Dr. Alex Jimenez, D.C., presents how hypertension affects the human body and some causes that can increase hypertension in many individuals in this 2-part series. We refer our patients to certified medical providers who provide multiple available treatments for many individuals suffering from hypertension associated with the cardiovascular and immune systems affecting the body. We encourage each of our patients by mentioning them to associated medical providers based on their analysis appropriately. We understand that education is a delightful way when asking our providers questions at the patient’s request and understanding. Dr. Jimenez, D.C., only makes use of this information as an educational service. Disclaimer
How To Look For Hypertension
Dr. Alex Jimenez, D.C., presents: Let’s go back to the decision tree so you can begin to think about how you will apply the go-to-it model in functional medicine to hypertension and how you will start better assessing somebody with hypertension rather than telling them that their blood pressure is elevated. Is the body influenced by inflammation, oxidative stress, or immune response? Is it affecting endothelial function or vascular smooth muscle from those three categories of reactions, inflammation, oxidative stress, or immune response? Do we choose a diuretic calcium channel blocker or an ACE inhibitor? And so to do that, it’s really important in our gather section. Taking the medical history and the timeline of their hypertension, you get a clue about the organ damage to the questionnaires. You’re looking at their anthropometrics.
This includes the following questions:
What are the inflammatory markers?
What are the biomarkers and clinical indicators?
Those are outlined through the clinical decision tree. And already just doing that, you’re going to expand and fine-tune your lens on what you might see in your hypertensive patient. Let’s add to the timeline when does hypertension begin? The timeframe of hypertension begins actually in prenatally. It’s important to ask your patient if they were early or large educational age. Was their mother stressed? Were they born early or premature? Was there nutritional stress in their pregnancy? If they know that, you can have two people with the same kidney size, but the person who didn’t have enough protein during pregnancy can have up to 40% less glomeruli. Knowing that will change how you adjust the medication decades later if you know they possibly have 40% less glomeruli.
The Timeline For Blood Pressure
Dr. Alex Jimenez, D.C., presents: So it’s important to take the timeline of their blood pressure. Then it’s also important to recognize what is happening when we begin to organize and collect data through the biomarkers; the basic biomarkers will give you clues about whether they have issues with insulin lipids, whether they have problems with vascular reactivity, autonomic nervous system balance, imbalance, coagulation, or immune toxin effects. So this is a reasonable thing to print off because, in your hypertensive patient, this is through just the biomarkers you can begin to get a clue as to what areas of dysfunction affect inflammation, oxidative stress, and immune response and how these biomarkers reflect that information for you. This is very reasonable to have in front of you to help change your thoughts about hypertension and also enables you to refine some of the characteristics of the person on the other side of your stethoscope in a more personalized, precise way.
But let’s start at the very beginning. Does your patient have high blood pressure? We know that depending on the end organ effects of their comorbidities, you may run someone a slightly higher blood pressure if you have a profusion issue in the brain and the kidneys or the heart, but some guidelines are there. Our 2017 American Heart Association guidelines for blood pressure categories are listed here. They’ve waxed and waned back and forth over the last couple of decades, but this is very clear. Having elevated blood pressure, anything above 120, really shifted how many people we start seeing or considering addressing the root causes of their blood pressure. So we will come back to this, especially in the case to help us look at how we categorize people with blood pressure issues.
The Criteria To Mesure Blood Pressure
Dr. Alex Jimenez, D.C., presents: What is the first step? It’s how do you have the blood pressure taken in your patient? Do they monitor it at home? Do they bring those numbers to you? How do you monitor blood pressure in your clinic? How do you get accurate readings in your clinic? Here are the criteria to accurately measure blood pressure and the questions to consider whether you’re doing all these.
Do you ask your patient whether they’ve had caffeine in the last hour?
Whether they’ve smoked in the previous hour?
Were they exposed to smoke in the last hour?
Is the place where you’re taking blood pressure warm and quiet?
Are they sitting with their back supported in a chair with their feet on the ground?
Do you use the roll-around side table to rest your arm at the heart level?
Are they sitting at the exam table with their feet dangling, and a nurse aide elevates their arm and puts in their axillary fold to hold their arm there?
Are their feet on the ground?
Have they sat there for five minutes?
Have they exercised in the previous 30 minutes?
You may have systolic blood pressure if everything is in the criteria. Here’s the challenge. There are 10 to 15 millimeters of mercury higher when it comes to sitting and taking blood pressure. What about the cuff size? We know last century; most adults had an upper arm circumference of fewer than 33 centimeters. Over 61% of people now have an upper arm circumference greater than 33 centimeters. So the size of the cuff is different for around 60% of your adult patients, depending on your population. So you have to use a large cuff. So take a look at how blood pressure is collected in your office. Let’s say the blood pressure is elevated in your patients; then we have to ask, is it normal? Great.
The Different Types Of Hypertension
Dr. Alex Jimenez, D.C., presents: Is it elevated because of white-coat hypertension? Do they have normal blood pressure, elevated outside the clinic, or masked hypertension? Or do they just have sustained hypertension which is a challenge? We’ll talk about that. So when you interpret, it is also important to consider ambulatory blood pressure monitoring. So if you have somebody who’s hypertensive and don’t know whether the blood pressure goes down and you’re trying to figure out whether they have sustained hypertension, you can use 24-hour blood pressure monitoring. The mean daytime blood pressure above 130 over 80 is hypertensive the mean nighttime blood pressure above 110 over 65 is hypertensive. So why is this important? The average blood pressure dips to around 15% at night because of the issue with blood pressure dipping. Failure to have blood pressure drop while you sleep at night could develop problems that can affect a person throughout the day.
If your patient sleeps at night, it should drop about 15% when they sleep. If they have non-dipping blood pressure, it is associated with comorbidities. What are some of those comorbidities in non-dipping blood pressure? Some of the conditions correlated with non-dipping blood pressure include:
Congestive Heart Disease
Cardiovascular Disease
Cerebrovascular Disease
Congestive Heart Failure
Chronic Renal Failure
Silent Cerebral Infractions
Co-morbidities Associated With Non-Blood Pressure
Dr. Alex Jimenez, D.C., presents: These are the comorbidities associated with non-blood pressure. All of us agree that elevated blood pressure is not necessarily good in all those conditions. So when you look at different people groups or other comorbidities, non-dipping blood pressure is most commonly associated with sodium-sensitive folks, people who have renal insufficiency, people who have diabetes, people who have left ventricular hypertrophy, people who have refractory hypertension or autonomic nervous system dysfunction and finally, sleep apnea. So, non-dipping blood pressure increases your association with subclinical cardiac damage. Okay, Reverse dipping means you are more hypertensive at night and is more ascent associated than during the day is more related to hemorrhagic stroke. And if you have somebody with nocturnal hypertension, you have to start thinking about things like the carotid arteries and increased carotid, internal medial thickness. You start thinking about left ventricular hypertrophy and may see it on EKG. Here’s what we know about nocturnal hypertension. Nocturnal hypertension is a nighttime blood pressure greater than 120 over 70. It is associated with greater predictability of cardiovascular morbidity and mortality.
If you have nocturnal hypertension, it increases your risk of mortality from cardiovascular disease by 29 to 38%. We must know what’s happening at night when we sleep, right? Well, what’s another refinement? Another refinement is recognizing that resting blood pressure is controlled by your renin-angiotensin system. Waking blood pressure is controlled by your sympathetic nervous system. So let’s talk about how their renal angiotensin system drives their nighttime hypertension, and you think about what medication they’re taking. You might change the medication dosing to nighttime. Well, studies have shown that if you have nighttime hypertension and are a non-dipper, it’s best to take your ACE inhibitors, ARBs, calcium channel blockers, and certain beta blockers at night before bed. But it makes sense that you wouldn’t move your diuretics to nighttime, or you will have a disruptive sleep.
Addressing Daytime & Nighttime Blood Pressure
Dr. Alex Jimenez, D.C., presents: So if we don’t address daytime and nighttime blood pressure, we have to consider the effect of blood pressure load. What is your average daytime blood pressure and your moderate sleeping blood pressure is. We know that blood pressure load in young adults is hypertensive only about 9% of the time. So meaning the systolic load is about 9% versus in the elderly, about 80% of the blood pressure load is systolic. And so when you have a higher systolic load, you have more complications and end-organ damage. So what we’re talking about is helping identify your patient with hypertension; what is their timeline? What is their phenotype? Are they only hypertensive during the day, or they’re hypertensive at night also? We have to look at what helps balance that.
Here’s the other point, only about 3.5% of people with hypertension do it have a genetic cause. Only 3.5% of people their genes cause hypertension. The power is at the bottom of the matrix and recognizing these patterns, right? So you look at exercise, sleep, diet, stress, and relationships. So we know that these four autonomic balances help determine blood pressure. We will examine the renal angiotensin system, plasma volume where they hold onto too much fluid, secondary salt load, and endothelial dysfunction. Abnormalities in any of these can lead to hypertension. We’ve been talking about another one that can lead to hypertension: the link between insulin resistance and hypertension.
This diagrammatically gives you an idea of the physiologic interactions between insulin resistance and hypertension. It affects increasing sympathetic tone and increasing renal-angiotensin system balance. So let’s spend a few minutes on the renin-angiotensin system pathway angiotensinogen down to angiotensin two. We take advantage of these enzymes by giving inhibitors to angiotensin-converting enzymes in our hypertensives patients. Elevated angiotensin two leads to cardiovascular hypertrophy, leads to sympathetic phase constriction, increased blood volume, sodium fluid, retention, and aldosterone release. Can you inquire about your patient biomarkers? Can you ask whether they have elevated renin levels?
Look For The Signs
Dr. Alex Jimenez, D.C., presents: Well, you can. You can check plasma renin activity and aldosterone levels. It’s important to do this if your patient is hypertensive and has never been on medication because this is where nitrous oxide is so important. This is where your endothelial nitric oxide synthase is present. This is where you have sheer and hemodynamic stress. This is where dietary intake of arginine or the environment that affects nitric oxide plays such a role in the health of this layer of endothelia. If you lay it all together somehow, miraculously, or at least in your mind’s eye, it’ll cover six tennis courts in the average adult. It’s a huge surface area. And the things that cause endothelial dysfunction are not new news to people in functional medicine. Increased oxidative stress and inflammation are two things we mentioned that play an effect.
And then, look at some of these other components, your ADMA being elevated and correlated with insulin resistance. It all begins to form together in a matrix that interacts. So you look at one comorbidity in cardiometabolic syndrome, and it affects another comorbidity. You suddenly see the interrelation between them or hyperhomocysteinemia, which is a one-carbon metabolism marker, meaning you’re looking at the adequacy of folate, b12, b6, riboflavin, and that activity of your one-carbon metabolism. So let’s look at some of these emerging risk markers to improve and track in patients with hypertension. Let’s reanalyze ADMA again. ADMA stands for asymmetric dimethyl arginine. Asymmetric, dimethyl arginine is a biomarker of endothelial dysfunction. That molecule inhibits nitric oxide synthase while impairing endothelial function, and in all of the comorbidities associated with cardiometabolic syndrome, ADMA can be elevated.
Conclusion
So, as a quick review, L-arginine is converted to nitric oxide via nitric oxide synthase, and nitric oxide adequacy leads to vasodilation. ADMA blocks this conversion. And if your ADMA levels are elevated and your nitric oxide levels are low, then you have decreased nitric oxide platelet aggregation increases in LDL oxidation. So many things reduce nitric oxide or are associated with lower nitric oxide levels, sleep apnea, low dietary arginine, protein, zinc insufficiency, and smoking.
Everybody deals with stress at some point in their lives. Whether it be a job interview, a huge deadline, a project, or even a test, stress is there to keep the body functioning in each scenario that the body is going through. Stress can help regulate the body’s immune system and help metabolize homeostasis as the body increases its energy throughout the day. When dealing with chronic stress can cause metabolic dysfunction in the body like gut disorders, inflammation, and an increase in blood glucose levels. Chronic stress can also affect a person’s mood and health, eating habits, and sleep quality. Today’s article will look at if stress is a good thing or a bad thing, how it affects the body, and the effects of what chronic stress does to the body. Refer patients to certified, skilled providers specializing in gut treatments for individuals that suffer from autonomic neuropathy. We guide our patients by referring to our associated medical providers based on their examination when it’s appropriate. We find that education is critical for asking insightful questions to our providers. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
Can my insurance cover it? Yes, it may. If you are uncertain, here is the link to all the insurance providers we cover. If you have any questions or concerns, please call Dr. Jimenez at 915-850-0900
Is Having Stress Good Or Bad?
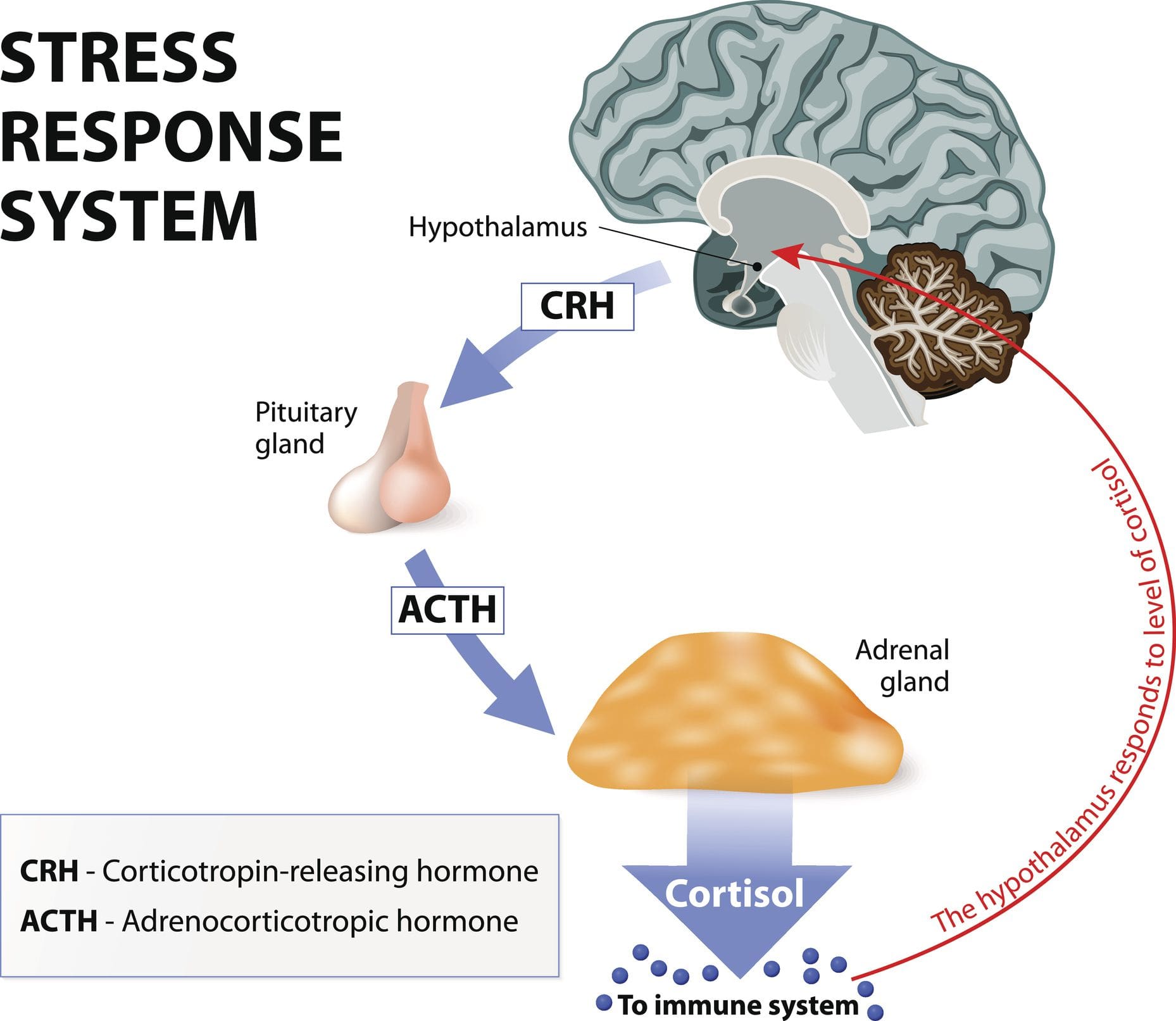
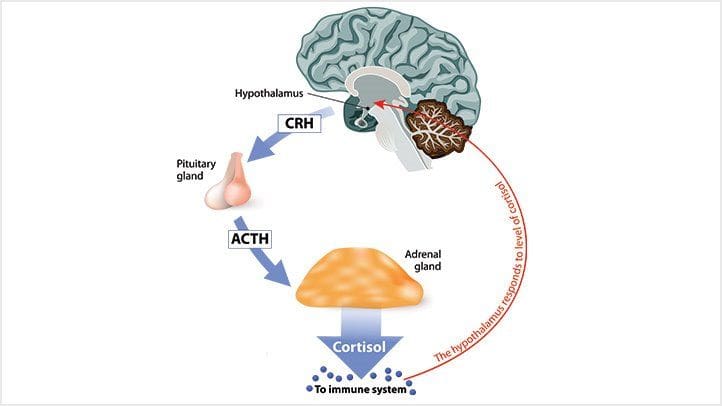
Do you feel anxious all the time? How about feeling headaches that are constantly being a nuisance? Feeling overwhelmed and losing focus or motivation? All these signs are stressful situations that a person is going through. Research studies have defined stress or cortisol as the body’s hormone that provides a variety of effects on different functions in each system. Cortisol is the primary glucocorticoid that is from the adrenal cortex. At the same time, the HPA (hypothalamus-pituitary-adrenal) axis helps regulates the production and secretion of this hormone to the rest of the body. Now cortisol can be beneficial and harmful to the body, depending on the situation a person is in. Additional research studies have mentioned that cortisol begins and affects the brain and the rest of the body as stress in its acute form can cause the body to adapt and survive. The acute responses from cortisol allow neural, cardiovascular, immune, and metabolic function in the body.
How Does It Affect The Body’s Metabolism?
Now cortisol affects the body’s metabolism when controlled in a slow, steady sleep cycle that decreases corticotropin‐releasing hormone (CRH) and increases growth hormone (GH). Research studies have shown that when the adrenal glands secrete cortisol, it starts to have a complex interaction with the hypothalamus and pituitary glands in the nervous and endocrine systems. This causes the adrenal and thyroid function in the body to be closely linked while under the control of the hypothalamus and tropic hormones. The thyroid competes with the adrenal organs for tyrosine. Research studies have found that tyrosine is used to produce cortisol under stress while preventing cognitive function decline that is responsive to physical stress. However, when the body can not produce enough tyrosine, it can cause hypothyroidism and cause the cortisol hormone to become chronic.
An Overview About Stress-Video
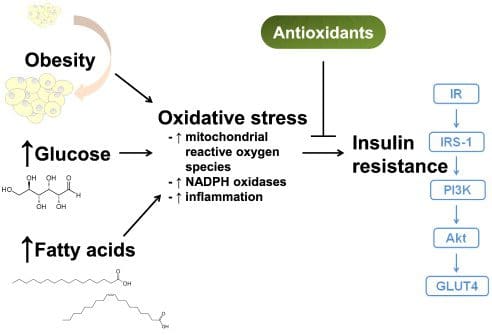
Have you experienced headaches that randomly show up out of nowhere? Have you constantly gained weight or lost weight? Do you feel anxious or stressed out always that it is affecting your sleep? These are all signs and symptoms of your cortisol levels turning into their chronic state. The video above shows what stress does to your body and how it can cause unwanted symptoms. When there is chronic stress in the body, the HPA axis (neuro‐endocrine) is imbalanced due to the stress‐mediated activators involved in autoimmune thyroid diseases (AITD). When there is chronic stress in the body, it can cause excessive production of inflammatory compounds in the body can generate IR. The inflammatory substances can damage or inactivate insulin receptors leading to insulin resistance. This then contributes to the breakdown of one or more factors needed to complete the glucose transport process in the body.
The Effects Of Chronic Cortisol In The Body
When there is chronic stress in the body and has not been treated or reduced right away, it can lead to something known as allostatic load. Allostatic load is defined as wear and tear of the body and brain due to chronic overactivity or inactivity of the body systems typically involved in environmental challenges and adaptation. Research studies have shown that allostatic load causes excess secretion of hormones like cortisol and catecholamine to respond to chronic stressors affecting the body. This causes the HPA axis to do one of two things: being overworked or failing to shut off after stressful events causing sleep disturbances. Other issues that chronic stress does to the body can include:
Increased insulin secretion and fat deposition
Altered immune function
Hypothyroidism (adrenal exhaustion)
Sodium and water retention
Loss of REM sleep
Mental and Emotional instability
Increase in cardiovascular risk factors
These symptoms cause the body to become dysfunctional, and research studies have pointed out that various stressors can damage the body. This can make it extremely difficult for a person to cope with stress and alleviate it.
Conclusion
Overall, stress or cortisol is a hormone the body needs to function correctly. Chronic stress in the body from various stressors can cause many metabolic dysfunctions like hypothyroidism, weight gain, insulin resistance, and metabolic syndrome, to name a few. Chronic stress can also cause sleep disorders since the HPA axis is wired up and can seem to calm down the slightest. When people start to find ways of dealing with these various stressors, they can reduce their stress levels back to normal and be stress-free.
References
Jones, Carol, and Christopher Gwenin. “Cortisol Level Dysregulation and Its Prevalence-Is It Nature’s Alarm Clock?” Physiological Reports, John Wiley and Sons Inc., Jan. 2021, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7749606/.
McEwen, Bruce S. “Central Effects of Stress Hormones in Health and Disease: Understanding the Protective and Damaging Effects of Stress and Stress Mediators.” European Journal of Pharmacology, U.S. National Library of Medicine, 7 Apr. 2008, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2474765/.
McEwen, Bruce S. “Stressed or Stressed out: What Is the Difference?” Journal of Psychiatry & Neuroscience : JPN, U.S. National Library of Medicine, Sept. 2005, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1197275/.
Rodriquez, Erik J, et al. “Allostatic Load: Importance, Markers, and Score Determination in Minority and Disparity Populations.” Journal of Urban Health : Bulletin of the New York Academy of Medicine, Springer US, Mar. 2019, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6430278/.
Young, Simon N. “L-Tyrosine to Alleviate the Effects of Stress?” Journal of Psychiatry & Neuroscience : JPN, U.S. National Library of Medicine, May 2007, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1863555/.
As the world is in constant motion, many people have to endure stressful situations affecting their bodies and health. The body needs hormones like cortisol to keep functioning as it affects the immune, nervous, cardiovascular, and musculoskeletal systems, to name a few. Another essential function the body needs is glucose, which requires energy to be in constant motion. Situations that cause the cortisol levels and glucose levels to rise in the body can lead to chronic issues like diabetes and chronic stress. This causes the individual to be miserable and be in a serious situation if it is not controlled right away. Today’s article examines how cortisol and glucose affect the body and the interwoven connection between stress and diabetes. Refer patients to certified, skilled providers specializing in stress management and endocrine treatments for diabetic individuals. We guide our patients by referring to our associated medical providers based on their examination when it’s appropriate. We find that education is critical for asking insightful questions to our providers. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
Can my insurance cover it? Yes, it may. If you are uncertain, here is the link to all the insurance providers we cover. If you have any questions or concerns, please call Dr. Jimenez at 915-850-0900.
How Does Cortisol Affect The Body?
Have you been experiencing sleeping problems at night? What about frequent headaches that are a nuisance throughout the entire day? Or have you noticed excessive weight loss or weight gain around your midsection? Some of these symptoms are signs that your cortisol and glucose levels are high and can affect your body. Cortisol is a hormone produced in the endocrine system and can be beneficial or harmful to the body if it is not regularly checked. Research studies have defined cortisol as one of the prominent glucocorticoids secreted out due to the response of the body’s biochemicals, characterized by the HPA (hypothalamic‐pituitary‐adrenal) axis helps cognitive events. However, when the cortisol levels turn chronic in the body due to circumstances that cause the body to become dysfunctional, it can significantly impact a person and cause an imbalance in the HPA axis. Some of the symptoms that chronic cortisol leads to the body can include:
Hormonal imbalances
Insulin resistance
Weight gain
Increases in visceral “belly” fat
Increased cortisol output
Immune problems
Allergies and Asthma
Inflamed Joints
Poor exercise recovery
Additional information has provided that the presence of cortisol in the body can help increase blood glucose availability to the brain. With cortisol providing organ functionality, the blood glucose provides energy for the body.
How Cortisol & Glucose Work In The Body
Cortisol helps stimulate mass glucose mobilization in the liver, allowing block protein synthesis to push amino acids into sugar for the body. This is known as fatty acid liberation biotransformed into glucose. When this happens, it helps stimulate visceral fat storage if excess glucose is not utilized, thus causing weight gain. Research studies have shown that a lack of cortisol can cause a decrease in hepatic glucose production in the body. This will cause hypoglycemia, where the body doesn’t have enough glucose in its system. Additional research shows that cortisol responds to any stressor that affects a person with low glucose levels but can also become positive after a glucose load. Managing the body’s glucose and cortisol levels can help progress the development of diabetes.
How Cortisol Is Linked With Type 2 Diabetes- Video
Have you experienced stressful situations that cause your muscles to tense up? How about feeling your blood sugar either spiking up or down? Do you feel inflammatory effects all over your body that makes them ache? Stress can cause harmful effects to the body, activating inflammation, increasing sympathetic tone, and reducing glucocorticoid responsiveness. Stress can also be linked to diabetes, as the video above shows how the stress hormone cortisol is linked with type 2 diabetes. Research studies have mentioned that cortisol can become negatively associated with the mechanics of insulin resistance, increasing the beta-cell function and increasing the insulin released in the body. This can become dangerous for many individuals that have pre-existing diabetes and have been dealing with stress constantly.
The Interwoven Connection Between Stress & Diabetes
The interwoven connection between stress and diabetes is shown as research studies have found that the pathophysiology of anxiety and diabetes has increased insulin resistance risk for the body. When a person is dealing with chronic stress, it can cause them to have many issues like:
Cold intolerance
Diminished cognition and mood
Food sensitivities
Low energy throughout the day
When this happens, the body is at a high risk of developing insulin resistance and type 2 diabetes. Research studies have mentioned that type 2 diabetes is characterized by insulin resistance and beta-cell dysfunction. The glucocorticoid in the body can become excessive to affect the cells, causing dysfunctionality. Additional research studies have shown that any perceived stress can become a vital risk factor that not only affects the body, like hypertension, BMI (body mass index), or diet quality but can cause a rise in type 2 diabetes. When individuals find ways to lower their chronic stress, it can help manage their glucose levels from reaching critical levels.
Conclusion
The body’s chronic stress can cause insulin resistance and cause diabetes to become pre-existing. The body needs cortisol and glucose to keep functioning and have the energy to move. When people start to suffer from chronic stress and diabetes, it can become challenging to manage; however, making minor changes to the body like finding ways to lower stress, eating healthy foods, and monitoring glucose levels can help the body reset the glucose and cortisol levels to normal. Doing this can relieve many individuals who want to continue their health journey being stress-free.
References
Adam, Tanja C, et al. “Cortisol Is Negatively Associated with Insulin Sensitivity in Overweight Latino Youth.” The Journal of Clinical Endocrinology and Metabolism, The Endocrine Society, Oct. 2010, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3050109/.
De Feo, P, et al. “Contribution of Cortisol to Glucose Counterregulation in Humans.” The American Journal of Physiology, U.S. National Library of Medicine, July 1989, https://pubmed.ncbi.nlm.nih.gov/2665516/.
Hucklebridge, F H, et al. “The Awakening Cortisol Response and Blood Glucose Levels.” Life Sciences, U.S. National Library of Medicine, 1999, https://pubmed.ncbi.nlm.nih.gov/10201642/.
Joseph, Joshua J, and Sherita H Golden. “Cortisol Dysregulation: The Bidirectional Link between Stress, Depression, and Type 2 Diabetes Mellitus.” Annals of the New York Academy of Sciences, U.S. National Library of Medicine, Mar. 2017, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5334212/.
Kamba, Aya, et al. “Association between Higher Serum Cortisol Levels and Decreased Insulin Secretion in a General Population.” PloS One, Public Library of Science, 18 Nov. 2016, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5115704/.
Lee, Do Yup, et al. “Technical and Clinical Aspects of Cortisol as a Biochemical Marker of Chronic Stress.” BMB Reports, Korean Society for Biochemistry and Molecular Biology, Apr. 2015, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4436856/.
Thau, Lauren, et al. “Physiology, Cortisol.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 6 Sept. 2021, https://www.ncbi.nlm.nih.gov/books/NBK538239.
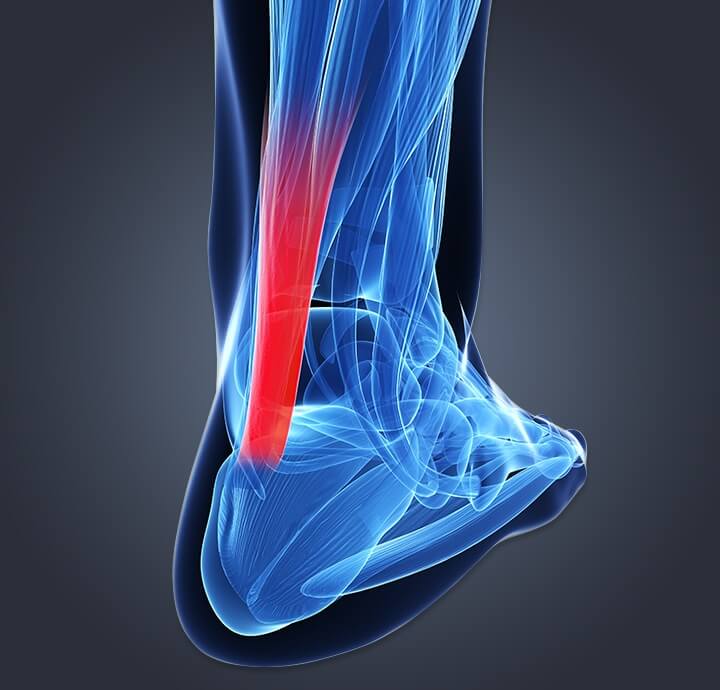
The body is a well-working machine that can endure anything that is thrown in its way. However, when it gets an injury, the body’s natural healing process will ensure that the body can get back to its daily activities. The healing process of an injured muscle varies throughout the body. Depending on how severe the damage is and how long the healing process will take, the body can recover to a mere few days to a few months. One of the most gruelly healing processes that the body has to endure is a ruptured calcaneal tendon.
The Calcaneal Tendon
The calcaneal tendon or the Achilles tendon is a thick tendon that is located in the back of the leg. This muscle-tendon is what makes the body move while walking, running, or even jumping. Not only that, the calcaneal tendon is the strongest tendon in the body, and it connects the gastrocnemius and soleus muscles at the heel bone. When the calcaneal tendon is ruptured, the healing process can last from weeks to months until it is fully healed.
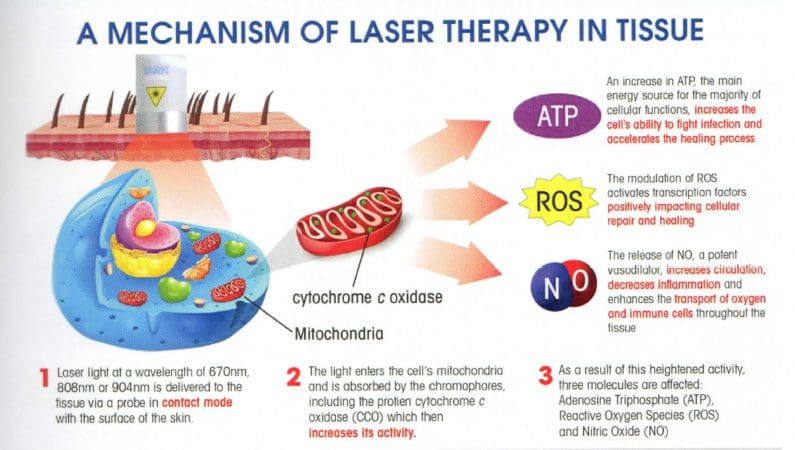
The Healing Effects of Low Laser Therapy
One of the ways that can help the damaged calcaneal tendons’ healing process is low laser therapy. Studies have shown that low laser therapy can speed up the damaged tendon repair after a partial lesion. Not only that but the combination of ultrasound and low laser therapy has been studied to be the physical agents for treating tendon injuries. The studies showed that the combination of low laser therapy and ultrasound has beneficial properties during the recovery process of treating calcaneal tendon injuries.
The study found that when patients are being treated for their calcaneal tendons, their hydroxyproline levels around the treated area are significantly increased with ultrasound and low laser therapy. The body’s natural biochemical and biomechanical structures on the injured tendon increase, thus affecting the healing process. Another study has shown that low laser therapy can help reduce fibrosis and prevent oxidative stress in the traumatized calcaneal tendon. The study even showed that after the calcaneal tendon is traumatized, inflammation, angiogenesis, vasodilation, and the extracellular matrix are formed in the affected area. So when patients are being treated with low laser therapy for about fourteen to twenty-one days, their histological abnormalities are alleviated, reducing collagen concentration and fibrosis; preventing oxidative stress from increasing in the body.
Conclusion
Overall, it is said that the effects of low laser therapy can help speed up the healing process of repairing the calcaneal tendon. The promising results have been proven since low laser therapy can help repair the damaged tendon, reducing oxidative stress and preventing fibrosis from escalating, causing more problems on the injured tendon. And with the combination of ultrasound, the calcaneal tendon can recover faster so the body can continue its everyday activities without any prolonged injuries.
References:
Demir, Huseyin, et al. “Comparison of the Effects of Laser, Ultrasound, and Combined Laser + Ultrasound Treatments in Experimental Tendon Healing.” Lasers in Surgery and Medicine, U.S. National Library of Medicine, 2004, https://pubmed.ncbi.nlm.nih.gov/15278933/.
Fillipin, Lidiane Isabel, et al. “Low-Level Laser Therapy (LLLT) Prevents Oxidative Stress and Reduces Fibrosis in Rat Traumatized Achilles Tendon.” Lasers in Surgery and Medicine, U.S. National Library of Medicine, Oct. 2005, https://pubmed.ncbi.nlm.nih.gov/16196040/.
Oliveira, Fla’via Schlittler, et al. Effect of Low Level Laser Therapy (830 Nm … – Medical Laser. 2009, http://medical.summuslaser.com/data/files/86/1585171501_uLg8u2FrJP7ZHcA.pdf.
Wood, Viviane T, et al. “Collagen Changes and Realignment Induced by Low-Level Laser Therapy and Low-Intensity Ultrasound in the Calcaneal Tendon.” Lasers in Surgery and Medicine, U.S. National Library of Medicine, 2010, https://pubmed.ncbi.nlm.nih.gov/20662033/.
Waking up tired even after getting six or more hours of sleep?
Under a high amount of stress?
If you are experiencing any of these situations, then it might be due to your melatonin and cortisol levels affecting your body and circadian rhythm.
Across the world, millions of people have trouble sleeping. In the United States, there are roughly about 50-70 million people who have a poor quality of sleep. When a person has slept for less than eight hours, they become tired, and many problems can come to them, especially if their lives are hectic. With a hectic lifestyle and poor sleep, it can cause the body to have low energy to get any task done, the cortisol stress hormone will be raised, and diseases like high blood pressure and diabetes can cause problems that can be chronic if it is not treated.
In functional endocrinology, melatonin and cortisol are hormones that the body produces naturally. The cortisol hormone or the stress hormone helps the body be in a state of “fight or flight” mode, which can be a good thing for anyone who is doing a project or going for a job interview. Although when cortisol hormone levels are high, it can lead the body to have complications like inflammation, chronic oxidative stress, and high blood pressure.
The Melatonin Circadian Rhythm
With the melatonin hormone, this hormone tells the body when it is time to sleep. Sometimes though, people do have a hard time sleeping, and taking melatonin supplements can actually relax the body and thus making the person fall asleep. Since the pineal gland produces melatonin from the brain, it can also be found in the eyes, the bone marrow, and the gut to relax the body and making the person fall asleep naturally. Some studies show that the circadian rhythm of the pineal gland that is producing melatonin. By doing this, the research shows that the administration of melatonin can:
One: induce sleep on individuals who have trouble falling asleep.
Two: inhibits the body to wake up naturally from the circadian pacemaker.
Three: shift the circadian biological clocks to increase sleep intake when a person is trying to sleep at an earlier time to get the full eight-hour benefits of sleep.
When a person is working at a 9 to 5 job, they are rising with their bodies and relaxing their bodies after a hard day at work. Studies found out that the melatonin and cortisol hormones help regulate the 24-hour pattern of the body’s function and responses tremendously. With the body’s hormone production cycle, it can be disturbed if the person is staying awake late at night or sleeping during the day. When this happens, the person can get disruptive disorders like mood swings, dizziness, be irritable and depressed, and have metabolic disorders. Not only that, but the body’s immune system and its endocrine system can also be damaged as well, causing the body to be a host to infections and diseases.
There have been more studies on the circadian rhythms in the body, as the studies show how people who work in the night shift have been associated with a vast number of adverse health problems that attack the cardiovascular and gastrointestinal system as well as disturbing the metabolic system. Anyone who has worked the night shift has to change their sleep schedule and adapt to the rapid reorientation in their sleep/wake schedule to go to work and do their job. Since everyone is working at a shift schedule, it can be stressful and can affect a worker’s body performance as well as affecting melatonin and cortisol secretion.
Ways To Support Cortisol and Melatonin
Surprisingly though, there are ways to lower cortisol levels and make sure that melatonin levels are working correctly for the body to function. For cortisol levels to be lowered, a person should do meditative practices, find an enjoyable hobby, and, most importantly, try deep breathing exercises to relax the body from unwanted stress. With deep breathing exercises, it can help the body to release any tension that a person is holding, and the muscles in the body began to relax, and the blood starts to flow. With the melatonin levels, they work together with the body’s circadian rhythm and make sure the body knows when it is time to wake up, sleep and eat. The melatonin hormone can also help regulate the body’s temperature, blood pressure, and hormone levels to make sure it is functioning correctly. When there are high levels of these systems, it can cause the body to develop chronic illnesses and harm the body in the process.
Research shows that melatonin hormones can bind to neurological receptors in the body, thus promoting relaxation. Since melatonin binds to neurological receptors, it can also reduce nerve activity and dopamine levels to make the eyes heavy, thus making the person fall asleep.
Conclusion
With the body being able to naturally produce melatonin and cortisol levels to make sure that the body does not get overly stressed throughout the entire day. Since melatonin is partnered with the body’s circadian rhythm, the body knows when to stay up and fall asleep. Since everyone has a hectic schedule, it is essential to take time and relax and get on a healthy sleep schedule so the body can be healthy and functioning. Some products are here to make sure that the endocrine system is functioning properly and supporting the adrenal glands and sugar metabolism.
The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
References:
Cajochen, C, et al. �Role of Melatonin in the Regulation of Human Circadian Rhythms and Sleep.� Journal of Neuroendocrinology, U.S. National Library of Medicine, Apr. 2003, www.ncbi.nlm.nih.gov/pubmed/12622846.
James, Francine O, et al. �Circadian Rhythms of Melatonin, Cortisol, and Clock Gene Expression during Simulated Night Shift Work.� Sleep, Associated Professional Sleep Societies, LLC, Nov. 2007, www.ncbi.nlm.nih.gov/pmc/articles/PMC2082093/.
Monteleone, P, et al. �Temporal Relationship between Melatonin and Cortisol Responses to Nighttime Physical Stress in Humans.� Psychoneuroendocrinology, U.S. National Library of Medicine, 1992, www.ncbi.nlm.nih.gov/pubmed/1609019.
Raman, Ryan. �How Melatonin Can Help You Sleep and Feel Better.� Healthline, Healthline Media, 3 Sept. 2017, www.healthline.com/nutrition/melatonin-and-sleep.
Zamanian, Zahra, et al. �Outline of Changes in Cortisol and Melatonin Circadian Rhythms in the Security Guards of Shiraz University of Medical Sciences.� International Journal of Preventive Medicine, Medknow Publications & Media Pvt Ltd, July 2013, www.ncbi.nlm.nih.gov/pmc/articles/PMC3775223/.
By informing individuals about how the National University of Health Sciences provides knowledge for future generations who want to make a difference in the world. The University offers a wide variety of medical professions for functional and integrative medicine.
Ever wondered why you feel sluggish from a long day? Or feel sick to the stomach when you ate something bad or overindulged on your favorite food? Could it be that your gut is showing signs of stress and discomfort due to certain habits that you may encounter and didn�t even know about it?
In our previous article, we talked about the six types of food that our gut needs to be healthy. Since our gut contains trillions of microbiomes, both good and bad, these microbiomes play an important role in our overall health. A healthy microbiome improves our gut health, heart health, brain health, controls our weight and regulates our blood sugar. With the good bacteria in our gut, the bacteria benefit us with a good digestive system and destroys the harmful bacteria. But certain lifestyles and diet choices can actually increase the bad bacteria and lower the good bacteria and overall health.
Here are five surprisingly lifestyle choices that are hurting your gut:
Not Eating a Wide Range of Foods
Our gut plays an important role in our overall health. When we eat good whole foods, our gut is happier; we have more energy to complete any task that is thrown at us and we are getting nutrients for our gut flora. However, during the past couple of decades, we have been leaning more into processed foods due to the economic pressures of increased food productions. FOA stated that �75 percent of the world�s food is generated from only 12 plants and five animal species� and that is very bad to our gut flora.
Here at Injury Medical & Chiropractic Clinic, we inform our patients about the importance of eating nutritious, whole foods to promote not only a healthy gut but a healthy mind. When the body gets introduced to a wide variety of whole foods (with a high fiber content), our gut starts to repair the damage of processed food that we may have consumed internally.
However, when you disregard prebiotics to your diet, you are harming your digestive health. Without prebiotics, our digestive system slows down the development and diversity for our gut flora. So in order to have a healthy microbiome development, you need to incorporate foods filled with both digestible and indigestible fibers to your diet. Some foods included in this category are oats, nuts, onions, garlic, leeks, asparagus, bananas, pears, chickpeas, and beans.
Sticking to a high fiber diet maybe challenging however, there is the option of taking prebiotic supplements. If you have a food allergen or food sensitivity to any high enriched fiber foods, taking prebiotic supplements can actually help grow Bifidobacterium and Faecalibacterium in your gut and be beneficial to your health without the discomfort.
Excessive Alcohol Consumption
Every adult enjoys alcohol once in a while. Yes, it�s one of those beverages that help you relax a bit after a long day, however, too much of it can lead to alcohol abuse and addiction. So, did you know that consuming that much alcohol is bad for your heart, liver, and brain; thus hurting your gut health and giving you dysbiosis?
One study stated, that the alcoholics with dysbiosis had a lower median abundance of Bacteroidetes and a high abundance of Proteobacteria. The ones that weren�t alcoholics were not affected by the study.
However; there is some good news on limiting yourself to alcoholism and that it can be beneficial to your gut bacteria. If you moderately consumed red wine responsibly, the polyphenols in the wine can help benefit your gut flora. So, enjoy a glass of wine once in a while as a small treat that should not be taken for granted.
Inadequate Sleep
In one of the previous articles, we talked about how to achieve a good night sleep through herbs. When we get little to no sleep through our hectic lives, it affects us through various health problems, including heart disease and obesity. In a 2016 study, researchers discovered the effect of short-term sleep deprivation on the gut microbiota after two days.
When our body doesn�t receive the recommended 8 hours of sleep, our gut takes a huge toll as we feel sluggish and exhausted. So, to make sure that our gut microbiome will be taken care of, we recommended to turn off your electronical devices at least 30 minutes before you get ready to settle down for the night. Turn off all the lights, and don�t drink any liquids at least two hours before bed, close your eyes and take a deep breath in a meditative state, and relax as you drift off into slumber town.
Inadequate Exercise
Through our fast-paced lifestyle and stressful jobs, it�s hard to find time to exercise. But when we actually do find time to exercise, not only do our minds feel good; but our body and gut feel good as well. However, things always come up when we are in an exercise routine and we have to skip exercising altogether. It happens to all of us and it�s hard to pick up where we left off when we tried to exercise.
When we don�t exercise at least a couple of times out of the week, our bodies take a huge toll on us as we gained weight, our stress is way too high, and we have a higher chance of getting a chronic disease. When this happens our gut flora is a huge disadvantage. Here at the clinic, we strive to inform our patients about the importance of exercising and that it not only changes their lives but also changes their mood entirely.
However, don�t just go into a hard exercise routine where you will injure yourself. Start off with a low-intensity workout then build it up as you go because your gut flora will thank you for it.
As a final say, we here at Injury Medical want to keep you informed on nutrition and ways to help you improve your ailments with these 5 surprises. But to also educate you on what may be hurting your gut. With these surprises and slight changes to your daily life, your gut will be thanking you for the long haul.
NCBI Resources
According to evidence from a 2016 research study, the gut�s immune system is fundamental towards preventing a variety of diseases and it may often contribute to metabolic disorders. However, it might also help provide a treatment goal when observing systemic inflammation in insulin resistance. Moreover, modified gut immunity has been linked with changes to the gut microbiota, intestinal barrier function, gut-residing immune cells, and resistance to antigens which enter the gastrointestinal, or GI, system. Although this has been previously believed to raise the danger of esophageal ailments including, pathogenic infections and chronic inflammation, which may ultimately lead to chronic health issues.
Ketone bodies are created by the liver and utilized as an energy source when glucose is not readily available in the human body. The two main ketone bodies are acetoacetate (AcAc) and 3-beta-hydroxybutyrate (3HB), while acetone is the third and least abundant, ketone body. Ketones are always present in the blood and their levels increase during fasting and prolonged exercise.�Ketogenesis is the biochemical process by which organisms produce ketone bodies through the breakdown of fatty acids and ketogenic amino acids.
Ketone bodies are mainly generated in the mitochondria of liver cells. Ketogenesis occurs when there are low glucose levels in the blood, particularly after other cellular carbohydrate stores, such as glycogen, have been exhausted. This mechanism can also occur when there is insufficient amounts of insulin. The production of ketone bodies is ultimately initiated to make available energy which is stored in the human body as fatty acids. Ketogenesis occurs in the mitochondria where it is independently regulated.
Abstract
Ketone body metabolism is a central node in physiological homeostasis. In this review, we discuss how ketones serve discrete fine-tuning metabolic roles that optimize organ and organism performance in varying nutrient remains and protect from inflammation and injury in multiple organ systems. Traditionally viewed as metabolic substrates enlisted only in carbohydrate restriction, recent observations underscore the importance of ketone bodies as vital metabolic and signaling mediators when carbohydrates are abundant. Complementing a repertoire of known therapeutic options for diseases of the nervous system, prospective roles for ketone bodies in cancer have arisen, as have intriguing protective roles in heart and liver, opening therapeutic options in obesity-related and cardiovascular disease. Controversies in ketone metabolism and signaling are discussed to reconcile classical dogma with contemporary observations.
Introduction
Ketone bodies are a vital alternative metabolic fuel source for all the domains of life, eukarya, bacteria, and archaea (Aneja et al., 2002; Cahill GF Jr, 2006; Krishnakumar et al., 2008). Ketone body metabolism in humans has been leveraged to fuel the brain during episodic periods of nutrient deprivation. Ketone bodies are interwoven with crucial mammalian metabolic pathways such as ?-oxidation (FAO), the tricarboxylic acid cycle (TCA), gluconeogenesis, de novo lipogenesis (DNL), and biosynthesis of sterols. In mammals, ketone bodies are produced predominantly in the liver from FAO-derived acetyl-CoA, and they are transported to extrahepatic tissues for terminal oxidation. This physiology provides an alternative fuel that is augmented by relatively brief periods of fasting, which increases fatty acid availability and diminishes carbohydrate availability (Cahill GF Jr, 2006; McGarry and Foster, 1980; Robinson and Williamson, 1980). Ketone body oxidation becomes a significant contributor to overall energy mammalian metabolism within extrahepatic tissues in a myriad of physiological states, including fasting, starvation, the neonatal period, post-exercise, pregnancy, and adherence to low carbohydrate diets. Circulating total ketone body concentrations in healthy adult humans normally exhibit circadian oscillations between approximately 100�250 �M, rise to ~1 mM after prolonged exercise or 24h of fasting, and can accumulate to as high as 20 mM in pathological states like diabetic ketoacidosis (Cahill GF Jr, 2006; Johnson et al., 1969b; Koeslag et al., 1980; Robinson and Williamson, 1980; Wildenhoff et al., 1974). The human liver produces up to 300 g of ketone bodies per day (Balasse and Fery, 1989), which contribute between 5�20% of total energy expenditure in fed, fasted, and starved states (Balasse et al., 1978; Cox et al., 2016).
Recent studies now highlight imperative roles for ketone bodies in mammalian cell metabolism, homeostasis, and signaling under a wide variety of physiological and pathological states. Apart from serving as energy fuels for extrahepatic tissues like brain, heart, or skeletal muscle, ketone bodies play pivotal roles as signaling mediators, drivers of protein post-translational modification (PTM), and modulators of inflammation and oxidative stress. In this review, we provide both classical and modern views of the pleiotropic roles of ketone bodies and their metabolism.
Overview of Ketone Body Metabolism
The rate of hepatic ketogenesis is governed by an orchestrated series of physiological and biochemical transformations of fat. Primary regulators include lipolysis of fatty acids from triacylglycerols, transport to and across the hepatocyte plasma membrane, transport into mitochondria via carnitine palmitoyltransferase 1 (CPT1), the ?-oxidation spiral, TCA cycle activity and intermediate concentrations, redox potential, and the hormonal regulators of these processes, predominantly glucagon and insulin [reviewed in (Arias et al., 1995; Ayte et al., 1993; Ehara et al., 2015; Ferre et al., 1983; Kahn et al., 2005; McGarry and Foster, 1980; Williamson et al., 1969)]. Classically ketogenesis is viewed as a spillover pathway, in which ?-oxidation-derived acetyl-CoA exceeds citrate synthase activity and/or oxaloacetate availability for condensation to form citrate. Three-carbon intermediates exhibit anti-ketogenic activity, presumably due to their ability to expand the oxaloacetate pool for acetyl-CoA consumption, but hepatic acetyl-CoA concentration alone does not determine ketogenic rate (Foster, 1967; Rawat and Menahan, 1975; Williamson et al., 1969). The regulation of ketogenesis by hormonal, transcriptional, and post-translational events together support the notion that the molecular mechanisms that fine-tune ketogenic rate remain incompletely understood (see Regulation of HMGCS2 and SCOT/OXCT1).
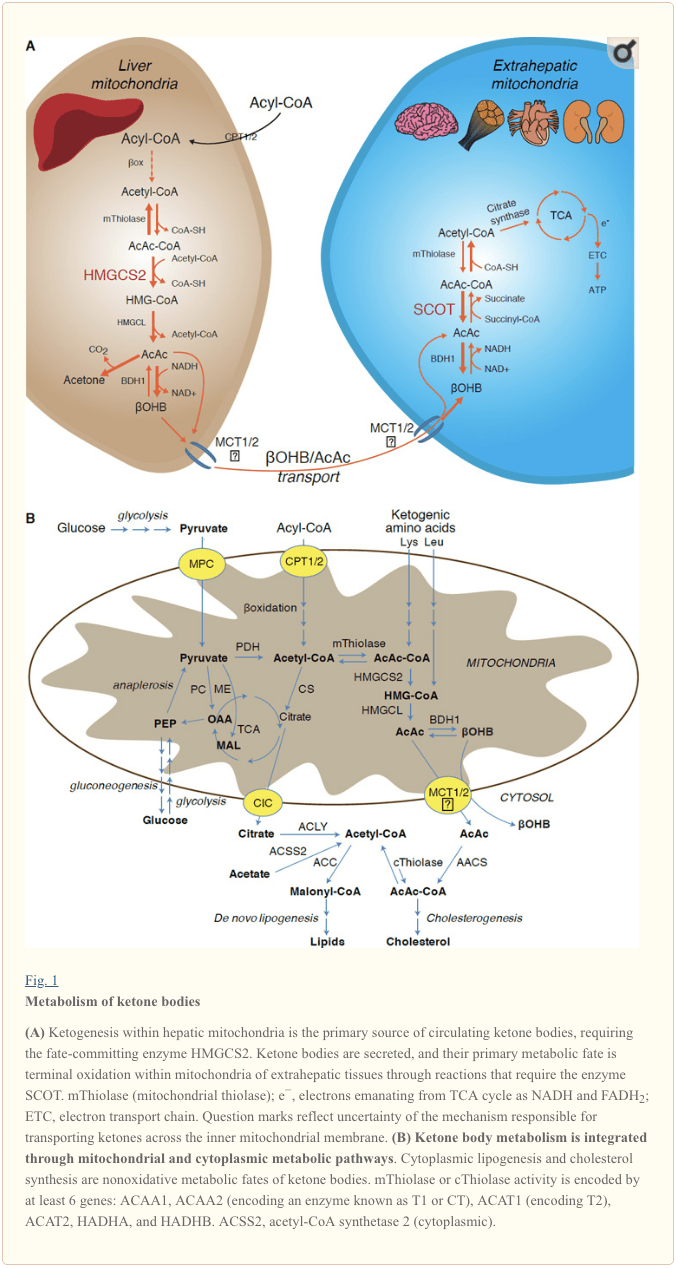
Ketogenesis occurs primarily in hepatic mitochondrial matrix at rates proportional to total fat oxidation. After transport of acyl chains across the mitochondrial membranes and ?-oxidation, the mitochondrial isoform of 3-hydroxymethylglutaryl-CoA synthase (HMGCS2) catalyzes the fate committing condensation of acetoacetyl-CoA (AcAc-CoA) and acetyl-CoA to generate HMG-CoA (Fig. 1A). HMG-CoA lyase (HMGCL) cleaves HMG-CoA to liberate acetyl-CoA and acetoacetate (AcAc), and the latter is reduced to d-?-hydroxybutyrate (d-?OHB) by phosphatidylcholine-dependent mitochondrial d-?OHB dehydrogenase (BDH1) in a NAD+/NADH-coupled near-equilibrium reaction (Bock and Fleischer, 1975; LEHNINGER et al., 1960). The BDH1 equilibrium constant favors d-?OHB production, but the ratio of AcAc/d-?OHB ketone bodies is directly proportional to mitochondrial NAD+/NADH ratio, and thus BDH1 oxidoreductase activity modulates mitochondrial redox potential (Krebs et al., 1969; Williamson et al., 1967). AcAc can also spontaneously decarboxylate to acetone (Pedersen, 1929), the source of sweet odor in humans suffering ketoacidosis (i.e., total serum ketone bodies > ~7 mM; AcAc pKa 3.6, ?OHB pKa 4.7). The mechanisms through which ketone bodies are transported across the mitochondrial inner membrane are not known, but AcAc/d-?OHB are released from cells via monocarboxylate transporters (in mammals, MCT 1 and 2, also known as solute carrier 16A family members 1 and 7) and transported in the circulation to extrahepatic tissues for terminal oxidation (Cotter et al., 2011; Halestrap and Wilson, 2012; Halestrap, 2012; Hugo et al., 2012). Concentrations of circulating ketone bodies are higher than those in the extrahepatic tissues (Harrison and Long, 1940) indicating ketone bodies are transported down a concentration gradient. Loss-of-function mutations in MCT1 are associated with spontaneous bouts of ketoacidosis, suggesting a critical role in ketone body import.
� With the exception of potential diversion of ketone bodies into non-oxidative fates (see Non-oxidative metabolic fates of ketone bodies), hepatocytes lack the ability to metabolize the ketone bodies they produce. Ketone bodies synthesized de novo by liver are (i) catabolized in mitochondria of extrahepatic tissues to acetyl-CoA, which is available to the TCA cycle for terminal oxidation (Fig. 1A), (ii) diverted to the lipogenesis or sterol synthesis pathways (Fig. 1B), or (iii) excreted in the urine. As an alternative energetic fuel, ketone bodies are avidly oxidized in heart, skeletal muscle, and brain (Balasse and Fery, 1989; Bentourkia et al., 2009; Owen et al., 1967; Reichard et al., 1974; Sultan, 1988). Extrahepatic mitochondrial BDH1 catalyzes the first reaction of ?OHB oxidation, converting it to back AcAc (LEHNINGER et al., 1960; Sandermann et al., 1986). A cytoplasmic d-?OHB-dehydrogenase (BDH2) with only 20% sequence identity to BDH1 has a high Km for ketone bodies, and also plays a role in iron homeostasis (Davuluri et al., 2016; Guo et al., 2006). In extrahepatic mitochondrial matrix, AcAc is activated to AcAc-CoA through exchange of a CoA-moiety from succinyl-CoA in a reaction catalyzed by a unique mammalian CoA transferase, succinyl-CoA:3-oxoacid-CoA transferase (SCOT, CoA transferase; encoded by OXCT1), through a near equilibrium reaction. The free energy released by hydrolysis of AcAc-CoA is greater than that of succinyl-CoA, favoring AcAc formation. Thus ketone body oxidative flux occurs due to mass action: an abundant supply of AcAc and rapid consumption of acetyl-CoA through citrate synthase favors AcAc-CoA (+ succinate) formation by SCOT. Notably, in contrast to glucose (hexokinase) and fatty acids (acyl-CoA synthetases), the activation of ketone bodies (SCOT) into an oxidizable form does not require the investment of ATP. A reversible AcAc-CoA thiolase reaction [catalyzed by any of the four mitochondrial thiolases encoded by either ACAA2 (encoding an enzyme known as T1 or CT), ACAT1 (encoding T2), HADHA, or HADHB] yields two molecules of acetyl-CoA, which enter the TCA cycle (Hersh and Jencks, 1967; Stern et al., 1956; Williamson et al., 1971). During ketotic states (i.e., total serum ketones > 500 �M), ketone bodies become significant contributors to energy expenditure�and are utilized in tissues rapidly until uptake or saturation of oxidation occurs (Balasse et al., 1978; Balasse and Fery, 1989; Edmond et al., 1987). A very small fraction of liver-derived ketone bodies can be readily measured in the urine, and utilization and reabsorption rates by the kidney are proportionate to circulating concentration (Goldstein, 1987; Robinson and Williamson, 1980). During highly ketotic states (> 1 mM in plasma), ketonuria serves as a semi-quantitative reporter of ketosis, although most clinical assays of urine ketone bodies detect AcAc but not ?OHB (Klocker et al., 2013).
Ketogenic Substrates and their Impact on Hepatocyte Metabolism
Ketogenic substrates include fatty acids and amino acids (Fig. 1B). The catabolism of amino acids, especially leucine, generates about 4% of ketone bodies in post-absorptive state (Thomas et al., 1982). Thus the acetyl-CoA substrate pool to generate ketone bodies mainly derives from fatty acids, because during states of diminished carbohydrate supply, pyruvate enters the hepatic TCA cycle primarily via anaplerosis, i.e., ATP-dependent carboxylation to oxaloacetate (OAA), or to malate (MAL), and not oxidative decarboxylation to acetyl-CoA (Jeoung et al., 2012; Magnusson et al., 1991; Merritt et al., 2011). In liver, glucose and pyruvate contribute negligibly to ketogenesis, even when pyruvate decarboxylation to acetyl-CoA is maximal (Jeoung et al., 2012).
Acetyl-CoA subsumes several roles integral to hepatic intermediary metabolism beyond ATP generation via terminal oxidation (also see The integration of ketone body metabolism, post-translational modification, and cell physiology). Acetyl-CoA allosterically activates (i) pyruvate carboxylase (PC), thereby activating a metabolic control mechanism that augments anaplerotic entry of metabolites into the TCA cycle (Owen et al., 2002; Scrutton and Utter, 1967) and (ii) pyruvate dehydrogenase kinase, which phosphorylates and inhibits pyruvate dehydrogenase (PDH) (Cooper et al., 1975), thereby further enhancing flow of pyruvate into the TCA cycle via anaplerosis. Furthermore, cytoplasmic acetyl-CoA, whose pool is augmented by mechanisms that convert mitochondrial acetyl-CoA to transportable metabolites, inhibits fatty acid oxidation: acetyl-CoA carboxylase (ACC) catalyzes the conversion of acetyl-CoA to malonyl-CoA, the lipogenic substrate and allosteric inhibitor of mitochondrial CPT1 [reviewed in (Kahn et al., 2005; McGarry and Foster, 1980)]. Thus, the mitochondrial acetyl-CoA pool both regulates and is regulated by the spillover pathway of ketogenesis, which orchestrates key aspects of hepatic intermediary metabolism.
Non-Oxidative Metabolic Fates of Ketone Bodies
The predominant fate of liver-derived ketones is SCOT-dependent extrahepatic oxidation. However, AcAc can be exported from mitochondria and utilized in anabolic pathways via conversion to AcAc-CoA by an ATP-dependent reaction catalyzed by cytoplasmic acetoacetyl-CoA synthetase (AACS, Fig. 1B). This pathway is active during brain development and in lactating mammary gland (Morris, 2005; Robinson and Williamson, 1978; Ohgami et al., 2003). AACS is also highly expressed in adipose tissue, and activated osteoclasts (Aguilo et al., 2010; Yamasaki et al., 2016). Cytoplasmic AcAc-CoA can be either directed by cytosolic HMGCS1 toward sterol biosynthesis, or cleaved by either of two cytoplasmic thiolases to acetyl-CoA (ACAA1 and ACAT2), carboxylated to malonyl-CoA, and contribute to the synthesis of fatty acids (Bergstrom et al., 1984; Edmond, 1974; Endemann et al., 1982; Geelen et al., 1983; Webber and Edmond, 1977).
While the physiological significance is yet to be established, ketones can serve as anabolic substrates even in the liver. In artificial experimental contexts, AcAc can contribute to as much as half of newly synthesized lipid, and up to 75% of new synthesized cholesterol (Endemann et al., 1982; Geelen et al., 1983; Freed et al., 1988). Because AcAc is derived from incomplete hepatic fat oxidation, the ability of AcAc to contribute to lipogenesis in vivo would imply hepatic futile cycling, where fat-derived ketones can be utilized for lipid production, a notion whose physiological significance requires experimental validation, but could serve adaptive or maladaptive roles (Solinas et al., 2015). AcAc avidly supplies cholesterogenesis, with a low AACS Km-AcAc (~50 �M) favoring AcAc activation even in the fed state (Bergstrom et al., 1984). The dynamic role of cytoplasmic ketone metabolism has been suggested in primary mouse embryonic neurons and in 3T3-L1 derived-adipocytes, as AACS knockdown impaired differentiation of each cell type (Hasegawa et al., 2012a; Hasegawa et al., 2012b). Knockdown of AACS in mice in vivo decreased serum cholesterol (Hasegawa et al., 2012c). SREBP-2, a master transcriptional regulator of cholesterol biosynthesis, and peroxisome proliferator activated receptor (PPAR)-? are AACS transcriptional activators, and regulate its transcription during neurite development and in the liver (Aguilo et al., 2010; Hasegawa et al., 2012c). Taken together, cytoplasmic ketone body metabolism may be important in select conditions or disease natural histories, but are inadequate to dispose of liver-derived ketone bodies, as massive hyperketonemia occurs in the setting of selective impairment of the primary oxidative fate via loss of function mutations to SCOT (Berry et al., 2001; Cotter et al., 2011).
Regulation of HMGCS2 and SCOT/OXCT1
The divergence of a mitochondrial from the gene encoding cytosolic HMGCS occurred early in vertebrate evolution due to the need to support hepatic ketogenesis in species with higher brain to body weight ratios (Boukaftane et al., 1994; Cunnane and Crawford, 2003). Naturally occurring loss-of-function HMGCS2 mutations in humans cause bouts of hypoketotic hypoglycemia (Pitt et al., 2015; Thompson et al., 1997). Robust HMGCS2 expression is restricted to hepatocytes and colonic epithelium, and its expression and enzymatic activity are coordinated through diverse mechanisms (Mascaro et al., 1995; McGarry and Foster, 1980; Robinson and Williamson, 1980). While the full scope of physiological states that influence HMGCS2 requires further elucidation, its expression and/or activity is regulated during the early postnatal period, aging, diabetes, starvation or ingestion of ketogenic diet (Balasse and Fery, 1989; Cahill GF Jr, 2006; Girard et al., 1992; Hegardt, 1999; Satapati et al., 2012; Sengupta et al., 2010). In the fetus, methylation of 5� flanking region of Hmgcs2 gene inversely correlates with its transcription, and is partially reversed after birth (Arias et al., 1995; Ayte et al., 1993; Ehara et al., 2015; Ferre et al., 1983). Similarly, hepatic Bdh1 exhibits a developmental expression pattern, increasing from birth to weaning, and is also induced by ketogenic diet in a fibroblast growth factor (FGF)-21-dependent manner (Badman et al., 2007; Zhang et al., 1989). Ketogenesis in mammals is highly responsive to both insulin and glucagon, being suppressed and stimulated, respectively (McGarry and Foster, 1977). Insulin suppresses adipose tissue lipolysis, thus depriving ketogenesis of its substrate, while glucagon increases ketogenic flux through a direct effect on the liver (Hegardt, 1999). Hmgcs2 transcription is stimulated by forkhead transcriptional factor FOXA2, which is inhibited via insulin-phosphatidylinositol-3-kinase/Akt, and is induced by glucagon-cAMP-p300 signaling (Arias et al., 1995; Hegardt, 1999; Quant et al., 1990; Thumelin et al., 1993; von Meyenn et al., 2013; Wolfrum et al., 2004; Wolfrum et al., 2003). PPAR? (Rodriguez et al., 1994) together with its target, FGF21 (Badman et al., 2007) also induce Hmgcs2 transcription in the liver during starvation or administration of ketogenic diet (Badman et al., 2007; Inagaki et al., 2007). Induction of PPAR? may occur before the transition from fetal to neonatal physiology, while FGF21 activation may be favored in the early neonatal period via ?OHB-mediated inhibition of histone deacetylase (HDAC)-3 (Rando et al., 2016). mTORC1 (mammalian target of rapamycin complex 1) dependent inhibition of PPAR? transcriptional activity is also a key regulator of Hmgcs2 gene expression (Sengupta et al., 2010), and liver PER2, a master circadian oscillator, indirectly regulates Hmgcs2 expression (Chavan et al., 2016). Recent observations indicate that extrahepatic tumor-induced interleukin-6 impairs ketogenesis via PPAR? suppression (Flint et al., 2016). Despite these observations, it is important to note that physiological shifts in Hmgcs2 gene expression have not been mechanistically linked to HMGCS2 protein abundance or to variations of ketogenic rate.
HMGCS2 enzyme activity is regulated through multiple PTMs. HMGCS2 serine phosphorylation enhanced its activity in vitro (Grimsrud et al., 2012). HMGCS2 activity is allosterically inhibited by succinyl-CoA and lysine residue succinylation (Arias et al., 1995; Hegardt, 1999; Lowe and Tubbs, 1985; Quant et al., 1990; Rardin et al., 2013; Reed et al., 1975; Thumelin et al., 1993). Succinylation of HMGCS2, HMGCL, and BDH1 lysine residues in hepatic mitochondria are targets of the NAD+ dependent deacylase sirtuin 5 (SIRT5) (Rardin et al., 2013). HMGCS2 activity is also enhanced by SIRT3 lysine deacetylation, and it is possible that crosstalk between acetylation and succinylation regulates HMGCS2 activity (Rardin et al., 2013; Shimazu et al., 2013). Despite the ability of these PTMs to regulate HMGCS2 Km and Vmax, fluctuations of these PTMs have not yet been carefully mapped and have not been confirmed as mechanistic drivers of ketogenesis in vivo.
SCOT is expressed in all mammalian cells that harbor mitochondria, except those of hepatocytes. The importance of SCOT activity and ketolysis was demonstrated in SCOT-KO mice, which exhibited uniform lethality due to hyperketonemic hypoglycemia within 48h after birth (Cotter et al., 2011). Tissue-specific loss of SCOT in neurons or skeletal myocytes induces metabolic abnormalities during starvation but is not lethal (Cotter et al., 2013b). In humans, SCOT deficiency presents early in life with severe ketoacidosis, causing lethargy, vomiting, and coma (Berry et al., 2001; Fukao et al., 2000; Kassovska-Bratinova et al., 1996; Niezen-Koning et al., 1997; Saudubray et al., 1987; Snyderman et al., 1998; Tildon and Cornblath, 1972). Relatively little is known at the cellular level about SCOT gene and protein expression regulators. Oxct1 mRNA expression and SCOT protein and activity are diminished in ketotic states, possibly through PPAR-dependent mechanisms (Fenselau and Wallis, 1974; Fenselau and Wallis, 1976; Grinblat et al., 1986; Okuda et al., 1991; Turko et al., 2001; Wentz et al., 2010). In diabetic ketoacidosis, the mismatch between hepatic ketogenesis and extrahepatic oxidation becomes exacerbated by impairment of SCOT activity. Overexpression of insulin-independent glucose transporter (GLUT1/SLC2A1) in cardiomyocytes also inhibits Oxct1 gene expression and downregulates ketones terminal oxidation in a non-ketotic state (Yan et al., 2009). In liver, Oxct1 mRNA abundance is suppressed by microRNA-122 and histone methylation H3K27me3 that are evident during the transition from fetal to the neonatal period (Thorrez et al., 2011). However, suppression of hepatic Oxct1 expression in the postnatal period is primarily attributable to the evacuation of Oxct1-expressing hematopoietic progenitors from the liver, rather than a loss of previously existing Oxct1 expression in terminally differentiated hepatocytes. In fact, expression of Oxct1 mRNA and SCOT protein in differentiated hepatocytes are extremely low (Orii et al., 2008).
SCOT is also regulated by PTMs. The enzyme is hyper-acetylated in brains of SIRT3 KO mice, which also exhibit diminished AcAc dependent acetyl-CoA production (Dittenhafer-Reed et al., 2015). Non-enzymatic nitration of tyrosine residues of SCOT also attenuates its activity, which has been reported in hearts of various diabetic mice models (Marcondes et al., 2001; Turko et al., 2001; Wang et al., 2010a). In contrast, tryptophan residue nitration augments SCOT activity (Br�g�re et al., 2010; Rebrin et al., 2007). Molecular mechanisms of residue-specific nitration or de-nitration designed to modulate SCOT activity may exist and require elucidation.
Controversies in Extrahepatic Ketogenesis
In mammals the primary ketogenic organ is liver, and only hepatocytes and gut epithelial cells abundantly express the mitochondrial isoform of HMGCS2 (Cotter et al., 2013a; Cotter et al., 2014; McGarry and Foster, 1980; Robinson and Williamson, 1980). Anaerobic bacterial fermentation of complex polysaccharides yields butyrate, which is absorbed by colonocytes in mammalians for terminal oxidation or ketogenesis (Cherbuy et al., 1995), which may play a role in colonocyte differentiation (Wang et al., 2016). Excluding gut epithelial cells and hepatocytes, HMGCS2 is nearly absent in almost all other mammalian cells, but the prospect of extrahepatic ketogenesis has been raised in tumor cells, astrocytes of the central nervous system, the kidney, pancreatic ? cells, retinal pigment epithelium (RPE), and even in skeletal muscle (Adijanto et al., 2014; Avogaro et al., 1992; El Azzouny et al., 2016; Grabacka et al., 2016; Kang et al., 2015; Le Foll et al., 2014; Nonaka et al., 2016; Takagi et al., 2016a; Thevenet et al., 2016; Zhang et al., 2011). Ectopic HMGCS2 has been observed in tissues that lack net ketogenic capacity (Cook et al., 2016; Wentz et al., 2010), and HMGCS2 exhibits prospective ketogenesis-independent �moonlighting� activities, including within the cell nucleus (Chen et al., 2016; Kostiuk et al., 2010; Meertens et al., 1998).
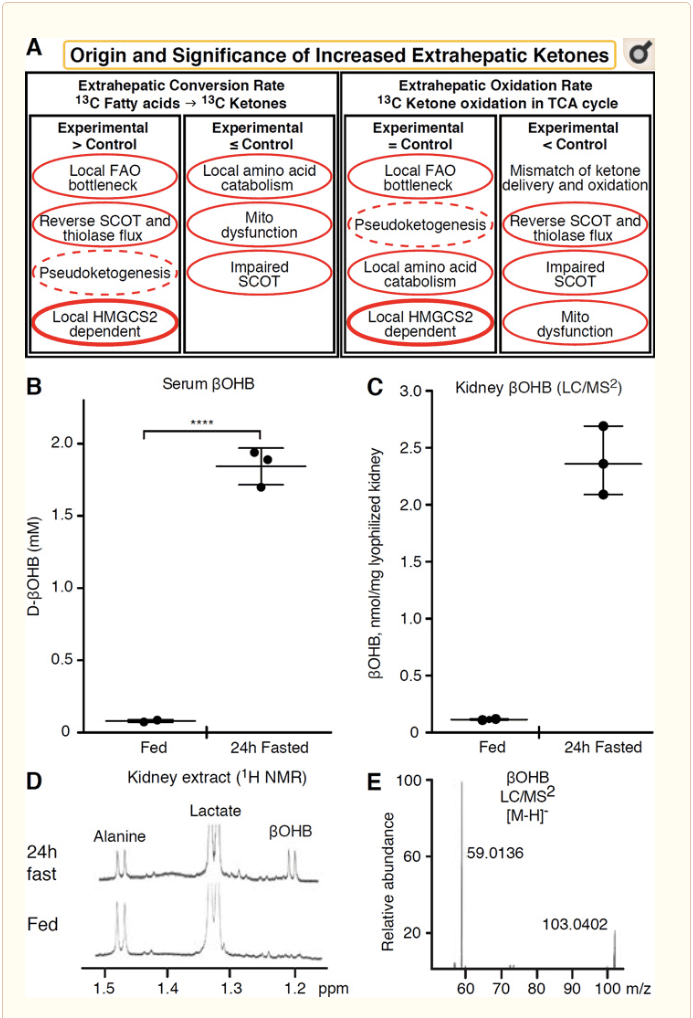
Any extrahepatic tissue that oxidizes ketone bodies also has the potential to accumulate ketone bodies via HMGCS2 independent mechanisms (Fig. 2A). However, there is no extrahepatic tissue in which a steady state ketone body concentration exceeds that in the circulation (Cotter et al., 2011; Cotter et al., 2013b; Harrison and Long, 1940), underscoring that ketone bodies are transported down a concentration gradient via MCT1/2-dependent mechanisms. One mechanism of apparent extrahepatic ketogenesis may actually reflect relative impairment of ketone oxidation. Additional potential explanations fall within the realm of ketone body formation. First, de novo ketogenesis may occur via reversible enzymatic activity of thiolase and SCOT (Weidemann and Krebs, 1969). When the concentration of acetyl-CoA is relatively high, reactions normally responsible for AcAc oxidation operate in the reverse direction (GOLDMAN, 1954). A second mechanism occurs when ?-oxidation-derived intermediates accumulate due to a TCA cycle bottleneck, AcAc-CoA is converted to l-?OHB-CoA through a reaction catalyzed by mitochondrial 3-hydroxyacyl-CoA dehydrogenase, and further by 3-hydroxybutyryl CoA deacylase to l-?OHB, which is indistinguishable by mass spectrometry or resonance spectroscopy from the physiological enantiomer d-?OHB (Reed and Ozand, 1980). l-?OHB can be chromatographically or enzymatically distinguished from d-?OHB, and is present in extrahepatic tissues, but not in liver or blood (Hsu et al., 2011). Hepatic ketogenesis produces only d-?OHB, the only enantiomer that is a BDH substrate (Ito et al., 1984; Lincoln et al., 1987; Reed and Ozand, 1980; Scofield et al., 1982; Scofield et al., 1982). A third HMGCS2-independent mechanism generates d-?OHB through amino acid catabolism, particularly that of leucine and lysine. A fourth mechanism is only apparent because it is due to a labeling artifact and is thus termed pseudoketogenesis. This phenomenon is attributable to the reversibility of the SCOT and thiolase reactions, and can cause overestimation of ketone body turnover due to the isotopic dilution of ketone body tracer in extrahepatic tissue (Des Rosiers et al., 1990; Fink et al., 1988). Nonetheless, pseudoketogenesis may be negligible in most contexts (Bailey et al., 1990; Keller et al., 1978). A schematic (Fig. 2A) indicates a useful approach to apply while considering elevated tissue steady state concentration of ketones.
� Kidney has recently received attention as a potentially ketogenic organ. In the vast majority of states, the kidney is a net consumer of liver-derived ketone bodies, excreting or reabsorbing ketone bodies from the bloodstream, and kidney is generally not a net ketone body generator or concentrator (Robinson and Williamson, 1980). The authors of a classical study concluded that minimal renal ketogenesis quantified in an artificial experimental system was not physiologically relevant (Weidemann and Krebs, 1969). Recently, renal ketogenesis has been inferred in diabetic and autophagy deficient mouse models, but it is more likely that multi-organ shifts in metabolic homeostasis alter integrative ketone metabolism through inputs on multiple organs (Takagi et al., 2016a; Takagi et al., 2016b; Zhang et al., 2011). One recent publication suggested renal ketogenesis as a protective mechanism against ischemia-reperfusion injury in the kidney (Tran et al., 2016). Absolute steady state concentrations of ?OHB from extracts of mice renal tissue were reported at ~4�12 mM. To test whether this was tenable, we quantified ?OHB concentrations in renal extracts from fed and 24h fasted mice. Serum ?OHB concentrations increased from ~100 �M to 2 mM with 24h fasting (Fig. 2B), while renal steady state ?OHB concentrations approximate 100 �M in the fed state, and only 1 mM in the 24h fasted state (Fig. 2C�E), observations that are consistent with concentrations quantified over 45 years ago (Hems and Brosnan, 1970). It remains possible that in ketotic states, liver-derived ketone bodies could be renoprotective, but evidence for renal ketogenesis requires further substantiation. Compelling evidence that supports true extrahepatic ketogenesis was presented in RPE (Adijanto et al., 2014). This intriguing metabolic transformation was suggested to potentially allow RPE-derived ketones to flow to photoreceptor or M�ller glia cells, which could aid in the regeneration of photoreceptor outer segment.
?OHB as a Signaling Mediator
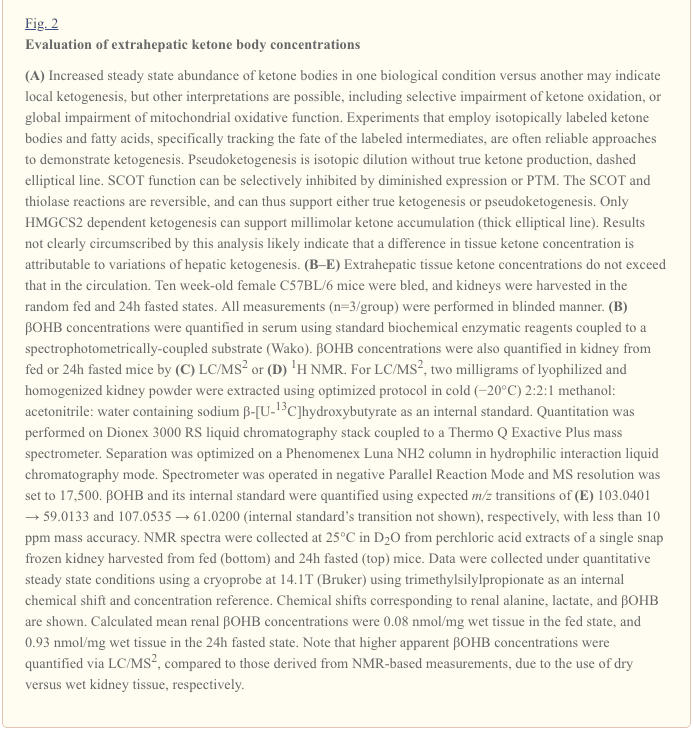
Although they are energetically rich, ketone bodies exert provocative �non-canonical� signaling roles in cellular homeostasis (Fig. 3) (Newman and Verdin, 2014; Rojas-Morales et al., 2016). For example, ?OHB inhibits Class I HDACs, which increases histone acetylation and thereby induces the expression of genes that curtail oxidative stress (Shimazu et al., 2013). ?OHB itself is a histone covalent modifier at lysine residues in livers of fasted or streptozotocin induced diabetic mice (Xie et al., 2016) (also see below, The integration of ketone body metabolism, post-translational modification, and cell physiology, and Ketone bodies, oxidative stress, and neuroprotection).
�
?OHB is also an effector via G-protein coupled receptors. Through unclear molecular mechanisms, it suppresses sympathetic nervous system activity and reduces total energy expenditure and heart rate by inhibiting short chain fatty acid signaling through G protein coupled receptor 41 (GPR41) (Kimura et al., 2011). One of the most studied signaling effects of ?OHB proceeds through GPR109A (also known as HCAR2), a member of the hydrocarboxylic acid GPCR sub-family expressed in adipose tissues (white and brown) (Tunaru et al., 2003), and in immune cells (Ahmed et al., 2009). ?OHB is the only known endogenous ligand of GPR109A receptor (EC50 ~770 �M) activated by d-?OHB, l-?OHB, and butyrate, but not AcAc (Taggart et al., 2005). The high concentration threshold for GPR109A activation is achieved through adherence to a ketogenic diet, starvation, or during ketoacidosis, leading to inhibition of adipose tissue lipolysis. The anti-lipolytic effect of GPR109A proceeds through inhibition of adenylyl cyclase and decreased cAMP, inhibiting hormone sensitive triglyceride lipase (Ahmed et al., 2009; Tunaru et al., 2003). This creates a negative feedback loop in which ketosis places a modulatory brake on ketogenesis by diminishing the release of non-esterified fatty acids from adipocytes (Ahmed et al., 2009; Taggart et al., 2005), an effect that can be counterbalanced by the sympathetic drive that stimulates lipolysis. Niacin (vitamin B3, nicotinic acid) is a potent (EC50 ~ 0.1 �M) ligand for GRP109A, effectively employed for decades for dyslipidemias (Benyo et al., 2005; Benyo et al., 2006; Fabbrini et al., 2010a; Lukasova et al., 2011; Tunaru et al., 2003). While niacin enhances reverse cholesterol transport in macrophages and reduces atherosclerotic lesions (Lukasova et al., 2011), the effects of ?OHB on atherosclerotic lesions remain unknown. Although GPR109A receptor exerts protective roles, and intriguing connections exist between ketogenic diet use in stroke and neurodegenerative diseases (Fu et al., 2015; Rahman et al., 2014), a protective role of ?OHB via GPR109A has not been demonstrated in vivo.
Finally, ?OHB may influence appetite and satiety. A meta-analysis of studies that measured the effects of ketogenic and very low energy diets concluded that participants consuming these diets exhibit higher satiety, compared to control diets (Gibson et al., 2015). However, a plausible explanation for this effect is the additional metabolic or hormonal elements that might modulate appetite. For example, mice maintained on a rodent ketogenic diet exhibited increased energy expenditure compared to chow control-fed mice, despite similar caloric intake, and circulating leptin or genes of peptides regulating feeding behavior were not changed (Kennedy et al., 2007). Among proposed mechanisms that suggest appetite suppression by ?OHB includes both signaling and oxidation (Laeger et al., 2010). Hepatocyte specific deletion of circadian rhythm gene (Per2)�and chromatin immunoprecipitation studies revealed that PER2 directly activates the Cpt1a gene, and indirectly regulates Hmgcs2, leading to impaired ketosis in Per2 knockout mice (Chavan et al., 2016). These mice exhibited impaired food anticipation, which was partially restored by systemic ?OHB administration. Future studies will be needed to confirm the central nervous system as a direct ?OHB target, and whether ketone oxidation is required for the observed effects, or whether another signaling mechanism is involved. Other investigators have invoked the possibility of local astrocyte-derived ketogenesis within the ventromedial hypothalamus as a regulator of food intake, but these preliminary observations also will benefit from genetic and flux-based assessments (Le Foll et al., 2014). The relationship between ketosis and nutrient deprivation remains of interest because hunger and satiety are important elements in failed weight loss attempts.
Integration of Ketone Body Metabolism, Post-Translational Modification, and Cell Physiology
Ketone bodies contribute to compartmentalized pools of acetyl-CoA, a key intermediate that exhibits prominent roles in cellular metabolism (Pietrocola et al., 2015). One role of acetyl-CoA is to serve as a substrate for acetylation, an enzymatically-catalyzed histone covalent modification (Choudhary et al., 2014; Dutta et al., 2016; Fan et al., 2015; Menzies et al., 2016). A large number of dynamically acetylated mitochondrial proteins, many of which may occur through non-enzymatic mechanisms, have also emerged from computational proteomics studies (Dittenhafer-Reed et al., 2015; Hebert et al., 2013; Rardin et al., 2013; Shimazu et al., 2010). Lysine deacetylases use a zinc cofactor (e.g., nucleocytosolic HDACs) or NAD+ as co-substrate (sirtuins, SIRTs) (Choudhary et al., 2014; Menzies et al., 2016). The acetylproteome serves as both sensor and effector of the total cellular acetyl-CoA pool, as physiological and genetic manipulations each result in non-enzymatic global variations of acetylation (Weinert et al., 2014). As intracellular metabolites serve as modulators of lysine residue acetylation, it is important to consider the role of ketone bodies, whose abundance is highly dynamic.
?OHB is an epigenetic modifier through at least two mechanisms. Increased ?OHB levels induced by fasting, caloric restriction, direct administration or prolonged exercise provoke HDAC inhibition or histone acetyltransferase activation (Marosi et al., 2016; Sleiman et al., 2016) or to oxidative stress (Shimazu et al., 2013). ?OHB inhibition of HDAC3 could regulate newborn metabolic physiology (Rando et al., 2016). Independently, ?OHB itself directly modifies histone lysine residues (Xie et al., 2016). Prolonged fasting, or steptozotocin-induced diabetic ketoacidosis increased histone ?-hydroxybutyrylation. Although the number of lysine ?-hydroxybutyrylation and acetylation sites was comparable, stoichiometrically greater histone ?-hydroxybutyrylation than acetylation was observed. Distinct genes were impacted by histone lysine ?-hydroxybutyrylation, versus acetylation or methylation, suggesting distinct cellular functions. Whether ?-hydroxybutyrylation is spontaneous or enzymatic is not known, but expands the range of mechanisms through ketone bodies dynamically influence transcription.
Essential cell reprogramming events during caloric restriction and nutrient deprivation may be mediated in SIRT3- and SIRT5-dependent mitochondrial deacetylation and desuccinylation, respectively, regulating ketogenic and ketolytic proteins at post-translational level in liver and extrahepatic tissues (Dittenhafer-Reed et al., 2015; Hebert et al., 2013; Rardin et al., 2013; Shimazu et al., 2010). Even though stoichiometric comparison of occupied sites does not necessarily link directly to shifts in metabolic flux, mitochondrial acetylation is dynamic and may be driven by acetyl-CoA concentration or mitochondrial pH, rather than enzymatic acetyltransferases (Wagner and Payne, 2013). That SIRT3 and SIRT5 modulate activities of ketone body metabolizing enzymes provokes the question of the reciprocal role of ketones in sculpting the acetylproteome, succinylproteome, and other dynamic cellular targets. Indeed, as variations of ketogenesis reflect NAD+ concentrations, ketone production and abundance could regulate sirtuin activity, thereby influencing total acetyl-CoA/succinyl-CoA pools, the acylproteome, and thus mitochondrial and cell physiology. ?-hydroxybutyrylation of enzyme lysine residues could add another layer to cellular reprogramming. In extrahepatic tissues, ketone body oxidation may stimulate analogous changes in cell homeostasis. While compartmentation of acetyl-CoA pools is highly regulated and coordinates a broad spectrum of cellular changes, the ability of ketone bodies to directly shape both mitochondrial and cytoplasmic acetyl-CoA concentrations requires elucidation (Chen et al., 2012; Corbet et al., 2016; Pougovkina et al., 2014; Schwer et al., 2009; Wellen and Thompson, 2012). Because acetyl-CoA concentrations are tightly regulated, and acetyl-CoA is membrane impermeant, it is crucial to consider the driver mechanisms coordinating acetyl-CoA homeostasis, including the rates of production and terminal oxidation in the TCA cycle, conversion into ketone bodies, mitochondrial efflux via carnitine acetyltransferase (CrAT), or acetyl-CoA export to cytosol after conversion to citrate and release by ATP citrate lyase (ACLY). The key roles of these latter mechanisms in cell acetylproteome and homeostasis require matched understanding of the roles of ketogenesis and ketone oxidation (Das et al., 2015; McDonnell et al., 2016; Moussaieff et al., 2015; Overmyer et al., 2015; Seiler et al., 2014; Seiler et al., 2015; Wellen et al., 2009; Wellen and Thompson, 2012). Convergent technologies in metabolomics and acylproteomics in the setting of genetically manipulated models will be required to specify targets and outcomes.
Anti- and Pro-Inflammatory Responses to Ketone Bodies
Ketosis and ketone bodies modulate inflammation and immune cell function, but varied and even discrepant mechanisms have been proposed. Prolonged nutrient deprivation reduces inflammation (Youm et al., 2015), but the chronic ketosis of type 1 diabetes is a pro-inflammatory state (Jain et al., 2002; Kanikarla-Marie and Jain, 2015; Kurepa et al., 2012). Mechanism-based signaling roles for ?OHB in inflammation emerge because many immune system cells, including macrophages or monocytes, abundantly express GPR109A. While ?OHB exerts a predominantly anti-inflammatory response (Fu et al., 2014; Gambhir et al., 2012; Rahman et al., 2014; Youm et al., 2015), high concentrations of ketone bodies, particularly AcAc, may trigger a pro-inflammatory response (Jain et al., 2002; Kanikarla-Marie and Jain, 2015; Kurepa et al., 2012).
Anti-inflammatory roles of GPR109A ligands in atherosclerosis, obesity, inflammatory bowel disease, neurological disease, and cancer have been reviewed (Graff et al., 2016). GPR109A expression is augmented in RPE cells of diabetic models, human diabetic patients (Gambhir et al., 2012), and in microglia during neurodegeneration (Fu et al., 2014). Anti-inflammatory effects of ?OHB are enhanced by GPR109A overexpression in RPE cells, and abrogated by pharmacological inhibition or genetic knockout of GPR109A (Gambhir et al., 2012). ?OHB and exogenous nicotinic acid (Taggart et al., 2005), both confer anti-inflammatory effects in TNF? or LPS-induced inflammation by decreasing the levels of pro-inflammatory proteins (iNOS, COX-2), or secreted cytokines (TNF?, IL-1?, IL-6, CCL2/MCP-1), in part through inhibiting NF-?B translocation (Fu et al., 2014; Gambhir et al., 2012). ?OHB decreases ER stress and the NLRP3 inflammasome, activating the antioxidative stress response (Bae et al., 2016; Youm et al., 2015). However, in neurodegenerative inflammation, GPR109A-dependent ?OHB-mediated protection does not involve inflammatory mediators like MAPK pathway signaling (e.g., ERK, JNK, p38) (Fu et al., 2014), but may require COX-1-dependent PGD2 production (Rahman et al., 2014). It is intriguing that macrophage GPR109A is required to exert a neuroprotective effect in an ischemic stroke model (Rahman et al., 2014), but the ability of ?OHB to inhibit the NLRP3 inflammasome in bone marrow derived macrophages is GPR109A independent (Youm et al., 2015). Although most studies link ?OHB to anti-inflammatory effects, ?OHB may be pro-inflammatory and increase markers of lipid peroxidation in calf hepatocytes (Shi et al., 2014). Anti- versus pro-inflammatory effects of ?OHB may thus depend on cell type, ?OHB concentration, exposure duration, and the presence or absence of co-modulators.
Unlike ?OHB, AcAc may activate pro-inflammatory signaling. Elevated AcAc, especially with a high glucose concentration, intensifies endothelial cell injury through an NADPH oxidase/oxidative stress dependent mechanism (Kanikarla-Marie and Jain, 2015). High AcAc concentrations in umbilical cord of diabetic mothers were correlated with higher protein oxidation rate and MCP-1 concentration (Kurepa et al., 2012). High AcAc in diabetic patients was correlated with TNF? expression (Jain et al., 2002), and AcAc, but not ?OHB, induced TNF?, MCP-1 expression, ROS accumulation, and diminished cAMP level in U937 human monocyte cells (Jain et al., 2002; Kurepa et al., 2012).
Ketone body dependent signaling phenomena are frequently triggered only with high ketone body concentrations (> 5 mM), and in the case of many studies linking ketones to pro- or anti-inflammatory effects, through unclear mechanisms. In addition, due to the contradictory effects of ?OHB versus AcAc on inflammation, and the ability of AcAc/?OHB ratio to influence mitochondrial redox potential, the best experiments assessing the roles of ketone bodies on cellular phenotypes compare the effects of AcAc and ?OHB in varying ratios, and at varying cumulative concentrations [e.g., (Saito et al., 2016)]. Finally, AcAc can be purchased commercially only as a lithium salt or as an ethyl ester that requires base hydrolysis before use. Lithium cation independently induces signal transduction cascades (Manji et al., 1995), and AcAc anion is labile. Finally, studies using racemic d/l-?OHB can be confounded, as only the d-?OHB stereoisomer can be oxidized to AcAc, but d-?OHB and l-?OHB can each signal through GPR109A, inhibit the NLRP3 inflammasome, and serve as lipogenic substrates.
Ketone Bodies, Oxidative Stress, and Neuroprotection
Oxidative stress is typically defined as a state in which ROS are presented in excess, due to excessive production and/or impaired elimination. Antioxidant and oxidative stress mitigating roles of ketone bodies have been widely described both in vitro and in vivo, particularly in the context of neuroprotection. As most neurons do not effectively generate high-energy phosphates from fatty acids�but do oxidize ketone bodies when carbohydrates are in short supply, neuroprotective effects of ketone bodies are especially important (Cahill GF Jr, 2006; Edmond et al., 1987; Yang et al., 1987). In oxidative stress models, BDH1 induction and SCOT suppression suggest that ketone body metabolism can be reprogrammed to sustain diverse cell signaling, redox potential, or metabolic requirements (Nagao et al., 2016; Tieu et al., 2003).
Ketone bodies decrease the grades of cellular damage, injury, death and lower apoptosis in neurons and cardiomyocytes (Haces et al., 2008; Maalouf et al., 2007; Nagao et al., 2016; Tieu et al., 2003). Invoked mechanisms are varied and not always linearly related to concentration. Low millimolar concentrations of (d or l)-?OHB scavenge ROS (hydroxyl anion), while AcAc scavenges numerous ROS species, but only at concentrations that exceed the physiological range (IC50 20�67 mM) (Haces et al., 2008). Conversely, a beneficial influence over the electron transport chain�s redox potential is a mechanism commonly linked to d-?OHB. While all three ketone bodies (d/l-?OHB and AcAc) reduced neuronal cell death and ROS accumulation triggered by chemical inhibition of glycolysis, only d-?OHB and AcAc prevented neuronal ATP decline. Conversely, in a hypoglycemic in vivo model, (d or l)-?OHB, but not AcAc prevented hippocampal lipid peroxidation (Haces et al., 2008; Maalouf et al., 2007; Marosi et al., 2016; Murphy, 2009; Tieu et al., 2003). In vivo studies of mice fed a ketogenic diet (87% kcal fat and 13% protein) exhibited neuroanatomical variation of antioxidant capacity (Ziegler et al., 2003), where the most profound changes were observed in hippocampus, with increase glutathione peroxidase and total antioxidant capacities.
Ketogenic diet, ketone esters (also see Therapeutic use of ketogenic diet and exogenous ketone bodies), or ?OHB administration exert neuroprotection in models of ischemic stroke (Rahman et al., 2014); Parkinson�s disease (Tieu et al., 2003); central nervous system oxygen toxicity seizure (D’Agostino et al., 2013); epileptic spasms (Yum et al., 2015); mitochondrial encephalomyopathy, lactic acidosis and stroke-like (MELAS) episodes syndrome (Frey et al., 2016) and Alzheimer�s disease (Cunnane and Crawford, 2003; Yin et al., 2016). Conversely, a recent report demonstrated histopathological evidence of neurodegenerative progression by a ketogenic diet in a transgenic mouse model of abnormal mitochondrial DNA repair, despite increases in mitochondrial biogenesis and antioxidant signatures (Lauritzen et al., 2016). Other conflicting reports suggest that exposure to high ketone body concentrations elicits oxidative stress. High ?OHB or AcAc doses induced nitric oxide secretion, lipid peroxidation, reduced expression of SOD, glutathione peroxidase and catalase in calf hepatocytes, while in rat hepatocytes the MAPK pathway induction was attributed to AcAc but not ?OHB (Abdelmegeed et al., 2004; Shi et al., 2014; Shi et al., 2016).
Taken together, most reports link ?OHB to attenuation of oxidative stress, as its administration inhibits ROS/superoxide production, prevents lipid peroxidation and protein oxidation, increases antioxidant protein levels, and improves mitochondrial respiration and ATP production (Abdelmegeed et al., 2004; Haces et al., 2008; Jain et al., 1998; Jain et al., 2002; Kanikarla-Marie and Jain, 2015; Maalouf et al., 2007; Maalouf and Rho, 2008; Marosi et al., 2016; Tieu et al., 2003; Yin et al., 2016; Ziegler et al., 2003). While AcAc has been more directly correlated than ?OHB with the induction of oxidative stress, these effects are not always easily dissected from prospective pro-inflammatory responses (Jain et al., 2002; Kanikarla-Marie and Jain, 2015; Kanikarla-Marie and Jain, 2016). Moreover, it is critical to consider that the apparent antioxidative benefit conferred by pleiotropic ketogenic diets may not be transduced by ketone bodies themselves, and neuroprotection conferred by ketone bodies may not entirely be attributable to oxidative stress. For example during glucose deprivation, in a model of glucose deprivation in cortical neurons, ?OHB stimulated autophagic flux and prevented autophagosome accumulation, which was associated with decreased neuronal death (Camberos-Luna et al., 2016). d-?OHB induces also the canonical antioxidant proteins FOXO3a, SOD, MnSOD, and catalase, prospectively through HDAC inhibition (Nagao et al., 2016; Shimazu et al., 2013).
Non-Alcoholic Fatty Liver Disease (NAFLD) and Ketone Body Metabolism
Obesity-associated NAFLD and nonalcoholic steatohepatitis (NASH) are the most common causes of liver disease in Western countries (Rinella and Sanyal, 2016), and NASH-induced liver failure is one of the most common reasons for liver transplantation. While excess storage of triacylglycerols in hepatocytes >5% of liver weight (NAFL) alone does not cause degenerative liver function, the progression to NAFLD in humans correlates with systemic insulin resistance and increased risk of type 2 diabetes, and may contribute to the pathogenesis of cardiovascular disease and chronic kidney disease (Fabbrini et al., 2009; Targher et al., 2010; Targher and Byrne, 2013). The pathogenic mechanisms of NAFLD and NASH are incompletely understood but include abnormalities of hepatocyte metabolism, hepatocyte autophagy and endoplasmic reticulum stress, hepatic immune cell function, adipose tissue inflammation, and systemic inflammatory mediators (Fabbrini et al., 2009; Masuoka and Chalasani, 2013; Targher et al., 2010; Yang et al., 2010). Perturbations of carbohydrate, lipid, and amino acid metabolism occur in and contribute to obesity, diabetes, and NAFLD in humans and in model organisms [reviewed in (Farese et al., 2012; Lin and Accili, 2011; Newgard, 2012; Samuel and Shulman, 2012; Sun and Lazar, 2013)]. While hepatocyte abnormalities in cytoplasmic lipid metabolism are commonly observed in NAFLD (Fabbrini et al., 2010b), the role of mitochondrial metabolism, which governs oxidative disposal of fats is less clear in NAFLD pathogenesis. Abnormalities of mitochondrial metabolism occur in and contribute to NAFLD/NASH pathogenesis (Hyotylainen et al., 2016; Serviddio et al., 2011; Serviddio et al., 2008; Wei et al., 2008). There is general (Felig et al., 1974; Iozzo et al., 2010; Koliaki et al., 2015; Satapati et al., 2015; Satapati et al., 2012; Sunny et al., 2011) but not uniform (Koliaki and Roden, 2013; Perry et al., 2016; Rector et al., 2010) consensus that, prior to the development of bona fide NASH, hepatic mitochondrial oxidation, and in particular fat oxidation, is augmented in obesity, systemic insulin resistance, and NAFLD. It is likely that as NAFLD progresses, oxidative capacity heterogenity, even among individual mitochondria, emerges, and ultimately oxidative function becomes impaired (Koliaki et al., 2015; Rector et al., 2010; Satapati et al., 2008; Satapati et al., 2012).
Ketogenesis is often used as a proxy for hepatic fat oxidation. Impairments of ketogenesis emerge as NAFLD progresses in animal models, and likely in humans. Through incompletely defined mechanisms, hyperinsulinemia suppresses ketogenesis, possibly contributing to hypoketonemia compared to lean controls (Bergman et al., 2007; Bickerton et al., 2008; Satapati et al., 2012; Soeters et al., 2009; Sunny et al., 2011; Vice et al., 2005). Nonetheless, the ability of circulating ketone body concentrations to predict NAFLD is controversial (M�nnist� et al., 2015; Sanyal et al., 2001). Robust quantitative magnetic resonance spectroscopic methods in animal models revealed increased ketone turnover rate with moderate insulin resistance, but decreased rates were evident with more severe insulin resistance (Satapati et al., 2012; Sunny et al., 2010). In obese humans with fatty liver, ketogenic rate is normal (Bickerton et al., 2008; Sunny et al., 2011), and hence, the rates of ketogenesis are diminished relative to the increased fatty acid load within hepatocytes. Consequently, ?-oxidation-derived acetyl-CoA may be directed to terminal oxidation in the TCA cycle, increasing terminal oxidation, phosphoenolpyruvate-driven gluconeogenesis via anaplerosis/cataplerosis, and oxidative stress. Acetyl-CoA also possibly undergoes export from mitochondria as citrate, a precursor substrate for lipogenesis (Fig. 4) (Satapati et al., 2015; Satapati et al., 2012; Solinas et al., 2015). While ketogenesis becomes less responsive to insulin or fasting with prolonged obesity (Satapati et al., 2012), the underlying mechanisms and downstream consequences of this remain incompletely understood. Recent evidence indicates that mTORC1 suppresses ketogenesis in a manner that may be downstream of insulin signaling (Kucejova et al., 2016), which is concordant with the observations that mTORC1 inhibits PPAR?-mediated Hmgcs2 induction (Sengupta et al., 2010) (also see Regulation of HMGCS2 and SCOT/OXCT1).
�
Preliminary observations from our group suggest adverse hepatic consequences of ketogenic insufficiency (Cotter et al., 2014). To test the hypothesis that impaired ketogenesis, even in carbohydrate-replete and thus �non-ketogenic� states, contributes to abnormal glucose metabolism and provokes steatohepatitis, we generated a mouse model of marked ketogenic insufficiency by administration of antisense oligonucleotides (ASO) targeted to Hmgcs2. Loss of HMGCS2 in standard low-fat chow-fed adult mice caused mild hyperglycemia and markedly increased production of hundreds of hepatic metabolites, a suite of which strongly suggested lipogenesis activation. High-fat diet feeding of mice with insufficient ketogenesis resulted in extensive hepatocyte injury and inflammation. These findings support the central hypotheses that (i) ketogenesis is not a passive overflow pathway but rather a dynamic node in hepatic and integrated physiological homeostasis, and (ii) prudent ketogenic augmentation to mitigate NAFLD/NASH and disordered hepatic glucose metabolism is worthy of exploration.
How might impaired ketogenesis contribute to hepatic injury and altered glucose homeostasis? The first consideration is whether the culprit is deficiency of ketogenic flux, or ketones themselves. A recent report suggests that ketone bodies may mitigate oxidative stress-induced hepatic injury in response to n-3 polyunsaturated fatty acids (Pawlak et al., 2015). Recall that due to lack of SCOT expression in hepatocytes, ketone bodies are not oxidized, but they can contribute to lipogenesis, and serve a variety of signaling roles independent of their oxidation (also see Non-oxidative metabolic fates of ketone bodies and ?OHB as a signaling mediator). It is also possible that hepatocyte-derived ketone bodies may serve as a signal and/or metabolite for neighboring cell types within the hepatic acinus, including stellate cells and Kupffer cell macrophages. While the limited literature available suggests that macrophages are unable to oxidize ketone bodies, this has only been measured using classical methodologies, and only in peritoneal macrophages (Newsholme et al., 1986; Newsholme et al., 1987), indicating that a re-assessment is appropriate given abundant SCOT expression in bone marrow-derived macrophages (Youm et al., 2015).
Hepatocyte ketogenic flux may also be cytoprotective. While salutary mechanisms may not depend on ketogenesis per se, low carbohydrate ketogenic diets have been associated with amelioration of NAFLD (Browning et al., 2011; Foster et al., 2010; Kani et al., 2014; Schugar and Crawford, 2012). Our observations indicate that hepatocyte ketogenesis may feedback and regulate TCA cycle flux, anaplerotic flux, phosphoenolpyruvate-derived gluconeogenesis (Cotter et al., 2014), and even glycogen turnover. Ketogenic impairment directs acetyl-CoA to increase TCA flux, which in liver has been linked to increased ROS-mediated injury (Satapati et al., 2015; Satapati et al., 2012); forces diversion of carbon into de novo synthesized lipid species that could prove cytotoxic; and prevents NADH re-oxidation to NAD+ (Cotter et al., 2014) (Fig. 4). Taken together, future experiments are required to address mechanisms through which relative ketogenic insufficiency may become maladaptive, contribute to hyperglycemia, provoke steatohepatitis, and whether these mechanisms are operant in human NAFLD/NASH. As epidemiological evidence suggests impaired ketogenesis during the progression of steatohepatitis (Embade et al., 2016; Marinou et al., 2011; M�nnist� et al., 2015; Pramfalk et al., 2015; Safaei et al., 2016) therapies that increase hepatic ketogenesis could prove salutary (Degirolamo et al., 2016; Honda et al., 2016).
Ketone Bodies and Heart Failure (HF)
With a metabolic rate exceeding 400 kcal/kg/day, and a turnover of 6�35 kg ATP/day, the heart is the organ with the highest energy expenditure and oxidative demand (Ashrafian et al., 2007; Wang et al., 2010b). The vast majority of myocardial energy turnover resides within mitochondria, and 70% of this supply originates from FAO. The heart is omnivorous and flexible under normal conditions, but the pathologically remodeling heart (e.g., due to hypertension or myocardial infarction) and the diabetic heart each become metabolically inflexible (Balasse and Fery, 1989; BING, 1954; Fukao et al., 2004; Lopaschuk et al., 2010; Taegtmeyer et al., 1980; Taegtmeyer et al., 2002; Young et al., 2002). Indeed, genetically programmed abnormalities of cardiac fuel metabolism in mouse models provoke cardiomyopathy (Carley et al., 2014; Neubauer, 2007). Under physiological conditions normal hearts oxidize ketone bodies in proportion to their delivery, at the expense of fatty acid and glucose oxidation, and myocardium is the highest ketone body consumer per unit mass (BING, 1954; Crawford et al., 2009; GARLAND et al., 1962; Hasselbaink et al., 2003; Jeffrey et al., 1995; Pelletier et al., 2007; Tardif et al., 2001; Yan et al., 2009). Compared to fatty acid oxidation, ketone bodies are more energetically efficient, yielding more energy available for ATP synthesis per molecule of oxygen invested (P/O ratio) (Kashiwaya et al., 2010; Sato et al., 1995; Veech, 2004). Ketone body oxidation also yields potentially higher energy than FAO, keeping ubiquinone oxidized, which raises redox span in the electron transport chain and makes more energy available to synthetize ATP (Sato et al., 1995; Veech, 2004). Oxidation of ketone bodies may also curtail ROS production, and thus oxidative stress (Veech, 2004).
Preliminary interventional and observational studies indicate a potential salutary role of ketone bodies in the heart. In the experimental ischemia/reperfusion injury context, ketone bodies conferred potential cardioprotective effects (Al-Zaid et al., 2007; Wang et al., 2008), possibly due to the increase mitochondrial abundance in heart or up-regulation of crucial oxidative phosphorylation mediators (Snorek et al., 2012; Zou et al., 2002). Recent studies indicate that ketone body utilization is increased in failing hearts of mice (Aubert et al., 2016) and humans (Bedi et al., 2016), supporting prior observations in humans (BING, 1954; Fukao et al., 2000; Janardhan et al., 2011; Longo et al., 2004; Rudolph and Schinz, 1973; Tildon and Cornblath, 1972). Circulating ketone body concentrations are increased in heart failure patients, in direct proportion to filling pressures, observations whose mechanism and significance remains unknown (Kupari et al., 1995; Lommi et al., 1996; Lommi et al., 1997; Neely et al., 1972), but mice with selective SCOT deficiency in cardiomyocytes exhibit accelerated pathological ventricular remodeling and ROS signatures in response to surgically induced pressure overload injury (Schugar et al., 2014).
Recent intriguing observations in diabetes therapy have revealed a potential link between myocardial ketone metabolism and pathological ventricular remodeling (Fig. 5). Inhibition of the renal proximal tubular sodium/glucose co-transporter 2 (SGLT2i) increases circulating ketone body concentrations in humans (Ferrannini et al., 2016a; Inagaki et al., 2015) and mice (Suzuki et al., 2014) via increased hepatic ketogenesis (Ferrannini et al., 2014; Ferrannini et al., 2016a; Katz and Leiter, 2015; Mudaliar et al., 2015). Strikingly, at least one of these agents decreased HF hospitalization (e.g., as revealed by the EMPA-REG OUTCOME trial), and improved cardiovascular mortality (Fitchett et al., 2016; Sonesson et al., 2016; Wu et al., 2016a; Zinman et al., 2015). While the driver mechanisms behind beneficial HF outcomes to linked SGLT2i remain actively debated, the survival benefit is likely multifactorial, prospectively including ketosis but also salutary effects on weight, blood pressure, glucose and uric acid levels, arterial stiffness, the sympathetic nervous system, osmotic diuresis/reduced plasma volume, and increased hematocrit (Raz and Cahn, 2016; Vallon and Thomson, 2016). Taken together, the notion that therapeutically increasing ketonemia either in HF patients, or those at high risk to develop HF, remains controversial but is under active investigation in pre-clinical and clinical studies (Ferrannini et al., 2016b; Kolwicz et al., 2016; Lopaschuk and Verma, 2016; Mudaliar et al., 2016; Taegtmeyer, 2016).
�
Ketone Bodies in Cancer Biology
Connections between ketone bodies and cancer are rapidly emerging, but studies in both animal models and humans have yielded diverse conclusions. Because ketone metabolism is dynamic and nutrient state responsive, it is enticing to pursue biological connections to cancer because of the potential for precision-guided nutritional therapies. Cancer cells undergo metabolic reprogramming in order to maintain rapid cell proliferation and growth (DeNicola and Cantley, 2015; Pavlova and Thompson, 2016). The classical Warburg effect in cancer cell metabolism arises from the dominant role of glycolysis and lactic acid fermentation to transfer energy and compensate for lower dependence on oxidative phosphorylation and limited mitochondrial respiration (De Feyter et al., 2016; Grabacka et al., 2016; Kang et al., 2015; Poff et al., 2014; Shukla et al., 2014). Glucose carbon is primarily directed through glycolysis, the pentose phosphate pathway, and lipogenesis, which together provide intermediates necessary for tumor biomass expansion (Grabacka et al., 2016; Shukla et al., 2014; Yoshii et al., 2015). Adaptation of cancer cells to glucose deprivation occurs through the ability to exploit alternative fuel sources, including acetate, glutamine, and aspartate (Jaworski et al., 2016; Sullivan et al., 2015). For example, restricted access to pyruvate reveals the ability of cancer cells to convert glutamine into acetyl-CoA by carboxylation, maintaining both energetic and anabolic needs (Yang et al., 2014). An interesting adaptation of cancer cells is the utilization of acetate as a fuel (Comerford et al., 2014; Jaworski et al., 2016; Mashimo et al., 2014; Wright and Simone, 2016; Yoshii et al., 2015). Acetate is also a substrate for lipogenesis, which is critical for tumor cell proliferation, and gain of this lipogenic conduit is associated with shorter patient survival and greater tumor burden (Comerford et al., 2014; Mashimo et al., 2014; Yoshii et al., 2015).
Non-cancer cells easily shift their energy source from glucose to ketone bodies during glucose deprivation. This plasticity may be more variable among cancer cell types, but in vivo implanted brain tumors oxidized [2,4-13C2]-?OHB to a similar degree as surrounding brain tissue (De Feyter et al., 2016). �Reverse Warburg effect� or �two compartment tumor metabolism� models hypothesize that cancer cells induce ?OHB production in adjacent fibroblasts, furnishing the tumor cell�s energy needs (Bonuccelli et al., 2010; Martinez-Outschoorn et al., 2012). In liver, a shift in hepatocytes from ketogenesis to ketone oxidation in hepatocellular carcinoma (hepatoma) cells is consistent with activation of BDH1 and SCOT activities observed in two hepatoma cell lines (Zhang et al., 1989). Indeed, hepatoma cells express OXCT1 and BDH1 and oxidize ketones, but only when serum starved (Huang et al., 2016). Alternatively, tumor cell ketogenesis has also been proposed. Dynamic shifts in ketogenic gene expression are exhibited during cancerous transformation of colonic epithelium, a cell type that normally expresses HMGCS2, and a recent report suggested that HMGCS2 may be a prognostic marker of poor prognosis in colorectal and squamous cell carcinomas (Camarero et al., 2006; Chen et al., 2016). Whether this association requires or involves ketogenesis, or a moonlighting function of HMGCS2, remains to be determined. Conversely, apparent ?OHB production by melanoma and glioblastoma cells, stimulated by the PPAR? agonist fenofibrate, was associated with growth arrest (Grabacka et al., 2016). Further studies are required to characterize roles of HMGCS2/SCOT expression, ketogenesis, and ketone oxidation in cancer cells.
Beyond the realm of fuel metabolism, ketones have recently been implicated in cancer cell biology via a signaling mechanism. Analysis of BRAF-V600E+ melanoma indicated OCT1-dependent induction of HMGCL in an oncogenic BRAF-dependent manner (Kang et al., 2015). HMGCL augmentation was correlated with higher cellular AcAc concentration, which in turn enhanced BRAFV600E-MEK1 interaction, amplifying MEK-ERK signaling in a feed-forward loop that drives tumor cell proliferation and growth. These observations raise the intriguing question of prospective extrahepatic ketogenesis that then supports a signaling mechanism (also see ?OHB as a signaling mediator and Controversies in extrahepatic ketogenesis). It is also important to consider independent effects of AcAc, d-?OHB, and l-?OHB on cancer metabolism, and when considering HMGCL, leucine catabolism may also be deranged.
The effects of ketogenic diets (also see Therapeutic use of ketogenic diet and exogenous ketone bodies) in cancer animal models are varied (De Feyter et al., 2016; Klement et al., 2016; Meidenbauer et al., 2015; Poff et al., 2014; Seyfried et al., 2011; Shukla et al., 2014). While epidemiological associations among obesity, cancer, and ketogenic diets are debated (Liskiewicz et al., 2016; Wright and Simone, 2016), a meta-analysis using ketogenic diets in animal models and in human studies suggested a salutary impact on survival, with benefits prospectively linked to the magnitude of ketosis, time of diet initiation, and tumor location (Klement et al., 2016; Woolf et al., 2016). Treatment of pancreatic cancer cells with ketone bodies (d-?OHB or AcAc) inhibited growth, proliferation and glycolysis, and a ketogenic diet (81% kcal fat, 18% protein, 1% carbohydrate) reduced in vivo tumor weight, glycemia, and increased muscle and body weight in animals with implanted cancer (Shukla et al., 2014). Similar results were observed using a metastatic glioblastoma cell model in mice that received ketone supplementation in the diet (Poff et al., 2014). Conversely, a ketogenic diet (91% kcal fat, 9% protein) increased circulating ?OHB concentration and diminished glycemia�but had no impact on either tumor volume or survival duration in glioma-bearing rats (De Feyter et al., 2016). A glucose ketone index has been proposed as a clinical indicator that improves metabolic management of ketogenic diet-induced brain cancer therapy in humans and mice (Meidenbauer et al., 2015). Taken together, roles of ketone body metabolism and ketone bodies in cancer biology are tantalizing because they each pose tractable therapeutic options, but fundamental aspects remain to be elucidated, with clear influences emerging from a matrix of variables, including (i) differences between exogenous ketone bodies versus ketogenic diet, (ii) cancer cell type, genomic polymorphisms, grade, and stage; and (iii) timing and duration of exposure to the ketotic state.
Ketogenesis is created by ketone bodies through the breakdown of fatty acids and ketogenic amino acids. This biochemical process provides energy to various organs, specifically the brain, under circumstances of fasting as a response to an unavailability of blood glucose. Ketone bodies are mainly produced in the mitochondria of liver cells. While other cells are capable of carrying out ketogenesis, they are not as effective at doing so as liver cells. Because ketogenesis occurs in the mitochondria, its processes are regulated independently. Dr. Alex Jimenez D.C., C.C.S.T. Insight
Therapeutic Application of Ketogenic Diet and Exogenous Ketone Bodies
The applications of ketogenic diets and ketone bodies as therapeutic tools have also arisen in non-cancerous contexts including obesity and NAFLD/NASH (Browning et al., 2011; Foster et al., 2010; Schugar and Crawford, 2012); heart failure (Huynh, 2016; Kolwicz et al., 2016; Taegtmeyer, 2016); neurological and neurodegenerative disease (Martin et al., 2016; McNally and Hartman, 2012; Rho, 2015; Rogawski et al., 2016; Yang and Cheng, 2010; Yao et al., 2011); inborn errors of metabolism (Scholl-B�rgi et al, 2015); and exercise performance (Cox et al., 2016). The efficacy of ketogenic diets has been especially appreciated in therapy of epileptic seizure, particularly in drug-resistant patients. Most studies have evaluated ketogenic diets in pediatric patients, and reveal up to a ~50% reduction in seizure frequency after 3 months, with improved effectiveness in select syndromes (Wu et al., 2016b). The experience is more limited in adult epilepsy, but a similar reduction is evident, with better response in symptomatic generalized epilepsy patients (Nei et al., 2014). Underlying anti-convulsant mechanisms remain unclear, although postulated hypotheses include reduced glucose utilization/glycolysis, reprogrammed glutamate transport, indirect impact on ATP-sensitive potassium channel or adenosine A1 receptor, alteration of sodium channel isoform expression, or effects on circulating hormones including leptin (Lambrechts et al., 2016; Lin et al., 2017; Lutas and Yellen, 2013). It remains unclear whether the anti-convulsant effect is primarily attributable to ketone bodies, or due to the cascade metabolic consequences of low carbohydrate diets. Nonetheless, ketone esters (see below) appear to elevate the seizure threshold in animal models of provoked seizures (Ciarlone et al., 2016; D’Agostino et al., 2013; Viggiano et al., 2015).
Atkins-style and ketogenic, low carbohydrate diets are often deemed unpleasant, and can cause constipation, hyperuricemia, hypocalcemia, hypomagnesemia, lead to nephrolithiasis, ketoacidosis, cause hyperglycemia, and raise circulating cholesterol and free fatty acid concentrations (Bisschop et al., 2001; Kossoff and Hartman, 2012; Kwiterovich et al., 2003; Suzuki et al., 2002). For these reasons, long-term adherence poses challenges. Rodent studies commonly use a distinctive macronutrient distribution (94% kcal fat, 1% kcal carbohydrate, 5% kcal protein, Bio-Serv F3666), which provokes a robust ketosis. However, increasing the protein content, even to 10% kcal substantially diminishes the ketosis, and 5% kcal protein restriction confers confounding metabolic and physiological effects. This diet formulation is also choline depleted, another variable that influences susceptibility to liver injury, and even ketogenesis (Garbow et al., 2011; Jornayvaz et al., 2010; Kennedy et al., 2007; Pissios et al., 2013; Schugar et al., 2013). Effects of long-term consumption of ketogenic diets in mice remain incompletely defined, but recent studies in mice revealed normal survival and the absence of liver injury markers in mice on ketogenic diets over their lifespan, although amino acid metabolism, energy expenditure, and insulin signaling were markedly reprogrammed (Douris et al., 2015).
Mechanisms increasing ketosis through mechanisms alternative to ketogenic diets include the use of ingestible ketone body precursors. Administration of exogenous ketone bodies could create a unique physiological state not encountered in normal physiology, because circulating glucose and insulin concentrations are relatively normal, while cells might spare glucose uptake and utilization. Ketone bodies themselves have short half-lives, and ingestion or infusion of sodium ?OHB salt to achieve therapeutic ketosis provokes an untoward sodium load. R/S-1,3-butanediol is a non-toxic dialcohol that is readily oxidized in the liver to yield d/l-?OHB (Desrochers et al., 1992). In distinct experimental contexts, this dose has been administered daily to mice or rats for as long as seven weeks, yielding circulating ?OHB concentrations of up to 5 mM within 2 h of administration, which is stable for at least an additional 3h (D’Agostino et al., 2013). Partial suppression of food intake has been observed in rodents given R/S-1,3-butanediol (Carpenter and Grossman, 1983). In addition, three chemically distinct ketone esters (KEs), (i) monoester of R-1,3-butanediol and d-?OHB (R-3-hydroxybutyl R-?OHB); (ii) glyceryl-tris-?OHB; and (iii) R,S-1,3-butanediol acetoacetate diester, have also been extensively studied (Brunengraber, 1997; Clarke et al., 2012a; Clarke et al., 2012b; Desrochers et al., 1995a; Desrochers et al., 1995b; Kashiwaya et al., 2010). An inherent advantage of the former is that 2 moles of physiological d-?OHB are produced per mole of KE, following esterase hydrolysis in the intestine or liver. Safety, pharmacokinetics, and tolerance have been most extensively studied in humans ingesting R-3-hydroxybutyl R-?OHB, at doses up to 714 mg/kg, yielding circulating d-?OHB concentrations up to 6 mM (Clarke et al., 2012a; Cox et al., 2016; Kemper et al., 2015; Shivva et al., 2016). In rodents, this KE decreases caloric intake and plasma total cholesterol, stimulates brown adipose tissue, and improves insulin resistance (Kashiwaya et al., 2010; Kemper et al., 2015; Veech, 2013). Recent findings indicate that during exercise in trained athletes, R-3-hydroxybutyl R-?OHB ingestion decreased skeletal muscle glycolysis and plasma lactate concentrations, increased intramuscular triacylglycerol oxidation, and preserved muscle glycogen content, even when co-ingested carbohydrate stimulated insulin secretion (Cox et al., 2016). Further development of these intriguing results is required, because the improvement in endurance exercise performance was predominantly driven by a robust response to the KE in 2/8 subjects. Nonetheless, these results do support classical studies that indicate a preference for ketone oxidation over other substrates (GARLAND et al., 1962; Hasselbaink et al., 2003; Stanley et al., 2003; Valente-Silva et al., 2015), including during exercise, and that trained athletes may be more primed to utilize ketones (Johnson et al., 1969a; Johnson and Walton, 1972; Winder et al., 1974; Winder et al., 1975). Finally, the mechanisms that might support improved exercise performance following equal caloric intake (differentially distributed among macronutrients) and equal oxygen consumption rates remain to be determined. Clues may emerge from animal studies, as temporary exposure to R-3-hydroxybutyl R-?OHB in rats was associated with increased treadmill time, improved cognitive function, and an apparent energetic benefit in ex vivo perfused hearts (Murray et al., 2016).
Future Perspective
Once largely stigmatized as an overflow pathway capable of accumulating toxic emissions from fat combustion in carbohydrate restricted states (the �ketotoxic� paradigm), recent observations support the notion that ketone body metabolism serves salutary roles even in carbohydrate-laden states, opening a �ketohormetic� hypothesis. While the facile nutritional and pharmacological approaches to manipulate ketone metabolism make it an attractive therapeutic target, aggressively posed but prudent experiments remain in both the basic and translational research laboratories. Unmet needs have emerged in the domains of defining the role of leveraging ketone metabolism in heart failure, obesity, NAFLD/NASH, type 2 diabetes, and cancer. The scope and impact of ‘non-canonical� signaling roles of ketone bodies, including regulation of PTMs that likely feed back and forward into metabolic and signaling pathways, require deeper exploration. Finally, extrahepatic ketogenesis could open intriguing paracrine and autocrine signaling mechanisms and opportunities to influence co-metabolism within the nervous system and tumors to achieve therapeutic ends.
In conclusion, ketone bodies are created by the liver in order to be used as an energy source when there is not enough glucose readily available in the human body. Ketogenesis occurs when there are low glucose levels in the blood, particularly after other cellular carbohydrate stores have been exhausted. The purpose of the article above was to discuss the multi-dimensional roles of ketone bodies in fuel metabolism, signaling, and therapeutics. The scope of our information is limited to chiropractic and spinal health issues. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief. �
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine