Chondromalacia patellae, also referred to as runner’s knee, is a health issue in which the cartilage beneath the patella,�or kneecap, becomes soft�and ultimately degenerates. This problem is prevalent among young athletes,�however, it may also develop in older adults who suffer from arthritis of the knee.
Sports injuries like chondromalacia patellae are frequently regarded as an overuse injury. Taking some time off from participating in physical activities and exercise may produce superior outcomes. In the instance that the individual’s health issues are due to improper knee alignment, rest may not offer pain relief. Symptoms of runner’s knee include knee pain and grinding sensations.
Contents
What Causes Chondromalacia Patellae?
The kneecap,�or the patella, is generally found through the front of the knee joint. If you bend your knee, the rear end of your kneecap slips over the cartilage of your femur, or thigh bone, at the knee. Complex soft tissues, such as tendons and ligaments, connect the kneecap to the shinbone and thigh muscle. Chondromalacia patellae�can commonly occur when any of these structures fail to move accordingly, causing the kneecap to rub against the�thigh bone. Poor kneecap motion may result from:
Misalignment due to a congenital health issue
Weakened hamstrings and quadriceps, or the muscles of the thighs
Muscle imbalance between the adductors and abductors, the muscles on the inside and outside of the thighs
Continuous pressure to the knee joints from certain physical activities and exercise like running, skiing, or jumping
a direct blow or injury for a kneecap
Who is at Risk for Chondromalacia Patellae?
Below is an assortment of factors which may increase an individual’s chance for developing chondromalacia patellae.
Age
Adolescents and young adults have the highest risk for this health issue. During growth spurts, bones and muscles can often grow too rapidly, causing short-term muscle and bone imbalances in the human body.
Gender
Females are more likely than males to develop runner’s knee, because women generally possess less muscle mass than men. This may result in abnormal knee placement, and more lateral pressure on the kneecap.
Flat Feet
Individuals who have flat feet can add more strain to the knee joints as compared to individuals who have higher arches.
Past Injury
Previous injuries to the kneecap, including a dislocation, can raise the chance of developing chondromalacia patellae.
Increased Physical Activity
Increased levels of physical activities and exercise can place pressure on the knee joints, which may raise the risk for knee issues.
Arthritis
Runner’s knee may also be an indication of arthritis, a well-known problem causing pain and inflammation to the tissue and joint. Swelling can prevent the proper function of the knee and its complex structures.
What are the Symptoms of Chondromalacia Patellae?
Chondromalacia patellae will generally present as pain in the knee, called patellofemoral pain, accompanied by sensations of cracking or grinding when extending or bending the knee. Pain may worsen after sitting for an extended period of time or through physical activities and exercises that apply intense pressure for your knees, like standing. It’s essential for the individual to seek immediate medical attention if the symptoms of chondromalacia patellae, or runner’s knee, do not resolve on their own.
Diagnosis and Chondromalacia Patellae Grading
A healthcare professional will search for areas of pain and inflammation on the knee. They might also look at the way the kneecap aligns with the thigh bone. A misalignment may indicate the presence of chondromalacia patellae. The doctor may also perform a series of evaluations to ascertain the presence of this health issue.
The healthcare professional may also ask for any of the following tests to help diagnose chondromalacia patellae, including:�x-rays to show bone damage or misalignments or arthritis; magnetic resonance imaging, or MRI, to see cartilage wear and tear; and�arthroscopic examination, a minimally invasive procedure which involves inserting an endoscope and camera inside the knee joint.
Grading
There are four levels of chondromalacia patellae, ranging from grade 1 to 4, which characterize the level of the patient’s runner’s knee. Grade 1 is considered mild while grade�4 is considered severe.
Grade 1 indicates the softening of the cartilage in the knee region.
Grade 2 suggests a softening of the cartilage followed by abnormal surface features, the start of degeneration.
Grade 3 reveals the thinning of the cartilage together with active degeneration of the complex soft tissues of the knee.
Grade 4, or the most severe grade, demonstrates exposure of the bone through a substantial part of the cartilage Bone exposure means that bone-to-bone rubbing is most likely happening in the knee.
What is the Treatment for Chondromalacia Patellae?
The goal of treatment for chondromalacia patellae is to first decrease the strain being placed on the kneecap, or patella, and the femur, or thigh bone. Rest and the use of ice and heat agains the affected knee joint is generally the first line of treatment. The cartilage damage associated with runner’s knee may often repair itself with these remedies along.
Moreover, the healthcare professional may prescribe anti-inflammatory drugs and/or medications, such as ibuprofen, to decrease pain and inflammation around the knee joint. When tenderness, swelling, and pain persist, the following treatment options could be explored. As mentioned above, individuals should seek immediate medical attention if symptoms persist.�
Chiropractic Care
Chiropractic care is a safe and effective, alternative treatment option which focuses on the diagnosis, treatment, and prevention of a variety of injuries and/or conditions associated with the musculoskeletal and nervous system, including chondromalacia patellae. Occasionally,�knee pain may originate due to spinal misalignments or subluxations. A doctor of chiropractic, or chiropractor, will use spinal adjustments and manual manipulations to carefully restore the natural integrity of the spine.�
Furthermore, a chiropractor may also recommend a series of lifestyle modifications, including nutritional advice and a physical activity or exercise guide to help ease symptoms associated with chondromalacia patellae. Rehabilitation may also focus on�strengthening the quadriceps, hamstrings, adductors, and abductors to improve muscular strength, flexibility, and mobility. The purpos of muscle balance is also to assist in preventing knee misalignment, among other complications.
Surgery
Arthroscopic surgery might be required to inspect the joint and ascertain whether there is a misalignment of the knee. This operation involves inserting a camera in the knee joint through a very small incision. A surgical procedure can repair the issue. One�common process is a lateral release. This surgery involves cutting a number of the ligaments to release tension and permit for more movement. Additional surgery may entail implanting the back of the kneecap, inserting a cartilage graft, or transferring the thigh muscle.
�
Chondromalacia patellae is characterized as the inflammation of the underside of the patella, or kneecap, caused by the softening of the cartilage surrounding the soft tissues of the knee joint. This well-known health issue is generally caused due to sports injuries in young athletes, although chondromalacia patellae may also occur in older adults with arthritis in the knee. Chiropractic care can help restore strength and balance to the knee joint and its surrounding soft tissues.
Dr. Alex Jimenez D.C., C.C.S.T. Insight
How to Prevent Chondromalacia Patellae
A patient can ultimately lower their chance of developing runner’s knee, or chondromalacia patellae, by:�
Avoiding repeated stress on the knees. In case the individual needs to spend time on their knees, they could wear kneepads.
Produce muscle balance by strengthening the quadriceps, hamstrings, abductors, and adductors.
Wear shoe inserts that correct flat feet. This may reduce the amount of pressure being placed on the knees to realign the kneecap, or patella.
Keeping a healthy body weight can also help prevent chondromalacia patellae. Following the nutritional advice and guidance from a healthcare profesional can help promote a healthy body weight. The scope of our information is limited to chiropractic and spinal health issues. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topic Discussion: Relieving Knee Pain without Surgery
Knee pain is a well-known symptom which can occur due to a variety of knee injuries and/or conditions, including�sports injuries. The knee is one of the most complex joints in the human body as it is made-up of the intersection of four bones, four ligaments, various tendons, two menisci, and cartilage. According to the American Academy of Family Physicians, the most common causes of knee pain include patellar subluxation, patellar tendinitis or jumper’s knee, and Osgood-Schlatter disease. Although knee pain is most likely to occur in people over 60 years old, knee pain can also occur in children and adolescents. Knee pain can be treated at home following the RICE methods, however, severe knee injuries may require immediate medical attention, including chiropractic care.
Result from valgus or varus stress with or w/o axial loading
Associated with periarticular soft tissues injury
High-stress injury m/c due to jumps falls and axial loading, often with the splitting of the tibial plateau. Men>women. Patients are in their 30s
Low impact or no trauma in patients with osteoporosis d/t insufficiency fractures
Impaction injury is more common with depression of tibial plateau. Women>men. Patients are in their 70s
Contents
Lateral Tibial Plateau Fractures More Common
Functional anatomy plays a significant role
60% of weight bearing is by the medial plateau
The medial plateau is more concave
Lateral plateau is slightly higher and more convex. Valgus stress impacts lateral plateau.
Tibial plateau fractures considered intra-articular and prone to delayed healing, non-union, meniscal injury (m/c lateral) ACL tear, secondary OA. Other complications: compartment syndrome, vascular injury.
Management: operative in many cases especially if >3-mm step-off at the plateau
If medial plateau or bicondylar Fxs present, ORIF will be required.
Imaging Plays A Crucial Role
Begins with x-radiography. X-radiography may not reveal the complexity and extent of this injury.
CT scanning w/o contrast will further delineate fracture complexity and pre-operative planning
MR imaging may be considered to evaluate for internal derangement: meniscal, ACL injuries.
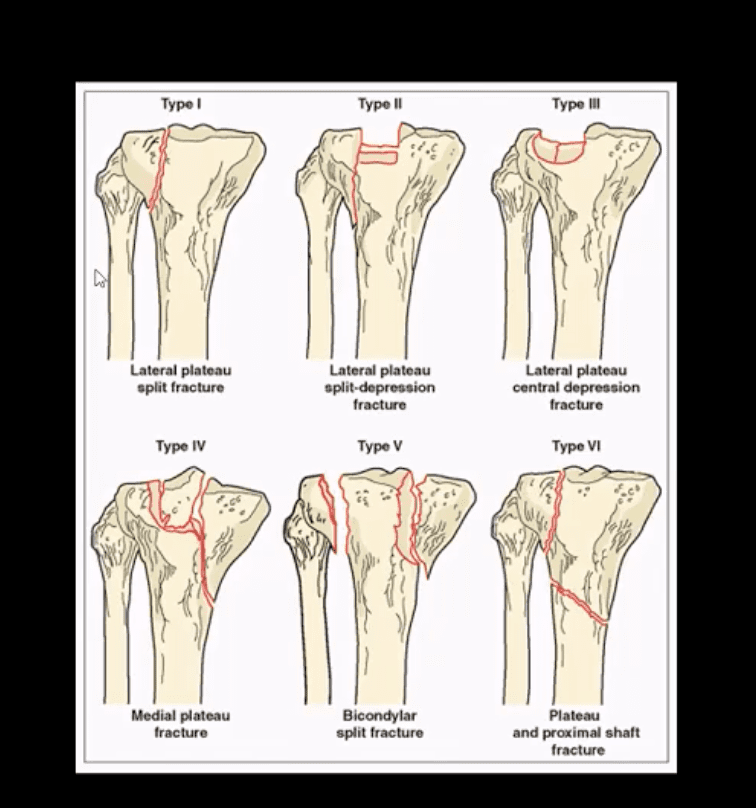
Shatzke classification may help to evaluate the complexity of this injury
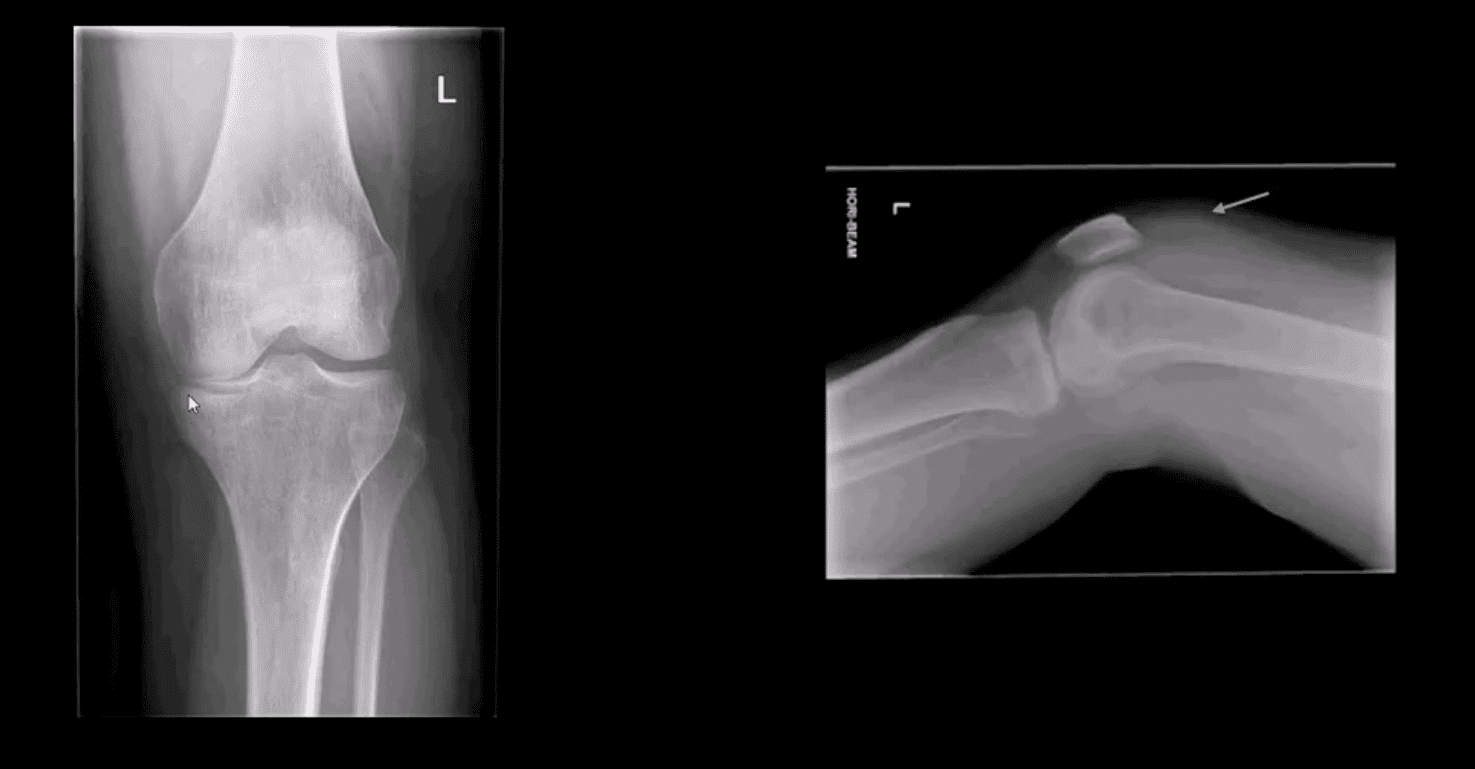
Key Diagnostic Sign
AP and lateral horizontal beam (cross table) left knee radiograph. Note subtle depression of the lateral plateau manifested by the lateral plateau appearing at the same level or lower as the medial. A critical diagnostic sign is the presence of fat-blood-interphase or FBI sign on cross-table lateral (above arrow) indicating intra-articular knee fracture
Lipohemarthorosis aka FBI Sign
Can be detected by radiography, CT or MR imaging
FBI sign is a reliable secondary radiographic sign of intra-articular knee fractures, regardless of how small they are
Mechanism: fracture results with acute hemarthrosis
Hemarthrosis will also occur w/o Fx. However, Fx will result with a fatty marrow being released into the joint cavity. Fat is a less dense medium (lighter) and will appear on the top of the hemorrhage if the patient is held in the supine position for 5-10-minutes before the cross-table radiograph is taken
FBI sign confirms the intra-articular Fx.
ACL/PCL, meniscal tears will not result in FBI sign
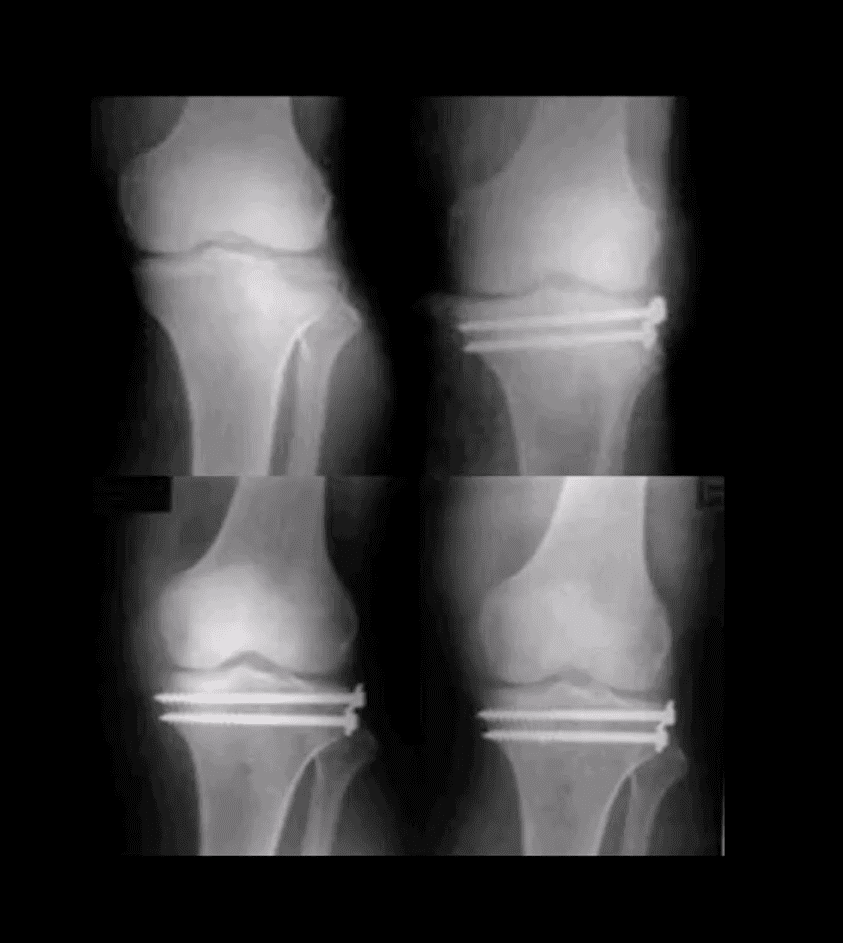
Lateral Tibial Plateau Fx
Lateral tibial plateau Fx that was managed operatively
Most common complication: premature secondary OA
More complex injuries may result in more extensive operative care
Knee Internal Derangement
Acute or chronic injuries of meniscal fibrocartilages and ligamentous restraints
Tears of the ACL and posterior horn of the medial meniscus are the most common
Acute ACL tears, however, often result with a lateral meniscus tear
Acute ACL tear may occur as a combined injury of the ACL, MCL, and medial meniscus
Functional anatomy: ACL prevents anterior displacement of the tibia and secondary varus stress
MCL functions together with ACL in resisting external rotation of the tibia especially when the foot is planted (closed chain position)
MCL is firmly attached to the medial meniscus, explaining the classic triad of ACL, MCL and medial meniscal tear (O’Donahue terrible triad)
Cruciate ligaments (ACL/PCL) are intra-articular but extra-synovial. Less likely to be torn in closed pack position (full extension). When all articular facets of tibia and femur are in full contact, the ACL/PCL are at least tension and stable
When the knee is flexed 20-30-degrees or more ACL is taut and remains unstable
ACL is a significant mechanoreceptor that feeds the info to CNS about the joint position. Thus the majority of previous ACL tears will lead to some degree of knee instability
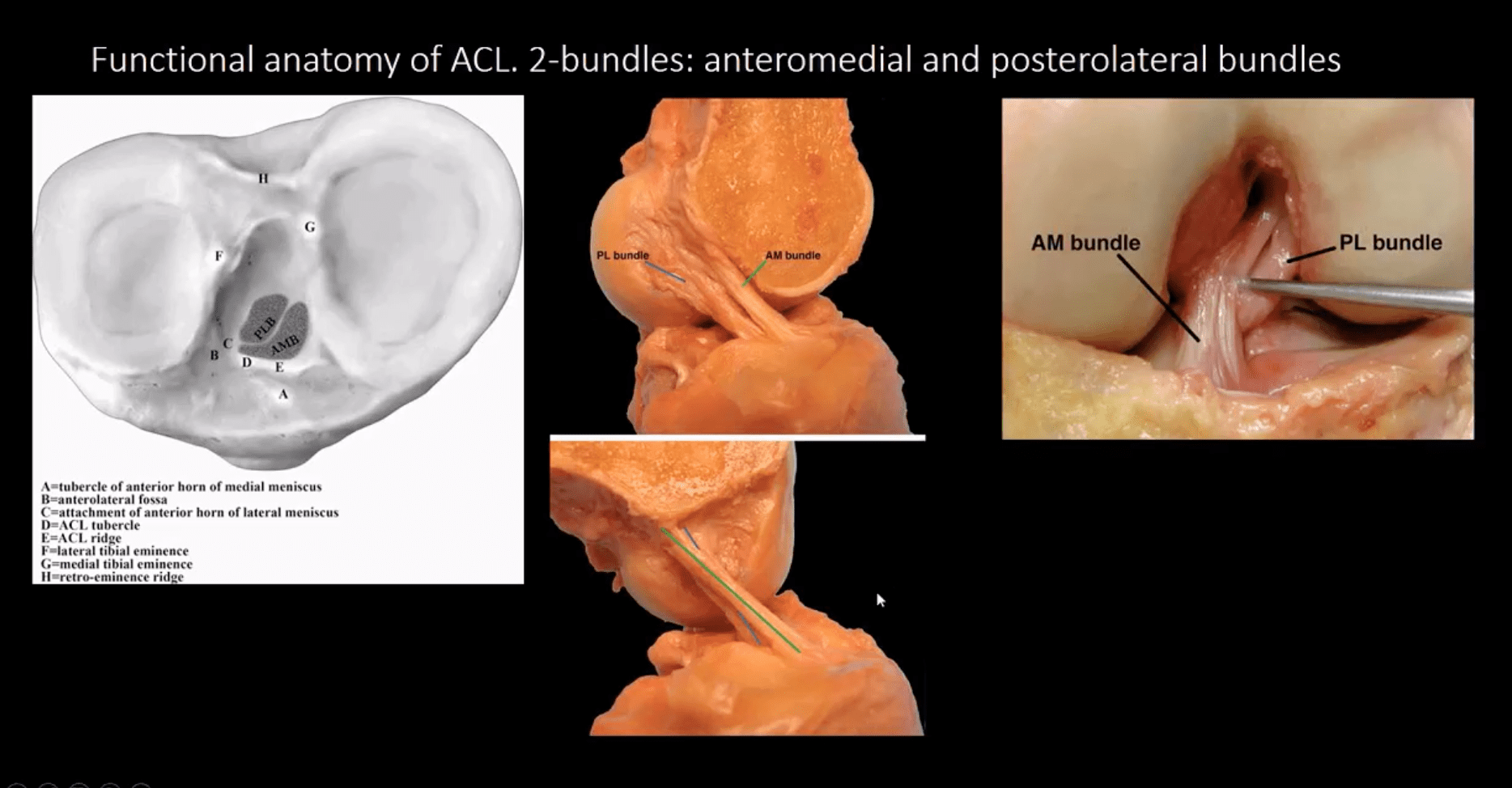
Functional Anatomy of ACL
Diagnosis of ACL Tear
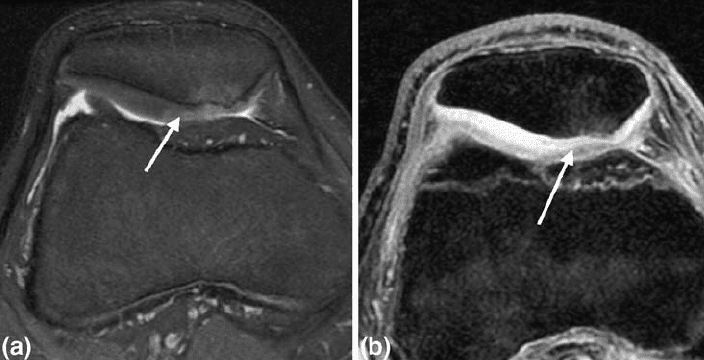
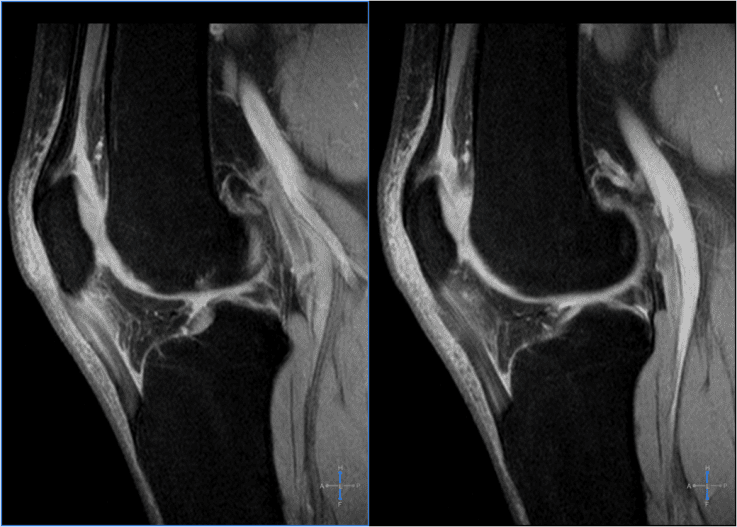
Diagnosis of ACL tear requires MR imaging
Concerns exist of not only ligamentous injuries but injuries to the articular cartilage and menisci.
Most vendors will perform at least: one T1 WI in coronal or sagittal planes. Sagittal and coronal Proton-density slices to evaluate cartilaginous structures. Fast spin-echo sagittal, axial and coronal T2 fat-saturated or sagittal and coronal STIR images are crucial to demonstrate edema within the substance of knee ligaments
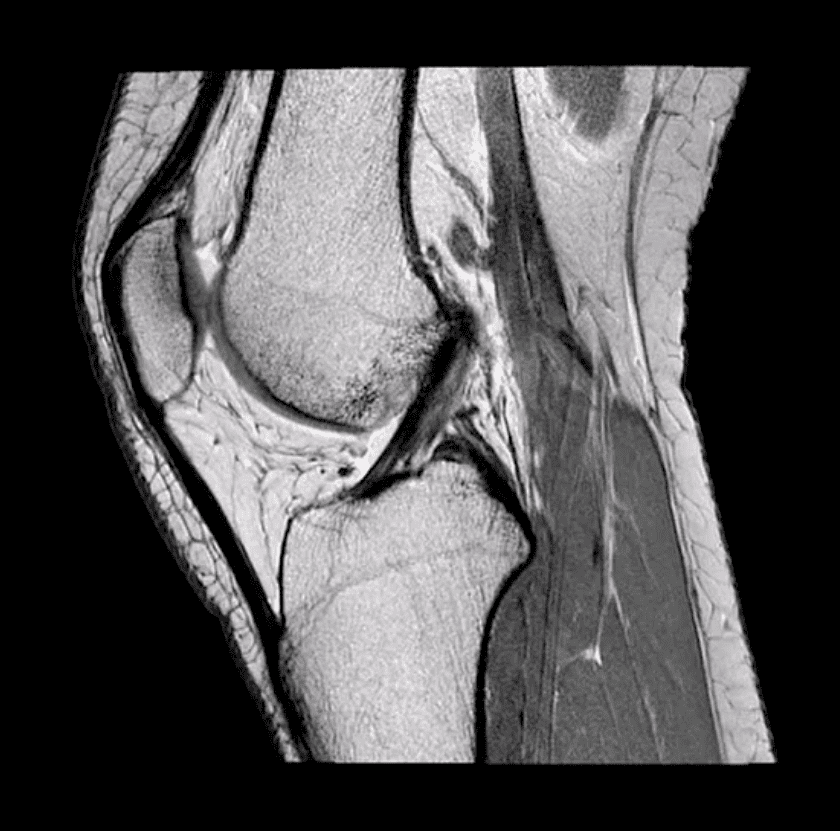
ACL is aligned along the Blumensaat line or oblique line corresponding the intercondylar roof of Femoral condyles. Lack of such alignment by the ACL is significant for ACL tear
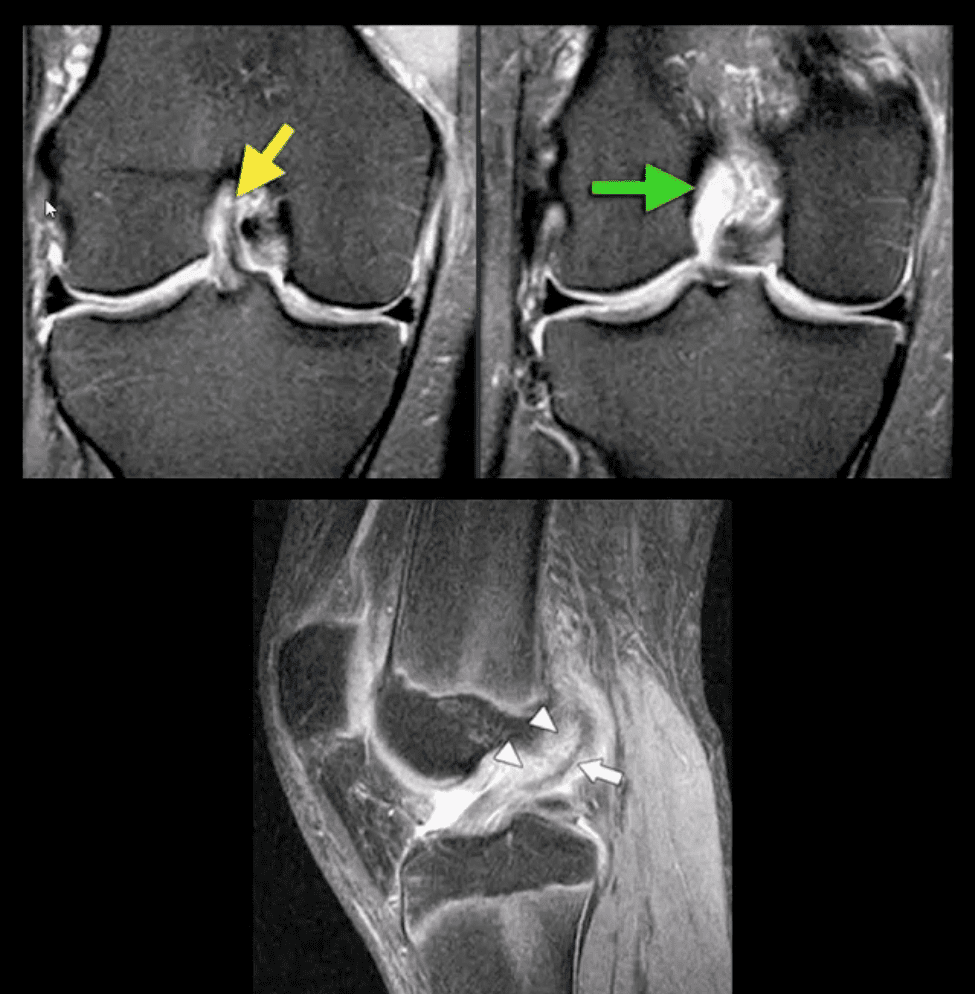
Imaging Dx of Internal Derangement
MRI shows 78-100% sensitivity and 78-100% specificity
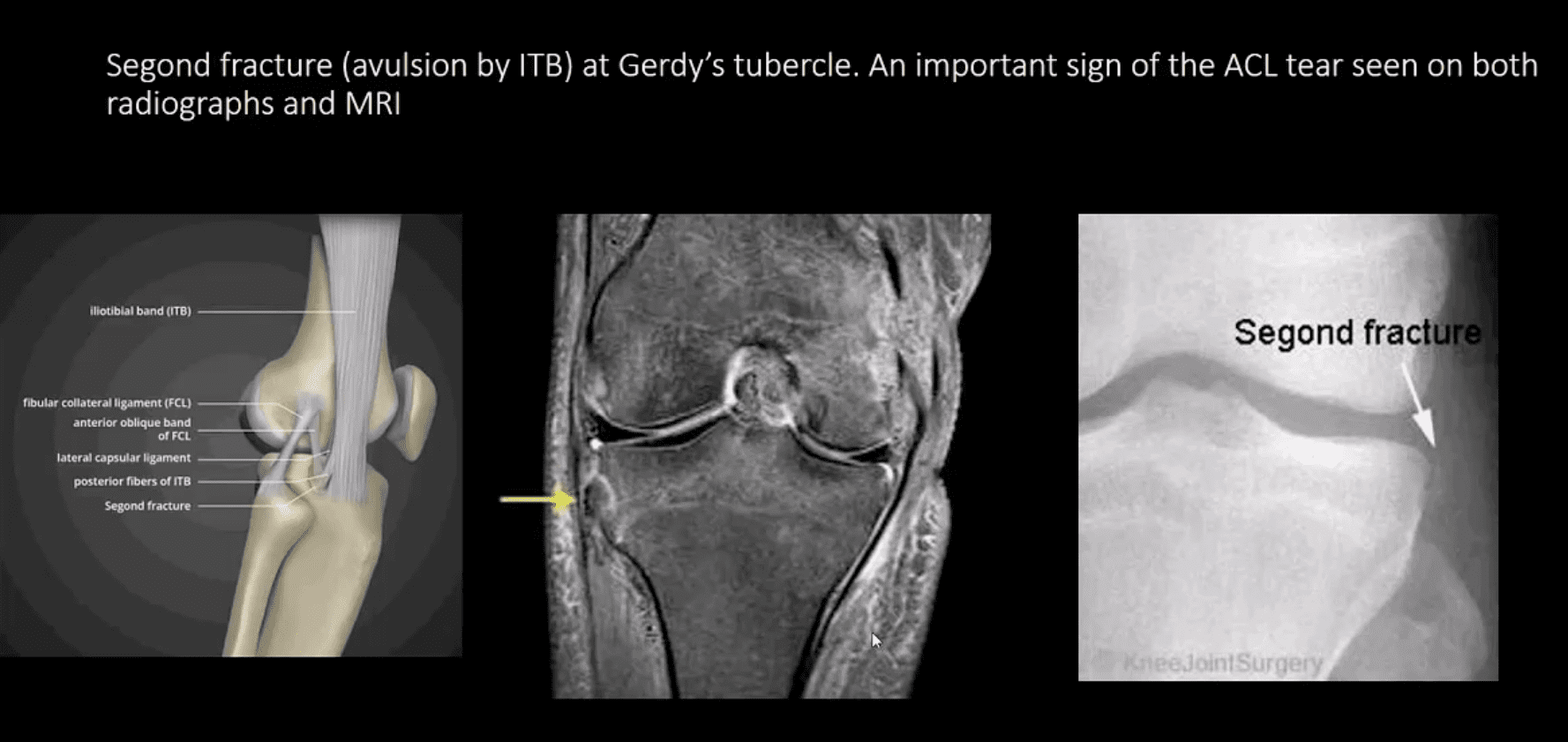
Primary signs of ACL tear: non-visualization of ACL (above green arrow), loss of its axis along the Blumensaat line (above triangle heads), wavy appearance and substance tear (above white arrow) or edema and cloud-like indistinctness (above yellow arrow)
Reliable Secondary Signs of ACL Tear
May be observed on the radiographs and MRI
Segond avulsion fracture (80% specificity for ACL tear) (next slide)
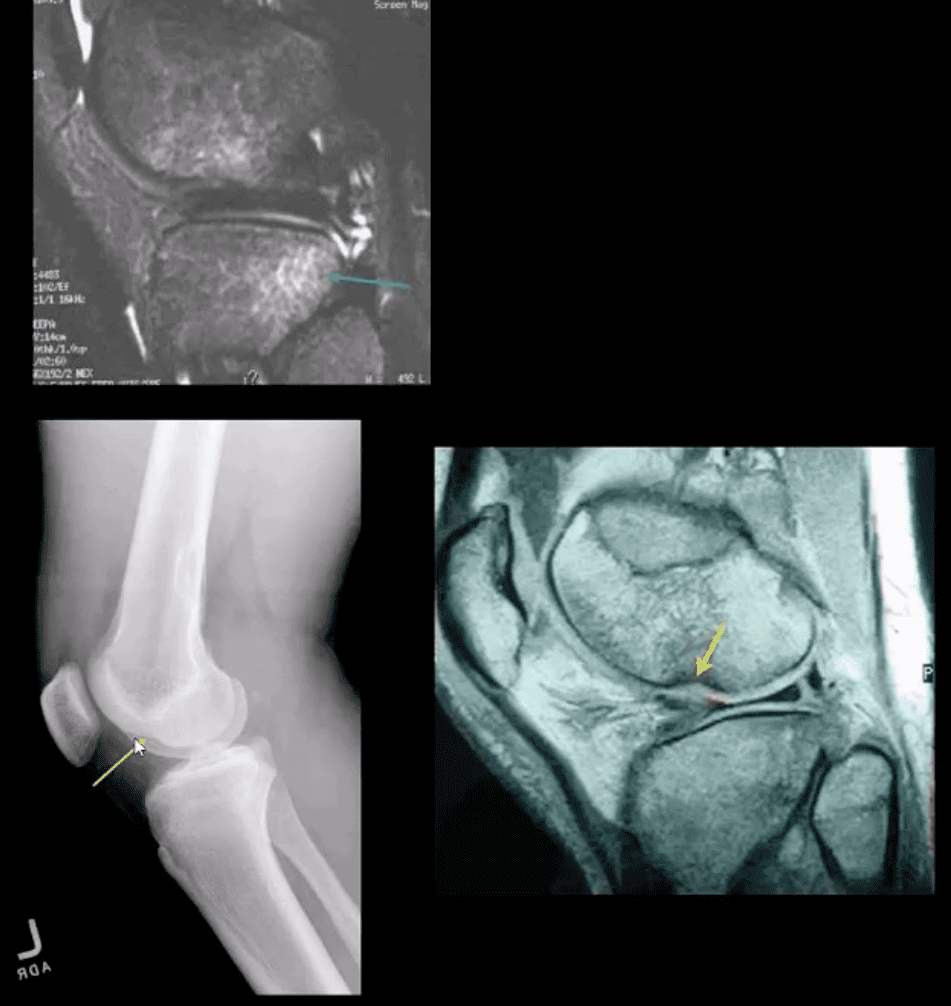
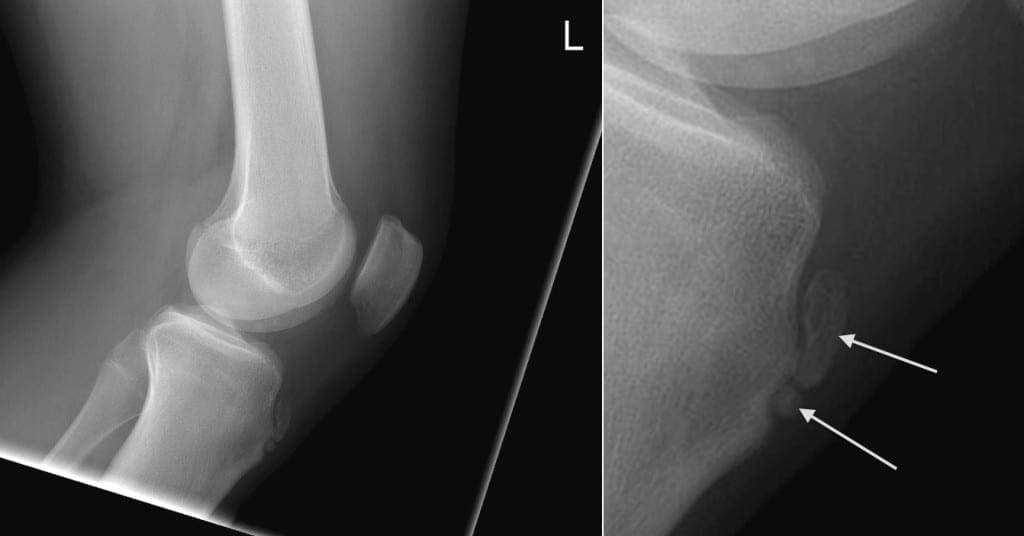
Deep femoral notch sign indicating osteochondral fracture (above bottom images) and
Pivot -shift bone marrow edema in the posterolateral tibial condyle d/t external rotation and often valgus impact by the lateral femoral condyles (above top image)
Segond Fracture (Avulsion by ITB)
Segond fracture at Gerdy’s tubercle. A vital sign of the ACL tear seen on both radiographs and MRI
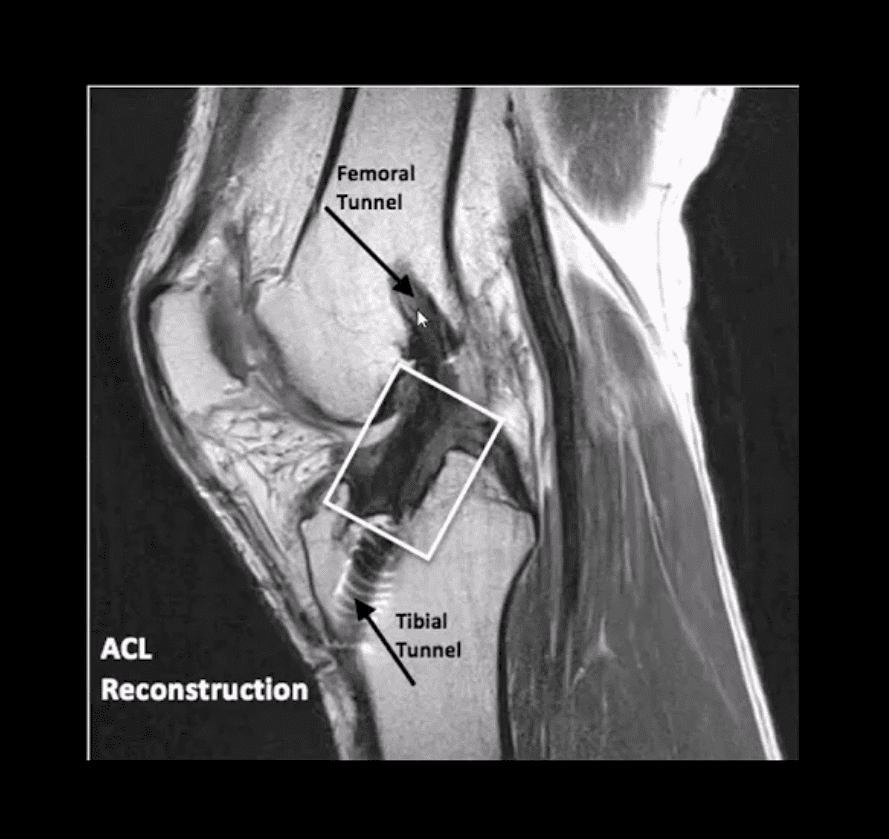
Management of ACL Tears
In acute cases, usually operative using cadaveric or autograft (patella ligament or hamstring) ACL reconstruction
Complications: graft tear, instability and premature DJD, joint stiffness d/t lack of postoperative rehab or gaft shortening. More rare, infection, a formation of intraosseous synovial cysts, etc.
Have you ever had a pain in the neck? And your kids or significant other don’t count. If you’ve ever had a stiff, sore neck, then you’ve more than likely experienced cervicalgia. You’re not alone. The American Osteopathic Association estimates that more than 25% of Americans have experienced or chronically experience neck pain. Neck pain is one of the primary causes of chronic pain, ranking number three behind knee pain (number two) and back pain (number one). Chronic pain affects around 65% of people in the United States, ranging in age 18 to 34. They either have experienced it firsthand or care for someone who has recently experienced it. That number increases as the population ages.
It is also worth noting that most doctors prescribe pain medications, but more than 33% of patients with chronic pain won’t take them because they are afraid of becoming addicted.
Contents
What is Cervicalgia?
Cervicalgia is a blanket term used to describe neck pain. It can range from a simple crick in the neck to severe pain that prevents you from turning your head.
Knowing the term for the pain, though, does not help when it comes to treatment because treatment lies in the cause of the pain. It can become quite complex because there are so many causes for the pain. Sometimes the cause itself must be eliminated before the treatments for the pain can be effective.
What are the Causes of Cervicalgia?
The causes of cervicalgia are vast and varied. A patient who sits at their desk for too long or sleeps in a poor position can develop neck pain.
Injuries such as sports injuries and whiplash fall at the more severe end of the spectrum. Even simple gravity can be a culprit.
The human head can weigh as much as 10 pounds, sometimes even more, and the neck is tasked with keeping it upright. Just the action of fighting gravity and keeping the head erect for long periods of time (like all day) can cause the neck muscles to become strained and fatigued. This can also cause neck injuries to heal slower because the neck is almost always in use and under consistent stress.
How is Cervicalgia Treated?
Treatment for cervicalgia depends on both the symptoms and the cause. If you have been injured, you should immediately seek medical attention to assess the injury’s severity.
You can apply ice to help reduce inflammation and swelling, but do not delay a medical evaluation. Some neck injuries can be severe, causing severe conditions, including paralysis.
After an assessment, your doctor may prescribe medication such as anti-inflammatories and stronger painkillers. A cervical collar may also be recommended since it allows the neck to rest, which will promote healing.
If the pain is caused by other reasons such as stress, poor posture, or sleeping on the wrong pillow (in other words, you have a crick in your neck), you can use an over-the-counter anti-inflammatory medication, and using a heating pad will help. Massage is also effective.
However, prevention is the best cure. When you know what is causing your cervicalgia, you can take steps to prevent it. Chiropractic can help both in prevent cervicalgia and in treating it.
Chiropractic for Cervicalgia
Chiropractic treatment can help relieve cervicalgia pain for many of the causes, including injury, stress, and misalignment. Depending on the cause, the chiropractor will use specific techniques to treat the root of the problem.
They will bring the body back into alignment, which also helps to prevent the pain of cervicalgia. The most attractive aspect is that it allows for pain management without the use of any medications.
When you get regular chiropractic care, you can reduce your chances of experiencing pain in your neck and back. That is why so many people are choosing chiropractic care for their neck and back pain instead of turning to traditional medicine because it works.
Osgood-Schlatter disease is a common cause of knee pain in growing adolescents. It is characterized by the inflammation of the site below the knee where the tendon from the kneecap, or the patellar tendon, attaches to the shinbone, or tibia. Osgood-Schlatter disease occurs during growth spurts when muscles, bones, tendons, and other tissues shift�rapidly.
Physical activities can place additional stress on the bones, muscles, tendons and other complex structures of young athletes. Children and adolescents who participate in running and jumping sports have a higher chance of developing this condition. However, less active children and adolescents may also experience this well-known health issue.
In the majority of instances, Osgood-Schlatter disease will resolve on its own and the pain can be managed with over-the-counter drugs and/or medications. Stretches and exercises can also help improve strength, flexibility and mobility. Alternative treatment options, such as chiropractic care, can also help relieve pain and restore the patient’s�well-being.
Contents
Osgood-Schlatter Disease Explained
The bones of children and adolescents have a special area where the bone grows, known as the growth plate. Growth plates are made up of cartilage, which harden into solid bone, when a child or adolescent is fully grown.
Some growth plates function as attachment sites for tendons, the strong soft tissues which connect muscles to bones. A bump, known as the tubercle, covers the growth plate at the end of the tibia. The set of muscles in the front of the thigh, or the quadriceps, then attaches to the tibial tubercle.
When a child or adolescent participates in physical activities, the quadriceps muscles pull the patellar tendon which then pulls the tibial tubercle. In some children and adolescents, this traction on the tubercle can cause pain and inflammation in the growth plate. The prominence, or bulge, of the tubercle may become pronounced as a result of this problem.
Osgood-Schlatter Disease Symptoms
Painful symptoms associated with Osgood-Schlatter disease are often brought on by running, jumping, and other sports-related pursuits. In some cases, both the knees have symptoms, although one knee might be worse. Common symptoms of Osgood-Schlatter disease also include:
Knee pain and tenderness in the tibial tubercle
Swelling in the tibial tubercle
Tight muscles at the front or back of the thigh
Osgood-Schlatter disease is the inflammation of the bone, cartilage and/or tendon at the top of the shinbone, or tibia, where the tendon attaches to the kneecap, or patella. Osgood-Schlatter disease is considered to be an overuse injury rather than a disorder or condition. Osgood-Schlatter disease is one of the most common causes of knee pain in children and adolescents. Although it can be very painful, the health issue generally goes away on its own within 12 to 24 months.
Dr. Alex Jimenez D.C., C.C.S.T. Insight
Osgood-Schlatter Disease Diagnosis
Throughout the consultation, the healthcare professional will discuss the children or adolescent’s symptoms regarding their overall health and wellness. They will then conduct a comprehensive evaluation of the knee. This will consist of applying pressure to the tibial tubercle, which should be painful for a patient with Osgood-Schlatter disease. Additionally, the doctor may also ask the child or adolescent to walk, run, jump, or kneel to see whether symptoms are brought on by the movements. Furthermore, the healthcare professional may also order an x-ray of the patienet’s knee to help support their diagnosis or to rule out any other health issues.
Osgood-Schlatter Disease Treatment
Treatment for Osgood-Schlatter disease focuses on reducing pain and inflammation. This generally requires limiting physical activities until symptoms improve. Sometimes, rest may be necessary for many months, followed by treatment and rehabilitation program. However, participation may be safe to continue if the patient experiences no painful symptoms. The doctor may recommend additional treatment, including:
Stretchex�and exercises. Stretches and exercises for the front and back of the thigh, or the quadriceps and the hamstring muscles, can help alleviate pain and prevent the disease from returning.
Non-steroidal anti-inflammatory drugs. Medications like ibuprofen and naproxen can also help reduce pain and inflammation.
Most symptoms will completely vanish when a child completes the adolescent growth spurt, around age 14 for girls and age 16 for boys. Because of this, surgery is often not recommended, although the prominence of the�tubercle will remain.�The scope of our information is limited to chiropractic and spinal health issues. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topic Discussion: Relieving Knee Pain without Surgery
Knee pain is a well-known symptom which can occur due to a variety of knee injuries and/or conditions, including sports injuries. The knee is one of the most complex joints in the human body as it is made-up of the intersection of four bones, four ligaments, various tendons, two menisci, and cartilage. According to the American Academy of Family Physicians, the most common causes of knee pain include patellar subluxation, patellar tendinitis or jumper’s knee, and Osgood-Schlatter disease. Although knee pain is most likely to occur in people over 60 years old, knee pain can also occur in children and adolescents. Knee pain can be treated at home following the RICE methods, however, severe knee injuries may require immediate medical attention, including chiropractic care.
You may have seen professional athletes, dancers, gymnasts, and others who engage in extremely physical activities using a type of tape on various points of their bodies. It is sometimes colored and does not seem to inhibit range of motion. While it looks like tape or maybe a very fancy bandage, it is a highly technical, specialized tape that is used to treat patients of all ages and activity levels. It is called Kinesio tape, and it is often used by chiropractors to help address specific injuries.
Contents
What is Kinesio Tape?
Also called Kinesio Tex Tape, Kinesio Tape is a special adhesive tape that has elastic properties. It was developed by Dr. Kenzo Kase, a chiropractor, and acupuncturist, in 1979. It is safe for all ages including pediatric and geriatric patients. The tape is comprised of a 100% cotton fiber strip with medical grade acrylic adhesive. It is soft and gentle, but it works.
The tape is hypoallergenic and latex free, so it is appropriate for a vast audience. It is also water resistant, making it wearable for many activities. When worn, the tape does not limit or inhibit range of motion, and the same tape can be worn for several days without losing its effectiveness.
How does Kinesio Tape Work?
The tape can stimulate or relax muscles, depending on the tension that it puts on the body when applied. When worn, it lifts the skin by microscopic increments which aids in lymphatic drainage.
It also helps to decrease inflammation and swelling which reduces pressure in the area. This allows the blood and lymphatic fluid to flow freer and more effectively in and out of the affected area.
When used correctly, Kinesio Tape can reduce inflammation, promote better circulation, prevent injury, facilitate healing, the re-educate the neuromuscular system. This helps the body return to homeostasis. It can be applied in many different configurations, but often the applications are a single �I,� �Y,� or �X.�
The Kinesio Taping Method
The Kinesio taping method is a systematic, therapeutic technique that offers a two-prong approach of supporting the patient and rehabilitating the condition or affected area. It can alleviate pain reduce swelling, providing relief to the patient. There are specific taping shapes that are specialized to address certain areas of the body as well as certain conditions. While it provides stability and support to the body�s joints and muscles, it does not restrict the range of motion. The technique is designed to address soft tissue injury by manipulating that area and facilitating healing.
What Conditions is Kinesio Taping used to Treat?
Many conditions throughout the body can benefit from Kinesio Taping. Chiropractors use it for:
Lower back strain
Plantar fasciitis
Back strain
Carpal tunnel syndrome
Rotator cuff injury
Ankle Sprains
Whiplash
Herniated disc
Post-surgery edema
Tennis elbow
Pre-surgery edema
Patella tracking
Athletes may also use it for additional support or to prevent injury. Because it relies on the body�s natural healing process, many people find it to be preferred treatment for many painful conditions. When combined with chiropractic care, Kinesio Tape is very effective.
When treating a condition with Kinesio Tape, the chiropractor may use a variety of techniques, depending on the illness or injury. They may use spinal manipulation, massage, and other treatments, combining them with recommendations for lifestyle changes and diet modifications.
The draw for this treatment is that it encourages the body to heal itself, eliminating the need for drugs with their undesired and unpleasant side effects, or more invasive procedures like surgery. Kinesio Taping is safe, natural, and a perfect complement to chiropractic care.
Robert “Bobby” Gomez first visited Dr. Alex Jimenez, doctor of chiropractic, after experiencing back pain due to a pelvic tilt on his hips. Born with cerebral palsy, Bobby always felt underestimated by his peers due to his condition. Thanks to chiropractic care, Robert Gomez received the support he needed to strengthen his body as well as to improve his flexibility and mobility. Bobby describes how he received more help than he expected with Dr. Alex Jimenez.
Rehabilitation For Cerebral Palsy
Cerebral palsy is a disorder of motion, muscular tone or posture that’s brought on by brain damage that happens before birth. The impact on functional abilities with cerebral palsy varies. Generally, cerebral palsy causes movement problems with reflexes or rigidity of the limbs and back posture, and unsteady walking. People with cerebral palsy may suffer a reduced range of movement in different areas of their body. The disability associated with cerebral palsy may be limited primarily to one limb or one side of the body, or it may affect the whole body.
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused on treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
If you have enjoyed this video and we have helped you in any way, please feel free to subscribe and recommend�us.
Sinding-Larsen-Johansson, or SLJ, syndrome is a debilitating knee condition that most commonly affects teens during periods of rapid growth. The kneecap, or patella, is attached to the shinbone, or tibia, from the patellar tendon. The tendon connects to an expansion plate at the bottom of the kneecap throughout growth.
Repetitive stress on the patellar tendon can make the growth plate within the knee become inflamed and irritated. SLJ mainly develops in children and adolescents between the ages of 10 and 15 because that is when most people experience growth spurts. SLJ is most common in young athletes due to excess or repetitive strain in the knee.
Contents
Causes of SLJ Syndrome
The large muscle group at the front of the upper leg is known as the quadriceps. When straightening the leg, the quadriceps pull to deliver the leg forward. This puts pressure on the growth plate at the bottom of the kneecap. During rapid growth, the bones and muscles don’t always grow at precisely the same rate.
Since the bones grow, tendons and muscles can get tight and stretched. This increases the strain around the patellar tendon and also on the growth plate it’s attached to. Repetitive or extra stress and pressure in this area can cause the growth plate to become irritated and painful. Matters that can contribute to growing SLJ syndrome are comprised of:
Sports that involve a lot of running and jumping, such as field and track or other sports such as football, gymnastics, basketball, lacrosse, and field hockey, can place stress on the knees.
Increased or incorrect physical activity can add strain on the knees. Improper form while training, shoes that don’t support the toes or an unusual way of jogging can increase chances of SLJ syndrome.
Tight or stiff quadriceps muscles can also lead to SLJ syndrome. Muscles that are more powerful and more elastic will work better, reducing the strain on the patellar and kneecap tendon.
Activities that place more pressure on the knees or demanding tasks for the knees, such as lifting heavy items, walking up and down stairs, and squatting can cause SLJ syndrome. If there’s already pain on the knee, then these movements may make it worse.
Symptoms of SLJ Syndrome
Symptoms demonstrating the presence of�Sinding-Larsen-Johansson, or SLJ, syndrome include: pain at the front of the knee or near the bottom of the kneecap, as this is the main symptom of SLJ; swelling and tenderness around the kneecap; pain that increases with physical activities like jogging, climbing stairs, or leaping; pain that becomes more acute when kneeling or squatting; and a swollen or bony bump at the bottom of the kneecap.
Sinding-Larsen-Johansson, or SLJ, syndrome is medically referred to as a juvenile osteochondrosis which affects the patella tendon in the kneecap which attaches to the inferior pole of the patella in the shinbone. Commonly characterized by knee pain and inflammation, SLJ is considered an overuse knee injury rather than a traumatic injury. Sinding-Larsen-Johansson syndrome is similar to Osgood-Schlatter syndrome.
Dr. Alex Jimenez D.C., C.C.S.T. Insight
Diagnosis of SLJ
Should you see a healthcare professional for knee problems, they will generally ask questions about how much pain the patient is experiencing and if they do any sports or other physical activities and exercises. Whether or not the patient has also had a recent growth spurt, the doctor will examine the patient’s knee for swelling and tenderness.
In very rare instances, the healthcare professional may also ask patients to acquire an X-ray or other imaging diagnostics, such as magnetic resonance imaging, or MRI, to rule out other health issues like fracture or disease.
Prevention of SLJ
The most significant way that patients can prevent getting SLJ is to stop doing physical activities which cause pain in the knee. The patient should limit themselves before the pain goes off.
It is crucial to warm up well and stretch before exercising, playing sports or engaging in any other physical activities. A jog around the track for a couple of minutes and some dynamic stretching is enough to warm up the body.
If the quadriceps muscles are tight, then you might want to do some specialized exercise and physical activity routines. Talk to your healthcare professional, such as a chiropractor or physical therapist, to discuss what’s best for you. Doing a few stretches and warm up exercises after sports or physical activities can help prevent SLJ syndrome from developing.
Treatment of SLJ
The first and most important way to treat SLJ is to stop any action that causes irritation in the knee. It’s essential for a patient to not resume any physical activities without first being cleared by a healthcare professional.
SLJ can be challenging to treat since it may not completely resolve before the bones have completely matured and the growth plates are completely shut. During physical activities, knee pain may come and go in the meantime. Other treatments to help ease SLJ syndrome include:
Use the RICE formula.
Rest. Limit physical activities as much as possible and keep weight off the knee. Walking must be kept to a minimum.
Ice. Apply ice or a cold compress to the affected area for 15 to 20 minutes every few hours. Repeat this for 2 to 3 days or until the painful symptoms have decreased.
Compress. Give the knee additional support with a strap, a band, or a ribbon. This will also�help manage symptoms.
Elevate. Keep the knee higher than the heart to reduce swelling.
Take anti-inflammatory or painkilling drugs. Painkillers like acetaminophen and ibuprofen can help relieve pain and decrease swelling.
Begin a stretching and strengthening program. After the pain and tenderness on your knee have been gone, speak with your physician or sports injury professional about a physical rehabilitation program to strengthen the muscles of your leg and increase their flexibility and range of movement.
It’s easy to become impatient when sidelined by an injury, but the proper treatment can help build the strength needed for future physical activities.�The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topic Discussion: Relieving Knee Pain without Surgery
Knee pain is a well-known symptom which can occur due to a variety of knee injuries and/or conditions, including sports injuries. The knee is one of the most complex joints in the human body as it is made-up of the intersection of four bones, four ligaments, various tendons, two menisci, and cartilage. According to the American Academy of Family Physicians, the most common causes of knee pain include patellar subluxation, patellar tendinitis or jumper’s knee, and Osgood-Schlatter disease. Although knee pain is most likely to occur in people over 60 years old, knee pain can also occur in children and adolescents. Knee pain can be treated at home following the RICE methods, however, severe knee injuries may require immediate medical attention, including chiropractic care.
aka Spondylodiscitis and vertebral osteomyelitis overall are relatively infrequent and may present with bimodal distribution: children and adults >50’s
Occasionally considered as two separate entities due to variations in the blood supply of pediatric vs. adult spines
Risk factors/causes: distant site of infection in the body (25-35%), e.g., oropharynx, urogenital infections, bacterial endocarditis, indwelling catheters, florid skin infections furunculosis/abscess, etc.
Iatrogenic:�operative (e.g., discectomy) interventional or diagnostic/therapeutic procedures
Penetrating trauma
Immunocompromised patients
Diabetics
Malnourished patients or patients with low protein
IV drug users
Chronic disease patients, cancer patients etc.
Contents
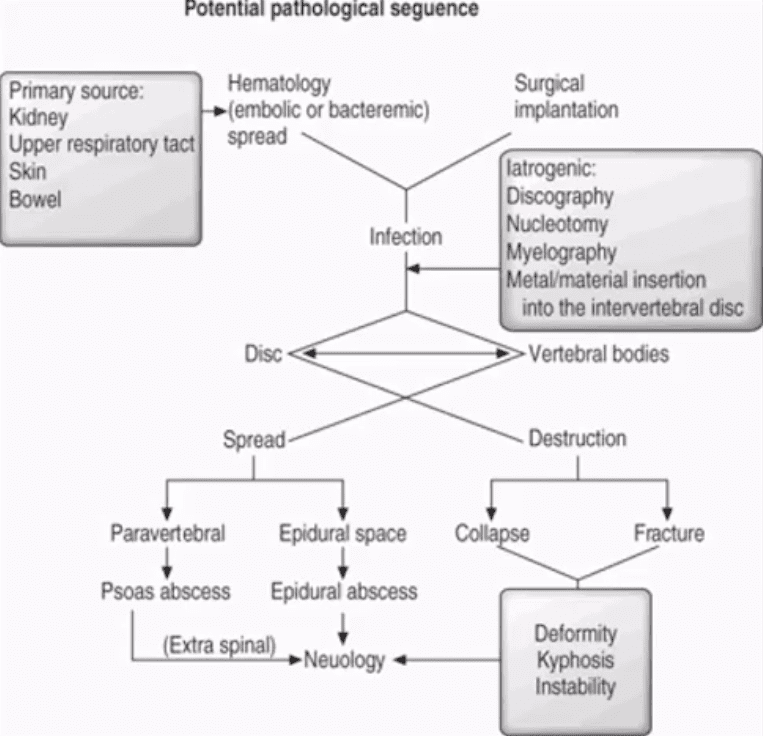
Potential Pathological Sequence
Clinical Presentation
Back pain with or w/o high fever and other “septic” signs. Fever may only present in 50% of children
Exacerbation of pre-existing back pain in post-surgical cases
Neurological complications in advanced cases of vertebral destruction and epidural abscess
Meningitis, septicemia etc.
Labs: Blood tests are unspecific, may or may not indicate elevated ESR/CRP, WBC
Diagnostic imaging is important but
If clinical suspicion is strong, prompt I.V. antibiotics are needed to prevent serious complications
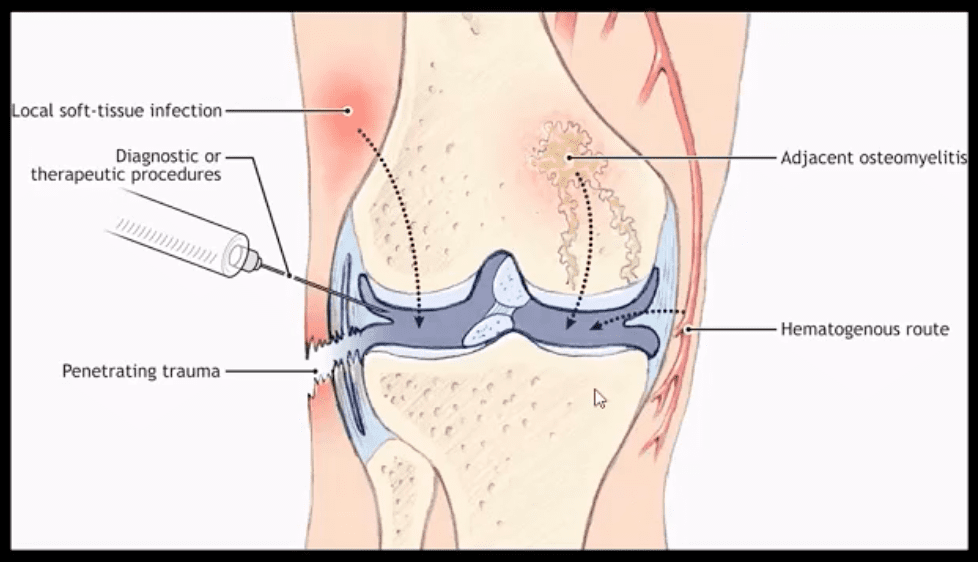
Routes of Infection
Infection routes to the spine are similar to bone in general
3-distinct routes:
1) Hematogenous spread as bacteremia (most common)
2) Adjacent site of infection (e.g., soft tissue abscess)
3)Direct inoculation (e.g., iatrogenic or traumatic)
M/C organism Staph. Aureus
Mycobacterium TB (tuberculous spinal osteomyelitis) aka Pott’s disease can be presented in cases of re-activated or disseminated pulmonary TB
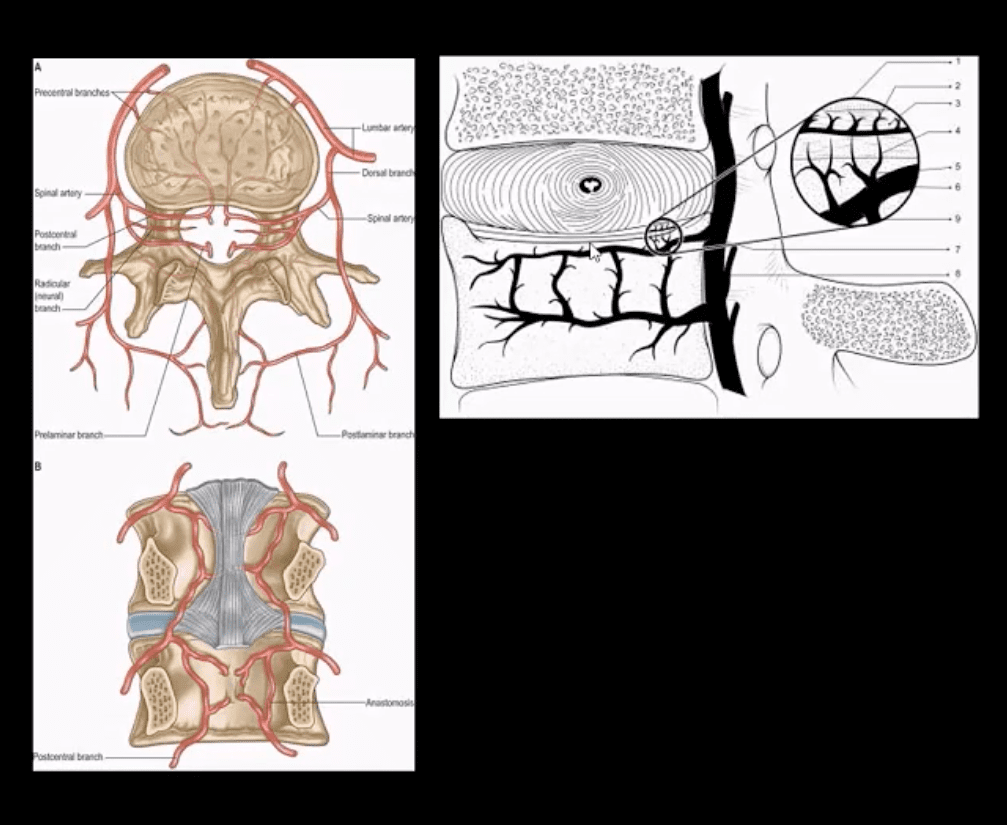
Mechanisms of Spinal Infection
May vary depending on the patients’ age
In children, the IVD receives direct blood supply and can be infected directly spreading to adjacent bone and causing spondylodiscitis
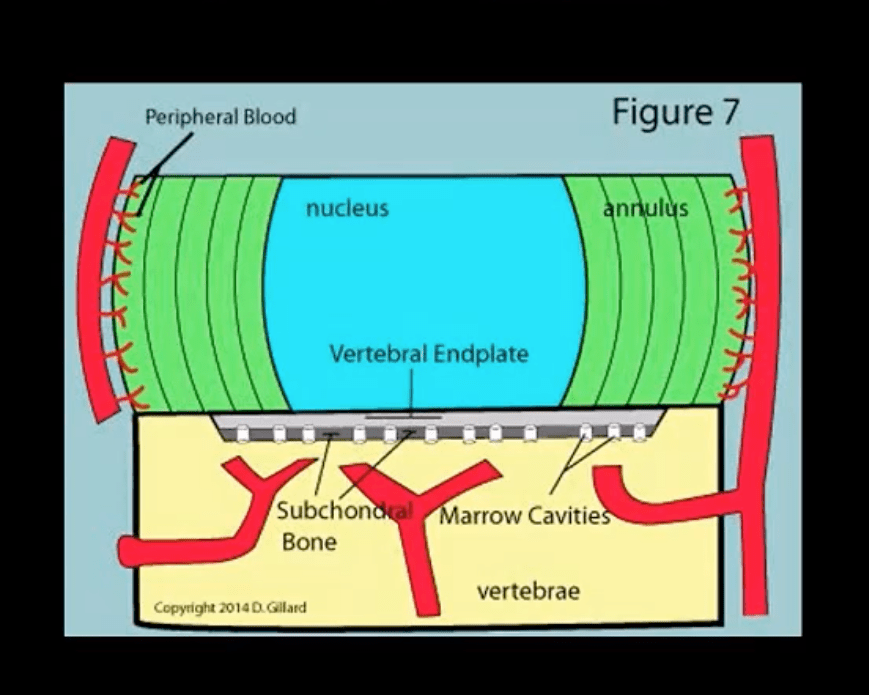
In Adults
The disc is avascular
Pathogens invade adjacent vertebral end-plates via end-arterial supply of the vertebral body that may facilitate infection due to slow, turbulent flow
Organisms may then quickly gain access to disc substance rich in nutrients (discitis) often w/o significant initially visible destruction to the bone
Thus, one of the earliest rad. findings of spinal infection or sudden reduction of disc height
Later end-plate irregularity/sclerosis may develop, subsequently affecting the entire adjacent vertebral bodies
Diagnostic Imaging
Initially, in most cases of MSK complaints, radiography is the 1st imaging step
Initially, X-radiography is often unrewarding and may appear unremarkable for 7-10 days or presents with some subtle soft tissue changes (e.g., obscuration of Psoas shadows etc.)
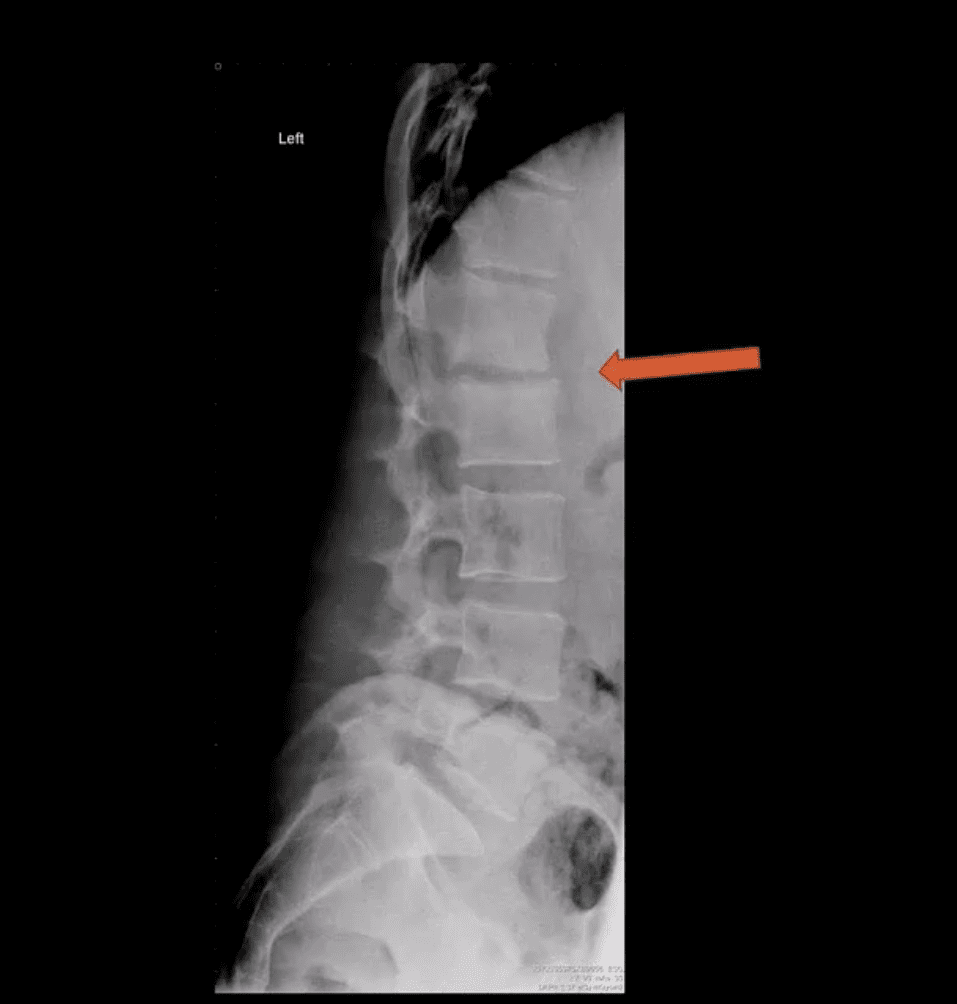
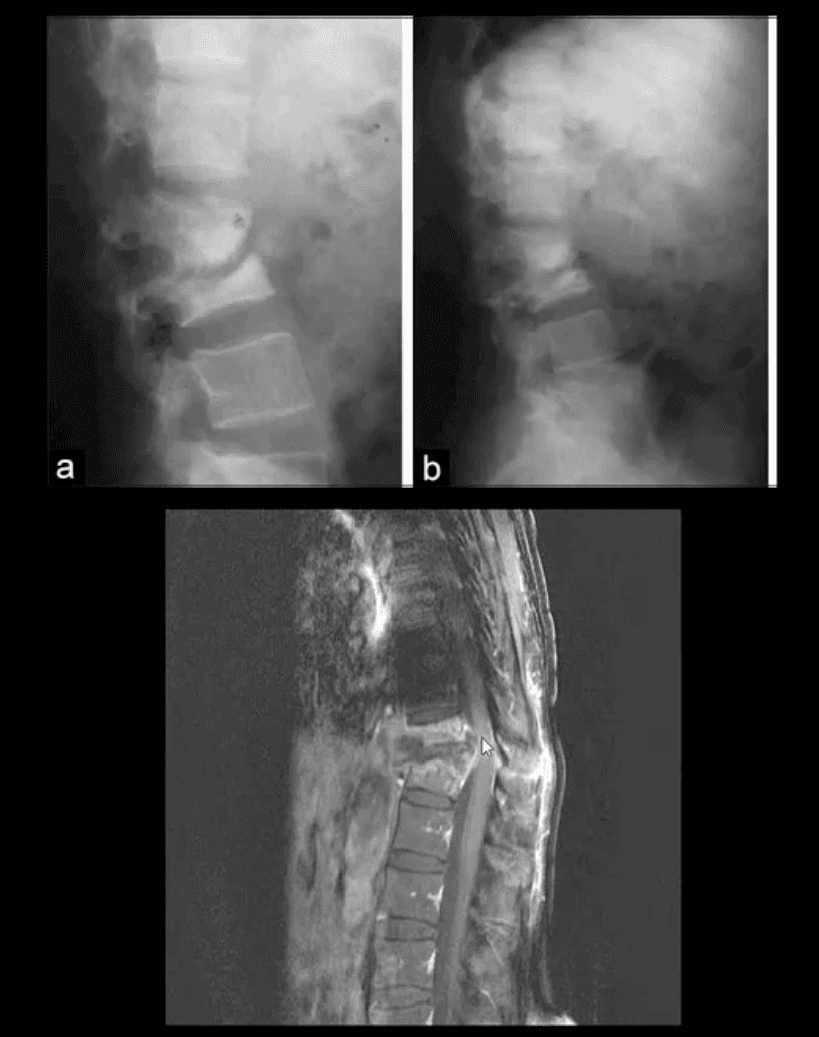
Some of the earliest x-ray signs of pyogenic spondylodiscitis: sudden reduction of disc height (above arrow) during initial 7-10 days
Subsequently (10-20 days) some end-plate irregularity and adjacent sclerosis may be noted
In more advanced cases, subsequent vertebral destruction and collapse may occur
N.B. Reliable feature to DDx between spinal infection and metastasis is the preservation of disc height in the latter
Note:�sudden disc narrowing with no appreciable spondylosis (above the first image) is suspicious for infection (discitis)
MRI +C is required to evaluate suspected infection
N.B. 50-60% of pyogenic spondylodiscitis occur in the lumbar region
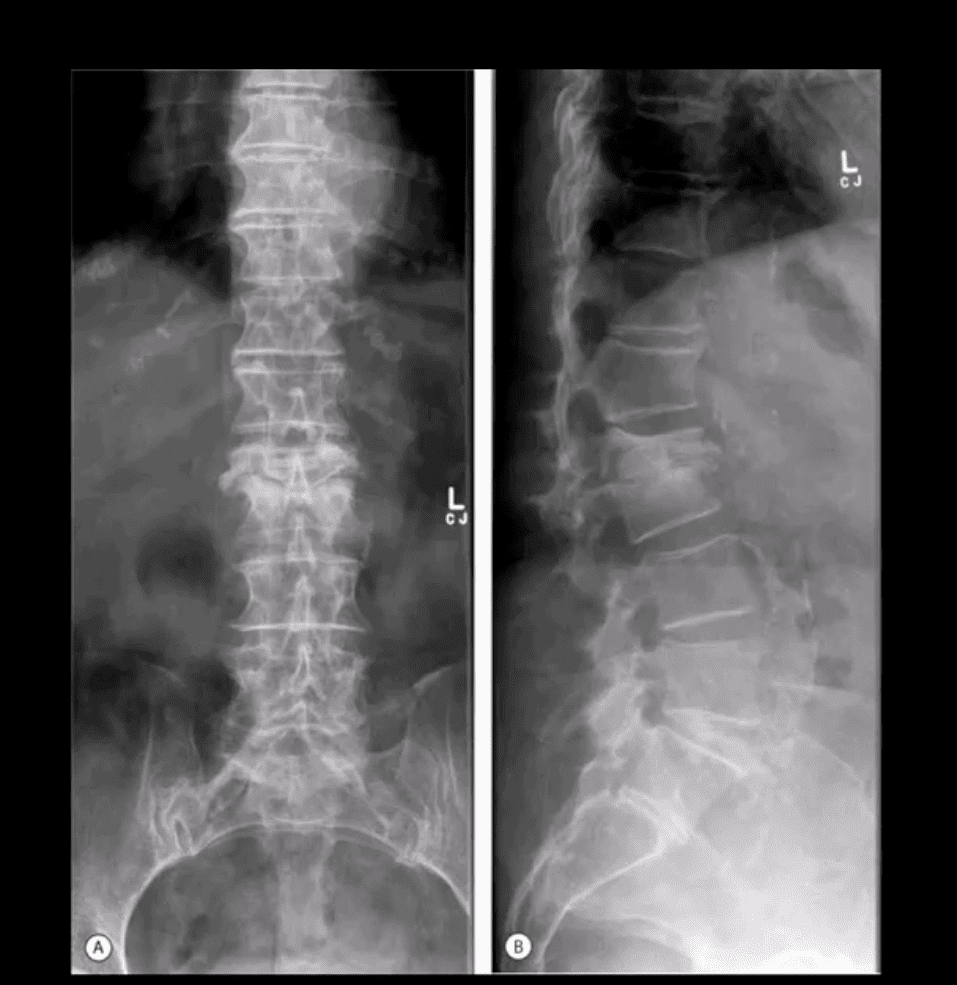
AP & Lateral Lumbar Radiographs
Note severe disc narrowing and adjacent vertebral body destruction at L1-L2 in a 68 -y.o.-female with a known Hx of type 2 DM
Additional imaging modalities should be used to support the Dx
Final Dx: Pyogenic Spondylodiscitis
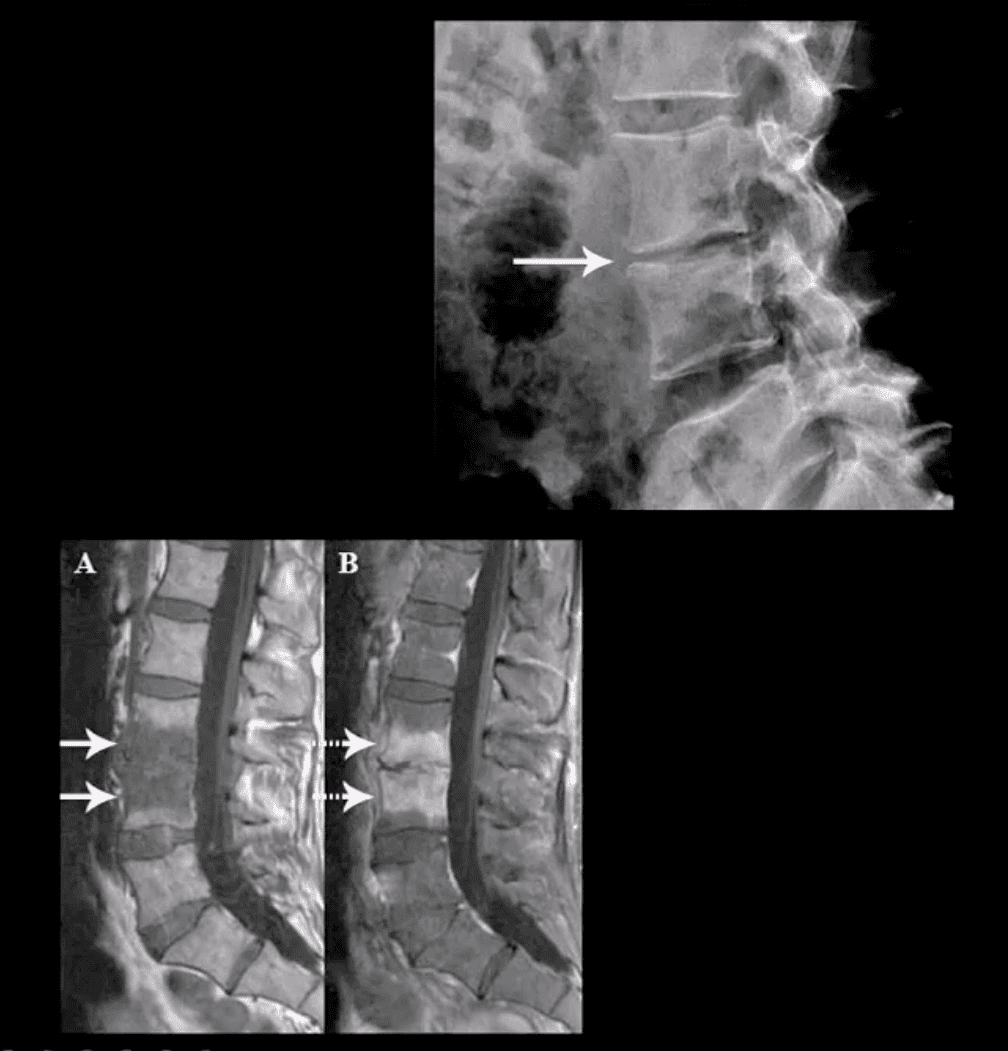
Sagittal T1 & T2 MRI
Weighted MRI slices of a patient who had laminectomy at L4
MR imaging with gad contrast is the modality of choice for Dx of spinal infection
Early septic changes affecting the disc and adjacent vertebral end-plates are readily demonstrated as a low signal on T1 and high T2/STIR d/t edema and inflammation
T1 FS +C gad images show avid enhancement of the lesion due to granulation tissue around the phlegmon. Peripheral enhancement is also characteristic of an abscess.
Epidural extension/abscess can also be successfully detected my MRI
N.B. 50% of epidural abscess cases present with neurological signs
STIR & T1 FS +C Gad Sagittal MRI
Marked septic collection and edema affecting L4-5 disc and vertebral body with some epidural extension and paraspinal soft tissue edema. Avid contrast enhancement is noted surrounding low signal foci within the bone and disc tissue, some gad. Enhancement is noted in posterior paraspinal muscles and dural spaces
Management: Dx of spondylodiscitis requires prompt I.V antibiotics. If instability and neurological complications develop referral to a Neurosurgeon is required
MRI Unavailable or Contraindicated
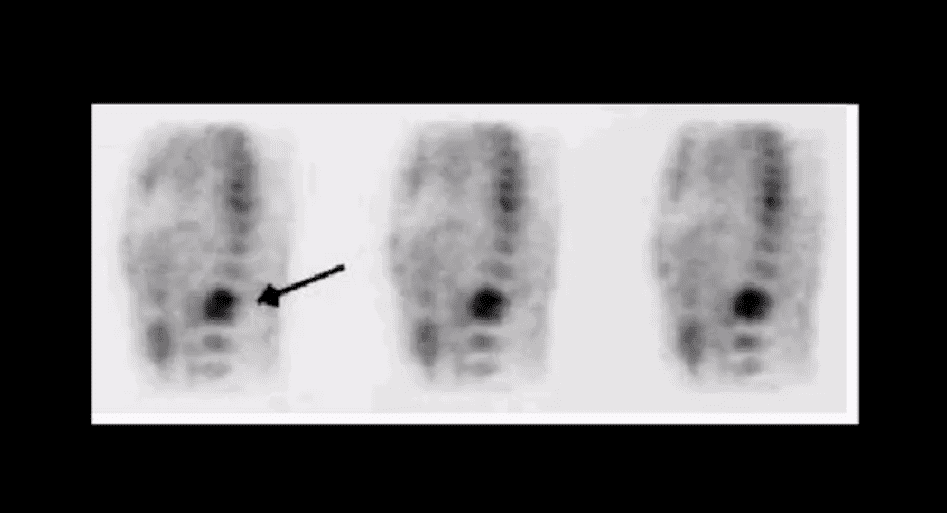
Bone scintigraphy is very sensitive but non-specific for spinal infection but overall is of great value d/t higher sensitivity than x-rays and relatively low cost.
An area of increased flow with radiopharmaceutical uptake is characteristic but not specific sign of spondylodiscitis
If neurological signs are present and MRI is contraindicated than CT myelography may be used
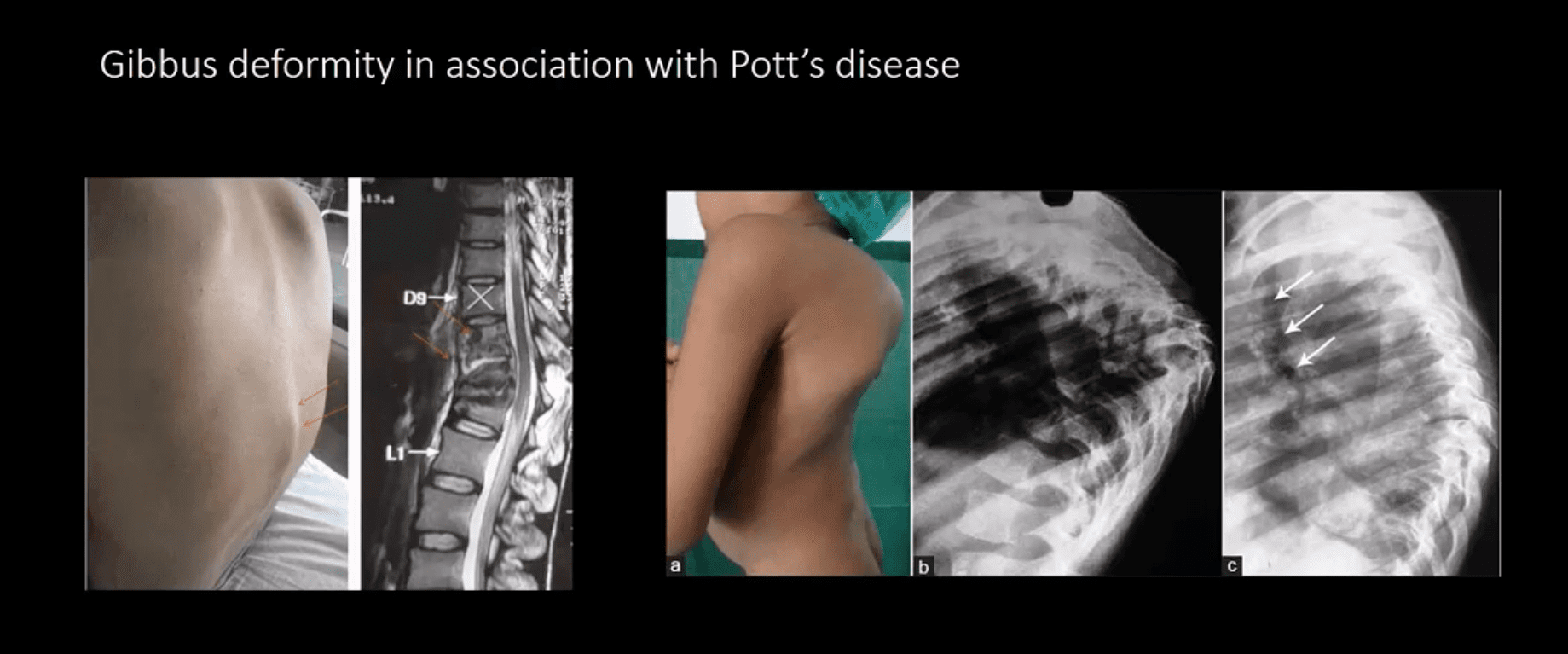
TB Osteomyelitis aka Pott’s Disease
TB osteomyelitis is increasing d/t HIV and other immunocompromised states. Extrapulmonary TB m/c affects the spine and especially the thoracic spine (60%)
Radiographic Pathology:�TB bacillus infects the vertebral body and often spreads subligamentously. “Cold” paraspinal abscess collection may develop and spreads along fascial planes, e.g., Psoas abscess. Disc spaces are preserved until v. late and skip areas are noted helping to DDx TB from pyogenic infection. Severe vertebral destruction aka Gibbus deformity may develop (>60-degree sometimes) and may become permanent. Neurologic and many regional complications may develop
Imagingapproach:�CXR with spinal x-rays 1st step that may be unrewarding but may potentially reveal VB destruction w/o disc narrowing. CT scanning is more superior than x-rays. MRI with gad C is a modality of choice
Patellar tendinitis is a common health issue characterized by the inflammation of the tendon which joins the kneecap, or patella, to the shinbone, or tibia. The knee pain associated with this problem may range from mild to severe depending on the circumstances of the knee injury.
Patellar tendinitis, or jumper’s knee, is a well-known sports injury among athletes who play in basketball and volleyball. Among recreational volleyball players, an estimated 14.4 percent of them have jumper’s knee, where the incidence is even higher for professional athletes. An estimated 40 to 50 percent of elite volleyball players have patellar tendinitis.
Contents
Causes of Patellar Tendinitis
Patellar tendinitis is caused by repetitive strain on the knee, most often from overuse in physical activities. Stress can create tears along the tendons which can cause inflammation in the complex structures of the knee.
Other contributing factors of patellar tendinitis include:
Tight or stiff leg muscles
Uneven leg muscle strength
Misaligned toes, ankles, and legs
Obesity
Sneakers without enough padding
Tough playing surfaces
Chronic health issues that weaken the tendon
Athletes have a higher chance of developing patellar tendinitis because running, jumping, and squatting put more force over the tendon. Running can place a force of as many as five times the body weight on the knees.
Intense physical activity for an extended amount of time has been previously associated with jumper’s knee. A 2014 research study noted that jump frequency was also a significant risk factor for amateur players.
Symptoms of Patellar Tendinitis
The initial symptoms of patellar tendinitis include pain,�discomfort, and tenderness at the base of the kneecap or patella. Other symptoms of patellar tendinitis may include a burning sensation. For many patients, getting up from a squat or kneeling down can also be particularly debilitating.
The pain associated with patellar tendinitis may be irregular at first, manifesting immediately after participating in physical activities. Damage or injury to the tendon can also make the pain worse. Jumper’s knee can affect regular daily activities, such as climbing stairs or sitting in a vehicle.
�
Patellar tendinitis, also known as “jumper’s knee”, is a particularly common cause of pain and discomfort in the patellar region of many athletes. While it frequently occurs as a result of repetitive or continuous jumping, research studies have demonstrated that patellar tendinitis may be associated with stiff ankle movements and ankle sprains, among other sports injuries.
Dr. Alex Jimenez D.C., C.C.S.T. Insight
Patellar Tendinitis Diagnosis
At the start of a�consultation, the healthcare professional will first ask the patient about their specific health issue. The doctor will then physically evaluate the patient’s knee, probe for where they are feeling pain, and test the assortment of knee motion by bending and extending the patient’s leg.
Furthermore, the healthcare professional may additionally order imaging diagnostics to find out if there’s any damage or injury to the tendon or even the bone. These tests can help rule out a broken bone, or fracture. The doctor may use an X-ray to look for a displaced or fractured kneecap, and an MRI or an ultrasound to reveal any harm to the soft tissue.
Patellar Tendinitis Treatment
Treatment for patellar tendinitis depends on the damage or injury to the knee. Conservative steps to reduce pain, such as rest or exercises are generally the first line of treatment. The healthcare professional will usually recommend a span of controlled rest, where they will prevent the patient from engaging in physical activities that put�pressure on the knee.
Drugs and/or Medications
The healthcare professional may prescribe over-the-counter drugs and/or medications for short-term pain relief and inflammation reduction.
These can consist of:
Ibuprofen (Advil)
Naproxen sodium (Aleve)
cetaminophen (Tylenol)
If the patient’s symptoms are severe, the healthcare professional may recommend the use of corticosteroid injection in the area around the patellar tendon. This treatment is effective in reducing acute pain.
Another method of utilizing corticosteroid for patellar tendinitis is by spreading the medication over the affected knee and use a low electrical charge to push it through the skin, in a process known as iontophoresis.
Chiropractic Care and Physical Therapy
The goal of chiropractic care and physical therapy for patellar tendinitis is to reduce pain and inflammation, among other symptoms, as well as to strengthen the leg and thigh muscles with stretches and exercises.
If the patient’s symptoms are severe, even while resting, the doctor may recommend that you wear a brace and then use crutches to avoid additional damage or injury to the tendon. If the patient has no painful symptoms, then they can start participating in a physical therapy activities.
A rehabilitation program generally consists of:
A warm-up interval
Massage, heat or ice to the�knee
Stretching exercises
Strengthening exercises
A doctor of chiropractic, or chiropractor, may use ultrasound and electrical stimulation to relieve the patient’s knee pain. A�knee brace or taping of the knee might also help reduce pain by supporting the kneecap when engaging in physical activities. The healthcare professional may develop a workout program that may include a series of stretches and exercises.
Surgery
When other treatments are not effective in relieving painful symptoms associated with patellar tendinitis, the doctor may advise surgery to repair the patellar tendon. Traditional surgery involves opening the knee to scrape on the kneecap and tendon. More recently,�arthroscopic surgery is used for this particular process. This surgical intervention involves making four small incisions in the knee and it has a shorter recovery time.
The recovery period for surgery varies per procedure. Some surgical intervention advise for immobilization with a cast. Others suggest�an immediate rehabilitation program. Regardless of the level of damage and/or injury, it’s essential for patients to seek medical attention for their patellar tendinitis. The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topic Discussion: Relieving Knee Pain without Surgery
Knee pain is a well-known symptom which can occur due to a variety of knee injuries and/or conditions, including sports injuries. The knee is one of the most complex joints in the human body as it is made-up of the intersection of four bones, four ligaments, various tendons, two menisci, and cartilage. According to the American Academy of Family Physicians, the most common causes of knee pain include patellar subluxation, patellar tendinitis or jumper’s knee, and Osgood-Schlatter disease. Although knee pain is most likely to occur in people over 60 years old, knee pain can also occur in children and adolescents. Knee pain can be treated at home following the RICE methods, however, severe knee injuries may require immediate medical attention, including chiropractic care.
Headaches are a real pain (insert eye-roll here). Many individuals suffer from them, and there are a variety of causes, symptoms, and treatment options. For some, they are a rare occurrence, while others deal with them weekly or even daily. They can range from minor inconveniences to full-fledged life-changing afflictions.
The first step in treating headaches is to understand the type of headache you are experiencing. Some people think they have a migraine when in fact, they are suffering from a tension headache. While tension headaches are more common, it’s estimated by the Migraine Research Foundation that 1 in 4 U.S. Households include someone with a migraine.
Determining which headache is being dealt with takes a bit of research. Individuals suffering from headaches need to ask themselves these questions to determine if they are having a migraine or experiencing a tension headache.
When in life did the headaches begin? According to the Mayo Clinic, migraines start in adolescence or early adulthood. In contrast, tension headaches can start at any time in a person’s life. If an adult just began suffering from headaches, they are most likely tension headaches.
Where does it hurt? The location of the pain is a vital indicator of the type of headache. Migraines typically occur on one side of the head. Tension headaches affect both sides of the head and can produce a feeling of pressure in the forehead area.
What kind of pain is it? If it is a dull pain, a feeling of pressure, or tenderness around the scalp, it’s most likely a tension headache. If, on the other hand, the pain is throbbing or pulsing pain, it could be a migraine. Both headaches can offer up severe pain, just different types.
Are there any other symptoms?Migraines typically come with symptoms beyond head pain. Nausea, light and sound sensitivity, bright flashing or sparkling lights, pins and needle sensations down one or both arms, or dizziness are common. Individuals who don’t experience any of these symptoms are most likely dealing with a tension headache.
Can you function? While painful and frustrating, many people with a tension headache can still perform their jobs, drive, read, and deal with daily life. A migraine is a different story. Lying in a dark, quiet room with a sleep mask on until the headache passes is how most people handle migraines. If the headache is life-disrupting, it could very well be a migraine.
Do regular painkillers work? Tension headaches can often be relieved by over-the-counter pain medications. Migraines don’t budge with these treatments. Once a migraine is in full force, the sufferer must ride it out. If a headache reacts well to a couple of non-prescription painkillers, it’s most likely a tension headache.
Most individuals will, unfortunately, deal with a headache at one point in their lives. It’s important to note that tension headaches are much more common than migraines, but that doesn’t rule out the possibility of a headache being a migraine. The answers to the above questions give insight into the type of headache occurring and how best to handle the treatment proactively. No matter the type of headache, if the pain is severe, or begins after a head injury, seek medical treatment immediately.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine