Can understanding the mechanics of the throwing motion help to understand why it may cause shoulder pain, the symptoms of a shoulder problem, the diagnosis, and the treatment options available?
Throwing a Ball and Shoulder Pain
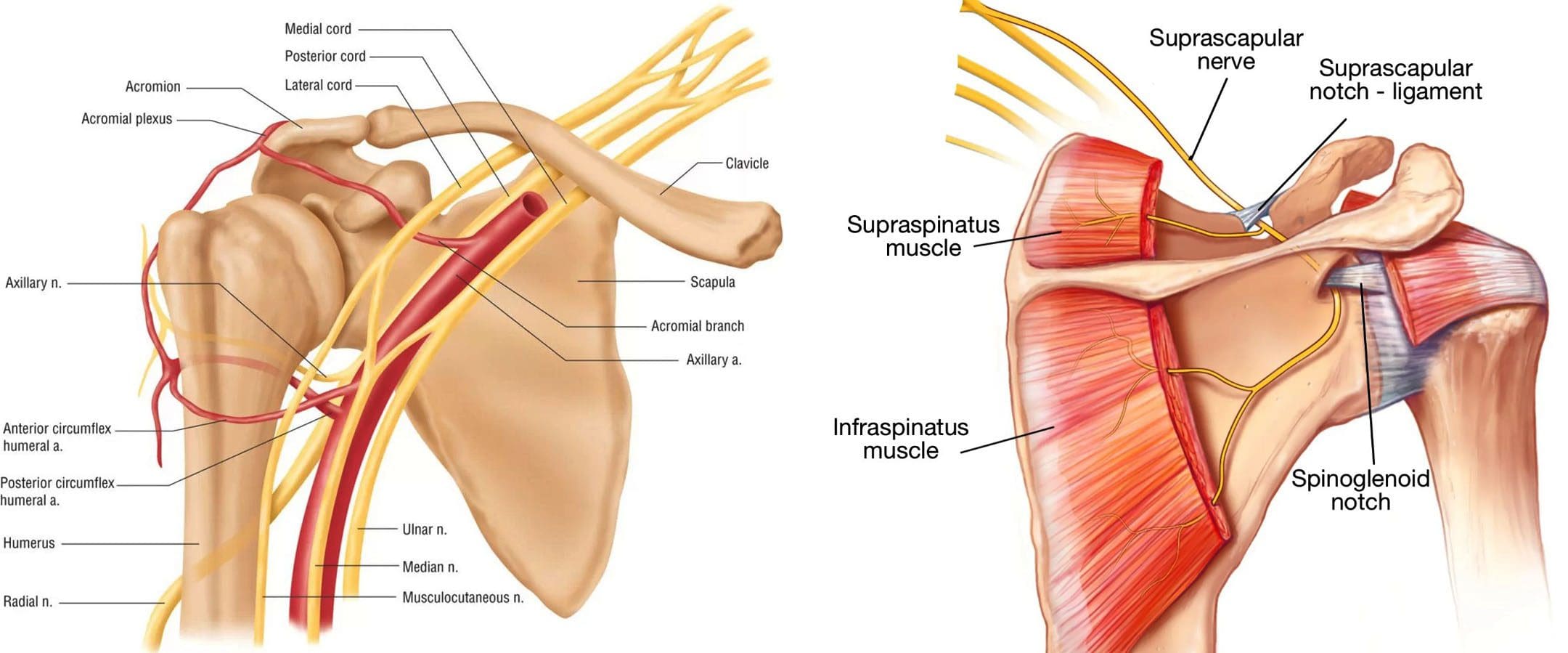
The throwing motion is a complex shoulder movement that requires the mechanics of muscles, tendons, joints, ligaments, and bones. They all must move in a synchronized and stable pattern to move the shoulder joint. When these mechanics are interrupted or altered, inflammation can result in pain symptoms. (Wardell M., Creighton D., & Kovalcik C., 2022)
The labrum stabilizes the ball in the socket of the shoulder.
The shoulder blade rotation coordinates with the arm to ensure mobility. (Itoigawa Y. et al., 2023)
The throwing motion generates high torque and acceleration forces acting on the shoulder joint and the surrounding muscles, ligaments, and tendons.
Causes of Pain
Pain when throwing can come from the:
Shoulder blade
Shoulder joint – cartilage and labrum
Rotator cuff muscles and tendons
Nerves that control the muscles’ function
The shoulder blade is attached to the upper back by ligaments, muscles, and tendons. The various muscles and tendons that control the movement of the shoulder blade impact movements. Abnormalities of any area can lead to shoulder dysfunction and pain when throwing. (Wardell M., Creighton D., & Kovalcik C., 2022) The most common is the tightness of the posterior shoulder capsule, causing a loss of normal internal rotation of the shoulder. If this is causing pain, individuals may notice that they can’t reach up as high on the side with the painful shoulder when reaching behind their back.
Symptoms
Whether an athlete or playing catch in the backyard, shoulder function abnormalities can cause significant pain. Some symptoms include.
Aching Pain
Often deep in the shoulder or extending down the upper arm.
Dead Arm
Lack of strength in the throwing motion.
Pain at Night
Pain can awaken you from sleep.
Diagnosis
Finding a healthcare provider familiar with sports injuries can be helpful. They can best determine if a structural abnormality needs to be addressed. (American Academy of Orthopaedic Surgeons, 2021)
Treatment
Most can improve with nonsurgical treatments. The earliest phase of treatment is resting the joint and reducing inflammation. Treatments can include:
Ice
Anti-inflammatory medications
Cortisone injection
Once the inflammation has subsided, the source of the discomfort can be addressed.
Physical Therapy
Therapy can include:
A structured shoulder stretching and strengthening program will help.
The physical therapist will focus on scapular mobility when managing shoulder joint problems.
Stretching to improve internal rotation or any other lost motion can help allow a more normal throwing motion.
Strength exercises are often aimed at the rotator cuff, as these muscles initiate proper shoulder movements and stabilize the shoulder joint.
Maintaining flexibility and strength of the periscapular muscles (muscles that attach to the scapula bone) is important to ensure that the scapular movements are coordinated with the throwing motion.
If improvements are not made within three months of therapy, or individuals can’t return to competitive sports within six months. In that case, the individual may need to return to their healthcare provider or see an orthopedic specialist who may recommend surgery. (American Academy of Orthopaedic Surgeons, 2024)
Injury Medical Chiropractic and Functional Medicine Clinic
As a Family Practice Nurse Practitioner, Dr. Jimenez combines advanced medical expertise with chiropractic care to address various conditions.
Wellness & Nutrition: Personalized plans to optimize health and prevent disease.
Chronic Pain Management: Non-invasive solutions for fibromyalgia, sciatica, and low back pain.
Personal Injury & Auto Accident Care: Tailored rehabilitation for whiplash, soft tissue injuries, and more.
Sports Injuries & Orthopedic Care: Treatment for sprains, strains, and complex injuries.
Functional Medicine: Root-cause analysis for chronic disorders, incorporating nutrition, lifestyle, and environmental factors.
Neuromusculoskeletal Health: Care for neck pain, migraines, herniated discs, and scoliosis.
Our clinic integrates Functional Medicine, Acupuncture, Electro-Acupuncture, and Sports Medicine to create customized care plans that promote natural healing, mobility, and long-term wellness. By focusing on flexibility, agility, and strength, we empower patients to thrive, regardless of age or health challenges.
At El Paso’s Chiropractic Rehabilitation Clinic & Integrated Medicine Center, we passionately focus on treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility, and agility programs tailored for all age groups and disabilities. We use in-person and virtual health coaching and comprehensive care plans to ensure every patient’s personalized care and wellness outcomes.
Lumbar Spine Injuries in Sports: Chiropractic Healing
References
Wardell, M., Creighton, D., & Kovalcik, C. (2022). Glenohumeral Instability and Arm Pain in Overhead Throwing Athletes: A Correlational Study. International journal of sports physical therapy, 17(7), 1351–1357. https://doi.org/10.26603/001c.39800
Itoigawa, Y., Koga, A., Morikawa, D., Kubota, A., Uehara, H., Maruyama, Y., Takazawa, Y., & Ishijima, M. (2023). Posterior shoulder stiffness was associated with shoulder pain during throwing in college baseball players: assessment of shear wave elastography. European journal of orthopaedic surgery & traumatology: orthopedie traumatologie, 33(4), 1237–1244. https://doi.org/10.1007/s00590-022-03286-z
American Academy of Orthopaedic Surgeons. (2021). Shoulder Injuries in the Throwing Athlete. https://orthoinfo.aaos.org/en/diseases–conditions/shoulder-injuries-in-the-throwing-athlete/
American Academy of Orthopaedic Surgeons. (2024). Shoulder Impingement/Rotator Cuff Tendinitis. https://orthoinfo.aaos.org/en/diseases–conditions/shoulder-impingementrotator-cuff-tendinitis
Triceps tendonitis can be frustrating, especially when you need to rest from normal activities. Can knowing the causes, symptoms, and diagnosis help individuals understand the treatment and prevention of the condition?
Triceps Tendonitis
Tendons are connective tissue that attach muscles to bones, enabling the joints to move. Triceps tendonitis is inflammation of the tendon at the back of the elbow. It is most often caused by overuse of the triceps muscles. The condition can cause pain, swelling, and loss of function. It’s common in jobs that require regular hammering, shoveling, and overhead reaching, as well as in weightlifters, gymnasts, and boxers.
Causes
The triceps muscle runs along the back of the upper arm and is attached to the point of the elbow by a tendon. This muscle straightens the elbow. Tendonitis develops from repeatedly straightening the elbow against resistance. This causes tiny tears in the tissue, which leads to inflammation. Triceps tendonitis commonly occurs from repetitive manual labor tasks or sports activities like throwing sports, gymnastics, or boxing. Exercises that target the triceps muscle can cause tendonitis to develop, including kickbacks, dips, push-ups, and bench presses. For this reason, triceps tendonitis is also known as weightlifter’s elbow. (Orthopedic & Spine Center, N.D.)
Symptoms
Inflammation leads to a series of chemical reactions in the area of the injury. There are five main symptoms of inflammation:
Redness
Warmth
Swelling
Pain
Loss of function
With triceps tendonitis, the pain and stiffness are felt at the back of the elbow. Weakness may also present when using the affected arm. Tendonitis usually causes more pain with movement than when resting. Pain can occur when straightening the elbow, which puts tension on the triceps, or bending the elbow, which stretches the tendon.
Diagnosis
A healthcare provider will ask questions and perform a physical exam to diagnose tendonitis. (Harvard Health Publishing, 2014) A healthcare provider will ask you to describe the pain and the activities that make it better or worse. The elbow will be assessed for movement issues, swelling, or deformities that could indicate a worse injury, like a tendon tear. A healthcare provider will order X-rays or other imaging, such as MRI, to assess for a bone fracture or more extensive damage to the tendon.
Treatment
Several types of treatments include self-care, physical therapy, and medications.
Self Care
Triceps tendonitis can be treated at home if symptoms are addressed early. These include:
Rest
Rest the triceps tendon by avoiding activities that cause pain for a few days.
Ice
Apply ice to the triceps tendon for 15 to 20 minutes, two to three times daily.
Massage the area with an ice cube for several minutes.
Range of Motion Exercises
Decrease stiffness in the elbow with gentle range of motion exercises.
Slowly bend and straighten the elbow in a pain-free range, 10 times.
Repeat several times per day.
Physical Therapy
Physical therapists use various therapies and tools when treating tendonitis, including (Prall J. & Ross M. 2019)
PT Modalities
Physical therapy modalities are used to decrease pain, inflammation, and stiffness.
Examples include ultrasound, electrical stimulation, and light therapy.
Manual Therapy
Manual techniques for tendonitis include soft tissue massage, friction massage, stretching, and joint mobilization.
Exercise
Stretching and strengthening exercises that target the triceps muscle and any other muscle weakness that might have contributed to the condition.
Activity Modification
A therapist will look at the activities that led to the tendonitis and ensure you use the correct form and proper body mechanics.
Sometimes, a physical therapist can make on-site changes in the work environment to help prevent further injury.
Nonsteroidal anti-inflammatory medications are often used to treat tendonitis.
Many are available over-the-counter, including Aleve, Bayer, and Advil.
These medications can also be prescribed in higher doses by a healthcare provider.
Pain-Relievers
Additional over-the-counter medications such as Tylenol can help decrease pain.
Oral Steroids
These medications might be prescribed for short-term use to decrease inflammation if over-the-counter medications are ineffective in treating symptoms.
Tendonitis is frequently treated with an injection of steroid medication to decrease inflammation.
However, having multiple injections in the same area can eventually cause tendons to weaken more. (NYU Langone Health, 2024)
Platelet-Rich Plasma
PRP is made by taking a small amount of blood and separating the platelets or cells that release growth factors to promote healing.
The liquid is then injected into the tendon.
PRP is controversial; some studies support its use, while others do not.
While PRP may show some promise, insurance may not cover PRP treatments because of the ambiguity in the clinical data.
Injury Medical Chiropractic and Functional Medicine Clinic
Prevention is key. Warming up before a workout, stretching, and using the proper form can help prevent triceps tendonitis. Temporarily halting activities to address symptoms can prevent more serious injury. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to build optimal health and wellness solutions. We focus on what works for you to relieve pain, restore function, prevent injury, and help mitigate issues through adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal problems.
Harvard Health Publishing. (2014). Tendonitis. https://www.health.harvard.edu/diseases-and-conditions/tendonitis
Prall, J., & Ross, M. (2019). The management of work-related musculoskeletal injuries in an occupational health setting: the role of the physical therapist. Journal of Exercise Rehabilitation, 15(2), 193–199. https://doi.org/10.12965/jer.1836636.318
Aurora Health Care. (2025). Tendonitis symptoms & treatment. https://www.aurorahealthcare.org/services/orthopedics/conditions/tendonitis
Spoendlin, J., Meier, C., Jick, S. S., & Meier, C. R. (2015). Oral and inhaled glucocorticoid use and risk of Achilles or biceps tendon rupture: a population-based case-control study. Annals of Medicine, 47(6), 492–498. https://doi.org/10.3109/07853890.2015.1074272
NYU Langone Health. (2024). Therapeutic injections for bursitis & tendinitis in adults. https://nyulangone.org/conditions/bursitis-tendinitis/treatments/therapeutic-injections-for-bursitis-tendinitis
Could older individuals who do not have symptoms of shoulder pain or loss of shoulder and arm function have a rotator cuff tear?
Rotator Cuff Tear Physical Therapy
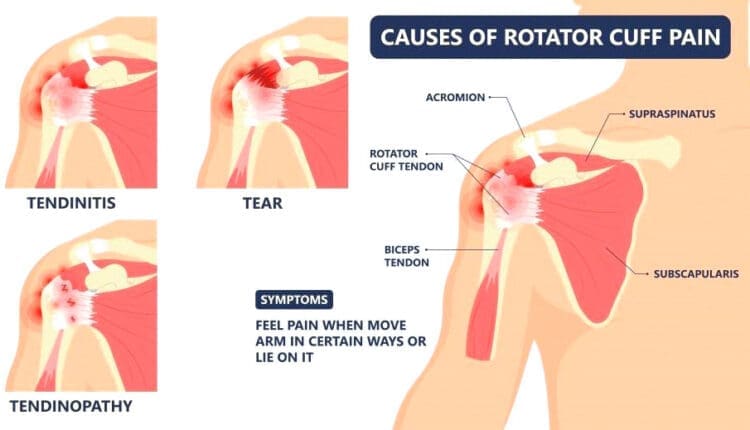
A rotator cuff tear is a common injury to the four muscles and tendons surrounding and stabilizing the shoulder joint. Studies have shown that (Geary M. B., & Elfar J. C. 2015)
30% of those under the age of 70
70% of those over age 80 have a rotator cuff tear.
Physical therapy is often recommended as a first-line initial treatment for rotator cuff pain. In most cases, a rotator cuff tear will not need surgical treatment. Determining when surgery is necessary depends on several factors a patient can discuss with their healthcare provider.
Causes
Overuse and repetitive motions
Trauma (e.g., falls, collisions)
Age-related degeneration
Symptoms
Shoulder pain, especially with overhead or rotational movements
Weakness and difficulty raising the arm
Clicking or grinding sounds in the shoulder
Limited range of motion
Treatment
The goal of physical therapy for a rotator cuff tear is not necessarily to heal the torn tendon but to relieve pain and improve strength by reducing inflammation and restoring shoulder joint mechanics. This is achieved through physical therapy, ice application, anti-inflammatory treatments like medications, and cortisone injections.
Physical Therapy
The goal of physical therapy is to improve the function of the muscles that surround the shoulder. Physical therapy targets the smaller muscles around the shoulder that are commonly neglected. By strengthening these muscles, the treatment can help compensate for damaged tendons and improve the mechanics of the shoulder joint. A chiropractic physical therapy team will develop a personalized exercise program. Generally, rehabilitation will start with gentle range of motion exercises that can be accomplished using the arms to lift a mobility stick/wand overhead.
Shoulder Pulleys
These improve shoulder range of motion and flexibility.
Isometric Exercises
These exercises are for the rotator cuff muscles and may then be started.
This exercise can improve the contracting of the muscles around the shoulder and offer more support to the shoulder joint.
Scapular Stabilization Exercises
These can also be done to improve the muscles surrounding the shoulder blade’s function.
This can help improve how the shoulder joint, arm, and scapulae move together when using the arm.
Advanced Strengthening
Advanced exercises can be done with a dumbbell or resistance band.
Consult your healthcare provider or physical therapist before starting these or any other exercises for a rotator cuff tear. Doing exercises correctly prevents further pain, injury, or shoulder problems. Specific, focused exercises can help expedite and regain normal shoulder function.
Injury Medical Chiropractic and Functional Medicine Clinic
The prognosis for rotator cuff tears depends on the severity of the tear and the individual’s overall health. With proper treatment, most people can regain the full function of their shoulders. However, some may experience ongoing pain or limitations in severe cases. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to build optimal health and wellness solutions. We focus on what works for you to relieve pain, restore function, prevent injury, and help mitigate issues through adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal problems.
Shoulder Pain Chiropractic Treatment
References
Geary, M. B., & Elfar, J. C. (2015). Rotator Cuff Tears in the Elderly Patients. Geriatric orthopaedic surgery & rehabilitation, 6(3), 220–224. https://doi.org/10.1177/2151458515583895
Can understanding the anatomy and function of the long thoracic nerve help individuals make informed healthcare decisions after an injury to the nerve?
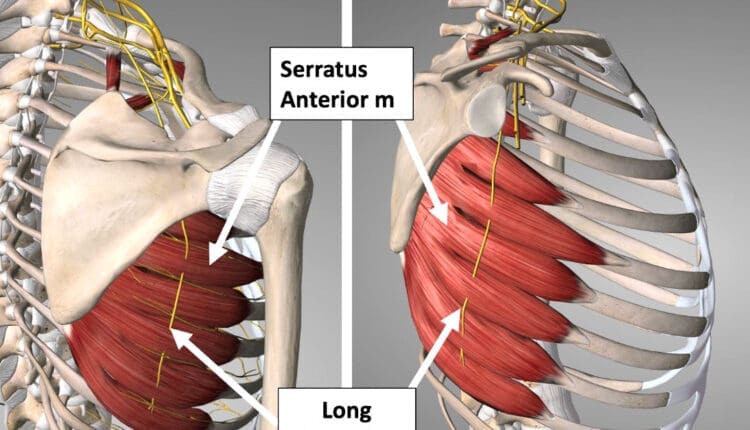
Long Thoracic Nerve
Also referred to as the posterior thoracic nerve, the long thoracic nerve/LTN is a thin superficial nerve that runs from the cervical spine to the chest wall side of the trunk. It supplies motor function to the thorax’s serratus anterior muscle, helping stabilize the shoulder blade. Injury to this nerve can cause limited or abnormal shoulder and shoulder blade motion, including difficulty raising the arm during overhead reaching.
Anatomy
The long thoracic nerve originates from the ventral rami of cervical nerves C5, C6, and C7. (Waxenbaum JA, Reddy V, Bordoni B. 2023) In some individuals, the root from C7 is absent; in others, a small nerve root branches from C8. The nerve roots from C5 and C6 go through the medial scalene muscle to join the C7 nerve. It travels behind the brachial plexus axillary artery and vein and courses down the lateral side of the thorax. The long thoracic nerve terminates at the lower portion of the serratus anterior muscle, sending small nerve tendrils to each muscle’s projections, which attach to the ribs. Because the long thoracic nerve is located on the lateral side of the chest, it is vulnerable to injury during sports or surgical procedures. The nerve also has a smaller diameter than other cervical and brachial plexus nerves, which increases its potential for injury.
Function
The long thoracic nerve attaches to the underside of the shoulder blade and inserts as muscular slips into the ribs. It supplies motor function to the serratus anterior muscle, essential for normal shoulder motion. When it contracts, it pulls the shoulder blade against the ribs and thorax, helping to move and stabilize the arm as it moves forward and up during shoulder motions. Injury to the long thoracic nerve causes a condition called scapular winging. This occurs when the serratus anterior muscle becomes weakened or paralyzed after injury. (Lung K, St Lucia K, Lui F. 2024)
Susceptibility to Injury
The LTN is relatively unprotected and can be damaged by several things, including:
Heavy backpacks
Sports
Activities the body is not used to, like digging
Using crutches
Conditions
Injury to the long thoracic nerve may occur as a result of trauma, lifting heavy weights above the shoulder, or a surgical procedure. Surgical procedures that may place the nerve at risk for injury may include: (Lung K, St Lucia K, Lui F. 2024)
Axillary lymph node dissection
Improperly placed intercostal drains
Chest tube placements
Mastectomy
Thoracotomy
The long thoracic nerve is protected during these procedures by the surgeon and proper surgical technique, but occasionally, difficulties arise during surgery, and the nerve may become injured. Individuals may also have an anatomical variance that places their nerves in varying positions. The surgeon may not see it and accidentally injure their nerves during surgery.
The superficial long thoracic nerve may also be injured during sports or trauma to the trunk. A blow to the side or a sudden overhead stretch to the shoulder may be enough to damage the nerve, paralyzing the serratus anterior muscle.
Weakness or paralysis of the serratus anterior muscle will result in a winged scapula. To test for this:
Stand about two feet from a wall, facing it.
Place both hands on the wall and gently push against it.
If one of the shoulder blades sticks out abnormally, it could be a winged scapula.
Have a family member or friend stand behind you and check the shoulder blade position.
If you suspect a winged scapula, visit a physician who can assess the condition and determine if there is a long thoracic nerve injury.
Winging the scapula may result in difficulty lifting the arm overhead. The serratus anterior muscle works with other scapular stabilizers, such as the upper trapezius and levator scapula, to properly position the shoulder blade when lifting the arm. Failure of the serratus to stabilize the shoulder blade may make lifting the arm impossible.
Clinical examination is usually used to diagnose a long thoracic nerve injury. X-rays and MRIs cannot show the nerve injury directly, although an MRI can show some secondary signs to help confirm the diagnosis. An electromyographic or EMG test may also be performed to examine the function of the long thoracic nerve.
Treatment and Rehabilitation
Treatment for LTN pain and reduced movement may include:
Rest
Heat or ice
Anti-inflammatory pain medication
Neck support or a pillow
Avoiding strenuous activity and driving
If the long thoracic nerve is severely injured and the serratus anterior is completely paralyzed, the best course of action is to be active and monitor the condition. Full recovery of arm function can take one to two years. If permanent nerve injury has occurred, surgery may be an option to restore shoulder motion and function. Several different kinds of surgery can be used to address winged scapula. (Vetter M. et al., 2017)
One involves transferring the pectoralis major tendon to the scapula (Vetter M. et al., 2017) so it functions as the serratus.
Often, the tendon has to be lengthened, which may be done using part of the hamstring tendon.
After surgery, individuals will likely wear a sling on their arm for a few weeks, and then gentle range-of-motion exercises will be initiated.
After eight to ten weeks, gentle progressive strengthening of the new tendon can begin.
Full shoulder motion and strength recovery are expected six to 12 months after surgery.
Lie on your back and raise both arms toward the ceiling.
Make a fist and punch up toward the ceiling.
Ensure the motion is steady and deliberate, and keep the elbow straight.
Hold the position for three seconds, then slowly lower the arm to the starting position.
Perform 10 to 15 repetitions.
Holding a small dumbbell in your hands can make the exercise more challenging.
Pushup
Lie on your stomach and place your hands flat on the ground by your shoulders as if you were going to perform a pushup.
Perform a pushup and press further, allowing the shoulder blades to wrap around the thorax.
Hold this position for three seconds, and slowly release.
Perform 10 to 15 reps.
If this is too difficult, perform the pushup against a wall to reduce the effect of gravity on the exercise.
Scapular Winging in Depth
References
Waxenbaum, J. A., Reddy, V., & Bordoni, B. (2024). Anatomy, Head and Neck: Cervical Nerves. In StatPearls. https://www.ncbi.nlm.nih.gov/pubmed/30844163
Lung, K., St Lucia, K., & Lui, F. (2024). Anatomy, Thorax, Serratus Anterior Muscles. In StatPearls. https://www.ncbi.nlm.nih.gov/pubmed/30285352
Vetter, M., Charran, O., Yilmaz, E., Edwards, B., Muhleman, M. A., Oskouian, R. J., Tubbs, R. S., & Loukas, M. (2017). Winged Scapula: A Comprehensive Review of Surgical Treatment. Cureus, 9(12), e1923. https://doi.org/10.7759/cureus.1923
Berthold, J. B., Burg, T. M., & Nussbaum, R. P. (2017). Long Thoracic Nerve Injury Caused by Overhead Weight Lifting Leading to Scapular Dyskinesis and Medial Scapular Winging. The Journal of the American Osteopathic Association, 117(2), 133–137. https://doi.org/10.7556/jaoa.2017.025
An axillary nerve injury can cause pain, weakness, and shoulder mobility loss. Can physical therapy help restore and maintain shoulder joint flexibility?
Axillary Nerve
The axillary nerve, or the circumflex nerve, is a peripheral nerve that runs through the shoulder and supports movement and sensation in the upper limbs. It originates in the neck at the brachial plexus, a network of nerves that extends from the neck and upper torso to the shoulders and arms. Its primary purpose is to supply nerve function to the shoulder joint and three muscles in the arm and also innervates some skin in the region.
Anatomy
Except for the cranial nerves, all the body’s nerves branch off from the spinal cord, emerge from between vertebrae and continue to branch off as they travel to various muscles and other structures. The axillary nerve is named after the axilla, the medical name for the armpit. Individuals have two, one on each side. After leaving the spinal column, the axillary nerve runs behind the axillary artery and continues to the shoulder blade’s lower edge of the subscapularis muscle. It winds back and travels down the arm along the posterior humeral circumflex artery, which then passes through the quadrangular space (a small area of the shoulder blade just above the armpit where there is a gap in the muscles that allows nerves and blood vessels to pass through to the arm before it divides into terminal branches, which are:
Anterior Division
Supplies motor innervation to the deltoid’s anterior and middle heads, allowing the arm to abduct or move away from the body.
It winds around the neck of the humerus/funny bone, goes beneath the deltoid muscle, and then connects to the forward edge of the deltoid.
A few small cutaneous branches serve the skin in that area.
Posterior Division
Innervates the teres minor muscles and the lower part of the deltoid.
It enters the deep fascia and becomes the superior lateral cutaneous nerve.
It then wraps around the lower edge of the deltoid, connects to the skin over the lower two-thirds of the muscle, and covers the long head of the triceps brachii.
Articular Branch
Comes from the trunk of the axillary nerve and enters the glenohumeral joint, which is in the shoulder, below the subscapularis muscle.
Anatomical Variations
In a case report, healthcare providers noted an incidence of the nerve branching directly off the upper trunk of the brachial plexus rather than the posterior cord. (Subasinghe S. K. and Goonewardene S. 2016) In this case, it innervated the subscapularis muscle, latissimus dorsi, and the deltoid and teres minor muscles and also had a communicating branch to the posterior cord. Another case documented multiple abnormalities in the course of the axillary nerve in an individual with pain and severely limited shoulder mobility. (Pizzo R. A. et al., 2019) During reverse shoulder arthroplasty, the surgeon discovered that the axillary nerve ran beside the coracoid process instead of underneath and stayed close to the subscapularis muscle instead of traveling through the quadrangular space. The case noted earlier reports of axillary nerves not running through the quadrangular space. In those cases, the nerve pierced the subscapularis muscle or split into branches before reaching the quadrangular space.
Function
The axillary nerve functions as a motor nerve that controls movement and a sensory nerve that controls sensations like touch or temperature.
Motor
As a motor nerve, the axillary nerve innervates three muscles in the arm and includes:
Deltoid
Allows flexing of the shoulder joint and rotating the shoulder inward.
Long Head of the Triceps
It runs down the back of the outer arm, allowing straightening, pulling the upper arm toward the body, or extending it backward.
The radial nerve can also innervate this muscle.
Teres Minor
One of the rotator cuff muscles starts outside the shoulder and runs diagonally along the bottom edge of the shoulder blade.
It works with other muscles to allow for the external rotation of the shoulder joint.
Sensory
In its sensory role, the nerve carries information to the brain from the following:
Glenohumeral joint or the ball-and-socket joint in the shoulder.
The skin on the lower two-thirds of the deltoid muscle through the superior lateral cutaneous branch.
Injuries and Conditions
Problems with the axillary nerve can be caused by injuries anywhere along the arm and shoulder and by disease. Common injuries include:
Dislocations
Of the shoulder joint, which can cause axillary nerve palsy.
Fracture
Of the surgical neck of the humerus.
Compression
This stems from walking with crutches, also known as crutch palsy.
Direct Trauma
This can be from an impact sports, work, automobile accident, collision, or laceration.
Added Pressure
This can be from wearing a cast or splint.
Surgical Accidental Injury
An injury or damage can come from shoulder surgery, especially arthroscopic surgery on the inferior glenoid and capsule.
Quadrangular Space Syndrome
This is where the axillary nerve is compressed where it passes through that space, which is most common in athletes who perform frequent overhead motions)
Nerve Root Damage
Between the fifth and sixth cervical vertebrae, where the nerve emerges from the spinal cord, which can be caused by traction, compression, spinal disc prolapse, or a bulging disc.
Systemic Neurological Disorders
Example – multiple sclerosis
Erb’s Palsy
A condition often is the result of a birth injury called shoulder dystocia, in which a baby’s shoulder/s becomes stuck during childbirth.
Axillary Nerve Palsy
Damage can result in a type of peripheral neuropathy that can cause weakness in the deltoid and teres minor muscles.
This can result in losing the ability to lift the arm away from the body and weakness in various shoulder movements.
If the damage is severe enough, it can cause paralysis of the deltoid and other minor muscles, resulting in flat shoulder deformity, in which individuals cannot lay their shoulders flat when lying down.
Axillary nerve damage also can lead to a change, reduction, or loss of sensation in a small part of the arm just below the shoulder.
Nerve Injury Statistics
Three times more common in men than women.
It may be present in as many as 65% of shoulder injuries.
The risk of injury due to dislocation is significantly increased after age 50.
Tests
If a healthcare provider suspects a problem with axillary nerve function, they’ll test the shoulder’s range of motion and skin sensitivity. A difference in the range of motion between the shoulders can indicate a nerve injury. Individuals may be sent for electromyography and a nerve conduction study to verify nerve palsy. In some cases, an MRI and/or X-rays may be ordered, especially if the cause of possible nerve damage is unknown.
Rehabilitation
Depending on the severity and cause of the injury, non-surgical treatments may be recommended, with surgery as a last resort. Non-surgical treatment can include some combination of immobilization, rest, ice, physical therapy, and anti-inflammatory meds. Physical treatment typically lasts about six weeks and focuses on strengthening and stimulating the muscles to prevent joint stiffness, which can impair long-term function.
Surgery
If conservative treatments don’t work, surgery may be recommended, especially if several months have passed without improvement. Surgical outcomes are generally better if surgery is performed within six months of the injury, and regardless of the time frame, the prognosis is considered positive in about 90% of cases. Surgical procedures performed for axillary nerve dysfunction or injury include:
Neurolysis
This procedure involves targeted damage/degeneration of nerve fibers, interrupts the nerve signals, and eliminates pain while the damaged area heals.
Neurorrhaphy
This procedure stitches a severed nerve back together.
Nerve Grafting
Grafting involves transplanting a portion of another nerve, usually the sural nerve, to reconnect severed nerves.
This helps, especially when the damaged portion is too large to be repaired by neurorrhaphy.
It allows a pathway for signals and encourages the regrowth of nerve axons.
Neurotization or Nerve Transfer
Similar to grafting but used when the nerve is too damaged to heal.
This procedure involves transplanting a healthy but less important nerve, or a portion of a nerve, to replace the damaged one and restore function.
Injury Medical Chiropractic and Functional Medicine Clinic
Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution. We focus on what works for you to relieve pain, restore function, and prevent injury. Regarding musculoskeletal pain, specialists like chiropractors, acupuncturists, and massage therapists can help mitigate the pain through spinal adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal issues.
Shoulder Pain Chiropractic Treatment
References
Subasinghe, S. K., & Goonewardene, S. (2016). A Rare Variation of the Axillary Nerve Formed as Direct Branch of the Upper Trunk. Journal of clinical and diagnostic research : JCDR, 10(8), ND01–ND2. https://doi.org/10.7860/JCDR/2016/20048.8255
Pizzo, R. A., Lynch, J., Adams, D. M., Yoon, R. S., & Liporace, F. A. (2019). Unusual anatomic variant of the axillary nerve challenging the deltopectoral approach to the shoulder: a case report. Patient safety in surgery, 13, 9. https://doi.org/10.1186/s13037-019-0189-1
Can determining whether arm numbness occurs suddenly or gradually and whether there are other symptoms help healthcare providers diagnose and treat the condition?
Arm Numbness
Arm numbness or tingling are common symptoms that various medical conditions can cause. Numbness can be caused by a sudden health emergency, nerve disorder, or nutritional deficiency. (National Institute of Neurological Disorders and Stroke, 2024) Sometimes, this symptom results from an arm falling asleep and could resolve after just a few minutes. The sensation may be temporary, caused by something like sleeping in the wrong position. However, arm numbness and tingling may also be caused by neuropathy and chronic and progressive nerve damage and can also suddenly occur due to serious conditions, such as a heart attack or a stroke.
Circulation Issues
Deficient blood circulation in the arm could cause numbness and tingling as the nerves cannot receive enough oxygen. Conditions can interfere with normal blood flow and include: (Bryan L. and Singh A. 2024)
Atherosclerosis – plaque buildup in the arteries that may require medication or surgery.
Severe frostbite can damage the blood vessels but can be resolved with proper warming and wound care.
Vasculitis – is inflammation of the blood vessels that can be treated with medication.
Sleeping Position
A common example of sudden numbness and tingling is the feeling that the arm has fallen asleep. This usually occurs after sleeping awkwardly or leaning on the arm for a long time. Known as paresthesia, this sensation is related to the compression or irritation of nerves. (Bryan L. and Singh A. 2024) Sleeping in certain positions has been associated with nerve compression, especially when the hands or wrists are tucked or curled under the body, as well as maintaining proper spine alignment when sleeping, is the best way to prevent arm numbness.
Nerve Injuries and Conditions
Numbness that persists may be related to an injury or underlying health problem that affects the brachial plexus, a group of nerves that runs from the lower neck to the upper shoulders and controls movement and sensation in the arms. (Mount Sinai, 2022) Possible injuries that affect these nerves include: (Smith, S. M. et al., 2021)
A herniated disc caused by aging or trauma causes the disc to leak out and press on the nerve root.
Many medications, like gabapentin, can be used to alleviate the sensations of arm numbness.
Some medications can cause numbness as a side effect.
Some medications can cause complications, and arm numbness could be a symptom of those complications.
Inform healthcare providers about medications being taken to determine the relationship between them and any sensory changes.
Vitamin Deficiency
Peripheral neuropathy can also be caused by nutritional deficiencies and vitamin imbalances, which can damage nerves and cause sensation loss in the left or right arm. The most common sources are vitamin B12 deficiency and excess vitamin B6. (National Institute of Neurological Disorders and Stroke, 2024) Excessive alcohol consumption and other disorders that affect nutritional intake can also lead to nerve damage.
Injury Medical Chiropractic and Functional Medicine Clinic
At Injury Medical Chiropractic and Functional Medicine Clinic, our areas of practice include Chronic Pain, Personal Injury, Auto Accident Care, Work Injuries, Back Injury, Low Back Pain, Neck Pain, Migraine Headaches, Sports Injuries, Severe Sciatica, Scoliosis, Complex Herniated Discs, Fibromyalgia, Chronic Pain, Complex Injuries, Stress Management, Wellness & Nutrition, Functional Medicine Treatments, and in-scope care protocols. We focus on what works for you to relieve pain and restore function. If other treatment is needed, individuals will be referred to a clinic or physician best suited to their injury, condition, and/or ailment.
Chiropractic Care: The Natural Way to Recover From Injuries
References
National Institute of Neurological Disorders and Stroke. (2024). Paresthesia. Retrieved from https://www.ninds.nih.gov/health-information/disorders/glossary-neurological-terms#paresthesia
Bryan, L., Singh, A. Sleep Foundation. (2024). Numbness in Hands While Sleeping: Causes and Remedies. https://www.sleepfoundation.org/physical-health/numbness-in-hands-while-sleeping
Mount Sinai. (2022). Brachial plexopathy. https://www.mountsinai.org/health-library/diseases-conditions/brachial-plexopathy
Smith, S. M., McMullen, C. W., & Herring, S. A. (2021). Differential Diagnosis for the Painful Tingling Arm. Current sports medicine reports, 20(9), 462–469. https://doi.org/10.1249/JSR.0000000000000877
National Heart, Lung, and Blood Institute. (2023). Vasculitis. Retrieved from https://www.nhlbi.nih.gov/health/vasculitis/symptoms#:~:text=Nerve%20problems%2C%20including%20numbness%2C%20tingling,can%20also%20occur%20with%20vasculitis.
Centers for Disease Control and Prevention. (2024). Stroke signs and symptoms. Retrieved from https://www.cdc.gov/stroke/signs-symptoms/?CDC_AAref_Val=https://www.cdc.gov/stroke/signs_symptoms.htm
National Heart, Lung, and Blood Institute. (2022). What Is a Heart Attack? Retrieved from https://www.nhlbi.nih.gov/health/heart-attack
National Institute of Arthritis and Musculoskeletal and Skin Diseases. (2023). Spinal Stenosis Basics. Retrieved from https://www.niams.nih.gov/health-topics/spinal-stenosis/basics/symptoms-causes
Senderovich, H., & Jeyapragasan, G. (2018). Is there a role for combined use of gabapentin and pregabalin in pain control? Too good to be true?. Current medical research and opinion, 34(4), 677–682. https://doi.org/10.1080/03007995.2017.1391756
National Institute of Neurological Disorders and Stroke. (2024). Peripheral Neuropathy. Retrieved from https://www.ninds.nih.gov/health-information/disorders/peripheral-neuropathy
Can weight and strength training increase speed and power in athletes that participate in throwing sports?
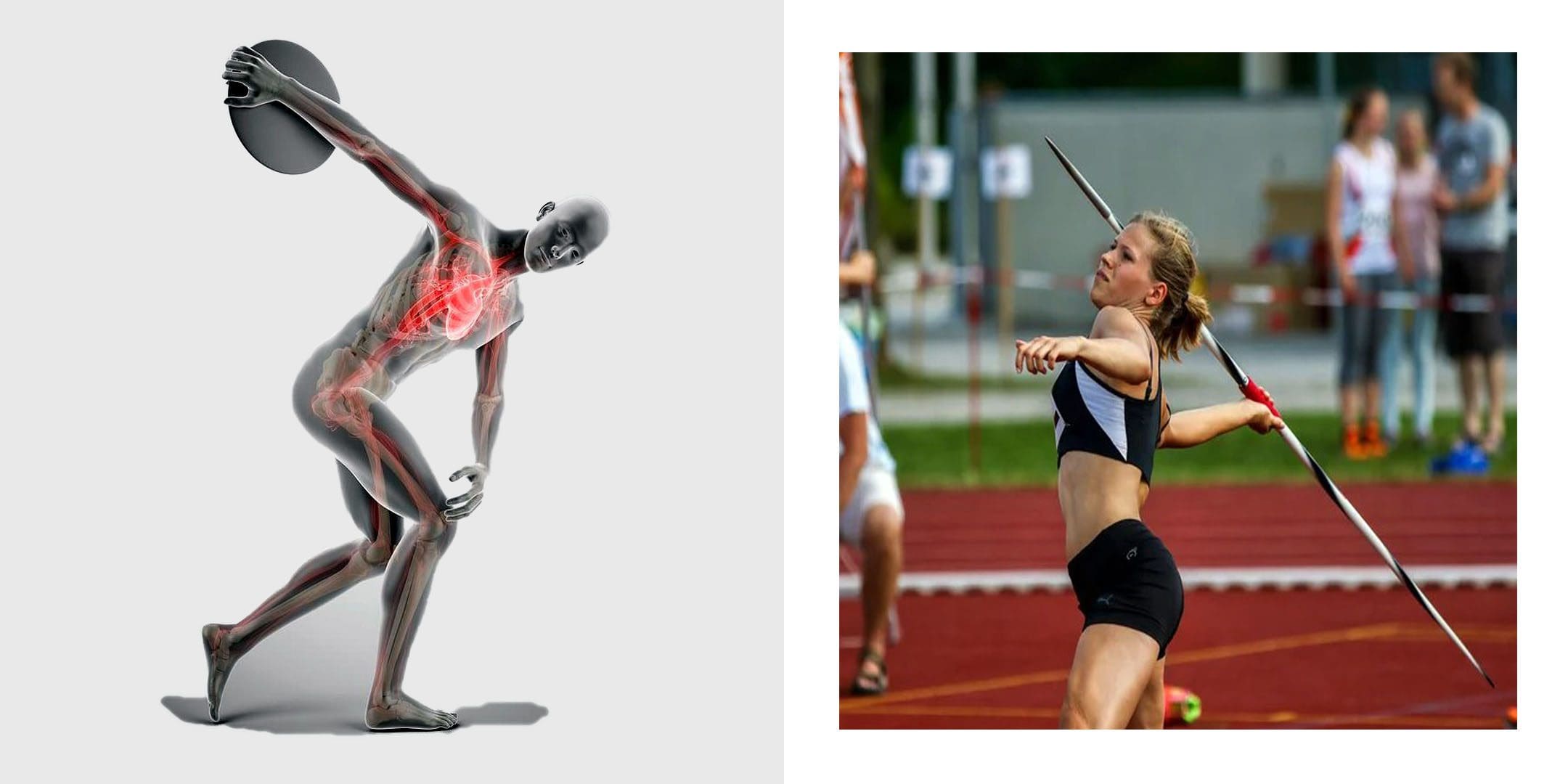
Throwing Sports
Top-throwing athletes have amazing arm speed. To succeed in throwing sports athletes need to be able to generate quick explosive power. This means the ability to propel the arm forward with substantial velocity for maximum object delivery like a baseball, javelin, hammer throw, shot put, discus, etc. Combined with sports technique training, throwing strength and power can be increased by training with weights. Here is a three-phase training plan to improve throwing performance.
Full Body
The arm provides only one part of the delivery process.
The legs, core, shoulders, and general flexibility need to work cooperatively to exert maximum thrust and achieve maximum object speed.
The natural ability to throw fast with power is largely determined by an individual’s muscle type, joint structure, and biomechanics. (Alexander E Weber, et al., 2014)
Preparation
Preparation should provide all-around muscle and strength conditioning for early pre-season conditioning.
Athletes will be doing throwing training as well, so fieldwork will need to be able to fit in.
It is recommended not to do weight training prior to throwing practice.
This leads to the start of competition and tournament play.
Frequency
2 to 3 sessions per week
Type
Strength and power – 60% to 70% for one-rep max/1RM
The one-repetition maximum test, known as a one-rep max or 1RM, is used to find out the heaviest weight you can lift once.
When designing a resistance training program, individuals use different percentages of their 1RM, depending on whether they’re lifting to improve muscular strength, endurance, hypertrophy, or power. (Dong-Il Seo, et al., 2012)
Throwing practice and competition are the priorities.
Before competition begins, take a 7- to 10-day break from heavyweight sessions while maintaining throwing workouts.
Weight training during competition should provide maintenance.
Frequency
1 to 2 sessions per week
Type
Power – lighter loads and faster execution than in the preparation stage.
Exercises
3 sets of 10
Rapid movement, 40% to 60% of 1RM.
Squats
Power hang clean and press
Romanian deadlift
Lat pulldown
Incline bench press
Crunches
Rest
Between sets 1 to 2 minutes.
Training Tips
Athletes have individual needs, so a general program like this needs modification based on age, sex, goals, skills, competitions, etc.
A certified strength and conditioning coach or trainer could help develop a fitness plan that can be adjusted as the athlete progresses.
Be sure to warm up prior to weight training and cool down afterward.
Don’t try to train through injuries or try to progress too fast – it is recommended not to throw or do weights when treating or recovering from an injury. (Terrance A Sgroi, John M Zajac. 2018)
Focus on the fundamentals and practice proper form.
Take a few weeks off at the end of the season to recover after hard training and competition.
Body Transformation
References
Weber, A. E., Kontaxis, A., O’Brien, S. J., & Bedi, A. (2014). The biomechanics of throwing: simplified and cogent. Sports medicine and arthroscopy review, 22(2), 72–79. https://doi.org/10.1097/JSA.0000000000000019
American College of Sports Medicine (2009). American College of Sports Medicine position stand. Progression models in resistance training for healthy adults. Medicine and science in sports and exercise, 41(3), 687–708. https://doi.org/10.1249/MSS.0b013e3181915670
Zaras, N., Spengos, K., Methenitis, S., Papadopoulos, C., Karampatsos, G., Georgiadis, G., Stasinaki, A., Manta, P., & Terzis, G. (2013). Effects of Strength vs. Ballistic-Power Training on Throwing Performance. Journal of sports science & medicine, 12(1), 130–137.
Seo, D. I., Kim, E., Fahs, C. A., Rossow, L., Young, K., Ferguson, S. L., Thiebaud, R., Sherk, V. D., Loenneke, J. P., Kim, D., Lee, M. K., Choi, K. H., Bemben, D. A., Bemben, M. G., & So, W. Y. (2012). Reliability of the one-repetition maximum test based on muscle group and gender. Journal of sports science & medicine, 11(2), 221–225.
Sakamoto, A., Kuroda, A., Sinclair, P. J., Naito, H., & Sakuma, K. (2018). The effectiveness of bench press training with or without throws on strength and shot put distance of competitive university athletes. European journal of applied physiology, 118(9), 1821–1830. https://doi.org/10.1007/s00421-018-3917-9
Sgroi, T. A., & Zajac, J. M. (2018). Return to Throwing after Shoulder or Elbow Injury. Current reviews in musculoskeletal medicine, 11(1), 12–18. https://doi.org/10.1007/s12178-018-9454-7
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine