How often do you get fatigued after meals? How often do you have difficulty falling into deep, restful sleep? How often do you feel more susceptible to pain? Chronic brain inflammation can cause numerous symptoms which are commonly associated with a wide variety of neurological diseases. Fortunately, researchers and healthcare professionals have found a natural remedy that can help improve chronic brain inflammation and it can provide many more health benefits: turmeric. �
For centuries, researchers and healthcare professionals alike have been studying the many health benefits of turmeric. In recent decades, however, research studies are attempting to verify the claims of our ancestors by testing turmeric in numerous clinical trials. Curcumin has been shown to have a wide variety of healing properties and practical uses. However, can turmeric improve chronic brain inflammation? In this article, we will discuss the benefits of turmeric for brain health. �
Turmeric and Brain Health
Turmeric, or curcumin, supplements have shown tremendous potential towards the safe and effective treatment of a variety of health issues. Research studies show that turmeric can help relieve arthritis and joint pain, lower blood pressure, and even enhance skincare. Turmeric may also ultimately help improve allergy symptoms and it may also help promote weight loss. �
New evidence from several research studies also suggests that turmeric may provide considerable health benefits for overall brain health, including the prevention of neurological diseases. Curcumin contains neuroprotective properties that can help preserve mental acuity. Therefore, turmeric may have the ability to boost memory function, reduce brain fog, and enhance overall cognition. Before we evaluate the research studies, we will discuss memory and brain fog in a bit more detail. �
Understanding Memory and Brain Fog
The lack of mental clarity is commonly associated with the inability to focus, poor levels of concentration, and memory problems. Best known as brain fog, or mental fatigue, this is a collection of symptoms related to reduced brain function rather than a single health issue.�The brain is an extremely complex organ. The extent with which turmeric can help depends on the cause of your brain fog, which we will discuss shortly. First, let�s review several core functions of the human brain. �
The brain acquires knowledge by using the senses as well as by experiences and thinking in what we know as cognition. Cognition ultimately includes memory, problem-solving, and decision making, among other brain functions.�
The brain is also capable of storing and recalling information. Memory is the collection of this data saved over time by neural connections in the brain. Information in the brain is made up of short-term memory and long-term memory.
The brain also other functions that work together with memory. The way we learn mainly includes how we acquire knowledge as well as how this information is remembered in the future. Learning can include changing these skills.
Brain plasticity, also known as neuroplasticity, is the way a person’s brain will change throughout their life. This helps make synapses stronger and/or weaker and it can ultimately help improve a person’s learning and memory capabilities.�
Turmeric and Brain Health: Benefits of Curcumin
One research study evaluated the effects of turmeric, or curcumin, on cognition and mood in a group of healthy, elderly individuals. The clinical trial included 60 subjects ranging between the ages of 60 and 85 years old, which consumed a 400 mg dose of curcumin. The research study was a double-blinded, placebo-controlled, and randomized clinical trial. �
One hour post-administration, researchers found considerable performance improvements in working memory tasks and sustained attention span compared to the placebo group. After four additional weeks of treatment, the turmeric, or curcumin, group experienced reduced psychological stress-induced fatigue, enhanced mood, and a better sense of calmness. �
Finally, the research study showed improvements in overall alertness and contentedness. Turmeric ultimately appears that it can also help enhance memory, focus, and concentration as well as cognition in elderly populations, among others. �
There are several mechanisms of action that turmeric takes on the human body to help prevent cognitive impairment. Turmeric reduces chronic low-grade systemic inflammation, enhances antioxidant activity, and reduces oxidative stress. �
By fighting free radicals in the human body, turmeric has also shown the potential to preserve neuronal integrity, which can inhibit the progression of cognitive decline. Furthermore, these processes demonstrate an innate ability to slow down brain aging and reduce brain fog symptomology caused by aging and disease, decreasing the risk or neurological diseases. �
Turmeric may also improve DHA, or docosahexaenoic acid, synthesis. DHA is the fatty acid most closely associated with brain health, brain development, and neuroprotection. If you have a DHA deficiency, you leave yourself at risk of developing several cognitive disorders, including anxiety, memory problems, inability to focus, etc. Researchers have found that turmeric increases multiple enzymes responsible for the synthesis of DHA from its precursor, alpha-lipoic acid, or ALA. �
According to research studies, another way in which curcumin can help improve brain health is by reducing the neurotoxicity caused by fluoride. It�s well-known that fluoride may have adverse effects on mental health and other core biological functions. Researchers performed a clinical trial testing curcumin�s neuroprotective health benefits on a group of mice. �
The results of the research study showed that fluoride increased lipid peroxidation, or LPO, a major cause of damage to cell membranes. In addition, fluoride also increased the number of neurodegenerative cells present in the hippocampus. With 30 days of curcumin administration from the research study, there was a considerable decrease in neurodegeneration and LPO. �
A second animal research study utilized curcumin to evaluate its effects on cognition and neurogenesis in a group of aged rats. Neurogenesis refers to the process of developing new neurons in the brain. Following the 12-week treatment period, researchers in the research study were ultimately able to demonstrate increased cognition and neurogenesis in the rats. �
The treated group also experienced enhanced spatial and non-spatial memory. These results suggest that turmeric may affect neuronal development, neurotransmission, synaptic plasticity, and signal transduction, among other brain functions. �
Additionally, another fundamental protein for cognition is the brain-derived neurotrophic factor, or BDNF, which promotes the growth and maturation of brain cells or, neurons. According to research studies, turmeric has shown that it can considerably help improve BDNF levels in people with premenstrual syndrome or PMS, diabetes, and obesity. �
The last research study we will look at further supports the hypothesis of utilizing turmeric to improve memory and reduce brain fog. A group of chronically stressed rats were given turmeric throughout a 20-day treatment period. �
Following turmeric administration, there was a notable reversal of impaired hippocampal neurogenesis, followed by increases in serotonin receptors and BDNF. The results of the research study ultimately suggest that turmeric, or curcumin, may overcome stress-induced abnormalities in the brain that can inhibit cognitive function, among other brain functions. �
Turmeric, or curcumin, is a powerful, natural remedy which has been demonstrated to have many health benefits, especially for brain health. Regarded as an antioxidant with anti-cancer, antidepressant, and anti-aging properties, turmeric can do much more than improve memory and brain fog. According to many research studies, turmeric or curcumin can help reduce brain inflammation or neuroinflammation by blocking the production of proinflammatory cytokines. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
Neurotransmitter Assessment Form
The following Neurotransmitter Assessment Form can be filled out and presented to Dr. Alex Jimenez. Symptoms listed on this form are not intended to be utilized as a diagnosis of any type of disease, condition, or any other type of health issue. �
In honor of Governor Abbott’s proclamation, October is Chiropractic Health Month. Learn more about the proposal. �
How often do you get fatigued after meals? How often do you have difficulty falling into deep, restful sleep? How often do you feel more susceptible to pain? Chronic brain inflammation can cause numerous symptoms which are commonly associated with a wide variety of neurological diseases. Fortunately, researchers and healthcare professionals have found a natural remedy that can help improve chronic brain inflammation and it can provide many more health benefits: turmeric. �
For centuries, researchers and healthcare professionals alike have been studying the many health benefits of turmeric. In recent decades, however, research studies are attempting to verify the claims of our ancestors by testing turmeric in numerous clinical trials. Curcumin has been shown to have a wide variety of healing properties and practical uses. However, can turmeric improve chronic brain inflammation? In this article, we will discuss the benefits of turmeric for brain health. �
The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Neural Zoomer Plus for Neurological Disease
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention. �
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link. *XYMOGEN-Catalog-Download
* All of the above XYMOGEN policies remain strictly in force.
We’ve all seen the commercials, web ads, emails, etc�about the best pillow around. Getting a good night’s sleep can be a struggle these days and any type of physical aid is welcome, specifically a pillow. This is especially true of people with chronic, acute cervical neck/back and neuropathic pain.�
Stores carry various lines of pillows that all claim to be the best pillow for neck pain.
With all the different designs out there, choosing the right pillow for your way of sleeping can be a challenge. Dr. Jimenez takes a look at finding the right pillow that will help you sleep, stay asleep and wake up refreshed and with no neck/back pain.
Throughout the sleep cycle, and therefore has a big responsibility. This guide will help you find the right one to meet your sleep needs.
Sleeping position and the pillow can play a major role in comfort or pain.
Example – Stomach sleepers usually have the most neck pain. This is because the neck is turned to the side and the spine is arched.
For relief, try sleeping either on your back or on the side. This along with a pillow that supports the neck and the natural curve of the spine.
Tips for Buying The Right One
These guidelines apply to anyone looking for a pillow that can support the spine. It should:
Keeps your spine naturally aligned meaning the head should rest directly over your shoulders and should not be propped up or pushed back too much
Can be adjusted for maximum support
Supports your head
Eliminates pressure on the cervical spine
Increases sleep duration
Hypoallergenic for those with allergies
Pillows come in all types and sizes, but don�t get it based on how it’s going to look on your bed. Take into account your body size and match that to the size of the pillow.
Picking Based On Your Sleep Position
Picking the right one for you and understanding how you sleep is important, as your sleep position can lead the way.
Stomach sleepers
Thin pillows are the way to go and sometimes not using a pillow at all could be beneficial.
Sleeping on your stomach puts more pressure on the lower back than any other sleeping position. Consider sleeping on your side/back or only sleep on your stomach for short periods then once comfortable switch to the side/back position.
Back sleepers
Thin pillows are also the way to go, but this pillow should have some lift at the bottom to help support your neck.
Memory foam is an option for back sleepers because it adjusts to your�head and neck shape.
Side sleepers
A firm pillow specifically one with a gusset or a piece of material that adds strength and thickness is more structured and can keep your spine aligned.
Specialty�
With severe spine pain or if pregnant, standard pillows do not work. There are specialty pillows that can provide comfort and pain relief.
Chiropractic
Known also as a cervical pillow, these can help if you have chronic neck or back pain that�s not allowing sleep. These are molded to your neck and keep your spine aligned during sleep, and come in a variety of styles and materials. A chiropractor can help you choose the right type and instruct you on how to use it correctly.
Pregnancy
These also come in different types but the aim is to provide support to your growing abdomen. Pregnancy pillows also come with extra body pillows designed to fit under the abdomen and between the knees supporting the entire body.
When To Replace Your Pillow
It is recommended that individuals should replace every 18 months to 2 years depending on how aggressively you sleep.
Using a pillow beyond its lifespan means there is no longer support for your spine which can exacerbate and create new injuries.
How to tell when a pillow is done its duty, fold it in half. If the pillow stays and does not return to the original position is a good indicator that it�s time for a new pillow.
El Paso, TX Neck Pain Chiropractic Treatment
Sleep allows your body to heal and the spine to rejuvenate. It helps you handle stress better and manage pain more effectively. It is an essential part of good health so making sure that you get good quality sleep should be a priority � and it is possible.
NCBI Resources
The�position that you sleep in can help relieve your back pain, but getting good quality sleep will help you manage your pain much better so it should be your goal to get proper sleep every night. And you should change it out on a regular basis.
They can get worn and no longer deliver the support they once did. If you are waking up with neck or back pain or headaches, it could be your pillow. Additionally, studies show that making your bed every day improves your quality of sleep. Make sure that the temperature is comfortable and avoid electronic devices for about an hour before bedtime. Be kind to your spine and make sleep�a priority.
How often do you feel agitated, easily upset, and nervous between meals? How often do you depend on coffee to keep yourself going?How often do you have difficulty concentrating before eating? Inflammation is an essential reaction of the human body. It’s triggered by the immune system to protect us from injury, infection, and/or illness. However, what happens if there is too much inflammation in the human body? And, what happens if there is too much inflammation in the brain?
Neuroinflammation can cause a variety of health issues, such as anxiety, stress, depression, brain fog, fatigue, and even lethargy, among other well-known symptoms. Fortunately, there is one natural remedy that can help tremendously reduce inflammation and improve brain function. According to research studies, curcumin can help combat neuroinflammation. The purpose of the article below is to discuss the anti-inflammatory effects of curcumin in microglia, brain health, and wellness.
Anti-inflammatory Effects of Curcumin in Microglial Cells
Abstract
Lipoteichoic acid (LTA) induces neuroinflammatory molecules, contributing to the pathogenesis of neurodegenerative diseases. Therefore, suppression of neuroinflammatory molecules could be developed as a therapeutic method. Although previous data supports an immune-modulating effect of curcumin, the underlying signaling pathways are largely unidentified. Here, we investigated curcumin�s anti-neuroinflammatory properties in LTA-stimulated BV-2 microglial cells. Inflammatory cytokine tumor necrosis factor-? [TNF-?, prostaglandin E2 (PGE2), and Nitric Oxide (NO] secretion in LTA-induced microglial cells were inhibited by curcumin. Curcumin also inhibited LTA-induced inducible NO synthases (iNOS) and cyclooxygenase-2 (COX-2) expression. Subsequently, our mechanistic studies revealed that curcumin inhibited LTA-induced phosphorylation of mitogen-activated protein kinase (MAPK) including ERK, p38, Akt, and translocation of NF-?B. Furthermore, curcumin induced hemeoxygenase (HO)-1HO-1 and nuclear factor erythroid 2-related factor 2 (Nrf-2) expression in microglial cells. Inhibition of HO-1 reversed the inhibition effect of HO-1 on inflammatory mediators released in LTA-stimulated microglial cells. Taken together, our results suggest that curcumin could be a potential therapeutic agent for the treatment of neurodegenerative disorders via suppressing neuroinflammatory responses. � Keywords:curcumin, neuroinflammation, TLR2, HO-1, microglial cells
Introduction
Chronic neuroinflammation plays an important role in various neurodegenerative diseases, including AD, Parkinson�s disease (PD), Huntington�s disease (HD), stroke, amyotrophic lateral sclerosis (ALS), and multiple sclerosis (MS) (Spangenberg and Green, 2017). Neuroinflammation is interceded by the activation of microglia, the prime effector cells and resident immune cells of the CNS (Nakagawa and Chiba, 2015). Microglial cells can be activated in response to neuronal death or neuronal damage induced by neuroinflammatory responses or by extracellular toxins, such as bacteria and pathogens (Larochelle et al., 2015). In neuroinflammation, activated microglia releases various kinds of cytokines, chemokines, reactive oxygen species, and reactive nitrogen species for the development and maintenance of inflammatory responses (Moss and Bates, 2001). Excessive production of these inflammatory mediators could cause neuronal damage and death. Accumulated evidence suggests that control of microglial activation could attenuate the severity of neurodegenerative disease (Perry et al., 2010). Therefore, the development of anti-neuro-inflammatory agents for the inhibition of microglial activation could be beneficial for the treatment of neurodegenerative diseases.
Microglia express pattern recognition receptors (PRR) that can bind to pattern-associated molecular patterns (PAMPs) and damage-associated molecular patterns (DAMPs) such as lipopolysaccharide (LPS) and lipoteichoic acid (LTA), respectively (Jack et al., 2005). TLRs, a major class of PRRs, play a crucial role in host defense by inducing innate immune responses. Increasingly, studies have indicated that TLR2 agonist LTA is involved in the pathogenesis of CNS infectious diseases and can induce neuronal damage (Neher et al., 2011). Inhibition of TLR2 activation attenuates microglial cell activation and amyloid ? accumulation in the brain (McDonald et al., 2016; Hossain et al., 2017). Signal transduction via TLR2 is mediated by different adaptor proteins, including MyD88, which promotes downstream signaling via MAPK and NF-?B activation leading to the expression of inflammatory mediators (Larochelle et al., 2015).
Inflammatory and oxidative molecules are very potent activators of Keap-Nrf2 (NF-E2-related factor 2), which induces the expression of Phase II detoxification enzymes to adapt to the oxidative stress condition (Rojo et al., 2010). Usually, Nrf2 acts in an inactive form. Upon stimulation, Nrf2 separates from Keap1 and translocates into the nucleus, where it binds to the antioxidant response element (ARE) to activate the transcription of antioxidant genes for cytoprotection (Ma, 2013; Cho et al., 2015). One of the Nrf2-regulated genes is heme oxygenase-1 (HO-1), which has an ARE sequence in its promoter region. Recently, HO-1 has been reported to be a predominant factor in controlling oxidative stress and inflammatory responses in neurodegenerative diseases (Schipper et al., 2009). HO-1 is the first inducible rate-limiting enzyme in the degradation of heme into by-products. HO-1 may provide neuroprotection or neurotoxic effect because of the balance between the beneficial and toxic effects of heme and heme products (Mancuso et al., 2010). One by-product of HO-1, Bilirubin, has been demonstrated to protect neurons from oxidative stress in vivo and in vitro. Bilirubin can be oxidized to biliverdin by scavenging peroxyl radicals (Chen, 2014). It has been suggested that HO-1, biliverdin, and CO have anti-inflammatory properties (Jazwa and Cuadrado, 2010). Another study has suggested that mice lacking HO-1 were vulnerable to pro-inflammatory stimuli and developed chronic inflammation due to reduced iron levels (Chora et al., 2007). Furthermore, a recent study suggested that the up-regulation of the Nrf2 and HO-1 pathways significantly inhibited the inflammatory reaction in activated microglia (Kim et al., 2016). Nrf2 inhibited microglial hyperactivation by suppressing p38 MAPK and the NF-?B signaling pathway (Kim B.W. et al., 2013). Knockdown of Nrf2 in mice was shown to be hypersensitive to neuroinflammation, as indicated by an increase in the inflammatory markers iNOS, IL-6, and TNF-? (Rojo et al., 2010). Consequently, Nrf2 and HO-1 have been considered as important therapeutic targets for neurodegenerative diseases (Koh et al., 2011; Zhang et al., 2014).
Curcumin, the main curcuminoid isolated from Curcuma longa L. (turmeric) has been used for centuries in Southeast Asia both as a medicinal remedy and as food (Kunnumakkara et al., 2017). Curcumin, demethoxycurcumin, bisdemethoxycurcumin, ar-turmerone, ?-turmerone, and ?-turmerone are the major bioactive compounds found in C. longa. In modern pharmacological studies, C. longa constituents, particularly curcumin, have shown promising pharmacological activities due to its anti-neuroinflammatory, neuroprotective, chemopreventive, immunomodulatory, and potentially chemotherapeutic effects (Garcia-Alloza et al., 2007; Zhou et al., 2017). A previous study showed that curcumin inhibited LPS-induced inflammatory responses in RAW264.7 macrophages, suggesting a potential role of curcumin in anti-Gram-negative bacterial infection (Zhou et al., 2017) and both in vivo and in vitro research have shown that curcumin exhibits anti-inflammatory effects (Garcia-Alloza et al., 2007; Prakobwong et al., 2011; Parada et al., 2015; Li et al., 2016). Furthermore, curcumin has also been reported to promote the development of the M2 microglial phenotype in an HO-1-dependent manner and reduce iNOS induction, protecting microglial cells against oxidative stress (Parada et al., 2015). In the present study, we investigated whether curcumin could affect LTA-induced microglial activation. The TLR2 ligand LTA is a major constituent of the cell wall of Gram-positive bacteria. We show that curcumin exhibits anti-inflammatory and antioxidant effects in LTA-stimulated BV2 microglia through activation of HO-1/Nrf2/ARE cytoprotective mechanisms.
Materials and Methods
Materials
Curcumin and other reagents were purchased from Sigma (C7727, >80%, St. Louis, MO, United States). Protoporphyrin IX (SnPP) and antibodies directed against HO-1 (sc-390991) – Nrf2 (sc-722), TATA-binding protein (TBP; sc-74595), ?-tubulin (sc-134237), and ?-actin (sc-130065) – were purchased from Santa Cruz Biotechnology, Inc., (Dallas, TX, United States). Antibodies directed against iNOS (13120) – phosphorylated (p)-MAPK (9910s), MAPK (9926), protein kinase B (Akt; 4685), p-Akt (13038), and an NF-?B pathway kit (9936) – were purchased from Cell Signaling Technology, Inc., (Danvers, MA, United States). LTA was obtained from InvivoGen (tlrl-pslta,Toulouse, France). Additionally, JNK inhibitor (JNK inhibitor II; 420119), Akt inhibitor (wortmannin; 12-338), ERK inhibitor (PD98059, 513000), and p38 inhibitor (SB230580, 559395) were purchased from EMD Millipore (Billerica, MA, United States). The cell culture medium, DMEM, and fetal bovine serum (FBS) were purchased from Gibco BRL (now Invitrogen Corporation, Carlsbad, CA, United States).
Cell Culture
Mouse BV-2 microglial cells were purchased from ATCC. Cells were cultured in DMEM supplemented with 10% heat-inactivated FBS and 0.1% penicillin-streptomycin (BioSource International, Camarillo, CA, United States) at 37�C in a humidified atmosphere of 5% CO2 and 95% air.
Cell Viability Assay
The cytotoxicity of curcumin was assessed using a microculture [3-(4,5-Dimethylthiazol-2-yl)-2,5-diphenyltetrazolium bromide] (MTT)-based colorimetric assay. Cells were incubated in 24-well plates at a density of 5 � 105 cells per well. The MTT solution (5 ml of 5 mg/ml) was added to each well (final concentration 62.5 mg/ml). After incubation for 3 h at 37�C in 5% CO2, the supernatant was removed and the formazan crystals produced in viable cells were solubilized with 150 ml of dimethylsulfoxide (DMSO). The absorbance of each well was then read at 570 nm using a microplate reader (Wallac 1420; PerkinElmer, Inc., Boston, MA, United States).
Measurement of Nitrite Concentration
NO synthesis in cell cultures was measured by the Griess method with microplate. To measure nitrite, 100-?l aliquots were removed from the conditioned medium and incubated with an equal volume of the Griess reagent [1% sulfanilamide/0.1%N-(1-naphthyl)-ethylenediaminedihydrochloride/2.5% H3PO4] at room temperature for 10 min. The nitrite concentration was determined by measuring the absorbance at 540 nm with a Vmax 96-well microplate spectrophotometer (Molecular Devices, Menlo Park, CA, United States). Sodium nitrite was used as a standard.
Measurement of TNF-? and PGE2 Concentration
The cells were incubated first with various concentrations of curcumin for 1 h and then with LTA for 16 h. Following 24 h incubation, TNF-? and PGE2 levels were quantified in the culture media using an enzyme-linked immunosorbent assay (ELISA) kit (R&D Systems, Minneapolis, MN, United States) according to the manufacturer�s instructions.
Preparation of Nuclear Extract
BV-2 microglial cells were washed three times with cold PBS and collected in 3000 ?l PBS using centrifugation at 800 �g for 5 min (4�C). The cell pellets were suspended in buffer A [10 mM HEPES-KOH (pH 7.9); 1.5 mM MgCl2; 10 mM KCl; 0.5 mM dithiothreitol (DTT); 0.2 mM protease inhibitor (PI)] and incubated for 5 min on ice. Buffer B [10 mM HEPES-KOH (pH 7.9); 1.5 mM MgCl2; 420 mM NaCl; 0.2 mM EDTA; glycerol 25% v/v; 0.1 mM DTT; 0.2 mM PI] was added to the cell extract and was incubated on ice for 5 min prior to centrifugation at 11,000 �g for 1 min at 4�C. Nuclear proteins were extracted with the addition of complete lysis buffer B [10 mM HEPES-KOH (pH 7.9); 1.5 mM MgCl2; 10 mM KCl; 0.5 mM DTT; 0.2 mM PI; 25% (w/v) glycerin; 420 mM NaCl; 0.2 mM EDTA] for 30 min at 4�C with occasional vortexing. Following centrifugation at 11,000 �g for 5 min at 4�C, the supernatants were collected and stored at -70�C.
Western Blot Analysis
BV-2 cells were harvested in an ice-cold lysis buffer (1% Triton X-100; 1% deoxycholate; 0.1% sodium dodecyl sulfate). The protein content of the cell lysates was subsequently determined using Bradford reagent (Bio-Rad Protein Assay Kit I5000001; Bio-Rad Laboratories, Inc., Hercules, CA, United States). Total proteins in each sample (50 ?g) were separated by 7.5% SDS-PAGE and transferred to polyvinylidene difluoride membranes. Following blocking of the non-specific binding sites with 5% non-fat milk at room temperature for 30 min, the membranes were incubated with primary antibodies directed against iNOS (1:500), p-Akt (1:1,000), p-MAPK (1:1,000), MAPK (1:1,000), p-p65, p65 (1:500), p-I?B?, I?B? (1:1,000), HO-1 (1:1,000), Nrf2 (1:1,000), TBP (1:3,000), ? (1:1,000), HO-1 (1:1.0), and actin (1:3,000) for 16 h at 4�C. This was followed by incubation with horseradish peroxidase-conjugated anti-rabbit (sc-2768; 1:5,000) or anti-mouse (sc-2371; 1:5,000) secondary antibodies (Santa Cruz Biotechnology, Inc.) at room temperature for 1 h. Tubulin was used as the loading control for each lane. The proteins were visualized using an enhanced chemiluminescence detection kit (GE Healthcare, Chicago, IL, United States). Following washing with PBS with Tween-20, the protein bands were visualized using the Gel Docsed as the loading control for each lane. The proteins were visualized using a Quant 350 analyzer (GE Healthcare).
Real-Time RT-PCR
Total RNA was isolated from cells using an RNA spin miniRNA isolation kit (GE Healthcare, Uppsala, Sweden) according to the manufacturer�s instructions. cDNA was synthesized from 1 ?g of total RNA using Maxime RT PreMix (Takara, Gyeonggi-do, Japan) and anchored oligo-dT15-primers. Real-time PCR was performed using a Chromo4TM instrument (Bio-Rad) and SYBR Green Master Mix (Applied Biosystems, Foster City, CA, United States). Relative amounts of target mRNA were determined using the comparative threshold (Ct) method by normalizing target mRNA Ct values to those for ?-actin (Ct). Prime sequences used in the study were shown in Table ?1.
Statistical Analysis
Data are expressed as the mean (standard deviation, SD). Each experiment was repeated at least three times. Statistical analysis was performed using the Statistical Package for GraphPad Prism software (version 16.0) to determine significant differences. We used either Student�s t-test or one-way analysis of variance (ANOVA) followed by Dunn�s post hoc tests for analyses. P-values < 0.05 were considered statistically significant.
Results
Curcumin Did Not Affect Cell Viability
Cell viability experiments were carried out to determine whether concentrations of curcumin used in this study affected the viability of BV2 microglia. Figure ?1 shows that curcumin at the concentration range of 5�20 ?M, together with or without 5 ?g/ml LTA, did not produce cytotoxicity in BV2 microglia. Therefore, we used these concentrations of curcumin for further study.
Curcumin Prevented the Production of Neuroinflammatory Molecules in LTA-Activated BV2 Microglia
To investigate the effects of curcumin on the secretion of inflammatory cytokines, BV2 cells were treated with LTA in the presence and absence of curcumin for 24 h. Curcumin was not removed before LTA addition. Release of NO, PGE2, and TNF-? were significantly and dose-dependently reduced by curcumin (Figures 2A�C). Furthermore, LTA increased the mRNA expression of iNOS and COX-2. Incubation with curcumin suppressed the mRNA expression of COX-2 and iNOS in BV2 microglial cells stimulated by LTA in a concentration-dependent manner (Figures 2D, E).
Curcumin Suppressed LTA-Induced Activation of NF-?B in BV-2 Microglial Cells
The genes encoding inflammatory protein expression in response to microglial activation were under the transcription control of NF-?B. Therefore, we examined the effect of curcumin on the activation of NF-?B in LTA-stimulated microglial cells. The results showed that LTA induced a characteristic increase in the phosphorylation of I?B?. Following pre-treatment with curcumin, levels of p-I?B? were significantly reduced in a concentration-dependent manner (Figure ?3 and Supplementary Figure S1). Consistently, the nuclear translocation of the NF-?B p65 subunit induced by LTA was also attenuated by pre-treatment with curcumin. Taken together, curcumin likely attenuates the expression of neuroinflammatory molecules by suppressing the nuclear translocation and activation of NF-?B. Quantification with statistical analysis was provided as supporting data.
Curcumin Inhibited LTA-Induced Activation of p38, and ERK MAPK in BV-2 Microglial Cells
Apart from NF-?B, MAPKs are also upstream modulators of neuroinflammatory molecules in microglial cells. Previous studies showed that curcumin antagonized LPS-induced MAPKs phosphorylation in microphage (Yang et al., 2008; Kunnumakkara et al., 2017). To investigate whether curcumin inhibits neuroinflammation through regulating MAPKs, we examined its effects on LTA-induced MAPK phosphorylation. BV-2 microglial cells were pre-treated with different concentrations of curcumin for 3 h and were then stimulated with LTA for 1 h. As shown in Figure ?4A and Supplementary Figure S2, curcumin inhibited LTA-induced ERK, p38, and Akt phosphorylation. However, up to 20 ?M curcumin did not affect LTA-induced JNK phosphorylation. MAPKs pathway has been reported to mediate the production of cytokines, chemokine, and other neuroinflammatory molecules. Therefore, we next investigated the role of ERK, p38, JNK, and Akt in BV2 cells� neuroinflammatory molecule production using the ERK, p38, JNK, and Akt inhibitors. However, only the p38 inhibitor SB203580 significantly decreased LTA-induced release of NO and mRNA expression levels of iNOS (Figures 4B, C). Although phosphorylation of JNK was not inhibited by curcumin, the JNK inhibitor II significantly inhibited LTA-induced NO release (Figure ?4B). The results suggest that MAPKs� signaling pathways are involved in curcumin�s anti-neuroinflammatory effects in LTA-stimulated microglial. Quantification with statistical analysis is provided as supporting data.
Inhibition of HO-1 Signaling Abolished Curcumin�s Inhibitory Effect on Neuroinflammatory Responses
HO-1 acts as an anti-inflammatory and antioxidant modulator in microglia (Schipper et al., 2009). Western blot and RT-PCR analyses showed that curcumin upregulated HO-1 expression at the protein and mRNA levels, as shown in Figures 5A�D and Supplementary Figure S3. The expression of HO-1 mRNA and protein was maximally increased in BV-2 microglial cells treated with 20?M curcumin for 4 h and 8 h respectively. Furthermore, curcumin increased Nrf2 nuclear translocation within 1 h and prolonged its nuclear translocation state to 2 h (Figures 5E, F and Supplementary Figure S3). Next, we investigated whether curcumin-induced HO-1 mediated an anti-neuroinflammatory response in LTA-stimulated BV-2 microglial cells. We treated cells with the HO-1 inhibitor SnPP. We then evaluated curcumin�s effect on LTA-induced NO and TNF-? release. Treatment with SnPP significantly suppressed curcumin-mediated inhibition of NO and TNF-a release (Figures 5G, H). Taken together, these results reveal that curcumin-dependent HO-1 and Nrf-2 signal activation plays a crucial role in downregulating neuroinflammatory responses. Quantification with statistical analysis is provided as supporting data.
Discussion
Microglia, the major resident macrophages of the CNS, has been reported to be the main effector cells in mediating neuroinflammation and selective neuronal death (Perry et al., 2010). Microglial cells increase the production of neuroinflammatory molecules after exposure to activators such as LPS and LTA via their surface receptors, TLR4 and TLR2, respectively (Perry and Holmes, 2014; Hossain et al., 2017). Increased expression and activation of TLR2 is associated with the progression of neurodegenerative diseases, such as PD and dementia (Dzamko et al., 2017). For example, activation of TLR2 could upregulate ?-synuclein in PD brains and play important roles in the pathogenesis of PD brains (Roodveldt et al., 2013). In addition, Kim C. et al. (2013) also showed that neurodegeneration was attenuated by either knockout or knockdown of TLR2 in rodent PD models. Thus, controlling TLR2-mediated microglia activation and neurotoxicity has been suggested as an important therapeutic approach to treating neurodegenerative diseases. A potential agent in this process could be curcumin, which has been shown to exert neuro-protective and anti-inflammatory effects in various experiment models (Parada et al., 2015; Li et al., 2016). Curcumin is a highly lipophilic natural compound. A previous study has well demonstrated that curcumin is able to cross the blood�brain barrier and that it is mainly concentrated in the hippocampus in the brain (Tsai et al., 2011). Some studies reported that curcumin inhibited HIV-1 gp120-induced neuronal damage and provided anti-neuroinflammatory effects in LPS-induced microglia (Gong et al., 2012). This protective effect of curcumin seems to be dependent on its anti-inflammatory actions. Curcumin could protect neurons against microglia-mediated neurotoxicity while becoming inefficient under microglia-depleted conditions (Park et al., 2001; Yang et al., 2008; Parada et al., 2015). Similar studies in peripheral cells also showed the anti-inflammatory effects of curcumin. Using RAW 264.7 murine macrophages, studies have shown that curcumin inhibited PGE2, NO, and TNF-? release following LPS stimulation (Pae et al., 2008). However, the effects of curcumin on TLR2-induced neuroinflammation in microglial cells are not fully understood.
Regulation of the signaling pathways in activated microglia is important in maintaining CNS homeostasis because deregulated neuroinflammatory responses can result in the death of adjacent neurons through the release of inflammatory molecules, such as cytokines, chemokines, NO, and ROS (Perry and Holmes, 2014; Spangenberg and Green, 2017). For example, excessive NO synthesis under endotoxins results in the formation of reactive nitrogen species and neuronal cell death (Perry et al., 2010). PGE2 has also been shown to contribute to neuronal death through activation of the MAPK/ERK pathway in microglia (Xia et al., 2015). In this present study, we showed that curcumin inhibited the secretion of inflammatory mediators TNF-?, NO, and PGE2, and expression of iNOS and COX-2 in BV2 microglia stimulated with LTA. We further showed that curcumin attenuated these effects of LTA without altering cell survival, suggesting that curcumin is safe and could be considered as a potential therapeutic agent in neuroinflammation.
NF-?B is the main transcription factor which plays critical roles in regulating redox homeostasis. NF-?B is considered the master regulator of microglial inflammatory responses to neuronal injury (Acharyya et al., 2007). Recent studies showed that NF-?B activation controlled the expression of inflammatory molecules, such as NO, PGE2, and TNF-?, and IL-1b production (Acharyya et al., 2007). Therefore, modulation of NF-?B activation is considered a critical way to control microglial activation. The activation of the NF-?B signaling pathway is mediated by the I?B protein. The phosphorylation of I?B results in NF-?B dissociation, which leads to the induction of inflammatory mediators. In this study, it was shown that curcumin produced dual inhibition of phosphorylation and degradation of I?B?, as well as nuclear translocation of p65, suggesting that this agent could stabilize NF-?B in the microglial cytoplasm following stimulation with LTA in BV-2 microglial cells.
In mammalian cells, MAPKs signaling pathways, including ERK, JNK, and p38, contribute to the production of a wide variety of neuroinflammatory mediators (Chantong et al., 2014). In this present study, pre-treatment with curcumin decreased the phosphorylation of p38 and ERK. Furthermore, the p38 inhibitor SB203580 significantly reduced the secretion of NO and the mRNA expression of the key pro-inflammatory gene, iNOS. These results suggested that curcumin initiated the anti-neuroinflammatory effects in LTA-stimulated BV-2 microglial cells, partially through inhibition of p38 MAPK activation. The PI3K/Akt-dependent signaling pathway promotes inflammatory responses in microglia. The involvement of the Akt pathway has been shown in the expression of inflammatory mediators in microglia through the activation of NF-?B in microglia (Lo et al., 2015). Curcumin suppressed the phosphorylated Akt, the downstream target of PI3K. However, the PI3K inhibitor wortmannin did not show any inhibitory effect on the secretion of NO or the mRNA expression of iNOS. Taken together, these data suggest that the anti-neuroinflammatory effect of curcumin occurs mainly through inhibiting the NF-?B and MAPKs signaling.
We also identified the intracellular pathway that negatively regulates the inflammatory-molecule expression in microglial cells. Nrf2 is a redox-sensitive transcription factor that regulates microglial inflammatory responses to brain infections. The effect of Nrf2 has been described in different in vivo models where knockdown of Nrf2 in mice enhanced vulnerability to asthma or emphysema (Ma, 2013). Moreover, the TLR2/TLR4 agonist promoted inflammatory responses in Nrf2 KO mice compared to WT mice (Kong et al., 2011). In the current study, we showed that curcumin increased the expression of Nrf2 and its downstream protein HO-1. HO-1 is a key signaling molecule implicated in the regulation of inflammatory and oxidative responses. The HO-1 gene has an ARE sequence in its promoter region, which is a binding site for the transcription factor Nrf2. Several studies have proposed that NF-?B interrupts the Nrf-2-ARE signaling pathway because many compounds that induced HO-1 and Nrf2 signaling incidentally repressed NF-?B activation (Li et al., 2016). HO-1 expression was essential for the microglial specific cytoprotective effect (Parada et al., 2015). Several studies have also shown an inverse correlation between HO-1 and inflammatory mediator secretion (Chora et al., 2007; Parada et al., 2015). In agreement, we observed that curcumin alone induced the expression of HO-1 in microglial cells. Furthermore, the HO-1 inhibitor abrogated curcumin anti-inflammatory effect in BV-2 microglial cells.
Conclusion
This study demonstrated that curcumin had anti-inflammatory activity in LTA-stimulated microglial cells that may through inhibiting NF-?B and p38 MAPK activation, and may induce the expression of Nrf2 and HO-1 (Figure ?6). Furthermore, curcumin does not have cytotoxic effects in BV-2 microglial cells at its anti-inflammatory dose. Curcumin may have therapeutic potential for some neuroinflammation-associated disorders caused by Gram-positive bacteria.
�
Curcumin, or turmeric, is a powerful anti-inflammatory which has been demonstrated to have many health benefits. Regarded as an antioxidant with anti-cancer, antidepressant, and anti-aging properties, curcumin can do much more than heal wounds and enhance memory. According to research studies, curcumin or turmeric can help reduce neuroinflammation or brain inflammation. This powerful anti-inflammatory can block the production of proinflammatory cytokines and promote overall well-being. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
Neurotransmitter Assessment Form
[wp-embedder-pack width=”100%” height=”1050px” download=”all” download-text=”” attachment_id=”72741″ /]
The following Neurotransmitter Assessment Form can be filled out and presented to Dr. Alex Jimenez. Symptoms listed on this form are not intended to be utilized as a diagnosis of any type of disease, condition, or any other type of health issue.
In honor of Governor Abbott’s proclamation, October is Chiropractic Health Month. Learn more about the proposal.
How often do you feel agitated, easily upset, and nervous between meals? How often do you depend on coffee to keep yourself going?How often do you have difficulty concentrating before eating? Inflammation is an important response of the human body. It’s activated by the immune system to guard us against injury, infection, and/or illness. However, what happens if there is too much inflammation in the human body? And, what happens if there is too much inflammation in the brain?�
Brain inflammation can cause a variety of health issues, such as anxiety, stress, depression, brain fog, fatigue, and even lethargy, among other common symptoms. Fortunately, there is one natural remedy that can help greatly reduce neuroinflammation and improve brain function. According to research studies, curcumin can combat brain inflammation. The purpose of the article above was to discuss the anti-inflammatory effects of curcumin in microglia and brain well-being
The following article has been referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Neural Zoomer Plus for Neurological Disease
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention.
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
For your convenience and review of the XYMOGEN products please review the following link. *XYMOGEN-Catalog-Download* All of the above XYMOGEN policies remain strictly in force.
If you are experiencing any of these situations, then try considering intermittent fasting.
Since becoming popular in recent years, intermittent fasting is a dietary approach that lots of individuals have been using in their healthy lifestyle. During the time of the hunter-gatherer society, people have used this method for centuries as a way of survival. Studies have been shown that people used it for medicinal purposes throughout history as a medicinal remedy. Ancient Rome, Greek and Chinese civilizations used intermittent fasting in their daily lives. Fasting has even been used for spiritual reasons in certain religions, like Buddhism, Islam, and Christianity as individuals use it as a way to reflect on themselves and be closer to their deities.
What is Fasting?
Fasting is where a person does not consume food or beverages at least for twelve hours during the day. When a person starts fasting, they will notice that their metabolism and their hormones will change in their bodies. There is upcoming research that intermittent fasting can promote amazing health benefits to the body. The health benefits that intermittent fasting provides are weight loss, protective effects in the brain, decreased inflammation and improving blood glucose and insulin levels in the body.
The Different Methods
There are other methods of fasting that involves fasting from food for several days or weeks. With these different methods, they involve a shorter period that is between 16 to 24 hours. Several types of intermittent fasting are determined by the feeding window duration (when to eat the food) and the fasting window (when to avoid the food). Here are some of the other methods of fasting, which includes:
Time-restricted feeding (TRF): This type of fasting has a feeding window period from 4 to 12 hours. For the remainder of the day, water is the only thing that is allowed to be consumed. The common variation to eat this type of fasting is 16/8. This means that a person has to fast at least 16 hours every day.
Early time-restricted feeding (eTRF): This is a different variety of time-restricted fasting that is from 8 a.m. to 2 p.m. After the 6 hours are up, the rest of the day is made up of this fasting period.
Alternate day fasting (ADF): This type of fasting involves a person eating one day and the next day they completely fast. They alternate between eating and fasting each day to get the benefits.
Period fasting (cycling fasting): This type of fasting involves one or two days fasting per week and for the fifth or sixth days of eating as much as a person desire. The variety of period fasting can be a 5:2 or a 6:1.
Modified fasting: This type of fasting has some methods of intermittent fasting that are similar to alternate-day fasting, but this fasting can be modified for anyone. A person can consume very-low-calorie substances during the fasting window period.
How Does It Work?
Intermittent fasting is the result of changes in the body as the hormone patterns and energy metabolism are being affected. Once a person finishes consuming food, the contents are being broken down and transforming into nutrients, so it can be absorbed into the digestive tract. What happens is that the carbohydrates are broken down and turn into glucose and absorb into the bloodstream, distributing it into the body’s tissue as the essential source of energy. The insulin hormone then helps regulate the blood glucose levels by signaling cells to take the sugars from the blood and turning into fuel for the body to function properly.
With intermittent fasting, a person is done with a meal and their glucose levels are depleted from the body. For the energy to meet its requirements the body has to break down the glycogen that is found in the liver and skeletal muscles causing gluconeogenesis. Gluconeogenesis is when the liver produces glucose sugars from non-carbohydrate sources in the body. Then once the insulin levels are low after 18 hours of fasting, a process called lipolysis begins. What lipolysis does is that the body begins to break down the fat components into free fatty acids. When there is a low quantity of glucose for the body to consume for energy, the body itself with start using fatty acids and ketones for energy. Ketosis is a metabolic state where liver cells start to help fatty acids breakdown and converting them into ketone acetoacetate and beta-hydro butyrate.
The muscle cells and neuron cells use these ketones to generate ATP (adenosine triphosphate) which is the main carrier for energy. Research has stated that the usage and availability of fatty acids combined with ketones as an energy replacement for glucose are beneficial for vital body tissues. This includes the heart, the liver, the pancreas, and the brain.
The four metabolic states are induced by fasting are referred to as the fast-fed cycle, and they are:
The fed state
The post-absorptive state
The fasting state
The starvation state
The physiological effect of intermittent fasting can also be achieved by following a ketogenic diet, which is very high fat and low carbohydrate diet. This diet’s purpose is to shift the body’s metabolic state into ketosis.
The Benefits of Fasting
There are tons of research that have demonstrated how intermittent fasting has a wide variety of health benefits, including:
Weight loss
Type 2 diabetes prevention and management
Improved cardiometabolic risk factors
Cellular cleansing
Decreased inflammation
Neuroprotection
Studies have been shown that several proposed mechanisms are responsible for these health effects of intermittent fasting and have proven to be beneficial to a person’s lifestyle.
Conclusion
Intermittent fasting has been practiced for centuries and has gain popularity in recent years. It involves abstaining from consuming foods for at least 12 consecutive hours by turning the fat cells into energy for the body to function. The health benefits that intermittent fasting provides is beneficial for an individual who is trying to maintain a healthy lifestyle. Some products help provide support to the gastrointestinal system as well as making sure that sugar metabolism is at a healthy level for the body to function.
The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
References:
Dhillon, Kiranjit K. �Biochemistry, Ketogenesis.� StatPearls [Internet]., U.S. National Library of Medicine, 21 Apr. 2019, www.ncbi.nlm.nih.gov/books/NBK493179/#article-36345.
Hue, Louis, and Heinrich Taegtmeyer. �The Randle Cycle Revisited: a New Head for an Old Hat.� American Journal of Physiology. Endocrinology and Metabolism, American Physiological Society, Sept. 2009, www.ncbi.nlm.nih.gov/pmc/articles/PMC2739696/.
Stockman, Mary-Catherine, et al. �Intermittent Fasting: Is the Wait Worth the Weight?� Current Obesity Reports, U.S. National Library of Medicine, June 2018, www.ncbi.nlm.nih.gov/pmc/articles/PMC5959807/.
Zubrzycki, A, et al. �The Role of Low-Calorie Diets and Intermittent Fasting in the Treatment of Obesity and Type-2 Diabetes.� Journal of Physiology and Pharmacology: an Official Journal of the Polish Physiological Society, U.S. National Library of Medicine, Oct. 2018, www.ncbi.nlm.nih.gov/pubmed/30683819.
In today’s busy world individuals need a little help when it comes to letting go of bad/negative behaviors and adopting/embracing positive behaviors to sustain optimal health and lifestyle. This is where a health coach�comes in.
More adults in the United States have a chronic disease and around thirty percent have two or more.
Many healthcare professionals do not know how to counsel patients on healthy living and, if they do, the information is limited to very basic knowledge like exercise and eat healthily. With this type of info and not a lot of enthusiasm, patients are not going to listen or make lasting changes.
Many providers do not listen to what’s going on and just tell patients what to do, instead of discussing the best options they have for their health. People being told what to do are not likely to listen or act upon the recommendations.
A health coach creates a custom getting healthy plan with you that fits your life, gets you going, sets up a strategy for the challenges and sees you through! This is what a health coach does.
Health coaching Involves
Communication
Motivation
Continued Support
This allows individuals to make meaningful behavior changes that will last forever.
Coaching centers on:
Thorough conversation
Listening
Clinical Intervention
Strategies
These are aimed to actively engage patients in positive behavior change.
Health coaches take on patients wherever they are in their health. An individual can be healthy and just want some advice to individuals that are extremely unhealthy with weight issues, chronic illness, disease or all of the above.
The point is to help individuals learn self-management techniques. The coach teaches, motivates and strategizes with the individual to make educated/informed decisions that will turn into regular healthy habits.
Coaching comes in the form of:
Setting�goals that are achievable�
A Patient’s Values
Strengths
Motivation
Encouraging the patient
This is how healthy attitudes and behaviors are developed.
The Health Journey Begins
The patient’s health history is taken into account. Then the coach asks:
Where they want to be in their health
What Values they hold close
What Goals they have in mind
The plan is Created
Progress is Tracked
Challenges are met
The long-term plan is Created
Patients oftentimes do not know where they are from a health perspective and might not be sure how to explain. This is where health coaches and their training can breakdown any questions/issues a patient may have.
A health coach will look at where a patient is healthwise based on:
Emotional factors
Environmental factors
Financial factors
Psychological factors
Physical factors
Recreational factors
Spiritual factors
Social factors
This health inventory is for the patient to reflect on where they are in their health and where they want to be.
Patients are welcome and encouraged to ask questions about the plan, make changes, reset goals, etc.
Motivating the Patient
Motivation can come in various forms. As people learn in various ways, so too are the motivational strategies to get patients to exercise the positive behavior outlined in their treatment plan. Some ways coaches motivate are:
They collaborate with patients and don’t approach the plan with an all-knowing mindset.
Understand the motivation of the individual to change.
Motivational Principles:
Empathy
Discrepancy
Support patient’s ability
Six stages of behavioral change:
Precontemplation – Patients do not see any problems and do not consider their behavior as negative, and do not see the problems their behavior is causing.
Contemplation – Patients start to think about healthy behaviors.
Preparation/Determination�– Patients are ready to take action toward behavior change and believe the new behavior will lead to a healthy life.
Action�– Change begins and the intention is to keep going.
Maintenance – Behavior change has been for more than six months and continuing on the right track.
Termination�– Negative behaviors are eliminated.
There are different strategies to get through each stage and on to the next until the positive behavior is achieved.
Helping the patient find the coaching plan that is right for them.
Patients are helped by figuring out what they want to change about their health based on what they see and
the most important changes for them. There is no correct answer, as it is different for everyone.
Understanding Your Values
Coaches encourage the patient to identify their values, and what is most important for each individual.
These include:
Family
Friendship
Health
Love
Values begin early in childhood and become reevaluated as life goes on, and can change.
Clarity is important to help the patient build self-awareness to make intelligent decisions and staying balanced.
A coach might ask questions like:
What made you choose the unhealthy product versus the healthy version?
How much stress do you think you have to deal with on a daily basis?
Do you make time for yourself?
For some, identifying negative behavior can help, as the patient grows and realizes how their health is changing, their values start to change.
This information helps to create a plan of action along with steps to help the patient’s decision making.
While working with the patient to determine goals and create steps, tools and methods are created help to ensure the patient understands their role in getting healthy.
Asking Questions
Coaches ask patients what they know and what they would like to know?�There are no incorrect questions, aks away, as the more an individual knows, as well as the more that the coach knows about the patient, the better the treatment plan will be.
Teaching
If the patient doesn�t understand, the process is repeated until the patient is able to explain the treatment plan back to the coach so everything is clear.
This technique is recognized by various associations, including the:
American Academy of Family Physicians
American Hospital Association
Primary Areas of Improvement
Before setting goals the patients go over the primary areas of their life that they want to improve/change.
These primary areas may be very similar to the patient�s values.
Examples include:
Health
Family
Career
Finances
Recreation
Social Relationships
Once a patient has identified what they would like to focus on, brainstorming sessions are put into action, as to what they want to change or improve for each primary area.
They are then broken down into smaller goals in the creation of the main plan of action.
As the patient moves forward they are more motivated and encouraged to take on bigger challenges.
Couple making a healthy smoothie
Goals
Patients understand what areas of their life they want to improve/change.
With the primary areas known, the patient begins the challenge of changing their current unhealthy status to healthy.
Areas to consider:
What exactly do I want to achieve?
How will I achieve this goal?
Timeframe to achieve this goal?
Why is this goal important to me?
Where to go to next once the goal is achieved?
SMART Goals
When the patient is ready, the coach will assist in developing:
Specific
Measurable
Attainable
Relevant
Timely
SMART goals that allow for structure and trackability and create clear milestones for the individual.
Planning
Once a health coach understands where the patient wants to go, the next phase is planning.
Patients help in creating their treatment plan.
This plan is an agreement between the patient and the health coach that describes the behavior change that the patient wants to make, how they’re going to go about it, and their commitment to the final result.
Example of goals a patient will follow to lose weight:
Try new fruits and vegetables
Find creative ways to incorporate exercise at work.
Stay hydrated by keeping a water bottle and refilling it every two hours.
Cooking healthy meals at first twice a week then three times and so on.
Walking after meals.
These small tasks make it easier for the patient to see their progress.
The coach will check with the patient regularly to make sure they are sticking to the plan.
Health Coach
Goal Progress
Health coaches can ensure a patient has consistent motivational support by creating a follow-up plan that works in conjunction with their primary treatment plan.
Follow-up care may include schedules for physical exams or tests, referrals, and recommendations to keep positive behavior development.
Coaches and patients work together to create realistic goals for the future.
As the patient progresses, the health coach may make additional recommendations or work with the patient to adjust their plan or making sure the patient knows where to turn to if they have questions.
Continued Support
Once goals are being achieved it is important to have support to continue the positive behavior. Traditional sources of support include:
Family
Friends
Colleagues
Community
Patients may not always have access to external support, coaches also teach the patients how to find positive support in various activities around town that can help patients and their overall health.
At Injury Medical Chiropractic & Functional Wellness clinic we have the best-rated team of health practitioners to get you to your best optimal health.
*Detox Your Body* | Detox Doctor | El Paso, TX (2019)
Fred Foreman is a basketball coach who depends on his overall health and wellness to be able to engage in his everyday responsibilities. As a result, coach Foreman started the 6 Day Detox Program, designed to help renew and enhance the human body’s cleansing and detoxification capabilities.
NCBI Resources
Good health is built on diet and exercise. The goal is to continually improve by maintaining healthy habits that develop more healthy behaviors. You do not have to do anything drastic. You will have an easier time making changes if you start small and gradually shift towards a lifestyle that is best for you. A health coach can get you operating and performing at the highest level!
How high is your stress level? How often do you feel overwhelmed? Anxiety is a well-known health issue that is, unfortunately, often misunderstood, especially when it manifests other misunderstood symptoms like brain fog. � Brain fog is commonly associated with reduced thinking and processing while anxiety is frequently associated with racing thoughts that can make people overly cautious as well as worries that can keep people awake, wired, and restless. How does anxiety cause brain fog? The purpose of the following article is to understand brain fog associated with anxiety. �
How Does Brain Fog with Anxiety Happen?
Brain fog is a symptom rather than a single health issue. It�s described as the sensation that your brain isn’t functioning properly. Anxiety involves symptoms of overthinking, excessive worrying, imagining negative outcomes, and fear. � Brain fog and anxiety happens because the symptoms of one health issue can ultimately cause the symptoms of the other health issue and vice versa. This can also worsen both conditions. Brain fog and anxiety can cause an infinite loop. �
Anxiety involves �what-ifs,� ruminations, and negative thinking
This can then lead to mental exhaustion or fatigue
Fatigue can also develop brain fog
Brain fog can in turn increase anxiety because it feels frightening, worrisome
Increased anxiety causes this cycle to repeat, seemingly endlessly
Brain fog associated with anxiety may vary from person to person. Several people will experience it often while others will experience it less frequently. It can also come and go quickly, or it can ultimately last for days, weeks, and even months. � Evaluating the symptoms and the causes of brain fog and anxiety will provide insights that can be used for treatment. �
Symptoms of Brain Fog with Anxiety
Brain fog and anxiety share a common symptom, frequently referred to as fatigue or tiredness. Brain fog, anxiety, and fatigue are well-known symptoms that are often connected. However, fatigue is believed to be at the heart of brain fog and anxiety. � Anxiety appears to take control of our entire brain and aggravates thoughts, emotions, and behaviors. Living in a state of constant anxiety is exhausting. Moreover, anxiety can cause sleeping problems. Fatigue can lead directly to brain fog. � Common symptoms of brain fog, anxiety, and fatigue can ultimately include: �
Difficulty concentrating and focusing
Muddled, unclear thoughts
Short-term memory problems
Difficulty reasoning logically
Trouble processing, storing, and retrieving information
Living in a fog that makes grasping comments, instructions, and conversations challenging
The vague sense that you just feel �off� but can�t do anything about it
Causes of Brain Fog with Anxiety
The brain fog that occurs with anxiety can have several causes, including: �
The�symptoms of anxiety, as previously discussed above
The brain�s mental, physical, and emotional response to anxiety
Stress as well as stress hormones and other substances or chemicals.
Understanding the cause of brain fog with anxiety can increase awareness of why these health issues can develop. � The brain�s own reaction to anxiety can also make it feel tired and foggy. The fight-or-flight response is an automatic fear response. The brain reacts in response to an extreme stressor to prepare to either stay and fight or run away to safety. �
Activity in the cortex, the area of rational thinking, decreases, which leads to the inability to think properly
Activity in the hippocampus, the area responsible for learning and memory, is suppressed, causing confusion
Activity in the amygdala accelerates to keep you hypervigilant and ready to leap before you look
The brain also controls the production of hormones in reaction to stress and anxiety. Cortisol, adrenaline, and norepinephrine travel through the brain and the body to keep you alert and ready for action but when these hormones are triggered for too long or in quantities that are too high, they overwhelm and exhaust the brain, causing brain fog. �
Treatment for Brain Fog and Anxiety
The best treatment for brain fog associated with anxiety is to treat it at its source. It’s essential to understand the symptoms of both brain fog and anxiety as well as take steps to reduce other symptoms like fatigue. Furthermore, know what is causing your symptoms so you can ultimately make positive changes to reduce them or even eliminate them, including: �
Develop stress management strategies
Take measures to increase the amount and quality of sleep
Address your anxiety, either with a therapist or other qualified healthcare professional
Listen to your body and brain; participate and engage in exercise, yoga, mindfulness, and meditation
� Brain fog and anxiety can be difficult. But by actively working on them, you can reduce both and promote overall well-being. �
Anxiety can commonly cause a variety of symptoms, including brain fog. Although it may seem like brain fog and anxiety are two separate as well as different health issues, they are frequently connected. Both anxiety and brain fog can cause concentration, focus, and memory problems, and stress is considered to be one of the most well-known causes of brain fog associated with anxiety. Treatment for anxiety and brain fog often involves treating the underlying source of the health issues. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
Neurotransmitter Assessment Form
The following Neurotransmitter Assessment Form can be filled out and presented to Dr. Alex Jimenez. Symptoms listed on this form are not intended to be utilized as a diagnosis of any type of disease, condition, or any other type of health issue. �
In honor of Governor Abbott’s proclamation, October is Chiropractic Health Month. Learn more about the proposal. �
How high is your stress level? How often do you feel overwhelmed? Anxiety is a well-known health issue that is, unfortunately, often misunderstood, especially when it manifests other misunderstood symptoms like brain fog. � Brain fog is commonly associated with reduced thinking and processing while anxiety is frequently associated with racing thoughts that can make people overly cautious as well as worries that can keep people awake, wired, and restless. How does anxiety cause brain fog? The purpose of the following article is to understand brain fog associated with anxiety. �
The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Neural Zoomer Plus for Neurological Disease
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention. �
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link. *XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force.
Like you have been diagnosed with Celiac Disease, Irritable Bowel Syndrome, Diverticulosis/Diverticulitis, or Leaky Gut Syndrome?
Excessive belching, burping, or bloating?
Abnormal distention after certain probiotics or natural supplements?
Suspicion of nutritional malabsorption?
Do digestive problems subside with relaxation?
If you are experiencing any of these situations, then you might be experiencing gut problems and might have to try the 4R Program.
Food sensitivities, rheumatoid arthritis, and anxiety have been associated with impaired gastrointestinal permeability. These various conditions can happen from many factors that can impact the digestive tract. If left untreated it can potentially be the result of dysfunction of the intestinal permeability barrier, causing inflammation, and severe health conditions that the gut can develop. The 4R program is used to restore a healthy gut in the body and involves four steps. They are: remove, replace, reinoculated, and repair.
Intestinal Permeability
The intestinal permeability helps protects the body and makes sure that harmful bacteria do not enter the gut. It protects the body from potential environmental factors that can be harmful and are entering through the digestive tract. It can be either toxin, pathogenic microorganisms, and other antigens that can harm the digestive tract causing problems. The intestinal lining is consisting of a layer of epithelial cells that are separated by tight junctions. In a healthy gut, the tight junction regulates the intestinal permeability by selectively allowing substances to enter and travel across the intestinal barrier and preventing harmful factors from being absorbed.
Certain environmental factors can damage the tight junction, and the result is that it can increase the intestinal permeability, which causes intestinal hyperpermeability or leaky gut in the body. Contributing factors can increase intestinal permeability like an excessive amount of saturated fats and alcohol, deficiencies in nutrients, chronic stress, and infectious diseases.
With an increased intestinal permeability in the gut, it can enable antigens to cross the gut mucosa and enter the bloodstream causing an immune response and inflammation to the body. There are certain gastrointestinal conditions that are associated with intestinal hyperpermeability and if left untreated it can trigger certain autoimmune conditions that can cause harm to the body.
4Rs Program
The 4Rs is a program that healthcare professionals advise their patients to use when they are addressing disruptive digestive issues and help support gut healing.
Removing the Problem
The first step in the 4Rs program is to remove harmful pathogens and inflammation triggers that are associated with increased intestinal permeability. Triggers like stress and chronic alcohol consumption can do much harm to an individual’s body. So targeting these harmful factors from the body is to treat it with medication, antibiotics, supplements, and the removal of inflammatory foods from the diet is advised, including:
– Alcohol
– Gluten
– Food additives
– Starches
– Certain fatty acids
– Certain foods that a person is sensitive to
Replacing the Nutrients
The second step of the 4Rs program is to replace the nutrients that are causing the gut problems through inflammation. Certain nutrients can help reducing inflammation in the gut while making sure that the digestive tract is being supported. There are some anti-inflammatory foods that are nutritious. These include:
– High-fiber foods
– Omega-3s
– Olive oil
– Mushrooms
– Anti-inflammatory herbs
There are certain supplements can be used to support digestive function by assisting and absorbing the nutrients to promote a healthy gut. What the digestive enzymes do is that they assist in helping to break down fats, proteins, and carbohydrates in the gut. This will help benefit individuals that have an impaired digestive tract, food intolerances, or having celiac disease. Supplements like bile acid supplements can help assist in nutrient absorption by merging lipids together. Studies have stated that bile acids have been used to treat the liver, gallbladder, and bile duct while preventing gallstone formation after bariatric surgery.
Reinoculated The Gut
The third step is of the 4rs program to reinoculated the gut microbe with beneficial bacteria to promote a healthy gut function. Studies have been shown that probiotic supplements have been used to improve the gut by restoring beneficial bacteria. With these supplements, they provide the gut an enhancement by secreting anti-inflammatory substances into the body, help support the immune system, altering the body’s microbial composition, and reducing the intestinal permeability in the gut system.
Since probiotics are found in fermented foods and are considered as a transient since they are not persistent in the gastrointestinal tract and are beneficial. Surprisingly, they still have an impact on human health due to influencing the gut by producing vitamins and anti-microbial compounds, thus providing diversity and gut function.
Repairing the Gut
The last step of the 4Rs program is to repair the gut. This step involves repairing the intestinal lining of the gut with specific nutrients and herbs. These herbs and supplements can help decrease intestinal permeability and inflammation in the body. Some of these herbs and supplements include:
– Aloe vera
– Chios mastic gum
– DGL (Deglycyrrhizinated licorice)
– Marshmallow root
– L-glutamine
– Omega-3s
� Polyphenols
– Vitamin D
– Zinc
Conclusion
Since many factors can adversely affect the digestive system in a harmful way and can be the contributor to several health conditions. The main goal of the 4Rs program is to minimize these factors that are harming the gut and reducing inflammation and increased intestinal permeability. When the patient is being introduced to the beneficial factors that the 4Rs provide, it can lead to a healthy, healed gut. Some products are here to help support the gastrointestinal system by supporting the intestines, improving the sugar metabolism, and targeting the amino acids that are intended to support the intestines.
The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
References:
De Santis, Stefania, et al. �Nutritional Keys for Intestinal Barrier Modulation.� Frontiers in Immunology, Frontiers Media S.A., 7 Dec. 2015, www.ncbi.nlm.nih.gov/pmc/articles/PMC4670985/.
Ianiro, Gianluca, et al. �Digestive Enzyme Supplementation in Gastrointestinal Diseases.� Current Drug Metabolism, Bentham Science Publishers, 2016, www.ncbi.nlm.nih.gov/pmc/articles/PMC4923703/.
Mu, Qinghui, et al. �Leaky Gut As a Danger Signal for Autoimmune Diseases.� Frontiers, Frontiers, 5 May 2017, www.frontiersin.org/articles/10.3389/fimmu.2017.00598/full.
Rezac, Shannon, et al. �Fermented Foods as a Dietary Source of Live Organisms.� Frontiers in Microbiology, Frontiers Media S.A., 24 Aug. 2018, www.ncbi.nlm.nih.gov/pmc/articles/PMC6117398/.
Sander, Guy R., et al. �Rapid Disruption of Intestinal Barrier Function by Gliadin Involves Altered Expression of Apical Junctional Proteins.� FEBS Press, John Wiley & Sons, Ltd, 8 Aug. 2005, febs.onlinelibrary.wiley.com/doi/full/10.1016/j.febslet.2005.07.066.
Sartor, R Balfour. �Therapeutic Manipulation of the Enteric Microflora in Inflammatory Bowel Diseases: Antibiotics, Probiotics, and Prebiotics.� Gastroenterology, U.S. National Library of Medicine, May 2004, www.ncbi.nlm.nih.gov/pubmed/15168372.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine









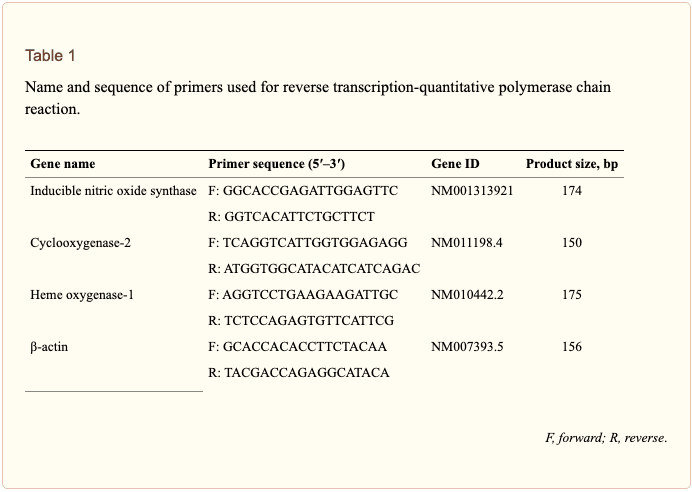
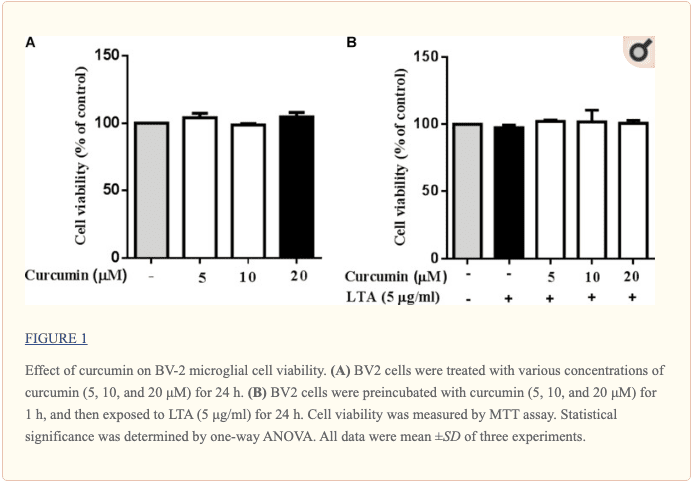
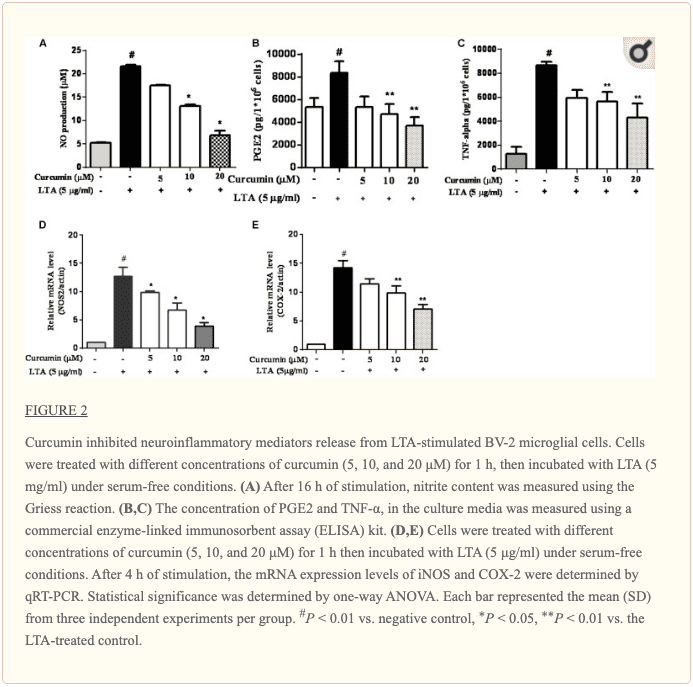
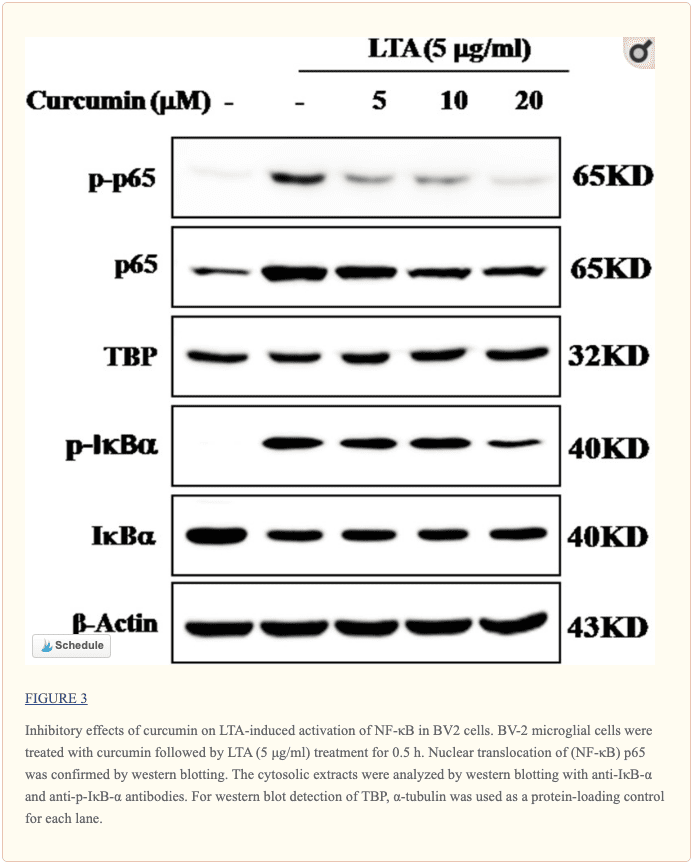
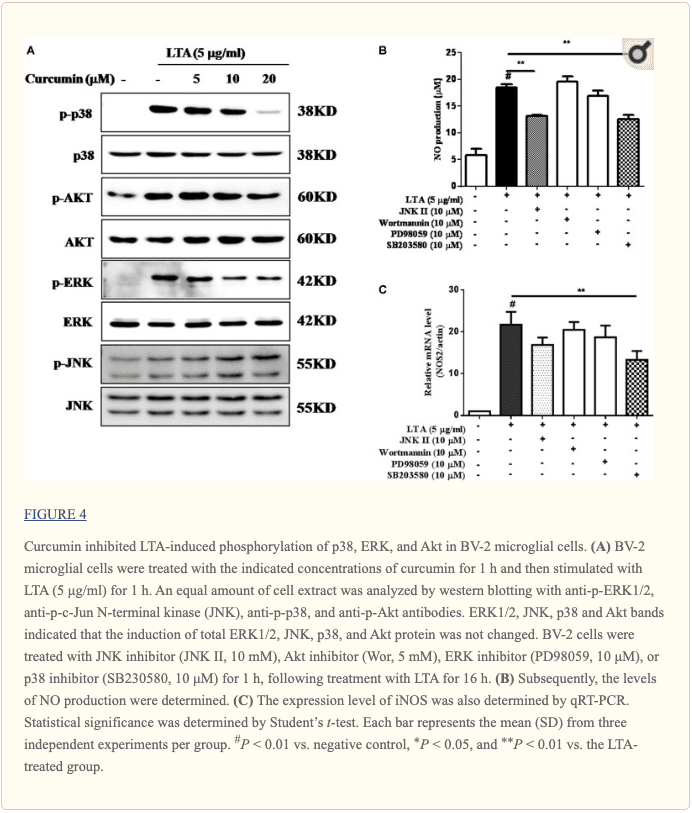
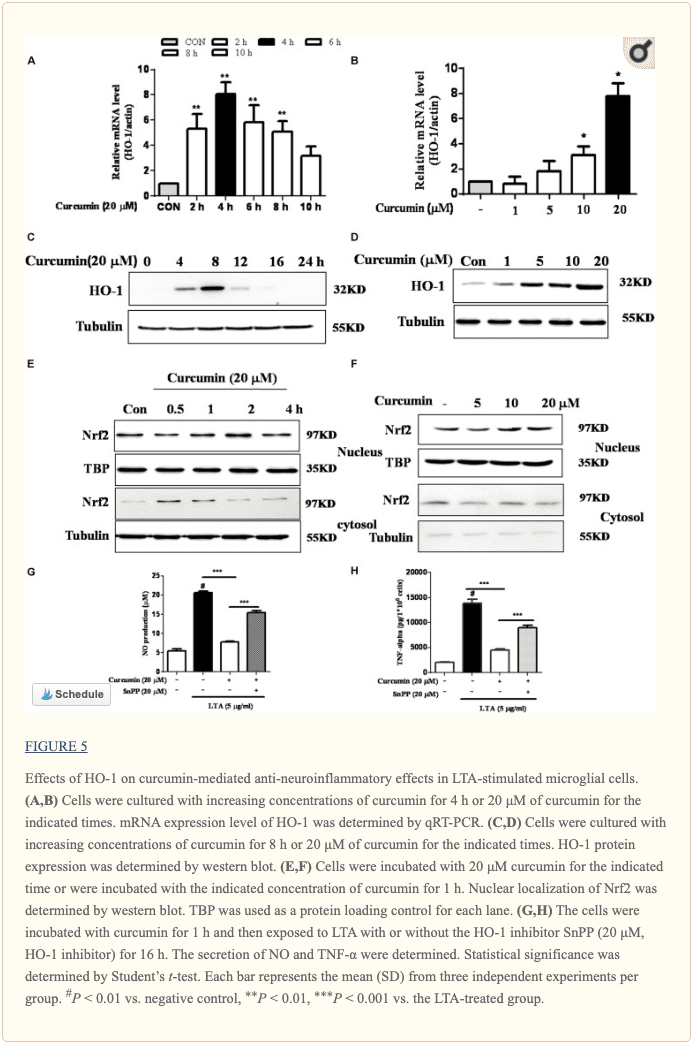
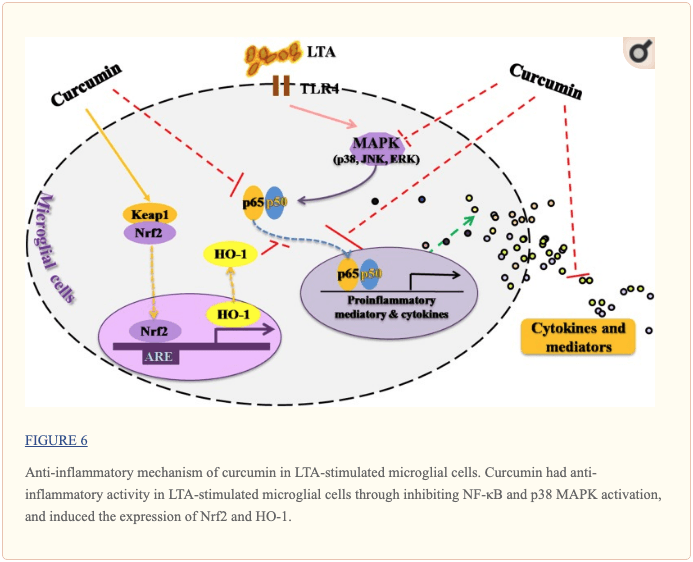 �
�