Before and after spine surgery the surgeon and medical staff prepare you for recovery. The recovery process can take a long time and be extremely challenging.
Pain after spine surgery is normal, but how to tell if it�s beyond the typical pain during recovery?
What indicates that the surgery failed?
Chiropractor Dr. Alex Jimenez has dealt with this issue throughout his career and discusses symptoms associated with failed back surgery syndrome (FBSS, also known as failed back surgery (FBS) or post-laminectomy syndrome).
Back Pain the most common symptom
Chronic back pain is the most common symptom from failed back surgery.
With FBSS, chronic pain in one patient can be very different from pain in another.
People with FBSS can experience a range of different types of pain based on:
Spinal disorder
Spinal procedure
The underlying cause of failed back surgery syndrome
Types of back and neck pain people with failed back surgery may experience. Some may have one or more types.
Chronic pain:
Sustained pain that lasts for more than 12 weeks.
Chronic pain is the opposite of acute pain, which is short-term�severe pain.
Acute pain is expected during spine surgery recovery but should fade during the healing.
Nociceptive pain:
Localized pain that can be dull or sharp.
This is the type of pain patients may experience immediately after surgery
Example: The pain felt around where the incision was made.
When most people think of pain, nociceptive pain is the type.
Neuropathic pain (neuropathy):
Nerve-related pain is caused by damage to the nerves or spinal cord.
Neuropathic pain shoots and moves around, thus affecting large areas of the body.
Examples of this type of pain include:
Numbness
Burning
Tingling
Weakness
Abnormal sensations (called paresthesia)
Radicular pain (radiculopathy):
A branch of nerve pain (neuropathy) is called radiculopathy, or radicular pain.
Radicular pain radiates from one area to another.
Examples include from the:
Low back
Down the buttocks
Legs
Feet
And then starts all over again, or goes in a different order.
Other symptoms:
The original symptoms return:
When the symptoms that put the patient in the surgery room return, then there is a definite possibility of failed back surgery.
New pain presents:
New pain, meaning pain in a different part of the spine or a different type merits a discussion with your doctor.
Mobility Reduced :
It does take time to recover and that process can affect:
Endurance
Flexibility
Movement
However, if mobility or limitation is different from what was talked about with the surgeon or develops after recovery, then it should be discussed with your doctor.
Example: A limited range of motion in the neck or low back.
Headaches begin to present:
If headaches were not an original part of your medical history, this may point to a nerve problem.
Nerve Symptoms & Quality of Life
Neuropathic pain/ neuropathy or nerve-related pain is the most complex, debilitating, and difficult-to-treat.
People who experience this type of pain find it lowers their quality of life.
An online survey of 1,000-2000 patients that underwent low back surgery responded and revealed the following:
94% of respondents reported post-surgery low back pain
A separate study noted that nerve-related pain suffered by people with FBSS is more life-altering than pain caused by joint and nerve disorders.
Patients with FBSS and neuropathic pain go through higher levels of pain and have less quality of life/physical function compared with people with osteoarthritis, rheumatoid arthritis, and fibromyalgia.
FBS Symptoms Emergency Treatment
After surgery, it can be difficult to tell whether the pain is within the bounds of normal recovery pain.
At follow-up appointments ask questions about the progress of your recovery and about any concerns.
Pain after surgery is normal, but there are some signs and symptoms that merit emergency attention.
If you experience any of the red flag symptoms, call your doctor immediately:
Symptoms of Failed Back Surgery Syndrome Are Different for Every Patient
Every patient goes through a unique surgical experience and if it fails, patients may experience unique symptoms.
Because failed back surgery has several possible causes, the symptoms are going to be different for each patient.
Before you are discharged and even before you go under, ask your surgeon questions about what to expect during the recovery process.
Educating yourself with possible expectations during recovery, you�ll be best positioned to know when things aren�t going as they should.
Low Back Pain Management El Paso, TX Chiropractor
Denise suffered an auto accident injury which resulted in back pain. When she realized she could not sit, walk or sleep for lengthy periods of time without having painful symptoms, Denise found chiropractic care with Dr. Alex Jimenez at El Paso, TX. Once she received therapy for her automobile accident injuries, Denise experienced relief from her symptoms and she was able to execute her regular tasks once again. Thanks to the education and maintenance Dr. Alex Jimenez supplied, Denise regained her initial health and health.
Back pain is more most common, with roughly nine out of ten adults undergoing it at some time in their lifetime, and five functioning adults developing it annually. Some quote around 95 percent of Americans will experience back pain at some time in their lifetime. It is undoubtedly the typical cause of chronic pain since it’s also a substantial contributor to missed work and handicap. In the United States alone, acute cases of lower back pain are the fifth most frequent reason for doctor visits and cause 40% of missed days off work. What’s more, it is the leading cause of disability worldwide.
NCBI Resources
Aside from the obvious invasiveness of the procedure as well as recovery time and probable physical therapy that would be required as part of your aftercare. Say you have neck or back pain. How will you treat it? Many people will go to a medical doctor who will look at the symptoms, such as pain, and treat it with a prescription or over the counter medications. In some cases, they may recommend surgery to manage the pain or correct the problem.
Say you have neck or back pain. How will you treat it? Many people will go to a medical doctor who will look at the symptoms, such as pain, and treat it with prescription or over the counter medications. In some cases, they may recommend surgery to manage the pain or correct the problem. But there is a safe and less expensive alternative. Chiropractic is the better choice over drugs and surgery!
An increasing number of people are foregoing the medical doctor and opting for chiropractic care for pain management � and often with excellent results. So, what is it about chiropractic that people feel makes it a better choice than drugs or surgery for their pain or mobility issues? There is more to the answer than you may realize.
Drug Therapy
When it comes to certain types of pain, particularly neck pain, medication is not the best way to manage it. Studies show that patients who opted to undergo chiropractic treatments and exercise regularly were more than twice as likely to significantly reduce their pain or even eliminate it entirely, compared to those who choose to take medication.
Aside from efficacy though, many medications have unpleasant and even dangerous side effects. Even over the counter medications can cause problems.
For instance, acetaminophen has been linked to serious health issues like pancreatitis and impaired liver function. NSAIDs like ibuprofen can upset the stomach and can cause rebound headaches in migraine patients (studies show that chiropractic is extremely effective in preventing migraines).
Prescription drugs can be highly addictive and lead to overdose. The Centers for Disease Control (CDC) has declared opioid addiction and overdose in the United States to be an epidemic. They have set forth guidelines for doctors who prescribe opioids for chronic pain, but the epidemic continues.
Surgery
Any treatment that can help a patient avoid invasive surgery is an optimal alternative, and chiropractic care provides that. One study shows that patients who saw a medical doctor as their first treatment option when dealing with back pain were more likely to have surgery than patients who say a chiropractor first.
Almost 43% of the medical patients eventually underwent surgery while only 1.5% of chiropractic patients had surgery. This means that if you are a medical patient trying to resolve your back pain you are 28 times more likely to eventually have surgery for it than you would if you went to a chiropractor.
Aside from the obvious invasiveness of the procedure as well as recovery time and probable physical therapy that would be required as part of your aftercare, there are many other downsides. The time and money necessary for the surgery, pre-surgery appointments, post-surgery appoints, recovery, and therapy can be significant.
However, a significant concern in hospital settings is the risk of C-diff (Clostridium difficile). C-diff is bacteria that can cause C. diff colitis, an inflammation of the colon or large intestine that can make you very sick. It can be passed from person to person but can also occur in people who take antibiotics � which are often given when a person undergoes surgery.
Chiropractic Care
Chiropractic care gets to the cause of the problem instead of treating the symptoms like most medical doctors. The whole-body approach also empowers patients to make lifestyle adjustments that aid in their care and healing. It allows them to take ownership of their health and pain management so that they feel more in control.
Chiropractors take a natural, holistic approach to pain management by bringing the body back into alignment if necessary and recommending exercises and other activities to help patients regain their normal range of motion and flexibility while relieving not only the pain symptoms but often correcting the problem that is causing the pain.
In the first part of this 2-part series, chiropractor, Dr. Alexander Jimenez looked at the likely signs and symptoms of disc Herniation, in addition to the selection standards for micro-discectomy surgery in athletes. In this report he discusses the lengthy rehab period following a micro-discectomy procedure, and provides a plethora of strength based exercises.
Surgeries to ease disc herniation, with or without nerve root compromise, comprise traditional open discectomy, micro-discectomy, percutaneous laser discectomy, percutaneous discectomy and micro- endoscopic discectomy (MED). Other surgical conditions are employed in The literature like herniotomy that’s interchangeable with fragmentectomy or sequestrectomy. The saying ‘herniotomy’ is defined as removal of the herniated disc fragment just, and the ‘standard discectomy’ as elimination of the herniated disc along with its degenerative nucleus in the intervertebral disc space.
When surgery is required, minimizing tissue disruption and strict adherence to an aggressive rehabilitation regimen may expedite an athlete’s return to perform(1), that explains why micro discectomy is a favored surgical procedure for athletes. Micro discectomy procedures entails Removing a small part of the vertebral bone over a nerve, or removing the fragmented disc stuff from under the compressed nerve root.
The surgeon can then enter the spine by removing the ligamentum flavum that insures the nerve roots. The nerve roots can be visualized with functioning eyeglasses or with an operating microscope. The surgeon will then move the nerve to your side and to subsequently remove the disc material from beneath the nerve root.
It’s also sometimes required to eliminate A small portion of the related facet joint to permit access into the nerve root, and additionally to relieve pressure on the nerve root resulting in the facet joint. This procedure is minimally invasive since the joints, muscles and ligaments are left intact, and the process doesn’t interfere with the mechanical construction of the spinal column.
Endoscopic Lumbar Discectomy
Local Doctor performs lumbar discectomy using minimally invasive techniques.�From the El Paso, TX. Spine Center.
Surgical Outcomes
In general, athletes with lumbar disc Herniation have a favorable prognosis with traditional therapy; more than 90 percent of athletes using a disc herniation improve with non-operative treatment. Many demonstrate a response to conservative treatment with increased pain and sciatica within 6 weeks of the initial onset(2). This implies that the requirement to function immediately could be considered hasty.
However, in case of failed Conservative therapy, or together with the pressure of a significant upcoming competition, surgery might be needed in some instances. Even though it involves surgical therapy, micro-discectomy has been reported to have a high success rate — over 90 percent in some studies(3,4). Patients generally have hardly any pain, are able to return to preinjury activity levels, and therefore are subjectively happy with their results.
The achievement rate of micro-discectomy is The following studies have been summarised to underline the success rate of micro-discectomy procedures:
1. In a survey on 342 professional athletes Diagnosed with lumbar disc herniation in sports like hockey, football, basketball and baseball, it was discovered that powerful return to perform occurred 82% of this time, and 81 percent of surgically treated athletes returned for an additional average of 3.3 years(5).
2. From a limb paresis which might be associated with a disc herniation following surgical treatment. If the preoperative paresis was mild then they could anticipate an 84% likelihood of full recovery. Patients with more severe paresis have less chance of recovery (55%)(6).
3. Wang et al (1999) in a study on 14 athletes demanding discectomy processes found that in single degree disc procedures, the return to game was 90%. However when the procedure involved 2 levels enjoyed considerably less favorable results(7).
4. In a study of 137 National Football League players with lumbar disc herniation, surgical treatment of lumbar disc herniation led to a significantly more career and greater return to play rate than those treated non-operatively(8).
5. Schroeder et al (2013) reported 85% RTP rates in 87 hockey players, with no substantial difference in outcomes or rates between the surgical and nonsurgical cohorts(9).
6. A study by Watkins et al (2003) coping with professional and Olympic athletes revealed the acceptable outcomes of micro-discectomy concerning return to play, since elite athletes in general were highly encouraged to return to perform(10). Also, athletes who had single-level micro- discectomy were more likely to come back to their original heights of sports activities than were people who’d two-level micro- discectomies.
7. A study by Anakwenze et al (2010) investigating open discectomy at National Basketball Association participants demonstrated that 75% of patients returned to perform again compared with 88 percent in control subjects who did not undergo the operation(11).
8. A recent review found that conservative therapy, or micro-discectomy, in athletes using lumbar disc herniation seemed to be satisfactory concerning returning the injured athletes into their initial levels of sports activities(12).
These studies conclude that though a Analysis of lumbar disc herniation has career-ending potential, most gamers have the ability to return to play and generate excellent performance-based outcomes, even if surgery is required.
What is also apparent from research Studies is the level of this disc herniation can also determine prognosis after surgery. Athletes shower a greater difference in progress between surgical and non-operative treatment for upper amount herniations (L2-L3 and L3-L4) compared to herniations at the L4-L5 and L5-S1 levels. Patients using the upper level herniations needed less progress with non-operative treatment and marginally better operative outcomes than those with lower degree herniations(13).
There are several possible explanations A range of studies have revealed that low spinal canal cross-sectional area is associated with an increased likelihood of symptomatic disc herniation, and increased intensity of herniation symptoms. The spinal cross-sectional region is the smallest (thus contains a larger possibility of nerve compromise) at the most upper posterior section and the cross-sectional region increases further down to the lower lumbar spine(14).
The location of the disc herniation�(foraminal, posterolateral or central) may also contribute to differences.�In this study, upper lumbar herniations were more likely to happen in the much lateral and foraminal positions than were people in the lower two intervertebral degrees(13).
Post-Surgical Rehab
After micro-discectomy surgery, the Small incision and restricted soft tissue injury makes it possible for the patient to be ambulatory reasonably fast, and they’re usually encouraged to start rehabilitation sooner or later during the 2-6 weeks after surgery.
In a review on the efficacy of busy Rehabilitation in patients following lumbar spine discectomy, it may be reasoned that individuals can safely take part in high or low-intensity supervised or home-based exercises initiated at 4 to 6 weeks following first-time lumbar discectomy(15).
Herbert et al (2010) discovered that with Effective post-surgical rehabilitation plans, there was a key accent on lumbar stabilisation exercises(16). Second, positive trials tended to initiate rehabilitation earlier in the postoperative interval compared to negative trials (about 4 vs 7 weeks).
Outcome Measures
The most widely used result Measure following back injury and/or disc surgery is the Oswestry Disability Questionnaire(17). This questionnaire is reported to have good levels of test-retest reliability, responsiveness, and also a minimum clinically important difference estimated as 6 percent(18) Furthermore, treatment success has been defined as a 50 percent decrease in the Modified Oswestry Disability Questionnaire score(19).
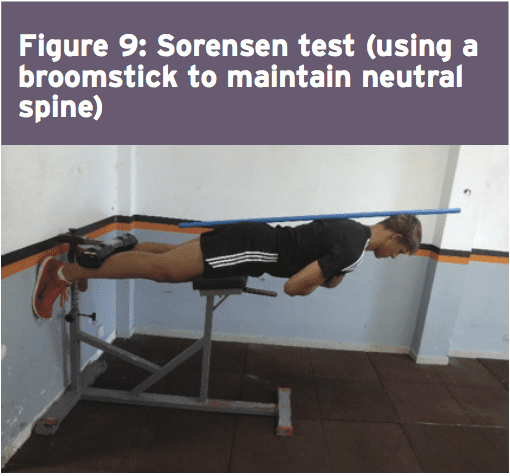
Concerning physical performance measures following back disc or pain operation, a commonly used clinical examination is that the Beiring-Sorensen Back Extension examination (see Figure 1)(20). This test is performed in a prone/horizontal body position with the spine and lower extremity joints at neutral position, arms crossed at the chest, lower extremities and pelvis supported with the top back unsupported against gravity.
Rehabilitation Program
Presented below is a five-stage rehabilitation program. The stages involved in rehabilitation are:
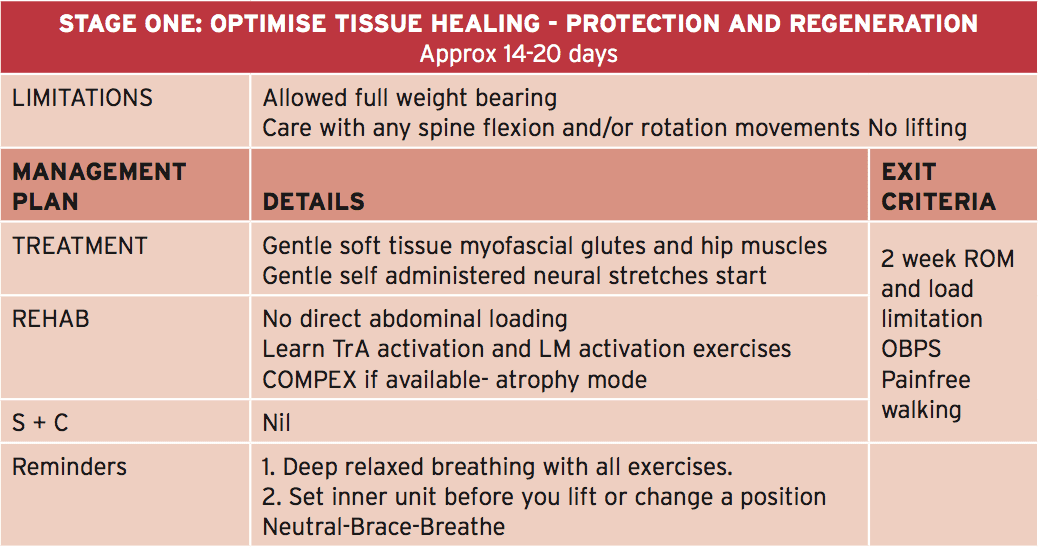
1. Optimize tissue healing — protection and regeneration
2. Early loading and foundation
3. Progressive loading
4. Load buildup
5. Maximum load
This program has been designed to get a field hockey player with had a L5/S1 lumbar spine discectomy. Even though the progressions from one point to the next are driven by the exit standards related to that stage, it might be anticipated that the athlete could progress in post-surgery to ‘fit to compete’ in about 12-13 weeks.
In this phase it’s anticipated that the athlete will remain relatively quiet for 2-3 weeks post surgery. This allows for full tissue recovery to happen, including scar tissue maturation. The athlete is allowed to completely mobilize in full weight-bearing; however care needs to be taken using any flexion and rotation motions and no lifting will be allowed.
The athlete can begin with the physiotherapist with the objective to manage any gluteal and lumbar muscle trigger points and start�nerve mobilization techniques that show how to engage the TrA and LM muscles (see Figures 2a and 2b).�If the physiotherapist has access to your muscle stimulator (Compex), then this can be utilized in atrophy manner on the lumbar spine multifidus and erector spinae. The key criteria to exit this early phase are curable walking as well as also an Oswestry Disability Score of 41-60%.
Early Loading & Foundation
The primary feature of this phase is that the athlete can start early and low-load strength exercises focusing on muscle activation in a neutral spine position, along with a progressive selection of motion program to improve lumbar spine flexion, extension and rotation. In this stage that the physiotherapist will guide the athlete through safe and gentle stretches to your hip quadrant muscles like the hip flexors, gluteals, hamstrings and adductors. The athlete also lasts gentle neuro-mobilization exercises to advance the freedom of the sciatic nerve — an issue in this condition as neurological tethering is a chance as a result of scar tissue formation caused by the surgical procedure.
The athlete can also be encouraged to start hydrotherapy in the form of walking in water (waist high) along with swimming fitnesscenter. In addition, he/she must start a string of low degree muscle activation drills in this stage (see Figure 3) that can be performed every day. This exercise teaches the athlete to hip flex (fashionable hinge) whilst maintaining a neutral spine. The neutral spine is maintained by using a light broomstick aligned with the back with the touch points being the occiput, the 6th thoracic vertebrae (T6) and the posterior sacrum.
Progressive Loading
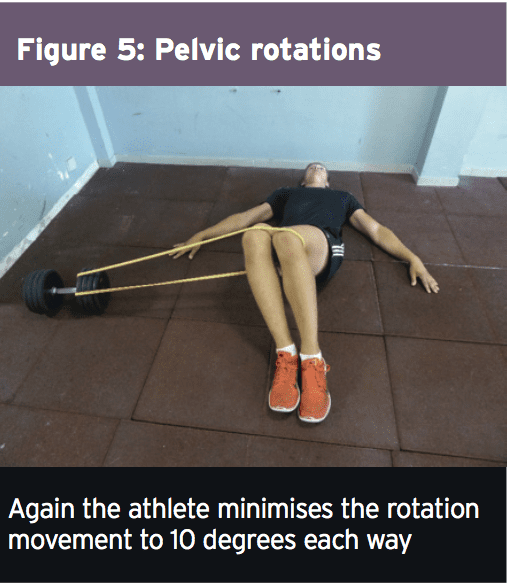
In this phase the athlete continues with a variety of movement progression along with the physiotherapist progresses manual therapy to the pelvis and lumbar spine. Neuro-mobilization techniques can also be progressed. The significant change in this phase is that the progression of load on many of the strength and muscle control exercises.�Two exercises here are the �standing twisties� and the �crook lying pelvic rotation� exercise (Figures 4 and 5).�These movements are the introductory spinning based movements. The primary progression about fitness drills is the athlete can begin pool running drills.
Load Accumulation
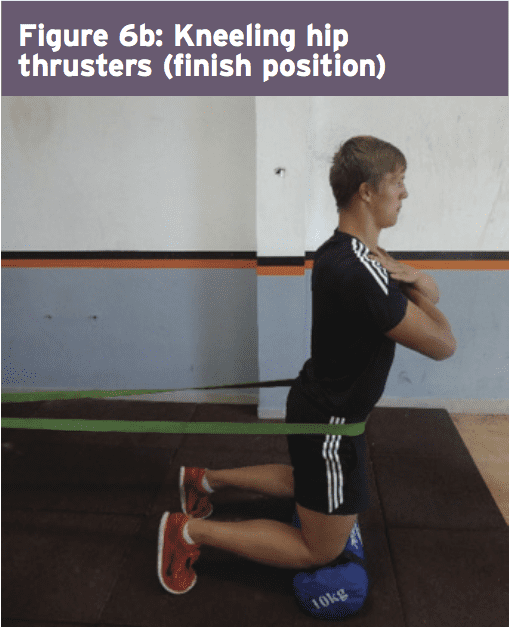
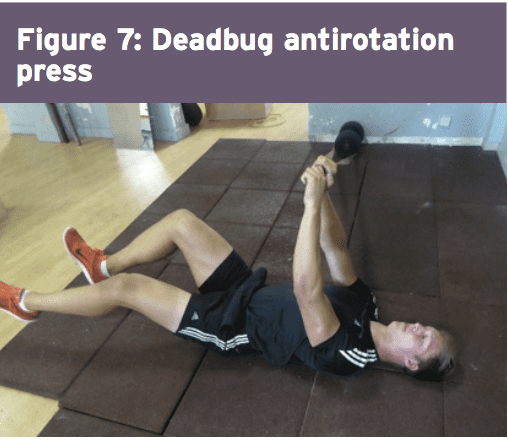
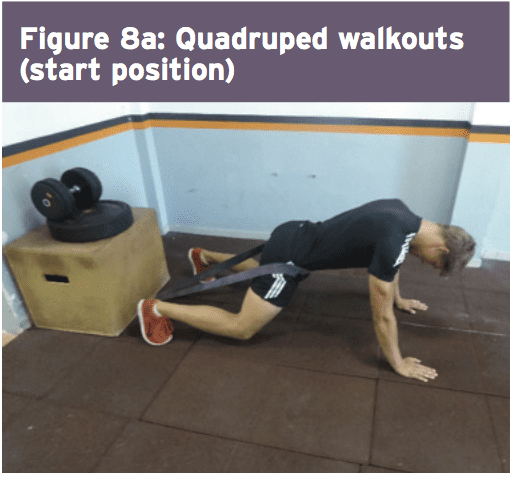
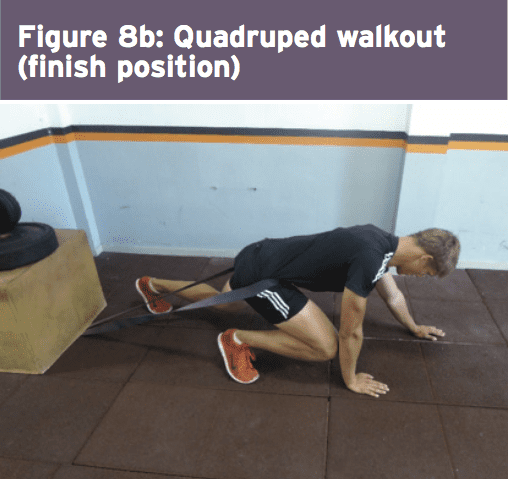
This is the stage where the athlete begins to advance the load in strength-based exercises. Resistance is used in the form of barbell load and band resistance. Three exceptional exercises performed here are the ‘kneeling hip thruster’, ‘deadbug antirotation press’ and also the ‘quadruped walkout’ (Figures 6-8 — explained in detail in the online database of exercises).
The athlete also begins running drills at this phase and it might be expected that as well as building running Amount, the athlete should progress over four weeks to close to full sprint speeds. This is also the stage whereby they would initiate mild to moderate sports special skills drills. Another characteristic of this stage is that the athlete starts the ‘Sorensen test’ exercise (Figure 9) and it will be expected that they can maintain the position for no less than 90 seconds before advancing to the next phase.
Maximum Load
In this final stage, the athlete spreads all core and strength exercises to maximum loads, and they work with the fitness trainer on coming to squat and functional fitness center lift movements. Skill progression can also be advanced alongside sprint and agility drills. The last exit standards prior to advancing to endless strength and training work is they have to keep the ‘Sorensen test’ for 180 seconds and their self documented Oswestry scale ought to be someplace between 0-20%.
Chiropractor, Dr. Alex Jimenez looks at lumbar spine disc herniation. What are the Likely signs and symptoms associated with disc herniation, and what would be the selection criteria for micro-discectomy operation in athletes? Complaint in the young college age athlete and professional athlete, and it’s been estimated that over 30% of athletes complain of back pain at least once in the profession(1).
Lumbar spinal disc herniation is one kind Of lumbar injury that can’t just cause painful low back pain, but can also compress nerve roots and create radicular referral of pain into the lower leg with related sensation changes and muscle contraction. This injury will not only influence the short-term opponent ability of the athlete, but might also reoccur and eventually become persistent possibly causing a career ending injury.
Managing disc herniation from the athlete Usually begins with conservative therapy and if this fails, surgical solutions are considered. But often elite athletes will request a quicker resolution to their symptoms to minimize time away from competitors. Therefore, providing the criteria for lumbar spine surgery are suggested, the conservative period will often be compressed, and surgery will be sought earlier. The favored surgical process for the athlete with a disc herniation is that the lumbar disc micro-discectomy.
Anatomy & Biomechanics
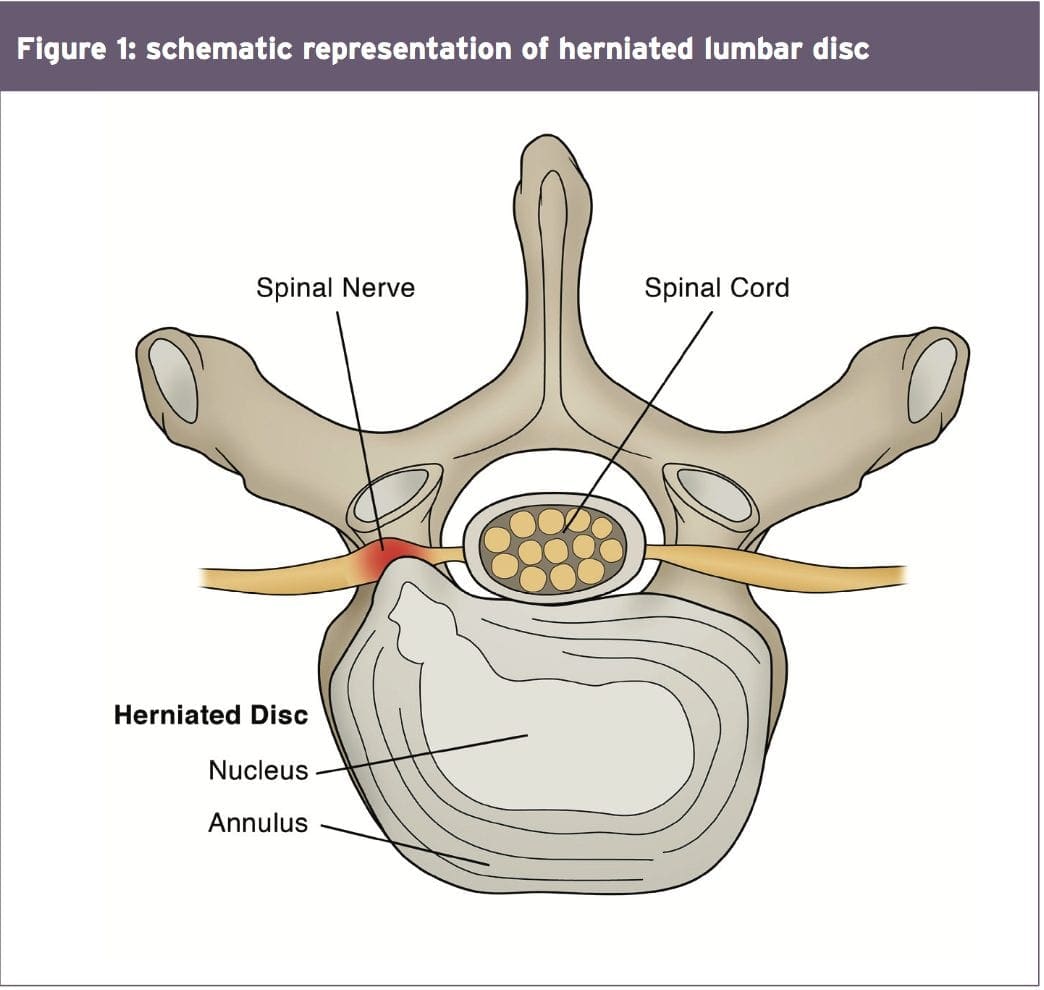
A significant biomechanical role in the spine, allowing for motion between the spinal segments while spreading compressive, shear, and torsional forces(2). These discs include a thick outer ring of fibrous cartilage termed the annulus fibrosis (akin to the onion rings enclosing the center of the onion), which encompasses a more gelatinous core called the nucleus pulposus, which is included within the cartilage end plates inferiorly and superiorly.
The intervertebral disc consists of Cells and substances such as collagen, proteoglycans, and thin fibrochondrocytic tissues, which enable transmission and absorption of forces arising from body weight and muscle activity. To do so, the disc depends mainly on the structural condition of the nucleus pulposus, annulus fibrosis and the vertebra lend plate. If the disc is normal and is functioning optimally, then forces are spread across the disc evenly(3).
But disc degeneration (mobile Degradation, lack of hydration( disc failure) may decrease the capacity of the disc to withstand extrinsic forces, as forces are no longer distributed and spread evenly. Tears and fissures from the annulus can lead, and with adequate external forces, the disc material may herniate. Alternatively, a sizable biomechanical force set on a healthy, ordinary disc may cause extrusion of disc material as a result of crushing failure of this annular fibers — illustrations include a hefty compression type mechanism because of a fall on the tailbone, or strong muscle contraction such as heavy weight lifting(4).
Herniations represent protrusions of Disc material beyond the confines of this annular lining and in the spinal canal (see Figure 1)(5). If the protrusion does not invade the canal or undermine nerve roots then back pain may be the only symptom.
Endoscopic Discectomy 3D Simulation
The pain associated with lumbar Radiculopathy happens due to a mix of nerve root ischemia (due to compression) and inflammation (because of neurochemical inflammatory mediators released from the disc). Throughout a herniation, the nucleus pulposus puts pressure on weakened regions of the annulus, and proceeds through the diminished websites in the annulus in which it ultimately forms a herniation(6 ft). It follows from this that some kind of disc degeneration may exist prior to the disc may really herniated(7).
In contrast to other respiratory Tissues, discs have a inclination to degenerate earlier in life, with some studies demonstrating adolescents presenting signs of degeneration between the ages of 11 to 16(8). With increasing age, there’s further degeneration of the intervertebral discs.
While the disc might be in danger of harm in All fundamental planes of motion, it’s particularly susceptible during repetitive flexion, or hyper-flexion, combined with lateral bending or rotation(10). Traumatic events such as excessive axial compression may also damage the inner structure of the disc. This can occur as a result of a fall or powerful muscular forces developed during tasks such as heavy lifting.
Athletes are generally exposed to high loading conditions. Examples of this include:
1. World-class power lifters, in which the calculated compressive loads on the backbone are involving 18800 Newtons (N) and also 36400N acting in the L3-4 motion segment(11).
2. Elite level football linesmen who have Been proven to present time-related hypertrophy of this disc and changes in vertebrae endplate in response to this repetitive high loading and axial pressure(12).
3. Long distance runners have been Shown to undergo significant strain into the intervertebral disc, indicated by a reduction in disc height(13).
Herniations could be classified depending on Ultimately, herniations are also identified based on level, with most herniations happening at the L4/5 and L5/S1 intervertebral disc level; these can then in turn affect the L5 and S1 nerve roots resulting in clinical sciatica(15). Upper level herniations are less common, and when they do occur with radiculopathy, they will affect the femoral nerve. Finally, the prevalence of disc injury rises increasingly caudally, with the best numbers at the L5/S1 degrees(16).
Herniation In Athletes
The offending movements implicated in The 20-35 age group are the most common group to herniate a disc, most likely because of the fluid nature of the nucleus pulposis and due to behavior(18). This age group are more likely to participate in sports which need high lots of flexion and spinning or are reckless with their positions and positions during loading.
The sports most at risk of disc herniation are:
Hockey
Wrestling
Soccer
Swimming
Basketball
Golf
Tennis
Weightlifting
Rowing
Throwing events
These are the sports that involve either significant Furthermore, those who take part in more and more severe training regimes seem to be at higher risk of spinal pathologies, as do people involved in sports.
Signs & Symptoms Indicating Discectomy
The efficacy of management programs for lumbar spine disc herniation — in terms of the decision to operate or treat conservatively — will be discussed in greater depth in part 2 of this series. However, the decision to operate within an athlete is generally driven by the motivation and approaching goals the athlete has put themselves. They may in fact favor a comparatively simple micro-discectomy instead of waiting for symptoms to abate through an extended period of rehabilitation.
This conservative period of Management may involve medicine therapy, epidural injections, relative back and back muscle recovery, acupuncture, osteo/chiropractic interventions. On the other hand, the normal presenting symptoms and signs that suggest a substantial disc herniation that will require surgical intervention in the athlete comprise:
Low back pain with pain radiating down one or both legs
Positive straight leg raise test
Radicular pain and neurological signs consistent with the nerve root level affected
Mild weakness of distal muscles such as extensor hallucis longus, peroneals, tibialis anterior and soleus. These would fit with the myotome relevant for the disc level
MRI confirming a disc herniation
Possible bladder and bowel symptoms
Failed conservative rehabilitation
Time span in which to enable conservative rehabilitation to be effective. In the overall population, medical practitioners will most likely prescribe a minimal 6-week traditional period of treatment with an overview at 6 weeks as to whether to expand the rehabilitation a further 6 weeks or to seek a specialist opinion. The expert may then attempt more medically orientated interventions such as epidural injections.
The athlete nevertheless will have these They might be more inclined to experience an epidural very early in the conservative period to assess the effectiveness of this procedure. If no signs of progress are evident in a couple of weeks then they may choose to get an immediate lumbar spine micro- discectomy.
Endoscopic Lumbar Discectomy
Local Doctor performs lumbar discectomy using minimally invasive techniques. From the El Paso, TX. Spine Center.
Imaging
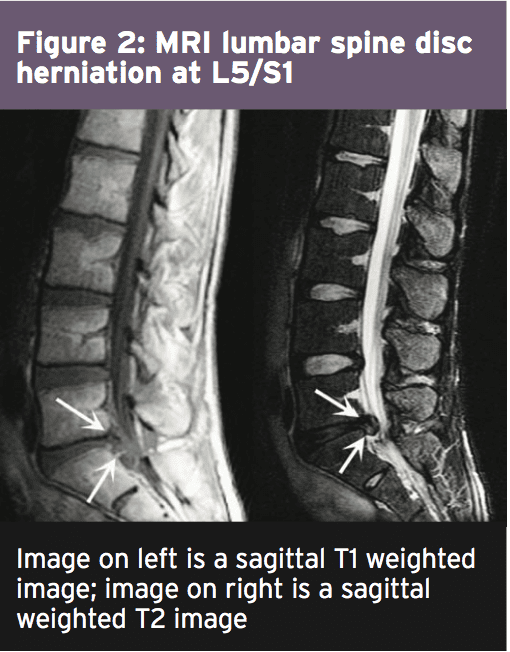
MRI remains the favored system of Identifying lumbar spine disc herniation, since it’s also very sensitive to detecting nerve root impingements(23). However, abnormal MRI scans can occur in otherwise asymptomatic patients(25); hence, clinical correlation is always essential before any surgical thought. What’s more, patients can present with clinical signs and symptoms which suggest the diagnosis of acute herniated disc, and yet lack evidence of sufficient pathology on MRI to warrant operation.
Therefore it has been proposed that a Volumetric analysis of a herniated disc on MRI may be potentially beneficial in checking the suitability for operation. Several writers have previously mentioned the possible value of volumetric evaluation of herniated disc on MRI as part of their selection criteria for lumbar surgery(26).
In a survey conducted in Michigan State University, it was found that the size and positioning of the herniated disc determined that the likelihood for operation with what researchers called ‘types 2-B’ and ‘types 2-AB’ being the most likely candidates for surgery(27).
The MRI protocol to your lumbar spine consists of (see Figure 2)
1.Sagittal plane echo T1- weighted sequence
2. Sagittal fast spin echo proton density sequence
3. Sagittal fast spin echo inversion recovery sequence
4.Axial spin echo T1- weighted sequence
Summary
Disc herniations are not a common Complaint in athletes, but they do happen in sports which involve high loads or repetitive flexion and rotation movements. Sufferers of a disc herniation will normally feel focused low-back pain, maybe with referral in the lower limb with associated neurological symptoms if the nerve root was compressed.
Managing a disc herniation within an General population as frequently the risk of a Protracted failed rehabilitation period is Bypassed for the protected and low risk Micro-discectomy procedure. In the Discuss the exact surgical alternatives involved Observing a lumbar spine micro-discectomy.
References
1. Sports Med. 1996;21(4):313�20
2. Radiology. Oct 2007;245(1):62-77
3. Arthritis Research & Therapy. 2003;5(3):120-30
4. The Journal of Bone and Joint Surgery. American volume. Feb 2004;86-A(2):382 � 96
5. Radiology. Oct 2007;245(1):43-61
6. Spine. Sep 15 1996;21(18):2149-55
7. Spine. May-Jun 1982;7(3):184-91
8. Spine. Dec 1 2002;27(23):2631-44
9. Lancet 1986;2:1366�7
10. Disease-A-Month:DM. Dec 2004;50(12):636-69
11. Spine. Mar 1987;12(2):146-9
12. The American Journal of Sports Medicine. Sep 2004;32(6):1434-9
13. The Journal of International Medical Research. 2011;39(2):569-79
14. Spine. 2001;26:E93-113
15. Spine. 1990;15:679-82
16. British Journal of Sports Medicine. Jun 2003;37(3):263-6
17. Prim Care. 2005;32(1):201�29
18. McGill, S.M. Low back disorders: Evidence based prevention and rehabilitation, Human Kinetics Publishers, Champaign, IL, U.S.A., 2002. Second Edition, 2007
19. Spine. Apr 1991;16(4):437-43
20. Skeletal radiology. Jul 2006;35(7):503-9
21. British Journal of Sports Medicine. Nov 2007;41(11):836-41
22. The American Journal of Sports Medicine. Jun 2009;37(6):1208-13
23. Spine. Mar 15 1995;20(6):699-709
24. Phys Sportsmed. 2005;33(4):21�7
25. J Bone Joint Surg Am 1990 . 2:403�408
26. J Orthop Surg (Hong Kong) 2001. 9:1�7
27. Eur Spine J (2010) 19:1087�1093
When diagnosed with degenerative disc disorder, among the primary things that lots of patients ask is, “Am I going to need surgery to repair this?” For many people, the answer is no. You in fact need to meet some rather stringent demands in order for your doctor to recommend operation:
You have attempted several months�ordinarily about six months�of non-operative treatments, plus they haven’t helped reduce your pain. What this means is that you simply have attempted physical therapy, medications, rest, among others, and your pain is still interfering with your life.
Your disc degeneration is at two levels not just one. When you have multi-level disc degeneration, you might not be the best candidate for surgery as you may lose an excessive amount of mobility in your back if you have a fusion (that sort of surgery is clarified below).
You’re comparatively young. Recovery from operation could be a tough procedure, so that your body requires in order to manage it. Younger individuals are somewhat more effective at recovering than older folks that are more prone to complications from operation. There’s not a certain “you should not have surgery if you are older than this” age. Your physician will probably be able to create that recommendation.
Operation could be required immediately for those who have among these red flags:
Loss in bladder or bowel control
Cauda equina syndrome is an incredibly serious ailment. Your cauda equina�or “horse’s tail”�is several nerves that resembles, competently enough, a horse’s tail. It is situated at the conclusion of the spinal cord, and it is a surgical emergency when the cauda equina is compressed. You might have extreme low back pain, weakness in your legs, radiculopathy (pain that goes out of your back and into your legs), and incontinence.
Types of Surgery for Degenerative Disc Disease
Up until lately, surgery for degenerative disc disease has called for two main parts: removal of what’s causing pain and then fusing the back to control movement. When the surgeon removes tissue that’s pressing on a nerve, it is called a decompression surgery. Fusion is a stabilization surgery, and frequently, a decompression and fusion are done at the exact same time.
Traditional surgical options that are decompression include:
Facetectomy: There are joints in your spine called facet joints; they help stabilize your back. Yet, facet joints can put pressure on a nerve. “Ectomy” means “removal of.” So a facetectomy involves removing the facet joint to reduce that pressure.
Foraminotomy: If part of the disc or a bone spur (osteophyte) is pressing on a nerve as it makes the vertebra (through an exit called the foramen), a foraminotomy might be done. “Otomy” means “to make an opening.” So a foraminotomy is making the opening of the foramen larger, therefore the nerve can depart without being compressed.
Laminectomy: At the rear of every vertebra, there is a bony plate that protects your spinal canal and spinal cord; it’s known as the lamina. It may be pressing in your spinal cord, hence by removing section or all of the lamina, the surgeon may make more room.
Laminotomy: Similar to the foraminotomy, a laminotomy makes a more substantial opening, this time in your bony plate shielding your spinal canal and spinal cord (the lamina). The lamina may be pressing therefore the surgeon may make more room for the nerves using a laminotomy.
All of the above decompression techniques are done from the back of the spine (posterior). Sometimes, though, a surgeon has to do a decompression from the front of the spine (anterior). As an example, a bulging disc or a herniated disc shoving into your spinal canal sometimes cannot be removed from behind because the spinal cord is in the way. In that case, the decompression procedure is normally performed from the front (anterior). The main anterior decompression techniques are:
Discectomy: It might be pressing on your own nerves in case you are in possession of a bulging disc or a herniated disc. In a discectomy, the surgeon will remove all or area of the disc. The surgeon can do a discectomy using a minimally invasive approach. Minimally invasive means that there are smaller incisions as well as the surgeon works with a microscope and very little surgical tools. You’ll possess a recovery period that is shorter when you possess a minimally invasive discectomy.
Corpectomy (or Vertebrectomy): Occasionally, surgeons will need to take the complete vertebral body out because disc substance becomes lodged between the spinal cord and also the vertebral body and can’t be removed by a discectomy. In other cases, osteophytes form between spinal cord and the vertebral body. In these situations, the whole vertebral body may need certainly to be removed to gain access to the disc material that is pressing on your nerve�that’s a corpectomy.
After portion of a disc or vertebra continues to be taken out, your back could be shaky, meaning that it proceeds in strange ways. That makes you more at risk for serious neurological harm, and you don’t want that. The surgeon will need to stabilize your spine. Traditionally, this has been done using a fusion, and it can be done from the back (posterior) or in the front (anterior).
In spine stabilization by fusion, the surgeon creates an environment where the bones in your back will fuse together over time (usually over several months or longer). The surgeon uses a bone graft (normally using bone from your own personal body, but it is possible to utilize donor bone as well) or a biological substance (which will stimulate bone growth). Your surgeon may use spinal instrumentation�wires, cables, screws, rods, and plates�to raise stability as the bones fuse. The fusion will cease movement between the vertebrae, providing long term stability.
New Surgical Options for Degenerative Disc Disease
A fruitful fusion restricts motion in the fused area. Now there’s a brand new surgical option that helps you keep freedom: an artificial disc. The surgeon will remove your disc (a discectomy), and insert an artificial disc in its area. The notion is that the artificial disc help you move more readily and with less pain and will keep your spine flexible.
Artificial discs have become new, but they’re a fascinating development in back surgery. But because they’re so new, there haven’t been many long-term studies in the US about the effectiveness of artificial discs. Short-term studies and studies from Europe are promising, though.
Risks of Spinal Surgery
As with absolutely any procedure, there are risks involved with spine surgery for degenerative disc disease. Before requesting one to sign a surgical consent form, your doctor will discuss possible risks along with you. Possible complications include, but are not limited to:
harm to nerves or your spinal cord
non-healing of the bony fusion (pseudoarthrosis)
failure to enhance
instrumentation breakage/failure
infection and/or bone graft site pain
pain and swelling in your leg veins (phlebitis)
urinary difficulties
Complications could result in more surgery, so again �make certain that you completely understand the risks along with your surgery before proceeding. The decision for surgery is yours and yours alone.
Recovering from Degenerative Disc Disease Surgery
After surgery for DDD, you will not immediately feel better. Should you have had a fusion, it will require some time (several months or longer) for the fusion to heal properly, and in the interim,, you could have pain in the region where you had surgery. Your incisions should heal in 7 to 14 days.
Your surgeon will provide you with special directions about what you’ll be able to and can’t do following surgery. Be sure to stick together with the healing plan and never overdo it or overstress your back. Report any issues�such as increased pain, temperature, or infection�to your physician immediately.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
By Dr. Alex Jimenez
Additional Topics: Preventing Spinal Degeneration
As we age, it’s natural for the spine, as well as the other complex structures of the spine, to begin degenerating. Without the proper care, however, the overall health and wellness of the spine can develop complications, such as degenerative disc disease, among others, which could potentially lead to back pain and other painful symptoms. Chiropractic care is a common alternative treatment option utilized to maintain and improve spine health.
Doctor of Chiropractic, Dr. Alex Jimenez examines Tiger Woods’ and his latest back surgery.
We have a look at Tiger Woods’ extensive history of injuries during his career. USA TODAY Sports
Tiger Woods Won�t Be Back For Some Time
Woods, that has made just three starts in a couple of years, likely won�t play again this year after he’d his back surgery that is fourth in Texas. The latest procedure alleviated pain in his back and leg, Woods announced on his web site Thursday.
That I’m confident this will relieve my back spasms and pain, and The operation went well,� Woods said in a statement. When fixed, �, I anticipate playing with my kids getting back to a normal life, competing in professional golf and living without the pain I’ve been fighting so long.�
Woods, who also has had four surgeries on his left knee, first had surgery on his back and then had two procedures in the autumn of 2015.
According to his statement, a disc in Woods back seriously narrowed because of causing sciatica, the three surgeries and severe back and leg pain. During the recent operation, the damaged disc was removed and the collapsed disc space was elevated to levels that were regular. The goal is to relieve the pressure on the nerve, the statement said. The procedure was performed by Dr. Richard Guyer of the Centre for Disc Replacement at the Texas Back Institute.
A Look At Tiger Woods’ Injury History
RELATED:
About playing on Champions Tour, Tiger Woods jokes around
Woods, 41, last played in February, where he shot a birdie-free 77 in the very first round before removing. Where he missed the cut his only other start was in the Farmers Insurance Open the week prior.
His only appearance on the golf course in 2016 arrived at the Hero World Challenge in December. While he finished 15th in the 17-man field, he tied for the tournament lead in birdies (24), seemed healthy and upbeat.
Before beginning therapy, he will be resting for several weeks. The recovery interval is usually about half a year. That would mean Woods, a winner of 14 major tournaments and 79 PGA Tour titles, won�t play in any of the four majors for a second straight year. He is now rated No. 788 in the world.
Woods is in good spirits after the surgery, said his agent, Mark Steinberg.
USA TODAY Sports, he believes somewhat that the large weight was lifted off his shoulders,� Steinberg told. �The three previous operations were somewhat temporary repairs. But it got to the point where the pain was more common and this latest surgery was something he had to do.�
Steinberg said Woods decided to take a conservative approach along with his back previously three years with his difficulties. That alternative wasn�t accessible this time.
�This just isn’t a temporary repair,� Steinberg said. � his physicians proposed him that this is the top path to a healthy, energetic lifestyle. He and his children were playing but he was in so much pain.
�Now he �ll possess a healthy life without pain.�
One, Steinberg said, that can include playing golf.
�Entirely,� Steinberg said. �He desires to get out (on the PGA Tour) again.�
Woods� last public appearance ahead of the operation was Tuesday in Hollister, Missouri, where he pronounced he�s designing his first public golf course. The course will probably be called Payne’s Valley in honor of Missouri native Payne Stewart. Woods is a partner on the project with CEO Johnny Morris and Bass Pro Shops founder.
Patients who go straight home from the hospital following hip or knee replacement surgery recover as well as, or better than, those who first go to a rehabilitation center, new research indicates.
And that includes those who live alone without family or friends, one of three studies shows.
“We can say with confidence that recovering independently at home does not put patients at increased risk for complications or hardship, and the vast majority of patients were satisfied,” said that study’s co-author, Dr. William Hozack. He is an orthopaedic surgery professor with the Rothman Institute at the Thomas Jefferson University Medical School in Philadelphia.
Hozack noted that while in the past it was “not uncommon for patients to enter a rehabilitation facility in order to receive additional physical therapy,” most patients today do not end up going to a secondary facility. In fact, roughly 90 percent of Hozack’s joint replacement patients are discharged directly home following surgery, he said. “Considerable evidence has now shown that most patients do just as well at home,” he noted.
Hozack and his colleagues are scheduled to present their findings in San Diego at a meeting of the American Academy of Orthopaedic Surgeons (AAOS).
Home Recovery Following Surgery
Two other studies being presented at the meeting also found that recovering at home may be the better option.
One study found that patients who are discharged directly home following a total knee replacement face a lower risk for complications and hospital readmission than those who first go to an inpatient rehab facility. The study was led by Dr. Alexander McLawhorn, an orthopaedic hip and knee surgeon at the Hospital for Special Surgery in New York City.
McLawhorn was also part of a second Hospital for Special Surgery study, led by Michael Fu. That study found that hip replacement patients admitted to an inpatient facility rather than being sent home faced a higher risk for respiratory, wound and urinary complications, and a higher risk for hospital readmission and death.
Dr. Claudette Lajam is chief orthopaedic safety officer with NYU Langone Orthopaedics in New York City. She was not involved with the studies, but agrees that home recovery is the best option for most patients.
“The home setting is the single best way to get people back into their routines as quickly as possible after surgery,” she said. “In some cases, this cannot be done,” Lajam acknowledged. “Some patients live in settings that are inaccessible, [such as] a 5th-floor walk-up apartment where the patient would need to go downstairs to let the visiting nurse and therapist in the door.” For some patients, anxiety about the recovery process could also pose a challenge, she added. But “being in an institutional setting after surgery only reinforces the idea that the patient is ‘sick,’ ” Lajam added. “We have learned that this type of thinking slows down recovery. We want our total joint patients to start using their new joints as quickly as possible, and staying in bed at a nursing facility is not the way to do this.”
Hozack and his colleagues set out to see whether patients who live alone fare as well as those who live with others. All 769 patients enrolled in the study by Hozack’s team went home following either a total hip replacement or a total knee replacement. Of those, 138 lived alone (about 18 percent). Once home, all were assessed on multiple levels, including functionality (ability to move); pain levels; hospital readmissions; emergency department visits; unscheduled doctor visits; dependency on assisted-walking devices; and time before returning to work or being able to drive again.
Hozack’s team observed no differences by any measure. And while those who lived with others indicated relatively higher satisfaction levels at the two-week mark, by the three-month point there was no appreciable difference between the two groups.
“We feel that giving patients back their independence early on is the best way to promote a safe and effective recovery,” said Hozack. His team concluded that single-household patients who go straight home can expect to fare as well as those who have live-in support.
A recent Mayo Clinic study calculated that between 2000 and 2010, the number of Americans who underwent hip replacement surgery more than doubled, rising from just under 140,000 to more than 310,000 per year.
Meanwhile, AAOS figures indicate that in 2010 more than 650,000 knee replacement procedures were performed, with about 90 percent involving total knee replacement. AAOS estimates from 2014 show that 4.7 million Americans now live with an artificial knee and 2.5 million have an artificial hip.
Findings presented at meetings should be viewed as preliminary until published in a peer-reviewed journal.
SOURCES: William J. Hozack, M.D., professor of orthopaedic surgery, Rothman Institute, Thomas Jefferson University Medical School, Philadelphia; Claudette Lajam, M.D. assistant professor and chief orthopedic safety officer, NYU Langone Orthopedics, New York City; March 14-18, 2017 presentations, American Academy of Orthopaedic Surgeons meeting, San Diego
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Additional Topics: What is Chiropractic?
Chiropractic care is a safe and effective, alternative treatment option utilized to diagnose, treat and prevent a variety of injuries and conditions associated with the musculoskeletal and nervous system. A chiropractor, or doctor of chiropractic, commonly uses spinal adjustments or manual manipulations to help correct the spine and it’s surrounding structures, improving and maintaining the patient’s strength, mobility and flexibility.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine





 In this phase it’s anticipated that the athlete will remain relatively quiet for 2-3 weeks post surgery. This allows for full tissue recovery to happen, including scar tissue maturation. The athlete is allowed to completely mobilize in full weight-bearing; however care needs to be taken using any flexion and rotation motions and no lifting will be allowed.
In this phase it’s anticipated that the athlete will remain relatively quiet for 2-3 weeks post surgery. This allows for full tissue recovery to happen, including scar tissue maturation. The athlete is allowed to completely mobilize in full weight-bearing; however care needs to be taken using any flexion and rotation motions and no lifting will be allowed.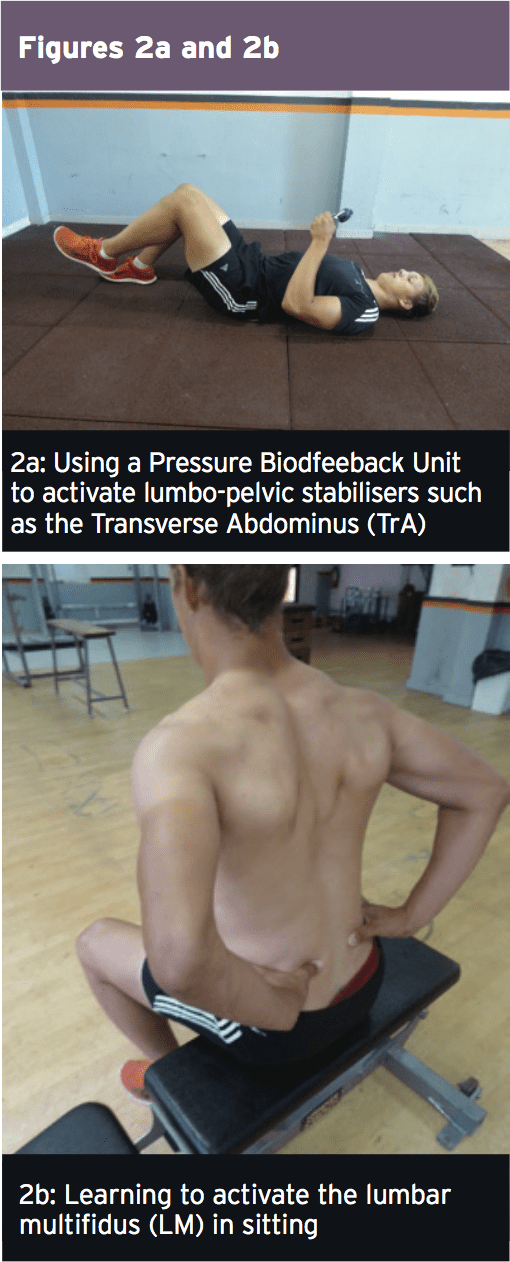 Early Loading & Foundation
Early Loading & Foundation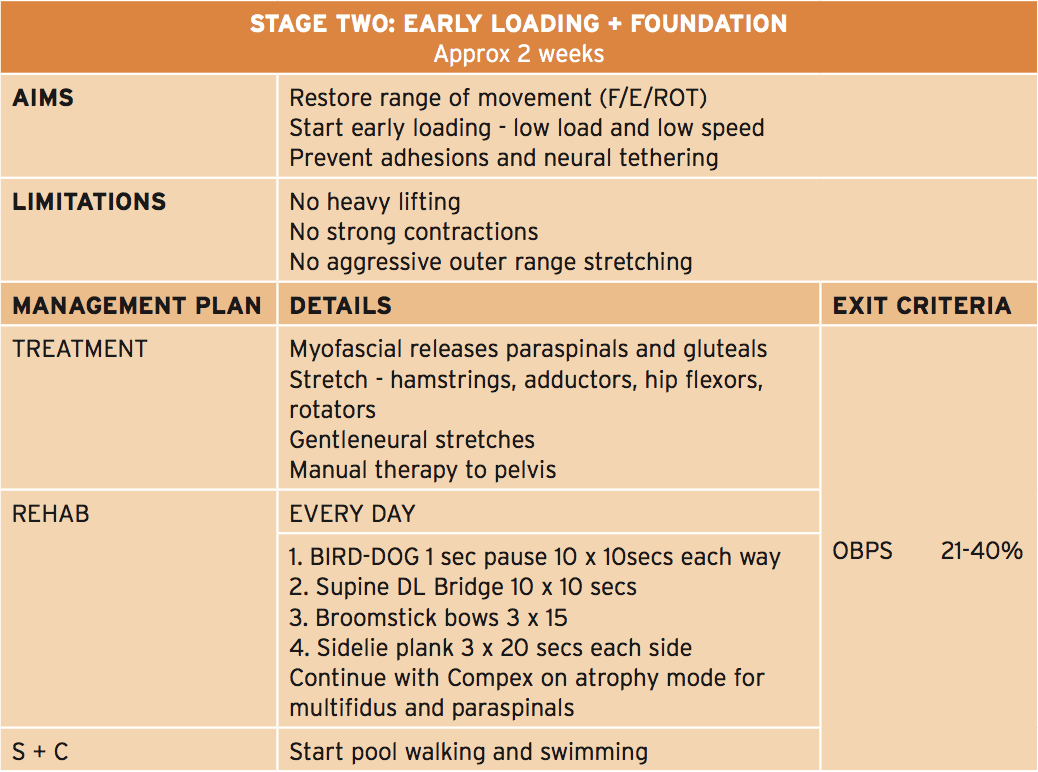 The primary feature of this phase is that the athlete can start early and low-load strength exercises focusing on muscle activation in a neutral spine position, along with a progressive selection of motion program to improve lumbar spine flexion, extension and rotation. In this stage that the physiotherapist will guide the athlete through safe and gentle stretches to your hip quadrant muscles like the hip flexors, gluteals, hamstrings and adductors. The athlete also lasts gentle neuro-mobilization exercises to advance the freedom of the sciatic nerve — an issue in this condition as neurological tethering is a chance as a result of scar tissue formation caused by the surgical procedure.
The primary feature of this phase is that the athlete can start early and low-load strength exercises focusing on muscle activation in a neutral spine position, along with a progressive selection of motion program to improve lumbar spine flexion, extension and rotation. In this stage that the physiotherapist will guide the athlete through safe and gentle stretches to your hip quadrant muscles like the hip flexors, gluteals, hamstrings and adductors. The athlete also lasts gentle neuro-mobilization exercises to advance the freedom of the sciatic nerve — an issue in this condition as neurological tethering is a chance as a result of scar tissue formation caused by the surgical procedure.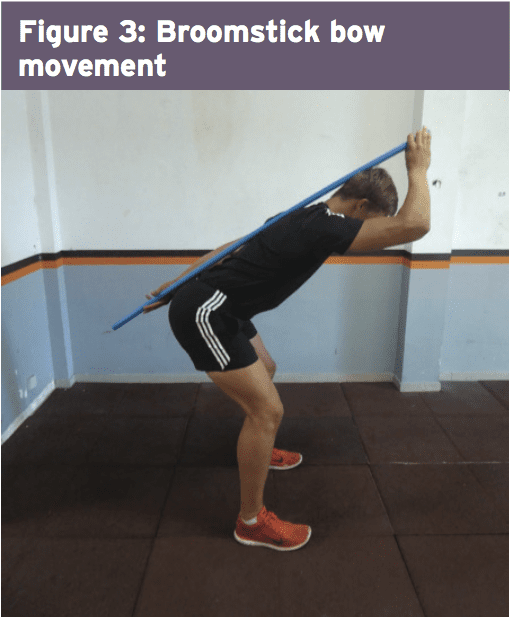 Progressive Loading
Progressive Loading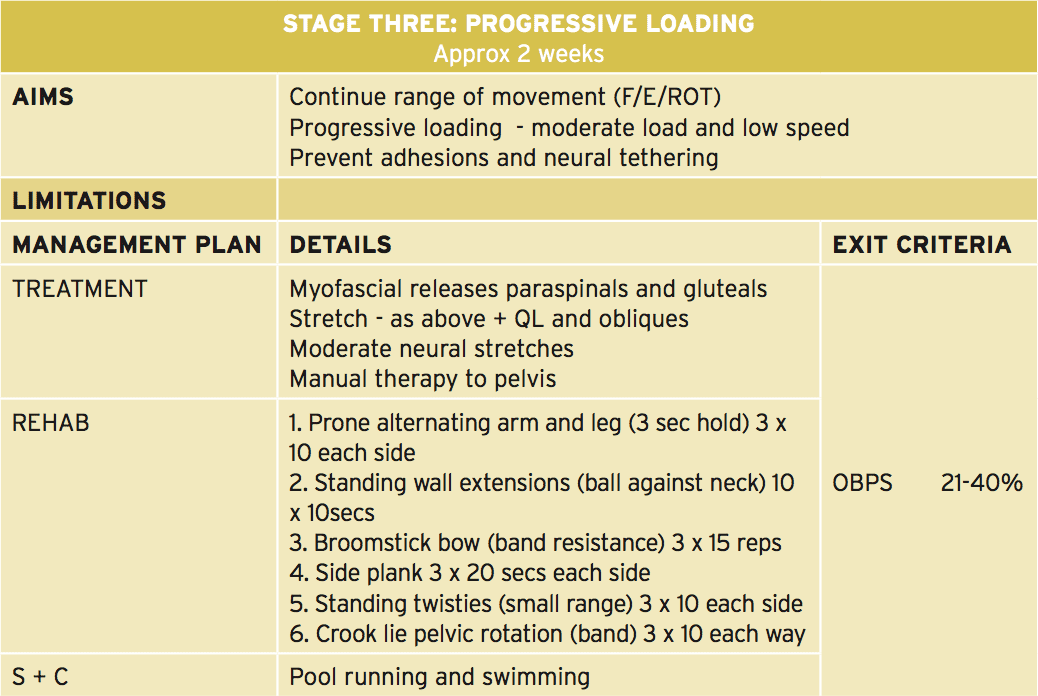 In this phase the athlete continues with a variety of movement progression along with the physiotherapist progresses manual therapy to the pelvis and lumbar spine. Neuro-mobilization techniques can also be progressed. The significant change in this phase is that the progression of load on many of the strength and muscle control exercises.�
In this phase the athlete continues with a variety of movement progression along with the physiotherapist progresses manual therapy to the pelvis and lumbar spine. Neuro-mobilization techniques can also be progressed. The significant change in this phase is that the progression of load on many of the strength and muscle control exercises.�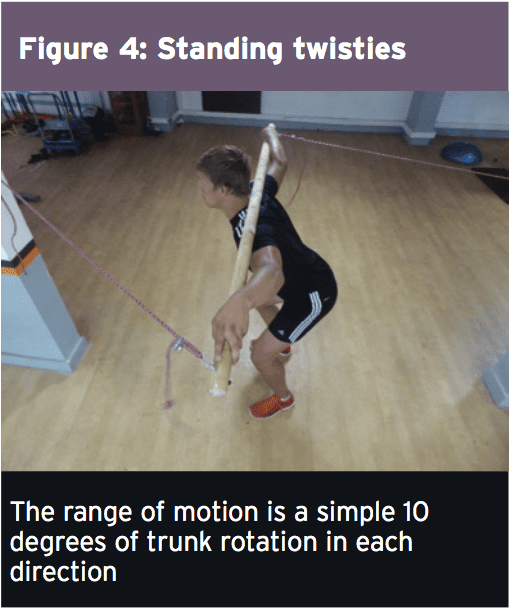
 Load Accumulation
Load Accumulation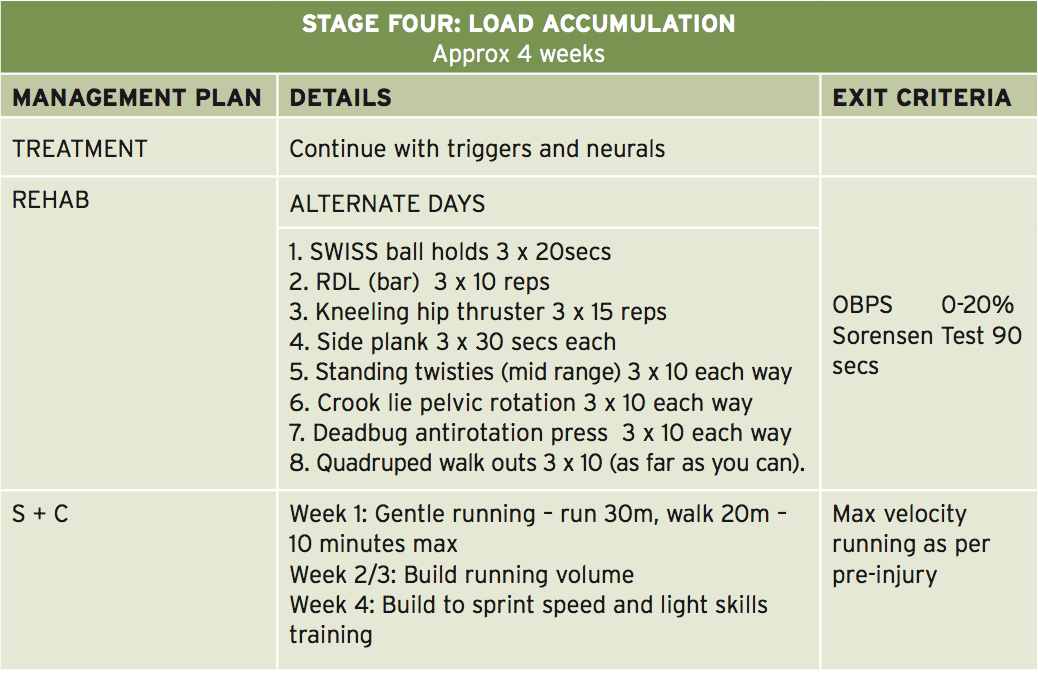 This is the stage where the athlete begins to advance the load in strength-based exercises. Resistance is used in the form of barbell load and band resistance. Three exceptional exercises performed here are the ‘kneeling hip thruster’, ‘deadbug antirotation press’ and also the ‘quadruped walkout’ (Figures 6-8 — explained in detail in the online database of exercises).
This is the stage where the athlete begins to advance the load in strength-based exercises. Resistance is used in the form of barbell load and band resistance. Three exceptional exercises performed here are the ‘kneeling hip thruster’, ‘deadbug antirotation press’ and also the ‘quadruped walkout’ (Figures 6-8 — explained in detail in the online database of exercises).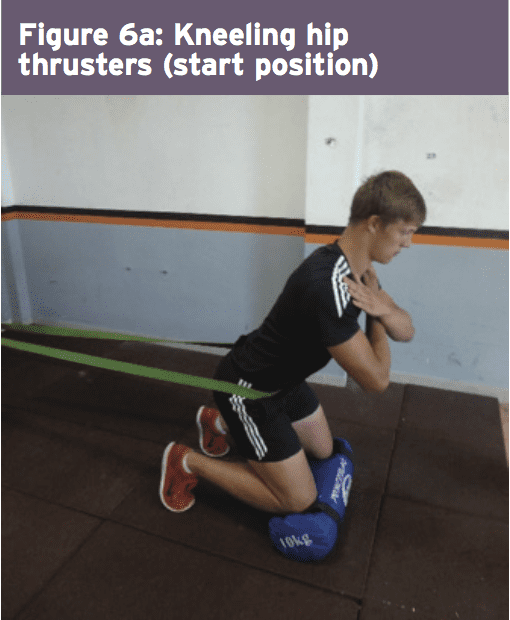
 The athlete also begins running drills at this phase and it might be expected that as well as building running Amount, the athlete should progress over four weeks to close to full sprint speeds. This is also the stage whereby they would initiate mild to moderate sports special skills drills. Another characteristic of this stage is that the athlete starts the ‘Sorensen test’ exercise (Figure 9) and it will be expected that they can maintain the position for no less than 90 seconds before advancing to the next phase.
The athlete also begins running drills at this phase and it might be expected that as well as building running Amount, the athlete should progress over four weeks to close to full sprint speeds. This is also the stage whereby they would initiate mild to moderate sports special skills drills. Another characteristic of this stage is that the athlete starts the ‘Sorensen test’ exercise (Figure 9) and it will be expected that they can maintain the position for no less than 90 seconds before advancing to the next phase.