Dr. Alex Jimenez, D.C., presents how various treatments can help with adrenal insufficiency and can help regulate hormone levels in the body in this 2-part series. Since hormones play a vital role in the body by controlling how the body functions, it is important to know what the trigger is that is causing overlapping issues in the body. In Part 1, we looked at how adrenal insufficiencies affect different hormones and their symptoms. We refer patients to certified providers that include hormone treatments that relieve adrenal insufficiencies affecting the body while ensuring optimal health and wellness for the patient through various therapies. We appreciate each patient by referring them to associated medical providers based on their diagnosis when it’s appropriate to understand better what they are feeling. We understand that education is an excellent and inquisitive way to ask our providers various intricated questions at the patient’s request and knowledge. Dr. Jimenez, D.C., utilizes this information as an educational service. Disclaimer
Treatments For Adrenal Insufficiencies
Dr. Alex Jimenez, D.C., presents: When it comes to adrenal insufficiencies, the body has various symptoms that can cause the person to feel low on energy and pain in different areas. Since hormones are produced in the adrenal glands, they help maintain how vital organs and muscles work to keep the body functional. When various factors affect the body, disrupting the adrenal glands, it can cause hormone production to over or underproduce. To that point, it can correlate to numerous symptoms that cause the body to be dysfunctional. Fortunately, there are various treatments that many people can incorporate into their daily lives to promote hormone regulation.
Now everyone has different ways to lower their stress, which is fine as there are various treatments that a person may like to try, and if they are in a treatment plan that their doctor developed for them, they can find ways to get their health and wellness back. Many individuals sometimes participate in meditation and yoga to practice mindfulness. Now meditation and yoga have amazing benefits in lowering oxidative stress and cortisol levels associated with chronic stress. By looking at how adrenal insufficiencies can cause an increase in insulin, cortisol, and DHEA dysfunction in the HPA axis, many doctors would devise a treatment plan for their patients that can help lower the oxidative stress markers and regulate hormonal production. So if one of the treatments is meditation or yoga, many individuals who practice yoga and meditation will begin to notice how they are feeling after taking a few deep breaths and begin to feel mindful of their surroundings. This causes many people to improve their quality of life associated with decreased cortisol levels.
How Mindfulness Can Lower Stress
Dr. Alex Jimenez, D.C., presents: Another available treatment that can help with adrenal insufficiencies is an 8-week mindfulness treatment that can help lower cortisol levels from escalating in the body to cause more issues than a person is dealing with. Depending on what stage the HPA axis dysfunction is affecting the body, taking the time for yourself can benefit you in the long run. An example would be taking a hike on a nature walk path. The change in the environment can help a person relax and be at ease. This allows the body to let go of unnecessary pent-up stress affecting a person’s mood, functionality, and mental health when a change of scenery can help them relax and recharge. To that point, it allows the HPA axis to relax as well.
Another example of how mindfulness can help treat adrenal insufficiencies associated with hormonal dysfunction is by providing neurofeedback to those with chronic PTSD. Individuals with traumatic experiences have PTSD, which can hinder their ability to function in the world. When they go through a PTSD episode, their bodies will begin to lock up and tense, causing their cortisol levels to rise. To that point, this causes an overlap of symptoms associated with muscle and joint pain. Now how does mindfulness plays its part when it comes to treatment? Well, many doctors specializing in treating PTSD will do an EMDR test. EMDR stands for eye, movement, desensitization, and reprogramming. This allows PTSD patients to have their HPA axis rewired and reduce the neuron signals in their brains and help lower any cortisol levels causing adrenal insufficiencies in their bodies. Incorporating EMDR testing into PTSD patients allows them to find the issue causing the trauma through brain spotting, where the brain replays the traumatic memories and helps rewire the brain to release the trauma out of the body and start the healing process.
Vitamins & Supplements
Dr. Alex Jimenez, D.C., presents: Another technique many individuals can begin if they want to regulate their hormones is by taking supplements and neutraceuticals to help replenish hormonal function and the body. Choosing the right vitamins and supplements is not difficult if you don’t want to consume them in pill form. Many vitamins and supplements can be found in nutritious whole foods with specific nutrients that can improve hormone production and make a person feel full. Some of the vitamins and supplements that can help with hormone balance include:
Magnesium
B vitamins
Probiotics
Vitamin C
Alpha-lipoic acid
Omega-3 Fatty Acid
Vitamin D
These vitamins and supplements can help communicate with the other hormones the body produces and help balance hormonal production. Now, these treatments can help many people with hormonal imbalances in their bodies, and there are times when the process can be tough. Just remember that making these small changes can have a huge effect in the long run regarding your health and wellness. By sticking with the treatment plan that your doctor has come up with you, you will feel better over time and take back your health as well.
Dr. Alex Jimenez, D.C., presents how adrenal insufficiencies can affect the hormone levels in the body. Hormones play a vital part in regulating body temperature and help function the vital organs and muscles. This 2-part series will examine how adrenal insufficiencies affect the body and its symptoms. In part 2, we will look at the treatment for adrenal insufficiencies and how many people can incorporate these treatments into their health and wellness. We refer patients to certified providers that include hormone treatments that relieve various issues affecting the body while ensuring optimal health and wellness for the patient. We appreciate each patient by referring them to associated medical providers based on their diagnosis when it’s appropriate to understand better what they are feeling. We understand that education is an excellent and inquisitive way to ask our providers various intricated questions at the patient’s request and knowledge. Dr. Alex Jimenez, D.C., utilizes this information as an educational service. Disclaimer
What Are Adrenal Insufficiencies?
Dr. Alex Jimenez, D.C., presents: Many factors can affect the body, whether eating habits, mental health, or lifestyle habits all play a role in maintaining hormone function in the body. Today, we will apply these common dysfunctional cortisol patterns that patients present when they go in for a daily examination. Most patients often come in and explain to their doctors that they are suffering from adrenal dysfunction because different symptoms are associated with various stages of adrenal dysfunction or HPA dysfunction. Now adrenal dysfunction or hypothalamic pituitary adrenal (HPA) dysfunction is when the adrenal glands are not producing enough hormone to regulate the body. This causes the body to go through different stages of adrenal dysfunction if it is not treated right this way, causing the body to deal with muscle and joint pain that a person hasn’t dealt with throughout their life.
Many doctors and healthcare providers use a systematic approach that can help many people address whether or not they have adrenal dysfunction in their bodies. Today, we will discuss the relationship between female hormones and mood disorders associated with adrenal dysfunction. When it comes to adrenal dysfunction associated with hormones, many people will often get medicated for mental illnesses like bipolar disease or depression when their hormones are imbalanced. When hormonal imbalances begin to affect women in their early fifties due to premenopause, the mental disorder would often worsens and cause many other overlapping issues that can affect their hormones and their bodies.
Adrenal Dysfunction Affect The Body
Dr. Alex Jimenez, D.C., presents: Many women would have healthy diets, take yoga, be involved in spiritual practices, and hang out with their friends; however, when their hormone levels are imbalanced, they are dealing with other issues associated with HPA imbalances or adrenal dysfunction. By looking at the 24-hour corticotropic activity and determining how the circadian rhythm controls it, many doctors can look at the data presented to the patient. The way the data is being presented to the patient on how their hormone levels fluctuate in the body in the morning and how they rise or decrease throughout the entire day until they go to sleep.
With this information, many doctors can diagnose why this individual is having trouble going to sleep, constantly waking up early in the night, or not getting enough rest, making them exhausted throughout the day. So how is adrenal dysfunction associated with 24-hour corticotropic activity? Many factors can cause adrenal dysfunction in the body and affect hormone levels. When the body begins to over or underproduces hormones from the adrenal glands or the thyroids, it can cause cortisol and insulin levels to lose control in the body and cause various issues that result in muscle and joint pain. Sometimes hormonal dysfunction can cause somato-visceral or visceral-somatic pain by affecting the vital organs like the gut and the brain and start to cause issues to the surrounding muscles and joints. When the surrounding muscles and joints are causing pain in the body, they could be causing overlapping issues that can affect a person’s mobility and make them miserable.
How To Diagnose Adrenal Insufficiencies?
Dr. Alex Jimenez, D.C., presents: When doctors diagnose a patient suffering from adrenal dysfunction will begin to look at the patient’s medical history. Many patients will start filling out a long, extensive questionnaire, and doctors will begin to look at the anthropometrics, biomarkers, and clinical indicators found in physical exams. Doctors must obtain the patient’s history to look for the signs and symptoms of HPA dysfunction and adrenal dysfunction to determine the issue affecting the individual. After the examination, doctors would use functional medicine to look at where the dysfunction lies in the body and how the symptoms are connected. The numerous factors causing adrenal dysfunction in the body could be how a person’s eating habits are causing these issues, how much exercise they are incorporating in their daily lives, or how stress impacts them.
Functional medicine provides a holistic approach that considers lifestyle components causing issues in the person’s body. By connecting the dots on what the patient is saying and how these factors are causing adrenal insufficiencies, it is important to get the whole story from the patient to devise a treatment plan catered to the individual. They would appreciate that someone finally understands what they are going through and will begin to restore their health and wellness. By looking for the root causes, triggers, and mediators causing adrenal dysfunction, we can look at the expanded history that the patient is telling us, whether it be their family history, their hobbies, or what they like to do for fun. All these things are important to consider to try and connect the dots of the underlying cause of adrenal insufficiencies in the body affecting a person’s hormone levels.
Adrenal Insufficiencies Affect Cortisol
Dr. Alex Jimenez, D.C., presents: Now, do adrenal insufficiencies correlate with increased DHEA and cortisol hormone levels? Well, DHEA is a hormone that is produced by the adrenal glands naturally. DHEA’s main function is to make other hormones like estrogen and testosterone to regulate the male and female body. Cortisol is a stress hormone that increases the glucose levels in the bloodstream. Cortisol’s main function is to allow the brain to use glucose in the body while repairing the affected muscle tissues. When the body begins to over or underproduces hormones from the adrenal glands, it can raise the cortisol levels to cause resilience to the body, and the HPA axis begins to decrease. When this happens, the body starts to feel sluggish, which can cause you to feel exhausted throughout the entire day, even though you may have gotten a good night’s sleep.
Adrenal Insufficiency Symptoms
Dr. Alex Jimenez, D.C., presents: This is known as adrenal fatigue and can be associated with various symptoms that affect the hormone balance in the body. This can include non-specific symptoms like sleep disturbances, digestive issues, fatigue, and body aches can affect the hormone levels inside the body. This causes many individuals to feel miserable due to feeling low energy. Adrenal fatigue can also be associated with the different stages of HPA axis dysfunction. These can include:
Trauma
Food allergies and sensitivities
Dysbiosis
Changes in the gut microbiota
Toxins
Stress
Insulin resistance
Metabolic syndrome
All these issues can affect a person’s hormone levels and cause elevated cortisol to overlap many factors that cause somato-visceral problems. An example would be someone having gut issues associated with chronic stress who can start to feel pain in their joints from the knees, back, and hips which cause their hormone levels can fluctuate.
Dr. Alex Jimenez, D.C., presents an insightful overview of how hormonal dysfunction can affect the body, increase cortisol levels, and be associated with PTSD in this 3-part series. This presentation provides important information to many individuals dealing with hormonal dysfunction associated with PTSD. The presentation also offers different treatment options to reduce the effects of hormonal dysfunction and PTSD through functional medicine. Part 1 looks at the overview of hormonal dysfunction. Part 2 will look at how various hormones in the body contribute to body functionality and how overproduction or underproduction can cause drastic effects on a person’s health. We refer patients to certified providers that incorporate various hormone treatments to ensure optimal health and wellness for the patient. We appreciate each patient by referring them to associated medical providers based on their diagnosis when it is appropriate to have a better understanding. We understand that education is an excellent and inquisitive way to ask our providers various intricated questions at the patient’s request and knowledge. Dr. Alex Jimenez, D.C., utilizes this information as an educational service. Disclaimer
A Look Into Hormonal Dysfunction
Dr. Alex Jimenez, D.C., presents: Now, looking into the exciting didactic here, we will discuss something rare but important to understand when looking at these steroid pathways. And this is something called congenital adrenal hyperplasia. Now, congenital adrenal hyperplasia can occur in the body through an inherited enzyme defect or 21 hydroxylases that can cause a severe decrease in the adrenal production of glucocorticoids. When the body is suffering from congenital adrenal hyperplasia, it can cause an increase in ACTH to make more cortisol.
So when the ACTH increases to make more cortisol in the body, it could lead to muscle and joint pain if it is not treated immediately. We also often think cortisol is bad, but you must have some congenital adrenal hyperplasia when you have the 21 hydroxide deficiency. To that point, your body is not making enough glucocorticoids, causing you to have a high level of ACTH. When there is hormone dysfunction from various environmental triggers, it can cause the hormones in the body to overproduce unnecessary hormones. For example, if you have too much progesterone, it can’t go down to the pathway to make cortisol due to those missing enzymes. It can be converted into androstenedione, causing people to become virilized.
What Happens When The Body Doesn’t Create Enough Hormones?
Dr. Alex Jimenez, D.C., presents: So when patients become virilized, they’re not making any cortisol; it is important to do hormonal therapy to decrease the ACTH stimulation to get the hormone levels back to normal When this happens, it diminishes the stress inside the body system to make more androgens. In the female body, however, progesterone has no peripheral conversion of steroids to be produced except during pregnancy. Progesterone comes from the ovaries and doesn’t get to be produced in the adrenal glands. Progesterone is excreted mostly in urine as many different breakdown products tend to be higher than normal due to that 21 hydroxide deficiency.
So now, let’s talk about androgens in premenopausal women. So the major androgens come from the ovary, the DHEA, androstenedione, and testosterone. At the same time, the adrenal cortex produces glucocorticoids, mineralocorticoids, and sex steroids to make some testosterone and about half of the DHEA hormone. The body also has peripheral conversion responsible for DHEA and testosterone production to normalizing hormone levels. This is due to all the different tissues that have these enzymes to make these various hormones in different concentrations. Premenopausal women are most likely to lose more estrogen after removing their ovaries. This causes them to lose DHEA, androstenedione, and testosterone production in their bodies.
PTSD & Hormonal Dysfunction
Dr. Alex Jimenez, D.C., presents: Now testosterone is carried by SHBG just like estrogen, and many factors that change SHBG are important to testosterone and estrogen. Interestingly, testosterone can decrease SHBG in small amounts to allow the body to have free testosterone, which causes a physiological effect. When it comes to testing for testosterone levels, many people don’t release that when their testosterone levels are elevated, it could be due to low SHBG. By measuring total testosterone in the body, many doctors can determine if their patients are producing too much androgen, which is causing excessive hair growth in their bodies, or they may have low SHBG levels due to hypothyroidism associated with obesity or elevated insulin.
Now when it comes to PTSD, how does it correlate to hormonal dysfunction and affect the body? PTSD is a common disorder many individuals suffer from when they have been through a traumatic experience. When traumatic forces begin to affect the individual, it can cause the cortisol levels to rise and cause the body to be in a state of tension. PTSD symptoms can vary for many individuals; thankfully, various therapies can help lower the symptoms while bringing the hormone levels back to normal. Many healthcare professionals will develop a treatment plan that can help reduce the symptoms of PTSD and help hormone levels function in the body properly.
Treatments To Regulate Hormone
Dr. Alex Jimenez, D.C., presents: Stress in the body can affect the musculoskeletal system by causing the muscle to lock up, leading to issues in the hips, legs, shoulders, neck, and back. Various treatments like meditation and yoga can help lower the cortisol levels from fluctuating higher, causing the body to deal with muscle tension that could overlap with joint pain. Another way to reduce stress in the body is by working out with an exercise regime. Exercising or participating in an exercise class can help loosen up the stiff muscles in the body, and keeping a workout routine can exert any pent-up energy to relieve stress. However, treatments to balance out hormones associated with PTSD can only go so far for many individuals. Eating nutritional, whole foods with vitamins and minerals can help regulate hormone production and provide energy to the body. Dark leafy greens, fruits, whole grains, and proteins can not only help with regulating hormone production. Eating these nutritional foods can also lower inflammatory cytokines that are causing more harm to vital organs like the gut.
Conclusion
Incorporating a healthy diet, an exercise routine, and getting treatment can help many individuals dealing with hormonal dysfunction associated with PTSD. Each person is different, and the symptoms overlap with hormonal dysfunction associated with PTSD and vary from person to person. When doctors work with associated medical providers, it allows them to develop a treatment plan catered to the individual and enables them to regulate their hormone production. Once the hormone production in their bodies is regulated, the symptoms causing the person pain will get better slowly but surely. This will allow the individual to continue on their wellness journey.
Dr. Alex Jimenez, D.C., presents an overview of hormonal dysfunction can affect the various hormones in the body that can increase cortisol levels in this 3-part series. This presentation provides valuable information to many individuals dealing with hormonal dysfunction and how to know the signs and utilize holistic approaches toward their health wellness. Part 1 will look at the overview of hormonal dysfunction. Part 3 will look at various holistic treatments that are available for hormonal dysfunction. We refer patients to certified providers incorporating various hormone therapies to ensure optimal health. We encourage and appreciate each patient by referring them to associated medical providers based on their diagnosis when it is appropriate. We understand that education is an excellent way when asking our providers intricated questions at the patient’s request and understanding. Dr. Alex Jimenez, D.C., only utilizes this information as an educational service. Disclaimer
An Overview Of Hormonal Expression
Dr. Alex Jimenez, D.C., presents: So the classic teaching about hormones is that they’re produced in an endocrine gland and then transported to the cells where the body will utilize them. But things are a little bit more complex. So every cell contains the genes necessary for hormone expression and functionality in the body.
And we know this because when de-differentiated from the late stage, unfortunately, cancer cells uncover gene expression. Those cells make hormones in inappropriate locations and at inconvenient times. So that means that any cell can make any hormones in the body. Still, the hormonal expression of certain genes indicates the presence of certain enzymes, which determines what hormones will reproduce. So, for example, you need to have the right precursors and enzymes. So in a reproductive female, the granulosa cells, the luteinize, and the corpus luteum are produced in the body. The granulosa cells are follicles, while the corpus odium is after ovulation. And these cells start the formation of the steroid hormones in response to FSH and LH. So FSH and LH come from the pituitary glands and stimulate the granulosa cells to start making estrogen. Steroid production will begin if the messaging from FSH and LH gets to the part of the cell that makes estrogen. This allows the body to regulate hormonal production and keep it functional. When issues disrupt hormonal regulation, the body can over or underproduce hormonal production, leading to metabolic issues associated with muscle and joint pain.
So this is a complex process, and there are many areas where this can go wrong. So you can have the right amounts of the hormone, but you’re not getting hormone production. So the messages must get into the cell first, and FSH and LH are too large to get into the cellular structure. So, they have to activate a membrane-based enzyme called adenylate cyclase to produce cyclic AMP to enter the cellular network and start hormonal formation in the body. This is the P, or the production of hormones. So by thinking about cellular membrane health, if a doctor does an essential fatty acid analysis, the patients may be very low in omega-3s; therefore, their cell membranes are more rigid and affect the body’s hormonal process. When patients are not taking their omega-3s, it could cause the inflammatory cytokines to cause more joint pain issues when various factors affect the body internally. Since inflammation can be good or bad in the body, it can cause hormonal dysfunction when they attack healthy cellular structures. That will affect this hormonal production process.
Hormonal Production Process In The Body
Dr. Alex Jimenez, D.C., presents: Once made, estradiol goes directly into the blood and is not stored, but it’s bound to SHBG and albumin. And SHBG is changed by obesity and insulin associated with hypothyroidism. So when women are obese or hyperinsulinemic will have less SHBG or hypothyroidism to transport the estrogen to the cells. This tells the body that the hormones are no longer FSH or LH and cyclic AMP, but this is estrogen. And so, estradiol is sensitive since estradiol has to go in and have a cytoplasmic receptor. So the estrogen receptor is in the cytoplasm. After it binds to the receptor, it goes into the nucleus, and it’s transcribed and then goes back out and translated to allow the body to make proteins that cause cell proliferation. Estrogen is a proliferative hormone. And once it’s acted on the cell after proliferation, it’s degraded in the cell with heat shock proteins or released back into the circulation in the body’s system.
Let’s talk about some of the basics of biochemistry because the steroidogenic pathway n the body has different ways to reduce carbons in the body. The body’s system could convert it into estrone or estriol, with less estrogen in circulation. And then estradiol, estrone, estriol, everything is eliminated through the detoxification pathways. So in the Living Matrix, healthy detoxification and estrogen metabolism pathways help the body stay functional. When the body goes through detoxification, it helps reduce the issues by figuring out what is causing the problems affecting the body’s system and slowing introducing or taking away the pain that can allow normal hormonal regulation. When the body reduces excessive carbon, it can lower cholesterol from reaching dangerous levels.
Cholesterol & Hormones
Dr. Alex Jimenez, D.C., presents: So it all starts with cholesterol, and the body can’t make enough cholesterol, so we consume food to allow it to enter the body and begin to biotransform into LDL (low-density lipoprotein) to initiate steroid hormone synthesis. So we need LDL in the body to decrease the carbons since it is a union directional. When it comes to hormone deficiency cases, sometimes women can come in with extremely low LDLs because they’re on statins, underweight, or over-athletic; these are connections and pattern recognition. In a female’s body, the ovaries on the left and right side of the female reproduction system produce all three sex steroids: estrogens, progesterones, and androgens, for optimal body function. They are different than the male’s reproduction system, which includes the testicles, due to the other enzymes. They differ from the testes in many ways due to additional hormonal output in the body, which is different than adrenal hormones. For example, if the body can’t make aldosterone or cortisol in the endocrine glands, they will be shunted to make sex hormones. And since each body is diverse, male or female, some hormones can’t make glucocorticoids or mineral corticoids.
So we must think about mitochondrial health for hormone production, which is critical for producing hormones. For expecting mothers, it allows the formation of pregnancy alone in the mitochondria. So mitochondrial health energy is related to hormone health, which causes cholesterol uptake by the mitochondria in the adrenal glands and ovaries that can stimulate ACTH. So the mitochondria can make hormones as we go while enabling the enzymes in the female’s body to induce pregnenolone formation. However, getting the cholesterol to the inner membrane and LDL to the inner membrane to the mitochondria is the rate-limiting step in all steroid hormone synthesis. Now it can develop and go into two different pathways in the body. It can create DHEA, or it can include progesterone when cholesterol is forming pregnenolone and can look diagrammatically in test results.
DHEA & Hormones
Dr. Alex Jimenez, D.C., presents: So if the mitochondria can enable the body’s pregnenolone to form DHEA or progesterone, let’s start with going over things with developing progesterone since it’s hydroxylated. It creates an enzyme called 17 hydroxy progesterone, the immediate precursor of the androgens and estrogens. So the 17 hydroxy progesterone will eventually form androgens or estrogens, and androstenedione can develop testosterone, and both can become estrogens by aromatization. So what does this mean? It means you must be concerned about too many androgens being around because they can become estrogen. The best way to remember this is that androstenedione can become estrone, and testosterone can become estradiol. This can cause progesterone to be the precursor to cortisol in the body and can go in two different directions.
So progesterone is also the precursor to aldosterone, which asks what will happen when the body needs cortisol or aldosterone. The body will then produce less progesterone causing it to be shunned in hormonal production and causing cortisol to overproduce. This is known as cortisol steal, and if it is not treated at the moment, it can cause muscle and joint inflammation in the body, leading to various issues that the person is dealing with.
A decreased formation of androgens and estrogens can inhibit the DHEA pathway. So when the body makes more cortisol, it can cause the hormones to develop an estrogen-dominate shape causing the cortisol hormone to stimulate aromatase. To that point, it can lead to breast cancer, fibroids, and endometriosis in the long term. Women can get stress, hot flashes, and decreased libido due to that hormonal decrease in their bodies.
Conclusion
Other issues like stress can cause increased cortisol formation, anxiety, inflammation, simple carbohydrates, et cetera to the body associated with joint and muscle pain. They can also inhibit sex and sex hormone production directly and indirectly. So this is where people have to be concerned if they’re giving DHEA because DHEA can convert itself into sex hormones. So that can be a good thing if you’re dealing with hormonal deficiency. But if you give too much DHEA, you can overproduce hormonal function.
Making and maintaining healthy lifestyle changes does not have to be as challenging when surrounded by family, friends, and loved ones who support those goals. Healthy gifts or the gift of wellness can be the real difference in improving one’s or another’s health this season. With the right health tools, individuals can make, see and feel the changes happening. Here is a list of a few of the best healthy holiday gifts to help your loved ones begin the New Year with a healthy perspective.
Healthy Gifts
Compact Treadmill and Walking Pad
Walking daily is an integral part of overall wellness. The body was designed to move, and walking about 8,000 steps daily has been shown to reduce all-cause mortality compared to sedentary lifestyles. Unfortunately, it’s estimated that many individuals only walk around 5,000 steps daily.
In inclement weather, they allow individuals to walk and complete a workout.
Smaller walking pads can be installed under a standing desk for easy and effective movement during the workday.
Top Blender
Individuals that take supplements could benefit from a high-quality, all-purpose blender.
A quality blender easily whips healthy smoothies, protein shakes, and other healthy beverages.
Athletes can incorporate protein powder into their drinks.
Certain high-tech blenders double as water infusers to reach hydration goals.
Percussive Massagers and Foam Roller Sets
Muscle recovery and maintaining flexibility are essential for body health. Recovery-specific tools can help immensely.
A personal percussive massager uses vibration therapy to keep the muscles loose and release endorphins.
Percussive massage treatment relieves soreness, stretches out the muscles, and improves flexibility and muscle strength in older individuals with sarcopenia or age-related muscle mass loss.
Self-myofascial release tools like foam rollers can help roll out sore muscles while improving range of motion and muscle strength.
Athletic Earbuds
Research from workout enthusiasts and athletes has shown that having the right music or podcast makes or breaks the workout or sport.
The research found that music can have an ergogenic effect on performance by increasing exercise duration and performance.
Sweat-free earbuds are recommended as they are designed specifically for athletes, increasing their comfort and staying in place during their entire workout, no matter how intense.
Air Fryer
Deep-fried foods can be full of unhealthy saturated fats and trans fats and are associated with various health concerns, including cardiovascular issues and type 2 diabetes.
Air frying offers a healthier way to cook favorite foods, like fried chicken, French fries, fried vegetables, etc.
Air fryers rely on convection heat that circulates to crisp up the food.
This method is healthier than traditional frying methods.
A study found that air-frying French fries led to a reduced formation of potential food hazards versus deep-frying.
In addition, air frying can also be incorporated into baking or roasting.
These units can keep track of lean body mass, metabolism, and neuromuscular function.
They measure body fluid balance, muscle mass, and fat distribution.
They offer real metrics for current skeletal muscle mass.
Data points help individuals better understand their health.
Meditation Mats and Benches
Mental health is as vital as physical health.
Incorporating mindfulness and meditation exercises daily can improve mental and physical well-being and encourage long-term behavioral changes.
Regular meditation practice can help improve sleep quality, mood, and body repair and recovery from work, school, sports, workouts, etc.
Meditation mats and benches can make seated and kneeling meditation practices more comfortable.
Therapeutic Environment of Insight
References
Dong, Lu et al. “Effects of Air Frying on French Fries: The Indication Role of Physicochemical Properties on the Formation of Maillard Hazards, and the Changes of Starch Digestibility.” Frontiers in nutrition vol. 9 889901. 27 Apr. 2022, doi:10.3389/fnut.2022.889901
Pinho, Alexandre S et al. “Can We Rely on Mobile Devices and Other Gadgets to Assess the Postural Balance of Healthy Individuals? A Systematic Review.” Sensors (Basel, Switzerland) vol. 19,13 2972. 5 Jul. 2019, doi:10.3390/s19132972
Rusch, Heather L et al. “The effect of mindfulness meditation on sleep quality: a systematic review and meta-analysis of randomized controlled trials.” Annals of the New York Academy of Sciences vol. 1445,1 (2019): 5-16. doi:10.1111/nyas.13996
Thakare, Avinash E et al. “Effect of music tempo on exercise performance and heart rate among young adults.” International journal of physiology, pathophysiology and pharmacology vol. 9,2 35-39. 15 Apr. 2017
Wu, S., Ning, HT., Xiao, SM. Effects of vibration therapy on muscle mass, muscle strength and physical function in older adults with sarcopenia: a systematic review and meta-analysis. Eur Rev Aging Phys Act 17, 14 (2020). https://doi.org/10.1186/s11556-020-00247-5
Dr. Alex Jimenez, D.C., presents how hormonal dysfunction can be assessed and treated through various therapies specializing in hormones and how to regulate them in this 3 part series. This presentation will provide valuable information to many people dealing with hormonal dysfunction and how to utilize different holistic methods to optimize their health and wellness. Part 2 will look at the assessment for hormonal dysfunction. Part 3 will look at various treatments available for hormonal dysfunction. We refer patients to certified providers incorporating various hormone therapies to ensure optimal health and wellness. We encourage and appreciate each patient by referring them to associated medical providers based on their diagnosis when it is appropriate. We understand that education is an excellent way when asking our providers intricated questions at the patient’s request and understanding. Dr. Alex Jimenez, D.C., only utilizes this information as an educational service. Disclaimer
What Are Hormones?
Dr. Alex Jimenez, D.C., presents: Today, we will look at utilizing foundational PTSD treatment strategy steps. As a treatment strategy, it is about the production, transportation, sensitivity, and detoxification of the hormone in PTSD. So let’s start with how interventions and major factors that influence these pathways within the access impact other body areas. How does an intervention on one hormone affect other hormones? So did you know that thyroid replacement can change the HPATG access in the body? So when people are dealing with hypothyroidism or subclinical hyperthyroidism and are being treated with suppressive thyroid hormone replacement, it induces changes in their bodies. This means they will become hypersensitive from ACTH to CRH or corticotropin-releasing hormone.
What this means is that they will produce and release more ACTH. When the patient becomes hypersensitive from an influx of hormones, it could lead to various issues with the other body systems that affect organ and muscle functionality. This is another reason patients feel great on even low doses of thyroid replacement; it stimulates the adrenals. Many patients tend to overrun their adrenals, and when they get treatment, they get a little hit to their adrenals when their doctors are helping their thyroid. So looking at the thyroid, we see the thyroid gland is producing t4, forming reverse T3 and t3. So when doctors look at the thyroid pharmacological doses of glucocorticoids, which is what they give for anti-inflammatory therapy to their patients, or if people have elevated glucocorticoids as in Cushing syndrome, what that does is it inhibit thyroid secretion because it reduces the TSH response to TRH, which makes less TSH. When there is less secretion in the thyroid can lead to overlapping issues associated with unnecessary weight gain, joint pain, and even metabolic syndrome.
To that point, stress inhibits the thyroid. In contrast, estrogens have the opposite effect, where they increase TSH secretion and the thyroid gland’s activity. So that’s a reason why women feel so much better on even low doses of estrogen replacement. So just like thyroid replacement in low amounts that bump the adrenals, if we’re giving low estrogen doses, it can bump up thyroid function. However, many doctors have to go slow when providing hormone treatments to patients because the additional hormones will affect the other hormones in the body. When it comes to hormone replacement therapy, it is important to learn how interventions within the communication node impact other nodes in the matrix. So, for example, let’s look at how the communication node affects the defense and repair node in the body. Research studies reveal HRT’s effects on inflammation markers and look at 271 women who used conjugated equine estrogen alone, who had a 121% increase in CRP after a year.
And if they used that in addition to synthetic progestin, they had a 150% increase in CRP after a year. So synthetic estrogen is not bioidentical; this is synthetic pregnant mare’s urine, and synthetic progestins are pro-inflammatory. What about the communication node and the assimilation node? This is an interesting study because many doctors are trying to help their patients and the future generation in society. So it’s important to know when the mother is stressed during pregnancy since that can change the baby’s microbiome. That means doctors have an opportunity to support early intervention in microbiome support. Knowing this is vital for prenatal stress based on questionnaires or elevated cortisol was strongly and persistently associated with infants’ microbiome and colonization patterns.
So we’re also here to learn how interventions on the matrix affect the hormone node or the communication node. So as an example, we’ll look at what happens in the assimilation node involving the communication node, as this affects antibiotics on the intestinal metabolome. Everyone knows about antibiotics’ impact on the microbiome, but a metabolome is a change in the metabolic function of a particular organ, the intestine. To that point, when there are so many metabolic pathways that antibiotics affect, the metabolism of steroid hormones was the most profoundly impacted. So eight metabolites that are part of this hormone pathway, which gives us PTSD, were increased in feces after antibiotic treatment. Then we have another way that the gut affects hormones, and this is looking at metabolic endotoxemia. Many doctors learn about metabolic endotoxemia in AFMCP, which mentions leaky gut or increased intestinal permeability. When many individuals are dealing with gut issues affecting their well-being, like problems in their joints or muscles causing them pain, we provide various solutions and develop a treatment plan with our associated providers based on the diagnosis.
Endotoxins Affecting Hormones
Dr. Alex Jimenez, D.C., presents: Endotoxins or lipopolysaccharides are from the cell membranes of bacteria. So bacterial endotoxins are translocated from the gut lumen because of increased intestinal permeability. So with that increased permeability, those endotoxins are translocated, which starts an inflammatory cascade. When endotoxins cause GI issues, the inflammatory markers can affect the upper and lower portions of the body and the gut-brain axis. When the gut-brain axis is affected by inflammation, it could lead to joint and muscle pain associated with somato-visceral and visceral-somatic problems. To that point, the inflammatory cascade from the leaky gut affects the ovary, reduces progesterone production, and contributes to luteal phase deficiency. That’s incredibly important for doctors to take care of patients that are there to optimize fertility. It is especially important for patients to let their doctors know when they have excess estrogen and that they are producing as much progesterone as possible. So we must worry about gut permeability in ovulation, luteal phase deficiency, and estrogen-progesterone imbalance. What about the biotransformation node? How does that affect the communication node? In preschool children, phthalates and thyroid function have an inverse association between the metabolites or the amount of folate and thyroid function in the system measured in children at age three. When inflammatory issues affect thyroid function in children, it can affect cognitive outcomes, thus reducing phthalates production in the thyroid, leading to mental problems.
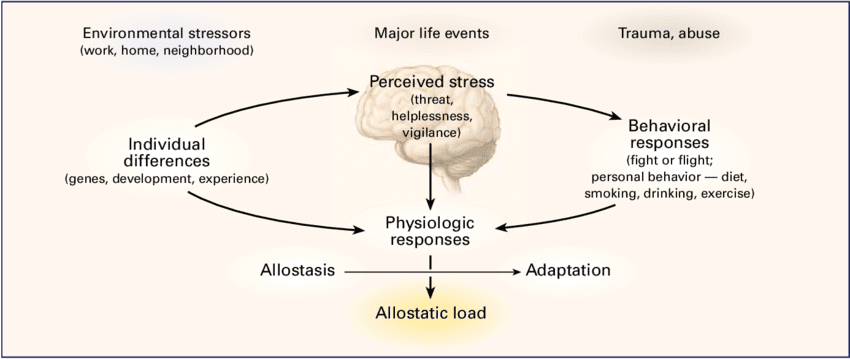
How do mental, emotional, and spiritual considerations contribute to the communication node? We want to start with the bottom of the matrix like we always do, which involves functional medicine. Functional medicine provides holistic approaches to identifying the root problem affecting the body and developing a personalized treatment plan for the patient. By looking at the lifestyle factors at the bottom of the Living Matrix, we can see how hormone dysfunction affects the communication nodes in the body. A recent paper found that there was a positive relationship between menopausal symptoms and social support and that menopausal symptom decrease as social support increases. Now let’s talk about how stress impacts HPA access. By looking at how stimulation from the sex hormone-producing parts of the body or the goads, the thyroid access, the adrenals, and the sympathetic nervous system (fight or flight) can add up all the stressors affecting us, called allostatic load.
And allostasis refers to our ability to respond to those stressors through stress-coping mechanisms. Many patients are asking us for guidance. They’re asking how they can frame their personal experiences and stressors. Still, they’re also asking how they prepare the societal events in a larger context, And many of us as functional medicine practitioners are seeking the same thing. And so, we’re going to show you in detail what stress does to the body and how to find ways of decreasing anxiety or stress in the body to prevent future issues in the organs, muscles, and joints.
How Stress Inhibits Estrogen
Dr. Alex Jimenez, D.C., presents: Does stress creates adrenal stress, and does it affect our fight or flight primary response hormone (adrenaline)? Stress can cause the sympathetic nervous system to increase blood pressure, respiration, heart rate, and general alertness while redirecting our blood to increase our adrenaline. So when you are in a situation, your adrenaline can cause you to fight or run, which causes your muscles to get blood, which decreases blood to your core or your non-essential organs. So the functional medicine model would identify various triggers or mediators, whether acute or chronic, that can act as an instigator of hormone dysfunction that can create overlapping issues that can disrupt adrenal function in the thyroid.
So, looking at these responses can help us see the physical problems that are happening if adrenaline is chronically increased over the long term, leading to anxiety, digestion problems, et cetera. Now cortisol is our vigilance hormone that helps maintain the emergency response to back up or support the adrenaline. An example would be a fire truck or police that come in after the immediate first responder. So cortisol facilitates the quick adrenaline response to keep the body going as needed. And it has many other roles as well. It helps with increased blood sugar and causes fat storage. So when people come in with weight around the middle and dealing with overlapping issues in their body, think of cortisol since it’s anti-inflammatory and regulates the nervous system. Cortisol can be both good and bad for the body, especially when an individual is dealing with stressful events affecting their health and causing issues affecting their mobility.
So now, let’s talk about how stress impacts the entire body and the immune system. Stress can increase susceptibility to infections, increasing their severity in the body. So here we see stress affecting the defense and repair node, leading to immune dysfunction and stress-induced immune dysfunction. An example would be if a person is dealing with a disorder that affects their gut, like SIBO or leaky gut; it can increase the production of pro-inflammatory cytokines and causes joint and muscle pain to the lower back, the hips, the knees, and overall wellness. When the pro-inflammatory cytokines affect the gut system, they can also cause thyroid dysfunction, disrupting hormone production.
So if someone’s taking that hormone replacement therapy (HRT), it can increase their inflammation, especially if they are stressed. So, as functional medicine practitioners, we’re always thinking and looking for pattern recognition as we start thinking about things differently from conventional methods regarding health and wellness.
What is it when you see a person dealing with chronic stress, and what is their response? They will usually answer, “I sweat a lot; I get nervous and anxious just remembering what has happened to me. I’m afraid of experiencing that ever again. Sometimes these pathways give me nightmares. Whenever I hear a loud noise, I think of carbon rings and get nauseous.” These are some tell-tale signs of someone dealing with chronic stress associated with PTSD, which can affect the hormone levels in the body. Many functional medicine providers can utilize available treatment regarding hormonal dysfunction in PTSD. So the general strategy for treating hormone dysfunction is the production, transport sensitivity, and detoxification of hormones in the body. Remember that when you have someone dealing with hormonal issues, it is best to devise a strategy to deal with this issue.
So what can we do to affect how hormones are produced or have been over-produced in the body? We want to look at how hormones are made, how they may be secreted within the body, and how they’re transported. Because what if they’re transported in a way that the transport molecule is low in concentration, allowing them to be free hormones? So that’s the interaction with other hormone sensitivity, and how do we change or look at cellular sensitivity to the hormonal signal? For example, progesterone affects estrogen receptors which cause detoxification or excretion of the hormone.
So before we think about giving or replacing a hormone, we ask what we can do to affect that hormone in the body. Specifically, how can we influence the hormone’s production, transport, sensitivity, detoxification, or elimination? So when it comes to hormone production, what are the building blocks for thyroid hormones and cortisol? So if we’re low on thyroid hormones, we want to ensure that we have the building blocks of serotonin. So what affects synthesis? If a gland is inflamed with autoimmune thyroiditis, it may not be able to make enough thyroid hormone. And that’s why people with autoimmune thyroiditis have low thyroid function. What about hormone transportation? Do the levels of one hormone in the body impact the levels of another? Estrogen and progesterone are often in a dance in the body. So does a hormone transport from the origin glands to the target tissue, which can impact its effectiveness?
If there is an overproduction of hormones attached to the transport protein, there won’t be enough free hormone, and there can be hormone deficiency symptoms. Or it can be the opposite if there needs to be more transport protein, then there will be too many free hormone molecules and hormone excess symptoms. Therefore, we want to know if we can impact the free hormone level and see if it is transformed. So we know that T4 becomes the active form of T3 or a thyroid inhibitor, reverse t3, and can we modulate those pathways? What about sensitivity? Are nutritional or dietary factors influencing the cellular response to cortisol, thyroid hormones, testosterone, estrogen, et cetera? With many cell membrane binding proteins, the cell membrane is involved in hormone metabolism. And if the cell membranes are rigid, insulin, for example, has a hard time getting in it now as we look into hormone detoxification. How do we alter the metabolism of estrogens or testosterone?
And what can we do to affect estrogen’s binding and excretion? So, can estrogen have to be eliminated healthily? And that depends on whether there’s hydroxylation on a particular carbon, but it also has to be excreted in terms of total amounts. So constipation, for example, will decrease the quantity of estrogen excreted. So we use the vault as a metaphor and the theme, as we said, is to treat the matrix first before directly addressing hormone dysfunction.
Cortisol Affecting The Communication Nodes
Dr. Alex Jimenez, D.C., presents: In the Living Matrix, we have to unlock or treat all the nodes to open the vault to get inside and address hormones. This is because the endocrine system is so complex it often self-corrects when other imbalances are addressed. And remember, hormonal imbalance is often an appropriate response by the body to imbalances elsewhere. That’s why treating other imbalances often addresses the hormonal issue. And also, remember hormones like picograms are in very low concentrations. So it’s very hard to be precise when we give patients hormones and allow the body to auto-correct. That’s why we say to treat the matrix first. And when we get inside the communication node in the body, we look at the center of the matrix and discover the body’s emotional, mental, and spiritual functions to help normalize hormones. And while these are addressed, how can we fix the hormonal communication nodes?
When inside the communication node, the treatment must follow an order: adrenal, thyroid, and sex steroids. So these are important concepts to remember, treat adrenals, thyroid, and finally, sex steroids. And the way we depict the pathways will be consistent. So here you see the standard representation we will use for the steroidogenic path. And you see all of the different hormones here. The enzymes in the steroidogenic pathway are color-coded, so many doctors can know which enzyme affects which step. Next, we will look at the modulation of the steroid pathways through lifestyle, like exercise, and how stress affects aromatase, making estrogen.
Now, as we get into the real, heavy part here about the steroid pathways, we inform many of our patients to take a deep breath as it shows that taking a deep breath can increase a person’s cognition and provide the ability to understand everything. So the big picture here is everything starts with cholesterol and how it affects the hormones in the body. So cholesterol forms the mineral corticoid aldosterone, which then develops cortisol, ultimately creating androgens and estrogens. When patients are given consultation on what is going on with their bodies, many don’t realize that high cholesterol could potentially lead to chronic stress, which is associated with cardiovascular issues that can ultimately invoke visceral-somatic disorders.
Dr. Alex Jimenez, D.C., presents: When a female patient is dealing with fibroids or endometriosis, many doctors devise a treatment plan with other medical providers to reduce the formation of the estrogen hormones by inhibiting and modulating the aromatase enzymes. This allows the patient to make small changes to their lifestyle habits by ensuring their zinc levels are normal, not drinking alcoholic beverages constantly, finding ways to reduce their stress levels, and normalizing their insulin intake. Each treatment plan caters to the individual as they find ways to reduce their cortisol levels and regulate healthy hormone production. This will allow the body to increase estrogen production while decreasing the aromatase. So when we are discussing stress, it can negatively impact the hormone pathways directly by increasing cortisol, thus causing the pituitary glands to increase the CTH when stress is responding to the body. Many individuals are dealing with chronic stress in their bodies, which can cause overlapping risk profiles to the musculoskeletal system, causing muscle and joint pain.
So the pituitary system produces cortisol when the body calls for it directly when the individual is dealing with acute stress. However, chronic stress can indirectly increase cortisol levels; it causes the enzyme 1720 lyase to be inhibited in the body, causing a decrease in anabolism, thus slowing down the body’s energy levels. So stress inhibits this enzyme. So when stress inhibits the 1720 lyase enzyme in the body, it can cause the pituitary system to produce more cortisol and cause more issues like joint to affect the individual. So those are the two ways that stress leads to more cortisol directly through ACTH and indirectly by inhibiting 1720 lyase.
Inflammation is important in the body as it also has a two-way path, as it can impact these pathways the same way stress does. Inflammation can inhibit the 1720 lyase enzyme, causing the body to be pro-inflammatory and can stimulate aromatase. Like stress, when the body is dealing with inflammation, the pro-inflammatory cytokines stimulate aromatase enzymes to cause an increase in estrogen formation. When this happens, it allows the doctors to notice why their patients are overly stressed and have inflammatory markers in their gut, muscles, and joints. To that point, inflammation can also increase an enzyme called 5alpha reductase. Now, 5alpha reductase causes the formation of a hormone called dihydrotestosterone (the active form of testosterone in the body cells other than the muscles, causing hair loss. So insulin, stress, and inflammation contribute to hair loss because insulin has the same effect. Insulin or blood sugar gives the body energy to move throughout the day. When individuals have too much or too little insulin in the body, it can lead to insulin resistance, correlating to metabolic syndrome associated with hair loss.
Holistic Methods For Hormones
Dr. Alex Jimenez, D.C., presents: How do insulin, cortisol, and inflammation play their part in the thyroid? Well, all of these hormones help make the body functional. When the thyroid has an underlying condition like hypo or hyperthyroidism, it can cause the body to over or underproduce hormones to regulate healthy normal body functions. So this forward feed cycle can cause the individual to have various issues affecting their body due to hormonal dysfunction. This combination of insulin resistance, high insulin, weight gain, and stress affects many patients, causing metabolic syndrome. To normalize hormonal function, we must look at all these factors driving hormonal dysfunction in patients.
When going for hormonal treatment, it is important to know about the different nutraceuticals and botanicals because before, it was called a lifestyle change back in the day. In a health clinic, specific neutraceuticals and botanicals can affect estrogen formation through the enzyme aromatase. However, various factors like diseases, medications, toxins, and elevated insulin can also increase aromatase enzymes, leading to more estrogen in the body. And then diseases, medications, and toxins do the same thing. A research study reveals that when men and women interact, the men’s cognitive performance declines, followed up with a mix-sex encounter. This can change how hormone function in the body when there are changes in formal function that can affect the central nervous system’s cognitive function in the body.
When middle age patients get examined by their doctors, the results can show if they have elevated insulin, an increase in stress and if there is inflammation in their bodies. This allows the doctors to work with associated specialists to develop a treatment plan that caters to the patient to begin small changes in their health and wellness journey.
Dr. Alex Jimenez, D.C., presents how to assess different hormones in the body and how different hormone tests can be used to determine the level in the body. This presentation allows many individuals to know what to expect when they are being diagnosed by their primary doctors. We refer patients to certified providers incorporating various hormone therapies to ensure optimal health and wellness. We encourage and appreciate each patient by referring them to associated medical providers based on their diagnosis when it is appropriate. We understand that education is an excellent way when asking our providers intricated questions at the patient’s request and understanding. Dr. Alex Jimenez, D.C., only utilizes this information as an educational service. Disclaimer
Assessing Hormones
Dr. Alex Jimenez, D.C., presents: Welcome to everything you need to know about assessing hormones and how to do the testing. We have decided to do this as a webinar because we only have a little time to do it during the module. After all, that’ll make your life easier. You’ll need to have this information under your belt because here is the most important thing you need to know. Hormone therapy is an art, not a science. If you find five or six practitioners who do hormone therapy, you will find five or six different ways to make a prescription and way more ways than that actually to do testing to monitor it.
Dr. Alex Jimenez, D.C., presents: The important thing is that you keep in mind what we know scientifically is a better or not-so-good way of taking care of the patients in terms of testing. Then find what works for you and become the expert in that. Because if you are consistent over time, you can work around the pros and cons of every given testing modality and figure out what you need to do, regardless of what type of test you end up doing. All right, so what do we need to worry about? There are many potential problems in measuring hormone levels because so many hormone levels fluctuate significantly. In order to evaluate hormones in the body, doctors need to know what, when, and who to test. So we’re going to talk about all of that.
Diagnosing Hormones In A Patient
Dr. Alex Jimenez, D.C., presents: Some vary during the day, some vary during a cycle, and some hormones don’t vary at all. So you need to remember which ones you need to worry about in terms of fluctuation. The studies that have been done don’t measure hormone levels. So, finding normal hormone levels is sometimes problematic. It may be different from what the labs currently use. And in the studies where they have come up with normal hormone levels, a lot of them are much older studies, and the methodology was more unreliable than what we use now. So by keeping that in mind regarding what people call normal hormone levels, many of these studies also would average out non-comparable groups. What this means is that they would be comparing, let’s say, a group of apples, oranges, and grapes and put them all together and say, oh yeah, so this average is going to work.
Dr. Alex Jimenez, D.C., presents: So it’s like doing a meta-analysis, and if you are taking a bunch of different data, you can’t necessarily say that this average makes sense. You probably are already aware of the fact that other labs end up developing different reference ranges. And so if you use multiple different labs, you can’t necessarily compare the test results you’re getting because the reference ranges are different. And, sometimes, even within a given lab, depending on which test kit patients use, like a test from Quest, they may one day use one test kit. So a reference range will be XYZ, and they went to the same lab another day, but they used a different test kit and have an entirely different reference range. And so you have to the point that out to the patients. If you’ve got a smart patient trying to track what’s happening with themselves, they may have the wrong impression during an examination.
Estrogen & Progesterone
Dr. Alex Jimenez, D.C., presents: If you’ve got different reference ranges showing up on your test results, it is best to keep track of that in case you need to remember. Now there are big variations between individuals and even within the same individual. The serum concentrations of both natural and synthetic steroids might need to be clarified between other individuals. There’s a huge variation irrespective of the root of the administration of the hormones. What you expect from one person may be different from the next person. And, of course, within any individual, you’re going to get levels of fluctuation throughout the day based on lots of different things. Everything from perceived or actual stress that will change their hormone levels to foods they were eating that day can make a difference. Hydration status can make a difference. So some of the variations you see within a person, but with different blood draws, can be based on what was going on that day.
Dr. Alex Jimenez, D.C., presents: So try to impress upon your patients as you’re getting testing done to keep the blood draw days the same. Now measuring in different body fluids like serum, urine, or saliva doesn’t necessarily tell us about concentration in other tissues, and doctors need to keep this in mind because the patient may get a false sense of security, and it won’t necessarily have anything to do with the tissue they are trying to treat. Now, many doctors must remember all the different kinds of estrogens they might need to keep track of during examination. So, when they notice estrogen, there’s an estrogen pool. There is free and bound estrogen in the body and estrogen production in the woman or a man in themselves. There are exogenous estrogens that you may be giving them. There are stored estrogens, metabolites, and all these different estrogens doctors need to keep track of. So this is just one example of having many estrogen levels in the body, and the patient is wondering, what is it the doctor is looking at? Could one test give me all this different information? And this is only estrogen. The same thing is true, although not quite as complicated. The same thing is true about the other hormones in the body.
Dr. Alex Jimenez, D.C., presents: Now for progesterone, it is the same ordeal. Other results look like this for estrogens and testosterone, and this is to remind us of all the different variability there is. By showing the variation between different people at their biological stages, for example, premenopausal and postmenopausal. The results that the doctor presents to the patient establish a lighter shade of green on the outside of the intercycle variability from within a given woman. And then the yellowy green is the inter-woman variability, meaning one woman to the next. And then that blue line in the middle is the average; this provides what information they might need to diagnose.
Testing Hormone Levels
Dr. Alex Jimenez, D.C., presents: All right, so let’s look at testing and assessing hormones as we look at all the hormone types, the different ways of testing them, and the pros and cons. There are decades of well-validated research on serum hormone levels. So for the estrogens, estrone, estradiol, and estriol, as well as the estrogen metabolites in the serum, the good news is it measures endogenous hormone production. So if you get a serum hormone level, we know what those results mean.
Dr. Alex Jimenez, D.C., presents: The bad news is these results give you the free and bound hormone. It shows you the total estrogens. However, you can’t order total estradiol and free estradiol test as they don’t offer them. There are limited data regarding serum levels of these metabolites in terms of prediction for health risk. And it can be difficult for some labs to get accurate quantification in postmenopausal women because the estrogen levels are very low. So, keeping that in mind is a matter of knowing your lab and how accurate they are. Now when it comes to saliva, the good news is it’s non-invasive. Patients can do this at home, making it convenient if doctors try to do a serial measurement of estradiols across a whole cycle in a premenopausal woman. Cause no one in the right mind will go to the lab and get blood drawn daily.
Dr. Alex Jimenez, D.C., presents: Knowing that salivary estradiol correlates well to free estradiol in serum allows doctors to see what’s in the saliva and what they want to see in the serum. The bad news about saliva is that there are fewer validation studies than serum. There are still quite a few, so it’s a valid testing method. It’s just that it’s not as well validated as a serum because it still needs to be done. Again, it can be very challenging for some labs because the estrogen levels in the saliva are much lower than in the serum. So doctors must ensure the lab is doing a good enough job assessing these very low levels. All saliva testing can be contaminated by blood from the oral mucosa.
Saliva Testing
Dr. Alex Jimenez, D.C., presents: So if the patient has periodontitis or something along those lines, doctors don’t want them to salivary levels; it is important to tell them to do it before they brush their teeth, not after, in case they bleed when they brush their teeth. But that’s true of any salivary test; you can’t get estrogen metabolites done through the saliva. And the bigger problem in a postmenopausal woman is that many get dry mouth after menopause. And so, it can be really difficult to do the test because they need to produce more saliva to get an adequate specimen. Now, if that happens, they can go for a 24-urine test. The 24-hour urine testing for estrogen and estrogen metabolites can be helpful if you’re trying to get the total daily production of the hormones. You can get measurements of estrogen metabolites, which are stable for a long time.
Dr. Alex Jimenez, D.C., presents: You have plenty of time for processing and get both free and conjugated estrogen measurements. So that’s helpful. The bad news, which is true for any 24-hour urine test, is it relies on accurate volume measurements and complete collections by the patients. Many patients will inadvertently screw that up. When they have a busy day, they’ll go pee and need to remember what they are supposed to do, which can be a problem. So, making sure the patient understands can help with the test results. You cannot use this for people with renal dysfunction because it’s based on creatinine correction. So if their creatinine is abnormal, they will need to be able to give you an adequate, appropriate level and sometimes give you some of these tests that do 24-hour urines will provide you with many metabolites that could be more clinically useful but are not.
Dr. Alex Jimenez, D.C., presents: Now for dried spot, you’re in testing, and you can get estrogen metabolites, which is good because the metabolites are stable for a long time, so that’s no problem. And you can measure both the free and conjugated estrogens on these spots in urine tests. The biggest problem here is that it has the least clinical validation studies. So, it’s a newer way of testing. It is popular and easy for patients, but there is little concern because of the few clinical validation studies they’ve done. Now, additional challenges are mentioned: to think about what a lab has to do; the measurements they need to be able to provide can vary enormously because there are very low levels of estrogen in older women, not on hormone replacement therapy.
Dr. Alex Jimenez, D.C., presents: And then up to measuring these super high doses in women getting ready for IVF. And, you know, the levels can vary by 10,000. Is it reasonable to assume that any test will be accurate for all those circumstances? It is also difficult to assess estrogen levels in women treated with aromatase inhibitors because they will likely have very low estrogen concentrations. So that may not be accurately detected by standardized testing. And then specificity is a problem because we talk about how estradiology focuses mostly on how it gets broken down into estrone and then how the estrones get broken down. But the reality is that estradiols convert it to more than a hundred different metabolites, which may interfere with accurate quantification.
Serum Testing
Dr. Alex Jimenez, D.C., presents: So, labs must keep that in mind and ensure that they’re getting adequate specificity for you. Another interesting tidbit is that exogenous sources of S-trial can lead to falsely elevated estradiol levels. So keep that in mind if you have a funny test result that makes no sense.
Dr. Alex Jimenez, D.C., presents: Progesterone and progesterone metabolites in the serum; there’s lots of literature to support using a progesterone level drawn hopefully on day 21 of a 28-day cycle to confirm ovulation. Progesterone has problems as it differs from estradiol. So it is acceptable to use serum progesterone levels for that, as the reproducibility of serum levels is limited if the serum levels are low. So if what that means is if you were to take a person in the first half of her cycle and draw a progesterone level three days in a row at the very beginning of the process and the progesterone should be low, you may not get similar numbers just because the hormone levels are low.
Dr. Alex Jimenez, D.C., presents: So the reproducibility makes doctors a little crazy, but that’s something they need to keep in mind with the serum. Again, saliva testing is not invasive; it’s convenient if you want to follow an entire cycle in a premenopausal woman. Also, research shows that a salivary level of 17 alpha hydroxyprogesterone is just as acceptable as a serum level for diagnosing congenital adrenal hyperplasia. Now the downside for progesterone’s metabolites salivary levels of progesterone in its metabolites is that you’ve got a rapid fluctuation of progesterone levels in the saliva. So, if you’ve got somebody who doesn’t wanna get their blood drawn and doesn’t mind spitting into a tube, you can use this instead.
Dr. Alex Jimenez, D.C., presents: So you should use more than one test result to make a decision; you may need serial sampling to get a feel for the average. There’s also a problem with cross-reactivity that might interfere with immunoassays and affect the results. And again, the same problem is having much lower progesterone levels in the saliva than in the serum. So for some labs, that can be challenging to get preliminary analysis and the same problem in terms of contamination by blood; however, that’s true of all cellular tests. The 24-hour urine and the spot dry urine testing for progesterone have the same problem because the progesterone metabolites will correlate with symptoms. So they’ve studied, for instance, allopregnanolone in urine. The level of that does connect with the sleep quality in perimenopausal women.
The Different Implications Of Hormone Testing
Dr. Alex Jimenez, D.C., presents: The implication is that if it’s correlating, it’s probably an accurate level; however, progesterone is hard to quantify in urine. And so, they use metabolites for assessment and determine the progesterone level based on the metabolites. That’s great, except there’s no literature describing the clinical utility of progesterone metabolites. So progesterone in the urine is relatively problematic regarding the accuracy and what you are getting. Part of the issue with serum progesterone is that very little of it is available, and non-protein ground, most of it is bound to all and other proteins; it’s the free progesterone that is available to the target tissues and also to saliva. So the progesterone that you’re measuring in the serum is mostly the bound-up progesterone, not what is clinically important.
Dr. Alex Jimenez, D.C., presents: Transdermal progesterone is extremely difficult to measure because anyone gets metabolism by five alpha reductases in the skin. It’s rapidly absorbed by red blood cell membranes and delivered to the tissue. And really, it comes down to that after the patient uses exogenous progesterone cream or gel, they get these crazy high levels of progesterone in the saliva and the capillary beds, but not in the serum. And so there could be a better way to measure what’s happening to the patient. So transdermal progesterone, trying to follow that with any testing is difficult.
Dr. Alex Jimenez, D.C., presents: There are decades of research on serum hormone levels. In serum testing, testosterone, and its metabolites, you can get both a total and a free hormone level test, and you can also get a DHT level, which is helpful. There are established serum ranges for the diagnosis of androgen insufficiency. So serum levels for testosterone are fine in general. It can be difficult to assist the whole serum if the levels are low, like in women and kids and hypogeal men. So, you need to know your lab and its methodology. Suppose you’re assessing testosterone in women, hypogeal men, or kids because they must ensure they’re doing the appropriate serum test to get these really low levels accurately.
Dr. Alex Jimenez, D.C., presents: For saliva testing, it is very convenient to obtain the sample. There are established ranges for diagnosis of antigen insufficiency, and it’s easy to use this testing for differentiating between gonadal and hypogonadal men. And you can get a free hormone level as lots of published research on using salivary levels for assessing testosterone. However, the problem is like with progesterone; you get this rapid fluctuation in saliva. You might need more than one saliva test result to get reliable information. So you don’t necessarily want to decide based on just one result. And again, you need to know your lab because the levels are much lower than in the serum. So it is challenging to get an accurate story and be careful about blood contamination. In urine testing, the 24-hour and spot urine have slightly different issues.
Dr. Alex Jimenez, D.C., presents: The 24-hour urine testing for testosterone can be used to get a total daily testosterone production. Patients will get a free hormone level and metabolites, which is nice. They can use that information to indirectly assess five alpha-reductase and aromatase activities based on how many different metabolites they’re getting. Only a few data support the clinical utility of all the measured metabolites. There is a polymorphism of UGT to B17; if the patient has that, their urinary testosterone level will return to zero, so keep that in mind if you ever get a test result. After all, it’s so low because it may be that your patient has this issue. Now spot urine will give you some of the same pros as you will get free hormone levels and metabolites. This allows you to use that information to assess the five alpha-reductase aromatase activities; however, the problem is there; like with the other hormones we’ve discussed, this testing generally has fewer clinical validation studies because it’s a newer form of testing, so keep that in mind.
Cortisol
Dr. Alex Jimenez, D.C., presents: Cortisol and its metabolites in the serum are similar to the other hormones mentioned, as there are validated reference ranges for cortisol. Lots of peer review literature detailing the use of this test, and patients can feel comfortable getting these results. It will tell them just total cortisol, not their free cortisol. So by keeping that in mind, they’ll get the diurnal pattern. They can only get a four-point test as they would with saliva because they don’t have normal ranges for four different times in the day. And many patients mention to their doctors as they get the serum cortisol, they go, “Wait, you don’t understand. I am so scared of my blood being drawn that it shoots my cortisol up, and I don’t normally look this bad.”
Dr. Alex Jimenez, D.C., presents: Keep in mind that in serum, they only have normal reference ranges for two times of the day, 7 to 9:00 AM and 3 to 5:00 PM. So you have to ensure that if you use serum cortisol, they go in fasting before nine o’clock, or they can go later in the day. And if they go later in the day, they don’t have to fast. So if you get cortisol at 10 or 11 in the morning, it isn’t very helpful to the results. Now the salivary testing, lots of people are becoming familiar with this.
Dr. Alex Jimenez, D.C., presents: You can get your diurnal pattern because many companies have kits where you’ve got four or five samples throughout the day. There is abundant peer-reviewed literature detailing the use of this. And this is for cortisol, not for the cortisol metabolic. It reflects the unbound plasma concentration, which is not what we’re seeing with the serum. The problem is that 11 beta hydroxy steroid dehydrogenase is an enzyme in the salivary glands that significantly converts cortisol to cortisone. So there are some questions about the results doctors are getting in the salivary cortisol and what’s happening or did it get converted to cortisone, and you’re not picking that up in the test?
Dr. Alex Jimenez, D.C., presents: So when looking at cortisol metabolites in the saliva, which some companies do and some don’t, the salivary cortisone correlates with cortisol exposure over 24 hours. There’s a moderate level of literature using this test but enough that you should feel comfortable. There are issues when your serum cortisol is really low, making it seem like the patient is crashing or under hydrocortisone therapy. That makes the salivary cortisone a superior serum marker compared to the salivary cortisol. Under these circumstances, because of how this is being processed, only a few companies are even looking at cortisone directly in the saliva. So at this point, because especially of the moderate literature level, you will primarily be doing cortisol levels in the saliva.
Urine Testing For Hormones
Dr. Alex Jimenez, D.C., presents: So let’s move on to the urine test. Now, in a 24-hour urine test, you can assess the cortisol ratio, which can be helpful when diagnosing. And 24-hour free cortisol correlates with the serum-free cortisol level; however, the only problem is there are limited clinical validation studies for this. And, in the 24-hour urine test, you’re not getting a diurnal cortisol pattern. And, in the spot urine, you can get the cortisol ratio, which can be helpful. You can have the patient do the spot urine test multiple times a day so you can get the diurnal change just like you would with saliva. But unfortunately, the spot you’re in testing has the least clinical validation studies. So you have to keep that in mind. So with this, primarily, people feel most comfortable with using either serum levels done at the right time of day, understanding that you’re not getting the unbound cortisol, or they’re doing a four-point salivary test.
Dr. Alex Jimenez, D.C., presents: The four-point salivary test could see a pattern between what the patient told their doctors about their energy level throughout the day and how they felt and compared that with what the result returned. Many doctors note what they had expected the test result to be before the national labs even had it available.
DHEA Testing
Dr. Alex Jimenez, D.C., presents: We will discuss DHEA and DHEA sulfates separately since DHEA in the serum has many clinical validation studies that can make you feel comfortable getting adequate results. Now, DHEA has a diurnal pattern. So you have to ensure they get it done at the right time of day since this is fasting before nine o’clock in the morning, just like with cortisol. A DHEA done later in the day means nothing; however, a DHEA sulfate in the serum doesn’t follow a circadian pattern, so a single test done at any time is okay.
Dr. Alex Jimenez, D.C., presents: There are numerous clinical validation studies about DHEA; unfortunately, there is a problem with DHEA sulfate since it has a little circadian pattern. You may miss small variations in a DHEA over time in a person based on how they’re feeling and stressed out. So occasionally, it’s nice to check the DHEA in a patient as long as they’re done in the morning because then you’ll get a feel for the changes over time in the same individual you wouldn’t see with the DHEA sulfate.
Dr. Alex Jimenez, D.C., presents: Salivary testing for DHEA is where you measure free DHEA in the body, which is great. There’s a correlation with serum levels, and it’s not invasive. The problem is that the concentration is inversely related to the salivary flow rate and is also affected by the salivary pH. An example would be someone walking past the bakery, starting to salivate heavily based on what they just smelled. This could change their results for their salivation rate when they are doing their DHEA test. DHEA sulfate has the same basic problem in the saliva, related to the salivary flow rate and the salivary pH. So keep that in mind if you’re looking at salivary levels in urine, whether this is 24-hour or spot urine; there are no clinical validation studies about looking at either DHEA or DHEA sulfate in the urine. So, keep that in mind if you’re doing urine testing and they’re giving you a whole panel that includes DHEA or DHEA sulfate, you may need to know what those results mean.
Dr. Alex Jimenez, D.C., presents: For pituitary hormones, the preferred testing is the FSH, LH, and prolactin serum. Not convenient for serial measurements throughout the day to detect the LH surge, for instance, but the results are very accurate. And in saliva, there’s limited peer-reviewed literature detailing salivary pituitary hormones and whether or not they’re adequate. LH detection kits at home are convenient for urine tests since they are widely used and have been around for a long time. The LH surge correlates with the urine and works well with the LH surge’s serum. So if you’re trying to help people figure out where they are in their cycle and whether or not they’ve ovulated, this test is the way to go. It doesn’t do a good job of quantifying it; it just tells you there’s a surge because these are bigger hormones, so they don’t get into urine very easily.
Dr. Alex Jimenez, D.C., presents: So you’re going to know whether or not you’ve gotten the surge, you’re not going to know what the actual level is, and that’s okay because most of the time, it doesn’t matter what the hormone level is. So essentially, unless you’re just trying to find out if they got an LH surge, you want to use the serum for either FSH, LH, or prolactin. For sex hormone-binding globulin, most clinical validation studies are in the serum; you can’t measure it in saliva or urine, so that’s easy to remember. So we’ve already talked about the issues with different forms of testing, and there are only a few forms of testing that will give you everything you need to know about every hormone you need to know.
When Is The Best Time For Hormones?
Dr. Alex Jimenez, D.C., presents: So now, when is the best time to test hormones? Early morning is when the hormones will be the highest for most hormones. So, the best way to go and test hormone levels like cortisol and gonadal hormones is first thing in the morning since you have to be consistent and fast because what you’ve eaten can change hormone levels. So if you’ve always fasting, at least you’ll find consistency between specimens and the same person. You also need to know where they were in their cycle for certain tests. So, women patients who are still cycling need to record the first day of their next period to know what day you did their testing. Otherwise, they’ll have to use ovulation kits to know exactly where they are.
Dr. Alex Jimenez, D.C., presents: And of course, the downside here is that if you’re trying, for instance, to get a day-21 progesterone, and she typically has a 28-day cycle, so you tell her to go on day 21, but that particular month she has a 35-day cycle, you didn’t get the level that you were looking for. So it can be a little problematic, but remind them to keep track of it so that you won’t be able to look back and know where they were when they had their tests done. So, when do we want these tests in pre and perimenopausal women? Suppose you want progesterone on day 21. You can also do a sex hormone-binding globulin on that day. Menstruating women shoot for as close to day three for estradiol, estrone, FSH, testosterone, or a sex hormone-binding globulin.
Dr. Alex Jimenez, D.C., presents: Now, even though these are ideal, can you get them on other days of their cycle? Yes, but they will have different accuracy. And, of course, it may be an additional day than day three because what if day three happens to land on the weekend and the lab’s not open? So, please consider that what you are looking for here is to test the hormone levels when they’re at their highest. And that’s why we’re shooting for three and 21. So, you know, here’s day three and four. And so the FSH is going to be a nice level here. The estradiol bounces around a lot at this point, so trying to get it in this part of the cycle would be less helpful. And, with progesterone, you’re going to get your peak here, so that’s why you want to try to shoot for 21 days because you know that’s going to be the easiest way to ensure you’re getting it. And also, it’ll help you be more consistent from cycle to cycle if you’re always trying to get it at the same time of the process.
Hormone Replacement Therapy
Dr. Alex Jimenez, D.C., presents: Now here’s where it gets tricky since it’s one thing to find out where the person is before you put them in any hormone replacement therapy; however, monitoring hormone replacement therapy gets more problematic still. If you’re using oral estrogen, it is recommended to get a serum baseline before HRT and then monitor during treatment; if you’re doing oral estrogen, the salivary levels don’t reflect the exogenous estrogen use at all, so they’re not very helpful.
Dr. Alex Jimenez, D.C., presents: And oral estrogen or any hormones that undergo this test must accurately reflect the liver’s first-pass metabolism and the urines’ levels. So if you’re doing oral estrogen replacement therapy, the only way to assess it is with serum because doctors will convince the patient with the module, so you probably don’t want to use oral estrogen anyway. If you’re using sublingual estrogen, the levels will rise and fall rapidly within hours. And so the serum’s not effective in terms of measuring. The saliva will make no sense if you’re doing sublingual because you just had your estrogen there. So what does it mean? It means that 24-hour urine and drive urine testing with sublingual hormones aren’t recommended because there’s always a question of how much you are swallowing and how much is getting absorbed sublingually.
Dr. Alex Jimenez, D.C., presents: Now, if you notice that it says in sublingual, there could be better testing methods. Since you don’t know how much was swallowed and got the first-pass metabolism effect, the result in a 24-hour or dried spot urine may need to be clarified. So that’s problematic. You can still do sublingual estrogen replacement therapy; it just means there’s no great way to test it. If you’re using estrogen creams, serum testing can be effective, and we know that clinical parameters correlate to serum levels when using estrogen creams, so we can do that. In saliva, estradiol and estriol are actively transported into the saliva; the levels are way higher than you would see in the serum and are highly variable. So salivary levels for creams don’t make sense, and there are no good peer-reviewed studies detailing the effective estrogen cream on urinary levels.
Using Hormone Creams & Patches
Dr. Alex Jimenez, D.C., presents: It is probably not a great idea to use urine levels for someone using estrogen creams at the time. If you’re using labial or vaginal estrogen, the serum test appears to be the best choice for monitoring absorption. The salivary levels don’t reflect any dose changes. So basically, it’s probably a waste of time to get a salivary level trying to do urine testing; using vaginal or labial estrogen might be problematic because how do you know you didn’t contaminate the urine specimen. And if you’re using a patch, serum values will rise dose-dependently and then rapidly decline the following removal. It may be helpful, we know that the serum values change based on when you put the patch on and when you take it off, but it is still problematic.
Dr. Alex Jimenez, D.C., presents: There’s no peer-reviewed evidence showing that salivary estrogen can be used to monitor the estrogen patch. And when it comes to the urine testing and the estrogen patch, it does appear that the values in the urine will go up dose-dependently. It may be relatively accurate, but it’s not the best clinically validated test for an estrogen patch. The take-home message here is that no testing is perfect and many of us adjust the dose to the lowest amount, the lowest level we can get, and still have our symptoms controlled. That doesn’t mean they don’t test; you must try to ensure you’re not overdosing on this person. But keep in mind that there are a lot of limitations around what testing can be helpful depending on what form of estrogen replacement you’re using.
Dr. Alex Jimenez, D.C., presents: Now, progesterone and oral progesterone, if you’re using that, the levels rise and fall quickly. You may not be able to catch a serum level that makes sense if you’re taking your progesterone in the evening and then measuring in the morning. Because most women, if they’re taking oral progesterone, will take it in the evening because it helps them sleep. There’s also a problem with the cross-reactivity of metabolites with the immunoassays. So progesterone replacement therapy, if oral, you must take the serum levels with a grain of salt. The same thing with saliva and 24-hour urine testing. We talked about how you’re not getting progesterone; you’re getting progesterone metabolites, so that might be useful. But there’s the problem of how clinically valid the use of progesterone metabolites is. So oral use of progesterone, getting a level, and following it is a little tricky.
Dr. Alex Jimenez, D.C., presents: Now with creams and transdermal progesterone, none of the tests makes any sense because you get mentally increased levels in the serum that don’t rise in any particular way that makes sense. Like all steroid hormones, these are fat-soluble, so if it goes and sits in adipose rather than getting into the bloodstream, it doesn’t necessarily reflect a serum level. Doesn’t necessarily reflect the tissue levels in the uterus and the breast, which is where we care about it. So a serum level for progesterone cream is problematic. Salivary levels after progesterone cream go way up and don’t correspond to symptoms at all. So don’t bother getting salivary level after a progesterone cream. There’s some evidence in urine testing that you can get small increases in the pregnant dial three glucosides if you use progesterone cream. And so it may turn out that we can use that as a measure of what your progesterone is doing.
Dr. Alex Jimenez, D.C., presents: But this still needs some more testing. So it would be best if you remembered that there needs to be a reliable method to track what’s happening when a person uses progesterone cream. So please take your time with getting a level and making a decision based on it. Now, vaginal progesterone suppositories have the same problem. You get minimally increased levels in the serum, which will not give you an adequate result. Progesterone melts or atrocious; you can use serum levels in at troche because you get a more accurate level in the serum than if you had taken it orally. There’s a lack of peer-reviewed research on salivary levels after vaginal progesterone suppositories. And you have to be careful if you’re trying to do urine testing because how do you know you didn’t contaminate the sample?
Dr. Alex Jimenez, D.C., presents: You can’t use a salivary level because you just had the troche or the melt in the person’s mouth. And then, there is at least a potential problem with getting a urine level for a troche or melt because, like a sublingual, how much of this are you swallowing? Individuals may consume some of it and are subject to first-pass metabolism, which means you won’t be able to pick it up in the urine. The larger portion will be absorbed into the capillary blood and probably be accurate in the 24-hour or dry urine test. But that needs to be adequately studied, so keep that in mind if you’re using atrocious or melts. And this is a study that showed that after applying topical progesterone, the saliva and the capillary blood levels were very different compared to those seen in the serum or whole blood.
It’s Important To Do Research
Dr. Alex Jimenez, D.C., presents: So this is just an important research study to remind you of the reliance on serum levels for progesterone. If you’re monitoring, topical dosing can lead to underestimated tissue levels, so you’ll give more than you need. So, be careful about relying on serum levels for topical progesterone because you’re going to overdose people like crazy. And remember, if you overdose on progesterone, it’s high up in the steroid hormone pathway, and you don’t know what this person’s body will do with it; they might turn it into pretty much anything else. Now, testosterone replacement therapy creams or gels can cause blood levels, and the serum level rapidly increases with the application and doesn’t reliably reflect dose changing, any dose changes. So the serum and blood levels are probably not the great way to go. In the saliva, the levels are much higher than the serum and are highly variable since they may give a false indication of overdose.
Dr. Alex Jimenez, D.C., presents: In the urine testing, there’s not good in the 24-hour urine. You probably want to use something other than 24-hour urine. The good news is the dried urine. Now in dried urine, the epitestosterone can be measured if there’s going to be suppression due to exogenous testosterone production if that’s what you think is going on. You can measure the epitestosterone in dry urine testing, which will tell you whether or not, you’ve suppressed this person’s production of testosterone by giving them some. Now, vaginal or labial application of testosterone, there’s no good way to get a blood level that makes sense. The salivary levels, like any other cream or application we might have on your hands, you have to be careful because if you’re handling the specimen vials, to get the saliva, you might get it into the testing medium.
Dr. Alex Jimenez, D.C., presents: And then, just like any vaginal or labial application, if you’re trying to get urine specimens, you have to be careful that you’re not contaminating the urine and getting a falsely elevated level. Blood levels are good if you’re doing testosterone injections, either injection or pellet. Get one-third baseline, and use them for monitoring. It gives you adequate levels. You’ll get a significant elevation in saliva after an IM injection, but there’s wide variability from person to person. So you must take that with a grain of salt regarding how accurate your result might be. The same thing happens in the 24-hour urine specimen. You’re going to get an elevation after an IM injection, but then, there’s a great deal of variability, so who knows how accurate it is?
Dr. Alex Jimenez, D.C., presents: With a salivary level, there’s only some correlation to the bioavailable testosterone. If you’re using a testosterone patch, you can get adequate levels, and there are good studies to show that a blood level will be okay. If you’re using a testosterone patch, the urinary levels, both in 24-hour urine and dry urinary levels, will reflect the increasing doses. You’re getting a reasonably good level with using that. Now, if you’re using DHEA treatment or oral DHEA, you’re going to get a rapid increase in the blood levels right after the oral supplementation as you get with the saliva. You get that also in saliva and also in urine. So you’re picking up on the fact that you took the DHEA test.
Conclusion
Dr. Alex Jimenez, D.C., presents: The problem is variability in the blood, saliva, and urine results. Many don’t particularly appreciate using a lot of oral DHEA anyway because, like all steroid hormones, your body’s going to take it to the liver, and the liver has the opportunity to change it into something else before it even gets into the bloodstream to do its job. Other applications may be more helpful, like transdermal DHEA or topical DHEA; you’ll have to see how the patient feels in terms of symptoms because if you use topical DHEA, the blood levels you’ll get a big rise right after the initial application.
Dr. Alex Jimenez, D.C., presents: So what does that mean because it drops right away? Then, in the saliva after transdermal application of DHEA, the levels will increase, but not linearly. So that doesn’t make any sense. And there is no peer-reviewed research detailing what happens in DHEA levels in the urine after transdermal application. The bigger issue then becomes you might want to keep an eye on what the downstream breakdown products are doing because if you’re not able to get a good DHEA level, you might want at least look at testosterone and estradiol. And that’ll give you some fuel if you’ve overdosed or underdosed on the DHEA. Now, with the vaginal or labial application, the levels in the blood don’t go off at all.
Dr. Alex Jimenez, D.C., presents: There’s no research detailing levels after vaginal application looking at salivary or urinary levels. So you can’t use that as a way of monitoring it. So again, this will be just a matter of following the person and how they feel after using it. You’re not going to need to worry about getting any measurements afterward. It’s simply clinical. The test you choose depends on what you’re giving the person, the form you’re giving it in, and then what you’re trying to find out. By finding a treatment form you like and feel comfortable with, understand whether or not to get testing depending on the structure and replacement you’re using. And then, make sure that you are getting helpful information and not misleading information.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine