What are some leg-strengthening exercises that will expedite recovery for athletes and physically active individuals who have undergone leg surgery?
Post Surgery Leg Strengthening
Leg muscles may weaken after hip, knee, ankle, or foot surgery. This happens because those muscles are not used as much during recovery. Gaining back strength and muscle endurance after an injury or surgery is an important step in recovery. Leg exercises can help regain mobility and prevent complications like blood clots and pressure sores after surgery or an injury, which is why engaging in post-surgery leg strengthening is important once the doctor gives the ok.
Benefits
Post-surgery leg strengthening exercises have several benefits, including
Rebuilds strength and confidence
Retraining for optimal mobility and flexibility
Prevents pressure sores
Prevents blood clots
When the leg muscles are contracted, they move blood like a pump, maintaining proper circulation. Moving in a bed after surgery also helps prevent pressure sores from forming and blood clots. A physical therapy team will determine the right leg exercises for each individual and their injury/condition. This is an important step when moving forward after surgery. (Hoogeboom T. J. et al., 2014)
This isometric exercise means the muscles contract while no motion occurs at the hip joints. To perform:
Lie on your back and tighten your buttock muscles.
Hold the muscles tight for 5 seconds, then relax.
Repeat 10 or 15 times.
Gluteal sets can be done several times per day.
Heel Slide
Heel slides can help regain strength in the major muscles of the leg. To perform:
Lie on your back.
Bend the knee of the surgical leg and slowly slide the heel toward your butt.
Slide as far as possible and hold for 5 seconds.
Slowly return to the starting position and repeat.
Short Arc Quad
The short arc quad, or SAQ, is a simple way to get the quadricep muscles working. To perform:
Lie on your back with a towel roll, small ball, or something similar under the knee.
Slowly straighten the knee.
Tighten the quad muscle on the top of the thigh.
Hold for 3 seconds, then relax.
Repeat 10 to 15 times.
Quad Set
This exercise helps get the quad muscles working. It also helps control the position of the kneecap. To perform:
Lie on your back.
Place a small towel roll under the knee.
Try to press the back of the knee flat against the floor.
Hold for 10 seconds and release.
Repeat 10 to 15 times.
Individuals can complete quad sets bilaterally or with both knees simultaneously. This makes the stronger leg help strengthen the weaker side.
Straight Leg Raise
To perform:
Lie on your back.
Lift your leg straight off the floor until it is at the height of the opposite bent knee.
Hold for 10 seconds and slowly lower.
Repeat 10 to 15 times.
Be sure to keep the knee straight for the entire exercise. Keep the opposite knee bent for comfort. To ensure the knee is straight, individuals can complete a quad set first and then the straight leg raise. The exercise can be more challenging by increasing repetitions or adding a 2- to 3-pound ankle weight on the thigh. For even more challenge, add the ankle weight to the ankle.
Hamstring Strengthening
Working out the hamstrings after injury or surgery is important. The hamstring muscles bend the knee and extend the hip backward. To perform:
Lie on your stomach.
Bend one knee to raise the lower limb straight in the air.
Hold for 5 seconds and lower slowly.
Repeat 10 to 15 times.
Once the exercise is easy to do, increase the repetitions to 30. Individuals can also try adding a 2- to 3-pound ankle weight.
Physical therapy can help individuals regain mobility after injury or surgery. A therapist may prescribe exercises as part of an at-home exercise program. Over time, progress will go from simple exercises to more challenging ones to improve balance and mobility. (Madara K. C. et al., 2019)
Injury Medical Chiropractic & Functional Medicine Clinic
Before starting this or any other exercise program, consult a doctor and a physical therapist to find the right exercises for your situation. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution. We focus on what works for you to relieve pain, restore function, and prevent injury. Regarding musculoskeletal pain, specialists like chiropractors, acupuncturists, and massage therapists can help mitigate the pain through spinal adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal issues.
Are You Recovering From Ankle Sprains?
References
Hoogeboom, T. J., Dronkers, J. J., Hulzebos, E. H., & van Meeteren, N. L. (2014). Merits of exercise therapy before and after major surgery. Current opinion in anaesthesiology, 27(2), 161–166. https://doi.org/10.1097/ACO.0000000000000062
Madara, K. C., Marmon, A., Aljehani, M., Hunter-Giordano, A., Zeni, J., Jr., & Raisis, L. (2019). PROGRESSIVE REHABILITATION AFTER TOTAL HIP ARTHROPLASTY: A PILOT AND FEASIBILITY STUDY. International Journal of Sports Physical Therapy, 14(4), 564–581.
Excessive alcohol consumption: what is alcoholic peripheral neuropathy?
Alcoholic Peripheral Neuropathy
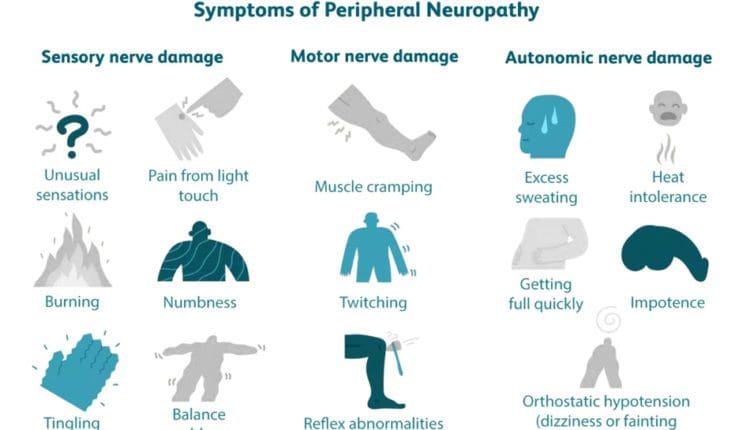
Alcoholic peripheral neuropathy (ALN) is a condition that damages the nerves in the body due to chronic alcohol consumption. It can cause sensory, motor, and autonomic dysfunction, which can lead to disability. This damage prevents the nerves from communicating information. Most symptoms generally start as mild but typically worsen over time as the neuropathy progresses. The most common symptoms are: (National Library of Medicine, 2023)
Numbness or tingling sensation in the extremities
Pain or a burning sensation in the extremities
Difficulty walking
Difficulty urinating
Difficulty talking or swallowing
Affected nerves include the peripheral and autonomic nerves, which help regulate internal body functions. Around 46% of chronic alcohol users will eventually develop the condition. (Julian T., Glascow N., Syeed R., & Zis P. 2019)
Causes
The exact cause of alcoholic neuropathy is unclear. But it is directly related to heavy and long-term alcohol consumption. (Julian T., Glascow N., Syeed R., & Zis P. 2019) It is believed overconsumption of alcohol can directly harm and hinder the nerves’ ability to communicate information. Unhealthy nutritional habits are often associated with it as well. Research shows that decreased thiamine/B vitamin plays a role, while others suggest an overall dietary deficiency may play a role. (Julian T., Glascow N., Syeed R., & Zis P. 2019) However, alcoholic neuropathy can also occur without the presence of malnutrition. (Julian T., Glascow N., Syeed R., & Zis P. 2019)
Neuropathy Development and Progression
Alcoholic peripheral neuropathy develops depending on many factors, including the amount of daily/nightly alcohol consumed, age and overall health, nutritional intake, and other individual factors. In most cases, the neuropathy takes several years or decades to develop, depending on the amount of alcohol consumed.
Pain or burning sensation in the arms, legs, or feet.
Symptoms that occur in the arms and legs typically affect both sides.
Cramps, aches, or weakness of the muscles.
Constipation or diarrhea.
Nausea and vomiting.
Difficulty urinating or incontinence.
Difficulty walking.
Difficulty talking or swallowing.
Heat intolerance.
Erection difficulties.
Most symptoms begin as mild and usually worsen over time as the neuropathy progresses. Alcoholic neuropathy affects individuals who consume excessive amounts of alcohol over a long time. (Julian T., Glascow N., Syeed R., & Zis P. 2019)
Healthcare providers will collect data involving past medical history and all current symptoms.
Physical Exam
This exam looks at other medical conditions contributing to symptoms, like diabetes or high blood pressure.
Neurological Exam
This is a noninvasive exam to determine the location and extent of neurological damage.
Healthcare providers may ask patients several questions and have them complete a series of small movements to check neurological function.
Blood and Urine Tests
These tests can detect diabetes, liver and kidney problems, infections, vitamin deficiencies, and other conditions that can cause neuropathic conditions.
Chronic alcohol use can also affect how the body stores and uses vitamins necessary for healthy nerve function. Vitamin levels that a healthcare provider may check include: (National Library of Medicine, 2023)
Vitamin A
Biotin
Folic acid
Niacin, or vitamin B3
Pyridoxine, or vitamin B6
Pantothenic acid
Liver Disease
Individuals with chronic liver disease often have neuropathy. The severity and stage are associated with a higher incidence of neuropathy. (Pasha MB, Ather MM, Tanveer MA, et al. 2019)
Treatment
Alcoholic neuropathy is not reversible, even when quitting drinking. However, individuals with the condition can make healthy changes to minimize symptoms and receive help for chronic alcohol use. The first step is stopping alcohol consumption. (Chopra K., & Tiwari V. 2012) Talk to a healthcare provider about what options are available. Treatment can include:
In-patient or outpatient rehab
Therapy
Medication
Social support from groups like Alcoholics Anonymous
A combination of treatments will likely be utilized. Other treatment options involve symptom management and preventing further injuries and may include:
Physical therapy
Keeping the head elevated while sleeping.
Orthopedic splints to maintain limb function and positioning.
Wearing compression stockings.
Adding vitamins and supplements.
Eating extra salt for those without hypertension
Medications to reduce pain and discomfort.
Intermittent catheterization or manual expression of urine for those with difficulty urinating.
Individuals with neuropathy may have reduced sensitivity in the arms and legs. If this occurs, additional steps need to be taken to prevent other injuries, that include (National Library of Medicine, 2023)
Wear special footwear to prevent foot injuries.
Checking feet daily for wounds.
Prevent burns by ensuring that bath and shower water is not too hot.
Injury Medical Chiropractic and Functional Medicine Clinic
Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to build optimal health and wellness solutions. We focus on what works for you to relieve pain, restore function, prevent injury, and help mitigate issues through adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal problems.
Peripheral Neuropathy Myths and Facts
References
National Library of Medicine. (2023). Alcoholic neuropathy. Retrieved from https://medlineplus.gov/ency/article/000714.htm
Julian, T., Glascow, N., Syeed, R., & Zis, P. (2019). Alcohol-related peripheral neuropathy: a systematic review and meta-analysis. Journal of Neurology, 266(12), 2907–2919. https://doi.org/10.1007/s00415-018-9123-1
National Institute of Neurological Disorders and Stroke. (2024). Peripheral neuropathy. Retrieved from https://www.ninds.nih.gov/health-information/disorders/peripheral-neuropathy
Pasha MB, A. M., Tanveer MA, et al. (2019). Frequency of peripheral neuropathy in chronic liver disease. Med Forum Monthly, 30(8), 23-26. https://medicalforummonthly.com/index.php/mfm/article/view/3761
Chopra, K., & Tiwari, V. (2012). Alcoholic neuropathy: possible mechanisms and future treatment possibilities. British journal of clinical pharmacology, 73(3), 348–362. https://doi.org/10.1111/j.1365-2125.2011.04111.x
Can a rowing machine provide a full-body workout for individuals looking to improve fitness?
A group of people exercise in the gym using a rowing machine together. A side view of a sportswoman exercising on a rowing machine in a CrossFit center. A muscular girl and a sporty man are working out on a training simulator at a CrossFit gym.
Rowing Machine
Today, rowing machines are widely recognized as effective fitness tools. They can be found in gyms, fitness centers, physical therapy, and sports rehabilitation clinics. Rowing is low-impact, allowing control of movement and pace, and is recommended for active recovery. It’s sometimes recommended as an exercise for individuals with early stages of osteoarthritis.
Benefits
The benefits include:
Rowing is a total-body workout that strengthens major muscle groups in the arms, legs, and core and increases cardiovascular endurance.
The upper and lower body are used on every stroke.
Strengthens and tones the muscles.
Rowing burns significant calories without placing added stress on the joints.
Improves endurance and heart and lung health.
Cardiovascular Fitness
Rowing is a rare exercise that involves power and endurance. It is an aerobic exercise that increases the body’s heart rate and oxygen, improving cardiovascular fitness. (Hansen RK, et al. 2023) Through continuous, rhythmic movement, which increases oxygen utilization, rowing enhances the heart and lungs’ ability to supply oxygen to the body and works on muscular endurance.
Full-Body Workout
A rowing workout is a comprehensive full-body workout that simultaneously works multiple body areas and muscle groups, specifically the arms, back, core, and legs. The motion moves major muscle groups through the full range of motion, promoting flexibility and muscle tone improvements that are great for individuals with trouble with weight-bearing exercises like running. Rowing can also improve physiological markers, depending on the intensity of the workout and the heart rate zone maintained.
Joint-Friendly
Rowing is a low-impact exercise, making it easier on joints and suitable for individuals with joint concerns or those looking for a joint-friendly workout. The workout engages the largest muscles in a low-impact way with no pounding on the joints or excessive rotation.
Burns Calories
Rowing can be an efficient way to burn calories. Its cardiovascular and resistance training combination makes it an effective tool for weight management and weight loss. Alternating between higher and lower intensities can enhance calorie burning during and after the exercise session from excess post-exercise oxygen consumption (EPOC),also known as the afterburn effect. (Sindorf, M. A. G. et al., 2021)
Improves Posture
Maintaining a healthy posture offers numerous benefits, such as improving breathing ability, aiding in digestion, and preventing injuries. (Kim D, 2015) Rowing can be an effective workout that enhances postural strength and awareness and reduces back pain risks. Proper spine activation is necessary for efficient rowing, which also helps to pull the shoulders back. The hip flexors help to lengthen during the drive phase while the shoulders open. Proper rowing technique involves:
Dorsiflexion of the foot.
Stretching of the Achilles tendon.
Engaging the tibialis.
Getting Started
Rowing is not too difficult to get started. Following techniques shared by experts will help improve the experience and reduce the risk of injury.
Maintaining Upright Posture
The back should be straight throughout the movement.
Brace the core muscles to keep the back from rounding while bending at the knees and hips during the movement.
This keeps the body aligned, prevents injuries, and makes the exercise more effective.
Maintain Stroke Sequences
There are four parts to the sequence:
The catch – is when you sit at the front of the machine with your knees bent and arms reaching out to hold the handle.
The drive – is the next step, which involves pushing into the platform with your heels and driving through your legs while engaging your legs, glutes, and core. During the drive, you want to lean back slightly as you push with your legs while pulling the handle to the bottom of the rib cage.
The finish – lean back a little more while pulling the handle to the lower chest level.
The recovery – extend your arms forward while bending the hips to bring the torso forward, using your legs to pull back to the starting position.
Adjust Resistance Accordingly
Most rowing machines have adjustable resistance settings. Beginners should start with a lower resistance level to focus on proper technique and gradually increase as they become more comfortable so that the resistance provides a challenge without compromising form. On a rowing machine, the individual should feel like they are gliding efficiently over water with strong, powerful strokes repeated for however many reps depending on the workout.
Breathing
Aerobic workouts require proper breathing. It is recommended to inhale during the recovery phase as you slide the seat forward and exhale during the drive phase when pushing through the legs. Breathing in sync with the rowing motion keeps the oxygen flow going, so the body maintains energy and smooth strokes.
Injury Medical Chiropractic and Functional Medicine Clinic
As with any fitness program, individuals should consult a healthcare professional or fitness expert, especially if pre-existing health conditions or concerns exist. At Injury Medical Chiropractic and Functional Medicine Clinic, we focus on what works for you and strive to better the body through researched methods and total wellness programs. We focus on treating patients’ injuries and chronic pain syndromes to create personalized care plans that improve ability through flexibility, mobility, and agility programs personalized to the individual. Using an integrated approach, our goal is to relieve pain naturally by restoring health and function to the body through Functional Medicine, Acupuncture, Electro-Acupuncture, and Sports Medicine protocols. If other treatment is needed, Dr. Jimenez has teamed up with the top surgeons, clinical specialists, medical researchers, and premier rehabilitation providers to provide the most effective treatments available.
Core Exercises and Back Pain
References
Hansen, R. K., Samani, A., Laessoe, U., Handberg, A., Mellergaard, M., Figlewski, K., Thijssen, D. H. J., Gliemann, L., & Larsen, R. G. (2023). Rowing exercise increases cardiorespiratory fitness and brachial artery diameter but not traditional cardiometabolic risk factors in spinal cord-injured humans. European journal of applied physiology, 123(6), 1241–1255. https://doi.org/10.1007/s00421-023-05146-y
Sindorf, M. A. G., Germano, M. D., Dias, W. G., Batista, D. R., Braz, T. V., Moreno, M. A., & Lopes, C. R. (2021). Excess Post-Exercise Oxygen Consumption and Substrate Oxidation Following High-Intensity Interval Training: Effects of Recovery Manipulation. International journal of exercise science, 14(2), 1151–1165.
Kim, D., Cho, M., Park, Y., & Yang, Y. (2015). Effect of an exercise program for posture correction on musculoskeletal pain. Journal of physical therapy science, 27(6), 1791–1794. https://doi.org/10.1589/jpts.27.1791
For individuals with back pain, can sleeping with a pillow between or under their knees help bring relief during sleep?
Sleep With A Pillow Between The Legs
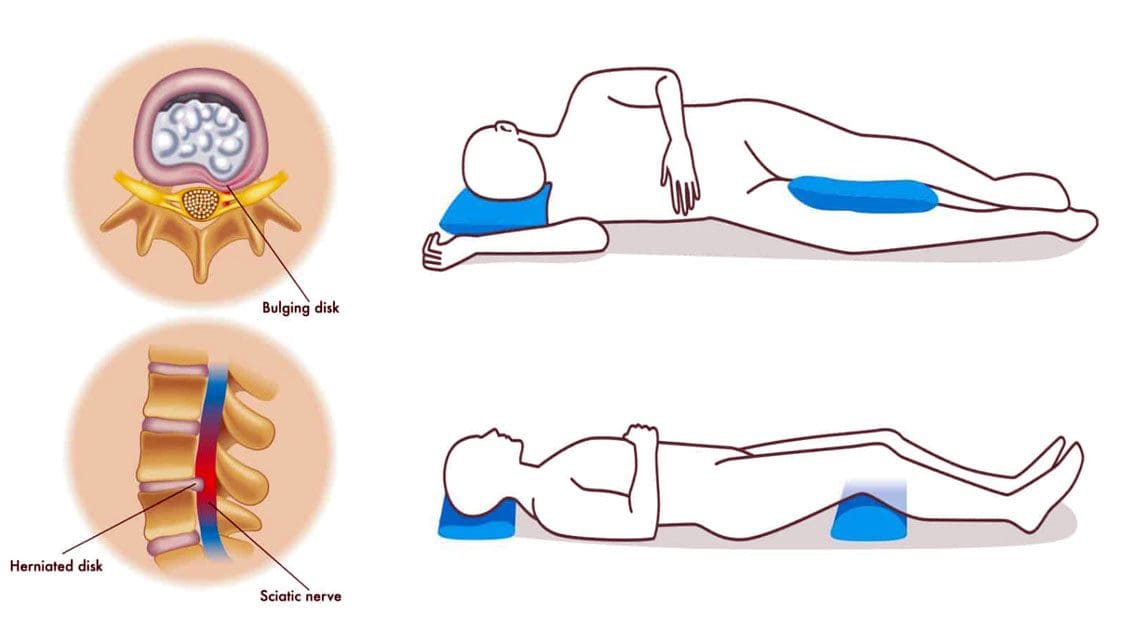
Healthcare providers may recommend that individuals with back pain due to pregnancy or conditions like a herniated disc and sciatica sleep with a pillow between their legs. Sleeping with a pillow between the legs may help relieve back and hip pain, as the position helps maintain pelvis and spinal alignment. Proper spinal alignment can help relieve back stress and pain.
The Benefits
Some potential benefits of sleeping with a pillow between the knees.
Reduce Back and Hip Pain
When sleeping on the side, the spine, shoulders, and hips may twist to maintain the position because the center of gravity is elevated, causing instability. (Gustavo Desouzart et al., 2015) Placing a pillow between the knees may help maintain stability and reduce back and hip pain. (Gustavo Desouzart et al., 2015) The pillow neutralizes the position of the pelvis by slightly elevating the leg on top. This decreases the pressure on the lower back and hip joints, which may help reduce pain and allow for improved sleep.
Reduce Sciatica Symptoms
Sciatica nerve pain travels from the lower back down one leg due to a compressed spinal nerve root in the lower back. (American Academy of Orthopaedic Surgeons, 2021) Sleeping with a pillow between the knees may help reduce symptoms and sensations. A pillow between the legs can help prevent twisting the back, rotating the spine, or tilting the pelvis during sleep.
Reduce Herniated Disc Symptoms
A herniated disc can pressure the spinal nerves, leading to pain and numbness. (Penn Medicine. 2024) Sleeping on the side can worsen herniated disc pain; however, placing a pillow between the knees keeps the pelvis in neutral alignment and prevents spinal rotation. Sleeping on the back with a pillow under the knees can also help reduce pressure on the disc. (University of Central Florida. N.D.)
Improve Posture
Maintaining healthy posture while sitting or standing is important to neuromusculoskeletal health and injury prevention. Proper alignment during sleep can help improve posture (Doug Cary et al., 2021). According to one study, individuals spend more than half of their time sleeping in a side-lying posture. (Eivind Schjelderup Skarpsno et al., 2017) Sleeping on the side with the top leg frequently falls forward, bringing the pelvis into a forward tilt that places added pressure on the hips and spine connective tissues. This position disrupts the body’s natural alignment. (Doug Cary et al., 2021) Placing a pillow between the knees improves sleeping posture by lifting the top leg and prevents forward shifting. (University of Rochester Medical Center. 2024)
Increased weight leads to increased pressure on joints.
Significant change in the center of gravity.
Hormonal changes make connective tissues more lax.
Pregnant women with hip or back pain are often recommended to sleep with a pillow between their knees to relieve pain and discomfort. Doctors agree that lying on the left side is the best sleep position during the second and third trimesters. This position ensures optimal blood flow for the mother and baby and helps kidney function. (Standford Medicine, 2024) Placing a pillow between the knees can help reduce the pressure on the joints and also help maintain the left-side lying position. (O’Brien LM, Warland J. 2015) (Standford Medicine, 2024) Larger maternity pillows supporting the abdomen and lower back can provide more comfort.
Consult a healthcare provider about sleeping with a pillow between the knees to see if it is right for you.
What Causes Disc Herniation?
References
Desouzart, G., Matos, R., Melo, F., & Filgueiras, E. (2015). Effects of sleeping position on back pain in physically active seniors: A controlled pilot study. Work (Reading, Mass.), 53(2), 235–240. https://doi.org/10.3233/WOR-152243
American Academy of Orthopaedic Surgeons. (2021). Sciatica. OrthoInfo. https://orthoinfo.aaos.org/en/diseases–conditions/sciatica
Penn Medicine. (2024). Herniated disc disorders. Penn Medicine. https://www.pennmedicine.org/for-patients-and-visitors/patient-information/conditions-treated-a-to-z/herniated-disc-disorders
University of Central Florida. (N.D.). The best sleeping position for lower back pain (and the worst). UFC Health Services. https://ucfhealth.com/our-services/lifestyle-medicine/best-sleeping-position-for-lower-back-pain/
Cary, D., Jacques, A., & Briffa, K. (2021). Examining relationships between sleep posture, waking spinal symptoms and quality of sleep: A cross sectional study. PloS one, 16(11), e0260582. https://doi.org/10.1371/journal.pone.0260582
Skarpsno, E. S., Mork, P. J., Nilsen, T. I. L., & Holtermann, A. (2017). Sleep positions and nocturnal body movements based on free-living accelerometer recordings: association with demographics, lifestyle, and insomnia symptoms. Nature and science of sleep, 9, 267–275. https://doi.org/10.2147/NSS.S145777
University of Rochester Medical Center. (2024). Good sleeping posture helps your back. Health Encyclopedia. https://www.urmc.rochester.edu/encyclopedia/content.aspx?ContentTypeID=1&ContentID=4460
Casagrande, D., Gugala, Z., Clark, S. M., & Lindsey, R. W. (2015). Low Back Pain and Pelvic Girdle Pain in Pregnancy. The Journal of the American Academy of Orthopaedic Surgeons, 23(9), 539–549. https://doi.org/10.5435/JAAOS-D-14-00248
Standford Medicine. (2024). Sleeping positions during pregnancy. Standford Medicine Children’s Health. https://www.stanfordchildrens.org/en/topic/default?id=sleeping-positions-during-pregnancy-85-P01238
O’Brien, L.M., Warland, J. (2015). Maternal sleep position: what do we know where do we go? BMC Pregnancy Childbirth, 15, Article A4 (2015). https://doi.org/doi:10.1186/1471-2393-15-S1-A4
For individuals experiencing gluteus minimus pain and are unsure where to start to deal with it, can a physical therapist, chiropractor, or general practitioner help diagnose lower extremity pain and develop an appropriate treatment plan?
Gluteus Minimus Muscles
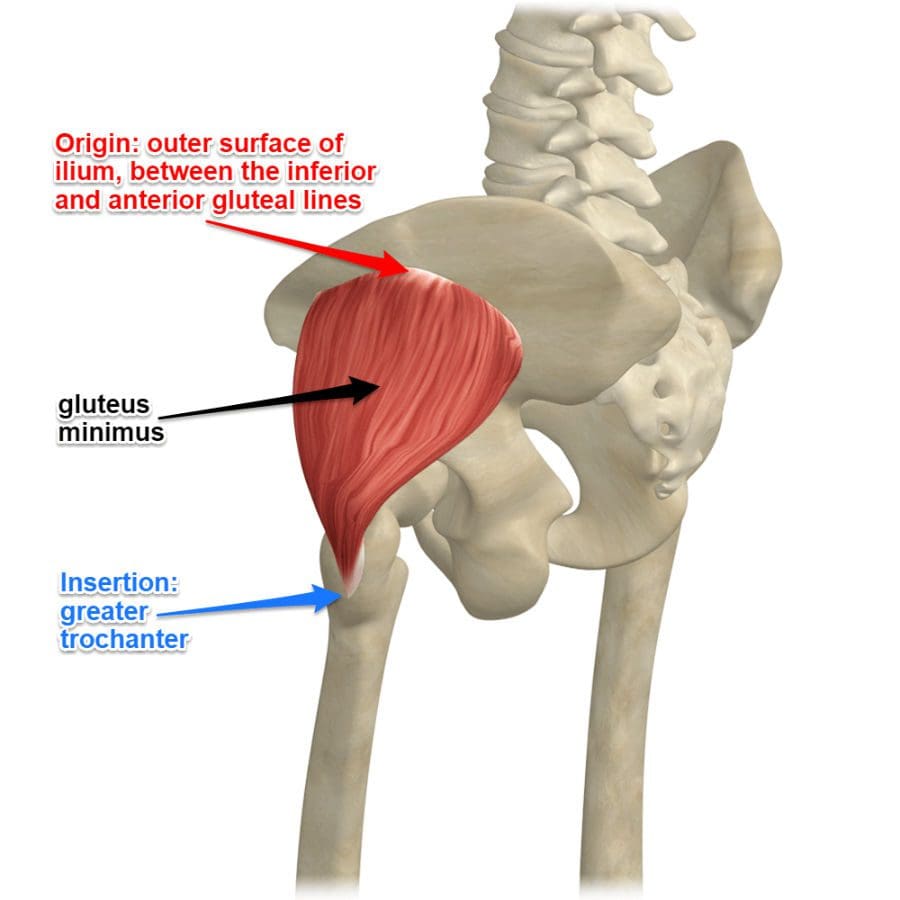
The gluteus minimus is the smallest muscle of the gluteal muscles. Combined with the gluteus maximus and gluteus medius, these muscles make up the glutes. The glutes help form the buttocks shape, stabilize the hips, rotate the legs, and raise the thighs. The gluteus minimus and medius specifically support the gluteus maximus’s ability to raise the leg to the side and rotate the thigh inwards. (ScienceDirect. 2011)
Anatomy
The gluteus minimus muscles are triangular and lie underneath the gluteus medius near the rotators of the hip joints. The muscles start in the lower ilium region, the upper and largest area of the hip bone that makes up the pelvis and attaches to the femur/thigh bone.
The fibers on the top part of the muscle are thick and compact, while the lower fibers are flat and spread out.
The superior gluteal nerves and blood vessels separate the gluteus minimus and the medius.
The gluteus medius muscles start on the upper ilium region, which covers the gluteus minimus muscle entirely. The location of the gluteus minimus muscles envelopes the sciatic notch or the area in the pelvis that houses the piriformis muscle, superior gluteal vein, and superior gluteal artery, which provide a certain amount of protection.
Function
Movement depends on the location of the femur. The gluteus minimus muscle’s function is to:
Flex
Rotate
Stabilize
When the thigh is extended, it helps abduct or swing the leg out away from the body.
When the hip bones are flexed, the gluteus minimus rotates the thigh inward with the help of the gluteus medius.
The movements are done with the support of the muscle fibers, which contract to move the thigh in both directions. (ScienceDirect. 2011)
The gluteus minimus and the medius also stabilize the hips and pelvis during movement and when resting.
Associated Conditions
One of the most common injuries is muscle wearing and tearing, which can cause pain over and around the greater trochanter. This is known as greater trochanteric pain syndrome or GTPS, a condition usually caused by a gluteus medius or minimus tendinopathy, which can include inflammation of the surrounding bursae. (Diane Reid. 2016) For a gluteus minimus tear, the pain/sensations will be felt outside the hip, especially when rolling or applying weight on the affected side. A tear can happen suddenly with no particular activity causing the tear to occur aside from normal use and stress on the muscle. Physical activities like walking may be painful.
Rehabilitation
Treatment depends on the severity of the condition. Usually, rest, ice, and over-the-counter medication can help reduce swelling and pain symptoms. For pain symptoms that are not subsiding, it’s recommended to see a healthcare provider who can run an MRI or X-ray to see the condition of the muscle and rule out other causes of pain. The healthcare provider will refer the patient to a physical therapy team that can evaluate the strength of the gluteus minimus and provide a list of exercises and stretches to help repair the muscle while conditioning the surrounding muscles. (SportsRec. 2017) Depending on the level of pain, sometimes the healthcare provider will prescribe a cortisone injection to the gluteus minimus muscle in conjunction with physical therapy. This will help alleviate the pain so that the physical therapy exercises can be done comfortably, allowing the gluteus maximus muscle to heal properly and strengthen. (Julie M. Labrosse et al., 2010)
Reid D. (2016). The management of greater trochanteric pain syndrome: A systematic literature review. Journal of orthopaedics, 13(1), 15–28. https://doi.org/10.1016/j.jor.2015.12.006
Labrosse, J. M., Cardinal, E., Leduc, B. E., Duranceau, J., Rémillard, J., Bureau, N. J., Belblidia, A., & Brassard, P. (2010). Effectiveness of ultrasound-guided corticosteroid injection for the treatment of gluteus medius tendinopathy. AJR. American journal of roentgenology, 194(1), 202–206. https://doi.org/10.2214/AJR.08.1215
A nerve becomes pinched/compressed when added pressure is placed on it by surrounding structures that can include muscles, bones, ligaments, tendons, or a combination. This injures and damages the nerve causing function problems and symptoms and sensations in that area or other parts of the body that are supplied by that nerve. Medical practitioners refer to this as nerve compression or entrapment. Although compressed nerves are more commonly associated with the neck, arms, hands, elbows, and lower back, any nerve in the body can experience irritation, spasms, inflammation, and compression. The causes and treatment of a compressed nerve in the knee.
Compressed Nerve In The Knee
There’s only one nerve that goes through the knee that has an increased risk of getting compressed. It’s a branch of the sciatic nerve called the peroneal nerve. The nerve goes around the outside of the knee before traveling down the outside of the lower leg. At the bottom of the knee, it lies between the bone and skin, making it vulnerable to irritation or compression by anything that can put pressure on the outside of the knee.
Causes
Traumatic injuries over time can lead to pressure on the nerve from inside the knee. Common causes of a compressed nerve in the knee include:
Frequently Crossing Legs
Compression by the opposite knee, while the legs are crossed is the most common cause.
Knee Brace
A too-tight or strong brace can compress the leg and nerve.
Thigh-High Compression Stockings
Designed to maintain pressure on the legs, if too tight these stockings can compress the nerve.
Squatting Posture For Long Periods
This position places pressure on the side of the knee.
Fractures
A fracture of the large lower leg bone/tibia or sometimes the small bone/fibula near the knee can entrap the nerve.
Lower Leg Cast
The portion of the cast around the knee can be tight and compress the nerve.
Tell the doctor if a cast or brace feels tight or is causing numbness or pain in the leg.
Knee-High Boots
The top of a boot can land right below the knee and be too tight pinching the nerve.
Knee Ligament Injury
The nerve can become compressed due to bleeding or inflammation from an injured ligament.
Knee Surgery Complications
This is rare, but the nerve can inadvertently get pinched during knee replacement surgery or an arthroscopic procedure.
Prolonged Bed Rest
When lying down the legs tend to rotate outward and the knees flex.
In this position, the mattress can place pressure on the nerve.
Tumors or Cysts
Tumors or cysts can develop right on top or next to a nerve irritating and compressing the area.
Abdominal or Gynecologic Surgery
The equipment used to keep the legs rotated outward and the knees flexed for gynecologic and abdominal surgeries can compress the nerve.
Symptoms
The peroneal nerve supplies sensation and movement to the outside of the lower leg and the top of the foot. When compressed, it becomes inflamed, which causes the symptoms of a compressed nerve. Usually, only the lining/myelin sheath around the nerve is what gets injured. However, when the nerve gets damaged, the symptoms are similar but more severe. Common symptoms include:
Weakness that limits the ability to lift the foot toward the leg aka dorsiflexion.
This causes dragging the foot when walking.
The ability to turn the foot outward and extend the big toe is also affected.
Symptoms can be felt on the outside of the lower leg and on the top of the foot and include:
Tingling or pins and needles sensations.
Numbness.
Loss of sensation.
Pain.
Burning.
For individuals that have had a pinched nerve for two or more weeks, the muscles supplied by the nerve can begin to waste away or atrophy.
Symptoms can be intermittent or continuous depending on the cause.
The other common cause is a pinched nerve in the lumbar/lower spine.
When this is the cause, sensations, and pain will present in the lower back or the back and outside of the thigh.
Diagnosis
A doctor will look at medical history and perform an examination to make a diagnosis, determine the cause, and lay out a personalized treatment plan. The nerve in the knee can be felt as it travels around the top of the tibia, so a doctor may tap on it. If there is shooting pain down the leg, a pinched nerve may be present. Tests a doctor may order can include:
Knee X-ray
Shows any bone fractures or abnormal masses.
Knee MRI
Can confirm the diagnosis
Shows masses within the nerve.
Shows details of fractures or other problems in the bones.
Electromyogram – EMG
Tests electrical activity in the muscles.
Nerve Conduction Test
Tests the signal speed of the nerve.
Treatment
Treatment is aimed at reducing pain and improving mobility.
Over-the-Counter Pain Medication
OTC medication can reduce inflammation and improve symptoms short term.
Ice and Heat
Applying either heat or ice for 15 to 20 minutes at a time can provide relief from the symptoms.
An ice pack can make symptoms worse if it adds more pressure on the nerve.
Chiropractic and Physical Therapy
Chiropractic and physical therapy can release the compressed nerve, realign the structures, strengthen the muscles, and provide gait training.
Orthotic Boot
If walking gait is affected because the foot cannot bend, an orthotic boot can help.
This is a support that maintains the foot in a neutral position to walk normally.
Corticosteroid Injection
A corticosteroid injection can reduce inflammation and relieve pressure on the nerve.
Surgery
The nerve can suffer permanent damage if it has been pinched for a long time.
If that happens, surgery cannot repair the damage.
A doctor can perform surgery to correct a fracture, tumor, or other invasive problem causing a compressed nerve.
If conservative treatment doesn’t work, a peroneal nerve decompression procedure can be done to remove the pressure.
If surgery is needed, symptoms can disappear immediately, but it takes around four months to recover and rehabilitate.
Injury Rehabilitation
References
Krych, Aaron J et al. “Is peroneal nerve injury associated with worse function after knee dislocation?.” Clinical orthopedics and related research vol. 472,9 (2014): 2630-6. doi:10.1007/s11999-014-3542-9
Lezak B, Massel DH, Varacallo M. Peroneal Nerve Injury. [Updated 2022 Nov 14]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK549859/
Soltani Mohammadi, Sussan, et al. “Comparing the squatting position and traditional sitting position for ease of spinal needle placement: a randomized clinical trial.” Anesthesiology and pain medicine vol. 4,2 e13969. 5 Apr. 2014, doi:10.5812/aapm.13969
Stanitski, C L. “Rehabilitation following knee injury.” Clinics in sports medicine vol. 4,3 (1985): 495-511.
Xu, Lin, et al. Zhongguo gu Shang = China Journal of Orthopedics and Traumatology vol. 33,11 (2020): 1071-5. doi:10.12200/j.issn.1003-0034.2020.11.017
Yacub, Jennifer N et al. “Nerve injury in patients after hip and knee arthroplasties and knee arthroscopy.” American Journal of physical medicine & Rehabilitation vol. 88,8 (2009): 635-41; quiz 642-4, 691. doi:10.1097/PHM.0b013e3181ae0c9d
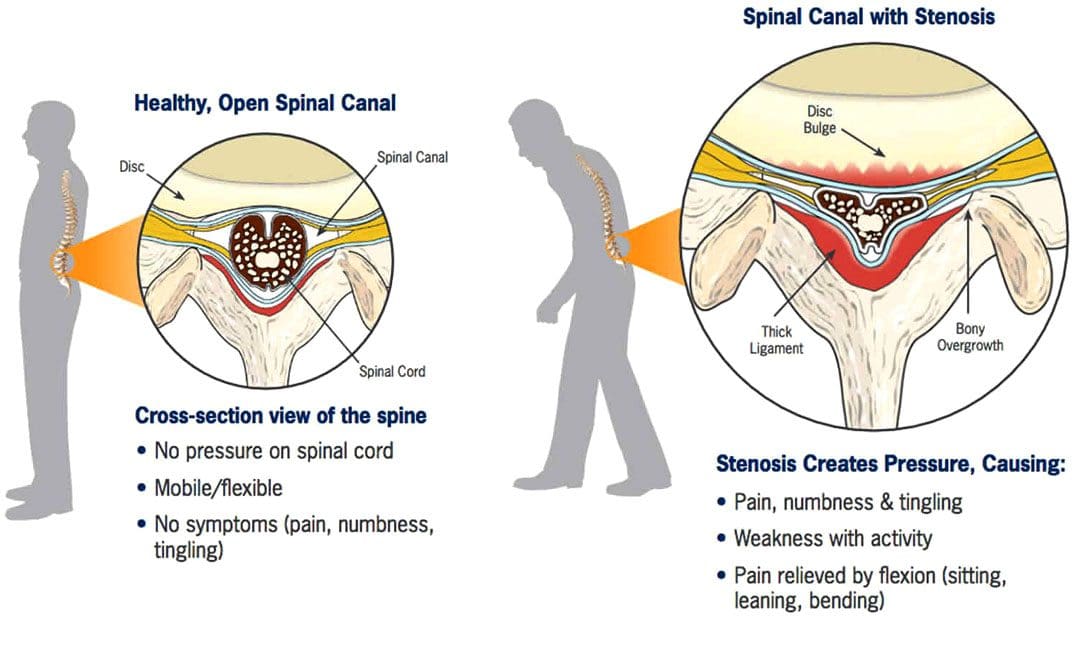
Spinal Stenosis Walking Issues:Stenosis means a narrowing. Spinal stenosis can happen in any spine region, but the neck and lower back are the most common locations. The spinal canal becomes narrower and can cause the nerves to become compressed, pinched, and irritated and can extend from the lumbar spine through the hips, buttocks, legs, and feet. Individuals with lumbar spinal stenosis may have difficulty walking caused by sensations of discomfort like numbness, electrical shocks, and pain, requiring the need to lean forward to relieve pressure and symptoms. Additionally, symptoms are likely to worsen the longer the walk. Chiropractic treatment can treat spinal stenosis because it corrects and re-aligns the spine, thus reducing pressure on the spinal cord, joints, and nerve roots.
Spinal Stenosis Walking Issues
The spine is made up of interlocking vertebrae. The regions are cervical, thoracic, lumbar, and sacral bones with a foramen opening. These openings form the protective tunnel/spinal canal surrounding the spinal cord. The spinal cord is a group of nerves that run through the tunnel. The narrowing suffocates the nerves supplying the lower extremities that can influence walking activity.
Symptoms
There may be no symptoms with early lumbar spinal stenosis. Most individuals develop symptoms gradually and may begin to notice them while walking or standing. These can include:
Lower back pressure sensations when standing upright or walking.
Leg numbness, tingling, weakness, burning, and/or cramping.
Muscle weakness.
Persistent pain in the back, hips, buttocks, or legs while walking.
Difficulty lifting the top part of the foot – known as drop foot.
Loss of sensation in the feet.
A weak foot that drops/slaps down when walking.
Loss of sexual ability.
In more serious cases, severe numbness, bladder problems, and inability to stand.
Individuals begin to lean forward when symptoms start, bringing relief by reducing the pressure on the nerves. However, constantly leaning forward leads to other posture and health problems.
Diagnosis
A doctor or chiropractor will ask questions about symptoms and medical history and perform a complete physical examination to diagnose lumbar spinal stenosis. During the physical examination, a healthcare provider will look for signs, such as loss of sensation, weakness, and abnormal reflexes.
Tests:
X-rays of the lumbar spine may show bone growths called spurs that push on spinal nerves and/or narrowing of the spinal canal.
Imaging tests – A CT or MRI scan can provide a detailed look at the spinal canal and nerve structures.
Other studies include – bone scans, myelogram, which is a CT scan that uses a color dye, and EMG, which is an electrical test of muscle activity.
Chiropractic Treatment
Chiropractic care combined with physical therapy is a tried-and-true treatment for spinal stenosis. A chiropractic treatment plan can include targeted and passive exercise programs. Targeted exercises involve strengthening the core and back muscles. Passive treatments include hot and cold therapy, massage, decompression, and electrical stimulation. The objective of chiropractic therapy is to:
Strengthen muscles in the core and legs
Correct posture and body mechanics.
Improve mobility.
Maintain ability to perform day-to-day activities.
Recommend stretches.
Educate on how to keep the spine and back muscles safe.
Train on using devices like a back brace, cane, or walker properly.
Advise about shoe inserts and splints.
Suggest work and home environment modifications, such as ergonomics and cushions.
Chiropractic Relief
References
Conway, Justin, et al. “Walking assessment in people with lumbar spinal stenosis: capacity, performance, and self-report measures.” The spine journal: official North American Spine Society journal vol. 11,9 (2011): 816-23. doi:10.1016/j.spinee.2010.10.019
Lurie, Jon, and Christy Tomkins-Lane. “Management of lumbar spinal stenosis.” BMJ (Clinical research ed.) vol. 352 h6234. 4 Jan. 2016, doi:10.1136/bmj.h6234
Macedo, Luciana Gazzi, et al. “Physical therapy interventions for degenerative lumbar spinal stenosis: a systematic review.” Physical therapy vol. 93,12 (2013): 1646-60. doi:10.2522/ptj.20120379
Tomkins-Lane, Christy C et al. “Predictors of walking performance and walking capacity in people with lumbar spinal stenosis, low back pain, and asymptomatic controls.” Archives of physical medicine and rehabilitation vol. 93,4 (2012): 647-53. doi:10.1016/j.apmr.2011.09.023
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine