Kapit, Wynn, and Lawrence M. Elson. The Anatomy Coloring Book. New York: HarperCollins, 1993.
Hip Anatomy, Function, and Common Problems. (Last updated 28July2010). Retrieved from http://healthpages.org/anatomy-function/hip-structure-function-common-problems/
Cluett, J. M.D. (Updated 22May2012). Labral Tear of the Hip Joint. Retrieved from http://orthopedics.about.com/od/hipinjuries/qt/labrum.htm
Hughes, M. D.C. (15July2010). Diseases of the Femur Bone. Retrieved from http://www.livestrong.com/article/175599-diseases-of-the-femur-bone/
A Patient�s Guide to Perthes Disease of the hip. (n.d.). Retrieved from http://www.orthopediatrics.com/docs/Guides/perthes.html
Hip Injuries and Disorders. (Last reviewed 10February2012). Retrieved from http://nlm.nih.gov/medlineplus/hipinjuriesanddisorders.html
Ligament of head of femur. (Updated 20December2011). Retrieved from http://en.wikipedia.org/wiki/Ligament_of_head_of_femur
Ewing�s sarcoma. (Last modified 06January2012). Retrieved from http://en.wikipedia.org/wiki/Ewing%27s_sarcoma
Hip Anatomy. (n.d.). Retrieved from http://www.activemotionphysio.ca/Injuries-Conditions/Hip
Iliotibial Band Friction Syndrome. (n.d.). Retrieved from http://www.physiotherapy-treatment.com/iliotibial-band-friction-syndrome.html
Snapping hip syndrome. (Last modified 09November2011). Retrieved from http://en.wikipedia.org/wiki/Snapping_hip_syndrome
Sekul, E. (Updated 03February2012). Meralgia Paresthetica. Retrieved from http://emedicine.medscape.com/article/1141848-overview
Yeomans, S. D.C. (Updated 07July2010). Sciatic Nerve and Sciatica. Retrieved from http://www.spine-health.com/conditions/sciatica/sciatic-nerve-and-sciatica
Mayo Clinic staff. (26July2011). Meralgia paresthetica. Retrieved from http://www.mayoclinic.com/health/meralgia-paresthetica/DS00914
Deep Vein Thrombosis (DVT)-Blood Clots in the Legs. (n.d.). Retrieved from http://catalog/nucleusinc.com/displaymonograph.php?MID=148
Petersilge, C. M.D. (03May2000). Chronic Adult Hip Pain: MR Arthrography of the Hip. Retrieved from http://radiographics.rsna.org/content/20/suppl_1/S43.full
Acetabular branch of medial circumflex femoral artery. (Last modified 17November2011). Retrieved from http://en.wikipedia.org/wiki/Acetabular_branch_of_medial_circumflex_femoral_artery
Cluett, J. M.D. (Updated 26March2011). Hip Bursitis. Retrieved from http://orthopedics.about.com/cs/hipsurgery/a/hipbursitis.htm
Steinbach, L. M.D., Palmer, W. M.D., Schweitzer, M. M.D. (10June2002). Special Focus Session MR Arthrography. Retrieved from http://radiographics.rsna.org/content/22/5/1223.full
Schueler, S. M.D., Beckett, J.M.D., Gettings, S.M.D. (Last updated 05August2010). Ischial Bursitis/Overview. Retrieved from http://www.freemd.com/ischial-bursitis/overview.htm
Hwang, B., Fredericson, M., Chung, C., Beaulieu, C., Gold, G. (29October2004). MRI Findings of Femoral Diaphyseal Stress Injuries in Athletes. Retrieved from http://www.ajronline.org/content/185/1/166.full.pdf
The Femur (Thigh Bone). (n.d.). Retrieved from http://education.yahoo.com/reference/gray/subjects/subject/59
Norman, W. PhD, DSc. (n.d.). Joints of the Lower Limb. Retrieved from http://home.comcast.net/~wnor/lljoints.htm
Femur. (Last modified 24September2012). Retrieved from http://en.wikipedia.org/wiki/Femur
Wheeless, C. III, M.D. (Last updated 25April2012). Ligaments of Humphrey and Wrisberg. Retrieved from http://wheelessonline.com/ortho/ligaments_of_humphrey_and_wrisberg
Muscle Strains in the Thigh. (Last reviewed August2007). Retrieved from http://orthoinfo.aaos.org/topic.cfm?topic=A00366
Shiel, W. Jr., M.D. (Last reviewed 23July2012). Hamstring Injuries. Retrieved from http://www.medicinenet.com/hamstring_injury/article.htm
Hamstring Muscle Injuries. (Last reviewed July 2009). Retrieved from http://orthoinfo.aaos.org/topic.cfm?topic=a00408
Knee. (Last modified 19September2012). Retrieved from http://en.wikipedia.org/wiki/Knee
DeBerardino, T. M.D. (Updated 30March2012). Quadriceps Injury. Retrieved from http://emedicine.medscape.com/article/91473-overview
Kan, J.H. (n.d.). Osteochondral Abnormalities: Pitfalls, Injuries, and Osteochondritis Dissecans. Retrieved from http://www.arrs.org/shopARRS/products/s11p_sample.pdf
Nerves of the Lower Limb. (Last updated 30March2006). Retrieved from http://download.videohelp.com/vitualis/med/lowrnn.htm
The Adductor Canal. (Last updated 30March2006). Retrieved from http://download.videohelp.com/vitualis/med/addcanal.htm
Nabili, S. M.D. (n.d.). Varicose Veins & Spider Veins. Retrieved from http://www.medicinenet.com/varicose_veins/article.htm
Basic Venous Anatomy. (n.d.). Retrieved from http://vascular-web.com/asp/samples/sample104.asp
Femoral nerve. (Last modified 23September2012). Retrieved from http://en.wikipedia.org/wiki/Femoral_nerve
Peron, S. RDCS. (Last modified 16October2010). Anatomy � Lower Extremity Veins. Retrieved from http://www.vascularultrasound.net/vascular-anatomy/veins/lower-extremity-veins
Medical Multimedia Group, L.L.C. (n.d.). Knee Anatomy. Retrieved from http://www.eorthopod.com/content/knee-anatomy
Knee Joint Anatomy, Function and Problems. (Last updated 06July2010). Retrieved from http://healthpages.org/anatomy-function/knee-joint-structure-function-problems/
Coronary ligament of the knee. (Last modified 09May2010). Retrieved from http://en.wikipedia.org/wiki/Coronary_ligament_of_the_knee
Walker, B. (n.d.). Patellar Tendonitis Treatment � Jumper�s Knee. Retrieved from http://www.thestretchinghandbook.com/archives/patellar-tendonitis.php
Osgood-Schlatter disease. (Last reviewed 12November2010). Retrieved from http://www.ncbi.nlm.nih.gov/pubmedhealth/PMH0002238/
Grelsamer, R. M.D. (n.d.). The Anatomy of the Patella and the Extensor Mechanism. Retrieved from http://kneehippain.com/patient_pain_anatomy.php
Oblique popliteal ligament. (Last modified 24March2012). Retrieved from http://en.wikipedia.org/wiki/Oblique_popliteal_ligament
Shiel, W. Jr., M.D. (Last reviewed 27July2012). Chondromalacia Patella (Patellofemoral Syndrome). Retrieved from http://www.medicinenet.com/patellofemoral_syndrome/article.htm
Knee. (Last modified 19September2012). Retrieved from http://en.wikipedia.org/wiki/Knee
Mosher, T. M.D. (Last updated 11April2011). MRI of Knee Extensor Mechanism Injuries Overview of the Knee Extensor Mechanism. Retrieved from http://emedicine.medscape.com/article/401001-overview
Carroll, J. M.D. (December 2007). Oblique Menisco-meniscal Ligament. Retrieved from http://radsource.us/clinic/0712
DeBerardino, T. M.D. (Last updated 30March2012). Medial Collateral Knee Ligament Injury. Retrieved from http://emedicine.medscape.com/article/89890-overview#a0106
Farr, G. (Last updated 31December2007). Joints and Ligaments of the Lower Limb. Retrieved from http://becomehealthynow.com/article/bodyskeleton/951/
Knee anatomy overview. (02March2008). Retrieved from http://www.kneeguru.co.uk/KNEEnotes/node/741
Dixit, S. M.D., Difiori, J. M.D., Burton, M. M.D., Mines, B. M.D. (15January2007). Management of Patellofemoral Pain Syndrome. Retrieved from http://www.aafp.org/afp/2007/0115/p194.html
Knee Muscles. (Last updated 05September2012). Retrieved from http://www.knee-pain-explained.com/kneemuscles.html
Popliteus muscle. (Last updated 20February2012). Retrieved from http://en.wikipedia.org/wiki/Popliteus_muscle
Kneedoc. (10February2011). Nerves. Retrieved from http://thekneedoc.co.uk/neurovascular/nerves
Wheeless, C. III, M.D. (Last updated 15December2011). Popliteal Artery. Retrieved from http://wheelessonline.com/ortho/popliteal_artery
The Popliteal Artery. (n.d.) Retrieved from http://education.yahoo.com/reference/gray/subjects/subject/159
Knee bursae. (Last updated 09May2012). Retrieved from http://en.wikipedia.org/wiki/Bursae_of_the_knee_joint
Hirji, Z., Hunjun, J., Choudur, H. (02May2011). Imaging of the Bursae. Retrieved from http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3177464/
Kimaya Wellness Limited. (n.d.). Organ>Popliteal Artery. Retrieved from http://kimayahealthcare.com/OrganDetail.aspx?OrganID=103&AboutID=1
Total Vein Care. (Last updated 24February2012). Varicose Vein Anatomy and Function for Patients. Retrieved from http://www.veincare.com/education/
Tibia. (Last updated 01April2012). Retrieved from http://en.wikipedia.org/wiki/Tibia
Norkus,S., Floyd, R. (Published 2001). The Anatomy and Mechanisms of Syndesmotic Ankle Sprains. Retrieved from http://www.ncbi.nlm.nih.gov/pmc/articles/PMC155405/
Soleus muscle. (Last updated 10April2012). Retrieved from http://en.wikipedia.org/wiki/Soleus_muscle
Achilles Tendinitis. (Last reviewed June2010). Retrieved from http://orthoinfo.aaos.org/topic.cfm?topic=A00147
Wheeless, C. III,M.D. (Last updated 11April2012). Sural Nerve. Retrieved from http://wheelessonline.com/ortho/sural_nerve
Medical Multimedia Group, L.L.C. (Last updated 26July2006). Ankle Syndesmosis Injuries. Retrieved from http://www.orthogate.org/patient-education/ankle/ankle-syndesmosis-injuries.html
Cluett, J. M.D. (Last updated 16September2008). Exertional Compartment Syndrome. Retrieved from http://orthopedics.about.com/od/overuseinjuries/a/compartment.htm
Leg Veins (Thigh, Lower Leg) Anatomy, Pictures and Names. (Last updated 21November2010). Retrieved from http://www.healthype.com/leg-veins-thigh-lower-leg-anatomy-pictures-and-names.html
Cluett, J.M.D. (Last updated 6October2009). Stress Fracture. Retrieved from http://orthopedics.about.com/cs/otherfractures/a/stressfracture.htm
Ostlere, S. (1December2004). Imaging the ankle and foot. Retrieved from http://imaging.birjournals.org/content/15/4/242.full
Inverarity, L. D.O. (Last updated 23January2008). Ligaments of the Ankle Joint. Retrieved from http://physicaltherapy.about.com/od/humananatomy/p/ankleligaments.htm
Golano, P., Vega, J., DeLeeuw, P., Malagelada, F.,Manzanares, M., Gotzens, V., van Dijk, C. (Published online 23March2010). Anatomy of the ankle ligaments:a pictorial essay. Retrieved from http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2855022/
Numkarunarunrote, N., Malik, A., Aguiar, R.,Trudell, D., Resnick, D. (11October2006). Retinacula of the Foot and Ankle: MRI with Anatomic Correlation in Cadavers. Retrieved from http://www.ajronline.org/content/188/4/W348.full
Medical Multimedia Group, L.L.C. (n.d.). A Patient�s Guide to Ankle Anatomy. Retrieved from http://www.eorthopod.com/content/ankle-anatomy
The Anterior Tibial Artery. (n.d.). Retrieved from http://education.yahoo.com/reference/gray/subjects/subject/160
Foot and Ankle Anatomy. (Last updated 28July2011). Retrieved from http://northcoastfootcare.com/pages/Foot-and-Ankle-Anatomy.html
Donnelly, L., Betts, J., Fricke, B. (1July2009). Skimboarder�s Toe: Findings on High-Field MRI. Retrieved from http://www.ajronline.org/content/184/5/1481.full
Foot. (Last updated 28August2012). Retrieved from http://en.wikipedia.org/wiki/Foot
Wiley, C. (n.d.). Major Ligaments in the Foot. Retrieved from http://www.ehow.com/list_6601926_major-ligaments-foot.html
Turf Toe: Symptoms, Causes, and Treatments. (Last reviewed 9August2012). Retrieved from http://www.webmd.com/fitness-exercise/turf-toe-symptoms-causes-and-treatments
Cluett, J. M.D. (Last updated 02April2012). Turf Toe. Retrieved from http://orthopedics.about.com/od/toeproblems/p/turftoe.htm
Neurology and the Feet. (n.d.) Retrieved from http://footdoc.ca/www.FootDoc.ca/Website%20Nerves%20Of%20The%20Feet.htm
The Veins of the Lower Extremity, Abdomen, and Pelvis. (n.d.). Retrieved from http://education.yahoo.com/reference/gray/subjects/subject/173
Corley, G., Broderick, B., Nestor, S., Breen, P., Grace, P., Quondamatteo, F., O�Laighin, G. (n.d.). The Anatomy and Physiology of the Venous Foot Pump. Retrieved from http://www.eee.nuigalway.ie/documents/go_anatomy_of_the_plantar_venous_plexus_manuscript.pdf
Morton�s neuroma. (Last modified 8August2012). Retrieved from http://en.wikipedia.org/wiki/Morton%27s_metatarsalgia








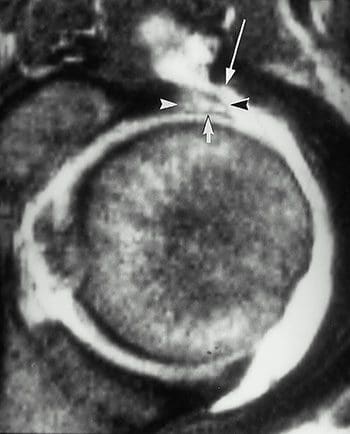
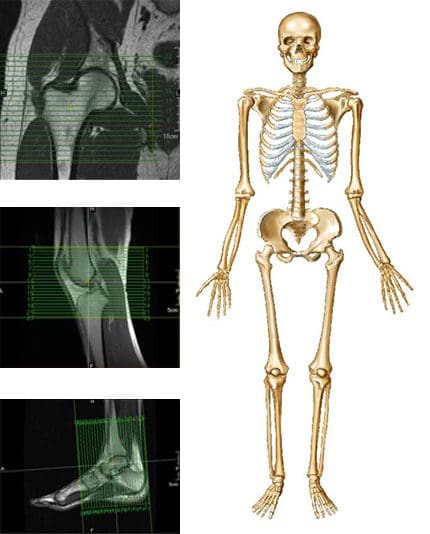 MRI may be requested for:
MRI may be requested for:




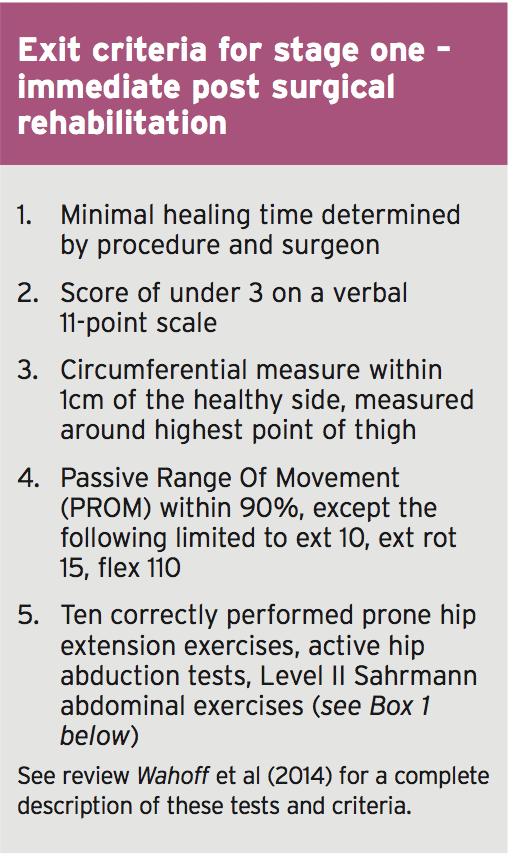
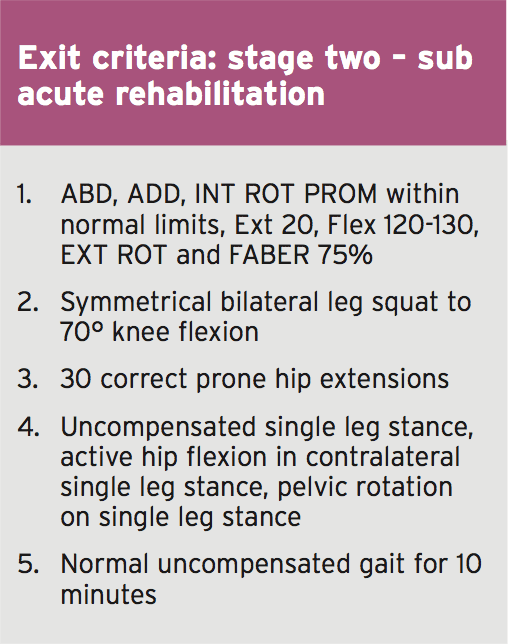
 So as to advance through the six clarified stages, the athlete may undergo extensive physiotherapy, focusing on hip range of movement exercises, manual therapy and trigger point releases, active stretching, potentially deloaded activities like hydrotherapy or Alta G walking/ running and strong hip rotator and gluteal strengthening exercises. Much of this will be ‘controlled’ and led by the wishes of the surgeon as they will provide the framework on if and what happens concerning loading.
So as to advance through the six clarified stages, the athlete may undergo extensive physiotherapy, focusing on hip range of movement exercises, manual therapy and trigger point releases, active stretching, potentially deloaded activities like hydrotherapy or Alta G walking/ running and strong hip rotator and gluteal strengthening exercises. Much of this will be ‘controlled’ and led by the wishes of the surgeon as they will provide the framework on if and what happens concerning loading. Hip Muscle Control
Hip Muscle Control
 Summary
Summary





