Taking an active role in personal spinal healthcould mean the difference between having to deal/manage back pain for the rest of your life and not having to. Most of us have experienced some form of back pain, whether lifting an object, bending, reaching, twisting, etc. Fortunately, it is usually not serious and we move on with our lives. However, not paying attention to those not so serious backaches can lead to chronic backaches that can lead to serious chronic back pain.
Chronic backache/s can be annoying, frustrating, and debilitating, especially when the cause is not obvious, cannot be found, or figured out. When back pain occurs from trauma or an automobile accident it’s a lot easier to diagnose.
But when it is the result of a gradual build-up of activities like sitting all day at a desk, in a truck or lifting objects, loading, unloading, pushing, pulling, stocking for several years, it could be a lot more serious than the individual might think. This is because although they are barely beginning to feel the ache or pain, the damage has been ongoing/worsening and has finally reared its ugly head.
Contents
Finding the Right Help
Getting on the right track means searching for a spinal professional that can identify and treat the source of the back pain, help with posture, diet advice, and help reach optimal health. Finding the source of the pain can be a challenge, but it is not impossible. The key is finding a knowledgeable, experienced back pain specialist and taking an active role in your spine’s health.
Chiropractors, doctors, and physicians begin with at least 4-6 weeks of non-invasive treatment. These start with tests, scans, x-rays, then move on to treatment, which can consist of ice/heat, physical therapy, adjustments, re-alignment combined with exercises, stretches. Prescription medication/s or surgery is the last option for fear of worsening conditions along with medication abuse. This approach has seen an increase in relief and favorable outcomes.
Patient Active Role
Many individuals have gone down the path of being over-medicated and are exhausted with the whole experience of being constipated, constant brain fog, etc. Those same individuals are taking that active role and getting involved by dealing with their back pain in a natural non-invasive way. Preparing before meeting with a spine professional is important to give as much information as possible.
Tips
Preparation
Write down notes about what is being felt in and around the body, not just the back. This is because of the psychological aspect of pain, which can manifest in a variety of ways.
Try To Go Back To When The Pain Started
Think about when the pain first began
Sitting at work/home one day when there was what you thought was a little shift or tingle
Sports activity
Exercising
Popping, clicking, grinding sensations and sounds
Warming, electrical, shooting sensation/s pain
Tingling/numbness in the leg, foot, toes
Try to describe all the details with the doctor/chiropractor even what you might consider trivial
Emotions/Stress Triggers need to be taken into account
Work
Bills
Marriage
Divorce
Children
Major life changes and stress affects the whole body, especially the spine
Family Friend Perspective and Support
Bringing along a close family member or friend that knows your activity habits could help the doctor get a better idea of what is causing the pain. Family or friends can remember a trip, fall, dance moment that didn’t go so well, work accident, etc.
Medical History
Prior medical injuries and conditions will help provide additional information as to whether there is a pattern when back pain strikes. This can be extremely important even if it does not seem to be related to the pain symptoms. Tell the doctor about any physical therapy or other holistic/conservative treatments performed before and after the pain began. Also, inform them of any medications, supplements, vitamins, herbs, over-the-counter medications that were taken prior to the pain and currently being taken. If there has been unexplained weight loss, fever, urination/bowel changes, should also be discussed.
Physical Tests
Unless the patient is in too much pain, the meeting with the chiropractic physician will be active, meaning the doctor may have the patient perform a series of movements like:
Sitting
Standing
Walking
Bending forward, backward, and to the side
Lifting the legs straight up while standing and lying down
Inform the doctor of any numbness or tingling pain while performing these musculoskeletal exercises/tests.
With a patient that can’t perform the exercises, the doctor will examine the patient while lying down, by carefully and slowly palpating the painful area/s, moving the leg/s, and raising the patient up, all the while taking notes of what position/s cause discomfort and pain.
Options
Depending on the physician’s assessment, initial treatment will take time, require the individual to take an active role, and possibly recommend the individual try different treatment options. Ask the doctor all the questions you have during the visit like:
Could there be more than one cause for my back pain?
Do the treatments hurt?
The treatment will keep me pain-free or just tolerable?
Are there self-therapies to assist healing and recovery?
If seeing a general physician you could ask for a recommended spine specialist
The ultimate goal is for the individual to live a happy, fulfilling life that is pain-free. The doctor will do everything they can to bring an optimum level of care. If the quality of life still does not improve or when various attempts for pain relief have proven unsuccessful, then a doctor could recommend stronger medications and surgical options. Don’t wait to get professional medical help! The longer an individual waits the worse the cause of the back pain gets. Get involved and take an active role in your spinal health.
Personal Injury Chiropractic Care
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
Analgesics are pain-relieving medications, also known as painkillers. These can be over-the-counter and prescription medications. Either could be part of a treatment plan for spine-related pain. Individuals dealing with back or neck conditions, typically take analgesics to reduce symptoms.
Analgesics are available over-the-counter/OTC and with a prescription
Prescription analgesics usually include the more powerful form of over-the-counter medications
Analgesics can be specialized with some to relieve pain, with others reducing inflammation/pain
Contents
Over-the-counter
Acetaminophen, Non-steroidal anti-inflammatory drugs, and topical analgesics are the most commonly used medications for various pain symptoms. Over-the-counter analgesics are most effective when taken at the first sign/presentation of acute pain. Whiplash, along with muscle sprains and strains are common injuries known to cause short term pain that can be mild to severe. Follow the medication’s instructions on dosage recommendations and precautions.
If the medication does not work or helps manage the pain, and/or pain symptoms worsen, contact your healthcare provider. This could be an indicator that a more powerful prescription analgesic is needed to help manage the pain, along with added therapy like physical therapy, and chiropractic to help avoid dependence on the prescription meds.
Acetaminophen
Tylenol is one form of medication taken for different types of pain and is one of the most popular over-the-counter analgesics. Acetaminophen’s purpose is exclusively to relieve pain. It does not reduce inflammation.
Non-steroidal anti-inflammatory drugs – NSAIDs
Non-steroidal anti-inflammatory drugs work to reduce inflammation and pain. Types of over-the-counter These include:
Aspirin
Ibuprofen
Naproxen
Topical analgesics
Topical analgesics like capsaicin cream and salicylates are an alternative to analgesics taken by mouth. These creams, balms, gels, and sprays are applied to the painful area. It is a very common application and is widely used for joint, muscle, and back pain. Salicylates are plant-based chemicals that operate to decrease the body’s production of prostaglandins. These are lipids that let the body know that there is a problem causing inflammation and pain.
Prescription
A doctor could prescribe an analgesic as part of a treatment plan to help manage short-term and chronic pain. It is extremely important to precisely follow the doctor’s instructions on how much and when to take the medication. Remember that any of these medications have the potential for side effects, which includes the risk of negative interactions when taken with other meds. Be sure to talk with a doctor about potential risks, and keep them informed about all medications like blood pressure and diabetes meds and natural herbs/vitamins/supplements taken for other medical conditions.
COX-2 Inhibitors
Cyclo-oxygenase-2 or COX-2 inhibitors are a prescription NSAID medication type that is formulated to target specific enzymes that trigger inflammation. Inflammation is not just a symptom but can also be a cause of pain related to many different spinal disorders. COX-2 inhibitors have a lower risk of causing/contributing to gastrointestinal problems.
There are other potential side effects and risks associated with COX-2 inhibitors. Potential side effects include an increased risk of cardiovascular problems, like a heart attack or blood clots. COX-2 inhibitors reduce the risk of stomach problems than classic NSAIDs but if gastrointestinal conditions exist to talk with a doctor before taking these medications.
Opioids
These are highly potent analgesics and are no longer the first type of pain-relieving medication that a doctor prescribes. They are now to be the last resort for reducing moderate to severe pain symptoms. These medications work by decreasing the perception and reaction to the pain. Opioids are prescribed for short-term use following surgical procedures and trauma. However, there are different situations where use is appropriate. When opioids are recommended, the doctor will begin with the lowest strength/dosage to manage the pain. Types of opioids include:
Analgesic medications are commonly used for various types of pain-causing conditions. When they are used properly with a doctor�s supervision they are safe and effective at managing pain and discomfort. If new symptoms present and/or the pain worsens or becomes different contact your doctor on appropriate instructions.
Chiropractic Neck Pain Treatment
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
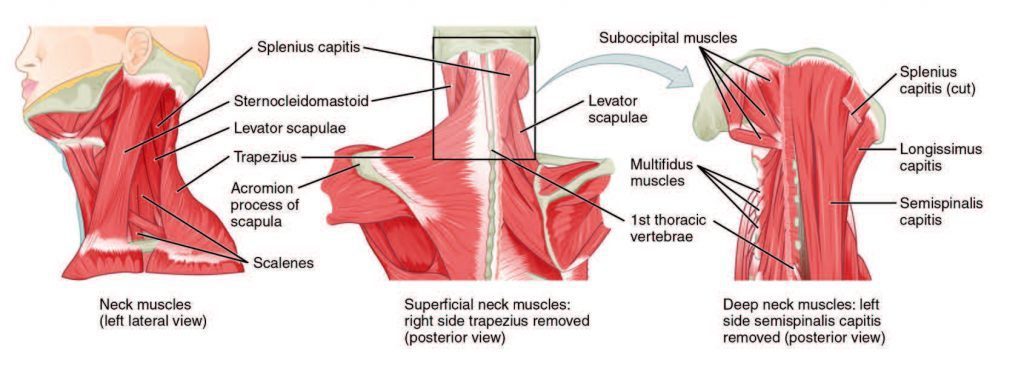
The spinal muscles and ligaments work in conjunction to help support the spine, maintain an upright posture, and control movements during activity and rest. The muscles are named based on shape, location, or a combination. Further categorization factors include muscle functions like flexion, extension, or rotation. Skeletal muscle is a form of striated muscle tissue that is voluntarily controlled by the somatic nervous system. Striated means it is striped in appearance. Most skeletal muscles are attached to bones by collagen fibers known as tendons.
Vertebral Muscle Types
Location
Forward flexors
Anterior
Lateral flexors
Lateral
Rotators
Lateral
Extensors
Posterior
It has the fastest contraction rate of all muscles. Before muscle/s contract, a nerve impulse starts in the brain and runs through the spinal cord to the muscle. For the muscles to contract and work properly they need energy/fuel. Mitochondria produce Adenosine triphosphate chemical cells that are needed for energy. Adenosine triphosphate is made as the mitochondria burn glucose or sugar. The blood vessels deliver the oxygen and nutrients that the mitochondria need to maintain a steady supply of adenosine triphosphate.
Contents
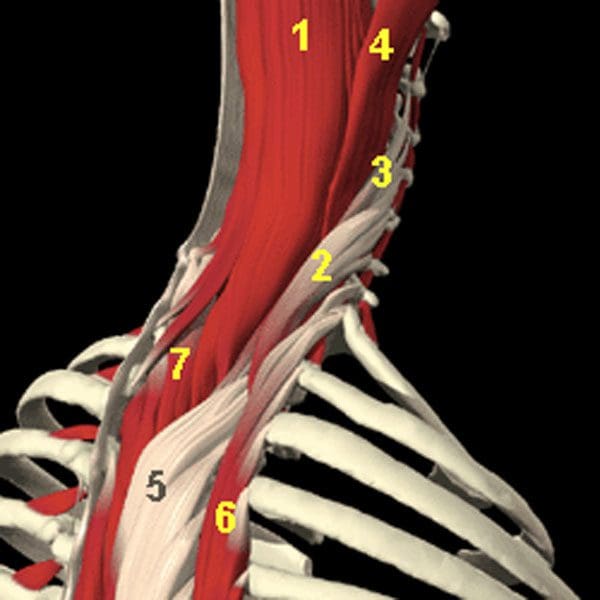
The Posterior Cervical and Upper Thoracic Spinal Muscles
Semispinalis Capitus – controls the head rotation and backward pulls
Iliocostalis Cervicis – extends the cervical vertebrae
The Longissimus Cervicus – extends the cervical vertebrae
Longissimus Capitus – controls the head’s rotation and backward pulls
Longissimus Thoracis – controls the extension/lateral flexion of the vertebral column and rib rotation
Iliocostalis Thoracis – controls the extension/lateral flexion of the vertebral column and rib rotation
Semispinalis Thoracis – extends and rotates the vertebral column
Muscles of the Spinal Column
Cervical muscles
Cervical Muscles
Function
Nerve
Sternocleidomastoid
Extends and rotates the head and flexes the vertebral column
C2, C3
Scalenus
Flexes and rotates the neck
Lower cervical
Spinalis Cervicis
Extends and rotates the head
Middle/lower cervical
Spinalis Capitus
Extends and rotates the head
Middle/lower cervical
Semispinalis Cervicis
Extends and rotates the vertebral column
Middle/lower cervical
Semispinalis Capitus
Rotates the head and pulls backward
C1-C5
Splenius Cervicis
Extends the vertebral column
Middle/lower cervical
Longus Colli Cervicis
Flexes the cervical vertebrae
C2-C7
Longus Capitus
Flexes the head
C1-C3
Rectus Capitus Anterior
Flexes the head
C2, C3
Rectus Capitus Lateralis
Bends the head laterally
C2, C3
Iliocostalis Cervicis
Extends the cervical vertebrae
Middle/lower cervical
Longissimus Cervicis
Extends the cervical vertebrae
Middle/lower cervical
Longissimus Capitus
Rotates the head and pulls backward
Middle/lower cervical
Rectus Capitus Posterior Major
Extends and rotates the head
Suboccipital
Rectus Capitus Posterior Minor
Extends the head
Suboccipital
Obliquus Capitus Inferior
Rotates the atlas
Suboccipital
Obliquus Capitus Superior
Extends and bends the head laterally
Suboccipital
Thoracic Muscles
Thoracic muscles
Function
Nerve
Longissimus Thoracis
Extension, lateral flexion of the vertebral column, and rib rotation
Perimysium is the sheath that groups the muscle fibers into bundles.
Endomysium is another type of connective tissue that sheaths each muscle fiber.
The cause of back pain and spinal muscle spasm/s can be caused by overuse, automobile accident, personal, work, or sports injury. The root cause of muscle spasm/s is usually a consequence of an injury to a structure within the lumbar spine. If there have been one or more episodes of muscle spasm in the low back, chances are it will re-occur. The muscles in the low back work together with the abdominal muscles. The spinal muscles add stability by maintaining an erect spine and maintain balance.
Back Pain Specialist
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
Finding the right surgeon that specializes in an individual’s specific spinal conditions and physical health means doing some research. There are several types of procedures for spinal problems. The type of surgery depends on the condition and an individual’s medical history. If surgery is recommended for a lumbar herniated disc or LHD combined with sciatica here are a few things to think about.
Devotes at least 50% of their practice to spinal conditions
Specializes in treating herniated disc/s and sciatica. This means they will have added/specialized knowledge and expertise.
It is extremely important that an individual feels comfortable and feels they are able to communicate freely with the surgeon. A professionally qualified surgeon should:
Spend adequate time with the individual
Answer all questions
Provide all information needed about the condition and treatment
Listen to what the individual has to say
Is open-minded
Is not hard to get in contact with
Has experience in the latest methods and techniques
What to look at and think about
Individuals can feel uncomfortable asking questions, but thorough communication is key. Remember, it is your body, and it is your right to know the details of the spinal disorder, along with non-surgical and surgical approaches to treatment that are available. There is time to consider the options and make an informed decision about the treatment plan as most spinal procedures are elective. Ask the surgeon all the questions you have to help decide wisely and with confidence. Make sure they address all concerns, and any others not listed.
The surgeon’s specialization/focus
Orthopedic surgeons and neurosurgeons perform spinal procedures. Each will have a specific interest and expertise in certain spinal condition/s. For example, some surgeons may specialize in treating adult or pediatric patients, and some may only treat either lumbar/low back or cervical/neck conditions. Within those groups, some focus on:
Spinal deformities
Tumors
Myelopathy a spinal cord disease
Specific spinal cord diseases
Minimal invasive surgery option
Minimally invasive spine involves tiny incisions, that reduces the recovery time needed to heal. With this type, individuals can be up and walking within hours after surgery. Unfortunately, not all conditions can take this approach.
Is the surgery absolutely necessary, or can it be treated non-surgically?
Sciatica and herniated discs can be quite painful and cause disability. Never rush into surgery just to relieve symptoms. As surgery can cause other types of pain symptoms and issues. Herniation and sciatica can be resolved with:
Chiropractic
Physical therapy
Medications
Injections
Lifestyle changes
Diet adjustments
Regular exercise
Weight loss
However, if there are neurologic symptoms, like weakness in the leg, foot, numbness, or loss of bladder or bowel control – this is considered a medical emergency – then surgery is absolutely needed.
The number of similar procedures performed
The surgeon�s experience is very important. The more experienced, the better. Ask if they can refer to other patients who have had similar procedures.
Recovery time
Every patient is unique, as is the type of surgery, and recovery times. They all vary accordingly. General health, physical condition, and the severity of the disorder play a role in how long and how involved recovery time will be. Experienced surgeons can provide more specific answers concerning recovery/healing time.
Complication rate
All surgeries carry some risk of complication. Complication rates that are more than 10% is a red flag. Possible post-surgery complications.
Infection rate
Surgeons should have an infection rate lower than 10%. However higher rates do not always mean that surgeon is at fault as higher rates can come from performing highly complex procedures. Another reason for high infection rates could be the patients themselves like smokers or individuals with diabetes have increased risks for infection. However, do not feel uncomfortable asking the surgeon to explain a high infection rate.
Decide to not opt for spine surgery
As a surgeon produces a diagnosis, they should present a recommended treatment plan, including alternative treatments/therapies. Ask for another explanation of any part of the evaluation, diagnosis, or available treatment options.
Get a second opinion
A second opinion should be encouraged. A second opinion can reinforce the surgeon�s recommendations and offers a new perspective. The surgeon should be comfortable with a second opinion. This does not mean that the individual does not trust the surgeon. It does mean that there is considerable interest in achieving optimal health and making sure that surgery is the absolute right thing to do. Pass on surgeons that discourage or disapprove of second opinions and continue looking.
Whiplash Chiropractic Massage Therapy
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
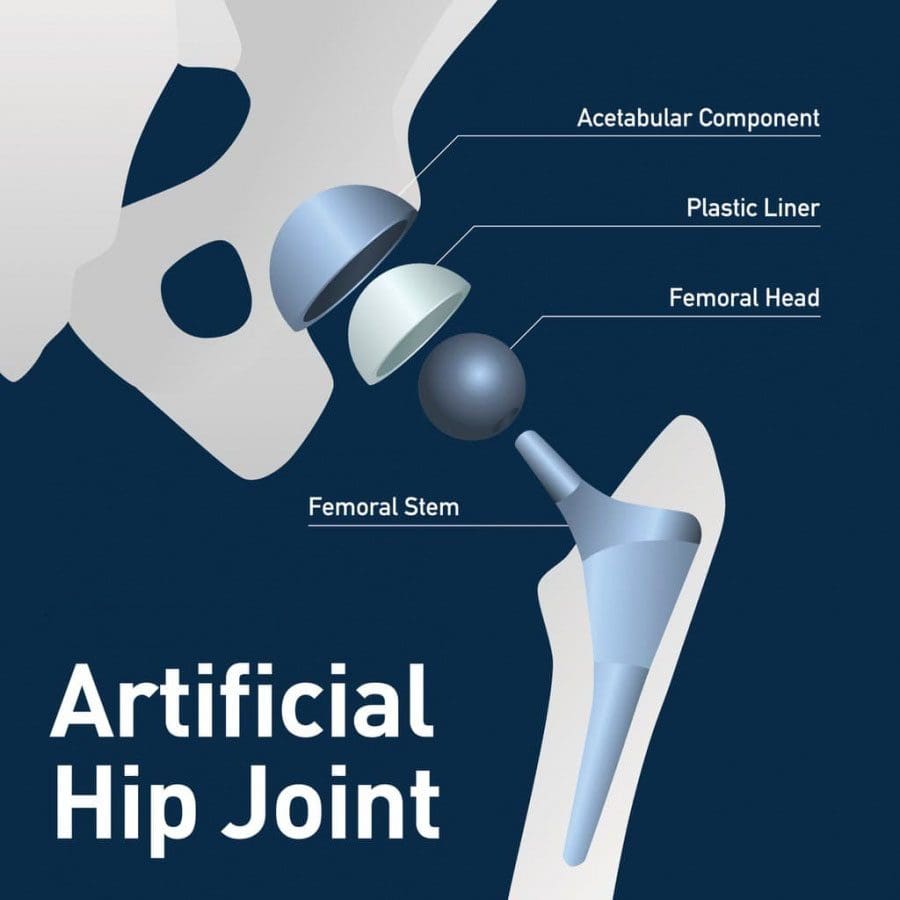
Back discomfort and pain could be caused by hip issues and could be resolved with hip replacement. According to a recent study, a total hip replacement solved back pain in four out of five individuals dealing with spinal discomfort and pain. When the hip/s are stiff or cannot move normally, this places added pressure on the spine. Studies show that low back pain was resolved in 82% of individuals after a total hip replacement known as total hip arthroplasty or THA. The body is designed as a fluid chain with fluid motion connecting the neck all the way down to the toes.
When a region like the hip tightens/stiffens, it generates added stress/pressure on the other areas of the body, which in this case happens to be the lower spine. Individuals with mild arthritis of the spine are able to experience increased pain reduction than individuals with severe arthritis. An insight into the relationship between the hips and low back that can lead to accurate diagnoses and optimal treatment plans.
Contents
Hip Issues
The hip/s move with the lower back during activities like walking, sitting, bending, etc. Tight muscles, normal wear-and-tear, and osteoarthritis can reduce hip movement, forcing the lower back to make awkward and poor posture causing adjustments. Individuals usually relieve the painful position by increasing the curve of their lower back.
If an individual has severe arthritis of the hip, they put a lot of stress and pressure on the low back that often results in low back pain. Advanced hip osteoarthritis is the breakdown of joint cartilage and the most common type of arthritis. Individuals with this type experience low back pain 50% of the time, and even higher depending on the individual’s condition. 80% to 90% of individuals with hip or knee arthritis, unfortunately, develop low back arthritis.
There is not yet a clear reason as to why this occurs. It is theorized that some osteoarthritis risk factors like obesity and high-impact/force activities can be modified with lifestyle adjustments. Other risk factors that include injury, trauma, age, and congenital conditions like hip dysplasia, cannot be avoided. Hip osteoarthritis isn�t the only hip issue that can also cause lower back pain. Other hip issues.
Sacroiliac joint dysfunction
The sacroiliac joint connects the sacrum to the pelvis. It is a shock absorber between the upper body, the pelvis and can stiffen with time. Sacroiliac joint pain affects around 15% to 25% of individuals with low back pain. It worsens when climbing stairs, getting up from a seated position or running. Symptoms include:
Low back pain
Pain in buttock/s
Groin pain
Stiffness
Instability
Piriformis syndrome
About 200,000 individuals each year are affected with piriformis syndrome and is often misdiagnosed as symptoms resemble sciatica. What happens is the piriformis muscle, which connects the sacrum to the top of the femur, tightens/irritates the sciatic nerve. Symptoms are often mistaken for sciatica with pain in the buttocks, numbness, and tingling that travels down the back of the leg and into the feet.
Diagnosis
A doctor or chiropractor will use a combination of diagnostic tools. This typically includes a physical exam, X-rays with other specific tests to help identify the source of pain. What typically happens is a patient will undergo a hip and lumbar spine X-ray, but the thoracic spine, pelvis, and hip areas are missed. Getting the middle segment is critical to see how the spine and hips are working together. It is critical to understand the hip-spine connection. All spine patients should have X-rays of the hips to make sure any problems don’t go undetected. The overlap of symptoms with these two areas could be overlooked.
If necessary a diagnostic injection into the hip joint can help precisely locate the pain source. This can be done at the clinic or doctor’s office using ultrasound or X-ray to guide the needle. If no pain relief results from the injection, hip replacement is still not considered because the pain could be coming from the spine. A critical part of the diagnosis is not just imaging. One of the most important parts is getting a thorough history of symptoms. X-rays and MRI show what the problem could be, however, the symptoms could coming from another area.
Treatment Options
Before total hip replacement is considered there are nonsurgical approaches to be considered. All diagnoses should start with conservative treatment. Physical therapy, chiropractic, gait training, and core strengthening can optimize the spine to better manage hip issues and arthritis. Conservative therapies could also include:
Weight loss
Activity modification like walking instead of running
Anti-inflammatory medication
Cortisone injections
Total hip replacement is the last option for individuals experiencing pain, difficulty walking, and limited mobility. The procedure removes the damaged cartilage and bone from the hip joint. This includes the head of the thighbone along with the socket where it fits and replaces it with artificial parts.
Conclusion
Get a second opinion. Individuals are encouraged to educate themselves as much as possible on the condition. The hip and spine is a complex relationship. The most important information for patients is that they understand along with their doctor where the pain is coming from, the hip, spine, or both.
Reduce Plantar Fasciitis Foot Pain
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
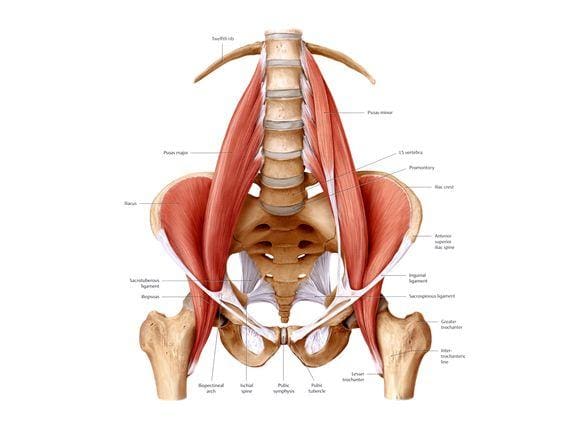
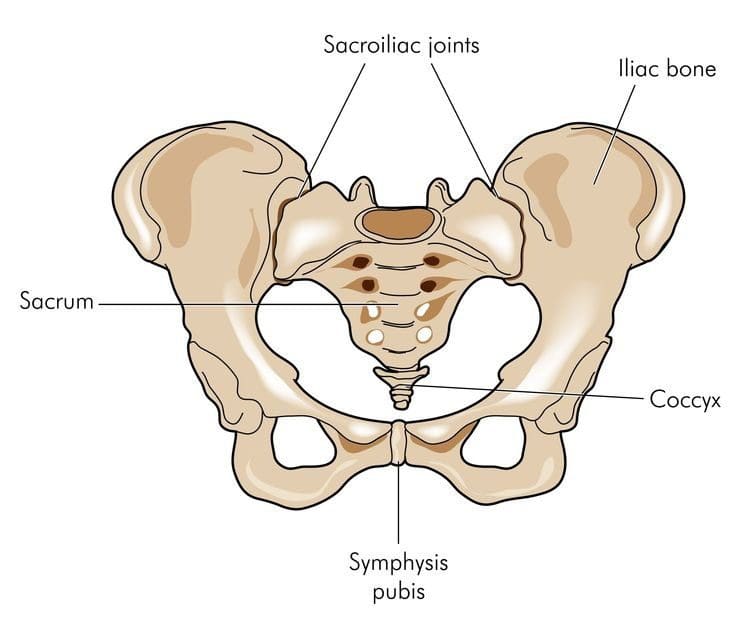
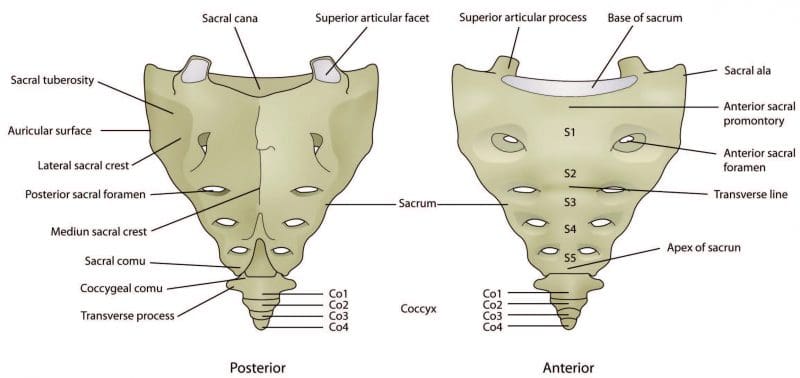
The sacrum and coccyx are part of the vertebral spinal column and could contribute to low back pain. They are not like the other bones in the spinal column. The sacrum, also known as the sacral vertebra, sacral spine, and S1 is a large, flat triangular-shaped bone that is between the hip bones and below the last lumbar vertebra known as L5. The coccyx, known as the tailbone, is positioned below the sacrum.
The sacrum and coccyx are made up of smaller bones that fuse and grow into a solid bone mass by the age of 30. The sacrum is composed of 5 fused vertebrae known as S1-S5 and 3 to 5 smaller bones that fuse creating the coccyx. Both are weight-bearing bones and are integral to walking, standing, and sitting functions.
Contents
Sacrum and the Lumbosacral Spine
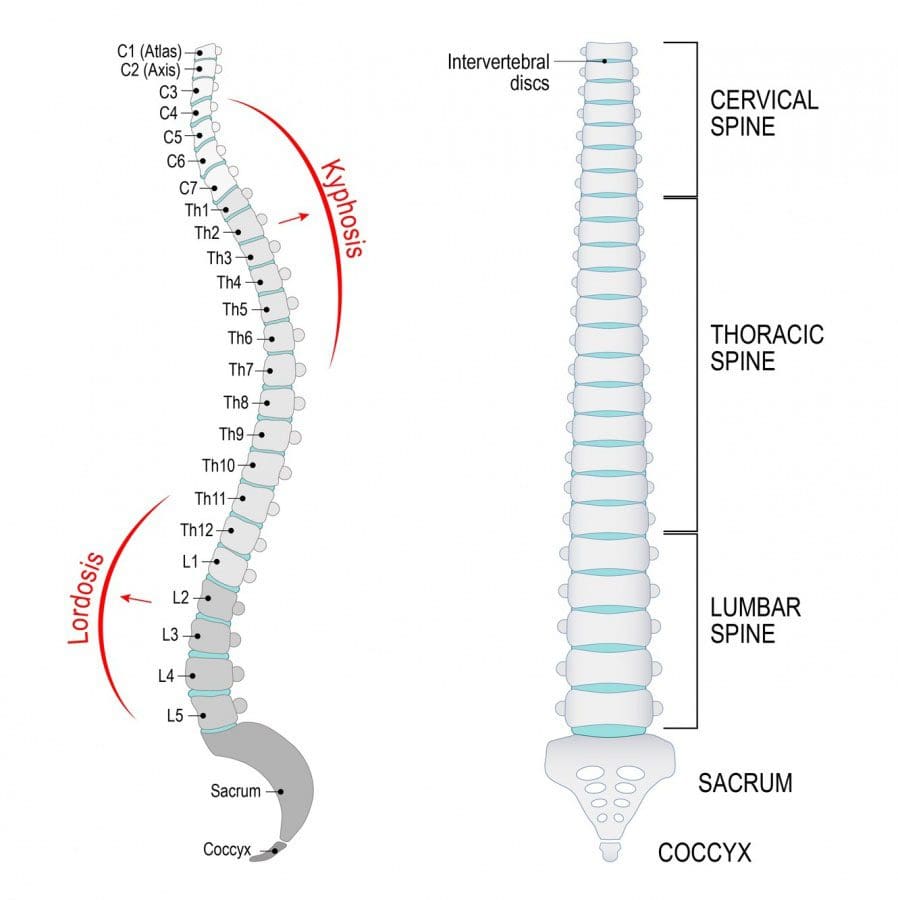
The sacrum forms the back of the pelvis. Along with the coccyx and the two sacroiliac joints make up the pelvic girdle. S1 is at the top of the sacrum and connects to the last lumbar vertebrae L5. Together they create the lumbosacral spine. Where they join forms the lumbosacral curves known as lumbar lordosis and lumbar kyphosis.
The curvature works to support the upper body, weight/force distribution maintains spinal balance and flexibility. Lordosis is the inward curve of the spine, but too much can cause swayback that can be associated with spondylolisthesis. Loss of this curve can cause spinal imbalance and can lead to Flatback syndrome.
Kyphosis is the outward curve of the spine. The location of the sacrum at the intersection of the spine and pelvis means it has an important role in the movement of the low back and hips. The sacrum�s joints help to bear weight and help stabilize the spinal column along with the ligaments, tendons, and muscles help support/stabilize joint movement.
Lumbosacral joint
Joint L5 and S1connect the lumbar spine to the sacrum. The pressure at this meeting point can be massive as the curve of the spine shifts from the lordotic forward curve to a kyphotic backward curve. The L5-S1 region bears weight, absorbs, and distributes the upper body�s weight when moving and resting. Disc herniation and spondylolisthesis are more common at L5-S1 for this reason.
Sacroiliac joints
The sacroiliac joints connect the sacrum to the left and right sides of the pelvis. The range of movement of the sacroiliac joints is minimal compared to other joints like the knees. However, the joints are essential for walking, standing, and stabilization of the hips. Sacroiliitis and sacroiliac joint dysfunction are two spinal disorders related to the joints. Other spinal disorders related to the sacral spine include:
The coccyx commonly known as the tailbone is just below the sacrum. It is smaller than the sacrum and has an important weight-bearing function. It helps supports weight while sitting.An example is leaning back while sitting. This motion and position increase the pressure/weight on the coccyx. An injury in this area can cause tailbone pain. Inflammation of the coccyx�s connective tissue that results in tailbone pain that gets worse when sitting is a common symptom. A traumatic event like a fall or auto accident that causes a tailbone fracture can also cause this pain.
Sacral and Coccygeal Nerves
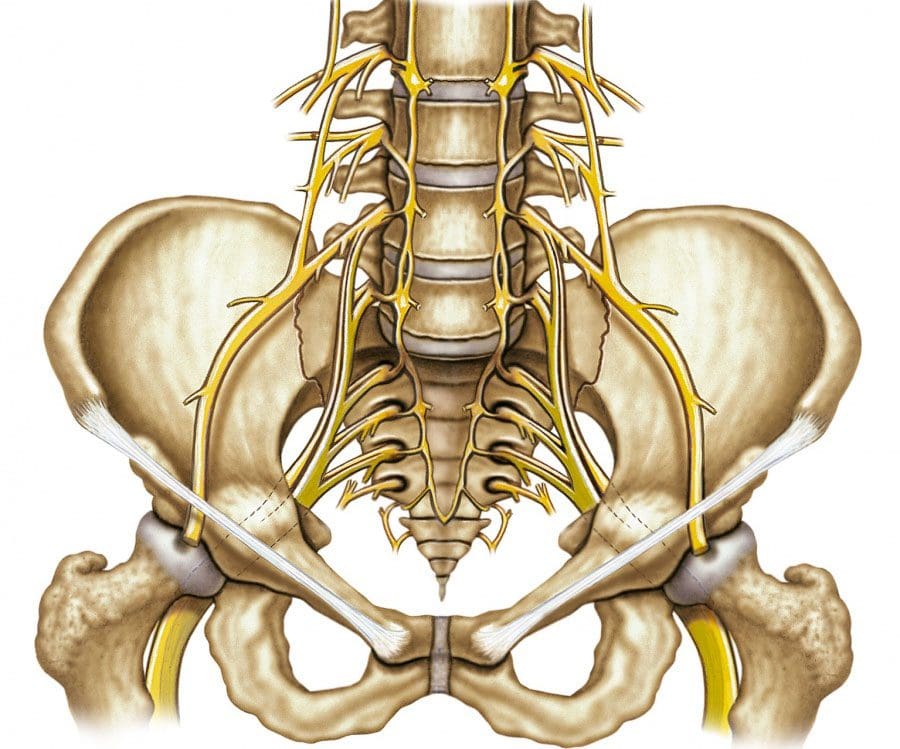
The spinal cord ends at L1-L2, which branches out into the cauda equina, which is a bundle of nerves that looks like a horse’s tail. In the sacrum, there are sacral nerves known as the sacral plexus. Plexus means a network of nerve structures. The sacral and lumbar plexus compose the lumbosacral plexus. This is where the sciatic nerve, which is the largest nerve in the sacral plexusconverges into the band. Sciatic nerve compression causes a combination of symptoms known as sciatica. It is very well known for causing low back and leg pain.
The coccygeal nerve serves the tailbone. There are five sacral nerves numbered S1 through S5 and are part of the spinal cord.
S1 supports groin and hip function
S2 the back of the thighs
S3 the middle of the buttock area
S4 and S5 the anus and vagina
Injury or trauma to the sacral spine can cause mild stress fractures to severe bone fractures. These fractures can cause sacral nerve compression and intense pain. Symptoms include:
A doctor or chiropractor, physical therapist are excellent sources for information to help prevent sacrum and coccyx pain. These medical professionals will utilize a patient’s medical history, recommend lifestyle changes and injury prevention guidelines.
If at risk of developing osteoporosis then a bone mineral density test could be recommended.
Proper posture must be maintained. Avoid slouching as this places added pressure on the lumbosacral spine and the sacroiliac joints.
Proper body mechanics when engaging in any activity needs to be observed.
Use legstrength to lift objects.
Avoid twisting while lifting or holding heavy objects, as this can cause sprain, strain, or serious injury of the lower spine.
Put on the seat belt. Auto accidents are a major cause of spine trauma. Exercise restraint when driving or riding in any vehicle even a golf cart.
Sciatica Pain Relief
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
Nutritional relief for acute and chronic back pain can be achieved by eating specific fruits and vegetables. Individuals dealing with acute and chronic back pain have recently been asking if their diets can be modified to reduce back pain. Absolutely, eating healthier will lead to weight loss and will help reduce back pain symptoms.
The big surprise was a nutritionist that did not know about this recommendation to help ease back pain symptoms. Life seems to throw a lot of curveballs especially in the midst of pain. Stress eating and just eating great tasting food is one method/technique of dealing with the pain, as it makes you feel good and forget the pain for a little while.
However, the problem is still present and becomes worse with the added weight. Not to mention the consequences of eating too much unhealthy food, like diabetes, high blood pressure, etc. Eating junk food and suffering in silence can become a way of life.
Contents
Pain Relief With Healthy Food
Most individuals will experience back pain at some point. There are a variety of causes from disease to injury and just normal wear and tear.Fortunately, for most, it will be short-lived. But for some chronic pain can develop, creating a new set of health issues and makes achieving back pain relief more complicated. It may sound too easy but making adjustments to your diet can make all the difference in dealing with and eliminating back pain.
Manage and eradicate back pain
Constantly going for the wrong foods, speeds up the inflammation process. Various studies show certain foods contain components that have anti-inflammatory properties. Experts agree that choosing healthy foods for and/or chronic illnesses reduces flare-ups, inflammation and helps heal the body back to top form.
The pain reduces because the inflammation triggers are kept in check. This means the grocery store and healthy foods can be a powerful tool for fighting inflammation. Our ancestors lived off the land eating organic natural foods and healed themselves without refined products.
Multi-colored vegetables and fruits
Dark green vegetables supply powerful nutrients that fight inflammation. Added benefits are they help remove cancer-causing free radicals. Examples include:
Spinach
Broccoli
Kale
Collard greens
Orange and yellow vegetables like:
Carrots
Squash
Pumpkin
Peppers
Pineapple
Carrots contain vitamin E and C and antioxidants that protect the healthy tissue around the inflamed area. Pineapple contains natural enzymes that help break down fibrin that forms around any acute injury. As the barrier is broken down nutrients are allowed to penetrate the area and ease the inflammation.
Nutritional Relief
The ability to heal the body with proper food choices should be a no brainer. But because humans are creatures of habit, breaking away from what is normal for the individual can be a challenge. Some simple ways to start eating toward healing:
Reduce the fat intake like butter, corn, red meat, and simple carbohydrates that are high in sugar and low in fiber.
When eating fill up with vegetables, fruits, and herbs and reduce the meat intake. Eat two to three servings of fruits and vegetables at all meals.
There are plenty of choices that can aid in healing the body from the inside out. Take nutritional relief steps now and start on the road to recovery.
Back Pain During Pregnancy Treatment
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
Children and adolescents are experiencing back pain. Why it happens, and how parents can help prevent it is the objective. When thinking of back pain the image is typically a man or woman, hunched over grabbing their backs and wincing in pain. However, back pain in children and adolescents is not that uncommon.
According to a 2020 study published in Spine, around thirty-four percent of children report having back pain, with almost nine percentexperiencing severe back pain. By the time they are fifteen, 20 to 70% of children will have experienced back pain at some point. Developing chronic back pain increases with age and is more common in girls.
The study found those that sought out early treatment, physical therapy, and chiropractic being the most prescribed lessened the need for more invasive treatments, like spinal injections, and surgery. Back pain can have a major impact on an adult’s life, and more so on a child. Prevention and treatment are important to help restore overall health and wellness.
Contents
Signs and Symptoms
Symptoms can vary, the most common:
Pain increases with movement, like bending or twisting
Increased pain after sitting or standing for an extended period
Sore and tender muscles around the spine
Tight muscles
Muscle spasms
Most back pain in children is mild. However, there are times when the child will require medical attention. A child should see a doctor if back pain persists for more than two or three days, if there is a fever, or if there is any numbness or weakness in the arms and legs.
Common Causes
Like adults, muscle sprains and strains are the most common cause of back pain. Strains are more common in the low back than around the neck or middle back and usually occur from overuse injuries, poor posture, poor body mechanics, and falls. Other common causes include:
Sitting and slouching in front of the computer for too long
Carrying an overloaded backpack
Spinal Conditions
Recreational and sports activities with injuries sustained are the most common causes of developing back pain. However, back pain can be brought on by underlying health and spine-related conditions. About a third of adolescents with low back pain could have a spinal condition. The most common conditions include:
Idiopathic Scoliosis
This is an abnormal curvature of the spine. This is usually not a painful condition. Some curvatures can be severe enough to cause pain and require medical care. Scoliosis can include the middle, low spine, or the entire spine. It is most common in adolescents 11-17 years of age. Symptoms include:
Tilted shoulders
Uneven hip bones
One side of the ribs projects out more than the other
Scheuermann�s kyphosis
This is a growth disorder of the vertebrae. It happens when the front of the spine does not grow as fast as the back of the spine. This can produce a humpback curvature. The spine bends forward but the child cannot stand up straight. Usually, it happens during accelerated growth periods.
Spondylolysis
The vertebrae can break in children and kids that do repetitive exercises involving bending and twisting. Sports like gymnastics and football create a heightened risk for spondylolysis. It usually affects the low back and presents with non-stop low back pain. The most common treatment is rest. Other causes include:
Spinal cord tumors
Sickle cell anemia
Infection
Tumors and infections are highly uncommon in children. They often present with pain and fever. If the nerves are pinched numbness, tingling, and weakness in the extremities can develop.
Common Treatments
Back pain in children is usually a short experience and can be treated with ice, rest, and over-the-counter medications like acetaminophen for children and nonsteroidal anti-inflammatory drugs like ibuprofen. A playing/exercise program can significantly help reduce child back pain.
However, there could be a need to modify the activity, so as to not worsen the injury or create new injury/s. The activities could be made to be lighter or a brace could be utilized. A specialist like a chiropractor/physical therapist can provide treatment, along with exercises, stretches, and lifestyle changes that will help reduce the pain. Complementary therapies like massage and acupuncture can enhance the child�s healing/recovery time and knock out the pain quickly.
Parental Prevention
Proper posture can and will prevent back pain. Children’s and adolescents’ musculoskeletal structures continue to develop at this stage. Therefore, sitting, standing, and lifting properly is paramount to preventing back pain. Along with this is avoiding activities that place repeated strain on the spine. An example is an overexertion while playing sports. Tips for keeping kids back-pain free:
Avoid activities that generate repeated strain on the same muscles
Stretching breaks need to be incorporated when sitting for a long time
As much as possible make the home a stress-free environment
Maintain a healthy weight and diet with balanced meals and snacks
Help promote overall mental and physical health
Children and kids that are stressed out or depressed have a greater risk of developing back pain. Encourage the kids to stay active, get proper sleep, stretch out, and eat foods that are healthy for the spine. If back pain is presenting, a customized treatment plan along with lifestyle changes will get the child back to their favorite activities.
Lower Back Pain Chiropractic Treatment
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
Acetaminophen, best known as Tylenol, is one of the most common medications for headaches and general pain. More than likely the most common back, neck, and overall pain medication around. However, it is only a pain reducer, and will not reduce inflammation.
Doctors often recommend this medicine before moving on to prescription medication. A member of the analgesic pain reliever class of medications. These can vary in strength along with side effects, but their purpose is to reduce pain. Acetaminophen can be found in over 600 prescriptions and over-the-counter medicines, including certain opioids. Other acetaminophen brand names include:
Tylophen
Tempra
FeverAll
Mapap
Pharbetol
Panadol
Contents
Strength and Weakness
When neck or back pain presents, over-the-counter medicines fall into two categories. These are acetaminophen or non-steroid anti-inflammatory drugs also known as NSAIDs. Acetaminophen and NSAIDs like Advil, aspirin both relieve pain. However, non-steroid anti-inflammatories also help in reducing inflammation. Although non-steroid anti-inflammatories have this added benefit, they can also present potential side effects like stomach and gastrointestinal problems.A spinal sprain or strain can cause acute back pain. Acetaminophen is typically recommended for acute back or neck pain and for pain that comes and goes quickly. Individuals that experience periodic pain usually take acetaminophen when the pain flares up. Individuals with chronic spinal pain report acetaminophen help to alleviate/reduce the pain. Many with chronic pain use acetaminophen regularly and not only when the pain presents. This helps manage before pain strikes.
Safety
Acetaminophen is gentle on the stomach, making some individuals preferring it over the non-steroid anti-inflammatories. But just like any other medication acetaminophen has its risks and can cause severe damage if used improperly.
Taking acetaminophen in large doses can cause severe liver damage. The Food and Drug Administration reports that acetaminophen overdoses send over fifty-thousand individuals to the emergency room every year. And over one-hundred Americans die yearly from accidental overdoses.
Using acetaminophen safely means taking no more than 3,000 milligrams a day and no more than 1,000 milligrams at a time. Take extra precautions when taking extra-strength. These can include as much as 650 mg per pill/capsule.Before taking acetaminophen for back and neck pain, talk to a doctor or pharmacist about the proper dosage. And tell the doctor about all the medications being taken including natural herbs and holistic. Another reason for telling the doctor is that many other medications have acetaminophen included without you knowing it. Part of the discussion should include alcohol consumption. This can elevate the risk of negative reactions.
Resources
If non-pharmacological treatments/therapies done for at least 4 months prove ineffective then an acetaminophen regimen could be a safe and effective part of a back and neck pain treatment plan. While this medicine is one of the most common treatments, it is not without risks and side effects. Talk to a doctor or pharmacist about all the medications and supplements to ensure the regimen supports health for the long-term. To learn more along with safety information go to Acetaminophen Patient Guide.
Severe Back Pain Chiropractic Treatment
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
Breathing exercises along with meditation can be beneficial for individuals with back pain. Breath control techniques, exercises, and meditation techniques help bring the mind and body into functional harmony.This can help ease and reduce back pain. The article discusses the benefits of how these techniques help promote spinal health.
Contents
Breathing Exercises
Developing the ability to rhythmically breathe properly and optimally helps reduce back pain. This is because it allows the individual to focus on breathing, keeping the brain from focusing on the back pain. Most individuals breathe in a shallow manner, taking short, uneven breaths. This does not allow for sufficient blood flow throughout the body. Only the minimum amount is being pumped, which does not help inflamed/injured areas.
Proper breathing technique involves taking deep slow, smooth breaths that reach into the abdominal area. Each inhale should be the same length when exhaling. One way to make sure is to inhale and hold for five seconds then exhale for five seconds. This can be done while sitting or lying down but these exercises should be practiced anywhere regularly to get into the habit of breathing fully. It could be in the car, at work, at a desk, the store, etc.
Meditation
Meditation helps the body and the brain relax. This helps to loosen and unclench the back muscle tension. It helps decrease the perception of pain by resetting the focus on something other than the pain. While meditating the objective is to let go of negative thoughts, specifically thoughts on pain, allowing the positive to take over.
There are various ways this can be achieved like listening or watching the rain, ocean waves, or nature soothing videos. It’s not about forgetting the back pain but a system to cope with it. Meditation helps an individual become more aware of their mind and body. Meditation should be done sitting or lying down in a comfortable position.
Connecting Mind and Body
Today local gyms and yoga studios offer workshops that focus on breathing and meditation combined with linking the mind and body. Check out DVDs and books available. These exercises/techniques are different for everyone. Try a variety to figure out which works for you, as it could be a combination. It’s all about finding safe natural ways to help relieve and prevent back pain. Although these are not considered strenuous physical activity, consult with a doctor or chiropractor before beginning a breathing/meditation regimen.
Back Pain Rehabilitation
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine