The iliacus muscle is a triangle-shaped muscle in the pelvic bone that flexes and rotates the thigh bone. It works with the other muscles in the hip and thigh to help bend, run, walk, sit, and maintain correct posture. Injuries and common medical conditions can affect its function, causing pain and stiffness. Can physical therapy help?
The Iliacus Muscle
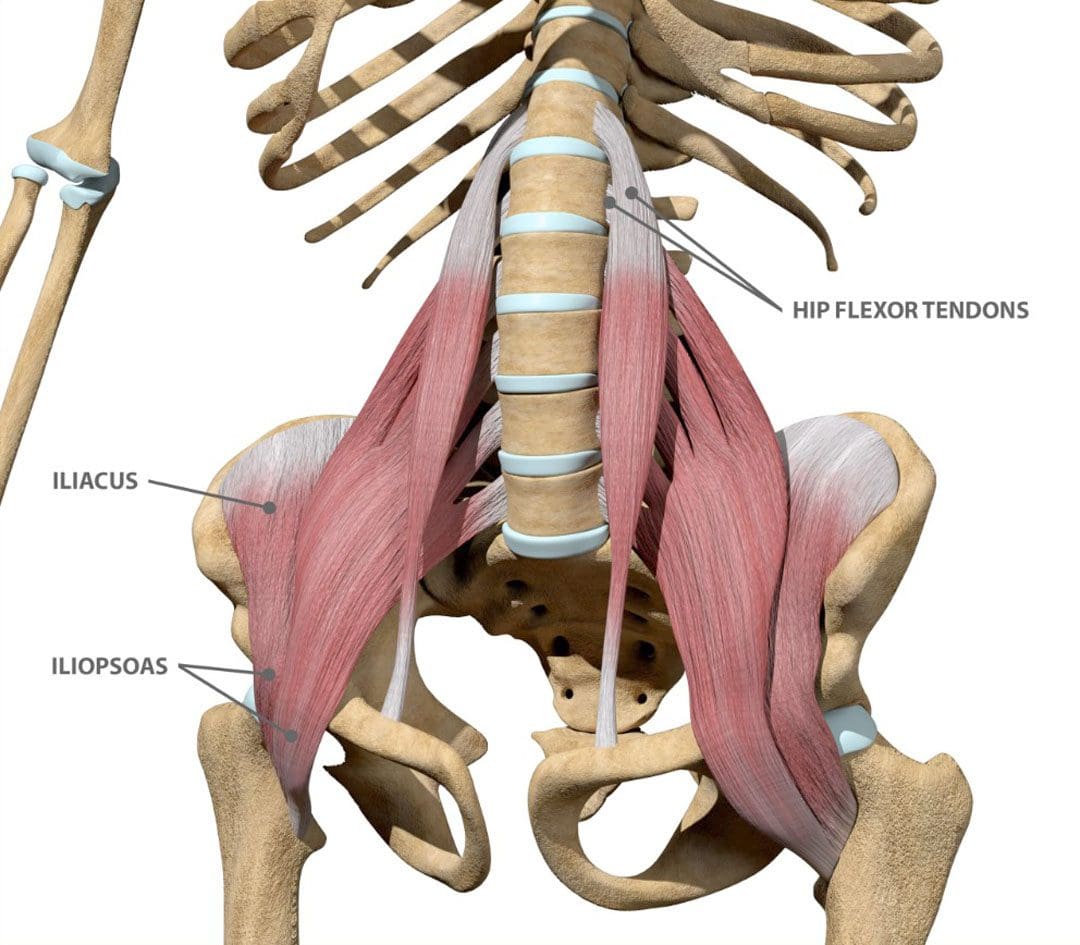
The iliacus is one of the body’s most important hip flexor muscles. The iliacus and surrounding muscles work together to produce the stability and range of motion required for bending, dancing, sitting, and walking.
Anatomy
The iliacus muscle is part of a complex muscle system in the hip and pelvis. Two iliacus muscles on each side of the pelvic bone enable the thigh to flex and rotate. They are innervated by the femoral nerve, which provides movement and sensation to the lower limbs. (Bordoni B. and Varacallo M. 2023) The iliacus muscle sits on the wing-shaped ilium and fits into the curved surface of the ilium, called the iliac fossa. The top of the muscle is attached to the upper wings of the ilium or iliac crest. It extends past the hip joint, which connects to the upper thigh bone/femur at the lesser trochanter protrusion. The iliacus is part of a major trio of muscles called the iliopsoas, including the major psoas and minor psoas muscles. These muscles are also attached to the upper femur but extend upward, connecting to the lumbar/lower spine at several attachment points. The iliopsoas also interact with the quadratus lumborum muscle, the deepest muscle of the lower back that starts at the iliac crest and attaches to the lumbar spine at several points. The quadratus lumborum enables flexion and elevation of the spine, while the iliopsoas enable the flexion and rotation of the hip and thigh.
Functions
The iliacus muscle has many functions that include: (Physiopedia, 2024)
Flexing and rotating the femur.
Helps maintain proper body posture while standing and sitting.
Produces hip movement that enables walking, running, and climbing stairs.
Provides hip flexion – bringing the knee to the chest.
Enables the forward tilt of the pelvis and side-bending.
Conditions
Several conditions can affect the iliacus muscle, specifically from under and/or overuse injuries. These conditions, collectively known as Iliopsoas syndrome, are typically the result of overuse/repetitive strain or injuries. These include:
Iliopsoas tendinopathy – which affects tendons.
Iliopsoas bursitis – which affects cushioning sacs known as bursae.
Iliopsoas syndrome can affect anyone but is common in:
Individuals and athletes who repeatedly use movements that flex the hips.
Track-and-field athletes
Gymnasts
Dancers
Iliopsoas Bursitis
This is the inflammation of the cushioning sac or bursa under the iliacus muscle, which helps the muscle slide over the pelvic bone. Symptoms can range from mild discomfort to pain that radiates through parts of the leg and hips. Runners, skiers, and swimmers are commonly affected, and individuals who regularly have tight hips and individuals with different forms of arthritis can also be affected. Early treatment can prevent the symptoms from worsening. Mild cases can be treated with self-care and stretching to help relieve tightness, rest, ice application, and over-the-counter nonsteroidal anti-inflammatory drugs. In severe cases, treatment options that may be recommended include: (Physiopedia, 2024)
Physical therapy
Assistant walking devices to relieve pressure – for example, a cane.
Corticosteroid steroid injections
Prescription anti-inflammatory medications
Iliopsoas Tendinopathy
Another condition affecting the iliacus muscles is iliopsoas tendinopathy, sometimes called snapping hip syndrome, because individuals can hear an audible snapping sound (Davenport KL. 2019). The condition is often experienced by dancers who repeatedly flex and hyperextend their hips and can result in hip and groin pain that gets worse with kicking or rotation. Treatment of iliopsoas tendinopathy can include:
Retraining muscle imbalances with strengthening and stretching exercises.
If these fail to provide relief, corticosteroid injections may be used. A saline hydro dissection can relieve stress around the tendon by injecting fluids that cushion and release trapped tissues.
Tendon release surgery may be recommended when all other options have failed. The surgical release involves severing the tendon to reduce pain and improve the range of motion.
Rehabilitation
Core muscle strengthening is essential to the rehabilitation of iliacus muscle injuries. The iliopsoas is an integral component of the core group and can benefit from stretching and strengthening exercises (Yogateket, 2019)
Lunge stretches
Straight leg raises
Knee-to-chest stretches
Standing hip flexion with resistance bands
Certain yoga poses can also help and include variations on the bridge pose that encourage hip flexion. (Yoga International, 2024)
Injury Medical Chiropractic and Functional Medicine Clinic
Iliopsoas pain is often felt at the front of the hips, thigh, mid-back, and lower back. Chiropractic care can help with iliacus muscle injuries through:
Evaluation
A chiropractor can evaluate the condition and determine if the iliacus muscle is causing pain.
Treatment plan
A chiropractor can create a personalized treatment plan that may include exercise instructions, manipulation, and other therapies.
Rehabilitation
A chiropractor can create a rehabilitation program to expedite healing.
Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution. We focus on what works for you to relieve pain, restore function, and prevent injury. Regarding musculoskeletal pain, specialists like chiropractors, acupuncturists, and massage therapists can help mitigate the pain through spinal adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal issues.
Hip Labral Tear and Chiropractic Care
References
Bordoni, B., & Varacallo, M. (2024). Anatomy, Bony Pelvis, and Lower Limb, Iliopsoas Muscle. In StatPearls. https://www.ncbi.nlm.nih.gov/pubmed/30285403
Davenport KL. (2019). The professional dancer’s hip. Performing Arts Medicine, 77-87. https://doi.org/https://doi.org/10.1016/B978-0-323-58182-0.00009-2
Yogateket. Lizette Pompa. (2019). Essential yoga body parts. Hip flexor/psoas and yoga. Yogateket. https://www.yogateket.com/blog/hip-flexor-psoas-and-yoga
For individuals looking to improve their spinal health, can understanding the anatomy of the intervertebral foramen help in injury rehabilitation and prevention?
Intervertebral Foramen
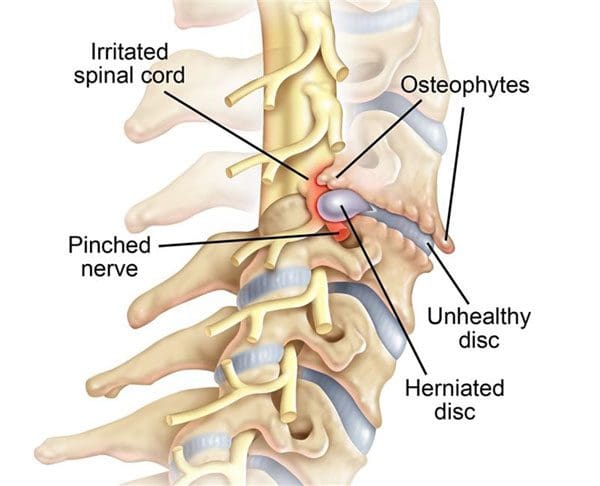
The intervertebral foramen, aka neural foramen, is the opening between the vertebrae through which spinal nerve roots connect and exit to other body areas. If the foramina narrows, it can place added pressure on the nerve roots near and around them, causing pain symptoms and sensations. This is known as neuroforaminal stenosis. (Sumihisa Orita et al., 2016)
Anatomy
The vertebrae comprise the spinal column.
They protect and support the spinal cord and most of the weight placed on the spine.
Foramen is the singular form, and foramina is the plural form.
Structure
The body is the large, round part of the bone that makes up each vertebra.
The body of each vertebra is attached to a bony ring.
Stenosis can occur in the spinal canal, known as central canal stenosis, and the foramina.
Pain brought on by neuroforaminal spinal stenosis and arthritis-related bone growth/bone spurs/osteophytes that are present in one or more foramen rub against the nerve root that passes through the space, causing radicular pain.
Pain accompanied by other sensations, like tingling or numbness, is known as radiculopathy. (Young Kook Choi, 2019)
The main symptom is pain.
Numbness and/or tingling can present depending on the injury.
Neurogenic claudication occurs as a result of ischemia or a lack of blood circulation to the nerves and typically presents with a heaviness in the legs.
It is typically associated with central stenosis rather than foraminal stenosis.
Most individuals with spinal stenosis feel better when flexing or bending forward and worse when arching their backs.
Stenosis treatment aims to relieve pain and prevent nerve symptoms from occurring or worsening. Conservative treatments are recommended and can be highly effective.
These include:
Myelopathy in the neck and/or upper or mid-back (myelopathy symptoms are spinal cord related and occur in central canal stenosis) (Cleveland Clinic. 2021)
Intense incapacitating pain
Different surgical techniques include:
Decompression laminectomy – entails removing the buildup of bone in the spinal canal.
Spinal fusion – when there is instability of the spine or severe foraminal stenosis.
Orita, S., Inage, K., Eguchi, Y., Kubota, G., Aoki, Y., Nakamura, J., Matsuura, Y., Furuya, T., Koda, M., & Ohtori, S. (2016). Lumbar foraminal stenosis, the hidden stenosis including at L5/S1. European journal of orthopaedic surgery & traumatology : orthopedie traumatologie, 26(7), 685–693. https://doi.org/10.1007/s00590-016-1806-7
American Academy of Orthopaedic Surgeons. (2020). Spine Basics (OrthoInfo, Issue. https://orthoinfo.aaos.org/en/diseases–conditions/spine-basics/
American Academy of Orthopaedic Surgeons. (2021). Lumbar spinal stenosis (OrthoInfo, Issue. https://orthoinfo.aaos.org/en/diseases–conditions/lumbar-spinal-stenosis/
Choi Y. K. (2019). Lumbar foraminal neuropathy: an update on non-surgical management. The Korean journal of pain, 32(3), 147–159. https://doi.org/10.3344/kjp.2019.32.3.147
Lee, S. Y., Kim, T. H., Oh, J. K., Lee, S. J., & Park, M. S. (2015). Lumbar Stenosis: A Recent Update by Review of Literature. Asian spine journal, 9(5), 818–828. https://doi.org/10.4184/asj.2015.9.5.818
Lurie, J., & Tomkins-Lane, C. (2016). Management of lumbar spinal stenosis. BMJ (Clinical research ed.), 352, h6234. https://doi.org/10.1136/bmj.h6234
“Various problems with the sacrum make up or contribute to a significant portion of lower back problems. Can understanding the anatomy and function help prevent and treat back injuries?”
The Sacrum
The sacrum is a bone shaped like an upside-down triangle located at the base of the spine that helps support the upper body when sitting or standing and provides pelvic girdle flexibility during childbirth. It comprises five vertebrae that fuse during adulthood and connect to the pelvis. This bone takes and endures all of the body’s pressure and stress from everyday activities and movements.
Formation
Humans are born with four to six sacral vertebrae. However, fusion does not take place in all sacral vertebrae simultaneously:
Fusion starts with the S1 and S2.
As the individual gets older, the overall shape of the sacrum begins to solidify, and the vertebrae fuse into a single structure.
The process usually starts in the mid-teens and finishes in the early to mid-twenties.
It is believed to start earlier in females than males.
The sacrum in a female is wider and shorter and has a more curved top or the pelvic inlet.
The male sacrum is longer, narrower, and flatter.
Structure
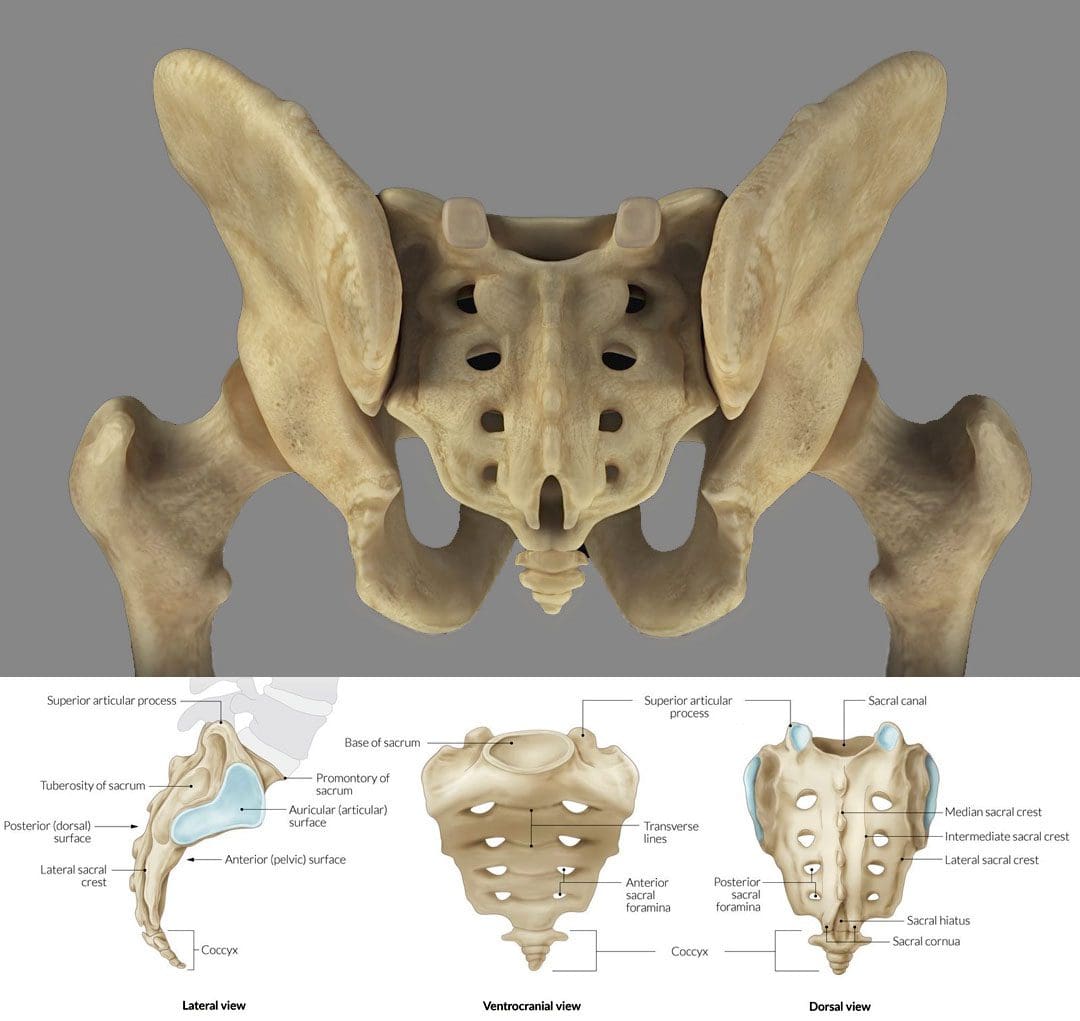
The sacrum is an irregular bone that makes up the back/posterior third of the pelvic girdle. There is a ridge across the front/anterior portion of the S1 vertebra known as the sacral promontory. Small holes/foramen on both sides of the sacrum are left over after the vertebrae fuse together. Depending on the number of vertebrae, there can be three to five foramen on each side, though there are usually four. (E. Nastoulis, et al., 2019)
Each anterior foramen is typically wider than the posterior or dorsal/backside foramen.
Each sacral foramina/plural of foramen provides a channel for the sacral nerves and blood vessels.
Small ridges develop between each of the fused vertebrae, known as transverse ridges or lines.
The top of the sacrum is called the base and is connected to the largest and lowest of the lumbar vertebrae – L5.
The bottom is connected to the tailbone/coccyx, known as the apex.
The sacral canal is hollow, runs from the base to the apex, and serves as a channel at the end of the spinal cord.
The sides of the sacrum connect to the right and left hip/iliac bones. The attachment point is the auricular surface.
Right behind the auricular surface is the sacral tuberosity, which serves as an attachment area for the ligaments that hold the pelvic girdle together.
Location
The sacrum is at the level of the lower back, just above the intergluteal cleft or where the buttocks split. The cleft starts at around the level of the tailbone or coccyx. The sacrum is curved forward and ends at the coccyx, with the curvature being more pronounced in females than males. It connects to the L5 lumbar vertebra by way of the lumbosacral joint. The disc between these two vertebrae is a common source of low back pain.
On either side of the lumbosacral joint are wing-like structures known as the sacral ala, which connect to the iliac bones and form the top of the sacroiliac joint.
These wings provide stability and strength for walking and standing.
Anatomical Variations
The most common anatomical variation applies to the number of vertebrae. The most common is five, but anomalies have been documented, including individuals with four or six sacral vertebrae. (E. Nastoulis, et al., 2019)
Other variations involve the sacrum’s surface and curvature, where the curvature differs widely between individuals.
In some cases, the first and second vertebrae do not fuse and remain separately articulated.
Failure of the canal to completely close during formation is a condition known as spina bifida.
Function
Studies on the sacrum are ongoing, but some proven functions include:
It serves as an anchor point for the spinal column to attach to the pelvis.
It provides stability for the body’s core.
It acts as a platform for the spinal column to rest on when sitting.
It facilitates childbirth, providing pelvic girdle flexibility.
It supports upper body weight when sitting or standing.
It provides extra stability for walking, balance, and mobility.
Conditions
The sacrum can be a main source or focal point for lower back pain. It is estimated that 28% of men and 31.6% of women aged 18 years or older have experienced low back pain in the past three months. (Centers for Disease Control and Prevention. 2020) Conditions that can cause sacrum pain symptoms include.
Sacroiliitis
This is a common condition of sacroiliac/SI joint inflammation.
A doctor only makes the diagnosis when all other possible causes of pain have been ruled out, known as a diagnosis of exclusion.
About half of all chordomas form in the sacrum, but the tumors can also develop elsewhere in the vertebral column or at the base of the skull. (National Library of Medicine. 2015)
Spina Bifida
Individuals can be born with conditions that affect the sacrum.
Spina bifida is a congenital condition that can arise from the malformation of the sacral canal.
Unlocking the Secrets of Inflammation
References
Gruss, L. T., & Schmitt, D. (2015). The evolution of the human pelvis: changing adaptations to bipedalism, obstetrics and thermoregulation. Philosophical transactions of the Royal Society of London. Series B, Biological sciences, 370(1663), 20140063. https://doi.org/10.1098/rstb.2014.0063
Nastoulis, E., Karakasi, M. V., Pavlidis, P., Thomaidis, V., & Fiska, A. (2019). Anatomy and clinical significance of sacral variations: a systematic review. Folia morphologica, 78(4), 651–667. https://doi.org/10.5603/FM.a2019.0040
Barros, G., McGrath, L., & Gelfenbeyn, M. (2019). Sacroiliac Joint Dysfunction in Patients With Low Back Pain. Federal practitioner : for the health care professionals of the VA, DoD, and PHS, 36(8), 370–375.
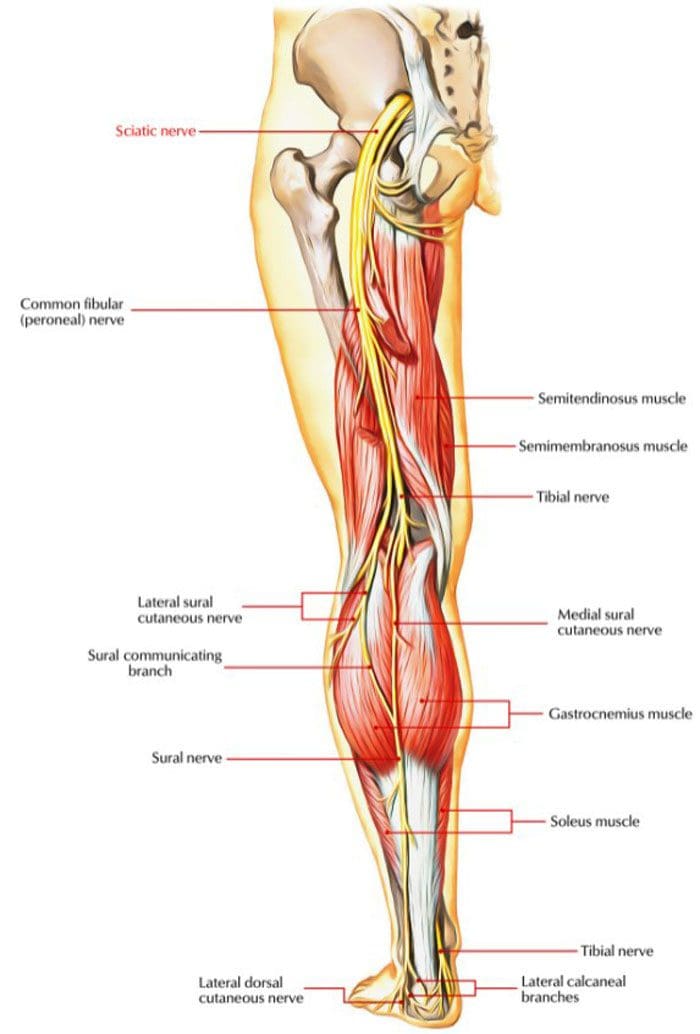
The sciatic nerve is formed through a combination of motor and sensory fibers based on the spinal nerves of the lower back L4 to S3, known as the lumbosacral plexus. It is the largest and longest nerve in the human body and about as wide as an adult thumb. It begins at the base of the spine, runs along the back of each leg, and ends at the foot supplying the areas with fresh blood and nutrients. There are sciatic nerve branches that consist of primary branches and smaller branches.
Sciatic Nerve Branches
The nerve splits into two main branches near the back of the knee called the popliteal fossa.
This fossa is located slightly above the joint behind the knee.
The popliteal fossa is a diamond-shaped space that acts as the conduit for the blood vessels and nerves.
Primary branches
From the popliteal fossa:
The tibial nerve continues down the back of the calf to the heel and bottom of the foot.
The common peroneal nerve, aka common fibular nerve, travels sideways along the outer part of the knee to the outer border of the lower leg and foot.
Both nerves convert into small sensory nerves in the calf that supply the outer side of each foot.
The sciatic nerve breaks off into smaller branches, known as collaterals, that include:
These are muscle branches that supply the muscles in the thigh, including the hamstring group and the adductor magnus muscles along the inner thigh.
Other small branches supply the leg and foot muscles.
Articular branches supply the back of the hip joint, the back and side of the knee joint.
The sciatic nerve does not supply structures in the buttocks; however, pain commonly radiates/spreads into this area when the nerve is impaired, impinged, and inflamed.
Blood Supply
The delivery of nutrients to the sciatic nerve is done through blood vessels that also contribute to the nerve’s function. Any interruption of blood flow to the sciatic nerve can cause pain and dysfunction. The sciatic nerve and the sciatic nerve branches receive their blood supply from two sources that include:
The extrinsic system is made up of nearby arteries and veins.
The intrinsic system includes arteries and veins that run along the nerve and are embedded deep in a sheath known as the epineurium of connective tissue that envelops the nerve.
The intrinsic blood supply can be affected by conditions like diabetes, which can contribute to symptoms associated with diabetic neuropathy.
Both systems connect at various junction points.
Nerve Function
The combination of sensory and motor fibers that make up the sciatic nerve provides the essential functions in the lower limbs allowing the body to:
Stand
Walk
Run
Climb
Lift
A healthy sciatic nerve is well protected around the low back and buttock muscles where it starts, and it cannot be palpated or felt by touching or pressing on the area. When the nerve gets inflamed, injured, or pinched, the leg can feel stiff and inflexible when trying to move and can lead to pain, weakness, and tingling in the lower back, buttock, leg/s, and feet.
Anatomical Variations of the Nerve
Individuals can have variations in the anatomical structure of the sciatic nerve. These variations are considered normal, but they can increase the risk of developing sciatica brought on by impingement, entrapment, or irritation of the nerve root/s. Variations in sciatic nerve branches include:
The nerve divides above the piriformis muscle; one portion passes through the piriformis, with the other portion exiting the pelvis below the muscle. This is the most common variation.
The nerve divides above the piriformis muscle; one portion passes through the piriformis, with the other portion exiting the pelvis above the muscle.
The nerve divides above the piriformis, with one portion traveling in front while the other travels behind it.
Undivided sciatic nerve exits through the piriformis muscle.
Undivided sciatic nerve exits from behind the top part of the piriformis.
Around 10% of individuals have a nerve that divides above the popliteal fossa and does not merge but courses down in two separate branches.
The sciatic nerve and the sciatic nerve branches are significant components of the body. It supplies motor functions to move the legs and feet and provides sensory functions along the nerve path. Keeping the sciatic nerve healthy is key in helping to prevent back and spinal issues. Chiropractic can help realign the sciatic nerve and educate on maintaining the nerve’s health.
Body Composition
Fitness Motivation
New workout routine
Individuals that don’t feel like returning to previous workout routines are recommended to try out other fitness options. If the gym isn’t cutting it or there is burnout with the current routine, switch things up. This can include:
Virtual group classes.
1-on-1 personal training.
Outdoor activities.
All are valid options to explore if in a rut with the current routine.
The important thing is to find what works for you.
Allow the body to rest
Individuals may want to push it to the limit to get back into shape, but rest days are essential for healthy muscle development and improved performance.
Noticing the body is more sore and exhausted after a workout is an indication that the body needs rest. This also includes:
Maintaining proper hydration.
Stretching out the muscles regularly.
Taking days off from exercising are necessary to:
Prevent muscle fatigue.
Reduce the risk of injury.
Allow for adequate muscle recovery.
Long term commitment is key
It can be discouraging to commit to a workout schedule only to notice minor changes to strength and fitness.
However, small improvements do accumulate over time.
Small increases over time can have a huge impact on overall strength and fitness.
Keep the bigger picture in mind to remain positive.
References
Davis D, Vasudevan A. Sciatica. [Updated 2019 Feb 28]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2019 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK507908/
Barral J, Croibier A. Manual Therapy for the Peripheral Nerves. Elsevier Health Sciences; 2007.
Ryan MM, Jones HR Jr. Mononeuropathies. In: Neuromuscular Disorders of Infancy, Childhood, and Adolescence. Elsevier; 2015:243-273. doi:10.1016/b978-0-12-417044-5.00014-7
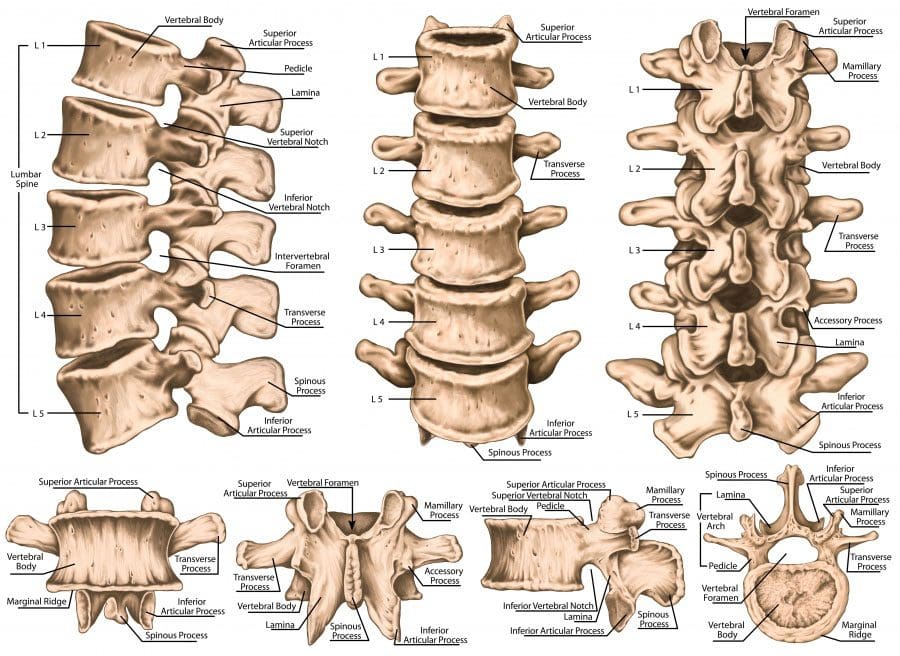
The lumbar spine is the lower back that starts below the last thoracic vertebra T12 and ends at the top of the sacral spine or sacrum S1. Each lumbar spinal level is numbered from top to bottom, L1 to L5, or L6. The low back bodies are larger, and thicker structures of dense bone. From the front or anterior, the vertebral body has a rounded shape.
The posterior bony structure is a different lamina, which is a thin bony plate that shields and protects access to the spinal canal. There are vertebral arches that create the hollow spinal canal for lumbar nerve structures and the cauda equina.
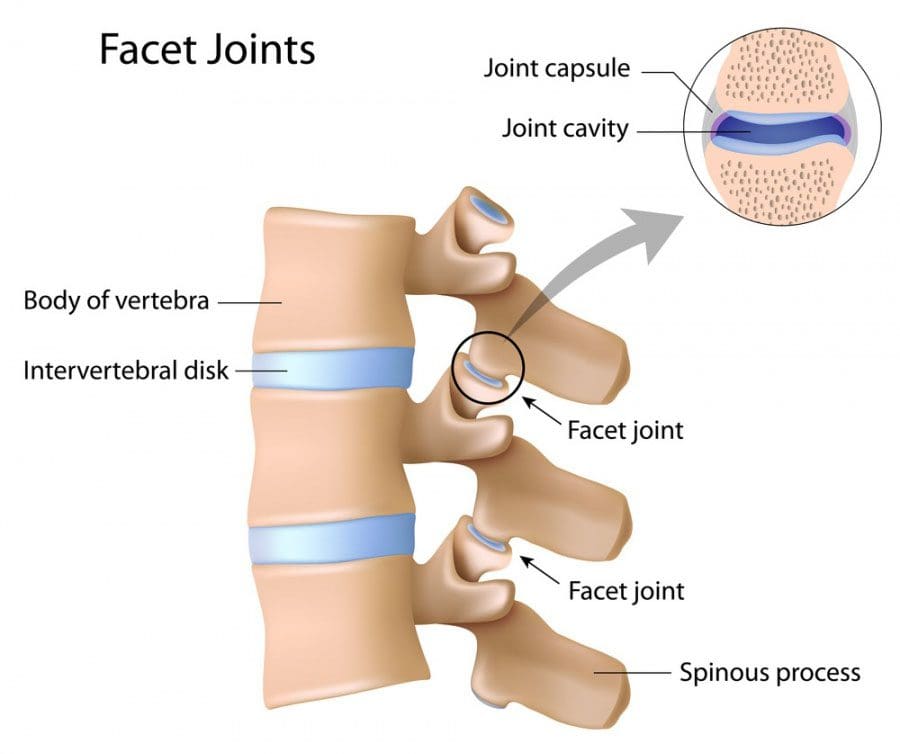
Lumbar Structure Strong Joint Complex
One intervertebral disc together with the facet joints forms a strong joint complex that allows the spine to bend and twist. One pair of facet joints from the top or superior vertebral body connects the lower or inferior set of facet joints. The facet joints are synovial joints, which means they are lined with cartilage and the capsule holds synovial fluid that enables joints to glide during movement. Think of it as hydraulics with smooth fluid motion.
Facet joint syndrome can develop from aging and degenerative spinal changes causing low back pain. The lumbar discs are secured in place by the fibrous endplates of the superior and inferior vertebral bodies.
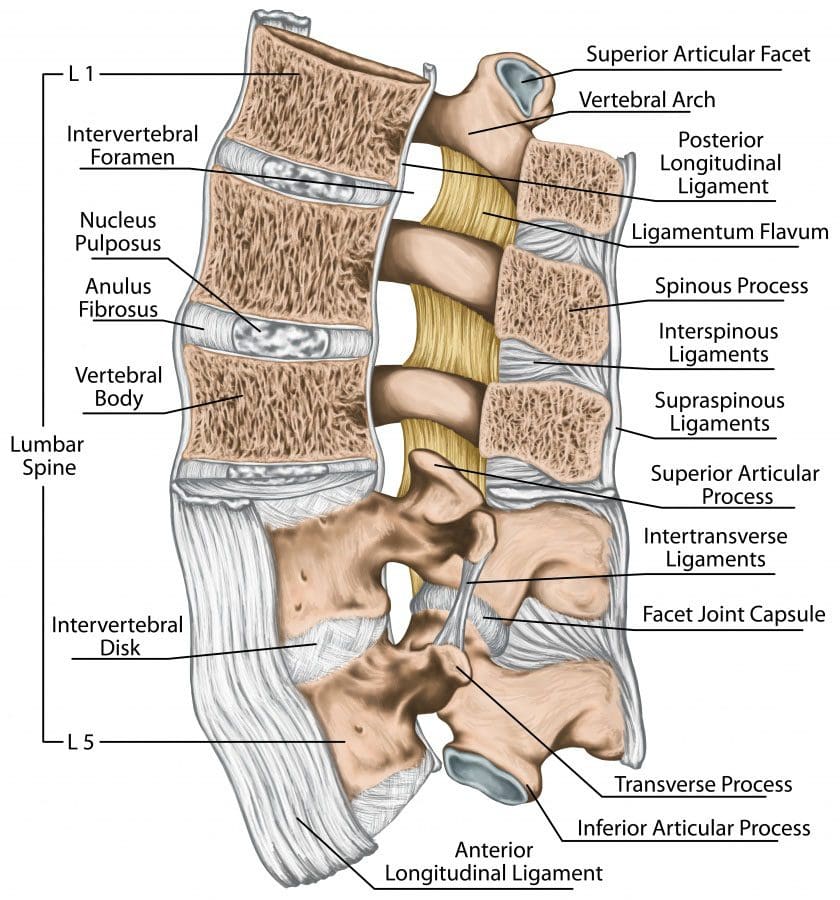
The jelly/gel center of each disc called the nucleus pulposus is surrounded by the annulus fibrosis, which is a tough layer of fibrocartilage that you can think of as a radial tire.
Discs are integral to the joint complex and function to:
Hold the superior and inferior vertebrae together
Take the weight
Absorb and distribute shock and forces when moving about
Create an open nerve passageway called foramen or neuroforamen
The neuroforaminal spaces on either side of the disc allow nerve roots to exit the spinal canal and leave the column.
Lumbar disc herniation is a common cause of low back pain that can spread out into one or both legs. This is called lumbar radiculopathy. This condition can develop when the nerves are compressed.
Low Back Support
Lumbar Ligaments
Tendons
Muscles
Systems of strong fibrous bands of ligaments hold the vertebrae and discs together and stabilize the spine by helping to prevent over/excessive movements.
The 3 major spinal ligaments are the:
Anterior longitudinal ligament
Posterior longitudinal ligament
Ligamentum flavum.
Spinal tendons attach muscles to the vertebrae and together work to limit excessive movement.
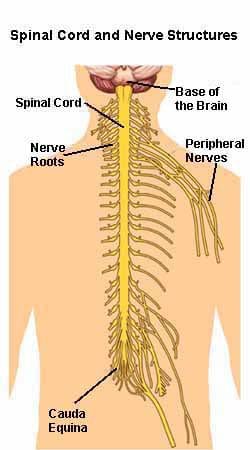
Lumbar Spine Nerves
The spinal cord comes to an end between the first and second lumbar vertebrae(L1-L2). Below this is the remaining nerves that form the cauda equina which is a bundle of nerves that looks like a horse�s tail. These nerves send messages between the brain and the lower body structures, including the:
Large intestine
Bladder
Abdominal muscles
Perineum
Legs
Feet
Protect Your Back
Around 80% of adults will see a doctor for low back pain at some point. Therefore take care of your lumbar spine to help avoid painful, unnecessary wear-and-tear. You can minimize the risk of a low back injury/pain by:
Losing weight. Even a loss of 5 pounds can help reduce back pain.
Strengthening the core/abdominal muscles. The abdominal and low back muscles work together to form a supportive band around the waist and low back. Stronger muscles help stabilize the low back and reduce the risk of injury.
Stopping smoking. Nicotine reduces blood flow to the spine’s structures. This includes the lumbar discs and accelerates age-related degeneration.
Proper posture and proper body mechanics. When lifting objects keep your spine erect and use your legs. Ask for help with heavy objects. The lumbar spine is can bend and twist simultaneously, try to avoid doing this, as it is a perfect setup for a strain or sprain.
Get Rid of Low Back Pain with Custom Foot Orthotics
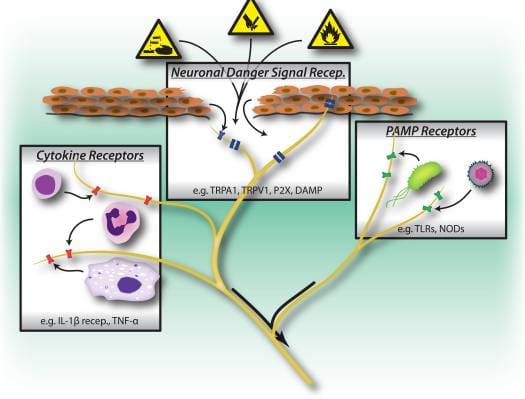
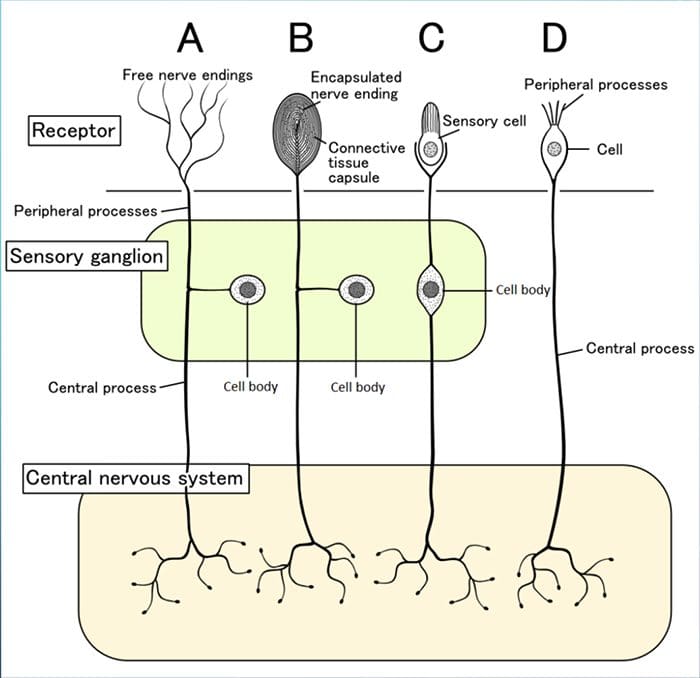
Understanding chronic pain and its alleviation requires an understanding of the anatomy of the nervous system. The nerves of the body are the carriers for the nervous system, as it sends messages to and from the brain. It is quite a complex system. The central nervous system consists of the spinal cord and the brain. The peripheral nervous system branches off the spinal cord.� Both the central and peripheral nervous systems can be affected by neuropathic pain, a type of chronic pain caused by nerve malfunction.
The peripheral nervous system contains 31 pairs of nerve roots that extend from the spinal cord to the rest of the body. There are the feeling nerves/sensory nerves and moving nerves/motor nerves. The chart shows how many pairs of spinal nerves are at each level of the spine.
Peripheral nervous system
The somatic nervous system is comprised of nerves that connect to the musculoskeletal system’s:
Bones
Ligaments
Tendons
Muscles
Skin
It’s what helps generate feeling and what generates the feeling of pain.
It makes sure the heart keeps pumping and the digestive system breaks down food correctly without thinking. Damage to any nerves can lead to the development of chronic pain. The nerves are responsible for sending pain messages, and if they get damaged, they can continually send a steady stream of pain messages.
Nociceptorsare another important part of the nerve body. Nociceptors are receptors at the nerve endings, which are activated when something happens and triggers a pain message.
Example: Nociceptors�in the finger turn on and send a pain message through the peripheral nerve to the spinal cord, on to the brain when a finger gets smashed in the car door. Before the finger was smashed, the nociceptors were not on because there was nothing to make them respond.
One possible cause of chronic pain could be malfunctioning nociceptors. Even if there is not a direct or root cause, they could be continually sending pain messages. Using the same example of the finger smashed in the car door. The finger heals after the smashing but pain signals are still being sent. The�finger’s�nociceptor’s nerves could be malfunctioning, which is why they are still sending pain messages. The result is chronic pain.
Chronic pain symptoms
Chronic pain is pain that does not stop for more than 6 months. Pain is a subjective experience, it is different for everyone and takes on many forms. The pain could be:
Aching
Burning
Constant Soreness
Constant Stiffness
Electric
Sharp
Shooting
Throbbing
Tight
Chronic pain can lead to other problems, specifically social, psychological and emotional. It can:
Cause sleeplessness
Drain the body’s energy
Cause depression
Withdraw from activities/friends/family
Weaken the immune system because so much energy is spent dealing with the pain
These added conditions feed off each other. Example: Sleeping is impossible when the pain is active, the next day nothing gets done because of the tiredness. As a result of the inactiveness, a loss of self-esteem begins to set in causing withdrawal from family and social life.
Alleviation
To get the best treatment possible, take note of activities, diet, accidents, injuries, etc before the pain began. Depending on the diagnosis, chiropractic care could help. Research studies have shown that two weeks of regular adjustments/manipulation can bring significant improvement.
Physical therapy combined with stretching and strengthening exercises is part of the treatment for chronic pain. Physical therapy could consist of ice, heat, transcutaneous electrical nerve stimulation, ultrasound, and myofascial release. A chiropractor and other pain professionals can help bring alleviation, so you can fully live your life.
The rule of 4 of the brainstem: a simplified method for understanding brainstem anatomy and brainstem vascular
syndromes for the non-neurologist.
The Rule Of 4 & The Brainstem
The rule of 4 is a simple method developed to help �students of neurology� to remember the anatomy of the brainstem and thus the features of the various brainstem vascular syndromes. As medical students, we are taught detailed anatomy of the brainstem containing a bewildering number of structures with curious names such as superior colliculi, inferior olives, various cranial nerve nuclei and the median longitudinal fasciculus. In reality when we do a neurological examination we test for only a few of these structures. The rule of 4 recognizes this and only describes the parts of the brainstem that we actually examine when doing a neurological examination. The blood supply of the brainstem is such that there are paramedian branches and long circumferential branches (the anterior inferior cerebellar artery (AICA), the posterior inferior cerebellar artery (PICA) and the superior cerebellar artery (SCA). Occlusion of the paramedian branches results in medial (or paramedian) brainstem syndromes and occlusion of the circumferential branches results in lateral brainstem syndromes. Occasionally lateral brainstem syndromes are seen in unilateral vertebral occlusion. This paper describes a simple technique to aid in the understanding of brainstem vascular syndromes.
Any attempt to over simplify things runs the risk of upsetting those who like detail and I apologize in advance to the anatomists among us, but for more than 15 years this simple concept has helped numerous students and residents understand, often for the first time, brainstem anatomy and the associated clinical syndromes that result.
In The Rule Of 4 There Are 4 Rules:
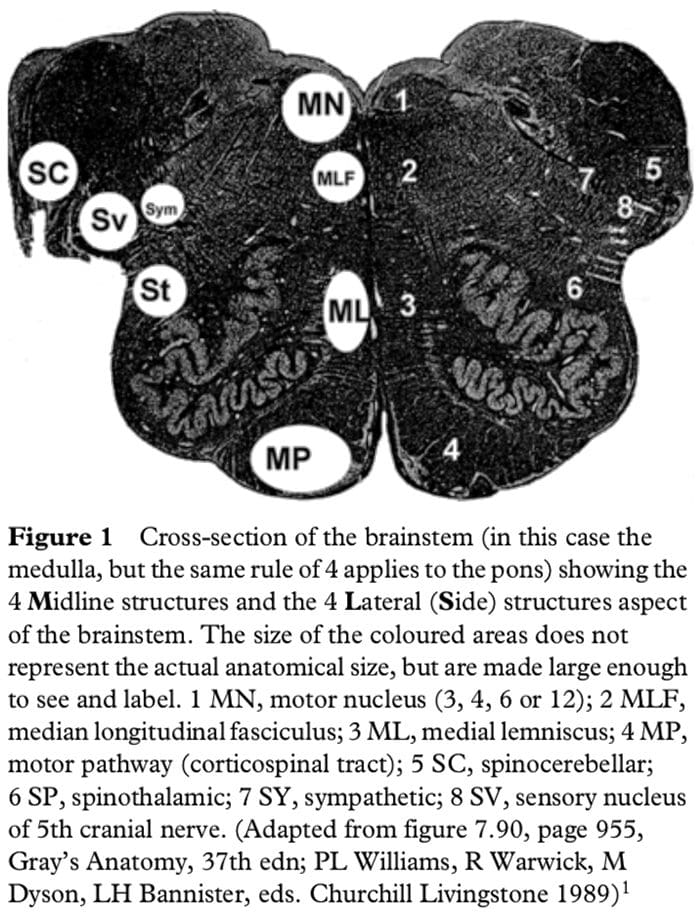
There are 4 structures in the �midline� beginning with M.
There are 4 structures to the side beginning with S.
There are 4 cranial nerves in the medulla, 4 in the pons and 4 above the pons (2 in the midbrain).
The 4 motor nuclei that are in the midline are those that divide equally into 12 except for 1 and 2, that is 3, 4, 6 and 12 (5, 7, 9 and 11 are in the lateral brainstem).
If you can remember these rules and know how to examine the nervous system, in particular the cranial nerves, then you will be able to diagnose brainstem vascular syndromes with ease.
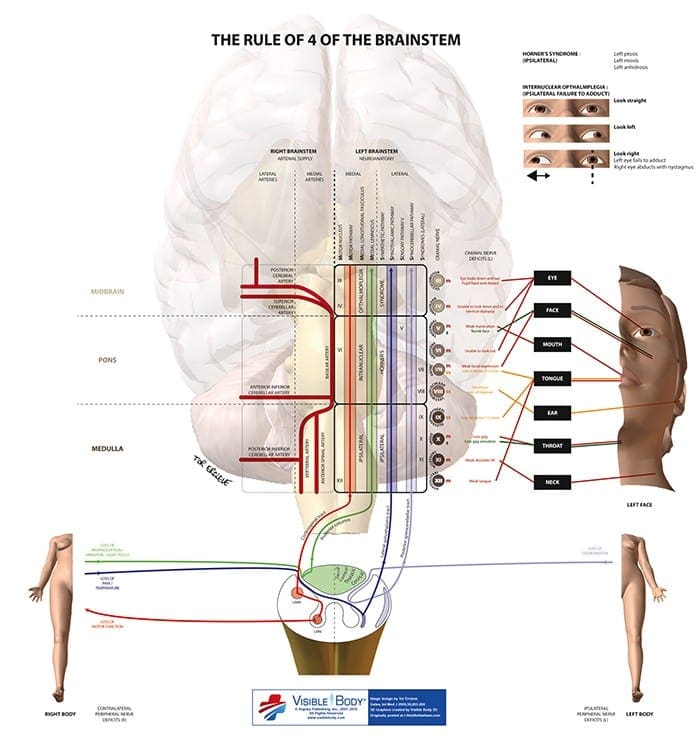
Figure 1 shows a cross-section of the brainstem, in this case at the level of the medulla, but the concept of 4 lateral and 4 medial structures also applies to the pons, only the 4 medial structures relate to midbrain vascular syndromes.
The 4 Medial Structures & The Associated Deficit Are:
The Motor pathway (or corticospinal tract): contra lateral weakness of the arm and leg.
The Medial Lemniscus: contra lateral loss of vibration and proprioception in the arm and leg.
The Medial longitudinal fasciculus: ipsilateral inter- nuclear ophthalmoplegia (failure of adduction of the ipsilateral eye towards the nose and nystagmus in the opposite eye as it looks laterally).
The Motor nucleus and nerve: ipsilateral loss of the cranial nerve that is affected (3, 4, 6 or 12).
The 4 Lateral Structures & The Associated Deficit Are:
The Spinocerebellar pathways: ipsilateral ataxia of the arm and leg.
The Spinothalamic pathway: contra lateral alteration of pain and temperature affecting the arm, leg and rarely the trunk.
The Sensory nucleus of the 5th: ipsilateral alteration of pain and temperature on the face in the distribution of the 5th cranial nerve (this nucleus is a long vertical structure that extends in the lateral aspect of the pons down into the medulla).
The Sympathetic pathway: ipsilateral Horner�s syndrome, that is partial ptosis and a small pupil (miosis)
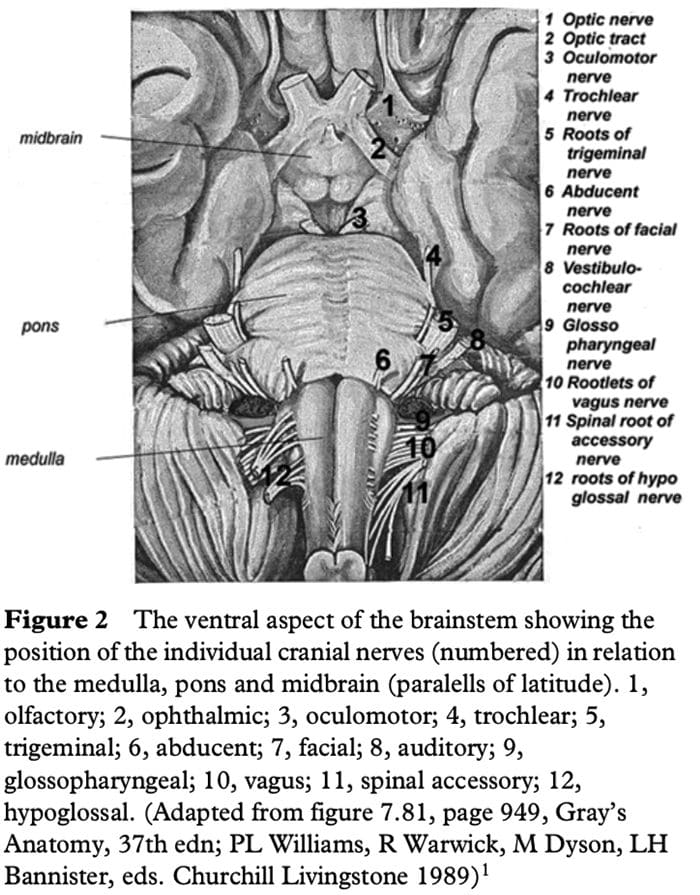
These pathways pass through the entire length of the brainstem and can be likened to �meridians of longitude� whereas the various cranial nerves can be regarded as �parallels of latitude�. If you establish where the meridians of longitude and parallels of latitude intersect then you have established the site of the lesion.
Figure 2 shows the ventral aspect of the brainstem.
The 4 Cranial Nerves In The Medulla Are:
9 Glossopharyngeal: ipsilateral loss of pharyngeal sensation. 10 Vagus: ipsilateral palatal weakness. 11 Spinal accessory: ipsilateral weakness of the trapezius and sternocleidomastoid muscles. 12 Hypoglossal: ipsilateral weakness of the tongue.
The 12th cranial nerve is the motor nerve in the midline of the medulla. Although the 9th, 10th and 11th cranial nerves have motor components, they do not divide evenly into 12 (using our rule) and are thus not the medial motor nerves.
The 4 Cranial Nerves In The Pons Are:
5 Trigeminal: ipsilateral alteration of pain, temperature and light touch on the face back as far as the anterior two-thirds of the scalp and sparing the angle of the jaw. 6 Abducent: ipsilateral weakness of abduction (lateral movement) of the eye. 7 Facial: ipsilateral facial weakness. 8 Auditory: ipsilateral deafness.
The 6th cranial nerve is the motor nerve in the pons.
The 7th is a motor nerve but it also carries pathways of taste, and using the rule of 4 it does not divide equally in to 12 and thus it is not a motor nerve that is in the midline. The vestibular portion of the 8th nerve is not included in order to keep the concept simple and to avoid confusion. Nausea and vomiting and vertigo are often more common with involvement of the vestibular connections in the lateral medulla.
The 4 Cranial Nerves Above The Pons Are:
4 Olfactory: not in midbrain. 5 Optic: not in midbrain. 6 Oculomotor: impaired adduction, supraduction and infraduction of the ipsilateral eye with or without a dilated pupil. The eye is turned out and slightly down. 7 Trochlear: eye unable to look down when the eye is looking in towards the nose.
The 3rd and 4th cranial nerves are the motor nerves in the midbrain.
Thus a medial brainstem syndrome will consist of the 4 M�s and the relevant motor cranial nerve, and a lateral brainstem syndrome will consist of the 4 S�sand either the 9�11th cranial nerve if in the medulla, or the 5th, 7th and 8th cranial nerve if in the pons.
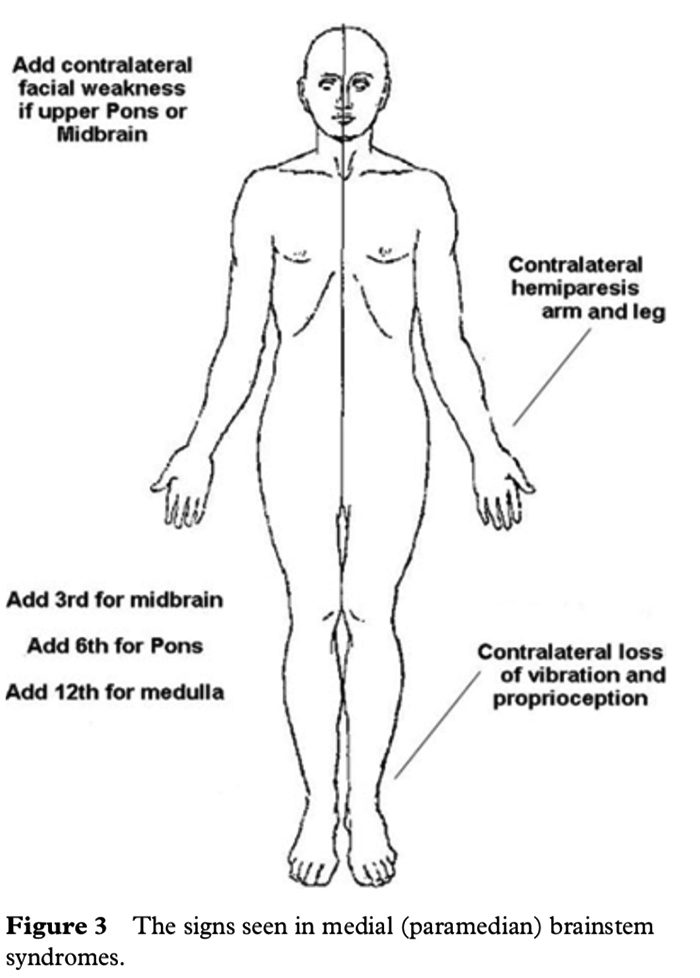
MEDIAL (PARAMEDIAN) BRAINSTEM SYNDROMES
Let us assume that the patient you are examining has a brainstem stroke. If you find upper motor neurone signs in the arm and the leg on one side then you know the patient has a medial brainstem syndrome because the motor pathways is paramedian and crosses at the level of the foramen magnum (decussation of the pyramids). The involvement of the motor pathway is the �meridian of longitude�. So far the lesion could be anywhere in the medial aspect of the brainstem, although if the face is also affected it has to be above the mid pons, the level where the 7th nerve nucleus is.
The motor cranial nerve �the parallels of latitude� indicates whether the lesion is in the medulla (12th), pons (6th) or midbrain (3rd). Remember the cranial nerve palsy will be ipsilateral to the side of the lesion and the hemiparesis will be contralateral. If the medial lemniscus is also affected then you will find a contra lateral loss of vibration and proprioception in the arm and leg (the same side affected by the hemiparesis) as the posterior columns also cross at or just above the level of the foramen magnum. The median longitudinal fasciculus (MLF) is usually not affected when there is a hemiparesis as the MLF is further back in the brainstem.
The MLF can be affected in isolation �a lacunar infarct� and this results in an ipsilateral internuclear ophthalmoplegia, with failure of adduction (movement towards the nose) of the ipsilateral eye and leading eye nystagmus on looking laterally to the opposite side of the lesion in the contra lateral eye. If the patient had involvement of the left MLF then, on being asked to look to the left, the eye movements would be normal, but on looking to the right the left eye would not go past the midline, while there would be nystagmus in the right eye as it looked to the right.
Figure 3 shows the clinical features of the medial brainstem syndromes.
LATERAL BRAINSTEM SYNDROMES
Once again we are assuming that the patient you are seeing has a brainstem problem, most likely a vascular lesion. The 4 S�s or �meridians of longitude� will indicate that you are dealing with a lateral brainstem problem and the cranial nerves or �parallels of latitude� will indicate whether the problem is in the lateral medulla or lateral pons.
A lateral brainstem infarct will result in ipsilateral ataxia of the arm and leg as a result of involvement of the Spinocerebellar pathways, contralateral alteration of pain and temperature sensation as a result of involvement of the Spinothalamic pathway, ipsilateral loss of pain and temperature sensation affecting the face within the distribution of the Sensory nucleus of the trigeminal nerve (light touch may also be affected with involvement of the spinothalamic pathway and/or sensory nucleus of the trigeminal nerve). An ipsilateral Horner�s syndrome with partial ptosis and a small pupil (miosis) is because of involvement of the Sympathetic pathway. The power tone and the reflexes should all be normal. So far all we have done is localize the problem to the lateral aspect of the brainstem; by adding the relevant 3 cranial nerves in the medulla or the pons we can localize the lesion to this region of the brain.
The lower 4 cranial nerves are in the medulla and the 12th nerve is in the midline so that 9th, 10th and 11th nerves will be in the lateral aspect of the medulla. When these are affected, the result is dysarthria and dysphagia with an ipsilateral impairment of the gag reflex and the palate will pull up to the opposite side; occasionally there may be weakness of the ipsilateral trapezius and/or sternocleidomastoid muscle. This is the lateral medullary syndrome usually resulting from occlusion of the ipsilateral vertebral or posterior inferior cerebellar arteries.
The 4 cranial nerves in the pons are: 5th, 6th, 7th and 8th. The 6th nerve is the motor nerve in the midline, the 5th, 7th and 8th are in the lateral aspect of the pons, and when these are affected there will be ipsilateral facial weakness, weakness of the ipsilateral masseter and pterygoid muscles (muscles that open and close the mouth) and occasionally ipsilateral deafness. A tumour such as an acoustic neuroma in the cerebello-pontine angle will result in ipsilateral deafness, facial weakness and impairment of facial sensation; there may also be ipsilateral limb ataxia if it compresses the ipsilateral cerebellum or brainstem. The sympathetic pathway is usually too deep to be affected.
If there are signs of both a lateral and a medial (paramedian) brainstem syndrome, then one needs to consider a basilar artery problem, possibly an occlusion.
In summary, if one can remember that there are 4 pathways in the midline commencing with the letter M, 4 pathways in the lateral aspect of the brainstem commencing with the letter S, the lower 4 cranial nerves are in the medulla, the middle 4 cranial nerves in the pons and the first 4 cranial nerves above the pons with the 3rd and 4th in the midbrain, and that the 4 motor nerves that are in the midline are the 4 that divide evenly into 12 except for 1 and 2, that is 3, 4, 6 and 12, then it will be possible to diagnose brainstem vascular syndromes with pinpoint accuracy.
P. GATES
The Geelong Hospital, Barwon Health, Geelong, Victoria, Australia
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine








 LATERAL BRAINSTEM SYNDROMES
LATERAL BRAINSTEM SYNDROMES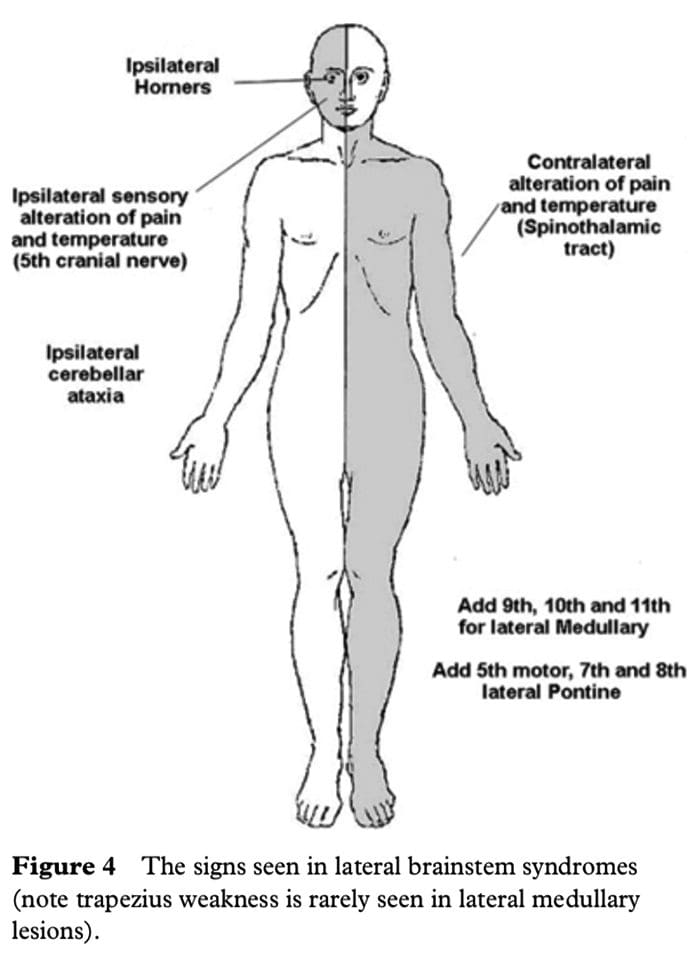 The lower 4 cranial nerves are in the medulla and the 12th nerve is in the midline so that 9th, 10th and 11th nerves will be in the lateral aspect of the medulla. When these are affected, the result is dysarthria and dysphagia with an ipsilateral impairment of the gag reflex and the palate will pull up to the opposite side; occasionally there may be weakness of the ipsilateral trapezius and/or sternocleidomastoid muscle. This is the lateral medullary syndrome usually resulting from occlusion of the ipsilateral vertebral or posterior inferior cerebellar arteries.
The lower 4 cranial nerves are in the medulla and the 12th nerve is in the midline so that 9th, 10th and 11th nerves will be in the lateral aspect of the medulla. When these are affected, the result is dysarthria and dysphagia with an ipsilateral impairment of the gag reflex and the palate will pull up to the opposite side; occasionally there may be weakness of the ipsilateral trapezius and/or sternocleidomastoid muscle. This is the lateral medullary syndrome usually resulting from occlusion of the ipsilateral vertebral or posterior inferior cerebellar arteries.





