Bone neoplasms and tumor-like conditions affecting the knee can be benign or malignant. Age at Dx is crucial for DDx
In patients <40: Benign bone neoplasms: Osteochondroma, Enchondroma are relatively frequent
Fibrous cortical defect (FCD) & Non-ossifying fibroma (NOF) are particularly frequent in children
Giant cell tumor (GCT) is the m/c benign neoplasm of the knee in patients between 20-40 years of age
Malignant bone neoplasms in <40: m/c Osteosarcoma and 2nd m/c Ewing sarcoma
In patients >40: malignant neoplasms: m/c are secondaries d/t bone metastasis. Primary bone malignancy:�the m/c
Multiple Myeloma (MM). Less frequently:�a 2nd�peak of Osteosarcoma (post-radiation or Paget�s), Fibrosarcoma or Malignant�Fibrous�Histiocytoma�(MFH) of bone.
Clinically: knee pain, pathological fracture
Some tumor-like conditions like FCD/Non-ossifying fibroma are asymptomatic and may regress spontaneously. Occasionally NOF may present with pathologic fracture. N.B. any knee/bone pain in a child/adolescents should be�treated with clinical suspicion and adequately investigated.
Imaging: 1st step: radiography
MRI with T1+C is crucial for lesion characterization/regional extent, staging and pre-operative planning. CT may�help with pathologic Fxs detection. If malignant bone neoplasms considered, CXR/CT, PET-CT to investigate�metastatic spread and staging are important
Imaging Approach Bone Neoplasms
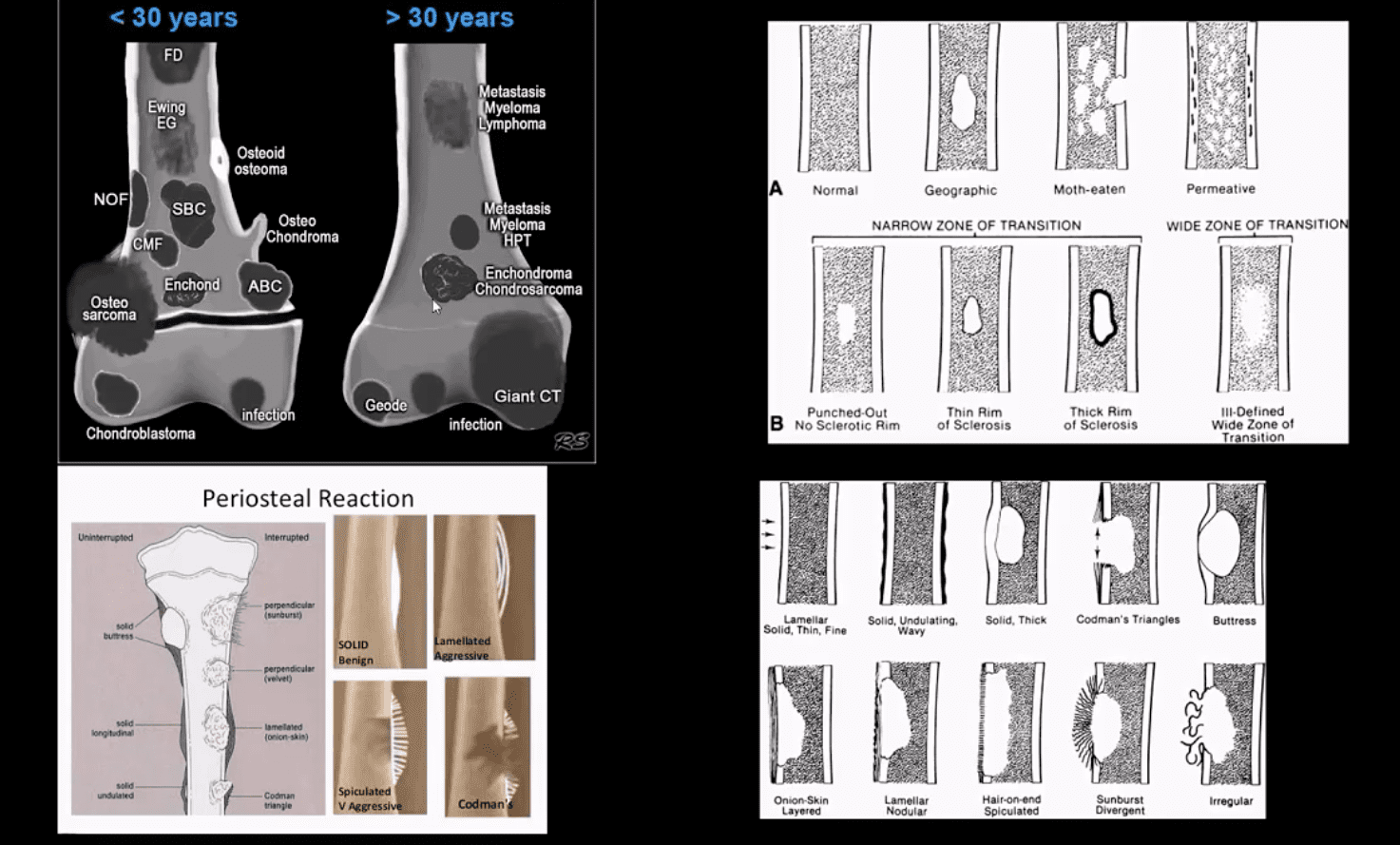
Approach to imaging Dx of bone neoplasms includes age, bone location (epiphysis vs. metaphysis vs. diaphysis), zone of transition surrounding the lesion, periosteal response, type of matrix, permeating or moth-eaten destruction vs. sclerotic, ground-glass, osteoid, cartilaginous matrix, soft tissue invasion, etc.
Key x-radiography features to DDx benign vs. malignant bone neoplasm:
Zone of transition: lesion is geographic with a narrow zone of transition vs. ill-defined wide zone of transition suggesting aggressive bone resorption
What type of bone destruction occurred: soap-bubbly appearance vs. osteolytic vs. osteosclerotic changes
Is there a round-glass matrix? Is there a well-defined rim of the sclerotic border with septations potentially suggesting slow growth and encapsulation like most benign processes.
Periosteal proliferation: solid vs. aggressive spiculated/sunburst/hair-on-end with local soft tissue invasion and Codman triangle (study next slide)
FCD & NOF
FCD & NOF or more appropriately Fibroxanthoma of the bone are benign bone processes that m/c seen in children. DDx based on the size with FCD presenting as <3-cm and NOF >3cm lesion composed of a fibrous heterogeneous matrix. FCD are asymptomatic and may regress in many cases. Some may progress to NOF. Location: identified in the knee region as an eccentric cortical based lesion.
FCD must be DDx from an avulsive irregularity d/t repeated stress along Linea aspera by extensors muscles
Dx: radiography
Management: leave-me-alone lesion. Occasionally NOF may progress and lead to pathologic fracture requiring orthopedic consult
Osteochondroma
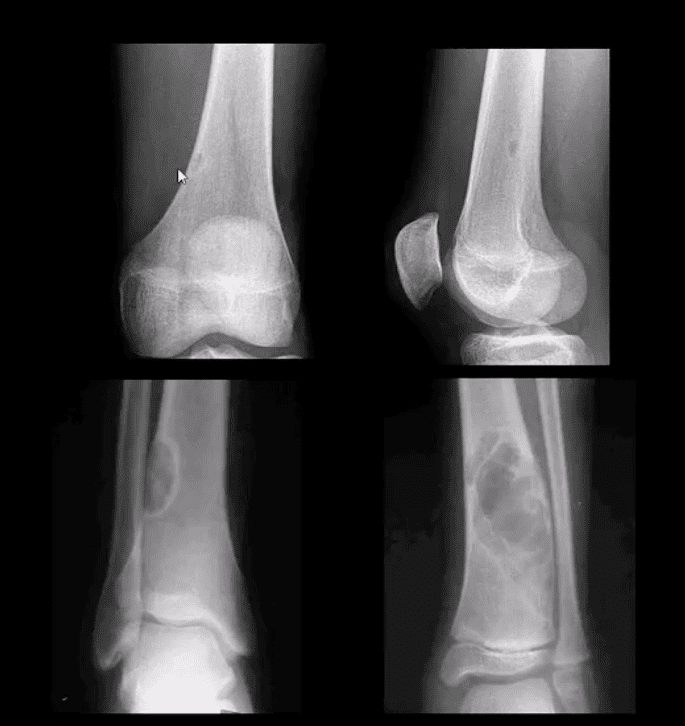
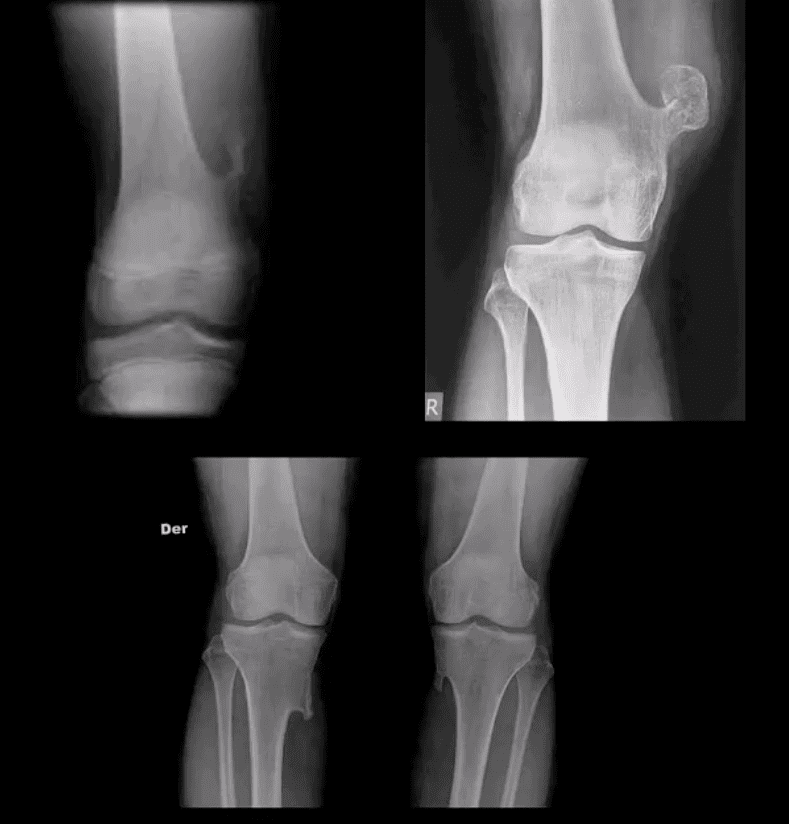
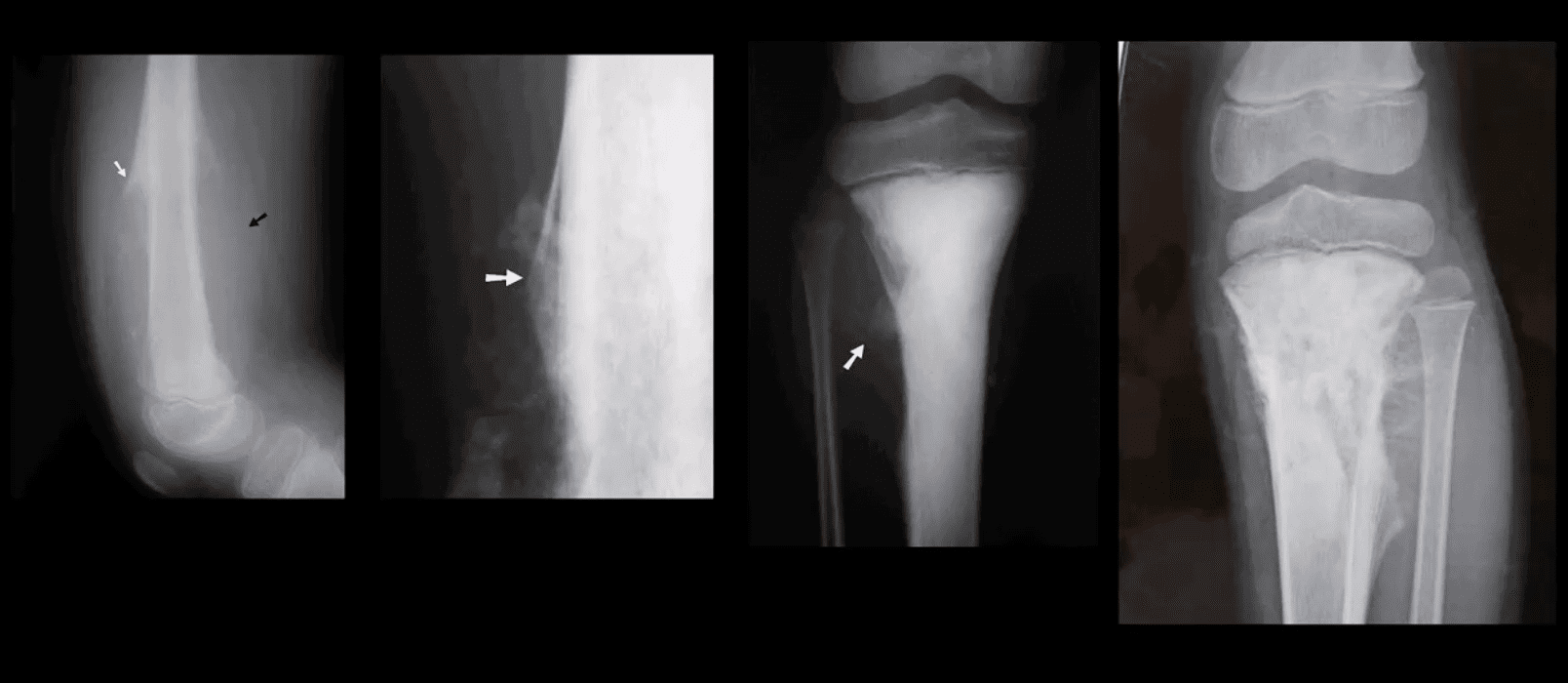
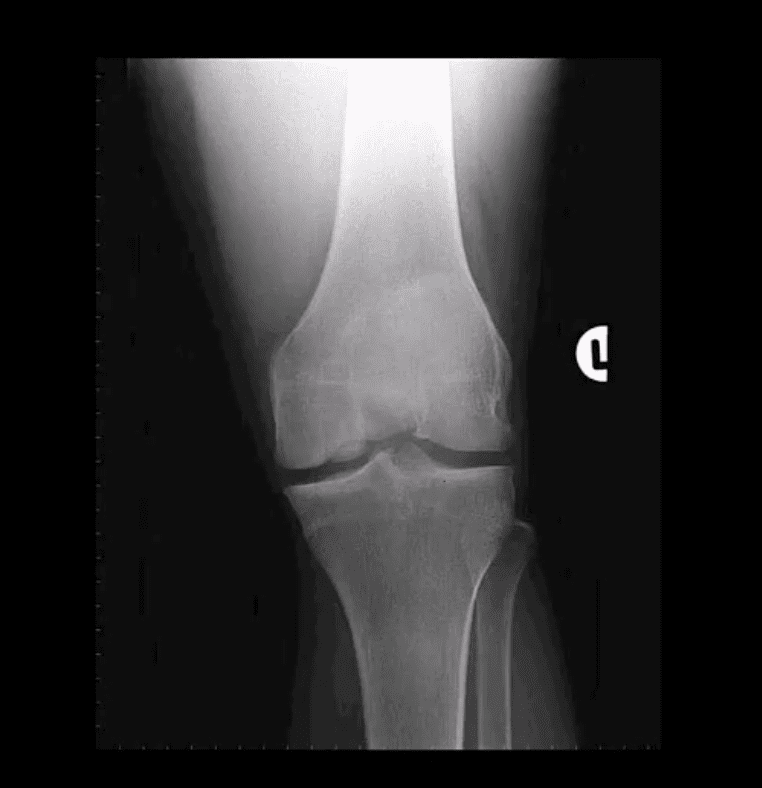
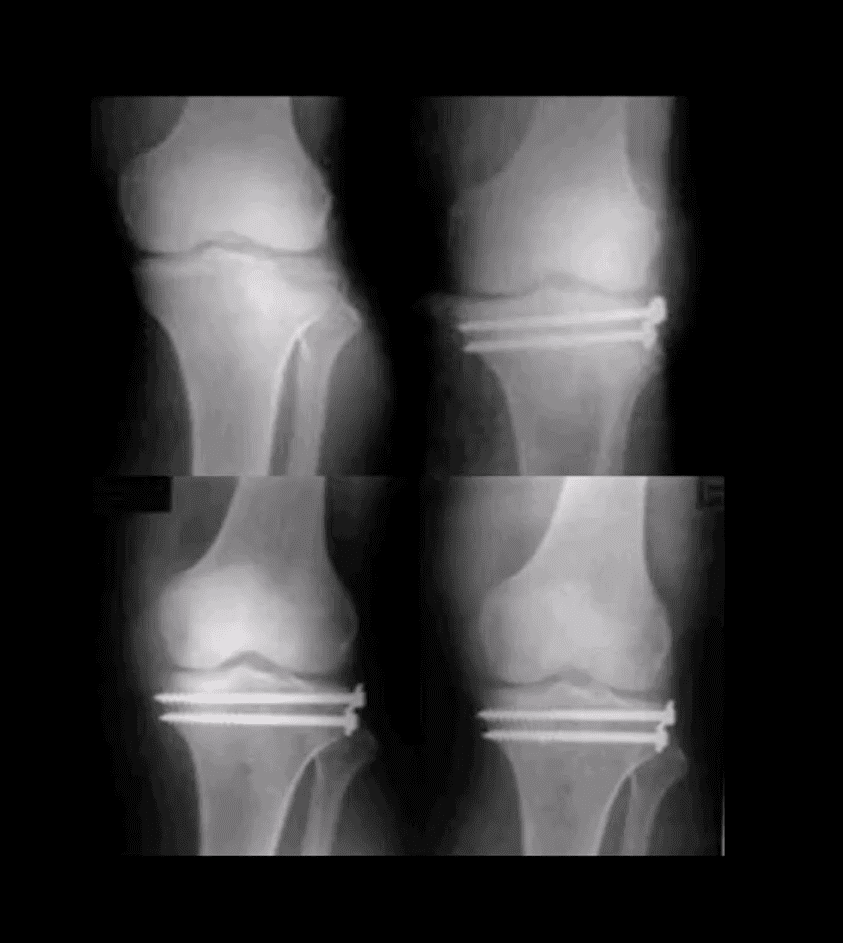
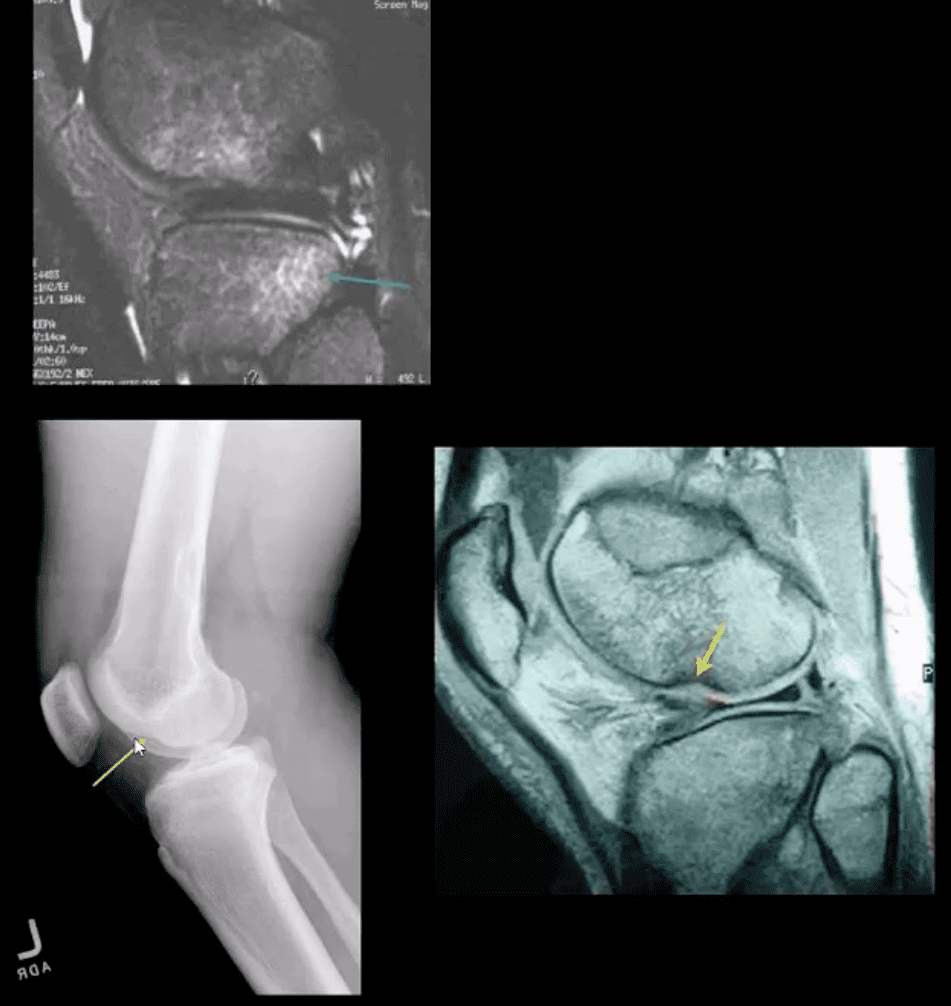
Osteochondroma: m/c benign bone neoplasm. Knee is the m/c location. Contains all bone elements with a cartilaginous cap. Presented as pedunculated or sessile bone exostosis pointing away from the joint.
1% malignant degeneration to chondrosarcoma if solitary lesion and 10-15% in cases of HME
Other complications: fracture (top left image) pseudoaneurysm of the Popliteal artery, adventitious bursa formation
Hereditary Multiple Exostosis (HME)– autosomal dominant process. Presents with multiple osteochondromas (sessile-type dominates). May lead to limb deformities (Madelung deformity, coxa valga) reactive ST pressure, malignant degeneration
Dx: radiography, MRI helps to Dx malignant degeneration to chondrosarcoma by changes in size and activity of cartilaginous cap (>2-cm in adults may manifest malignant degeneration). MRI will also help with Dx of regional complications
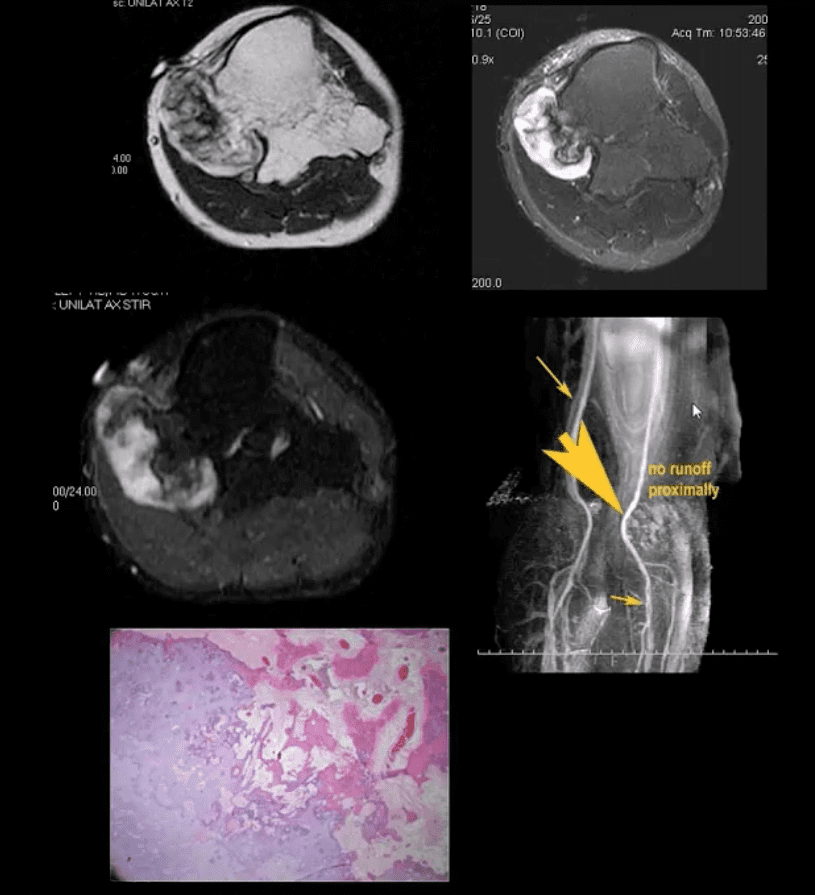
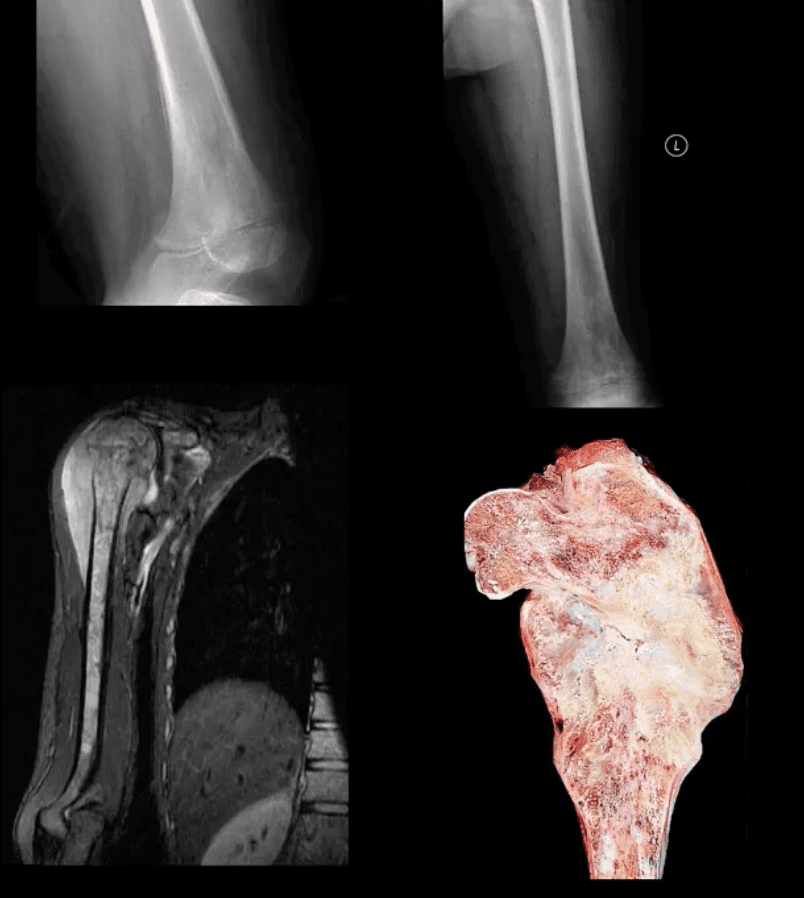
HME & Knee Pain
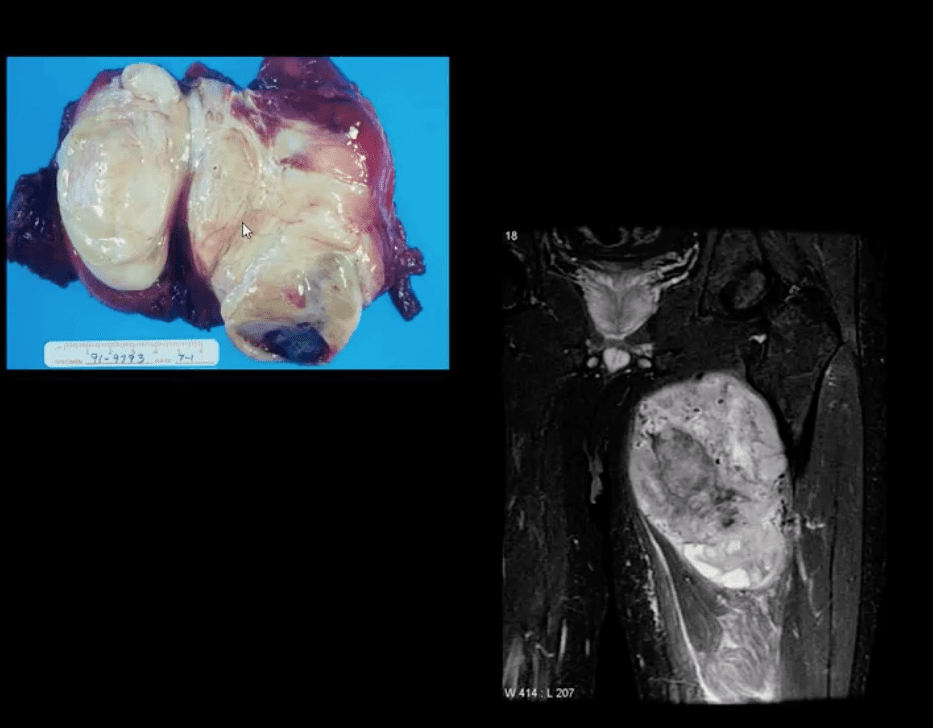
37-y.o male with HME and knee pain. Axial T1, T2 and STIR MRI slices at the popliteal region. Large cartilaginous cap and possible compression of the popliteal artery by osteochondroma. MRA was performed to evaluate popliteal A. pseudoaneurysm (large arrow). Pathology specimen obtained from the cartilaginous cap showed increased cellularity suggestive of malignant degeneration. Operative care was planned
Giant Cell Tumor (GCT) aka Osteoclastoma
GCT- is a relatively common primary benign bone neoplasm. Age 25-40. M>F slightly.
GCT is the M/C benign sacral tumor. In 50% of cases, GCT occurs about the knee.
GCT is histologically benign, but lung Mets may develop esp. if in distal radius and hands, often termed Malignant GCT
<1% unresponsive/recurring GCTs may undergo malignant transformation to high-grade bone sarcoma
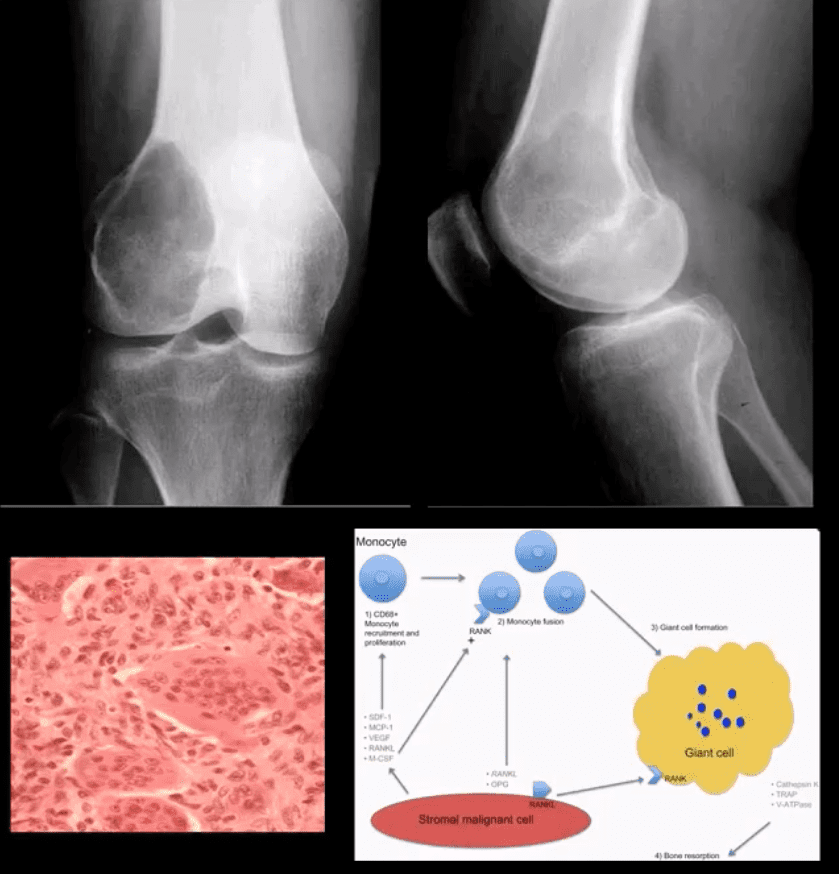
Pathology: histologically composed of osteoclasts-multinucleated giant cells with stromal cells derived from precursors monocyte-macrophage type. Produces cytokines and osteolytic enzymes. GCT may contain blood and associated with secondary Aneurysmal Bone Cyst (ABC)
Clinically: knee pain unresponsive to conservative care. Pathologic Fx may occur
Imaging: always begins with radiography followed by MRI and surgical biopsy that are crucial to Dx.
Rx: operative with curettage and cementing, a surgical appliance may be used if pathological fx present and cortical breach. In more severe cases other options available
Radiologic-Pathologic Dx
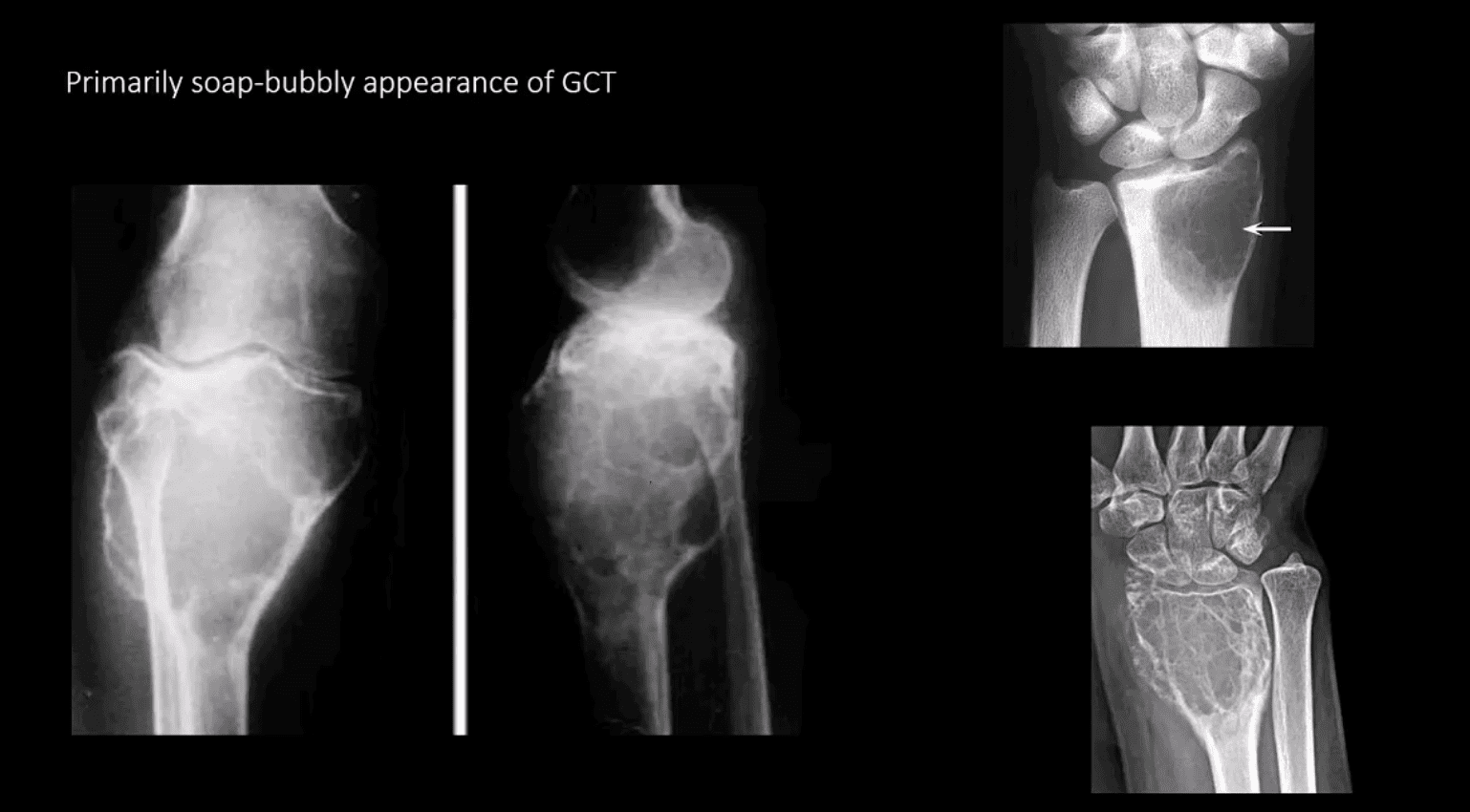
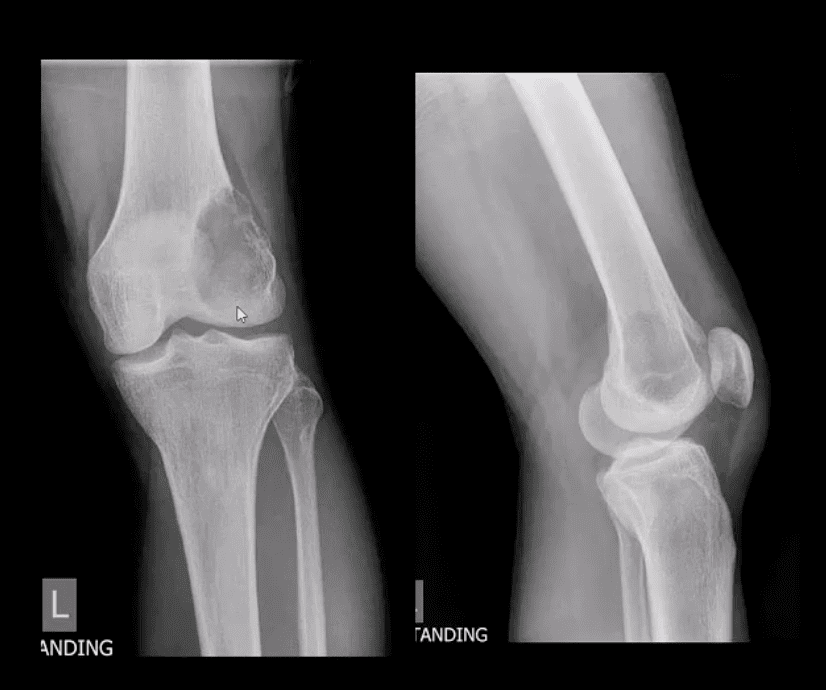
Radiologic-pathologic Dx: osteolytic and soap-bubbly lesion typically involving metaphysis and into epiphysis (classic key feature) with subarticular extension. Zone of transition is generally narrow but occasionally in aggressive lesions wide zone of transition may be seen.
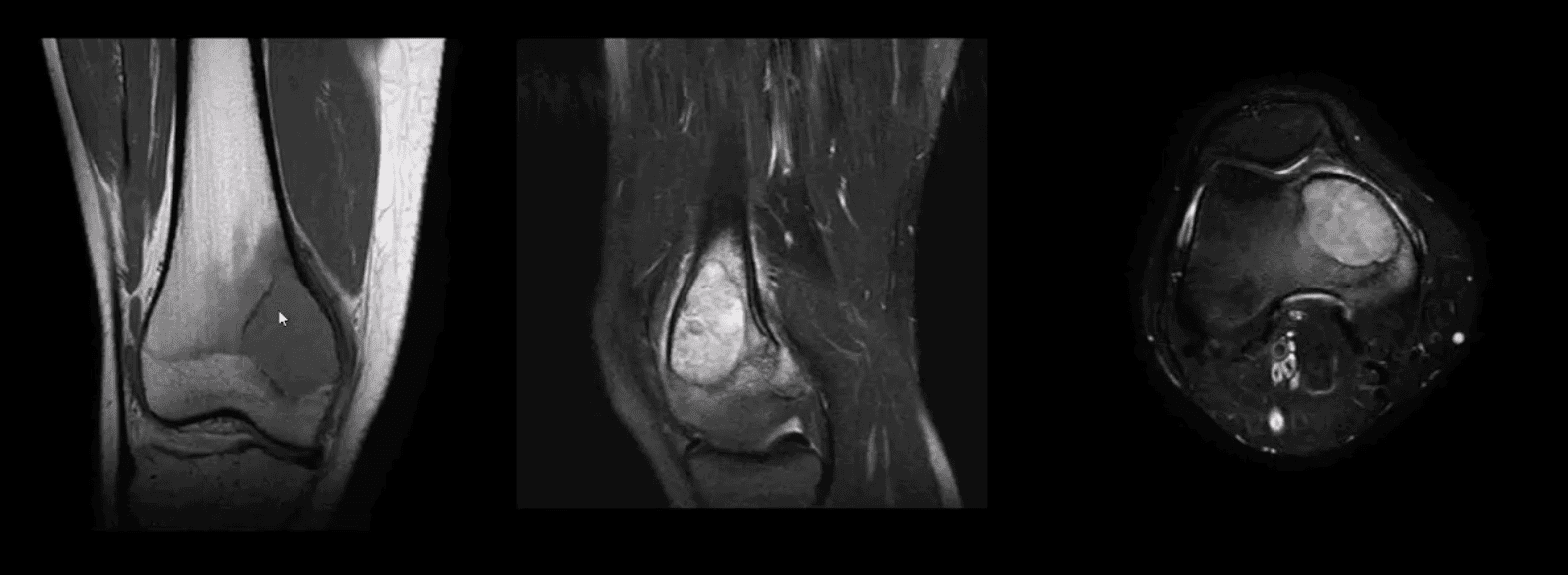
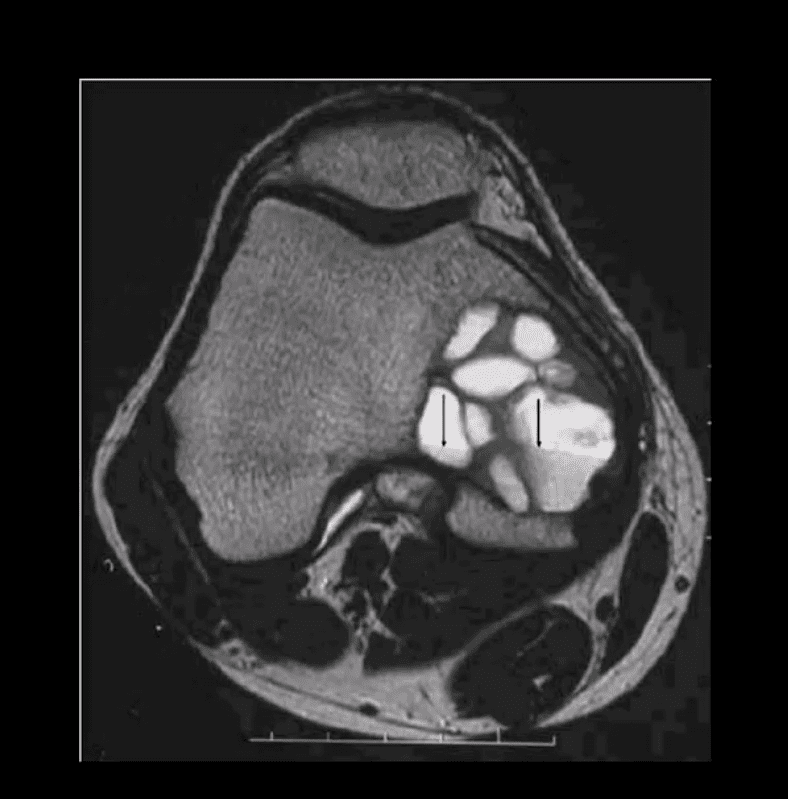
MRI: low T1, highT2/STIR, characteristic fluid-fluid levels noted that are present in GCT and ABC. Histology is crucial to Dx.
DDx: ABC, Brown cell tumor of HPT (osteoclastoma), Telangiectatic Osteosarcoma
Radiological rule: if the physeal growth plate is present Dx of GCT is taken off the list in favor of chondroblastoma and vice versa.
Primarily Soap-Bubbly Appearance of GCT
Coronal, Fat-Sat Sagittal & Axial MRI Slices of GCT
T1 coronal, T2 fat-sat sagittal and T2 axial MRI slices of GCT. Typically: low T1, highT2/STIR and fluid-fluid levels
Characteristic MRI Appearance of GCT
Fluid-fluid levels d/t different composition of blood degradation products
Important DDx: ABC
Malignant Neoplasms About the Knee
In children and very young adults, m/c primary malignant neoplasm is central aka intramedullary (osteogenic) osteosarcoma (OSA). Second peak of OS: >70 y.o d/t Paget�s (1%) and/or post radiation OSA.
The knee is the m/c location of OSA (distal femur, prox. Tibia)
A 2nd m/c malignant pediatric primary is Ewing sarcoma.
In adults >40 y.o. the m/c primary is Multiple Myeloma (MM) or Solitary Plasmacytoma
Overall m/c bone neoplasms in adults d/t bone Mets from lung, breast, prostate, renal cell, thyroid (discussed)
Dx: clinical and radiological with surgical biopsy
Imaging is crucial to Dx. 1st step x-radiography. MRI+ gad C is vital
CT scanning occasionally helps to evaluate pathological fracture
Central (Intramedullary) Osteosarcoma (OSA)
m/c age: 10-20. m/c location: knee, males>females. Increased risk in some
congenital syndromes and mutation of the retinoblastoma gene: Rothmund-Thompson AR syndrome.
Early Dx is important d/t 10-20% present with Lung Mets at Dx. Prognosis depends on stages. Early stages with local bone invasion and no
mets 76% of survival.
Rx: limb salvage procedures preferred with 8-12 weeks of chemo, amputation if encased neurovascular tissue, path Fx, etc.
Imaging: radiography and MRI.
Clinically: bone pain, Inc. Alkaline Phosphatase
Chest CT if lung Mets considered
Classic Rad Features of OSA
Osteoid forming a sclerotic mass with aggressive hair-on-end/speculated/sun-burst periosteal reaction, Codman’s triangle and soft tissue invasion. Order MRI for staging and extent. Chest CT is crucial for Lung Mets dx.
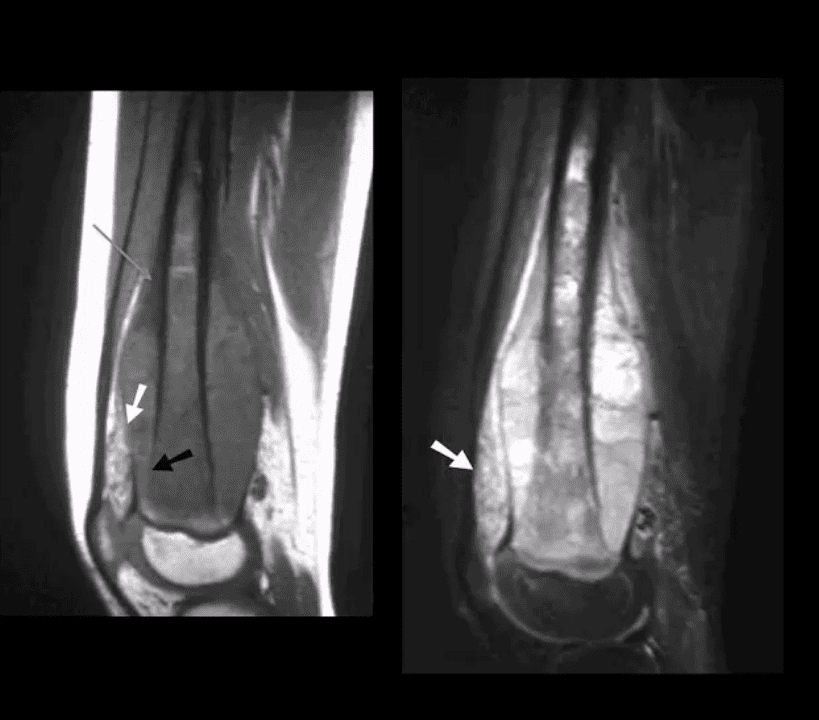
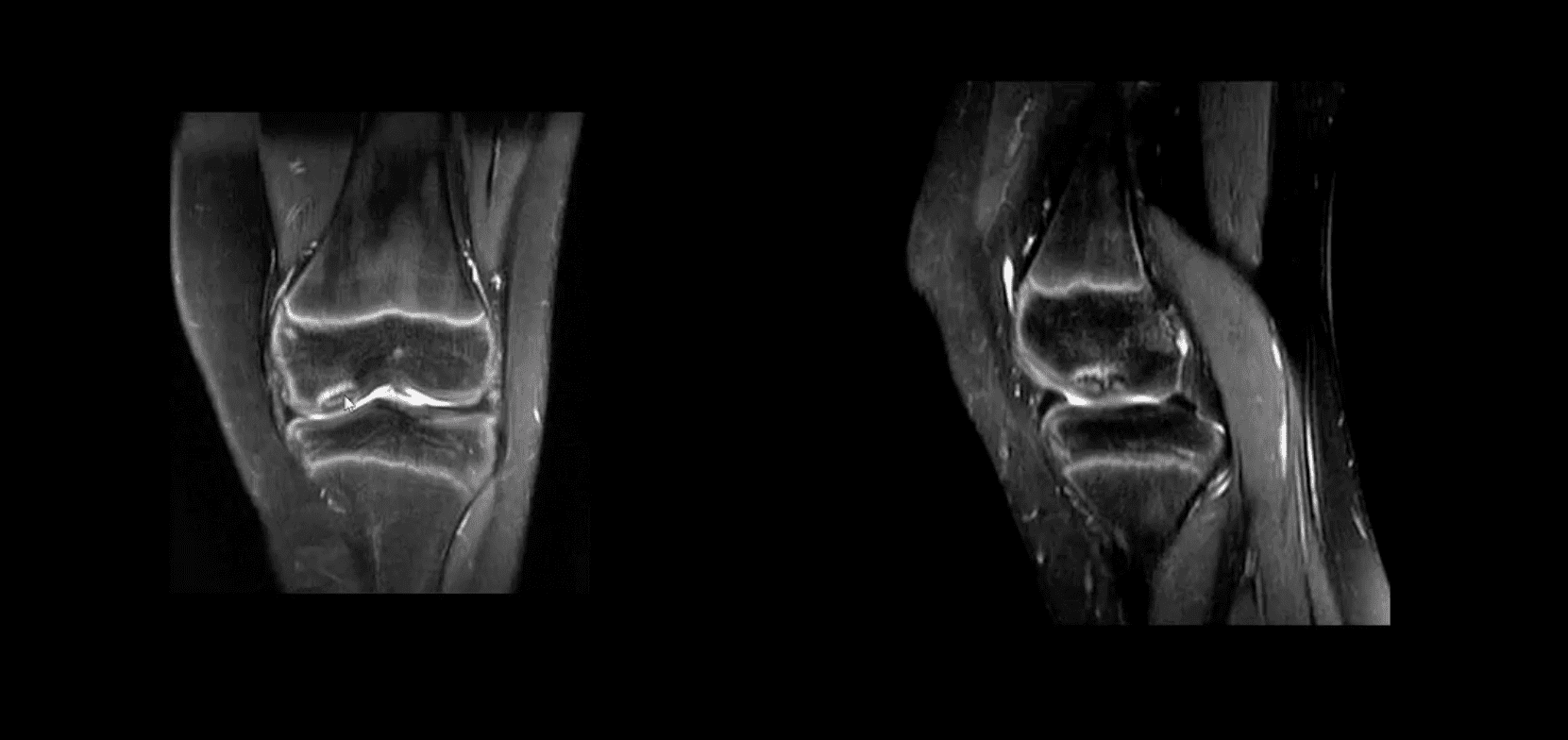
MRI is Crucial for Dx/Staging
Note sagittal T1 (left) and STIR (right) MR slices: large mass extending from distal femoral metaphysis to remaining shaft. A low signal on T1 and high on STIR d/t marrow invasion with edema, hemorrhaging and tumor invasion. Local ST invasion seen (white arrows). Periosteal lifting and Codman�s triangle (green arrow) are additional signs of aggressive neoplasm.
Note an interesting feature that the epiphysis is spared d/t physeal plate serving temporarily as an additional barrier to the tumor spread.
Ewing Sarcoma
Ewing sarcoma: age: 2-20, uncommon in black patients. 2nd m/c highly malignant bone neoplasm in children that typically arises from medullary cavity (Round cell tumors). Key symptom: bone pain that may mimic infection (ESR/CRP/WBC) Considered PNET Key Rad Dx: aggressive moth-eaten/permeative lucent lesions in the shaft of long bones with sizeable soft tissue invasion/typical onion skin periostitis. May produce saucerisation May affect flat bones. May appear as sclerotic in 33%. Early lung Mets (25-30%) bone-to-bone Mets Poor prognosis if delayed Dx. Imaging steps: 1st step x-rad, MRI is v. important followed by a biopsy. CXR/CT PET-CT Rx: combined rad-chemo, operative.
Note aggressive expansile osteolytic lesion in the distal femur metaphysis into epiphysis. No periosteal reaction present. Following further work up with abdominal and chest CT scanning, Dx of Renal cell carcinoma was established
Distal Mets into lower extremity are more common with lung, renal cell, thyroid and breast CA.
Renal cell and Thyroid will typically present with aggressive osteolytic expansile mass aka �blowout Mets.�
In general, imaging approach should consist of Radiographic knee series, followed by MRI if x-rays are unrewarding
Tc99 Bone scintigraphy is the modality of choice to evaluate metastatic bone disease
Soft Tissue Neoplasms About the Knee
Malignant fibrous histiocytoma (MFH) reclassified as Pleomorphic Undifferentiated Sarcoma (PUS) is the m/c S.T. sarcoma. MFH is aggressive biologically with poor prognosis M>F (1.2:1) 30-80 with a peak in a 6th decade. 25-40% of all adults sarcomas m/c extremities. Retroperitoneum next (worst prognosis d/t late Dx and large growth w/o symptoms) Clinically: painful, hard mass typically about the knee or thigh. Histology: poorly differentiated/undifferentiated malignant fibroblasts, myofibroblasts, and other mesenchymal cells Imaging: MRI is the modality of choice with T1, T2, T1+C. Typically appears as an aggressive heterogeneous mass intermediate to low signal on T1 and high signal on T2 with areas of necrosis and enhancement on T1+C. May appear misleadingly encapsulated w/o true capsule Management: operative with radiation and chemotherapy. Tumor depth is crucial for prognosis. 80% 5-year survival if <5cm deep in ST and 50% if >5-cm deep in ST.
Synovial Sarcoma
Synovial sarcoma: common malignant ST neoplasm esp. in younger patients or older children/adolescents. M/C found in knee area Clinically: can present slowly as a palpable mass in the extremity often ignored d/t slow growth Imaging is the key: radiography may reveal ST. density/mass. Some synovial sarcomas may show calcification and mistaken for Myositis Ossificanse or heterotopic bone formation MRI with T1, T2 and T1+C are Dx modality of choice. Other modalities: US, CT are non-specific DDx: MFH Management: operative, chemo-radiation Prognosis: variable depending on size, invasion, metastasis
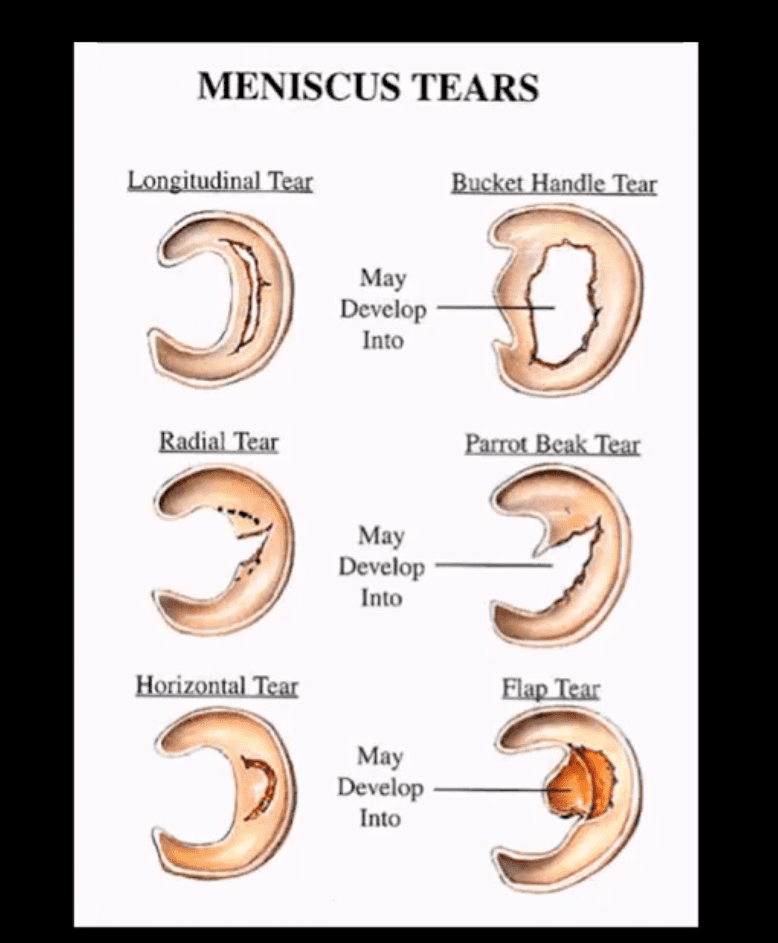
Types, location, and stability of tears are v. important during MRI Dx
Vertical/longitudinal tears especially occur in acute ACL tears. Some longitudinal tears found at the periphery or “red zone” may heal
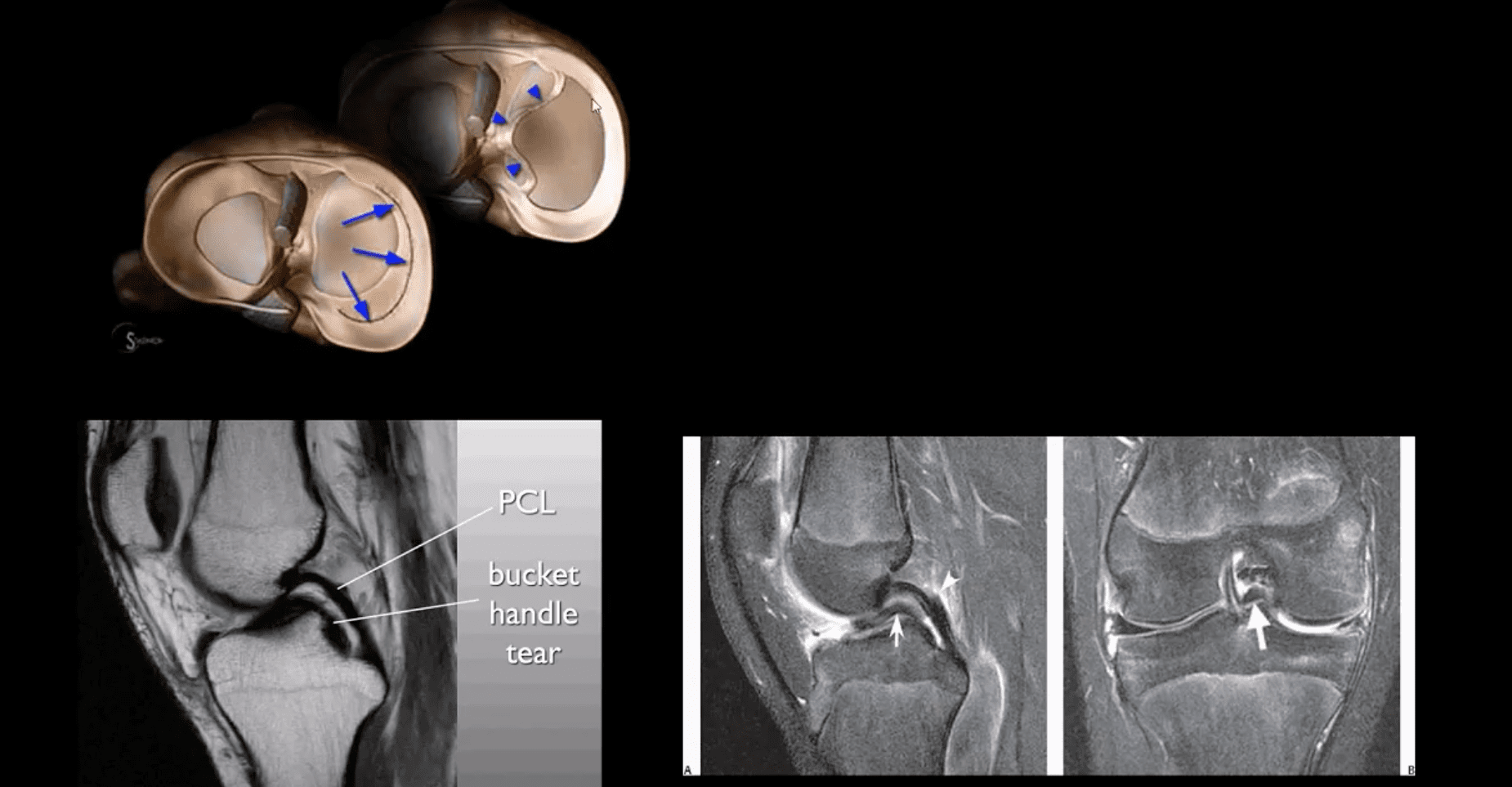
Bucket handle tear: longitudinal tear in the inner edge that is deep and vertical extending through the long axis and may displace into a notch
Oblique/flap/parrot-beak are complex tears
Radial tear at 90-degree to plateau
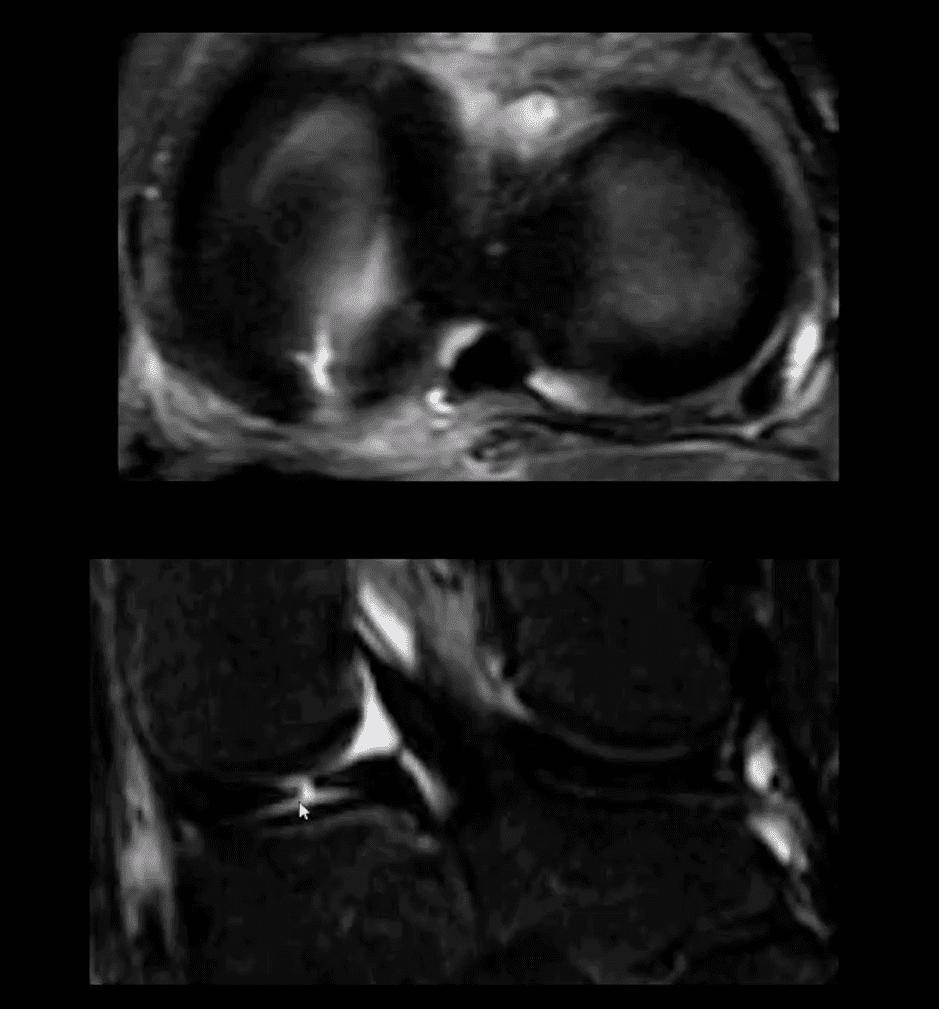
Axial T2
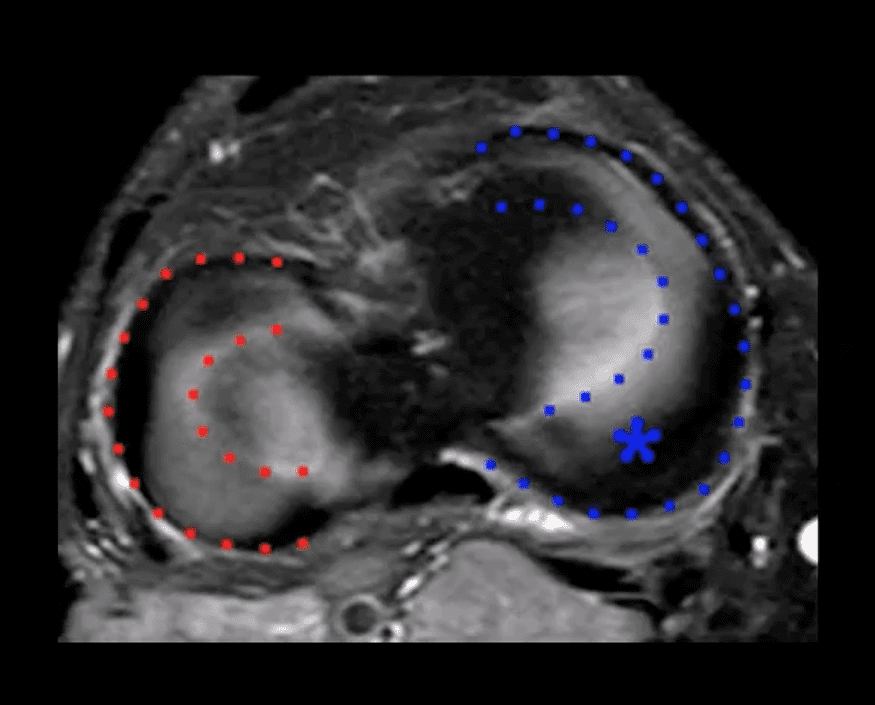
Axial T2 WI fat-sat and coronal STIR slices of the posterior horn of the medial meniscus.
Note a radial tear of the posterior horn of the medial meniscus near the meniscal root. This is potentially an unstable lesion requiring operative care
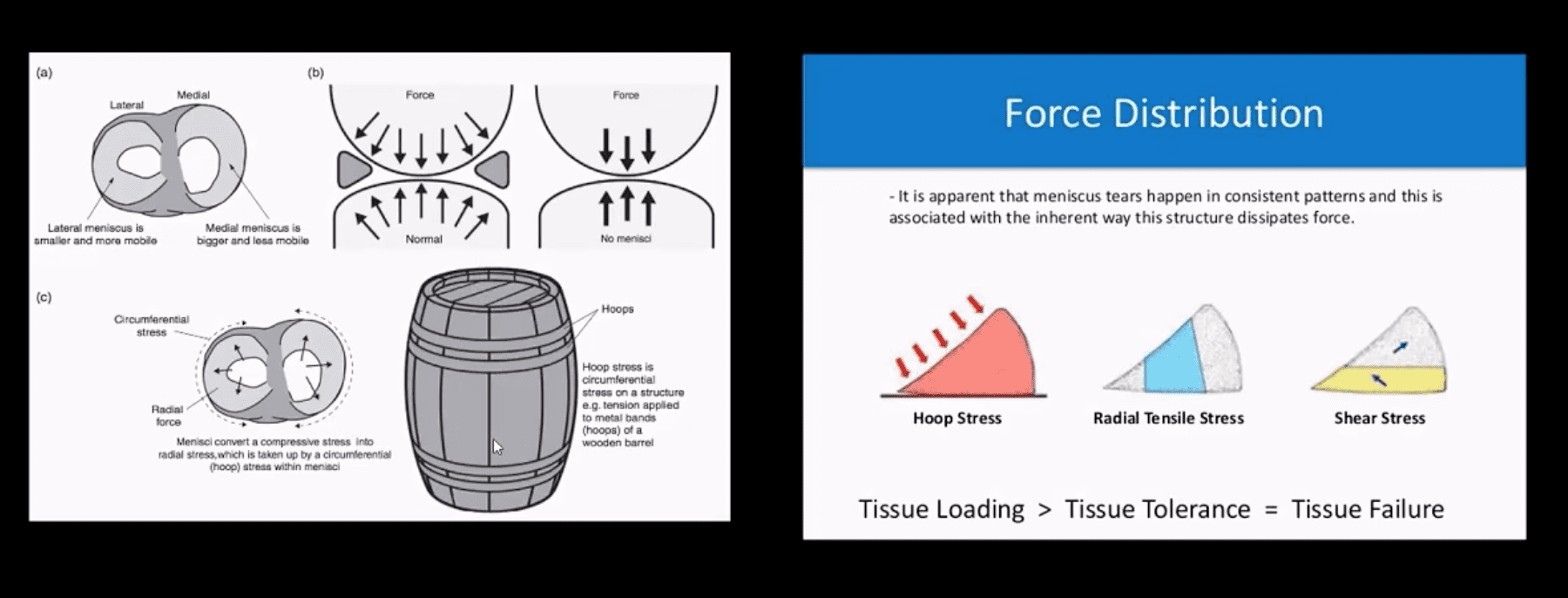
The meniscus, in this case, is unable to provide a “hoop-stress mechanism.”
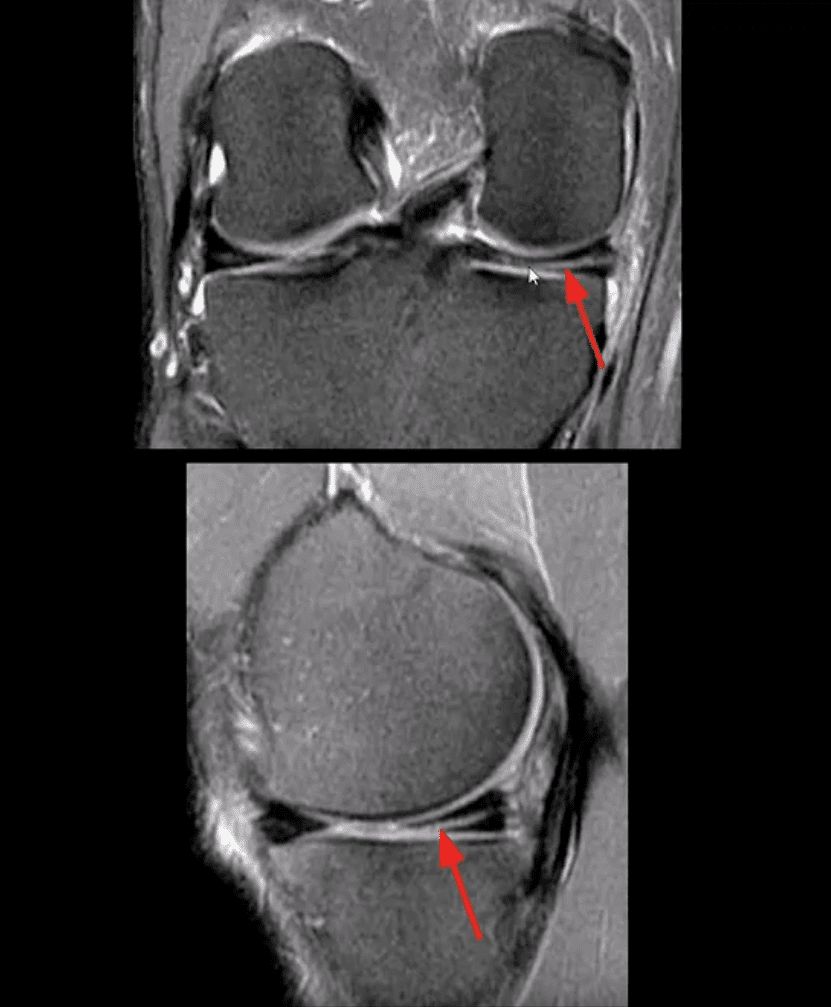
MRI Slices Coronal & Sagittal
Fat-sat coronal and sagittal proton density MRI slices revealing horizontal (cleavage) tear that is more typical in the aged meniscus
In some cases, when this tear does not contain a radial component, it may partially heal obviating the need for operative care
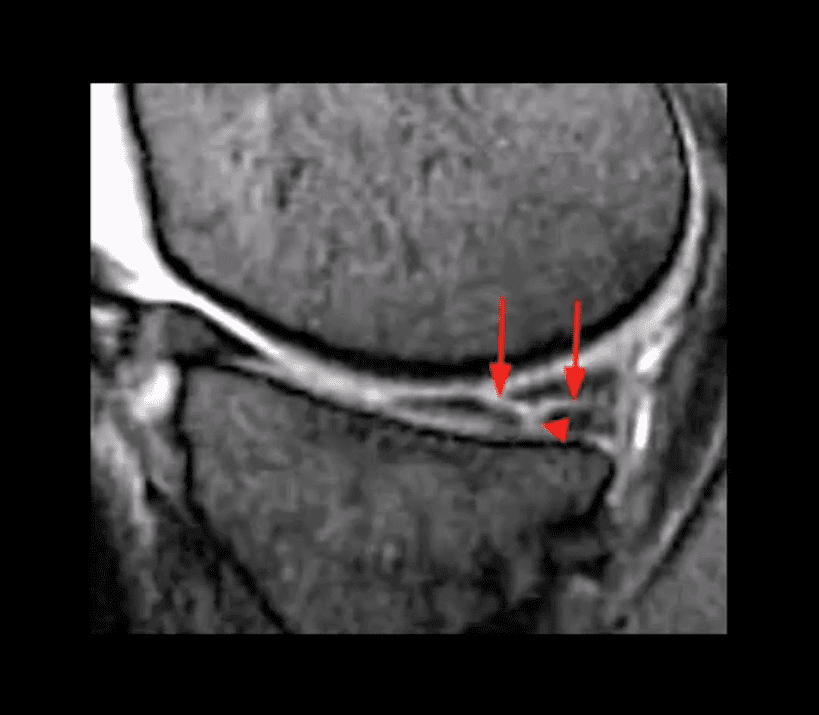
T2 w GRE Sagittal MRI Slice
Complex tear with a horizontal oblique and radial component.
This type of tear is very unstable and in most cases may need operative care
Bucket Handle Tear
Bucket handle tear are m/c in the medial meniscus esp. with acute ACL and MCL tear
MRI signs; double PCL sign on sagittal slices
Absent “bow-tie” sign and others
Most cases require operative care
DDx From Meniscal Degeneration
Occasionally meniscal tears need to be DDx from meniscal degeneration which may also appear bright (high signal) on fluid-sensitive MRI
The simplest rule is that if there is a true meniscal tear aka Grade 3 lesion, it always reaches/extends to the tibial plateau surface
The Role of MSK Ultrasound (US) in Knee Examination
MSK US of the knee permits high resolution and dynamic imaging of primarily superficial anatomy (tendons, bursae, capsular ligaments)
MSK US cannot adequately evaluate cruciate ligaments and the menisci in their entirety
Thus MR imaging remains modality of choice
Potential Pathologies Successfully Evaluated by MSK US
Patellar tendionosis/patellar tendon rupture
Quadriceps tendon tear
Prepatellar bursitis
Infrapatellar bursitis
Pes Anserine bursitis
Popliteal cyst (Baker cyst)
Inflammation/joint effusion with synovial thickening and hyperemia can be imaged with US (e.g., RA) especially with the addition of color power Doppler
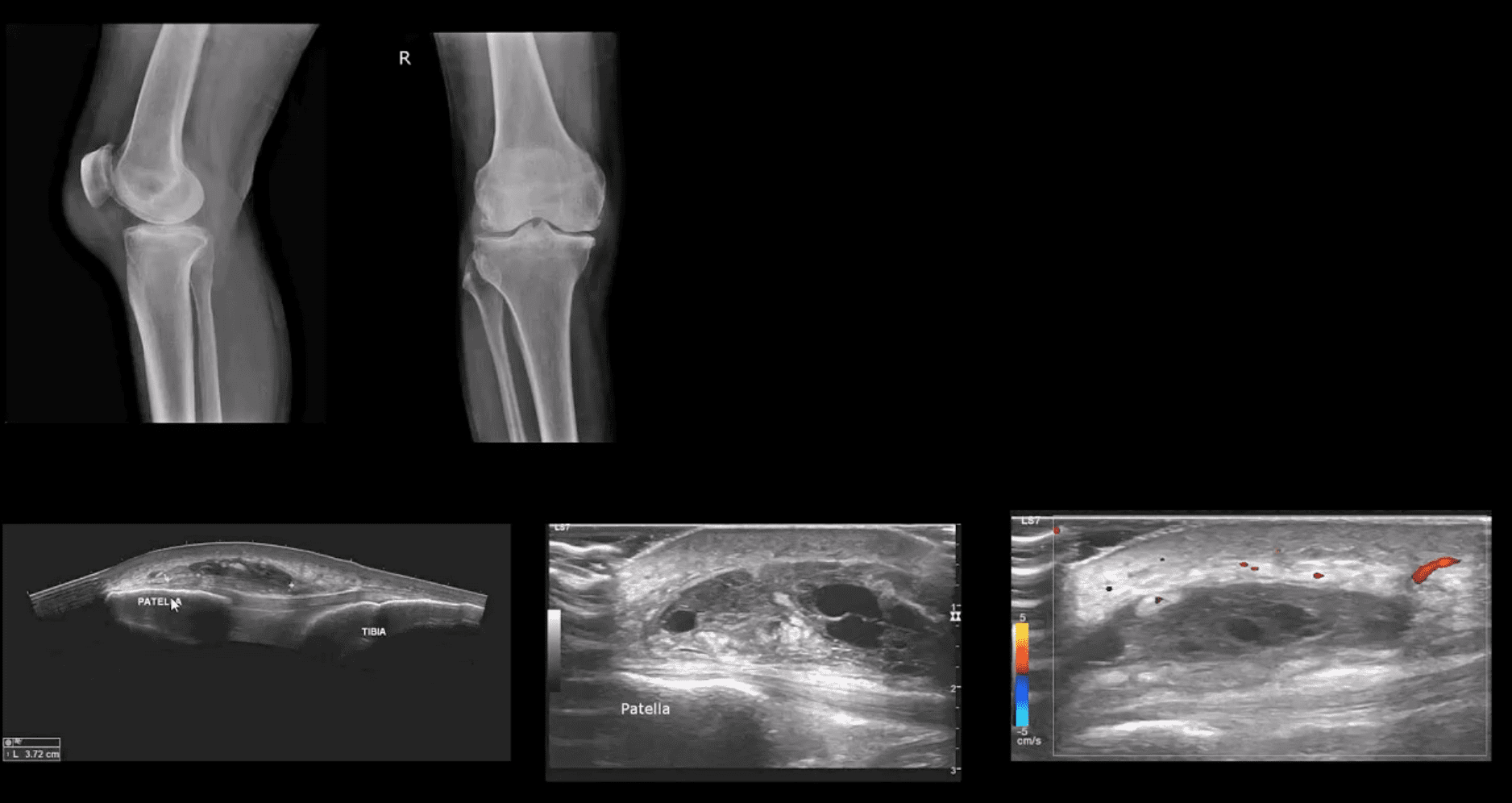
Patient Presented With Atraumatic Knee Pain & Swelling
Radiography revealed sizeable soft tissue density within the superficial pre-patella region along with mild-to-moderate OA
MSK US demonstrated large septated heterogeneous fluid collection with mild positive Doppler activity on the periphery indicating inflammation d/t Dx of Superficial pre-patella bursitis
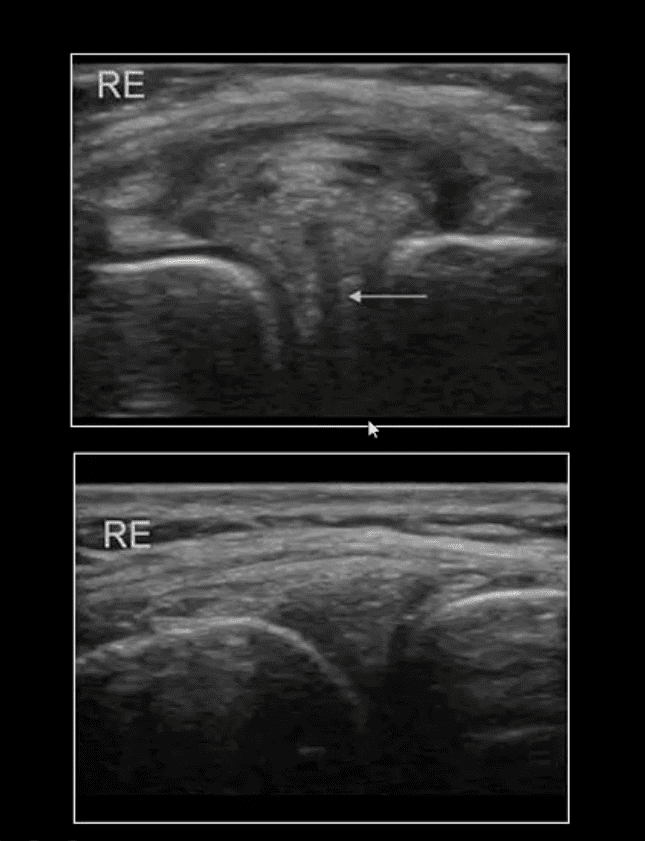
Long Axis US Images
Note normal lateral meniscus and fibers of LCL (above bottom image) compared to
Horizontal degenerative cleavage tear along with protrusion of lateral meniscus and LCL bulging (above top image)
Major limitation: unable to visualize the entire meniscus and the ACL/PCL
MRI referral is suggested
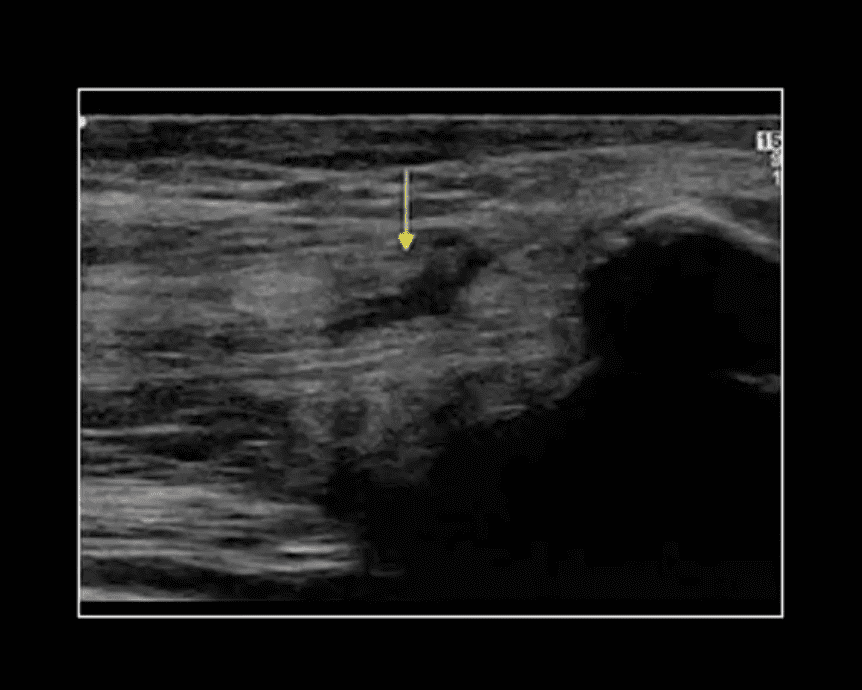
Rupture of Distal Tendon of Quadriceps
Note rupture of distal tendon of the Quadriceps muscle presented as fiber separation and fluid (hypo to anechoic) fluid collection within the substance of the tendon
Advantages of MSK US over MRI to evaluate superficial structures:
Dynamic imaging
Availability
Cost-effective
Patient’s preparation
Disadvantages: limited depth of structures, inability to evaluated bone and cartilage, etc.
Osteochondral Knee Injuries (OI)
osteochondral knee injuries can occur in children 10-15 y.o presented as Osteochondritis Dissecance (OCD) and in mature skeleton m/c following hyperextension and rotation trauma, particularly in ACL tear.
OCD-typically develops from repeated forces in immature bone and affects m/c postero-lateral portion of the medial femoral condyle.
OI in mature bone occurs m/c during ACL tears mainly affecting so-called terminal sulcus of the lateral femoral condyle at the junction of the weight-bearing portion opposed to tibial plateau and the part articulating with the patella
Osteochondral injuries may potentially damage the articular cartilage causing secondary OA. Thus need to be evaluated surgically
Imaging plays an important role and should begin with radiography often followed by MR imaging and orthopedic referral.
OCD Knee
95% associated with some trauma. Other etiology: ischemic bone necrosis especially in adults
Other common location for osteochondral injuries: elbow (capitellum), talus
1st step: radiography may detect osteochondral fragment potentially attached or detached
Location: a posterior-lateral aspect of the medial femoral condyle. Tunnel (intercondylar notch) view is crucial
MRI: modality of choice >90% specificity and sensitivity. Crucial for further management. T1-low signal demarcating line with T2 high signal demarcating line that signifies detachment and unlikely healing. Refer to orthopedic surgeon
Management: stable lesion esp. in younger children>off weight-bearing-heals in 50-75%
Unstable lesion and older child or impending physeal closure>operative fixation.
Result from valgus or varus stress with or w/o axial loading
Associated with periarticular soft tissues injury
High-stress injury m/c due to jumps falls and axial loading, often with the splitting of the tibial plateau. Men>women. Patients are in their 30s
Low impact or no trauma in patients with osteoporosis d/t insufficiency fractures
Impaction injury is more common with depression of tibial plateau. Women>men. Patients are in their 70s
Lateral Tibial Plateau Fractures More Common
Functional anatomy plays a significant role
60% of weight bearing is by the medial plateau
The medial plateau is more concave
Lateral plateau is slightly higher and more convex. Valgus stress impacts lateral plateau.
Tibial plateau fractures considered intra-articular and prone to delayed healing, non-union, meniscal injury (m/c lateral) ACL tear, secondary OA. Other complications: compartment syndrome, vascular injury.
Management: operative in many cases especially if >3-mm step-off at the plateau
If medial plateau or bicondylar Fxs present, ORIF will be required.
Imaging Plays A Crucial Role
Begins with x-radiography. X-radiography may not reveal the complexity and extent of this injury.
CT scanning w/o contrast will further delineate fracture complexity and pre-operative planning
MR imaging may be considered to evaluate for internal derangement: meniscal, ACL injuries.
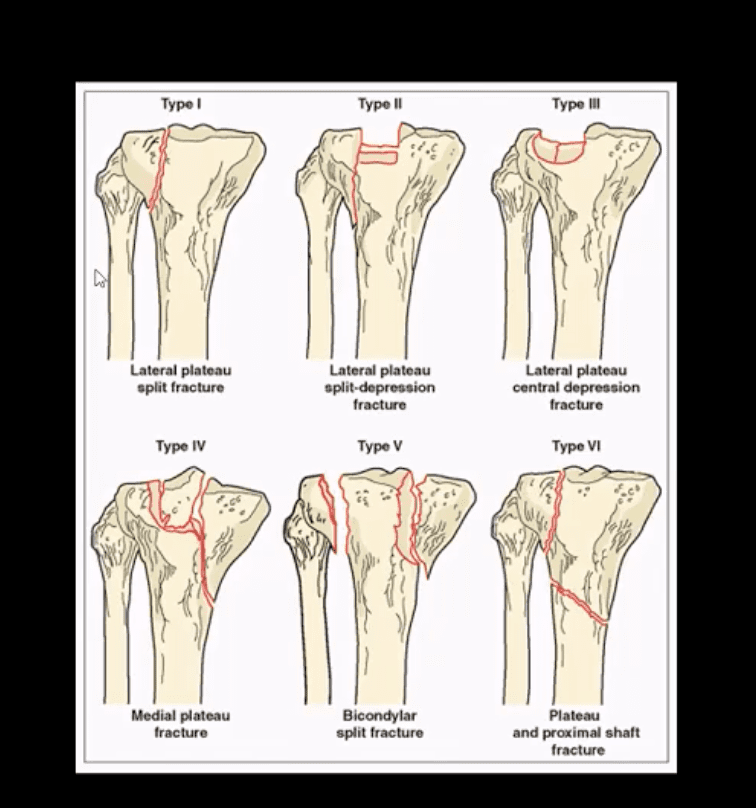
Shatzke classification may help to evaluate the complexity of this injury
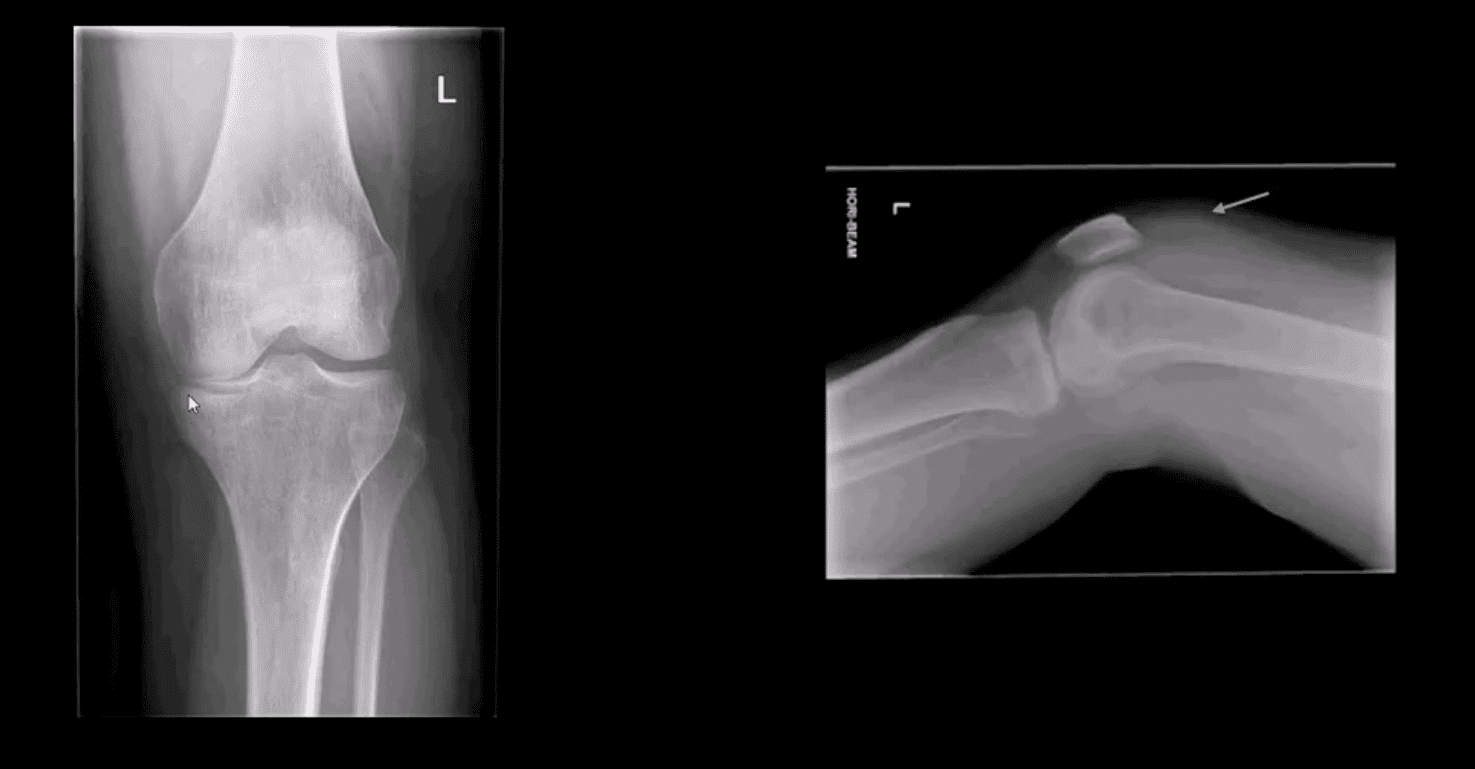
Key Diagnostic Sign
AP and lateral horizontal beam (cross table) left knee radiograph. Note subtle depression of the lateral plateau manifested by the lateral plateau appearing at the same level or lower as the medial. A critical diagnostic sign is the presence of fat-blood-interphase or FBI sign on cross-table lateral (above arrow) indicating intra-articular knee fracture
Lipohemarthorosis aka FBI Sign
Can be detected by radiography, CT or MR imaging
FBI sign is a reliable secondary radiographic sign of intra-articular knee fractures, regardless of how small they are
Mechanism: fracture results with acute hemarthrosis
Hemarthrosis will also occur w/o Fx. However, Fx will result with a fatty marrow being released into the joint cavity. Fat is a less dense medium (lighter) and will appear on the top of the hemorrhage if the patient is held in the supine position for 5-10-minutes before the cross-table radiograph is taken
FBI sign confirms the intra-articular Fx.
ACL/PCL, meniscal tears will not result in FBI sign
Lateral Tibial Plateau Fx
Lateral tibial plateau Fx that was managed operatively
Most common complication: premature secondary OA
More complex injuries may result in more extensive operative care
Knee Internal Derangement
Acute or chronic injuries of meniscal fibrocartilages and ligamentous restraints
Tears of the ACL and posterior horn of the medial meniscus are the most common
Acute ACL tears, however, often result with a lateral meniscus tear
Acute ACL tear may occur as a combined injury of the ACL, MCL, and medial meniscus
Functional anatomy: ACL prevents anterior displacement of the tibia and secondary varus stress
MCL functions together with ACL in resisting external rotation of the tibia especially when the foot is planted (closed chain position)
MCL is firmly attached to the medial meniscus, explaining the classic triad of ACL, MCL and medial meniscal tear (O’Donahue terrible triad)
Cruciate ligaments (ACL/PCL) are intra-articular but extra-synovial. Less likely to be torn in closed pack position (full extension). When all articular facets of tibia and femur are in full contact, the ACL/PCL are at least tension and stable
When the knee is flexed 20-30-degrees or more ACL is taut and remains unstable
ACL is a significant mechanoreceptor that feeds the info to CNS about the joint position. Thus the majority of previous ACL tears will lead to some degree of knee instability
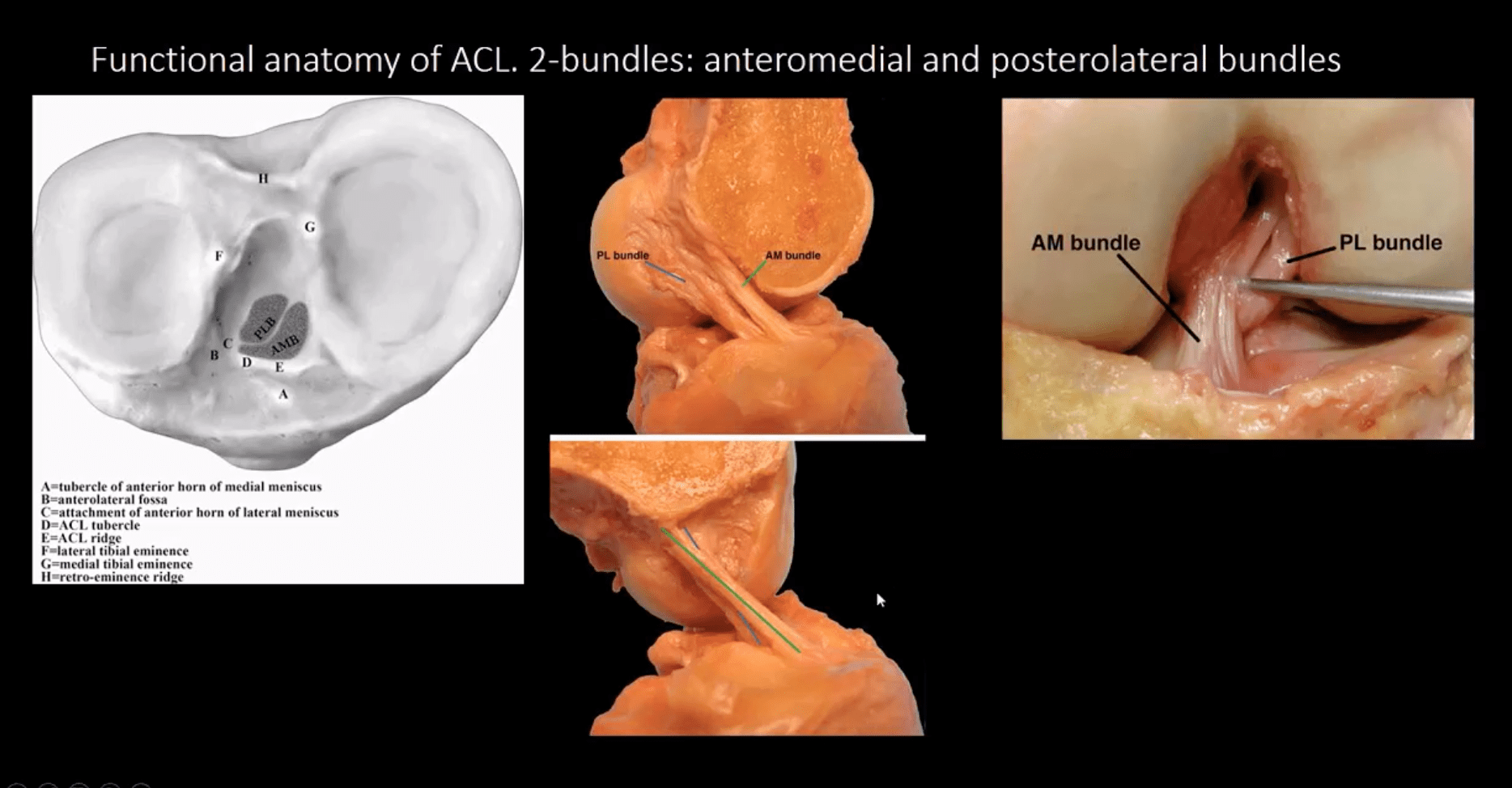
Functional Anatomy of ACL
Diagnosis of ACL Tear
Diagnosis of ACL tear requires MR imaging
Concerns exist of not only ligamentous injuries but injuries to the articular cartilage and menisci.
Most vendors will perform at least: one T1 WI in coronal or sagittal planes. Sagittal and coronal Proton-density slices to evaluate cartilaginous structures. Fast spin-echo sagittal, axial and coronal T2 fat-saturated or sagittal and coronal STIR images are crucial to demonstrate edema within the substance of knee ligaments
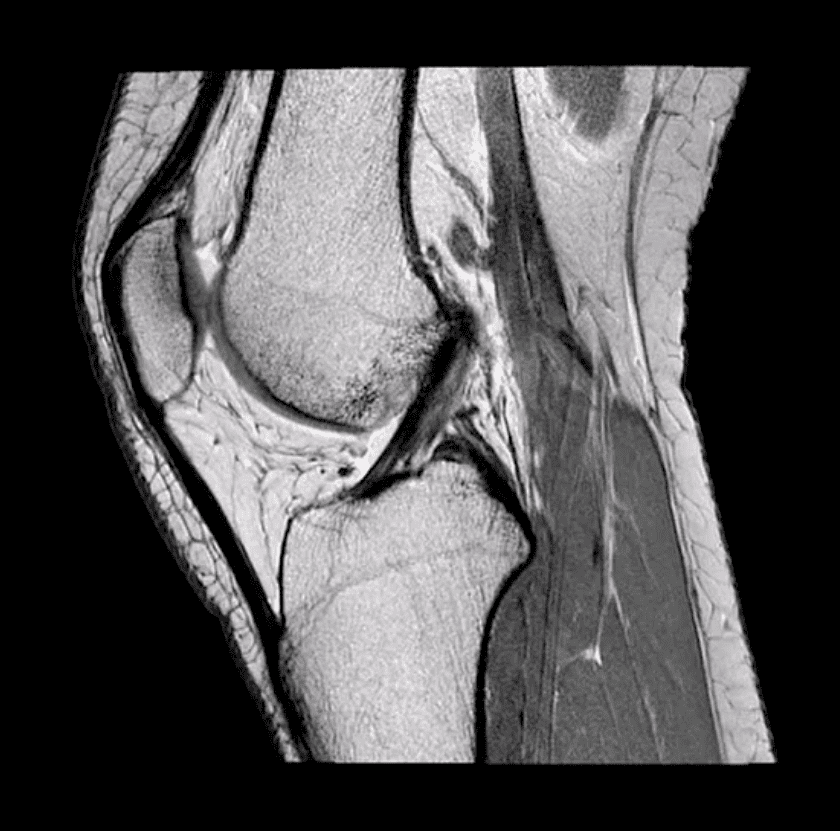
ACL is aligned along the Blumensaat line or oblique line corresponding the intercondylar roof of Femoral condyles. Lack of such alignment by the ACL is significant for ACL tear
Imaging Dx of Internal Derangement
MRI shows 78-100% sensitivity and 78-100% specificity
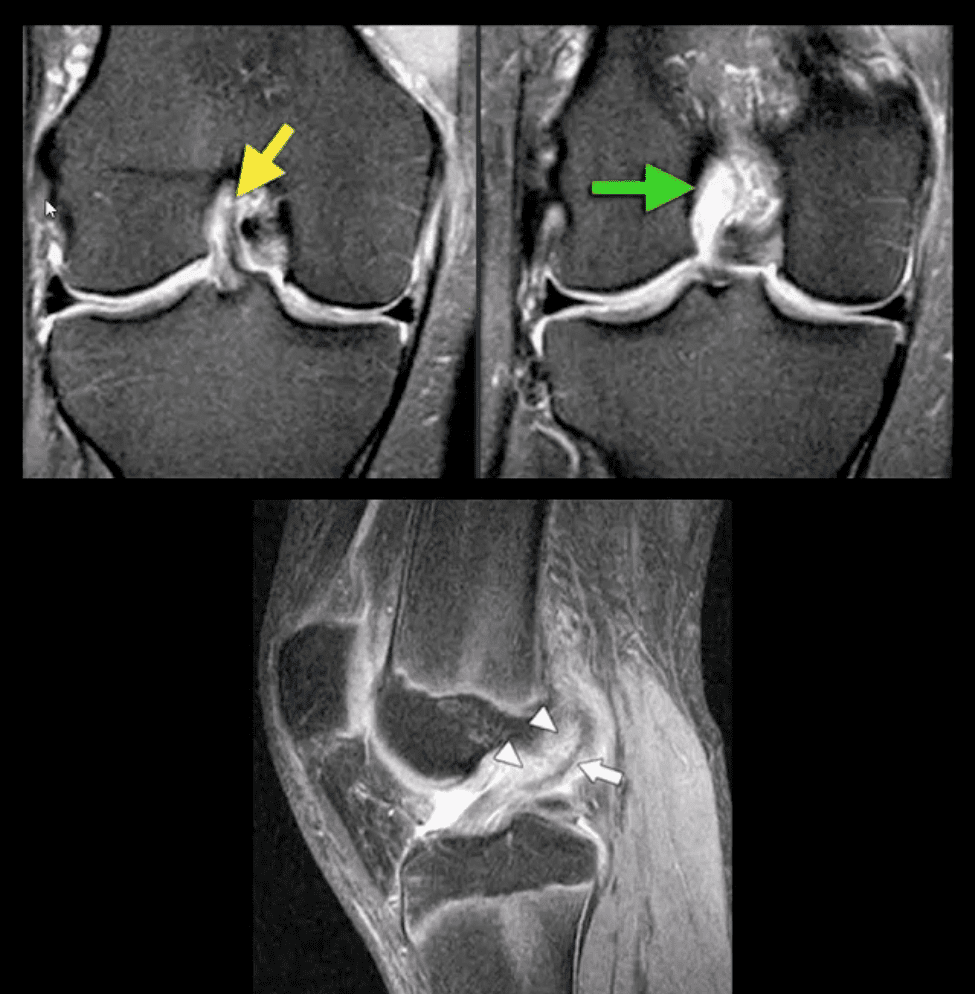
Primary signs of ACL tear: non-visualization of ACL (above green arrow), loss of its axis along the Blumensaat line (above triangle heads), wavy appearance and substance tear (above white arrow) or edema and cloud-like indistinctness (above yellow arrow)
Reliable Secondary Signs of ACL Tear
May be observed on the radiographs and MRI
Segond avulsion fracture (80% specificity for ACL tear) (next slide)
Deep femoral notch sign indicating osteochondral fracture (above bottom images) and
Pivot -shift bone marrow edema in the posterolateral tibial condyle d/t external rotation and often valgus impact by the lateral femoral condyles (above top image)
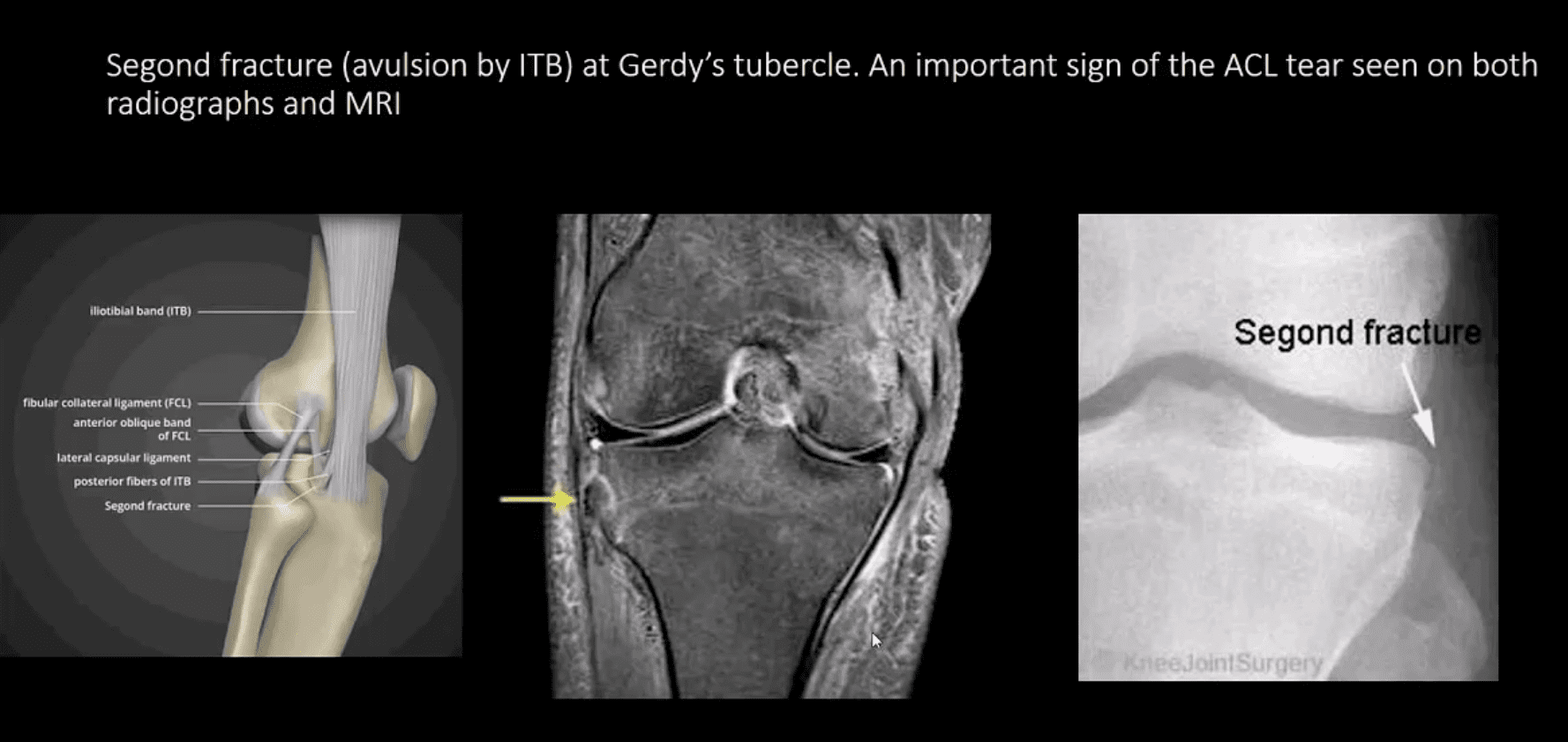
Segond Fracture (Avulsion by ITB)
Segond fracture at Gerdy’s tubercle. A vital sign of the ACL tear seen on both radiographs and MRI
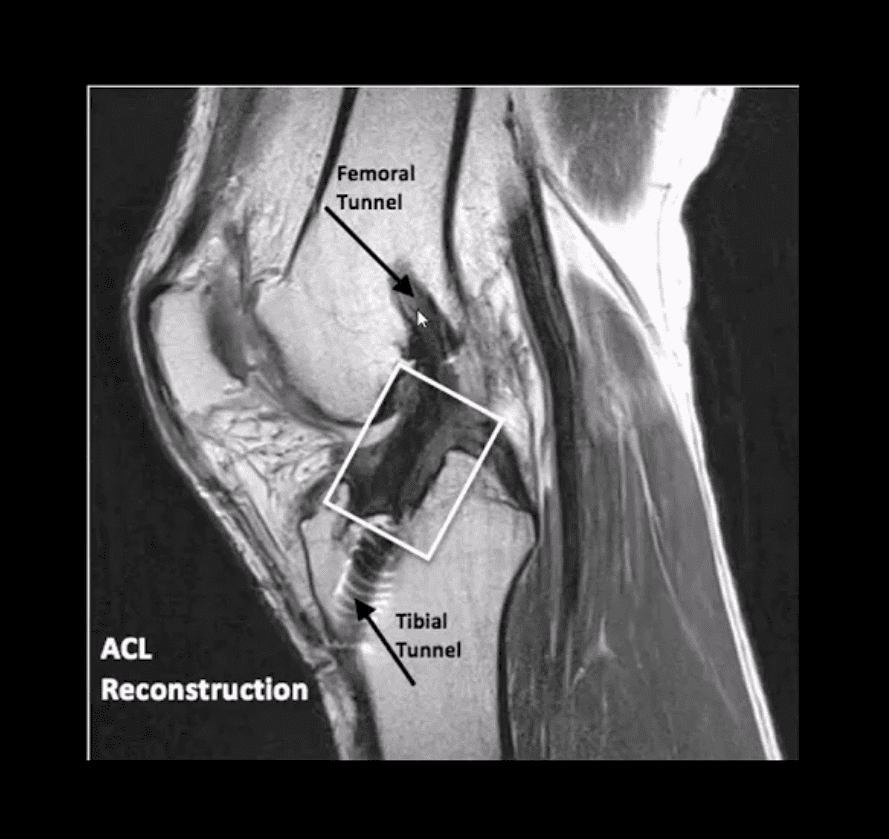
Management of ACL Tears
In acute cases, usually operative using cadaveric or autograft (patella ligament or hamstring) ACL reconstruction
Complications: graft tear, instability and premature DJD, joint stiffness d/t lack of postoperative rehab or gaft shortening. More rare, infection, a formation of intraosseous synovial cysts, etc.
Knock knee is a condition that many children acquire when they are toddlers. Often, within a few years they grow out of it and their legs straighten naturally with no lasting effects.
Occasionally, though, a child�s legs don�t straighten and this is a cause for concern. There are many problems that can stem from knock knees, some of which will follow the child into adulthood and for the rest of his or her life. While there are several recognized treatments for knock knee, including surgery, chiropractic care has an excellent track record in managing and remedying this disorder.
What Is Knock Knee?
Knock knee, or genu valgum, is a condition that causes a person�s knees to bow in toward each other. In other words, when they stand with their knees touching and feet flat, parallel to each other, facing forward, their ankles do not touch. There may be a few inches between them or a foot, depending on its severity.
Most children go through a stage at around 3 or 4 years where they are knock kneed but by around age 8 or 10 they grow out of it and their legs straighten. Many parents become concerned when they first see their child becoming knock kneed. This is why it is vital that they understand a child�s normal growth patterns. It helps them worry less about something completely normal as well as know when to seek help if the condition does not right itself.
Aside from normal physiological child development, the atypical version of knock knees can be caused by several factors including:
Bone deformities
Knee malalignment
Genetics
Infection
Weak knee infrastructure
Injury
Rickets Disease
Scurvy
Blount�s Disease
What Health Problems Can Be Caused By Knock Knee?
Knock knee can cause pain and inflammation in the knees, ankles, and feet, as well as the hip and back. The pain can make mobility difficult. This is exacerbated if the patient is overweight because the added pressure on the joints as they are set at an unnatural position that does not adequately support the body can result in injuries to the bone, ligaments, and tendons.
A difference in leg length, a common issue with knock knee, can also cause the body to become misaligned, leading to back and hip pain. Over the long term and in severe cases, knock knee can lead to arthritis in adults and children.
How Is Knock Knee Treated?
Treatment for knock knee depends on the cause and age of the child. If the child is young and it has been determined that the knock knee is just a normal part of their growth pattern, very little action is taken although some experts advise laying a good foundation for the child by teaching them the importance of a healthy diet, regular exercise, and good posture.
Cases that are caused by some underlying factor, or that extend beyond the age that the child�s legs are expected to straighten, may require bracing. If there is an underlying cause such as infection or injury, that will need to be addressed in order to correct or manage the problem. In severe (and rare) cases, surgery may be necessary.
Is Chiropractic Care An Effective Treatment For Knock Knee?
Chiropractic care is an exceptional treatment for children of all ages who have knock knee. For younger patients who are experiencing it as a normal stage of development, it will help to keep their spine aligned and encourage good, healthy posture. In children who have an underlying cause, it can help to relieve any pain while increasing mobility as well as bringing the spine into proper alignment.
Many of the factors that cause knock knee can be addressed through chiropractic treatment and it has the added benefit of providing a whole-body wellness approach that teaches proper diet, exercise, and lifestyle changes. This noninvasive, gently, natural treatment can give children their best chance at being free from this condition.
Injury Medical Clinic:�Chiropractic Care Knee Injury
Vincent Garcia, an athlete training in mixed martial arts, or MMA, suffered a knee injury and developed turf toe, but that has not stopped him from engaging in his normal training regimen. In order to return to as well as enhance his first physical performance, Vincent Garcia found treatment with Dr. Alex Jimenez, doctor of sports chiropractic. Now recovering from his sports injuries, Vincent Garcia looks forward to regaining his strength, flexibility and freedom to go back to sport.
Sports Injury Chiropractic Treatment
Exercising is important for overall health and wellness, but occasionally, an individual can suffer an injury when playing sports or engaging in physical activities. Accidents, poor training methods, or improper equipment can cause them. Some people today get hurt because they aren’t in shape. Not warming up or stretching enough can also lead to injuries. Treatment often begins with the RICE (Rest, Ice, Compression, and Elevation) method to relieve pain, reduce swelling, and speed recovery. Other possible treatments include pain relievers, rehabilitation, and sometimes surgery, if needed.
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
If you have enjoyed this video and/or we have helped you in any way please feel free to subscribe and recommend�us.
Chiropractic is a very effective treatment for back pain, but what many patients don�t realize is that they can stretch to make it even better. By employing simple stretches, a chiropractic patient can improve his or her range of motion and increase flexibility. These are some great stretches that you can do at just about any fitness level.
Stretch
Knee To Chest
Lie on a firm, flat surface for this exercise. You can place a mat or towel underneath you to make it a little more comfortable. If you aren�t able to flatten your back right away, fold a small towel and place it under the small of your back to provide a little support.
Lie on your back, knees bent so that your feet are flat on the floor.
Press your lower back into the floor.
While keeping your left foot on the floor, inhale, bringing your right knee to your chest, pulling gently just until you feel a stretch. Hold it for 20 to 30 seconds. You can also keep your left leg straight if that is more comfortable. Make sure you keep your back pressed to the floor.
Exhale, releasing your right knee and return to the starting position.
Repeat the movement with the left leg.
Repeat this stretch 3 to 5 times with each leg.
Child�s Pose
This gives you a very nice stretch all through your back. If you are unable to get on your knees or if you can�t sit on your knees, you can do this while standing.
Hold onto the back of a chair and bend forward. Don�t pull and don�t rest put all of your weight on the chair, just let your body fall gently forward with your neck relaxed and your head drooping. Take baby steps backward until you feel a good stretch, then hold it while breathing normally for 20 to 30 seconds. Walk your feet back in a bit to keep your balance and stand. Repeat 4 or 5 times.
Get on your hands and knees, keeping your knees a little wider than your hips. Turn your toes inward so that they touch.
Bend your knees, pushing your hips back over your heels. Get to a comfortable sitting position.
Slowly slide your arms out in front of you, rounding out your back as you exhale. Keep your neck relaxed so that your head falls forward. Allow yourself to feel the stretch throughout your back.
Hold for 20 to 30 seconds then return to the sitting position.
Repeat the movement 4 or 5 times, keeping your movements slow, fluid, and deliberate.
Cat � Camel
If you can�t get on your knees, stand in front of a chair and place your hands on the seat. Position your feet about where your knees would be if you were on your hands and knees. Relax your neck, allowing your head to droop. Complete steps 2 through 5.
Get on your hands and knees, back straight, your hands shoulder width apart, and your knees slightly apart. Relax your neck so that your head droops. Breathe normally.
Exhale as you round your back up toward the ceiling. Press until you feel a good stretch all along your back. Hold for about 20 to 30 seconds.
Return to the starting position, keeping your back straight.
Inhale as you sway your back, pushing your stomach toward the floor. Tilt your pelvis to get a maximum stretch. Hold for 20 to 30 seconds.
Patellofemoral Syndrome: As the weather warms and spring is in full swing, more and more runners are heading outside, hitting the pavement to train for upcoming races or to just step up their game after a long winter. While there are some die hard runners who don�t let even the most brutal winter stop them, most tend to retreat indoors, waiting for warmer days and a more pleasant environment. Unfortunately, increased activity can also lead to an increased risk of injury, particularly patellofemoral pain syndrome (PFPS), also known as runner�s knee.
What Is Patellofemoral Pain Syndrome?
Runner�s knee is often used to describe PFPS, but runner�s knee is actually a broader term describing several different knee injuries or ailments. PFPS is a painful condition that is caused when the tissue that is between the femur (thigh bone) and the patella (kneecap) becomes inflamed or irritated.
Most people will notice pain in the front portion or anterior part of the knee, but pain can be experienced in other parts of the knee and even back pain may occur. Running increases the discomfort, as does sitting for long periods and going up or down stairs.
The causes of PFPS can also vary widely. Overuse is often the first thing that people think, but a problem with the way the knee is aligned is actually the most common reason.
If the patella is not properly aligned, when it moves through the groove that is at the end of the femur, it causes irritation to the surrounding tissues. This usually happens because the muscles and joints are out of balance.
For instance, if the quad muscle on one side is weaker than the other side it throws the entire system out of balance, causing the knee to become misaligned. This leads to knee pain and discomfort.
Treatment For Patellofemoral Syndrome – Runner�s Knee
When treating PFPS, rest is usually first on the list, followed by icing the area to reduce inflammation. Once the pain is under control, the next step is to determine what is causing the problem. It is important to rule out more serious conditions or injuries first in order to determine the best course of treatment.
If it is indeed PFPS, strengthening the muscles in and around the knee is generally the first step in treatment. It is important that the muscle strength is balanced so that the knee can be properly aligned. Getting a good pair of running shoes is also recommended so that future injury can be prevented.
Chiropractic For Runner�s Knee
Runner�s knee, or PFPS, responds very well to chiropractic treatment. The chiropractor is able to do a complete exam and find the cause of the problem, then tailor the treatment accordingly. This is typically done on a case by case basis with treatment that is based on the individual�s unique needs. The chiropractor may do various chiropractic alignments and manipulations on the spine, hip, ankle, and knee in order to bring the body back into proper balance.
The chiropractor may also recommend other complimentary treatments including special supplements, dietary adjustments, and an exercise plan. The chiropractor may also recommend certain stretching exercises to aid in healing. Kinesio taping is another common treatment that may be used in conjunction with chiropractic care. It is particularly beneficial when there is a muscular strength imbalance. The tape can help support the weaker muscle group.
Chiropractic care is a very effective treatment for patellofemoral syndrome and the associated knee pain. It works to correct the problem by bringing the body back into proper alignment, allowing it to function as it should.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine