Should you be worried about that nagging neck pain that’s been bothering you for the previous couple of days? If you wait until it goes away or do you call a doctor and/or chiropractor?
It Could Be A Muscle Strain
Did you lift something heavy recently? Or maybe you slept wrong on your neck last night? If that’s the case, your neck muscles may have been hyperextended (you stretched them past normal range), which may be causing stiffness. Muscle strains on your neck usually are not severe, but that isn’t always true. Watch your symptoms over the next few days.�If they get worse, call your doctor or chiropractor.
It Could Be Whiplash
Whiplash can cause acute neck pain, which means your pain and soreness lasts a few days or weeks. It usually goes away by itself. If you notice that your pain is getting worse or develop other symptoms, i.e. weakness, numbness, and tingling, call your doctor right away.If you have been in an auto accident, it’s important to get checked out. Sometimes ligaments can stretch and lead to spine problems.
It Could Be Poor Posture
If you’re sitting hunched over a desk all day, tight neck muscles may be causing your neck pain. Chronically tense muscles never get a break, so work with a chiropractor, physical therapist or personal trainer who will teach you easy neck exercises in addition to how to keep good posture. Also, take frequent stretch breaks throughout the afternoon, and elevate your monitor so you don’t need to hunch over it.
It Could Be A Herniated Or Bulging Disc
For those who have neck pain that does not go away even with rest, it might be a herniated or bulging disc. This usually means an intervertebral disc in your cervical spine (neck) may be pressing on a nerve, which could be causing pain. Or it may lead to pain down your arm and into your hand. Let your physician or chiropractor know if you experience these symptoms.
When To Call Your Doctor
Call your doctor immediately if your neck pain becomes worse and you develop other symptoms, including tingling, weakness, dizziness, or loss of bowel or bladder control. It’s far better to be safe when it comes to your neck health. The bottom line is that you never really know whether that neck pain is severe or not, so don’t be afraid to talk about your health.
Question: My car was rear-ended. Since then, my neck hurts, feels rigid, and I have upper back pain. My wife says it’s whiplash and that I should see a physician. Is there anything that I can do to accelerate my recovery? Should I see my physician and/or chiropractor? How long will my pain last?
El Paso, TX
Answer: Your symptoms are typical of a whiplash injury caused by a vehicle accident. Whiplash is cervical spine strain caused when the head and neck are thrust quickly forward and backward. To fully grasp how whiplash can lead to neck pain, you want to recognize the head, which weighs 8-13 pounds and is supported and moved by the neck. Because of this, it’s easy to understand how soft neck muscles and ligaments are stretched during a whiplash accident!
The seriousness of whiplash is dependent on the force of the impact, the way you were seated in your vehicle, and if you were properly restrained with a shoulder and seat belt. By way of instance, if your head was turned, your neck injury may be more painful.
Whiplash Home Treatment Tips
1. Even though your neck injury occurred last week, you may try ice and heat. Ice will help to reduce swollen overstretched muscles and ligaments. Heat increases circulation and eases tight stiff muscles.
Ice: Apply an ice pack for 15 minutes as often as once each hour.
Heat: Apply warmth (moist is greatest!) For 15 minutes every 2 or 3 hours.
Skin Safety:
Never sleep with a ice or heat pack!
Wrap heat or ice in a towel to protect your skin.
Discard punctured store-bought ice or heat products.
2. If your doctor agrees, try an over-the-counter anti-inflammatory medication.
3. Move your neck softly to assist in preventing additional stiffness.
4. Should you work in a computer or desk, take regular breaks to relax your neck muscles.
5. Avoid cradling the phone between your shoulder and head.
6. Avoid carrying heavy packages, especially things such as a pocket book or backpack slung over only one shoulder.
Check With Your Doctor & Chiropractor
Neck pain is common either immediately after or several days following a whiplash injury. Other symptoms can develop too. Fortunately, most symptoms go away in two to four weeks. If your symptoms worsen, or you develop headache, dizziness, blurred vision, difficulty swallowing, arm or hand numbness, check-in with your physician or chiropractor. If necessary, you’ll be referred to a spine specialist.
Your physician or chiropractor will carry out a physical and neurological examination, and acquire a neck X-ray. After they produce a diagnosis, treatment is coordinated for your recovery! Treatment may include prescription pain medication, anti inflammatory drugs, muscle relaxants, a cervical collar, massage and physical therapy.
Other�Symptoms Associated With Whiplash Or Neck Strain:
Headache
Dizziness
Ringing in your ears
Blurred vision
Difficulty concentrating
Difficulty chewing or swallowing
Hoarse voice
Upper back, shoulder, and/ or arm pain
Back pain
Abnormal sensations such as numbness, burning or prickling
Fatigue and sleep problems
Keep in Mind
Most individuals with whiplash improve quickly within a matter of weeks. When you have concerns, we recommend you to speak to a doctor or chiropractor.
Editors Note: The information provided here was forwarded to Planet Chiropractic by a chiropractor in Texas. Far too many people (including chiropractors) are not aware of historical events that took place during the 1917 � 1918 Spanish Flu years, which involved chiropractors caring for thousands that suffered influenza infection during those times. With such a firestorm of media coverage and fear surrounding the Swine Flu Pandemic, it would be irresponsible not to attempt seeking knowledge regarding influenza events of the past.
The Official History of Chiropractic in Texas By Walter R. Rhodes, DC
Published by the Texas Chiropractic Association � 1978
CHAPTER VI: THE THREE GREAT SURVIVAL FACTORS [Excerpts by Dan Murphy, DC]
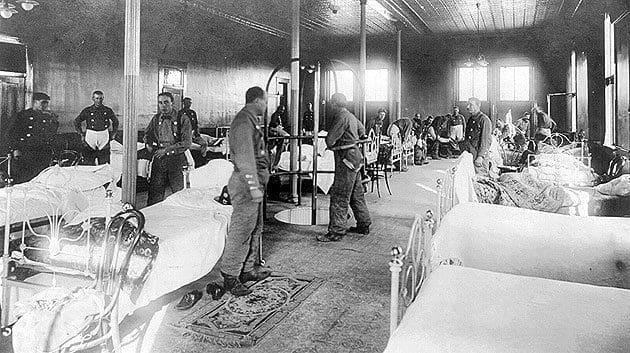
�The 1917 � 1918 influenza epidemic swept silently across the world bringing death and fear to homes in every land. Disease and pestilence, especially the epidemics, are little understood even now and many of the factors that spread them are still mysterious shadows, but in 1917-1918 almost nothing was known about prevention, protection, treatment or cure of influenza. The whole world stood at its mercy, or lack of it.�
�But out of that particular epidemic, the young science of chiropractic grew into a new measure of safety. While many struggles would lie ahead this successful passage of the profession into early maturity assured its immediate survival and made the eventual outcome of chiropractic a matter for optimism. If there had been any lack of enthusiasm among the doctors of chiropractic, or a depleting of the sources of students then the epidemic took care of them too. These chiropractic survivors of the flu epidemic were sure, assured, determined, and ready to fight any battle that came up. The effect of the epidemic becomes evident in interviews made with old-timers practicing in those years. The refrain comes repeatedly,�
�I was about to go out of business when the flu epidemic came � but when it was over, I was firmly established in practice.�
�Why? The answer is reasonably simple. Chiropractors got fantastic results from influenza patients while those under medical care died like flies all around.� �Statistics reflect a most amazing, almost miraculous state of affairs. The medical profession was practically helpless with the flu victims but chiropractors seemed able to do no wrong.�
�In Davenport, Iowa, 50 medical doctors treated 4,953 cases, with 274 deaths. In the same city, 150 chiropractors including students and faculty of the Palmer School of Chiropractic, treated 1,635 cases with only one death.�
�In the state of Iowa, medical doctors treated 93,590 patients, with 6,116 deaths � a loss of one patient out of every 15. In the same state, excluding Davenport, 4,735 patients were treated by chiropractors with a loss of only 6 cases � a loss of one patient out of every 789.�
II.
�National figures show that 1,142 chiropractors treated 46,394 patients for influenza during 1918, with a loss of 54 patients � one out of every 886.�
�Reports show that in New York City, during the influenza epidemic of 1918, out of every 10,000 cases medically treated, 950 died; and in every 10,000 pneumonia cases medically treated 6,400 died. These figures are exact, for in that city these are reportable diseases.�
�In the same epidemic, under drugless methods, only 25 patients died of influenza out of every 10,000 cases; and only 100 patients died of pneumonia out of every 10,000 cases. This comparison is made more striking by the following table:�
Influenza Cases Deaths � Under medical methods � Under drugless methods �In the same epidemic reports show that chiropractors in Oklahoma treated 3,490 cases of influenza with only 7 deaths. But the best part of this is, in Oklahoma there is a clear record showing that chiropractors were called in 233 cases where medical doctors had cared for the patients, and finally gave them up as lost. The chiropractors saved all these lost cases but 25.�
�Statistics alone, however, don�t put in that little human element needed to spark the material properly. Dr. S. T. McMurrain [DC] had a makeshift table installed in the influenza ward in Base Hospital No. 84 unit stationed in Perigau, in Southwestern France, about 85 kilometers from Bordeaux [during WWI]. The medical officer in charge sent all influenza patients in for chiropractic adjustments from Dr. McMurrain [DC] for the several months the epidemic raged in that area. Lt. Col. McNaughton, the detachment commander, was so impressed he requested to have Dr. McMurrain [DC] commissioned in the Sanitary Corps.�
III.
�Dr. Paul Myers [DC] of Wichita Falls was pressed into service by the County Health Officer and authorized to write prescriptions for the duration of the epidemic there � but Dr. Myers [DC] said he never wrote any, getting better results without medication.�
Dr. Helen B. Mason [DC], whose �son, when only a year old, became very ill with bronchitis. My husband and I took him to several medical specialists without any worthwhile results. We called a chiropractor, as a last resort, and were amazed at the rapidity of his recovery. We discussed this amazing cure at length and came to the decision that if chiropractic could do as much for the health of other individuals as it had done for our son we wanted to become chiropractors.�
Dr. M. L. Stanphill [DC] recounts his experiences: �I had quite a bit of practice in 1918 when the flu broke out. I stayed (in Van Alstyne) until the flu was over and had the greatest success, taking many cases that had been given up and restoring them back to health. During the flu we didn�t have the automobile. I went horseback and drove a buggy day and night. I stayed overnight when the patients were real bad. When the rain and snow came I just stayed it out. There wasn�t a member of my family that had the flu.�
When he came to Denison he said: �I had a lot of trouble with pneumonia when I first came. Once again took all the cases that had been given up. C. R. Crabetree, who lived about 18 miles west of Denison, had double pneumonia and I went and stayed all night with him and until he came to the next morning. He is still living today. That gave me a boost on the west side of town.�
�And when interviews of the old timers are made it is evident that each still vividly remembers the 1917-1918 influenza epidemic. We now know about 20 million persons [recent estimates are as high as 100 million deaths] around the world died of the flu with about 500,000 Americans among that number. But most chiropractors and their patients were miraculously spared and we repeatedly hear about those decisions to become a chiropractor after a remarkable recovery or when a close family member given up for dead suddenly came back to vibrant health.�
�Some of these men and women were to become the major characters thrust upon the profession�s stage in the 20�s and 30�s and they had the courage, the background and the conviction to withstand all that would shortly be thrown against them� [including being thrown in jail for practicing medicine without a license].
�The publicity and reputation of such effectiveness in handling flu cases also brought new patients and much acclaim from people who knew nothing of chiropractic before 1918.�
IV.
�The first survival factor for chiropractic: they were the legal and legislative salvation. But the fabulous success of chiropractic in combating the 1917-1918 influenza outbreak was the public relations breakthrough that can certainly be called the second great survival factor. Better acceptance by the public followed and more patients meant financial safety for practicing chiropractors. Dedicated chiropractors came into the profession in increasing numbers and they had a sure sense of certainty, heady conviction, and a great willingness to fight for the cause.�
Other Texas Chiropractic History (view more at chirotexas.com)
1916 � Texas State Chiropractic Association Formed
1916 � First TSCA annual convention held at the St. Anthony Hotel in San Antonio
1917 � First chiropractic bill introduced into Texas Legislature
1923 � Second chiropractic bill introduced into Texas Legislature
The Narrative Of JFK Shows The Difficulty In Diagnosing & Treating Spinal Disorders.
At age 43, John F. Kennedy was the youngest president elected into U.S. workplace, and has been depicted as full of youth and vitality. But he was far from healthy, and spent most of his adult life fighting with many medical issues, including back pain which started during college and continued until his death, according to a recent review article from the Journal of Neurosurgery: Spine.
John F. Kennedy’s back pain is thought to have started following a football injury, while Kennedy was in undergraduate school at Harvard, clarified coauthor Justin T. Dowdy, MD, who is a neurosurgeon at Hot Springs Neurosurgery Clinic, in Hot Springs, Arkansas.
Based on 10 years of study on Kennedy’s medical documents and reported symptoms, senior author T. Glenn Pait, MD, believes Kennedy had discogenic disease stemming from an accident in his childhood that began a cascade of problems in his low back. Dr. Pait is Director of the Jackson T. Stephens Spine and Neurosciences Institute at the University of Arkansas for Medical Sciences.
Kennedy was originally rejected when trying to enlist in the Army due to his medical issues, such as back pain, but was eventually accepted in the U.S. Naval Reserve during his dad’s connections. “This is a testament to his decision to serve his country,” Dr. Pait said. “Kennedy was originally given a desk job, but that was not enough for him, and he was later admitted into a patrol torpedo program.”
Kennedy’s back issues worsened when his naval boat was hit by a Japanese destroyer, and Kennedy drifted for 5 hours to a nearby island while towing an injured crewman to shore by holding the ring of the man’s life jacket between his teeth, Drs. Dowdy and Pait noted in their newspaper.
The review article refers to a series of 4 ineffective surgeries, including a sacroiliac (SI) and lumbosacral fusion. Various doctors who treated Kennedy had different theories about the reason for his back pain, also suggested a variety of different treatments ranging from trigger point injections and an exercise program (swimming and weight lifting), to massage and a back brace, to methamphetamine-containing shots. The exercise program, started later in his life, produced “dramatic” improvement, according to the researchers. The program consisted of weight lifting three times each week and everyday swimming plus massage and heat therapy.
“JFK’s narrative illustrates the difficulty and complexity in diagnosing and treating spinal disorders, especially in the context of chronic pain,” Dr. Dowdy advised SpineUniverse. “Our spines age as we age if it’s degenerative disk disease, pinched nerves, or spinal stenosis–imaging abnormalities are certain to appear later in life. Treating and preventing these disorders is just as much of an art as it’s a science, particularly in determining those individuals who will probably benefit from surgery.”
Dr. Dowdy noted that much progress has been made in how spinal conditions are diagnosed and treated as the time when Kennedy sought attention, such as “that the refinement of both less-invasive spine surgery methods and diagnostic imaging.” Dr. Dowdy also emphasized an important point that applies to any era: “the significance of having a trusted spine surgeon who is prepared and capable of supplying the right surgery in the appropriate conditions.”
John F. Kennedy’s story also suggests that “the most beneficial methods to prevent chronic back pain may be accessible and affordable,” Dr. Dowdy stated. “Often the most appropriate strategy for chronic low back pain is actively pursuing proper spine hygiene: maintaining healthy body weight, refraining from smoking, and pursuing a nutritious diet and exercise–especially workouts comprising yoga-style stretches,” Dr. Dowdy emphasized. “It boils down to pursuing a healthy and active way of life.”
“Individuals who suffer from chronic pain may hopefully be inspired to know that Kennedy remained physically energetic and driven to accomplish his goals despite his annoyance,” Dr. Dowdy concluded.
Backpack pain is an all too common condition of school-age children. While back pain is a known and widely-studied issue in adults, its prevalence in school-aged children has received relatively little scientific attention. Elementary, middle, and high school students must often carry backpacks that weigh enough to trigger chronic back pain, bad posture, and even decreased lung volume. I have written about this issue earlier, but lately, several studies reveal the truths behind childhood back pain and ways to mitigate it.
Are Backpacks Too Heavy For Kids?
Recent research supports that children carrying backpack loads of over ten percent of their body weight have a greater chance of creating back pain and related difficulties. An global study found that an alarmingly large percentage of school-age kids in Australia, France, Italy, and the United States often carried backpacks weighing more than the ten percent threshold.
In a second study involving a sample of 1540 metropolitan school-aged children, more than a third of the children surveyed reported backpack pain. Along with carrying heavy backpacks, female students and those diagnosed with scoliosis had a larger association with back pain pain. Children with access to lockers reported less pain.
The number of straps on the back had little effect on the respondent’s replies. Children also reported restricted physical activity due to back pain, and some took drugs to alleviate the pain.
Girls who transported bags in addition to wearing a backpack reported considerably greater back pain. Adolescents with back pain spent more time watching television than their peers. More than 80 percent of the surveyed thought that carrying a heavy backpack due to their back pain.
Backpack Pain Solutions
The research revealed several things that might help reduce back pain in school-aged children. The best way to prevent back pain is to refrain from carrying heavy loads.
Kids ought to make the most of locker breaks and only carry items necessary for a couple of courses at one time. When lifting a back pack, children should crouch down and bend their knees rather than curve the spine.
Backpack Safety
Appropriate Backpack Carrying Techniques
While not conclusive, research also supports that carrying the weight otherwise, e.g., by hand rather than by back pack, may help stop or reduce back pain. The American Occupational Therapy Association and the American Chiropractic Association provide these additional safe backpack etiquette tips:
Children should avoid carrying over 10 percent of the bodyweight in their backpack. For instance, an 8th-grader weighing 120 pounds should take no more than 12 lbs.
Place the heaviest objects at the back of the pack.
Make sure the items fit as snugly as possible to minimize back pain due to shifting weight.
Adjust the shoulder straps so they fit snugly over your kid’s shoulders and the back pack doesn’t drag your child backward. The bottom of the pack ought to be less than four inches under your child’s waist.
Children should avoid carrying backpacks slung over one shoulder, as it could cause spinal pain and general discomfort.
Encourage your child to carry only necessary items in their own backpack. Extra items can be carried in hand.
Look for backpacks with useful features like multiple compartments for even weight distribution, cushioned straps to protect the neck and shoulders, and waist belt.
If your child’s school permits, think about a roller pack, which rolls on the floor like luggage.
If problems persist, talk to your child’s teacher or principal about implementing paperback textbooks, lighter materials, or electronic versions.
Chiropractic, Massages & Spinal Injections Are Your Papal Prescription For Low Back & Leg Pain.
Should you suffer from the low back and leg symptoms of sciatica, the pope feels your pain. Reports reveal that Pope Francis has spent part of his 2017 summer undergoing spinal shots and massage therapy to help manage his sciatica.
Sciatica is intense low back and leg pain which runs along the course of the sciatic nerve, that is the longest and largest nerve in the human system. The sciatic nerve extends from your low back all the way down to a foot. Several spinal ailments can irritate the sciatic nerve and cause sciatica, including a herniated disc, lumbar spinal stenosis, spondylolisthesis, and trauma (you can read more in common sciatica causes). The root reason for Pope Francis’ sciatica is unclear.
The 80-year-old pope has suffered from sciatica for many years, having first remarked on his struggle with it in a 2013 through a media conference when he said, “Sciatica is very painful, very painful! I don’t wish it on anyone!”
More recently, the pope has received epidural steroid shots and massages twice a week to handle his back pain pain, according to the Italian news magazine Famiglia Cristiana.
Sciatica PSA
How Spinal Injections & Massage Can Help Relieve Sciatica
Pope Francis’ routine of epidural steroid injections and massages underscores the fact that while the pain of sciatica can be extreme–almost indescribable–spine operation isn’t always the answer. The pope’s non-surgical approach to sciatica pain management is one that many individuals suffering from the illness adopt.
With epidural steroid shots, strong anti-inflammatory drugs known as corticosteroids are injected near the spinal nerve roots. The therapy works with varying success, but some people experience decreased pain for months following an injection.
With massage, a therapist can target the muscle tension that may be compressing the sciatic nerve or associated nerve roots. Deep tissue massage treatment may be type of massage used, since it utilizes direct pressure and friction to release the pressure in the soft tissues (ligaments, tendons, muscles) surrounding the sciatic nerve.
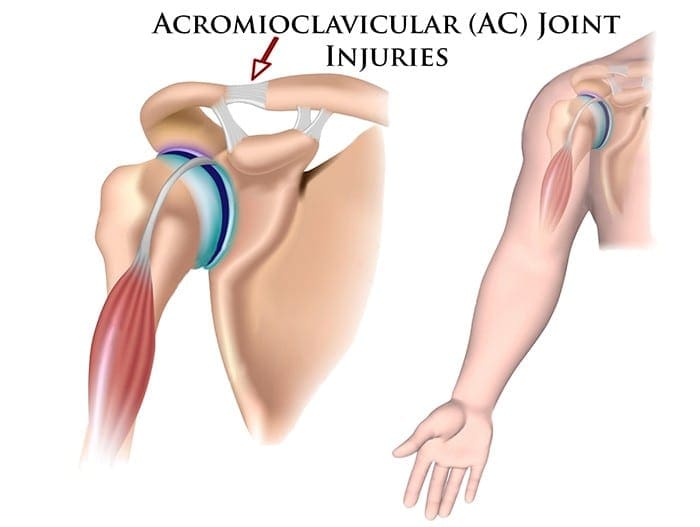
Two surgeons discuss the diagnosis and treatment of acromioclavicular injuries in athletes. El Paso, TX. Chiropractor, Dr. Alexander Jimenez follows the discussion.
Acromioclavicular (AC) joint injuries most often occur in athletic young adults involved in collision sports, throwing sports, along with overhead activities like upper-extremity strength training. They account for 3% of all shoulder injuries and 40% of shoulder sports injuries. Athletes in their second and third decade of life are more often affected(1), and men are injured more commonly than women (5:1 to 10:1)(1,2).
Acromioclavicular dislocation was known as early as 400 BC by Hippocrates(3). He cautioned against mistaking it for glenohumeral (shoulder joint) dislocation and advocated treating with a compressive bandage in an attempt to hold the distal (outer) end of the clavicle in a diminished position. Almost 600 decades later Galen (129 AD) recognized his own acromioclavicular dislocation, which he sustained while wrestling(3). He left the tight bandage holding the clavicle down as it was too uneasy. In today’s era this injury is better known, but its treatment remains a source of fantastic controversy.
Anatomy
The acromioclavicular joint combines the collarbone to the shoulder blade and therefore links the arm to the axial skeleton. The articular surfaces are originally hyaline cartilage, which affects to fibrocartilage toward the end of adolescence. The average joint size is 9mm by 19mm(4). The acromioclavicular joint contains an intra-articular, fibrocartilaginous disc which may be complete or partial (meniscoid). This helps absorb forces in compression. There is marked variability in the plane of the joint.
Stabilizers
There is little inherent bony stability in the AC joint. Stability is provided by the dynamic stabilizers — namely, the anterior deltoid muscle arising from the clavicle and the trapezius muscle arising from the acromion.
Additionally, there are ligamentous stabilizers. The AC ligaments are divided into four — superior, inferior, anterior and posterior. The superior is most powerful and blends with muscles. The acromioclavicular ligaments contribute around two- thirds of the constraining force to superior and posterior displacement; however, with greater displacement the coracoclavicular ligaments contribute the major share of the resistance. The coracoclavicular ligament consists of the conoid and trapezoid. The conoid ligament is fan-shaped and resists forwards motion of the scapula, while the more powerful trapezoid ligament is level and resists backward movement. The coracoclavicular ligament helps bunch scapular and glenohumeral (shoulder joint) motion and the interspace averages 1.3 cm.
Mechanism Of Injury
The athlete who sustains an acromioclavicular injury commonly reports either one of two mechanisms of harm: direct or indirect.
Direct force: This is when the athlete falls onto the point of the shoulder, with the arm usually at the side and adducted. The force drives the acromion downwards and medially. Nielsen(5) found that 70 percent of acromioclavicular joint injuries are caused by an direct injury.
Indirect force: This is when the athlete falls onto an outstretched arm. The pressure is transmitted via the humeral head into the acromion, therefore the acromioclavicular ligament is disrupted and the coracoclavicular ligament is stretched.
On Examination
The athlete presents soon after the severe injury with his arm splinted to his side. The patient may state that the arm feels better using superiorly directed support on the arm. Most motions are limited secondary to pain near the top of the shoulder; the degree varies with the grade of sprain. The hallmark finding is localized swelling and tenderness over the acromioclavicular joint.
In dislocations, the outer part of the collarbone will appear superiorly displaced using a noticeable step deformity (in fact, it is the shoulder which sags beneath the clavicle). Occasionally, the deformity may only be apparent later, if first muscle spasm reduces acromioclavicular separation. Forced cross-body adduction (yanking the affected arm across the opposite shoulder) provokes discomfort. The clavicle can frequently be moved relative to the acromion.
Acromioclavicular Visualisation
The typical joint width measures 1-3mm. It’s regarded as abnormal if it is more than 7mm in men, and 6mm in women. Routine anteroposterior views of the shoulder reveal the glenohumeral jointnonetheless, that the acromioclavicular joint is over penetrated and so dark to interpret. Reduced exposure enhances visualization. The individual stands with both arms hanging unsupported, both acromioclavicular joints on one film. Weighted viewpoints (stress X-rays) are obtained with 10-15 lb weights not held but suspended from the individual’s wrists. They help differentiate type II-III injuries, but are of little clinical significance and therefore are no longer recommended in our practice.
Classification Of AC Separation
The importance of identifying the injury kind can’t be over emphasized because the treatment and prognosis hinge on an accurate diagnosis. The injuries are graded on the basis of that ligaments are injured and how badly they’re torn.
Allman (6) classified acromioclavicular sprains as grades I, II and III, representing respectively, no involvement, partial tearing, and total disruption of the coracoclavicular ligaments. More recently, Rockwood (1) has further classified the more severe injuries as standard III-VI.
The injuries are classified into six categories:
Type I This is the most common injury encountered. Only a mild force is needed to sustain such an injury. The acromioclavicular ligament is sprained with an intact coracoclavicular ligament. The acromioclavicular joint remains stable and symptoms resolve in seven to 10 days. This injury has an excellent prognosis.
Type II The coracoclavicular ligaments are sprained; however, the acromioclavicular ligaments are ruptured. Most players can return to their sport within three weeks. There is anecdotal evidence to suggest that steroid injections into the acromioclavicular joint speed up the resolution of symptoms, but this practice is not universal.
Type III The acromioclavicular joint capsule and coracoclavicular ligaments are completely disrupted. The coracoclavicular interspace is 25-100% greater than the normal shoulder.
Type IV This is a type III injury with avulsion of the coracoclavicular ligament from the clavicle, with the distal clavicle displaced posteriorly into or through the trapezius.
Type V This is type III but with exaggeration of the vertical displacement of the clavicle from the scapula-coracoclavicular interspace 100-300% greater than the normal side, with the clavicle in a subcutaneous position.
Type VI This is a rare injury. This is type III with inferior dislocation of the lateral end of the clavicle below the coracoid
Treatment
The treatment of acromioclavicular joint injuries varies based on the seriousness or grade of the injury.
Initial treatment: These can be quite painful injuries. Ice packs, anti-inflammatories plus a sling are utilized to immobilize the shoulder and then take the weight of the arm. As pain starts to subside, it is important to start moving the fingers, wrist and elbow to prevent shoulder stiffness. Next, it’s important to begin shoulder motion in order to stop shoulder stiffness.
Un-displaced injuries only require rest, ice, and then a slow return to activity over two to six weeks. Major dislocations require surgical stabilization in athletes if their dominant arm is involved, and if they participate in upper-limb sports
Type I & II: Ice pack, anti-inflammatory agents and a sling are used. Early motion based on symptoms is introduced. Pain usually subsides in about 10 days. Range-of-motion exercises and strength training to restore normal motion and strength are instituted as the patient�s symptoms permit. Some symptoms may be relieved by taping (taking stress off acromioclavicular joint). The length of time needed to regain full motion and function depends upon the severity or grade of the injury. The sport and the position played determine when a player can return to a sporting activity. A football player, who does not have to elevate his arm, can return sooner than a tennis or rugby player. When a patient returns to practice and competition in collision sports, protection of the acromioclavicular joint with special padding is important. A simple �doughnut� cut from foam or felt padding can provide effective protection. Special shoulder- injury pads, or off-the-shelf shoulder orthoses, can be used to protect the acromioclavicular joint after injury.
Some Type II injuries may develop late degenerative joint changes and will need a resection of the distal end of the clavicle for pain relief. It is important to note that after a resection of the distal end of the clavicle, particularly in a throwing athlete, there may be formation of heterotopic bone on the under surface of the clavicle which can cause a painful syndrome which presents like shoulder impingement.
Type III: The treatment of type III injury is less controversial than in past years. In the 1970s, most orthopaedic surgeons recommended surgery for type III acromioclavicular sprains(7). By 1991, most type III injuries were treated conservatively(8). This change in treatment philosophy was prompted by a series of retrospective studies(9). These showed no outcome differences between operative and nonoperative groups.
What’s more, the patients treated non-operatively returned to full activity (work or athletics) earlier than surgically treated groups(10, 11). The exceptions to this recommendation include people who perform repetitive, heavy lifting, people who operate with their arms above 90 degrees, and thin patients who have prominent lateral ends of the clavicles. These patients may benefit from surgical repair(12).
Any discussion about the management of acute injuries to the AC joint must deal with which of the many methods of surgical therapy described is the best for their situation, but whether surgery should be considered at all. Surgery is generally avoided in athletes participating in contact sports since they will often re-injure the shoulder later on.
Type IV-VI: Account for more than 10-15% of total acromioclavicular dislocations and should be managed surgically. Failure to reduce and fix these will lead to chronic pain and dysfunction.
Surgery
Surgical repair can be divided into anatomical or non- anatomical, or historically into four types:
? Coracoclavicular repairs (Bosworth screws(13), cerclage, Copeland and Kessel repair).
? Distal clavicular excision.
? Dynamic muscle transfers.
? Disadvantages of surgery are that there are risks of infection, a longer time to return to full function and continued pain in some cases.
For the individual with a chronic AC joint dislocation or subluxation that remains painful after three to six months of closed treatment and rehabilitation, surgery is indicated to improve functioning and comfort.
For sequelae of untreated type IV-VI, or painful type II and III injuries, the Weaver Dunn technique is advocated. This�entails removing the lateral 2cm of the clavicle and reattaching the acromial end of the coracoacromial ligament to the cut end of the clavicle, thus reducing the clavicle to a more anatomical position.
Postoperatively, the arm is supported in a sling for up to six weeks. Following the first two weeks, the patient is permitted to use the arm for daily activities at waist level. After six weeks, the sling or orthosis is discontinued, overhead actions are allowed, formal passive stretching is instituted, and light stretching using elastic straps is initiated. Stretching and strengthening are begun slowly and gradually. The athlete shouldn’t return to their sport without restriction until full strength and range of motion has been recovered. This usually occurs four to six months following operation.
Conclusion
AC joint injuries are an important source of pain at the shoulder area and have to be assessed carefully. The management of these injuries is nonoperative in the majority of cases. Type I and II injuries are treated symptomatically. The present trend in uncomplicated type III injuries are a non operative strategy. In the event the athlete develops following problems, a delayed reconstruction might be undertaken. In athletes involved in heavy lifting or prolonged overhead activities, surgery may be considered acutely. Type IV-VI injuries are generally treated operatively.
No matter what kind of treatment is chosen, the ultimate purpose is to restore painless function to the wounded AC joint so as to reunite the athlete safely and as quickly as possible back to their sport. It is possible in the vast majority of acromioclavicular joint injuries.
References
Reza Jenabzadeh and Fares Haddad
1. Rockwood CA Jr, Williams GR, Young CD. Injuries of the Acromioclavicular Joint. In CA Rockwood Jr, et al (eds), Fractures in Adults. Philadelphia: Lippincott-Raven, 1996; 1341-1431.
2. Dias JJ, Greg PJ. Acromioclavicular Joint Injuries in Sport: Recommendations for Treatment. Sports Medicine 1991; 11: 125-32.
3. Adams FL. The Genuine Works of Hippocrates (Vols 1,2). New York, William Wood 1886.
4. Bosworth BM. Complete Acromioclavicular Dislocation. N Eng J Med 2 41: 221-225,1949.
5. Nielsen WB. Injury to the Acromioclavicular Joint. J Bone Joint Surg 1963; 45B:434-9.
6. Allman FL Jr. Fractures and Ligamentous Injuries of the Clavicle and its Articulation. J Bone Joint Surg Am 1967;
49:774- 784.
7. Powers JA, Bach PJ: Acromioclavicular Separations: Closed or Open Treatment? Clin Orthop 1974; 104 (Oct): 213-223
8. Cox JS: Current Methods of Treatment of Acromioclavicular Joint Dislocations. Orthopaedics 1992; 15(9): 1041-1044
9. Clarke HD, Mc Cann PD: Acromioclavicular Joint Injuries. Orthop Clin North Am 2000; 31(2): 177-187
10. Press J, Zuckerman JD, Gallagher M, et al: Treatment of Grade III Acromioclavicular Separations: Operative versus
Nonoperative Management. Bull Hosp Jt Dis 1997;56(2):77-83
11. Galpin RD, Hawkins RJ, Grainger RW: A Comparative Analysis of Operative versus Nonoperative Treatment of Grade III Acromioclavicular Separations. Clin Orthop 1985; 193 (Mar): 150-155
12. Larsen E, Bjerg-Nielsen A, Christensen P: Conservative or Surgical Treatment of AC Dislocation: A Prospective, Controlled, Randomized Study. J Bone Joint Surg Am 1986;68(4):552-555
13. Bosworth BM. Complete Acromioclavicular Dislocation. N Engl. J. Med. 241: 221-225,1949.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine



 It Could Be Poor Posture
It Could Be Poor Posture







 Are Backpacks Too Heavy For Kids?
Are Backpacks Too Heavy For Kids?