We are very excited to announce that another Spinal Research Foundation facilitated research has been published in a highly reputable journal.�The study, undertaken by Heidi Haavik, Kelly Holt, Bernadette Murphy and others is�published in the�Journal of Neural Plasticity. And the results are very exciting for chiropractic!
The�Journal of Neural Plasticity boasts an impact factor of 3.5 (as a comparison, The Journal of Manipulative and Physiological Therapeutics has an impact factor of 1.5.)
This from Heidi Haavik:
�WE DO KNOW THAT SPINAL FUNCTION DOES AFFECT BRAIN FUNCTION.�THERE�S NOW SOLID EVIDENCE THAT ADJUSTING THE SPINE CHANGES BRAIN FUNCTION. THIS IS THE FOURTH TIME THAT THE EFFECT OF ADJUSTING THE SPINE HAS ON THE BRAIN HAS BEEN STUDIED. THIS LAST TIME IT WAS STUDIED AND CONFIRMED BY AN INDEPENDENT MEDICAL RESEARCHER.�
This study�was conducted�in an independent medical professor�s lab, where his bioengineer collected and analyzed the data. This is an important�bonus for this study ��that all data was collected and analyzed by scientists who had no preconceived ideas about chiropractic.�This greatly�lowers the level of bias.��These were scientists from Aalborg University Hospital in Denmark.
A Vitally Important Implication
More than just confirming once again that adjusting the spine has an effect on the brain, this study indicates that adjustments impact the function of the prefrontal cortex. Haavik is particularly excited about what this implies:
�The latest study suggests that the changes that we do see in the brain when we adjust the spine do occur in the prefrontal�cortex. That part of the brain is like the conductor in the brain.�
The research shows that�when we adjust the spine, we significantly increase activity in the prefrontal cortex. �The study showed a change in brain function by almost 20% on average�. The prefrontal cortex is the area in the brain where higher learning and�cognition happens. Haavik explains:
�An effect on the function of the prefrontal cortex could explain many previous research results, such as improvements in sensorimotor function relevant to falls-prevention; better joint-position sense in both the upper limb and the lower limb; improved muscle strength in lower limb muscles; better pelvic floor control; and better ability to carry out mental rotation of objects.�
Chiropractors have long observed a wide variety of changes in the people under their care following adjustments. Along the wide spectrum of claims from those under care are those who say they feel better or focus better and those who notice improvements in movement and coordination. This study takes us a little further down the path of understanding why this could be.
These are important control mechanisms run by the prefrontal cortex. For example,�joint position sense is the brain�s ability to know where the arms and legs are in space. And mental rotation is important, because as Haavik explains:
�Being able to accurately perceive the world around you is a vital skill we need all day every day. To recognize some objects you may need to mentally rotate them. For example to recognize the letter p versus b if they were not upright you would need to rotate them in your mind to figure out which letter it was. We all do mentally rotate shapes and objects we see, but we may not often think about that we do it, or how important this is in our daily life.�
Haavik and her team are excited about the evidence regarding the location of changes post-adjustment.
�THIS IS SOLID SCIENTIFIC EVIDENCE THAT ADJUSTING THE SPINE CHANGES THE WAY THE PREFRONTAL CORTEX OF THE BRAIN IS PROCESSING INFORMATION FROM THE ARM. IT DEMONSTRATES WE CHANGE THE WAY THE BRAIN WORKS AND SHOWS THAT SPINAL FUNCTION IMPACTS BRAIN FUNCTION. ONE OF THE MOST INTERESTING THINGS ABOUT THE CHANGES WE OBSERVED WAS THAT THE PREFRONTAL CORTEX IS RESPONSIBLE FOR BEHAVIOR, GOAL DIRECTED TASKS, DECISION MAKING, MEMORY AND ATTENTION, INTELLIGENCE, PROCESSING OF PAIN AND EMOTIONAL RESPONSE TO IT, AUTONOMIC FUNCTION, MOTOR CONTROL, EYE MOVEMENTS AND SPATIAL AWARENESS.�
If, as this research suggests, adjusting improves prefrontal cortex activity, a part of the brain that is responsible for just so much higher level function, then what does this mean in terms of chiropractic�s impact on things like�behavior, decision making, memory and attention, intelligence, processing of pain and emotional response to it, autonomic function, motor control, eye movements and spatial awareness?
We already know that adjustments cause improvements in sensorimotor function relevant to falls-prevention; better joint-position sense in both the upper limb and the lower limb; improve muscle strength in lower limb muscles; better pelvic floor control; and better ability to carry out mental rotation of objects.
Why This Study Matters
Again, this study not only shows that when we adjust subluxations we change brain function. It changes�activity by 20% just by adjusting.
And this effect may be on the conductor in the brain.
This shows us that every time we�re adjusting someone, we�re having a big, positive effect on the brain. And a brain that�s functioning differently and conducting its activities better is sure to have an effect on the body.
Download a Poster
Keen to share�these amazing results with the people under your care in your practice?�Download a Poster�to use in practice.
What�s Next
The project�involved collaboration with researchers from Denmark, Canada and Australia.
We are proud to be able to facilitate studies like this one, as they help back our profession with peer-reviewed certainty.
Getting the word out to people in your practice is imperative. Knowledge is powerful, not just for chiropractors but for those whose lives have been touched by the power of chiropractic care. Too often, they know it works but they don�t know why.
Once again research shows adjusting the spine has an effect on the brain. This study indicates that adjustments impact the function of the prefrontal cortex.�For Answers to any questions you may have please call Dr. Jimenez at 915-850-0900
How a chiropractic adjustment works: A displaced or luxated vertebra is when the joint surfaces are completely separated. Subluxation is a partial or incomplete separation: one in which the articulating surfaces remain in partial contact. This latter condition is so often referred to and known by chiropractors as sub-luxation.
The relationship existing between bones and nerves are so nicely adjusted that anyone of the 200 bones, more especially those of the vertebral column, cannot be displaced ever so little without impinging upon adjacent nerves. Pressure on nerves excites, agitates, creates an excess of molecular vibration, whose effects, when local, are known as inflammation, when general, as fever.
A subluxation does not restrain or liberate vital energy. Vital energy is expressed in functional activity. A subluxation may impinge against nerves, the transmitting channel may increase or decrease the momentum of impulses, not energy.
�According to BJ Palmer, a subluxation represents a displaced bone that’s impinged on a nerve, which interferes with the transmission of vital nerve energy (or, more specifically, �mental impulses.�)�
For over hundred years, chiropractors have explained chiropractic medicine by teaching patients and the medical community that bones compress which irritate spinal nerves. The ensuing nervous system dysfunctions have negative effects on the function of peripheral nervous systems, central nervous systems and patients� overall ability to maintain homeostasis.
Essentially, they go into states of dis-ease.� These discussions were in large part due to the teachings of D.D. Palmer and B.J. Palmer as previously cited. Based on the results rendered in chiropractic offices across the country and in a patient-driven model of success, the general consensus in both private practice and chiropractic academia had been to maintain status quo and simply teach what has worked in the absence of conclusive evidence, particularly in light of a lack of serious governmental funding and support for chiropractic research.� In addition, dogma has also created blinders for many, as evidence evolves to further chiropractic and its understanding, application and expansion.
Research has been published and has begun to verify D.D. and B.J. Palmer�s hypotheses were correct. While clarifying the specific physiological mechanisms related to chiropractic�s ability to alleviate pain.� As a result of initially studying pain mechanisms, contemporary research has also begun to set the foundation for understanding why chiropractic works with systemic and autonomic dysfunction and potential disease treatment through the adjustment � central nervous system connection.
It is the understanding of that connection with pain that is helping people to begin to understand the full impact of the chiropractic spinal adjustment and render the evidence to help more get well.
CENTRAL NERVOUS SYSTEM & PAIN REDUCTION
Reductions in pain sensitivity, or hypoalgesia, after spinal manipulative therapy or a chiropractic adjustment may point to a mechanism related to the central nervous system processing of pain.�These findings indicate that a chiropractic spinal adjustment affects the dorsal horns at the root levels which are located in the central nervous system.
This is the beginning of the �big picture� since once we identify the mechanism by which we can positively influence the central nervous system, we can then study that process and its effects in much more depth.
One question asked, does a chiropractic adjustment cause a general response of pain sensitivity or if the response is specific to the area where adjustment is applied? For example, changes in pain sensitivity over the cervical facets following a cervical spine SMT would indicate a local and specific effect while changes in pain sensitivity in the lumbar facets following a cervical spine SMT would suggest a general effect.�
We observed a favorable change for increased PPT [pressure pain threshold] when measured at remote anatomical sites and a similar, but non-significant change at local anatomical sites. These findings lend support to a possible general effect of SMT beyond the effect expected at the local region of SMT application.
The adjustment mechanism is theorized to result from both spinal cord mediated mechanisms and the brain. A recent model of the mechanisms of manual therapy suggests changes in pain related to SMT result from an interaction of neurophysiological responses related to the peripheral nervous system and the central nervous system at the spinal and supraspinal level.
This demonstrates that�chiropractic adjustment influences the peripheral nervous system and the central nervous system.
ACTIVATION OF BRAIN & DESCENDING NERVE PATHWAYS BEYOND AREAS TREATED
CHIROPRACTIC ADJUSTMENT VS. SPINAL MOBILIZATION
Manual therapy has clinically shown to boost pressure pain thresholds (i.e., decrease sensitivity) in both symptomatic and asymptomatic subjects. Cervical spinal manipulation has been shown to result in unilateral as well as bilateral mechanical hypoalgesia.
Compared with no manual therapy, oscillatory spinal manual therapy at T12 and L4 produced significantly higher paraspinal pain thresholds at T6, L1, and L3 in individuals with rheumatoid arthritis.
The immediate and widespread hypoalgesia associated with manual therapy treatments has been attributed to alterations in peripheral and/or central pain processing including activation of descending pain inhibitory systems.
Manual therapy triggers the central nervous system which affects areas around those being treated.�Clinical studies show spinal manipulation or an adjustment alters the central processing of mechanical stimuli. This is proven by an increased pressure pain threshold and decreased pain sensitivity in asymptomatic and symptomatic subjects following manipulation.
The thalamus also regulates states of sleep and wakefulness which plays a major role in regulating arousal, the level of awareness, and activity (Thalamus�http://en.wikipedia.org/wiki/Thalamus).
Therefore, a�chiropractic adjustment reduces pain through the thalamus. �In addition, with current knowledge of chiropractic adjustment effecting the thalamus, we can begin to offer an explanation of how the first historically reported chiropractic adjustment by D.D. Palmer helped Harvey Lilard regain his hearing.
CHIROPRACTIC REDUCES PAIN IN MULTIPLE REGIONS DUE TO LOCAL AND CNS STIMULATION
Significant changes were observed on sensory parameters, supporting the hypothesis of centrally mediated effects of a single adjustment. This suggests that the�chiropractic spinal adjustment affects the nociceptors and the mechanoreceptors at the joint level causing central modulation of an effect at the cord and/or brain level(s) and pain reductions in multiple areas as a result.
AN ADJUSTMENT WILL CREATE HIGHER FUNCTION IN CORTICAL AREAS
MT or manual therapy/chiropractic adjustment reduce pain intensity and pain sensitivity. it is reasonable to assume that the underlying therapeutic effect of MT is likely to include a higher cortical component.
In other words, thoracic adjustments produced direct and measureable effects on the central nervous system across multiple regions, which in the case of the responsible for the processing of emotion (cingulate cortex, aka limbic cortex) are regarding the insular cortex which also responsible for regulating emotion as well has homeostasis.
The motor cortex is involved in the planning and execution of voluntary movements, the amygdala�s primary function is memory and decision making (also part of the limbic system), the somatosensory cortex is involved in processing the sense of touch (remember the homunculus) and, finally, the periaqueductal gray is responsible for descending pain modulation (the brain regulating the processing of painful stimuli).
Periaqueductal Gray � � � Ascending and descending spinothalamtic tracts carrying pain and temperature fibers
The global effects of a chiropractic adjustment simply put, the processing of pain may be modulated or regulated from an external force without the use of pharmacy or surgery? Pain is deeply tied to the most primitive regions of the central nervous system and it appears (as chiropractors have observed clinically for 116 years) that therapeutically speaking, we can have an influence on these higher centers with little or no side-effects.
Chiropractic spinal adjustments create functional changes in multiple regions of the brain. In addition, this has far reaching effects in setting the foundation for understanding how the adjustment works in systemic and possibly autonomic changes by being able to measure and reproduce functional changes within the brain as direct sequellae.
MUSCLE IMPAIRMENT CREATES CNS ALTERATIONS & THE�NECESSITY FOR BOTH SHORT-TERM & LONG-TERM�CHIROPRACTIC CARE
ADJUSTMENTS WORK � SPINAL MOBILIZATION DOES NOT
What this means is that there are observable changes in the function of the central nervous system seen in patients with musculoskeletal conditions.� That is something that chiropractors have observed clinically and shows the medical necessity for chiropractic care for both short and long term management as well as in the prevention of pain syndromes.
Evidence suggests that muscle damage occurs early in spinal complaints, and that such muscle damage does not automatically resolve even when pain symptoms improve. This has led some authors to suggest that the deficits in proprioception and motor control, rather than the pain itself, may be the main factors defining the clinical picture and chronicity of various chronic pain conditions.
This evidence suggests that chiropractic manipulation may have a positive neuromodulatory effect on the central nervous system, and this may play a role in the effect it has in the treatment of neck pain.
When the input signal is no longer encoded as a result of joint dysfunction and altered afferent input, the cerebellum must adjust to new encodings that dictate the body schema and affect proper execution of the motor task.
The significance is that it suggests that chiropractic adjustments improve neck dysfunction, and through plasty changes in the cerebellum, there is resultant motor learning and increased function.
CONCLUSION
Chiropractic adjustments influence the peripheral nervous system and the central nervous system. In the central nervous system, chiropractic spinal adjustments reduce pain by effecting the thalamus and descending central pain pathways.
The areas of the brain affected by chiropractic adjustments effect the following functions: emotions, learning, motivation, memory, consciousness, homeostasis, perception, motor control, self-awareness, cognitive function, voluntary movements, decision making, touch, temperature, pain of the skin- epithelial tissue-skeletal muscles-bones-internal organs and cardiovascular system.
For over hundred years, chiropractors have explained chiropractic medicine by teaching patients and the medical community that bones compress which irritate spinal nerves. People have begun�to understand the full impact of the chiropractic spinal adjustment and render the evidence to help more people get well.
Most people don�t go to a chiropractor for a better sex life, but that extra benefits is a pretty happy accident. �People come in with back pain, but after adjustments, they come back and tell me their sex life is so much better,� says Jason Helfrich, co-founder and CEO of 100% Chiropractic. �It�s no surprise to us�it�s amazing what the body will do when you take away the pressure on the nervous system.�
And what are those amazing feats, exactly?
Let�s start with what a chiropractor really does. Every function in your body is controlled from the nervous system, but when vertebra are off position�known as a subluxation�the nerves traveling between your brain and your muscles can become blocked, compromising your body�s ability to function as it needs to. Every chiropractor�s goal is to remove these subluxations, since they can both cause pain and impede feeling, Helfrich says.
But these fixes help more than just back pain. The lumbar region (your lower back) is a huge hub for the nerves that extend into your reproductive regions. Removing lumbar subluxations can improve nerve flow to your sexual organs, increasing things like blood flow to your clitoris or, for your husband, the penis.
The flow of nerve signals is a two-way street, though, meaning that adjustments also allow your organs to send messages to the brain more easily. This means that you not only do you become physically aroused faster, but your brain also registers that ready-for-action, heightened sense of pleasure more quickly, so you move past the mental obstacles that may be keeping you from orgasming, Helfrich explains.
The other key adjustment area for a better sex life?
Right below your brain stem, around the vertebrae known as C1 and C2. �Libido and fertility require a delicate balance of estrogen, progesterone, and other hormones, many of which are released in the upper cervical and neck area,� he explains. If there are any blockages right out of the brain, the impingement up there will have an effect all the way down.
Even your fertility is affected by the nerves and hormones coming out of the spine, as they control your reproductive cycle.
But beyond all of the physiological benefits of tweaking your spine to perfection, chiropractic adjustments can also simply give your muscles more range of motion. This means you can try previously impossible positions under the sheets.
�We want to improve people�s health, and health is about living life as its intended. Having a great sex life is huge part of that,� Helfrich adds. No arguments here!
Most people don�t go to a chiropractor for a better sex life, but the extra benefit is a pretty happy accident. �People come in with back pain, but after an adjustment, they come back and tell me their sex life is so much better.�
Proven�research is now indicating that receiving Chiropractic adjustments to the pelvis can�increase vertical jump height. �This new research further solidifies the stance of many professional and collegiate teams with providing Chiropractic care for their athletes. In addition to injury prevention this research proves that chiropractic care results in an increase in sports performance.
[Purpose] This study aimed to investigate the effect of pelvic adjustment on vertical jump height (VJH) in female university students with functional leg length inequality (FLLI). [Subjects] Thirty female university students with FLLI were divided into a pelvic adjustment group (n = 15) and a stretching (control) group (n = 15). [Methods] VJH was measured using an OptoGait. [Results] After the intervention, jump height improved significantly compared with the pre-intervention height only in the pelvic adjustment group, while FLLI showed statistically significant improvement in both groups. [Conclusion] Pelvic adjustment as per the Gonstead method can be applied as a method of reducing FLLI and increasing VJH.
Key words:�Pelvic adjustment, Functional leg length inequality, Vertical jump height
INTRODUCTION
The pelvis, a structure located between the hip joint and the lumbosacral spine and attached to several muscles, regulates the movement of the hip joint and lumbosacral spine. The position of the pelvis is the most critical factor determining the sagittal alignment and posture of the human body). Only when the pelvis is in the neutral position can be in the right posture, move the upper and lower body in the dynamic posture, and improve daily movements and ambulatory ability).
Functional leg length inequality (FLLI) worsens due to pelvic tilt in the medial plane and pelvic rotation in the sagittal plane). Therefore, FLLI might be improved by pelvic adjustment. High-velocity and low-amplitude (HVLA) adjustment has been widely utilized as a general chiropractic adjustment method). Many studies have indicated that leg length inequality (LLI) causes posture alteration), limiting exercise and causing tension of the muscles and other soft tissues5). LLI is accompanied by several clinical symptoms6)�such as lumbar pain)�and hip pain). Correcting leg length inequality reportedly reduces pain, increases mobility, and improves posture).
Vertical jumping is practiced to enhance the muscular strength and endurance of the leg and serves as a barometer of muscular strength). There have been studies in which plyometric training was undertaken to improve leg muscle strength), dynamic stretching was applied after jogging for 5 minutes to improve vertical jump height (VJH), or HVLA manipulation was performed for talocrural joint dysfunction). However, there has been no study in which FLLI was corrected and VJH was measured as a barometer for leg muscle strength. Many studies have assessed the effect of pelvic adjustment on FLLI), posture), pressure on the foot, and balance). However, no study has investigated the changes in FLLI and VJH resulting from just a single adjustment. Therefore, this study aimed to assess the immediate effects of a single pelvic adjustment on FLLI and VJH in female university students with FLLI.
SUBJECTS AND METHODS
A total of 30 female university students with an FLLI of more than 10?mm between the left and right legs were selected and randomly assigned to one of two groups: the pelvic adjustment group (adjustment group, n = 15) and control group (stretching group, n = 15). The exclusion criteria were as follows: anatomical LLI; degenerative osteoarthritis; muscle, bone, or nervous system problems; ankle joint, knee joint, hip joint, or lumbar pain; limited range of motion due to burn or postsurgical scarring; and regular leg exercise. This study was approved by Korea Nazarene University�s Institutional Review Board, and the safety of all subjects was protected during all parts of the experiment. All subjects understood the purpose of this study and provided written informed consent prior to participation in accordance with the ethical standards of the Declaration of Helsinki.
The age, height, and weight of the subjects in the adjustment group were 23.5�4.7?years, 163.0�5?cm, and 54.1�5?kg, while those in the stretching group were 22.2�6.3?years, 162.7�6?cm, and 53.1�6?kg, respectively. Gender was analyzed using the ?2�test, while age, height, and weight were analyzed using the independent t-test. As these analyses detected no statistically significant differences (p>0.05), the two groups were deemed identical.
The pelvic adjustment performed in the adjustment group consisted of an HVLA technique administered in the prone posture in accordance with Gonstead�s theory. Subjects were instructed to lie prone, their pelvic height was checked, and the posterior-inferior innominate bone was given an anterior-superior impact while the anterior-superior pelvis was given a posterior-inferior impact. When making these impacts, the therapist put one of his hands on top of the other, placed them on the posterior-superior iliac spine or the ischial spine, and then gave the impact using his own weight, gravity, and acceleration). This adjustment was performed 3�5 times by one skilled physical therapist with more than 10?years of clinical experience. The control group stretched the backbone erector, rectus abdominis, iliac muscle, psoas major, quadriceps muscle, leg adductor, and quadratus lumborum adjacent to the pelvis in order to resolve muscular imbalance that could further the pelvic imbalance. In the process, the therapist assisted the subjects in performing additional height training for each muscle and maintaining each posture at the maximum height for 10�15 seconds. The subjects then resumed the initial posture, rested for 5 seconds, and repeated the stretching one more time. Stretching was done three times per posture for a total of 15 minutes).
For leg length measurement, subjects lay straight on a bed, and the tape measure method (TMM) was used to measure the leg from the anterior superior iliac spine (ASIS) to the medial malleolus. Beattie et al. reported that LLI as measured by the TMM did not show a significant difference from radiological findings. We were therefore confident in the reliability of using the TMM for measuring leg length). The measurement started from the ASIS so that pelvic bone-related problems such as pelvic tilt and pelvic asymmetry could be included.
We used an OptoGait (Microgate Srl, Bolzano, Italy), a system for optical detection, to analyze ambulation and measure VJH. On its signal-sending bar, there are 96 LEDs that communicate via an infrared frequency. The signal-receiving bar has an identical number of LEDs. We installed the signal-sending and signal-receiving bars of the OptoGait one meter apart on a flat surface. When a subject performs a vertical jump between the bars, the bars calculate the time at which the subject touches the floor or stays in the air and communicates this information by sending and receiving 1,000 signals per second, generating accurate data. Based on this basic data, the OptoGait software calculates the precise VJH.
Leg length and VJH were measured before and after the intervention. The measured data were analyzed using the statistics program SPSS 12.0 KO (SPSS, Chicago, IL, USA), and the collected data are presented as averages and standard deviations. The significance of pre- and post-intervention differences was tested using the paired t-test, and the significance of between-group differences was tested using the independent t-test. The p-value ? was set at 0.05.
RESULTS
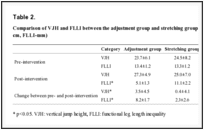
In the pre- and post-intervention comparison, VJH improved significantly only in the adjustment group, while FLLI improved significantly in both the adjustment group and the stretching group (p<0.05) (Table 1). When comparing the pre-intervention data, post-intervention data, and changes between the pre- and post-intervention data, VJH showed statistical significance only for the changes between the pre-and post-intervention data, while FLLI showed statistical significance for post-intervention data and changes between the pre- and post-intervention data (p<0.05) (Table 2).
Table 1.
Comparison of the Pre- and post-intervention data for VJH and FLLI in each group (mean�SD) (Unit: VJH-cm, FLLI-mm)
Table 2.
Comparison of VJH and FLLI between the adjustment group and stretching group (mean�SD) (Unit: VJH-cm, FLLI-mm)
DISCUSSION
The pelvis supports the abdomen, connects the spine and legs, and is involved in transferring weight from the spine to the legs when a person stands up, maintaining a straight posture and enabling smooth arm movements). Due to their erect ambulation, human beings are exposed to gravity and can thus be subject to a malalignment of the pelvis and legs affecting posture, ambulatory pattern, and balance. LLI is easily observed clinically and causes functional disturbance of normal biomechanics).
Winter and Pinto reported that pelvic obliquity is caused by LLI), and Mccaw and Bates explained the relation between biomechanics and spinal deformity due to LLI). Defrin et al. reported that when a shoe insert was used in 22 chronic back pain patients with LLI of 10?mm and less, pain intensity and muscular weakening were reduced), which appears to be due to reduced pain and muscular weakening attributed to decreased pelvic tilt resulting from LLI adjustment. On the basis of previous studies on pelvic adjustment, Alcantara et al. reported that following adjustments using fast and slow speed amplitudes in patients with sacroiliac joint obliquity, pain was reduced, and patients could resume daily life and work). Park et al. reported that balance in 20 elderly men was improved through pelvic adjustment according to the Gonstead method). In this study, FLLI was reduced after pelvic adjustment, a finding similar to a previous study in which pelvic adjustment helped reduce FLLI and the pressure difference between soles).
In this study, stretching was not associated with increased VJH, while pelvic adjustment was. In a previous study by Ryan et al. in which subjects jogged for 5 minutes in order to improve VJH, a barometer for leg strength, and then performed dynamic stretching, VJH was increased as compared with a control group that only jogged for 5 minutes). In the present study, it is suspected that VJH did not increase because only static stretching was applied. Hedlund et al. reported that VJH showed a statistically significant increase following 3 weeks of chiropractic HVLA manipulation in 22 female handball players with talocrural joint dysfunction, which is similar to the findings of the present study).
Pelvic adjustment balances the left and right pelvic height and left and right anterior and posterior rotation of the hip bones, which, in turn, leads to FLLI improvement. It also balances the left and right muscle lengths of the rectus femoris and sartorius, which are involved in the hip bone�s anterior rotation, and the hamstring and gluteus maximus, which are involved in posterior rotation. This seems to explain the improvement in vertical jump ability. We recommend that pelvic adjustment be applied for decreasing FLLI and increasing VJH, a barometer for leg muscle strength, in the future.
Research now indicates that receiving Chiropractic Adjustments to the pelvis can�increase vertical jump height. �This research solidifies many professional and collegiate teams that�provide chiropractic care for their athletes. In addition to injury prevention this research proves that chiropractic care results in greater athletic performance.
are impairments in detecting, modulating, interpreting, or responding to sensory stimuli. One study estimates that 5 percent of elementary aged children met the criteria for SPD. These conditions are closely related to other neurodevelopmental disorders and often overlap with autism and ADHD. Recent studies have shown the benefits of chiropractic in enhancing the functionality of individuals with SPD and Autism.
In 2011, we have more children and young adults affected by neurodevelopmental disorders than ever before in history. There are many factors involved in this such as birth and/or early childhood trauma, environmental toxins, food allergens, the avoidance of breast feeding and heavy vaccination. These are all areas that show promise as causative factors in the formation of neurodevelopmental disorders.
Birth trauma can come in the form of a forceps or vacuum extraction delivery. Even normal vaginal or cesarean birth processes can be particularly traumatic. The most vulnerable area of the infant�s body is the upper cervical spine. This also happens to be the area where the brain stem ties into the top of the spinal cord. Birth trauma can significantly damage this region andcreate a neurological insult that is referred to as subluxation.
Subluxation alters neurological processing
Subluxation is a term used to describe mechanical compression and irritation to spinal joints and nerves. Subluxation scrambles the neurological feedback loop by causing altered rhythms of neurological flow. Subluxation insults the neurology of the infant and affects normal development and maturation. This can often create an environment conducive to the formation of neurodevelopmental disorders such as autism, ADHD andSPD.
Many chiropractors specialize in the location, diagnosis and correction of subluxation patterns in infants and young children. These chiropractors often have unique training with digital technology that uses thermographic and surface electromyography to calibrate the function of the nervous system and identify areas of neurological insult. They are also gifted with palpation, posture and body motion observations to locate specific biomechanical and neurological imbalances in the young child.
Spinal Decompression Therapy
Two recent studies published in the 2011 edition of the Journal of Pediatric, Maternal & Family Health showed the benefits of chiropractic on SPD and Autism. In both cases the children were diagnosed with upper cervical subluxation patterns that were thought to have occurred from early childhood traumas. The children also showed signs of neurological imbalance and subluxation in other regions of the spine. Results of their care were startling and would naturally be considered major breakthroughs in the medical model.
The children�s care consisted of specific chiropractic adjustments for a period of weeks to remove subluxation and balance the neurology. They also followed an anti-inflammatory nutritional program that involved a gluten-free, casein-free diet and nutritional supplements such as probiotics and digestive enzymes.Most natural health practitioners would agree that the majority of children with neurodevelopmental disorders have neurological and digestive damage. The digestive issues typically involve leaky gut syndrome, gut dysbiosis, Candida infections and chronic food allergens. These problems typically present together and can be remedied with an anti-inflammatory diet and nutritional supplements.
There are 10 other case studies of children with similar neurodevelopmental issues who have seen significant improvements through chiropractic care. This is evidence of the role that subluxation plays in affecting normal sensory system maturation and development.
Hopefully these recent studies will shine a light on the impact of subluxation correction on healthy neurological balance. This can range from immune system disorders, chronic disease and neurodevelopmental problems. More research dollars should be spent on inexpensive, low risk, non-invasive modalities such as chiropractic care for childhood health problems and normal brain and immune system maturation processes.
Sensory Processing Disorders (SPD) are impairments in detecting, modulating, interpreting, or responding to sensory stimuli. One study estimates that 5 percent of elementary aged children met the criteria for SPD.
CHIROPRACTORS HAVE CLAIMED FOR YEARS THAT WE CAN BE MORE COST-EFFECTIVE. BCBS HAS THE DATABASE THAT WOULD PROVE OUR THESIS, BUT THERE SEEMS TO BE A RELUCTANCE TO ALLOW OUR PROFESSION TO ACCESS THE DATA THAT WOULD PROVE US RIGHT.
In August 1999, Blue Cross/Blue Shield (BCBS) of Kansas presented a study titled �Lumbago Treatment.� This data was made available from a new program installed by BCBS called the McKesson Episode Profiler.
This program gave BCBS the ability to sort data according to specific diagnoses and compared the costs, frequency, and other factors between peer groups.
The data revealed that while less than eight percent of the study group were chiropractors, 38 percent of the patients chose to seek chiropractic care rather that allopathic medicine. This fact indicates that patients desire and are satisfied with the management techniques of the chiropractor.
The study did not include any hospitalization costs for surgery or any fees paid to orthopedists or neurosurgeons for costs associated with surgery. If the data included costs for these procedures, the savings for chiropractic would have been much greater.
When sorted by the average cost per episode, chiropractic is more cost-effective than anesthesiology; neurosurgery; neurology; registered physical therapy; orthopedic reconstructive surgery; physical medicine and rehabilitation; and rheumatology.
The greatest cost-effectiveness of chiropractic is demonstrated when one considers the global cost of allopathic care. The physical therapist can only receive referrals from an allopathic provider. An allopath can only write prescriptions. The allopathic provider primarily orders surgeries, nerve conduction tests MRIs, and CT scans. Hospitalization charges are totally allopathic charges that cannot be associated with chiropractic. When these charges are considered, the tremendous economy of chiropractic management becomes indelibly clear.
The majority of chiropractic charges were associated with the basic office-treatment-related services performed. Eighty-nine percent of the chiropractic charges were for services related to the treatment, while only 45 percent of the family practice costs were related to treatment of the condition. The remainder of the costs were for expensive diagnostics.
Patients who visit the family practice provider have about a 15 percent chance that they will have a MRI or CAT scan. These services cost an average of over $1,000 and provide no treatment, only a diagnosis.
For each 100 episodes, the chiropractor provided 265 modalities. For each 100 episodes, the registered physical therapist provided 885 modalities: over three times as many units of physical therapy provided by RPTs than chiropractors. This is a cost that has to be globally charged to the family practice providers, since patients cannot access RPTs without a referral from a medical doctor.
Registered physical therapists provided 303 office visits per 100 episodes, compared to 255 by the chiropractor. When RPTs are combined with the other allopathic portals, there are 598 office visits per 100 episodes. Therefore, the myth claiming chiropractors treat the patient more than the allopathic portals is obviously just diversionary, and not based on facts.
Patients had a willingness to return to the chiropractor that was 22 percent greater than the combined totals of allopathic portals. This indicates a level of satisfaction that is demonstrated by the patient�s willingness to return, based on results and confidence.
The BCBS lumbago study demonstrates that chiropractic is not only cost-effective but also quality effective. Adding chiropractic services would only decrease the cost to the plan. What is hard to explain is the prejudice against chiropractic in the design of BCBS plans, and their reluctance to push the study and analysis of the data to the next level. It almost seems as though there is a fear that exists in the minds of those in positions of power, preventing them from presenting the cost comparisons with the global cost of allopathic portals to chiropractic. Chiropractors have claimed for years that we can be more cost-effective. BCBS has the database that would prove our thesis, but there seems to be a reluctance to allow our profession to access the data that would prove us right.
I guess the million-dollar questions are �Why?� and �What are they afraid of?� Perhaps it is the fear of knowing how to handle the data once it proved that chiropractic was more cost-effective. Perhaps it is getting past the mindset that adding chiropractic benefits is going to increase reimbursement levels. Perhaps they cannot see that there would not be a cost increase but a cost savings from directing patients to more cost-effective portals. Allowing osteopaths to treat broken arms did not increase the number of fractures; it simply shifted the point of access to treatment. Likewise, allowing patients to freely access chiropractic services would not increase the number of spinal related injuries; it would simply allow the patient access to desired and more cost-effective services.
I imagine that BCBS of Kansas regrets releasing the amount of information they already have. There seems to be a reluctance to push the analysis of the data to the next level. It is now up to the profession to �hold their feet to the fire� and push for more data to support the fact that chiropractic can be more cost-effective.
“Lumbago Study”�reveals 38 percent of patients chose to seek chiropractic care rather that allopathic medicine. This fact shows�that patients desire and are satisfied with management techniques of chiropractic care.
Chiropractors who provide care for children � and families � can attest to the many benefits of a healthy spine to a growing child. However, this relatively new area of focus for chiropractic is susceptible to many misconceptions, among the public and the health-care community.
Many of the public perceptions about chiropractic care for children, however, are far from the truth. We explore these misconceptions and spoke to the experts to get the real facts about this thriving chiropractic focus area.
Myth #1 Chiropractic care of children is new.
When some individuals first learn that DCs treat children as well as adults, they may get the wrong idea that chiropractic for kids is new � which is to say untested, experimental and dangerous.
That isn�t the case. Sure, the modern era of this field dates only as far back as the 1980s. But the fact is, the practice actually has much older and stronger roots. �If you go back to 1910, [founder of chiropractic] D.D. Palmer indicated how important it is to check a child�s spine from birth and throughout life,� notes Jeanne Ohm, CEO of the International Chiropractic Pediatrics Association (ICPA), a non-profit organization in Philadelphia.�
By the 1980s, many DCs had developed their practices to treat adults specifically. In 1986, Dr. Larry Webster in the U.S. helped re-establish chiropractic care for children as a legitimate area of focus. He started teaching his child-friendly techniques, and he created the ICPA to further help chiropractors treat children.
Webster passed away in 1997, but his legacy continues. The ICPA now has more than 4,000 members and hundreds of DCs are studying to become chiropractors with a special focus on kids.
Myth #2 Children don�t need chiropractic care.
DCs who treat kids often hear questions along these lines: Why in the world would a child need to see a chiropractor? What good does chiropractic do for a toddler, or even a newborn?
Chiropractors have a few good answers.
�We may see a one-week-old child who is already showing signs of favoring, turning her head to one side versus the other,� says Dr. Judy Forrester, owner of Synergea Family Health Centre, a multidisciplinary clinic in Calgary, Alta. �That may seem minimal� but if we can determine any imbalances or asymmetry with the muscular function or the joint alignment, and we address it early, it�s better. Once those postural patterns and habits develop as they grow, they can be much more difficult to change.�
Dr. Liz Anderson-Peacock is a Barrie, Ont., chiropractor who focuses on care for children. She notes the link between the central nervous systems and various childhood afflictions.
�Children may have symptoms like ear infections, difficulty breathing, colic, attention deficit. We do not treat those things per se. We see those as expressions of the body not interpreting the world properly,� explains Anderson-Peacock, who also serves in the editorial board for the Journal of Maternal, Pediatric and Family Health.
�The organizing system for us to respond to the world is the nervous system. The questions we ask are: if there is something going on with the nervous system, what is it, and can chiropractic care help?�
Anderson-Peacock now spends most of her time travelling around the world doing lectures and other speaking engagements. She also conducts seminars for the ICPA about chiropractic care for children and families.
Ohm from the ICPA links chiropractic to the very moment a child emerges from the womb. �Birth can be traumatic,� she says. The event could cause physical damage that leads to difficulties later. So if a baby develops breathing trouble, �the real cause may simply be a misalignment to the spine from the birth process. Parents who get that will stop at the clinic on the way home from the birth centre to make sure everything is OK.�
Chiropractic & Children
Myth #3 Chiropractors use the same techniques on children as adults.
�That�s what terrifies a lot of chiropractors about adjusting children, as well as parents,� Anderson-Peacock says. �They think we�re going to adjust them like an adult.�
But DCs who treat children do not apply heavy pressure. �Often, it�s a matter of moving the child into a position of ease, holding that position and things will reset quite nicely on their own,� Anderson-Peacock says. Care, she points out, is nowhere near as forceful as it may be for adults.
�That�s why extra training is so crucial. These children are not like miniature adults. For example, spines are primarily cartilaginous until the age of six, and we know cartilage will deform when we have abnormal function. So we want to make sure that function is restored normally. And since the bones are immature, the alignment issues are different. We want to minimize rotations and traction, because children have different needs, due to the immaturity of their musculoskeletal and ligamentous structures.�
The ICPA aims to validate techniques for chiropractic care for children, particularly to help dispel the idea that DCs use the same pressure on kids as they do on adults, Ohm notes. The organization is working with Walter Herzog, co-director of the Human Performance Laboratory at the University of Calgary, to study the pressure required when caring for children. The report should be out by the end of 2015.
Chiropractic & Children with Chronic Conditions
Myth #4 There are no real experts in chiropractic care for children.
In Canada, chiropractic care for children is not a recognized area of specialty, which leads some people to think there are no genuine experts in the field. But that isn�t true.
Many DCs follow accredited courses to develop child-specific skills. Anderson-Peacock spent three years studying at the International Chiropractors Association�s Council on Chiropractic Education (CCE)-accredited program in pediatric chiropractic. She achieved her Diplomate in Clinical Chiropractic Pediatrics (DICCP) in 1996.
Dr. Stacey Hornick is owner of Market Mall Family Chiropractic in Saskatoon, Sask. She attended McTimoney College of Chiropractic, operated by BPP University � a post-secondary institution in London, England. Over three years, she took courses by correspondence and traveled to Thailand, Hong Kong and Australia to complete the residency portion of the program. Having succeeded in her studies last year, she was granted a master�s degree in Chiropractic Paediatrics.
Hundreds of DCs have taken the ICPA�s programs. The ICPA Diplomate Program involves a total of 400 hours of learning and achieved through the successful completion of two levels of study.
The first part � a 200-hour certification program � involves 14 classroom modules, participation in two ICPA Practice Based Research Network projects, and successful completion of the comprehensive certification� final exam.
The second part is a 200-hour advanced competency program. It requires 200 hours of work with more emphasis on research, including either a published research case study or a publishable thesis, as well as clinic work. Enrollment in the first level (200-hour certification program) is a prerequisite to enroll in part two.
Chiropractic care for kids may not be a recognized specialty in Canada, but chiropractic associations recognize it as a legitimate area of focus.
In a statement, the Alberta College and Association of Chiropractors (ACAC) has acknowledged, �chiropractic treatment is as beneficial to children as it is to adults and that the efficacy and benefits of the delivery of chiropractic care to individuals 18 years of age and under are well supported by a body of ongoing research and documented case histories.�
Chiropractic & Teens with Back Pain
Myth #5 Chiropractors don�t collaborate with pediatricians and medical doctors.
Hornick says this simply isn�t the case.
�I often refer pediatric patients to their medical doctors and to medical specialists, and we communicate clearly in the best interests of the child. I see our roles as complementary.�
Forrester also says she has good ties with medical doctors. �The majority of them are very much in favor of working together. Every once in a while you run into someone who thinks we�re all a bunch of quacks and they�re not up to date with the sorts of things we do. But by far the relationship with pediatricians is healthy and puts the patients� best interests first.�
Reality recap
Chiropractic care for kids is not new. Children benefit from chiropractic care. Techniques for children are safe and nowhere near as forceful as they may be for adults. Many DCs are qualified experts, and many child-focused chiropractors establish strong connections with medical doctors. The truth is, DCs can and do share the benefits of their profession with patients across the entire age spectrum.
Mastering pediatrics
Late last year, Dr. Stacey Hornick, a Saskatoon, Sask.-based DC focused on chiropractic care for children became one of the first Canadians to attain a Master�s of Science in Chiropractic Paediatrics.She studied at McTimoney College of Chiropractic, operated by BPP University, a post-secondary institution in London, England. The McTimoney program is the only pediatric chiropractic program that meets the academic requirements for entry into doctoral studies (PhD) in the specific content area of chiropractic pediatrics, an opportunity never before afforded the chiropractic profession, she says.
�For me, it was important to seek out a highly respected qualification in pediatric care,� Hornick says. �There were no university-accredited courses in pediatrics in North America that I was aware of at the time. I liked the idea of studying abroad and at the same time becoming an expert in pediatric-specific assessment, and adjusting techniques that were gentle yet neurologically precise.�
It takes stamina and smarts to get into and complete this tough three-year course. Read on for the requirements. Do you have what it takes?
To enter the program, a candidate must have: a professional qualification in chiropractic and registration with a relevant chiropractic governing body
In each of the first two years of the program, the student must complete:
Work at two residential schools � Hornick explains that usually, students complete their residencies at U.K. chiropractic facilities, but McTimoney also gives students the chance to practice outside of the U.K. For her part, Hornick completed her first-year residency in Thailand, which was memorable. �We stayed at the Children of the Golden Triangle Training Center. It�s a safe haven when kids can go to school and avoid the whole child-trafficking danger, which is a heart-wrenching reality in that part of the world. Many of the children at the facility were orphans � 450 of them. We got to stay with them, and between five chiropractors, we adjusted all of them in three days.�
Online course work � Subjects range from the fundamentals of chiropractic pediatrics to specific requisite topics. Hornick says first-year courses include substrates of chiropractic pediatrics, physical assessment in chiropractic skills and pediatric neurology. �The second year is more application of knowledge.� Courses include normal and variant radiology anatomy in pediatrics, clinical research methodology, and four clinical pediatrics programs.
Structured clinical education, directed and self-directed
Objective structured clinical exam
In the third year of the program, students must complete a research project, including project design, implementation and report at a publishable standard. Hornick�s dissertation: The Effect of Chiropractic on Cortisol Levels in Infants with Colic. The investigation aimed to help doctors understand why chiropractic adjustment has a positive influence on colicky infants. Hornick found that infants with colic who receive chiropractic care demonstrate salivary cortisol release patterns similar to those seen in infants with no colic.
Public�Perceptions about chiropractic care for children are far from the truth. Let’s�explore these misconceptions and speak to experts in order to get the real facts about chiropractic care for children.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine





 Most people don�t go to a
Most people don�t go to a 



 A total of 30 female university students with an FLLI of more than 10?mm between the left and right legs were selected and randomly assigned to one of two groups: the pelvic adjustment group (adjustment group, n = 15) and control group (stretching group, n = 15). The exclusion criteria were as follows: anatomical LLI; degenerative osteoarthritis; muscle, bone, or nervous system problems; ankle joint, knee joint, hip joint, or lumbar pain; limited range of motion due to burn or postsurgical scarring; and regular leg exercise. This study was approved by Korea Nazarene University�s Institutional Review Board, and the safety of all subjects was protected during all parts of the experiment. All subjects understood the purpose of this study and provided written informed consent prior to participation in accordance with the ethical standards of the Declaration of Helsinki.
A total of 30 female university students with an FLLI of more than 10?mm between the left and right legs were selected and randomly assigned to one of two groups: the pelvic adjustment group (adjustment group, n = 15) and control group (stretching group, n = 15). The exclusion criteria were as follows: anatomical LLI; degenerative osteoarthritis; muscle, bone, or nervous system problems; ankle joint, knee joint, hip joint, or lumbar pain; limited range of motion due to burn or postsurgical scarring; and regular leg exercise. This study was approved by Korea Nazarene University�s Institutional Review Board, and the safety of all subjects was protected during all parts of the experiment. All subjects understood the purpose of this study and provided written informed consent prior to participation in accordance with the ethical standards of the Declaration of Helsinki.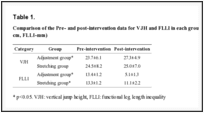




 �We may see a one-week-old child who is already showing signs of favoring, turning her head to one side versus the other,� says Dr. Judy Forrester, owner of Synergea Family Health Centre, a multidisciplinary clinic in Calgary, Alta. �That may seem minimal� but if we can determine any imbalances or asymmetry with the muscular function or the joint alignment, and we address it early, it�s better. Once those postural patterns and habits develop as they grow, they can be much more difficult to change.�
�We may see a one-week-old child who is already showing signs of favoring, turning her head to one side versus the other,� says Dr. Judy Forrester, owner of Synergea Family Health Centre, a multidisciplinary clinic in Calgary, Alta. �That may seem minimal� but if we can determine any imbalances or asymmetry with the muscular function or the joint alignment, and we address it early, it�s better. Once those postural patterns and habits develop as they grow, they can be much more difficult to change.�