Can postural assessments help identify problems with how a person stands or sits, which can lead to various musculoskeletal issues?
Postural Assessment
Proper posture is an exercise in which the muscles support the skeleton in a comfortable, stable, and efficient alignment. Healthy posture is present when the body is still and when moving. However, numerous factors can affect and hinder posture. These include daily wear and tear, injury, illness, or a condition. A posture assessment is a process that identifies posture issues and their root causes, often using visual and palpation techniques, and can help determine appropriate treatment or exercises. (Science Direct, 2007)
Visual Assessment
Observing the body’s alignment and symmetry from different angles (anterior, posterior, and lateral views).
Consider their daily activities, work environment, and any previous injuries. (Du, S. H. et al., 2023)
Wall Test
The patient stands against a wall with their feet shoulder-width apart and heels about 6 inches from the baseboard.
If they have good posture, their ears will be vertically aligned with their shoulders, and their head will be no more than three finger widths from the wall. (Physiopedia, 2025)
Professionals Who Can Perform a Posture Assessment
Physiotherapists
Professionals trained in assessing and treating musculoskeletal problems.
Chiropractors
Professionals who focus on the spine and nervous system.
Fitness Professionals
Personal trainers or other fitness professionals can use posture assessments to help clients improve their posture and movement.
Ergonomists
Professionals who specialize in designing workspaces and environments to promote good posture and reduce strain.
Injury Medical Chiropractic & Functional Medicine Clinic
Talk to a healthcare provider to learn what interventions would help the most. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution. We focus on what works for you to relieve pain, restore function, and prevent injury. Regarding musculoskeletal pain, specialists like chiropractors, acupuncturists, and massage therapists can help mitigate the pain through spinal adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal issues.
Singla, D., & Veqar, Z. (2014). Methods of postural assessment used for sports persons. Journal of clinical and diagnostic research: JCDR, 8(4), LE01–LE4. https://doi.org/10.7860/JCDR/2014/6836.4266
Du, S. H., Zhang, Y. H., Yang, Q. H., Wang, Y. C., Fang, Y., & Wang, X. Q. (2023). Spinal posture assessment and low back pain. EFORT open reviews, 8(9), 708–718. https://doi.org/10.1530/EOR-23-0025
For individuals looking to improve their fitness health, can a fitness assessment test identify potential areas and help evaluate overall health and physical status?
Fitness Assessment
A fitness test, also known as a fitness assessment, helps evaluate an individual’s overall and physical health. It comprises a series of exercises to design an appropriate exercise program for general health and fitness. (National Strength and Conditioning Association. 2017) Fitness assessment testing benefits include:
Identifying areas that need improvement.
Assisting professionals in understanding what types of exercise are safest and most effective.
Helping measure fitness progress over time.
Allowing for an individualized plan that can help prevent injuries and maintain the body’s overall health.
An assessment can comprise a wide range of tests, including:
Body composition tests.
Cardiovascular stress tests.
Endurance tests.
Range of motion tests.
They are meant to ensure the individual won’t be at risk of injury and provide the trainer with the insights needed to establish clear and effective fitness goals. Individuals who wonder whether fitness testing would benefit them should consult their healthcare provider.
General Health
Before starting a fitness program, it is important to inform the trainer of individual medical history and get the necessary approval from a primary healthcare provider. (Harvard Health Publishing. Harvard Medical School. 2012) Fitness specialists usually use one or more screening tools to help determine individual baseline health.
This may include obtaining vital sign measurements like height and weight, resting heart rate/RHR, and resting blood pressure/RBP. Many trainers will also use a physical activity readiness questionnaire/PAR-Q comprising questions about general health. (National Academy of Sports Medicine. 2020) Among the questions, individuals may be asked about the medications being taken, any problems with dizziness or pain, or medical conditions that may impair their ability to exercise.
Body Composition
Body composition describes total body weight components, including muscles, bones, and fat. The most common methods for estimating body composition include:
Bioelectrical Impedance Analysis – BIA
During BIA, electrical signals are sent from electrodes through the soles of the feet to the abdomen to estimate body composition. (Doylestown Health. 2024)
These measurements use calipers to estimate the amount of body fat in a fold of skin.
Cardiovascular Endurance
Cardiovascular endurance testing, also known as stress testing, measures how efficiently the heart and lungs work to supply oxygen and energy to the body during physical activity. (UC Davis Health, 2024) The three most common tests used include:
12-minute Run Tests
Twelve-minute run tests are performed on a treadmill, and an individual’s pre-exercise heart and respiration rates are compared with post-exercise heart and respiration rates.
Exercise Stress
Exercise stress testing is performed on a treadmill or stationary bike.
It involves using a heart monitor and blood pressure cuff to measure vital signs during exercise.
VO2 Max Testing
Performed on a treadmill or stationary bike.
V02 max testing uses a breathing device to measure the maximum rate of oxygen consumption during physical activity (UC Davis Health, 2024)
Some trainers will incorporate exercises like sit-ups or push-ups to measure response to specific exercises.
These baseline results can be used later to see if health and fitness levels have improved.
Strength and Endurance
Muscle endurance testing measures the length of time a muscle group can contract and release before it fatigues. Strength testing measures the maximal amount of force a muscle group can exert. (American Council on Exercise, Jiminez C., 2018) The exercises used include:
The push-up test.
Core strength and stability test.
Sometimes, a trainer will use a metronome to measure how long the individual can keep up with the rhythm. The results are then compared to individuals of the same age group and sex to establish a baseline level. Strength and endurance tests are valuable as they help the trainer spot which muscle groups are stronger, vulnerable, and need focused attention. (Heyward, V. H., Gibson, A. L. 2014).
Flexibility
Measuring the flexibility of joints is vital in determining whether individuals have postural imbalances, foot instability, or limitations in range of motion. (Pate R, Oria M, Pillsbury L, 2012)
Shoulder Flexibility
Shoulder flexibility testing evaluates the flexibility and mobility of the shoulder joint.
It is performed by using one hand to reach behind the neck, between the shoulders, and the other hand to reach behind the back, toward the shoulders, to measure how far apart the hands are. (Baumgartner TA, PhD, Jackson AS, PhD et al., 2015)
Fitness assessment testing has various benefits. It can help trainers design a personalized workout program, help individuals identify fitness areas that need improvement, measure progress, and add intensity and endurance to their routine, which can help prevent injuries and help maintain overall health. We focus on what works for you and strive to better the body through researched methods and total wellness programs. These natural programs use the body’s ability to achieve improvement goals. Ask a healthcare professional or fitness professional for guidance if you need advice.
PUSH Fitness
References
National Strength and Conditioning Association. (2017). Purposes of assessment. https://www.nsca.com/education/articles/kinetic-select/purposes-of-assessment/
Harvard Health Publishing. Harvard Medical School. (2012). Do you need to see a doctor before starting your exercise program? HealthBeat. https://www.health.harvard.edu/healthbeat/do-you-need-to-see-a-doctor-before-starting-your-exercise-program
National Academy of Sports Medicine. (2020). PAR-Q-+ The Physical Activity Readiness Questionnaire for Everyone. https://www.nasm.org/docs/pdf/parqplus-2020.pdf?sfvrsn=401bf1af_24
Doylestown Health. (2024). Bio-Electrical Impedance Analysis (BIA)-Body Mass Analysis. https://www.doylestownhealth.org/service-lines/nutrition#maintabbed-content-tab-2BDAD9F8-F379-403C-8C9C-75D7BFA6E596-1-1
National Heart, Lung, and Blood Institute. U.S. Department of Health and Human Services. (N.D.). Calculate your body mass index. Retrieved from https://www.nhlbi.nih.gov/health/educational/lose_wt/BMI/bmicalc.htm
UC Davis Health. (2024). VO2max and Aerobic Fitness. https://health.ucdavis.edu/sports-medicine/resources/vo2description
American Council on Exercise. Jiminez C. (2018). Understanding 1-RM and Predicted 1-RM Assessments. ACE Fitness. https://www.acefitness.org/fitness-certifications/ace-answers/exam-preparation-blog/2894/understanding-1-rm-and-predicted-1-rm-assessments/
Heyward, V. H., Gibson, A. L. (2014). Advanced Fitness Assessment and Exercise Prescription. United Kingdom: Human Kinetics. https://www.google.com/books/edition/Advanced_Fitness_Assessment_and_Exercise/PkdoAwAAQBAJhl=en&gbpv=1&dq=Strength+and+endurance+tests+muscle+groups+are+stronger+and+weaker&pg=PA173&printsec=frontcover#v=onepage&q=Strength%20and%20endurance%20tests%20muscle%20groups%20are%20stronger%20and%20weaker&f=false
Pate R, Oria M, Pillsbury L, (Eds). (2012). Health-related fitness measures for youth: Flexibility. In R. Pate, M. Oria, & L. Pillsbury (Eds.), Fitness Measures and Health Outcomes in Youth. https://doi.org/10.17226/13483
Baumgartner, T. A., Jackson, A. S., Mahar, M. T., Rowe, D. A. (2015). Measurement for Evaluation in Kinesiology. United States: Jones & Bartlett Learning. https://www.google.com/books/edition/Measurement_for_Evaluation_in_Kinesiolog/_oCHCgAAQBAJ?hl=en&gbpv=1&dq=Measurement+for+Evaluation+in+Kinesiology+(9th+Edition).&printsec=frontcover#v=onepage&q&f=false
American Council of Exercise. Metcalf A. (2014). How to improve flexibility and maintain it. ACE Fitness. https://www.acefitness.org/resources/everyone/blog/3761/how-to-improve-flexibility-and-maintain-it/
Doctors define chronic pain, as any pain that lasts for 3 to 6 months or more. The pain effects an individual’s mental health and day to day life. Pain comes from a series of messages that run through the nervous system. Depression seems to follow pain. It causes severe symptoms that affect how an individual feels, thinks, and how the handle daily activities, i.e. sleeping, eating and working. Chiropractor, Dr. Alex Jimenez delves into potential biomarkers that can help in finding and treating the root causes of pain and chronic pain.
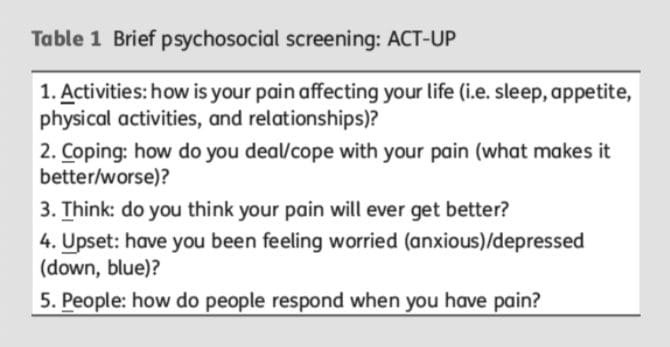
The first step in successful pain management is a comprehensive biopsychosocial assessment.
The extent of organic pathology may not be accurately reflected in the pain experience.
The initial assessment can be used to identify areas that require more in-depth evaluation.
Many validated self-report tools are available to assess the impact of chronic pain.
Assessment Of Patients With Chronic Pain
Chronic pain is a public health concern affecting 20�30% of the population of Western countries. Although there have been many scientific advances in the understanding of the neurophysiology of pain, precisely assessing and diagnosing a patient’s chronic pain problem is not straightforward or well-defined. How chronic pain is conceptualized influences how pain is evaluated and the factors considered when making a chronic pain diagnosis. There is no one-to-one relationship between the amount or type of organic pathology and pain intensity, but instead, the chronic pain experience is shaped by a myriad of biomedical, psychosocial (e.g. patients’ beliefs, expectations, and mood), and behavioral factors (e.g. context, responses by significant others). Assessing each of these three domains through a comprehensive evaluation of the person with chronic pain is essential for treatment decisions and to facilitate optimal outcomes. This evaluation should include a thorough patient history and medical evaluation and a brief screening interview where the patient’s behavior can be observed. Further assessment to address questions identified during the initial evaluation will guide decisions as to what additional assessments, if any, may be appropriate. Standardized self-reported instruments to evaluate the patient’s pain intensity, functional abilities, beliefs and expectations, and emotional distress are available, and can be administered by the physician, or a referral for in depth evaluation can be made to assist in treatment planning.
Pain is an extremely prevalent symptom. Chronic pain alone is estimated to affect 30% of the adult population of the USA, upwards of 100 million adults.1
Despite the soaring cost of treating people with chronic pain, relief for many remains elusive and complete elimination of pain is rare. Although there have been substantial advances in the knowledge of the neurophysiology of pain, along with the development of potent analgesic medications and other innovative medical and surgical interventions, on average the amount of pain reduction by available procedures is 30�40% and this occurs in fewer than one-half of treated patients.
The way we think about pain influences the way in which we go evaluate pain. Assessment begins with history and physical examination, followed, by laboratory tests and diagnostic imaging procedures in an attempt to identify and/or confirm the presence of any underlying pathology causing the symptom/s or the pain generator.
In the absence of identifiable organic pathology, the healthcare provider may assume that the report of symptoms stems from psychological factors and may request a psychological evaluation to detect the emotional factors underlying the patient’s report. There is duality where the report of symptoms are attributed to either somatic or psychogenic mechanisms.
As an example, the organic bases for some of the most common and recurring acute (e.g. headache)3 and chronic [e.g. back pain, fibromyalgia (FM)] pain problems are largely unknown,4,5 while on the other hand, asymptomatic individuals may have structural abnormalities such as herniated discs that would explain pain if it were present.6,7�There is a lacking in adequate explanations for patients with no identified organic pathology who report severe pain and pain-free individuals with significant, objective pathology.
Chronic pain affects more than just the individual patient, but also his or her significant others (partners, relatives, employers and co-workers and friends), making appropriate treatment essential. Satisfactory treatment can only come from comprehensive assessment of the biological aetiology of the pain in conjunction with the patient’s specific psychosocial and behavioral presentation, including their emotional state (e.g. anxiety, depression, and anger), perception and understanding of symptoms, and reactions to those symptoms by significant others.8,9 A key premise is that multiple factors influence the symptoms and functional limitations of individuals with chronic pain. Therefore, a comprehensive assessment is needed that addresses biomedical, psychosocial, and behavioral domains, as each contributes to chronic pain and related disability.10,11
Comprehensive Assessment Of An Individual With Chronic Pain
Turk and Meichenbaum12 suggested that three central questions should guide assessment of people who report pain:
What is the extent of the patient’s disease or injury (physical impairment)?
What is the magnitude of the illness? That is, to what extent is the patient suffering, disabled, and unable to enjoy usual activities?
Does the individual’s behavior seem appropriate to the disease or injury, or is there any evidence of symptom amplification for any of a variety of psychological or social reasons (e.g. benefits such as positive attention, mood-altering medications, financial compensation)?
To answer these questions, information should be gathered from the patient by history and physical examination, in combination with a clinical interview, and through standardized assessment instruments. Healthcare providers need to seek any cause(s) of pain through physical examination and diagnostic tests while concomitantly assessing the patient�s mood, fears, expectancies, coping efforts, resources, responses of significant others, and the impact of pain on the patients� lives.11 In short, the healthcare provider must evaluate the �whole person� and not just the pain.
The general goals of the history and medical evaluation are to:
(i) determine the necessity of additional diagnostic testing
(ii) determine if medical data can explain the patient’s symptoms, symptom severity, and functional limitations
(iii) make a medical diagnosis
(iv) evaluate the availability of appropriate treatment
(v) establish the objectives of treatment
(vi) determine the appropriate course for symptom management if a complete cure is not possible.
Significant numbers of patients that report chronic pain demonstrate no physical pathology using plain radiographs, computed axial tomography scans, or electromyography (an extensive literature is available on physical assessment, radiographic and laboratory assessment procedures to determine the physical basis of pain),17 making a precise pathological diagnosis difficult or impossible.
Despite these limitations, the patient’s history and physical examination remain the basis of medical diagnosis, can provide a safeguard against over-interpreting findings from diagnostic imaging that are largely confirmatory, and can be used to guide the direction of further evaluation efforts.
In addition, patients with chronic pain problems often consume a variety of medications.18 It is important to discuss a patient’s current medications during the interview, as many pain medications are associated with side-effects that may cause or mimic emotional distress.19 Healthcare providers should not only be familiar with medications used for chronic pain, but also with side-effects from these medications that result in fatigue, sleep difficulties, and mood changes to avoid misdiagnosis of depression.
The use of daily diaries is believed to be more accurate as they are based on real-time rather than recall. Patients may be asked to maintain regular diaries of pain intensity with ratings recorded several times each day (e.g. meals and bedtime) for several days or weeks and multiple pain ratings can be averaged across time.
One problem noted with the use of paper-and-pencil diaries is that patients may not follow the instruction to provide ratings at specified intervals. Rather, patients may complete diaries in advance (�fill forward�) or shortly before seeing a clinician (�fill backward�),24 undermining the putative validity of diaries. Electronic diaries have gained acceptance in some research studies to avoid these problems.
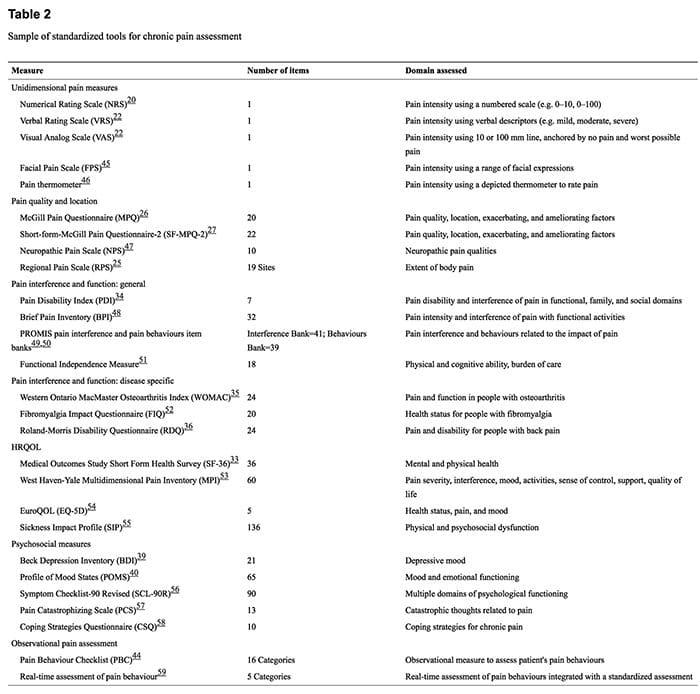
Research has demonstrated the importance of assessing overall health-related quality of life (HRQOL) in chronic pain patients in addition to function.31,32 There are a number of well established, psychometrically supported HRQOL measures [Medical Outcomes Study Short-Form Health Survey (SF-36)],33 general measures of physical functioning [e.g. Pain Disability Index (PDI)],34 and disease-specific measures [e.g. Western Ontario MacMaster Osteoarthritis Index (WOMAC);35 Roland-Morris Back Pain Disability Questionnaire (RDQ)]36 to assess function and quality of life.
Disease-specific measures are designed to evaluate the impact of a specific condition (e.g. pain and stiffness in people with osteoarthritis), whereas generic measures make it possible to compare physical functioning associated with a given disorder and its treatment with that of various other conditions. Specific effects of a disorder may not be detected when using a generic measure; therefore, disease-specific measures may be more likely to reveal clinically important improvement or deterioration in specific functions as a result of treatment. General measures of functioning may be useful to compare patients with a diversity of painful conditions. The combined use of disease-specific and generic measures facilitates the achievement of both objectives.
The presence of emotional distress in people with chronic pain presents a challenge when assessing symptoms such as fatigue, reduced activity level, decreased libido, appetite change, sleep disturbance, weight gain or loss, and memory and concentration deficits, as these symptoms can be the result of pain, emotional distress, or treatment medications prescribed to control pain.
Instruments have been developed specifically for pain patients to assess psychological distress, the impact of pain on patients� lives, feeling of control, coping behaviors, and attitudes about disease, pain, and healthcare providers.17
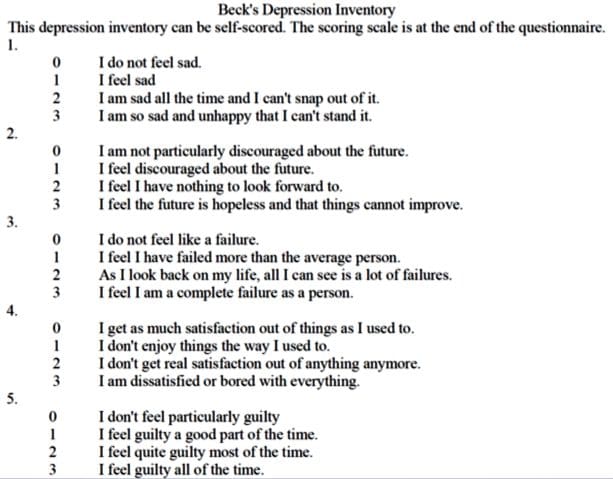
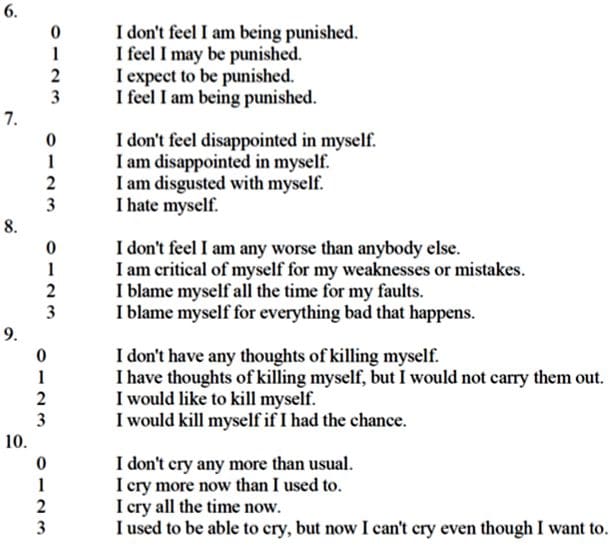
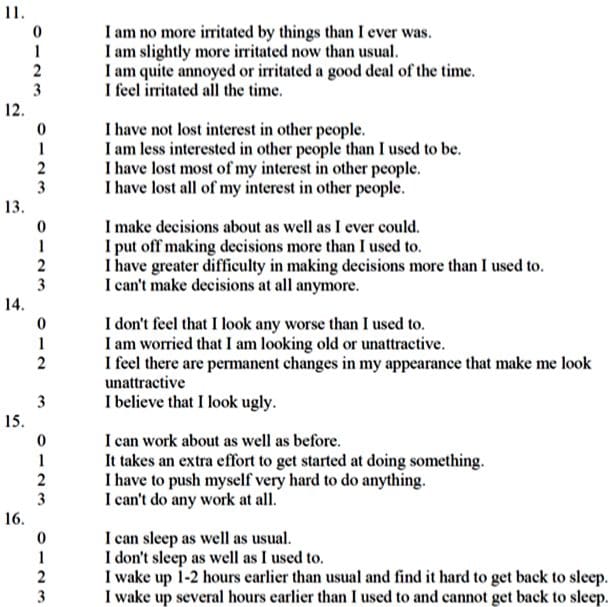
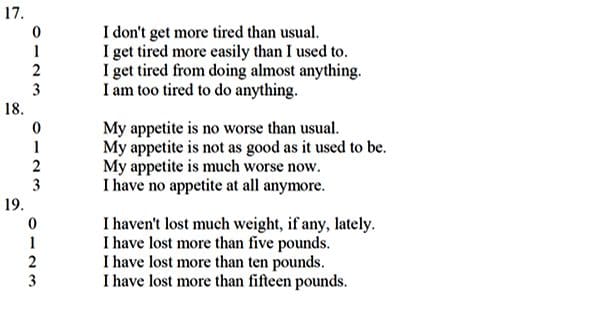
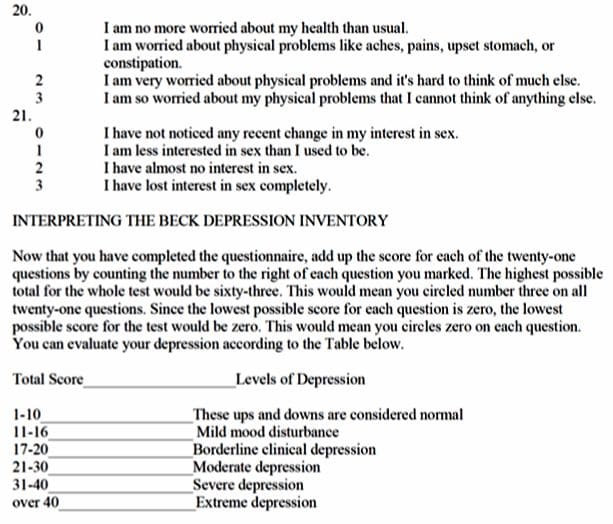
For example, the Beck Depression Inventory (BDI)39 and the Profile of Mood States (POMS)40 are psychometrically sound for assessing symptoms of depressed mood, emotional distress, and mood disturbance, and have been recommended to be used in all clinical trials of chronic pain;41 however, the scores must be interpreted with caution and the criteria for levels of emotional distress may need to be modified to prevent false positives.42
Lab Biomarkers For Pain
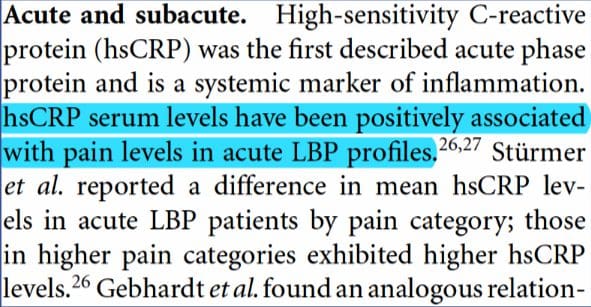
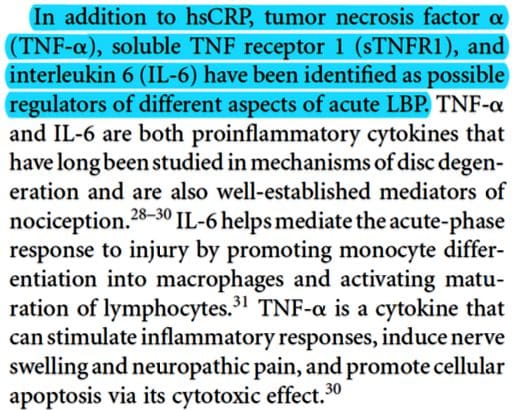
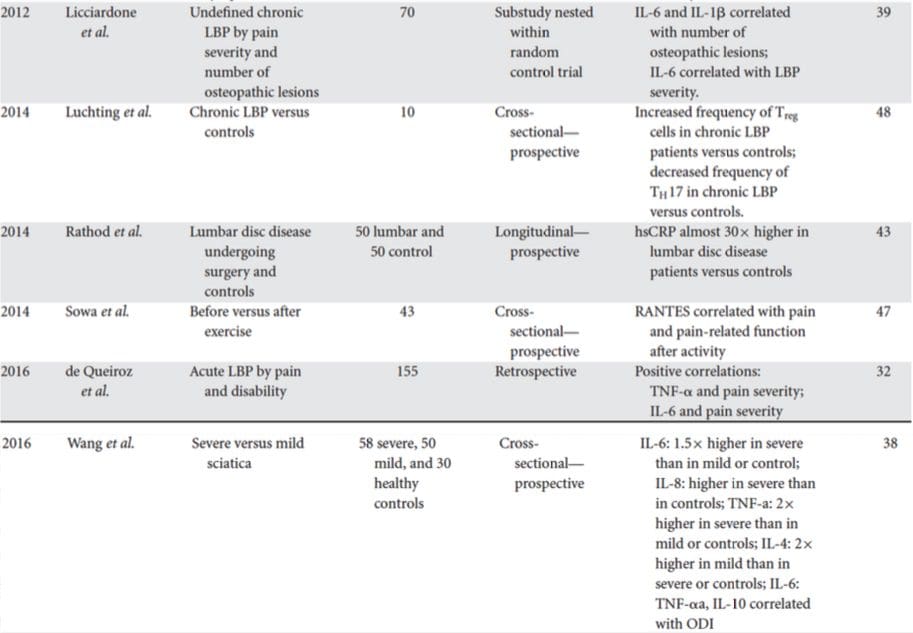
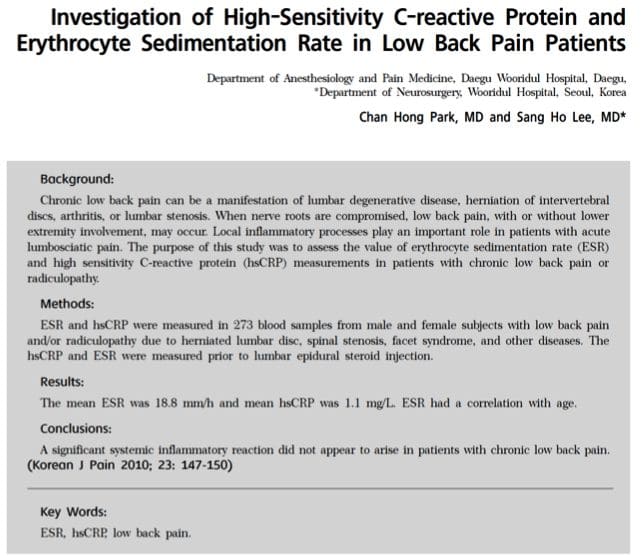
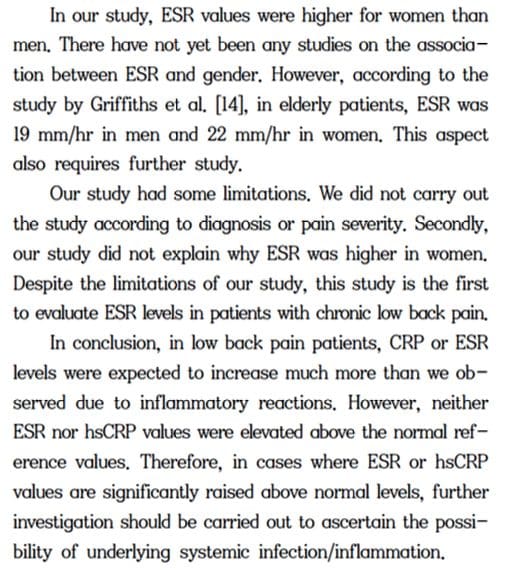
Biomarkers are biological characteristics that can be used to indicate health or disease. This paper reviews studies on biomarkers of low back pain (LBP) in human subjects. LBP is the leading cause of disability, caused by various spine-related disorders, including intervertebral disc degeneration, disc herniation, spinal stenosis, and facet arthritis. The focus of these studies is inflammatory mediators, because inflammation contributes to the pathogenesis of disc degeneration and associated pain mechanisms. Increasingly, studies suggest that the presence of inflammatory mediators can be measured systemically in the blood. These biomarkers may serve as novel tools for directing patient care. Currently, patient response to treatment is unpredictable with a significant rate of recurrence, and, while surgical treatments may provide anatomical correction and pain relief, they are invasive and costly. The review covers studies performed on populations with specific diagnoses and undefined origins of LBP. Since the natural history of LBP is progressive, the temporal nature of studies is categorized by duration of symptomology/disease. Related studies on changes in biomarkers with treatment are also reviewed. Ultimately, diagnostic biomarkers of LBP and spinal degeneration have the potential to shepherd an era of individualized spine medicine for personalized therapeutics in the treatment of LBP.
Biomarkers For Chronic Neuropathic Pain & Potential Application In Spinal Cord Stimulation
This review was focused on understanding which substances inside the human body increase and decrease with increasing neuropathic pain. We reviewed various studies, and saw correlations between neuropathic pain and components of the immune system (this system defends the body against diseases and infections). Our findings will especially be useful for understanding ways to reduce or eliminate the discomfort, chronic neuropathic pain brings with it. Spinal cord stimulation (SCS) procedure is one of the few fairly efficient remedial treatments for pain. A follow-up study will apply our findings from this review to SCS, in order to understand the mechanism, and further optimize efficaciousness.
Pro-inflammatory cytokines such as IL-1?, IL-6, IL-2, IL-33, CCL3, CXCL1, CCR5, and TNF-?, have been found to play significant roles in the amplification of chronic pain states.
After review of various studies relating to pain biomarkers, we found that serum levels of pro-inflammatory cytokines and chemokines, such as IL-1?, IL-6, IL-2, IL-33, CCL3, CXCL1, CCR5, and TNF-?, were significantly up-regulated during chronic pain experience. On the other hand, anti-inflammatory cytokines such as IL-10 and IL-4 were found to show significant down-regulation during chronic pain state.
Biomarkers For Depression
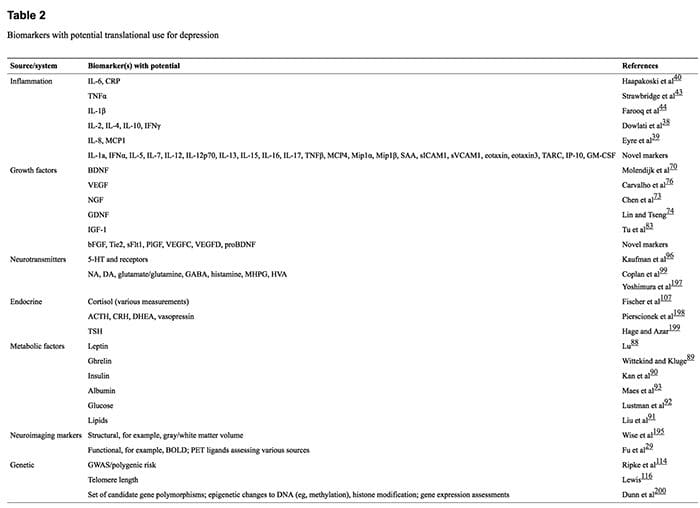
A plethora of research has implicated hundreds of putative biomarkers for depression, but has not yet fully elucidated their roles in depressive illness or established what is abnormal in which patients and how biologic information can be used to enhance diagnosis, treatment and prognosis. This lack of progress is partially due to the nature and heterogeneity of depression, in conjunction with methodological heterogeneity within the research literature and the large array of biomarkers with potential, the expression of which often varies according to many factors. We review the available literature, which indicates that markers involved in inflammatory, neurotrophic and metabolic processes, as well as neurotransmitter and neuroendocrine system components, represent highly promising candidates. These may be measured through genetic and epigenetic, transcriptomic and proteomic, metabolomic and neuroimaging assessments. The use of novel approaches and systematic research programs is now required to determine whether, and which, biomarkers can be used to predict response to treatment, stratify patients to specific treatments and develop targets for new interventions. We conclude that there is much promise for reducing the burden of depression through further developing and expanding these research avenues.
References:
Assessment of patients with chronic pain�E. J. Dansiet and D. C. Turk*t�
Inflammatory biomarkers of low back pain and disc degeneration: a review.
Khan AN1, Jacobsen HE2, Khan J1, Filippi CG3, Levine M3, Lehman RA Jr2,4, Riew KD2,4, Lenke LG2,4, Chahine NO2,5.
Biomarkers for Chronic Neuropathic Pain and their Potential Application in Spinal Cord Stimulation: A Review
Chibueze D. Nwagwu,1 Christina Sarris, M.D.,3 Yuan-Xiang Tao, Ph.D., M.D.,2 and Antonios Mammis, M.D.1,2
Biomarkers for depression: recent insights, current challenges and future prospects. Strawbridge R1, Young AH1,2, Cleare AJ1,2.
These assessment and treatment recommendations represent a synthesis of information derived from personal clinical experience and from the numerous sources which are cited, or are based on the work of researchers, clinicians and therapists who are named (Basmajian 1974, Cailliet 1962, Dvorak & Dvorak 1984, Fryette 1954, Greenman 1989, 1996, Janda 1983, Lewit 1992, 1999, Mennell 1964, Rolf 1977, Williams 1965).
Clinical Application of Neuromuscular Techniques: the Subscapularis Muscle
The subscapularis is a large triangular muscle which fills the subscapular fossa and inserts into the lesser tubercle of the humerus and the front of the capsule of the shoulder-joint.
The subscapularis rotates the head of the humerus medially (internal rotation) and adducts it; when the arm is raised, it draws the humerus forward and downward. It is a powerful defense to the front of the shoulder-joint, preventing displacement of the head of the humerus.
Damage or trauma from an injury or an aggravated condition can cause shortness in the subscapularis muscle. The following assessments and treatments can help improve structure and function.
Assessment of Shortness in the Subscapularis Muscle
Subscapularis shortness test (a) Direct palpation of subscapularis is required to define problems in it, since pain patterns in the shoulder, arm, scapula and chest may all derive from subscapularis or from other sources.
The patient is supine and the practitioner grasps the affected side hand and applies traction while the fingers of the other hand palpate over the edge of latissimus dorsi in order to make contact with the ventral surface of the scapula, where subscapularis can be palpated. There may be a marked reaction from the patient when this is touched, indicating acute sensitivity.
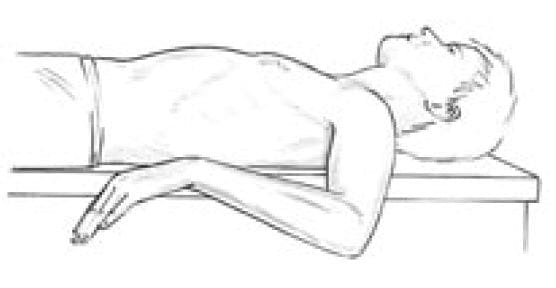
Subscapularis shortness test (b) (as seen on Fig. 4.39 below) The patient is supine with the arm abducted to 90�, the elbow flexed to 90�, and the forearm in external rotation, palm upwards. The whole arm is resting at the restriction barrier, with gravity as its counterweight.
If subscapularis is short the forearm will be unable to rest easily parallel with the floor but will be somewhat elevated.
Figure 4.39A, B Assessment and MET self-treatment position for subscapularis. If the upper arm cannot rest parallel to the floor, possible shortness of subscapularis is indicated.
Care is needed to prevent the anterior shoulder becoming elevated in this position (moving towards the ceiling) and so giving a false normal picture.
Assessment of Weakness in the Subscapularis Muscle
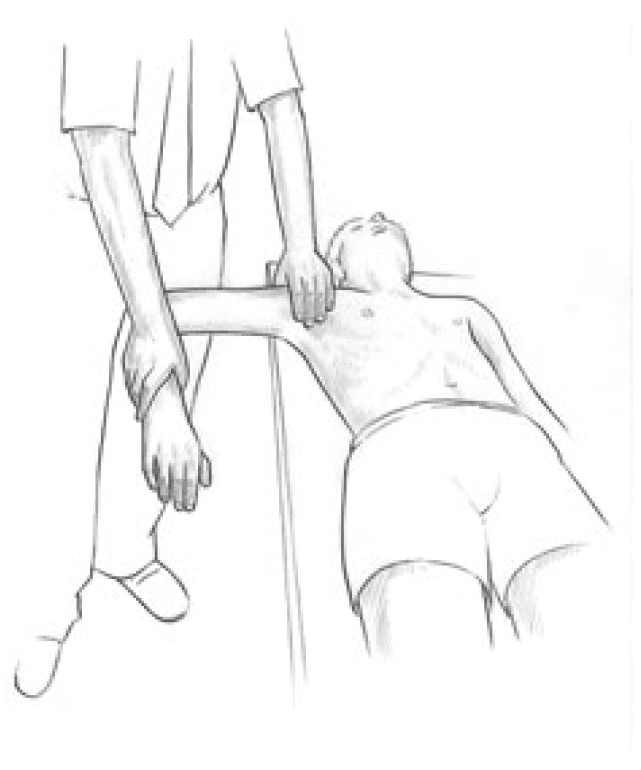
The patient is prone with humerus abducted to 90� and elbow flexed to 90�. The humerus should be in internal rotation so that the forearm is parallel with the trunk, palm towards ceiling. The practitioner stabilises the scapula with one hand and with the other applies pressure to the patient�s wrist and forearm as though taking the humerus towards external rotation, while the patient resists.
The relative strength is judged and the method discussed by Norris (1999) should used to increase strength (isotonic eccentric contraction performed slowly).
MET Treatment of the Subscapularis Muscle
The patient is supine with the arm abducted to 90�, the elbow flexed to 90�, and the forearm in external rotation, palm upwards. The whole arm is resting at the restriction barrier, with gravity as its counterweight. (Care is needed to prevent the anterior shoulder becoming elevated in this position (moving towards the ceiling) and so giving a false normal picture.)
The patient raises the forearm slightly, against minimal resistance from the practitioner, for 7�10 seconds and, following relaxation, gravity or slight assistance from the operator takes the arm into greater external rotation, through the barrier, where it is held for not less than 20 seconds.
Dr. Alex Jimenez offers an additional assessment and treatment of the hip flexors as a part of a referenced clinical application of neuromuscular techniques by Leon Chaitow and Judith Walker DeLany. The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
By Dr. Alex Jimenez
Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.
These assessment and treatment recommendations represent a synthesis of information derived from personal clinical experience and from the numerous sources which are cited, or are based on the work of researchers, clinicians and therapists who are named (Basmajian 1974, Cailliet 1962, Dvorak & Dvorak 1984, Fryette 1954, Greenman 1989, 1996, Janda 1983, Lewit 1992, 1999, Mennell 1964, Rolf 1977, Williams 1965).
Clinical Application of Neuromuscular Techniques: Infraspinatus
Assessment of Shortness in the Infraspinatus
Infraspinatus shortness test (a) The patient is asked to reach upwards, backwards and across to touch the upper border of the opposite scapula, so producing external rotation of the humeral head. If this effort is painful infraspinatus shortness should be suspected.
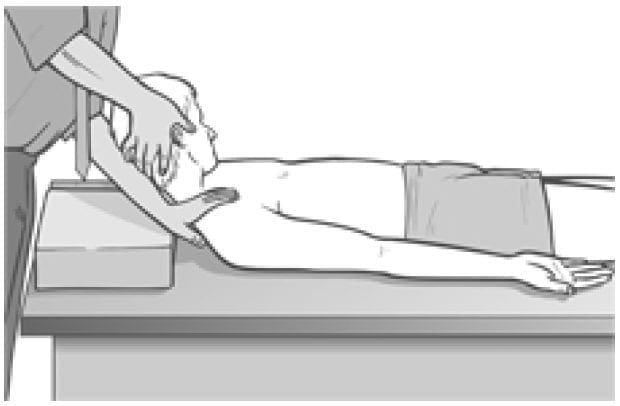
Infraspinatus shortness test (b) (see Fig. 4.37 below) Visual evidence of shortness is obtained by having the patient supine, upper arm at right angles to the trunk, elbow flexed so that lower arm is parallel with the trunk, pointing caudad with the palm downwards. This brings the arm into internal rotation and places infraspinatus at stretch. The practitioner ensures that the shoulder remains in contact with the table during this assessment by means of light compression.
Figure 4.37 Assessment and self-treatment position for infraspinatus. If the upper arm cannot rest parallel to the floor, possible shortness of infraspinatus is indicated.�If infraspinatus is short, the lower arm will not be capable of resting parallel with the floor, obliging it to point somewhat towards the ceiling.
Assessment for Infraspinatus Weakness
The patient is seated. The practitioner stands behind. The patient�s arms are flexed at the elbows and held to the side, and the practitioner provides isometric resistance to external rotation of the lower arms (externally rotating them and also the humerus at the shoulder). If this effort is painful, an indication of probable infraspinatus shortening exists.
The relative strength is also judged. If weak, the method discussed by Norris (1999) should be used to increase strength (isotonic eccentric contraction performed slowly).
NOTE: In this as in other tests for weakness there may be a better degree of cooperation if the practitioner applies the force, and the patient is asked to resist as much as possible. Force should always be built slowly and not suddenly.
MET Treatment of Infraspinatus
Figure 4.38 MET treatment of infraspinatus. Note that the practitioner�s left hand maintains a downward pressure to stabilise the shoulder to the table during this procedure.
The patient is supine, upper arm at right angles to the trunk, elbow flexed so that lower arm is parallel with the trunk, pointing caudad with the palm downwards. This brings the arm into internal rotation and places infraspinatus at stretch.
The practitioner ensures that the posterior shoulder remains in contact with the table by means of light compression. The patient slowly and gently lifts the dorsum of the wrist towards the ceiling, against resistance from the practitioner, for 7�10 seconds.
After this isometric contraction, on relaxation, the forearm is taken towards the floor (combined patient and practitioner action), so increasing internal rotation at the shoulder and stretching infraspinatus (mainly at its shoulder attachment).
Care needs to be taken to prevent the shoulder from rising from the table as rotation is introduced, so giving a false appearance of stretch in the muscle. In order to initiate stretch of infraspinatus at the scapular attachment, the patient is seated with the arm (flexed at the elbow) fully internally rotated and taken into full adduction across the chest. The practitioner holds the upper arm and applies sustained traction from the shoulder in order to prevent subacromial impingement.
The patient is asked to use a light (20% of strength) effort to attempt to externally rotate and abduct the arm, against resistance offered by the practitioner, for 7�10 seconds.
After this isometric contraction, and with the traction from the shoulder maintained, the arm is taken into increased internal rotation and adduction (patient and practitioner acting together) where the stretch is held for at least 20 seconds.
Dr. Alex Jimenez offers an additional assessment and treatment of the hip flexors as a part of a referenced clinical application of neuromuscular techniques by Leon Chaitow and Judith Walker DeLany. The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
By Dr. Alex Jimenez
Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.
These assessment and treatment recommendations represent a synthesis of information derived from personal clinical experience and from the numerous sources which are cited, or are based on the work of researchers, clinicians and therapists who are named (Basmajian 1974, Cailliet 1962, Dvorak & Dvorak 1984, Fryette 1954, Greenman 1989, 1996, Janda 1983, Lewit 1992, 1999, Mennell 1964, Rolf 1977, Williams 1965).
Clinical Application of Neuromuscular Techniques: Levator Scapulae (As Seen on Fig. 4.36 Below)
Assessment of the Levator Scapulae
Levator scapula �springing� test (a) The patient lies supine with the arm of the side to be tested stretched out with the supinated hand and lower arm tucked under the buttocks, to help restrain movement of the shoulder/scapula. The practitioner�s contralateral arm is passed across and under the neck to cup the shoulder of the side to be tested, with the forearm supporting the neck. 11 The practitioner�s other hand supports the head. The forearm is used to lift the neck into full pain-free flexion (aided by the other hand). The head is placed fully towards side-flexion and rotation, away from the side being treated.
Figure 4.36 MET test (a) and treatment position for levator scapula (right side).
With the shoulder held caudally and the head/ neck in the position described (each at its resistance barrier) stretch is being placed on levator from both ends.
If dysfunction exists and/or levator scapula is short, there will be discomfort reported at the attachment on the upper medial border of the scapula and/or pain reported near the levator attachment on the spinous process of C2.
The hand on the shoulder gently �springs� it caudally.
If levator is short there will be a harsh, wooden feel to this action. If it is normal there will be a soft feel to the springing pressure.
Levator scapula observation test (b) A functional assessment involves applying the evidence we have seen (see Ch. 2) of the imbalances which commonly occur between the upper and lower stabilisers of the scapula. In this process shortness is noted in pectoralis minor, levator scapulae and upper trapezius (as well as SCM), while weakness develops in serratus anterior, rhomboids, middle and lower trapezius � as well as the deep neck flexors.
Observation of the patient from behind will often show a �hollow� area between the shoulder blades, where interscapular weakness has occurred, as well as an increased (over normal) distance between the medial borders of the scapulae and the thoracic spine, as the scapulae will have �winged� away from it.
Levator scapula test (c) To see the imbalance described in test (b) in action, Janda (1996) has the patient in the press-up position (see Fig. 5.15). On very slow lowering of the chest towards the floor from a maximum push-up position, the scapula(e) on the side(s) where stabilisation has been compromised will move outwards, laterally and upwards � often into a winged position � rather than towards the spine.
This is diagnostic of weak lower stabilisers, which implicates tight upper stabilisers, including levator scapulae, as inhibiting them.
MET Treatment of Levator Scapula (Fig. 4.36)
Treatment of levator scapulae using MET enhances the lengthening of the extensor muscles attaching to the occiput and upper cervical spine. The position described below is used for treatment, either at the limit of easily reached range of motion, or a little short of this, depending upon the degree of acuteness or chronicity of the dysfunction.
The patient lies supine with the arm of the side to be tested stretched out alongside the trunk with the hand supinated. The practitioner, standing at the head of the table, passes his contralateral arm under the neck to rest on the patient�s shoulder on the side to be treated, so that the practitioner�s forearm supports the patient�s neck. The practitioner�s other hand supports and directs the head into subsequent movement (below).
The practitioner�s forearm lifts the neck into full flexion (aided by the other hand). The head is turned fully into side-flexion and rotation away from the side being treated.
With the shoulder held caudally by the practitioner�s hand, and the head/neck in full flexion, sideflexion and rotation (each at its resistance barrier), stretch is being placed on levator from both ends.
The patient is asked to take the head backwards towards the table, and slightly to the side from which it was turned, against the practitioner�s unmoving resistance, while at the same time a slight (20% of available strength) shoulder shrug is also asked for and resisted.
Following the 7�10 second isometric contraction and complete relaxation of all elements of this combined contraction, the neck is taken to further flexion, sidebending and rotation, where it is maintained as the shoulder is depressed caudally with the patient�s assistance (�as you breathe out, slide your hand towards your feet�). The stretch is held for 20�30 seconds.
The process is repeated at least once.
CAUTION: Avoid overstretching this sensitive area.
Facilitation of Tone in Lower Shoulder Fixators Using Pulsed MET (Ruddy 1962)
In order to commence rehabilitation and proprioceptive re-education of a weak serratus anterior:
The practitioner places a single digit contact very lightly against the lower medial scapula border, on the side of the treated upper trapezius of the seated or standing patient. The patient is asked to attempt to ease the scapula, at the point of digital contact, towards the spine (�press against my finger with your shoulder blade, towards your spine, just as hard [i.e. very lightly] as I am pressing against your shoulder blade, for less than a second�).
Once the patient has learned to establish control over the particular muscular action required to achieve this subtle movement (which can take a significant number of attempts), and can do so for 1 second at a time, repetitively, they are ready to begin the sequence based on Ruddy�s methodology (see Ch. 10, p. 75).
The patient is told something such as �now that you know how to activate the muscles which push your shoulder blade lightly against my finger, I want you to try do this 20 times in 10 seconds, starting and stopping, so that no actual movement takes place, just a contraction and a stopping, repetitively�.
This repetitive contraction will activate the rhomboids, middle and lower trapezii and serratus anterior � all of which are probably inhibited if upper trapezius is hypertonic. The repetitive contractions also produce an automatic reciprocal inhibition of upper trapezius, and levator scapula.
The patient can be taught to place a light finger or thumb contact against their own medial scapula (opposite arm behind back) so that home application of this method can be performed several times daily.
Treatment for Eye Muscles (Ruddy 1962)
Ruddy�s treatment method for the muscles of the eye is outlined in the notes below.
Ruddy�s Treatment for the Muscles of the Eye (Ruddy 1962)
Osteopathic eye specialist Dr T. Ruddy described a practical treatment method for application of MET principles to the muscles of the eye:
The pads of the practitioner�s index, middle and ring finger and the thumb are placed together to form four contacts into which the eyeball (eye closed) can rest (middle finger is above the cornea and the thumb pad below it).
These contacts resist the attempts the patient is asked to make to move the eyes downwards, laterally, medially and upwards � as well as obliquely between these compass points � up and half medial, down and half medial, up and half lateral, down and half lateral, etc.
The fingers resist and obstruct the intended path of eye motion.
Each movement should last for a count �one� and then rest between efforts for a similar count, and in each position there should be 10 repetitions before moving on around the circuit. Ruddy maintained the method released muscle tension, permitted better circulation, and enhanced drainage. He applied the method as part of treatment of many eye problems.
Dr. Alex Jimenez offers an additional assessment and treatment of the hip flexors as a part of a referenced clinical application of neuromuscular techniques by Leon Chaitow and Judith Walker DeLany. The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
By Dr. Alex Jimenez
Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.
These assessment and treatment recommendations represent a synthesis of information derived from personal clinical experience and from the numerous sources which are cited, or are based on the work of researchers, clinicians and therapists who are named (Basmajian 1974, Cailliet 1962, Dvorak & Dvorak 1984, Fryette 1954, Greenman 1989, 1996, Janda 1983, Lewit 1992, 1999, Mennell 1964, Rolf 1977, Williams 1965).
Clinical Application of Neuromuscular Techniques: Sternocleidomastoid (SCM)
Assessment for Shortness of Sternocleidomastoid�(see also Box 4.10)
Assessment for SCM is as for the scalenes � there is no absolute test for shortness but observation of posture (hyperlordotic neck, chin poked forward) and palpation of the degree of induration, fibrosis and trigger point activity can all alert to probable shortness of SCM. This is an accessory breathing muscle and, like the scalenes, will be shortened by inappropriate breathing patterns which have become habitual. Observation is an accurate assessment tool.
Box 4.10 Notes on Sternocleidomastoid
Sternocleidomastoid (SCM) is a prominent muscle of the anterior neck and is closely associated with the trapezius. SCM often acts as postural compensator for head tilt associated with postural distortions found elsewhere (spinal, pelvic or lower extremity functional or structural inadequacies, for instance) although they seldom cause restriction of neck movement.
SCM is synergistic with anterior neck muscles for flexion of the head and flexion of the cervical column on the thoracic column, when the cervical column is already flattened by the prevertebral muscles. However, when the head is placed in extension and SCM contracts, it accentuates lordosis of the cervical column, flexes the cervical column on the thoracic column, and adds to extension of the head. In this way, SCM is both synergist and antagonist to the prevertebral muscles (Kapandji 1974).
SCM trigger points are activated by forward head positioning, �whiplash� injury, positioning of the head to look upwardly for extended periods of time and structural compensations. The two heads of SCM each have their own patterns of trigger point referral which include (among others) into the ear, top of head, into the temporomandibular joint, over the brow, into the throat, and those which cause proprioceptive disturbances, disequilibrium, nausea and dizziness. Tenderness in SCM may be associated with trigger points in the digastric muscle and digastric trigger points may be satellites of SCM trigger points (Simons et al 1998).
Simons et al (1998) report: When objects of equal weight are held in the hands, the patient with unilateral trigger point [TrP] involvement of the clavicular division [of SCM] may exhibit an abnormal Weight Test. When asked to judge which is heaviest of two objects of the same weight that look alike but may not be the same weight (two vapocoolant dispensers, one of which may have been used) the patient will [give] evidence [of] dysmetria by underestimating the weight of the object held in the hand on the same side as the affected sternocleidomastoid muscle. Inactivation of the responsible sternocleidomastoid TrPs promptly restores weight appreciation by this test. Apparently, the afferent discharges from these TrPs disturb central processing of proprioceptive information from the upper limb muscles as well as vestibular function related to neck muscles.
Lymph nodes lie superficially along the medial aspect of the SCM and may be palpated, especially when enlarged. These nodes may be indicative of chronic cranial infections stemming from a throat infection, dental abscess, sinusitis or tumour. Likewise, trigger points in SCM may be perpetuated by some of these conditions (Simons et al 1998).
Lewit (1999) points out that tenderness noted at the medial end of the clavicle and/or at the transverse process of the atlas is often an indication of SCM hypertonicity. This will commonly accompany a forward head position and/or tendency to upper chest breathing, and will almost inevitably be associated with hypertonicity, shortening and trigger point evolution in associated musculature, including scalenes, upper trapezius and levator scapula (see crossed syndrome notes in Ch. 2).
Since SCM is only just observable when normal, if the clavicular insertion is easily visible, or any part of the muscle is prominent, this can be taken as a clear sign of tightness of the muscle.�If the patient�s posture involves the head being held forward of the body, often accompanied by cervical lordosis and dorsal kyphosis (see notes on upper crossed syndrome in Ch. 2), weakness of the deep neck flexors and tightness of SCM is suspected.
Functional SCM Test (see Fig. 5.14A, B)
The supine patient is asked to �very slowly raise your head and touch your chin to your chest�. The practitioner stands to the side with his head at the same level as the patient. At the beginning of the movement of the head, as the patient lifts this from the table, the practitioner would (if SCM were short) note that the chin was lifted first, allowing it to jut forwards, rather than the forehead leading the arc-like progression of the movement. In marked shortness of SCM the chin pokes forward in a jerk as the head is lifted. If the reading of this sign is unclear then Janda (1988) suggests that a slight resistance pressure be applied to the forehead as the patient makes the �chin to chest� attempt. If SCM is short this will ensure the jutting of the chin at the outset.
MET Treatment of Shortened SCM (Fig. 4.35)
The patient is supine with the head supported in a neutral position by one of the practitioner�s hands. The shoulders rest on a cushion or folded towel, so that when the head is placed on the table it will be in slight extension. The patient�s contralateral hand rests on the upper aspect of the sternum to act as a cushion when pressure is applied during the stretch phase of the operation (as in scalene and pectoral treatment). The patient�s head is fully but comfortably rotated, contralaterally.
Figure 4.35 MET of sternocleidomastoid on the right.
The patient is asked to lift the fully rotated head a small degree towards the ceiling, and to hold the breath. When the head is raised there is no need for the practitioner to apply resistance as gravity effectively provides this.
After 7�10 seconds of isometric contraction (ideally with breath held), the patient is asked to slowly release the effort (and the breath) and to place the head (still in rotation) on the table, so that a small degree of extension occurs.
The practitioner�s hand covers the patient�s �cushion� hand (which rests on the sternum) in order to apply oblique pressure/stretch to the sternum, to ease it away from the head and towards the feet.
The hand not involved in stretching the sternum caudally should gently restrain the tendency the head will have to follow this stretch, but should not under any circumstances apply pressure to stretch the head/neck while it is in this vulnerable position of rotation and slight extension.
The degree of extension of the neck should be slight, 10�15� at most.
This stretch, which is applied as the patient exhales, is maintained for not less than 20 seconds to begin the release/stretch of hypertonic and fibrotic structures. Repeat at least once. The other side should then be treated in the same manner.
CAUTION: Care is required, especially with middle aged and elderly patients, in applying this useful stretching procedure. Appropriate tests should be carried out to evaluate cerebral circulation problems. The presence of such problems indicates that this particular MET method should be avoided.
Dr. Alex Jimenez offers an additional assessment and treatment of the hip flexors as a part of a referenced clinical application of neuromuscular techniques by Leon Chaitow and Judith Walker DeLany. The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
By Dr. Alex Jimenez
Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine





 References:
References: