstrating as allodynia. It needs to be set directly on the symptomatic area for 12 hours and eliminated for another 12 hours and may be used for years this way. Besides local skin reactions, it is often well tolerated by many patients with neuropathic pain.
Miscellaneous Drugs
Clonidine, an alpha-2-agonist, was shown to be effective in a subset of patients with diabetic peripheral neuropathy. Cannabinoids have been found to play a role in experimental pain modulation in animal models and evidence of the efficacy is accumulating. CB2-selective agonists suppress hyperalgesia and allodynia and normalize nociceptive thresholds without inducing analgesia.
Interventional Pain Management
Invasive treatments might be considered for patients who have intractable neuropathic pain. These treatments include epidural or perineural injections of local anesthetics or corticosteroids, implantation of epidural and intrathecal drug delivery methods and insertion of spinal cord stimulators. These approaches are reserved for patients with intractable chronic neuropathic pain who have failed conservative medical management and also have experienced thorough psychological evaluation. In a study by Kim et al, it was shown that a spinal cord stimulator was effective in treating neuropathic pain of nerve root origin.
Dr. Alex Jimenez’s Insight
With neuropathic pain, chronic pain symptoms occur due to the nerve fibers themselves being damaged, dysfunctional or injured, generally accompanied by tissue damage or injury. As a result, these nerve fibers can begin to send incorrect pain signals to other areas of the body. The effects of neuropathic pain caused by nerve fiber injuries includes modifications in nerve function both at the site of injury and at areas around the injury. Understanding the pathophysiology of neuropathic pain has been a goal for many healthcare professionals, in order to effectively determine the best treatment approach to help manage and improve its symptoms. From the use of drugs and/or medications, to chiropractic care, exercise, physical activity and nutrition, a variety of treatment approaches may be used to help ease neuropathic pain for each individual’s needs.
Additional Interventions for Neuropathic Pain
Lots of patients with neuropathic pain pursue complementary and alternative treatment options to treat neuropathic pain. Other well-known regimens used to treat neuropathic pain include acupuncture, percutaneous electrical nerve stimulation, transcutaneous electrical nerve stimulation, cognitive behavioral treatment, graded motor imagery and supportive treatment, and exercise. Among these however, chiropractic care is a well-known alternative treatment approach commonly utilized to help treat neuropathic pain. Chiropractic care, along with physical therapy, exercise, nutrition and lifestyle modifications can ultimately offer relief for neuropathic pain symptoms.
Chiropractic Care
What is known is that a comprehensive management application is crucial to combat the effects of neuropathic pain. In this manner, chiropractic care is a holistic treatment program that could be effective in preventing health issues associated with nerve damage. Chiropractic care provides assistance to patients with many different conditions, including those with neuropathic pain. Sufferers of neuropathic pain often utilize non-steroidal-anti-inflammatory medications, or NSAIDs, such as ibuprofen, or heavy prescription painkillers to help ease neuropathic pain. These may provide a temporary fix but need constant use to manage the pain. This invariably contributes to harmful side effects and in extreme situations, prescription drug dependence.
Chiropractic care can help improve symptoms of neuropathic pain and enhance stability without these downsides. An approach such as chiropractic care offers an individualized program designed to pinpoint the root cause of the issue. Through the use of spinal adjustments and manual manipulations, a chiropractor can carefully correct any spinal misalignments, or subluxations, found along the length of the spine, which could lower the consequences of nerve wracking via the realigning of the backbone. Restoring spinal integrity is essential to keeping a high-functioning central nervous system.
A chiropractor can also be a long-term treatment towards enhancing your overall well-being. Besides spinal adjustments and manual manipulations, a chiropractor may offer nutritional advice, such as prescribing a diet rich in antioxidants, or they may design a physical therapy or exercise program to fight nerve pain flair-ups. A long-term condition demands a long-term remedy, and in this capacity, a healthcare professional who specializes in injuries and/or conditions affecting the musculoskeletal and nervous system, such as a doctor of chiropractic or chiropractor, may be invaluable as they work to gauge favorable change over time.
Physical therapy, exercise and movement representation techniques have been demonstrated to be beneficial for neuropathic pain treatment. Chiropractic care also offers other treatment modalities which may be helpful towards the management or improvement of neuropathic pain. Low level laser therapy, or LLLT, for instance, has gained tremendous prominence as a treatment for neuropathic pain. According to a variety of research studies, it was concluded that LLLT had positive effects on the control of analgesia for neuropathic pain, however, further research studies are required to define treatment protocols that summarize the effects of low level laser therapy in neuropathic pain treatments.
Chiropractic care also includes nutritional advice, which can help control symptoms associated with diabetic neuropathy. During a research study, a low fat plant-based diet was demonstrated to improve glycemic control in patients with type 2 diabetes. After about 20 weeks of the pilot study, the individuals involved reported changes in their body weight and electrochemical skin conductance in the foot was reported to have improved with the intervention. The research study suggested a potential value in the low-fat plant-based diet intervention for diabetic neuropathy. Moreover, clinical studies found that the oral application of magnesium L-threonate is capable of preventing as well as restoring memory deficits associated with neuropathic pain.
Chiropractic care can also offer additional treatment strategies to promote nerve regeneration. By way of instance, enhancing the regeneration of axons has been suggested to help improve functional recovery after peripheral nerve injury. Electrical stimulation, together with exercise or physical activities, was found to promote nerve regeneration after delayed nerve repair in humans and rats, according to recent research studies. Both electrical stimulation and exercise were ultimately determined to be promising experimental treatments for peripheral nerve injury which seem ready to be transferred to clinical use. Further research studies may be needed to fully determine the effects of these in patients with neuropathic pain.
Conclusion
Neuropathic pain is a multifaceted entity with no particular guidelines to take care of. It’s best managed using a multidisciplinary approach. Pain management requires ongoing evaluation, patient education, ensuring patient follow-up and reassurance. Neuropathic pain is a chronic condition that makes the option for the best treatment challenging. Individualizing treatment involves consideration of the impact of the pain on the individual’s well-being, depression and disabilities together with continuing education and evaluation. Neuropathic pain studies, both on the molecular level and in animal models, is relatively new but very promising. Many improvements are anticipated in the basic and clinical fields of neuropathic pain hence opening the doorways to improved or new treatment modalities for this disabling condition. The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Back Pain
Back pain is one of the most prevalent causes for disability and missed days at work worldwide. As a matter of fact, back pain has been attributed as the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience some type of back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
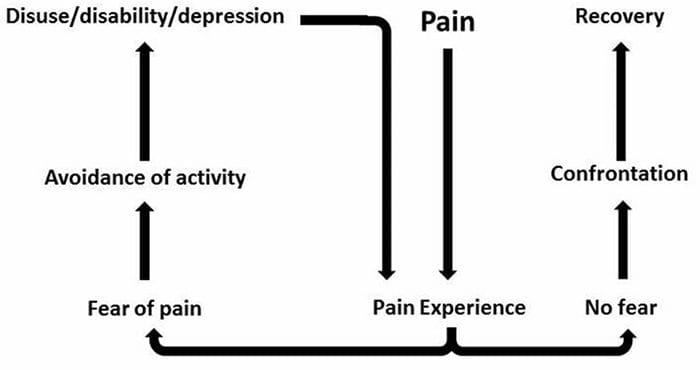
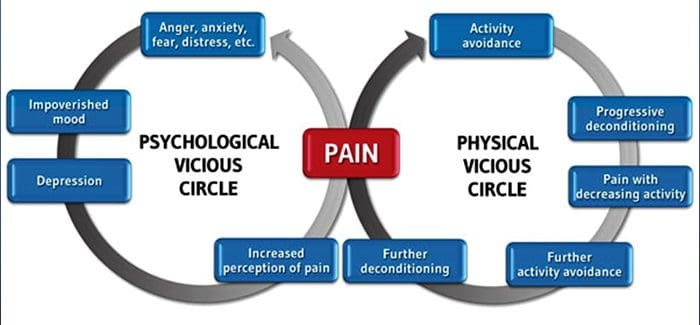
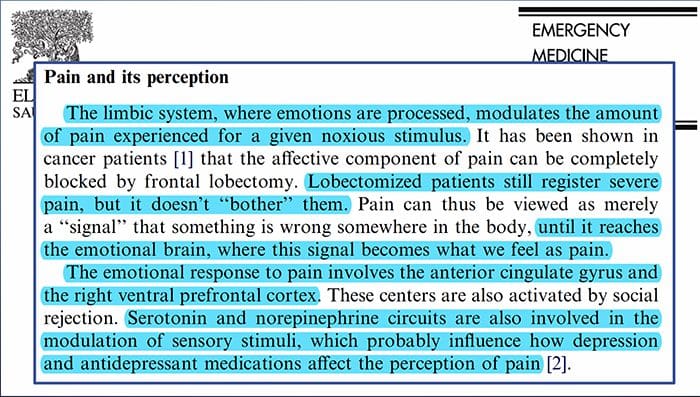
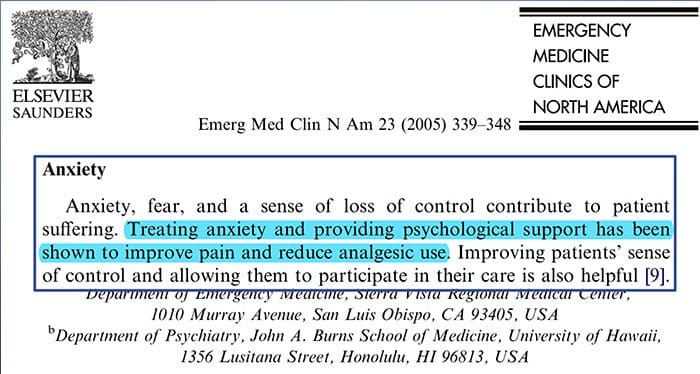
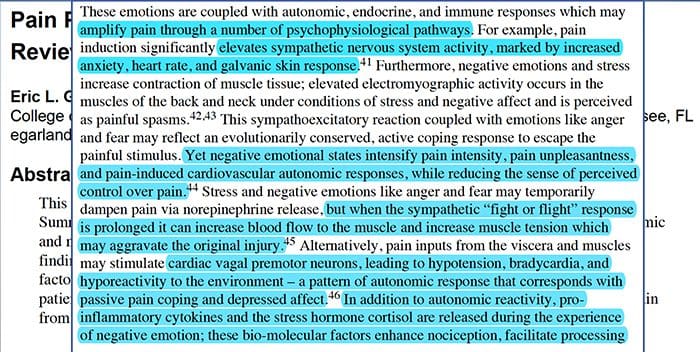
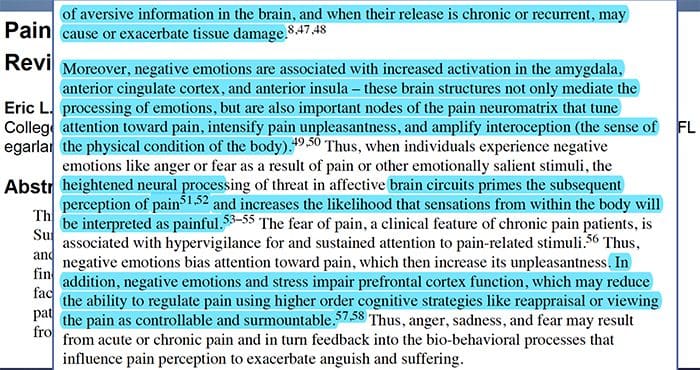
Pain Anxiety Depression�Everyone has experienced pain, however, there are those with depression, anxiety, or both. Combine this with pain and it can become pretty intense and difficult to treat. People that are suffering from depression, anxiety or both tend to experience severe and long term pain more so than other people.
The way anxiety, depression, and pain overlap each other is seen in chronic and in some disabling pain syndromes, i.e. low back pain, headaches, nerve pain and fibromyalgia. Psychiatric disorders contribute to the pain intensity and also increase the risk of disability.
Depression:�A (major depressive disorder or clinical depression) is a common but serious mood disorder. It causes severe symptoms that affect how an individual feels, thinks, and how the handle daily activities, i.e. sleeping, eating and working. To be diagnosed with depression, the symptoms must be present for at least two weeks.
Persistent sad, anxious, or �empty� mood.
Feelings of hopelessness, pessimistic.
Irritability.
Feelings of guilt, worthlessness, or helplessness.
Loss of interest or pleasure in activities.
Decreased energy or fatigue.
Moving or talking slowly.
Feeling restless & having trouble sitting still.
Difficulty concentrating, remembering, or making decisions.
Thoughts of death or suicide & or suicide attempts.
Aches or pains, headaches, cramps, or digestive problems without a clear physical cause and/or that do not ease with treatment.
Not everyone who is depressed experiences every symptom. Some experience only a few symptoms while others may experience several. Several persistent symptoms in addition to low mood are�required�for a diagnosis of major depression. The severity and frequency of symptoms along with the duration will vary depending on the individual and their particular illness. Symptoms can also vary depending on the stage of the illness.
Contents
PAIN ANXIETY DEPRESSION
Objectives:
What is the relationship?
What is the neurophysiology behind it?
What are the central consequences?
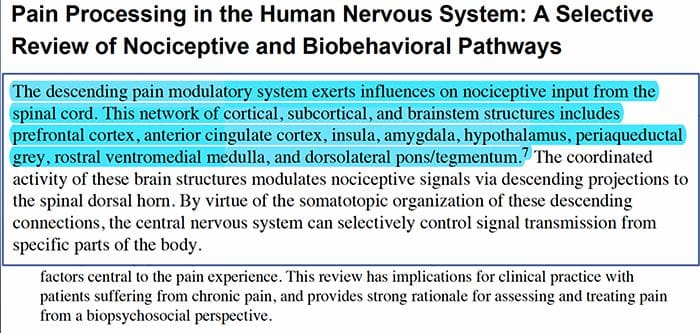
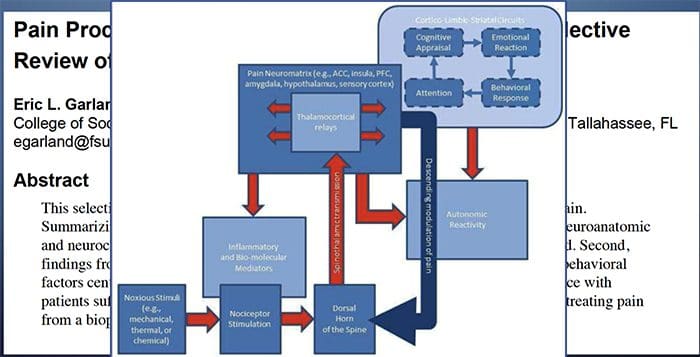
Brain Changes In Pain
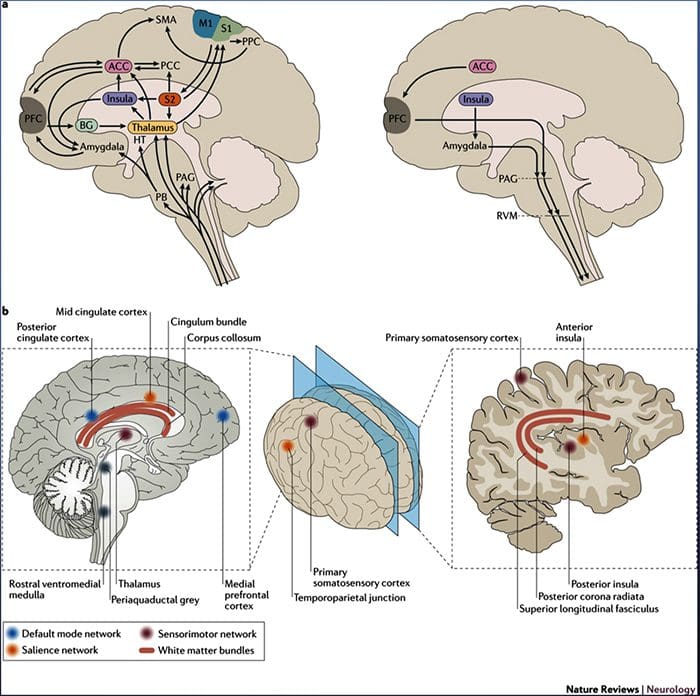
Figure 1 Brain pathways, regions and networks involved in acute and chronic pain
Davis, K. D. et al. (2017) Brain imaging tests for chronic pain: medical, legal and ethical issues and recommendations Nat. Rev. Neurol. doi:10.1038/nrneurol.2017.122
PAIN, ANXIETY AND DEPRESSION
Conclusion:
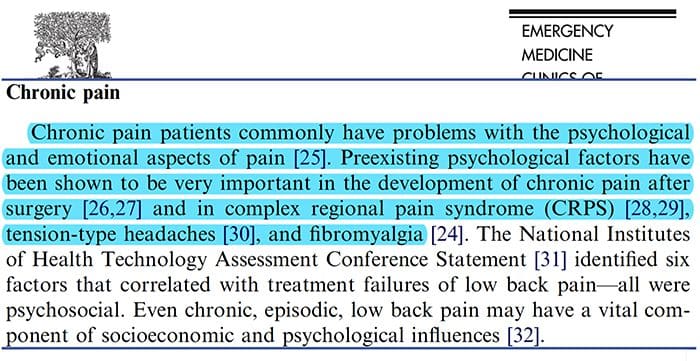
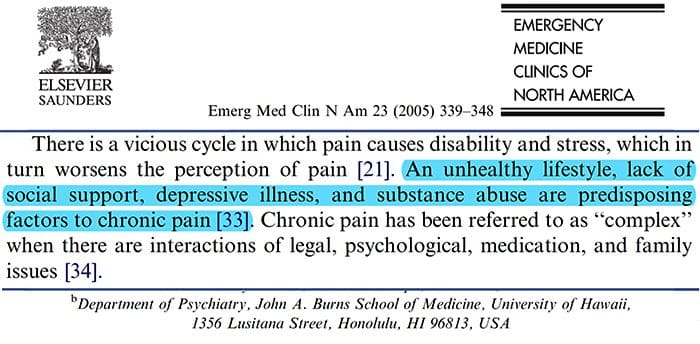
Pain, especially chronic is associated with depression and anxiety
The physiological mechanisms leading to anxiety and depression can be multifactorial in nature
Pain causes changes in brain structure and function
This change in structure and function can alter the ability for the brain to modulate pain as well as control mood.
Functional short leg is a fairly common condition that typically occurs due to inflexibility or muscle weakness at the pelvis, ankle, and foot complex. Runners sometimes experience the condition when running over certain surfaces that are unstable or not level. It can also occur due to inappropriate footwear.
This condition can cause pain in the lower spine, hips, buttock, and leg. If left untreated, it can lead to balance issues, neck and shoulder problems, and incorrect weight distribution. Chiropractic care has been proven to effectively treat functional leg syndrome.
Contents
What Is Functional Short Leg?
Patients with a functional short leg have an apparent short leg although structurally both legs are the same length when measured. The most common method for measuring leg length is from the medial malleolus (inside ankle bone) to the ASIS (front of the pelvis). When the legs are measured in the case of a functional short leg, they are equal in length.
Mothers who always carry a child on one hip or individuals who always sleep on the same side can experience functional short leg syndrome. In fact, any movement, posture, or activity that causes increased stresses on the joints, nerves, and muscles involved can create an imbalance.
Functional Short Leg vs Anatomical Short Leg
Where with functional short leg syndrome one leg is apparently shorter than the other but not structurally so, an anatomical short leg is structurally shorter. This can happen due to growth problems, structural issues, and curvature of the spine.
The differences between the two conditions are significant, particularly when it comes to treatment. Both conditions can be treated by chiropractic for pain. Functional short leg syndrome can greatly benefit from chiropractic care as it helps to realign the body.
Symptoms Of Functional Short Leg
Functional short leg syndrome symptoms can remain confined to the leg, lower back, and hip region, or it can affect the entire body. When walking it can affect the way your feet hit the ground, causing pain in the foot and ankle.
However, it can even affect how you chew your food and how your teeth come together. When a person has short leg syndrome, they will often adjust their body in order to compensate, but that is when the real problems start. Symptoms of functional short leg syndrome include:
Pain in the lower back
Pain in the knee of both the long and short legs
Pain in the leg and lower back due to inflammation or sciatica
The human body is a marvelous, mysterious machine. When part of the machine is not working properly, the body will naturally attempt to fix it. If it cannot fix the problem, it finds a work around to compensate for the problem. This can lead to misalignment of the spine and imbalance in the body.
Chiropractic Treatment For Functional Short Leg
When you go to a chiropractor for functional short leg, he or she will do a thorough exam on you including diagnostic tests like MRI and x-ray. Once a diagnosis has been confirmed, the chiropractor will begin what is usually a multi-faceted approach that incorporates spinal alignment, a heel lift, lifestyle change recommendations, and exercises that you can do at home.
The chiropractic adjustments will return the spine to its natural position and bring the body back into balance. Patients will usually experience a dramatic decrease in pain or the pain will go away completely. They will also enjoy increased mobility and flexibility as well and an overall sense of wellness.
Injury Medical Clinic: Athletic Recovery & Rehabilitation
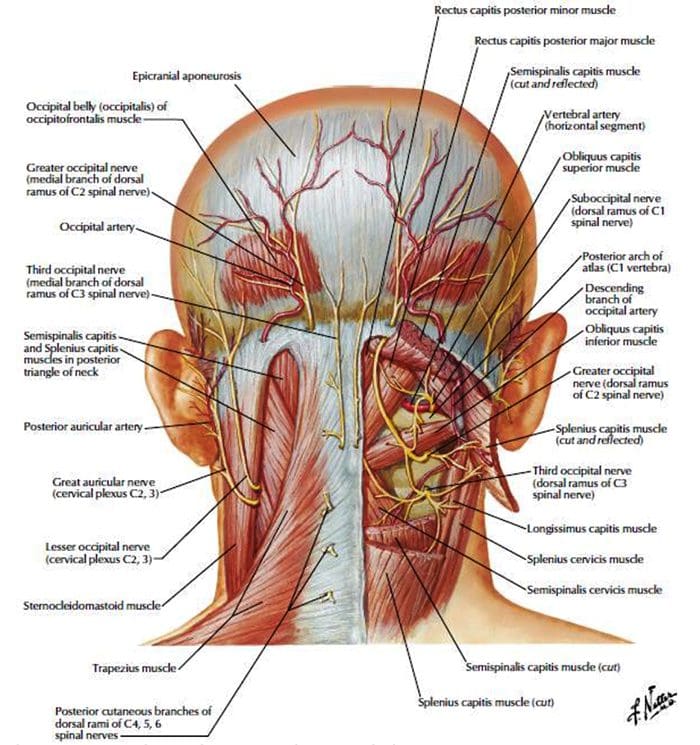
Origin: The most common cause of�migraines/headaches�can relate to neck complications. From spending excessive time looking down at a laptop, desktop, iPad, and even from constant texting, an incorrect posture for extended periods of time can begin to place pressure on the neck and upper back leading to problems that can cause headaches. The majority of these type of headaches occurs as a result of tightness between the shoulder blades, which in turn causes the muscles on the top of the shoulders to also tighten and radiate pain into the head.
Arteriovenous malformations and expanding aneurysms
Lupus cerebritis
Venous sinus thrombosis
Cervical fracture or malformation
Fracture or dislocation
Occipital neuralgia
Vertebral artery dissection
Chiari malformation
Metabolic
Hypoglycemia
Hypercapnea
Carbon monoxide
Anoxia
Anemia
Vitamin A toxicity
Glaucoma
Subarachnoid Hemorrhage
Usually due to ruptured aneurysm
Sudden onset of severe pain
Often vomiting
Patient appears ill
Often nuchal rigidity
Refer for CT and possibly lumbar puncture
Meningitis
Patient appears ill
Fever
Nuchal rigidity (except in elderly and young children)
Refer for lumbar puncture – diagnostic
Neoplasms
Unlikely cause of HA in average patient population
Mild and nonspecific head pain
Worse in the morning
May be elicited by vigorous head shaking
If focal symptoms, seizures, focal neurologic signs, or evidence of increased intracranial pressure are present rule our neoplasm
Subdural Or Epidural Hemorrhage
Due to hypertension, trauma or defects in coagulation
Most often occurs in the context of acute head trauma
Onset of symptoms may be weeks or months after an injury
Differentiate from the common post-concussion headache
Post-Concussive HA may persist for weeks or months after an injury and be accompanied by dizziness or vertigo and mild mental changes, which will all subside
Exquisite tenderness and/or swelling over the temporal or occipital arteries
Evidence of arterial insufficiency in the distribution of branches of the cranial vessels
High ESR
Cervical Region HA
Neck trauma or with symptoms or signs of cervical root or cord compression
Order MR or CT cord compression due to fracture or dislocation
Cervical instability
Order cervical spine x-rays lateral flexion and extension views
Ruling Out Dangerous HA
Rule our history of serious head or neck injury, seizures or focal neurologic symptoms, and infections that may predispose to meningitis or brain abscess
Check for fever
Measure blood pressure (concern if diastolic >120)
Ophthalmoscopic exam
Check neck for rigidity
Auscultate for cranial bruits.
Complete neurologic examination
If needed order complete blood cell count, ESR, cranial or cervical imaging
Episodic Or Chronic?
<15 days per month = Episodic
>15 days per month = Chronic
Migraine HA
Generally due to dilation or distension of cerebral vasculature
Serotonin In Migraine
AKA 5-hydroxytryptamine (5-HT)
Serotonin becomes depleted in migraine episodes
IV 5-HT can stop or reduce severity
Migraine With Aura
History of at least 2 attacks fulfilling the following criteria
One of the following fully reversible aura symptoms:
Visual
Somatic sensory
Speech or language difficulty
Motor
Brain stem
2 of the following 4 characteristics:
1 aura symptom spreads gradually over ?5 min, and/or 2 symptoms occur in succession
Each individual aura symptom lasts 5-60 min
1 aura symptom is unilateral
Aura accompanied or followed in <60 min by headache
Not better accounted for by another ICHD-3 diagnosis, and TIA excluded
Migraine Without Aura
History of at least 5 attacks fulfilling the following criteria:
Headache attacks lasting 4-72 h (untreated or unsuccessfully treated)
Unilateral pain
Pulsing/pounding quality
Moderate to severe pain intensity
Aggravation by or causing avoidance of routine physical activity
During headache nausea and/or sensitivity to light and sound
Not better accounted for by another ICHD-3 diagnosis
Cluster Headache
Severe unilateral orbital, supraorbital and/or temporal pain
�Like an ice pick stabbing me the eye�
Pain lasts 15-180 minutes
At least one of the following on the side of headache:
Conjunctival injection
Facial sweating
Lacrimation
Miosis
Nasal congestion
Ptosis
Rhinorrhea
Eyelid edema
History of similar headaches in the past
Tension Headache
Headache pain accompanied by two of the following:
Pressing/tightening (non-pulsing) quality
�Feels like a band around my head�
Bilateral location
Not aggravated by routine physical activity
Headache should be lacking:
Nausea or vomiting
Photophobia and phonophobia (one or the other may be present)
History of similar headaches in the past
Rebound Headache
Headache occurring on ?15 days a month in a patient with a pre-existing headache disorder
Regular overuse for >3 months of one or more drugs that can be taken for acute and/or symptomatic treatment of headache
Due to medication overuse/withdrawal
Not better accounted for by another ICHD-3 diagnosis
Sources
Alexander G. Reeves, A. & Swenson, R. Disorders of the Nervous System. Dartmouth, 2004.
When the sensory system is affected by injury or disease, the nerves within that system can’t work properly to transmit sensations and feelings into the brain. This frequently contributes to a feeling of numbness, or lack of sensation. However, in certain cases, when this system is damaged, people may experience pain in the affected area.
Neuropathic pain does not start abruptly or resolve quickly; it’s a chronic pain condition which leads to persistent pain symptoms. For most individuals, the intensity of their symptoms may wax and wane throughout the day. Although neuropathic pain is supposed to be related to peripheral nerve health issues, like neuropathy caused by diabetes or spinal stenosis, injuries to the brain or spinal cord may also lead to chronic neuropathic pain. Neuropathic pain is also referred to as nerve pain.
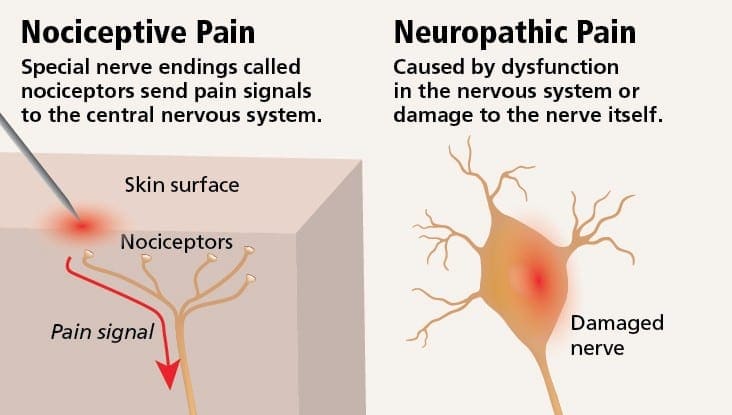
Neuropathic pain may be contrasted to nociceptive pain. Neuropathic pain does not develop to any specific circumstance or outside stimulus, but rather, the symptoms occur simply because the nervous system may not be working accordingly. As a matter of fact, individuals can also experience neuropathic pain even when the aching or injured body part is not actually there. This condition is called phantom limb pain, which may occur in people after they’ve had an amputation.
Nociceptive pain is generally acute and develops in response to a specific circumstance, such as when someone experiences a sudden injury, like hammering a finger with a hammer or stubbing a toe when walking barefoot. Moreover, nociceptive pain tends to go away once the affected site heals. The body contains specialized nerve cells, known as nociceptors, which detect noxious stimuli that could damage the body, such as extreme heat or cold, pressure, pinching, and exposure to chemicals. These warning signals are then passed along the nervous system to the brain, resulting in nociceptive pain.
Contents
What are the Risk Factors for Neuropathic Pain?
Anything that contributes to a lack of function within the sensory nervous system can lead to neuropathic pain. As such, nerve health issues from carpal tunnel syndrome, or similar conditions, can ultimately trigger neuropathic pain. Trauma, resulting in nerve injury, may lead to neuropathic pain. Other conditions which could predispose individuals to developing neuropathic pain include: diabetes, vitamin deficiencies, cancer, HIV, stroke, multiple sclerosis, shingles, and even some cancer treatments.
What are the Causes of Neuropathic Pain?
There are many causes from which individuals may develop neuropathic pain. But on a cellular level, one explanation is an increased release of certain receptors that indicate pain, together with a diminished ability of the nerves to modulate these signals, leads to the sensation of pain originating from the affected region. Additionally, in the spinal cord, the region which exerts painful signs is rearranged with corresponding changes in hormones and loss of normally-functioning mobile bodies. Those alterations result in the perception of pain in the absence of external stimulation. In the brain, the ability to block pain can be affected following an injury, such as stroke or trauma from an injury. As time passes, additional cell damage happens and the feeling of pain continues. Neuropathic pain is also related to diabetes, chronic alcohol intake, certain cancers, vitamin B deficiency, diseases, other nerve-related diseases, toxins, and specific drugs.
What are the Symptoms of Neuropathic Pain?
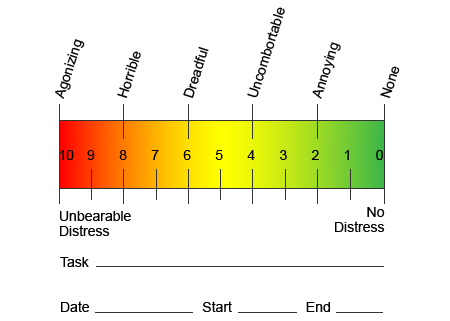
Contrary to other neurological conditions, identification of neuropathic pain can be challenging. However, several, if any, objective signals may be present. Healthcare professionals have to decipher and translate an assortment of words which patients use to describe their pain. Patients may describe their symptoms as sharp, dull, hot, cold, sensitive, itchy, deep, stinging, burning, among a variety of other descriptive terms. Additionally, some patients may experience pain through light touch or pressure.
In an effort to help identify how much pain patients could be undergoing, different scales are often used. Patients are asked to rate their pain according to a visual scale or numerical graph. Many examples of pain scales exist, such as the one demonstrated below. Often, pictures of faces depicting a variety of levels of pain may be helpful when individuals have a difficult time describing the quantity of pain they are experiencing.
Chronic Pain and Mental Health
For many, the impact of chronic pain may not be limited to the pain ; it may also negatively influence their mental state. New research studies conducted by scientists at the Northwestern University in Chicago can explain why individuals who have chronic pain also suffer with seemingly unrelated health issues, such as depression, stress, lack of sleep and difficulty concentrating.
The evaluation demonstrated that people with chronic pain show different regions of the brain which are always active, most specifically, the area associated with mood and attention. This continuous action rewires nerve connections from the brain and leaves chronic pain sufferers at greater risk for psychological problems. Researchers suggested that getting pain signals constantly could result in mental rewiring that adversely affects the mind. The rewiring compels their brains to devote mental resources differently to deal with everyday tasks, from mathematics, to recalling a shopping list, to feeling happy.
The pain-brain connection has been well recorded, at least anecdotally, and lots of healthcare professionals say they’ve seen first-hand the way the patient’s mental state can go downhill when they endure chronic pain. Misconceptions about the pain-brain connection may have emerged from a lack of evidence that pain has a measurable, lasting influence on the brain. Researchers expect that with additional research into the mechanisms of how chronic pain makes people more susceptible to mood disorders, people are going to have the ability to better manage their overall well-being.
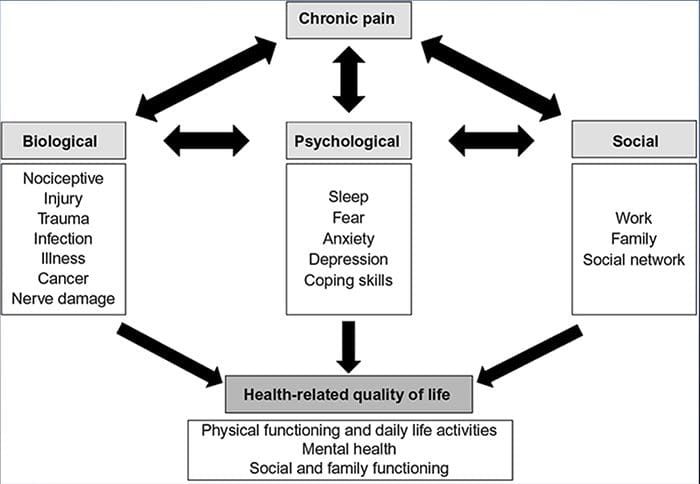
Culture and Chronic Pain
Many things contribute to the way we experience and express pain, however, it has also been recently suggested by researchers that culture relates directly into the expression of pain. Our upbringing and societal values affect how we express pain and also its own nature, intensity and length. However, these variables aren’t as obvious as socio-psychological values, such as age and sex.
Research states that chronic pain is a multifaceted process and the concurrent interplay between pathophysiology, cognitive, affective, behavioral and sociocultural factors summate to what is referred to as the chronic pain experience. It’s emerged that chronic pain is experienced differently among patients of varied cultures and ethnicities.
Some cultures encourage the expression of pain, particularly in the southern Mediterranean and Middle East. Other individuals suppress it, as in the many lessons to our kids about behaving bravely and not crying. Pain is recognized as part of the human experience. We are apt to assume that communication about pain will seamlessly cross cultural boundaries. But people in pain are subject to the manners their civilizations have trained them to experience and express pain.
Both individuals in pain and healthcare professionals experience difficulties communicating pain across ethnic borders. In a matter like pain, where effective communication can have far-reaching implications for medical care, quality of life and potentially survival, the role of culture in pain communicating remains under-evaluated. Persistent pain is a multidimensional, a composite encounter formed by interweaving and co-influencing biological and psychosocial factors. Knowing the culmination of these factors is critical to understanding the differences of its manifestation and management.
How is Neuropathic Pain Diagnosed?
The diagnosis of neuropathic pain relies upon additional evaluation of an individual’s history. If underlying nerve damage is suspected, then analysis of the nerves together with testing may be justified. The most common means to assess whether or not a nerve is injured is using electrodiagnostic medicine. This medical subspecialty utilizes techniques of nerve conduction studies with electromyelography (NCS/EMG). Clinical evaluation may show evidence of loss of work, and can include evaluation of light touch, the capacity to differentiate sharp out of dull pain and the ability to discern temperature, as well as the evaluation of vibration.
After a thorough clinical examination is completed, the electrodiagnostic analysis could be planned. These studies are conducted by specially trained neurologist and physiatrists. If neuropathy is suspected, a hunt for reversible causes ought to be accomplished. This can include blood function for vitamin deficiencies or thyroid problems, and imaging studies to exclude a structural lesion affecting the spinal cord. Depending on the results of this testing, there might be a means to decrease the intensity of the neuropathy and possibly reduce the pain that a patient is undergoing.
Regrettably, in many conditions, even good control of the underlying cause of the neuropathy can’t reverse the neuropathic pain. This is commonly seen in patients with diabetic neuropathy. In rare instances, there may be signs of changes in the skin and hair growth pattern in an affected region. These alterations may be associated with changes in perspiration. If present, these changes can help identify the likely presence of neuropathic pain related to a condition known as complex regional pain syndrome.
Dr. Alex Jimenez’s Insight
Neuropathic pain is a chronic pain condition which is generally associated with direct damage or injury to the nervous system or nerves. This type of pain is different from nociceptive pain, or the typical sensation of pain. Nociceptive pain is an acute or sudden sensation of pain which causes the nervous system to send signals of pain immediately after the trauma occurred. With neuropathic pain, however, patients may experience shooting, burning pain without any direct damage or injury. Understanding the possible causes of the patient’s neuropathic pain versus any other type of pain, can help healthcare professionals find better ways to treat chronic pain conditions.
What is the Treatment for Neuropathic Pain?
Various medicines are used in an attempt to treat neuropathic pain. The majority of these drugs are utilized off-label, which means that the medicine was approved by the FDA to treat different conditions and was then recognized as being advantageous to treat neuropathic pain. Tricyclic antidepressants, such as amitriptyline, nortriptyline and desipramine, have been prescribed for management of neuropathic pain for several years.
Some individuals find that these may be very effective in giving them relief. Other kinds of antidepressants have been shown to offer some relief. Selective serotonin reuptake inhibitors, or SSRIs, such as paroxetine and citalopram, and other antidepressants , such as venlafaxine and bupropion, have been utilized in certain patients. Another frequent treatment of neuropathic pain incorporates antiseizure medications, including carbamazepine, phenytoin, gabapentin, lamotrigine, and others.
In acute cases of painful neuropathy which don’t respond to first-line brokers, drugs typically utilized to treat heart arrhythmias may be of some benefit; however, these can lead to significant side effects and often have to be monitored closely. Medications applied directly to the skin can offer modest to perceptible benefit for some patients. The forms commonly used include lidocaine (in patch or gel type) or capsaicin.
Treating neuropathic pain is dependent on the underlying cause. If the cause is reversible, then the peripheral nerves can regenerate and the pain will abate; nonetheless, this reduction in pain may take several months to years. Several other alternative treatment options, including chiropractic care and physical therapy, may also be utilized in order to help relieve tension and stress along the nerves, ultimately helping to improve painful symptoms.
What is the Prognosis for Neuropathic Pain?
Many individuals with neuropathic pain are able to get some measure of aid, even when their pain persists. Although neuropathic pain isn’t dangerous to a patient, the presence of chronic pain can negatively affect quality of life. Patients with chronic nerve pain might suffer from sleep deprivation or mood disorders, including depression, anxiety and stress, as previously mentioned above. Because of the inherent alopecia and lack of sensory feedback, patients are at risk of developing injury or infection or unknowingly causing an escalation of a present injury. Therefore, it’s essential to seek immediate medical attention and follow specific guidelines directed by a healthcare professional for safety and caution.
Can Neuropathic Pain be Prevented?
The best way to prevent neuropathic pain is to avoid the development or progression of neuropathy. Monitoring and changing lifestyle options, including restricting the use of alcohol and tobacco; keeping a healthy weight to lower the chance of diabetes, degenerative joint disease, or stroke; and having great ergonomic form at work or when practicing hobbies to lower the risk of repetitive stress injury are strategies to decrease the probability of developing neuropathy and potential neuropathic pain. Make sure to seek immediate medical attention in the case of any symptoms associated with neuropathic pain in order to proceed with the most appropriate treatment approach.�The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Back Pain
Back pain is one of the most prevalent causes for disability and missed days at work worldwide. As a matter of fact, back pain has been attributed as the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience some type of back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
Tension headaches are the most prevalent types of headaches, occurring more often in women than in men. Research shows that 48 percent of women and 38 percent of men suffer from tension headaches.
Each year, patients spend more than $2 billion on over the counter headache medications. In fact, people spend a lot of money and effort seeking remedies for headaches. From prescription medication to over the counter drugs to alternative headache treatments like meditation, acupuncture, and chiropractic.
In fact, chiropractic is a proven treatment for these types headaches, but there is more to it than just adjustments. Chiropractic offers a whole body approach to treatment that can not only relieve the pain of these headaches, but help prevent them as well.
Contents
What Are Tension Headaches?
The most common type of headache is the tension headache which is described as pain ranging from mild to moderate that feels like a tight band is wrapped around the head. While stress can be a factor in the cause of these headaches, it still isn�t well understood how these headaches originate. Symptoms of a tension headache include:
Aching, dull pain in the head
Sensation of pressure or tightness on the back and sides of the head or across the forehead
Tenderness in the shoulder muscles, neck, and scalp
There are two categories of tension headaches: chronic and episodic. There are two primary factors that identify each type. The length of the headache and the frequency can help you determine which type of tension headache you have.
Chronic Tension Headaches
Length of Headache � hours and can be continuous
Frequency of Headache � occur 15 days or more a month for three or more months
Episodic Tension Headaches
Length of Headache – half hour to a week
Frequency of Headache � occur less than 15 days a month for three or more months
There are two primary risk factors for tension headaches:
Women � Research shows that nearly 90 percent of women will experience tension headaches throughout the course of their life. Only 70 percent of men will experience tension headaches in their lifetime.
Middle Age � Tension headaches increase as people approach 40 and peak at middle age, or when a person is in their 40s. However, anyone can get a tension headache, regardless of age.
Lifestyle Changes To Treat Tension Headaches
A chiropractor can treat tension headaches through traditional spinal manipulation and adjustments, but they also provide advice on lifestyle and nutrition. Several things that your chiropractor may suggest include applying heat or ice to the area around your neck, shoulders, or head. A warm bath or shower may also help.
Stress management is another way that you can learn to manage and prevent tension headaches. This is typically a combination of minimizing stress in your life and learning relaxation techniques. Your chiropractor may also help you improve your posture. Poor posture is a very common contributing factor for many types of headaches.
Chiropractic for Tension Headaches
Your Doctor of Chiropractic will sit down with you to discuss your history, including your headaches. He or she will conduct diagnostic tests including x-rays, MRIs and other to determine if there are underlying causes for your headaches. They will recommend various lifestyle changes including dietary changes and exercises that you can do.
Your doctor may also perform chiropractic adjustments, or spinal manipulation which will help return the body to proper balance, improving spinal function and alleviating stress on the body and system. This helps to relieve pain as an immediate treatment, but when performed consistently, chiropractic can also help prevent tension headaches, allowing you to live pain free.
Injury Medical Clinic: Migraine Treatment & Recovery
Facet syndrome, also called facet joint sprain or facet joint syndrome is a common cause of back pain. There are many treatments that are used, but most mainstream medical treatments involve pain medication which can have undesirable side effects and may even lead to addiction.
Chiropractic is a proven, reliable treatment for relieving the pain and discomfort of facet syndrome. It helps restore mobility and flexibility while providing pain relief. Some patient notice significant relief from the pain and inflammation of this condition with chiropractic treatment and it is often recommended to facet syndrome patients.
Contents
What Is Facet Syndrome?
Facet syndrome is the result of an injury to the facet joints. Zygapophyseal joints, or facet joints reside at the posterior of the spine. At each level there are two joints, one on each side of the spine.
The facet joints are enclosed in a joint capsule. They are synovial joints so the capsule contains synovial fluid. The surface of the joints is covered with hyaline cartilage.
Other joints, such as the ankle, contain this type of cartilage covering. These joints are constructed in this way due to their role in the body � to control excessive or extensive movement. This would include hyper extension and rotation. By doing so they help to stabilize the spine.
Facet syndrome occurs when there is an injury to the facet joints. There are numerous causes, but basically, it is a sprain that is brought about by excessive movement.
This damages the joint capsule and the result is inflammation, swelling, and pain. The pain triggers a protective mechanism in the spine called a reactive muscle spasm which causes great difficulty in moving comfortable and severe, sudden pain.
It is difficult to rest the back because of its integral function in supporting the entire body. A severe sprain can take weeks to heal, typically 2 to 6 weeks. This means that the pain and lack of mobility is impacting you on a daily basis. It can be very difficult to pursue day to day activities and enjoy your typical lifestyle.
Chiropractic For Facet Syndrome
Chiropractic care is a proven, effective treatment for facet syndrome. When you visit your chiropractor, he or she will conduct a physical exam, discuss your medical history, and may send you for diagnostic tests like x-rays and MRIs. Once they have a clear picture of your condition and a facet syndrome diagnosis has been confirmed, they will discuss with you a recommended course of treatment that may include:
Exercise � they will recommend specific exercises to help relieve the pain and strengthen the muscles in the back so that they can better support the spine.
Posture � posture is extremely important in spinal health and overall wellness. Your chiropractor will help you achieve good, healthy posture and give you exercises to do at home to help you maintain good posture and retrain your body to have better posture.
Heat or cold therapy � heat wraps and hot showers or ice packs and cold pad applications may be recommended to help control pain.
Changes in activities � you may be advised to take frequent breaks if you sit at a desk all day or to shorten your commute. There may be some activities that you won�t be able to do for a while � or won�t be able to do for long periods of time until your back heals.
Chiropractic treatment � spinal manipulation is the most common chiropractic treatment for facet syndrome. Your chiropractor may include other types of treatments though, depending on your specific condition and lifestyle.
Chiropractic is a safe, effective, non-invasive, and drug free way to treat facet syndrome, relieve back pain, and help you regain your mobility. Talk to your chiropractor about your treatment options for facet syndrome.
Injury Medical Clinic: Back Pain Care & Treatments
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine