Many individuals do not realize they are in pain until they begin to feel symptoms of stiffness or tenderness in certain areas of their body. Many people have two most common complaints: back and shoulder pain. The shoulder and the back have a casual relationship that stabilizes the upper body and protects the spine’s thoracic region. When injuries or ordinary factors affect not only the shoulders but the back, it can lead to symptoms of pain and stiffness along the muscles, causing the development of trigger points along the upper back and shoulder muscles. One of the muscles affected by trigger points is the rhomboid muscles located in the upper back behind the scapula (shoulder blades). Today’s article looks at the rhomboid muscle, how superficial backaches and round shoulders can affect the rhomboid muscle, and managing trigger points associated with the rhomboid muscle. We refer patients to certified providers specializing in back pain treatments to aid individuals suffering from trigger points associated with the upper back along the rhomboid muscles. We also guide our patients by referring them to our associated medical providers based on their examination when appropriate. We ensure that education is a great solution to asking our providers insightful questions. Dr. Jimenez DC observes this information as an educational service only. Disclaimer
What Is The Rhomboid Muscle?
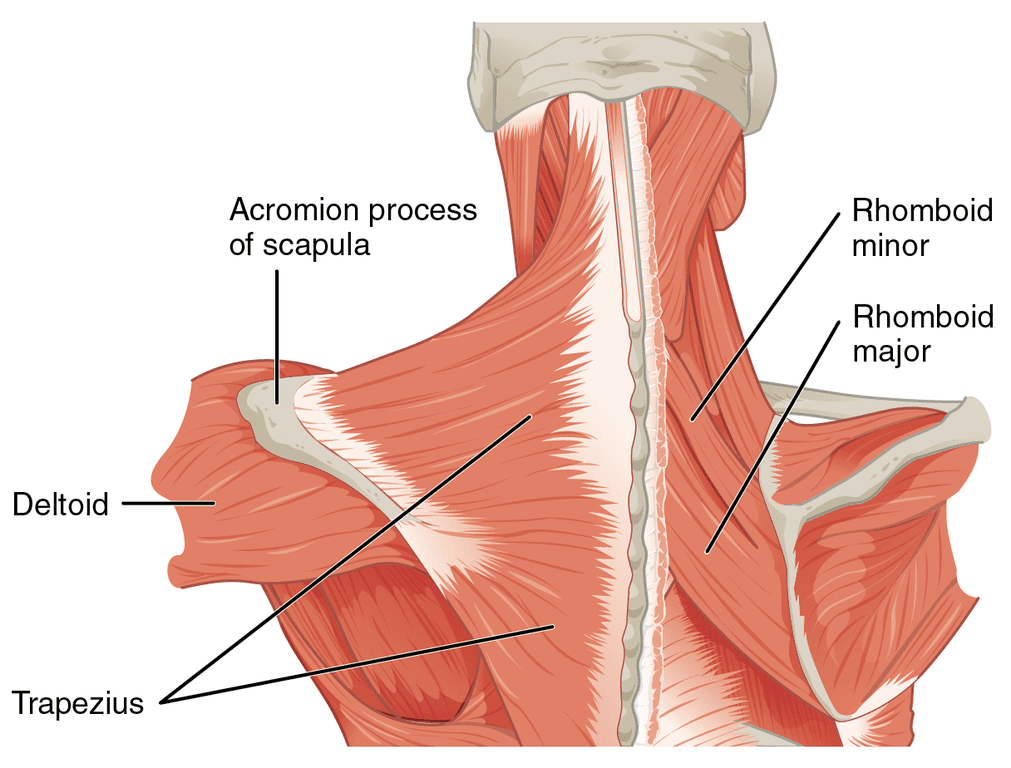
Do muscle stiffness in your shoulders seem to be causing you pain? Have you noticed that your shoulders seem more rounded than usual? What about the unexplainable upper backaches after being in a hunched position for a long period? Many individuals with these pain symptoms could be associated with the rhomboid muscles. The rhomboid muscles are a collective group of muscles important for upper limb movement and stability for the shoulder’s girdle and scapula. The rhomboid muscles consist of two separate muscles: the rhomboid minor and the rhomboid major, deep within the trapezius muscle and behind the scapula (shoulder blades). The functionality of the rhomboid is that they provide stability to the shoulder and when they are active, the upper arms move back and forth while walking.
How Superficial Backaches & Round Shoulders Affect The Rhomboid
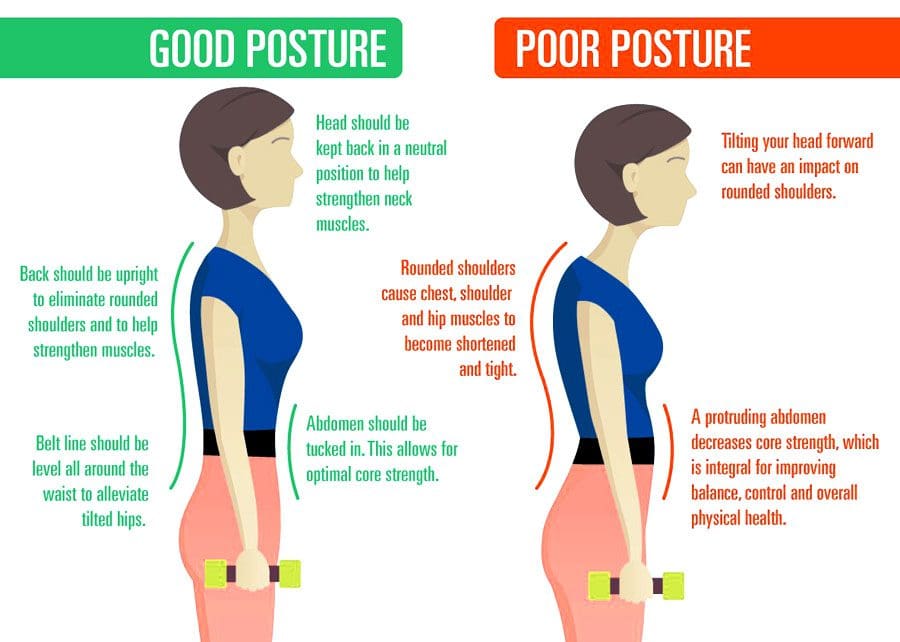
While the rhomboid muscles provide stability to the shoulders, they can succumb to pain like any muscles in different body sections. Ordinary factors like a bad sitting posture can cause the upper back and shoulder muscles to contract and strain. Studies reveal that the effects of bad sitting posture can lead to the development of a forwarding head posture with rounded shoulders, causing pain in the rhomboid muscles. When the shoulder muscles, like the rhomboid muscles, experience this sort of change over time, it can increase muscle tone and continuous stress in the neck and shoulders. To that point, it can lead to various symptoms like pain, numbness, loss of functionality in the upper limbs, and nerve root symptoms. Other issues like back pain can also be one of the symptoms that can lead to referred pain in the rhomboid muscles and can potentially lead to the development of trigger points along the shoulders and rhomboid muscles.
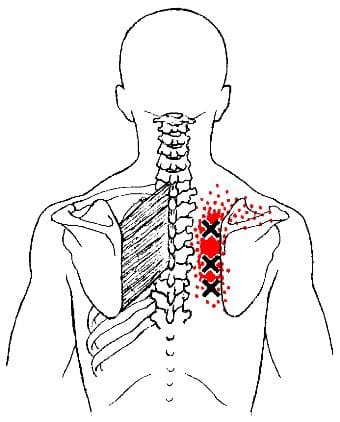
Other issues that can affect the rhomboid muscles are trigger points. Trigger points can be latent or active as they are tiny knots formed in the body’s muscle fibers. For the rhomboid muscles according to Dr. Janet G. Travell, M.D., when a person hears snapping and crunching noises during the movement of the shoulder blades, it may be due to the trigger points in the rhomboid muscles. Studies reveal that since trigger points can be either active or latent and elicit local referred pain, that can lead to muscle imbalance, weak and impaired motor function, and expose the joints to suboptimal loading. This means that trigger points in the rhomboid muscles can cause referred pain to the shoulder and mimic other chronic symptoms.
Stretching The Rhomboid Muscle & Managing Trigger Points-Video
Do you hear any snapping or crunching noises when rotating your shoulders? What about muscle stiffness along your shoulders or upper back? Or do you feel muscle aches from being hunched over for a long time? These symptoms could potentially involve trigger points associated with the rhomboid muscles. The rhomboid muscles help stabilize the shoulders and provide movement to the arms. When people overuse their shoulder muscles, it can cause the surrounding muscles to develop trigger points and inflict pain-like symptoms on the shoulders and upper back. Thankfully, all is not lost, as various treatments are available to relieve shoulder and upper back pain associated with trigger points along the rhomboid muscles. The video above explains where the trigger points are located on the rhomboid muscles and how to stretch that muscle to relieve trigger points from causing referred pain to the shoulders.
Managing Trigger Points Associated With The Rhomboid Muscle
Since the rhomboid muscles can become stiff due to overuse and could develop trigger points to inflict pain along the upper back and shoulders, this can cause many symptoms associated with pain and make the individual feel hopeless. Thankfully, various treatments can help manage trigger point pain associated with the rhomboid muscles. Studies reveal that thoracic spinal manipulation can relieve pain pressure sensitivity of the rhomboid muscles. Chiropractors are excellent when finding trigger points along the musculoskeletal system by utilizing spinal manipulation on the thoracic spine to loosen up the stiff muscles along the shoulders and upper back. Another way to manage trigger points associated with the rhomboid muscle is to stretch the shoulder muscles after a hot shower. This allows the muscles to relax and prevent future trigger points from forming along the rhomboid muscles.
Conclusion
The rhomboid muscles are a collective muscle group that has an important function in stabilizing the shoulder’s girdle and scapula (shoulder blades) while providing upper limb movement. The rhomboid muscles consist of two separate muscles: rhomboid minor and rhomboid major, which are behind the shoulder blades and deep within the trapezius muscles. When ordinary factors like poor posture or shoulder injuries affect the rhomboid muscles, it can develop trigger points that can cause stiffness in the rhomboid muscles. Various techniques can alleviate the referred pain along the shoulders, causing trigger points to develop along the rhomboid muscles. When these treatments are utilized on the rhomboid muscles, they can help prevent future shoulder issues.
References
Farrell, Connor, and John Kiel. “Anatomy, Back, Rhomboid Muscles.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 20 May 2022, https://www.ncbi.nlm.nih.gov/books/NBK534856/.
Haleema, Bibi, and Huma Riaz. “Effects of Thoracic Spine Manipulation on Pressure Pain Sensitivity of Rhomboid Muscle Active Trigger Points: A Randomized Controlled Trial.” JPMA. The Journal of the Pakistan Medical Association, U.S. National Library of Medicine, July 2021, https://pubmed.ncbi.nlm.nih.gov/34410234/.
Ribeiro, Daniel Cury, et al. “The Prevalence of Myofascial Trigger Points in Neck and Shoulder-Related Disorders: A Systematic Review of the Literature.” BMC Musculoskeletal Disorders, BioMed Central, 25 July 2018, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6060458/.
Yoo, Won-Gyu. “Effects of Pulling Direction on Upper Trapezius and Rhomboid Muscle Activity.” Journal of Physical Therapy Science, The Society of Physical Therapy Science, June 2017, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5468195/.
The low back is a common source of discomfort and soreness among volleyball players because of repetitive jumping, bending, and rotating of the trunk. Adolescents have an increased risk of this injury because their vertebral bones are still developing, which increases the risk for stress fractures. Chiropractic care, massage therapy, decompression, rest, and athletic training can help expedite pain relief and heal the injury.
Volley Back Pain
Muscle or ligament strains are the most common injury from repetitive jumping, bending, rotating movements, and hyperextension during serving, hitting and setting. This can lead to excessive compression forces on the discs and joints, causing reduced blood circulation, increasing the risk of overload injuries. One study reported that low back pain is experienced in 63% of players. However, if low-back pain is accompanied by pain that runs down the leg along with numbness or weakness in the foot or ankle, the issue could be a herniated disc.
Causes
One common reason is endurance imbalances in the muscles that stabilize the low back. The core muscles provide stability to the low back and spine for all movements. If imbalances are present, a player may spike or serve the ball with intense turning and arching. The added actions cause increased pressure in the joints and hip, gluteal, and leg muscles, affecting the spine’s stability.
The gluteals run from the back of the pelvis/hip bones down to the outside of the thigh.
The gluteal muscles prevent the trunk and hips from overbending forward when landing.
If the gluteal muscles do not have the strength and endurance to perform this motion, the upper body will bend too far forward, causing poor landing posture and decreased spine stability.
Anterior Pelvic Tilt
Studies have shown that players with low back pain tend to stand and land with an anterior pelvic tilt. This is an unhealthy posture when the front of the pelvis tilts forward, and the back of the pelvis raises. Landing hard with an anterior pelvic tilt causes increased arching and increases the pressure in the joints.
Chronic back pain
Warning signs of a more serious back problem include:
Pain that has lasted for more than 1 week and is not improving or getting worse.
Pain that prevents sleep or causes the individual to constantly wake up.
Difficulty sitting.
Back soreness when performing basic tasks and chores.
Significant pain on the court when jumping, landing, or rotating.
Chronic pain ranges from aches to shooting or throbbing pain that can run down the buttocks and legs.
Chiropractic Care
A chiropractor can alleviate volleyball back pain, rule out a more severe injury, such as a stress fracture or herniated disc, and provide a healthier and faster recovery. According to a study, athletes who received chiropractic care showed better speed and mobility. Quick reflexes and hand-eye coordination depend on an optimal functioning nervous system. 90% of the central nervous system travels through the spine. When one or more spinal segments are misaligned, the effect on the nervous system can seriously impact and disrupt nerve circulation, affecting speed, mobility, reflexes, and hand-eye coordination. Chiropractic adjustments will:
Relax and reset the back muscles.
Realign and decompress the spine.
Remove the pressure around the nerve roots.
Strengthen the core.
Improve and increase range of motion, strength, and overall endurance.
Anterior Pelvic Tilt
References
Haddas R, Sawyer SF, Sizer PS, Brooks T, Chyu MC, James CR. “Effects of Volitional Spine Stabilization and Lower-Extremity Fatigue on the Knee and Ankle During Landing Performance in a Population With Recurrent Low Back Pain.” J Sport Rehabil. 2017 Sep;26(5):329-338. doi: 10.1123/jsr.2015-0171.
Hangai M. et al., Relationship Between Low Back Pain and Competitive Sports Activities During Youth, Am J Sports Med 2010; 38: 791-796; published online before print January 5, 2010, doi:10.1177/0363546509350297.
Jadhav, K.G., Deshmukh, P.N., Tuppekar, R.P., Sinku, S.K.. A Survey of Injuries Prevalence in Varsity Volleyball Players. Journal of Exercise Science and Physiotherapy, Vol. 6, No. 2: 102-105, 2010 102
Mizoguchi, Yasuaki, et al. “Factors associated with low back pain in elite high school volleyball players.” Journal of physical therapy science vol. 31,8 (2019): 675-681. doi:10.1589/jpts.31.675
Movahed,Marziehet al. (2019). “Single leg landing kinematics in volleyball athletes: A comparison between athletes with and without active extension low back pain.”
Sheikhhoseiniet al. (2018). “Altered Lower Limb Kinematics during Jumping among Athletes with Persistent Low Back Pain”
Look how young children position their backs. There is a natural S curve, and their movements are effortless. As the body ages, too much sitting, slouching, and inactivity can cause muscle fatigue and tension leading to posture issues. Rounded shoulders describe a resting position that has shifted the shoulders out of the body’s natural alignment, which can worsen if left untreated. Chiropractic care can realign the shoulders, as well as the spine, and restore musculoskeletal health to optimum levels.
Rounded Shoulders
Rounded shoulders are an excessive thoracic kyphosis referring to an uneven forward rounding or curvature of the middle and upper back. Rounded shoulders shift out of proper alignment with the spine, causing posture-related problems like shoulder/neck/back discomfort, tightness, stiffness, and pain. Overall unhealthy posture contributes to the following:
The head constantly being in a forward or backward position
Headaches
Body aches and pains
Muscle fatigue
Chronic back soreness
Bent knees when standing or walking
Body movement dysfunction
Joint problems
Potbelly
Rounded shoulders
Body responses to rounded shoulders include:
Chronic musculoskeletal aches and pains
Breathing problems
Limited body function
Impaired mobility performance
Increased mental and musculoskeletal stress
Causes
Rounded shoulders are typically caused by unhealthy posture, but can also be caused by muscle imbalances from, for example, overfocusing on building chest strength but neglecting the core and upper back. Other causes include:
Standing and sitting for long periods
Stress
Lack of physical activity
Environmental factors
Too much exercise, sports, and physical activities
Musculoskeletal Imbalance
Postural imbalances anywhere in the body can cause rounded shoulders.
For example, when an individual tilts their head forward to look at their phone, the upper back has to round forward to hold the head. Constantly tilting can begin to generate an unhealthy muscle memory causing the neck and shoulder muscles to remain in a semi-flexed position that starts to become the norm.
Another example is when the arms are held out and in front for prolonged periods, like driving, typing, and cooking, the chest muscles get shortened. As time goes on, this causes the shoulder blades to move forward on the ribcage, making the upper back and shoulder area hunch awkwardly and unhealthily.
Stress
When the brain perceives a threat, the body physically prepares to take action through the fight or flight response. Common reactions include:
Jaw tensing
Tightening the abdominal muscles
Holding one’s breath
Rounding the shoulders
Stressors can include:
Job worries
Money issues
Relationship problems
Family responsibilities
All can cause changes in the body that result in rounded shoulders.
Environmental Factors
Respiratory conditions like asthma, COPD, and allergies can affect the body’s breathing and the ability of the diaphragm to contract and relax correctly.
Ribcage restrictions caused by chronic breathing problems can result in the thoracic/middle back tightening up, causing excessive shoulder rounding.
Exercise and Physical Activities
Exercise and physical activities can contribute to rounded shoulders because of the long periods of spinal flexion. These can include:
Bike riding, martial arts, and swimming.
Knitting requires the arms to be out in front.
Gardening requires kneeling and being hunched over.
Chiropractic Treatment
Chiropractic adjustments, therapeutic massage, and decompression therapy can unlock tight shoulder and chest muscles. A chiropractor uses gentle targeted adjustments to relieve pain, restore function, and retrain the muscles.
The doctor will look at the individual’s resting position while standing.
An individual with slumped shoulders can slouch, even when standing up straight.
Their hands will likely face behind them, with their thumbs pointed at each other.
Once the adjustments are made, a correct standing posture will make the hands face the body with the thumbs facing ahead.
Exercises will be recommended to strengthen the core and stretches to maintain the adjustments.
Posture Chiropractic
References
Fathollahnejad, Kiana, et al. “The effect of manual therapy and stabilizing exercises on forward head and rounded shoulder postures: a six-week intervention with a one-month follow-up study.” BMC musculoskeletal disorders vol. 20,1 86. 18 Feb. 2019, doi:10.1186/s12891-019-2438-y
Go, Seong-Uk, and Byoung-Hee Lee. “Effects of scapular stability exercise on shoulder stability and rehabilitative ultrasound images in office workers.” Journal of physical therapy science vol. 28,11 (2016): 2999-3002. doi:10.1589/jpts.28.2999
Kwon, Jung Won, et al. “Changes in upper-extremity muscle activities due to head position in subjects with a forward head posture and rounded shoulders.” Journal of physical therapy science vol. 27,6 (2015): 1739-42. doi:10.1589/jpts.27.1739
Lee, Do Youn, et al. “Changes in rounded shoulder and forward head posture according to exercise methods.” Journal of physical therapy science vol. 29,10 (2017): 1824-1827. doi:10.1589/jpts.29.1824
Park, Sang-In, et al. “Effects of shoulder stabilization exercise on pain and functional recovery of shoulder impingement syndrome patients.” Journal of physical therapy science vol. 25,11 (2013): 1359-62. doi:10.1589/jpts.25.1359
Spinal disc deterioration from aging is normal, but health issues or injuries can advance the degenerative process. Disc protrusions are related to herniated discs but are the mildest form of the condition and are a common form of spinal disc deterioration that can cause neck and back issues. However, individuals may have a small protruding disc that can go undetected unless it irritates or compresses the surrounding nerves. Chiropractic care, decompression, and massage therapy can realign the disc back into position, relieving discomfort and pain.
Disc Protrusion
A disc is like a sturdy soft rubber shock absorber/cushion with added gel inside. The gel acts as a shock absorber. When the gel begins to protrude out slightly, this is a disc protrusion. Once a protruding disc begins to develop, it usually remains in that position. The disc can sometimes reabsorb on its own and realign back into position, but there is no way of knowing that will happen or how long it will take. With age and/or injuries, the body’s parts change. The spine’s discs dehydrate and lose elasticity weakening the discs and making them more vulnerable to herniation stages:
First Stage
Following natural weakening can be classified as a disc protrusion when the disc’s core begins pushing into the spinal column.
Disc protrusions can be tiny or push out an entire side of the disc.
Second Stage
Disc deterioration often consists of a bulging disc when the core pushes out farther around the circumference beyond the disc’s outer layer, called the annulus fibrosus, creating the telltale bulge.
A bulging disc involves more than 180 degrees of the disc’s circumference.
Third Stage
The third stage is a herniated disc, meaning the disc’s outer wall has torn, allowing the inner gel to leak out, usually irritating the surrounding nerves.
Fourth Stage
The fourth stage is sequestration, a herniated disc in which a piece of the nucleus breaks free of the vertebral disc fragments and falls into the spinal canal.
Types
A disc protrusion is one type of disc herniation that pushes out but remains connected. Different types compress and irritate the discs differently and produce various symptoms, including:
Paracentral
This is the most common, where the disc protrusion jams the space between the central canal and the foramen.
Central
This is where the disc protrusion impinges into the spinal canal, with or without spinal cord compression.
Foraminal
The disc intrudes into the foramen, the space through which nerve roots branch off the spinal cord and exit the vertebrae.
Symptoms, Diagnosis, and Chiropractic Care
Individuals with a disc protrusion can have symptoms similar to sciatica, which includes back, buttock, and leg discomfort, numbness, and pain sensations.
Treatment for disc protrusion will be based on the individual’s symptoms.
A chiropractor will take a detailed medical history and perform a physical examination.
A spinal MRI test could be ordered depending on the injury or condition.
A customized treatment plan will be developed to fit the individual’s medical needs.
Most disc protrusions improve after a few weeks of rest, avoiding strenuous activities, activity modification, an anti-inflammatory diet, and gentle exercises that the chiropractic team will provide.
True Spinal Decompression
References
Fardon, David F et al. “Lumbar disc nomenclature: version 2.0: Recommendations of the combined task forces of the North American Spine Society, the American Society of Spine Radiology and the American Society of Neuroradiology.” The spine journal: official journal of the North American Spine Society vol. 14,11 (2014): 2525-45. doi:10.1016/j.spinee.2014.04.022
Mysliwiec, Lawrence Walter, et al. “MSU classification for herniated lumbar discs on MRI: toward developing objective criteria for surgical selection.” The European spine journal: official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society vol. 19,7 (2010): 1087-93. doi:10.1007/s00586-009-1274-4
Herniated, slipped, or ruptured discs affect 80% or more of the population. Most individuals don’t even realize they suffered a vertebral subluxation, as it shifted slightly but returned on its own and healed itself. Herniated disc/s symptoms can subside over time and can heal on their own. However, there are times when chiropractic is necessary to help the slipped or ruptured disc back into correct alignment and to help prevent re-injury or the development of new ones.
When Chiropractic Is Necessary
When an individual’s ability to move is limited is definitely when chiropractic is necessary. Individuals twist and turn their bodies, and the rotational force that comes from lifting and moving objects at home, work, school, sports, or lifting weights increases the risk of disc injury.
The lumbar spine or lower back is the most common location for a herniated disc injury.
The pain can spread to the glutes and legs, causing sciatica or sciatica-like symptoms.
When back pain spreads to the shoulder through the arm, it s caused by a herniated neck/cervical disc.
When the cushioning material from the disc/nucleus pulposus presses on surrounding nerves, it causes inflammation, pain, and numbness.
Individuals can suffer a herniated disc after changing a flat tire, stepping/slipping out of the bath/shower, or coughing and sneezing.
Healing
Herniated discs can be treated with ice packs and heat, over-the-counter medications, and anti-inflammatories. However, if these approaches are not producing results, chiropractic and physical therapy could be necessary to address the pain, reactivate the body’s healing system, and get the body’s circulation energy flowing. Exercises/movements are recommended depending on the injury to allow the musculoskeletal system to realign and circulate the nutrient-rich blood.
Evaluation
The chiropractic team must check if the individual is cleared for chiropractic care. Some individuals cannot undergo chiropractic adjustments because of the following:
The chiropractor will assess the injury and damage by evaluating the spine’s overall health, not just the painful areas.
They will inquire about medical history and conduct a physical examination.
Diagnostic tests could be necessary depending on the condition.
The team will evaluate the following criteria:
If reflexes are normal.
If there is muscle loss or decreased muscle strength.
If there is numbness or loss of sensation.
Loss of reflexes, muscle strength, and sensation could indicate the need for more aggressive treatment.
Depending on what is found, they may refer the individual to a spinal surgeon or specialist.
Techniques
Chiropractic focuses on restoring structural integrity to the body, reducing pressure on neurological tissue, and re-establishing a normal range of motion. With this treatment, pain and inflammation will be reduced or eliminated, and regular movement and reflexes will return. The body is realigned, stress is reduced, and the body’s natural energy can repair the damage. Adjustments involve:
HVLA is a high velocity, low amplitude short thrust to vertebrae that are out of position.
Mobilization involves low-velocity manipulation, stretching, and moving affected muscles and joints.
Joint cavitation expels oxygen, nitrogen, and carbon dioxide from the vertebrae and releases pressure on the affected area.
This technique uses a drop table while the chiropractor uses quick thrust and release manipulation.
Logan Basic Technique
This technique uses a light touch to level the sacrum.
Thompson Terminal Point Technique or Thompson Drop
This table technique adjusts with a weight mechanism to keep the patient in the correct position before the thrust is applied.
DOC Decompression Table
References
Danazumi, Musa S et al. “Two manual therapy techniques for management of lumbar radiculopathy: a randomized clinical trial.” Journal of osteopathic medicine vol. 121,4 391-400. 26 Feb. 2021, doi:10.1515/jom-2020-0261
Kerr, Dana, et al. “What Are Long-term Predictors of Outcomes for Lumbar Disc Herniation? A Randomized and Observational Study.” Clinical orthopedics and related research vol. 473,6 (2015): 1920-30. doi:10.1007/s11999-014-3803-7
Lurie, Jon D et al. “Surgical versus nonoperative treatment for lumbar disc herniation: eight-year results for the spine patient outcomes research trial.” Spine vol. 39,1 (2014): 3-16. doi:10.1097/BRS.0000000000000088
Wang, Jeffrey C et al. “Epidural injections for the treatment of symptomatic lumbar herniated discs.” Journal of spinal disorders & techniques vol. 15,4 (2002): 269-72. doi:10.1097/00024720-200208000-00001
Yussen, P S, and J D Swartz. “The acute lumbar disc herniation: imaging diagnosis.” Seminars in ultrasound, CT, and MR vol. 14,6 (1993): 389-98. doi:10.1016/s0887-2171(05)80032-0
When it comes to the body, many factors can cause low back pain without a person knowing they encounter it. Simple actions like sitting, standing, and walking can be difficult or helpful, depending on the person’s actions. Since low back pain tends to vary from person to person and the possible factors that can cause low back pain make diagnosing a bit difficult. Fortunately, there are available treatments that can help manage low back pain symptoms and can help alleviate its associated symptoms in the body. Today’s article examines the causes and symptoms of low back pain, aqua therapy for low back pain, and how chiropractic care goes hand in hand with aqua therapy. We refer patients to certified providers specializing in musculoskeletal treatments and hydrotherapy to help many individuals with low back pain. We also guide our patients by referring to our associated medical providers based on their examination when it’s appropriate. We find that education is the solution to asking our providers insightful questions. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
The Causes Of Low Back Pain
Have you been feeling aches along the sides of your back? Do you feel stiff when hunched over for an extended period? Or does sitting down make the pain go away or worsen? Many of these factors are associated with signs that you could be suffering from low back pain. Low back pain is considered the leading disability causes worldwide, as studies reveal, which can be influenced by many factors that a person is going through. Anyone can risk developing low back pain as it can derive from different sources that overlap many potential issues. Some of the causes associated with low back pain vary depending on how severely the factors affect the individual, which includes:
Muscle and ligament sprain (Overused muscles and ligaments from injuries, poor posture, or lifting heavy objects)
When it comes to the symptoms of low back pain, many individuals will experience pain ranging from a dull ache to a sudden shooting burning pain that travels down the legs. Many individuals often feel pain from one location of the lower half of the body; instead, it is located on the other side, known as referred pain. Low back pain can potentially mean that another issue is affecting the body. Some of the symptoms associated with low back pain include:
Muscle stiffness
Sciatica
Muscle spasms
Limited mobility on the hips and pelvis
Inflammation
Muscle tenderness
All is not lost, as treatments are available to manage low back pain symptoms and alleviate the body’s pain.
Aqua Therapy For Spine Health-Video
Have you been experiencing muscle stiffness in your lower back? Do hip pain and sciatic symptoms cause mobility issues in your legs? Or does it hurt when you are bending down to pick something up? You could be dealing with low back pain associated with chronic symptoms affecting the body, so why not try aqua therapy? The video above demonstrates what aqua therapy does to the body and the exercises used to relieve low back pain. Studies reveal that the therapeutic purposes of water have dated back to ancient Egypt, Greek, and Roman civilization; that helps cleanse the body from ailments. Many physical therapists utilize aqua therapy to enable individuals with low back pain. Aqua therapy engages the waters, buoyancy, resistance, and hydrostatic pressure that helps rehabilitate injuries and maintain health.
Aqua Therapy For Low Back Pain
Many individuals that suffer from low back pain will try to find ways to alleviate the pain. Aqua therapy is one available treatment that doesn’t strain the lower back and has therapeutic properties. Studies reveal that the beneficial properties of aqua therapy allow the body to improve muscle strength and range of motion while reducing muscle fatigue by using water buoyancy to take the pressure off the spine. Since low back pain is a common health issue associated with environmental factors for many individuals, studies reveal that water buoyancy can eliminate the gravitational forces impacting the body weight by counteracting it. To that point, this reduces joint stress on the body to perform the water aerobic exercises with ease. Individuals who incorporate aqua therapy in their health and wellness journey may be more motivated to exercise in the water without worrying about constant pain.
Aqua Therapy Goes Hand In Hand With Chiropractic Care
Like any treatment, chiropractic care and aqua therapy have an excellent relationship as they work together to assess and analyze the individual’s problem and devise a plan for them. Chiropractors utilize spinal manipulation to determine where the pain is located. So when a person is dealing with low back pain due to spinal subluxation or misalignment, a chiropractor can help the individual by loosening the stiff muscles and increasing the range of motion back to the spine. At the same time, aqua therapy incorporates the same benefits associated with land-based physical therapy, including a treatment plan tailored to the individual. Chiropractors and physical therapists work together to determine the best possible action to speed up the recovery process when it comes to a person’s pain, giving them the best chance to get back their quality of life.
Conclusion
Low back pain is one of many individuals’ most common complaints worldwide. The many factors associated with low back pain vary and range from a dull ache to a sharp pain radiating down the legs as part of the symptoms of low back pain. Treatments like aqua therapy can help take the load off the spine through water buoyancy and can help reduce the stress on the joints in the lumbar spine while reducing muscle fatigue. Combined with chiropractic care, many individuals can recover faster from their low back pain and bring back their quality of life without being in so much pain.
References
Abadi, Fariba Hossein, et al. “The Effect of Aquatic Exercise Program on Low-Back Pain Disability in Obese Women.” Journal of Exercise Rehabilitation, Korean Society of Exercise Rehabilitation, 31 Dec. 2019, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6944883/.
Allegri, Massimo, et al. “Mechanisms of Low Back Pain: A Guide for Diagnosis and Therapy.” F1000Research, F1000Research, 28 June 2016, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4926733/.
Carayannopoulos, Alexios G, et al. “The Benefits of Combining Water and Land-Based Therapy.” Journal of Exercise Rehabilitation, Korean Society of Exercise Rehabilitation, 26 Feb. 2020, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7056478/.
Cole, Andrew, and Bruce Becker. “Water Therapy Exercise Program.” Spine, Spine-Health, 26 Feb. 2010, https://www.spine-health.com/wellness/exercise/water-therapy-exercise-program.
The body is designed to move. For individuals who spend a significant amount of time driving each day, whether for a living or a long commute, over time can lead to headaches, neck and back pain, sciatica, and increases the risk for serious injury. Chiropractic can retrain individuals to practice healthy driving posture. This is accomplished through decompression and massage therapy combined with recommended stretches/exercises, and an anti-inflammatory diet will bring pain relief and help prevent injury.
Healthy Driving Posture
Two main reasons driving impacts the back are poor posture and being in a fixed position for an extended period. Individuals who regularly drive for more than 4 hours a day are more at risk. An unhealthy driving posture can lead to an increased risk of discomfort/pain in the:
Over time these issues can become chronic, making the body vulnerable to various injuries.
Back Pain Symptoms
Sometimes back pain needs immediate medical attention if any of the following symptoms present:
Inflammation in the back.
Swelling on the back.
Constant pain does not go away or ease up after resting or movement.
Pain in the upper back that radiates to the chest.
A high temperature.
Unexplained weight loss.
Loss of bladder or bowel control.
Numbness or tingling around the buttocks or groin area.
Driving Recommendations
Spine Support
Slide the tailbone as close to the back of the seat as possible.
Leave a gap between the back of the knees and the front of the seat.
If the vehicle doesn’t allow for the proper position, a back support cushion can help.
Raise The Hips
If possible, adjust the area you sit on, so the thighs are supported along their entire length.
The knees should be slightly lower than the hips.
This will increase circulation to the back muscles while opening up the hips.
Sitting Too Close
An individual should be able to comfortably reach the pedals and depress them through their full range with the entire foot.
A safety study found that drivers whose chests were closer to the wheel were significantly more likely to suffer head, neck, and chest injuries in front and rear-end collisions.
Proper Height
Ensure the seat raises the eye level a few inches above the steering wheel to allow sufficient clearance between the head and roof.
Seat Angle
The angle of the back of the seat should go a little beyond 90 degrees to 100-110 degrees places minimal pressure on the back.
Leaning too far back forces the individual to raise/push their head and neck forward, which can cause neck pain, shoulder pain, and tingling in the fingers.
Headrest Height
The top of the headrest should be between the top of the ears and the top of the head.
It should slightly touch the back of the head when sitting with a healthy driving posture.
This exercise activates the abdominal and external oblique muscles.
Press the lower back into the car seat.
Inhale and tilt the pelvis forward to create an arch in the lower back.
Hold for 3 seconds, then release.
Repeat ten times.
Posture is more than just how one carries themselves. The effects of unhealthy posture can carry over into an individual’s physical, mental, and emotional health. Whether it’s caused by injury, stress, work, or sports, a professional chiropractor will help you get back to optimal health.
Driving Position
References
Cvetkovic, Marko M et al. “Assessing Post-Driving Discomfort and Its Influence on Gait Patterns.” Sensors (Basel, Switzerland) vol. 21,24 8492. 20 Dec. 2021, doi:10.3390/s21248492
Pope, Malcolm H et al. “Spine ergonomics.” Annual review of biomedical engineering vol. 4 (2002): 49-68. doi:10.1146/annurev.bioeng.4.092101.122107
Tinitali, Sarah, et al. “Sitting Posture During Occupational Driving Causes Low Back Pain; Evidence-Based Position or Dogma? A Systematic Review.” Human factors vol. 63,1 (2021): 111-123. doi:10.1177/0018720819871730
van Veen, Sigrid, and Peter Vink. “Posture variation in a car within the restrictions of the driving task.” Work (Reading, Mass.) vol. 54,4 (2016): 887-94. doi:10.3233/WOR-162359
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine