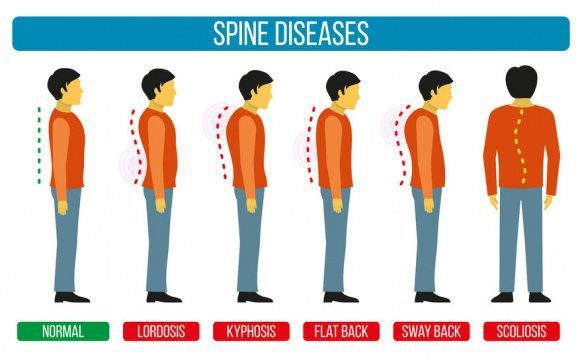
Sometimes there are abnormalities of the spine and it causes a misalignment of the natural curvatures or some curvatures may be exaggerated. These unnatural curvatures of the spine are characterized by three health conditions called lordosis, kyphosis, and scoliosis.
It is not intended to be naturally bent, twisted, or curved. The natural state of a healthy spine is somewhat straight with slight curves running front to back so that a side view would reveal them.
Viewing the spine from the back, you should see something completely different � a spine that runs straight down, top to bottom with no side to side curves. This doesn�t always happen though.
The spine is comprised of vertebrae, small bones that are stacked on top of each other with impact cushioning discs between each one. These bones act as joints, allowing the spine to bend and twist in a variety of ways.
They gently curve, sloping slightly inward at the small of the back, and again slightly at the neck. The pull of gravity, combined with body movement, can put a great deal of stress on the spine and these slight curves help absorb some of the impact.
Different conditions for different types of spinal curvatures
Each of these three spinal curvature disorders affects a certain area of the spine in a very specific way.
Hyper or Hypo Lordosis � This spinal curvature disorder affects the lower back, causing the spine to curve inwards or outwards significantly.
Hyper or Hypo Kyphosis � This spinal curvature disorder affects the upper back, causing the spine to bow, resulting in that area rounding or flattening abnormally.
Scoliosis � This spinal curvature disorder can affect the entire spine, causing it to curve sideways, forming a C or S shape.
What are the symptoms?
Each type of curvature exhibits its own set of symptoms. While some symptoms may overlap, many are unique to the specific curvature disorder.
Lordosis
A �swayback� appearance where the buttocks stick out or are more pronounced.
Discomfort in the back, typically in the lumbar region
When lying on a hard surface on the back, the lower back area does not touch the surface, even when attempting to tuck the pelvis and straighten the lower back.
Difficulty with certain movements
Back pain
Kyphosis
A curve or hump to the upper back
Upper back pain and fatigue after sitting or standing for long periods (Scheuermann�s kyphosis)
Leg or back fatigue
The head bends far forward instead of being more upright
Scoliosis
Hips or waist are uneven
One shoulder blade is higher than the other
The person leans to one side
What are the causes?
Many different health issues can cause the spine to become misaligned or to form a spinal curvature. Each of the spinal conditions mentioned is affected by different conditions and situations.
Lordosis
Osteoporosis
Achondroplasia
Discitis
Obesity
Spondylolisthesis
Kyphosis
Kyphosis
Arthritis
Tumors on or in the spine
Congenital kyphosis (abnormal development of the vertebrae while the person is in utero)
Spina bifida
Scheuermann’s disease
Spine infections
Osteoporosis
Habitual slouching or poor posture
Scoliosis is still a bit of a mystery to doctors. They are not certain what exactly causes the most common form of scoliosis that is typically seen in children and adolescents. Some of the causes that they have pinpointed include:
There are screenings available for both children and adults to identify any spinal curvatures in their early stages through your chiropractor. Early detection of these disorders is crucial in identifying them before they become too serious.
Personalized Spine & *SCIATICA TREATMENT* | El Paso, TX (2019)
Imaging diagnostics of the spine consist from radiographies to computed tomography scanning, or CT scans, in which CT is utilized in conjunction with myelography and most recently with magnetic resonance imaging, or MRI. These imaging diagnostics are being used to determine the presence of abnormalities of the spine, scoliosis, spondylolysis and spondylolisthesis. The following article describes various imaging modalities and their application in the evaluation of common spinal disorders described.
Achondroplasia
Achondroplasia is the most common cause of rhizomelic (root/proximal) short-limb dwarfism. Patients are of normal intelligence.�
It shows multiple distinct radiographic abnormalities affecting long bones, pelvis, skull, and hands.
Vertebral column changes may present with significant clinical and neurological abnormalities.�
Achondroplasia is an autosomal dominant disorder with about 80% of cases from a random new mutation. Advanced paternal age is often linked. Achondroplasia results from a mutation in the fibroblast growth factor gene (FGFR3) which causes abnormal cartilage formation.
All bones formed by endochondral ossification are affected.
Bones that form by intra-membranous ossification are not normal.
Thus, skull vault, iliac wings develop normally vs. the base of the skull, some facial bones, vertebral column, and most tubular bones are abnormal.
�
Dx: is usually made at birth with many features becoming apparent during the first few years of life.
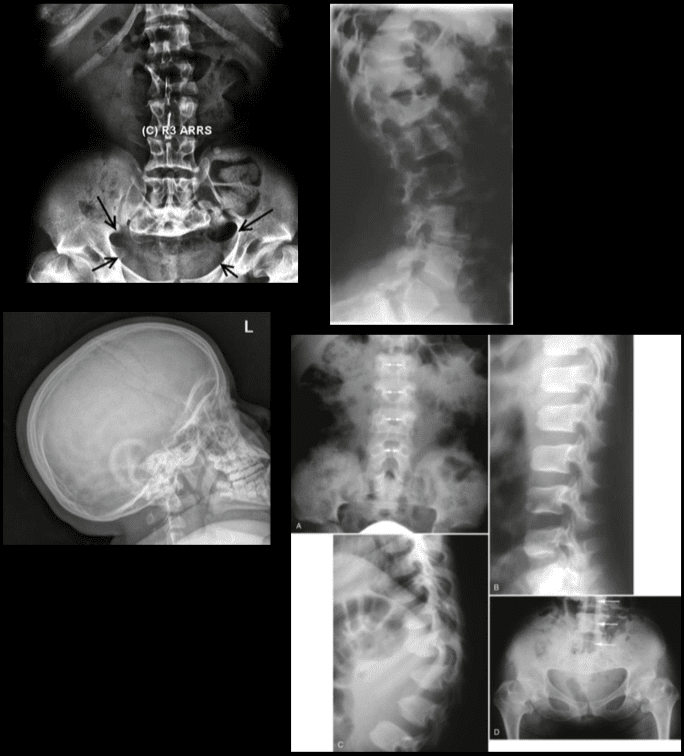
Radiography plays an important part of clinical diagnosis.
Typical features include: shortening and widening of tubular bones, metaphyseal flaring, Trident hand with short, broad metacarpals and proximal and middle phalanges. Longer Fibular, Tibial bowing, markedly short humeri often with dislocated Radial head and elbow flexion deformity.
Spine: characteristic narrowing of L1-L5 interpedicular distance on AP views. Lateral view shows shortening of pedicles and vertebral bodies, �bullet shaped vertebrae� can be a characteristic feature. Early degenerative changes and canal narrowing occur. The horizontal sacral inclination is an important feature.
Pelvis is broad and short with characteristic �champagne glass� pelvis appearance.
Femoral heads are hypoplastic, but hip arthrosis is normally not observed even in older patients likely due to reduced leverage and lightweight (50kg) of patients.
Management of Achondroplasia
Recombinant human growth hormone (GH)�is currently being used to augment the height of patients with achondroplasia.
Most complications of Achondroplasia are related to the spine: vertebral canal stenosis, thoracolumbar kyphosis, narrowed foramen magnum and others.
Laminectomy extending to pedicles/lateral recess with foraminotomies and discectomies can be performed.
Cervical manipulations are contraindicated.
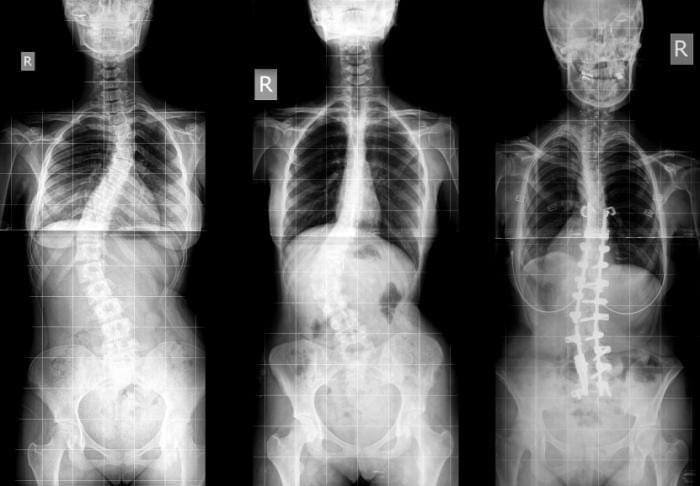
Imaging diagnostics play a fundamental role in the diagnosis the of scoliosis, an abnormality of the spine which is believed to occur due to an underlying health issue, although most cases of scoliosis are idiopathic. More over, radiographies, CT scans, and MRI, among others, can help monitor the changes of the deformity of the spine associated with this spinal manifestation. Chiropractors can provide imaging diagnostics to patients with scoliosis before proceeding with treatment.�
Dr. Alex Jimenez D.C., C.C.S.T.
�
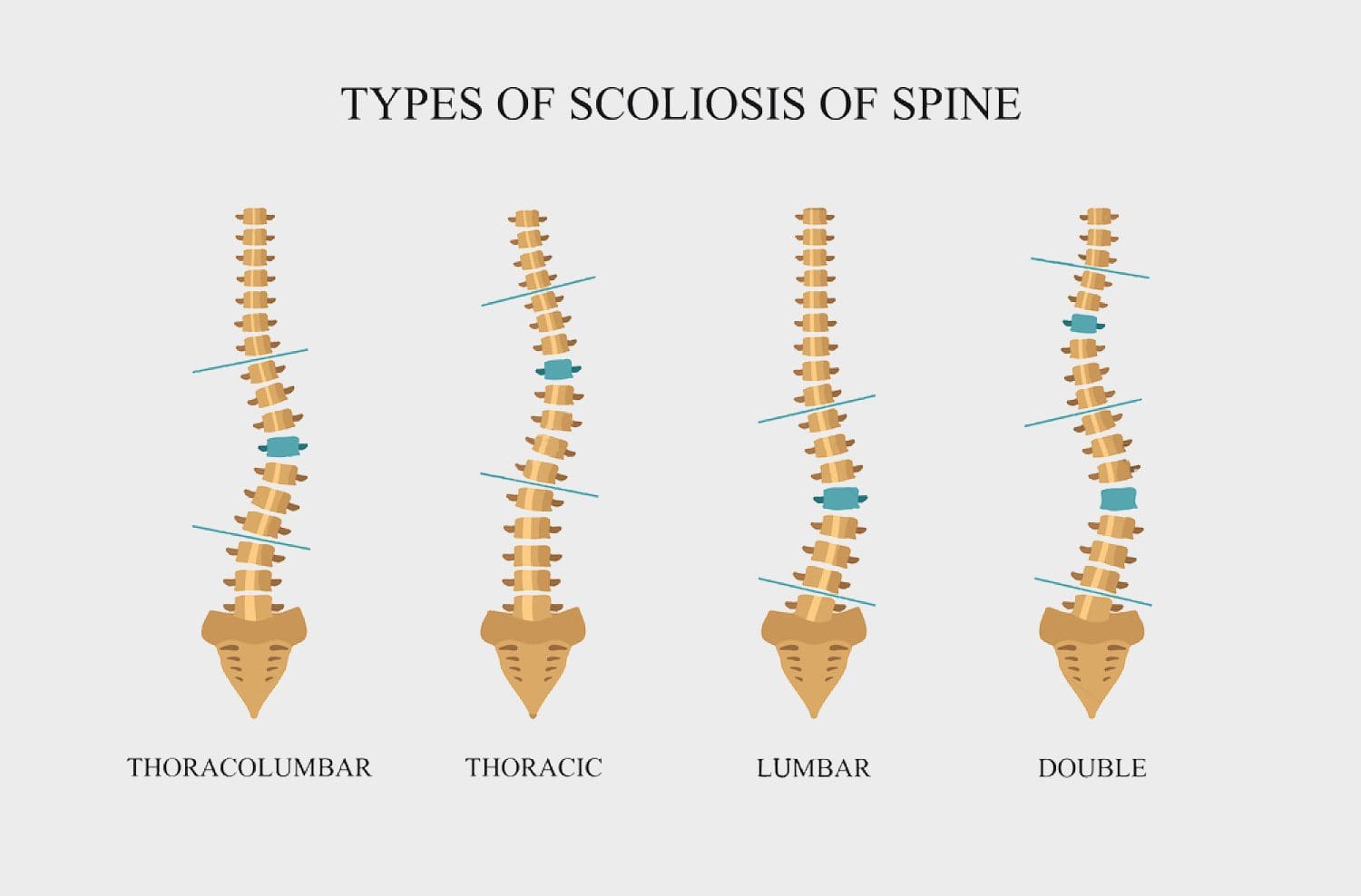
Scoliosis
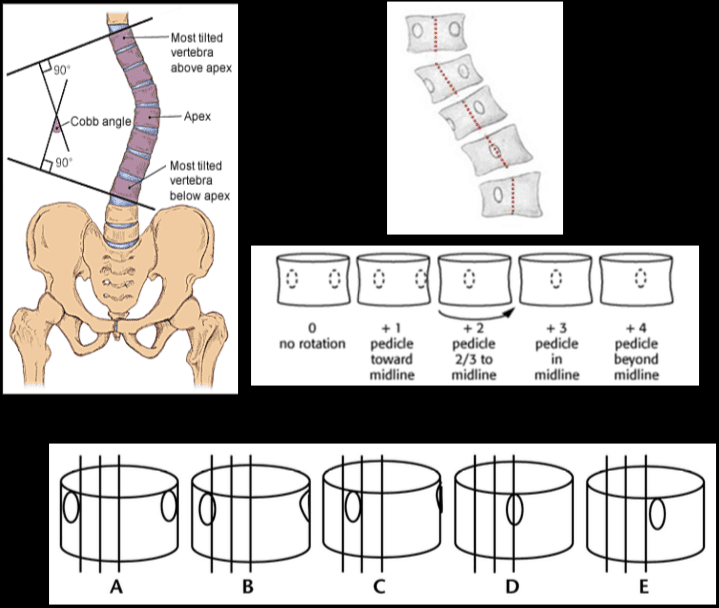
Scoliosis is defined as the abnormal lateral curvature of the spine >10-degree when examined by Cobb�s method of mensuration.
Scoliosis can be described as postural and structural.
Postural scoliosis is not fixed and can be improved by lateral flexion to the side of the convexity.
Structural scoliosis has multiple causes ranging from: ? Idiopathic (>80%) ? Congenital (wedge or hemivertebra, blocked vertebra, Marfan syndrome, skeletal dysplasias) ? Neuropathic (neurofibromatosis, neurological conditions like tethered cord, spinal dysraphism, etc.) ? Scoliosis d/t Spinal neoplasms ? Post-traumatic etc.
Idiopathic scoliosis is the most common type (>80%).
Idiopathic scoliosis can be of 3-types ( infantile, juvenile, adolescent).
Idiopathic adolescent scoliosis if patients >10y.o.
Infantile scoliosis if <3 y.o. M>F.
Juvenile scoliosis if >3 but <10-y.o.
Idiopathic Adolescent scoliosis is the most common with F:M 7:1 (adolescent girls are at particular risk).
Etiology: unknown thought to be the result of some disturbance of proprioceptive control of the spine and spinal musculature, other hypotheses exist.
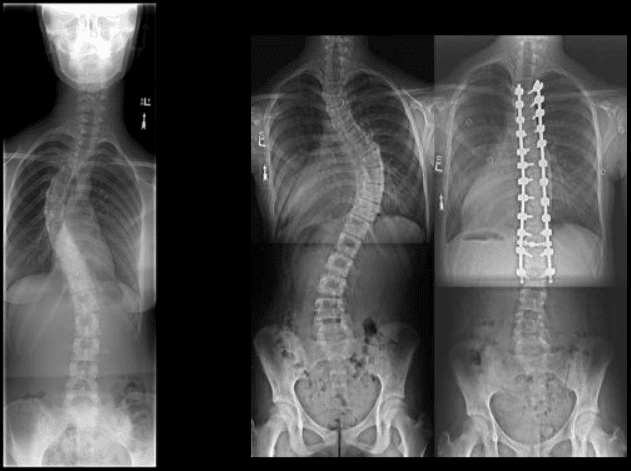
Most seen in the thoracic region and most commonly convex to the right.
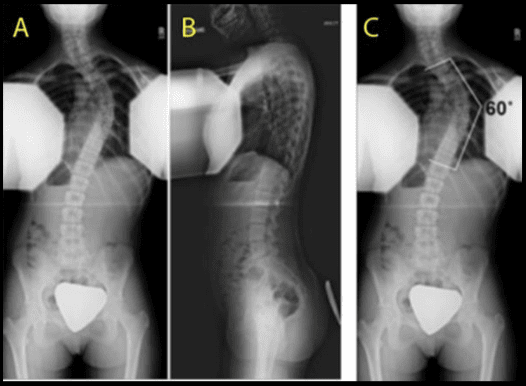
Dx: full spine radiography with gonadal and breast shielding (preferably PA views to protect breast tissue).
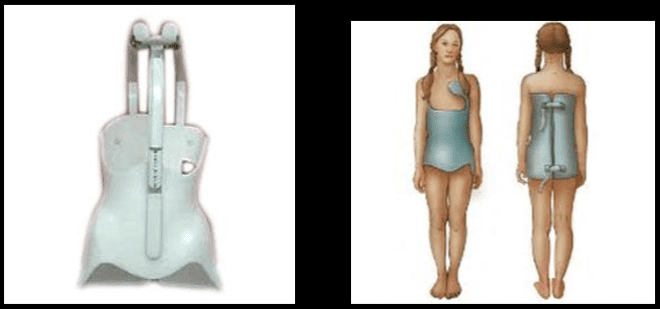
� Curves that are 50-degrees or greater and rapidly progressing will require operative intervention to prevent severe deformity of the thorax & ribs leading to cardiopulmonary abnormalities. � �? If curvature is < 20-degree, no treatment is required (observation). � �? For curves that are >20-40-degrees bracing may be used (orthosis).
Milwaukee (metal) brace (left).
Boston brace polypropylene lined with polyethylene (right) often preferred because it can be worn under clothing.
Bracing wearing is required for 24-hours for the duration of the treatment.
Note Cobb�s method of mensuration to record spinal curvature. It has some limitations: 2D imaging, not able to estimate rotation, etc.
Cobb�s method is still a standard evaluation performed in Scoliosis studies.
Nash-Moe method: determines pedicle rotation in scoliosis.
Risser index is used to estimate spinal skeletal maturity.
Iliac growth apophysis appears at ASIS (F- 14, M-16) and progresses medially and expected to be closed in 2-3-years (Risser 5).
Scoliosis progression ends at Risser 4 in females & Risser 5 in males.
During radiographic evaluation of scoliosis, it is crucial to report if Risser growth apophysis remains open or closed.
Spondylolysis and spondylolisthesis are health issues which can result in back pain. Spondylolysis is believed to be caused by repeated microtrauma leading to stress fractures in the pars interarticularis. Patients with bilateral pars defects can develop spondylolisthesis, where the degree of slippage of the adjacent vertebrae can progress gradually over time. Patients with suspected spondylolysis and spondylolisthesis may initially be evaluated with pain radiography. Chiropractic care can also help provide imaging diagnostics for these health issues.
Dr. Alex Jimenez D.C., C.C.S.T.
�
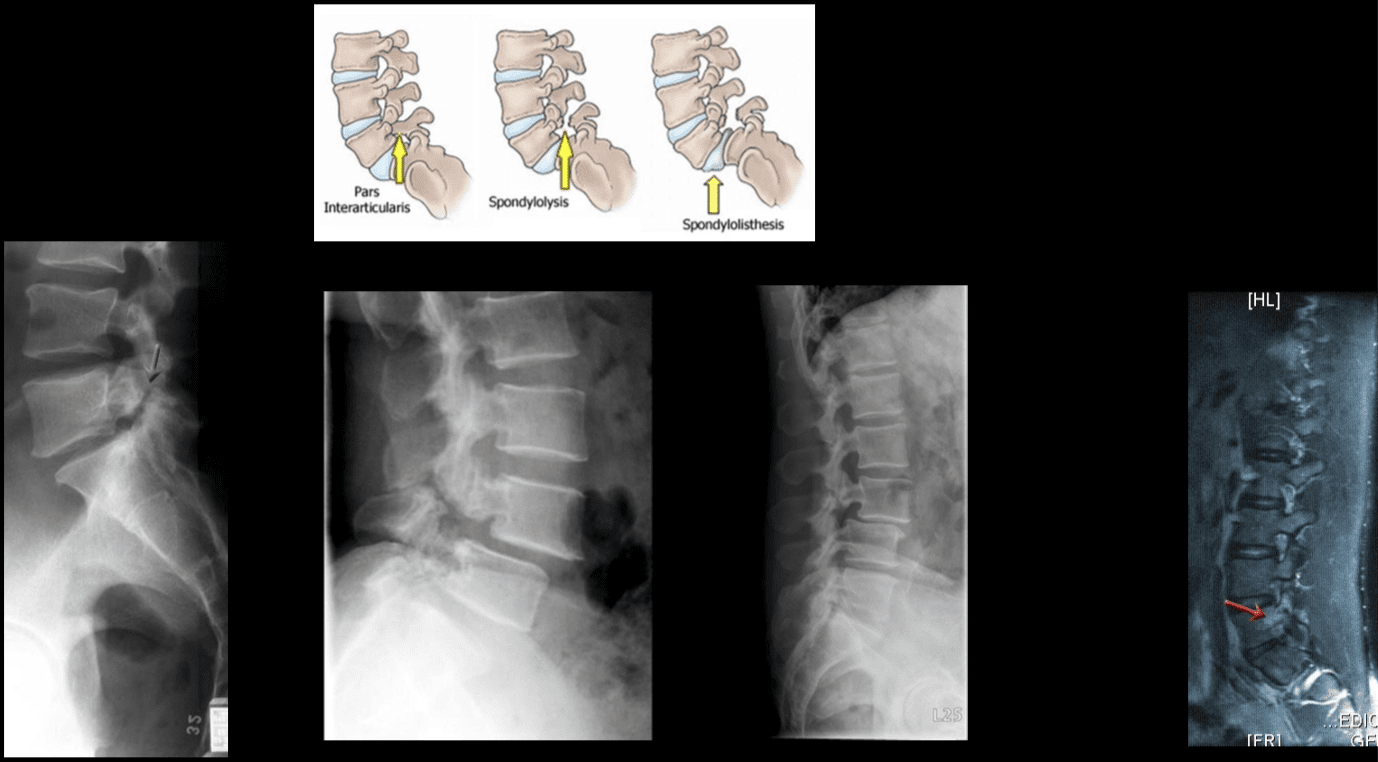
Spondylolysis & Spondylolisthesis
Spondylolysis defect in pars interarticularis or osseous bridge between superior and inferior articular processes.
Pathology stress fracture of the pars, believed to be after repeated microtrauma on extensions Men > Women, affects 5% of the general population especially in athletic adolescents.
Clinically postulated that adolescent back pain cases may be related to this process.
Typically spondylolysis remains asymptomatic.
Spondylolysis can be present with or w/o spondylolisthesis.
Spondylolysis is found in 90% at L5 with the remaining 10% in L4.
Can be uni or bilateral.
In 65%�of�cases, spondylolysis is associated with spondylolisthesis.
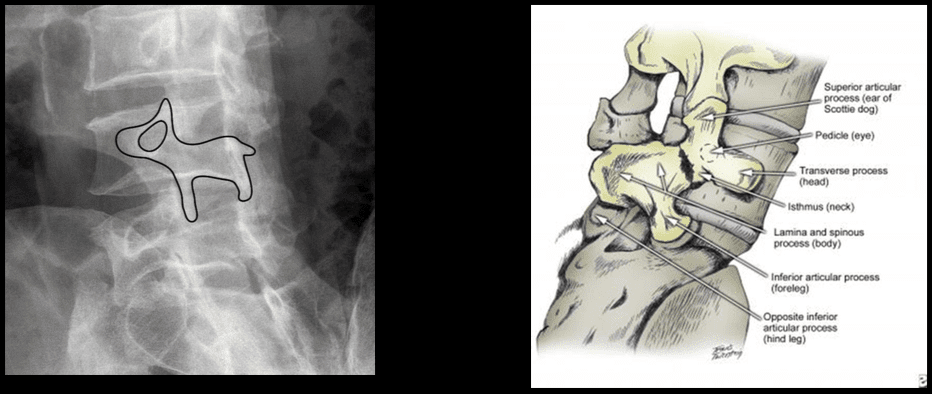
Radiographic Features: break in the Scotty dog collar around the neck on oblique lumbar views.
Radiography has low sensitivity compared to SPECT. SPECT is associated with ionizing radiation, and MRI is currently a preferred method of imaging diagnosis.
MRI can help to show reactive marrow edema next to pars defect or w/o defect so-called pending or potential to develop spondylolysis.
Types of Spondylolisthesis
Type 1 – Dysplastic, rare and found in congenital dysplastic malformation of the sacrum allowing anterior displacement of L5 on S1. Often no pars defect.
Type 2 – Isthmic, most common, often the result of a stress fracture.
Type 3 – Degenerative from the remodeling of articular processes.
Type 4 – Traumatic in an acute posterior arch fracture.
Type 5 – Pathologic due to bone disease locally or generalized.
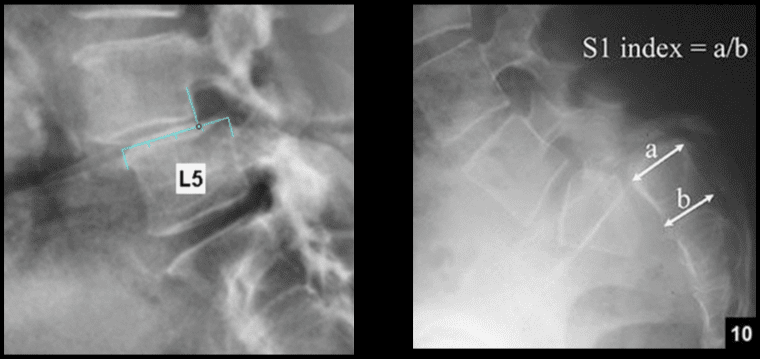
Grading of spondylolisthesis is based on the Myereding Classification. This classification refers to the overhanging part of the superior body in relation to anterior-posterior part of the inferior body.
Grade 1 – 0-25% anterior slip
Grade 2 – 26-50%
Grade 3 – 51%-75%
Grade 4 – 76-100%
Grade 5 – >100% spondyloptosis
Note degenerative spondylolisthesis at L4 and retrolisthesis at L2, L3.
This abnormality develops due to degeneration of facets and disc with decreased local stability.
Rarely progresses beyond Grade 2.
Must be recognized in the imaging report.
Contributes to vertebral canal stenosis.
Canal stenosis is better delineated by cross-sectional imaging.
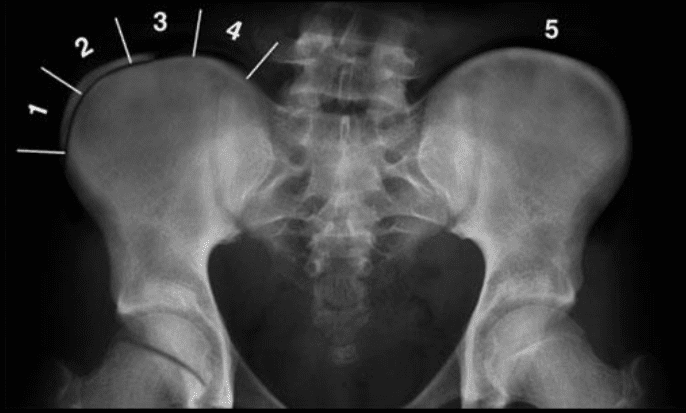
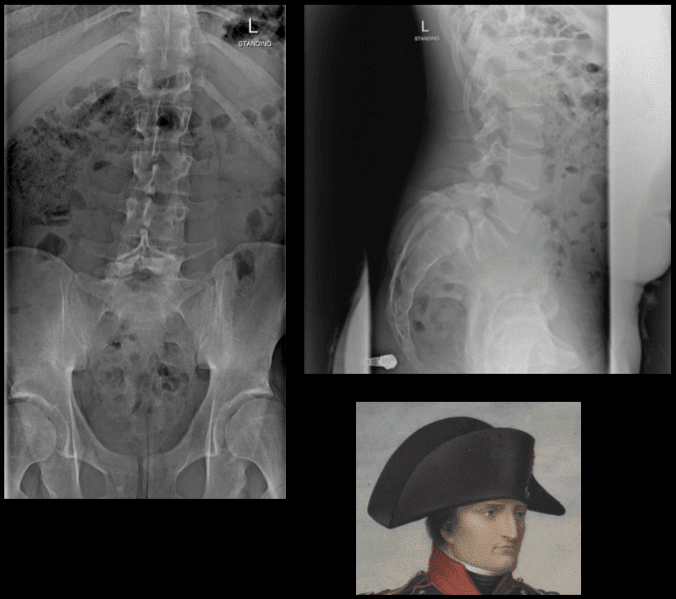
The inverted Napoleon hat sign -�seen on the frontal lumbar/pelvic radiographs at L5-S1.
Represents bilateral spondylolysis with marked anterolisthesis of L5 on S1 often with spondyloptosis and marked exaggeration of the normal lordosis.
Spondylolysis resulting in this degree of spondylolisthesis is more often congenital and/or traumatic in origin and less often degenerative.
The “brim” of the hat is formed by the downward rotation of the transverse processes, and the “dome” of the hat is formed by the body of L5.
In conclusion,�imaging diagnostics for the spine are recommended for patients with specific abnormalities of the spine, however, their increased use can help determine�their best treatment option. Understanding the abnormalities of the spine described above can help healthcare professionals and patients create a treatment program to improve their symptoms. The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Acute Back Pain
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
Why does localized damage or injury caused by trauma lead to chronic, intractable pain in certain patients? What’s in charge of the translation of local injury with acute pain into a chronic pain condition? Why does some pain respond to anti-inflammatory drugs and/or medications, whereas other forms of pain require opiates?
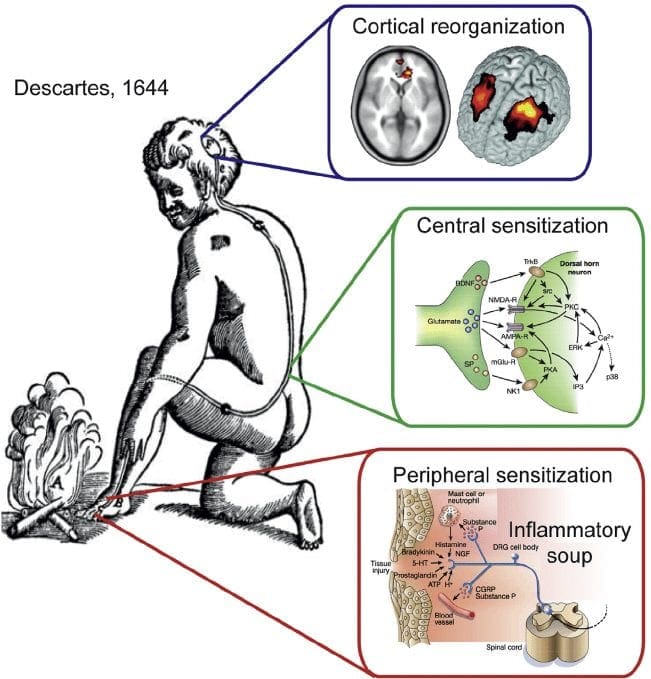
Pain is an intricate process involving both the peripheral nervous system (PNS) and the central nervous system (CNS). Tissue injury triggers the PNS, which transmits signals via the spinal cord into the brain, in which pain perception occurs. However, what causes the intense experience of pain to develop into an unremitting phenomenon? Can anything be done to prevent it? Evidence indicates that chronic pain results from a combination of mechanisms, such as neurological “memories” of preceding pain.
Nociception: The Simplest Pathway
Acute or nociceptive pain is characterized as the regular experience of discomfort which occurs in response to very basic damage or injury. It is protective, warning us to move away from the origin of the insult and take care of the trauma. The mechanisms that create nociceptive pain include transduction, which extends the external traumatic stimulation into electrical activity in specialized nociceptive primary afferent nerves. The afferent nerves then conduct the sensory information from the PNS to the CNS.
In the CNS, the pain data is transmitted by the primary sensory neurons into central projection cells. After the information is transferred to all those areas of the brain which are responsible for our perception, the actual sensory experience happens. Nociceptive pain is a relatively simple reaction to a particularly simple, acute stimulus. But the mechanics in charge of nociceptive pain cannot identify phenomena, such as pain that persists despite removal or healing of the stimulation, such as in the instance of phantom limb pain.
Pain and the Inflammatory Response
In circumstances of more severe injury, such as surgical wounds, tissue damage may stimulate an inflammatory reaction. However, other conditions, especially arthritis, can also be characterized by continuing cases of inflammation associated with intense pain symptoms. The mechanisms for this type of pain related to tissue damage and an inflammatory response are different from early-warning nociceptive pain.
Observing the incision or site of other damage or injury, a cascade of hyperexcitable events occur in the nervous system. This bodily “wind-up” phenomenon begins at the skin, where it is potentiated along the peripheral nerves, and culminates at a hypersensitivity response along the spinal cord (dorsal horn) and the brain. Inflammatory cells then surround the regions of tissue damage and also produce cytokines and chemokines, substances which are intended to mediate the process of healing and tissue regeneration. But, these agents may also be considered irritants and adjust the properties of the primary sensory neurons surrounding the area of trauma.
Thus, the major factors which trigger inflammatory pain include damage to the high-threshold nociceptors, known as peripheral sensitization, changes and alterations of the neurons in the nervous system, and the amplification of the excitability of neurons within the CNS. This represents central sensitization and is accountable for hypersensitivity, where areas adjacent to those of the true injury will experience pain as if these were injured. These tissues can also react to stimulation which normally doesn’t create pain, such as a touch, wearing clothing, light pressure, or even brushing your own hair, as if they were truly painful, referred to as allodynia.
Neuropathic pain results from damage or injury to the nervous system, such as carpal tunnel syndrome, postherpetic neuralgia and diabetic neuropathy. Although some of the mechanisms which seem to cause neuropathic pain overlap with those responsible for inflammatory pain, many of them are different, and thus will need a different approach towards their management.
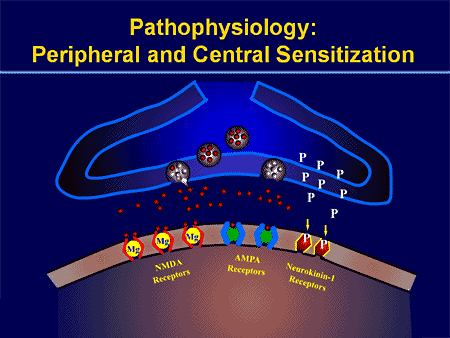
The process of peripheral and central sensitization is maintained, at least theoretically and experimentally, during the excitatory neurotransmitter, glutamate, which is believed to be released when the N-methyl-D-aspartate (NMDA) receptor is activated.
The nervous system is made up of either inhibitory or excitatory neurotransmitters. Most of what permits our nervous system to respond appropriately to damage or injury is the fine-tuning or inhibition of a variety of processes. The overexcitation of the nervous system is seen to be an issue in a number of different disorders. For instance, overactivation of an NMDA receptor can also be related to affective disorders, sympathetic abnormalities, and even opiate tolerance.
Even ordinary nociceptive pain, to some degree, activates the NMDA receptor and is believed to lead to glutamate release. Nonetheless, in neuropathic pain, oversensitivity to the NMDA receptor is key.
With other types of chronic pain, such as fibromyalgia and tension-type headaches, some of the mechanisms active in inflammatory and neuropathic pain may also create similar abnormalities in the pain system, including central sensitization, higher excitability of the somatosensory pathways, and reductions in central nervous system inhibitory mechanisms.
Peripheral Sensitization
Cyclo-oxygenase (COX) also plays an essential function in both peripheral and central sensitizations. COX-2 is one of the enzymes which are induced during the inflammatory process; COX-2 converts arachidonic acid into prostaglandins, which increase the sensitivity of peripheral nociceptor terminals. Virtually, peripheral inflammation also causes COX-2 to be produced from the CNS. Signals from peripheral nociceptors are partially responsible for this upregulation, but there also seems to be a humoral component to the transduction of the pain signals across the blood-brain barrier.
For instance, in experimental models, COX-2 is generated from the CNS even if animals receive a sensory nerve block prior to peripheral inflammatory stimulation. The COX-2 that is expressed over the dorsal horn neurons of the spinal cord releases prostaglandins, which act on the central terminals, or the presynaptic terminals of nociceptive sensory fibers, to increase transmitter release. Additionally, they act postsynaptically on the dorsal horn neurons to produce direct depolarization. And finally, they inhibit the activity of glycine receptor, and this is an inhibitory transmitter. Therefore, the prostaglandins create an increase in excitability of central neurons.
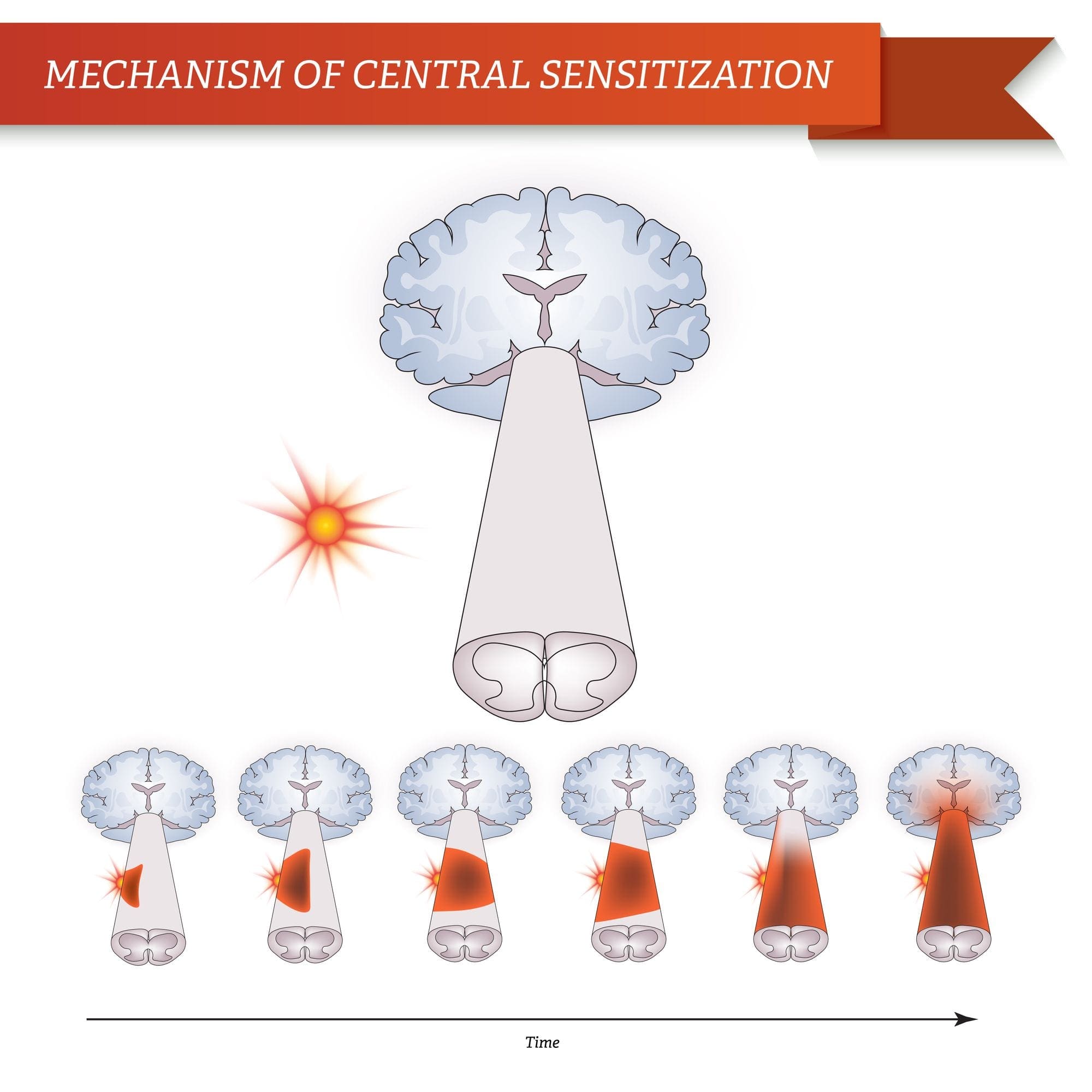
Brain Plasticity and Central Sensitization
Central sensitization describes changes which happen in the brain in reaction to repeated nerve stimulation. After repeated stimuli, amounts of hormones and brain electric signals change as neurons develop a “memory’ for reacting to those signs. Constant stimulation creates a more powerful brain memory, so the brain will respond more rapidly and effectively when undergoing the identical stimulation in the future. The consequent modifications in brain wiring and reaction are referred to as neural plasticity, which describe the capability of the brain to alter itself readily, or central sensitization. Therefore, the brain is activated or sensitized by previous or repeated stimuli to become more excitable.
The fluctuations of central sensitization occur after repeated encounters with pain. Research in animals indicates that repeated exposure to a painful stimulation will change the animal’s pain threshold and lead to a stronger pain response. Researchers think that these modifications can explain the persistent pain that could occur even after successful back surgery. Although a herniated disc may be removed from a pinched nerve, pain may continue as a memory of the nerve compression. Newborns undergoing circumcision without anesthesia will react more profoundly to future painful stimulation, such as routine injections, vaccinations, and other painful processes. These children haven’t only a higher hemodynamic reaction, known as tachycardia and tachypnea, but they will also develop enhanced crying too.
This neurological memory of pain was studied extensively. In a report on his previous research studies, Woolf noted that the improved reflex excitability following peripheral tissue damage or injury doesn’t rely on continuing peripheral input signals; rather, hours after a peripheral trauma, spinal dorsal horn neuron receptive fields continued to enlarge. Researchers also have documented the significance of the spinal NMDA receptor to the induction and maintenance of central sensitization.
Significance for Pain Management
Once central sensitization is established, bigger doses of analgesics are often required to suppress it. Preemptive analgesia, or therapy before pain progresses, may lower the effects of all of these stimulation on the CNS. Woolf demonstrated that the morphine dose required to stop central hyperexcitability, given before short noxious electrical stimulation in rats, was one tenth the dose required to abolish activity after it had grown. This translates to clinical practice.
In a clinical trial of 60 patients undergoing abdominal hysterectomy, individuals who received 10 mg of morphine intravenously at the time of induction of anesthesia required significantly less morphine for postoperative pain control. Furthermore, pain sensitivity around the wound, referred to as secondary hyperalgesia, was also reduced in the morphine pretreated group. Preemptive analgesia was used with comparable success in an assortment of surgical settings, including prespinal operation and postorthopaedic operation.
A single dose of 40 or 60 mg/kg of rectal acetaminophen has a clear morphine-sparing effect in day-case surgery in children, if administered in the induction of anesthesia. Furthermore, children with sufficient analgesia with acetaminophen experienced significantly less postoperative nausea and vomiting.
NMDA receptor antagonists have imparted postoperative analgesia when administered preoperatively. Various reports exist in the literature supporting the use of ketamine and dextromethorphan in the preoperative period. In patients undergoing anterior cruciate ligament reconstruction, 24-hour patient-controlled analgesia opioid consumption was significantly less in the preoperative dextromethorphan category versus the placebo group.
In double-blind, placebo-controlled research studies, gabapentin was indicated as a premedicant analgesic for patients undergoing mastectomy and hysterectomy. Preoperative oral gabapentin reduced pain scores and postoperative analgesic consumption without gap in side effects as compared with placebo.
Preoperative administration of nonsteroidal anti-inflammatory drugs (NSAIDs) has demonstrated a significant decrease in opioid use postoperatively. COX-2s are preferable due to their relative lack of platelet effects and significant gastrointestinal safety profile when compared with conventional NSAIDs. Celecoxib, rofecoxib, valdecoxib, and parecoxib, outside the United States, administered preoperatively reduce postoperative narcotic use by more than 40 percent, with many patients using less than half of the opioids compared with placebo.
Blocking nerve conduction in the preoperative period appears to prevent the development of central sensitization. Phantom limb syndrome (PLS) has been attributed to a spinal wind-up phenomenon.�Patients with amputation
often have burning or tingling pain in the body part removed. One possible cause is that nerve fibers at the stump are stimulated and the brain interprets the signals as originating in the amputated portion. The other is the rearrangement within the cortical areas so that area say for the hand now responds to signals from other parts of the body but still interprets them as coming for the amputated hand.
However, for patients undergoing lower-extremity amputation under epidural anesthesia, not one of the 11 patients who received lumbar epidural blockade with bupivacaine and morphine for 72 hours before operation developed PLS. For people who underwent general anesthesia without prior lumbar epidural blockade, 5 of 14 patients had PLS at 6 weeks and 3 continued to experience PLS at 1 year.
Woolf and Chong have noted that perfect preoperative, intraoperative, and postoperative treatment comprises of “NSAIDs to reduce the activation/centralization of nociceptors, local anesthetics to block sensory inflow, and centrally acting drugs such as opiates.” Decreasing perioperative pain with preemptive techniques enhances satisfaction, hastens discharge, spares opioid use, along with diminished constipation, sedation, nausea, and urinary retention, and may even stop the development of chronic pain. Anesthesiologists and surgeons should consider integrating these techniques in their everyday practices.
When pain occurs as a result of damage or injury in consequence of surgery, the spinal cord can attain a hyperexcitable state wherein excessive pain reactions occur that may persist for days, weeks or even years.
Why does localized injury resulting from trauma result in chronic, intractable pain in some patients? Tissue injury leads to a constellation of changes in spinal excitability, including elevated spontaneous firing, greater response amplitude and length, decreased threshold, enhanced discharge to repeated stimulation, and expanded receptive fields. The persistence of these changes, which are collectively termed central sensitization, appears to be fundamental to the prolonged enhancement of pain sensitivity which defines chronic pain. Numerous drugs and/or medications as well as local anesthetic neural blockade may limit the magnitude of the central nervous system (CNS) windup, as evidenced by diminished pain and diminished opioid consumption in the preemptive analgesic models.
Dr. Alex Jimenez’s Insight
Chiropractic care is an alternate treatment option which utilizes spinal adjustments and manual manipulations to safely and effectively restore as well as maintain the proper alignment of the spine. Research studies have determined that spinal misalignments, or subluxations, can lead to chronic pain. Chiropractic care is commonly utilized for pain management, even if the symptoms are not associated to an injury and/or condition in the musculoskeletal and nervous system. By carefully re-aligning the spine, a chiropractor can help reduce stress and pressure from the structures surrounding the main component of out body’s foundation, ultimately providing pain relief.
Enteric Nervous System Function and Pain
When it comes to the diminished use of drugs and/or medications, including opioids, in order to prevent side-effects like gastrointestinal health issues, the proper function of the enteric nervous system may be at play.
The enteric nervous system (ENS) or intrinsic nervous system is one of the key branches of the autonomic nervous system (ANS) and consists of a mesh-like system of nerves which modulates the role of the gastrointestinal tract. It’s capable of acting independently of the sympathetic and parasympathetic nervous systems, even though it might be affected by them. The ENS can also be called the second brain.�It is derived from neural crest cells.
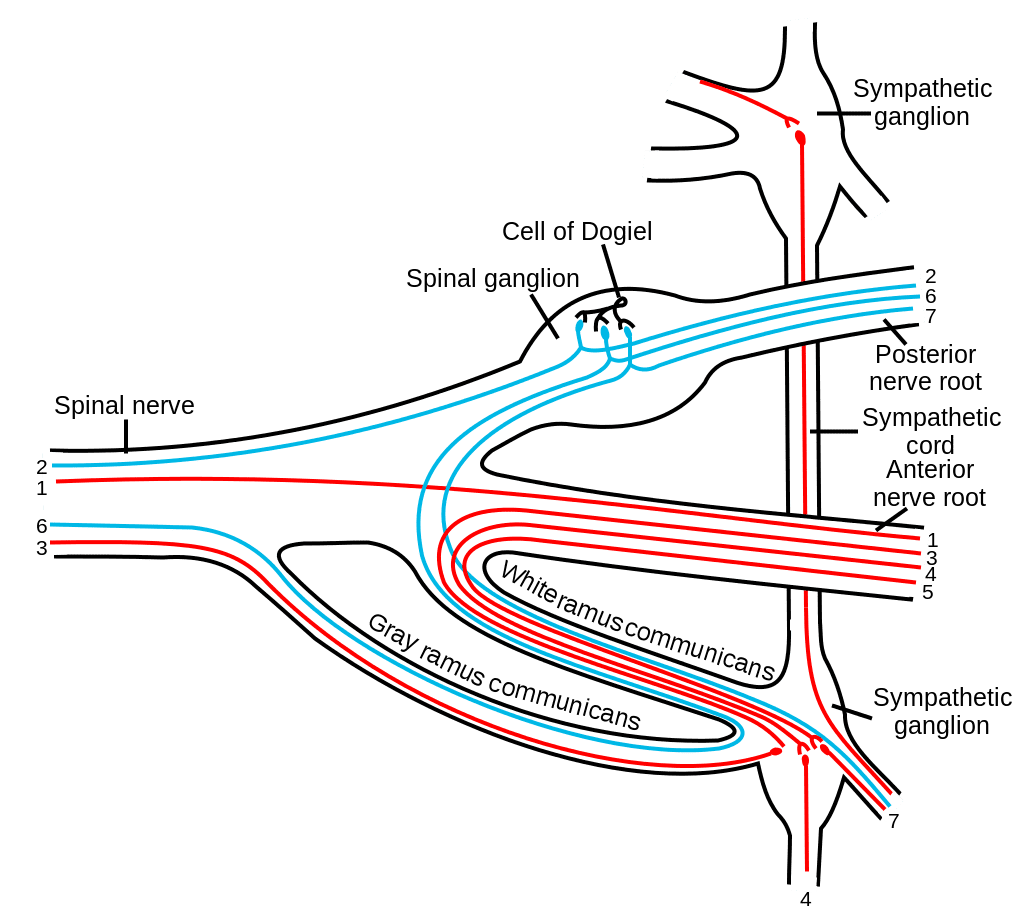
The enteric nervous system in humans is made up of some 500 million neurons, including the numerous types of Dogiel cells, approximately one two-hundredth of the amount of neurons in the brain. The enteric nervous system is inserted into the lining of the gastrointestinal system, beginning at the esophagus and extending down to the anus. Dogiel cells, also known as cells of Dogiel, refers to some kind of multipolar adrenal tissues within the prevertebral sympathetic ganglia.
The ENS is capable of autonomous functions, such as the coordination of reflexes; even though it receives considerable innervation in the autonomic nervous system, it does and can operate independently of the brain and the spinal cord.�The enteric nervous system has been described as the “second brain” for a number of reasons. The enteric nervous system may operate autonomously. It normally communicates with the central nervous system (CNS) via the parasympathetic, or via the vagus nerve, and the sympathetic, that is through the prevertebral ganglia, nervous systems. However, vertebrate studies reveal that when the vagus nerve is severed, the enteric nervous system continues to function.
In vertebrates, the enteric nervous system includes efferent neurons, afferent neurons, and interneurons, all of which make the enteric nervous system capable of carrying reflexes and acting as an integrating center in the absence of CNS input. The sensory neurons report on mechanical and chemical conditions. The enteric nervous system has the ability to change its response based on such factors as nutrient and bulk composition. In addition, ENS contains support cells that are much like astroglia of the brain and a diffusion barrier around the capillaries surrounding ganglia that’s like the blood-brain barrier of blood vessels.
The enteric nervous system (ENS) plays a pivotal role in inflammatory and nociceptive processes. Drugs and/or medications that interact with the ENS have recently raised considerable interest because of their capacity to regulate numerous aspects of the gut physiology and pathophysiology. In particular, experiments in animals have demonstrated that�proteinase-activated receptors (PARs) may be essential to neurogenic inflammation in the intestine. Moreover, PAR2 agonists seem to induce intestinal hypersensitivity and hyperalgesic states, suggesting a role for this receptor in visceral pain perception.
Furthermore, PARs, together with the proteinases that activate them, represent exciting new targets for therapeutic intervention on the ENS. The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Sciatica
Sciatica is medically referred to as a collection of symptoms, rather than a single injury and/or condition. Symptoms of sciatic nerve pain, or sciatica, can vary in frequency and intensity, however, it is most commonly described as a sudden, sharp (knife-like) or electrical pain that radiates from the low back down the buttocks, hips, thighs and legs into the foot. Other symptoms of sciatica may include, tingling or burning sensations, numbness and weakness along the length of the sciatic nerve. Sciatica most frequently affects individuals between the ages of 30 and 50 years. It may often develop as a result of the degeneration of the spine due to age, however, the compression and irritation of the sciatic nerve caused by a bulging or herniated disc, among other spinal health issues, may also cause sciatic nerve pain.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine