Today local chiropractors will be giving a description of the wheat zoomer. We will be giving a brief description of each panel, its markers, and the basic interpretations of the test. We will also be discussing the considerations for the patients and providers before we take The Wheat Zoomer test.
What is a Wheat Zoomer test?
The Vibrant wheat zoomer has 6 test in one to identify if the patient has wheat and gluten sensitivity. The Vibrant wheat zoomer does give our patients a thorough evaluation and we ask our patients if they started to be gluten-free or was gluten-free, either from birth or not and how much gluten-contained food did they eat. One of the best ways to ensure that our patients may have a gluten sensitivity is that if they have a food diary for us to look over and that way we can determine how severe of the wheat zoomer.
IgA vs IgG
In order for us to know about the wheat zoomer in our patient�s body, we must know about the immunoglobulins. The first one is IgA. IgA immunoglobulins are mucosal and are found primarily in the epithelial lining of the body: intestinal tract, lungs esophagus, blood-brain barrier and around internal organs. They are:
The first line of defense.
More accurate to our gut.
IgG immunoglobulins found in the blood system and are numerous in the body They are considered �systemic� and are non-specific to any one location. Not all IgG antibodies are sensitive though, some of them can indicate that an antigen has �leaked� into the blood and the immune system tagged that antigen as a �non-self�. And they are not diagnostic as IgG+IgA, but if IgA is absent, the antibodies are more relevant.
If the patient is recently gluten-free, the antibodies will tell us that the antigen hasn�t cleared out in the patient�s system from past weeks of eating gluten.
Celiac
Celiac is a growing autoimmune disease, about 1% of the population is affective and 1 in 7 Americans have a reaction to wheat or wheat gluten disorder. The Vibrant test can determine a 99% sensitivity and 100% specify on the celiac antibodies.
Total IgA and Total IgG measure both the IgA and IgG to determine the patient�s reactivity to gluten
Cut off for IgA is 160 as well as a bottom 1/3rd
Not all traditional markers for celiac disease doesn�t need to be elevated if tTg2 is elevated.
Intestinal Permeability
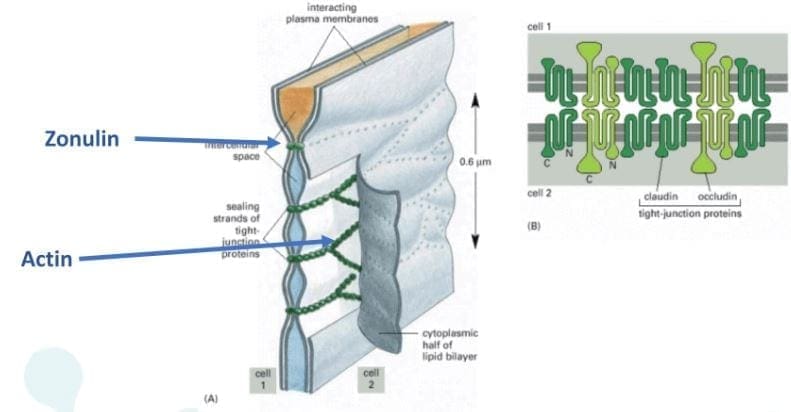
Zonulin is the gatekeeper for the intestines and controls nutrient flows and molecules across the membrane. It is a protein complex inside the intestinal tight junctions and can be increased by either gluten and high-fat meals.
Anti-Actin, especially f-Actin is in the smooth muscle of the intestines. Actin is part of the actomyosin complex. Vibrant can isolate f-Actin to get a more accurate picture of the patient�s immune response to the intestines. While antibodies in actin can identify intestinal destruction and indicate autoimmune diseases like connective tissue disease and autoimmune hepatitis.
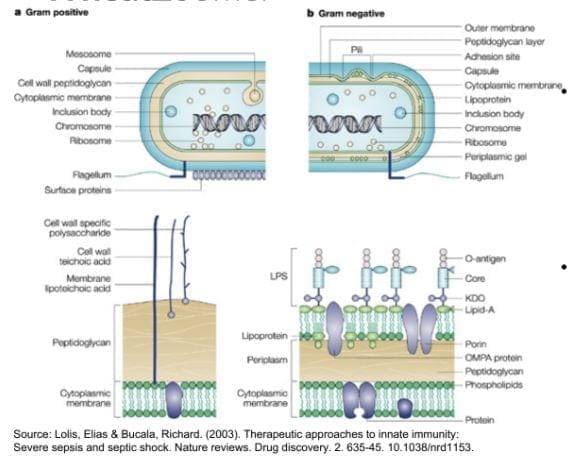
Lipopolysaccharide (LPS) is produced by gram-negative enterobacteria. It is very potent and can cause inflammation. Plus it�s one of the indications of a leaky gut. Practitioners can draw additional lab test for cardiovascular, inflammatory markers, and diabetes/insulin resistance.
Here at Injury Medical Clinic, we suggest to our patients to try a Vibrant GutZoomer to identify the source of their ailments before we add the Vibrant WheatZoomer.
Gluten-mediated Autoimmunity
Fusion Peptide is the new addition to Wheat Zoomer in 2017. It is cross-linked to tTg and can identified celiac progression from 14 months to 4 years.
Differential Transglutaminases can detect autoimmune reactions to gluten that are not celiac or are becoming celiac. However, gluten is still a trigger but react differently in the celiac autoimmune disease such as:
Transglutaminase 3= skin manifestations of autoimmunity like dermatitis herpetiformis, eczema, and psoriasis.
Transglutaminases 6= neurological manifestations of autoimmunity in the cerebellum like gluten ataxia, gate abnormalities, balance and coordination issues.
Wheat Germ Agglutinin
Wheat Germ Agglutinin is the lectin component of wheat but, it is not a component to gluten. Dr. Jimenez can detect a patient’s low level of Vitamin D absorption from the patient�s results. And Wheat Germ Agglutinin is commonly used as an additive in supplements and the supplement can still be called gluten-free due to the different protein structure.
Gliadin, Glutenin, and Prodynorphin
Gliadin and glutenin are what makes up the super protein in gluten. Most people are reacting to the Gliadin portion of gluten and gliadin binds with tTg2 in celiac and binds zonulin to a leaky gut in patients. Gliadin reacts to any antigens can indicate a sensitivity to gluten in patients and gluteomorphin are peptides in wheat and react as a euphoria receptor to the brain. Prodynorphins antibodies can indicate that gluten reacts to signaling hormones and affect the patient’s mood.
Sadly though, patients do have a hard time withdrawing gluten in their diet since their antibodies are used to the compound and it up to us, here at Injury Medical Clinic to gently push our patients to have the will power to fix what is causing them to have ailments.
Wheat Allergin
Wheat Allergen is the true allergen body. Some patients that already know that they are allergic to wheat from a young age but it doesn�t decrease when wheat is eliminated and can remain long term after the allergic response happens.
Glutenin
Glutenin is the other part of the gluten compound. However it is less common to some people, but some individuals do show reactivity to glutenin, thus still have a gluten sensitivity. But there is no clinical difference to the reactivity to glutenin from high to low molecular weight.
Non-Gluten Wheat Proteins
Surprisingly Vibrant has an advantage to their test as they have a panel for patients that don�t have a gluten sensitivity but a wheat sensitivity. The Vibrant advantage to the unique non-gluten wheat panel shows us that:
Proteins in wheat unrelated to gluten but relevant to immune reactions.
It is 30% of the protein molecular weight of wheat.
Some individuals are more reactive to wheat proteins than gluten itself.
If they are trying to be gluten-free, patients still have to read the labels to see if any hidden wheat starches are in the ingredients. But not all food products are gluten-free if they have the wheat protein in them.
Conclusion
If the patient is trying to be gluten-free but previously ate gluten compound food. They can still feel the reaction if they discovered that they have a sensitivity to gluten by their practitioner. And must take precautions when they are reading the labels of the products they are going to buy and consume. In the next four articles, we will discuss what the Wheat Zoomer can provide as well as, discussing about what causes leaky gut, what actually goes on in our patient�s intestines, and wrapping up on what to do after the Wheat Zoomer heals and restores the gut barrier.
Ever wonder what goes through your chiropractors head when treating your moderate back pain? Using a patient as an example, Dr. Jimenez shares his thought process through the treatment of a patient with moderate low back pain. All the way through the first appointment through to the recovery process.
Patient’s Background
Louis is a 47-year-old programmer who plays tennis regularly, especially tournaments.
However, low back pain has put Louis’ game on hold as he�s not able to manage the pain with the regular heating pad, ice, and over-the-counter pain reliever.
His primary physician referred him to Dr. Jimenez.
Louis’ is referred to chiropractic
Dr. Jimenez: Louis’ primary physician referred him to me instead of a spine surgeon because first, the pain is not yet serious enough for surgery. And so there was a window to treat with a non-invasive approach. Secondly, I specialize in sports medicine and so maximize conservative, non-operative techniques/methods.
The United States has 5 times the surgical rate of other countries, so going to a non-operative spine specialist/chiropractor is the best approach at the beginning before the pain becomes severe/acute/chronic.
Louis’ first appointment, medical history, and current back pain
Dr. Jimenez: Once I went through his medical history, I saw it was pretty straightforward. So I dug deeper into other areas of Louis’ lifestyle.
I asked about:
Diet
Physical activity
Emotional well-being
Smoking status
Also, a factor, his occupation was contributing to his pain. He�s a programmer, so spends a lot of time sitting at a desk. Sitting for prolonged periods and usually improperly/poor posture are two of the worst things you can do to your spine.
Sitting for a long time without moving around causes the hip muscles to get tight, and glutes and spine muscles to weaken.
Louis sits most of the day working and spends the weekend if not doing house chores, then playing tennis. Just imagine using weakened muscles during the week and then jumping into a sports activity on the weekend will definitely cause pain.
Louis said that his pain would worsen when serving, hitting a forehand and bending over to pick up a ball. The pain would ease down once he was resting and sleeping.
Louis’ physical exam
Dr. Jimenez: With the physical examination, I looked at
Alignment
Motion
Inflexibilities (not just the spine but the hips and lower extremities)
Muscular imbalances
Weaknesses
I saw that Louis had a flattened lumbar lordosis, meaning the gentle curve in his low back was now flat. Restricted motion in one direction� or a flexion. And weakness in the buttock muscles and hips, and tightness in the lower extremity muscles.
Pushing on certain areas along his spine, presented tenderness in the mid to lower lumbar spine and joint areas.
Initial treatment for Louis’ moderate low back pain
Chiropractic
Physical therapy
Exercises
Stretching
Re-education – proper sitting/standing
Diet
Foot orthotics if necessary
The best initial treatment is to work chiropractically on the muscular imbalances of the spine and lower extremities that are affecting the body’s biomechanics.
Other exams?
Dr. Jimenez: If necessary, a functional movement screening examination.
This test is used in sports medicine to check for imbalances from the feet all the way up to the neck.
After this, Louis would be tested to see if foot orthotics could help and receive specially designed exercises from a physical therapist to address the muscular imbalances.
Radiographic, CT, or MRI imaging
Dr. Jimenez: Many believe that imaging tests are essential to the diagnostic process.
My goal for Louis and all my patients is to get them pain-free, functional and back to health.
Are imaging tests important?
Dr. Jimenez: Imaging tests are important when there are neurologic discoveries/complaints, like muscle weakness, sensory loss, and immobility, as this can indicate the need for surgery.
Imaging tests are helpful for guiding targeted treatment like an epidural injection.
And if your doctor believes there is something serious, e.g., a spinal tumor, infection, then get an imaging test right away.
Louis’ diagnosis
Dr. Jimenez: Because Louis’ pain worsened while playing tennis and then ease during sleep, I diagnosed him with mechanical low back pain.
This type of back pain comes on through mechanical activities or applying a load to the spine.
Non-mechanical low back pain is pain that exists all the time.
Thought process while developing Louis’ treatment plan
Dr. Jimenez: The treatment plan is focused on controlling pain and inflammation.
I first recommended chiropractic treatment, physical therapy/massage, and heat/ice compress.
After completing the course of treatment I suggested Louis take naturally derived supplements:
Turmeric
Bromelain
High-dose omega 3’s
This would help reduce inflammation.
They have been proven to be effective without the serious side effects of both over-the-counter and prescription medications.
Louis and I also discussed his diet
I recommended cutting back on carbohydrate and processed sugar intake thus curbing inflammation and upped healthy fat consumption of and natural sugars that are found in nuts and berries.
I taught Louis proper basic movement techniques, including positioning himself at work and stretches to do throughout the day.
I suggested that Louis work with a fitness physical therapist to build strength and flexibility, that would take shape in 4 to 6 weeks.
After a few sessions, the goal is to be able to do the exercises without help.
Return to tennis
Dr. Jimenez: Very soon, as long as, he uses his natural anti-inflammatory supplements and follows through with regular chiropractic/physical therapy.
Slow and steady is the key to pain relief. Jumping into a tennis set before finishing treatment would set him back and possibly cause new injuries.
I recommended he start by playing non-competitive tennis and just rally after completing the treatment and then take a day or 2 to see how it feels.
Taking it slow should bring back full strength within 2 months after the initial visit.
Preventive tips:
A proper tennis swing should put minimal force on the spine.
Tennis professionals start and stop, jump, slide, dive and run, run, run. That is where a significant overload of the lower back occurs and all the energy goes right into the spine.
The key to a proper swing is to rotate the hips, take the proper arm swing, and hit through the ball.
If you don�t have proper hip rotation, your body will pay for it through the spine.
Bending at the hips and knees when picking up balls will greatly reduce stress on your low back.
Work with a tennis pro that can teach you proper swing and specific tennis training especially movement.
This will help you play well, alleviate/avoid back pain and enjoy the game.
Low Back Pain Treatment | El Paso, Tx
Low back pain which gradually influenced his quality of life was developed. David Garcia was unable to walk as his symptoms worsened and his back pain became excruciating. He first visited Dr. Alex Jimenez, a chiropractor in El Paso, TX, following a recommendation from his sister. Dr. Jimenez managed to supply David Garcia with all the aid he deserved for his low back pain, restoring his well-being. David Garcia clarifies the wonderful service Dr. Alex Jimenez and his team have given him to offer him relief from his painful symptoms and he highly recommends chiropractic care as the non-surgical pick for low back pain, among other health problems.
NCBI Resources
A chiropractor is the ideal medical professional to consult with for any unexplained pain in the musculoskeletal system. They are highly qualified professionals that their specialty is treating conditions like moderate lower back pain and they are very affordable. 31 million Americans experience moderate low back pain at any given time. This condition affects many, but finding the exact cause can be a challenge. Chiropractors are spinal specialists that are trained to not only alleviate pain but also find and help correct the cause of the problem.
The human brain comprises approximately billions of small cells that utilize electrical impulses and chemical signals to communicate with one another and other parts of the human body. These are known as neurons. When neurons stop functioning properly, it can cause various brain disorders, such as Alzheimer’s disease, epilepsy, and even depression.
Researchers developed several treatment methods and techniques of brain stimulation which allow them to control neural activity to understand better and regulate these type of health issues. In conventional treatment methods and techniques of deep brain stimulation, electrical neurostimulators, also known as brain pacemakers, are surgically implanted in the brain.
Researchers also developed non-invasive treatment approaches to stimulate cells found deep within the brain. While several researchers utilize magnetic pulses or sound waves to stimulate neurons, researchers in optogenetics utilize light therapy. Shuo Chen, Ph.D., winner of Science and PINS Prize for Neuromodulation, was recognized for his work in this area.
Dr. Chen demonstrated that near-infrared light, when utilized with certain nanoparticles, allowed the stimulation of neurons deep within the brain, stated Dr. Karl Deisseroth, professor of bioengineering, psychiatry, and behavioral sciences at Stanford University. More research studies are needed to make this a useful process, he said, but Dr. Chen took a key step.
Developing Light-Sensitive Neurons
Dr. Karl Deisseroth, one of the leading pioneers of optogenetics, developed a treatment method or technique in which the brain cells or neurons are genetically engineered to respond to light therapy. Through this method or technique of brain stimulation, researchers transmit fragments of genetic codes from algae and other microbes into the brain cells of mice and other animals. That genetic code ultimately causes neurons to produce light-responsive proteins known as opsins.
When opsin-producing neurons are exposed to specific wavelengths of visible-spectrum light, those brain cells turn on or off. By activating or suppressing the neurons, researchers can learn more about the fundamental role of neurons in brain function and brain disorders. Dr. Karl Deisseroth has also demonstrated the effects of developing light-sensitive neurons.
By developing light-sensitive brain cells, the causal role of cellular activity can be determined in the tissue and the behavior of interest of any species, ranging from memory to mood, stated Dr. Deisseroth. Furthermore, optogenetics brings the unmatched capability for speaking the brain’s natural language regarding cell-type specificity and speed, he added.
Developing Non-Invasive Treatment Approaches
Opsin-producing neurons, however, respond to visible-spectrum light which cant penetrate brain tissue. Therefore, optogenetic stimulation required the insertion of fiber-optic light sources inside the brain to stimulate neurons. Dr. Deisseroth and his colleague Polina Anikeeva, Ph.D., developed the utilization of near-infrared (NIR) light, a non-invasive type of light therapy.
NIR light can ultimately penetrate through the skull and brain tissue without inserting internal light sources inside the brain. However, NIR light also doesn’t trigger a response from opsin-producing neurons. To promote the tissue-penetrating abilities of NIR light therapy, Dr. Karl Deisseroth and Dr. Anikeeva developed a treatment approach known as NIR upconversion, which coats opsin-producing neurons in nanoparticles to convert NIR light into visible-spectrum light.
Dr. Shuo Chen utilized this treatment method and technique, demonstrating for the first time that NIR upconversion optogenetics can ultimately be utilized to control neurons deep in the brains of mice. In addition, Dr. Chen’s research studies utilized this method and technique to stimulate the release of dopamine in a region of the brain believed to play a role in depression.
Overcoming the challenge of optical penetration depth will be the fundamental key to realizing non-invasive remote optogenetics with high clinical translation potential, wrote Dr. Chen in his prizewinning essay on the topic. Our research study utilized a nanomaterial-assisted approach that shifts the existing optogenetic tools into the near-infrared region.
Brain Stimulation for the Human Brain
While researchers continue to research optogenetics in mice and other animals, it hasn’t been utilized to treat brain disorders in humans. Furthermore, more research studies are required to develop and evaluate non-invasive methods of light therapy and non-invasive methods and techniques for transmitting genetic code into brain cells or neurons.
It is too soon to predict which treatment approach will emerge at the forefront of next-generation non-invasive brain stimulation technology, Dr. Chen said in a press release issued by the American Association for the Advancement of Science. However, we believe that a variety of fundamental achievements, such as NIR upconversion optogenetics, are quickly unlocking development pathways and paving the way towards a bright therapeutic future for brain diseases, he continued.
In the meantime, other methods and techniques of non-invasive brain stimulation are also being developed, evaluated, and utilized in humans. For example, transcranial magnetic stimulation (TMS) is a non-invasive treatment approach that utilized magnetic fields to stimulate nerve cells in the brain. The Food & Drug Administration (FDA) has already allowed TMS marketing as a treatment approach for major depression as well as obsessive-compulsive disorder and migraine headaches.
There are also several non-invasive methods and techniques which don’t require the utilization of gene therapies, such as transcranial magnetic and electrical stimulation, which are commonly utilized with human subjects on an experimental, regular basis, stated Ed Boyden, Ph.D., a professor of neurotechnology at the Massachusetts Institute of Technology (MIT).
Members of Boyden”s research study group have also conducted research studies on transcranial electric stimulation (TES), a non-invasive treatment approach to brain stimulation in which electrodes are placed on the scalp. Researchers hope for this method and technique to reach neurons or cells deep within brain tissue with greater precision than TMS.
Although research studies have demonstrated that light therapy can stimulate brain cells or neurons of mice and other animals, urther research studies are required to determine how light therapy treatment methods and techniques can stimulate the human brain. According to these same research studies, light therapy can alter neurons or brain cells which can ultimately cause Alzheimers disease, epilepsy, and other brain diseases. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
The human brain consists of billions of small cells or neurons which communicate with one another and other parts of the human body. When neurons stop functioning properly, it can cause a variety of brain disorders. Researchers have developed a variety of light therapy treatment approaches to help stimulate the brain ultimately. The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues and functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900
Curated by Dr. Alex Jimenez
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals; however, chronic pain is different from the average pain type. The human body will continue sending pain signals to the brain with chronic pain, regardless of the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility, reducing flexibility, strength, and endurance.
Neural Zoomer Plus for Neurological Disease
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual’s reactivity to 48 neurological antigens with connections to various neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention.
Mostly everyone in the world has a gluten allergy or gluten sensitivity when they consume food. When it comes to food that has the gluten compound, most people read the labels on the products that contain it and have cut the compound out of their diets completely. However, did you know that different foods and products have hidden gluten in them? Even though now and days we read labels from products, as well as, cutting off the source of the problem that is making us ill. Hidden additives like gluten, even in small amounts, can cause problems to those that are allergic or sensitive to the compound. Especially when it comes to the product itself, some regulations may or may not be required to label products that contain gluten.
What is Gluten?
Gluten is the main protein that is found in many grains such as wheat, rye, and barley. It is formed by two proteins which are glutenin and gliadin. And the word �gluten� is Latin for �glue� and when mixed with water, it rises and stretches. Most gluten can be found in some bread, pasta, cereal, and beer.
But in this article, we are going to inform you 8 products that have hidden gluten. Because here at Injury Medical Clinic, we take the time to talk with our patients on what ails their bodies and work on discovering what kind of food allergen or food sensitivity they may have. As well as, finding alternatives to prevent inflammation in their bodies.
8 Products with Hidden Gluten
Medications: Yes, you�ve read that correctly, there is gluten in medication. Surprisingly though, a lot of prescription medicine contains excipients (containing gluten) that actually binds the pills together. This is mostly found in generic over the counter medications but the labeling for the ingredients are not always there.
However, labeling standards are changing due to the Gluten in Medicine Disclosure Act of 2019. This was proposed on April 3, 2019, and introduced by Representatives Tim Ryan (D-OH) and Tom Cole (R-OK). The bill�s intent was to make it easier to identify gluten in prescription medicine and it is telling drug manufacturers that it is required to label medications with the list of their ingredients, their sources and whether the gluten compound is present.
Hopefully with enough signatures and votes that the bill will be passed, however, if you are taking medication and the labels look different; always verify with a pharmacist to see if it is correct. Plus, you can always talk with your pharmacist to confirm that your medicine is gluten-free, so that way you won�t get a bad reaction from it.
Sauces and gravy: Everybody loves any sauces and gravies in the meals they prepared and are excellent in mash potatoes and Thanksgiving dinners. But sauces like soy or teriyaki do contain wheat protein, hydrolyzed wheat starch or wheat flour. While others sometimes contain soy sauce or malt vinegar.
In any recipe that contains a type of sauce for the food you are preparing, especially in creamy sauces and gravies, mostly requires a roux; which is wheat flour mixed with butter. So, whenever you are at your favorite restaurant or have a favorite meal to prepare, get familiar with the sauces, so that way you can know that if they are gluten-free or not.
Starches: When we think of starches, our minds go to the potatoes. However, wheat can also be found in starches and starch derivatives. So, whenever you are looking at products that are starchy, look at the ingredient labels and for terms like �wheat starch�, �hydrolyzed wheat starch�, or �contains wheat.�
In order for starches that contain wheat starch to be gluten-free, the wheat compound must remove to less than 20 ppm. And especially in FDA regulated food labels, if the product says �contain wheat�, it is not safe. But food labels don�t apply to barley, rye, or oats, still continue to read the ingredient labels in the case for the wheat compound and if it is not there then the product is safe. For gluten-free starches for those who don�t want to miss out, tapioca starch, rice starch, and potato starch are perfect for frying.
Brown Rice Syrup: This type of sweetener is made from fermented brown rice with enzymes or from barley, which breaks down the starch and transforms it into sugar. Sadly though, this sweetener is not gluten-free and it can be used on its own or be used as an ingredient in a multi-ingredient product. Some companies use brown rice syrup in their products by listing it as �barley� or �barley malt.� And it is a bit problematic for those who have a gluten allergen to this sweetener.
Soups: Who doesn�t love soups. Soup is there for us when we are sick and for comfort when it gets really cold in the fall and winter seasons. But companies use wheat flour or wheat starch as a thickener for those creamier soups that we love in a can and those thickeners can be hidden in the ingredients label. So, if you want pre-packaged soup bases and canned soups for those colder seasons, be sure to read the labels carefully, especially for those creamed-based soup bases and bouillons because they might contain gluten.
Salad dressings: Did you know that many standard salad dressings can wheat flour, soy, or malt vinegar? Not only that but it can contain wheat or gluten-containing additives as a thickener. Plus salad dressings often have artificial colors, flavorings and many other additives that can contain gluten as a sub ingredient. However, if you want to be safe and not have gluten in your salad dressings, simply put in olive oil, lemon, salt, and pepper, and you got yourself a gluten-free salad dressing.
Chips and fries: Chips and fries are the staples for a good burger or hot dog on every barbeque events and parties. Yes, the potato that makes the chips and fries are gluten-free; but the seasonings like malt vinegar and wheat starch do contain gluten. And when we are frying cut potatoes into French fries and chips; the oil that is used to make them can be cross-contaminated with gluten-containing fried foods.
Processed meats: Meat is most likely to be the last place you think that has gluten. However, processed hamburger patties, meatballs, meatloaf, sausages, and deli meats contain gluten. Wheat-based fillers are used to either improve the texture of the meat or bind the meat together. Plus, seasoned or marinated eats can sometimes contain hydrolyzed wheat protein or soy sauce with breadcrumbs are added to bulk up the product.
Conclusion
So if you are at the grocery store getting some food for dinner or meal prepping, it is important to actually read the labeling of the products that you are buying. Whether you have a food allergy or food sensitivity to gluten or any food products, we here at Injury Medical Clinic, listen to what is causing our patients pain to their bodies and offer solutions to fix whatever ailments that the problem is causing.
Sleep and weight are like a double edge sword. Less sleep will cause you to gain weight and gaining weight will cause you to sleep less. Since everyone wants to get a better night sleep, we need to cut those tight bonds so that our overall health and mental state to improve.
Less Sleep= More Weight
With our busy fast-paced lives, we tend to take on more commitments than we want. As well as, being stressed all the time. This lifestyle is not good for our bodies when we want to have a better lifestyle. In our previous article, lack of sleep can lead to chronic illness and loss of productivity. Not even that, Japan hold the number one spot of less sleep with 5 hours and less; while the U.S. holds the number two spot with 6 hours and less.
So, when we don�t get enough sleep due to causative factors, two major hormones in our body are affected and not in a good way either. It is our pituitary glands and our hormonal cortisol that get affected when we don�t get the recommended seven to eight hours of sleep. Our pituitary glands are the master controller to all our hormones and are sensitive when we don�t get enough sleep. When we actually get the recommended seven to eight hours of sleep, our pituitary glands release our growth and thyroid hormones as well as suppressing the stress hormone cortisol.
But in today�s society, according to the National Sleep Foundation, the average American sleeps only about seven hours per night-while other sleep five to six hours per night on a regular basis. With these studies, our body will be more or less in a constant state of partial sleep deprivation. Or if you have an anxious mind or have mental health issues, partial sleep deprivation can lead to chronic sleep deprivation. Chronic sleep deprivation can lead to elevated cortisol in the evening, a crucial time for the levels should be diminishing.
Cortisol Levels
When our cortisol levels get too high, we can develop insulin resistance, thus leading to weight gain and the high risk for type 2 diabetes. Chronic sleep deprivation can also change your growth hormone release. Instead of sending out one large pulse of growth hormones as soon as our heads hit the pillow, our bodies send out two small pulses, one before we go to bed and one after, thus leading us to have sleep deprivation. The one large pulse is responsible for the exposure of our tissues and reducing our glucose tolerance.
When we don�t get enough sleep throughout the day, the fat cells can�t handle the insulin in our bodies and will drop as much as 30 percent. When our cells resist insulin in our bodies, our blood sugar goes up and the excess sugar we produce is stored in our bodies as fat. This is dangerous to our health because not only we will gain the weight, but we will be at the risk for type 2 diabetes, high blood pressure, heart disease, and cancer. According to the CDC, 11.1 percent, adults who snooze less than 7 hours per night have type 2 diabetes, while 8.6 percent of adults who snooze more than 7 hours per night may already have the disease.
Late Night Munchies
One study stated that, people who snooze less tend to be heavier than people who sleep the recommended amount. The study looked at the younger age group and discovered that short sleep duration appears independently associated with weight gain. And the CDC also stated, 33 percent of adults who snooze less than 7 hours are obese, while 26.5 percent of adults who sleep more than 7 hours are obese as well. But the question still remains, why do we gain more weight when we snooze less?
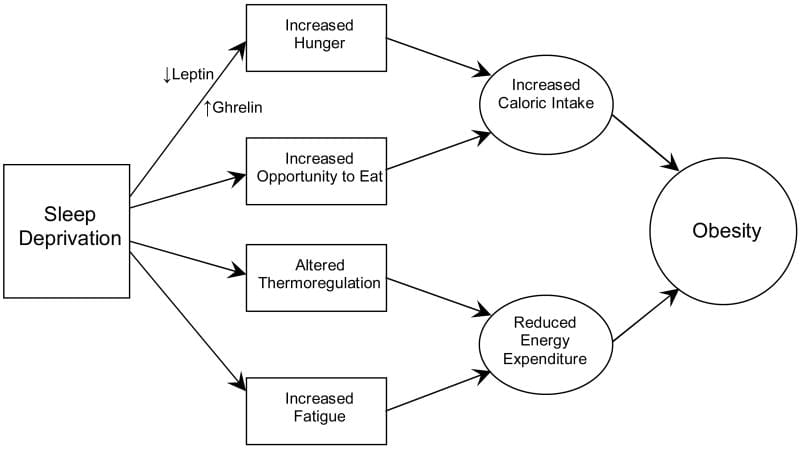
The answer is that our hormones are the ones that get affected the most when we don�t get enough sleep. Hence why we get the late-night munchies. When we are supposed to get our full 8 hours of sleep, our bodies release hormone leptin, which regulates how satiated we feel, and releases hormone ghrelin, which stimulates our appetite. So, when our hormone leptins go down and ghrelins go up, our minds think that we are very hungry and that we need to get up to satisfy that hunger with carbohydrates, thus making us loose those few extra minutes of sleep. So, it�s not your willpower that is making you wake up to eat at around 2 a.m., it is your lack of sleep that is causing the imbalance in your body.
More Weight= Less Sleep
Like we stated in the beginning, sleep and weight are like a double edge sword. Being overweight or obese can keep you from getting enough sleep as well. There are some weight-related issues like, sleep apnea, COPD (chronic obstructive pulmonary disease) and arthritis that can be an issue from getting those recommended snoozes.
Sleep apnea is very common for obese or overweight adults. When we have sleep apnea, our airways collapse or is blocked when we snooze. Our breathing gets very shallow or even stop while you sleep and can last for a few seconds to a couple of minutes or even longer.
We do wake up with a choking noise or snort then we go back to sleep, but when it�s the day time we are at risk for daytime sleepiness. Sleep apnea can be treated with breathing devices but major lifestyle changes can help you lose this medical condition.
When you are suffering from COPD, you will notice a shortness of breath and have more trouble sleeping. People with COPD may be overweight or obese can actually exercise to combat this condition. However, you must consult with your doctor if you want to change your lifestyle and fix this condition.
Painful, arthritic joints can keep you up at night. Granted that there are anti-inflammatory and pain medication that may help you sleep; but if you are overweight or obese taking those medications, they will add on more problems like digestive discomforts or a dependence.
Conclusion
Here at Injury Medical Clinic, we do consult with our patients about the importance of exercising and eating healthy to assist whatever ailments they may have. Whether it is stress or medical conditions, we strive to make our patients feel good.
In conclusion, sleep is highly important and should be on the top of the list for a better lifestyle as well as placing weight in second. Granted with our busy work schedules, and fast-pace lifestyles, we ignore sleep and we gain the weight. If you have any sleep conditions like COPD or sleep apnea, please seek professional help to get it under control. But if you change your lifestyle a little bit by eating right, focusing on mental health, exercising, and sleeping at the appropriate times; not only your mood changes but your body will heal tremendously and you will feel like you can conquer the world.
The Most Effective Chiropractor | El Paso, Tx (2019)
Neck pain and back pain are common symptoms which can develop because of sports accidents, automobile crash injuries, and a variety of other wellness issues. Painful symptoms can ultimately impact an individual’s daily physical activities, tremendously affecting their well-being. Patients clarify their neck pain and spine pain symptoms improved after they visited Dr. Alex Jimenez. Chiropractic care focuses on the diagnosis, therapy, and prevention of a variety of injuries and/or aggravated conditions associated with the musculoskeletal and nervous system. Patients highly recommend Dr. Alex Jimenez and his team as the non-surgical alternative for neck pain and spine pain related to sports injuries, auto accident injuries, and other health problems towards pain relief.
NCBI Resources
Chiropractic can help you sleep. In fact, one-third of people who undergo chiropractic adjustment report sleeping better immediately, according to the�National Sleep Foundation. The benefits are not just for adults � 40 percent of infants slept better after just one chiropractic session. That is good news, considering one-fourth of babies experience sleep problems and when babies don�t sleep, nobody else in the house sleeps either!
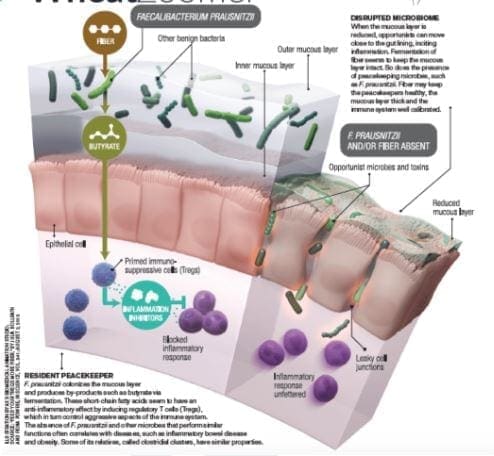
The microbiome is a crucial part of the body and how effectively it functions.� The microbiome plays a significant role in the immune system, the digestion of food, how the body metabolizes drugs, detoxification, vitamin production, as well as protection from foreign innovators. However, just like many other parts of the human body, it is greatly influenced by stress, environmental factors, and sleep which can ultimately impact intestinal permeability.
Ideally, the best functioning microbiome is diversified. The more diversity a microbiome has, the more stable and resilient to antibiotics it becomes. In addition to this, a diversified microbiome also has stronger pathogen resistance.
The microbiome is filled with many different bacteria strains that all play essential roles in keeping the gut healthy and controlling intestinal permeability.
Bacillus is a spore-forming bacteria whose major role is the production of B and K2 vitamins in the gut.
Clostridia compromise about 10-50% of the microbiome and are anaerobes that are not found in probiotics. These thrive on high fiber and polyphenols.
Akkermansia makes up 1-3% of the microbiome and helps to reduce inflammation and protect against inflammatory bowel disease.
Lipopolysaccharides are bound on gram negatives residing in the gut and protecting the bacteria from bile salts. (Lipopolysaccharides are normal in the gut, but they are not normal in the bloodstream)
The main reason it is important to have a diversified and healthy gut is to avoid problems with intestinal permeability or “leaky gut syndrome”.� A leaky gut refers to how easily substances that are not fully digested pass through the intestinal wall. This occurs when the tight junctions of the walls become loose, allowing the gut to be more permeable.� This is how bacteria and toxins pass from the gut into the bloodstream, causing inflammation and other autoimmune diseases.
Keys to a healthy gut:
Eat more organic fruits, vegetables, and fermented food
Try to limit the amount of food that is boiled as boiled foods contain fewer polyphenols
�Supplements such as Vitamin D, Vitamin C and Omega 3’s
Detox: sauna, yoga, meditation, and regular exercise
Prebiotics and Probiotics
It is important to remember that the best thing for a healthy gut is diet. Suppliments and pills can help, but in the long run, a diet is the most important and influenctial factor to the gut. A gut healthy diet will aslo help to maximize liver detoxifaction. If you do not know where to begin, I recommend getting a gut zoomer blood test and consulting with a doctor about what probiotics and diet are best for you. – Kenna Vaughn, Health Coach�
Now and days, mostly everyone has a gluten sensitivity or a gluten allergen in their bodies. This could happen to anyone whenever they are eating gluten-contained food or products and suddenly feel unwell or their gut acts differently throughout the day. Or they actually get tested by their physicians and realizes that they have celiac disease. In the last article and the previous one after that, we talked about the 8 products that have hidden gluten in them; as well as the introduction of the wheat zoomer we use for our patients.
Here at Injury Medical Clinic, Dr. Alexander Jimenez consults with our patients about certain zoomers that can actually aid the patient�s body. In this article, we review the factors that affect test results such as medication and fasting after taking the Wheat Zoomer, as well as, focusing heavily on the mechanism of the intestinal permeability, the structure and function of the epithelium. We also focus about important immunomodulatory metabolites, epithelial cell types and the roles in the epithelial barrier.
Intestinal Permeability
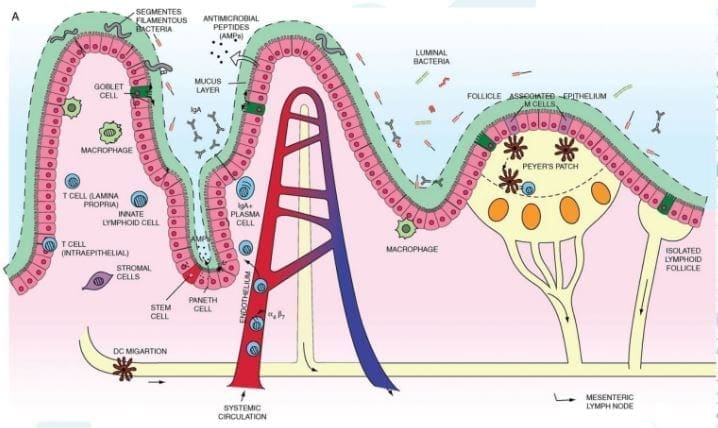
Let�s start with the mechanisms of intestinal permeability. The main purpose of the intestinal epithelium is to keep the good things in and the bad things out. While the system is complex and ever changing, it still sends out a message to the host and maintain balance both physical and biochemical as a protective barrier.� There is an abundance of antigen sampling to regulates the flow of nutrients in the host�s body, as well as, keeping an eye on the body by the mucosal immune system. Not only that, if you have an injury or an acute inflammation, the intestinal epithelium will support tissue repair by coordinating with microbiota.
Another thing that the epithelium does is that it responds to the microbial signals that will make our bodies tolerate any continuous exposure to commensal bacteria. But we do want to keep the good bacteria in our bodies but get rid of the bad bacteria, so our bodies feel good. The intestinal epithelium also convey microbial signals to the mucosal immune cells, while promoting a coordinating immune response to battle against commensal bacteria and the enteric pathogens, since these two microsomes should not be in places they are not allowed in.
While the epithelium is battling with the bad bacteria in our system, it also regulates the B and T cell response to either, control inflammation, squash inflammation, or cause inflammation on the intestinal barrier, depending on the situation. Plus the epithelium locally regulates the immune response at the intestinal barrier by influencing innate and adaptive immune responses to the body�s intestines.
However, if there is something disrupting the intestines, like chronic inflammation or leaky gut; the epithelium barrier can be compromised. In order for us to fix a leaky gut, we must learn what is causing the inflammation in the first place. The epithelium is home to many microbes, immune cells and can determined if we need the immune response on any harsh exposure. If we can learn more about these mechanisms, then we can calm down the inflammation by resetting it back to its calm, natural state.
But the immune cells in our intestinal epithelium can also cause disruption on our gut by leaking out of the protective barriers and attacking the pathogens anywhere in our system. So epithelial permeability can not only cause inflammation but prevent it in our intestines, which is both good and bad depending on the situation.
Dr. Alexander Jimenez consults with our patients with natural alternatives of healing inflammation in their gastral intestines.� If he can find the sources of what causes the inflammations in your gut, then he can work with aiding them with functional medicines while informing you what they can do to heal your gut.
Now let�s looks at the intestines and the many microsomes that they contain. Here are some microsomes we will be discussing as well as what is their key roles in the intestines; so we can figure out how to prevent a leaky gut.
�
The Mucosa
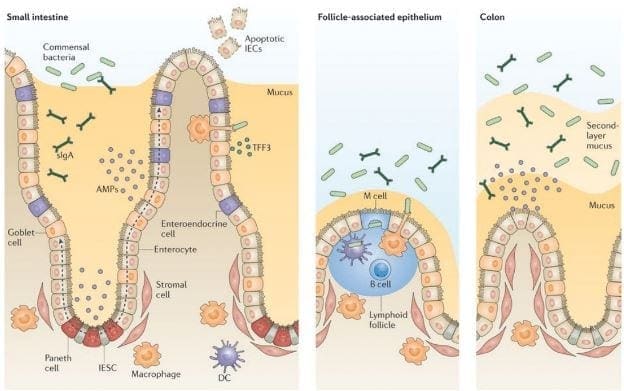
This is in both the small intestines and the large intestines and are completely different. The small intestines has one mucus layer and has limited microbes inside it�s mucosa, while the large intestines has an attached inner mucosa and a loose outer mucosa. The mucosa plays an important role in the intestines because it can tell �Friend� from �Foe� in the immune system.
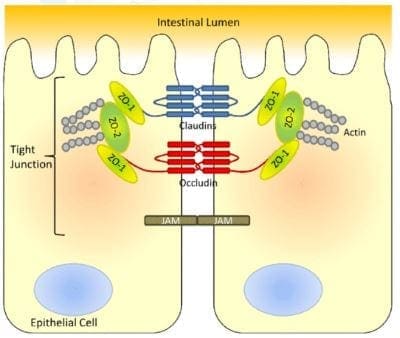
Important Tight Junction Proteins
The tight junction is an important function in the intestinal epithelium as it is one of the barriers that separates what comes in and what comes out in our gut.
Actin: Are the structure and functions of tight junctions. But they constantly disassemble and reassemble actin filaments if they are anti-Actins. It is controlling the tight junctions cells as it acts like a contractable belt by pulling or contracting the junctions in the intestinal cells.
Zonulin: They are the �gatekeeper� proteins that are responsible for opening or closing the tight junctions. Zonulin acts the mortar of the intestines and is associated when gluten sensitivity is present, if there are low counts of zonulin thus causing inflammation.
LPS(Lipopolysaccharide): These sent out a signal to the tight junction permeability as they find signs of bacterial endotoxin by translocating across the epithelial barrier and entering circulation. LPS is made up of gram negative bacteria in the GI tract. LPS outside the epithelial cell wall and reacts to fatty acids, which can lead to obesity for individuals.
Cell Receptors Involved in the Barrier Integrity
These cells are protectors of the epithelial barrier walls as they strengthen the immune intolerance and digestive tract, as well as causing or preventing inflammation when necessary.
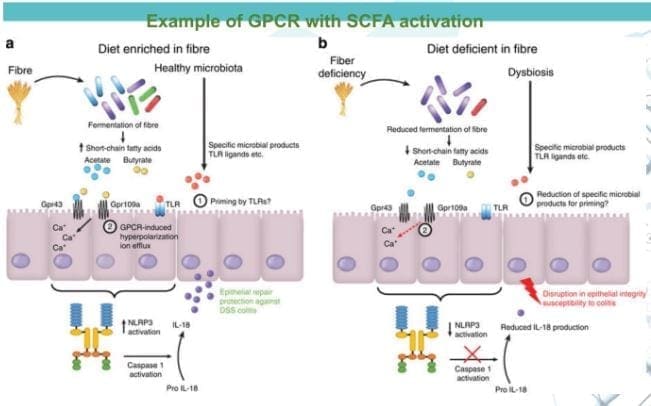
G Protein Coupled Receptors (GPCRs): GPCRs are the main players of the immune system in the epithelial system. A wide variety of substances can bind with GPCRs depending what the substances are. Short chain fatty acids, omega-3�s and any food that we eat is fermented by our gut and stimulate repair on the epithelial barrier. However if there is a consumption of low or zero-fiber in our diet, the food will not be fermented and causes inflammation.
Aryl Hydrocarbon Receptors (AhRs): AhRs interact with a range of aromatic hydrocarbons like food and microbes both in and out of the gut. These receptors respond strongly to compounds found in cruciferous vegetables, thus preventing a heighten immune reaction and reducing epithelial damage as well as promoting functioning intraepithelial lymphocytes (IELs).
But if we are not eating enough cruciferous vegetables, the IELs are being produced less, the epithelial barrier is compromised and will cause inflammation.
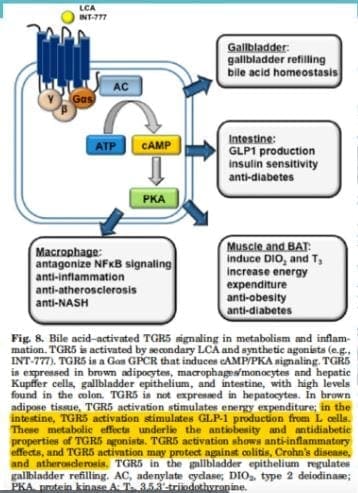
Bile Acid Receptors (BARs): BARs recognize primary and secondary bile acid. The primary bile acids comes from the liver and then transformed into secondary bile acids by microbes. BARs play an important role in in metabolic regulation, however if there is suppression of bile in the GI tract; then the intestinal barrier is more susceptible to destruction. However, if you are producing a low bile count or obstructed bile flow, it can be the result of the microbes translocating to the small intestines and causing mucosal inflammation, SIBO and leaky gut.
Epithelial Cells Involved in the Barrier Integrity
These cells are very important to the intestinal epithelial barrier as they can either protect the barrier walls or can lead them to their demised.
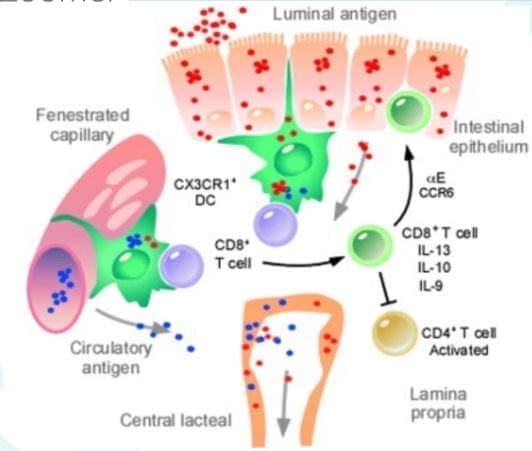
Dendritic cells: Dendritic cells are presenting antigen cells that are found the epithelial layer. These cells sample and present antigens it to Tcells, thus activating immune response. Dendritic cells help the Tcells tell the difference between self and non-self because if we eat commonly consumed foods or foreign antigens are present, we don�t want our immune system to rise up�most of the times.
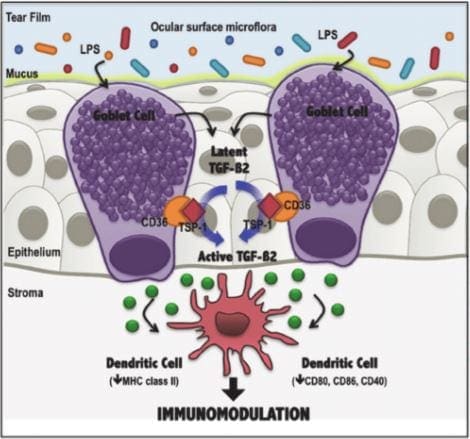
Goblet cells: Goblet cells are very important of the epithelial barrier because they provide the mucus barrier that coats and protects the intestinal walls. Without this mucus barrier, we will sick and any harmful bacteria will come in and out of the intestinal barriers.
Enteroendocrine cells: Enteroendocrine cells host receptors and produce a wide range of hormones, enzymes and neurotransmitters that affect or control our appetite, digestive functions, motility and interacts with microbial communities. However, these cells can either be beneficial or not if the host diet is in played.
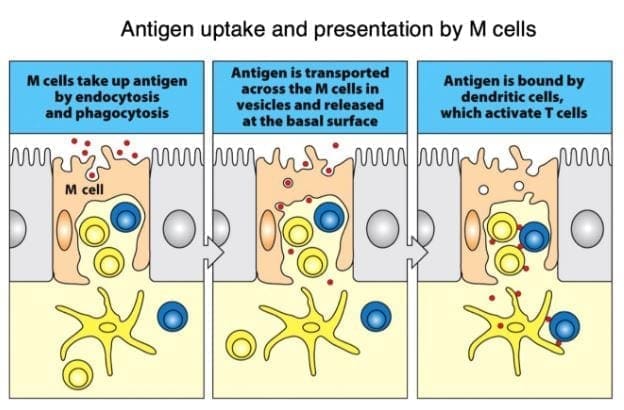
M cells: Microfold cells or M cells are located over the Peyer�s patches and they constantly sample outside the intestinal epithelial barriers for any microbes that pose a threat. They also present antigens from the outside to the dendritic cells to activate the Tcell response, as well as consuming the antigen by neutralizing it. Without the M cells, we risk of losing tolerance to microbes, thus causing inflammation on our intestinal barriers.
Conclusion
In total, we now have a deeper knowledge of our gut system as well as taking an in depth look on what our intestinal gut goes through to stop inflammation. In order to stop leaky gut, we must change our eating habits gradually when we want a healthier life. Dr. Alexander Jimenez does discuss to our patients the importance of protecting our gut with functional medicine as well as, encouraging our patients to take that first step into a healthy lifestyle.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine