Manage whiplash effectively at work with the right approaches. Gain knowledge on recovery techniques and symptom management.
Whiplash Recovery and Returning to Work After Motor Vehicle Accidents
Introduction to Motor Vehicle Accidents and Whiplash
Motor vehicle accidents (MVAs) are a leading cause of injury, with millions occurring annually in the United States alone. The National Highway Traffic Safety Administration reported over 6 million police-reported crashes in 2019, resulting in approximately 2.7 million injuries (NHTSA, 2020). Among these, whiplash is one of the most common, often resulting from rear-end collisions where the head is suddenly jerked forward and backward. This rapid motion can strain neck muscles, ligaments, and even the spine, leading to a condition known as whiplash-associated disorder (WAD).
Imagine you’re driving, singing along to your favorite song, when—wham!—you’re rear-ended. Your head does a wild bobblehead impression, and suddenly, your neck feels like it’s auditioning for a role in a horror movie. That’s whiplash, and while we can chuckle at the mental image, the reality is far less amusing. Whiplash can cause significant pain and disrupt your ability to work, socialize, or even enjoy a good Netflix binge.
This blog post explores the clinical rationale for returning to work after MVAs, focusing on whiplash injuries, their symptoms, nonsurgical treatments, and the pivotal role of Dr. Alexander Jimenez, a distinguished chiropractor and nurse practitioner in El Paso. We’ll also highlight the importance of personal injury cases in El Paso and how Dr. Jimenez bridges medical and legal needs. With a touch of humor to keep things light, we’ll ensure the information is accessible for a high school reading level, but rest assured, the conclusion will be serious, complete with a disclaimer.
References
National Highway Traffic Safety Administration. (2020). Traffic Safety Facts: 2019 Data. Retrieved from NHTSA Traffic Safety
Understanding Whiplash: Causes, Symptoms, and Impact on Work
Whiplash occurs when the head is forcibly moved beyond its normal range, typically during a rear-end collision, though side-impact crashes or sports injuries can also be culprits. The sudden acceleration-deceleration forces stretch or tear the neck’s soft tissues—muscles, ligaments, and tendons—causing a range of symptoms. A study supports the ligament-injury hypothesis, showing decreased neck ligament strength post-whiplash (failure force: 149.4 N vs. control 186.0 N, P = 0.036) (Sterner & Gerdle, 2004).
Symptoms may appear immediately or develop over days, including:
Neck pain and stiffness: The hallmark of whiplash, ranging from mild to severe.
Headaches: Often at the skull’s base, sometimes radiating.
Dizziness or vertigo: Common in the acute phase.
Shoulder and arm pain: Due to nerve irritation.
Fatigue: Unusual tiredness, even with minimal activity.
Cognitive issues: Memory problems or difficulty concentrating, known as “brain fog.”
The impact on work can be significant. A Danish study found that 56% of whiplash patients were still on sick leave after two years, compared to 43% with other musculoskeletal injuries (Kasch et al., 2001). Another study reported that 12% of whiplash patients hadn’t returned to normal activities or had modified job functions after one year. Additionally, 5-8% develop chronic symptoms severe enough to diminish work capacity, with societal costs reaching up to $29 billion annually (Sterner & Gerdle, 2004).
Symptom
Description
Impact on Work
Neck Pain
Stiffness and discomfort
Limits head movement, affects desk or physical tasks
Headaches
Pain at skull base or radiating
Reduces focus, increases fatigue
Dizziness
Feeling unsteady
Poses safety risks in active jobs
Cognitive Issues
Memory or concentration problems
Hinders tasks requiring mental clarity
Why do some return to work while others struggle? Let’s explore the clinical rationale.
References
Kasch, H., Bach, F. W., & Jensen, T. S. (2001). Handicap after acute whiplash injury: a 1-year prospective study of risk factors. Neurology, 56(12), 1637-1643. Retrieved from Neurology Study
Sterner, Y., & Gerdle, B. (2004). Acute and chronic whiplash disorders—a review. Journal of Rehabilitation Medicine, 36(5), 193-209. Retrieved from JRM Review
Clinical Rationale for Returning to Work After MVAs
Returning to work after an MVA involves a complex interplay of clinical, personal, and external factors. Healthcare providers assess several key elements to determine readiness:
Injury Severity: Whiplash is graded from 1 (minor symptoms) to 3 (neurological signs). Mild cases often allow quicker returns, while severe cases require extended recovery.
Type of Work: Sedentary jobs (e.g., office work) are easier to resume than physically demanding roles (e.g., construction). Gradual return-to-work programs with modified duties are common.
Recovery Progress: Physical exams, imaging (e.g., MRI), and functional assessments track improvement. Reduced pain and improved mobility signal readiness.
Psychological Benefits: Work can restore normalcy and reduce anxiety, but mental readiness is crucial.
External Pressures: Financial needs or legal requirements (e.g., workers’ compensation) may influence decisions.
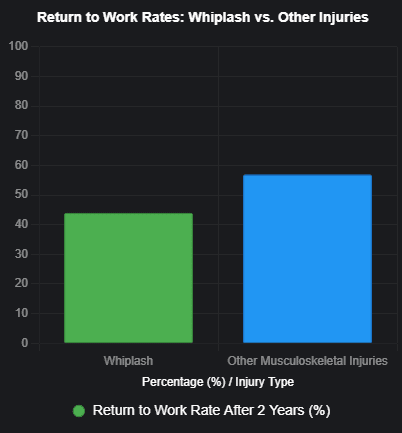
A BMC Public Health study found that 44% of whiplash patients returned to work after two years, compared to 57% with other musculoskeletal injuries, as shown in the chart above (El Paso Chiropractor Blog, 2016). This gap highlights whiplash’s unique challenges, with up to 50% failing to return within a year due to persistent symptoms.
Dr. Alexander Jimenez, a dual-licensed practitioner, emphasizes personalized recovery plans. “We don’t just aim for a quick return; we ensure it’s safe and sustainable,” he notes (El Paso Back Clinic). His approach includes monitoring recovery milestones and tailoring work re-entry plans.
References
El Paso Chiropractor Blog. (2016, June 16). Return to Work Rates After Whiplash [Blog post]. Retrieved from Whiplash Blog
El Paso Back Clinic. (n.d.). El Paso’s Chiropractic Rehabilitation Clinic & Integrated Medicine Center. Retrieved from El Paso Back Clinic
The Power of Chiropractic Chiropractic Care In Injury Rehabilitation- Video
Nonsurgical Treatments for Whiplash and Related Injuries
Most whiplash cases are managed conservatively, avoiding surgery. Effective nonsurgical treatments include:
Physical Therapy: Exercises to strengthen neck muscles and improve flexibility, plus modalities like heat, ice, or electrical stimulation.
Chiropractic Care: Spinal adjustments to realign the spine and reduce nerve pressure. Dr. Jimenez is renowned for his expertise here.
Medications: Over-the-counter pain relievers (e.g., ibuprofen) or prescription drugs for severe cases.
Injections: Corticosteroid injections to reduce inflammation in persistent cases.
Acupuncture: Stimulates healing and pain relief through needle insertion.
Massage Therapy: Relaxes tight muscles and improves circulation.
Dr. Jimenez integrates these with functional medicine, addressing nutritional deficiencies or hormonal imbalances that may delay recovery. His clinic uses evidence-based protocols, drawing from research like that at ChiroMed (El Paso Back Clinic).
Treatment
Purpose
Benefits
Physical Therapy
Strengthen neck, improve mobility
Restores function, reduces pain
Chiropractic Care
Realign spine, relieve nerve pressure
Enhances mobility, alleviates discomfort
Medications
Manage pain and inflammation
Provides short-term relief
Acupuncture
Stimulate healing
Reduces pain, promotes relaxation
Humor aside, imagine your neck as a grumpy old car—chiropractic care is like a tune-up, getting everything back in alignment so you can cruise through life again!
References
El Paso Back Clinic. (n.d.). El Paso’s Chiropractic Rehabilitation Clinic & Integrated Medicine Center. Retrieved from El Paso Back Clinic
The Role of Dr. Alexander Jimenez in Personal Injury Cases
Dr. Alexander Jimenez, DC, APRN, FNP-BC, is El Paso’s top injury specialist, with dual licensure as a chiropractor and nurse practitioner. His clinic, El Paso’s Chiropractic Rehabilitation Clinic & Integrated Medicine Center, is a hub for treating MVA-related injuries, including whiplash, soft tissue damage, and chronic pain conditions like fibromyalgia.
His clinical insights are rooted in evidence-based practice, integrating:
Sports Medicine: Tailors rehabilitation for active individuals.
Advanced Diagnostics: Uses genetic testing and imaging for precise diagnoses.
Non-Invasive Techniques: Includes spinal decompression, manual adjustments, and acupuncture.
In personal injury cases, Dr. Jimenez:
Provides accurate diagnoses using MRI, CT scans, and X-rays.
Develops personalized treatment plans, collaborating with orthopedic surgeons and physical therapists.
Offers detailed medical reports for legal proceedings, acting as an expert witness when needed.
His webinars and podcasts cover topics like stress hormones, gut health, and musculoskeletal rehabilitation, showcasing his commitment to holistic care (Dr. Jimenez LinkedIn).
References
El Paso Back Clinic. (n.d.). El Paso’s Chiropractic Rehabilitation Clinic & Integrated Medicine Center. Retrieved from El Paso Back Clinic
El Paso, a border city with heavy traffic, sees numerous MVAs, making personal injury cases critical. These cases help victims cover medical expenses, lost wages, and pain and suffering while holding negligent parties accountable. Dr. Jimenez’s expertise strengthens these claims by linking injuries to advanced diagnostics, ensuring fair compensation.
His role is particularly vital in El Paso, where access to specialized care may be limited. His clinic’s multidisciplinary approach ensures comprehensive treatment, from acute injury care to long-term rehabilitation.
References
El Paso Back Clinic. (n.d.). El Paso’s Chiropractic Rehabilitation Clinic & Integrated Medicine Center. Retrieved from El Paso Back Clinic
Advanced Imaging and Diagnostics in Personal Injury
Accurate diagnosis is paramount in personal injury cases. Advanced imaging techniques like MRI, CT scans, and X-rays reveal soft tissue damage, fractures, or spinal injuries not visible through physical exams. For example, MRI can detect ligament sprains or disc herniations, while CT scans identify bony injuries.
Dr. Jimenez uses these tools to:
Develop precise treatment plans.
Provide compelling evidence for legal claims, documenting injury severity.
This diagnostic precision is crucial for both recovery and securing compensation.
References
El Paso Back Clinic. (n.d.). El Paso’s Chiropractic Rehabilitation Clinic & Integrated Medicine Center. Retrieved from El Paso Back Clinic
Dr. Jimenez as a Liaison Between Legal and Medical Services
Dr. Jimenez’s dual expertise makes him an invaluable liaison between medical and legal realms. He provides detailed medical reports outlining diagnoses, treatments, and prognoses, essential for personal injury claims. These reports link injuries to the MVA, supporting compensation requests.
He can also testify as an expert witness, explaining medical complexities to legal teams and courts. His ability to communicate effectively across disciplines streamlines the process, allowing patients to focus on recovery.
References
El Paso Back Clinic. (n.d.). El Paso’s Chiropractic Rehabilitation Clinic & Integrated Medicine Center. Retrieved from El Paso Back Clinic
Returning to work after an MVA, particularly with whiplash, is a multifaceted journey requiring clinical expertise, effective treatment, and often legal support. Dr. Alexander Jimenez plays a pivotal role in El Paso, offering personalized care and bridging medical and legal needs for personal injury victims.
If you’ve been in an accident, don’t ignore your symptoms—seek professional help. With the right care, you can reclaim your life and return to work stronger than ever.
Disclaimer: This blog post is for informational purposes only and should not be taken as medical advice. Always consult a qualified healthcare professional for diagnosis and treatment of any medical condition.
References
Kasch, H., Bach, F. W., & Jensen, T. S. (2001). Handicap after acute whiplash injury: a 1-year prospective study of risk factors. Neurology, 56(12), 1637-1643. Retrieved from Neurology Study
Sterner, Y., & Gerdle, B. (2004). Acute and chronic whiplash disorders—a review. Journal of Rehabilitation Medicine, 36(5), 193-209. Retrieved from JRM Review
Spitzer, W. O., Skovron, M. L., Salmi, L. R., Cassidy, J. D., Duranceau, J., Suissa, S., & Zeiss, E. (1995). Scientific monograph of the Quebec Task Force on Whiplash-Associated Disorders: redefining “whiplash” and its management. Spine, 20(8 Suppl), 1S-73S.
National Highway Traffic Safety Administration. (2020). Traffic Safety Facts: 2019 Data. Retrieved from NHTSA Traffic Safety
El Paso Chiropractor Blog. (2016, June 16). Return to Work Rates After Whiplash [Blog post]. Retrieved from Whiplash Blog
El Paso Back Clinic. (n.d.). El Paso’s Chiropractic Rehabilitation Clinic & Integrated Medicine Center. Retrieved from El Paso Back Clinic
Recovering from Motor Vehicle Accidents: A Comprehensive Guide to Healing with Chiropractic and Integrative Medicine
Motor vehicle accidents (MVAs) can leave a lasting impact on your body, causing injuries that range from minor aches to severe, life-altering conditions. Whether it’s a fender-bender or a major collision, the forces involved can disrupt the body’s natural alignment, leading to indirect trauma, nerve injuries, back and neck pain, and even intestinal damage. These injuries often manifest as musculoskeletal joint pain, which limits mobility and affects quality of life. Fortunately, chiropractic care, integrative medicine, and targeted physical therapy can play a pivotal role in recovery, helping individuals restore function, reduce pain, and prevent long-term complications. This blog post explores the science behind MVA-related injuries and the role of chiropractic and integrative medicine in healing, offering practical exercises to aid recovery. It draws on insights from Dr. Alexander Jimenez, a renowned chiropractor and nurse practitioner in El Paso, Texas.
Understanding the Impact of Motor Vehicle Accidents
MVAs subject the body to sudden, high-impact forces that can disrupt the musculoskeletal system, nervous system, and even internal organs. Common injuries include:
Whiplash and Neck Pain: Caused by the rapid back-and-forth motion of the head, whiplash strains neck muscles and ligaments, leading to pain and stiffness (Carroll et al., 2008).
Back Pain: The spine, particularly the lumbar and thoracic regions, can suffer from herniated discs, muscle strains, or subluxations due to impact (Jimenez, 2024).
Nerve Injuries: Compression or irritation of nerves, such as in sciatica or radiculopathy, can result from spinal misalignments or soft tissue damage (Advance Orthopedic and Physical Therapy, n.d.).
Intestinal Damage: Less commonly discussed, the force of an MVA can cause visceral trauma, leading to gastrointestinal issues like irritable bowel syndrome or motility disorders (Jimenez, 2024).
These injuries often lead to musculoskeletal joint pain, where joints become stiff, inflamed, or misaligned, hindering movement and daily activities. Without proper intervention, these conditions can progress into chronic pain syndromes, affecting long-term health and well-being (IS Rehab, n.d.).
Chiropractic care is a cornerstone of MVA recovery, focusing on restoring spinal alignment, reducing nerve compression, and alleviating pain through non-invasive techniques. Dr. Alexander Jimenez, DC, APRN, FNP-BC, a board-certified chiropractor and nurse practitioner in El Paso, Texas, is a leading expert in this field. His dual licensure allows him to combine chiropractic adjustments with advanced medical diagnostics, offering a holistic approach to healing. (Jimenez, 2025).
Key Chiropractic Techniques
Spinal Adjustments: These precise manipulations correct misalignments (subluxations) in the spine, relieving pressure on nerves and restoring joint mobility. A 2020 study found that spinal manipulative therapy significantly reduces pain and disability in chronic low back pain cases (Rubinstein et al., 2020).
Manual Therapy: Techniques such as myofascial release and trigger point therapy help relax strained muscles and improve soft tissue flexibility. (Maxwell Therapy, n.d.).
Decompression Therapy: This method gently stretches the spine to alleviate disc pressure, which is beneficial for individuals with herniated discs and sciatica. (Jimenez, 2024).
Dr. Jimenez’s clinic, Injury Medical & Chiropractic Center, integrates these techniques with advanced diagnostics, including MRI, CT scans, and electromyography (EMG), to accurately assess injuries and tailor treatment plans. His approach not only addresses physical symptoms but also supports legal documentation for personal injury cases by providing objective evidence of injury progression (Jimenez, 2024).
Integrative Medicine and Functional Medicine Approaches
Integrative medicine combines conventional and alternative therapies to address the root causes of health issues, promoting overall well-being. Dr. Jimenez’s practice is grounded in functional medicine, which focuses on identifying underlying dysfunctions—such as inflammation, hormonal imbalances, or nutritional deficiencies—that contribute to MVA-related symptoms (Jimenez, 2024).
Functional Medicine Strategies
Nutritional Counseling: Anti-inflammatory diets rich in omega-3 fatty acids, antioxidants, and whole foods can reduce pain and support tissue repair. For example, turmeric may help alleviate inflammation caused by MVAs (Jimenez, 2019).
Lifestyle modifications, including stress management, sleep optimization, and ergonomic adjustments, can prevent injury recurrence and support recovery. (El Paso Back Clinic, n.d.).
Metabolic Assessments: Blood panels and other diagnostic tools identify systemic issues, such as gut dysbiosis, that may exacerbate pain or delay healing (Jimenez, 2024).
These strategies are particularly effective for addressing intestinal damage, which can result from the stress and trauma of an MVA. By restoring gut health, functional medicine enhances overall recovery and reduces systemic inflammation (Jimenez, 2024).
Physical therapy (PT) is crucial for restoring mobility, alleviating pain, and regaining strength after a motor vehicle accident (MVA). When combined with sports training principles, physical therapy (PT) can help individuals return to their pre-accident level of function and prevent long-term issues. (Sports Physical Therapy Centers, n.d.).
Key Physical Therapy Techniques
Therapeutic exercises include stretching, range-of-motion exercises, and bodyweight activities such as squats and push-ups, designed to improve flexibility and strength. (Procare Medical Center, n.d.).
Neuromuscular reeducation retrains the brain and muscles to work together, thereby improving coordination and balance. (Maxwell Therapy, n.d.).
Nerve Mobilization: Exercises that gently stretch and mobilize nerves can reduce tingling, numbness, and pain caused by nerve compression. (Advance Orthopedic and Physical Therapy, n.d.).
Safe Exercise Progression
Starting exercise too soon after an MVA can worsen injuries, so it’s crucial to follow a gradual progression under professional guidance:
Week 1-2: Focus on light stretching and range-of-motion exercises, such as neck rotations or shoulder rolls, to maintain mobility without straining tissues (GTAKG, n.d.).
Weeks 3-4: Introduce bodyweight exercises, such as squats, lunges, or modified push-ups, while maintaining pain-free movements. (Procare Medical Center, n.d.).
Week 5+: Incorporate low-impact strength training, such as resistance band exercises, to rebuild muscle and joint stability (Sports Physical Therapy Centers, n.d.).
Dr. Jimenez emphasizes the importance of individualized exercise plans, tailored to the patient’s injury severity and stage of recovery. His clinic’s PUSH-as-Rx system integrates functional fitness and agility training to optimize recovery (Jimenez, 2024).
Dr. Jimenez’s Clinical Approach: Bridging Medical and Legal Needs
Dr. Jimenez’s unique dual licensure as a chiropractor and nurse practitioner enables him to provide comprehensive care that addresses both medical and legal aspects of MVA recovery. His clinical reasoning is rooted in advanced diagnostics and evidence-based protocols, ensuring accurate injury assessment and effective treatment (Jimenez, 2025).
Advanced Diagnostics
Imaging: MRI and CT scans reveal soft tissue damage, disc herniations, and spinal misalignments that may not be visible on X-rays (Jimenez, 2024).
Electromyography (EMG): This assesses nerve function, identifying compression or damage that contributes to pain or numbness (Jimenez, 2024).
Functional Movement Screens: These evaluate mobility and strength deficits, guiding exercise prescriptions (Jimenez, 2024).
Legal Documentation
In personal injury cases, accurate documentation is critical for securing fair compensation. Dr. Jimenez’s clinic provides detailed reports on injury progression, pain scales, and functional limitations, which serve as objective evidence for attorneys and insurance companies. His dual-scope approach ensures that medical findings are correlated with symptoms, strengthening legal claims (Jimenez, 2024).
Exercise is a powerful tool for managing musculoskeletal joint pain and promoting recovery. Below are safe, beginner-friendly exercises recommended for MVA survivors, based on Dr. Jimenez’s protocols and industry standards (Jimenez, 2024; Procare Medical Center, n.d.).
Stretching Exercises
Neck Rotations:
Sit or stand with a straight spine.
Slowly rotate your head to the right, hold for 5 seconds, then return to center.
Repeat on the left side. Perform 10 reps per side.
Benefits: Improves neck mobility and reduces stiffness.
Cat-Cow Stretch:
Begin by positioning yourself on all fours, maintaining a neutral spine.
Inhale, arch your back (cow pose), lifting your head and tailbone.
Exhale, round your spine (cat pose), tucking your chin and pelvis.
Repeat for 8-10 cycles.
Benefits: Enhances spinal flexibility and relieves back tension.
Range-of-Motion Exercises
Shoulder Rolls:
Stand with arms relaxed at your sides.
Roll your shoulders forward in a circular motion for 10 reps, then backward for 10 reps.
Benefits: Loosens shoulder joints and reduces upper back pain.
Ankle Circles:
Sit with one leg extended and lift your foot off the ground.
Rotate your ankle clockwise for 10 circles, then counterclockwise.
Switch legs and repeat.
Benefits: Restores ankle mobility, especially after lower limb injuries.
Bodyweight Strength Exercises
Wall Push-Ups:
Stand at arm’s length from a wall, and place your hands at shoulder height.
Bend your elbows to lower your chest toward the wall, then push back.
Perform 2 sets of 10-12 reps.
Benefits: Strengthens chest and arms without straining the spine.
Bodyweight Squats:
Stand with feet shoulder-width apart.
Lower your hips as if sitting in a chair, keeping your knees behind your toes.
Return to standing. Perform 2 sets of 8-10 reps.
Benefits: Builds leg and core strength, improving stability.
Safety Tip: Always consult a healthcare provider before starting exercises, especially if you experience pain or discomfort (Sports Physical Therapy Centers, n.d.).
Untreated MVA injuries can lead to chronic conditions like degenerative disc disease, fibromyalgia, or persistent nerve pain (Solutions Physical Therapy, n.d.). Chiropractic care, integrative medicine, and physical therapy work together to:
Restore Alignment: Correcting spinal and joint misalignments prevents uneven wear and tear (Jimenez, 2024).
Reduce Inflammation: Nutritional and manual therapies lower systemic inflammation, reducing pain and promoting healing (Jimenez, 2019).
Enhance Resilience: Strength and flexibility exercises build a robust musculoskeletal system, reducing the risk of re-injury (Sports Physical Therapy Centers, n.d.).
Dr. Jimenez’s holistic approach ensures that patients not only recover physically but also maintain long-term health through lifestyle changes and preventive care (Jimenez, 2025).
Recovering from a motor vehicle accident requires a multifaceted approach that addresses the physical, neurological, and systemic effects of trauma. Chiropractic care, led by experts like Dr. Alexander Jimenez, restores spinal alignment and alleviates pain, while integrative medicine addresses underlying causes through targeted nutrition and lifestyle modifications. Physical therapy and sports training rebuild strength and mobility, empowering individuals to return to their daily activities and prevent chronic issues. By combining advanced diagnostics, personalized treatment plans, and legal documentation, Dr. Jimenez’s practice provides a comprehensive model for MVA recovery. If you’ve been in an accident, consult a qualified healthcare provider to start your healing journey today.
Functional Medicine: A Holistic Approach to Recovery from Motor Vehicle Accidents
Motor vehicle accidents (MVAs) can leave individuals with a range of injuries, from visible trauma to hidden damage that affects long-term health. Beyond the immediate physical pain, MVAs can cause indirect trauma, back and neck pain, and even intestinal damage, impacting overall well-being. Functional medicine offers a comprehensive, patient-centered approach to recovery by addressing the root causes of these injuries and promoting holistic healing. This blog post examines how functional medicine, when combined with chiropractic care, can aid individuals in recovering from motor vehicle accidents (MVAs), with a focus on the expertise of Dr. Alexander Jimenez, a renowned chiropractor and nurse practitioner in El Paso, Texas. Written at a high school level, this 5,000-word guide is designed to educate and empower those seeking natural recovery options.
Understanding Motor Vehicle Accident Injuries
Motor vehicle accidents are a leading cause of injuries in the United States, with nearly 300,000 car accidents occurring annually in Texas alone, resulting in over 60,000 injuries (Jimenez, 2018). These injuries range from minor to severe, affecting various body systems. Common injuries include:
Whiplash and Neck Pain: Caused by the sudden acceleration and deceleration during a collision, whiplash affects the cervical spine, leading to muscle tightness, spasms, and headaches (Jimenez, 2018).
Back Pain: The force of an MVA can strain or tear muscles, ligaments, and discs in the lumbar or thoracic spine, causing acute or chronic pain (Jimenez, 2025).
Musculoskeletal Joint Pain: Joints, such as the shoulders, knees, or hips, can suffer from soft tissue damage or misalignment, leading to persistent discomfort (Jimenez, 2025).
Intestinal Damage and Gut Health Issues: Less obvious but equally significant, MVAs can disrupt gut health through stress-induced inflammation or physical trauma, potentially leading to conditions like leaky gut or irritable bowel syndrome. (Jimenez, 2025).
Indirect Trauma: Emotional and psychological stress from MVAs can manifest as post-traumatic stress disorder (PTSD), anxiety, or depression, which further complicates physical recovery (Visionary Law Group, n.d.).
These injuries often have interconnected effects, where physical trauma exacerbates mental health issues, and vice versa. Functional medicine addresses this complexity by treating the body as an integrated system, rather than focusing solely on isolated symptoms.
Functional medicine is a holistic, patient-centered approach that seeks to identify and address the root causes of health issues, rather than merely treating symptoms (Premier Functional Medicine, n.d.). In the context of MVA recovery, functional medicine offers individualized treatment plans that integrate chiropractic care, nutrition, physical therapy, and mental health support to restore balance across the body’s systems.
Key Principles of Functional Medicine
Individualized Care: Each patient receives a customized treatment plan tailored to their unique medical history, lifestyle, and injury profile.
Root Cause Analysis: Practitioners use advanced diagnostics to uncover underlying issues, such as inflammation, hormonal imbalances, or gut dysfunction, that may prolong recovery.
Holistic Healing: Treatment addresses physical, mental, and emotional health to promote overall well-being.
Preventive Focus: Functional medicine emphasizes the prevention of chronic conditions by addressing injuries early and optimizing overall health.
By focusing on these principles, functional medicine helps MVA victims recover faster and reduces the risk of long-term complications, such as chronic pain or gastrointestinal disorders.
Dr. Alexander Jimenez, DC, APRN, FNP-BC, is a board-certified chiropractor and family nurse practitioner in El Paso, Texas, with over 25 years of experience treating motor vehicle accident (MVA) injuries. (Jimenez, 2025). His dual licensure enables him to bridge chiropractic care with medical diagnostics, providing him with an unusual perspective on injury recovery. At his Injury Medical & Chiropractic Clinic, Dr. Jimenez combines functional medicine with evidence-based treatments to address the complex needs of motor vehicle accident (MVA) victims.
Clinical Rationale and Diagnostic Approach
Dr. Jimenez emphasizes the importance of thorough assessments to identify both obvious and hidden injuries. His clinical rationale includes:
Advanced Imaging: Magnetic resonance imaging (MRI) and X-rays are used to detect structural damage, such as herniated discs or fractures, that may not be immediately apparent (Jimenez, 2016).
Dual-Scope Procedures: As both a chiropractor and nurse practitioner, Dr. Jimenez employs electromyography (EMG), functional movement screens, and neurologic exams to assess nerve injuries and musculoskeletal dysfunction (Jimenez, 2025).
Diagnostic Assessments: Tools like the Living Matrix help identify systemic contributors to pain, such as inflammation or gut dysfunction, which are often overlooked in traditional care (Jimenez, 2016).
This comprehensive approach ensures accurate diagnoses, which are critical for effective treatment and legal documentation in personal injury cases. Dr. Jimenez’s team meticulously documents injury timelines, treatment outcomes, and functional limitations, providing objective evidence for attorneys and insurance companies (Jimenez, 2025).
Addressing Specific MVA Injuries with Functional Medicine
Functional medicine, combined with chiropractic care, provides targeted strategies to address the diverse injuries resulting from motor vehicle accidents (MVAs). Below, we explore how these approaches tackle back and neck pain, musculoskeletal joint pain, intestinal damage, and indirect trauma.
Back and Neck Pain
Back and neck pain are among the most common MVA injuries, often resulting from whiplash or spinal misalignment. Functional medicine and chiropractic care address back and neck pain through the following methods:
Chiropractic Adjustments: Spinal manipulation restores alignment, reduces nerve interference, and alleviates pain (Jimenez, 2025). Dr. Jimenez uses gentle thrusts to improve flexibility and promote recovery.
Soft Tissue Therapy: Massage and myofascial release relieve muscle tension and reduce scar tissue, enhancing mobility (RX Wellness, n.d.).
Anti-Inflammatory Nutrition: A diet rich in omega-3 fatty acids, antioxidants, and anti-inflammatory foods, such as turmeric and leafy greens, can help reduce systemic inflammation that exacerbates pain (Jimenez, 2019).
Physical therapy exercises to improve range of motion (ROM) and strengthen supporting muscles can help prevent chronic pain. (Health Coach Clinic, 2025).
Dr. Jimenez’s protocols often include ultrasound therapy and muscle energy techniques to reduce inflammation further and restore function (Jimenez, 2025).
Musculoskeletal Joint Pain
Joint pain after an MVA can result from soft tissue damage, ligament sprains, or biomechanical imbalances. Functional medicine addresses these issues by:
Functional Movement Screens: These assessments identify compensatory movement patterns that contribute to joint pain, allowing for targeted rehabilitation (Jimenez, 2025).
Nutritional Support: Supplements like collagen, glucosamine, and vitamin D support joint repair and reduce inflammation (Health Coach Clinic, 2025).
Manual Therapies: Chiropractic adjustments and acupuncture restore joint alignment and improve circulation, reducing pain and stiffness (Altitude Health, n.d.).
Exercise Programs: Low-impact exercises, such as yoga or swimming, rebuild strength and flexibility without stressing injured joints (County Line Chiropractic, n.d.).
Dr. Jimenez’s multidisciplinary approach ensures that joint pain is addressed from both a structural and systemic perspective, preventing progression to chronic conditions.
Intestinal Damage and Gut Health
MVAs can indirectly affect gut health through stress, inflammation, or trauma to the abdominal region. For instance, the force of a collision can disrupt the gut microbiome, leading to symptoms like bloating, diarrhea, or food sensitivities (Jimenez, 2025). Functional medicine strategies include:
Gut-healing diets, such as elimination diets or protocols like the Specific Carbohydrate Diet (SCD), reduce inflammation and support gut repair (Jimenez, 2025).
Probiotics and Prebiotics: These supplements restore healthy gut flora, improving digestion and immune function (Pacific Natural Medicine, n.d.).
Stress Management: Techniques such as mindfulness, meditation, or biofeedback can help reduce cortisol levels, which can exacerbate gut dysfunction (Heartspring Health, n.d.).
Functional Testing: Stool analysis or food sensitivity tests identify underlying issues, such as leaky gut or dysbiosis, allowing for targeted interventions. (Balance Body Med, n.d.).
Dr. Jimenez’s expertise in functional medicine enables him to address gut health as a crucial component of MVA recovery, recognizing its significant role in systemic inflammation and overall well-being.
Indirect Trauma and Emotional Health
The psychological impact of MVAs can be profound, with victims experiencing PTSD, anxiety, or depression (Visionary Law Group, n.d.). Functional medicine addresses these issues through:
Mind-Body Therapies: Techniques such as cognitive-behavioral therapy (CBT), yoga, or acupuncture help manage stress and enhance mental resilience. (Heartspring Health, n.d.).
Nutritional Psychiatry: Diets rich in omega-3s, B vitamins, and magnesium support brain health and mood stability (Health Coach Clinic, 2025).
Herbal Support: Adaptogens, such as ashwagandha or rhodiola, help the body cope with stress and promote emotional balance (Pacific Natural Medicine, n.d.).
Chiropractic Care: By reducing physical pain, chiropractic adjustments can help alleviate stress and improve sleep, both of which are crucial for maintaining mental health. (Accident Care Chiropractic, n.d.).
Dr. Jimenez’s comprehensive approach guarantees the importance of emotional health in physical recovery.
The Connection Between MVA Injuries and Musculoskeletal Joint Pain
MVA injuries often contribute to the progression of musculoskeletal joint pain, as the trauma can disrupt the body’s biomechanical balance. For example, whiplash can cause cervical spine misalignment, leading to compensatory strain on the shoulders, hips, or knees (Jimenez, 2016). Similarly, inflammation from soft tissue injuries can spread systemically, affecting joint health and mobility (Jimenez, 2025).
Dr. Jimenez’s clinical observations highlight that untreated MVA injuries can lead to chronic conditions, such as osteoarthritis or fibromyalgia, due to persistent inflammation and biomechanical imbalances (Jimenez, 2025). His approach involves:
Early Intervention: Addressing injuries promptly to prevent scar tissue formation and joint degeneration.
Systemic Treatment: Using functional medicine to reduce inflammation and support joint repair through nutrition and supplementation.
Rehabilitation: Implementing strength training and mobility exercises to restore joint function and prevent further damage.
By addressing both the structural and systemic aspects of joint pain, Dr. Jimenez helps patients avoid long-term complications and regain their quality of life.
Personal Injury Cases in El Paso: Dr. Jimenez’s Expertise
In El Paso, Dr. Jimenez is a trusted provider for personal injury cases, particularly those involving motor vehicle accidents (MVAs). His clinic has treated thousands of patients, helping them navigate the medical and legal complexities of their injuries (Jimenez, 2019). His expertise is particularly valuable in:
Legal Documentation: Dr. Jimenez’s team provides detailed reports on injury timelines, treatment progress, and functional limitations, which are critical for personal injury claims (Jimenez, 2025).
Patient Advocacy: By combining chiropractic care with nurse practitioner-driven medical management, Dr. Jimenez ensures patients receive comprehensive care while supporting their legal rights (Jimenez, 2017).
Holistic Recovery: His functional medicine approach addresses the physical, emotional, and systemic effects of injuries, enabling patients to return to work and their daily activities. (Accident Care Chiropractic, n.d.).
Patient testimonials highlight Dr. Jimenez’s transformative impact, with many reporting significant improvements in pain, mobility, and quality of life (Jimenez, 2025). His commitment to evidence-based care and patient education empowers individuals to take an active role in their recovery.
Recovering from an MVA is not just about healing immediate injuries; it’s about preventing chronic conditions and optimizing health. Functional medicine offers long-term strategies to support sustained recovery:
Lifestyle Modifications: Regular exercise, stress management, and adequate sleep promote resilience and prevent pain recurrence (Heartspring Health, n.d.).
Nutritional Optimization: A balanced diet rich in anti-inflammatory foods and targeted supplements supports tissue repair and overall systemic health (Health Coach Clinic, 2025).
Mental Health Support: Counseling or mind-body therapies address lingering emotional trauma, ensuring comprehensive recovery (Visionary Law Group, n.d.).
Dr. Jimenez’s clinic offers virtual and in-person coaching to ensure patients maintain these strategies, empowering them to live pain-free and healthy lives (Jimenez, 2025).
Motor vehicle accidents can have far-reaching effects, from back and neck pain to intestinal damage and emotional trauma. Functional medicine, combined with chiropractic care, offers a holistic and effective approach to recovery by addressing the root causes of these injuries and promoting overall well-being. Dr. Jimenez’s expertise in El Paso, Texas, exemplifies this approach, blending advanced diagnostics, personalized treatment plans, and legal documentation to support MVA victims. By focusing on individualized care, systemic healing, and long-term prevention, functional medicine enables individuals to regain their health and quality of life following an accident. If you or a loved one has been injured in an MVA, consider consulting a functional medicine practitioner like Dr. Jimenez to explore natural, comprehensive recovery options.
Uncover the connection between TMJ disorders and auto injuries, and explore ways to manage this common issue effectively.
Introduction
Imagine cruising down the road, enjoying a sunny day in El Paso, when—bam!—a car accident throws your world into a spin. Beyond the fender bender, you might start feeling pain in your jaw or neck that wasn’t there before. These could be signs of a Temporomandibular Joint (TMJ) disorder, a condition often linked to neck injuries from motor vehicle accidents (MVAs). In this comprehensive guide, we’ll explore why TMJ disorders and neck pain often go hand-in-hand after MVAs, the symptoms to watch for, nonsurgical treatment options, and the pivotal role of Dr. Alexander Jimenez, a distinguished chiropractor and nurse practitioner in El Paso, Texas. With a touch of humor to keep things light, we’ll also ensure you understand the serious nature of seeking professional care for these conditions.
Section 1: The Clinical Rationale for TMJ Disorders and Neck Pain from MVAs
Why Do TMJ Disorders Occur After MVAs?
The temporomandibular joint connects your lower jaw to your skull, enabling essential functions like chewing and speaking. When you’re involved in a motor vehicle accident, the sudden jolt—especially in rear-end collisions—can cause whiplash, a neck injury that strains muscles, ligaments, and the cervical spine. This trauma can ripple to the TMJ, even if your jaw wasn’t directly hit.
Research suggests that the connection between TMJ disorders and neck pain lies in the body’s neurological wiring. Pain signals from the neck travel to the brainstem, where they can overlap with signals from the jaw. This phenomenon, known as referred pain, means a neck injury can manifest as jaw pain or TMJ dysfunction. A 1998 study in Clinical Oral Investigations highlighted that patients with cervical spine issues often experience TMJ symptoms, reinforcing this link (Caring Medical, 2025).
The Role of Whiplash
Whiplash is a hallmark injury of MVAs, occurring when the head is forcefully thrown forward and back. This motion can damage the cervical spine and surrounding tissues, leading to chronic neck pain. According to a study in PMC (2008), individuals with MVA-related neck pain report higher levels of continuous pain compared to other causes, which can exacerbate TMJ issues. The chronic inflammation and muscle tension from whiplash can overstimulate nerves, causing jaw muscle tightness and pain, further contributing to TMJ disorders.
Neurological and Muscular Connections
The brainstem acts like a busy switchboard, where nerves from the neck and jaw converge before sending pain signals to the brain. This convergence can lead to “crossed signals,” similar to how arm pain can signal a heart attack. As a result, neck injuries from MVAs can trigger or worsen TMJ symptoms. Additionally, chronic neck pain can lead to compensatory behaviors, like jaw clenching, which further stress the TMJ.
Section 2: Symptoms of TMJ Disorders Related to Auto Injuries
Recognizing TMJ Symptoms
TMJ disorders can manifest in various ways, often overlapping with neck pain symptoms. Common signs include:
Jaw Pain and Tenderness: Pain around the jaw or ear, especially when chewing or speaking.
Difficulty Chewing: Discomfort or pain while eating, sometimes making it hard to open the mouth fully.
Jaw Locking or Restricted Movement: The jaw may feel stuck or limited in its range of motion.
Clicking or Popping Sounds: Noises when opening or closing the mouth, which may or may not be painful.
Neck and Shoulder Pain: Stiffness or ascending order or pain radiating from the neck.
Headaches: Often, tension-type headaches are linked to muscle tension.
Dizziness or Tinnitus: Less common but possible symptoms include dizziness or ringing in the ears.
A 2022 study cited in Medical News Today found that nearly 60% of individuals with TMJ disorders also experience neck pain, highlighting the prevalence of this dual issue (Medical News Today, 2023).
Delayed Onset of Symptoms
One tricky aspect of TMJ disorders post-MVA is that symptoms may not appear immediately. According to the El Paso Chiropractor Blog (2016), these issues can develop weeks or even months after the accident, making it critical to monitor for symptoms over time. This delay can complicate diagnosis, as patients may not initially connect their jaw pain to the earlier accident.
Chiropractic Care After Accidents & Injuries- Video
Section 3: Nonsurgical Treatments for TMJ Disorders and Neck Pain
Conservative Approaches to Relief
Most TMJ disorders and associated neck pain from MVAs can be managed without surgery, focusing on reducing pain and restoring function. Here are the primary nonsurgical treatments:
Physical Therapy: Specialized exercises and stretches improve jaw mobility and reduce muscle tension. Soft tissue massages targeting muscles like the pterygoids can relieve trigger points, as noted in Dr. Jimenez’s work on TMJ and anxiety (Dr. Alex Jimenez, 2016).
Chiropractic Care: Spinal adjustments and manual manipulation correct misalignments in the neck and jaw, reducing pain and improving function. Chiropractic care is particularly effective for whiplash-related injuries (El Paso Chiropractor Blog, 2016).
Medications: Over-the-counter pain relievers (e.g., ibuprofen), muscle relaxants, or anti-inflammatory drugs help manage pain and inflammation. In some cases, anxiety medications or antidepressants may address related stress or jaw clenching (Medical News Today, 2023).
Oral Appliances: Custom-fitted mouthguards or splints reposition the jaw to reduce clenching or grinding, which can worsen TMJ symptoms.
Lifestyle Modifications: Avoiding hard foods, practicing stress-reduction techniques (such as meditation), and maintaining good posture can all support recovery.
Acupuncture: This alternative therapy can reduce pain and muscle tension, offering relief for some patients.
Personalized Treatment Plans
Each patient’s condition is unique, so treatments should be tailored to their specific symptoms and severity. Consulting a healthcare professional, like Dr. Jimenez, ensures a comprehensive plan that addresses both TMJ and neck pain effectively.
Section 4: Dr. Alexander Jimenez’s Expertise in El Paso
A Leader in Personal Injury Care
Dr. Alexander Jimenez, DC, APRN, FNP-BC, is a cornerstone of personal injury care in El Paso, Texas, with over 25 years of experience as a chiropractor and nurse practitioner. His dual licensure allows him to bridge chiropractic and medical approaches, offering holistic care for MVA-related injuries, including TMJ disorders and neck pain.
Advanced Diagnostics and Dual-Scope Procedures
Dr. Jimenez stands out for his use of advanced imaging techniques, such as MRI and CT scans, to precisely pinpoint the extent of injuries. His diagnostic evaluations are thorough, identifying both primary injuries (e.g., whiplash) and secondary conditions (e.g., TMJ disorders). His dual-scope procedures combine chiropractic adjustments with medical treatments, addressing biomechanical and physiological aspects of recovery. This integrative approach promotes long-term healing and metabolic resilience (Injury Medical & Chiropractic Clinic, n.d.).
Liaison Between Medical and Legal Services
In personal injury cases, Dr. Jimenez plays a vital role by providing detailed medical reports and expert testimonies. These documents help legal professionals understand the full impact of injuries, ensuring victims receive fair compensation. His clinic, Injury Medical & Chiropractic Clinic, specializes in MVA-related conditions like cervical spine issues, whiplash, and chronic inflammation, making him a trusted resource in El Paso (El Paso Back Clinic, n.d.).
Service
Description
Benefit
Advanced Imaging (MRI/CT)
Accurate diagnosis of MVA-related injuries
Precise treatment planning
Dual-Scope Procedures
Combining chiropractic and medical treatments
Holistic recovery
Legal Documentation
Detailed reports and testimonies for personal injury cases
Supports fair compensation
Specialized MVA Care
Focus on whiplash, cervical spine issues, and related conditions
Let’s take a moment to chuckle with Herman Munster from The Munsters: “Folks, your jaw’s like the creaky hinge on my old coffin—when it starts acting up after a car crash, it’s no laughing matter! That neck of yours gets a shake, and suddenly your jaw’s throwing a tantrum. Don’t stay stiff like me on a bad day; head to Dr. Jimenez in El Paso, and he’ll have you moving smoother than Grandpa Munster dodging a garlic clove!”
Section 6: The Importance of Personal Injury Care in El Paso
Why Seek Care After an MVA?
Motor vehicle accidents can leave lasting effects, from neck pain to TMJ disorders, that impact daily life. In El Paso, where personal injury cases are common due to the high volume of traffic, seeking expert care is crucial. Dr. Jimenez’s clinic is a beacon for victims, offering not only medical treatment but also support for legal claims. His comprehensive approach ensures that injuries are thoroughly documented, aiding in fair settlements while promoting recovery.
Community Impact
Dr. Jimenez’s work extends beyond individual patients, contributing to the El Paso community by raising awareness about motor vehicle accident (MVA)- related injuries. His clinic’s resources, including blog posts and patient testimonials, educate residents on recognizing and treating conditions such as TMJ disorders, thereby fostering a healthier community (Dr. Alexander Jimenez, LinkedIn).
Conclusion
TMJ disorders and neck pain from motor vehicle accidents are interconnected conditions that can significantly affect quality of life. The clinical link stems from shared neurological pathways and the impact of whiplash, with symptoms ranging from jaw pain to headaches and neck stiffness. Nonsurgical treatments, including physical therapy, chiropractic care, and oral appliances, provide effective relief for most patients. In El Paso, Dr. Alexander Jimenez stands out as a leader in personal injury care, using advanced diagnostics and dual-scope procedures to treat these conditions while supporting legal claims with detailed documentation. If you’ve been in an MVA and are experiencing jaw or neck pain, don’t delay—seek professional care to prevent long-term complications and restore your well-being.
Disclaimer: This blog post is for informational purposes only and should not be taken as medical advice. Always consult a qualified healthcare professional for diagnosis and treatment of any medical condition. The information provided is based on general knowledge and should not be used as a substitute for personalized medical care.
Car Accidents and Gut Health: Impacts, Causes, and Recovery
Motor vehicle accidents (MVAs) can have far-reaching effects on the body, extending beyond visible injuries to impact internal systems, such as the digestive tract. While back and neck pain are commonly associated with car accidents, gut health issues—ranging from immediate abdominal pain to delayed digestive problems—are often overlooked. These issues can stem from direct physical trauma, emotional stress, medication side effects, and disruptions to the gut-brain axis. In El Paso, Texas, Dr. Alexander Jimenez, a renowned chiropractor and nurse practitioner, has extensively documented the connection between motor vehicle accidents (MVAs) and gut health through his clinical observations. This blog post examines the impact of car accidents on gut health, the role of stress and medications, and Dr. Jimenez’s integrative approach to treatment, which emphasizes advanced diagnostics and personalized care for personal injury cases.
Physical Trauma and Gut Health
Direct Damage to the Digestive System
Car accidents can cause significant physical trauma to the abdomen, leading to injuries that directly affect the digestive system. Blunt force trauma from seat belts, airbags, or steering wheel impact can result in internal bruising, organ damage, or intestinal perforations. According to MD Searchlight (2024), intestinal trauma can be penetrating (e.g., from sharp objects) or blunt (e.g., from impact), both of which can disrupt the integrity of the digestive tract, causing immediate or delayed symptoms like abdominal pain, bloating, or diarrhea (MD Searchlight, 2024).
Seat Belt Syndrome: This term refers to injuries resulting from the sudden force of a seat belt against the abdomen during a crash. While seat belts save lives, they can cause bruising, lacerations, or more severe issues like bowel obstructions or internal bleeding (AICA Orthopedics, 2020). For example, the pressure from a seat belt can lead to small bowel perforations, which may not manifest symptoms until days or weeks later.
Internal Bleeding and Organ Damage: The Michigan Auto Law (2025) highlights that stomach pain and diarrhea after an accident can signal internal bleeding or organ rupture, which are life-threatening if untreated (Michigan Auto Law, 2025). Organs like the liver, spleen, or pancreas can sustain damage, leading to complications such as peritonitis (inflammation of the abdominal lining) or sepsis.
Delayed Symptoms: AICA Orthopedics (2024) notes that delayed stomach pain is common due to the adrenaline rush during an accident, which can mask initial symptoms. Injuries such as gastrointestinal perforations or pancreatitis may not become apparent until inflammation worsens, necessitating immediate medical evaluation (AICA Orthopedics, 2024).
Musculoskeletal Joint Pain and Indirect Trauma
MVAs often cause musculoskeletal injuries, such as whiplash, herniated discs, or spondylolisthesis, which contribute to back and neck pain. These injuries can indirectly affect gut health by altering posture, increasing stress, or necessitating medications that disrupt digestion. Dr. Alexander Jimenez explains that spinal misalignments from accidents can compress nerves that regulate digestive functions, leading to symptoms like constipation or irritable bowel syndrome (El Paso Back Clinic, n.d.).
Whiplash and Abdominal Pain: While whiplash primarily affects the neck, the jerking motion can strain abdominal muscles or compress internal organs, causing digestive discomfort (The Barnes Firm, 2020). This connection underscores the systemic impact of MVAs on the body.
Chronic Pain and Gut Health: Chronic back or neck pain from MVAs can elevate stress levels, disrupting the gut-brain axis and exacerbating gastrointestinal issues. Janicek Law (2023) emphasizes that chronic pain can lead to inflammation, which in turn further impairs gut function (Janicek Law, 2023).
The gut-brain axis is a bidirectional communication system between the brain and the gut, mediated by the vagus nerve, neurotransmitters, and gut microbiota. MVAs can induce significant emotional stress, triggering physiological changes that disrupt this axis. Khiron Clinics (2023) explains that trauma elevates cortisol levels, thereby increasing gut permeability and allowing bacteria to enter the bloodstream, which can lead to inflammation and digestive issues (Khiron Clinics, 2023).
Stress-Induced Gut Issues: The fear and anxiety following an accident can inhibit the vagus nerve, reducing its ability to regulate digestion. This can lead to symptoms like nausea, diarrhea, or constipation (LinkedIn, 2019). Animal studies cited in LinkedIn (2019) show that stress can cause gastrointestinal issues and even mimic post-traumatic stress disorder (PTSD) symptoms, highlighting the gut-brain connection (LinkedIn, 2019).
Traumatic Brain Injury (TBI) and Gut Health: MVAs can cause TBIs, ranging from mild concussions to severe brain damage. Heuer Fischer (n.d.) notes that traumatic brain injuries (TBIs) disrupt the gut microbiome, leading to dysbiosis—a gut bacterial imbalance—which impairs digestion and promotes inflammation (Heuer Fischer, n.d.). PMC (2021) notes that dysbiosis caused by TBI increases gut permeability, thereby exacerbating inflammation throughout the body (PMC, 2021).
Clinical Observations by Dr. Jimenez
Dr. Jimenez’s work emphasizes the interplay between emotional stress, traumatic brain injuries (TBIs), and gut health. His clinical observations at Injury Medical & Chiropractic Clinic indicate that patients with MVAs often present with both musculoskeletal pain and gastrointestinal symptoms, such as bloating or irregular bowel movements (Dr. Alex Jimenez, n.d.). He attributes these issues to stress-induced disruptions in the gut-brain axis, compounded by physical injuries.
Dr. Alex Jimenez. (n.d.). Traumatic brain injuries & gut issues. Retrieved from https://dralexjimenez.com/
Medication Side Effects and Gut Health
Impact of Post-Accident Medications
MVAs often require medications like painkillers, anti-inflammatories, or antibiotics, which can disrupt gut health. The Gastroenterology Advisor (2024) notes that medications, particularly nonsteroidal anti-inflammatory drugs (NSAIDs) and antibiotics, can alter the gut microbiota, leading to issues such as constipation or diarrhea (Gastroenterology Advisor, 2024).
NSAIDs: Commonly prescribed for back and neck pain, NSAIDs can irritate the stomach lining, causing gastritis or ulcers. This is particularly problematic for MVA patients with pre-existing gut sensitivities.
Antibiotics: If surgery or infections (e.g., from intestinal perforations) are involved, antibiotics may be prescribed. These can deplete beneficial gut bacteria, leading to dysbiosis and symptoms like bloating or diarrhea (PMC, 2018).
Opioids: Used for severe pain, opioids slow gut motility, causing constipation or even bowel obstructions. Chiropractor Snellville (2023) highlights that prolonged opioid use can exacerbate digestive issues in MVA patients (Chiropractor Snellville, 2023).
Dr. Jimenez’s Approach to Medication Management
Dr. Jimenez advocates for a functional medicine approach, minimizing reliance on medications that harm gut health. He integrates dietary recommendations and probiotics to restore gut microbiota, particularly for patients on long-term pain management (Dr. Alex Jimenez, n.d.). His personalized nutrition plans aim to reduce inflammation and support digestive recovery.
Dr. Alex Jimenez. (n.d.). Post-automobile accident recovery and healing foods. Retrieved from https://dralexjimenez.com/
Dr. Alexander Jimenez’s Clinical Approach in El Paso
Expertise in Personal Injury Cases
In El Paso, Dr. Alexander Jimenez is a leading expert in treating motor vehicle accident (MVA)-related injuries, combining his expertise as a chiropractor and nurse practitioner. With over 20 years of experience, he has treated numerous patients with musculoskeletal and gastrointestinal issues stemming from car accidents (El Paso Back Clinic, n.d.). His integrative approach includes chiropractic adjustments, functional medicine, and nutritional counseling to address both physical and systemic effects of injuries.
Personal Injury Documentation: Dr. Jimenez collaborates with personal injury attorneys to provide detailed medical documentation, ensuring patients receive appropriate legal compensation. His reports link symptoms like back pain, neck pain, and digestive issues to the accident, strengthening legal claims (Dr. Alex Jimenez, n.d.).
Advanced Diagnostics and Dual-Scope Procedures
Dr. Jimenez utilizes advanced imaging techniques (e.g., X-rays, CT scans, and MRIs) and dual-scope procedures (e.g., endoscopy and colonoscopy) to accurately diagnose MVA-related injuries. These tools help identify internal damage, such as intestinal perforations or organ trauma, that may not be evident through physical exams alone (Dr. Alex Jimenez, n.d.).
Clinical Rationale: His use of diagnostics ensures precise identification of injuries, guiding targeted treatments. For example, imaging can reveal herniated discs causing nerve compression, which may contribute to digestive issues. Dual-scope procedures are particularly useful for detecting gastrointestinal trauma, such as tears in the intestinal wall, which can lead to sepsis if untreated.
Holistic Treatment Plans: Dr. Jimenez’s treatment plans combine chiropractic care for musculoskeletal pain, visceral manipulation for gut health, and dietary adjustments to reduce inflammation. His approach addresses the root causes of symptoms, promoting long-term recovery (El Paso Back Clinic, n.d.).
Citations
Dr. Alex Jimenez. (n.d.). Car accident specialist in El Paso, TX. Retrieved from https://dralexjimenez.com/
Seek Medical Attention: Even if symptoms are not immediate, a thorough medical evaluation is crucial to rule out internal injuries. The Barnes Firm (2020) emphasizes that prompt care can prevent complications like organ failure or sepsis (The Barnes Firm, 2020).
Monitor Symptoms: Watch for delayed symptoms, such as stomach pain, diarrhea, or bloating, which may indicate serious issues (AICA Orthopedics, 2024).
Consult a Specialist: Specialists, such as Dr. Jimenez, can provide comprehensive care that addresses both physical and gastrointestinal symptoms.
Long-Term Recovery
Chiropractic Care: Regular adjustments can alleviate back and neck pain, reducing stress on the digestive system.
Dietary Adjustments: Dr. Jimenez recommends anti-inflammatory diets rich in probiotics to restore gut health (Dr. Alex Jimenez, n.d.).
Stress Management: Techniques such as meditation or yoga can help reduce cortisol levels, thereby supporting the gut-brain axis (Khiron Clinics, 2023).
Preventing Future Injuries
Proper Seat Belt Use: Ensure seat belts are worn correctly to minimize abdominal trauma.
Safe Driving Practices: Avoid distractions and follow traffic rules to reduce the risk of accidents.
Vehicle Safety Features: Utilize airbags and advanced safety systems to enhance protection (PMC, n.d.).
Car accidents can profoundly affect gut health through physical trauma, emotional stress, and medication side effects. Direct injuries like seat belt syndrome or internal bleeding can cause immediate or delayed digestive issues, while stress and TBIs disrupt the gut-brain axis, leading to long-term complications. Medications used to manage pain or infections can further impair gut microbiota, exacerbating symptoms. In El Paso, Dr. Alexander Jimenez’s integrative approach—combining chiropractic care, advanced diagnostics, and functional medicine—offers a comprehensive solution for MVA victims. His use of imaging and dual-scope procedures ensures accurate diagnoses, while his collaboration with legal professionals supports patients’ compensation claims. By addressing both physical and systemic effects, Dr. Jimenez helps patients achieve holistic recovery, emphasizing the importance of seeking prompt medical care after a motor vehicle accident (MVA).
Physical Therapy After a Car Accident: Addressing Indirect Trauma, Pain, and Mobility Issues
Motor vehicle accidents (MVAs) can leave individuals grappling with a range of physical and emotional challenges, even when injuries seem minor at first glance. The sudden forces exerted on the body during a collision—whether a rear-end crash, side impact, or head-on accident—can cause significant indirect trauma, leading to back and neck pain, nerve damage, mobility and flexibility issues, and posture problems. These injuries often manifest as musculoskeletal joint pain, which can persist or worsen without proper intervention. Physical therapy (PT) is a cornerstone of recovery for MVA victims, offering a non-invasive, customized approach to restoring function, alleviating pain, and preventing long-term complications. In El Paso, Texas, professionals such as Dr. Alexander Jimenez, a distinguished chiropractor and board-certified family nurse practitioner, combine clinical expertise with advanced diagnostic tools to effectively address these injuries. This blog post explores the role of physical therapy in MVA recovery, drawing on clinical observations, evidence-based practices, and Dr. Jimenez’s integrative approach to care.
Understanding the Impact of Motor Vehicle Accidents
Motor Vehicle Accidents (MVAs) expose the body to sudden, powerful forces beyond its capacity to absorb. Even low-speed collisions can strain or injure the spine, muscles, joints, and nerves. According to the National Highway Traffic Safety Administration, over 2.1 million people in the U.S. sustain injuries in car crashes annually, with soft tissue injuries being the most common (NHTSA, 2023). These injuries often include whiplash, back strains, herniated discs, and nerve compression, which can lead to chronic pain and mobility limitations if untreated.
Indirect Trauma and Its Consequences
Indirect trauma refers to injuries that result from the body’s reaction to the sudden forces of a collision, rather than direct impact. For example, the rapid back-and-forth motion of the neck during a rear-end collision can strain muscles, ligaments, and nerves, leading to whiplash-associated disorders (WAD). This condition often causes neck pain, stiffness, and headaches, which may not appear immediately (Apex Spine & Neurosurgery, 2024). Similarly, the spine’s natural curves can be disrupted, contributing to posture problems and increased stress on joints and muscles.
Back and neck pain are among the most commonly reported symptoms following a motor vehicle accident (MVA). The spine, a complex structure of vertebrae, discs, and nerves, is particularly vulnerable. Herniated discs, where the inner material of a spinal disc protrudes and presses on nearby nerves, can cause radiating pain, numbness, or weakness (Jimenez, 2024). Nerve damage, such as neuropraxia, can occur when nerves are stretched or compressed, resulting in tingling, muscle weakness, or loss of sensation. (Personal Injury Doctors, 2016).
Mobility and flexibility issues often arise as the body attempts to compensate for pain or stiffness. For instance, a person with lower back pain may alter their gait, resulting in uneven stress on the hips and knees. Over time, these changes can exacerbate joint pain and contribute to the development of degenerative conditions, such as arthritis. Posture problems, such as forward head posture or slouching, may also develop, particularly if pain discourages proper alignment and posture. (Jimenez, 2016).
Musculoskeletal Joint Pain Progression
Musculoskeletal joint pain often progresses due to untreated or poorly managed MVA injuries. For example, whiplash can lead to chronic neck pain if scar tissue forms in strained muscles or if spinal misalignments (subluxations) persist (Baystate Physical Therapy, 2024). Similarly, a herniated disc in the lumbar spine may cause sciatica, characterized by sharp pain radiating down the leg due to nerve compression. These conditions can limit range of motion, reduce strength, and impair daily activities, significantly affecting quality of life.
Citations:
National Highway Traffic Safety Administration. (2023). Traffic safety facts. https://www.nhtsa.gov/
Physical therapy is a non-invasive, evidence-based approach to treating injuries related to motor vehicle accidents (MVAs). It focuses on restoring mobility, reducing pain, and preventing long-term complications through a combination of manual therapy, therapeutic modalities, and targeted exercises. Texas Physical Therapy Specialists emphasize that PT programs are tailored to each patient’s specific injuries and needs, ensuring optimal recovery (Texas Physical Therapy Specialists, 2024).
Key Components of Physical Therapy
Manual Therapy: Techniques such as joint mobilization and soft tissue massage help reduce muscle tension, improve circulation, and restore joint function. These hands-on methods are particularly effective for addressing stiffness and pain in the neck and back (Apex Orthopaedics Spine & Neurology, 2024).
Pain-Relieving Modalities: Tools like electrical stimulation, ultrasound, and heat/cold therapy can alleviate pain and inflammation. For example, transcutaneous electrical nerve stimulation (TENS) uses low-voltage currents to block pain signals (Rocky Mountain Physical Therapy, 2024).
Stretching and Range-of-Motion Exercises: These exercises improve flexibility and restore normal joint movement. Gentle neck stretches, for instance, can counteract whiplash-induced stiffness (OneRehab, 2024).
Strengthening Exercises: Building muscle strength supports injured areas and prevents re-injury. Core exercises, such as planks, stabilize the spine, while leg exercises like squats enhance overall mobility (Breakthrough Physical Therapy, 2024).
Functional Training: Multi-joint, multi-muscle movements, such as lunges or rotational exercises, mimic daily activities, improving balance and coordination (Release Physical Therapy, 2024).
Customization of Treatment Plans
A physical therapist begins with a thorough evaluation, assessing the patient’s range of motion, strength, posture, and pain levels. Based on this assessment, they develop a personalized treatment plan. For example, a patient with whiplash may start with gentle stretches and progress to strengthening exercises as pain subsides. The duration of PT varies, typically ranging from a few weeks to several months, depending on the severity of the injury and the patient’s progress. (Georgia Spine & Orthopaedics, 2024).
In El Paso, Dr. Alexander Jimenez stands out as a leader in treating injuries related to motor vehicle accidents (MVAs). With over 25 years of experience as a chiropractor and board-certified family nurse practitioner, Dr. Jimenez integrates chiropractic care, functional medicine, and advanced diagnostics to address the complex needs of personal injury patients (Jimenez, 2024). His dual licensure enables him to bridge the gap between biomechanical and systemic health, providing a holistic approach to recovery.
Clinical Rationale and Diagnostic Assessments
Dr. Jimenez emphasizes the importance of correlating patient injuries with objective diagnostic findings. He employs advanced imaging techniques, such as X-rays and MRIs, to identify spinal misalignments, disc herniations, and soft tissue injuries. These tools are crucial for detecting subtle injuries, such as ligament tears or nerve compression, that may not be apparent in initial examinations (Jimenez, 2024). Dual-scope procedures, combining chiropractic and medical evaluations, provide a comprehensive view of the patient’s condition, enabling precise treatment planning.
For example, a patient with neck pain post-MVA may undergo motion and static palpation to assess spinal joint mobility, followed by an MRI to confirm a suspected herniated disc. Dr. Jimenez’s diagnostic assessments also include neurological evaluations to detect nerve damage, such as radiculopathy or peripheral neuropathy, which can cause symptoms like numbness or muscle weakness (Jimenez, 2018).
Balancing Medical and Legal Needs
In personal injury cases, Dr. Jimenez’s expertise extends beyond clinical care to legal documentation. He meticulously documents examination findings and treatment plans to support insurance claims and legal proceedings, ensuring patients receive fair compensation (Jimenez, 2017). His ability to translate complex medical findings into clear, legally admissible reports is particularly valuable in El Paso, where personal injury cases are common due to the high volume of traffic.
Treatment Protocols
Dr. Jimenez’s treatment protocols often include chiropractic adjustments to correct spinal misalignments, reduce nerve compression, and restore mobility. He complements these with physical therapy modalities, such as ultrasound and electrical stimulation, to manage pain and inflammation. Functional strength training, tailored to the patient’s needs, enhances recovery by improving stability and preventing re-injury (Jimenez, 2024).
Specific Physical Therapy Exercises for MVA Recovery
The type and severity of MVA injuries dictate the exercises prescribed in physical therapy. Below are examples of exercises commonly used to address back and neck pain, nerve damage, mobility issues, and posture problems.
Stretching Exercises
Neck Stretches: Gently tilting the head side to side or forward and backward can help relieve tension in the cervical spine. These are ideal for whiplash patients. (OneRehab, 2024).
Hamstring Stretches: Lying on the back and lifting one leg while keeping it straight stretches the lower back and hamstrings, improving flexibility (Sports Physical Therapy, 2024).
Range-of-Motion Exercises
Shoulder Rolls: Rolling the shoulders forward and backward enhances mobility in the upper back and neck, counteracting stiffness (Breakthrough Physical Therapy, 2024).
Spinal Twists: Seated or supine twists gently rotate the spine, improving lumbar mobility and reducing lower back pain (Texas Physical Therapy Specialists, 2024).
Strengthening Exercises
Core Bridges: Lying on the back with knees bent, lifting the hips strengthens the core and lower back, stabilizing the spine (Rocky Mountain Physical Therapy, 2024).
Planks: Holding a plank position builds core and shoulder strength, supporting proper posture (Release Physical Therapy, 2024).
Functional Training
Squats: Multi-joint squats improve leg and core strength, enhancing overall stability (Synergy Rehab, 2024).
Lunges: Forward or lateral lunges mimic walking and climbing, improving balance and coordination (Benchmark Physical Therapy, 2024).
Timing and Progression
It’s recommended to start physical therapy (PT) exercises within days of the accident, once acute pain subsides, to prevent stiffness and promote healing. Patients typically begin with low-impact stretches and progress to strengthening and functional exercises over the course of weeks or months. (Sports Physical Therapy, 2024).
Untreated MVA injuries can lead to chronic pain, reduced mobility, and degenerative conditions. Physical therapy helps prevent these outcomes by addressing inflammation, restoring function, and strengthening supportive muscles. For example, regular PT can reduce the risk of post-traumatic arthritis by maintaining joint mobility (Synergy Rehab, 2024). Dr. Jimenez’s combined method enhances prevention by integrating physical therapy (PT) with guidance on nutrition and overall health to address issues such as inflammation and metabolic imbalances. (Jimenez, 2024).
Motor vehicle accidents can cause a cascade of physical challenges, from indirect trauma and pain to mobility, flexibility, and posture issues. Physical therapy, with its focus on manual therapy, pain relief, and targeted exercises, is a vital tool for recovery. In El Paso, Dr. Alexander Jimenez’s expertise in chiropractic care, functional medicine, and diagnostic assessments ensures that MVA victims receive comprehensive, personalized treatment. By addressing both the medical and legal aspects of personal injury cases, Dr. Jimenez helps patients recover their health and regain their quality of life. If you’ve been in a car accident, consult a physical therapist or specialist like Dr. Jimenez to start your journey to recovery.
Explore the impact of cervical spine injuries associated with auto injuries and understand how to recognize and address them effectively.
Introduction: The Impact of MVAs on Your Neck
Picture this: you are cruising down the road, maybe humming along to your favorite tune, when—BAM!—a car rear-ends you, and suddenly your neck feels like it is auditioning for a role in a horror movie. Motor vehicle accidents (MVAs) are a leading cause of cervical spinal pain, affecting thousands of people each year. According to a study, approximately 869,000 traffic crash-related cervical spine injuries are seen in U.S. hospitals annually (Estimating Cervical Spine Injuries). These auto injuries can range from minor sprains to severe fractures, turning your daily routine into a painful plot twist.
In this guide, we will explore the clinical reasons behind cervical spinal pain resulting from motor vehicle accidents (MVAs), delve into the expertise of Dr. Alexander Jimenez, a distinguished chiropractor in El Paso, and highlight why personal injury cases are significant in this Texas city. With a touch of humor to keep things light, because who does not need a chuckle when dealing with neck pain?—We will cover everything from injury mechanisms to advanced treatments. So, let us straighten out the kinks in your knowledge, much like a chiropractor aligns your spine!
Clinical Rationale for Cervical Spinal Pain from MVAs
When your car gets hit, your neck often takes the brunt of the impact, like a delicate stack of china plates teetering on the edge of a table. The seven vertebrae in the cervical spine (C1-C7) are particularly vulnerable due to their flexibility and role in supporting your head. A medical policy document outlines specific conditions and procedures for treating cervical spine injuries from trauma like MVAs (Blue Cross Blue Shield of North Carolina, n.d.). We will examine the main key factors that contribute to post-crash neck pain.
Spinal Cord Compression
Spinal cord compression is like your spine’s worst nightmare—a traffic jam where the spinal cord gets squeezed, potentially causing pain, numbness, or even paralysis. In MVAs, this can happen due to displaced bone fragments, herniated discs, or hematomas. Symptoms might include weakness, tingling, or loss of sensation. A review of traumatic cervical spinal cord injuries suggests that early surgical intervention can improve outcomes by relieving pressure and stabilizing the spine (Epstein & Hollingsworth, 2015).
Hyperextension Injury
Ever seen a movie where someone’s head snaps back dramatically? That is hyperextension in action, common in rear-end collisions. This injury stretches or tears the anterior longitudinal ligament, potentially damaging discs or causing fractures. You might feel stiffness or pain that makes turning your head feel like solving a Rubik’s Cube. Treatment ranges from physical therapy to surgery for severe cases, depending on how extensive the damage is to the cervical spine.
Facet Subluxation and Dislocation
The facet joints are like the hinges on the door of your spine, allowing smooth movement. In MVAs, especially those with twisting forces, these joints can slip out of place (subluxation) or fully dislocate, resulting in pain and potential nerve damage. Treatment may involve manually realigning the joints or surgical stabilization if the damage is severe.
Other Severe Injuries
MVAs can also cause facet fractures, epidural hematomas, or foreign bodies lodging in the spine. These conditions often require urgent procedures like cervical discectomy, laminotomy, or fusion to prevent long-term complications. The policy document emphasizes that methods such as anterior or posterior cervical fusion are indicated when imaging reveals cord or root compression corresponding to symptoms (Blue Cross Blue Shield of North Carolina, n.d.).
Epstein, N. E., & Hollingsworth, R. (2015). Diagnosis and management of traumatic cervical central spinal cord injury: A review. Surgical Neurology International, 6(Suppl 4), S140-S153. https://doi.org/10.4103/2152-7806.156552
Personal Injury Rehabilitation- Video
Biomechanics of Cervical Spine Injuries
To understand why your neck feels like it has been through a blender after a motor vehicle accident (MVA), we need to discuss biomechanics—think of it as the physics of your spine’s movement. The cervical spine’s flexibility makes it prone to injury when sudden forces are applied, and different types of crashes produce unique injury patterns.
Rear-End Collisions
Rear-end collisions are the classic culprits behind whiplash, where your head snaps back and forth like a bobblehead on a bumpy road. This rapid motion strains muscles, ligaments, and discs, leading to whiplash-associated disorders (WAD). A study notes that soft tissue injuries, like sprains, are common in these crashes (Soft Tissue Cervical Injuries).
Frontal and Side-Impact Collisions
Frontal crashes can cause flexion injuries, where the head jerks forward, potentially compressing discs or fracturing vertebrae. Side-impact collisions add a twist—literally—causing lateral or rotational injuries. Research shows that compression-flexion is a common mechanism for severe injuries like quadriplegia in survivors (Cervical Spine Injuries IEEE).
Factors Influencing Injury
Injury severity depends on factors such as crash speed, seatbelt use, and the position of your body. For example, tensing up before impact can increase the risk of muscle strain (Common Neck Injuries). A clinical commentary highlights that occupant characteristics, like age or pre-existing conditions, also play a role (McMurry et al., 2016).
McMurry, T. L., et al. (2016). Mechanisms and mitigation of head and spinal injuries due to motor vehicle crashes. Journal of Orthopaedic & Sports Physical Therapy, 46(10), 845-856. https://doi.org/10.2519/jospt.2016.6716
Dr. Alexander Jimenez, DC, APRN, FNP-BC, is El Paso’s leading expert in pain management, with over 30 years of experience in addressing the complexities of motor vehicle accident (MVA)- related injuries. His clinic, El Paso Back Clinic (El Paso Back Clinic), is a hub for chiropractic care, functional medicine, and holistic recovery. Let us take a look at his approach, which is like a well-choreographed dance to get your spine back in rhythm.
The Chronic Pain Challenge
Dr. Jimenez cites a University of Alberta study that tracked 268 people with grade 1 or 2 neck injuries from MVAs. At three months, 38% reported pain, dropping to 22% at six months and 18% at one year (Auto Injuries and Neck Pain). This shows that while many recover, some face lingering pain without prompt care. A 2009 British study he references adds that up to 5% may be permanently disabled, with over 5% experiencing pain for a decade or more.
Chiropractic Care as a Game-Changer
Dr. Jimenez emphasizes chiropractic adjustments to realign the spine, much like straightening a crooked picture frame. These adjustments, combined with manual manipulations, reduce pain and restore mobility. His clinic also offers physical therapy, nutritional counseling, and wellness programs to support overall healing (Benefits of Chiropractic).
Early Intervention Matters
The sooner you see a chiropractor like Dr. Jimenez, the better your chances of avoiding chronic pain. His team employs a multidisciplinary approach, incorporating nurse practitioners and nutritionists, to develop personalized treatment plans that address both symptoms and underlying causes.
El Paso’s streets witness their fair share of motor vehicle accidents, resulting in a high number of personal injury cases. These cases often involve victims seeking compensation for various cases like medical bills, lost wages, and pain and suffering. Law firms, such as Chavez Law Firm, note that accidents caused by negligence can turn lives upside down, making legal and medical support critical (El Paso Personal Injury).
Dr. Jimenez’s team in Legal Support
Dr. Jimenez stands out in El Paso by combining medical care with legal needs. His detailed medical evaluations, backed by advanced imaging, provide clear evidence linking injuries to MVAs. This documentation is crucial for personal injury claims, as it enables attorneys to establish the extent of damages. His LinkedIn profile highlights his commitment to patient education and community outreach, making him a trusted ally for accident victims (Dr. Jimenez’s profile).
Why Medical Documentation Matters
In personal injury cases, precise medical records can significantly impact the outcome of a claim. Dr. Jimenez’s ability to correlate symptoms with imaging findings ensures that victims have the evidence needed to secure fair compensation while also focusing on their recovery.
Diagnosing neck injuries is like solving a puzzle—each piece (or scan) reveals part of the picture. Dr. Jimenez uses cutting-edge tools like MRI, CT scans, and X-rays to pinpoint the exact nature of cervical spine injuries. His clinic may collaborate with facilities like Diagnostic Outpatient Imaging in El Paso, which offers state-of-the-art radiology services (Diagnostic Outpatient Imaging).
MRI and CT Scans
MRI is excellent for detecting soft tissue damage, such as ligament tears or disc herniations, while CT scans excel at showing bone fractures. These tools enable Dr. Jimenez to create precise treatment plans, ensuring that no injury goes unnoticed.
Dual-Scope Procedures
Dr. Jimenez’s expertise extends to coordinating dual-scope procedures, where multiple diagnostic methods are used to confirm findings. This thorough approach strengthens both medical treatment and legal documentation, giving patients a solid foundation for recovery and claims.
Dr. Jimenez’s treatment plans are like a tailored suit—customized to fit each patient’s needs. His clinic offers a range of therapies to address MVA-related neck pain, with a focus on non-invasive methods whenever possible.
Chiropractic Adjustments
Chiropractic care is the cornerstone of his approach, using spinal adjustments to correct misalignments and reduce pain. It is like hitting the reset button on your spine, helping it function smoothly again (Musculoskeletal Ligaments Treatment).
Physical Therapy and Rehabilitation
Physical therapy strengthens neck muscles and improves range of motion, preventing future issues. Dr. Jimenez’s team designs rehabilitation programs to help patients bounce back like a well-tuned spring.
Functional Medicine
By incorporating nutrition and lifestyle changes, Dr. Jimenez addresses the underlying factors that may be correlated to prolonged pain. This holistic approach ensures long-term wellness, not just a quick fix (Ligamentous Injuries Recovery).
When Surgery Is Needed
For severe cases, Dr. Jimenez may refer patients to specialists for surgical options, such as cervical fusion, ensuring a seamless care continuum.
Table 2: Treatment Options for MVA-Related Neck Pain
While you cannot always avoid accidents, you can take steps to protect your neck and spine. It is always important to wear a seatbelt and adjust your headrest to support the natural curve of your neck. After a motor vehicle accident (MVA), watch for symptoms such as pain, stiffness, or numbness and seek medical care immediately. Dr. Jimenez’s blog offers tips on recognizing delayed symptoms, which can sneak up like an uninvited guest (Delayed Symptoms Auto Accident).
Cervical spinal pain from motor vehicle accidents is a serious issue that demands prompt attention. From understanding the biomechanics of injuries to seeking expert care from professionals like Dr. Alexander Jimenez, taking action early can prevent chronic pain and support El Paso’s personal injury law. If you have been in an accident, do not wait—your neck deserves better than a starring role in a pain-filled sequel.
Disclaimer This guide is provided for academic purposes only and should not be considered for professional medical advice as a substitute. Please consult with qualified healthcare providers for diagnosis and treatment of any medical condition.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine