For individuals experiencing back pain from a herniated disc, can understanding the difference between surgery and chiropractic help individuals find the right treatment plan?
Surgery or Chiropractic
Living with back pain can be a nightmare, and yet many struggle without seeking care. Today, there are a vast number of surgeries and noninvasive techniques that are better at treating spine and back problems and managing symptoms. For individuals who may have a herniated disc or are curious about ways to relieve their back pain, a health care provider, physical therapist, spine specialist, and chiropractor can inform them of treatment options. Surgery and chiropractic therapy are popular treatments for a herniated, bulging, or slipped disc.
A herniated disc is when the cartilage discs that cushion the vertebrae shift out of position and leak out.
Surgery for a herniated disc involves removing or repairing the disc.
Chiropractic nonsurgically repositions the disc and realigns the spine.
Both treatments have the same goals with key differences.
Chiropractic Care
Chiropractic is a system of therapy that focuses on adjusting and maintaining spinal alignment to help with back and posture problems. Chiropractors are trained and licensed medical professionals who take a nonsurgical approach, a proven therapy for chronic pain, flexibility, and mobility issues.
The Way It Works
Chiropractic treatment encourages and supports the body’s natural healing processes. It is considered for joint pain in the back, neck, legs, arms, feet, and hands. It typically involves sessions in which the chiropractor physically and carefully adjusts the vertebrae by hand, also known as spinal manipulation or chiropractic adjustments. (MedlinePlus. 2023). A chiropractor performs a thorough medical evaluation and runs tests to establish a diagnosis. A chiropractor will develop a treatment plan that may involve a team of massage and physical therapists, acupuncturists, health coaches, and nutritionists to treat affected areas with various techniques, recommend targeted exercises, adjust lifestyle and nutrition to support the treatment, and monitor progress. Combined with stretching and sustained pressure, the multiple methods can increase joint mobility and relieve pain symptoms. (National Center for Complimentary and Integrative Health. 2019) Added protocols to support or enhance chiropractic therapy include:
Heating and ice therapies to reduce inflammation and increase blood circulation.
Using devices to stimulate muscles and nerves electrically.
Developing relaxation and deep breathing techniques.
Incorporating exercises to promote rehabilitation.
Establishing a regular fitness routine.
Making adjustments to diet and lifestyle.
Taking certain dietary supplements.
Spinal manipulation and chiropractic adjustments have been shown to improve symptoms and restore mobility in cases of chronic back pain. One review found that individuals with chronic lumbar/low back pain reported significant improvement after six weeks of chiropractic treatment. (Ian D. Coulter et al., 2018)
Prices
The out-of-pocket expenses of chiropractic treatment depend on a variety of factors.
Insurance may or may not cover the treatment, and the amount an individual has to pay can vary based on the severity of their case, what their plan covers, and where they live. One review found the cost can range between $264 and $6,171. (Simon Dagenais et al., 2015)
Surgery
There is a range of minimally invasive surgical procedures to treat herniated discs. These work to ease nerve compression by removing or replacing damaged discs or stabilizing the vertebrae, relieving pain and inflammation.
The Way It Works
A herniated disc can happen in any part of the spine but is more common in the lower back/lumbar spine and in the neck/cervical spine. Surgery is recommended when: (American Academy of Orthopaedic Surgeons. 2022)
More conservative treatments, like medications and physical therapy, are unable to manage symptoms.
The pain and symptoms impact daily life and functioning.
Standing or walking becomes difficult or impossible.
The herniated disc causes difficulty walking, muscle weakness, and bladder or bowel control loss.
The individual is reasonably healthy, without infection, osteoporosis, or arthritis.
Specific surgical procedures used include:
Fusion Surgery
Spinal fusion is the most common procedure for a lower back herniated disc.
It involves using artificial bone material to fuse vertebrae to increase stability and release and prevent nerve irritation and compression. (American Academy of Neurological Surgeons. 2024)
Laminotomy and Laminectomy
Herniated disc symptoms appear from compression placed on the nerves.
Laminotomy involves making a small cut in the lamina, or the arch of the spinal vertebrae, to release the pressure.
Another approach involves implanting an artificial disc.
This is most often used for hernia in the lower spine; the worn or damaged disc is removed, and a specialized prosthetic replaces the removed disc. (American Academy of Orthopaedic Surgeons. 2022)
This allows for more mobility.
The success of herniated disc surgery depends on different factors. Advances in minimally invasive techniques have significantly improved long-term outcomes, with one review finding that around 80% reported good—excellent results at a six-year follow-up. (George J. Dohrmann, Nassir Mansour 2015) However, there is the possibility of recurrence. About 20% to 25% of individuals with herniated lumbar discs experience re-herniation at some point. (American Academy of Neurological Surgeons. 2024)
Prices
Surgery for a herniated disc is specialized, and the costs depend on the scope and scale of the treatment.
The individual’s specific insurance plan also determines the expenses.
When choosing between chiropractic and surgery for a herniated disc, a number of factors can determine the decision, including:
Chiropractic is the less invasive nonsurgical option.
Chiropractic adjustments cannot help certain severe cases of herniated discs.
Chiropractic adjustments prevent the herniated disc from getting worse and ease symptoms.
Surgery provides pain and symptom relief faster than chiropractic or conservative treatment but requires significant recovery time and is expensive. (Anna N A Tosteson et al., 2008)
Surgery may not be appropriate for individuals with osteoarthritis or osteoporosis.
Chiropractic therapy is among the more conservative treatment options for a herniated disc and may be tried first before proceeding with surgery. Generally, surgery is only recommended when noninvasive methods haven’t been able to stop or manage the pain and symptoms. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution that fully benefits the individual to get back to normal.
Quick Patient Process
References
MedlinePlus.MedlinePlus. (2023). Chiropractic. Retrieved from https://medlineplus.gov/chiropractic.html
National Center for Complimentary and Integrative Health. (2019). Chiropractic: in depth. Retrieved from https://www.nccih.nih.gov/health/chiropractic-in-depth
Coulter, I. D., Crawford, C., Hurwitz, E. L., Vernon, H., Khorsan, R., Suttorp Booth, M., & Herman, P. M. (2018). Manipulation and mobilization for treating chronic low back pain: a systematic review and meta-analysis. The spine journal : official journal of the North American Spine Society, 18(5), 866–879. https://doi.org/10.1016/j.spinee.2018.01.013
Dagenais, S., Brady, O., Haldeman, S., & Manga, P. (2015). A systematic review comparing the costs of chiropractic care to other interventions for spine pain in the United States. BMC health services research, 15, 474. https://doi.org/10.1186/s12913-015-1140-5
American Academy of Orthopaedic Surgeons. (2022). Herniated disk in the lower back. https://orthoinfo.aaos.org/en/diseases–conditions/herniated-disk-in-the-lower-back/
American Academy of Neurological Surgeons. Surgeons, A. A. o. N. (2024). Herniated disc. https://www.aans.org/en/Patients/Neurosurgical-Conditions-and-Treatments/Herniated-Disc
Dohrmann, G. J., & Mansour, N. (2015). Long-Term Results of Various Operations for Lumbar Disc Herniation: Analysis of over 39,000 Patients. Medical principles and practice : international journal of the Kuwait University, Health Science Centre, 24(3), 285–290. https://doi.org/10.1159/000375499
Tosteson, A. N., Skinner, J. S., Tosteson, T. D., Lurie, J. D., Andersson, G. B., Berven, S., Grove, M. R., Hanscom, B., Blood, E. A., & Weinstein, J. N. (2008). The cost effectiveness of surgical versus nonoperative treatment for lumbar disc herniation over two years: evidence from the Spine Patient Outcomes Research Trial (SPORT). Spine, 33(19), 2108–2115. https://doi.org/10.1097/brs.0b013e318182e390
Spinal stenosis is the term used to describe a narrowing spine. Treatments vary because everybody’s case is different. Some individuals experience mild symptoms, while others experience severe symptoms. Can knowing treatment options help the patient and healthcare team customize and personalize a treatment plan to the individual’s condition?
Spinal Stenosis Treatments
Spaces within the spine can become narrower than they’re supposed to be, which can cause pressure on nerve roots and the spinal cord. Anywhere along the spine can be affected. The narrowing can cause pain, burning, and/or aching in the back and weakness in the legs and feet. Spinal stenosis has several primary treatments. When working through spinal stenosis treatments, a healthcare provider will assess symptoms and start treatment with first-line therapy, such as pain medication and/or physical therapy. These are often the first among individuals with the disease.
Medication
Chronic pain is one of the main symptoms. The first-line treatment often involves using pain-relieving medication/s. Commonly prescribed medications are nonsteroidal anti-inflammatories or NSAIDs. These medications reduce pain and inflammation. However, NSAIDs are not recommended for long-term use, and other medications may need to be used to relieve pain that includes: (Sudhir Diwan et al., 2019)
Tylenol – acetaminophen
Gabapentin
Pregabalin
Opioids for severe cases
Exercise
Exercise can reduce spinal stenosis symptoms by taking pressure off the nerves, which can reduce pain and improve mobility. (Andrée-Anne Marchand et al., 2021) Healthcare providers will recommend the most effective exercises for the individual. Examples include:
Another primary spinal stenosis treatment is physical therapy, which is often used alongside pain medications. Typically, individuals undergo six to eight weeks of physical therapy, with sessions two to three times a week. Utilizing physical therapy has been shown to (Sudhir Diwan et al., 2019)
Reduce pain
Increase mobility
Reduce pain medications.
Reduce mental health symptoms like anger, depression, and mood changes.
For severe cases, physical therapy following surgery can reduce recovery times.
Back Braces
Back braces can help reduce movement and pressure on the spine. This is helpful because even small spinal movements can lead to nerve irritation, pain, and worsening symptoms. Over time, the bracing can lead to a positive increase in mobility. (Carlo Ammendolia et al., 2019)
Injections
Epidural steroid injections may be recommended to relieve severe symptoms. Steroids act as anti-inflammatories to reduce pain and swelling caused by inflammation and irritation of the spinal nerves. They are considered nonsurgical medical procedures. According to research, injections can effectively manage pain for two weeks and up to six months, and some research has found that after a spinal injection, relief can last 24 months. (Sudhir Diwan et al., 2019)
Thickened Ligaments Decompression Procedure
Some individuals may be recommended to undergo a decompression procedure. This procedure involves using a thin needle tool inserted into the back. The thickened ligament tissue is removed to reduce the pressure on the spine and nerves. Research has found that the procedure can reduce symptoms and the need for more invasive surgery. (Nagy Mekhail et al., 2021)
Alternative Treatments
In addition to first-line treatments, individuals may be referred to alternative therapies for symptom management, including:
Acupuncture
This involves the insertion of thin-tipped needles into various acupoints to relieve symptoms.
Some research has found that acupuncture may be more effective at reducing symptoms than physical therapy alone. Both options are viable and can improve mobility and pain. (Hiroyuki Oka et al., 2018)
Chiropractic
This therapy reduces pressure on nerves, maintains spinal alignment, and helps to improve mobility.
Massage
Massage helps to increase circulation, relax the muscles, and reduce pain and stiffness.
New Treatment Options
As spinal stenosis research continues, new therapies are emerging to help relieve and manage symptoms in individuals who don’t respond to traditional medicine or cannot partake in conventional therapies for various reasons. However, some evidence presented is promising; medical insurers may consider them experimental and not offer coverage until their safety has been proven. Some new treatments include:
Acupotomy
Acupotomy is a form of acupuncture that uses thin needles with a small, flat, scalpel-type tip to relieve tension in painful areas. Research on its effects is still limited, but preliminary data shows it could be an effective complementary treatment. (Ji Hoon Han et al., 2021)
Stem Cell Therapy
Stem cells are the cells from which all other cells originate. They act as the raw material for the body to create specialized cells with specific functions. (National Institutes of Health. 2016)
Individuals with spinal stenosis can develop soft tissue damage.
Stem cell therapy uses stem cells to help repair injured or diseased tissues.
Stem cell therapy can help repair or improve the damaged areas and provide symptom relief.
Clinical studies for spinal stenosis report that it could be a viable treatment option for some.
However, more research is needed to confirm whether the therapy is effective enough to be widely used. (Hideki Sudo et al., 2023)
Dynamic Stabilization Devices
LimiFlex is a medical device undergoing research and analysis for its ability to restore mobility and stability in the spine. It is implanted into the back through a surgical procedure. According to research, individuals with spinal stenosis who receive the LimiFlex often experience a higher reduction in pain and symptoms than with other forms of treatment. (T Jansen et al., 2015)
Lumbar Interspinous Distraction Decompression
Lumbar interspinous distraction decompression is another surgical procedure for spinal stenosis. The surgery is performed with an incision above the spine and places a device between two vertebrae to create space. This reduces movement and pressure on the nerves. Preliminary results show positive short-term relief from symptoms; long-term data is not yet available as it is a relatively new spinal stenosis treatment option. (UK National Health Service, 2022)
Surgical Procedures
There are several surgical procedures are available for spinal stenosis. Some include: (NYU Langone Health. 2024) Surgery for spinal stenosis is often reserved for individuals with severe symptoms, like numbness in the arms or legs. When these symptoms develop, it indicates a more notable compression of the spinal nerves and the need for a more invasive treatment. (NYU Langone Health. 2024)
Laminectomy
A laminectomy removes part or all of the lamina, the vertebral bone covering the spinal canal.
The procedure is designed to reduce pressure on nerves and the spinal cord.
Laminotomy and Foraminotomy
Both surgeries are used if an individual’s spinal stenosis negatively affects an opening in the vertebral foramen.
Ligaments, cartilage, or other tissues that constrict the nerves are removed.
Both reduce pressure on the nerves traveling through the foramen.
Laminoplasty
A laminoplasty relieves pressure on the spinal cord by removing parts of the spinal canal’s lamina.
This surgical procedure involves removing herniated or bulging discs that are placing pressure on the spinal cord and nerves.
Spinal fusion
Spinal fusion involves joining two vertebrae using metal pieces like rods and screws.
The vertebrae are more stable because the rods and screws act as a brace.
Which Treatment Is The Right One?
Because all treatment plans differ, determining the most effective is best suited for a healthcare provider. Each approach will be personalized to the individual. To decide what therapy is best, healthcare providers will assess: (National Institute of Arthritis and Musculoskeletal and Skin Diseases. 2023)
The severity of symptoms.
The current level of overall health.
The level of damage that’s occurring in the spine.
The level of disability and how mobility and quality of life are affected.
Injury Medical Chiropractic and Functional Medicine Clinic will work with an individual’s primary healthcare provider and/or specialists to help determine the best treatment options and concerns regarding medications or other forms of treatment.
Unlocking Wellness
References
Diwan, S., Sayed, D., Deer, T. R., Salomons, A., & Liang, K. (2019). An Algorithmic Approach to Treating Lumbar Spinal Stenosis: An Evidenced-Based Approach. Pain medicine (Malden, Mass.), 20(Suppl 2), S23–S31. https://doi.org/10.1093/pm/pnz133
Marchand, A. A., Houle, M., O’Shaughnessy, J., Châtillon, C. É., Cantin, V., & Descarreaux, M. (2021). Effectiveness of an exercise-based prehabilitation program for patients awaiting surgery for lumbar spinal stenosis: a randomized clinical trial. Scientific reports, 11(1), 11080. https://doi.org/10.1038/s41598-021-90537-4
Ammendolia, C., Rampersaud, Y. R., Southerst, D., Ahmed, A., Schneider, M., Hawker, G., Bombardier, C., & Côté, P. (2019). Effect of a prototype lumbar spinal stenosis belt versus a lumbar support on walking capacity in lumbar spinal stenosis: a randomized controlled trial. The spine journal : official journal of the North American Spine Society, 19(3), 386–394. https://doi.org/10.1016/j.spinee.2018.07.012
Mekhail, N., Costandi, S., Nageeb, G., Ekladios, C., & Saied, O. (2021). The durability of minimally invasive lumbar decompression procedure in patients with symptomatic lumbar spinal stenosis: Long-term follow-up. Pain practice : the official journal of World Institute of Pain, 21(8), 826–835. https://doi.org/10.1111/papr.13020
Oka, H., Matsudaira, K., Takano, Y., Kasuya, D., Niiya, M., Tonosu, J., Fukushima, M., Oshima, Y., Fujii, T., Tanaka, S., & Inanami, H. (2018). A comparative study of three conservative treatments in patients with lumbar spinal stenosis: lumbar spinal stenosis with acupuncture and physical therapy study (LAP study). BMC complementary and alternative medicine, 18(1), 19. https://doi.org/10.1186/s12906-018-2087-y
Han, J. H., Lee, H. J., Woo, S. H., Park, Y. K., Choi, G. Y., Heo, E. S., Kim, J. S., Lee, J. H., Park, C. A., Lee, W. D., Yang, C. S., Kim, A. R., & Han, C. H. (2021). Effectiveness and safety of acupotomy on lumbar spinal stenosis: A pragmatic randomized, controlled, pilot clinical trial: A study protocol. Medicine, 100(51), e28175. https://doi.org/10.1097/MD.0000000000028175
Sudo, H., Miyakoshi, T., Watanabe, Y., Ito, Y. M., Kahata, K., Tha, K. K., Yokota, N., Kato, H., Terada, T., Iwasaki, N., Arato, T., Sato, N., & Isoe, T. (2023). Protocol for treating lumbar spinal canal stenosis with a combination of ultrapurified, allogenic bone marrow-derived mesenchymal stem cells and in situ-forming gel: a multicentre, prospective, double-blind randomised controlled trial. BMJ open, 13(2), e065476. https://doi.org/10.1136/bmjopen-2022-065476
National Institutes of Health. (2016). Stem cell basics. U.S. Department of Health and Human Services. Retrieved from https://stemcells.nih.gov/info/basics/stc-basics
Jansen, T., Bornemann, R., Otten, L., Sander, K., Wirtz, D., & Pflugmacher, R. (2015). Vergleich dorsaler Dekompression nicht stabilisiert und dynamisch stabilisiert mit LimiFlex™ [A Comparison of Dorsal Decompression and Dorsal Decompression Combined with the Dynamic Stabilisation Device LimiFlex™]. Zeitschrift fur Orthopadie und Unfallchirurgie, 153(4), 415–422. https://doi.org/10.1055/s-0035-1545990
UK National Health Service. (2022). Lumbar decompression surgery: How It’s performed. https://www.nhs.uk/conditions/lumbar-decompression-surgery/what-happens/
NYU Langone Health. (2024). Surgery for spinal stenosis. https://nyulangone.org/conditions/spinal-stenosis/treatments/surgery-for-spinal-stenosis
Columbia Neurosurgery. (2024). Cervical laminoplasty procedure. https://www.neurosurgery.columbia.edu/patient-care/treatments/cervical-laminoplasty
National Institute of Arthritis and Musculoskeletal and Skin Diseases. (2023). Spinal stenosis: Diagnosis, treatment and steps to take. Retrieved from https://www.niams.nih.gov/health-topics/spinal-stenosis/diagnosis-treatment-and-steps-to-take
For individuals experiencing or managing low back pain and/or sciatica, can lumbar traction therapy help provide consistent relief?
Lumbar Traction
Lumbar traction therapy for lower back pain and sciatica could be a treatment option to help restore mobility and flexibility and safely support an individual’s return to an optimal level of activity. It is often combined with targeted therapeutic exercise. (Yu-Hsuan Cheng, et al., 2020) The technique stretches the space between the vertebrae in the lower spine, relieving lower back pain.
Lumbar or low back traction helps to separate the spaces between the vertebrae.
Separating the bones restores circulation and helps relieve the pressure on pinched nerves like the sciatic nerve, decreasing pain and improving mobility.
Research
Researchers say lumbar traction with exercise did not improve individual outcomes compared to physical therapy exercises on their own (Anne Thackeray et al., 2016). The study examined 120 participants with back pain and nerve root impingement who were randomly selected to undergo lumbar traction with exercises or simple exercises for pain. Extension-based exercises focused on bending the spine backward. This movement is considered effective for individuals with back pain and pinched nerves. The results indicated that adding lumbar traction to physical therapy exercises did not offer significant benefits over extension-based exercise alone for back pain. (Anne Thackeray et al., 2016)
A 2022 study found that lumbar traction is helpful for individuals with lower back pain. The study investigated two different lumbar traction techniques and found that variable-force lumbar traction and high-force lumbar traction helped to relieve lower back pain. High-force lumbar traction was also found to reduce functional disability. (Zahra Masood et al., 2022) Another study found lumbar traction improves the range of motion in the straight leg raise test. The study examined different forces of traction on herniated discs. All the levels improved the individuals’ range of motion, but the one-half body-weight traction setting was associated with the most significant pain relief. (Anita Kumari et al., 2021)
Treatment
For individuals with only low back pain, exercise, and postural correction may be all that is needed to provide relief. Research confirms physical therapy exercises can help decrease pain and improve mobility (Anita Slomski 2020). Another study revealed the importance of centralizing sciatic symptoms during repetitive movements. Centralization is moving the pain back to the spine, which is a positive sign that the nerves and discs are healing and occurs during therapeutic exercise. (Hanne B. Albert et al., 2012) A chiropractor and physical therapy team can educate patients on preventing back pain episodes. Chiropractors and physical therapists are body movement experts who can show which exercises are best for your condition. Starting an exercise program that centralizes symptoms can help individuals return to their normal lifestyle quickly and safely. Consult a healthcare provider before starting any exercise program for back pain.
Movement Medicine: Chiropractic
References
Cheng, Y. H., Hsu, C. Y., & Lin, Y. N. (2020). The effect of mechanical traction on low back pain in patients with herniated intervertebral disks: a systemic review and meta-analysis. Clinical rehabilitation, 34(1), 13–22. https://doi.org/10.1177/0269215519872528
Thackeray, A., Fritz, J. M., Childs, J. D., & Brennan, G. P. (2016). The Effectiveness of Mechanical Traction Among Subgroups of Patients With Low Back Pain and Leg Pain: A Randomized Trial. The Journal of orthopaedic and sports physical therapy, 46(3), 144–154. https://doi.org/10.2519/jospt.2016.6238
Masood, Z., Khan, A. A., Ayyub, A., & Shakeel, R. (2022). Effect of lumbar traction on discogenic low back pain using variable forces. JPMA. The Journal of the Pakistan Medical Association, 72(3), 483–486. https://doi.org/10.47391/JPMA.453
Kumari, A., Quddus, N., Meena, P. R., Alghadir, A. H., & Khan, M. (2021). Effects of One-Fifth, One-Third, and One-Half of the Bodyweight Lumbar Traction on the Straight Leg Raise Test and Pain in Prolapsed Intervertebral Disc Patients: A Randomized Controlled Trial. BioMed research international, 2021, 2561502. https://doi.org/10.1155/2021/2561502
Slomski A. (2020). Early Physical Therapy Relieves Sciatica Disability and Pain. JAMA, 324(24), 2476. https://doi.org/10.1001/jama.2020.24673
Albert, H. B., Hauge, E., & Manniche, C. (2012). Centralization in patients with sciatica: are pain responses to repeated movement and positioning associated with outcome or types of disc lesions?. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society, 21(4), 630–636. https://doi.org/10.1007/s00586-011-2018-9
For individuals suffering from neck pain and headaches, can craniosacral head massage therapy help provide relief?
Craniosacral Therapy
Craniosacral therapy is a gentle massage to release fascia or connective tissue network tension. The therapy is not new but has gained new attention because of the public interest in natural pain treatments and therapies. Studies are limited, but clinical research is ongoing to see if the therapy can become a mainstream treatment option. The therapy aims to alleviate the symptoms of various health ailments and conditions, including:
By relieving compression in the lower back, head, and spinal column, cerebrospinal fluid circulation is restored, and the body rhythms within the nervous system are reset. This provides pain relief, lowers stress, and improves overall well-being.
The focus areas are those along the fascia, the connective tissue that holds organs, blood vessels, bones, nerve fibers, and muscles in place. By working this tissue through gentle-pressure massage, practitioners help to calm the fight-or-flight response by relaxing the sympathetic nervous system. The symptoms will determine what areas of the body necessitate craniosacral therapy. Individuals with headaches will be given a head or neck massage. Other areas involved in craniosacral therapy include: (Heidemarie Haller, Gustav Dobos, and Holger Cramer, 2021)
Back
Around the spinal column.
Other areas like the joints or muscles.
The pressure applied during craniosacral therapy is light and not the same as a deep tissue massage.
The parasympathetic and sympathetic nervous systems control various body responses.
The parasympathetic nervous system supports proper rest and digestive functions, and the sympathetic nervous system regulates the body’s fight-or-flight response. (Cleveland Clinic. 2022)
Therapy Techniques
The massage techniques used in craniosacral therapy rely on low pressure intended to be as gentle as possible. The fingertips are often used to avoid applying too much pressure. Healthcare providers work the areas between the skull and the bottom of the spine to identify and reset imbalances within the body and the cerebrospinal fluid. If there is an imbalance in cerebrospinal fluid, the massage therapist will reposition the individual or press on the area to release and/or increase circulation. The techniques work to improve the body’s ability to regulate physiological responses. (Heidemarie Haller et al., 2019) During and after the session, individuals may experience different sensations, including: (Biodynamic Craniosacral Therapy Association of North America, 2024)
Relaxation.
Feeling like being in a meditative state.
Sleepiness.
Energized.
Feeling a sense of warmth.
Deeper breathing.
Feeling the body is straighter and taller.
Individuals Who Should Not Receive Craniosacral Therapy
Craniosacral therapy is considered safe; however, some individuals should avoid it or consult a healthcare provider before trying it. Those recommended not to receive the treatment include individuals with the following ailments or disorders:
Concussion or other traumatic brain injuries.
Blood clots.
Brain swelling.
Brain aneurysm – a blood-filled bulge in a blood vessel in or around the brain.
Conditions that cause cerebrospinal fluid buildup.
Treatment
Craniosacral therapy is offered by several healthcare providers, including:
Craniosacral therapy licensed massage therapists
Physical therapists
Occupational therapists
Osteopaths
Chiropractors
These professionals know how to perform the massage technique correctly.
Tension Headaches
References
Haller, H., Lauche, R., Sundberg, T., Dobos, G., & Cramer, H. (2019). Craniosacral therapy for chronic pain: a systematic review and meta-analysis of randomized controlled trials. BMC musculoskeletal disorders, 21(1), 1. https://doi.org/10.1186/s12891-019-3017-y
Haller, H., Dobos, G., & Cramer, H. (2021). The use and benefits of Craniosacral Therapy in primary health care: A prospective cohort study. Complementary therapies in medicine, 58, 102702. https://doi.org/10.1016/j.ctim.2021.102702
Biodynamic Craniosacral Therapy Association of North America. (2024). What is a session like? https://www.craniosacraltherapy.org/what-is-a-session-like-
For individuals practicing a low-carbohydrate eating style or want to try an alternative flour, can incorporating almond flour help in their wellness journey?
Almond Flour
Almond flour and almond meal are gluten-free alternatives to wheat products in certain recipes. They are made by grinding almonds and can be bought prepared or made at home with a food processor or grinder. The flour is higher in protein and lower in starch than other gluten-free flour.
Almond Flour and Almond Meal
The flour is made with blanched almonds, meaning the skin has been removed. Almond meal is made with whole or blanched almonds. The consistency for both is more like corn meal than wheat flour. They can usually be used interchangeably, although using the blanched flour will produce a more refined, less grainy result. Superfine almond flour is great for baking cakes but is difficult to make at home. It can be found at grocery stores or ordered online.
Carbohydrates and Calories
A half cup of commercially prepared flour contains about:
The glycemic index of almond flour is less than 1, which means it should have little effect on raising blood glucose levels.
The high glycemic index of whole wheat flour is 71, and rice flour is 98.
Using Almond Flour
It is recommended for making gluten-free quick bread recipes, such as gluten-free:
Muffins
Pumpkin bread
Pancakes
Some cake recipes
Individuals are recommended to start with a recipe already adapted for almond flour and then make their own. A cup of wheat flour weighs around 3 ounces, while a cup of almond flour weighs almost 4 ounces. This will make a significant difference in baked goods. The flour is beneficial for adding nutrients to foods.
Almond Meal
Almond meal can be cooked as polenta or grits such as shrimp and grits.
Cookies can be made gluten-free with almond meal.
Almond meal biscuits can be made, but pay attention to the recipe.
Almond meal can be used to bread fish and other fried foods, but it must be taken care of so as not to burn.
Almond meal is not recommended for breads that require true dough with a developed gluten structure, like wheat flour.
More eggs are needed when baking with almond meal to provide the structure gluten in flour creates.
Adapting recipes to substitute almond meal for wheat flour can be a challenge that requires plenty of trial and error.
Sensitivities
Almonds are a tree nut, one of the eight most common food allergies. (Anaphylaxis UK. 2023) While peanuts are not tree nuts, many with peanut allergies can also have an almond allergy.
Making Your Own
It can be made in a blender or food processor.
Care must be taken not to grind it too long, or it will become almond butter, which can also be used.
Add a little at a time and pulse until it is ground into meal.
Store unused flour immediately in the refrigerator or freezer because it will go rancid quickly if left out.
Almonds are shelf-stable, and almond flour is not, so it is recommended that you grind only what is needed for the recipe.
Store Bought
Most health food stores sell almond flour, and more supermarkets are stocking it as it has become a popular gluten-free product. Packaged flour and meal will also go rancid after opening and should be kept in the refrigerator or freezer after opening.
Integrative Medicine
References
USDA FoodData Central. (2019). Almond Flour. Retrieved from https://fdc.nal.usda.gov/fdc-app.html#/food-details/603980/nutrients
Anaphylaxis UK. (2023). Allergy Factsheets (Anaphylaxis UK A brighter future for people with serious allergies, Issue. https://www.anaphylaxis.org.uk/factsheets/
Atkinson, F. S., Brand-Miller, J. C., Foster-Powell, K., Buyken, A. E., & Goletzke, J. (2021). International tables of glycemic index and glycemic load values 2021: a systematic review. The American journal of clinical nutrition, 114(5), 1625–1632. https://doi.org/10.1093/ajcn/nqab233
“For individuals who want to exercise but have fears or concerns, can understanding what they are scared of help ease their minds?”
Overcoming Exercise Fears
One reason for the ongoing weight problem is that individuals don’t move around enough, and one reason individuals don’t exercise is fear (Craig M. Hales et al., 2020). For individuals, physical exertion and moving the body to the point of increased heart rate, heavy breathing, and excessive sweating can cause anxiety and be scary when they haven’t done it in a while or have never worked out. Some anxieties and fears individuals may experience include the following:
Looking Foolish
Anything can happen when exercising. When individuals can’t figure out how a machine works or aren’t sure if they’re doing an exercise correctly, falling off a machine or dropping a weight can cause a feeling of foolishness. Knowing how to use machines and weights takes practice. Ask a gym employee or personal trainer for guidance, as educating individuals on doing exercises correctly and safely is their job. And most individuals working out are happy to help as well.
Experiencing Pain
Some avoid exercise, fearing intense pain. Exercise is not supposed to be painful, but it will cause soreness because individuals use muscles that they haven’t used for a while or at all. For instance, the muscles will experience a slight burning sensation when lifting weights. The body reacts to the workout and adapts to exercise. As the body gets stronger, individuals recognize their body’s response and are able to challenge themselves with heavier weights, longer runs, walks, and workouts. When beginning an exercise program, start slow. Some trainers recommend doing slightly less than an individual thinks they can for the first weeks. This helps to build a habit without the risk of burnout.
Injuries
When starting an exercise program, individuals can feel changes all over their bodies, like everything is pulling and tearing apart. Individuals who haven’t exercised much may be unable to distinguish between the normal discomfort from exercising for the first time and pain from an injury. Shin splints, side stitches, or other common side effects may develop from beginning an exercise program. Individuals may need to stop exercising, treat the injury, and start again.
If there are sharp pains in the joints, tearing in the muscles or ligaments, or anything else that doesn’t feel normal, stop and seek medical attention.
Exercise Mindfulness
The body will feel something while exercising, but separating real injury pain from normal sensations is important.
Be aware of how the body feels throughout the workout.
Follow instructions and pay attention to proper form to minimize the risk of injury.
Proper Footwear
Wearing the right workout shoes is a good idea to avoid and prevent injuries.
Invest in a quality pair of shoes to give the body the support it needs.
Proper Form
If lifting weights, one way to sustain an injury is using incorrect form or posture.
If you are unsure how to do the exercises, consult a trainer or gym employee to explain how the machine works.
Warm Up
Jumping into a workout without warming up can lead to injuries that can lead to chronic pain conditions.
If lifting weights, do a little cardiovascular exercise first or a warm-up set with lighter weights.
Workout Within Fitness Levels
Injuries happen when trying to do too much too soon.
Start with a light program.
Work up to more intense and frequent workouts.
For example, if only able to walk for 10 minutes, start there and increase gradually.
Failure
When it comes to exercise, failure can be experienced in different ways, like losing weight, failing to make it through a workout, being unable to stick to an exercise program, etc. This is part of the process, but individuals can overcome exercise fears through perseverance.
Setting the bar too high can become an excuse to quit.
A simple way to deal with this is to set a reachable goal.
Long-term goals can be set to work toward.
Do what you can handle now.
Individuals take risks whenever they do something out of their comfort zone. However, taking risks may be necessary to overcome exercise fears, keep going, and achieve success.
Weight Loss Techniques
References
Hales CM, C. M., Fryar CD, Ogden CL. (2020). Prevalence of obesity and severe obesity among adults: United States, 2017–2018. NCHS Data Brief, no 360. Hyattsville, MD: National Center for Health Statistics. Retrieved from https://www.cdc.gov/nchs/products/databriefs/db360.htm#Suggested_citation
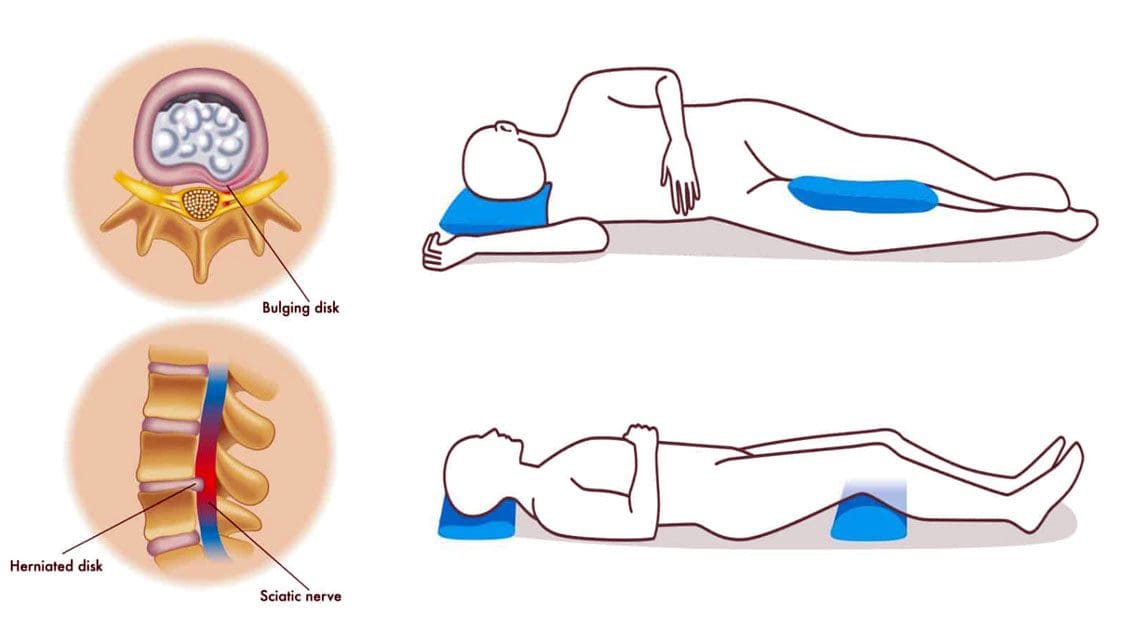
For individuals with back pain, can sleeping with a pillow between or under their knees help bring relief during sleep?
Sleep With A Pillow Between The Legs
Healthcare providers may recommend that individuals with back pain due to pregnancy or conditions like a herniated disc and sciatica sleep with a pillow between their legs. Sleeping with a pillow between the legs may help relieve back and hip pain, as the position helps maintain pelvis and spinal alignment. Proper spinal alignment can help relieve back stress and pain.
The Benefits
Some potential benefits of sleeping with a pillow between the knees.
Reduce Back and Hip Pain
When sleeping on the side, the spine, shoulders, and hips may twist to maintain the position because the center of gravity is elevated, causing instability. (Gustavo Desouzart et al., 2015) Placing a pillow between the knees may help maintain stability and reduce back and hip pain. (Gustavo Desouzart et al., 2015) The pillow neutralizes the position of the pelvis by slightly elevating the leg on top. This decreases the pressure on the lower back and hip joints, which may help reduce pain and allow for improved sleep.
Reduce Sciatica Symptoms
Sciatica nerve pain travels from the lower back down one leg due to a compressed spinal nerve root in the lower back. (American Academy of Orthopaedic Surgeons, 2021) Sleeping with a pillow between the knees may help reduce symptoms and sensations. A pillow between the legs can help prevent twisting the back, rotating the spine, or tilting the pelvis during sleep.
Reduce Herniated Disc Symptoms
A herniated disc can pressure the spinal nerves, leading to pain and numbness. (Penn Medicine. 2024) Sleeping on the side can worsen herniated disc pain; however, placing a pillow between the knees keeps the pelvis in neutral alignment and prevents spinal rotation. Sleeping on the back with a pillow under the knees can also help reduce pressure on the disc. (University of Central Florida. N.D.)
Improve Posture
Maintaining healthy posture while sitting or standing is important to neuromusculoskeletal health and injury prevention. Proper alignment during sleep can help improve posture (Doug Cary et al., 2021). According to one study, individuals spend more than half of their time sleeping in a side-lying posture. (Eivind Schjelderup Skarpsno et al., 2017) Sleeping on the side with the top leg frequently falls forward, bringing the pelvis into a forward tilt that places added pressure on the hips and spine connective tissues. This position disrupts the body’s natural alignment. (Doug Cary et al., 2021) Placing a pillow between the knees improves sleeping posture by lifting the top leg and prevents forward shifting. (University of Rochester Medical Center. 2024)
Increased weight leads to increased pressure on joints.
Significant change in the center of gravity.
Hormonal changes make connective tissues more lax.
Pregnant women with hip or back pain are often recommended to sleep with a pillow between their knees to relieve pain and discomfort. Doctors agree that lying on the left side is the best sleep position during the second and third trimesters. This position ensures optimal blood flow for the mother and baby and helps kidney function. (Standford Medicine, 2024) Placing a pillow between the knees can help reduce the pressure on the joints and also help maintain the left-side lying position. (O’Brien LM, Warland J. 2015) (Standford Medicine, 2024) Larger maternity pillows supporting the abdomen and lower back can provide more comfort.
Consult a healthcare provider about sleeping with a pillow between the knees to see if it is right for you.
What Causes Disc Herniation?
References
Desouzart, G., Matos, R., Melo, F., & Filgueiras, E. (2015). Effects of sleeping position on back pain in physically active seniors: A controlled pilot study. Work (Reading, Mass.), 53(2), 235–240. https://doi.org/10.3233/WOR-152243
American Academy of Orthopaedic Surgeons. (2021). Sciatica. OrthoInfo. https://orthoinfo.aaos.org/en/diseases–conditions/sciatica
Penn Medicine. (2024). Herniated disc disorders. Penn Medicine. https://www.pennmedicine.org/for-patients-and-visitors/patient-information/conditions-treated-a-to-z/herniated-disc-disorders
University of Central Florida. (N.D.). The best sleeping position for lower back pain (and the worst). UFC Health Services. https://ucfhealth.com/our-services/lifestyle-medicine/best-sleeping-position-for-lower-back-pain/
Cary, D., Jacques, A., & Briffa, K. (2021). Examining relationships between sleep posture, waking spinal symptoms and quality of sleep: A cross sectional study. PloS one, 16(11), e0260582. https://doi.org/10.1371/journal.pone.0260582
Skarpsno, E. S., Mork, P. J., Nilsen, T. I. L., & Holtermann, A. (2017). Sleep positions and nocturnal body movements based on free-living accelerometer recordings: association with demographics, lifestyle, and insomnia symptoms. Nature and science of sleep, 9, 267–275. https://doi.org/10.2147/NSS.S145777
University of Rochester Medical Center. (2024). Good sleeping posture helps your back. Health Encyclopedia. https://www.urmc.rochester.edu/encyclopedia/content.aspx?ContentTypeID=1&ContentID=4460
Casagrande, D., Gugala, Z., Clark, S. M., & Lindsey, R. W. (2015). Low Back Pain and Pelvic Girdle Pain in Pregnancy. The Journal of the American Academy of Orthopaedic Surgeons, 23(9), 539–549. https://doi.org/10.5435/JAAOS-D-14-00248
Standford Medicine. (2024). Sleeping positions during pregnancy. Standford Medicine Children’s Health. https://www.stanfordchildrens.org/en/topic/default?id=sleeping-positions-during-pregnancy-85-P01238
O’Brien, L.M., Warland, J. (2015). Maternal sleep position: what do we know where do we go? BMC Pregnancy Childbirth, 15, Article A4 (2015). https://doi.org/doi:10.1186/1471-2393-15-S1-A4
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine