Can understanding the body’s hinge joints and how they operate help with mobility and flexibility problems and manage conditions for individuals with difficulty fully bending or extending their fingers, toes, elbows, ankles, or knees?
Hinge Joints
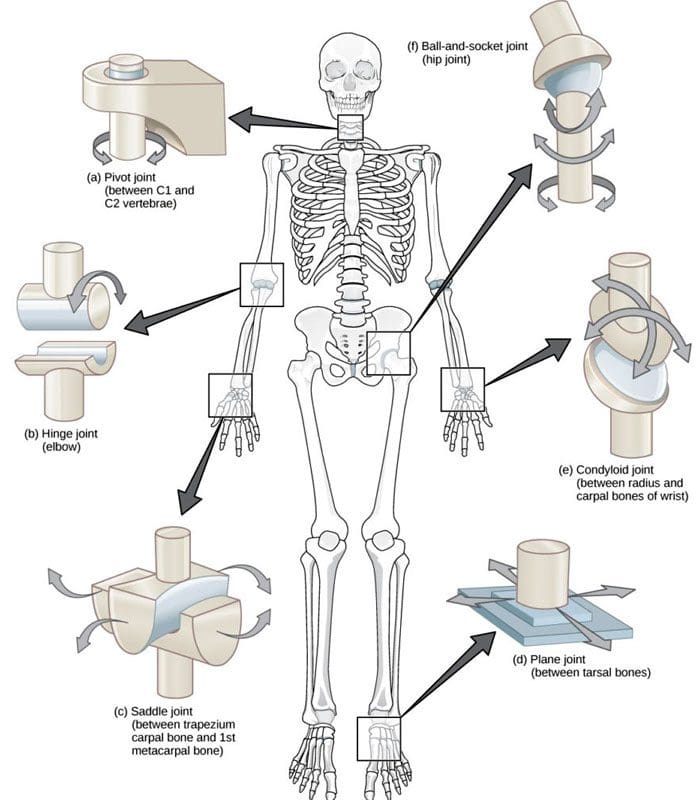
A joint forms where one bone connects to another, allowing motion. Different types of joints differ in structure and movement depending on their location. These include hinge, ball and socket, planar, pivot, saddle, and ellipsoid joints. (Boundless. General Biology, N.D.) Hinge joints are synovial joints that move through one plane of motion: flexion and extension. Hinge joints are found in the fingers, elbows, knees, ankles, and toes and control movement for various functions. Injuries, osteoarthritis, and autoimmune conditions can affect hinge joints. Rest, medication, ice, and physical therapy can help alleviate pain, improve strength and range of motion, and help manage conditions.
Anatomy
A joint is formed by the joining of two or more bones. The human body has three main classifications of joints, categorized by the degree to which they can move. These include: (Boundless. General Biology, N.D.)
Synarthroses
These are fixed, immovable joints.
Formed by two or more bones.
Amphiarthroses
Also known as cartilaginous joints.
A fibrocartilage disc separates the bones that form the joints.
These movable joints allow for a slight degree of movement.
Diarthroses
Also known as synovial joints.
These are the most common freely mobile joints that allow movement in multiple directions.
The bones that form the joints are lined with articular cartilage and enclosed in a joint capsule filled with synovial fluid that allows for smooth motion.
Synovial joints are classified into different types depending on differences in structure and the number of motion planes they allow. A hinge joint is a synovial joint that allows movement in one plane of motion, similar to a door hinge that moves forward and backward. Within the joint, the end of one bone is typically convex/pointed outward, with the other concave/rounded inward to allow the ends to fit smoothly. Because hinge joints only move through one plane of movement, they tend to be more stable than other synovial joints. (Boundless. General Biology, N.D.) Hinge joints include:
The finger and toe joints – allow the fingers and toes to bend and extend.
The elbow joint – allows the elbow to bend and extend.
The knee joint – allows the knee to bend and extend.
The talocrural joint of the ankle – allows the ankle to move up/dorsiflexion and down/plantarflexion.
Hinge joints allow the limbs, fingers, and toes to extend away and bend toward the body. This movement is essential for activities of daily living, such as showering, getting dressed, eating, walking, standing up, and sitting down.
Conditions
Osteoarthritis and inflammatory forms of arthritis can affect any joint (Arthritis Foundation. N.D.) Autoimmune inflammatory forms of arthritis, including rheumatoid and psoriatic arthritis, can cause the body to attack its own joints. These commonly affect the knees and fingers, resulting in swelling, stiffness, and pain. (Kamata, M., Tada, Y. 2020) Gout is an inflammatory form of arthritis that develops from elevated levels of uric acid in the blood and most commonly affects the hinge joint of the big toe. Other conditions that affect hinge joints include:
Injuries to the cartilage within the joints or ligaments that stabilize the outside of the joints.
Ligament sprains or tears can result from jammed fingers or toes, rolled ankles, twisting injuries, and direct impact on the knee.
These injuries can also affect the meniscus, the tough cartilage within the knee joint that helps cushion and absorb shock.
Rehabilitation
Conditions that affect hinge joints often cause inflammation and swelling, resulting in pain and limited mobility.
After an injury or during an inflammatory condition flare-up, limiting active movement and resting the affected joint can reduce increased stress and pain.
Applying ice can decrease inflammation and swelling.
Once the pain and swelling start to subside, physical and/or occupational therapy can help rehabilitate the affected areas.
A therapist will provide stretches and exercises to help improve the joint range of motion and strengthen the supporting muscles.
For individuals experiencing hinge joint pain from an autoimmune condition, biologic medications to decrease the body’s autoimmune activity are administered through infusions delivered every several weeks or months. (Kamata, M., Tada, Y. 2020)
Cortisone injections may also be used to decrease inflammation.
At Injury Medical Chiropractic and Functional Medicine Clinic, we passionately focus on treating patients’ injuries and chronic pain syndromes and improving ability through flexibility, mobility, and agility programs tailored to the individual. Our providers use an integrated approach to create personalized care plans that include Functional Medicine, Acupuncture, Electro-Acupuncture, and Sports Medicine protocols. Our goal is to relieve pain naturally by restoring health and function to the body. If the individual needs other treatment, they will be referred to a clinic or physician best suited for them. Dr. Jimenez has teamed up with the top surgeons, clinical specialists, medical researchers, and premier rehabilitation providers to provide the most effective clinical treatments.
Kamata, M., & Tada, Y. (2020). Efficacy and Safety of Biologics for Psoriasis and Psoriatic Arthritis and Their Impact on Comorbidities: A Literature Review. International journal of molecular sciences, 21(5), 1690. doi.org/10.3390/ijms21051690
What are the healing times of common sports injuries for athletes and individuals who engage in recreational sports activities?
A young, happy sportswoman is getting tens-electrotherapy treatments at a medical clinic.
Healing Times for Sports Injuries
Healing time from sports injuries depends on various factors, such as the location and extent of the injury and the health of the skin, joints, tendons, muscles, and bones. It is also important to take the time to recuperate or not rush back into physical sports activities before the bones or tissues have fully healed. To prevent re-injury, ensure the doctor clears health before returning to sports or strenuous physical activity.
According to CDC research, an average of 8.6 million sports and recreation-related injuries occur annually. (Sheu, Y., Chen, L. H., and Hedegaard, H. 2016) However, most sports injuries are superficial or caused by low-grade strains or sprains; at least 20% of injuries result from bone fractures or more serious injuries. Bone fractures take longer than sprains or strains, and complete tendon or muscle ruptures can take months before one can fully return to activities. Individuals in decent physical shape with no underlying illness or impairment, here is what they can expect when recovering from the following sports injuries:
Bone Fractures
In sports, the highest rate of bone fractures occurs with football and contact sports. Most are centered around the lower extremities but can involve the neck and shoulder blades, arms, and ribs.
Simple Fractures
Depends on the individual’s age, health, type, and location.
Generally, takes at least six weeks to heal.
Compound Fractures
In this case, a bone is broken in several places.
It may require surgery to stabilize the bone.
Healing time can take up to eight months.
Fractured Clavicle/Collarbone
It may require the immobilization of the shoulder and upper arm.
It can take five to ten weeks to heal fully.
Fractured fingers or toes can heal in three to five weeks.
Fractured Ribs
Part of the treatment plan includes breathing exercises.
Painkillers may be needed short term.
Usually, it takes around six weeks to heal.
Neck Fractures
It may involve any one of the seven neck vertebrae.
A neck brace or a halo device that is screwed into the skull for stability may be used.
A sprain is the stretching or tearing of ligaments or the tough bands of fibrous tissue that connect two bones at a joint.
A strain is the overstretching or tearing of muscles or tendons.
Sprained Ankles
It can heal in five days if there are no complications.
Severe sprains involving torn or ruptured tendons can take three to six weeks to heal.
Calf Strains
Classified as grade 1 – a mild strain can heal in two weeks.
A grade 3 – severe strain may require three months or more to heal completely.
The use of calf suppression sleeves can expedite the recovery of strains and sprains in the lower leg.
Acute Neck Strain
A tackle, impact, fall, quick shifting, or whipping motion can cause a whiplash injury.
Healing time can take a couple of weeks to six weeks.
Other Injuries
ACL Tears
Involving the anterior cruciate ligament.
Usually, it requires months of recuperation and rehabilitation, depending on several factors, including the type of sports activity.
Full recovery from surgery takes six to 12 months.
Without surgery, there is no specific timeline for rehabilitation.
Achilles Tendon Ruptures
It is a serious injury.
These occur when the tendon is either partially or completely torn.
Individuals will more than likely require surgery.
Recovery time is four to six months.
Cuts and Lacerations
Depends on the depth and location of the injury.
It can take anywhere from a week to a month to heal.
If there are no accompanying injuries, stitches can be removed within two to three weeks.
If a deep cut requires stitches, more time is necessary.
Mild Contusions/Bruises
Are caused by a trauma to the skin, causing blood vessels to break.
In most cases, a contusion will take five to seven days to heal.
Shoulder Separations
When treated properly, it usually takes around two weeks of rest and recovery before the patient returns to activity.
Multidisciplinary Treatment
After the initial inflammation and swelling have subsided, a doctor will recommend a treatment plan that usually involves physical therapy, self-performed physical rehabilitation, or supervision by a physical therapist or team. Fortunately, athletes and individuals who regularly exercise tend to have a faster healing time because they are in top physical shape, and their cardiovascular system provides a stronger blood supply that speeds up the healing process. At El Paso’s Chiropractic Rehabilitation Clinic & Integrated Medicine Center, we passionately focus on treating patients’ injuries and chronic pain syndromes. We focus on improving ability through flexibility, mobility, and agility programs tailored to the individual. We use in-person and virtual health coaching and comprehensive care plans to ensure every patient’s personalized care and wellness outcomes.
Our providers use an integrated approach to create personalized care plans that include Functional Medicine, Acupuncture, Electro-Acupuncture, and Sports Medicine principles. Our goal is to relieve pain naturally by restoring health and function to the body.
If the chiropractor feels the individual needs other treatment, they will be referred to a clinic or physician best suited for them. Dr. Jimenez has teamed up with the top surgeons, clinical specialists, medical researchers, and premier rehabilitation providers to provide the top clinical treatments for our community. Providing highly noninvasive protocols is our priority, and our personalized patient-based clinical insight is what we provide.
Lumbar Spine Injuries in Sports: Chiropractic Healing
References
Sheu, Y., Chen, L. H., & Hedegaard, H. (2016). Sports- and Recreation-related Injury Episodes in the United States, 2011-2014. National health statistics reports, (99), 1–12.
For individuals experiencing pelvic pain, it could be a disorder of the pudendal nerve known as pudendal neuropathy or neuralgia that leads to chronic pain. The condition can be caused by pudendal nerve entrapment, where the nerve becomes compressed or damaged. Can knowing the symptoms help healthcare providers correctly diagnose the condition and develop an effective treatment plan?
Pudendal Neuropathy
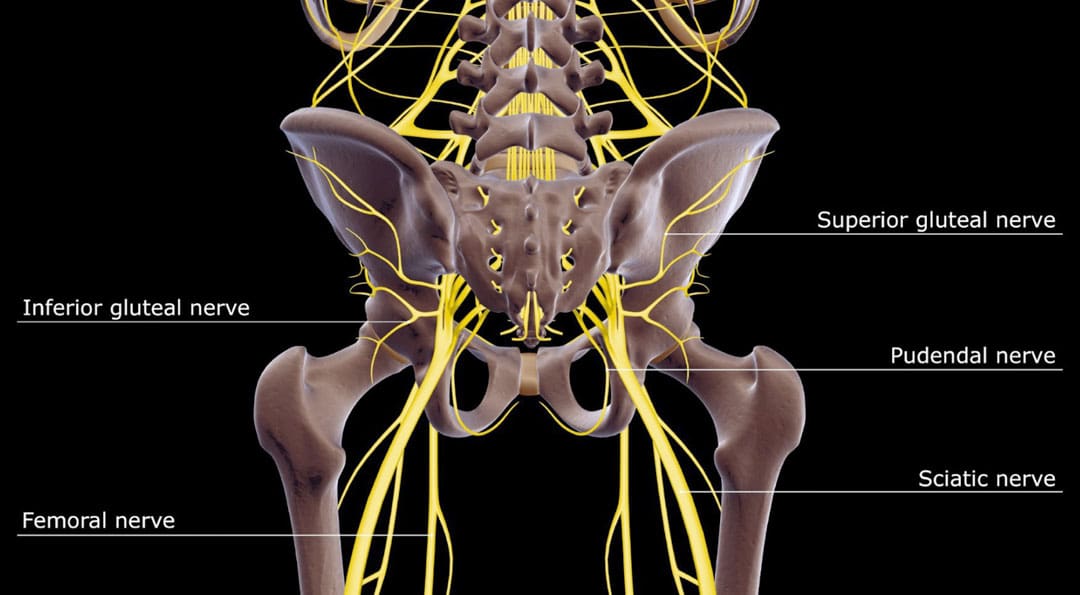
The pudendal nerve is the main nerve that serves the perineum, which is the area between the anus and the genitalia – the scrotum in men and the vulva in women. The pudendal nerve runs through the gluteus muscles/buttocks and into the perineum. It carries sensory information from the external genitalia and the skin around the anus and perineum and transmits motor/movement signals to various pelvic muscles. (Origoni, M. et al., 2014) Pudendal neuralgia, also referred to as pudendal neuropathy, is a disorder of the pudendal nerve that can lead to chronic pelvic pain.
Causes
Chronic pelvic pain from pudendal neuropathy can be caused by any of the following (Kaur J. et al., 2024)
Excessive sitting on hard surfaces, chairs, bicycle seats, etc. Bicyclists tend to develop pudendal nerve entrapment.
Trauma to the buttocks or pelvis.
Childbirth.
Diabetic neuropathy.
Bony formations that push against the pudendal nerve.
Thickening of ligaments around the pudendal nerve.
Symptoms
Pudendal nerve pain can be described as stabbing, cramping, burning, numbness, or pins and needles and can present (Kaur J. et al., 2024)
In the perineum.
In the anal region.
In men, pain in the scrotum or penis.
In women, pain in the labia or vulva.
During intercourse.
When urinating.
During a bowel movement.
When sitting and goes away after standing up.
Because the symptoms are often hard to distinguish, pudendal neuropathy can often be hard to differentiate from other types of chronic pelvic pain.
Cyclist’s Syndrome
Prolonged sitting on a bicycle seat can cause pelvic nerve compression, which can lead to chronic pelvic pain. The frequency of pudendal neuropathy (chronic pelvic pain caused by entrapment or compression of the pudendal nerve) is often referred to as Cyclist’s Syndrome. Sitting on certain bicycle seats for long periods places significant pressure on the pudendal nerve. The pressure can cause swelling around the nerve, which causes pain and, over time, can lead to nerve trauma. Nerve compression and swelling can cause pain described as burning, stinging, or pins and needles. (Durante, J. A., and Macintyre, I. G. 2010) For individuals with pudendal neuropathy caused by bicycling, symptoms can appear after prolonged biking and sometimes months or years later.
Take breaks at least 20–30 seconds after each 20 minutes of riding.
While riding, change positions frequently.
Stand up to pedal periodically.
Take time off between riding sessions and races to rest and relax the pelvic nerves. 3–10 day breaks can help in recovery. (Durante, J. A., and Macintyre, I. G. 2010)
If pelvic pain symptoms are barely starting to develop, rest and see a healthcare provider or specialist for an examination.
Seat
Use a soft, wide seat with a short nose.
Have the seat level or tilted slightly forward.
Seats with cutout holes place more pressure on the perineum.
If numbness or pain is present, try a seat without holes.
Bike Fitting
Adjust the seat height so the knee is slightly bent at the bottom of the pedal stroke.
The body’s weight should rest on the sitting bones/ischial tuberosities.
Keeping the handlebar height below the seat can reduce pressure.
The Triathlon bike’s extreme-forward position should be avoided.
A more upright posture is better.
Mountain bikes have been associated with an increased risk of erectile dysfunction than road bikes.
Shorts
Wear padded bike shorts.
Treatments
A healthcare provider may use a combination of treatments.
The neuropathy can be treated with rest if the cause is excessive sitting or cycling.
Injury Medical Chiropractic and Functional Medicine Clinic care plans and clinical services are specialized and focused on injuries and the complete recovery process. Our areas of practice include Wellness and nutrition, Chronic Pain, Personal Injury, Auto Accident Care, Work Injuries, Back Injury, Low Back Pain, Neck Pain, Migraine Headaches, Sports Injuries, severe sciatica, Scoliosis, Complex Herniated Discs, Fibromyalgia, Chronic Pain, Complex Injuries, Stress Management, and Functional Medicine Treatments. If the individual requires other treatment, they will be referred to a clinic or physician best suited for their condition, as Dr. Jimenez has teamed with the top surgeons, clinical specialists, medical researchers, therapists, trainers, and premiere rehabilitation providers.
Pregnancy and Sciatica
References
Origoni, M., Leone Roberti Maggiore, U., Salvatore, S., & Candiani, M. (2014). Neurobiological mechanisms of pelvic pain. BioMed research international, 2014, 903848. doi.org/10.1155/2014/903848
Durante, J. A., & Macintyre, I. G. (2010). Pudendal nerve entrapment in an Ironman athlete: a case report. The Journal of the Canadian Chiropractic Association, 54(4), 276–281.
Chiaramonte, R., Pavone, P., & Vecchio, M. (2021). Diagnosis, Rehabilitation and Preventive Strategies for Pudendal Neuropathy in Cyclists, A Systematic Review. Journal of functional morphology and kinesiology, 6(2), 42. doi.org/10.3390/jfmk6020042
For individuals who have exhausted all other treatment options for low back pain and nerve root compression, can laser spine surgery help alleviate nerve compression and provide long-lasting pain relief?
Laser Spine Surgery
Laser spine surgery is a minimally invasive surgical procedure that uses a laser to cut through and remove spinal structures that are compressing nerves and causing intense pain. The minimally invasive procedure often results in less pain, tissue damage, and faster recovery than more extensive surgeries.
How It Works
Minimally invasive procedures result in less scarring and damage to surrounding structures, often reducing pain symptoms and a shorter recovery time. (Stern, J. 2009) Small incisions are made to access spinal column structures. With open-back surgery, a large incision is made down the back to access the spine. The surgery differs from other surgeries in that a laser beam, rather than other surgical instruments, is used to cut structures in the spine. However, the initial incision through the skin is made with a surgical scalpel. Laser is an acronym for Light Amplification Stimulated by Emission of Radiation. A laser can generate intense heat to cut through soft tissues, especially those with a high water content, like spinal column discs. (Stern, J. 2009) For many spine surgeries, the laser cannot be used to cut through bone as it generates instant sparks that can damage surrounding structures. Rather, laser spine surgery is primarily used to perform a discectomy, which is a surgical technique that removes a portion of a bulging or herniated disc that is pushing against the surrounding nerve roots, causing nerve compression and sciatic pain. (Stern, J. 2009)
Surgical Risks
Laser spine surgery may help resolve the cause of nerve root compression, but there is an increased risk of damage to nearby structures. Associated risks include: (Brouwer, P. A. et al., 2015)
Infection
Bleeding
Blood clots
Remaining symptoms
Returning symptoms
Further nerve damage
Damage to the membrane around the spinal cord.
Need for additional surgery
A laser beam is not precise like other surgical tools and requires practiced mastery and control to avoid damage to the spinal cord and nerve roots. (Stern, J. 2009) Because lasers cannot cut through bone, other surgical instruments are often used around corners and at different angles because they are more efficient and allow greater accuracy. (Atlantic Brain and Spine, 2022)
Purpose
Laser spine surgery is performed to remove structures that are causing nerve root compression. Nerve root compression is associated with the following conditions (Cleveland Clinic. 2018)
Bulging discs
Herniated discs
Sciatica
Spinal stenosis
Spinal cord tumors
Nerve roots that are injured or damaged and constantly send chronic pain signals can be ablated with laser surgery, known as nerve ablation. The laser burns and destroys the nerve fibers. (Stern, J. 2009) Because laser spine surgery is limited in treating certain spinal disorders, most minimally invasive spine procedures do not use a laser. (Atlantic Brain and Spine. 2022)
Preparation
The surgical team will provide more detailed instructions on what to do in the days and hours before surgery. To promote optimal healing and a smooth recovery, it is recommended that the patient stay active, eat a healthy diet, and stop smoking prior to the operation. Individuals may need to stop taking certain medications to prevent excess bleeding or interaction with anesthesia during the operation. Inform the healthcare provider about all prescriptions, over-the-counter drugs, and supplements being taken.
Laser spine surgery is an outpatient procedure at a hospital or outpatient surgical center. The patient will likely go home on the same day of the operation. (Cleveland Clinic. 2018) Patients cannot drive to or from the hospital before or after their surgery, so arrange for family or friends to provide transportation. Minimizing stress and prioritizing healthy mental and emotional well-being is important to lowering inflammation and aiding recovery. The healthier the patient goes into surgery, the easier the recovery and rehabilitation will be.
Expectations
The surgery will be decided by the patient and healthcare provider and scheduled at a hospital or outpatient surgical center. Arrange for a friend or family member to drive to the surgery and home.
Before Surgery
The patient will be taken to a pre-operative room and asked to change into a gown.
The patient will undergo a brief physical examination and answer questions about medical history.
The patient lies on a hospital bed, and a nurse inserts an IV to deliver medication and fluids.
The surgical team will use the hospital bed to transport the patient in and out of the operating room.
The surgical team will assist the patient in getting onto the operating table, and the patient will be administered anesthesia.
The patient may receive general anesthesia, which will cause the patient to sleep for the surgery, or regional anesthesia, injected into the spine to numb the affected area. (Cleveland Clinic. 2018)
The surgical team will sterilize the skin where the incision will be made.
An antiseptic solution will be used to kill bacteria and prevent the risk of infection.
Once sanitized, the body will be covered with sterilized linens to keep the surgical site clean.
During Surgery
For a discectomy, the surgeon will make a small incision less than one inch in length with a scalpel along the spine to access the nerve roots.
A surgical tool called an endoscope is a camera inserted into the incision to view the spine. (Brouwer, P. A. et al., 2015)
Once the problematic disc portion causing the compression is located, the laser is inserted to cut through it.
The cut disc portion is removed, and the incision site is sutured.
After Surgery
After surgery, the patient is brought to a recovery room, where vital signs are monitored as the effects of the anesthesia wear off.
Once stabilized, the patient can usually go home one or two hours after the operation.
The surgeon will determine when the individual is clear to resume driving.
Recovery
Following a discectomy, the individual can return to work within a few days to a few weeks, depending on the severity, but it can take up to three months to return to normal activities. Length of recovery can range from two to four weeks or less to resume a sedentary job or eight to 12 weeks for a more physically demanding job that requires heavy lifting. (University of Wisconsin School of Medicine and Public Health, 2021) During the first two weeks, the patient will be given restrictions to facilitate the spine’s healing until it becomes more stable. Restrictions can include: (University of Wisconsin School of Medicine and Public Health, 2021)
No bending, twisting, or lifting.
No strenuous physical activity, including exercise, housework, yard work, and sex.
No alcohol in the initial stage of recovery or while taking narcotic pain medications.
No driving or operating a motor vehicle until discussed with the surgeon.
The healthcare provider may recommend physical therapy to relax, strengthen, and maintain musculoskeletal health. Physical therapy may be two to three times weekly for four to six weeks.
Process
Optimal recovery recommendations include:
Getting enough sleep, at least seven to eight hours.
Maintaining a positive attitude and learning how to cope and manage stress.
Maintaining body hydration.
Following the exercise program as prescribed by the physical therapist.
Practicing healthy posture with sitting, standing, walking, and sleeping.
Staying active and limiting the amount of time spent sitting. Try to get up and walk every one to two hours during the day to stay active and prevent blood clots. Gradually increase the amount of time or distance as recovery progresses.
Do not push to do too much too soon. Overexertion can increase pain and delay recovery.
Learning correct lifting techniques to utilize the core and leg muscles to prevent increased pressure on the spine.
Discuss treatment options for managing symptoms with a healthcare provider or specialist to determine if laser spine surgery is appropriate. Injury Medical Chiropractic and Functional Medicine Clinic care plans and clinical services are specialized and focused on injuries and the complete recovery process. Dr. Jimenez has teamed with the top surgeons, clinical specialists, medical researchers, therapists, trainers, and premiere rehabilitation providers. We focus on restoring normal body functions after trauma and soft tissue injuries using Specialized Chiropractic Protocols, Wellness Programs, Functional and integrative Nutrition, Agility and mobility Fitness Training, and Rehabilitation Systems for all ages. Our areas of practice include Wellness & Nutrition, Chronic Pain, Personal Injury, Auto Accident Care, Work Injuries, Back Injury, Low Back Pain, Neck Pain, Migraine Headaches, Sports Injuries, Severe Sciatica, Scoliosis, Complex Herniated Discs, Fibromyalgia, Chronic Pain, Complex Injuries, Stress Management, Functional Medicine Treatments, and in-scope care protocols.
Brouwer, P. A., Brand, R., van den Akker-van Marle, M. E., Jacobs, W. C., Schenk, B., van den Berg-Huijsmans, A. A., Koes, B. W., van Buchem, M. A., Arts, M. P., & Peul, W. C. (2015). Percutaneous laser disc decompression versus conventional microdiscectomy in sciatica: a randomized controlled trial. The spine journal : official journal of the North American Spine Society, 15(5), 857–865. doi.org/10.1016/j.spinee.2015.01.020
University of Wisconsin School of Medicine and Public Health. (2021). Home Care Instructions after Lumbar Laminectomy, Decompression or Discectomy Surgery. patient.uwhealth.org/healthfacts/4466
Individuals may discover a lump, bump, or nodule under the skin around their lower back, hips, and sacrum that can cause pain by compressing nerves and damaging the fascia. Can knowing the conditions linked to them and their symptoms help healthcare providers determine a correct diagnosis and develop an effective treatment plan for experiencing?
Painful Bumps, Nodules Around Low Back, Hips, and Sacrum
Painful masses in and around the hips, the sacrum, and the lower back are lumps of fat or lipomas, fibrous tissue, or other types of nodules that move when pressed on. Some healthcare providers and chiropractors, in particular, use the non-medical term back mice (In 1937, the term was used to describe lumps associated with episacroiliac lipoma) to describe the bumps. Some healthcare professionals argue against calling the masses mice because it is not specific and could lead to misdiagnoses or incorrect treatment.
Most show up in the lower back and hip area.
In some cases, they protrude or herniate through the lumbodorsal fascia or the network of connective tissue that covers the deep muscles of the lower and middle back.
Other lumps can develop in the tissue under the skin.
Today, many conditions are associated with back mice lumps, including:
Iliac crest pain syndrome
Multifidus triangle syndrome
Lumbar fascial fat herniation
Lumbosacral (sacrum) fat herniation
Episacral lipoma
Related Conditions
Iliac Crest Pain Syndrome
Also known as iliolumbar syndrome, iliac crest pain syndrome develops when a tear in the ligament occurs.
The ligament band connects the fourth and fifth lumbar vertebrae with the ilium on the same side. (Dąbrowski, K. Ciszek, B. 2023)
Causes include:
Tearing the ligament from repeated bending and twisting.
Trauma or fracture of the ilium bone caused by a fall or vehicle collision accident.
Multifidus Triangle Syndrome
Multifidus triangle syndrome develops when the multifidus muscles along the spine weaken and diminish function or ability.
These muscles can atrophy, and intramuscular fatty tissue can replace the muscle.
The lumbodorsal fascia is a thin fibrous membrane covering the back’s deep muscles.
Lumbar fascial fat herniation is a painful mass of fat that protrudes or herniates through the membrane, gets trapped and inflamed, and causes pain.
The causes of this type of herniation are currently unknown.
Lumbosacral (Sacrum) Fat Herniation
Lumbosacral describes where the lumbar spine meets the sacrum.
Lumbosacral fat herniation is a painful mass like lumbar facial herniation in a different location around the sacrum.
The causes of this type of herniation are currently unknown.
Episacral Lipoma
Episacral lipoma is a small painful nodule under the skin that primarily develops over the top outer edges of the pelvic bone. These lumps occur when a portion of the dorsal fat pad protrudes through a tear in the thoracodorsal fascia, the connective tissue that helps hold the back muscles in place. (Erdem, H. R. et al., 2013) A healthcare provider may refer an individual to an orthopedist or orthopedic surgeon for this lipoma. An individual may also find pain relief from a massage therapist familiar with the condition. (Erdem, H. R. et al., 2013)
Symptoms
Back lumps can often be seen under the skin. They are typically tender to the touch and can make sitting in a chair or lying on the back difficult, as they often appear on the hip bones and sacroiliac region. (Bicket, M. C. et al., 2016) The nodules may:
Be firm or tight.
Have an elastic feel.
Move under the skin when pressed.
Cause intense, severe pain.
The pain results from pressure on the lump, which compresses the nerves.
Damage to the underlying fascia can also cause pain symptoms.
Diagnosis
Some individuals do not realize they have nodules or lumps until pressure is applied. Chiropractors and massage therapists often find them during treatments but do not diagnose the abnormal fatty growth. The chiropractor or massage therapist will refer the patient to a qualified dermatologist or medical professional who can perform imaging studies and a biopsy. Determining what the lumps are can be challenging because they are non-specific. Healthcare providers sometimes diagnose the nodules by injecting them with a local anesthetic. (Bicket, M. C. et al., 2016)
Differential Diagnosis
The fatty deposits can be any number of things, and the same applies to the sources of nerve pain. A healthcare provider may further diagnose by ruling out other causes, which can include:
Sebaceous Cysts
A benign, fluid-filled capsule between the layers of skin.
Subcutaneous Abscess
A collection of pus beneath the skin.
Usually painful.
It can become inflamed.
Sciatica
Radiating nerve pain down one or both legs that is caused by a herniated disc, bone spur, or spasming muscles in the lower back.
Liposarcoma
Malignant tumors can sometimes appear as fatty growths in the muscles.
Liposarcoma is typically diagnosed by biopsy, where some tissue is removed from the nodule and examined for cancer cells. (Johns Hopkins Medicine. 2024)
An MRI or CT scan may also be performed to determine the exact location of the nodule.
Painful lipomas are also associated with fibromyalgia.
Treatment
Back nodules are usually benign, so there’s no reason to remove them unless they’re causing pain or mobility problems (American Academy of Orthopedic Surgeons: OrthoInfo. 2023). However, they should be examined to make sure they are not cancerous. Treatment usually involves injected anesthetics, such as lidocaine or corticosteroids, as well as over-the-counter pain relievers like NSAIDs.
Surgery
If pain is severe, surgical removal may be recommended. This involves cutting out the mass and repairing the fascia for lasting relief. However, removal may not be recommended if there are many nodules, as some individuals can have hundreds. Liposuction may be effective if the lumps are smaller, more extensive, and comprise more fluid. (American Family Physician. 2002) Complications of surgical removal can include:
Scarring
Bruising
Uneven skin texture
Infection
Complementary and Alternative Treatment
Complimentary and Alternative Medicine treatments like acupuncture, dry needling, and spinal manipulation can help. Many chiropractors believe back nodules can be successfully treated with complementary and alternative therapies. A common approach uses acupuncture and spinal manipulation in combination. A case study reported that anesthetic injections followed by dry needling, which is similar to acupuncture, improved pain relief. (Bicket, M. C. et al., 2016)
Injury Medical Chiropractic and Functional Medicine Clinic specializes in progressive therapies and functional rehabilitation procedures focused on restoring normal body functions after trauma and soft tissue injuries and the complete recovery process. Our areas of practice include Wellness & Nutrition, Chronic Pain, Personal Injury, Auto Accident Care, Work Injuries, Back Injury, Low Back Pain, Neck Pain, Migraine Headaches, Sports Injuries, Severe Sciatica, Scoliosis, Complex Herniated Discs, Fibromyalgia, Chronic Pain, Complex Injuries, Stress Management, Functional Medicine Treatments, and in-scope care protocols. If the individual requires other treatment, they will be referred to a clinic or physician best suited for their condition, as Dr. Jimenez has teamed with the top surgeons, clinical specialists, medical researchers, therapists, trainers, and premiere rehabilitation providers.
Beyond the Surface
References
Dąbrowski, K., & Ciszek, B. (2023). Anatomy and morphology of iliolumbar ligament. Surgical and radiologic anatomy : SRA, 45(2), 169–173. doi.org/10.1007/s00276-022-03070-y
Seyedhoseinpoor, T., Taghipour, M., Dadgoo, M., Sanjari, M. A., Takamjani, I. E., Kazemnejad, A., Khoshamooz, Y., & Hides, J. (2022). Alteration of lumbar muscle morphology and composition in relation to low back pain: a systematic review and meta-analysis. The spine journal : official journal of the North American Spine Society, 22(4), 660–676. doi.org/10.1016/j.spinee.2021.10.018
Erdem, H. R., Nacır, B., Özeri, Z., & Karagöz, A. (2013). Episakral lipoma: Bel ağrısının tedavi edilebilir bir nedeni [Episacral lipoma: a treatable cause of low back pain]. Agri : Agri (Algoloji) Dernegi’nin Yayin organidir = The journal of the Turkish Society of Algology, 25(2), 83–86. doi.org/10.5505/agri.2013.63626
Bicket, M. C., Simmons, C., & Zheng, Y. (2016). The Best-Laid Plans of “Back Mice” and Men: A Case Report and Literature Review of Episacroiliac Lipoma. Pain physician, 19(3), 181–188.
When sciatica or other radiating nerve pain presents, can learning to distinguish between nerve pain and different types of pain help individuals recognize when spinal nerve roots are irritated or compressed or more serious problems that require medical attention?
Spinal Nerve Roots and Dermatomes
Spinal conditions such as herniated discs and stenosis can lead to radiating pain that travels down one arm or leg. Other symptoms include weakness, numbness, and/or shooting or burning electrical sensations. The medical term for pinched nerve symptoms is radiculopathy (National Institutes of Health: National Institute of Neurological Disorders and Stroke. 2020). Dermatomes could contribute to irritation in the spinal cord, where the nerve roots cause symptoms in the back and limbs.
Anatomy
The spinal cord has 31 segments.
Each segment has nerve roots on the right and left that supply motor and sensory functions to the limbs.
The anterior and posterior communicating branches combine to form the spinal nerves that exit the vertebral canal.
The 31 spine segments result in 31 spinal nerves.
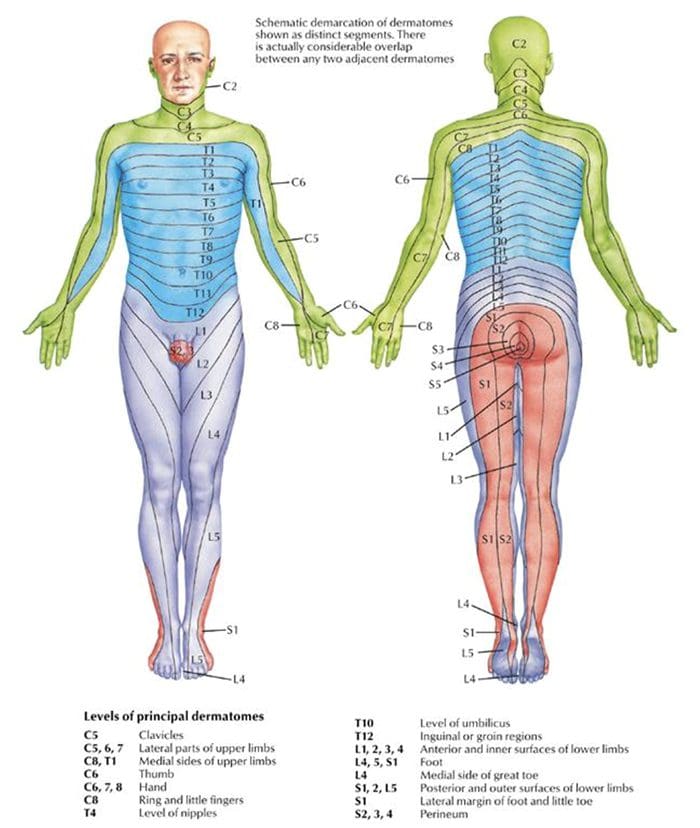
Each one transmits sensory nerve input from a specific skin region on that side and area of the body.
These regions are called dermatomes.
Except for the first cervical spinal nerve, dermatomes exist for each spinal nerve.
The spinal nerves and their associated dermatomes form a network all over the body.
Dermatomes Purpose
Dermatomes are the body/skin areas with sensory input assigned to individual spinal nerves. Each nerve root has an associated dermatome, and various branches supply each dermatome off that single nerve root. Dermatomes are pathways through which sensational information in the skin transmits signals to and from the central nervous system. Sensations that are physically felt, like pressure and temperature, get transmitted to the central nervous system. When a spinal nerve root becomes compressed or irritated, usually because it comes into contact with another structure, it results in radiculopathy. (National Institutes of Health: National Institute of Neurological Disorders and Stroke. 2020).
Radiculopathy
Radiculopathy describes symptoms caused by a pinched nerve along the spine. Symptoms and sensations depend on where the nerve is pinched and the extent of the compression.
Cervical
This is a syndrome of pain and/or sensorimotor deficiencies when nerve roots in the neck are compressed.
It often presents with pain that goes down one arm.
Individuals may also experience electrical sensations like pins and needles, shocks, and burning sensations, as well as motor symptoms like weakness and numbness.
Lumbar
This radiculopathy results from compression, inflammation, or injury to a spinal nerve in the lower back.
Sensations of pain, numbness, tingling, electrical or burning sensations, and motor symptoms like weakness traveling down one leg are common.
Diagnosis
Part of a radiculopathy physical examination is testing the dermatomes for sensation. The practitioner will use specific manual tests to determine the spinal level from which the symptoms originate. Manual exams are often accompanied by diagnostic imaging tests like MRI, which can show abnormalities in the spinal nerve root. A complete physical examination will determine if the spinal nerve root is the source of the symptoms.
Treating Underlying Causes
Many back disorders can be treated with conservative therapies to provide effective pain relief. For a herniated disk, for example, individuals may be recommended to rest and take a nonsteroidal anti-inflammatory medication. Acupuncture, physical therapy, chiropractic, non-surgical traction, or decompression therapies may also be prescribed. For severe pain, individuals may be offered an epidural steroid injection that can provide pain relief by reducing inflammation. (American Academy of Orthopaedic Surgeons: OrthoInfo. 2022) For spinal stenosis, a provider may first focus on physical therapy to improve overall fitness, strengthen the abdominals and back muscles, and preserve motion in the spine. Pain-relieving medications, including NSAIDs and corticosteroid injections, can reduce inflammation and relieve pain. (American College of Rheumatology. 2023) Physical therapists provide various therapies to decrease symptoms, including manual and mechanical decompression and traction. Surgery may be recommended for cases of radiculopathy that don’t respond to conservative treatments.
Injury Medical Chiropractic and Functional Medicine Clinic care plans and clinical services are specialized and focused on injuries and the complete recovery process. Our areas of practice include Wellness & Nutrition, Chronic Pain, Personal Injury, Auto Accident Care, Work Injuries, Back Injury, Low Back Pain, Neck Pain, Migraine Headaches, Sports Injuries, Severe Sciatica, Scoliosis, Complex Herniated Discs, Fibromyalgia, Chronic Pain, Complex Injuries, Stress Management, Functional Medicine Treatments, and in-scope care protocols. We focus on restoring normal body functions after trauma and soft tissue injuries using Specialized Chiropractic Protocols, Wellness Programs, Functional and integrative Nutrition, Agility, and mobility Fitness Training, and Rehabilitation Systems for all ages. If the individual requires other treatment, they will be referred to a clinic or physician best suited for their condition. Dr. Jimenez has teamed with the top surgeons, clinical specialists, medical researchers, therapists, trainers, and premiere rehabilitation providers to bring El Paso, the top clinical treatments, to our community.
Reclaim Your Mobility: Chiropractic Care For Sciatica Recovery
For individuals who suffer from migraine headaches, can incorporating physical therapy help decrease pain, improve mobility, and manage future attacks?
Migraine Physical Therapy
Cervicogenic migraine headaches can cause pain, limited motion, or confusing symptoms like dizziness or nausea. They may originate from the neck or cervical spine and be called cervicogenic headaches. A chiropractic physical therapy team can assess the spine and offer treatments that help improve mobility and decrease pain. Individuals may benefit from working with a migraine physical therapy team to perform treatments for specific conditions, quickly and safely relieving pain and returning to their previous level of activity.
Cervical Spine Anatomy
The neck is comprised of seven stacked cervical vertebrae. The cervical vertebrae protect the spinal cord and allow the neck to move through:
Flexion
Extension
Rotation
Side bending
The upper cervical vertebrae help support the skull. There are joints on either side of the cervical level. One connects to the back of the skull and allows motion. This suboccipital area is home to several muscles that support and move the head, with nerves that travel from the neck through the suboccipital area into the head. The nerves and muscles in this area may be a source of neck pain and/or headaches.
Symptoms
Sudden motions can trigger symptoms of cervicogenic migraine, or they may come on during sustained neck postures. (Page P. 2011) The symptoms are often dull and non-throbbing and may last several hours to days. Symptoms of cervicogenic migraine headache may include:
Pain on both sides of the back of the head.
Pain in the back of the head that radiates to one shoulder.
Pain on one side of the upper neck that radiates to the temple, forehead, or eye.
Pain in one side of the face or cheek.
Reduced range of motion in the neck.
Sensitivity to light or sound
Nausea
Dizziness or vertigo
Diagnosis
Tools a physician may use may include:
X-ray
MRI
CT scan
Physical examination includes neck range of motion and palpation of the neck and skull.
When first visiting a physical therapist, they will go through medical history and conditions, and questions will be asked about the onset of pain, symptom behavior, medications, and diagnostic studies. The therapist will also ask about previous treatments and review medical and surgical history. Components of the evaluation may include:
Palpation of the neck and skull
Measures of neck range of motion
Strength measurements
Postural assessment
Once the evaluation is completed, the therapist will work with the individual to develop a personalized treatment program and rehabilitation goals. Various treatments are available.
Exercise
Exercises to improve neck motion and decrease pressure on cervical nerves may be prescribed and may include. (Park, S. K. et al., 2017)
Cervical rotation
Cervical flexion
Cervical side bending
Cervical retraction
The therapist will train the individual to move slowly and steadily and avoid sudden or jerky movements.
Postural Correction
If forward head posture is present, the upper cervical spine and the suboccipital area could compress the nerves that travel up the back of the skull. Correcting posture may be an effective strategy for treatment and can include:
Performing targeted postural exercises.
Utilizing a supportive neck pillow for sleep.
Using a lumbar support when sitting.
Kinesiology taping may help increase tactile awareness of back and neck position and improve overall postural awareness.
Heat/Ice
Heat or ice may be applied to the neck and skull to help decrease pain and inflammation.
Heat can help relax tight muscles and improve circulation and may be used before performing neck stretches.
Massage
If tight muscles are limiting neck motion and causing head pain, a massage can help improve mobility.
A special technique called suboccipital release loosens the muscles that attach the skull to the neck for improved motion and decreased nerve irritation.
Manual and Mechanical Traction
Part of the migraine physical therapy plan may involve mechanical or manual traction to decompress the neck’s discs and joints, improve motion in the neck, and decrease pain.
Joint mobilizations may be used to improve neck motion and manage pain. (Paquin, J. P. 2021)
Electrical Stimulation
Electrical stimulation, like electro-acupuncture or transcutaneous neuromuscular electrical stimulation, may be used on the neck muscles to decrease pain and improve headache symptoms.
Therapy Duration
Most migraine physical therapy sessions for cervicogenic headaches last about four to six weeks. Individuals may experience relief within a few days of starting therapy, or symptoms may come and go in different phases for weeks. Some experience continued migraine headache pain for months after starting treatment and use techniques they learned to help control symptoms.
Injury Medical Chiropractic and Functional Medicine Clinic specializes in progressive therapies and functional rehabilitation procedures focused on restoring normal body functions after trauma and soft tissue injuries. We use Specialized Chiropractic Protocols, Wellness Programs, Functional and integrative Nutrition, Agility and mobility Fitness Training, and Rehabilitation Systems for all ages. Our natural programs use the body’s ability to achieve specific measured goals. We have teamed up with the city’s premier doctors, therapists, and trainers to provide high-quality treatments that empower our patients to maintain the healthiest way of living and live a functional life with more energy, a positive attitude, better sleep, and less pain.
Chiropractic Care For Migraines
References
Page P. (2011). Cervicogenic headaches: an evidence-led approach to clinical management. International journal of sports physical therapy, 6(3), 254–266.
Headache Classification Committee of the International Headache Society (IHS) (2013). The International Classification of Headache Disorders, 3rd edition (beta version). Cephalalgia : an international journal of headache, 33(9), 629–808. doi.org/10.1177/0333102413485658
Rana M. V. (2013). Managing and treating headache of cervicogenic origin. The Medical clinics of North America, 97(2), 267–280. doi.org/10.1016/j.mcna.2012.11.003
Park, S. K., Yang, D. J., Kim, J. H., Kang, D. H., Park, S. H., & Yoon, J. H. (2017). Effects of cervical stretching and cranio-cervical flexion exercises on cervical muscle characteristics and posture of patients with cervicogenic headache. Journal of physical therapy science, 29(10), 1836–1840. doi.org/10.1589/jpts.29.1836
Paquin, J. P., Tousignant-Laflamme, Y., & Dumas, J. P. (2021). Effects of SNAG mobilization combined with a self-SNAG home-exercise for the treatment of cervicogenic headache: a pilot study. The Journal of manual & manipulative therapy, 29(4), 244–254. doi.org/10.1080/10669817.2020.1864960
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine