Can adding calisthenics resistance training to a fitness routine provide health benefits like flexibility, balance, and coordination?
Calisthenics Resistance Training
Calisthenics resistance training requires no equipment, they can be done with minimal space, and are a great way to get a quick burn.
They are a form of resistance training using your own body weight that is low-impact, which makes it accessible to individuals of all ages and fitness levels.
They effectively help build agility, and cardiovascular health, and improve balance, coordination, and flexibility.
Benefits
Muscle Strength
Because calisthenics are easily adaptable to any fitness level, require minimal or no equipment, and are great for beginners and experienced exercise enthusiasts it is a fantastic full-body workout and an excellent way to build strength and muscle. Research supports that calisthenics resistance training can improve muscle strength in various ways.
One study found that eight weeks of calisthenics not only improved posture and body mass index/BMI but can impact strength, even with exercises not routinely performed. (Thomas E, et al., 2017)
During the study, one group did calisthenics and the other maintained regular training routines.
The researchers discovered that the group that did calisthenics increased their repetitions of exercises that were not included.
The group who continued with their regular training routines did not improve on what they could do before the eight-week study. (Thomas E, et al., 2017)
Cardiovascular Fitness
Regular participation in calisthenic resistance training can lead to improved cardiovascular health, including increased endurance and a healthier heart.
Certain calisthenic exercises, like burpees and mountain climbers, are high-intensity movements that can increase heart rate and blood circulation just from the movements.
Gradually performing these exercises at a faster pace, research indicates could potentially experience the same cardiovascular benefits from interval or treadmill running. (Bellissimo GF, et al., 2022) – (Lavie CJ, et al., 2015)
Balance, Coordination, and Flexibility
The movements require a full range of motion that stretches and strengthens the muscles, tendons, and ligaments.
These exercises can help decrease the risk of injury and make daily physical activities easier to perform without over-exertion.
Incorporating calisthenics resistance training on a regular basis can help improve posture, balance, and flexibility, depending on which exercises are recommended.
Exercises like stretches, lunges, and squats help to improve flexibility and mobility.
Exercises like single-leg squats and one-arm push-ups can work the balance, coordination, and proprioception of the body.
Mental Health
Exercise, in general, is known to improve mood, reduce stress, and improve overall well-being.
Calisthenic resistance training can have additional impacts on mental well-being.
For example, the discipline and focus required to perform the movements can help concentration and mental clarity.
One study found that calisthenics can reduce cognitive decline and may be useful for dementia prevention. (Osuka Y, et al., 2020)
Another study found that calisthenics helped mental well-being in individuals with diseases like ankylosing spondylitis and multiple sclerosis. (Taspinar O, et al., 2015)
Types
Bodyweight exercises that use an individual’s own body weight as resistance are the foundation. Common examples include push-ups, squats, and lunges. An overview of some of the types of exercises.
Pulling
These exercises focus on training the muscles for pulling movements, which include the back, shoulders, and arms.
Examples include pull-ups, chin-ups, and rows.
Pushing
These exercises focus on training the muscles for pushing movements, like the chest, shoulders, and triceps.
Examples include dips, push-ups, and handstand push-ups.
Core
Core exercises focus on training the abdominal and lower back muscles, which are responsible for maintaining stability and balance.
Examples of core exercises include planks, sit-ups, and leg raises.
Single-Leg
Single-leg exercises focus on training one leg at a time.
These target the muscles of the legs, hips, and core.
Examples of single-leg exercises include single-leg squats, lunges, and step-ups.
Plyometric
Calisthenics resistance training focuses on powerful explosive movements.
Plyometric exercises challenge the muscles to work quickly and forcefully.
Examples include jump squats, clap push-ups, and box jumps.
Getting Started
Start by making sure calisthenics is an appropriate workout option, especially if you are a beginner or have pre-existing medical conditions.
Once cleared to exercise start with familiar movements that can be done with the correct form.
Pushups, bodyweight squats, planks, lunges, and other basic movements are a good place to start.
Make sure to warm up with light and easy motions that mimic the workout movements.
Aim to work each body part during the workout.
Try for at least two workouts a week.
It is recommended to split the movement patterns.
Reps can be counted or set a timer to switch exercises every minute. This is called EMOM-style or every minute on the minute.
Pick four to five exercises that target various areas.
For example, sit-ups can be done for the core, lunges for the glutes and thighs, planks can be done for the shoulders and core, and jumping jacks or jumping rope for cardiovascular.
Calisthenic resistance training is easily modifiable and can be adjusted to individual needs.
Core Strength
References
Thomas, E., Bianco, A., Mancuso, E. P., Patti, A., Tabacchi, G., Paoli, A., … & Palma, A. (2017). The effects of a calisthenics training intervention on posture, strength, and body composition. Isokinetics and exercise science, 25(3), 215-222.
Bellissimo, G. F., Ducharme, J., Mang, Z., Millender, D., Smith, J., Stork, M. J., Little, J. P., Deyhle, M. R., Gibson, A. L., de Castro Magalhaes, F., & Amorim, F. (2022). The Acute Physiological and Perceptual Responses Between Bodyweight and Treadmill Running High-Intensity Interval Exercises. Frontiers in physiology, 13, 824154. https://doi.org/10.3389/fphys.2022.824154
Osuka, Y., Kojima, N., Sasai, H., Ohara, Y., Watanabe, Y., Hirano, H., & Kim, H. (2020). Exercise Types and the Risk of Developing Cognitive Decline in Older Women: A Prospective Study. Journal of Alzheimer’s disease: JAD, 77(4), 1733–1742. https://doi.org/10.3233/JAD-200867
Taspinar, O., Aydın, T., Celebi, A., Keskin, Y., Yavuz, S., Guneser, M., Camli, A., Tosun, M., Canbaz, N., & Gok, M. (2015). Psychological effects of calisthenic exercises on neuroinflammatory and rheumatic diseases. Zeitschrift fur Rheumatologie, 74(8), 722–727. https://doi.org/10.1007/s00393-015-1570-9
Lavie, C. J., Lee, D. C., Sui, X., Arena, R., O’Keefe, J. H., Church, T. S., Milani, R. V., & Blair, S. N. (2015). Effects of Running on Chronic Diseases and Cardiovascular and All-Cause Mortality. Mayo Clinic Proceedings, 90(11), 1541–1552. https://doi.org/10.1016/j.mayocp.2015.08.001
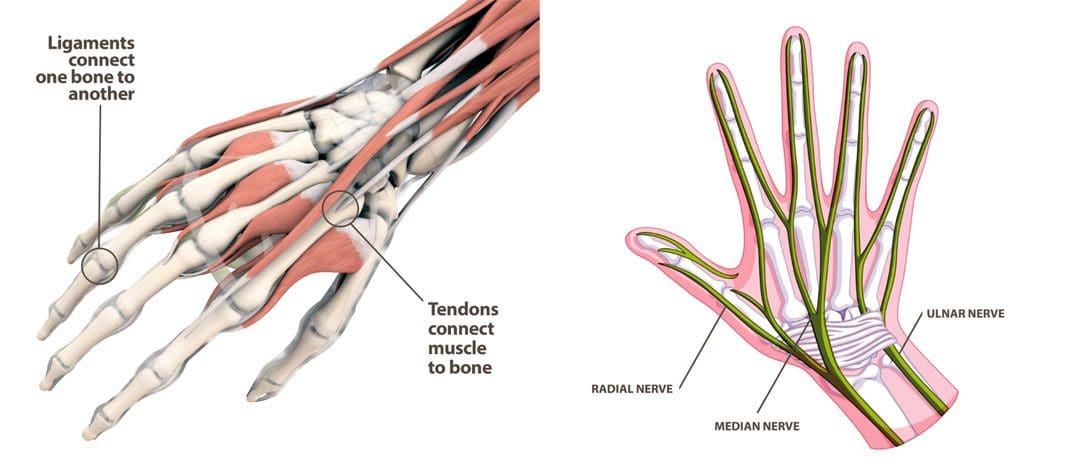
Golfing wrist injuries are common with treatment requiring 1-3 months of rest and immobilization and if tears are present surgery. Can chiropractic treatment help avoid surgery, expedite recovery, and rehabilitation?
Golfing Wrist Injuries
Golfing Wrist Injuries: According to a study, there are over 30,000 golf-related injuries treated in American emergency rooms every year. (Walsh, B. A. et al, 2017) Nearly a third are related to a strain, sprain, or stress fracture.
This causes pain and inflammation and is usually accompanied by a grinding sensation when moving the thumb and wrist.
Chiropractic Treatment
Given the nature of these injuries, medical attention should be sought out for image scans to look at any damage and properly immobilize the wrist. Once a fracture has been ruled out or healed, golfing wrist injuries can benefit from chiropractic and physical therapy. (Hulbert, J. R. et al, 2005) A typical treatment may involve a multifaceted approach involving various therapies including:
Active release therapy, myofascial release, athletic taping, corrective exercise, and stretching.
A chiropractor will examine the wrist and its functioning to determine the nature of the injury.
A chiropractor may recommend using a splint to immobilize the wrist, particularly in cases of overuse.
They will relieve pain and swelling first, then focus on strengthening the joint.
They may recommend a regimen of icing the hand.
Adjustments and manipulations will relieve pressure on the nerves to reduce swelling and restore mobility.
Peripheral Neuropathy Successful Recovery
References
Walsh, B. A., Chounthirath, T., Friedenberg, L., & Smith, G. A. (2017). Golf-related injuries treated in United States emergency departments. The American journal of emergency medicine, 35(11), 1666–1671. https://doi.org/10.1016/j.ajem.2017.05.035
Moon, H. W., & Kim, J. S. (2023). Golf-related sports injuries of the musculoskeletal system. Journal of exercise rehabilitation, 19(2), 134–138. https://doi.org/10.12965/jer.2346128.064
Ray, G., Sandean, D. P., & Tall, M. A. (2023). Tenosynovitis. In StatPearls. StatPearls Publishing.
Zouzias, I. C., Hendra, J., Stodelle, J., & Limpisvasti, O. (2018). Golf Injuries: Epidemiology, Pathophysiology, and Treatment. The Journal of the American Academy of Orthopaedic Surgeons, 26(4), 116–123. https://doi.org/10.5435/JAAOS-D-15-00433
Tan, H. K., Chew, N., Chew, K. T., & Peh, W. C. (2014). Clinics in diagnostic imaging (156). Golf-induced hamate hook fracture. Singapore medical journal, 55(10), 517–521. https://doi.org/10.11622/smedj.2014133
Hulbert, J. R., Printon, R., Osterbauer, P., Davis, P. T., & Lamaack, R. (2005). Chiropractic treatment of hand and wrist pain in older people: systematic protocol development. Part 1: informant interviews. Journal of chiropractic medicine, 4(3), 144–151. https://doi.org/10.1016/S0899-3467(07)60123-2
Individuals at work, school, etc, perform all kinds of repetitive physical tasks that put their bodies through a great deal of musculoskeletal stress, what are the effects and benefits of joint manipulation therapy for pain relief?
Joint Manipulation Health Benefits
Joint manipulation is a form of manual therapy that involves applying force to the spinal or peripheral joints to:
Relieve pain symptoms.
Realign the joints to their proper position.
Restore flexibility.
Improve mobility.
Increase range of motion.
Chiropractors, massage, and physical therapists use various manipulation techniques to help move and feel better after an injury or illness that causes loss of functional mobility. Here we explain joint manipulation, its applications, and if the technique is safe for you and your condition.
Joint Popping
The joints in the body are places where two or more bones come together to allow movement.
The cartilage allows the joint surfaces to glide/slide smoothly.
If the cartilage is injured or damaged, pain and limited motion can present.
When a joint doesn’t move properly, the muscles surrounding that joint don’t contract properly.
If a joint is dysfunctional for some time, significant muscle wasting and atrophy can occur around the joint, leading to difficulty with mobility like standing, walking, or reaching. (Hurley MV.1997)
The body is made up of cells that breathe by converting energy and releasing waste materials. One type of waste material from cell respiration is carbon dioxide. The gas is transported through the blood and delivered out of the body while breathing. Small pockets of gas can get trapped in the joints that expand and contract as pressure around the joint changes during movement, known as cavitation. When the gas is released through joint manipulation, there can be a popping or snapping sound as the joint is moved. Once the gas is released, joint pressure is decreased and mobility is increased. (Kawchuk, et al., 2015)
Causes
Non-medical
There are non-medical and medical causes of joint dysfunction and derangement that include:
Overuse and repetitive strain.
Unhealthy sitting and/or standing posture.
Lack of physical activity.
Over-stretching or stretching incorrectly.
In these situations, the joints can be temporarily placed in a dysfunctional/compromised position. When moving to the correct position, a popping sound can present as built-up pressure is released.
Medical
Joint problems can occur from medical conditions that can include:
Herniated cervical or lumbar discs.
Spinal arthritis.
Rheumatoid arthritis.
Osteoarthritis.
Joint contracture after being immobilized for some time.
In these cases, a medical problem can be causing a limitation in the joint’s position and movement. (Gessl, et al., 20220)
Benefits
If a chiropractic practitioner determines there is joint dysfunction then manipulation may be a treatment option. The benefits include:
Pain Relief
When a chiropractor or therapist gets an injured joint moving properly, the receptors in and around the area get reset allowing for pain relief.
Improved Muscle Activation
As a chiropractor manipulates a joint into its correct anatomical position, the surrounding muscles can flex and contract properly.
Improved Range of Motion
The joint is repositioned for proper movement.
This improves the range of motion and relieves tightness and stiffness.
Improved Functional Mobility
Once a joint is manipulated, the improved range of motion and muscle activation around the joint can lead to improved overall functional mobility. (Puentedura, et al., 2012)
Candidates
Joint manipulation is a safe manual therapy technique for certain individuals. (Puentedura, et al., 2016) This includes:
Individuals with acute neck, back, or peripheral joint pain.
Adults aged 25 to 65 with no serious medical conditions.
Athletes who have been injured from their sport.
Individuals who have been immobilized after injury or surgery.
Joint manipulation is not recommended for everyone and can be dangerous or lead to injury in individuals with certain conditions. (Puentedura, et al., 2016) These include individuals with:
Osteoporosis
Weakened bones may fracture if a high-velocity force is applied to a joint via manipulation
Joint fractures
Individuals with a joint fracture, should not have that specific joint manipulated.
Post Spinal Fusion Surgery
Individuals that have had spinal fusion in the neck or lower back should avoid spinal joint manipulations or adjustments for at least one year after the procedure.
The bones need time to heal thoroughly.
Manipulation can cause a failure of the fusion.
Individuals with Arterial Insufficiency In Their Neck
A rare but dangerous side effect of a neck adjustment is the risk of tearing an artery in the neck known as the vertebrobasilar artery. (Moser, et al., 2019)
If there is pain, loss of movement, or decreased mobility after an injury or surgery, a chiropractic adjustment with joint manipulation can be beneficial to help regain movement. Manual techniques can help improve joint mobility, alleviate pain, and increase strength and stability around the joints. Joint manipulation isn’t for everyone and is recommended to consult with a healthcare professional to see if it is safe for your specific condition.
Gessl, I., Popescu, M., Schimpl, V., Supp, G., Deimel, T., Durechova, M., Hucke, M., Loiskandl, M., Studenic, P., Zauner, M., Smolen, J. S., Aletaha, D., & Mandl, P. (2021). Role of joint damage, malalignment, and inflammation in articular tenderness in rheumatoid arthritis, psoriatic arthritis, and osteoarthritis. Annals of the rheumatic diseases, 80(7), 884–890. https://doi.org/10.1136/annrheumdis-2020-218744
Hurley M. V. (1997). The effects of joint damage on muscle function, proprioception, and rehabilitation. Manual therapy, 2(1), 11–17. https://doi.org/10.1054/math.1997.0281
Kawchuk, G. N., Fryer, J., Jaremko, J. L., Zeng, H., Rowe, L., & Thompson, R. (2015). Real-time visualization of joint cavitation. PloS one, 10(4), e0119470. https://doi.org/10.1371/journal.pone.0119470
Moser, N., Mior, S., Noseworthy, M., Côté, P., Wells, G., Behr, M., & Triano, J. (2019). Effect of cervical manipulation on the vertebral artery and cerebral hemodynamics in patients with chronic neck pain: a crossover randomized controlled trial. BMJ open, 9(5), e025219. https://doi.org/10.1136/bmjopen-2018-025219
Puentedura, E. J., Cleland, J. A., Landers, M. R., Mintken, P. E., Louw, A., & Fernández-de-Las-Peñas, C. (2012). Development of a clinical prediction rule to identify patients with neck pain likely to benefit from thrust joint manipulation to the cervical spine. The Journal of orthopedic and sports physical therapy, 42(7), 577–592. https://doi.org/10.2519/jospt.2012.4243
Puentedura, E. J., Slaughter, R., Reilly, S., Ventura, E., & Young, D. (2017). Thrust joint manipulation utilization by U.S. physical therapists. The Journal of manual & manipulative therapy, 25(2), 74–82. https://doi.org/10.1080/10669817.2016.1187902
The digestive system breaks down the foods eaten so the body can absorb the nutrients. During digestion, the unnecessary parts of these foods are turned into waste/stool, which is evacuated during a bowel movement. When the digestive system stops functioning properly due to factors such as diet change, eating unhealthy foods, lack of physical activity/exercise, medications, and certain health conditions, can cause constipation. Constipation occurs when the body cannot have a regular bowel movement. The distention, gas, bloating and not being able to have a bowel movement cause irritability and stress, which can worsen constipation. Incorporating recommended nutrition can help restore regular bowel movements and gut function.
Recommended Nutrition For Constipation
Symptoms like abdominal pain, bloating, and difficult bowel movements are common. Diet and proper hydration have a significant role in digestive health, especially in relieving and preventing constipation. High-fiber foods, prebiotics, and adequate hydration from foods and beverages are essential for healthy bowel movements.
Fiber is found in whole grains, starches, fruits, and vegetables.
Soluble and insoluble fiber are important for digestive health.
Focusing on incorporating high-fiber fruits, vegetables, and whole grains.
Foods rich in prebiotics like fermented foods are recommended when constipated.
The recommended nutrition for constipation, according to a dietitian includes.
Avocados
Avocados can be paired with just about anything and are full of nutrients and fiber.
One avocado contains around 13.5 grams of fiber.
One avocado will provide almost half daily fiber needs.
Other high-fiber fruits: pomegranates, guava, raspberries, blackberries, and passionfruit.
Figs
Figs can be eaten fresh and dried.
Figs are considered a laxative and have been shown to treat and reduce constipation.
They contain antioxidants, polyphenols, polyunsaturated fatty acids, and vitamins.
Other fruits similar to a fig: dried apricots, prunes, and plums.
Plums
Plums, prunes dried plums are packed with fiber and prebiotics that have a natural laxative effect.
The added H2O makes the stools softer and easier to pass.
Natural fruit juices, like pear, apple, or prune are often prescribed for constipation.
Other fruits that aid in bowel movements: peaches, pears, and apples.
Kefir
Fermented foods like kefir are rich in beneficial bacteria that work to maintain digestive system health.
It can be consumed on its own or used in smoothies, cooking, and baking recipes.
Other fermented foods: kombucha, yogurt, sauerkraut, kimchi, miso, and tempeh.
Oat Bran
Oat bran is oatmeal that has not had the bran removed.
The bran contains beneficial nutrients including fiber, antioxidants, vitamins, and minerals.
Oat bran contains soluble and insoluble fiber, as well as beta-glucan/non-starchy polysaccharides.
All improve the composition of gut bacteria and promote healthy bowel movements.
Other beneficial grains: oatmeal, wheat bran, rye, and barley.
Incorporating Gut-Beneficial Foods
How to incorporate recommended nutrition gut-beneficial foods into a regular menu:
Smoothie
Use kefir or yogurt as a base then balance it out with fiber-rich fruits like mango, blueberries, and kiwi.
Snacks
Diversify snacks with a plate of fiber and prebiotics.
Nuts, cheese, crackers, fruit, and a yogurt or avocado dip.
Oatmeal
Try oat bran to increase fiber.
Sprinkle a serving of flaxseeds, chia seeds, or hemp seeds for added fiber and healthy fats.
Parfait
Yogurt parfaits can maximize nutrients, flavor, and textures in a bowl.
Layer up on a favorite yogurt with granola, nuts, fruit, and seeds.
Grain Bowl
Fiber found in whole grains and seeds like barley, farro, and quinoa, helps promote healthy digestion.
Make a bowl with a grain base, then top with a protein, fresh or grilled veggies, avocado, and dressing.
Talk with a registered nutritionist or other healthcare provider to discuss recommended nutrition plan options.
Balancing Body and Metabolism
References
Arce, Daisy A et al. “Evaluation of constipation.” American family physician vol. 65,11 (2002): 2283-90.
Bharucha, Adil E. “Constipation.” Best practice & research. Clinical gastroenterology vol. 21,4 (2007): 709-31. doi:10.1016/j.bpg.2007.07.001
Gray, James R. “What is chronic constipation? Definition and diagnosis.” Canadian Journal of Gastroenterology = Journal Canadien de Gastroenterology vol. 25 Suppl B, Suppl B (2011): 7B-10B.
Jani, Bhairvi, and Elizabeth Marsicano. “Constipation: Evaluation and Management.” Missouri medicine vol. 115,3 (2018): 236-240.
Naseer, Maliha, et al. “Therapeutic Effects of Prebiotics on Constipation: A Schematic Review.” Current clinical pharmacology vol. 15,3 (2020): 207-215. doi:10.2174/1574884715666200212125035
National Institute of Diabetes and Digestive and Kidney Diseases. Symptoms and Causes of Constipation.
National Institute of Diabetes and Digestive and Kidney Disease. Your Digestive System and How It Works.
Sinclair, Marybetts. “The use of abdominal massage to treat chronic constipation.” Journal of bodywork and movement therapies vol. 15,4 (2011): 436-45. doi:10.1016/j.jbmt.2010.07.007
Hiking is a form of exercise accessible to a wide range of physical abilities, which makes it a great outdoor activity for all. The health benefits include improved blood pressure, sleep, and reduced stress and anxiety. However, being out in the elements without conditioning the body can lead to serious injuries and other health issues. Many trails are rough, uneven, and have elevation gain, so even the easiest courses require balance and strength to avoid injury. Hiking training that includes strength, cardio, and practice will help condition the body to allow the trip to be more enjoyable and safe.
Hiking Training
Two of the most common hiking injuries are rolling the ankle and ankle sprains. Individuals that are out of shape or haven’t been active for some time are recommended to start with basic movements and exercises to warm up the muscles and increase heart rate.
Walk/Run Through Sand
This builds the muscles that protect the knees and ankles.
Increase Range of Motion
Using a resistance band will strengthen muscles through their full extension.
Standing on a tennis ball or balance disc is great as it builds the small stabilizer muscles around the ankles and knees.
Crunches
Building core strength will help maintain balance on uneven surfaces.
Squats and Lunges
Keep the back straight and take each squat and lunge slowly to strengthen the core muscles.
Push-ups
Sufficient upper body strength, especially the back muscles will help on long trips and when carrying a heavy pack.
Cardiovascular
Walking around the neighborhood, on a treadmill, or stationary bike will work to increase cardiovascular ability.
The objective is to get the heart rate up to build lung capacity.
Step-ups
Before a backpacking trip, weigh the pack – try 20 lbs. – and step up onto a park bench 16 to 18 inches high.
Add 5 pounds a week until the pack is as heavy as it will be on the hike.
Strength Hiking Training for Backpacking
Carrying a heavy pack activates many muscles, including those of the arms and shoulders, and back. Hiking for an extended period with a backpack requires getting used to the weight and feel of it. Nothing conditions the body for a pack better than actually experiencing it.
Shoulder and Neck
The trapezius muscles radiate out from the base of the neck.
This is where the shoulder harness of the pack sits.
Strong traps help prevent soreness.
Most of the pack’s weight should be on and around the hips, but it doesn’t always happen due to pack design and body shape.
Shoulder and Arm
The shoulder of the arm used to put on and take off the pack does a lot of work at awkward angles.
The rotator cuff of the shoulder is vulnerable to these loads.
Upper Back
The muscles of the upper and mid back contract to stabilize the pack, especially with heavy loads.
Beginning hikers and backpackers tend to get a dull pain right in the center of the shoulder blades.
Lower Back
The lower back takes the brunt of the force from lifting and twisting the posterior chain of muscles.
Abdominal Muscles
The abdominal muscles work to stabilize the pack when twisting and turning.
Legs
Walking, squatting, and standing with the pack requires strong support from the legs.
Strong legs, especially thighs, make a difference.
Start small and go slow until you feel comfortable in the surroundings. Start off with lightweight and short distances and gradually extend to heavier weights and longer distances. Remember to go at your own pace and don’t try to be an expert.
Hikers Strength Training
References
Chrusch, Adam, and Michelle Kavin. “Survey of Musculoskeletal Injuries, Prehike Conditioning, and On-Trail Injury Prevention Strategies Self-Reported by Long-Distance Hikers on the Appalachian Trail.” Wilderness & environmental medicine vol. 32,3 (2021): 322-331. doi:10.1016/j.wem.2021.04.004
Fleg, Jerome L. “Aerobic exercise in the elderly: a key to successful aging.” Discovery Medicine vol. 13,70 (2012): 223-8.
Gatterer, H et al. “Effect of weekly hiking on cardiovascular risk factors in the elderly.” Zeitschrift fur Gerontologie und Geriatrie vol. 48,2 (2015): 150-3. doi:10.1007/s00391-014-0622-0
Huber, Daniela, et al. “Sustainability of Hiking in Combination with Coaching in Cardiorespiratory Fitness and Quality of Life.” International journal of environmental research and public health vol. 19,7 3848. 24 Mar. 2022, doi:10.3390/ijerph19073848
Liew, Bernard, et al. “The Effect of Backpack Carriage on the Biomechanics of Walking: A Systematic Review and Preliminary Meta-Analysis.” Journal of applied biomechanics vol. 32,6 (2016): 614-629. doi:10.1123/jab.2015-0339
Li, Simon S W, et al. “Effects of a backpack and double pack loads on postural stability.” Ergonomics vol. 62,4 (2019): 537-547. doi:10.1080/00140139.2018.1552764
Li KW, Chu JC, Chen CC. Strength decrease, perceived physical exertion, and endurance time for backpacking tasks. Int J Environ Res Public Health. 2019;16(7):1296. doi:10.3390/ijerph16071296
Mitten, Denise, et al. “Hiking: A Low-Cost, Accessible Intervention to Promote Health Benefits.” American Journal of lifestyle medicine vol. 12,4 302-310. 9 Jul. 2016, doi:10.1177/1559827616658229
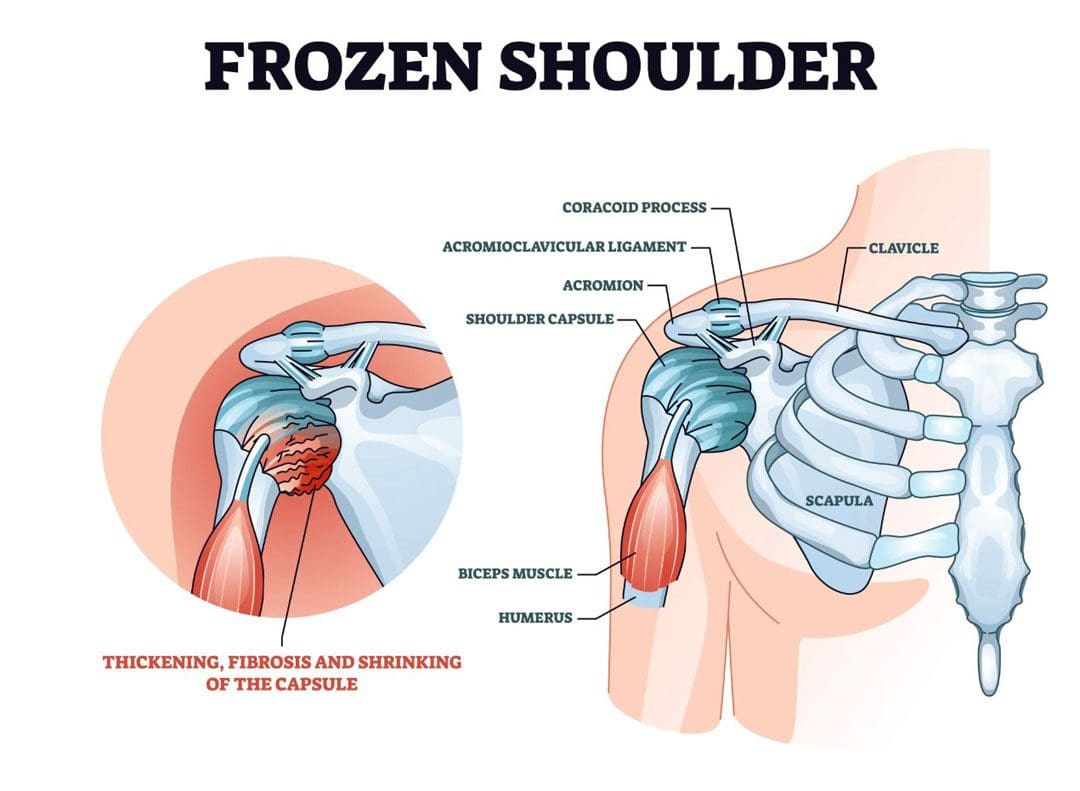
Stiffness and pain developing in the shoulder could be adhesive capsulitis, (frozen shoulder), a condition in the shoulder’s ball-and-socket joint/glenohumeral joint. It usually develops over time and limits the functional use of the arm. The pain and tightness restrict arm movement, and the duration of symptoms can persist for 12-18 months. The cause is often unknown, but it is more common in individuals over 40, individuals with diabetes, thyroid disease, and cardiac conditions have an increased risk of developing the condition, and women tend to develop the condition more than men. Chiropractic treatment can be effective at relieving pain and expediting recovery.
Stiffness and Pain
The shoulder joint allows more movement than any other joint in the body. A frozen shoulder causes the capsule surrounding the shoulder joint to contract and form scar tissue. The capsule contraction and the formation of adhesions cause the shoulder to become stiff, restrict movement, and cause pain and discomfort symptoms.
Stages
The progression is marked by three stages:
Freezing
Stiffness and pain begin to restrict motion.
Frozen
Movement and motion are severely restricted.
Thawing
The shoulder starts to loosen up.
It can take years to fully resolve symptoms.
In mild cases, a frozen shoulder can go away on its own but that does not mean that it is truly healed and correctly aligned.
Even in mild cases seeking treatment is recommended, rather than just waiting for it to go away.
Symptoms
Limited range of motion.
Stiffness and tightness.
Dull or aching pain throughout the shoulder.
Pain can radiate into the upper arm.
Pain can be triggered by the smallest movements.
The symptoms are not always due to weakness or injury, but actual joint stiffness.
Causes
Most frozen shoulders occur with no injury or discernible cause but the condition is often linked to a systemic condition or one that affects the entire body.
Age and Gender
Frozen shoulder most commonly affects individuals between the ages of 40 to 60, and is more common in women than in men.
Endocrine Disorders
Individuals with diabetes have an increased risk of developing a frozen shoulder.
Other endocrine abnormalities like thyroid problems can also lead to the development of this condition.
Shoulder Trauma and/or Surgery
Individuals who sustain a shoulder injury, or undergo surgery on the shoulder can develop a stiff and painful joint.
When injury or surgery is followed by prolonged immobilization/resting the arm, the risk of developing a frozen shoulder increases.
Other Systemic Conditions
Several systemic conditions such as heart disease have also been associated with an increased risk of developing the condition and can include:
High cholesterol
Adrenal disease
Heart and lung disease
Parkinson’s disease
Stiffness and pain can also be associated with damage to the joint from injuries or other shoulder problems that include:
A frozen shoulder associated with any of these causes is considered secondary.
Treatment
A diagnosis is made by observing the range of motion in the shoulder, considering the two types:
Active Range
This is how far an individual can move a body part on their own.
Passive Range
This is how far another person like a therapist or doctor can move the body part.
Therapies
Chiropractic, massage, and physical therapy involve stretches, realignment, and exercises to relieve pain symptoms and restore mobility and function.
Usually, strength is not affected by a frozen shoulder but a chiropractor may want to strengthen the surrounding muscles to better support the shoulder and prevent worsening the injury or causing a new injury.
Anti-inflammatory medications and corticosteroid injections may help manage pain symptoms.
Getting a diagnosis and treatment during the freezing stage can keep the condition from progressing and expedite recovery time.
Enhancing Health: Evaluation and Treatment
References
Brun, Shane. “Idiopathic frozen shoulder.” Australian Journal of general practice vol. 48,11 (2019): 757-761. doi:10.31128/AJGP-07-19-4992
Chan, Hui Bin Yvonne, et al. “Physical therapy in the management of frozen shoulder.” Singapore medical journal vol. 58,12 (2017): 685-689. doi:10.11622/smedj.2017107
Cho, Chul-Hyun, et al. “Treatment Strategy for Frozen Shoulder.” Clinics in orthopedic surgery vol. 11,3 (2019): 249-257. doi:10.4055/cios.2019.11.3.249
Duzgun, Irem, et al. “Which method for frozen shoulder mobilization: manual posterior capsule stretching or scapular mobilization?.” Journal of Musculoskeletal & neuronal interactions vol. 19,3 (2019): 311-316.
Jain, Tarang K, and Neena K Sharma. “The effectiveness of physiotherapeutic interventions in the treatment of frozen shoulder/adhesive capsulitis: a systematic review.” Journal of back and musculoskeletal rehabilitation vol. 27,3 (2014): 247-73. doi:10.3233/BMR-130443
Kim, Min-Su, et al. “Diagnosis and treatment of calcific tendinitis of the shoulder.” Clinics in shoulder and elbow vol. 23,4 210-216. 27 Nov. 2020, doi:10.5397/cise.2020.00318
Millar, Neal L et al. “Frozen shoulder.” Nature reviews. Disease primers vol. 8,1 59. 8 Sep. 2022, doi:10.1038/s41572-022-00386-2
Individuals spend around one-third of their life sleeping or resting. Every person has their own preferred sleeping position. However, not all sleep positions are comfortable and supportive to the body, especially the spine. Individuals that sleep on their side or stomach that experience back pain might want to consider switching to sleeping on their back. Changing preferred sleeping positions can seem impossible, however, learning to sleep on your back is possible with a little training and adjustment period.
Learning To Sleep On Your Back
After side sleeping, back sleeping is the second most common position. Individuals that are stomach or side sleepers that suffer from:
Learning to sleep on your back is recommended because its health benefits can potentially solve all these problems and more.
Adapting this sleeping position can help maintain proper spinal alignment.
Relieves waking up with tension headaches.
Relieve sinus problems.
Individuals that are not natural back sleepers understand how difficult it is to force oneself to adapt to a new sleeping position. There are ways to condition the mind and body to fall and stay asleep on your back, resulting in healthy rest. These include:
A Pillow Under The Knees
It may help to place a supportive pillow under the knees.
The knees should be slightly bent and feel comfortable.
Check to make sure that the neck and spine feel comfortable and are in alignment.
Make adjustments as needed.
A Pillow Under The Low Back
In the beginning, switching to back sleeping can increase discomfort in the low back.
Placing a pillow under the lower back can help.
Using too large or thick a pillow could create added discomfort.
Try a few different pillows to find what works best and feels right.
Pillow Surround
Individuals that are active sleepers and tend to roll onto their side or stomach soon after falling asleep, can place pillows around the midsection and hips.
A small barrier of pillows around the body can assist in learning to sleep on your back.
The pillows help prevent the body from rolling.
It’s recommended to place pillows closely against either side of the body.
Using the pillows as an enclosure will force the body to remain in a neutral position throughout the night.
Sleeping On The Right Pillow
Individuals will want to make sure they are using the right sleeping pillow.
In addition to supporting the spine’s alignment, a quality pillow will also support the neck.
The recommended pillow for back sleeping should cradle the head and ensure it stays elevated.
A pillow that is too flat or too thick can cause the head to become unlevel with the body leading to:
Neck and upper body pain
Restricted airflow, which may cause you to snore or suffer from sleep apnea.
Digestive issues like acid reflux and heartburn.
Consider a pillow that’s made out of some type of memory foam to assist with learning to sleep on your back.
The thickness and hugging sensation can help to stay on the back and prevent inadvertently flipping over.
Sleeping On The Right Mattress
A positive back sleeping experience begins with the right mattress. There are so many mattress types to choose from. It is recommended to consider the materials, the firmness level, and the size. For comfortably sleeping on your back, the firmness level is essential.
Consider the positioning of your spine.
The objective is to keep the spine as straight as possible, which is achieved with the proper firmness.
A mattress that is too firm will create unwanted pressure and tension on the shoulders and the pelvic region.
A mattress that is too soft will cause the hips to sink, throwing spinal alignment off and causing back pain symptoms.
A medium-firm mattress is recommended.
Memory foam is a great option for learning to sleep on your back.
Memory foam cradles the natural curve of the body, and hugs the body during sleep, which helps avoid accidentally rolling onto your side or stomach.
Memory foam mattresses with integrated gel can provide cooling and ventilation to keep the body refreshed throughout the night.
A medium-firm memory foam mattress will make sure the body stays straight, with the proper cushioning around the pelvis and hips.
Training To Sleep On Your Back
References
Anderson, Ngaire H et al. “Association of Supine Going-to-Sleep Position in Late Pregnancy With Reduced Birth Weight: A Secondary Analysis of an Individual Participant Data Meta-analysis.” JAMA network open vol. 2,10 e1912614. 2 Oct. 2019, doi:10.1001/jamanetworkopen.2019.12614
Desouzart, Gustavo, et al. “Effects of sleeping position on back pain in physically active seniors: A controlled pilot study.” Work (Reading, Mass.) vol. 53,2 (2015): 235-40. doi:10.3233/WOR-152243
Khan, Bashir Ahmad, et al. “Effect of bed head elevation during sleep in symptomatic patients of nocturnal gastroesophageal reflux.” Journal of Gastroenterology and Hepatology vol. 27,6 (2012): 1078-82. doi:10.1111/j.1440-1746.2011.06968.x
Portale, G et al. “When are reflux episodes symptomatic?.” Diseases of the esophagus: official journal of the International Society for Diseases of the Esophagus vol. 20,1 (2007): 47-52. doi:10.1111/j.1442-2050.2007.00650.x
Skarpsno, Eivind Schjelderup, et al. “Sleep positions and nocturnal body movements based on free-living accelerometer recordings: association with demographics, lifestyle, and insomnia symptoms.” Nature and Science of Sleep vol. 9 267-275. 1 Nov. 2017, doi:10.2147/NSS.S145777
Surdea-Blaga, Teodora, et al. “Food and Gastroesophageal Reflux Disease.” Current medicinal chemistry vol. 26,19 (2019): 3497-3511. doi:10.2174/0929867324666170515123807
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine