The legs are important for standing and motion. Various problems can affect any part, including the bones, tendons, joints, blood vessels, and connective tissues of the entire leg, foot, ankle, knee, or hip. Common problems include unbalanced/unevenness, muscle sprains and strains, joint dislocations, nerve compression, and fractures. These issues can benefit from chiropractic leg adjustments to relieve the symptoms, realign the body, restore mobility, strengthen the muscles, and prevent further complications.
Leg Adjustments
The legs are composed of two major sections: upper and lower. The ball-and-socket hip joint connects the upper portion, with only one bone comprising the upper leg, the femur, the largest bone in the body. The lower leg goes from the knee to the ankle and is composed of two bones, the fibula, and the tibia.
The tibia makes up the knee together with the base of the femur.
The fibula starts from the knee joint and is connected to the tibia.
Muscles
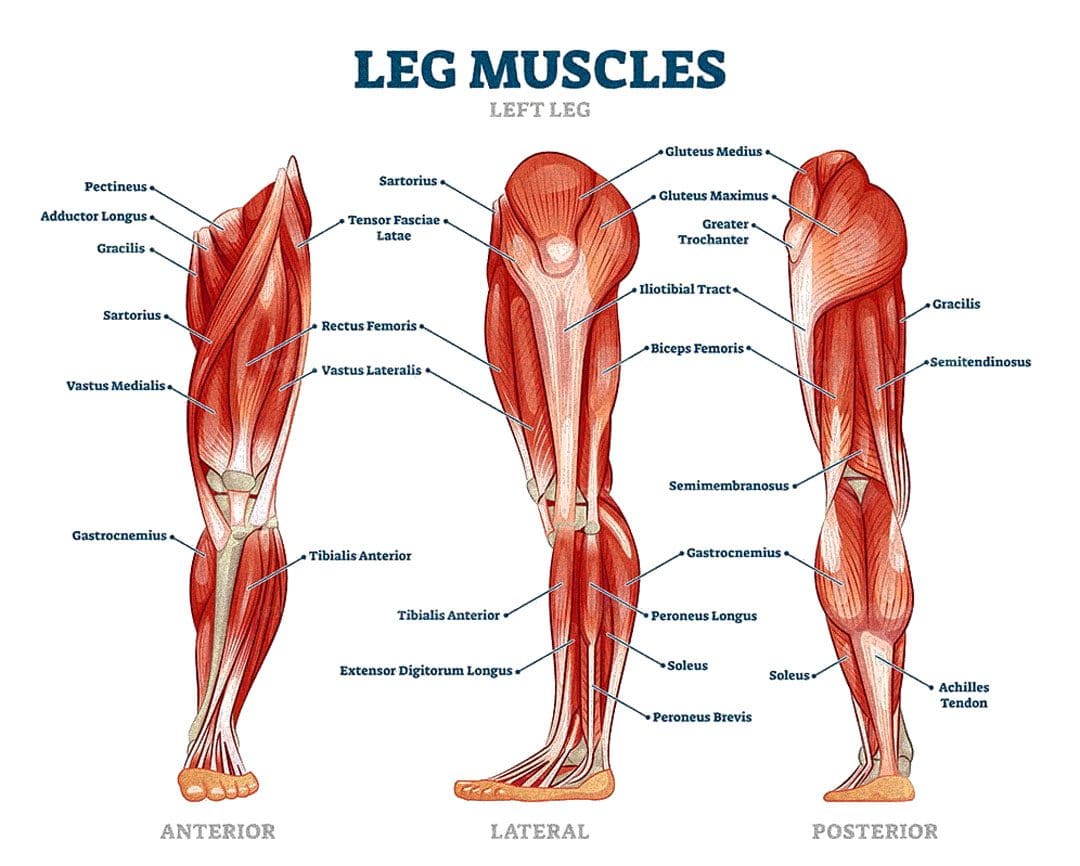
The leg muscles support standing and sitting, carry the body’s weight, and provide movement. Several muscles in the upper and lower legs work together to enable walking, running, jumping, flexing, and pointing the toes.
Upper Leg
The upper leg muscles support the body’s weight and movement. Their jobs include:
Anterior muscles: These muscles stabilize the body and help with balance. They also allow:
Bending and extension of the knees.
Flexion of the thigh at the hip joints.
Rotation of the legs at the hips.
Medial muscles assist in hip adduction – moving the leg toward the body’s center. They also allow flexion, extension, and rotation of the thigh.
Posterior muscles help move the leg from front to back and rotate at the hip socket.
Lower Leg
Anterior muscles are in the front/anterior part of the lower leg and help lift and lower the foot and toe extension.
Lateral muscles run outside the lower leg and stabilize the foot when walking or running. They also allow side-to-side movement.
Posterior muscles: These muscles are in the back of the lower leg. Some are superficial (close to the skin surface), and some sit deeper inside the leg. They help:
Flex and point the toes.
Jump, run and push off.
Lock and unlock the knee.
Maintain a healthy posture by stabilizing the legs.
Stand up straight by supporting the arch of the feet.
Causes
There are different causes of leg discomfort symptoms. Age, work, physical activity, sports, and misalignments can all cause leg issues to develop.
Musculoskeletal
Musculoskeletal system injuries, conditions, and disorders are related to the bones, muscles, tendons, and ligaments. This includes bruising, tendonitis, muscle strain, overuse, and fractures can all lead to musculoskeletal issues.
Neurological
Neurological symptoms are related to a problem with the nerves and the nervous system. Damaged and pinched nerves can contribute to leg issues.
Vascular
If there are blood vessel issues, it can also lead to leg symptoms. Depending on the cause, leg symptoms can vary from moderate to severe and may be non-stop or come and go.
Chiropractic care is a proven way of reducing swelling and discomfort throughout the body. Chiropractic leg adjustments help release restrictions and misalignments. This results in increased mobility of the joints, decreased inflammation, and improved function. A chiropractic adjustment on the leg is known as a long-axis distraction adjustment. This adjustment is designed to open the affected joint in the direction the chiropractor pulls. They can adjust their contact to open the femur from the acetabulum of the pelvis, the knee joint, the ankle joints, and the low back. This encourages proper joint space and motion in the affected areas, promoting healthy movement and space and allowing more nutrient flow and pressure removal from the surrounding nerves to help with symptom relief.
Hip Long Axis Distraction
References
Binstead JT, Munjal A, Varacallo M. Anatomy, Bony Pelvis, and Lower Limb, Calf. (www.ncbi.nlm.nih.gov/books/NBK459362/) [Updated 2020 Aug 22]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan-. Accessed 12/29/2021.
Eid K, Tafas E, Mylonas K, Angelopoulos P, Tsepis E, Fousekis K. Treatment of the trunk and lower extremities with Ergon® IASTM technique can increase hamstrings flexibility in amateur athletes: A randomized control study. Phys Ther Sport. 2017;28:e12. doi:10.1016/J.PTSP.2017.08.038
Jeno SH, Schindler GS. Anatomy, Bony Pelvis, and Lower Limb, Thigh Adductor Magnus Muscles. (www.ncbi.nlm.nih.gov/books/NBK534842/) [Updated 2020 Aug 10]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan-. Accessed 12/29/2021.
McGee S. Stance and gait. In: McGee S. Evidence-Based Physical Diagnosis. 3rd ed. Philadelphia, PA: Elsevier Saunders; 2012:chap 6.
Ransom AL, Sinkler MA, Nallamothu SV. Anatomy, Bony Pelvis, and Lower Limb, Femoral Muscles. (www.ncbi.nlm.nih.gov/books/NBK500008/) [Updated 2020 Oct 30]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2021 Jan-. Accessed 12/29/2021.
Reflex pain is a complex condition that involves the body’s pain withdrawal reflexfailing to turn off after the event that triggered the pain, so the pain sensations continue. This is a neurological condition known as the withdrawal reflex. It occurs when the body and brain undergo a chain of reactions to remove an affected body part from dangerous situations/stimuli. A typical example is a vehicle crash or accident. During the process, the body’s reflex muscle\s in the injured area tighten to protect the specific body part/s from further damage.
The reflex can feel like a muscle spasm that goes away over time. However, in the case of reflex pain, the signals keep firing. Reflex pain can occur all over the body as the muscles overcompensate to handle the prolonged pain; secondary injuries often develop. An example could be reflex pain in the ankle caused by injury or problems in the hips and back, where the individual tries to avoid moving the ankle in a specific way to prevent and avoid the pain symptoms. Individuals with reflex pain also experience headaches and referred spine and extremity pain. Reflex pain can become a cycle of symptoms that include:
Unusual tightness
Stiffness
Pain
Contracture – hardening or shortening of the affected muscles, tendons, or other tissues.
Decreased functional abilities.
Somatic Pain
Somatic pain causes receptors in tissues including the skin, muscles, connective tissues, joints, and skeleton to be activated. Stimuli like force trauma, vibration, extreme temperature, or inflammation/swelling activate these receptors. The pain is often described as:
Aching
Gnawing
Cramping
Sharp
Somatic pain is often localized to a particular area that is constant and stimulated by movement. There are two types.
Superficial painoccurs when everyday injuries activate pain receptors in the skin and mucous membranes.
Deep somatic pain occurs when stimuli activate pain receptors deeper in the body, including the tendons, joints, bones, and muscles. Deep body pain usually feels more like aching.
Pain can be confined to a local area or radiate to other areas of the body, depending on the extent of the injury.
Somatic pain can come from a variety of different potential causes that include:
Injury to joints or bones.
Trauma.
Fall or collision that damages connective tissues.
Sometimes these reflexes can stay in the on position and keep the body from achieving full relaxation.
In the nervous system, a body part is stimulated, and the message travels through the spinal cord and into the brain. The information is processed, then sent back through the spinal cord to the level that activates the specific body part. The reflexes transmit faster staying at the same spinal level without having to travel to the brain and back again.
During reflex pain, the body’s muscles are unable to relax, which is necessary for motion/movement. This prolonged contraction generates added pain and causes imbalances that can decrease excitabilityin the muscles. This can increase the activation of brain receptors that receive pain signals to respond by telling them to shorten and contract.
Therapy
Body misalignment can cause muscles to spasm, causing the nerves to stretch in an awkward way, compress, and get twisted and tangled around other nerves or other tissues. This disrupts communication resulting in pain, illness, and ailments that can lead to other health problems. Chiropractic care can address reflex pain by realigning the spine and improving joint motion and nerve conduction.
Chiropractic restores the body to its full and proper function by activating the natural healing abilities. Manual and mechanical spinal decompression realigns the vertebrae, reducing swelling, blockages, and nerve stress. A comprehensive examination will identify potential dysfunctional areas of the body using palpitations to identify which muscles are involved. Once identified, chiropractic, massage, and physical therapy options can be prescribed to rebalance the body’s muscles, and restore their ability to contract and relax normally.
Patient education will be provided concerning self-assessment techniques, instruction on how to treat pain, and an anti-inflammatory diet.
An exercise and stretching program will help maintain the adjustments, keep the body flexible, and strengthen the body.
Patients are helped to understand how to take control of their pain.
Spinal Decompression Testimonials
References
Biurrun-Manresa J, Neziry A, Curatolo M, Arendt-Nielson L, Anderson O. Test-retest reliability of the nociceptive withdrawal reflex and electrical pain thresholds after single and repeated stimulation in patients with chronic low back pain. Eur J Appl Physiol. 2011;111:83-92
Derderian C, Tadi P. Physiology, Withdrawal Response. [Updated 2021 Nov 12]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: www.ncbi.nlm.nih.gov/books/NBK544292/
Muir, J M, and H Vernon. “Complex regional pain syndrome and chiropractic.” Journal of manipulative and physiological therapeutics vol. 23,7 (2000): 490-7. doi:10.1067/mmt.2000.108816
Neziri A, Haesler S, Steen P, et al. Generalized expansion of nociceptive reflex receptive fields in chronic pain patients. Pain. 2010;151(3):798-805
Szynkowicz, Peter, and Anthony Petrucci 4th. “Chiropractic Care of a Patient With Complex Regional Pain Syndrome Type 1 (CRPS-1): A Case Report.” Journal of chiropractic medicine vol. 19,2 (2020): 145-151. doi:10.1016/j.jcm.2020.05.001
Yezierski R, Vierck C. Reflex and pain behaviors are not equivalent: Lessons from spinal cord injury. Pain. 2010;151(3):569-577
Sciatica is a radiculopathy, which is irritation of the nerve as it exits the spine and is typically caused by compression/pinching along the nerve’s path. Most sciatica cases improve within a few weeks of the injury incident. Left untreated, it can become chronic sciatica and can have long-term repercussions and effects. A herniated disc is the most common cause if it bulges next to the nerve; it can pinch off the nerve or leak fluid onto the nerve, causing inflammation, swelling, pain, numbness, and weakness. Another common cause is spinal stenosis. As the body ages, the canal through which the nerve and spinal cord run can begin to narrow, placing pressure on the nerves. Then there are muscle spasms, spinal fractures, and spinal cancer. Anything that changes the curvature of the spine, including pregnancy, can cause sciatica.
Repercussions From Sciatica
The repercussions can vary or be a combination that includes:
Chronic Pain
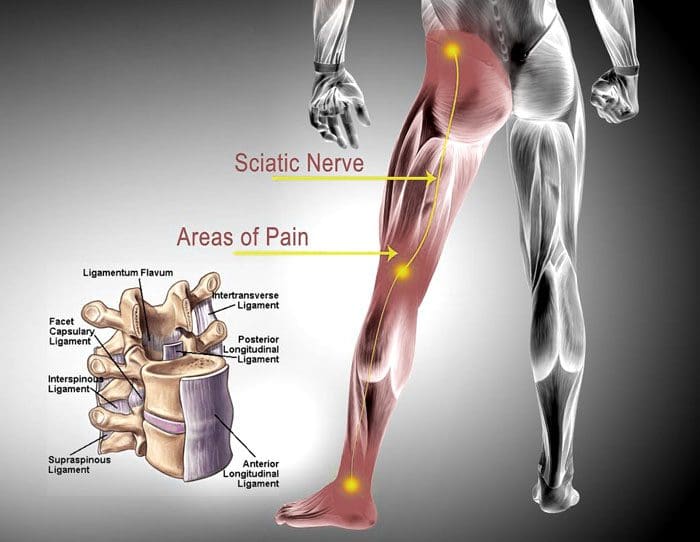
The pain can be anywhere along the nerve; typically, it travels from the lower spine through the buttocks, down the back of the leg, and into the foot.
The condition can cause various types of pain: Burning, electrical, or shooting pain in the low back.
Symptoms can come and go and may present only when sitting, standing, lying, or engaged in a particular activity.
The severity of the pain can vary from mild to severe, mildly uncomfortable, to limiting function.
Posture Problems
When the body experiences chronic pain in a localized area, the body’s natural reaction is to avoid placing pressure, twisting or bending, or using a specific body part, manipulating healthy posture or walking gait to protect the low back or legs from pain.
This is referred to as muscle/posture guarding, which removes pressure from the site but alters the body’s natural alignment, affecting the spine’s characteristics and causing adverse side effects, like upper back and neck pain, headaches, and fatigue.
Unhealthy and awkward postures can negatively affect digestion, organ function, and breathing.
Loss of Balance
Sciatica commonly causes numbness and tingling in the leg, calf, foot, and toes.
The hidden danger behind numbness; it alters the body’s proprioception or awareness of its position.
When proprioception becomes inhibited or altered, communication signals from the body to the brain/vice versa get jumbled/interrupted, confusing the brain, throwing the body off balance.
Sciatica is more problematic if the pain comes with neurological symptoms like numbness, muscle, or leg weakness.
This means there is an increased level of possible nerve damage if muscular weakness, which requires aggressive treatment.
Declining Reflexes
Depending on where the nerve is compressed, pain and numbness can affect the lower leg area and feet.
Damage to the nerve can cause the inability to flex the foot up.
The knee-jerk reflex, known as the patellar reflex, is the kicking motion of the lower leg when tapped on the patellar tendon.
Sciatica can numb the area, causing a delayed reaction or severe unresponsiveness to stimulation.
Permanent Nerve Damage
If left untreated, neurological symptoms like numbness and leg weakness can progress to permanent nerve damage.
However, this happens rarely but explains the importance of taking the injury seriously so full recovery is achievable.
Non-Surgical Sciatica Relief
References
Berry, James A et al. “A Review of Lumbar Radiculopathy, Diagnosis, and Treatment.” Cureus vol. 11,10 e5934. Oct 17 2019, doi:10.7759/cureus.5934
Davis D, Maini K, Vasudevan A. Sciatica. [Updated 2022 Feb 4]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: www.ncbi.nlm.nih.gov/books/NBK507908/
Giuffre BA, Jeanmonod R. Anatomy, Sciatic Nerve. [Updated 2021 Jul 29]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: www.ncbi.nlm.nih.gov/books/NBK482431/
Nori, Subhadra L. and Michael F. Stretanski. “Foot Drop.” StatPearls, StatPearls Publishing, Dec 15, 2021.
The sciatic nerve is the largest in the body and is created by five nerve roots that come together and exit the lower spine. It goes through the buttocks on either side and down the thighs all the way to the heels and soles of the feet. The sciatic nerve connects the spinal cord to the muscles of the thigh, leg, and foot. Any type of pain and/or neurological symptom/s that comes from the sciatic nerve is known as sciatica. The symptoms can be felt along the nerve’s path. This could be the:
When the nerve is compressed, neurological symptoms can accompany the pain. These include:
Thigh muscle weakness
If the thigh muscles are affected, weakness can be felt when bending or flexing the knee.
Leg and foot muscle weakness
Weakness can be felt while attempting to bend the knee or pointing the foot/toes upward/downward. This can lead to foot drop, which makes lifting the front part of the foot when walking difficult. Difficulty can also present when getting up from a sitting position or walking on the tiptoes.
Numbness
Loss of sensation can happen when the nerve impulses/transmissions cannot pass all the way through. Common areas affected by numbness are the:
Side of the calf
Side of the heel
Bottom of the foot
Top of the foot
Paresthesia
This is an abnormal sensation felt on the skin. It is brought on by improper nerve transmission. This sensation can include:
Tingling
Tightness
Pins-and-needles
Crawling feeling along the back of the thigh and/or leg
The Sciatic Nerve Gets Affected
The sciatic nerve can become:
Irritated
Compressed
Inflamed
This lumbar/low back radiculopathy means that the pain originates in and around the lumbar and/or sacral/sacrum nerve roots.
Compression
Physical forces could affect the nerve following common conditions:
Disc Herniation
A disc in the lower back can bulge or herniate. This causes irritation that can lead to compression of a nerve root.
Stenosis
Stenosis means the opening where the sciatic nerve exit into the buttocks begins to get narrow in size. This creates a clog with the other nerve roots that compresses or irritates the sciatic nerve. Degenerative changes in the spine like the thickening of the facet joint capsules and/or ligaments can also compress the sciatic nerve.
Instability
Instability of a vertebral segment happens when one vertebra slips over the one below it, known as spondylolisthesis. There are also vertebral defects like spondylolysis which is a complete dislocation of one or more vertebrae. This can directly compress the sciatic nerve roots.
Inflammatory Response
The body’s own chemicals can irritate the nerve causing inflammation. These chemical irritants include:
Hyaluronic acid
Fibronectin protein fragments leak out of degenerated or herniated discs onto and around the sciatic nerve roots.
There are times when degenerated discs can cause nerve tissues to grow into a disc. The tissue penetrates the outer and inner layers of the disc, causing inflammation and pain.
Some studies have shown how an immune system response can contribute to sciatic pain when there is exposure to the disc material from herniated disc/s.
Glycosphingolipids which are fats, and neurofilaments which are protein polymers. They are secreted by the immune system and have been found to have high levels in individuals with sciatica. It is believed they are released in reaction to the nerve roots and exposed disc material. This can lead to inflammation of the sciatic nerve.
Body Composition
The physical characteristics of an individual can also affect the sciatic nerve. Research has shown an increased risk of sciatica in:
Overweight individuals
Obese individuals
Older individuals
Tall individuals
Work Injuries
Individuals with certain jobs can have an increased risk of developing sciatica. Examples include:
Semi-Truck operators
Machine operators
Construction workers
Hairstylists
Office workers
Athletes that lift weights
This comes from:
Sitting for long amounts of time
Poor posture
Constant bending forward or sideways
Regularly lifting the arms above shoulder level
All are risk factors.
Vitamin B12 deficiency
Adequate levels of vitamin B12 are important for nerve health. Vitamin B12 supports the myelin sheath that covers and protects the nerves. It is important in nerve function and in transmitting impulses. Sciatica can present from vitamin B12 deficiency. However, this is more common in individuals 60+.
Body Analysis
Alleviating Nerve Pain Through Clinical Nutrition
Clinical nutrition is a powerful tool to help alleviate sciatica. Many individuals can relieve their pain through diet adjustments. Here are a few diet tips to alleviate sciatic nerve pain through clinical nutrition:
Sometimes, sciatica can be triggered by constipation from an unhealthy diet
Oily fish like salmon and halibut are rich in omega 3 fatty acids
Fresh pineapples and berries are anti-inflammatories that support healing and boost the immune system
2-3 cups of green tea
Add turmeric, ginger, and garlic to meals
B-Vitamins are important to take in when going through sciatica and are found in green peas, spinach, navy beans, nuts, bananas
Foods that are rich in A-Vitamins like dairy products, dark leafy vegetables, orange-colored fruits, eggs, and oily fish
Foods rich in C-Vitamins, like citrus and tomatoes
K-Vitamins like broccoli and spinach
Drink plenty of water, between 6 to 8 glasses a day
Foods to Avoid
Nutritionists recommend cutting out meat products except for oily fish for the first two weeks.
Foods that contain sunflower oil, corn oil, sesame oil, margarine, and partially hydrogenated oil.
Stressor foods like caffeine, processed food, soda, refined sugars, and chocolate.
Alcohol
References
Giuffre BA, Jeanmonod R. Anatomy, Sciatic Nerve. [Updated 2018 Dec 16]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: www.ncbi.nlm.nih.gov/books/NBK482431/.
Heuch I, Heuch I, Hagen K, Zwart JA. Association between body height and chronic low back pain: a follow-up in the Nord-Trøndelag Health Study [published correction appears in BMJ Open. 2015;5(10):e006983]. BMJ Open. 2015;5(6):e006983. Published 2015 Jun 15. doi:10.1136/bmjopen-2014-006983.
Kumar, M. Epidemiology, pathophysiology and symptomatic treatment of sciatica: A review. nt. J. Pharm. Bio. Arch. 2011, 2.
Quero L, Klawitter M, Schmaus A, et al. Hyaluronic acid fragments enhance the inflammatory and catabolic response in human intervertebral disc cells through modulation of toll-like receptor 2 signaling pathways. Arthritis Res Ther. 2013;15(4): R94. Published 2013 Aug 22. doi:10.1186/ar4274.
Shiri R, Lallukka T, Karppinen J, Viikari-Juntura E. Obesity as a Risk Factor for Sciatica: A Meta-Analysis. American Journal of Epidemiology. 2014;179(8):929-937. doi:10.1093/aje/kwu007.
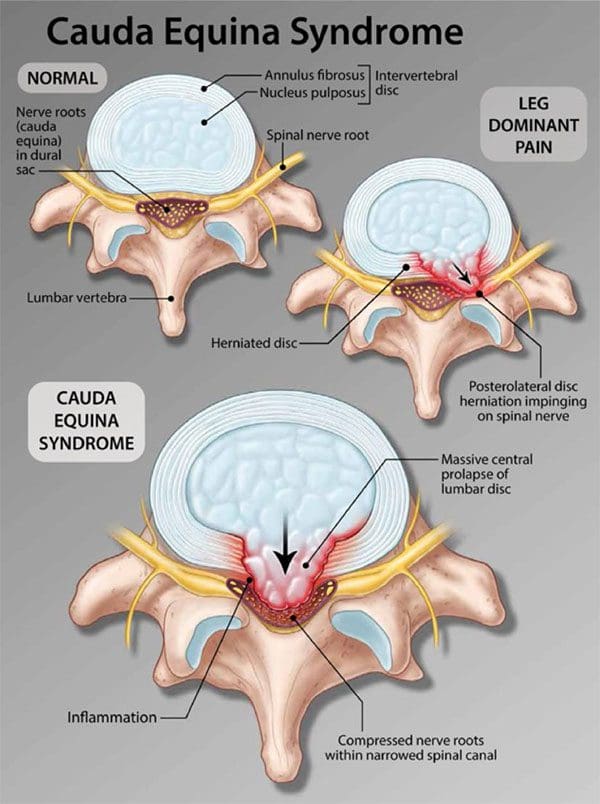
Cauda equina syndrome is an emergency that needs to be treated as soon as possible. It is a form of spinal nerve compression, but if left untreated, it can lead to permanent paralysis of one or both legs and permanent loss of bowel/bladder control. Lower back pain after sitting for too long or improperly lifting something heavy happens to most if not all of us.
However, sometimes pain in the lower back can be an indicator of something more serious. Especially, for individuals that are dealing with or managing back pain. One condition is cauda equina syndrome. It�s not like sciatica or arthritis, but it does have specific symptoms that individuals should be aware of.
Cauda Equina Syndrome
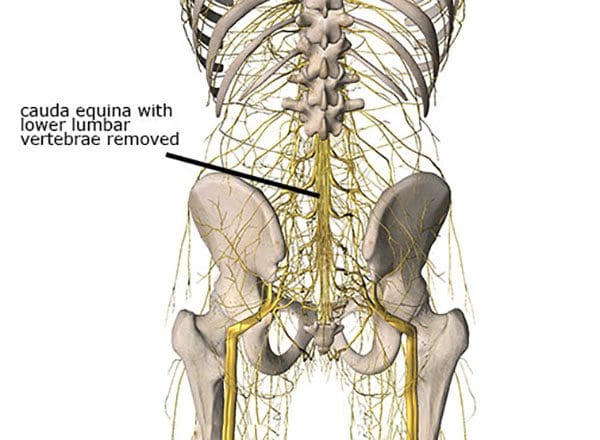
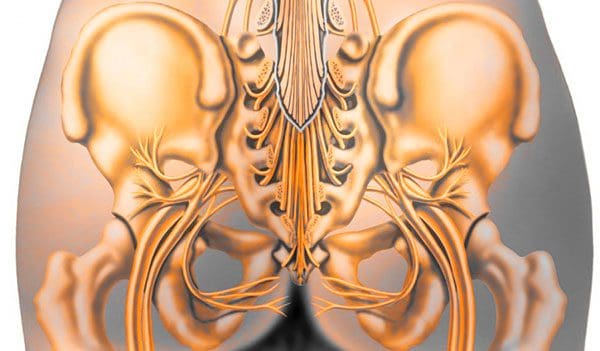
The term comes from Latin that means horse�s tail. The cauda equina forms the group of nerves that run through the lumbar spinal canal. Generally, the condition means two things:
There is nerve compression of most of the lumbar spinal canal
Compression symptoms like numbness or weakness in the leg/s
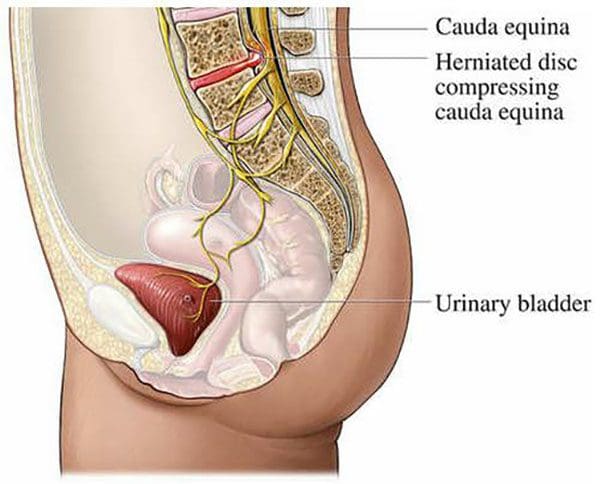
How cauda equina syndrome differs from typical compression of the lumbar spinal canal is that it can be caused by different issues, from fractures, tumors, and infections. More commonly, it is disc herniations that cause the problems. The key difference is the degree of nerve compression, and the number of nerves compressed.
For example, compression of a single nerve will not cause loss of bladder function. But compression of multiple nerves, especially the sacral nerves can cause loss of function. Nerve compression that leads to pain or numbness can be treated differently. Surgery is reserved for severe cases and for individuals that are not improving with non-invasive treatment.
Sneaky Presentation
One of the major factors is long-term compression that individuals do not realize they have. Individuals are more likely to be aware of symptoms from another spinal condition before cauda equina syndrome presents. However, the condition presents quickly but often other overlapping back problems mask cauda equina syndrome.
Causes
The syndrome can be brought on from anything that compresses the nerves. Most commonly, it is a root compression from degenerative processes, specifically lumbar disc herniations. Other causes include:
A doctor will examine any significant changes in bladder, bowel, or leg function that are considered red flags prompting an early and complete assessment. A physician will ask for a complete/detailed history of the onset and progression of symptoms.
The second is a close physical examination which includes testing sensation and strength along with a rectal exam to assess voluntary contraction. Also checking the body’s reflexes, assess walking gait and alignment. If most or all of the symptoms are presenting this will set in motion spinal imaging or an MRI. If the symptoms, exam, and imaging match, it will lead to an emergency admission to the hospital.
Body Composition Spotlight
Obesity and Osteoarthritis Connection
A variety of factors contribute to the development of osteoarthritis, including genetic factors and lifestyle choices. Research supports obesity is a significant risk factor in the development of osteoarthritis. It is pretty straightforward as body weight increases this equals increased load on the spine, and joints, especially the weight-bearing ones like the hips and knees. Increased pressure leads to early wearing, tearing, and eventual development of osteoarthritis. Added weight affects the body’s biomechanics and gait patterns.
However, obesity has also been shown to be a risk factor even on the non-weight-bearing joints. This is based on adipose tissue, which is more than just insulation. Adipose tissue is metabolically active and is involved in the secreting adipokines and cytokines which promote an inflammatory response. Pro-inflammatory adipokines and cytokines can have detrimental effects on joint tissue including damage to cartilage, synovial joints, and subchondral bone. The effect of inflammation on the joints in the body can contribute to the development of osteoarthritis.
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at�915-850-0900. The provider(s) Licensed in Texas& New Mexico*
Functional neurology primarily focuses on the fundamentals of neuron health and it is mainly based on neuroplasticity theories. It’s believed that the brain and the nervous system are capable of changing, and can become malleable, due to a reaction to certain stimulation. The brain can be shaped by sensory, motor, cognitive, or emotional experiences. �
The creation of synapses in the nervous system depends on the stimulation they receive. Neurons which receive too much stimulation are the ones which become stronger and those which don’t receive stimulation become weaker and eventually diminish. It is believed that it is possible to create new neurons even after there has been damage to the nervous system. �
The Role of Functional Neurology
Functional neurology evaluates changes in the nervous system before these become severe health issues. The practice of functional neurology has been adopted by several modalities of practice, such as chiropractic, psychology, occupational therapy and even by conventional healthcare professionals. Functional neurology is commonly practiced by chiropractors. �
The practice of neurology involves applying neuroscience research from laboratory studies to determine how it can be practically applied in health care. The brain is protected by supporting the nervous system. The ultimate goal of functional neurology is to treat brain and nervous system health issues without the utilization of drugs or together with conventional treatment approaches. Functional neurologists can help treat a wide variety of neurological health issues, including: �
Neurodegenerative disorders: Alzheimer�s disease, Parkinson�s disease, dementia, and multiple system atrophy.
Demyelinating conditions: Multiple sclerosis, transverse myelitis, and leukodystrophies.
Trauma and brain injuries: Concussions and whiplash-associated disorders.
Vestibular conditions: Motion sickness, dizziness/disequilibrium, labyrinthitis, vertigo, and Meniere’s disease.
Movement disorders: Tics, restless leg syndrome, myoclonus, and dystonia.
Neuro-developmental conditions: Autism spectrum disorders, ADHD, Asperger’s syndrome, Tourette syndrome, dyslexia, processing disorders, and global developmental delay.
Headaches and pain syndromes: Cluster headaches, complex regional pain syndrome, migraines, and fibromyalgia
Functional neurological disorders which are best referred to as a group of physical, sensory and cognitive symptoms which do not seem to have an identifiable organic etiology.
Functional Neurology Treatment
The primary goal of functional neurology is to promote, support, and restore the optimal function of the brain and the nervous system, as opposed to the absence of pathology. Sometimes it’s not always possible to determine the natural source of a person’s neurological disease and its symptoms. Functional neurology can be particularly beneficial in these instances. �
The patient’s medical history and a non-invasive evaluation are required for diagnosis. Treatment is determined based on the patient’s current and targeted well-being. Any blood tests, x-rays, MRIs and/or other tests are also evaluated. During the evaluation, the healthcare professional will observe all aspects of the patient, including eye movements and posture, which can demonstrate the function of the brain and the nervous system. Blood pressure, pulse, and reflexes are also evaluated. �
Neuro-developmental conditions and behavioral disorders are generally treated with functional neurology. Anxiety is commonly increased in patients with these type of health issues, therefore, it is recommended that the non-invasive evaluation is performed in a way which does not trigger anxiety in the patient. Functional neurology treatment is individualized and every part of the treatment approach is customized to the individual’s treatment requirements. �
Functional neurology emphasizes on encouraging patients to practice self-care so that face-to-face treatment with a healthcare professional does not continue for months or years without end. Home exercise programs are developed to treat the associated health issues, meaning that functional neurology treatment is incorporated into the patient’s daily activities. �
Biochemistry and Nutrition in Functional Neurology
Functional neurology treatment focuses on retraining the brain. Neurons need energy and stimulation to survive and thrive, therefore, functional neurology treatment may involve exercises, such as eye exercises, cognitive activities, balancing activities, and joint adjustments. Different stimulation can affect different regions and pathways in the human brain. �
Moreover, functional neurology treatment may also involve a nutritional and biochemical approach by eliminating several factors which may potentially affect neurons. These can ultimately include toxins, chemicals, and infection, among other factors. Dietary modifications and supplementation may also be included to provide optimal energy for neurons. �
An individualized treatment approach is applied to each individual otherwise there exists the risk of over-stimulating and exceeding the capacity of a patient’s nervous system. The goal of functional neurology treatment is to improve brain and nervous system health, neural processing, communication, and all signaling involving the brain and the entire human body. �
Functional neurology focuses on the diagnosis and treatment of the human brain and the nervous system utilizing sensory and cognitive based treatment methods and techniques to promote, support, and restore neuroplasticity, integrity, and functional optimization. Functional neurology can be utilized to help improve a variety of neurological diseases and health issues, including Alzheimer’s disease. Functional neurology is frequently practiced by chiropractors. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
The purpose of the article above is to discuss the purpose of functional neurology in the treatment of neurological disease. Neurological diseases are associated with the brain, the spine, and the nerves. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force. �
Glutamate is the main excitatory neurotransmitter in the central nervous system, or CNS, of mammals and it primarily interacts with both metabotropic and ionotropic receptors to activate and regulate postsynaptic responses. Both AMPA and NMDA receptors are fundamental mediators of synaptic plasticity, the ability of synapses to strengthen or weaken, where dysregulation of those receptors leads to neurodegeneration in a variety of disorders, including Alzheimer’s disease. �
The main difference between AMPA and NMDA receptors is that sodium and potassium increases in AMPA receptors where calcium increases along with sodium and potassium influx in NMDA receptors. Moreover, AMPA receptors do not have a magnesium ion block while NMDA receptors do have a calcium ion block. AMPA and NMDA are two types of ionotropic, glutamate receptors. They are non-selective, ligand-gated ion channels, which mainly enable the passage of sodium and potassium ions. Furthermore, glutamate is a neurotransmitter which creates excitatory postsynaptic signals in the CNS. �
�
What are AMPA Receptors?
AMPA, also known as ?-amino-3-hydroxy-5-methyl-4-isoxazole-propionate, receptors are glutamate receptors which are in charge of maintaining the rapid, synaptic transmission in the central nervous system. AMPA receptors have four subunits, GluA1-4. Moreover, the GluA2 subunit is not permeable to calcium ions because it contains arginine from the TMII region. �
Furthermore, AMPA receptors are involved in the transmission of the majority of the rapid, excitatory synaptic signals. The increase of the post-synaptic response depends on the amount of receptors in the post-synaptic surface. The type of agonist which activates the AMPA receptors is ?-amino-3-hydroxy-5-methyl-4-isoxazole propionic acid. The activation of the AMPA receptors leads to the non-selective transportation of cations, such as sodium and potassium ions, into the cell. This generates an action potential in the postsynaptic membrane. Figure 1 below demonstrates a diagram of AMPA receptors. �
What are NMDA Receptors?
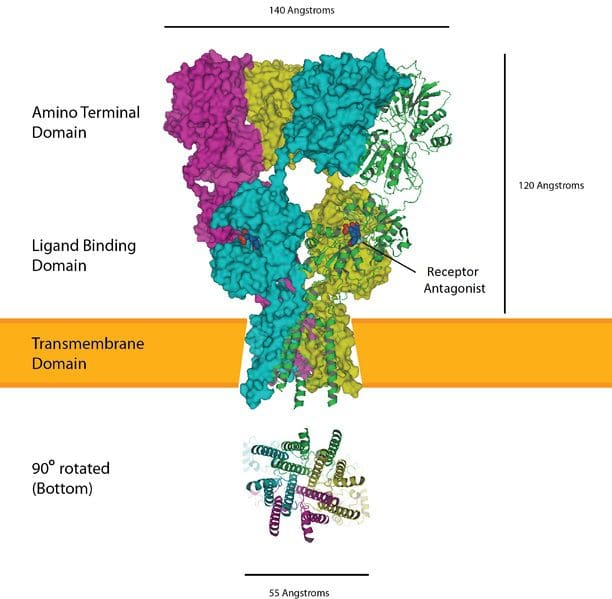
NMDA, also known as N-methyl-d-aspartate, receptors are glutamate receptors which are found in the postsynaptic membrane. The NMDA receptors are made up of two varieties of subunits: GluN1 and GluN2. The GluN1 subunit is fundamental for the role of the receptor. This subunit can associate with one of the four types of GluN2 subunits, GluN2A-D. �
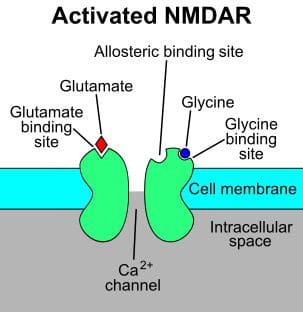
Furthermore, the main utilization of the NMDA receptors is to maintain the synaptic response. In the resting membrane potential, these receptors are inactive due to the creation of a magnesium block. The agonist of the NMDA receptor is N-methyl-d-aspartic acid. L-glutamate, including glycine, can connect to the receptor to activate it. Upon stimulation, NMDA receptors activate the calcium influx along with the potassium and sodium influx. Figure 2 demonstrates NMDA receptors. �
Similarities Between AMPA and NMDA Receptors
AMPA, NMDA, and kainate receptors are the three main types of glutamate receptors.
These are ligand-gated ion channels which activate and regulate sodium and potassium ions.
These are known due to the type of agonist which activates the receptor.
Moreover, the activation of these receptors produces excitatory postsynaptic responses or ESPSs.
Furthermore, several protein subunits connect together to form these receptors.
Difference Between AMPA and NMDA Receptors
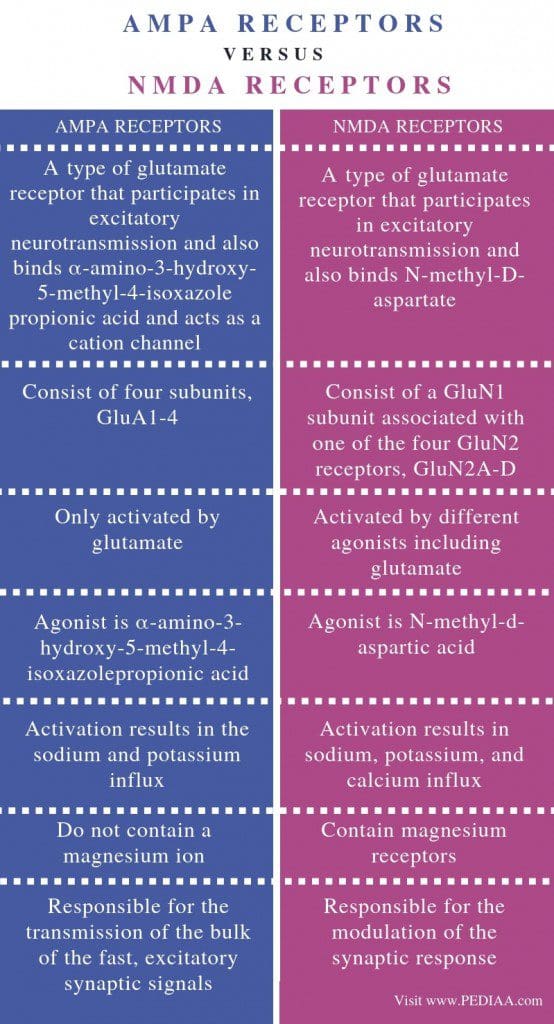
AMPA receptors are best known as a type of glutamate receptor which activates in excitatory neurotransmission and connects ?-amino-3-hydroxy-5-methyl-4-isoxazole propionic acid which additionally works as a cation channel. Where the NMDA receptors are best known as a type of glutamate receptor which helps in excitatory neurotransmission and also connects N-methyl-D-aspartate. This is the most fundamental difference between AMPA and NMDA receptors. �
AMPA receptors have four subunits, GluA1-4 while NMDA receptors have a GluN1 subunit associated with one of the four GluN2 receptors, GluN2A-D. Activation can also be a difference between AMPA and NMDA receptors. AMPA receptors are only activated by glutamate while NMDA receptors are activated by different agonists. The agonist for AMPA receptors is ?-amino-3-hydroxy-5-methyl-4-isoxazole propionic acid where the agonist for NMDA receptors is N-methyl-d-aspartic acid. �
Ion influx is a fundamental difference between AMPA and NMDA receptors. Activation of AMPA receptors results in the sodium and potassium influx while the activation of NMDA receptors leads to an increase in potassium, sodium, and calcium. Another distinction between AMPA and NMDA receptors is that AMPA receptors do not contain a calcium ion where NMDA receptors contain magnesium receptors. Also, AMPA receptors are responsible for the transmission of the majority of the rapid, excitatory synaptic signals while NMDA receptors are responsible for the modulation of the synaptic response. �
AMPA receptors are glutamate receptors which lead to the influx of sodium and potassium ions. NMDA receptors are another type of glutamate receptors which result in the influx of calcium ions with potassium and sodium ions. The main difference between AMPA and NMDA receptors is the type of ion influx associated with their activation and regulation. �
Several varieties of ionotropic glutamate receptors have been demonstrated in the following article. Three of these main excitatory neurotransmitter in the central nervous system, or CNS, are ligand-gated ion channels best known as AMPA receptors, NMDA receptors, and kainate receptors. These ionotropic glutamate receptors are best referred to after the agonists which activate and regulate them: AMPA or ?-amino-3-hydroxy-5-methyl-4-isoxazole-propionate, NMDA or N-methyl-d-aspartate, and kainic acid. – Dr. Alex Jimenez D.C., C.C.S.T. Insight
The purpose of the article above is to demonstrate the difference between AMPA and NMDA receptors for brain health. Neurological diseases are associated with the brain, the spine, and the nerves. The scope of our information is limited to chiropractic, musculoskeletal and nervous health issues as well as functional medicine articles, topics, and discussions. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900 . �
Curated by Dr. Alex Jimenez �
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
�
For your convenience and review of the XYMOGEN products please review the following link.*XYMOGEN-Catalog-Download �
* All of the above XYMOGEN policies remain strictly in force. �
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine

 Leg Adjustments
Leg Adjustments








 �
�