Endocrine disruptors are chemicals that may interfere with the body’s endocrine system and produce adverse developmental, reproductive, neurological, and immune effects in humans. It can be pesticides, plasticizers, antimicrobials, and flame retardants that can be EDCs. EDCs (endocrine-disrupting chemicals) can disrupt the hormonal balance and can result in developmental and reproductive abnormalities in the body.
There are four points about endocrine disruption:
Low dose matters
Wide range of health benefits
Persistence of biological effects
Ubiquitous exposure
EDC can cause significant risks to humans by targeting different organs and systems in the body. The interactions and the mechanisms of toxicity created by EDC and environmental factors can be concerning a person’s general health problems. Including endocrine disturbances in the body since many factors can cause endocrine disruptors, one of the disruptors in the food contaminated with PBDEs (polybrominated diphenyl esters) in fish meat and dairy.
Researchers also pointed out that once the contaminated foods eliminated from a person’s diet, then the endocrine disruptors decline, and the body began to heal properly. When a person eliminates the food that is causing discomfort to their bodies, they are more aware of reading the food labels to prevent discomfort anymore to the body systems.
Obesogen
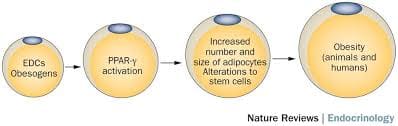
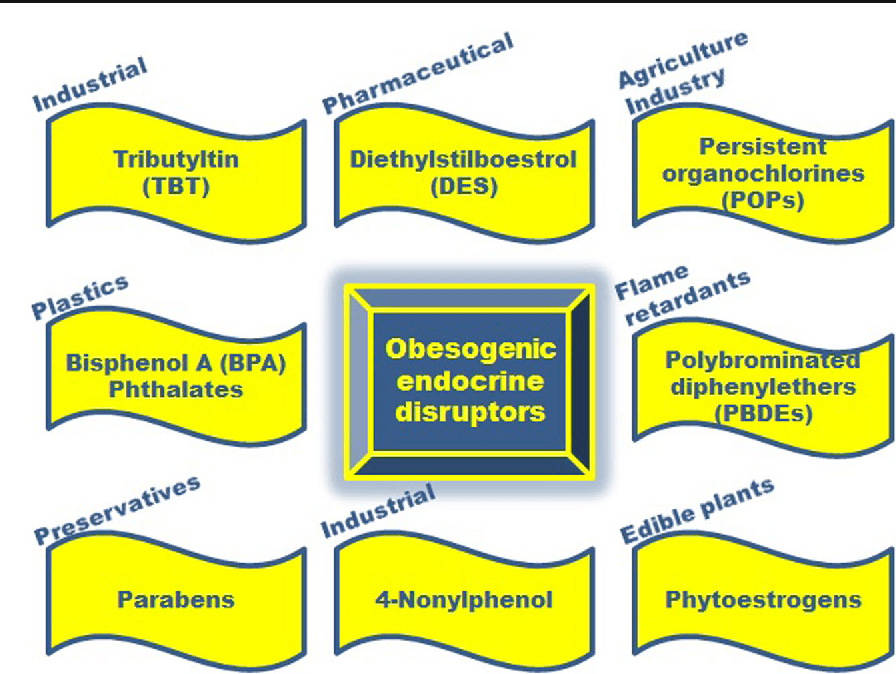
Obesogen is a subclass of endocrine-disrupting chemicals (EDC) that might predispose individuals to the development of obesity. Their structure is mainly lipophilic, and they can increase fat deposition. Since the fat cell’s primary role is to store and release energy, researchers have found that different obesogenic compounds may have different mechanisms of action.
Some of these actions can affect the number of fat cells that are producing, while others affect the size of the fat cells, and some obesogenic compounds can affect the hormones. These compounds will affect the appetite, satiety, food preferences, and energy metabolism when the endocrine system plays a fundamental role in the body to regulate the metabolism of fats, carbohydrates, and proteins. Any alternations in the body can result in an imbalance in the metabolism and causing endocrine disorders.
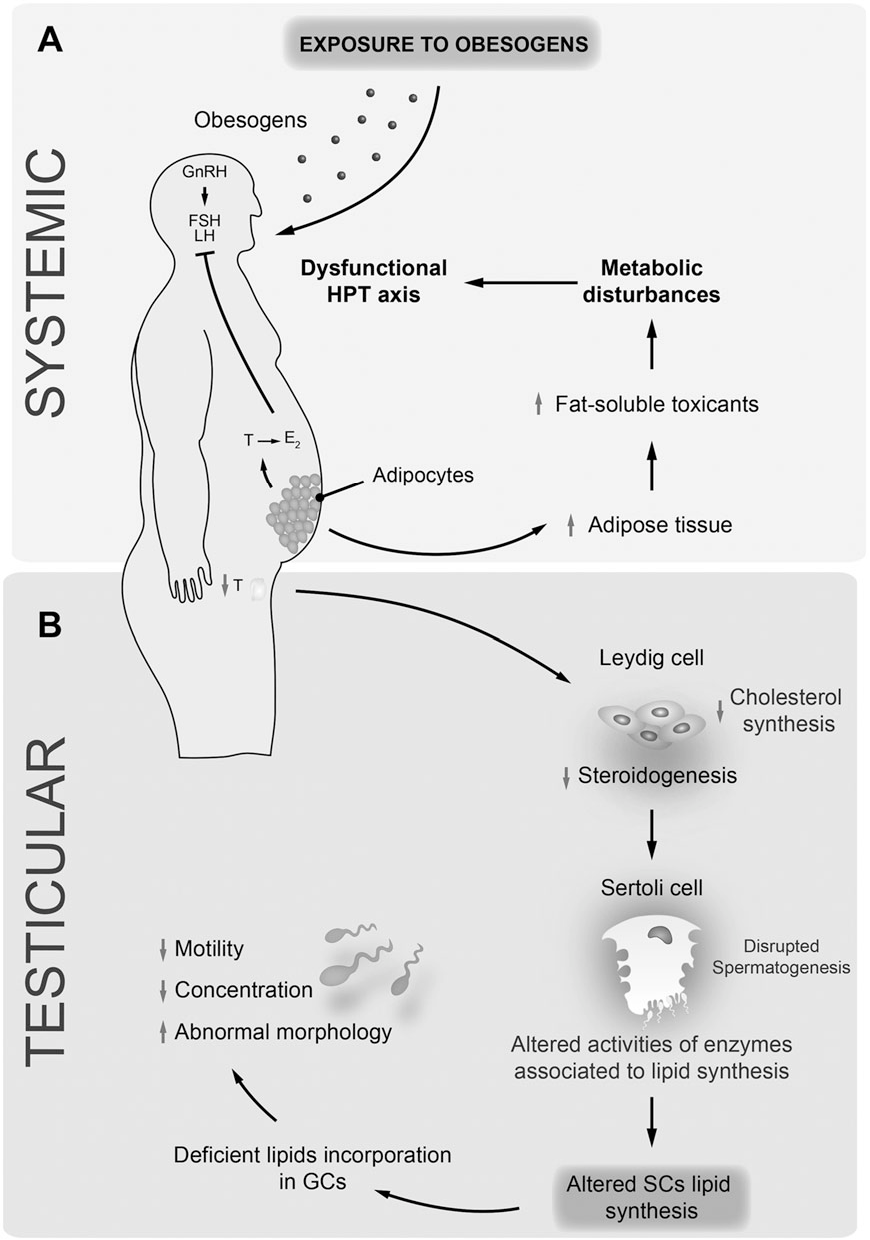
Studies even stated that exposure to obesogens could be found either before birth on utero or in the neonatal period. Obesogens can even cause a decrease in male fertility. When this disruption happens to the male body, environmental compounds can cause a predispose to weight gain, and obesogens can appoint as one of the contributors because of their actions as endocrine disruptors. Obesogens can even change the functioning of the male reproductive axis and testicular physiology. The metabolism in the male human body can be pivotal for spermatogenesis due to these changes.
Endocrine Disruptors and Obesity
Some endocrine disruptors that can affect the body can be through pharmaceutical drugs that can cause weight gain. A variety of prescription drugs can have an adverse effect that can result in weight gain since the chemicals found in prescription drugs have similar structures, and modes of action might have a role in obesity. Prescription medicine can stimulate the gut to consume more food, thus involving the body to gain weight.
Another endocrine disruptor is PAHs (polycyclic aromatic hydrocarbons). These are a family of environmental chemicals that occur in oil, coal, and tar deposits. They produce as by-products of fuel-burning like fossil fuel, biomass, cigarette smoke, and diesel exhaust. PAHs can either be manufactured to be used as medicines and pesticides or be released naturally from forest fires and volcanoes.
There are standard ways a person can be exposed to PAHs. One is through eating grilled, charred, or charcoal-broiled meats that a person eats. The other is through inhalation of smoke from cigarettes, vehicle exhaust, or emissions from fossil fuels that can irritate the eyes and breathing passageways in the body.
Coping with EDC Exposure
Even though obesity can adversely affect the body in a variety of health outcomes, there are ways to cope and minimize the exposure of EDC. Research shows that a person can minimize EDC exposure by consuming organic fruits, vegetables, and grain products insofar as possible. This includes an increasing number of fungicides routinely applied to fruits and vegetables that are being identified as obesogens and metabolic disruptors in the body.
Xenoestrogen vs. Phytoestrogen
When a person has an endocrine disorder, it might be due to the food they are consuming. Phytoestrogens are plant-derived compounds that are in a wide variety of food, mostly in soy. They are presented in numerous dietary supplements and widely marketed as a natural alternative to estrogen replacement therapy.
There is a health impact on phytoestrogen, and the plant-derived compound can either mimic, modulate, or disrupt the actions of endogenous estrogen. Xenoestrogen�are synthetically derived chemical agents from certain drugs, pesticides, and industrial by-products that mimic endogenous hormones or can interfere with endocrine disruptors. These chemical compounds can cause an effect on several developmental anomalies to humans. It can also interfere with the production and metabolism of ovarian estrogen in females.
Conclusion
Endocrine disruptors can interfere with the body’s endocrine system causing a health risk to an individual. EDC (endocrine-disrupting chemicals) can target many different organs and systems of the body by various factors that the human body is being exposed to. One of the EDC factors is obesogen, and it can cause a person to gain weight and be obese. Another factor is the exposure of PAHs (polycyclic aromatic hydrocarbons) through environmental factors like smoke inhalation or consuming charcoal-broiled meats. There are ways to cope with EDC exposure, and one is eating organic foods, especially fresh fruits and vegetables. Another is products that target the endocrine system and helps support the liver, intestines, body metabolism, and estrogen metabolism to ensure not only a healthy endocrine system but also a healthy body to function correctly.
October is Chiropractic Health Month. To learn more about it, check out Governor Abbott’s proclamation on our website to get full details on this historic event.
The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or chronic disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
References:
Cardoso, A M, et al. �Obesogens and Male Fertility.� Obesity Reviews : an Official Journal of the International Association for the Study of Obesity, U.S. National Library of Medicine, Jan. 2017, www.ncbi.nlm.nih.gov/pubmed/27776203.
Darbre, Philippa D. �Endocrine Disruptors and Obesity.� Current Obesity Reports, Springer US, Mar. 2017, www.ncbi.nlm.nih.gov/pmc/articles/PMC5359373/.
Holtcamp, Wendee. �Obesogens: an Environmental Link to Obesity.� Environmental Health Perspectives, National Institute of Environmental Health Sciences, Feb. 2012, www.ncbi.nlm.nih.gov/pmc/articles/PMC3279464/.
Janesick, Amanda S, and Bruce Blumberg. �Obesogens: an Emerging Threat to Public Health.� American Journal of Obstetrics and Gynecology, U.S. National Library of Medicine, May 2016, www.ncbi.nlm.nih.gov/pmc/articles/PMC4851574/.
Janesick, Amanda S, and Bruce Blumberg. �Obesogens: an Emerging Threat to Public Health.� American Journal of Obstetrics and Gynecology, U.S. National Library of Medicine, May 2016, www.ncbi.nlm.nih.gov/pubmed/26829510.
L�r�nd, T, et al. �Hormonal Action of Plant Derived and Anthropogenic Non-Steroidal Estrogenic Compounds: Phytoestrogens and Xenoestrogens.� Current Medicinal Chemistry, U.S. National Library of Medicine, 2010, www.ncbi.nlm.nih.gov/pubmed/20738246.
Patisaul, Heather B, and Wendy Jefferson. �The Pros and Cons of Phytoestrogens.� Frontiers in Neuroendocrinology, U.S. National Library of Medicine, Oct. 2010, www.ncbi.nlm.nih.gov/pmc/articles/PMC3074428/.
Singleton, David W, and Sohaib A Khan. �Xenoestrogen Exposure and Mechanisms of Endocrine Disruption.� Frontiers in Bioscience : a Journal and Virtual Library, U.S. National Library of Medicine, 1 Jan. 2003, www.ncbi.nlm.nih.gov/pubmed/12456297.
Unknown, Unknown. �Endocrine Disruptors.� National Institute of Environmental Health Sciences, U.S. Department of Health and Human Services, 2015, www.niehs.nih.gov/health/topics/agents/endocrine/index.cfm.
Unknown, Unknown. �Polycyclic Aromatic Hydrocarbons (PAHs): Your Environment, Your Health | National Library of Medicine.� U.S. National Library of Medicine, National Institutes of Health, 31 Apr. 2017, toxtown.nlm.nih.gov/chemicals-and-contaminants/polycyclic-aromatic-hydrocarbons-pahs.
Yang, Oneyeol, et al. �Endocrine-Disrupting Chemicals: Review of Toxicological Mechanisms Using Molecular Pathway Analysis.� Journal of Cancer Prevention, Korean Society of Cancer Prevention, 30 Mar. 2015, www.jcpjournal.org/journal/view.html?doi=10.15430%2FJCP.2015.20.1.12.
Over-the-counter or OTC remedies don’t do anything but give some temporary relief, if any at all, but the thing to take away here is that this kind of treatment can exacerbate the issue.
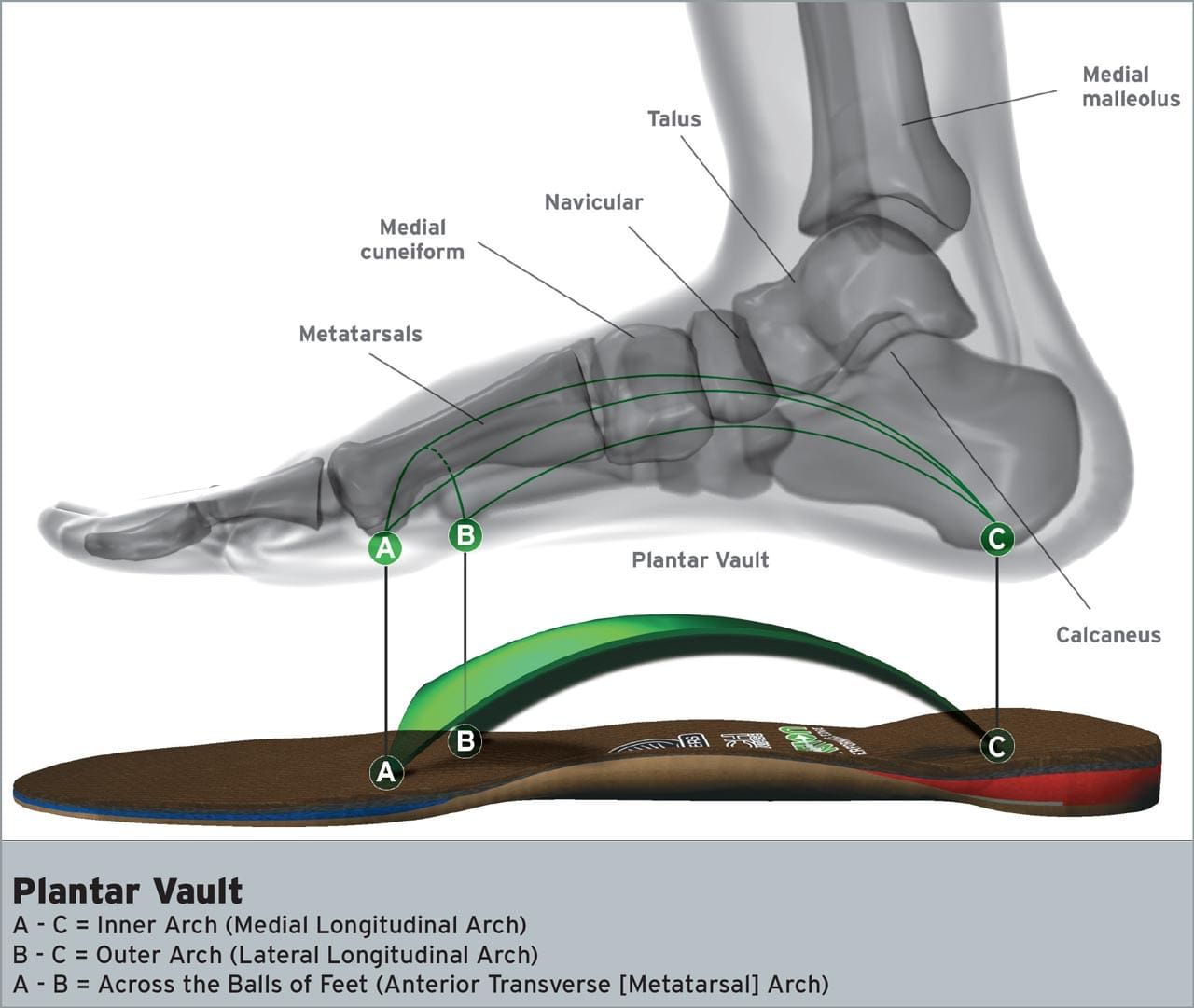
An example of this remedy solution is using store-bought shoe inserts that don’t provide support for the feet and can worsen the condition.
Over the counter, treatment can cost more money in the end, and all this without relief.
These types of insoles are not designed for long-term, daily use. This means they have to be replaced sooner.
Options like wraps and tape also give short-term relief but are not designed to treat the root cause to get rid of it.
Work with a professional to help you get a customized plant like an orthotic insole that will effectively treat the plantar fasciitis and bring long-lasting relief.
Self-Diagnosing & Treatment
This condition can be difficult to identify because of the varying symptoms. Patients could have all or only a few of them.
Symptoms include:
Sharp pain when waking up
Heel spurs
Painful arches
The causes can also vary and include:
Lifestyle
Weight
Age
Gender
Unique composition, shape, and size of the foot
Since it is different for everyone, many try to self-diagnose and do it incorrectly.
Then they try to create their own treatment plans which can be ineffective and dangerous.
Proper treatment requires professional medical attention and not just looking up symptoms online. Treatment is also more than just changing shoes or buying an insole at the local drug or shoe store.
Looking up symptoms and self-diagnosing is not a bad thing, but get a second opinion from a health professional like a chiropractor to make sure that you’re correct and to guide you in obtaining the proper treatment.
Pain Reliever Overuse
Pain relievers are not for treating pain caused by plantar fasciitis.
The convenience of pain relievers like Tylenol and acetaminophen makes it easy to take as soon as the pain kicks in.
The problem is that overuse can be dangerous to the body and can cause:
Kidney problems
Mask symptoms
Disguise other serious issues
Addiction potential�
The best treatment does not require pain relievers.
A professional can help you find relief without pills.
Not Listening to Professional Advice
Trying to schedule a doctor�s appointment can be overwhelming.
Trying to figure out what your insurance covers
Trying to find the time to see a doctor
Finding the right one
Many avoid it altogether and hope the pain goes away.
Many make assumptions about treatment that makes them avoid the doctor,
People have anxiety and are scared of the doctor or what the doctor will find.
There are plenty of excuses for not seeing a qualified professional that specializes in whatever condition you may have.
This is not the case here, the physical therapy or chiropractic care doesn’t go on for weeks or a bunch of follow up appointments.
Relief can be as simple as a customized orthotic insole and an adjustment to the lower back.
Reach out to a chiropractor that can identify, treat and get you moving and pain-free.
Pain and discomfort do not have to be part of normal life.
Saying age or lifestyle is the cause and there’s nothing you can do about it is ridiculous. Remember there are solutions to help prevent and maintain comfort within your body. Give us a call and let us help you live your life pain-free.
Plantar Fasciitis, Reduce *FOOT PAIN* with Custom Orthotics | El Paso, TX (2019)
Gloria Casillas experienced painful symptoms before visiting Dr. Alex Jimenez, a chiropractor in El Paso, TX. Gloria describes how her foot pain gradually developed into plantar fasciitis and how it tremendously affected her quality of life. Gloria Casillas discusses how custom foot orthotics helped her achieve foot pain relief from her plantar fasciitis. Gloria highly recommends Dr. Jimenez as the non-surgical choice for foot pain and plantar fasciitis. Gloria Casillas is grateful for the use of custom foot orthotics.
NCBI Resources
Feet are important. When you consider what your feet go through, taking 8,000 steps over the course of a day, according to the�Illinois Podiatric Medical Association�(IPMA), it�s easy to see how 75 percent of all Americans will have some type of�foot pain�at some point in their lives.�Plantar fasciitis is a common and very painful foot condition that can become chronic if not treated. It is also a condition that responds very well to chiropractic care. Chiropractic adjustments made to the heel and foot take the pressure off of the plantar fascia, allowing it to relax.
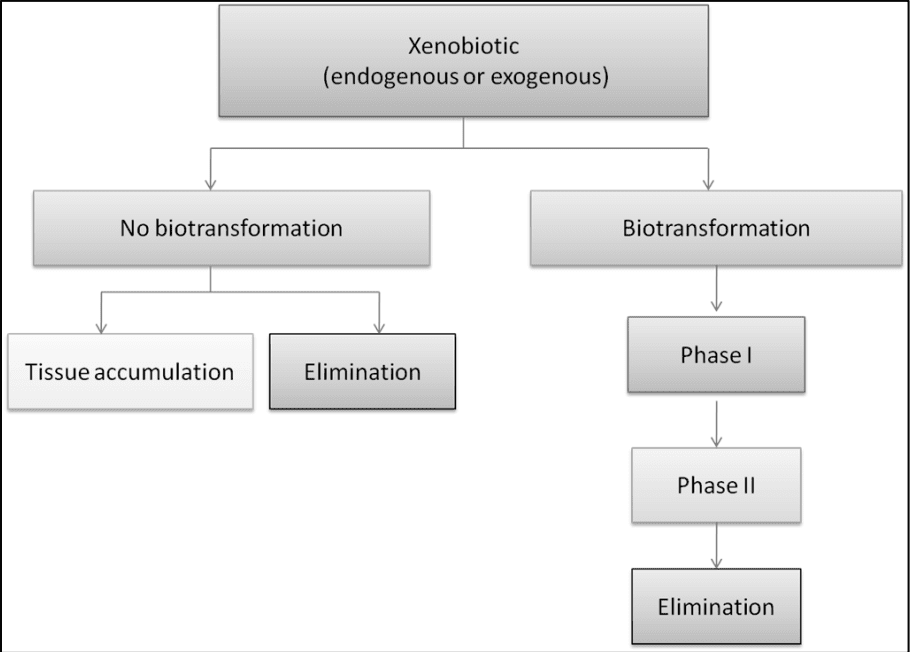
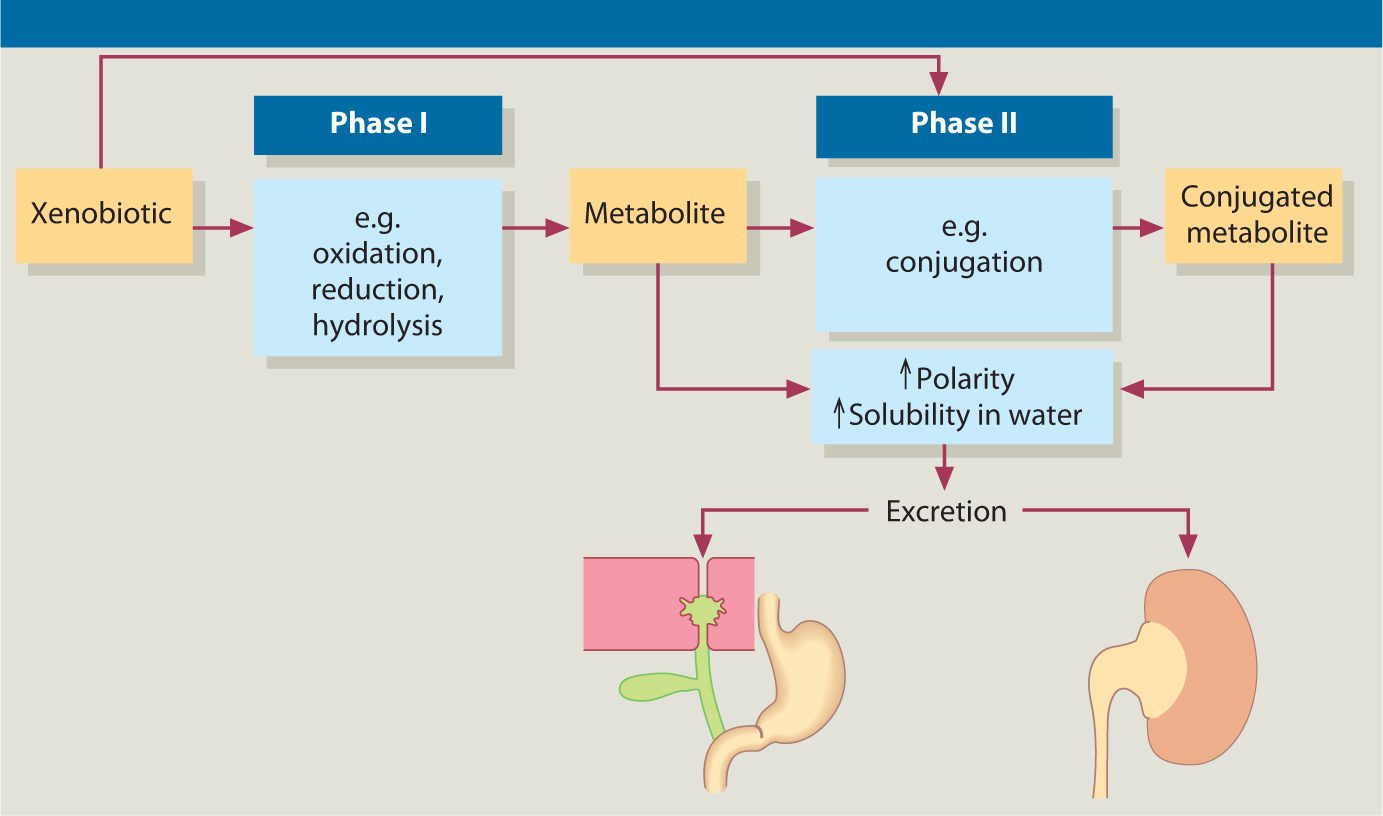
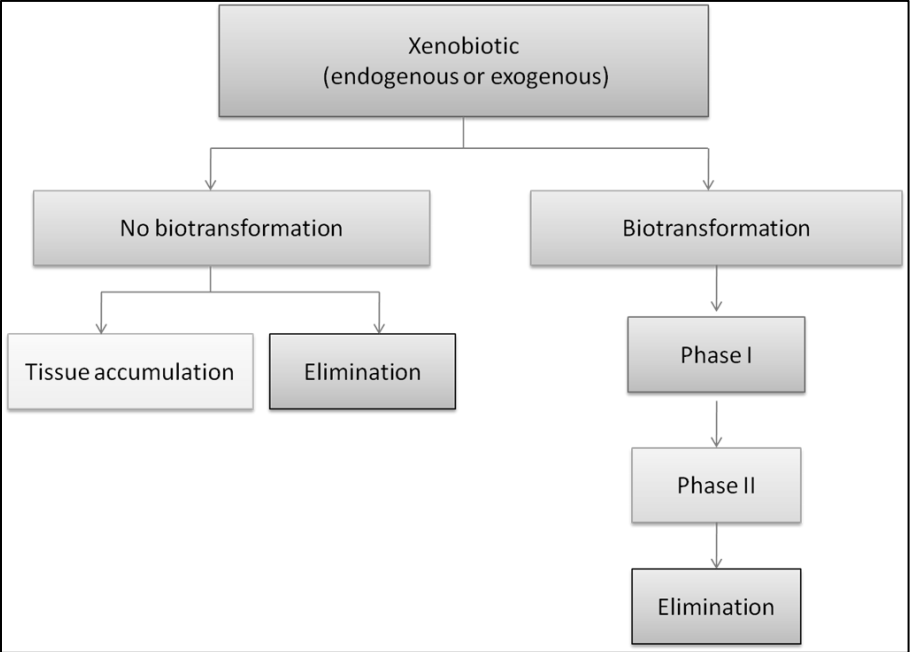
Biotransformation is the process of a substance changes from one chemical to another being transformed by a chemical reaction within the body. In the human body though, biotransformation is the process of rendering nonpolar (fat-soluble) compounds to polar (water-soluble) substances so they can be excreted in urine, feces, and sweat. It also serves as an important defense mechanism in the body to eliminate toxic xenobiotics out of the body through the liver. The liver is the one that takes these toxins and transformed them into suitable compounds to excrete out of the body as biotransformation.
Detoxification is also known as �detoxication� in literature. It is also a type of alternative medicine treatment that aims the body to get rid of unspecified �toxins.� It is highly important for a person to detox their body and with biotransformation, it can be classified into two categories, under normal sequences, which tends to react with a xenobiotic. They are called Phase 1 and Phase 2 reactions that help the body with detoxification.
Phase 1 Reactions
Phase 1 reaction is consisting of oxidation-reduction and hydrolysis. Research shows that Phase 1 is generally the first defense employed by the body to biotransform xenobiotics, steroid hormones, and pharmaceuticals. They create CYP450 (cytochrome P450) enzymes and are described as functionalization microsomal membrane-bound that are located in the liver but can also be in enterocytes, kidney, lungs and the brain in the body. The CYP450 enzymes can be beneficial or have consequences for an individual�s response to the effect of a toxin they are exposed to.
Studies have been shown that phase 1 reactions have been affecting the elderly population. It states that hepatic phase 1 reaction involving oxidation, hydrolysis, and reduction appears to be more altered by age since the elderly population comprises the fastest-growing segment of the world�s population. It also states that there is a predictable, age-related decline in cytochrome P-540 function and combined with the polypharmacy that much of the elderly population experiences, this may lead to a toxic reaction of medication.
Phase 2 Reaction
Phase 2 reaction is part of the cellular biotransformation machinery and is a conjugation reaction in the body. They can involve the transfer of a number of hydrophilic compounds to enhanced the metabolites, and the excretion in the bile or urine in the body. The enzymes in Phase 2 reaction can also comprise multiple proteins and subfamilies to play an essential role in eliminating the biotransformed toxins and metabolizing steroid hormones and bilirubin in the body.
Phase 2 enzymes can function not only in the liver but also in other tissues like the small intestines. When it combined with Phase 1, they can help the body naturally detox the toxins that the body may encounter. Hormones, toxins, and drugs undergo a hepatic transformation by Phase 1 and Phase 2 pathways in the liver, then are eliminated by phase 3 pathways.
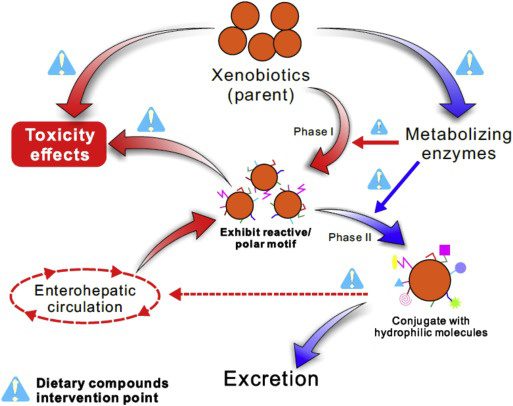
Xenobiotics
Xenobiotics has been defined as chemicals that undergo metabolism and detoxication to produce numerous metabolites, some of which have the potential to cause unintended effects such as toxicity. They can also block the action of enzymes or receptors used for endogenous metabolism and produce liver damage to a person. Xenobiotics like drugs, chemotherapy, food additives, and environmental pollutants can generate serval free radicals that lead to an increase of oxidative stress in the cells. Accumulation of oxidative stress in the body can lead to an increase in potential cellular reduction in the body.
Research shows that the body has a major challenge when it is detoxifying xenobiotics out of the body system and the body must be able to remove the almost-limitless number of the xenobiotic compounds from the complex mixture of chemicals that are involved in normal metabolism.
Studies even show that if the body doesn�t have a normal metabolism, many xenobiotics would reach toxic concentrations. It can even reach the respiratory tract either through airborne toxins or the bloodstream. It is important to make sure that the body and especially the liver to be healthy. Since the liver is the largest internal organ, it is responsible for detoxifying the toxins out of the body as urine, bile, and sweat.
Conclusion
Biotransformation is the process of substance changes from one chemical to another. In the body, it is a process of rendering fat-soluble compounds to water-soluble compounds, so it can be excreted out of the body as either urine, feces, or sweat. The liver is the one that causes toxic xenobiotics to transform into biotransformation and going through phase 1 and 2 to excrete the toxins out of the body for a healthy function.
Phase 1 reactions in the body are the first line of defense of the body detoxifying itself. Phase 2 creates CYP450 (cytochrome P450) that helps the body take the xenobiotic toxins and oxidates to reduce and hydrolysis the toxins to metabolites. Those metabolites then transform into Phase 2 reactions, which conjugates the metabolites in the body to be excreted out of the body. There are many factors that can make the body have xenobiotics, but the liver is the main organ to detoxify the xenobiotics out of the system. If there is an abundance of xenobiotics in the body, it can cause toxicity reaction causing the body to develop chronic illnesses. These products are known to help support the intestines and liver detoxication as well as, to help support hepatic detoxication for optimal healthy body function.
October is Chiropractic Health Month. To learn more about it, check out Governor Abbott�s bill on our website to get full details.
The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or chronic disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
References:
Chang, Jyh-Lurn, et al. �UGT1A1 Polymorphism Is Associated with Serum Bilirubin Concentrations in a Randomized, Controlled, Fruit and Vegetable Feeding Trial.� The Journal of Nutrition, U.S. National Library of Medicine, Apr. 2007, www.ncbi.nlm.nih.gov/pubmed/17374650/.
Croom, Edward. �Metabolism of Xenobiotics of Human Environments.� Progress in Molecular Biology and Translational Science, U.S. National Library of Medicine, 2012, www.ncbi.nlm.nih.gov/pubmed/22974737.
Hindawi, Unknown. �Xenobiotics, Oxidative Stress, and Antioxidants.� Xenobiotics, Oxidative Stress, and Antioxidants, 17 Nov. 2017, www.hindawi.com/journals/omcl/si/346976/cfp/.
Hodges, Romilly E, and Deanna M Minich. �Modulation of Metabolic Detoxification Pathways Using Foods and Food-Derived Components: A Scientific Review with Clinical Application.� Journal of Nutrition and Metabolism, Hindawi Publishing Corporation, 2015, www.ncbi.nlm.nih.gov/pmc/articles/PMC4488002/.
Kaye, Alan D, et al. �Pain Management in the Elderly Population: a Review.� The Ochsner Journal, The Academic Division of Ochsner Clinic Foundation, 2010, www.ncbi.nlm.nih.gov/pmc/articles/PMC3096211/.
panelEdwardCroom, Author links open overlay, et al. �Metabolism of Xenobiotics of Human Environments.� ScienceDirect, Academic Press, 11 Sept. 2012, www.sciencedirect.com/science/article/pii/B9780124158139000039.
Sodano, Wayne, and Ron Grisanti. �The Physiology and Biochemistry of Biotransformation/Detoxification.� Functional Medicine University, 2010.
Unknown, Unknown. �ToxTutor – Introduction to Biotransformation.� U.S. National Library of Medicine, National Institutes of Health, 2017, toxtutor.nlm.nih.gov/12-001.html.
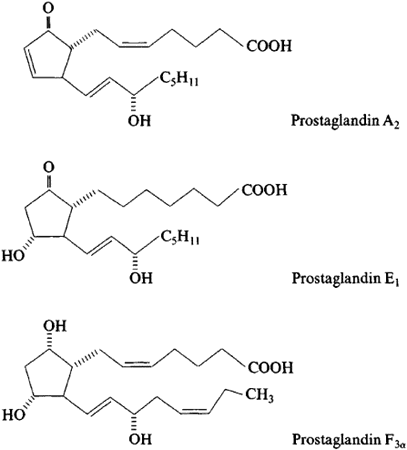
Prostaglandins are different than hormones. They are not secreted from a gland that can be carried through the bloodstream and work on specific areas around the body. Prostaglandins are made by a chemical reaction in the body that can be made in all the organs and are part of the body�s way of dealing with injuries and illnesses.
When any part of the body has been damaged, prostaglandins are made at the site of tissue damage or infection where they cause inflammation, pain and fever as part of the body�s healing process. When there is a high level of prostaglandins in the body due to the natural healing process from injuries and inflammation, it can contribute to several diseases from the unwanted inflammation.
Prostaglandins in the Omega fatty acids
In omega-6 fatty acids, DGLA (dihomo-gamma-linolenic acid) creates Prostaglandin E1(PG-1) as anti-inflammatory receptors in the body. In omega-3 fatty acids, they can create Prostaglandin E3 (PG-3) that are also anti-inflammatory receptors as well. PG-1 and PG-3 help prevent blood clotting in the body system.
When it comes to pro-inflammatory receptors, omega-6 fatty acids have these receptors as well. Pro-inflammatory receptors are created by arachidonic acid. Arachidonic acid creates Prostaglandin E2 (PG-2), which is responsible for inflammation, swelling and clotting as well.
There has to be a balance between PG-2 and PG-1,3 to provide a healthy function in the body and an ideal hormone signaling response. When one of the PGs are being disrupted by trans-fatty acids from food, it can cause health problems to a person.
Deficiencies in Prostaglandins
Trans fatty acids are a form of unsaturated fats that can be either natural or artificial. They are produced either by hydrogenation of unsaturated oils or by biohydrogenation in the stomach of ruminant animals. Numerous studies have been shown that consuming trans fatty acids continuously can increase the risk of cardiovascular diseases. This can also increase the ratio of LDL cholesterol to HDL cholesterol in the body. Trans fatty acids can block the activity of D6D (delta-6-desaturase), which is the first step in prostaglandin synthesis from essential fats in the diet.
The excess sugar consumption, insulin surges, inflammation, protein deficiencies hypothyroidism, and alcohol consumption will impair the activity of D6D and be a marker of accelerating aging to the human body. When a person has an increased consumption from fried foods and vegetable oils in an Western diet will shift the omega-6 pathway from PG-1 and into PG-2 production in the body. With the current American diet, people consume a high quantity of omega-6 fatty acids and low quantity of omega-3 fatty acids. This will cause a strong reaction of an inflammatory prostaglandin shift.
Since prostaglandins are caused by injuries and inflammation to heal the body, when an individual consumes a high omega-6 diet, it can cause an excessive amount of inflammation to the body and it can lead to chronic illnesses.
More Deficiencies in Prostaglandins
A deficiency in nutrients like nicotinic acid, pyridoxal 5� -phosphate, calcium, magnesium, zinc, and molybdenum is required for the desaturase and elongase enzymes in omega-6 and omega-3 fatty acids. Their deficiency can lead to improper production of prostaglandins. So EFAs from diets cause overconsumption of omega-6 and a lack of essential fatty acids in the body.
After that happens, then the EFAs can be synthesized into prostaglandins with desaturase and elongase enzymes. This will then cause nutrient deficiencies and metabolic factors can impair and downregulate those enzymes and causing the body to be prone to pro-inflammatory.
When that happens, prostaglandin formation will suddenly turn into abnormal ratios in the body causing problems, excessive inflammation in the endocrine glands and the body organs, and soon later on if it is not fixed, chronic illnesses will cause proper hormones to alter their components and either stop producing or create an abundance in the body.
Conclusion
Prostaglandins are a chemical reaction to the body that are different than hormones. They are caused when the body is injured and it causes inflammation so it can naturally heal itself. When there is an excessive amount of prostaglandins in the body it can lead to chronic inflammation and cause an abnormal shift in the body�s functional state. A factor that can affect the prostaglandins as well is the excessive consumption of omega-6 fatty acids. This consumption can cause inflammation and can make the body feel sluggish and not feeling great. There are products that can help the body, especially balancing the production of essential fatty acids and metabolizing the body for optimal health.
October is Chiropractic Health Month. To learn more about it, check out Governor Abbott�s bill on our website to get full details.
The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or chronic disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
References:
F.Horrobin, David. �Loss of Delta-6-Desaturase Activity as a Key Factor in Aging.� Medical Hypotheses, Churchill Livingstone, 22 Mar. 2004, www.sciencedirect.com/science/article/abs/pii/0306987781900645.
Horrobin, D F. �Fatty Acid Metabolism in Health and Disease: the Role of Delta-6-Desaturase.� The American Journal of Clinical Nutrition, U.S. National Library of Medicine, May 1993, www.ncbi.nlm.nih.gov/pubmed/8386433.
Innes, Jacqueline K, and Philip C Calder. �Omega-6 Fatty Acids and Inflammation.� Prostaglandins, Leukotrienes, and Essential Fatty Acids, U.S. National Library of Medicine, May 2018, www.ncbi.nlm.nih.gov/pubmed/29610056.
Iqbal, Mohammad Perwaiz. �Trans Fatty Acids – A Risk Factor for Cardiovascular Disease.� Pakistan Journal of Medical Sciences, Professional Medical Publicaitons, Jan. 2014, www.ncbi.nlm.nih.gov/pmc/articles/PMC3955571/.
Leech, Joe. �What Are Trans Fats, and Are They Bad for You?� Healthline, 30 July 2019, www.healthline.com/nutrition/why-trans-fats-are-bad.
Ricciotti, Emanuela, and Garret A FitzGerald. �Prostaglandins and Inflammation.� Arteriosclerosis, Thrombosis, and Vascular Biology, U.S. National Library of Medicine, May 2011, www.ncbi.nlm.nih.gov/pmc/articles/PMC3081099/.
Tallima, Hatem, and Rashika El Ridi. �Arachidonic Acid: Physiological Roles and Potential Health Benefits – A Review.� Journal of Advanced Research, Elsevier, 24 Nov. 2017, www.ncbi.nlm.nih.gov/pmc/articles/PMC6052655/.
Unknown, Unknown. �Prostaglandins.� You and Your Hormones, Dec. 2016, www.yourhormones.info/hormones/prostaglandins/.
Wang, Xiaoping, et al. �Multiple Roles of Dihomo-?-Linolenic Acid against Proliferation Diseases.� Lipids in Health and Disease, BioMed Central, 14 Feb. 2012, www.ncbi.nlm.nih.gov/pmc/articles/PMC3295719/.
Dr. John Coppola and Dr. Valerie Monteiro understand the symptoms associated with peripheral neuropathy. While many healthcare professionals describe peripheral neuropathy as an irreversible and permanent health issue which can only be managed through the utilization of drugs/medications, Dr. John Coppola and Dr. Valerie Monteiro can help treat peripheral neuropathy symptoms by treating the source of the health issue.
Low-level laser therapy (LLLT) is a non-invasive treatment approach that can help naturally increase oxygen, blood flow, and circulation in the human body. LLLT can also stimulate the mitochondria, often known as the powerhouses of the cell, to stimulate recovery in the human body. Dr. John Coppola and Dr. Valerie Monteiro explain how low-level laser therapy can help treat peripheral neuropathy symptoms and stimulate overall well-being. Dr. Alex Jimenez, a chiropractor in El Paso, TX, can help treat peripheral neuropathy symptoms as well as a variety of other health issues.
Low-Level Laser Therapy (LLT) for Peripheral Neuropathy El Paso, TX.
Neuropathy is a medical term used to describe a collection of general diseases or malfunctions which affect the nerves.
The causes of neuropathy, or nerve damage, can vary among individuals and these may be caused by different:
Diseases
Injuries
Infections
Vitamin deficiencies
Neuropathy can also be classified according to the location of the nerves being affected and according to the disease-causing it.
Furthermore, depending on which nerves are affected will depend on the symptoms that will manifest.
Peripheral neuropathy is simply referred to as neuropathy, which is a state that happens when the nerves become damaged or injured, oftentimes simply disturbed.
It�s estimated that neuropathy affects roughly 2.4 percent of the general populace and approximately 8 percent of people older than age 55.
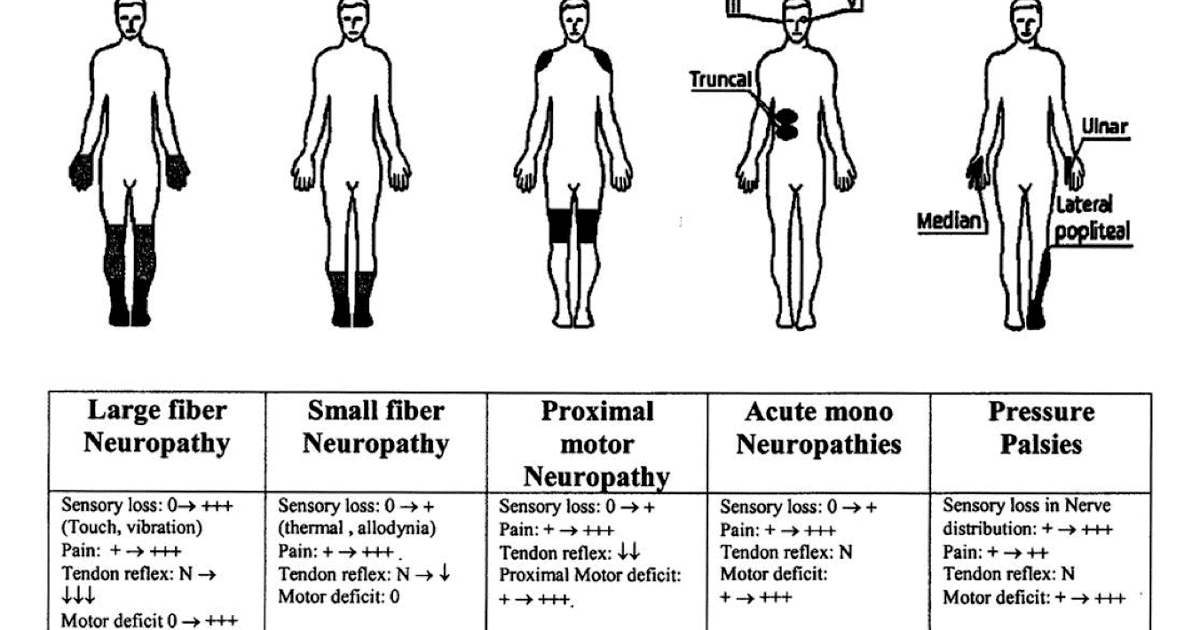
Type
Neuropathy can affect any of the three types of peripheral nerves:
Sensory nerves�transmit messages from sensory organs:
Eyes
Nose
Brain
Motor nerves track the movement of the muscles
Autonomic nerves regulate the involuntary body functions
Sometimes, neuropathy will only impact one nerve. This is medically referred to as mononeuropathy and instances of it include:
Ulnar neuropathy affects the elbow
Radial neuropathy affects the arms
Peroneal neuropathy affects the knees
Femoral neuropathy affects the thighs
Cervical neuropathy affects the neck
Sometimes, two or more isolated nerves in separate regions of the body can become damaged, injured or disrupted, resulting in mono neuritis multiplex neuropathy.
Most of the time, multiple peripheral nerves malfunction at the same time, a condition called polyneuropathy.
Cause
Neuropathies are often inherited from birth or they develop later in life.
The most frequent inherited neuropathy is the Charcot-Marie-Tooth disease, which affects 1 in 2,500 people in the USA.
Although healthcare professionals are sometimes not able to pinpoint the exact reason for an acquired neuropathy, medically referred to as idiopathic neuropathy.
There are many known causes for them, including:
Systemic diseases – a systemic disease is one that affects the whole body.
Physical trauma
Infectious diseases
Autoimmune disorders
The most frequent systemic cause behind peripheral neuropathy is diabetes, which can lead to chronically high blood glucose levels that harm nerves.
Other systemic issues can cause neuropathy, including:
Kidney disorders permit high levels of nerve-damaging toxic chemicals to flow in the blood
Toxins from exposure to heavy metals include:
Arsenic
Lead
Mercury
Thallium
Drugs/medications, including anti-cancer medications, anticonvulsants, antivirals, and antibiotics
Chemical imbalances because of liver illnesses.
Hormonal diseases, like hyperthyroidism, which disturbs metabolic processes, and potentially induces cells and body parts to exert pressure on the nerves.
Deficiencies in vitamins, such as E, B1 (thiamine), B6 (pyridoxine), B12, and niacin can be vital for healthy nerves.
Alcohol abuse induces vitamin deficiencies and could harm nerves.
Cancers and tumors can exert damaging pressure on nerve fibers and paths.
Chronic inflammation can damage protective tissues around nerves, which makes them more vulnerable to compression, getting inflamed and swollen.
Blood diseases and blood vessel damage, which may damage or injure nerve tissue by decreasing the available oxygen supply
Symptoms
Depending on the reason and unique to each patient, signs, and symptoms of neuropathy can include:
Symptoms are dependent on autonomic, sensory, or motor nerves or a combination are affected.
Autonomic nerve damage can start a chain reaction of physiological functions like blood pressure or create gastrointestinal problems and issues.
Damage or dysfunction in the sensory nerves may impact sensations and sense of equilibrium or balance, while injury to motor nerves affects movement and reflexes.
When both sensory and motor nerves are involved, the condition is known as sensorimotor polyneuropathy.
Complications
Peripheral�neuropathy�may result in several complications, as a result of disease or its symptoms.
Numbness from the ailment can allow you to be less vulnerable to temperatures and pain, making you more likely to suffer from burns and serious wounds.
The lack of sensations in the feet, for instance, can make you more prone to developing infections from minor traumatic accidents, particularly for diabetics, who heal more slowly than other people, including foot ulcers and gangrene.
Furthermore, muscle atrophy may cause you to develop particular physical disfigurements, such as pes cavus, a condition marked by an abnormally high foot arch, and claw-like deformities in the feet and palms.
Treatment
The first step in neuropathy treatment should be finding the root cause that’s causing the neuropathy.
Treatment of diseases such as:
Diabetes
Guillain-Barre syndrome
Rheumatoid arthritis
Sarcoidosis
Other underlying diseases
Prevents continued nerve damage and in cases heals the damaged nerves.
If you are unaware of any underlying disease that is causing the peripheral neuropathy, make sure to let your doctor know of abnormal symptoms.
Medication
Peripheral neuropathy can be treated with various medications.
The first type used to treat mild symptoms are:
Over-the-counter pain medications
In more severe cases:
Opiates
Narcotic medications
Anti-seizure medications
A doctor may prescribe a lidocaine patch or anti-depressants to relieve symptoms.
Patients should thoroughly discuss�neuropathymedication with a doctor before proceeding.
Chiropractic/Massage/Physical Therapy
Various manual therapies can benefit symptoms in neuropathy treatment.
A therapist or chiropractor will perform various manipulation techniques, and teach exercises and stretches to help improve symptoms combined with increased muscle strength/control.
A therapist may also recommend braces or splints to improve mobility.
Patients should attend all physical therapy sessions to gain maximum benefits.
Low-level-laser-therapy LLT
The primary and most debilitating symptom of diabetic peripheral neuropathy is a sensation of tingling, prickling, buzzing, pinching, burning, and/or sharp jabbing stabbing pain in the feet.
Low-Level Laser Therapy (LLLT) takes information from the receptors on the membrane of the cell and mitochondrion or the engine of the cell.
This information reaches the cell’s DNA, that directly controls cell function.
When cells receive better information, they work better, along with the tissues they make up like:
Bones
Cartilage
Tendons
Ligaments
LLT promotes the healing and regeneration of damaged tissues,� and its�systemic effects on tissue function are also carried throughout the body by blood and meridians or energy channels.
The key basic physiological effects of low-level laser light include:
Increased cell membranepolarization/permeability
Adenosine-5-triphosphate (ATP) production and respiratory activity
Enzyme activity
Collagen and epithelial production
Capillary formation
Macrophage (immune system) activity
Analgesic effects due to elevated endorphin production
Electrolytic nerve blockage
Improved blood and lymph flow
An anti-inflammatory effect from improved circulation and accelerated tissue regeneration
Increased production of antioxidants
An additional benefit is that the light energy from low-level lasers will only be absorbed by cells and tissues that are not functioning normally and do not go after healthy cells.
Low-level laser therapy has the potential of providing an effective means of reducing low back pain that is:
Simple
Quick
Non-invasive
Side-effect free
Acids
Supplements like:
Essential acids called ALA (alpha-Lipoic acid)
GLA (gamma-linolenic acid) and omega-3 fatty acids
These can have a beneficial effect on diabetic peripheral neuropathy.
L-Carnitine
L-carnitine is a substance that the body makes and stores in the:
Liver
Brain
There have been reports that certain diabetics with neuropathy symptoms could regain regular sensation in the limbs when they increased their consumption of carnitine called acetyl-L-carnitine.
Red meat
Peanut butter
Dairy products
Are good dietary sources of this nutrient.
Supplements are also available at health food stores and pharmacies and health/wellness clinics.
While every type of neuropathy, such as diabetic neuropathy or autoimmune disease-associated neuropathy, develops its own unique group of symptoms, many patients will often report common complaints. Individuals with neuropathy generally describe their pain as stabbing, burning or tingling.�Low-level laser therapy can help relieve these symptoms.
If you experience unusual or abnormal tingling or burning sensations, weakness and/or pain in your hands and feet, it�s essential to seek immediate medical attention in order to receive a proper diagnosis of the cause of your specific signs and symptoms. Early diagnosis can help prevent further nerve injury.� And early laser treatment can help before symptoms really become severe. Visit http://www.neuropathycure.org.
Of all of the wide array of health issues that healthcare professionals talk to their patients about, there is one which is tremendously overlooked and not taken seriously: brain fog. Many people suffer from brain fog and fatigue and unfortunately, many people are left to fend for themselves when it comes to this health issue. Patients describe feeling as if they’re living in a haze, their lives passing them by. Instead of being engaged in the present moment, patients describe feeling as though they’re seeing life from a distance. Their thinking is no longer sharp, and their brilliant minds are sidelined. �
Why do health issues like these fall through the cracks of conventional medicine? This may be because there’s currently no definitive treatment available for brain fog. The purpose of the following article is to discuss the causes of inflammation and brain fog. Understanding the reasons for this type of health issue may hopefully help shine a new light on future treatments. �
Brain Fog and Inflammation
Inflammation is an essential part of the immune system. We need inflammation to protects us from injury, infection, and illness. However, as with everything else in the human body, it is all about balance. An excessive amount of inflammation can cause the blood-brain barrier (BBB) to become more permeable, leading to brain inflammation. Neuroinflammation is sometimes known as “leaky brain syndrome” and this inflammatory oxidative stress (OS) in the hypothalamus of the brain is ultimately believed to be the root cause of brain fog, among other neurological diseases, such as Alzheimer’s disease. �
Hidden Causes of Inflammation and Brain Fog
“Brain fog”, however, is very much considered to be a general term for the actual health issue. The name tells you exactly what it is (diminished brain function), however, it doesn’t exactly tell you what’s causing the brain inflammation in the first place. Let’s dig deeper into the reasons for brain fog. We will describe the main causes of brain fog, according to researchers. �
Thyroid Problems
Every cell in the human body depends on thyroid function to be healthy and to be able to operate at full capacity. Thyroid hormone imbalances have been demonstrated to cause inflammatory reactions. The thyroid functions by receiving the proper messages in the brain during the hypothalamic-pituitary-thyroid (HPT) axis. Therefore, if the hypothalamus is inflamed, it can cause dysfunction in the brain-thyroid axis. The final result? A vicious cycle of inflammation. �
Adrenal Fatigue
As you’ve got the brain-thyroid axis, you also have the brain-adrenal (HPA) axis. Dysfunctions of the hormonal circadian rhythm are known as an adrenal disorder. During fatigue, your stress hormone cortisol can be found all over the region and this imbalance can stress out your system. The same as thyroid problems, brain fog can be both the cause and the consequence of adrenal fatigue because of the brain-hormone connection, among other essential functions in the body. �
Viral Infections
Low-grade chronic viral infections, such as Epstein-Barr virus (EBV), are connected to a wide array of inflammatory ailments like chronic fatigue syndrome. The brain needs vitamin D to flourish and EBV has been demonstrated to actually block the body from utilizing it. Viral infections, if left untreated, can also trigger excess inflammation, leading to many health issues.
Leaky Gut Syndrome
The gut and the brain are unmistakenly connected, they are even formed from the exact same fetal tissue when you’re growing in your mother’s uterus. According to a variety of research studies, leaky gut syndrome is associated with an increase in gut toxins, known as LPS, which have been demonstrated to affect inflammation and brain fog. �
Candida Overgrowth
Researchers state that excess yeast in the microbiome, by way of instance, candida overgrowth, can also ultimately increase the inflammatory cells IL-1, IL-6, and TNF, which may contribute to too much inflammation in the human brain and body. �
Histamine Intolerance
Several people, especially people with all of the gut problems mentioned above, are more prone to experiencing something known as histamine intolerance. This happens when the body does not break down the cell histamine and it causes a discharge of superoxide, a well-known free radical which brings about a lot of inflammation and other health issues. �
Inflammatory Foods
Inflammatory foods high in sugar, gluten (wheat, rye, barley, spelt, and oats), or casein (dairy products) are a problem for many men and women. Free radical harm can triple by higher blood glucose levels from these inflammatory foods. �
Toxins
Toxins like mold and heavy metals are just two overlooked factors that can contribute to brain fog in patients. �
Poor Sleep
If you’re not sleeping properly at night, you don’t need me to tell you that it affects your brain health. The antioxidant glutathione, which increases stress from the hypothalamus, can ultimately cause brain fog due to a lack of sleep. �
Methylation Impairments
Methylation is a big biochemical superhighway that happens 1 billion times every second in the human body. It makes your brain healthy and it can help detox your body. People who have hereditary methylation problems may often have a difficult time detoxing and their body may ultimately not be able to regulate or manage inflammation, including neuroinflammation. �
Brain inflammation has been associated with a variety of signs and symptoms, including brain fog. Inflammation in the brain can also cause a variety of neurological diseases, such as Alzheimer’s disease. Inflammation is an essential function of the human body, however, too much brain inflammation, can cause brain fog and other health issues. In the following article, inflammation and brain fog can be caused by a variety of factors, including leaky gut syndrome and inflammatory foods, among others. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
Metabolic Assessment Form
The following Metabolic Assessment Form can be filled out and presented to Dr. Alex Jimenez. Symptom groups listed on this form are not intended to be utilized as a diagnosis of any type of disease, condition, or any other type of health issue. �
In honor of Governor Abbott’s proclamation, October is Chiropractic Health Month. Learn more about the proposal. �
Of all of the wide array of health issues that healthcare professionals talk to their patients about, there is one which is tremendously overlooked and not taken seriously: brain fog. Many people suffer from brain fog and fatigue and unfortunately, many people are left to fend for themselves when it comes to this health issue. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or chronic disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
References:
Cole, William. �Here’s Exactly What To Do About Brain Fog: A Functional Medicine Expert Explains.� Mindbodygreen, Mindbodygreen, 17 Feb. 2017, www.mindbodygreen.com/0-28772/heres-exactly-what-to-do-about-brain-fog-a-functional-medicine-expert-explains.html.
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Neural Zoomer Plus for Neurological Disease
� �
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention. �
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force.
Inflammation is the human body’s natural response to injury, infection, or illness. However, too much inflammation can affect your overall health and wellness, especially when you have inflammation in the brain. Brain inflammation can even affect your mental and emotional well-being. Understanding the causes and symptoms of inflammation in the brain can help determine the best treatment option. Dr. Santosh Kesari describes that brain inflammation can be due to various reasons, including toxins like tobacco or alcohol, diabetes, hypertension, infections, trauma, aging, diet, and stress. �
“Some inflammation is acute, short-lasting, and possibly reversible but other types of inflammation are chronic and continue to cause brain damage,” Dr. Kesari states. “These may be cumulative and not readily reversible, such as Alzheimer’s disease.” With an overactive immune system, such as in people who have multiple sclerosis or encephalitis which is inflammation in the brain, several people may already be genetically predisposed to experience brain inflammation. Severe inflammation can lead to a variety of symptoms, it may also result in coma, brain damage, or death. The following 7 signs and symptoms may indicate inflammation in the brain. Make sure to seek immediate medical attention if brain inflammation is suspected. �
Brain Fog
If we’re talking about chronic inflammation caused by exposure to toxins or due to poor lifestyle habits, brain fog, as well as decreased cognitive abilities, can be some signs and symptoms of inflammation in the brain. You may ultimately lose your train of thought constantly when you have brain fog and you’ll frequently have trouble focusing on your regular tasks and daily activities. As Dr. Carolyn Dean, author of 365 Ways to Boost Your Brain Power, states, restricting dairy consumption or foods that can cause inflammation, smoking, and alcohol, may help improve these signs and symptoms of brain fog.
Mood Changes
As soon as your brain is inflamed, you may also experience signs and symptoms of depression. This type of brain inflammation is generally associated with poor lifestyle habits. As a nutritional therapist and health coach, Christina Tsiripidou informs us that eating meals that are high in proteins or altered proteins as well as low in veggies and fats, can contribute to brain inflammation. Not getting enough sleep and stress can also make these signs and symptoms worse. �
Fatigue
When your brain has inflammation, you may not only experience brain fog but you may also experience fatigue which commonly accompanies it. According to Caleb Wellness, Health and Backe Expert for Maple Holistics, small modifications in diet and lifestyle habits can be very powerful. Besides curbing your sugar and caffeine intake, it’s important to eat foods which are full of B vitamins and fatty acids. “Besides providing you with a much-needed energy boost, these types of foods also function by minimizing inflammation, which has been linked to increased brain fog and other health issues,” Backe says. �
Headaches And Migraines
Occasionally, headaches and migraines can be caused by poor lifestyle habits, but sometimes, it may also be brought on by more serious health issues that may require immediate medical attention. By way of instance, acute headaches can be an indication of inflammation and even swelling in the brain. As Dr. Kesari says, “This is very uncommon and it is generally associated with other neurological signs and symptoms typically due to either mass lesions or illnesses.” Often times, you also can’t really tell if a headache is brought on by a much more serious health issue, so he proposes that you should ultimately consult with your healthcare professional if your headaches last more than usual and they seem unusual. �
Neck Stiffness
Another more serious sign and symptom of brain inflammation is neck stiffness. As Dr. Dean states, this too can indicate swelling in the brain. Meningitis and encephalitis, which are disorders that cause inflammation around the brain and spinal cord, are often caused by viruses or bacteria. If you’re experiencing neck stiffness accompanied by fever, along with headaches or migraines, make sure to see your healthcare professional right away as this may suggest a serious health issue. �
Nausea or Vomiting
Encephalitis may give you feelings of nausea, Dr. Dean says. The usual cause of this type of brain inflammation is a viral infection, such as the herpes simplex virus. In reality, brain inflammation due to herpes constitutes 10 percent of all cases of encephalitis in the United States annually. Other common signs and symptoms include a stiff neck, general weakness, and nausea or vomiting. Make sure to talk to your healthcare professional if you notice any of these signs and symptoms. �
Vision Problems
Healthcare professionals can test your eyes and detect early signs and symptoms of a stroke, a brain tumor, or even Alzheimer’s disease, among other health issues associated with brain inflammation. The brain and the eyes are connected. It is not surprising that when your brain has inflammation, your vision can also ultimately be influenced, Dr. Dean says. � If you’re experiencing any of these signs and symptoms, talk to your healthcare professional. According to Dr. Kesari, the treatment depends on the signs and symptoms. Brain imaging, blood work, and spinal fluid analysis may be needed based on the clinical presentation. For severe symptoms, inflammation is treated with different immunosuppressive treatments including steroids, IVIG, plasmapheresis, and Rituxan. When the source of chronic brain inflammation is lifestyle-related, adjustments to diet, working on stress and also the elimination of habits, such as smoking, may ultimately help. �
Acute and chronic brain inflammation has been associated with a variety of signs and symptoms, including depression, cognitive, and other mental health issues. Inflammation in the brain can even cause a variety of neurological diseases, such as Alzheimer’s disease. Inflammation is an essential function of the human body, however, too much inflammation, especially in the brain, can alter our overall health and wellness. Make sure to talk to your healthcare professional if you experience any unusual signs and symptoms associated with brain inflammation. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
Metabolic Assessment Form
The following Metabolic Assessment Form can be filled out and presented to Dr. Alex Jimenez. Symptom groups listed on this form are not intended to be utilized as a diagnosis of any type of disease, condition, or any other type of health issue. �
In honor of Governor Abbott’s proclamation, October is Chiropractic Health Month. Learn more about the proposal. � Inflammation is the human body’s natural response to injury, infection, or illness. However, too much inflammation can affect your overall health and wellness, especially when you have inflammation in the brain. Brain inflammation can even affect your mental and emotional well-being. Inflammation in the brain is associated with neurological disorders. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or chronic disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Neural Zoomer Plus for Neurological Disease
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention. �
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force.
Trouble concentrating, mood swings, headaches, and fatigue could be a common occurrence in one’s day to day life.� These symptoms are commonly brushed off as lack of sleep but did you know these symptoms are also side effects of hormone imbalance?�
Hormone imbalance is fairly common and can be tested for and treated. One of the most accurate tests to date that checks for hormone imbalances is the D.U.T.C.H test.�
What Is It?
D.U.T.C.H is a type of hormone testing that stands for Dried Urine Test for Comprehensive Hormones. Dried urine samples make it possible for scientists to see a whole day of hormones and quantify aspects that are distinct. Unlike obtaining information from a blood draw, urine contains different components that provide scientists with a new line of insight.
What Is The Goal?
When it comes to a hormone imbalance, the adrenal glands may have a large impact. The adrenals are two small glands that sit on top of the kidneys. These small glands are responsible for producing vital hormones such as sex hormones and cortisol. These hormones help the body respond to stress along with other functions.�
With the turn around time being around 10 business days, individuals can gain control and receive the insight they may have been missing. �Precision Analytical (the founders of D.U.T.C.H) employs the most innovative instruments to achieve the best outcomes for patients. The main purpose is to create an understanding of what is currently going on in the patient’s body and allows the treatment to become more specific and targeted to the needs of the individual.
There are different D.U.T.C.H tests that may be completed depending on the patient’s needs. The three main tests are
Dutch Complete– This is a comprehensive assessment of sex and adrenal hormones and their metabolites. This test measures progesterone, androgen, estrogen metabolites, cortisol, cortisone, cortisol metabolites, creatine, DHEA-S.�
Dutch Plus– This test uses 5 -6 saliva samples as well as 4 urine samples to provide the up and down pattern of cortisol and cortisone throughout the day. This test adds salivary cortisol measurements of the cortisol awakening response (CAR) to the dutch complete to bring another important piece of the HPA axis into focus
Dutch Test Cycle Mapping– This test maps the progesterone and estrogen pattern throughout the menstrual cycle. It provides the full picture of a woman’s cycle to answer important questions for patients with month-long symptoms, infertility, and PCOS. This test is targeted to measure 9 estrogens and progesterone that are taken throughout the cycle to characterize the follicular, ovulatory, and luteal phases.�
How Does This Operate?
Precision Analyical, Inc. has found a way to utilize scientists who have extensive experience and coupled them with the most advanced analytical methods and instruments. This permits them to achieve the best outcomes when it comes to the D.U.T.C.H test.
One of the reasons that many practicing offices have started to utilize D.U.T.C.H evaluations is because they have an extremely simple sample collection. Patients will collect dried urine samples within a span of 24 hours. The urine samples offer results that are excellent because the collections provide the span of a patients entire day of hormones.�
For the D.U.T.C.H test, the patient will collect 4-5 urine samples throughout a 24 hour time period. Upon opening the kit, the patient will be faced with a folder. This folder includes step by step instructions as well as a pocket. Inside the pocket, the patient will find a requisition form, an envelope, and a small clear plastic bag containing the collection paper.�
Each sample will be completed on a separate collection sheet that is labeled with the time. Once the patient opens this bag, they will be able to unfold the first sample paper. The patient will obtain the initial sample at approximately 5pm ( dinnertime). Once the samples are taken, they are to be left open to dry for 24 hours. The second sample is to be taken around 10 pm (bedtime). This third sample depends upon each individual, but in the event, the patient awakens to urinate during the night, a sample is to be gathered. The next sample ought to be collected within 10 minutes of rising. It’s very important that the patient does not lay in bed after waking and they amass this sample within the 10 minute time period that is allotted. Once the patient has collected their morning sample upon rising, they should set an alarm for two hours, since this is when the final sample will be collected. As soon as all the samples have been collected and set out open to dry for 24 hours, the patient can fold them back up and fill out the information on the back of the card ( i.e first name, last name, date of collection, time, and day of cycle for women) and place them inside the clear plastic bag.�
From here, the patient can place the plastic bag full of their samples along with the requestion form in the envelope provided. Next, place 8 stamps in the correct corner, and send it off to the lab!�
For the D.U.T.C.H Plus test, individuals will collect dried urine samples as well as saliva samples. This is best so researchers can utilize information from both collection samples to measure the cortisol and cortisone markers as well. For this test, it is completed in a 24 hour time window with 4 dried urine samples and 5 or 6 (depending on the individual) salvia samples. This test may sound more complicated, but it has a fairly easy schedule that makes it just as simple as the D.U.T.C.H complete. The kit will include labeled urine and salvia collection methods along with easy to read instructions.�
When opening this test, the patient will find an instruction book, a requisition form, 4 collection sheets for the urine (labeled with the time) and 6 labeled tubes for the saliva. For all the urine samples, fill out the backside of the card as prompted (last name, first name, date, and time). Saturate the filter paper or urinate into a clean cup and dip the filter paper for 5 seconds. Once this step is completed, leave the sample open to dry for 24 hours.�
For the saliva samples, take out the appropriate tube for the time it is to be collected. Just as done with the urine, fill out the allotted area requesting last name, first time, sample date and time. The saliva tubes have a blue cap that needs to be removed. After this cap is removed, a long cotton swab will be visible. Take out the cotton swab but leave the small tube in the long tube. The patient will then take the cotton swab and leave it in their mouth until it is fully saturated. Once this is done, place the cotton swab back in the tube as it was found and place the blue cap back on. The small tube should stay intact. There is no need to spit in the tubes.�
The first sample will be salvia and urine. These samples are to be collected immediately upon waking (no brushing of the teeth). The next two samples will be saliva. These are to be taken 30 minutes and 60 minutes after waking. After these are completed, the patient may brush their teeth. The fourth sample will be collected 2-3 hours after waking and is urine only. The fifth and sixth samples will be urine and salvia. The patient will collect these around 4-5 pm (dinnertime) and again anywhere from 10pm-midnight (bedtime). Place all saliva tubes in the freezer until they are ready to be shipped.�
The seventh saliva sample is optional. This will be collected at the time the patient wakes throughout the night if they do so.�
After all the samples have been collected and urine has dried for 24 hours, fold up the urine samples and place them back in the small plastic bag in which they came. Then, take the frozen saliva samples out of the freezer and place them in the plastic bag they arrived in. From here, take the urine samples, the frozen saliva, and the requestion form and place them all back in the kit box. Place the kit box in the return envelope provided and return using the provided carrier.�
The D.U.T.C.H cycle mapping test is the most extensive test provided, with 25 urine samples needed. Due to the fact that this test is for cycle mapping, the collection time frame will be one entire cycle. To start, the patient will need to identify the type of cycle they have ( less than 24 days (normal) long (34 days or more) or no cycle). When the patient opens this kit, they will see an instruction book, 25 urine collection cards, a requestion form, a clear bag, and an envelope.
Day one of the patient’s cycle is the first day of full menstrual flow. The collections for this test will begin on the seventh day and the last four samples will be collected on the fourth day of the patient’s next menstrual cycle. Inside the instruction book, the patient will find an easy to use collection schedule to keep track of their samples.
The ideal time to collect samples throughout this test is upon waking. This will give the lab the most concentrated urine, making the results more conclusive. The patient will collect their sample every morning for day 7 through day 36. Once collected, the patient will leave the urine sample out to dry for 24 hours before putting it in the clear bag provided. It is important for the patient to write the date of the sample on the collection schedule included in the kit.�
The final four samples (22-25) are all to be collected on the same day. Sample 22 should be taken within 10 minutes of waking. Sample 23 is to be taken two hours after waking. Sample 24 should be collected at dinnertime and the patient should not have any fluids two hours before this sample. The final sample should be collected at the patient’s bedtime (approximately 10pm).�
Once the patient has collected all of the samples and let them dry for 24 hours, they are to be placed in the clear plastic bag that was provided in the kit. Next, the patient is to place the clear bag full of samples, the completely filled out collection schedule, and the requisition form in the envelope provided in the kit. Finally, place 8 stamps on the indicated corner and send it off to the lab!�
When sent to the lab as you can see above, these urine samples will be dry. Studies show that dried urine samples will give an accurate representation of the hormone and are stable for weeks. From here, the outcomes are gone over on a team call that includes the patient’s physician and clinicians at Precision Analytical. This helps to ensure that the treatment protocol is created specifically to fit the patients needs.��
Testing is now able to be done by using top of the line integrative techniques. There are numerous reasons and advantages for an individual to complete a hormone evaluation. These tests have the capability to help a patient understand their cycle, testosterone levels, estrogen levels, why they are tired upon waking, throughout there day, and much more.
Hormone imbalances can affect anyone. People tend to associate hormone imbalance with those who are aging, but in reality, it can affect anyone of any gender or age! It might seem like a hassle at first to compelete these tests, but in reality, they are very simple and provide a great deal of information! The symptoms are common and should be discussed with a healthcare practitioner. October is Chiropractor Health Month and our office can help if you are an individual who has these symptoms. Our office implements the D.U.T.C.H test, which allows us a hassle free and easy way to let us help you get back to feeling how you used to. – Kenna Vaughn, Senior Health Coach
The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or chronic disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
All fats, including saturated fatty acids, have very important roles in the body. The most important fats are the ones that the body can�t make and must be coming from the foods that a person eats. �Essential fatty acids are lipids that are involved in various biological processes and produce many compounds when they are metabolized in the body. The two primary EFAs (essential fatty acids) are linoleic acid (Omega-6) and alpha-linolenic acid (Omega-3). These two omegas are essential for the body since they are consumed from dietary sources because the body does not have the ability to synthesize them and EFAs are synthesized into prostaglandins, which are necessary for proper hormone signaling in the body.
Omega-6
Omega-6 fatty acids or linoleic acid are polyunsaturated fatty acids that are primarily used for energy and can be converted into longer omega-6 fats called ARA (arachidonic acid). ARA are used to produce eicosanoids, but they are prone to be more pro-inflammatory. Studies have shown that pro-inflammatory eicosanoids are important chemicals in the immune systems, however, when there are too many to produce, they can increase inflammation and inflammatory diseases in the body.
Researchers state that even though omega-6 fats are essential for a healthy body, the modern Western diet is making individuals consume more omega-6 fatty acids than the recommended amount. In a regular healthy diet, the ratio of omega-6 to omega-3s is 4:1 or less. In a Western diet however, the ratio is between 10:1 and 50:1.
Even though, an individual should consume the recommended amount of omega-6 fatty acids, research has shown that omega-6 fatty acids can lower the risk of cardiovascular diseases and treat symptoms that cause chronic diseases. In certain oils that contains omega-6 fatty acids, GLA (gamma-linolenic acid), which is an anti-inflammatory component and when consumed it converts to DGLA (dihomo-gamma-linolenic acids), which has anti-inflammatory and anti-proliferative properties against cancer.
A study has shown that when an individual takes a high dose of GLA in their diet, it can significantly reduce a number of symptoms caused by rheumatoid arthritis, and another study found that taking GLA supplements with a breast cancer drug is more effective in lowering breast cancer.
Omega-3
Just like omega-6 fatty acids, omega-3 fatty acids are polyunsaturated fats that play important roles in providing a number of health benefits for a functional body. Omega-3 fatty acids contain three important compounds that are found in foods, they are ALA (alpha-linolenic acid); which converts into energy for the body, DHA (docosahexaenoic acid); which is the key component for a functional brain and retina, and lastly, EPA (eicosapentaenoic acid); which has cardiovascular benefits including lowering serum triglyceride and non-HDL-C (non-high-density lipoprotein cholesterol) in the body.
When it comes to those three important components in omega-3s, ALA is mainly found in plants, while DHA and EPA are found in mostly animal products and algae. What makes these three components work well in the omega-3 supplements is that they are a crucial part of the human cell membrane and improve heart health, support mental health, decrease liver fats and fight inflammation.
With omega-3 fatty acids, lots of people don�t consume it as much as omega-6, due to not eating a lot of fatty fish as often and consuming omega-6 through fried food being cooked in refined vegetable oils. To balance a healthy diet, individuals can take an omega-3 supplement to balance out the omega-6 consumption to make sure the body is receiving these fatty health benefits.
Prostaglandins
Prostaglandins are a component of this regulatory system, they affect multiple hormone synthesis and secretion pathways in the hypothalamus-pituitary axis. They are a group of endogenously occurring acidic lipids that appear to play a role in the reproductive physiology.
Since prostaglandins are bioactive lipids, they exert an autocrine or paracrine function by binding to specific GPCRs (G-protein-coupled receptors) to activate intracellular signaling and gene transcription. As key regulators of reproductive processes, prostaglandins has many functions like having a role in the hypothalamic and pituitary control of gonadotropin secretion, ovulation, in luteinization and in the corpus luteum regression.
Prostaglandins also play a key role in the inflammatory response in the body. Their biosynthesis is significantly increased in inflamed tissues and can contribute to the development of the cardinal signs of acute inflammation in the body.
Researchers stated that prostaglandins have a plethora of actions in the central nervous system that can affect the progress of inflammation in the body differently, however, further studies are being tested to inhibit the role of these lipid mediators.
Conclusion
All fats play a very important role in the body. Essential fatty acids produce many compounds in the body when they are being metabolized in the body. Since the body can not produce essential fatty acids, they have to be consumed through food. The two important essential fatty acids are omega-6 and omega-3. These two fatty supplements help the body gain the nutrients the body needs to synthesize. Prostaglandins are also a key role in the body since they affect the pathways in the hypothalamus-pituitary axis and plays the role of regulating the reproductive physiology. Some products are formulated to target the immune support by creating micronized structure to increase the surface-to-volume ratio of particles to be more available to enzymatic actions.
October is Chiropractic Health Month. To learn more about it, check out Governor Abbott�s proclamation on our website to get full details on this declaration.
The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or chronic disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
References:
Bardin, T P. �The Role of Prostaglandins in Reproductive Physiology.� The Ohio State Medical Journal, U.S. National Library of Medicine, Oct. 1970, www.ncbi.nlm.nih.gov/pubmed/4918753.
Behrman, H R. �Prostaglandins in Hypothalamo-Pituitary and Ovarian Function.� Annual Review of Physiology, U.S. National Library of Medicine, 1979, www.ncbi.nlm.nih.gov/pubmed/373605.
Brinton, Eliot A, and R Preston Mason. �Prescription Omega-3 Fatty Acid Products Containing Highly Purified Eicosapentaenoic Acid (EPA).� Lipids in Health and Disease, BioMed Central, 31 Jan. 2017, www.ncbi.nlm.nih.gov/pubmed/28137294.
Calder, Philip C. �n-3 Polyunsaturated Fatty Acids, Inflammation, and Inflammatory Diseases.� The American Journal of Clinical Nutrition, U.S. National Library of Medicine, June 2006, www.ncbi.nlm.nih.gov/pubmed/16841861.
Di Pasquale, Mauro G. �The Essentials of Essential Fatty Acids.� Journal of Dietary Supplements, U.S. National Library of Medicine, 2009, www.ncbi.nlm.nih.gov/pubmed/22435414.
Dinan, Timothy, et al. �Investigating the Inflammatory Phenotype of Major Depression: Focus on Cytokines and Polyunsaturated Fatty Acids.� Journal of Psychiatric Research, U.S. National Library of Medicine, Jan. 2009, www.ncbi.nlm.nih.gov/pubmed/18640689.
Gibson, Robert A, et al. �Conversion of Linoleic Acid and Alpha-Linolenic Acid to Long-Chain Polyunsaturated Fatty Acids (LCPUFAs), with a Focus on Pregnancy, Lactation and the First 2 Years of Life.� Maternal & Child Nutrition, U.S. National Library of Medicine, Apr. 2011, www.ncbi.nlm.nih.gov/pubmed/21366864.
Guesnet, Philippe, and Jean-Marc Alessandri. �Docosahexaenoic Acid (DHA) and the Developing Central Nervous System (CNS) – Implications for Dietary Recommendations.� Biochimie, U.S. National Library of Medicine, Jan. 2011, www.ncbi.nlm.nih.gov/pubmed/20478353.
Gunnars, Kris. �What Are Omega-3 Fatty Acids? Explained in Simple Terms.� Healthline, 23 May 2019, www.healthline.com/nutrition/what-are-omega-3-fatty-acids.
Innes, Jacqueline K, and Philip C Calder. �Omega-6 Fatty Acids and Inflammation.� Prostaglandins, Leukotrienes, and Essential Fatty Acids, U.S. National Library of Medicine, May 2018, www.ncbi.nlm.nih.gov/pubmed/29610056.
Jabbour, H N, and K J Sales. �Prostaglandin Receptor Signalling and Function in Human Endometrial Pathology.� Trends in Endocrinology and Metabolism: TEM, U.S. National Library of Medicine, Oct. 2004, www.ncbi.nlm.nih.gov/pubmed/15380812.
Kapoor, Rakesh, and Yung-Sheng Huang. �Gamma Linolenic Acid: an Antiinflammatory Omega-6 Fatty Acid.� Current Pharmaceutical Biotechnology, U.S. National Library of Medicine, Dec. 2006, www.ncbi.nlm.nih.gov/pubmed/17168669.
Kenny, F S, et al. �Gamma Linolenic Acid with Tamoxifen as Primary Therapy in Breast Cancer.� International Journal of Cancer, U.S. National Library of Medicine, 1 Mar. 2000, www.ncbi.nlm.nih.gov/pubmed/10699943.
Khanapure, Subhash P, et al. �Eicosanoids in Inflammation: Biosynthesis, Pharmacology, and Therapeutic Frontiers.� Current Topics in Medicinal Chemistry, U.S. National Library of Medicine, 2007, www.ncbi.nlm.nih.gov/pubmed/17305573.
Kim, Kyu-Bong, et al. �?-Linolenic Acid: Nutraceutical, Pharmacological and Toxicological Evaluation.� Food and Chemical Toxicology : an International Journal Published for the British Industrial Biological Research Association, U.S. National Library of Medicine, Aug. 2014, www.ncbi.nlm.nih.gov/pubmed/24859185.
M.Shewchuk, Brian. �Prostaglandins and n-3 Polyunsaturated Fatty Acids in the Regulation of the Hypothalamic�Pituitary Axis.� Prostaglandins, Leukotrienes and Essential Fatty Acids, Churchill Livingstone, 28 Sept. 2014, www.sciencedirect.com/science/article/abs/pii/S0952327814001495.
Parker, Helen M, et al. �Omega-3 Supplementation and Non-Alcoholic Fatty Liver Disease: a Systematic Review and Meta-Analysis.� Journal of Hepatology, Centre for Reviews and Dissemination (UK), Apr. 2012, www.ncbi.nlm.nih.gov/pubmed/22023985.
Petersen, Martin, et al. �Effect of Fish Oil versus Corn Oil Supplementation on LDL and HDL Subclasses in Type 2 Diabetic Patients.� Diabetes Care, U.S. National Library of Medicine, Oct. 2002, www.ncbi.nlm.nih.gov/pubmed/12351465.
Ph.D., Catharine Paddock. �Could Omega-6 Fatty Acids Help Us Live Longer?� Medical News Today, MediLexicon International, 20 Mar. 2018, www.medicalnewstoday.com/articles/321266.php.
Simopoulos, Artemis P. �The Importance of the Omega-6/Omega-3 Fatty Acid Ratio in Cardiovascular Disease and Other Chronic Diseases.� Experimental Biology and Medicine (Maywood, N.J.), U.S. National Library of Medicine, June 2008, www.ncbi.nlm.nih.gov/pubmed/18408140.
Wang, Xiaoping, et al. �Multiple Roles of Dihomo-?-Linolenic Acid against Proliferation Diseases.� Lipids in Health and Disease, BioMed Central, 14 Feb. 2012, www.ncbi.nlm.nih.gov/pmc/articles/PMC3295719/.
Weylandt, Karsten H, et al. �Omega-3 Polyunsaturated Fatty Acids: The Way Forward in Times of Mixed Evidence.� BioMed Research International, Hindawi Publishing Corporation, 2015, www.ncbi.nlm.nih.gov/pmc/articles/PMC4537707/.
Zurier, R B, et al. �Gamma-Linolenic Acid Treatment of Rheumatoid Arthritis. A Randomized, Placebo-Controlled Trial.� Arthritis and Rheumatism, U.S. National Library of Medicine, Nov. 1996, www.ncbi.nlm.nih.gov/pubmed/8912502.
Inflammatory reactions in the central nervous system (CNS) are currently known to be associated with many neurological disorders. In neurodegenerative diseases, such as Alzheimer’s disease (AD) and Parkinson’s disease (PD), there is considerable penetration of different leukocyte subsets into the CNS or there is severe activation of microglial cells which increases many inflammatory mediators in the CNS. In acute CNS disorders, including delayed corrosion associated with vasospasm after subarachnoid hemorrhage (SAH), ischemic stroke, spontaneous intracerebral hemorrhage (ICH), and traumatic brain injury (TBI), current evidence from a variety of research studies reveal that inflammation may be a possible target for treatment. Inflammation is becoming a promising region of research study for new treatments. �
To speed up the process of translating this information to clinical applications, a number of significant problems have to be addressed as their capacity to continuously identify characteristic cerebral deficits in people with neurodegenerative diseases, the connections of brain injuries to clinical symptoms and genetic diagnosis as well as the level to which the harm respond to various treatment approaches. In this article, findings that address some of these problems are reported by several researchers. �
Inflammation and Neurological Disorders
In neurodegenerative diseases, a research study reviewed the function of chronic neuroinflammation in the pathogenesis of Alzheimer’s disease (AD). With the glial fibrillary acidic protein-interleukin 6 (GFAP-IL6) transgenic mice model, the researchers demonstrated that this animal model, in which chronic neuroinflammation triggered the expression of the cytokine interleukin-6 (IL-6) in astrocytes, could serve as a great tool for drug and/or medicine discovery and validation in vivo. �
Another research study assessed the role of inflammation in the neuropathology of Parkinson’s disease (PD). They supplied a synopsis of current knowledge on the temporal profile of immune reactions in PD and discussed the potential effects of central and peripheral inflammation. The research study utilized TRODAT-1 SPECT to rate leukocyte apoptosis from PD patients and its association with central dopamine neuron loss. The leukocyte apoptosis and striatal dopamine transporter uptake ratios were associated with the duration of the disease and increased severity. The interaction between brain and systemic inflammation may be liable for the neurodegenerative disease progression. Another research study utilized the Longitudinal Health Insurance Database 2000 (LHID2000) to analyze and evaluate the probability of dementia between patients clinically diagnosed with autoimmune rheumatic diseases (ARD) and non-ARD patients during a 5-year follow-up interval. Their findings indicate that patients with and without ARD had comparable risks of developing dementia. �
In severe critical CNS diseases, the research study utilized traumatic brain injury (TBI) models to determine whether simvastatin, together with an antioxidant, could cause cerebral vascular endothelial inflammatory responses after traumatic brain injury in rat models. Their findings support that simvastatin combined with an antioxidant could offer neuroprotection and it could possibly be attributed to cerebral vascular inflammatory reactions. The analysis utilized a structural equation modeling to evaluate the predictive value of admission Glasgow Coma Scale (GCS) scores, duration of unconsciousness, neurosurgical intervention, and countercoup lesion associated with the impairment of memory and processing rate functions six months after a TBI. The analysis also revealed that admission GCS score is a tremendous predictor of memory/processing speed dysfunctions after TBI. �
One research study investigated serum thiobarbituric acid-reactive substances (TBARS) and free thiol levels in a variety of subtypes of acute ischemic stroke (AIS) where they evaluated their association with clinical results. They discovered that patients with the disease have greater oxidative stress but reduced antioxidant defense compared to those with disease following AIS. Serum TBARS level at the acute phase of a stroke is a predictor for the outcome. Along with other research studies, these aimed to ascertain whether serum adhesion molecules are associated with septic encephalopathy (SE). Their findings reveal that SE suggests higher mortality in nontraumatic patients with sepsis. Serum vascular cell adhesion molecule-1 (VCAM-1) degree on presentation is a much more effective predictor of SE in these patients than lactate concentration and other adhesion molecules on admission, according to research studies. �
From the CNS health issues, research studies investigated the relationship between protein expressions of two autophagy markers, LC3B and Beclin-1, with clinical trials in astrocytoma patients. Their results suggest that targeting the cancer stem-like cell in astrocytoma can offer an approach that astrocytoma cancer stem-like cells together with improved autophagy may lead to resistance. Along with another research study, researchers researched DAPK protein expression and promoter hypermethylation in central neurocytoma and oligodendroglioma. Their results demonstrated that repressed expression and DAPK promoter hypermethylation of DAPK protein were prevalent in central neurocytoma than in oligodendroglioma. DAPK promoter hypermethylation can be useful for differential diagnosis between these two types of tumors. �
In conclusion, the article above emphasizes several essential research strategies that are making it more evident that neuroinflammation or inflammatory reactions are of translational significance for different types of neurological disorders. The results from these research studies not only enable us to understand the pathogenesis of these disorders but these also show great potential to provide desperately objective biomarkers for analysis and clinical investigation. Knowledge and comprehension of those conditions have contributed to the development of effective treatments, animal models, and innovative tools to characterize these medical conditions and provide better treatment options to patients. �
Neuroinflammation is ultimately characterized as the inflammation of the nervous tissue. It can commonly occur due to a variety of factors, including toxins, infections, autoimmune diseases, and even traumatic brain injury (TBI). In the central nervous system (CNS), the microglial cells are in charge of activating inflammatory reactions associated with these factors. However, excess microglia activation can ultimately cause a variety of health issues, including neurological diseases, among others. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
Metabolic Assessment Form
The following Metabolic Assessment Form can be filled out and presented to Dr. Alex Jimenez. Symptom groups listed on this form are not intended to be utilized as a diagnosis of any type of disease, condition, or any other type of health issue. �
In honor of Governor Abbott’s proclamation, October is Chiropractic Health Month. Learn more about the proposal. �
Inflammatory reactions in the central nervous system (CNS) are currently known to be associated with many neurodegenerative diseases, such as Alzheimer’s disease (AD) and Parkinson’s disease (PD). The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or chronic disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Neural Zoomer Plus for Neurological Disease
� �
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention. �
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine