According to healthcare professionals, metabolic syndrome is a collection of conditions or disorders that can increase the risk of developing a variety of health issues, including diabetes, stroke, and heart disease. A combination of several of these risk factors, such as high blood pressure, high blood sugar levels, and excess waist fat, can ultimately increase the risk of a patient being diagnosed with metabolic syndrome and its associated health issues.
What is Metabolic Syndrome?
Metabolic syndrome affects approximately 23 percent of adults and the most common underlying causes of this collection of conditions or disorders include, excess weight and obesity, sedentary lifestyle, genetic factors, and age. As previously mentioned above, having 3 or more metabolic syndrome risk factors can increase the risk of developing a variety of other health issues, including diabetes, stroke, and heart disease, among other health issues.
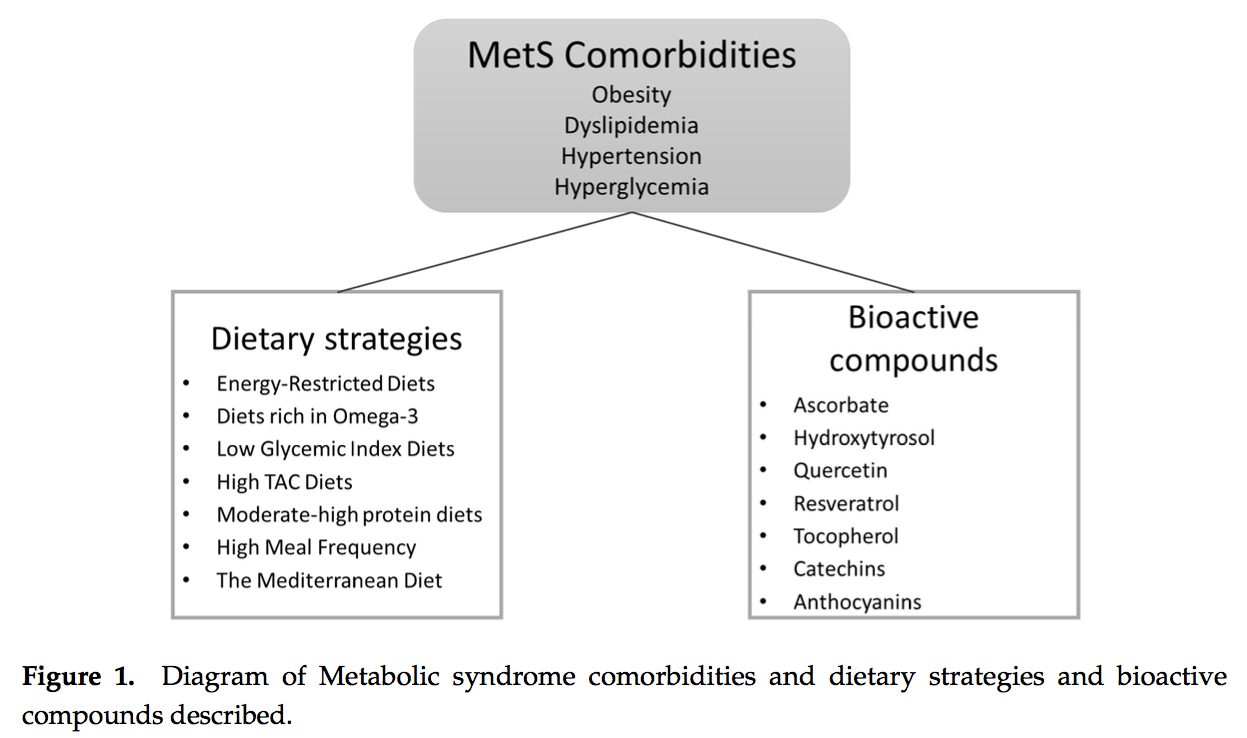
Metabolic syndrome is characterized by three or more of the following metabolic measurements, including:
Excess waist fat (> 40 inches in men, and > 35 inches in women)
High blood pressure (130/85 mm Hg)
Hight blood sugar or glucose levels (100 mg/dL or greater)
High triglyceride levels (150 mg/dL or greater)
Low HDL cholesterol (< 40 mg/dL in men or < 50 mg/dL in women)
The Importance of Understanding Metabolic Syndrome
Healthcare professionals diagnose metabolic syndrome when a patient has a collection of conditions or diseases that can increase the risk of developing diabetes, stroke, and heart health. Moreover, research studies found that people with metabolic syndrome have a much higher chance of developing these health issues compared with individuals who do not have metabolic syndrome. Chances increase when more of these risk factors are present.
Metabolic syndrome has become increasingly common in the United States. Several factors increase the likelihood of acquiring metabolic syndrome:
Excess weight/obesity. These are critical and potential causes of metabolic syndrome. Too much fat in the abdomen is most commonly associated with metabolic syndrome. The reasons why excess weight/obesity and metabolic syndrome seem to be linked are complex and misunderstood.
Insulin resistance: This has been closely associated with metabolic syndrome. Several people are genetically predisposed to insulin resistance.
Race and gender: People of certain races, as are men more than women, ultimately have�a greater risk of developing metabolic syndrome.
As previously mentioned above, people with metabolic syndrome have an increased risk of developing the following health issues, including:
Cardiovascular disease and heart attacks. If the arteries that supply blood to the heart are narrowed or blocked by fatty deposits, known as plaque, they decrease the amount of blood and oxygen reaching the heart, which can cause chest pain (angina) or a heart attack.
Type 2 diabetes. Diabetes is another well-known health issue that happens when the body can’t produce enough insulin or is unable to utilize insulin properly. This causes sugar to build-up in the blood and increases the risk of developing kidney failure and heart disease.
Metabolic syndrome is also commonly associated with another well-known health issue, known as insulin resistance. People with insulin resistance experience problems where their own body prevents itself from utilizing insulin efficiently. Healthcare professionals and researchers alike sometimes refer to metabolic syndrome as insulin resistance syndrome. Furthermore, high blood sugar and insulin resistance are associated with diabetes.
Diagnosis and Treatment of Metabolic Syndrome
Healthcare professionals will look for the presence of three or more of the following risk factors to diagnose metabolic syndrome, including:
Excess waist fat (> 40 inches in men, and > 35 inches in women)
High blood pressure (130/85 mm Hg)
Hight blood sugar or glucose levels (100 mg/dL or greater)
High triglyceride levels (150 mg/dL or greater)
Low HDL cholesterol (< 40 mg/dL in men or < 50 mg/dL in women)
Metabolic syndrome treatment requires addressing several risk factors that can increase the risk of developing a variety of health issues, including:
Eating better. Follow a diet rich in fruits, vegetables, whole grains, lean meats, skinless poultry, and non-fried fish as well as low-fat or fat-free dairy products. Avoid processed foods, which are often high in saturated and trans fats, sodium and added sugar, among other processed foods.
Get active. Add at least 150 minutes of exercise and physical activity to a regular routine. Walking is the easiest place to start but you may want to find something else that gets your heart rate up. If necessary, break your exercise and physical activity into several short, sessions throughout the day.
Lose weight. Learn your recommended calorie intake, the number of food calories you’re consuming, and the energy calories you’re burning off with different levels of exercise and physical activity. Balance healthy eating with a healthy level of exercise and physical activity to lose weight.
If diet and lifestyle modifications alone do not control the conditions or diseases associated with metabolic syndrome, a healthcare professional may ultimately prescribe drugs/medications to help control blood pressure, cholesterol, and other symptoms. Carefully following your healthcare professional’s instructions can help prevent long term effects of metabolic syndrome. Your hard work and attention will make a difference in overall health and wellness.
Approximately 23 percent of adults in the United States have metabolic syndrome. Although the risk factors for developing the cluster of conditions or diseases are significant, there are good news. Many of the risk factors associated with metabolic syndrome can be addressed through diet and lifestyle modifications, such exercise and physical activity. By making these changes, people can ultimately significantly reduce their risks of developing a variety of other health issues, including diabetes, stroke, and heart disease. Although metabolic syndrome can be a serious health issue, people can significantly reduce their risks by reducing their weight; increasing exercise and physical activity; eating a heart-healthy diet that’s rich in fruits, vegetables, whole grains, and fish; as well as working with a healthcare professional to regulate blood pressure, blood sugar, blood cholesterol.
Dr. Alex Jimenez D.C., C.C.S.T. Insight
According to healthcare professionals, metabolic syndrome is a collection of conditions or disorders that can increase the risk of developing a variety of health issues, including diabetes, stroke, and heart disease. A combination of several of these risk factors, such as high blood pressure, high blood sugar levels, and excess waist fat, can ultimately increase the risk of a patient being diagnosed with metabolic syndrome and its associated health issues.
The scope of our information is limited to chiropractic, musculoskeletal, and nervous health issues or functional medicine articles, topics, and discussions. We use functional health protocols to treat injuries or disorders of the musculoskeletal system. Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. To further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.�
Heart Staff. �Your Risk for Metabolic Syndrome.� Www.heart.org, Heart Media, 31 July 2016, www.heart.org/en/health-topics/metabolic-syndrome/your-risk-for-metabolic-syndrome.
Heart Staff. �Symptoms and Diagnosis of Metabolic Syndrome.� Www.heart.org, Heart Media, 31 July 2016, www.heart.org/en/health-topics/metabolic-syndrome/symptoms-and-diagnosis-of-metabolic-syndrome.
Heart Staff. �Prevention and Treatment of Metabolic Syndrome.� Www.heart.org, Heart Media, 31 July 2016, www.heart.org/en/health-topics/metabolic-syndrome/prevention-and-treatment-of-metabolic-syndrome.
Dr. Alex Jimenez Podcast: Metabolic Syndrome
Metabolic syndrome is a cluster of risk factors that can ultimately increase the risk of developing a variety of health issues, including heart disease, stroke, and diabetes, among other problems. Central obesity, high blood pressure, high blood sugar, high triglycerides, and low HDL or good cholesterol levels are the 5 risk factors associated with metabolic syndrome. Having at least three of the five risk factors may suggest the presence of metabolic syndrome. Dr. Alex Jimenez, Alexander Jimenez, Truide Torres, Kenna Vaughn, and Astrid Ornelas explain the 5 risk factors associated with metabolic syndrome, in further detail, as they recommend diet and lifestyle modification advice and guidelines, such as the ketogenic diet or the keto diet, as well as demonstrate the biochemical and chemical pathways that the body goes through during ketosis to help people with metabolic syndrome improve their overall health and wellness. From eating good fats and staying hydrated to exercise and better sleep, Dr. Alex Jimenez, Alexander Jimenez, Truide Torres, Kenna Vaughn, and Astrid Ornelas discuss how diet and lifestyle modifications, such as the ketogenic diet or keto diet, can help improve the 5 risk factors associated with metabolic syndrome to prevent the risk of developing a variety of other health issues, including heart disease, stroke, and diabetes. – Podcast Insight
Neural Zoomer Plus for Neurological Disease
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention.
Food Sensitivity for the IgG & IgA Immune Response
Dr. Alex Jimenez utilizes a series of tests to help evaluate health issues associated with a variety of food sensitivities and intolerances. The Food Sensitivity ZoomerTM is an array of 180 commonly consumed food antigens that offers very specific antibody-to-antigen recognition. This panel measures an individual�s IgG and IgA sensitivity to food antigens. Being able to test IgA antibodies provides additional information to foods that may be causing mucosal damage. Additionally, this test is ideal for patients who might be suffering from delayed reactions to certain foods. Utilizing an antibody-based food sensitivity test can help prioritize the necessary foods to eliminate and create a customized diet plan around the patient�s specific needs.
Gut Zoomer for Small Intestinal Bacterial Overgrowth (SIBO)
Dr. Alex Jimenez utilizes a series of tests to help evaluate gut health associated with small intestinal bacterial overgrowth (SIBO). The Vibrant Gut ZoomerTM offers a report that includes dietary recommendations and other natural supplementation like prebiotics, probiotics, and polyphenols. The gut microbiome is mainly found in the large intestine and it has more than 1000 species of bacteria that play a fundamental role in the human body, from shaping the immune system and affecting the metabolism of nutrients to strengthening the intestinal mucosal barrier (gut-barrier). It is essential to understand how the number of bacteria that symbiotically live in the human gastrointestinal (GI) tract influences gut health because imbalances in the gut microbiome may ultimately lead to gastrointestinal (GI) tract symptoms, skin conditions, autoimmune disorders, immune system imbalances, and multiple inflammatory disorders.
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
For your convenience and review of the XYMOGEN products please review the following link. *XYMOGEN-Catalog-Download
* All of the above XYMOGEN policies remain strictly in force.
Modern Integrated Medicine
The National University of Health Sciences is an institution that offers a variety of rewarding professions to attendees. Students can practice their passion for helping other people achieve overall health and wellness through the institution’s mission. The National University of Health Sciences prepares students to become leaders in the forefront of modern integrated medicine, including chiropractic care. Students have an opportunity to gain unparalleled experience at the National University of Health Sciences to help restore the natural integrity of the patient and define the future of modern integrated medicine.
Metabolic syndrome is a cluster of risk factors that can ultimately increase the risk of developing a variety of health issues, including heart disease, stroke, and diabetes, among other problems. Central obesity, high blood pressure, high blood sugar, high triglycerides, and low HDL or good cholesterol levels are the 5 risk factors associated with metabolic syndrome. Having at least three of the five risk factors may suggest the presence of metabolic syndrome. Dr. Alex Jimenez, Alexander Jimenez, Truide Torres, Kenna Vaughn, and Astrid Ornelas explain the 5 risk factors associated with metabolic syndrome, in further detail, as they recommend diet and lifestyle modification advice and guidelines, such as the ketogenic diet or the keto diet, as well as demonstrate the biochemical and chemical pathways that the body goes through during ketosis to help people with metabolic syndrome improve their overall health and wellness. From eating good fats and staying hydrated to exercise and better sleep, Dr. Alex Jimenez, Alexander Jimenez, Truide Torres, Kenna Vaughn, and Astrid Ornelas discuss how diet and lifestyle modifications, such as the ketogenic diet or keto diet, can help improve the 5 risk factors associated with metabolic syndrome to prevent the risk of developing a variety of other health issues, including heart disease, stroke, and diabetes. – Podcast Insight
[00:00:14] All right, guys, we’ve come to another podcast. And welcome to Dr. Jimenez and crew podcast. Welcome. And you have a family here.
[00:00:23] We’re gonna go over metabolic syndrome today. Metabolic syndrome is a disorder that ultimately affects a whole lot of people. What happens is it actually affects one of the largest populations in El Paso, pretty much in this region. And what we have is, it’s not a disease. OK. First of all, it’s a combination of presentations that medical doctors and the World Health Organization have determined that high-risk factors in order to have a stroke, kidney disorders and even problems with dementia. But overall, it’s pretty much if you have metabolic syndrome, you really feel crummy. So today what we’re going to do is we’re gonna discuss the issues and we’d like to at least present it to you so that it becomes useful for you. And the information provided by us is going to be helpful for you or a family member. So if you have the opportunity and it’s something that you enjoy, please go ahead and at the bottom area, there’s a little bell to subscribe and a little belt in markets so that you could be the very first person to get information in the future when we ever post it. And it also gives you the opportunity to present or ask us for things that are important to you in the health-related realm. And now what we’re going to do today, my name is Dr. Alex Jimenez, I have my entire staff here. We’re gonna go ahead and we’re going to present each one of them in different moments. And we’re gonna do some really interesting dynamics. We also have our resident biochemist at the National University of Health Science who’s actually going to chime in, who’s gonna give us a little bit of a foundation about chemistry. This information is gonna be helpful. We’re gonna try to make it as simple but as useful as possible. Now, bear in mind everything that we’re gonna be talking about today revolves around the metabolic syndrome. Metabolic syndrome is what the health care organizations have determined as well as the cardiac departments have determined, as five major symptoms, now, you have to have three of them at least in order to be classified as metabolic syndrome. Now, the first thing is to ask, what do you feel? Pretty much you feel like crap. And it’s not really a good feeling to feel this way, but you’ll see that if you have some of these presentations, you’re gonna notice that your doctor may give you a diagnosis of metabolic syndrome. Now, the first thing that happens is you have usually a little bit of belly fat. Now, the belly fat that people have, people measure it. Now, for men, it’s a belly, kind of like the lonja, the belly that actually hangs over. And it’s about a good I’d say about 40 inches or greater in the male, in women it’s 35 inches or more. Now, that’s one of the first presentations. Now, the other presentation is high blood pressure. Now the high blood pressure that they use is 135 milligrams over deciliter. Oh, sorry. Yeah. Miller Mercury’s millimeters or Mercury or the slaters over to determine exactly the diastolic and the systolic. So the systolic is gonna be 135. The diastolic is going to be over 85. Now that doesn’t, again, you’re gonna notice something. These aren’t really extreme ranges. Okay. Now metabolic syndrome has high triglycerides. Now the high triglycerides are going to be noted in the blood. Okay. Now one of the things that can be determined early on is high blood pressure which is also a study associated with metabolic syndrome. So the other final one is the elevation of or decrease actually of HDL or the good fragments of cholesterol. Alexander is going to be a resident biochemist, is going to talk to us a little bit more about that in the latter part of the show. Now, bear in mind, I’ve given five things A, fat, B, high blood pressure, C, the blood glucose levels and also the triglycerides along with the lowering of the HDL. The question is, how are we going to be able to control this? Now, I want to give you some real good basic ways that you can actually control metabolic syndrome. And by the time we’re done today, we’re going to be able to assess the situation. And even if you have it, you basically will be able to control it. There are rare diseases that you can actually have. And again, this is not a disease. It’s a combination of syndromes or symptoms, collectively called a syndrome. So metabolic syndrome is one that can be misconstrued. Now, you’ll notice that the level of blood glucose is going to be elevated, usually over a hundred. Now, these are really relatively normal numbers that people have. But if they’re higher than that, they do create issues. Now, also, when you have the belly fat 40, that much. A lot of people have it. People have also blood glucose levels that are higher than 5.6 on your blood glucose when we would see now these numbers, along with the 150 milligrams per deciliter of triglycerides, they’re all normal. But in combination together, they do ultimately create a scenario that is not favorable to a cardiac issue. Cardiovascular issues do present as a result. So what we’re gonna try to do is try to bring down and control these issues. Now, what are the things that cause metabolic syndrome? Well, one of the things is stress, smoking, a sedentary lifestyle, and also even sleep problems and disturbances. Each one of these we’re going to be elaborating in the future podcasts but we’re gonna be able to tell exactly what’s actually going on in a better way. We also have issues of inflammation and processed foods. Now, at the core, metabolic syndrome, the main issue is insulin sensitivity issues along with high blood pressure issues and inflammation. So what are we going to do to control that? I want you to know that every single one of these five issues, whether its blood glucose, high triglycerides, low HDL counts or blood glucose, they’re all relatable to one disorder. It’s insulin sensitivity, insulin sensitivity controls every one of these factors from raising high blood pressure, the kidneys actually are controlled by the insulin causing their increase in blood pressure. We’ll discuss that issue and the correlation of it so we can bring ourselves to control the blood glucose. We ultimately have the fastest and the surest way to provide the fastest route to heal and to fix an individual with metabolic syndrome. So let’s go ahead and talk about the issues that are going to be resulting from that. Now, as I’ve got this, we’re gonna notice that if over a period of time you continue to have a lifestyle that has high levels of these particular five factors, you’re going to notice that you’re going to tend to have high cardiac risks. Now we have a team here and I want to introduce each one. We have Kenna Vaughn, who is our health coach. Our health coach is the one that’s going to be the one that explains to our patients what is going on. I’ll bring her in. We also have the clinical liaison, which is Truide Torres, the individual that is going to be able to bring out and ask the questions and determine what kind of issues and treatments are appropriate for you. So we’ll be discussing those. And we have our resident chief editor Astrid Ornelas, who’s gonna be the one that also explains the studies on it. All the way from Illinois. We also have Alexander, which we have here. Right. We added the backway. You can’t see him, but he’s presenting in. Say Hello, Alexander. You got him there. Hello. All right. So he’s out there. He’s going to be able to discuss the issues on the biochemistry side of things. And we’re looking forward to being able to explain those issues. Now, one of the things we have to do is go back to the issue of insulin sensitivity. Insulin sensitivity is at the root of all these issues. So what we’re gonna do is we’re going to discuss exactly how insulin can actually be controlled. But what we’ve learned through these studies and I’m going to bring in Mrs. Ornelas here to discuss the studies that we have pertaining to how to control blood glucose and blood sensitivity study. What did you find out recently that actually shows the proof and actually presents the easiest way to control blood, insulin and elevate HDL?
[00:08:08] OK. Well, first of all, just as you mentioned, metabolic syndrome, it’s a collection of health issues that can increase the risk of developing heart disease, stroke, and diabetes. Basically like, you know, it can affect our overall health and wellness.
[00:08:29] And I’ve done quite some research. And I’ve found through the National Center of Biotechnology Information, the NCBI, there’s a variety of research which basically states that metabolic syndrome or people with metabolic syndrome, one of the easiest, you know, quote-on-quote, easiest. Or one of the best ways maybe out there that can be used to help.
[00:09:04] Restore it, yeah, to help restore or reverse your metabolic syndrome would be through the ketogenic diet, or the Keto diet, as a lot of people know it best by. It is a low carbohydrate, high-fat diet, which according to research studies, offers many benefits to people with metabolic syndrome.
[00:09:28] It can help improve or promote weight loss. And it can help reduce diabetes.
[00:09:38] Basically, you know what I mentioned right there?
[00:09:42] I have found nothing faster to lower blood glucose and actually reverse triglycerides issues in HDL issues. Than the ketogenic diet. So in essence, if you want to do it fast, it’s amazing the speed at which it restores the body back. What else is there?
[00:10:00] Yeah. Yeah. Yeah. So basically the human body normally uses glucose or sugar. It is supposed to be our main source of fuel. Our main source of energy. But for people that have metabolic syndrome. People who have obesity. Insulin resistance. Diabetes or an increased risk of diabetes. The ketogenic diet can be very beneficial towards that because the ketogenic diet, first of all, it is a low carbohydrate diet. Carbohydrates essentially turn into sugar or glucose and we don’t want that.
[00:10:41] Like if people have metabolic syndrome, they have, you know, diabetes and insulin resistance. You don’t want sugar in their bodies because they produce too much of it. They have too much blood sugar.
[00:10:53] But by increasing the number of fats that you eat and then decreasing the number of carbohydrates, you actually keep a low amount.
[00:11:05] If you keep insulin low by eating more fats, you basically make the body go into a state of ketosis.
[00:11:18] You know what? Let me ask you something. I’m going to feed this over to right now to Kenna. And I’m gonna ask Kenna. Kenna, in your experiences with the blood sugar issues, how is it that we contain and we learn to be able to manage someone’s blood sugar the quickest, the fastest? What is it that you do in terms of coaching individuals, helping them back by coaching individuals?
[00:11:41] I definitely always evaluate their diet. And the main thing I like to focus on is education because so many people are not educated about, as she was saying, carbs and how they actually feed your body. A Big Mac might have 54 carbs and a sweet potato might have 30 carbs. And people don’t really realize that they’re that different. They only see 20 points or something like that. But the way that the carbohydrate breaks down in the body is huge. And that’s why the ketogenic diet works so well because you’re using those good carbs that are going to actually contain protein as well. And so it’s going to help to break it down slower versus a Big Mac, which is just going to spike your insulin way out.
[00:12:23] And what part of the Big Mac is the thing that spikes the sugar? I mean, in terms of.
[00:12:26] Right. So the bread, the carbs in the bread, it actually breaks down differently in the body than a sweet potato would. And so that’s what’s going to give you that high glucose level. And then after that, you’re gonna have the fall of the glucose level, which just your blood sugar going up and down does not feel great.
[00:12:43] So it’s not good. Of course, you’re paying for the sugars. When you ask the types of sugars that you have. You just mentioned right now that the quality of the type of carbohydrate matters.
[00:12:52] Yes, a little bit about the quality. Like I was saying, sweet potatoes, avocados, things like that. They’re going to have the carbohydrates that are better for you, meaning you break them down differently than you would faster sugar like sucrose and things like that.
[00:13:12] So simple sugars are out, basically, which is the reason that, first of all, metabolic syndrome did not even exist prior to the advent of refined foods. So refined sugars have caused this problem. So what we want to do is, sugar leads to inflammation. Sugar leads to triglyceride issues, sugar or basically insulin sensitivity issues are the things that are the basis of this process. All roads lead to insulin sensitivity in this process and in the organ that provides us with insulin. The greatest amount is in the pancreas. The pancreas is nonstop. And depending on how the pancreas responds to this blood sugar drama, it really determines the fate of the individual. It will alter the triglycerides. They will alter the blood pressure by having a direct effect of holding sodium in the kidneys. The body prepares, it retains the sodium, and by nature of sodium, the blood pressure soars, so the fastest way to lower your blood pressure is a ketogenic diet. And this is amazing because it really is simple. It’s not that complex. We can go extreme. And I know that our state really had a good research document on that. Tell me a bit about what you noticed.
[00:14:24] Yeah, basically, like what I was saying before. A lot of people don’t know the difference between what type of carbohydrates they want to eat. Like, for example, as you said, you know, a lot of people will eat a Big Mac and don’t eat that sweet potato. And they don’t know the difference between a good carbohydrate. Basically, we want to eat what you call complex carbohydrates. We want to eat whole wheat or we want to eat good starches because the body breaks those down into glucose, into sugar. But they’re used much more slowly. The body won’t immediately use them. And then you’ll get that crash, that sugar crash, because of the insulin spike.
[00:15:11] Right. So that controls the spike. You know what? I want to bring in our resident biochemist here. OK, so our biochemist is Alexander. He’s got a presentation here, actually, if I can see it there and see if it pops up here. Let me see it. And there he is. Alex, can you tell us a bit about what you’re trying to explain here on the biochemistry side of things?
[00:15:30] So as you guys were mentioning, just in general. Glucose is the main energy source in the way that we use it for the breakdown. Its breakdown of energy consumption is called glycolysis. So without getting too much into it, our end goal here is pyruvate, which then goes into the citric acid cycle to be turned into an acetyl-CoA in normal conditions. It’s good to have a carbohydrate meal, but in excess, you produce too much acetyl-CoA. When too many acetyl-CoA is used? You end up inducing fatty acid synthesis which is induced by large levels of insulin. So by doing so, you have an acetyl-CoA that ends up turning into palpitate. And one thing that I was mentioning is that not all foods are of equal quality. So here we can kind of see all the different types of fatty acids. So without going too much into the biochemistry, but kind of just giving you an idea of what’s going on here, these numbers on the left side represent the number of carbons in a row and then the numbers to the right of the semicolon are the number of double bonds. And normally double bonds will play a large role until you get into the effect of digestion in the way the body uses these. So by having more double bonds, it’s more fluid. So you notice the difference between a piece of lard and olive oil. What’s the difference? The only difference really is the number of carbons and the number of double ones. So here we have olive oil and then we have some sort of saturated fat. We can see that the difference is large in the number of carbons as well as double bonds. Double bonds allow for a lower melting point. That’s why olive oil is a liquid at room temperature vs. fatty acids and this plays a large role when it comes into how the body uses these types of things.
[00:17:26] Alex, are you saying that, obviously we all know that the good work of olive oil and avocado oil and coconut oil are the best thing. Is this the reason why this happens?
[00:17:35] Exactly. So the more double bonds they have, the more fluid it is going to be within the body and allow for the body to use those fats in a timely manner versus clogging up arteries and creating plaques within those arteries?
[00:17:48] Excellent. You know what? One of the things that insulin does? It packs away carbohydrates and energy in the cell. If you do that, what happens with this blood sugar? Eventually, insulin spikes it and puts it in the cells. Eventually, the cell grows. Hence the belly fat. That is ultimately what happens to the belly, it starts gaining fat cells and they start getting bigger, bigger, and bigger because they get injected in there. That stuff starts seeping out and once it can’t go anymore, it ends up in places like the pancreas. It ends up in places like the liver. It ends up in the intramuscular, in the muscular tissue. And that’s why we have the accumulation. And when you have a big belly, that’s what tips off the doctor, not only with the triglycerides and the blood glucose levels but also the belly fat. And that’s one of the things we have to kind of assess. So is this.
[00:18:36] Now, these fatty acids, which are fatty acids used for, almost everything within the body, especially for energy consumption. It’s like saying, would you rather be able to go five miles or 10 miles a week? Or go 10 miles. Right. And so gram for gram fat as an energy source is much more fuel-efficient and glucose or carbs.
[00:19:04] So carbs provide four grams of calories per gram and fats are around nine. So it’s almost more than double, the amount of energy that you’re producing from these sites, from these fatty acids. The difficult part is just knowing which ones are good. So kind of going into the good fatty acids which are going to be the ones with the double bonds. So I mean, any plant oils, animal fats, depending on which ones, we tend to want to stay away from large amounts of acid that tend to cause inflammation responses through the inflammation path. But the rest of these are really, really good, especially EPA and DHA. So DHA is actually used within the nervous system. It’s turned into neurotic acid any day as well. So getting these marine oils are really, really going to be good for your system just in general.
[00:19:55] You know what, as I understand these processes and I start realizing the biochemistry behind it, bring it home to this process, down to the cellular component it honors and it shows appreciation in terms of what creates the fatty acid excess. Now, again, what happens as a result of too much of these fatty acids or carbohydrates in the bloodstream? The body tries to store it in the form of fat and it’s shoved into the pancreas. So you get this fat inside the pancreas. If it can’t do it there, it eventually puts it in the liver. And like we mentioned, it gets it in the stomach or that’s when we see it as a final thing. I’d like to take the explanation and break apart one other point. The high blood pressure component. Insulin has a direct effect on the kidneys. Insulin tells the kidneys.
[00:20:43] Look, we need to pack this stuff into the fat and without getting beyond too much of the chemistry dynamics. You can see that what’s going to occur is that the kidneys are going to be commanded to hold more sodium. What we learned in chemistry and in biochemistry and in clinical sciences that the more sodium we retain, the blood pressure rises. In essence, that’s how quick the blood pressure goes. So you do that for a period of time and then you force the collection of atherosclerotic plaques because of the fat that is in there and it can’t go anywhere. You’re going to have a problem in the long-term future. So speaking about the oils, as Alexander just did, one of the things we ask, well, what oils do we not want to use? Canola oil, corn oil, sesame seed oil. I love sesame seeds. But the problem is that sesame seed oil causes inflammation, as Alex said, with acids. So what we got to do is we got to figure out exactly what types of oils we can do. And avocados, as Kenna had mentioned, are a great source of fats that we can use and make things more able to be processed. Our bodies and the old pyramid of diet is really bad because it’s heavy on carbohydrates. So one of the things that we look at is maintaining all those components. So we talked about the triglycerides, right? We talked about the belly fat, how it’s put together. And in each one of these, I wanted to point this out again. Each one of these, the high blood pressure, which is 135, high blood pressure is not considered high. High blood pressure at 135 usually it’s at 140, OK. So, why are we using triglycerides at 150 are not considered excessive. You know, HDL is lower than 50 are not considered horrible, but in combination together, if you have one at all, these three of these components out of the five, that’s what leads to a preposition of being sick and feeling crummy, let alone any prolonged period of this will end up leading to metabolic disorders, heart problems, stroke problems, dementias that actually occur as a result of prolonged metabolic syndrome, states that are within the individual. I know Alexander when I ask Alexander, he’s got some really interesting dynamics as I want to present right now. I’m going to show his screen right here because he’s got some interesting components on what also affects metabolic syndrome.
[00:23:00] Alexander. So kind of going into what it is, I guess, ketosis, because everyone wonders kind of what goes on. So I kind of got this diagram here to draw for you guys. We’re going to ignore the Federer pathway over here, but just in general. So what’s going to happen first is you’re going to deplete any glucose that you have. So the body normally stores around 100 grams of glucose in the liver and around 400 grams within the muscle components of the entire body. So if you times, 500 times four, that’s about 2000 calories, which is your daily limit. So you’ve got about a day worth of glucose always stored within your body. But once you deplete that, your body’s gonna start looking for other things. In the meantime, it takes a few days for your body to switch over from burning sugar, which is glucose, to burning ketone bodies from fat. So what’s going to happen? Your, first of all, your adrenals are releasing epinephrine, its precursor is norepinephrine. And it causes a couple of different things?
[00:23:56] You’re gonna get a little jittery at first and you can feel really bad for the first couple days. But then your body is gonna start switching over as your brain starts to start using these ketone bodies for its energy source. So as you’re producing norepinephrine, these are just like this is the cell surface here. These are just different precursor markers. So we have B1, B2, B3 and eight. So by doing these, they’re going to mark and signal to the G.S. protein, which is going to allow for adenosine class to activate ATP into cyclic AMP. Now, cyclic AMP is a very important component of degradation of fatty acids and the cool part is it’s actually inhibited by phosphodiesterases. So when people come in and say, why is caffeine a good fat burner? The main reason why is because caffeine actually inhibits phosphodiesterase to a certain extent. You don’t want to go too crazy with the caffeine and start doing lots of cups.
[00:24:52] Alex should I have like 8 glasses of coffee or how many?
[00:24:56] I think one glass of coffee is definitely more than enough. So by having cyclic AMP more active, you end up activating this thing called protein kinase which activates ATP and then it activates hormone-sensitive light base, once hormone-sensitive light base is activated. It begins degradation against a breakdown, fatty acids. Once these fatty acids enter and are broken down, they then become they then enter into the mitochondria and the mitochondria will then end up producing heat from this. So that’s why people who are in ketosis are always really warm. So what do I recommend when people are starting Keto. Ketosis Diet, Water, Keto diet. Definitely water. And as well as I would say L-carnitine. So as we’re looking at L-carnitine here, we could see that during fatty acid degradation you use L-carnitine as a main transporter between the outer mitochondrial membrane and the inner mitochondrial membrane. So by using fatty acids here, fatty acetyl-CoA after we’ve broken down these fatty acids. It’s going to enter CBT-1 which is carnitine. Poly transferase one. It’s going to enter and interact with carnitine and then it’s gonna turn it to acetylcarnitine. Once acetylcarnitine turns into it that it can enter the inner mitochondrial membrane through these two enzymes translocated and CPT-2 to be broken down back into acetyl-CoA, which is the same biproduct as glucose eventually.
[00:26:29] So then your mitochondria can use these in beta-oxidation. One thing to note is you have to drink a lot of water because people who are going through ketosis are going to be up-regulating the urea cycle. So you need to make sure that you drink a lot of water throughout the day. I would say anyone who’s doing it could drink a minimum of a gallon of water throughout the day. Not all at once. Throughout the day.
[00:26:51] It’s amazing, Alex, that you put that together because that makes perfect sense to me. And also explains why people do say when we put them on the ketogenic diet that they do increase body temperature and the water obviously helps you kind of keep the whole system pumping because that’s what we’re pretty much made of. And also the pathways that you indicated, the hydrogen in the water are necessary for the process to occur.
[00:27:15] Yes. Yes. There are certain aspects within each of these that they fuel each other, it’s all an interconnected pathway. But you will up-regulate the urea cycle during ketosis much more than when you’re not. For example, cats are notoriously known for having a rancid urine smell.
[00:27:37] And we have to take a look at that from the reason why. Right. So, in general, in humans, the urea contents in our urine is 3 percent. In cats, on the other hand, it’s anywhere between 6 to 9 percent. You have to think about it. What is the only mammal on the planet that is a carnivorous animal that only eats meat? The feline family.
[00:27:57] So since they only eat meat, they upregulate the urea cycle, thus having more urea in their urine. So if you’re only a meat-eater, you’re gonna have more urea. Thus you need to drink more water to flush it out through your kidneys.
[00:28:09] That’s amazing because it explains why we make sure that everybody drinks a lot. And then they feel better. And I guess if we don’t monitor it. Right, if we don’t do it right. We get that thing called the ketogenic flu. Right. And then the body just feels kind of crummy until it restores and it stabilizes the blood glucose through ketones. Now, the body can use ketones for sugar as it’s known. So one of the things that we do is we teach the people exactly how to go through the process. And I know we got some research articles here. And Astrid wants to discuss a little bit about that.
[00:28:42] So basically, as Alex mentioned, when people start following the ketogenic diet.
[00:28:49] You know, as he said, we want to make sure that they stay hydrated. But more so than that.
[00:28:56] I guess another thing that we want to educate people on is that not a lot of people know that we need to store up the body with good fats so that as the body adjusts, it starts up basically burning fat as a fuel rather than sugar or glucose. So we want to teach people what are the good fats that we want them to basically eat because like we need to store up fat in these parts so the body can go into ketosis and it can go through the whole process that Alex just explained.
[00:29:39] You know what? I’d like to bring Truide here because she’s the one that actually connects with the patients at the moment. We do assess someone to have metabolic syndrome in terms of the resources. How do we? How do you go through the process of presenting? Hello, Truide. And what we’re gonna do there is going to ask you, how do you bring this? Because she’s our clinical liaison, our wellness liaison. And she’s the one that basically is going to give us the information that helps the patient in the right direction.
[00:30:05] Well, hello. You know, it is all great information. And, you know, which is amazing that we are able to provide this to the public. And I know this can be very overwhelming for people that don’t have this information. So that’s where I come in. When people come, you know, either call us or come in inquiring about different symptoms that they have. They don’t necessarily know that they’re experiencing metabolic syndrome. But, you know, one of the main concerns is their weight gain based on their concerns. I connect them either to their primaries, which is Kenna, and they go ahead and say, OK, well, what is it that, what are the steps that we have to take and Kenna certainly educates them as far as ok this is your lab work, we’re going to have to take, we connect them with Dr. Jimenez. After we know exactly what is their main concern. And we’re going to start kind of peeling things apart like an onion to get to the bottom of things and get them feeling better. They’re not only going to walk away with the specific results, but they’re also going to walk away with like what Astrid was saying, what are the good fats to have? What should I be eating? They’re going to be walking away with a lot of information, but also structure. Another thing that we’re offering is that Kenna is always going to be there to answer any questions. And also, Dr. Jimenez. So they don’t have to feel overwhelmed with the processes they’re going through for a better, healthy lifestyle.
[00:31:27] You know what? That’s one of the things is it’s, there’s a lot of confusion out there. And I got to be honest with you, there’s a lot of misinformation out there. This misinformation can be categorized as intentional or kind of old or not. It’s just not up to date with these five elements and an individual having three of them. It’s very important to make it repeat. Exactly how to fix this issue with the individual and how to change your lives, because there’s nothing quicker to change the body than the ketogenic diet. We also have to monitor the individuals with the monitor them through the process. Now we have Kenna Vaughn that she’s got some methods that we use, that we employ in the office and are useful for that. Doctors do this around the country, but it’s very helpful in helping guide and allow for interaction and communication between us, the providers and the patient. What kind of things do we offer?
[00:32:18] We have one on one coaching, which is great for when you’re just starting something out like they were talking about the ketogenic diet. You might be confused and there is misinformation. So what this one on one coaching, it’s great because we can connect through an app that we have and you just pull out your phone. You can send a quick text message, hey, I saw that I could one website said that I could eat this, but another said this. Can I have this? Things like that. We can clear up that confusion fast, which can really keep you on track rather than doing that guessing game. We also have scales that connect to this app which allows us to monitor the water weight that they have as well as the fat that they have. And we can also monitor their activity through a wristband that we can constantly check the steps that they’re taking. Make sure that they’re doing exercise because exercise is also great to help lower blood glucose level.
[00:33:08] You know, you mentioned that about the monitoring. We do that in the office along where we send the patients home with actual scales that actually are BIAs. Many BIAs along with their hand and wrist. We can pretty much for those patients that want to have a connection with our office. We directly can get the information downloaded and we can actually see their BIAs changing. We also use the InBody system, which we do a deep analysis of the basal metabolic rate along with other factors that we’ve discussed on prior podcasts. This allows us to put together a quantifiable method to assess how the body is changing and a very quick way of restoring the body back to or away from metabolic syndrome episodes. It’s a very uncomfortable feeling. It really can. There’s nothing that destroys the body as these combination of issues at one time. However, it’s easy to see that the body does everything really quickly and it fixes, a ketogenic diet removes body weight. It decreases the fat in the liver, it decreases the intramuscular fat, it restores the blood sugar. It gets the mind working better. It actually helps the HDL through some studies. And I know that Astrid knows there’s a study out there that actually pulls the information up on the on how the HDL is actually are actually elevated with and with a ketogenic diet. We have a study here actually presented put it on the screen right there that I think you found that actually shows that the HDL. Am I correct? And the apple protein, the lipid part of the HDL also is raised and activates the genetic component. Tell me about that.
[00:34:53] So basically something that a lot of researchers, something that a lot of health care professionals out there, doctors, they often say is that people have high cholesterol.
[00:35:07] You know we’re usually talking about the bad cholesterol and they have high-bat cholesterol or the LDL. It’s generally associated with the genetic predisposition, like according to several research articles out there. If your parents, if your grandparents had high cholesterol, there is also like an increased risk of you having a genetic predisposition to already having high cholesterol plus like add that like your diet. And if you have if you follow a sedentary lifestyle and you don’t do it enough exercise or physical activity, you do have an increased risk of having higher bad cholesterol.
[00:35:59] You know, I’m going to pull the information from my notice that Alexander is pulling something information up here on the screen. And he’s actually presenting the monitor where you can actually see his blood glucose and the screens that he’s going. Go ahead and put that up there for him. There you go. Alex, tell me which you’re talking about right there. I see that you’re talking about the apoprotein and the lipoproteins and the HDL fragments there.
[00:36:23] So I’m kind of going into a little bit of everything here. So what happens when you eat something that is going to cause an increase in cholesterol? So first of all, is you have these genes called kilomicrons that are within the intestinal lumen or within your GI tract. And they have apoprotein B-48. The reason they have 48 percent of apoprotein B 100. So it’s just a little different variation. These kilomicrons are actually going to bring these in through the body and transfer it into the capillaries using apoprotein C2 and apoprotein E once they enter the capillaries. They are going to degrade and allow for different aspects of the body to use them. So I have three tissues. We have adipose tissue, cardiac tissue, and skeletal muscle.
[00:37:14] So cardiac tissue has the lowest KM and adipose tissue has the highest KM. So what is KM? KM is just a measurement of the way that the enzymes use. So a low KM means a high specificity for binding to these fatty acids and a high KM means that it has a low specificity for them. So what are the three parts of the body they use the most energy?
[00:37:40] It’s the brain, the heart, and the kidneys. Those are the most caloric consumption parts of the body. Just to stay alive. So first of all, the heart relies large amounts on these fatty acids here.
[00:37:52] And transferring them to the heart uses mostly fatty acids. I think it’s about 80 percent, 70 to 80 percent of its fuel comes from fatty acids. And to deliver these, your body uses these KM. So once the KMs exits the capillaries. It’s already as an LDL. So it needs to have it has two choices. The LDL. It can be taken back to the liver or it can switch its contents with HDL and the deals can deliver them correctly to the proper places.
[00:38:25] So that’s why HDL is so important because they deliver them to the proper places in the event that these� kilomicrons or these LDL aren’t transferred correctly back to the liver. So why are LDL so detrimental to the system of our body? So here’s a couple of reasons why. So as an LDL is scavenged throughout the body, they are seen as a foreign object by our macrophages or macrophages are our cells that are used for immune response. So macrophages end up engulfing these LDLs and they turn it into these things called foam cells. Foam cells become plaques eventually. But what they do is they actually embed themselves within or under the surface of the epithelial lining, causing a buildup of these foam cells here and eventually blocking the pathways, causing a plaque. So by eating better fats, having a higher amount of HDL as you can get these plaques and avoid plaques which are clogging up your arteries.
[00:39:27] You know, actually the link between sclerotic plaques and metabolic syndrome, you’ve made it very, very clear at this point, and that is the reason why prolonged states of metabolic syndrome do create these disorders. I want to take a moment to thank the entire crew here because what we’re doing is we’re bringing in a lot of information and a lot of teams. And if someone has an issue, I want them to meet the face that they’re going to see when they walk in the office. So, Truide, tell them how we greet them and what we do with them when they walk in if they feel that they may be a victim of metabolic syndrome.
[00:40:01] Well, we’re very blessed to have a very exciting and energized office. You’re always going to feel at home. You’re always going to if we don’t have the right answer at that moment, we’re certainly going to research. We’re not going to toss you aside we’re always going to get back with you. Everybody gets treated as an individual. You know, each vessel that we have, it’s unique in its own way. So we certainly don’t create a cookie-cutter approach. We’re always going to make sure that, as I said, you walk away with the most valuable informed option for yourself. We’re just a phone call away. We’re just a click away. And you don’t ever feel that there’s not a reasonable question. We always want to make sure that all the questions and concerns that you have they always get the best answer possible.
[00:40:50] Guys, I want to tell you. Thank you. And I want to also share with you that we happen to be in one of the most amazing facilities when we do, there’s exercise involved with returning the body back to a normal state. We function out of the PUSH Fitness Center. We’re actually actually. Doing the podcast from the fitness center. And you can actually see the information here with Danny Alvarado. And he’s the one that or Daniel Alvarado, who is the director of Push Fitness, who we work with, a bunch of therapists and physical therapists to help you restore your body back to where it should be. We look forward to coming back. And like I say, if you appreciate or you like what we have here, you reach down on the little bottom, hit the little button and hit subscribe and then make sure you hit the bell so you can be the first to hear what we got to go on. OK. Thank you, guys. And we welcome you again. And God bless. Have a good one.
The following Neurotransmitter Assessment Form can be filled out and presented to Dr. Alex Jimenez. The following symptoms listed on this form are not intended to be utilized as a diagnosis of any type of disease, condition, or any other type of health issue.
Podcast: Metabolic Syndrome Explained
Metabolic syndrome is a collection of risk factors that can ultimately increase the risk of developing a variety of health issues, including heart disease, stroke, and diabetes, among other problems. Central obesity, high blood pressure, high blood sugar, high triglycerides, and low HDL are the 5 risk factors associated with metabolic syndrome. Having at least three of the five risk factors may suggest the presence of metabolic syndrome. Dr. Alex Jimenez and Dr. Mario Ruja explain the 5 risk factors associated with metabolic syndrome, in further detail, as they recommend diet and lifestyle modification advice and guidelines to help people with metabolic syndrome improve their overall health and wellness. From eating fiber and staying hydrated to exercise and better sleep, Dr. Alex Jimenez and Dr. Mario Ruja discuss how diet and lifestyle modifications can help improve the 5 risk factors associated with metabolic syndrome to ultimately prevent the risk of developing a variety of other health issues, including heart disease, stroke, and diabetes. – Podcast Insight
Neural Zoomer Plus for Neurological Disease
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention.
Food Sensitivity for the IgG & IgA Immune Response
Dr. Alex Jimenez utilizes a series of tests to help evaluate health issues associated with a variety of food sensitivities and intolerances. The Food Sensitivity ZoomerTM is an array of 180 commonly consumed food antigens that offers very specific antibody-to-antigen recognition. This panel measures an individual�s IgG and IgA sensitivity to food antigens. Being able to test IgA antibodies provides additional information to foods that may be causing mucosal damage. Additionally, this test is ideal for patients who might be suffering from delayed reactions to certain foods. Utilizing an antibody-based food sensitivity test can help prioritize the necessary foods to eliminate and create a customized diet plan around the patient�s specific needs.
Gut Zoomer for Small Intestinal Bacterial Overgrowth (SIBO)
Dr. Alex Jimenez utilizes a series of tests to help evaluate gut health associated with small intestinal bacterial overgrowth (SIBO). The Vibrant Gut ZoomerTM offers a report that includes dietary recommendations and other natural supplementation like prebiotics, probiotics, and polyphenols. The gut microbiome is mainly found in the large intestine and it has more than 1000 species of bacteria that play a fundamental role in the human body, from shaping the immune system and affecting the metabolism of nutrients to strengthening the intestinal mucosal barrier (gut-barrier). It is essential to understand how the number of bacteria that symbiotically live in the human gastrointestinal (GI) tract influences gut health because imbalances in the gut microbiome may ultimately lead to gastrointestinal (GI) tract symptoms, skin conditions, autoimmune disorders, immune system imbalances, and multiple inflammatory disorders.
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
For your convenience and review of the XYMOGEN products please review the following link. *XYMOGEN-Catalog-Download
* All of the above XYMOGEN policies remain strictly in force.
Modern Integrated Medicine
The National University of Health Sciences is an institution that offers a variety of rewarding professions to attendees. Students can practice their passion for helping other people achieve overall health and wellness through the institution’s mission. The National University of Health Sciences prepares students to become leaders in the forefront of modern integrated medicine, including chiropractic care. Students have an opportunity to gain unparalleled experience at the National University of Health Sciences to help restore the natural integrity of the patient and define the future of modern integrated medicine.
Metabolic syndrome is a collection of risk factors that can ultimately increase the risk of developing a variety of health issues, including heart disease, stroke, and diabetes, among other problems. Central obesity, high blood pressure, high blood sugar, high triglycerides, and low HDL are the 5 risk factors associated with metabolic syndrome. Having at least three of the five risk factors may suggest the presence of metabolic syndrome. Dr. Alex Jimenez and Dr. Mario Ruja explain the 5 risk factors associated with metabolic syndrome, in further detail, as they recommend diet and lifestyle modification advice and guidelines to help people with metabolic syndrome improve their overall health and wellness. From eating fiber and staying hydrated to exercise and better sleep, Dr. Alex Jimenez and Dr. Mario Ruja discuss how diet and lifestyle modifications can help improve the 5 risk factors associated with metabolic syndrome to ultimately prevent the risk of developing a variety of other health issues, including heart disease, stroke, and diabetes. – Podcast Insight
[00:00:07] And we are live. Yes, we are. Hi, this is Dr. Alex Jimenez. Today we’re gonna be talking with Dr. Mario Ruja. We’re here together today. We’re testing out a new technology of head to head conversations regarding the whole process. Mario, how you feeling, baby?
[00:00:24] Feeling incredibly metabolic, Alex.
[00:00:29] Yes, really metabolic. I’m about to go through this mic right now. That’s what I’m talking about. Hey, we’re here.
[00:00:37] Mario and I are, you know, we’re gonna be hitting you every day. Every week. Every time we can. As much as we can. We’re gonna be going through the airways. Yeah. And we’re gonna be using the new technology to discuss exactly what we’re up to. Today, we’re focusing on an interesting disorder called metabolic syndrome. Many of you have heard the word. But really, you know, tying in exactly what it is that we’re talking about requires kind of elaborate conversation. You’ve seen it in many pictures. Mario, you can pop up the picture there PIP and you can see that a lot of times people see this gut thing going on. And that’s one of the components of it. Metabolic syndrome, when you break it down is ultimately and people notice it when they go to their doctors. Doctors are very good at assessing clinical assessments at the point where they show up in the lab work. Now, metabolic syndrome is one of these issues that many people have. And when they’re diabetic, well, they are pretty much in that range already.
[00:01:39] But before it happens, the body can stray into a metabolic area where a lot of times, for example, if your blood sugar is over 100 and you’re starting to feel like really bad, your bellies are really large. We need to have some parameters to determine it. But most people end up having metabolic syndrome and just feeling like crap. So the idea behind this process and understanding what metabolic syndrome is, understanding that there are some underlying pathologies with it. So what we’re going to talk about today is we’re going to talk about issues that are related to it. Now, in the areas of diabetes, we have, you know, complicating issues such as sleep apnea, large waistline, people who take metformin, liver disorders, nonalcoholic delivered diseases that we have heard of all fall under the realm of metabolic. But we have certain criteria that we can do that actually determines what metabolic syndrome is. Now, Mario, you’ve noticed some things regarding blood pressure. Yeah. Now, if you can show the PIP and when we see this, we can actually determine if you can kind of explain that a little bit.
[00:02:44] Yeah, it’s very simple, when you’re looking at blood pressure, your whole system. When you are out of balance in terms of your sugar, Alex, and your gut is overflowing your belt and you have issues tucking in your shirt. Now that blood has to pump hard. It has to work as a turbo. So what happens is this, at that point, this is what we call the breaking point. Anything over 140. OK, and over 90.
[00:03:27] Systolic, diastolic. Now you’re running into problems that that engine has so much pressure to make up for the resistance.
[00:03:38] Yeah, OK. Yes. The overweight, the diabetic factor, the inflammatory factor. You’re talking about triglycerides over 150. You’re talking about type 2 diabetes. OK, again, type 2 diabetes, basically, you know, you’re not born with it. It’s something that you create. You create that diabetes. Where that insulin is out of balance. And now you’re talking about, again, a very large waistline, abdominal obesity. So a lot of times if you look at people, Alex, they look great.
[00:04:16] From the chest up. Yeah. And that mid-abdomen. That torso is scary. Yeah. Yeah. It’s a showstopper, as they say. OK. So this is where the high blood pressure comes in because again, that abdominal aorta, that pressure on it puts so much pressure that it goes above 140 and sometimes it goes over 180, which is like critical, critical. And again, with these characteristics, again, it creates abdominal cholesterol. It creates blood glucose over. We mentioned that over a plus 100 and again, high blood pressure connected with what stroke? So you have triglycerides.
[00:05:15] Clogging up. Triglycerides and yes, this is huge when the arteries clog up.
[00:05:21] Yeah. We have an issue with ultimately all the roads metabolically lead to the liver. Right. So one of the things that we’ve noticed is that when we assess the liver, sometimes they look pretty good and the symptoms may be highly elevated. There’s a huge range of liver enzymes. But what we’re noticing is that if we start having a blood sugar that is elevated. If we start having enzymes, if we start having disorders like what we call nonalcohol, this was a new disease that actually just came aboard. We always knew about alcoholic liver disease or cirrhosis. Now we have nonalcoholic liver cirrhosis and liver disease. Now, how did that happen? Because our sugar was too high and the triglycerides add these fats into the fat level of the liver and start actually destroying the liver. So we started having this disorder and it’s a huge issue, as you indicated, when we start having HDL levels and that which we measure, we start noticing greater levels in 40, lower levels than 40 for men and 50 for women. We start noticing little trends. We also start noticing abdominal obesity, high blood pressure. There are other areas like ovarian cysts.
[00:06:35] Mario, you’ve noticed that there are other areas that are indicated that are collaborative or even equal or what we use to determine metabolic syndrome.
[00:06:44] What are the ones you have noticed? The two major ones where we’re looking at the studies that you see. I’m going to pull this up for you. So we can kind of get a grasp on that. We’re looking at two just very simple.
[00:07:04] Let’s make things simple for the listeners and viewers. Number one.
[00:07:11] Right away. You’re talking about.
[00:07:15] Abdominal obesity. OK, that’s number one. Number two, insulin resistance. So what happens is that your whole sugar balance within your system is not tolerating, the insulin is not effective in your body. So this is where people, Alex, are always hungry and are always eating. And so what I call it. It’s almost like you’re overeating and you’re starving at the same time. Yeah. Because that sugar is in your blood vessels. Okay. And it’s not being taken into the cells. So the cells are starving. But your whole body is overeating. Does that make sense?
[00:08:01] Mario, you know, in your practice. Like, how many people? What percentage of people? Do you notice that even have metabolic syndrome?
[00:08:10] Just a scan and again, the literature says 23 percent of the population now, I would say and in our past community here, I would say at least double that to 40 to 45. And it’s really, really a point. This is why we’re here today. You know, we’re here to educate, inspire and most of all, give people simple understanding and solutions on what to do. And one thing that I can tell you with a lot of my patients, number one, increase your fiber intake. Like, eat more vegetables. You know, I tell them that. So what do you eat? Yeah. OK. You know, so, I mean, you come in and people want to get on treadmills and they want to climb mountains. They want to do burpees. It’s like, yeah, you know what? You’re 100 pounds overweight. Those burpees are going to kill you. Okay. You’re going to wake up tomorrow morning. You can’t get out of bed. So the major factor to really start to address this is not getting in and starting a workout in gyms. First, we’ve gotta handle and we need to really educate the public on, the food intake is the solution. That is the primary solution. Medicine of the body. The food is primary medicine. And this is what we’re talking about, becoming more vegetarian, increasing fiber, reducing alcohol intake. I know I’m hurting some folks right now. Yeah. Yeah. And the point is, you know, again, reducing. It doesn’t say, you know, if you want to have a beer or something, that’s great. But again, let’s be mindful. This metabolic syndrome is a beast. OK.
[00:10:07] It’s a beast that’s affecting our parents, our grandparents. And now, Alex, I can see these patterns in elementary school kids, OK? And what they’re eating, they’re eating a lot of sugars, right? They’re eating a lot of fast foods, processed foods. This is one thing like right now I’m looking at you and you’re drinking this green. Green, you know?
[00:10:32] Yeah. There you go. Yeah.
[00:10:35] It’s like a jolly green giant drink. OK. That is a live food. It’s uncooked. It’s raw. The vitamins are there. The nutrition is there. It’s not denatured. OK. Anytime we cook food, you kill it. Right. Anytime you bottle it up and you preserve it for a month and two months.
[00:11:02] I can tell you right now, you are not eating live. So the rule that I share with my patients and when I do seminars all over the nation and people invite me over, I say, look, if you want to be alive, why are you eating dead? Simply, why are you eating dead? Right. And like right now, you know, let’s make it simple. Number one, increase hydration. Right. OK. Have a gallon of water or more is a must. Excellent. That’s number one. Number two, increase live foods. Live foods are what? Vegetables. Fruits, right? Juice them. Eat them.
[00:11:38] I mean, from what I understand and what I do is that everything leads to, any sort of nutritional component, whether it’s a treatment for diabetes or a treatment for, let’s say, rheumatoid issues when there is a nutritional component, many times it’s hard getting the foods that you need. So the world has turned on smoothies. Smoothies can date different formats. And these smoothies, as we work them, ultimately have the solution. Now, what kind of smoothies? What’s the best type of approach with them? Well, we have that stuff in terms of awareness in our offices and gladly we’ll share that stuff whenever it’s necessary. However, the reason is that those inner parts of the cells, those living enzymes, those DNA molecules, those proteins, those…
[00:12:37] Actually, probiotics, even in the fiber, prebiotics, because when you do these smoothies or even do juicing that fiber you eat, that fiber that sometimes is lost while you do it juicy, juicing. This is important for the bacteria. So that helps even with disorders, such as leaky gut or intestinal dysbiosis, because they all come together. Someone who has metabolic syndrome most likely has leaky gut and vise versa. And not every single time, we can assess that, but what we want to do is we want to assess a person completely in terms of the drugs. You pretty much know that your doctor is trying to get you away from diabetes because you’re in that losing control place when you’re taking metformin.
[00:13:20] Metformin is very powerful, it’s a special medication that ultimately guides to restores the blood sugar back to where or it makes it more effective or makes you less insulin tolerant and more sensitive. So there’s a lot of things that we’re looking at that are useful for us. But one of the things is, well, what am I going to do with this?
[00:13:41] How am I going to get better? Well, diet? Diet has everything to start with. You start with your diet. You start with being vegetarian. You start with Mediterranean style foods. What kind of techniques do you use in terms of diets? Because I can go off and explain those things. But I want you to kind of get. Simple.
[00:13:56] You know, simplicity is golden. Complexity is chaos, Alex. The more complex we make it for ourselves, the more likely it is that we’re going to quit. OK. You can’t sustain complex things. We need to make them simple. So number one, as much as possible, eat raw, eat live foods. That’s number one. Number two. Number two, stop eating processed things like you’re talking about like high corn sirup, like simple, stop drinking Cokes and all of these fruity drinks and everything else, you know. And it tells you right there on the bottle, right there on a can. It’s 10 percent fruit. Do you know what 10 percent means? It’s not 100 percent. There’s a missing zero, baby. OK. It’s missing. So you know what? After a while, you’re gonna be missing off the planet. OK. You’re going to be extinct. Yeah. So, yeah. We need to get real, you know, this is real stuff. Like I can tell you, you know, I visit, I do home visits sometimes because I give back to the community and I go to families and I sit there and, you know, people are losing legs. People are losing limbs. They have wound care, you know. They have, you know, they have issues in terms of that. And that’s painful, not only for the person but for the whole family. So you know what? I take this very seriously. We take this very seriously at the show. You know, we want to make it live. We want to make it interesting. But I want to tell you right now, I’m not playing games. This is not game time. This is showtime. And so in terms of that, get off the Cokes, get off the fruity drinks, get off the candy bars. OK. You know, I think that commercial with Snickers, they need to change that. You know, instead of the Snickers satisfy, how about the Snickers gonna kick your ass? How about that one? Yeah, yeah. I said it. Thank you. I think we are physicians so we can say that word. Right. So that’s what’s happening. And then again, the lifestyle. If you’re drinking, the two things I can tell you right now. Yeah. Two things that are going to kick you in your gut, no pun intended. Metabolic boys and girls. OK. Number one is going to be smoking. And number two is going to be alcohol. You do those two.
[00:16:16] OK. And here it is. I’m going to tell you what it’s, you know, can you find that on the slide. OK. It’s gonna be the statistic. Oh, here it is. There. Bam, right there. Pull that up. Yeah, ok. Bam. OK. So if you’re looking at that, I’m going to tell you this is scary. Lifestyle factors, the two factors right there. Can you enlarge that? So we can see that. We can do that. OK. Excellent. I appreciate that. That’s all big. There it is. So now watch this. Do you see this? OK. Here it is. The number one life factor right here. Number one, is that? Yes. The one right here? OK. Now watch. I want to circle this. OK, where is it? It’s right there. Tools. I’ll get it for you. OK. Go ahead. Circle that, smoking and heavy drinking. Okay. I just want everyone to kind of take note, smoking and heavy drinking. That is one of the most destructive things that you can do right now. And guess what? Most people do them together, don’t they? Yes, sir. That’s it. So now watch, the ratio that metabolic syndrome affecting the man. OK. This is, again, something new. Mm-hmm. It’s affecting the man less than the women. Do you see that, guys? Yes, I do. Look at that. The women is 4.45. The women are affected most out of everyone. Out of everyone. And the men are at1.85. Now, the lesser evil is heavy drinking and poor diet, and the less one is smoking and physical activity. But if you really look at it, that’s what’s scary, smoking and heavy drinking. And this has really come down to a shift.
[00:18:04] You know, you used to be that men smoked and men drink. Now it’s changed, Alex. This is scary because it’s affecting, you know, momma is the boss. And to me, you know, mom is the doctor in the house. OK. And no, I don’t want to take responsibility for the man because you know what? We need to be the head, not the tail, but at the same time, who is going to take care of the kids?
[00:18:28] It’s got to be mama. You know, most of the time. Who’s going to take the kids to the doctor? Who’s gonna be wrong? So we need moms healthy. We need moms healthy. OK. We can, you know, because there’s a saying that says this, Alex. When mom ain’t happy. Dad ain’t happy.
[00:18:44] Nobody’s happy. No, thank you. Here, even the dog ain’t happy, Alex. He’s leaving now. He’s gone. He’s gone.
[00:18:52] I happen to know a lot of, I think after about 40, I think that in general there’s a tendency for the love of wine and it gets a little crazy for a wine to three a night. Yeah. This leads to metabolic syndrome. So we need to. Moderation is key. Right. Yeah. So we’re going to you know, if you’re if one of the biggest treatments is cardio, well why give yourself those extra calories and doing their process?
[00:19:19] Now one glass is fine. I understand that. But we don’t have to go crazy with the wine in the evening because it’s a more relaxing thing. You know, there’s always women’s night out, right? You know, I mean, it’s shot here, but women’s night out. You know, and when there’s women’s night out. And for many women, it’s a little bit of vino. So we need to kind of cater to those things, shall I say.
[00:19:39] And it’s woman’s night out. But it’s not all night, baby, you know?
[00:19:42] Yeah, OK. I mean, you know, there is.
[00:19:45] Exactly. I mean, you know, let’s have a glass but not the bottle, baby. Come on. Well, you know. Right. If you have 4 people a bottle is OK. OK. I said wine. Okay. I’m sorry. I lost. I lost the meaning of that. Go ahead Alex. Yeah.
[00:19:57] So the bottom line is, that we’re here to bring in awareness of this disorder, which is metabolic syndrome.
[00:20:05] Honestly, I’ve been going to school for a long time. And this is a new revelation of the last decade.
[00:20:12] The gastroenterologist is really focusing on. They’re the first to see it, the dimensions of. And here’s the thing. Crazy metabolic syndrome leads to nonalcoholic, fatty liver disease. And you were seeing this in rampant levels, literally. Gallstones. Exactly. Because the liver, the cholesterol issues, all these dynamic changes are affecting even our children. We’re having kids with nonalcoholic fatty liver disease. Why? Too much sugar? Too much sugar? We have to control the sugars. And there are things that we can do in our diets. Plan on bringing all those concepts.
[00:20:46] But we want to bring awareness as to what happens. Lack of sleep, cortisol raising, you know, all this kind of stuff alters the blood sugar in our system. So it’s very important to do the best we can. Exercising is awesome for this stuff in terms of cardiogenic exercises, cardiometabolic dynamics, though. That’s where we want to still focus on. We have to do a little bit of cardio. We got to, you know, eat more of vegetables, greens, juicing, those kinds of things sleep better. It’s important to sleep.
[00:21:15] Alex. Oh, OK. I want to jump in because I know we’re jumping here, you know, and people and I like the fact what you mentioned earlier, you know, we want to, you know, get some wine and some things to relax. Why don’t we do this? I encourage people to meditate. OK. And to try to create some stress management strategies. OK. Right.
[00:21:38] Like a nice, you know, nice warm cup of tea an hour before we go to sleep. You know, some chamomile tea and I mean, you know, chamomile, you know, and.
[00:21:50] Yeah. Good stuff. Yerba buena. You know, stuff like that. You heard about it? Yeah. Yeah. So.
[00:21:56] So you know, all of these things. Meditation because why? Stress levels, as you mentioned, I’m on one accord with that stress level increase cortisol, which contracts, arterial function and then decreases dopamine.
[00:22:13] OK, and oxytocin, which is like the love thing going on. OK. And so now all of this creates sleep apnea. And how many people do you know, Alex, that suffers from sleep apnea and instead of dealing with the causation? OK. So this is why chiropractic is such a beautiful thing.
[00:22:35] You know, for 25 plus years, a quarter of a century plus, you know, between both of us, we’re like, gosh, 60 plus years. Correct? Yes, 60 plus years. All right. Chiropractic and chiropractors have such a beautiful story and beautiful platform because we’re all about natural healing and helping our community and our country at very, very cost-effective.
[00:23:09] You know, we do one of the most cost-effective ways of not only treating health but preventing health. And we are ambassadors of health. I mean. And so this is where when we’re talking about, again, sleep apnea, meditation, I see so many people in my practice, they’re taking a pill to go to sleep.
[00:23:32] Every night.
[00:23:34] They suffer from depression. They suffer from anxiety. Okay. And then I look and I go, you know what? Let’s talk about your lifestyle. What are you doing? What are you doing every day to put your body in a high, intense, inflammatory system in high, intense stress? Yeah, you’re redlining. I always tell people. Right now you’re redlining it’s just like a car. You cannot maintain it. You better change gears, otherwise, you’re going to blow the engine. And this is what I see, sleep apnea. Sleep is again, all the way from athletics to life function. That is where the neuroreceptors neuroplasticity, Alex. Okay. That’s where we heal. We recover. We reset for the next fight, which is early in the morning. And if we don’t do that, we go to the next day with that fog. Yeah. You know that mental fog. Alex. Hey, you know, and this is where people say, you know, I can’t focus. I’m forgetting, you know, and I don’t know what’s happening, you know, and I’m going, you know why you’re not sleeping?
[00:24:47] Exactly. You know, we’ve done the studies and the studies specifically about sleep. If you’re a person that you need seven hours of sleep and you miss one hour, just one hour of sleep.
[00:24:58] The mind is very just speaking about just the brain fog that happens with this metabolic syndrome because it really starts disrupting everything. One hour of sleep actually diminishes your ability to be creative. Creativity. Yes, the brain is altered. And you may think that you know, 25 percent by one hour, it makes a difference. But literally two hours of sleep, you lose 50 percent of your creativity if you lose four hours of sleep. Well, no one of those when you just push it like four hours. Your creativity is so low that even just trying to figure out how to find where your keys are or creativity, how to solve problems, how to deal with issues, you go to work and someone’s got some drama. It stresses you out and metabolically and then what would a lot of people do? You go to work. You jack yourself up with some coffee and then you grab what? Many people grab the donut instantly, send in the blood sugar into chaos. This constant repetitive issue of habits leads to the disorder of metabolic syndrome.
[00:26:02] The body, the body. Alex cannot sustain us. You know, you can’t. As I mentioned before, you can’t drive that, that your car in first gear going 80 miles an hour. You cannot. And so it’s going to rip at the seams. The gasket is going to come off. The oil is going to spray out. OK. And this is what’s happening. If you really look at the body, we look at the HDL cholesterol, it’s lower than 40. They should be the highest, high density.
[00:26:33] High density should be the highest. Cholesterol, good cholesterol stuff.
[00:26:37] You know, you want, LDL should be low and the HDL should be high. You’re looking at insulin. You’re looking at strokes. You’re looking at again, you know, triglycerides over 150, you know, sleep apnea again, more than ever. Now I’m hearing about it. Polycystic ovaries. I just hear this, you know. You know, I have another surgery. You know, I have cysts.
[00:27:04] I have this with all of these things. If we really look at it, we are seeing that we are pushing ourselves over the cliff. Yeah, OK. And then I’m going to throw this in there with the onset of overuse of cell phones by adults and by youth. Now it is disrupting the cognitive pattern, the focus pattern. And it’s throwing people where they don’t go to sleep because they have a cell phone in front of them at 11 o’clock at night in bed. You know, and then you’re talking about like one hour less than two hours. Well, let me tell you, the worst thing you could do, Alex, is have your cell phone next to your head with the radiation, with the sounds every time that phone beeps. Tweaks a bell, sounds for an email or your Facebook. Guess what your subconscious in your brain does? It wakes up. It wakes up and bam, it blows up.
[00:28:11] That REM sleep you only have. What is it, Alex? What, ten, 10 minutes, less than 15 minutes, of REM sleep? Oh, there’s a lot of. What is it?
[00:28:20] What happens is the body goes into a bunch of different stages as it does. What we’ve learned over the years is that we used to believe that REM was something intermittent. It goes into these deep, deep levels throughout the night.
[00:28:31] Your body temperature, what your blood sugars at, what’s your mental state, what’s your tired levels is, what your electrolyte balance is. This matters. So sleeping is very important. So in the restoration of your body through to get it back in order. Sleep is one of the greatest ways to be able to restore the body. So it’s important to try to you know, if you go to bed at 10, push yourself to start working the process, to go to bed probably about an hour earlier or start working. And the TV is going to be there. They’re going to keep on going 24/7. But, you know, we’re the ones dealing with the issue later on in the next day where we are brain doesn’t work well.
[00:29:10] Our bodies are needing carbohydrates, our foods are. And don’t eat, you know, and put yourself on one of the things that I encourage. Again, my children and, you know, Karen and the kids. Is this. Put your cell phone in the kitchen and get a real alarm clock. I don’t think they make them anymore, do they? They don’t make alarm clocks anymore. Now, forget it. What’s an alarm clock? It’s kind of like a pager, Alex. You know what? We’re gonna get to the point where we’re going to say, hey, do you have an alarm clock? And I go, now I’ve got a pager. All right. Okay. It’s ridiculous. We need to have a phone in the kitchen. You remember back in the days with that long cord. About like 80 yards. You used to take it in your room for those private sessions, you know, with your girlfriend and all of that.
[00:29:58] Well, let me tell you, that cell phone needs to be in the kitchen. It needs to be turned off. Okay. And then you need to have an alarm clock next to your bed. You need to honor sleep. You cannot eat foods before you go to sleep. Go to sleep hungry.
[00:30:16] One of the things that I’m reading more and more in terms of research and in terms of data. Go to sleep, hunger, you’re not going to die. All right. Calm down. Well, I know what you’re talking about. Yes. Intermittent fasting. Absolutely. OK. Yeah. Yeah. You can’t. I mean, at the end, you know, let’s say 8:00. That’s enough. Put the burger down.
[00:30:35] Yeah. Look at that. You know.
[00:30:37] You know, 300 years ago, we would be we many of us were nomadic. You know, people live culturally on the sides of the earth. And the terrain was different. We got the food during the daytime. Nighttime was a time when you kind of just, you know, settled in. All right. If you did, have you had some grains, some nuts, and it was different. So just by using the sunlight in order to kind of like you, as soon as the sun comes up, you can eat and shut off at night if you get really good and you start using what we’re learning, that is a great method, which is intermittent fasting. The body has the ability to rectify itself. This is an amazing, metabolic syndrome or not. The body even activity stream has the ability to rectify itself.
[00:31:23] So if you allow the body to cleanse itself throughout the day, let’s say you do an eating cycle of only eight hours on a window, so to speak. Well, you got a good, you know, 16 hours of what period of where your body breaks things down. Well, the metabolic processes of the breakdown of usually the mitochondria, the mitochondria, as it starts working, the process needs to rest. Our bodies need to rest. I mean, if I told you to cut the grass, Mario, you know, cut the grass. And as soon as you walked in the house and you were done and I gave you some lemonade and you were just kinda, that was rough. And I said, go back and cut it again. Right. And then also you go back out and you’re like, wow, this is crazy. When what kind of guy? And then right when you’re tired and you’re shaking because you have no energy and you’re about to go to bed. All right. And you go get up because you’re gonna go cut the grass again and you never let the body rest. Eventually, your body breaks down. That’s what happens with mitochondria. If you’re constantly eating, you’re constantly going through a process, burn out, burning, burning and burning. It needs time to settle and relax, to recover. And that’s what metabolic syndrome recovery process is. Do we try to calm the body through sleep, through lifestyle changes, through blood sugar issue changes? And little by little, we’ll start getting back control of your life because otherwise you have increased steroid or what we call a cortisol steroid production, which then makes the body store fat. Right. And then that’s where you get the belly issues because one of the first indicators of metabolic syndrome is a big belly. Right. For a woman, it’s over a certain amount, over 35 inches. And for men, anywhere over 40, that’s a lot of people over 40 inches. You pretty much have a kickoff towards metabolic syndrome.
[00:33:00] And how many times have you heard in your practice, Alex? You know, people come in and go, you know, I just need to lose weight. I just need to lose weight. And, you know, I look at him and I go, you know, forget about the weight.
[00:33:14] What are you doing?
[00:33:15] Are you sleeping well? All right. Right. Exactly. I mean, first. I mean, let’s forget about the weight. The body knows how to calibrate, Alex. It knows how to calibrate. It knows the zone, the sweet zone, the target zone. It knows genetically DNA, RNA. We have an innate intelligence. OK. We learned this in school and chiropractic school.
[00:33:38] The body has innate intelligence to know how to heal, to know how to recover, to know how to grow. And to know how to survive when we put undue stress to our system, to that fiber optics, to that circuit, we blow it and then it goes a wall. And that’s what happened. So I tell people, you know, no, the answer is not for you to go to a gym for 20 hours a day. No. Why don’t you start with letting go of high corn, syrup high fructose corn, syrup drinks?
[00:34:17] Why don’t you do that first? That’s what I tell them right away. Do that first. Number two, eat more fiber. What does fiber mean? Eat more legumes. Spinach, OK. Like broccoli. And instead of cooking them. And I know most people don’t want to eat raw. Why don’t you just steam them? OK. Just kind of steam them a little bit. OK. Don’t fire. Don’t kill them. Steam them. The other thing you want to do is, you know, get up on a Mediterranean diet, you know, fresh seafood, things like that, regular exercise, just get up in the morning. The first thing that I would share with people is just make things simple.
[00:34:53] Wake up when the rest of the animals wake up, OK? Wake up. And just go for a walk.
[00:35:02] At least, you know, let’s not get on a treadmill and break a record, OK? Let’s not do that because you’re gonna do that twice. You’re gonna get hurt and you’re gonna quit for the next three months to recover. So why don’t you just get up and walk? And then next time walk a little more and walk a little faster and next time walk a little faster and jog. So we need to create that patterning, rituals. We need healthy rituals, Alex, in our lives instead of rituals that are killing us slowly. OK. And so in terms of that, I look at eating more fresh vegetables, Mediterranean, sleep better and honor that sleep. Get up earlier, get up before 5 o’clock. OK. Get up. Get into a routine that way when you when you’re not sleeping late. OK. Your body’s tired. So now you can go to sleep at nine-thirty, at ten o’clock, OK. And then create a new pattern to where you let go of the cell phone. And I would say, you know how people do like fasting or cleansing. I recommend at least two cleanses a year, two cleanses a year. You know, stop eating meats.
[00:36:15] OK. Stop eating meats.
[00:36:17] And just go vegetarian. Okay. Let your body cleanse, I know you have wonderful programs at your clinic. Alex, in terms of detox, I believe in that twice a year. You gotta do it. It’s just like flushing your car. Alex Right.
[00:36:31] From detoxing. We start we really begin the process at the intestine. So from the things we start eating. So one of the best ways to do it is to go through a detox program and the detox programs help us cleanse it.
[00:36:45] You know what? If your garage is full of mud, if you’re you know, you just open the garage, you see it’s just a mess and your body’s metabolically a wreck similar to a garage as an analogy. Well, you can have a couple of things. The first thing we do is we open up the garage and we got to plunge that garage. We’ve got to get the hose. Or you can take the broom. And you know what? Many times you’ll realize that taking the hose is probably the best thing. So when we do detox programs, we begin by helping with the colon cleanse. And we basically clean out the colon and eventually also repurpose the direction where the probiotics go. We actually add probiotics in the diet. We add the fibers, the prebiotics, the post probiotics. And we start working from the intestine out. The body instantly starts recovering. And little things that we can do in the mornings on a regular basis such as increase water, take a lemon, for example. We start with water. We start with let’s say you squeeze four or five, three lemons, just three lemons, squeeze the juice, put it in a drink that you’re gonna spend all day. Take one whole lemon to squeeze it nice and just take it as a shot. Some people use apple cider vinegar. Exactly. So what we do is we start that well, that goes into the intestines, into the stomach. It is much it just basically showers the liver with a process that begins the process of cleansing as the body starts recovering. You start eating better. You let’s say you do a fast and you begin your process of eating at around 12:00 and you stop at six or maybe seven or maybe eight. And it gives you an eight-hour window, six to eight-hour window and that’s it. And then you start recovering in that process. So early on, we start doing the changes with the beautiful thing about the body if you give it time, it’s all recoverable to do it. And if you teach the body, you don’t have to be taken metformin the rest of your life. Now, if your doctor thinks it’s appropriate, well, then, you know, you speak to your doctor. And here’s the other thing is, is that when you’re dealing with metabolic issues and you’ve got someone that’s giving you metformin and as it or other diabetes or different types of medications that help with diabetes, it is appropriate to have it under a doctor’s control. Now, the constant taking medications without, having lifestyle changes or not having dietary alterations is inappropriate. It’s malpractice, I believe, in my opinion, after being here so long, you just don’t give people pills and not change their diet. You got to have a doctor who’s willing to sit down and help you out with lifestyle changes, diet or someone that has some staff to support you or a dietician or a registered dietetic dietitian. So that can help you or a nutritionist. Sorry. Or a health coach that can help you. We have to have people that can do that. So to help you with the process, because it’s not just saying, hey, take a pill and go off on your own, that confuses a lot of people. We have to have a change and we’re here to help you with that. So as we go through this process over the next couple of weeks, Mario, as we discuss each one of these particular topics, we’re going to bring it to you. We’re going to talk about ways that you can change your diet that simple. Just make it simple and it adapts. So I know you’ve got some points you want to mention again.
[00:39:50] Absolutely. You know, with metabolic syndrome, the two things that are markers are number one, your belly fat. OK, so let’s get going in at home. Yeah. Let’s wrap it up. You know, let’s button this thing up and make it simple. First of all, it’s belly fat. So. So if your belt, when you’re buying a belt and you’re looking at the little notches and the little holes and they’re over 40 inches, OK, 40, you’re in trouble. For male. Yeah, for male. And if you’re over 35 for a female, you’ve got issues.
[00:40:24] Metabolic syndrome. Absolutely. Absolutely. And the other point is this. If you have a hard time and you can’t even wear a belt, then I don’t need to explain any further. It’s time to come in and get a coach, get a health coach, get someone to make you accountable because time is ticking. Time is ticking and we need to be proactive instead of reactive. And at the same time, when you are always hungry, you’re overeating and you keep being hungry. You cannot lose weight. Now the things are coming to fruition. And on top of that, if you have blood pressure, over 140, over 90. So let’s say 145 over 100, let’s say 150 over 105. It’s time to get real. You can do this. Just go buy a blood pressure cuff, OK? Quit playing games. Get-go. Go to Walgreens. Get a blood pressure cuff and check it tonight. And if it’s over. Check it at least. I always tell people, don’t do it once. Keep a record and do it for at least three, three to four days. OK. And take it in the morning. In the afternoon at night so you can see a cycle. Bring that over and find yourself a team. Find yourself a team that will that has a program for you to naturally empower you and give you the right tools to get back to your best life ever. It is up to you. It’s called self-responsibility. No pill is going to take the responsibility from you. And at the same time, you can enjoy your family more, enjoy your life, and be happier in the process.
[00:42:19] So I really appreciate it, Alex. And I want to thank our listeners and viewers and we look forward to continue the conversation of health and wealth. Because I want to tell you, the message for today is your health is your ultimate wealth. Thank you. And we’ll leave it there.
[00:42:38] All right, guys. Thank you.
[00:42:39] And we’ll come back tomorrow and we’ll add another health nugget, so to speak, for you guys. Two miners.
Podcast: BIA and Basal Metabolic Rate Explained
Dr. Alex Jimenez and Dr. Mario Ruja discuss basal metabolic rate, BMI, and BIA. Body mass and body fat can be measured in a variety of ways, however, several measurement tools may ultimately be inaccurate for many athletes. According to Dr. Alex Jimenez and Dr. Mario Ruja, calculating an individual’s body mass and body fat utilizing various tools is essential to determine overall health and wellness. BMI uses a person’s height divided by twice their weight. The results may be inaccurate for athletes because their body mass and body fat are different, in terms of weight, compared to the average person. Dr. Alex Jimenez and Dr. Mario Ruja demonstrate that BIA, or bioelectrical impedance analysis, and various other tools, such as the DEXA test, the Tanita scale, and the InBody, among others, can help more accurately determine an athlete’s body mass and body fat. Basal metabolic rate, BMI, and BIA are essential for parents that have young athletes as well as for the general population. Healthcare professionals that have these tools available can ultimately help provide individuals with the results they may need to maintain overall health and wellness.
Neural Zoomer Plus for Neurological Disease
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention.
Food Sensitivity for the IgG & IgA Immune Response
Dr. Alex Jimenez utilizes a series of tests to help evaluate health issues associated with a variety of food sensitivities and intolerances. The Food Sensitivity ZoomerTM is an array of 180 commonly consumed food antigens that offers very specific antibody-to-antigen recognition. This panel measures an individual�s IgG and IgA sensitivity to food antigens. Being able to test IgA antibodies provides additional information to foods that may be causing mucosal damage. Additionally, this test is ideal for patients who might be suffering from delayed reactions to certain foods. Utilizing an antibody-based food sensitivity test can help prioritize the necessary foods to eliminate and create a customized diet plan around the patient�s specific needs.
Gut Zoomer for Small Intestinal Bacterial Overgrowth (SIBO)
Dr. Alex Jimenez utilizes a series of tests to help evaluate gut health associated with small intestinal bacterial overgrowth (SIBO). The Vibrant Gut ZoomerTM offers a report that includes dietary recommendations and other natural supplementation like prebiotics, probiotics, and polyphenols. The gut microbiome is mainly found in the large intestine and it has more than 1000 species of bacteria that play a fundamental role in the human body, from shaping the immune system and affecting the metabolism of nutrients to strengthening the intestinal mucosal barrier (gut-barrier). It is essential to understand how the number of bacteria that symbiotically live in the human gastrointestinal (GI) tract influences gut health because imbalances in the gut microbiome may ultimately lead to gastrointestinal (GI) tract symptoms, skin conditions, autoimmune disorders, immune system imbalances, and multiple inflammatory disorders.
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
For your convenience and review of the XYMOGEN products please review the following link. *XYMOGEN-Catalog-Download
* All of the above XYMOGEN policies remain strictly in force.
Modern Integrated Medicine
The National University of Health Sciences is an institution that offers a variety of rewarding professions to attendees. Students can practice their passion for helping other people achieve overall health and wellness through the institution’s mission. The National University of Health Sciences prepares students to become leaders in the forefront of modern integrated medicine, including chiropractic care. Students have an opportunity to gain unparalleled experience at the National University of Health Sciences to help restore the natural integrity of the patient and define the future of modern integrated medicine.
Dr. Alex Jimenez and Dr. Mario Ruja discuss basal metabolic rate, BMI, and BIA. Body mass and body fat can be measured in a variety of ways, however, several measurement tools may ultimately be inaccurate for many athletes. According to Dr. Alex Jimenez and Dr. Mario Ruja, calculating an individual’s body mass and body fat utilizing various tools is essential to determine overall health and wellness. BMI uses a person’s height divided by twice their weight. The results may be inaccurate for athletes because their body mass and body fat is different, in terms of weight, compared to the average person. Dr. Alex Jimenez and Dr. Mario Ruja demonstrate that BIA, or bioelectrical impedance analysis, and various other tools, such as the DEXA test, the Tanita scale, and the InBody, among others, can help more accurately determine an athlete’s body mass and body fat. Basal metabolic rate, BMI, and BIA is essential for parents that have young athletes as well as for the general population. Healthcare professionals that have these tools available can ultimately help provide individuals with the results they may need to maintain overall health and wellness.
Podcast Insight
[00:00:08] All right. It’s Mario and Alex time. The two favorite chiropractors from El Paso, TX. Ok. We’re going to be… Functional medicine, Alex. That’s what we’re gonna do. It’s about functional medicine in 2020, baby.
[00:00:21] This 2020, we’re gonna be focusing on BMI and we’re gonna be focusing on everything. Mario, my awesome co-host here we’re tearing it up. We’re gonna give some points of view. We’re gonna be discussing certain things. Today our focus is going to be on anthropometric measurements and measuring the body composition rationale and its interpretation.
[00:00:46] Now I’m afraid of that. All right.
[00:00:49] I’m afraid of measurements, Alex, I’m telling you right now, I don’t want measurements around my body.
[00:00:55] Okay. Thank you. All right Mario. Yeah.
[00:01:00] Mario, we’ve got to get a little bit of knowledge here. Okay. Well, what we’re not going to do is we’re not going to try to make this boring. No. If you really want to see boring. I think we have plenty of examples of what boring looks like. Yeah. Have you seen those boring guys, Mario? You know, it’s like the measurement of what’s going on. Yeah. Here you go.
[00:01:20] Video plays in the background.
[00:01:31] You know what? I can go to sleep with that one, Alex. Now, that’s what I’m talking about Mario. I can go to sleep and just shut it off.
[00:01:40] But, you know, learning has to be fun. It has to be interactive and it has to be functional.
[00:01:47] So that’s what we’re… Absolutely I totally agree. So what we’re gonna do is we’re gonna try to bring the facts as it can be and we’re gonna try to bring it with a little bit of slapstick fun.
[00:01:56] So it’s gonna be fun. Mario, tell me a little bit about your interpretation of BMI as how people understand basal metabolic rate.
[00:02:05] Well, this is what I understand and what I hear about basal metabolic rate.
[00:02:13] Bottom line is, can you put your belt around your pants and can you tuck your shirt in? How about that?
[00:02:25] You know, that’s pretty scientific. Right. That is scientific. Yes, that is scientific. Yes. We could talk pear, we could talk apple, sizes, apple-shaped bodies types.
[00:02:33] But we’re going to get specific here because people want to know, Ok, what’s going on. Let’s start. One of the things that we can do is we can start discussing calculating energy requirements, because one of the things that we want to see, as you can see, I put up here a little bit of facts so that it can help us out a little bit in terms of figuring out what’s the best approach in terms of what we do. Now, you can tell here that sedentary, no exercise, what we want to do is talk about basal metabolic rate. Ok. So this is a measurement that has occurred by height as well as weight index. So it comes out to that number and we can start looking at calorie, caloric intake burn. But when we do a BMR and we calculate this number, we typically want to get about a 1.2. And that’s what would be normal in most situations if you’re sedentary, light activity, we start noticing that there’s an increased activity expenditure and BMR should be one point 1.375. If you are moderately active, you should start doing that. So in its interpretation…
[00:03:33] Mario, when you see these kind of things and these kind of figures, what does it bring to mind for you in terms of these numbers? As we keep on going back to this, we’ll be able to see exactly what’s going on. What’s your incentive sense of the rates and the metabolic processes?
[00:03:52] Well, again, very simple, when you look at it as the more active you are, the higher your metabolic rate is. That’s it. So at the end of the day, we want to put it in very simplistic terms to the public. We want to be more active about that. So science is supporting that, you know, park the car as far away as possible from the Wal-Mart entrance and your work. So by doing that every day, you are creating a higher function. Ok, metabolic, that’s the burn. That’s your whole system burning fuel within yourself. So it’s simple. And the studies are showing that the more active you are, the higher your metabolic rate is. It can go up to a 1.9 from a 1.2. Correct.
[00:04:50] Exactly. So what we’re looking at here is that the requirements are going to be pretty high. If you are one of those people that are very active. So ultimately, our goal is to get you as active or what you’re your lifestyle could require. So, you know, if you’re a mechanic, you say moderately active. If you’re someone who works in, let’s say, an office, your BMR is going to be calculable. Using these numbers for the body mass index, the whole idea is to try to figure out the body mass index using the BMR. So the BMR allows us to kind of give an estimate, the best estimate as to where you’re BMR should be at and then we can use the same number, this BMR to assess your body mass index. So our goal is to continue with kind of learning about this thing. And as we kind of go through that, we look at body measurement types. Now, in the past, what we’ve looked at in terms of this, we assess the body in a bunch of different ways. Historically, we’ve been able to do a weight, underwater weight assessment. Remember, Mario, we used to have like a tank and put someone in water, have them float, actually measure the oxygen consumption. Those were the old methods, the true standard way of doing our fat analysis.
[00:05:57] Pretty expensive. Sometimes, though, we use the DEXA test. The DEXA test is a similar test that is used for bone density. We can actually do that. We also have, historically the body pod test. Now, I know that you have noticed different types of tests and we’re going to put up here.
[00:06:13] What are the other tests that you’ve seen? Alex, on that one. When you’re talking about the underwater weighing and DEXA and even the body pod, those are again, more research-based, more scientific.
[00:06:30] Exactly. In that. So when you’re looking at that, I look at it from my perspective.
[00:06:38] You know what’s functional? What’s can everyone do? Exactly. Skinfold is easy. Yeah. You know, skinfold and the BIA and the Tanita scale. Yeah. I mean that one, electrical impulses going through and you’re looking at resistance and impedance. Those are simple. You can’t just buy them from Wal-Mart or anywhere and step on it. Make sure you don’t eat and make sure you don’t drink before you do your test. So do it early morning. Let’s say six, seven o’clock. Right. On an empty stomach so you can get some good readings with the scan. And also, you know, skin fold is easy.
[00:07:21] And again, with the BMI, you’re looking at weight divided by twice your height, your height squared. Exactly.
[00:07:31] So that’s kind of like a simplistic view in terms of BMI. Anyone can do this. Yes. So those are right now. Those are the standards. Those are things, most of the time, when you go to your trainer. Most of the time when you go workout in your CrossFit gym or your, you know, what I call functional gym. Now people are going into more a functional aspect of fitness.
[00:07:55] So they incorporate less wear-and-tear and trauma. Now they’re looking at skin fold and InBody. They even have the new InBody systems that are very popular that give you a nice ratio even of your hydration, which is really nice.
[00:08:13] You know, when you actually say that, when we look at this thing like the Tanita, these scales, like you said, that you can get them at home. The BIA is where it’s at. What we’re finding is that a lot of the studies are reflecting that the BIA actually shows quite a correlation with accuracy with these more complex underwater weighing as well as the DEXA test. So these standards research-based, you’d always want to maintain some sort of research-based, at least collaborative information that makes sense. Right. So now the BIA assessment machines, they can actually determine through OHMS, through impedance to fat analysis to actually measuring the electrical current of the body, a very accurate approach to weight assessment. And by, you know, basal metabolic rates. So now the studies are actually better and they’re easier for people to do. And we don’t have to do some real complex things.
[00:09:09] Yeah. And, you know, if you can show everyone the body part, I think that’s really cool. That’s like a cool thing. You know, I mean, look at that. Can you. Yeah.
[00:09:21] Yeah. That’s really cool. So when you look at a body pod. Right.
[00:09:24] This is an incredible thing. But this is not something you would want to have in your office. Right? Thirty, Forty-thousand dollars. Right. Jesus, man.
[00:09:31] Yeah, you know, it’s crazy, I mean, they’re probably looking at you like they should have you on an alien channel or something. But the simple one, if you can scroll up on the BIA, it’s a simple machine and the readings are awesome. You know, the readings are very good. They’re portable. And you can see the resistance level and you can see the phase angle, which is really nice because then you’re looking at very specific patterns and turns your metabolism.
[00:10:06] Absolutely. These tests now are available in most clinics, or at least the clinics that focus on functional fitness. We have them at the fitness centers and many fitness centers have them. And you and I are used to using these things in our offices. So as we do these things, as we assess these things, we really can give kind of the patients a quantitative point of view that really helps them figure out exactly how everything is.
[00:10:38] You’re exactly right, Alex. You know, in my work, you know, working with athletes and also what I call performance professions, where we’re talking about military S.F., Special Forces, Rangers, things like that. It’s all about performance. So in that, we use calipers. You know, those are very, very useful, easy to use. And the one that I particularly like, which.
[00:11:08] Again, with BMI, there are a lot of discrepancies, Alex, and you know, this being, you know, in the world of bodybuilding and athletics and all of our kids are athletes. I mean, they’re, that’s just part of the family structure. That’s who we are. So now you got to run, jump, catch a ball or kick a ball or do something. Right. So the point is in that what I have found out is that the BMI is not very accurate. Not very accurate at all Alex, when it comes down to athletes. Right. So this is where the discrepancy comes in, where it gets crazy because now you go to a regular assessment, a regular assessment or a regular, I don’t want to say regular doctor, but, you know, your doctor and then he’ll test your BMI and you’re gonna be off, you’re going to be high and you’re going to say, you know, you need to get your BMI lower. Yeah, the point is that the BMI is the mass, right? So again, muscle is heavier than fat. So in your environment of bodybuilding, what do you think about that?
[00:12:22] I mean because I’m sure it was crazy. Well, one of the things that I’ve been able to see over the years is that when you have someone, as we understand this, that the BMR is obviously the thing that we’re using to assess height and weight. But those numbers get skewed when you have an athlete and they don’t work well for the muscular individual, someone that’s I mean, my son, for example, he was 195 pounds, 5′ 8″. In all reality, he’s clinically obese. Right. Yet he’s shredded and ripped. And he was a national champion in wrestling. Literally had no body fat. So the caliper method, the BMR, the BMI based on height and weight has deficiencies. And that’s where the BIA came in and the body impedance assessment. That’s where the studies became very popular. And as what we see, Mario is that in essence, when we look at these situations, we find out that there are great assessment tools out there. These tools are the ones that are actually going to give us the ability to kind of come up with an accurate for a large range of individuals, whether they’re bodybuilders, whether they’re women. There’s a standard between, you know, a good 13 percent body fat and 29 percent body fat for females. Women typically have a larger number of between 18 and 29 percent body fat. At times, that’s a range that is kind of in there. Hopefully, they can stick around 22 to 24, boys in the 13 range just because the body density is different in a female. Right. So what we look at is what’s the norm? One of the things that we can do is try to calibrate people for their numbers so that they make sense for that individual and be able to work them towards it because a true athlete will be able to almost blow the BMR, BMI into the wrong number skew. And if we can get it to a nice number, we’re gonna have to use a lot of different tools. Now, what we’re going to present today are our ideas and fundamental philosophies and knowledge points that we use to determine actual true health. Right. So we’re going to be discussing those particular issues and we’re going to go over those particular areas here. Now, the BIA is the body impedance. Okay. So when we look at the bioimpedance areas, we can see that these kinds of tests are not only just affordable, but they actually determine the electrical current. And because of the body amount of muscle fat and the fat that occurs, we are using the fat as kind of like the thing that allows us to assess body dynamics as well as body density. Right. So as the more, there’s more impedance or more ohms or more resistance in the body, the greater the body fat. So it’s very important that these tests be done properly. Many of the times before you do a BIA, you’ve got to kind of, you know, you’ve got to not take, first of all, you’ve got to be dry. Ok. Because if you’re sweaty, it throws it off. Right. If you eat too much or too many fluids. So typically you try to keep away from foods, eating food prior to this and you try to get this thing to work. So resistance, as we look at it, are the things that we’re trying to measure. So one of the things that, when you look at these particular graphs, you see low resistance associated with large amounts of body fat mass, which is where the body is stored. Right. So when we look at this, this is one of the areas we can kind of put together when we look at the resistance numbers. Now, as we look at different angles, let’s say we got the phase angles. We also look at the ability. This is the new number that is assessing actually the intracellular and extracellular activity as well as the permeability of the cells. Ok. Now, as we range this. They’re looking at ranges between 0 and 20 percent. But the higher the phase angle, Ok, the higher the number where it pops, the better it is for the individual, the lower it is. It’s not as good. So what we want to do is we want to see where your phase angle is and we want to be able to assess it as it gets calculated. So one of the things that we look at, we assess this and our tools that we use, such as the BIA assessments, such as the InBody testing systems, we can actually determine the ranges that are for the individuals. But here’s where things make sense. But what we’re in general, when you look at this, Mario, what is your take from when we assess this particular type of under fundamental research technology as we can apply to athletes? Your daughters are athletes, right? And do you? What have you used in the past for this?
[00:17:07] Usually, when they go on to programs, I mean, they’re super fit, first of all. So they’re looking more at anywhere between like performance in terms of speed, agility, and sustainability. Right. Like, you know, vertical in terms of explosiveness, those types of things. In the area of recovery and energy. This is where I can tell you with the girls and even the boys, they really focused on the energy consistency. Ok. And I can see even with this, which is critical that the phase angle, again, the lower the phase angle, it shows the inability of the cell to store, you know, energy.
[00:18:09] So that’s why that storage of energy, Alex, is real critical because why that is where we get the maximum output and everyone is talking about performance and performance is about what, output. So if that cell can not store the energy, it cannot release the energy and perform. So that’s how nice these are nice markers. I would say that with the latest technology, we need to use them. We need to use them and we need to have benchmarks where it’s not just generalities. A lot of times we talk about generalities. How do you doing? I’m doing good. You know, I had a good workout. Well, what does it mean to you to have a good workout? And what does it mean to have a great workout? The difference is, show me proof. Show me results. It’s all about results. So the better, I guess a good takeaway. A good, good. Kind of, you know, assessment for people. Look at number one. Go to a professional and get your BMR and BMI done. That’s number one. And use the equipment.
[00:19:26] And the specifics so you can mark and you can assess them afterward.
[00:19:34] If you don’t have a straight baseline of pre, you will not have a post. And this is the same thing in performance. If you don’t have your electronic time and track your pre, then your post is meaningless. You really don’t know where you’re going. So for a lot of the performance, you know, to me, life is performance. You’re going to have to perform either at work or at home or you’re going to perform on the field, whatever that may be. On a mat. On a field, you know, in your sports. It’s about keeping track of markers, your pre and post. That way, you know where you’re going and you know your performance in our world. We love scores. Just imagine, go into a game and you never have a score. We don’t keep score. We just want to have fun. It doesn’t. It’s not fun anymore. Right. So.
[00:20:34] So for the things that we’re covering today in terms of the instruments, the methods of measuring body composition all the way from professional, DEXA and water displacement and body pods to skin folds, you know, everyday use, that you can just buy it at your local Wal-Mart anywhere and do the count protest.
[00:21:02] That’s a great baseline.
[00:21:06] And with a lot of the trainers, make sure that when you are training with someone, make sure that they do a baseline so you know and they know where you’re at and the performance and the programming.
[00:21:23] It’s really important to understand programming. There has to be a scaling. There has to be a periodicity in that development. And I know when little Alex was training for state, you know, in the wrestling, there has to be a periodicity. You can’t just go hard and go home like everybody says. No. You have to have your point of performance and you’ve got to have your track, your flow to that. Just like when Mia is training for nationals or international competition in tennis, there has to be a plan where she is developing to peak at that time. Is that correct? Yes, yes, yes, yes. That’s so critical. And we, you, cannot create that plan to peak at that specific if you’re in the dark in terms of having a knowledge of where you’re at. And I think for our listeners and our viewers, it’s critical and it’s very, very easy to get. I think sometimes people get lost, like all, you know, BMI. I would venture to say 80 percent of the people that are listening today. Right. That are watching this video. Have no clue what BMI means. They’ve heard about it, but they have no clue what it is. Yeah, they think it’s some scientific something. No, it’s not. All right. We want to bring it down to earth, down into your living room, where you can actually do a BMI for your kids, right? Yeah. Why don’t we do that? Why don’t we do a BMI for your kids? Do it for your husband, your wife. Make sure you know where you’re at again, with a BMI. And this, you know, refresh my memory. The target is from 19 to 20. Ok, 19 to 20. Anything beyond that is obesity. If you’re talking about 25 BMI, you’re in the obesity range. Right. If you’re talking about 30, you are morbidly obese. And the word morbidly obese means death. That should get everyone’s attention. Oh, yes. Yes, it does. It kinda like wakes you up. So what we’re looking at is, number one, understand where you are. Then measurements and then also understand that these measurements fit the profile of a person. So if you’re a bodybuilder, if you are very heavy muscle-bound. Ok. Then you already know you need to go into impedance. Not measurements. But what I have found out. A very reliable measurement is. The measurement for your waist and that’s where, Alex, I want to kind of share this with our listeners and viewers. Just a simple waist measurement is so powerful because it is actually…
[00:24:24] Some people say it’s better than BMI. It sure is. Right. I mean, actually, yes, it’s yes, it’s very much. That waist measurement gets down and makes it so simple because that abdominal mass, that abdominal fat is the one that’s gonna kill you.
[00:24:41] That’s the one that has the highest risk. Is that correct?
[00:24:44] That’s correct. And if your belly is wide. If it sticks over your belt, we got issues. Ok. So we’re noticing that if there is a certain distance between the chest and the waist, those are better measurements in general. Yeah. So as those numbers are calculated, you don’t need a high-level test. To do this. Ok. I like that. So it’s a very important component to look at. But as we advance and we’re dealing with high-performance athletes, people want to know and you can take a sport like, let’s say, just wrestling, for example, you got these individuals. Or soccer. Huge. We’re dealing with to assess a tight BMI or in a tight body mass index. You got to have body fat. You got to have body fat to be able to sustain the loads of an exercise routine. You’re going to see that during season you got some guys that got some good body fat density. Right. And let’s say their weight class is 198, for example. And the guy is about 215 pounds. Well, if he drops from 215 to 198 overnight, he’s going to be exorbitantly exhausted. And this is something that we’re going to see now if he slowly works towards the goal towards the arena of 198 over a period of two weeks. Or he is better off. But let’s assume he gets there to the exact bodyweight 198 and its 3 days before competition, right? It’s going to be exhausting. He’s gonna be tired. However, if he can get there two weeks earlier and adapt his body as his body starts getting better, it will be able to respond better during the loads that it needs.
[00:26:31] And this is what we are talking about, that it needs to be sports specific. You follow me Alex? Exactly. So that same conversation cannot be held with a soccer player. Exactly. A football player and a tennis player or anything in that what I call long aerobics exertion of over, you know, over, let’s say 10, 15 minutes. And this is what’s happening is and I love it when you said that example with wrestlers, you know, I would say the same goes towards MMA fighters, which I take care of. Yes. MMA fighters in Phoenix and in different areas that then you’re talking about also boxers. Again, they have to make weight. Yes. Ok. Though the world of making weight is a beast, that is a world where you have to be on or you’re going to die. Exactly. You either go into that fight feeling like a beast or you’re praying that it ends quickly. And so. Yeah. Yeah. You gotta pin him in the first 10 seconds. Yes. So. So this is where it’s so important that the training, the measurements, the analytics, and metrics. We’re in a world of analytics and metrics, Alex. We’re not in a world of. Oh, he looks good.
[00:28:09] No, no, we’re past that. We’re way past. No, Mario, we’re in the world of making sure that when we wait, when we compare the athlete, we can measure their changes. And every stage down the road as they compete, as they become more and more in tune to that moment of competition, their body changes, their bodies adapt, their bodies become more refined. And as the season gets better or further along in the season, towards the competitions, towards the season, towards the heavy loads. Yeah. That’s when we can kind of see how the body’s changing. So these tests can actually help us determine how the body reacts. And once these competitors have years of competing and during those years they have offseason and on the season and we need to be able to measure those things in an easy way. That’s what these tests do in terms of tennis, for example, when you’ve done these kind of things. What have you noticed in terms of, let’s say, just the athlete of tennis or even the boxers that you deal with? What have you noticed in terms of the, specifically the…
[00:29:15] Progression through the season. It’s critical, it’s critical and Alex, I can tell you this, that it’s not just performance. The other conversation that I think really needs to be. Dialed in is recovery, recovery, Alex. Ok. And the other one that fits together with recovery is the phase angle. Yes. And decreasing injuries. Exactly. That’s where it kind of gets real, real crazy because you can not have this sustainable pattern. Without recovery and without that specificity and knowing when to push it, one to max out, as they say, and when to shut it down or when to go half-speed, and these are conversations that are really, really critical for young athletes. Alex. Yeah, I see a lot of them, you know, and they’re starting nowadays. They’re starting earlier. They’re starting at six and seven years old. Six and seven. I mean, tell your body hasn’t even woke up to the conversation of sports yet. And they are practicing three times a week, having games every weekend, or some of them practice three times a week with one team and then go with another team and practice the other two days just so they can be at their best peak.
[00:30:48] What sports are you dealing with that kids are doing at six or seven?
[00:30:53] They’re running like right now. I have patients that are doing basketball and track at the same time.
[00:31:01] Yeah. And during middle school.
[00:31:05] That’s amazing. This is crazy. Yeah. So this is my question. Our question. We’re here to help the community. We’re here to help the parents because their vision is my little kid’s gonna be a superstar, right. He’s going to sign a D1 contract. UT Austin, Texas tag, guns up, baby. Yeah, guns up or U of A. You have Wildcats wildcat.
[00:31:34] No, you know walk-ins.
[00:31:35] Yes. And I’m thinking you’re not gonna make it past high school. I mean, you’re not gonna make it past Montwood or past Franklin. I mean, you are going to hit the wall so hard, so hard with repetitive traumas. Ok. And so those are the components that to me as a health care provider, as a, you know, a sports functional medicine…
[00:32:05] Cognitive.
[00:32:08] Coach, I mean, I need to teach people this, forget taking care of injuries. I want to teach you so you don’t get injured. It’s critical. And then they go into middle school and high school and there’s no season off. There is no season off.
[00:32:24] So in your opinion, what have you seen these tests do in order to help the parent or the athlete or the individual or the coach, for that matter? Understand, as a form of betterment for them? What do we get out of these tests in terms of the athlete?
[00:32:46] Very simple. There is a time to turn it on and a time to turn it off. Ok. So, you reach your goal, rest. Ok. You’ve done the tournament, recover, get the recovery, get the mind and body to recover, Alex. A lot of times we don’t even think about the mind. Yeah, the mind gets beat up in the war, in the battlefield of performance, the mind gets beat up. Yes. Ok. It affects your sleep pattern. It affects your focus. Emotions, anger management, all of those things. So what I would say is we’re here to share knowledge and tools or health. But most of all, for performance. Yes. So that way. Each child and each person, let’s say you’re not in middle school, high school. Let’s say you’re in your 20s and 30s and 40s. Well, you’re performing for life. And so let’s really invite everyone to learn more to look up BMI, BMR, all of these and incorporate them into their plan of workouts and challenge them and ask them, when’s the last time you got measured? How about that? Yeah.
[00:34:13] When’s the last time? We have to kind of teach people that these tests are not, you know, at any point. Just one test. You have to follow through these tests for a lifetime to see what’s actually going on. If you really have a center where you can go and the BIA tests are so simple now that we and the correlation between the highest level of research show that we’re very, very tight. Less than 1 percent variation from clinical research methods. So we know that the BIA works in terms of extremity inflammation, in terms of joint swelling, in terms of the metabolic processes for the mass density in the…
[00:34:56] In each extremity. So if you have one muscle that is larger on one side as a result of an injury from the other extremity, we’ll be able to see the changes.
[00:35:05] So the studies are very clear now. We use phase angles to determine health. We use fat analysis. We use the changes and the progression during a very athletic era or a very athletic season is very important to be able to determine. So that today we’re starting the children a lot younger. We’re starting them at four, five, six years old as the child has to around 4 years old, as long as he can focus is in long as he can pay attention. That’s when we start him active. So it is wise to start the process of understanding the metabolism methods that we use to calculate body mass index through their ages so that we have a measurement of what’s normal for that particular child. Because what we really have to see is what’s good for that individual. Specific gravity is another method to determine if you’re cutting down too much. But that’s another topic running. This particular issue is, particularly on the body mass index. And what we want to do is we want to bring that to the towns and to El Paso, particularly because we have those research capacities here, specifically the ones that we have liked is, you know, body mass index so InBody is one of the most top used. They use it at UTEP. They use it at the top research centers. And it’s pretty much the standard now. And, you know, and since we use it, it offers us an ability to quickly assess an individual. I’ve been at UTEP. I’ve seen the types that they use and it’s very accurate. And since we’ve seen the research said that it follows now we know that this stuff is very accurate. And specifically, now you can actually assess your own and have it online and the determinant through methods where you can keep up with your child, see what’s going on. Any other ideas, any other comments that you have, Mario, in terms of bringing this logic or this kind of approach to understanding basal metabolic indexes to the public?
[00:37:10] I would say, Alex. Number one, let’s make it very simple. You know, let’s make it very simple. So with that, this is as simple as getting on a scale to see how much you weigh. That’s it. So let’s bring that conversation to everyone so everyone gets a scan. Minimal. Minimal. I would say seasonal every season. You should get a scan. You should get a BMI. You should have you should log it in just like your weight. You know, let’s be functional. Let’s think of ourselves as important as our cars. Right. So. So I look at it as you have a little tag up on your windshield that says oil change, you know. So why don’t we do this? Why don’t we have? And I really challenge everyone listening. And, you know, we’re here because we need to take care of our community. You know, our community is probably one of the highest rates of diabetes in the nation. Ok. And all of that starts… Mario. Mario. Yeah. Yeah.
[00:38:20] I’m sorry. I don’t want to say it, but you have to. There’s a big elephant in the room. But El Paso, our town was considered the fattest, sweatiest town in the whole United States at one point. That sickened me when I heard it. It was a different town. We are much more advanced. There were very few gyms. Now we’re all about fitness. So if we’re gonna be the leaders out there and man, I gotta tell you, we got some beautiful athletes coming out of El Paso now. Absolutely. We are one of the tops. We can put our athletes against the best, even the most. Well-bred. Top schools. So as we compete in those areas, we really want to use the tools that all the other places use in order to assess our athletes, our children, and our high-performance individuals. So it’s very important we do that kind of stuff now because we have the technology. And no longer is El Paso going to be the fattest, sweetest town of the United States. That’s unforgivable. You definitely agree with that.
[00:39:23] So just bring in that and the division that I would like to share. Is that the measurement, the simplicity of just getting your weight and your height is now complemented with a BMI that you understand. You have some goals. It’s 2020. Yeah, yeah. It’s 2020, baby. You know what, 2020 means that let’s do better than last year. Let’s be healthier than last year and let us integrate and have a better understanding and better objective plan for our own health. And with this, I would say this test and the body measurement index is a word and an understanding that needs to be spread throughout families. So the family can talk about that, like, hey, what are we doing? How are we doing? Ok. And then with that, use it accordingly. Ok. Accordingly. To create positive outcomes where there is just to be able to play with your child if you have children. That’s your sport. Your sport is not to sit and watch. Your sport is to participate. Throw the ball. Kick the ball. Run with your child. Or if your child is really into sports. Give him the tools. Give her the best tools. They’re not that expensive. Now they’re available. So that way they can get training that is on point and results that are extraordinary.
[00:41:04] Exactly. I couldn’t have said it better myself. We have the technology. It’s here. This is not the six million dollar man, kind of world or this is not outside of our realm. We can give it to our kids. We can show them, parents become the educators.
[00:41:22] They are the ones that seek out the coaches. They are the ones that are the nutritionist for the children. They are the ones that are the psychologists that every aspect of developing a child requires a lot of different aspects. So those parents that have athletes, athletes that want to learn more about their bodies and the world of heavy tech research methods are over. Now, it’s simple. You get on scale really accurate methods and you can monitor your body a few times a year, two, three, four times a year, depending on your type of sport and your level of performance. These are the things we can do. And we need to provide that information so that you have tools in order to gage.
[00:42:11] You can’t get in a car without looking at a speedometer. So if don’t know how fast you’re going. You don’t know if you’ve gone too far. You don’t know if you’re having protein metabolic catabolism, which is breakdown or if you’re anabolic. So these are the tools that help us figure things out. You don’t know if certain joints or certain extremities are swollen because of just water or if it’s this protein breakdown. These tools we can actually see inside the body and monitor the improvement or changes. So the world changed. So now El Paso, we have the ability to change the way we understand our own physiology as well as the patient’s physiology and our client’s physiology. So I welcome this technology. And by no means is it limited to anything that we do. This is many providers in the town who can do this. Many hospitals have it. But for a facility, it’s within our practices as well. So we use those things. So I look forward to being able to share this with the patients as well as the town.
[00:43:15] Absolutely.
[00:43:16] I second emotion on that, Alex, and the challenge and the motivation and passion that we’re going to have this year in 2020. Absolutely.
[00:43:26] As to not only motivate and be cheerleaders for functional health and fitness, but also to educate and empower the community with the latest technology and knowledge so they can do their best.
[00:43:43] Amen, brother. This is awesome. And I look forward to being able to continue. We’re going to be coming at you often because we’re motivated.
[00:43:53] We’re parents and we want to be able to touch our El Paso and make it a better place because, you know, without getting too crazy, we’re pretty badass, as they say.
[00:44:11] They’re gonna shut me down. No, no, no, no.
[00:44:16] We won’t do that later, guys. We’ll go ahead and see the show. And it’s been a blessing. So from all of us here, we can actually see how you guys are doing. So. Blessings to you guys. Thank you, guys. Bye-bye.
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Neural Zoomer Plus for Neurological Disease
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention.
Food Sensitivity for the IgG & IgA Immune Response
Dr. Alex Jimenez utilizes a series of tests to help evaluate health issues associated with a variety of food sensitivities and intolerances. The Food Sensitivity ZoomerTM is an array of 180 commonly consumed food antigens that offers very specific antibody-to-antigen recognition. This panel measures an individual�s IgG and IgA sensitivity to food antigens. Being able to test IgA antibodies provides additional information to foods that may be causing mucosal damage. Additionally, this test is ideal for patients who might be suffering from delayed reactions to certain foods. Utilizing an antibody-based food sensitivity test can help prioritize the necessary foods to eliminate and create a customized diet plan around the patient�s specific needs.
Gut Zoomer for Small Intestinal Bacterial Overgrowth (SIBO)
Dr. Alex Jimenez utilizes a series of tests to help evaluate gut health associated with small intestinal bacterial overgrowth (SIBO). The Vibrant Gut ZoomerTM offers a report that includes dietary recommendations and other natural supplementation like prebiotics, probiotics, and polyphenols. The gut microbiome is mainly found in the large intestine and it has more than 1000 species of bacteria that play a fundamental role in the human body, from shaping the immune system and affecting the metabolism of nutrients to strengthening the intestinal mucosal barrier (gut-barrier). It is essential to understand how the number of bacteria that symbiotically live in the human gastrointestinal (GI) tract influences gut health because imbalances in the gut microbiome may ultimately lead to gastrointestinal (GI) tract symptoms, skin conditions, autoimmune disorders, immune system imbalances, and multiple inflammatory disorders.
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
For your convenience and review of the XYMOGEN products please review the following link. *XYMOGEN-Catalog-Download
* All of the above XYMOGEN policies remain strictly in force.
Modern Integrated Medicine
The National University of Health Sciences is an institution that offers a variety of rewarding professions to attendees. Students can practice their passion for helping other people achieve overall health and wellness through the institution’s mission. The National University of Health Sciences prepares students to become leaders in the forefront of modern integrated medicine, including chiropractic care. Students have an opportunity to gain unparalleled experience at the National University of Health Sciences to help restore the natural integrity of the patient and define the future of modern integrated medicine.
[00:00:08] Welcome to the Dr. J. Hour with our crew here and our entire staff. We’re gonna be talking today about basal metabolic rate, BMI, and BIA. What does BIA stand for?
[00:00:33] BIA is a bioelectrical impedance analysis. Right. And we’re gonna be talking about weight analysis and figuring things out. We got a couple of guests online. We have Alexander Jimenez. Which is going to come in, pop him in, please. Let’s hear and as you can see him here on the line there. He’s on the corner side of the HDMI. So on the HDMI, you can actually see him. Hey, Alex, how are you doing? Where are you calling from? Where are we getting in with you?
[00:00:58] I’m doing good. I’m calling here from Lombard, Illinois. And what is it you do, Alexander? Right now I’m going to school for chiropractic and ND, which is naturopathic doctor, kind of doing a little bit of a dual degree program here up north.
[00:01:11] All right. That sounds good. We also have on the line here we have Kenna Vaughn, who is the senior health coach over at our domain. We also have two wonderful individuals. We have Truide who is basically the director and the patient flow analysis individual. And we have Astrid, who is the chief editor at Injury Medical Clinic, where she writes and documents everything according to that. Can everyone hear okay? Yeah, yeah, yeah. All right. We’re all live. All right. So what we’re gonna be discussing today is the basal metabolic index. Okay. And one of the things that we do here is we’re gonna be able to assess the findings. Ok, so our goal today is to determine exactly what the primary assessment is and the assessment. So stay on me. Stay on me. You know you got that. And what we want to do is we want to see what BMI is and why is it useful? Ok. The main topics are what we’ve used to assess body fat analysis and determine the indications and the reasons…
[00:02:11] We use BMI alongside BIA, along with we got waist circumference variables allows also with waist-hip circumference variables and what it means because what we’re finding today is that these are great analysis tools that can be used to determine nature’s kind of a healthy cadence. It’s like blood pressure. We can kind of assess it. Then as long as we have other assessments and other evaluations, we can come up with a plan to kind of comparative. Now, all of them have their issues and we’re gonna discuss each one of them in the costs and what’s the easiest and most cost-effective methods that we can use. But one of the things that we can do is to see, why would we do this and what are the purposes. Now, there are quite a few reasons for this now in terms of it, what I’ve noticed is I’d like for you to, let’s look at the HDMI, we have the assessments here and we can actually see on the live the origination of this. We can see that there are different types over the history of BMI. We’ve gone from calipers that were just a method of measuring behind the arm, behind the waist, along with kind of in the thigh region. We would come up with a measurement of which we were probably about five to 10 percent away from accuracy. But in that process, even using those as long as you did use it on a consistent basis, you had a comparative accuracy and a method of kind of determining a change in your body dynamics and composition. It may not be accurate, but it was accurately inaccurate if that makes sense. Right. So what we did here is we’ve looked at here on our graph here. We have one thing that’s called the underwater way. But that was the standard. It is a research method. It is one of the most important things. And to determine actually what your body metabolism is we have to use things of oxygen consumption because that’s what determines the great spot of metabolism. The metabolism is controlled by the amount of cellular activity that is happening in the body. So calculating how much oxygen debt and how much oxygen use is a great way of researchers finding it out. But we don’t always have a laboratory that has I’d say, you know, one hundred million dollars of stuff and like a university. So it’s pretty much used in a research setting, the DEXA test, you may have heard it because it’s used as the clinical standard to look at bone density specifically on the hip side and the lumbar spine. We use that to determine things such as osteoporosis, osteopenia. We get a variable number and based on that number we can calculate the changes in bone density. There are certain types of medications we use to determine a better outcome for those that have estrogen deficiency. Some people have radical hysterectomy where they do remove all of both ovaries at a young age for whatever the reason is and the estrogen level is changed at that point a DEXA test every few years is determinable. The standard of care for the DEXA is one every two to three years after the age of about 50 to determine the changes in bone density. Now the skin fold that we just looked at here and you can actually, as I kind of draw it out, forgive me that I’m not drawing this, but we can actually see that the BIA and the skin fold tests are other tests that are easy to find, but as we discussed, are inaccurate. The Body Pod test, as you see here, you can see the cost of it, it’s about thirty to forty thousand. It’s extremely accurate and it allows for your body to relax. Each one of these tests has certain standards. One of the things that we have to do is prep for a BIA test or a BMI test. Now, the BMI is something that calculates an easy way of figuring out just height versus weight. However, someone like Alexander, you are how tall Alex? I am 5′ 8″. So a 5’8″ individual. How much do you weigh when you were at your deep competition and you were at your healthiest. Probably around 195 to 197. If you have a person that is 5′ 8 and 187 and I’ve seen him range from 210 and he’s still shredded as can be, he would be having a very high and he would characteristically show as minimally obese. Now you can tell that he’s not obese. So in essence, the BMI has flaw issues and bone density issues. Also, there are other disorders that sometimes fool you like sarcopenia, which is muscle wasting, and you wouldn’t be able to see the differences between those on the BMI. So what clinical assessments have determined is that the BMI and the BIA can be used together. But we have led a new technological world where we actually measure impedance. Impedance is kind of like the filtering or the kind of slowing of electrons or how fast and how quickly they go through. If electrons travel faster or something, there is low impedance or if it goes slowly through it or takes a longer time, there’s higher impedance or actually a lower flow, which allows us to understand that fat is not good a good conductor.
[00:07:03] So the more fat you have, the indirect relationship is, the slower the electrical current goes, therefore it’s less healthy. So using these electronic methods and what we have used in recent technology, we’ve used different companies such as Tanita, also InBody has an awesome system. We will be discussing those that assess the BIA in a way that it’s the most accurate if the most accurate is underwater weighing. And let’s give that relative value of 1.0 the actual BIA test are so accurate they are at .98. OK, so once we see that ratio, we can see that we’re the closest with the BIA test, specifically with an eight-point contact. Now any point contact means with your fingers, your palm of your hand, that’s two, both hands before. And then you have two points of the foot that can actually hit on each foot and that would be four from the feet if you can send that electrical current through the body. In that way, the BIA assessments such as done by the InBody design, we can actually determine a much more accurate assessment. So as we look at these tests, we can actually see what’s actually going on. So one of the things is we’re going to start looking at different companies and we can actually look at what a BMI is looked at. So BMI is used so you can look at it from a relative number. And it’s measuring kilograms per meter squared. And it’s measuring basically the height of the body, base of the body weight. Right. So the higher the number, as you can see, 25 to 29, you’re going to notice that the person is pretty much overweight. OK. I would venture to say that Alex would just because he’s in a situation where he would actually rate because he’s a much more muscular guy. He would not be healthy. He would basically almost reach close to 30 just because he has a large size and weight. But it’s clearly measuring only height and weight. So in order to determine the true health, that’s where the BIA and its bioelectrical impedance analysis, okay. Right. I should remember the words. So this is very typical. So one of the things is I like to show you here on these things, what kind of, Astrid, show a copy of what a BIA, kind of machine would look like. Okay. We have like here, here we have bioelectrical impedance analysis and this is what it looks like. If you notice, you’ll be able to see. And I’ll kinda take you through here and we can kind of see the ability to look at this particular region. You can see that the palm of the hand has one and you’ll notice the two points on each foot. What we’re missing is the final contact, but it’s eight and it takes only 15 seconds to be .98 versus one. Accuracy is a pretty efficient way.
[00:09:48] It also takes seconds to do this and not 45 minutes to do something like the Body Pod. So one of the things that we have to do is ask ourselves, why would someone do these kinds of things? Why would we do this? There are more accurate, more powerful ones, such as the 550 model, which we do not have in our office. And the model that we have is the 770 in our office. So you can see it’s much more accurate and we’re gonna discuss exactly what goes on. But one of the things we want to do is how could someone do something at home that is logical? Kenna, you got some thoughts on how someone could check out their basic health by doing some measurements? What are those measurements?
[00:10:25] Right. So one thing that’s really easy to do at home is gonna be to check your waist circumference, which is relatively cheap. You just need one of those flexible tape measurers you can get at the dollar store or it comes in almost all your basic sewing kits. And what you’re going to do is just gonna stand up nice and straight and you’re going to take that tape measurer, you’re going to want to make sure that you have no bulky clothes on. It’s best done just right on the skin. And you’re going to take it and you’re gonna fold it around where your belly button lies because that’s generally the largest part of your waist. So you’re just gonna wrap it around. You don’t want it to be too tight where it’s squeezing you or anything like that, because that’s going to give you inaccurate results. Take a deep breath in and on your exhale. That’s when you’re gonna get the best measurement and it’s best to do it about three times that way you make sure you’re really getting that accurate read.
[00:11:12] And what is that going to give us in terms of, what’s the circumference going to give us in terms of the assessment?
[00:11:18] What will we get from measuring our girth. That’s gonna help to see if you’re high risk for cardiovascular disease or type 2 diabetes. If you hold more of your fat around your abdomen, it shows that individuals are at higher risk for developing these later on in their life.
[00:11:34] Got it. Got it. There’s another one that we’ve used that most people can use at home.
[00:11:40] It’s a really simple one, which is that one? That one’s gonna be the waist to hip ratio. So you are going to start with that waist ratio that I just explained. But in addition to that measurement, you’re going to go ahead and also take your hip circumference.
[00:11:53] Alexander, one of the things that you did when you did your competition, when you were doing your stuff as a competitor, one of the things that you were doing is you were competing and weight was very important. Tell us what how that kind of stuff affected you and how could the BIA be useful in the world of, let’s say high-performance collegiate wrestling?
[00:12:15] So when it came to wrestling, there were a couple of different things that you just do to strategically approach the season, so the season is around six months. Most of the time wrestlers tend to gain weight in the offseason. So you do a couple of different things at the beginning of the season, they would have you use a caliper by a trained individual and they would measure your body fat and do a pretty much a calculation to see how much weight you could lose in a timely manner that was considered healthy for an average individual. And these individuals were allowed to cut a certain amount of weight within that time frame. So you kind of they pretty much gave you a plan of what you could and could not cut. I think the lowest I was ever allowed to cut was 184. And kind of just showing you kind of what’s going on here. So what they would do is kind of show you what your BMI is. I’m going to switch over to my screen here and you can kind of see just kind of just the reference ranges here. So below 18.5, they have underweight 18.5 to the rest of this kind of going into those reference ranges. And like Kenna was saying, they were doing an analysis depending on what type you had. So there’s a couple you have, your android, which is more of that apple-shaped and then your pear, which is gynoid. So they would measure for females and males completely different. So as your approach, you would either take a couple different dietary regimens and kind of approach to a different aspect of how you would go to cutting weight. So whether it was certain people did better just doing fats and protein. Some people did better just managing their carbs. Some people did better just lowering their caloric intake. So by having that BMI, you can see what your total calorie output for the day for living costs is a good way of saying it. So what’s the cost of living for every day for all your cells to function and what or how much exercise you would do. So most of us were burning between 1000 to 1800 calories between running in the morning or working out and then a two and a half hour to three-hour wrestling practice, which is all cardio intensive training. So as the month went on, we were allowed to cut weight and they would measure the weight that we were cutting at each tournament. So we were kind of scanned in, in a way to allow for us to cut weight correctly. One thing that they did start implementing when I joined, when I started wrestling in high school, was morning weigh-ins, which prevented people from really cutting weight the wrong way and not having a good benefit, because before you could cut all this amount of weight and you’d still have a 15, 16-hour window to replenish all those glycogen storages and gain 15 to 20 pounds depending on how dehydrated you are. So it was not a very healthy approach to cutting weight in that sense. So now with everything that’s going on, athletes are training smarter.
[00:15:01] They’re cutting weight better. They’re managing pretty much themselves a lot better in that aspect.
[00:15:07] So this is a great example of when you use these assessments. I remember as we’ve done a lot with the wrestling, one of the way that the university got involved and they do BIAs for people, but for the athletes, they start them out with the standard specific gravity test and that’s a urine test to determine which protein is within their urine. Also, there are electrolytes such as potassium, sodium, calcium. If the person is highly dehydrated, what happens is the specific gravity rises and they also measure specific gravity. In the beginning, it’s something to be able to measure. And we can say that the kid who weighs 200 pounds, his specific gravity is a certain amount. Right. So we don’t want a kid cutting down with the specific gravity of their body concentration. Blood constriction is too high because that means they’re dehydrated. Those individuals can, once we got that number, we can assess the person, not just with body weight, but we can use BIA to follow them through the season in a much more accurate way. So that allows a very expensive test, which is a specific gravity to go through the BIAs. We also have issues and we’re going to touch upon these. But there are other special dynamics that parents can be involved and parents like Truide, you’re a parent of an athlete. What would you want to know in a BIA?
[00:16:22] Well, I have two athletes. Well, basically, I guess at what point is it safe with children to start watching, you know, and being concerned about, you know, BIA? Because certainly as young adolescents, you don’t want them prone to having eating disorders or being so self-conscious about their body composition that then you have other types of side effects of psychological approaches. So that will be one of my concerns. When is it safe from a parental stand to be watching about BIA and BMI?
[00:16:59] You know, that’s a very good question. And I guess what we would want to know is that we know that our kids are healthy when they’re with us, but when they’re going through certain dynamic changes. We want to follow up. We want to see when is it getting too concentrated? When is the kid losing too much protein? When is the child running the risk of hurt because we do have the stories of the 180 pounder cutting down to 135. That individual is not only running themselves at risk. But in the world that they’re wrestling someone, their own body weight, they’re running the risk of being injured. So as a parent, I see that very important. The BIA offers us the ability to be able to quantify and to see the measurable changes as the child goes through the process. Now, if you can look at these areas, now there are other areas. And one of the things that we have here, our chief editor has found out some really interesting dynamics, specifically how assessing BMI actually has other consequences and things that we can assess for those things. Astrid, one of the things that you’ve seen in the process when you have gone through the process, tell us a little bit about what you’ve found out about the BMI and BIA in terms of brain health.
[00:18:09] OK. So there are actually quite a few research studies that have been conducted on pretty much the importance of BMI and BIA and why it’s, you know, we all want to know these, I guess, these values so that, you know, because obesity or having excess weight, you know, which you use BMI and BIA to determine, you know, it can affect a variety of functions. And like you said, research studies have actually found that obesity can actually affect your brain health. And there’s actually like probably one of the biggest things like there are several things that obesity, can affect brain health because it increases inflammation in your body and it could even speed up the neurodegeneration process like your brain ages a lot faster.
[00:19:09] Wait a second. Wait a second. So, it actually makes your brain kind of lose its intelligence.
[00:19:15] I wouldn’t say it makes you lose your intelligence. It just makes it work slower. Slower. Yes. Ok.
[00:19:21] So brains that get smaller. Or let’s say dementia. Well, let’s say the brain becomes, loses its size and dimension.
[00:19:29] So those things we could, are correlated to BMI as well.
[00:19:34] Well, you want to know your, it’s important to know your BMI or your BIA.
[00:19:39] You know, interchangeably like depending on what would it be more important to know or the person? Because like research studies have found that if you have excess weight or if you have obesity, that it can actually change the size of your brain and it can decrease or just alter the gray matter and the white matter of the brain and that can age your brain a lot faster and it can slow down your cognitive functions and it can even affect your memory. And you’ll have a harder time remembering things simply by having excess weight.
[00:20:25] I read something today that said even dopamine is affected by, the production of dopamine potentially is correlatable or associated with BMI values.
[00:20:36] Ok. So what scientists have found is that if you have a lot of excess weight, you know, if you’re overweight or if you have, you’re a person with obesity.
[00:20:49] The thing is that.
[00:20:52] Excess weight or obesity, it can go as far as affecting what’s known as your pleasure and reward center of the brain. And that is, it’s pretty much the region of the brain that controls the release of dopamine. Just being like having obesity in itself could even cause your brain to release less amount of dopamine. And that can cause a variety of mental health issues. And it could even lead to depression just by having excess weight.
[00:21:26] So BMI, you know, let’s pop it up first to Alexander, make his screen bigger, let’s go to the HDMI. He’s noticed some things here. Alex, can you tell us a bit about what you’re actually putting up on there?
[00:21:36] Perfect. So you guys can see my screen right there? Yes, we sure can. Awesome. So like Astrid was saying that adipose tissue does have an effect on certain things.
[00:21:46] We have to take a look at adipose tissue at the cellular level. Normally, adipose tissue, large amounts in certain areas were meant for producing hormones and not all adipose tissue is created equally. So we could see that, here’s the average individual that would have what people call a beer gut. And here’s the pear-shaped as what a normal individual would have as well, for most females. So we could see that we have pear, which would be gynoid, and android, which would be apple. But we could see that males who tend to have these tend to produce a little bit more estrogen, affects the males differently. We can also see the ratio of significant health risks. So males have a 95 percent increase in percentage for developing other health risks while females are different. Now, when it comes to losing this type of way, we have to keep in mind that not all adipose tissue is created equally, as my professor likes to say. So we can see that even though we have the same amount of adipose tissue in both areas, they’re in completely different areas.
[00:22:48] So most of the time you’ll hear the saying that some women have trouble losing weight, which is correct because of their adipose tissue located in different areas. It’s not as metabolically active, which is good for them because they don’t produce as much hormones from it. They don’t get much stress from it. Now, on the other hand, the visceral fat releases hormones and this is the one that is problematic to individuals but can also be reduced a lot quicker. So when you’re kind of coming down to the breakdown of the main macromolecules of the bodies, we could see there were 5 percent minerals, calcium, 15 percent fat, 1 percent carbs, and 60 percent water mostly. So we can kind of see what the reference ranges are here for the reference man aged 20 to 24 years and the reference woman 20 to 24. And coming back to Mrs. Truide when she was mentioning what is the safe and recommended way? Well, it’s hit and miss. It’s different from males and females. For males you want to keep anywhere between always stay above 3 percent body fat, anything below that becomes detrimental and your body starts to break down. But for females, on the other hand, we can see that once they start dropping below 15 percentage, they actually will miss their period if it drops below that. So if a female athlete or a tri triathlete does this, it will, honestly. So there’s been cases where female athletes develop osteoporosis just because they produce less estrogen, only because they drop below that 15 percent body weight. And females need more adipose tissue than men. It’s just the way we came through evolution and we were designed and it’s just the way it is and needs to be. So for females, as long as they’re above 15 percent body fat, they’re always gonna be healthy. For males, it’s a long as long as it’s above 3 percent, they’re always going to be healthy. It’s very hard to attain 3 percent for males, but as long as they usually stay between this, you can kind of see what body masses, lean body masses muscle on kind of the breakdown of everything from there.
[00:24:48] Answering the question regarding Truide’s particular question, cause that’s the bottom line is, what is the 25-year-old mom? What is the mom that’s 27, 28 years old with a five year old little boy, with a 10 year old little boy. What is she got to do? Go ahead and put up the 550 up there for me. What we’re looking at here is we want to be able to quantify these things. And one of the things I’d like to show you that is available in today’s research is the ability to determine certain things. Body composition analysis takes a lot of different studies and a lot of different dynamics in its research. We’ve been able to look at questions that are more specific for someone like Truide and her child to be able to assess the variable changes, body composition. And we’re going to follow up with the follow up videos discussing this particular issue. But the studies today, we can actually see in this particular area that we can assess muscle body fat analysis and the ranges versus the total body fat. We can look at obesity analysis and we can measure the ranges, Ok? We can look at percent body fat. We can look at extremity segmental lean body analysis versus one arm versus the other. This particularly comes in and true because let’s assume someone has an ACL injury on the right leg or left leg. You’ll notice that there will be a variation of body mass changes and to be able to determine if the body protein in that leg is getting more developed, in a leg that has noted atrophy there will be obvious changes in terms of the amount of protein or the amount of difference in percent body fat as well as water retention in that area. If someone has a swollen knee, you can also see the difference. Now the total area and the body weight, we can start measuring and just start noticing this. This is what helps mother Truide’s around the world understand the continuous. You’ll notice down here on the bottom that there are reference dates here where we can actually see the changes as time goes by. And once you see the changes as time goes by, it gives you a lot better tools. Now, the other thing that we’ve noticed here in terms of this particular area is the awareness that we can actually do visceral body fat that Alexander referred to. We want to be able to see what is inside the body. Now, visceral body fat is if you open a body up, there’s fat that surrounds each area, like the liver, the intestines. We call it the peritoneal area, Pernille, area that basically holds the body fat and holds the amount of tissue to protect it. And that’s how nature has done it. But we want to know how much it is. And if it does produce hormones that are bad like cortisol or produces hormones, that we know about that for a different video, we can see that that would mean not good. So the person with fat that’s around the viscera is at higher risk. So that analysis and to be able to give a point and see the changes is very important. So one of the things is that we can do. And as we talked about here, you can actually see the impedance by the individual depending on which extremity it is. So the tests on a regular basis, those simple as that may be standing on a thing. They’re very complex and very accurate. So it does bode well for someone that really needs it, that has a family that is going through these kinds of techniques so that we can reassess. Initially, you can start someone with a, to be real detailed and to be accountable to the individual by specific gravity to determine the concentration of body, metabolites in the body, and the proteins, and the level of dehydration the person may have. Then you can follow up with a BIA repetitively through the history of a season and you can really get a lot of information as to how your child is going if it’s a healthy form of weight loss. So, Alex, I notice that you put up some things up there. Can you open that up? And you’re putting up some interesting dynamics there. What is it that you’re noticing there? What did you put there?
[00:28:32] So we can see that these are some of the graphs that I just got from classes here so we can see that correlation is not cause for causation, but it does correlate to the data of many individuals. This was taken from a study. And what they found is that people with a higher body mass index tend to have a higher risk for certain diseases, such as cardiovascular disease or cancer or all other causes, just illnesses in general. And we also have to keep in mind that women do have more receptors for those hormones produced by adipose tissue. So they are more susceptible to cancers. So we have to ask ourselves, what is the point of, you know, losing weight besides just the cancer thing? So we come down here, we can just see the correlation of the lifestyle of individuals just if they lose 10 percent body weight. So if their obesity is decreased, their life expectancy increases for about seven years. But not only that, but you can see where the circle of lifestyle changes for this individual who not only begins to change their lifestyle but also operates those healthy choices into their daily environment.
[00:29:42] Makes sense. So these are very, very important things to assess on a regular basis. So what I’ve learned is the BIA, BMI, in general, is a very important method to be able to assess the overall health and the progression of health. So we want to get a better BMI and we want to get a better, be able to assess the regions of the body and to assess the dynamics of what someone can do to monitor their true health. We’re going to be following through with follow-up studies and the follow-up information and on these follow-up programs to teach about what we use here in our little town of El Paso, which is a big town. But we’re gonna be bringing families. We’re gonna be bringing athletes to discuss those things. We’re gonna get real technical right on the screen right now. We have a real interesting dynamics to the level that we’re gonna be pushing the knowledge of. Can you pull back to the screen? You actually can see it right there. You can actually see biochemistry. And we have our resident and biochemistry expert right there. Alexander, tell us what we’re looking at there.
[00:30:46] So here we’re kind of going through the synthesis of cholesterol and what it takes to actually produce cholesterol. So it’s kind of a very complex pathway. But we can also see that it takes your body a lot of stress to really produce high cholesterol levels as well as cortisol levels. So kind of coming into the main breakdown of what kind of goes down, if you have a very increased dietary cholesterol intake, not only are you putting more stress on the liver, but you’re also increasing more LDL. LDL just tends to be bad in general because the LDL is…
[00:31:23] I’m sorry, Alex was is LDL?
[00:31:25] Low-density lipoprotein. Got it. So the problem with the low-density lipoproteins is that their main job is to drop off the correct cholesterol to the proper levels. Now if they turn into LDLs, the problem is that if they don’t get reabsorbed by the liver or a good way, I think of it as, they are thought of as a suicide bomber. Pretty much so. What they do is they deposit. If they don’t deposit and don’t get absorbed by the liver because the liver is being bombarded by too much cholesterol, they will actually deposit themselves into other tissues, specifically the epithelial lining of the extracellular part of capillaries. Then at that point macrophages will actually try to eat them up and create these things called foam cells. Foam cells tend to aggregate and they’re really large cells that have no purpose other than to aggregate within the layers of the capillaries.
[00:32:24] Is that what the protective mechanism, is that what the body does?
[00:32:27] It pretty much just tries to seal it off so it can’t affect anything else. But in doing so, it clogs arteries.
[00:32:33] Okay. So BMI would be able to determine the overall health of the body and fat. So it would tend to, we would tend to say that a person with a, let’s say a high BMI, extremely high BMI and the obese level would have more of this action happening. Right?
[00:32:49] Exactly. But we also have to take a look at a different thing. So let’s say this person is already morbidly obese and their cholesterol is high. So they go to an M.D., their M.D. gives them a statin. So statins are good to an extent. So, yes, they’re going to decrease the level of cholesterol, but they’re also going to decrease. See if I can find it here. The levels of all these other hormones being produced because cholesterol is the driving force for all these hormones. So if you are decreasing your cholesterol, you are decreasing for women their progesterone for men, their testosterone, their dihydrotestosterone was kind of what people describe as the old man’s strength. As you get older, you produce more DHT, but you’re also decreasing these. Not only are you decreasing cholesterol, but you’re also decreasing by 50 percent coenzyme-Q. Coenzyme-Q it was the main electron transporter for the electron transport chain and it transports electrons that certain parts in the pathway which we won’t go into. But if you decrease that by 50 percent, most of these people feel tired all the time. And what’s the tissue that has the most mitochondria in the entire body? Muscle. The heart. Oh, okay. So the heart. So not only are they decreasing their energy levels, they’re decreasing the ability of their actual lifeline, pretty much, their heart to produce and pump blood and get energy. So by just decreasing body weight, decreasing cholesterol intake in a moderate amount because cholesterol is good, we need it for everything. Too much of one thing can kill you, though. So within moderate amounts, exercise, dietary regimens, you won’t need to be put on statins and you can be weaned off of those in time as your cholesterol levels get to an appropriate level.
[00:34:37] That’s amazing, Alex. So that’s at the microscopic level. At the macroscopic level, we can assess that by visceral fat. So the more visceral fat you got, the more hormones you got going haywire. And it’s fair to say that we have a situation where you’re less healthy with visceral fat. Ok. So does anyone else have any input in here? Any other questions that you would want to know about Mrs. Truide as a mom of athletes?
[00:35:02] No, I guess just the woman on a side note, if all of this is very complex. The bottom line is if you’re having to lay down in your bed to tie your jeans, you’re not having a healthy BMI.
[00:35:14] That’s very true. Right. So basically, if your gut hangs over, you’re in trouble, right? So that’s where you can use the simple tests of the waist circumference or the waist-hip balance. And if pretty much the belly is three inches bigger than the hips, you are probably at a BMI that you shouldn’t have. So I hope. OK, go ahead. Astrid, you want to say something.
[00:35:36] So essentially, it’s just super important to find out your, I guess, your BMI or your BIA interchangeably pretty much for overall health, because just having excess weight, as we’ve found out here, it can affect a whole variety of functions. Brain health, cardiovascular, health, and finding your BMI and your BIA seems like such an easy, you know, like an easy way to kind of find out if your weight is like at a healthier range. And it all kind of goes like hand-in-hand with all these things, as you’ve explained and as Alex explained. Pretty much like being, having obesity or excess weight, it can just disrupt our entire body, our entire system.
[00:36:37] Exactly. Kenna. Any other comments in terms of specifics on questions?
[00:36:43] Not for questions, just for that waist to hip ratio. We’re gonna want to make sure that for women, they’re under one. And the same thing for males. So you’re gonna divide your waist by your hip ratio to get that number. Right.
[00:36:58] So the numerator hopefully won’t be too bigger than the denominator, right? Yeah. So that would be the numerator would be the waist and the denominator would be the hip. Right. So we want to keep those in line. So all those kinds of things are very important. We’ve learned a lot today. We’re going to come back with a much more elaborate and we’re gonna splice this up in many ways. I want to thank Alexander for coming in from Illinois at the National University of Health Sciences way out there. This probably about 2000 miles away. We have Truide, Mrs. Truide who’s giving us a point of view. We have Astrid who’s given us the scientific approach of the brain and dopamine connection. But we also need to know that there’s a lot of reasons why the BMI. As we learn every day through the NCBI research institutes of information, that there are lots of reasons why to keep a BMI low and also to make sure you watch your BIAs in time. So we look forward to bringing it to you. And we thank you for watching us and we look forward to giving more information. Alexander, thank you so much for coming from a distance and making it real cool for us all.
[00:38:01] Ok, thank you. Thank you for having me. You’re welcome. Appreciate it. Thanks.
Additional Topic Discussion: Chronic Pain
Sudden pain is a natural response of the nervous system which helps to demonstrate possible injury. By way of instance, pain signals travel from an injured region through the nerves and spinal cord to the brain. Pain is generally less severe as the injury heals, however, chronic pain is different than the average type of pain. With chronic pain, the human body will continue sending pain signals to the brain, regardless if the injury has healed. Chronic pain can last for several weeks to even several years. Chronic pain can tremendously affect a patient’s mobility and it can reduce flexibility, strength, and endurance.
Neural Zoomer Plus for Neurological Disease
Dr. Alex Jimenez utilizes a series of tests to help evaluate neurological diseases. The Neural ZoomerTM Plus is an array of neurological autoantibodies which offers specific antibody-to-antigen recognition. The Vibrant Neural ZoomerTM Plus is designed to assess an individual�s reactivity to 48 neurological antigens with connections to a variety of neurologically related diseases. The Vibrant Neural ZoomerTM Plus aims to reduce neurological conditions by empowering patients and physicians with a vital resource for early risk detection and an enhanced focus on personalized primary prevention.
Food Sensitivity for the IgG & IgA Immune Response
Dr. Alex Jimenez utilizes a series of tests to help evaluate health issues associated with a variety of food sensitivities and intolerances. The Food Sensitivity ZoomerTM is an array of 180 commonly consumed food antigens that offers very specific antibody-to-antigen recognition. This panel measures an individual�s IgG and IgA sensitivity to food antigens. Being able to test IgA antibodies provides additional information to foods that may be causing mucosal damage. Additionally, this test is ideal for patients who might be suffering from delayed reactions to certain foods. Utilizing an antibody-based food sensitivity test can help prioritize the necessary foods to eliminate and create a customized diet plan around the patient�s specific needs.
Gut Zoomer for Small Intestinal Bacterial Overgrowth (SIBO)
Dr. Alex Jimenez utilizes a series of tests to help evaluate gut health associated with small intestinal bacterial overgrowth (SIBO). The Vibrant Gut ZoomerTM offers a report that includes dietary recommendations and other natural supplementation like prebiotics, probiotics, and polyphenols. The gut microbiome is mainly found in the large intestine and it has more than 1000 species of bacteria that play a fundamental role in the human body, from shaping the immune system and affecting the metabolism of nutrients to strengthening the intestinal mucosal barrier (gut-barrier). It is essential to understand how the number of bacteria that symbiotically live in the human gastrointestinal (GI) tract influences gut health because imbalances in the gut microbiome may ultimately lead to gastrointestinal (GI) tract symptoms, skin conditions, autoimmune disorders, immune system imbalances, and multiple inflammatory disorders.
Formulas for Methylation Support
XYMOGEN�s Exclusive Professional Formulas are available through select licensed health care professionals. The internet sale and discounting of XYMOGEN formulas are strictly prohibited.
Proudly,�Dr. Alexander Jimenez makes XYMOGEN formulas available only to patients under our care.
Please call our office in order for us to assign a doctor consultation for immediate access.
If you are a patient of Injury Medical & Chiropractic�Clinic, you may inquire about XYMOGEN by calling 915-850-0900.
For your convenience and review of the XYMOGEN products please review the following link. *XYMOGEN-Catalog-Download
* All of the above XYMOGEN policies remain strictly in force.
Modern Integrated Medicine
The National University of Health Sciences is an institution that offers a variety of rewarding professions to attendees. Students can practice their passion for helping other people achieve overall health and wellness through the institution’s mission. The National University of Health Sciences prepares students to become leaders in the forefront of modern integrated medicine, including chiropractic care. Students have an opportunity to gain unparalleled experience at the National University of Health Sciences to help restore the natural integrity of the patient and define the future of modern integrated medicine.
We usually talk of energy in general terms, as in �I don�t have a lot of energy today� or �You can feel the energy in the room.� But what really is energy? Where do we get the energy to move? How do we use it? How do we get more of it? Ultimately, what controls our movements? The three metabolic energy pathways are the�phosphagen system, glycolysis�and the�aerobic system.�How do they work, and what is their effect?
Albert Einstein, in his infinite wisdom, discovered that the total energy of an object is equal to the mass of the object multiplied by the square of the speed of light. His formula for atomic energy, E = mc2, has become the most recognized mathematical formula in the world. According to his equation, any change in the energy of an object causes a change in the mass of that object. The change in energy can come in many forms, including mechanical, thermal, electromagnetic, chemical, electrical or nuclear. Energy is all around us. The lights in your home, a microwave, a telephone, the sun; all transmit energy. Even though the solar energy that heats the earth is quite different from the energy used to run up a hill, energy, as the first law of thermodynamics tells us, can be neither created nor destroyed. It is simply changed from one form to another.
ATP Re-Synthesis
The energy for all physical activity comes from the conversion of high-energy phosphates (adenosine�triphosphate�ATP) to lower-energy phosphates (adenosine�diphosphate�ADP; adenosine�monophosphate�AMP; and inorganic phosphate, Pi). During this breakdown (hydrolysis) of ATP, which is a water-requiring process, a proton, energy and heat are produced: ATP + H2O ���ADP + Pi�+ H+�+ energy + heat. Since our muscles don�t store much ATP, we must constantly resynthesize it. The hydrolysis and resynthesis of ATP is thus a circular process�ATP is hydrolyzed into ADP and Pi, and then ADP and Pi�combine to resynthesize ATP. Alternatively, two ADP molecules can combine to produce ATP and AMP: ADP + ADP ���ATP + AMP.
Like many other animals, humans produce ATP through three metabolic pathways that consist of many enzyme-catalyzed chemical reactions: the phosphagen system, glycolysis and the aerobic system. Which pathway your clients use for the primary production of ATP depends on how quickly they need it and how much of it they need. Lifting heavy weights, for instance, requires energy much more quickly than jogging on the treadmill, necessitating the reliance on different energy systems. However, the production of ATP is never achieved by the exclusive use of one energy system, but rather by the coordinated response of all energy systems contributing to different degrees.
1. Phosphagen System
During short-term, intense activities, a large amount of power needs to be produced by the muscles, creating a high demand for ATP. The phosphagen system (also called the ATP-CP system) is the quickest way to resynthesize ATP (Robergs & Roberts 1997). Creatine phosphate (CP), which is stored in skeletal muscles, donates a phosphate to ADP to produce ATP: ADP + CP ���ATP + C. No carbohydrate or fat is used in this process; the regeneration of ATP comes solely from stored CP. Since this process does not need oxygen to resynthesize ATP, it is anaerobic, or oxygen-independent. As the fastest way to resynthesize ATP, the phosphagen system is the predominant energy system used for all-out exercise lasting up to about 10 seconds. However, since there is a limited amount of stored CP and ATP in skeletal muscles, fatigue occurs rapidly.
2. Glycolysis
Glycolysis is the predominant energy system used for all-out exercise lasting from 30 seconds to about 2 minutes and is the second-fastest way to resynthesize ATP. During glycolysis, carbohydrate�in the form of either blood glucose (sugar) or muscle glycogen (the stored form of glucose)�is broken down through a series of chemical reactions to form pyruvate (glycogen is first broken down into glucose through a process called�glycogenolysis). For every molecule of glucose broken down to pyruvate through glycolysis, two molecules of usable ATP are produced (Brooks et al. 2000). Thus, very little energy is produced through this pathway, but the trade-off is that you get the energy quickly. Once pyruvate is formed, it has two fates: conversion to lactate or conversion to a metabolic intermediary molecule called acetyl coenzyme A (acetyl-CoA), which enters the mitochondria for oxidation and the production of more ATP (Robergs & Roberts 1997). Conversion to lactate occurs when the demand for oxygen is greater than the supply (i.e., during anaerobic exercise). Conversely, when there is enough oxygen available to meet the muscles� needs (i.e., during aerobic exercise), pyruvate (via acetyl-CoA) enters the mitochondria and goes through aerobic metabolism.
When oxygen is not supplied fast enough to meet the muscles� needs (anaerobic glycolysis), there is an increase in hydrogen ions (which causes the muscle pH to decrease; a condition called acidosis) and other metabolites (ADP, Pi�and potassium ions). Acidosis and the accumulation of these other metabolites cause a number of problems inside the muscles, including inhibition of specific enzymes involved in metabolism and muscle contraction, inhibition of the release of calcium (the trigger for muscle contraction) from its storage site in muscles, and interference with the muscles� electrical charges (Enoka & Stuart 1992; Glaister 2005; McLester 1997). As a result of these changes, muscles lose their ability to contract effectively, and muscle force production and exercise intensity ultimately decrease.
3. Aerobic System
Since humans evolved for aerobic activities (Hochachka, Gunga & Kirsch 1998; Hochachka & Monge 2000), it�s not surprising that the aerobic system, which is dependent on oxygen, is the most complex of the three energy systems. The metabolic reactions that take place in the presence of oxygen are responsible for most of the cellular energy produced by the body. However, aerobic metabolism is the slowest way to resynthesize ATP. Oxygen, as the patriarch of metabolism, knows that it is worth the wait, as it controls the fate of endurance and is the sustenance of life. �I�m oxygen,� it says to the muscle, with more than a hint of superiority. �I can give you a lot of ATP, but you will have to wait for it.�
The aerobic system�which includes the�Krebs cycle�(also called the�citric acid cycle or TCA cycle) and the�electron transport chain�uses blood glucose, glycogen and fat as fuels to resynthesize ATP in the mitochondria of muscle cells (see the sidebar �Energy System Characteristics�). Given its location, the aerobic system is also called�mitochondrial respiration.�When using carbohydrate, glucose and glycogen are first metabolized through glycolysis, with the resulting pyruvate used to form acetyl-CoA, which enters the Krebs cycle. The electrons produced in the Krebs cycle are then transported through the electron transport chain, where ATP and water are produced (a process called�oxidative phosphorylation) (Robergs & Roberts 1997). Complete oxidation of glucose via glycolysis, the Krebs cycle and the electron transport chain produces 36 molecules of ATP for every molecule of glucose broken down (Robergs & Roberts 1997). Thus, the aerobic system produces 18 times more ATP than does anaerobic glycolysis from each glucose molecule.
Fat, which is stored as triglyceride in adipose tissue underneath the skin and within skeletal muscles (called�intramuscular triglyceride), is the other major fuel for the aerobic system, and is the largest store of energy in the body. When using fat, triglycerides are first broken down into free fatty acids and glycerol (a process called�lipolysis). The free fatty acids, which are composed of a long chain of carbon atoms, are transported to the muscle mitochondria, where the carbon atoms are used to produce acetyl-CoA (a process called�beta-oxidation).
Following acetyl-CoA formation, fat metabolism is identical to carbohydrate metabolism, with acetyl-CoA entering the Krebs cycle and the electrons being transported to the electron transport chain to form ATP and water. The oxidation of free fatty acids yields many more ATP molecules than the oxidation of glucose or glycogen. For example, the oxidation of the fatty acid palmitate produces 129 molecules of ATP (Brooks et al. 2000). No wonder clients can sustain an aerobic activity longer than an anaerobic one!
Understanding how energy is produced for physical activity is important when it comes to programming exercise at the proper intensity and duration for your clients. So the next time your clients get done with a workout and think, �I have a lot of energy,� you�ll know exactly where they got it.
Energy System Characteristics
Energy System Workouts
Have clients warm up and cool down before and after each workout.
Phosphagen System
An effective workout for this system is short, very fast sprints on the treadmill or bike lasting 5�15 seconds with 3�5 minutes of rest between each. The long rest periods allow for complete replenishment of creatine phosphate in the muscles so it can be reused for the next interval.
2 sets of 8 x 5 seconds at close to top speed with 3:00 passive rest and 5:00 rest between sets
5 x 10 seconds at close to top speed with 3:00�4:00 passive rest
Glycolysis
This system can be trained using fast intervals lasting 30 seconds to 2 minutes with an active-recovery period twice as long as the work period (1:2 work-to-rest ratio).
8�10 x 30 seconds fast with 1:00 active recovery
4 x 1:30 fast with 3:00 active recovery
Aerobic System
While the phosphagen system and glycolysis are best trained with intervals, because those metabolic systems are emphasized only during high-intensity activities, the aerobic system can be trained with both continuous exercise and intervals.
60 minutes at 70%�75% maximum heart rate
15- to 20-minute tempo workout at lactate threshold intensity (about 80%�85% maximum heart rate)
5 x 3:00 at 95%�100% maximum heart rate with 3:00 active recovery
Brooks, G.A., et al. 2000.�Exercise Physiology: Human Bioenergetics and Its Applications.Mountain View, CA: Mayfield.
Enoka, R.M., & Stuart, D.G. 1992. Neurobiology of muscle fatigue.�Journal of Applied Physiology, 72�(5), 1631�48.
Glaister, M. 2005. Multiple sprint work: Physiological responses, mechanisms of fatigue and the influence of aerobic fitness.�Sports Medicine, 35�(9), 757�77.
Hochachka, P.W., Gunga, H.C., & Kirsch, K. 1998. Our ancestral physiological phenotype: An adaptation for hypoxia tolerance and for endurance performance?�Proceedings of the National Academy of Sciences, 95,�1915�20.
Hochachka, P.W., & Monge, C. 2000. Evolution of human hypoxia tolerance physiology.�Advances in Experimental and Medical Biology, 475,�25�43.
McLester, J.R. 1997. Muscle contraction and fatigue: The role of adenosine 5′-diphosphate and inorganic phosphate.�Sports Medicine, 23�(5), 287�305.
Robergs, R.A. & Roberts, S.O. 1997.�Exercise Physiology: Exercise, Performance, and Clinical Applications.�Boston: William C. Brown.
Abstract: Metabolic syndrome (MetS) is established as the combination of central obesity and different metabolic disturbances, such as insulin resistance, hypertension and dyslipidemia. This cluster of factors affects approximately 10%�50% of adults worldwide and the prevalence has been increasing in epidemic proportions over the last years. Thus, dietary strategies to treat this heterogenic disease are under continuous study. In this sense, diets based on negative-energy-balance, the Mediterranean dietary pattern, n-3 fatty acids, total antioxidant capacity and meal frequency have been suggested as effective approaches to treat MetS. Furthermore, the type and percentage of carbohydrates, the glycemic index or glycemic load, and dietary fiber content are some of the most relevant aspects related to insulin resistance and impaired glucose tolerance, which are important co-morbidities of MetS. Finally, new studies focused on the molecular action of specific nutritional bioactive compounds with positive effects on the MetS are currently an objective of scientific research worldwide. The present review summarizes some of the most relevant dietary approaches and bioactive compounds employed in the treatment of the MetS to date.
It was during the period between 1910 and 1920 when it was suggested for the first time that a cluster of associated metabolic disturbances tended to coexist together [1]. Since then, different health organisms have suggested diverse definitions for metabolic syndrome (MetS) but there has not yet been a well-established consensus. The most common definitions are summarized in Table 1. What is clear for all of these is that the MetS is a clinical entity of substantial heterogeneity, commonly represented by the combination of obesity (especially abdominal obesity), hyperglycemia, dyslipidemia and/or hypertension [2�6].
Obesity consists of an abnormal or excessive fat accumulation, for which the main cause is a chronic imbalance between energy intake and energy expenditure [7,8]. The excess of energy consumed is primarily deposited in the adipose tissue as triglycerides (TG) [9].
Dyslipidemia encompasses elevated serum TG levels, increased low density lipoprotein- cholesterol (LDL-c) particles, and reduced levels of high density lipoprotein-cholesterol (HDL-c) [10]. It is associated with hepatic steatosis [11], dysfunction of pancreatic ?-cells [12] and elevated risk of atherosclerosis [13], among others.
Another main modifiable MetS manifestation is hypertension, which is mainly defined as a resting systolic blood pressure (SBP) ? 140 mmHg or diastolic blood pressure (DBP) ? 90 mmHg or drug prescription to lower hypertension [14]. It usually involves narrowed arteries and is identified as a major cardiovascular and renal risk factor, related to heart and vascular disease, stroke and myocardial infarction [13,15�17].
Hyperglycemia, related insulin resistance and type 2 diabetes mellitus are characterized by an impaired uptake of glucose by the cells, that lead to elevated plasma glucose levels, glycosuria and ketoacidosis [18]. It is responsible for different tissue damage that shortens the life expectancy of diabetics, involving cardiovascular diseases (CVD), atherosclerosis, hypertension [19], ?-cell dysfunction [12], kidney disease [20] or blindness [21]. Currently, diabetes is considered the leading cause of death in developed countries [22].
Moreover, oxidative stress and low grade inflammation are two important mechanisms implicated in the etiology, pathogenesis, and development of MetS [23]. Oxidative stress is defined as an imbalance between the pro-oxidants and antioxidants in the body [24]. It plays a key role in the development of atherosclerosis by different mechanisms such as the oxidation of LDL-c particles [25] or impairment of HDL-c functions [26]. Inflammation is an immune system response to injury hypothesized to be a major mechanism in the pathogenesis and progression of obesity related disorders and the link between adiposity, insulin resistance, MetS and CVD [27].
Although the prevalence of the MetS varies broadly around the word and depends on the source used for its definition, it is clear that over the last 40�50 years the number of people presenting with this syndrome has risen in epidemic proportions [28]. Moreover, the frequency of this syndrome is increased in developed countries, sedentary people, smokers, low socioeconomic status population, as well as in individuals with unhealthy dietary habits [29,30].
For all of this, there is currently a wide concern to find effective strategies to detect, treat and control the comorbidities associated with MetS. This is a complex challenge as MetS is a clinical entity of substantial heterogeneity and therefore, the different cornerstones implicated in its development should be addressed. In this review we compiled and examined different dietary patterns and bioactive compounds that have pointed out to be effective in MetS treatment.
2. Dietary Patterns
Several dietary strategies and their potential positive effects on the prevention and treatment of the different metabolic complications associated to the MetS, are described below and summarized in Table 2.
2.1. Energy-Restricted Diet Strategies
Energy restricted diets are probably the most commonly used and studied dietary strategies for combating excess weight and related comorbidities. They consist in personalized regimes that supply less calories than the total energy expended by a specific individual [31].
A hypocaloric diet results in a negative energy balance and subsequently, in body weight reduction [31]. Weight loss is achieved via fat mobilization from different body compartments as a consequence of the lipolysis process necessary to provide energy substrate [32,33]. In people who are overweight or suffering from obesity, as is the case of most people with MetS, weight loss is important as it is associated with improvement of related disorders such as abdominal obesity (visceral adipose tissue), type 2 diabetes, CVD or inflammation [32�36].
Moreover, as described above, low grade inflammation is associated with MetS and obesity. Therefore, of particular importance is the fact that in obese individuals following a hypocaloric diet, a depletion of plasma inflammatory markers such as interleukin (IL)-6 has been observed [34]. Thus, caloric restriction in obese people suffering MetS may improve the whole-body pro-inflammatory state.
At the same time, body weight reduction is associated with improvements in cellular insulin signal transduction, increments in peripheral insulin sensitivity and higher robustness in insulin secretory responses [32,36]. People with excess body weight who are at risk of developing type 2 diabetes, may benefit from a hypocaloric regime by improving plasma glucose levels and insulin resistance.
In addition, different intervention trials have reported a relationship between energy restricted diets and lower risk of developing CVD. In this sense, in studies with obese people following a hypocaloric diet, improvements in lipid profile variables such as reductions of LDL-c and plasma�TG levels, as well as improvements in hypertension via depletion of SBP and DBP levels have been observed [35,37].
Among the different nutritional intervention trials, a reduction of 500�600 kcal a day of the energy requirements is a well-established hypocaloric dietary strategy, which has demonstrated to be effective in weight reduction [38,39]. However, the challenge lies in maintaining the weight loss over time, as many subjects can follow a prescribed diet for a few months, but most people have difficulty in maintaining the acquired habits over the long term [40,41].
2.2. Diets Rich in Omega-3 Fatty Acids
The very long-chain eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) are essential omega-3 polyunsaturated fatty acids (n-3 PUFAs) for human physiology. Their main dietary sources are fish and algal oils and fatty fish, but they can also be synthesized by humans from ?-linolenic acid [40].
There is a moderate body of evidence suggesting that n-3 PUFAs, mainly EPA and DHA, have a positive role in the prevention and treatment of the pathologies associated to MetS [42].
In this context, it has been described that EPA and DHA have the ability to reduce the risk of developing CVD and cardiometabolic abnormalities as well as CVD-related mortality [42]. These beneficial effects are thought to be mainly due to the ability of these essential fatty acids to reduce plasma TG levels [43].
Moreover, different studies have shown that people following an increased n-3 PUFA diet have reduced plasma levels of the pro-inflammatory cytokines IL-6 and tumor necrosis factor-alpha (TNF?), as well as plasma C-reactive protein (CRP) [44]. These effects are probably mediated by resolvins, maresins and protectins, which are EPA and DHA metabolic products with anti-inflammatory properties [44].
There are some studies that have observed an association between n-3 ingestion and improvements or prevention of type 2 diabetes development. However, other studies found opposite results [44]. Thus, it cannot be made any specific affirmation in this respect.
The European Food Safety Authority recommends and intake of 250 mg EPA + DHA a day, in the general healthy population as a primary prevention of CVD [45]. These amounts can be achieved with an ingestion of 1�2 fatty fish meals per week [45].
2.3. Diets Based on Low Glycemic Index/Load
Over the last ten years, the concern about the quality of the carbohydrates (CHO) consumed has risen [46]. In this context, the glycemic index (GI) is used as a CHO quality measure. It consists in a ranking on a scale from 0 to 100 that classifies carbohydrate-containing foods according to the postprandial glucose response [47]. The higher the index, the more promptly the postprandial serum glucose rises and the more rapid the insulin response. A quick insulin response leads to rapid hypoglycemia, which is suggested to be associated with an increment of the feeling of hunger and to a subsequent higher caloric intake [47]. The glycemic load (GL) is equal to the GI multiplied by the number of grams of CHO in a serving [48].
There is a theory which states that MetS is a consequence of an elevated intake of high GI foods over time, among others unhealthy dietary habits [49]. In this sense, following a diet rich in high GI CHO has been associated with hyperglycemia, insulin resistance, type 2 diabetes, hypertriglyceridemia, CVD, and obesity [47,50,51], abnormalities directly related to MetS.
On the contrary, a low GI diet has been associated with slower absorption of the CHO and subsequently smaller blood glucose fluctuations, which indicate better glycemic control [46]. In patients with type 2 diabetes, diets based on low GI are associated with reductions in glycated hemoglobin (HbA1c) and fructosamine blood levels, two biomarkers used as key monitoring factors in diabetes management [52,53].
For all of this, it is common to find the limitation of CHO at high GI among the advice for MetS treatment [28], in particular with respect to �ready-to-eat processed foods� including sweetened beverages, soft drinks, cookies, cakes, candy, juice drinks, and other foods which contain high amounts of added sugars [54].
2.4. Diets with High Total Antioxidant Capacity
Dietary total antioxidant capacity (TAC) is an indicator of diet quality defined as the sum of antioxidant activities of the pool of antioxidants present in a food [55]. These antioxidants have the capacity to act as scavengers of free radicals and other reactive species produced in the organisms [56]. Taking into account that oxidative stress is one of the remarkable unfortunate physiological states of MetS, dietary antioxidants are of main interest in the prevention and treatment of this multifactorial disorder [57]. Accordingly, it is well-accepted that diets with a high content of spices, herbs, fruits, vegetables, nuts and chocolate, are associated with a decreased risk of oxidative stress-related diseases development [58�60]. Moreover, several studies have analyzed the effects of dietary TAC in individuals suffering from MetS or related diseases [61,62]. In the Tehran Lipid and Glucose Study it was demonstrated that a high TAC has beneficial effects on metabolic disorders and especially prevents weight and abdominal fat gain [61]. In the same line, research conducted in our institutions also evidenced that beneficial effects on body weight, oxidative stress biomarkers and other MetS features were positively related with higher TAC consumption in patients suffering from MetS [63�65].
In this sense, the World Health Organization (WHO) recommendation for fruit and vegetables consumption (high TAC foods) for the general population is a minimum of 400 g a day [66]. Moreover, cooking with spices is recommended in order to increase the TAC dietary intake and, at the same time, maintain flavor while reducing salt [67].
2.5. Moderate-High Protein Diets
The macronutrient distribution set in a weight loss dietary plan has commonly been 50%�55% total caloric value from CHO, 15% from proteins and 30% from lipids [57,68]. However, as most people have difficulty in maintaining weight loss achievements over time [69,70], research on increment of protein intake (>20%) at the expense of CHO was carried out [71�77].
Two mechanisms have been proposed to explain the potential beneficial effects of high-moderate protein diets: the increment of diet-induced thermogenesis [73] and the increase of satiety [78]. The increment of the thermogenesis is explained by the synthesis of peptide bonds, production of urea and gluconeogenesis, which are processes with a higher energy requirement than the metabolism of lipids or CHO [75]. An increment of different appetite-control hormones such as insulin, cholecystokinin or glucagon-like peptide 1, may clarify the satiety effect [79].
Other beneficial effects attributed to moderate-high protein diets in the literature are the improvement of glucose homeostasis [80], the possibility of lower blood lipids [81], the reduction of blood pressure [82], the preservation of lean body mass [83] or the lower of cardiometabolic disease risk [84,85]. However, there are other studies that have not found benefits associated to a moderate-high protein diet [76]. This fact may be explained by the different type of proteins and their amino acid composition [80], as well as by the different type of populations included in each study [85]. Therefore, more research in the field is needed in order to make these results consistent.
In any case, when a hypocaloric diet is implemented, it is necessary to slightly increase the amount of proteins. Otherwise it would be difficult to reach the protein energy requirements, established as 0.83 g/kg/day for isocaloric diets and which should probably be at least 1 g/kg/day for energy-restricted diets [86].
2.6. High Meal Frequency Pattern
The pattern of increasing meal frequency in weight loss and weight control interventions has currently become popular among professionals [87,88]. The idea is to distribute the total daily energy�intake into more frequently and smaller meals. However, there is no strong evidence about the efficacy of this habit yet [89]. While some investigations have found an inverse association between the increment of meals per day and body weight, body mass index (BMI), fat mass percentage or metabolic diseases such as coronary heart disease or type 2 diabetes [71,88,90�92], others have found no association [93�95].
Different mechanisms by which high meal frequency can have a positive effect on weight and metabolism management have been proposed. An increment of energy expenditure was hypothesized; however, the studies carried out in this line have concluded that total energy expenditure does not differ among different meal frequencies [96,97]. Another postulated hypothesis is that the greater the number of meals a day, the higher the fat oxidation, but again no consensus has been achieved [89,98]. An additional suggested mechanism is that increasing meal frequency leads to plasma glucose levels with lower oscillations and reduced insulin secretion which is thought to contribute to a better appetite control. However, these associations have been found in population with overweight or high glucose levels but in normal-weight or normoglycaemic individuals the results are still inconsistent [93,99�101].
2.7. The Mediterranean Diet
The concept of the Mediterranean Diet (MedDiet) was for the first time defined by the scientific Ancel Keys who observed that those countries around the Mediterranean Sea, which had a characteristic diet, had less risk of suffering coronary heart diseases [102,103].
The traditional MedDiet is characterized by a high intake of extra-virgin olive oil and plant foods (fruits, vegetables, cereals, whole grains, legumes, tree nuts, seeds and olives), low intakes of sweets and red meat and moderate consumption of dairy products, fish and red wine [104].
There is a lot of literature supporting the general health benefits of the MedDiet. In this sense, it has been reported that a high adherence to this dietary pattern protects against mortality and morbidity from several causes [105]. Thus, different studies suggested the MedDiet as a successful tool for the prevention and treatment of MetS and related comorbidities [106�108]. Moreover, recent meta-analysis concluded that the MedDiet is associated with less risk of developing type 2 diabetes and with a better glycemic control in people with this metabolic disorder [107,109,110]. Other studies have found a positive correlation between the adherence to a MedDiet pattern and reduced risk of developing CVD [111�114]. In fact, many studies have found a positive association between following a MedDiet and improvements in lipid profile by reduction of total cholesterol, LDL-c and TG, and an increase in HDL-c [111�115]. Finally, different studies also suggest that the MedDiet pattern may be a good strategy for obesity treatment as it has been associated with significant reductions in body weight and waist circumference [108,116,117].
The high amount of fiber which, among other beneficial effects, helps to weight control providing satiety; and the high antioxidants and anti-inflammatory nutrients such as n-3 fatty acids, oleic acid or phenolic compounds, are thought to be the main contributors to the positive effects attributed to the MedDiet [118].
For all these reasons, efforts to maintain the MedDiet pattern in Mediterranean countries and to implement this dietary habits in westernized countries with unhealthy nutritional patterns should be made.
3. Dietary: Single Nutrients and Bioactive Compounds
New studies focused on the molecular action of nutritional bioactive compounds with positive effects on MetS are currently an objective of scientific research worldwide with the aim of designing more personalized strategies in the framework of molecular nutrition. Among them, flavonoids and antioxidant vitamins are some of the most studied compounds with different potential benefits such as antioxidant, vasodilatory, anti-atherogenic, antithrombotic, and anti-inflammatory effects [119]. Table 3 summarizes different nutritional bioactive compounds with potential positive effects on MetS, including the possible molecular mechanism of action involved.
3.1. Ascorbate
Vitamin C, ascorbic acid or ascorbate is an essential nutrient as human beings cannot synthesize it. It is a water-soluble antioxidant mainly found in fruits, especially citrus (lemon, orange), and vegetables (pepper, kale) [120]. Several beneficial effects have been associated to this vitamin such as antioxidant and anti-inflammatory properties and prevention or treatment of CVD and type 2 diabetes [121�123].
This dietary component produces its antioxidant effect primarily by quenching damaging free radicals and other reactive oxygen and nitrogen species and therefore preventing molecules such as LDL-c from oxidation [122]. It can also regenerate other oxidized antioxidants like tocopherol [124].
Moreover, it has been described that ascorbic acid may reduce inflammation as it is associated with depletion of CRP levels [125]. This is an important outcome to take in consideration in the treatment of MetS sufferers, as they usually present low grade inflammation [27].
Supplementation with vitamin C have also been associated with prevention of CVD by improving the endothelial function [126] and probably by lowering blood pressure [121]. These effects are thought to be exerted by the ability of vitamin C to enhance the endothelial nitric oxide synthase enzyme (eNOS) activity and to reduce HDL-c glycation [127].
Additionally, several studies have attributed to ascorbate supplementation an antidiabetic effect by improving whole body insulin sensitivity and glucose control in people with type 2 diabetes [123]. These antidiabetic properties are thought to be mediated by optimization of the insulin secretory function of the pancreatic islet cells by increasing muscle sodium-dependent vitamin C transporters (SVCTs) [128].
Despite all of this, it should be taken into account that most people reach ascorbic acid requirements (established at 95�110 mg/day in the general population) from diet and do not need supplementation [122,129]. Besides, it should be considered that an excess of vitamin C ingestion leads to the opposite effect and oxidative particles are formed [130,131].
3.2. Hydroxytyrosol
Hydroxytyrosol (3,4-dihydroxyphenylethanol) is a phenolic compound mainly found in olives [132].
It is considered the strongest antioxidant of olive oil and one of the main antioxidants in nature [133]. It acts as a powerful scavenger of free radicals, as a radical chain breaker and as metal chelator [134]. It has the ability of inhibiting LDL-c oxidation by macrophages [132]. In this sense, it is the only phenol recognized by the European Food Safety Authority (EFSA) as a protector of blood lipids from oxidative damage [135].
Hydroxytyrosol has also been reported to have anti-inflammatory effects, probably by suppressing cyclooxygenase activity and inducing eNOS expression [136]. Thus, enhancement of olives/olive oil intakes or hydroxytyroxol supplementation in people suffering from MetS may be a good strategy in order to improve inflammatory status.
Another beneficial effect attributed to this phenolic compound is its cardiovascular protective effect. It presents anti-atherogenic properties by decreasing the expression of vascular cell adhesion protein 1 (VCAM-1) and intercellular adhesion molecule 1 (ICAM-1) [132,137], which are probably the result of an inactivation of the nuclear factor kappa-light-chain-enhancer of activated B cells (NF?B), activator protein 1 (AP-1), GATA transcription factor and nicotinamide adenine dinucleotide phosphate (NAD(P)H) oxidase [138,139]. Hydroxytyrosol also provides antidyslipidemic effects by lowering plasma levels of LDL-c, total cholesterol and TG, and by rising HDL-c [138].
Despite the beneficial effects attributed to hydfroxytyrosol as an antioxidant, for its antiinflamatory properties and as cardiovascular protector, it should be taken into account that most studies focused on this compound have been performed with mixtures of olive phenols, thus a synergic effect cannot be excluded [140].
3.3. Quercetin
Quercetin is a predominant flavanol naturally present in vegetables, fruits, green tea or red wine. It is commonly found as glycoside forms, where rutin is the most common and important structure found in nature [141].
Many beneficial effects that can contribute to MetS improvement have been attributed to quercetin. Among them, its antioxidant capacity should be highlighted, as it has been reported to inhibit lipid peroxidation and increase antioxidant enzymes such as superoxide dismutase (SOD), catalase (CAT) or glutathione peroxidase (GPX) [142].
Moreover, an anti-inflammatory effect mediated via attenuation of tumor necrosis factor ? (TNF-?), NF?B and mitogen-activated protein kinases (MAPK), as well as depletion of IL-6, IL-1?, IL-8 or monocyte chemoattractant protein-1 (MCP-1) gene expression has also been attributed to this polyphenol [143].
As most people with MetS are overweight or obese, the role of quercetin in body weight reduction and obesity prevention has been of special interest. In this sense, it stands out the capacity of quercetin to inhibit adipogenesis through inducing the activation of AMP-activated protein kinase (AMPK) and decreasing the expression of CCAAT-enhancer-binding protein-? (C/EBP?), peroxisome�proliferator-activated receptor gamma (PPAR?), and sterol regulatory element-binding protein 1 (SREBP-1) [141,144].
According to the antidiabetic effects, it is proposed that quercetin may act as an agonist of peroxisome proliferator-activated receptor gamma (PPAR?), and thus improve insulin-stimulated glucose uptake in mature adipocytes [145]. Moreover, quercetin may ameliorate hyperglycemia by inhibiting glucose transporter 2 (GLUT2) and insulin dependent phosphatidylinositol-3-kinase (PI3K) and blocking tyrosine kinase (TK) [142].
Finally, different studies observed that quercetin has the ability to reduce blood pressure [146�148]. However, the mechanisms of action are not clear, since some authors have suggested that quercetin increases eNOS, contributing to inhibition of platelet aggregation and improvement of the endothelial function [146,147], but there are other studies that have not come across these results [148].
3.4. Resveratrol
Resveratrol (3,5,4?-trihidroxiestilben) is a phenolic compound mainly found in red grapes and derived products (red wine, grape juice) [149]. It has shown antioxidant and anti-inflammatory activities, and cardioprotective, anti-obesity and antidiabetic capacities [150�156].
The antioxidant effects of resveratrol have been reported to be carried out by scavenging of hydroxyl, superoxide, and metal-induced radicals as well as by antioxidant effects in cells producing reactive oxygen species (ROS) [150].
Moreover, it has been reported that the anti-inflammatory effects of resveratrol are mediated by inhibiting NF?B signaling [151]. Furthermore, this polyphenol reduces the expression of proinflammatory cytokines such as interleukin 6 (IL-6), interleukin 8 (IL-8), TNF-?, monocyte chemoattractant protein-1 (MCP-1) and eNOS [152]. In addition, resveratrol inhibits the cyclooxygenase (COX) expression and activity, a pathway involved in the synthesis of proinflammatory lipid mediators [152].
Concerning the effects of resveratrol against development of type 2 diabetes, it has been reported that treatment of diabetes patients with this polyphenol provides significant improvements in the status of multiple clinically relevant biomarkers such as fasting glucose levels, insulin concentrations or glycated hemoglobin and Homeostasis Model Assessment Insulin Resistance (HOMA-IR) [153,154].
Additionally, cardioprotective effects have been attributed to resveratrol. In this sense, it is suggested that resveratrol improves the endothelial function by producing nitric oxide (NO) through increasing the activity and expression of eNOS. This effect is thought to be conducted through activation of nicotinamide adenine dinucleotide-dependent deacetylase sirtuin-1 (Sirt 1) and 5? AMP-activated protein kinase (AMPK) [155]. Besides, resveratrol exerts endothelial protection by stimulation of NF-E2-related factor 2 (Nrf2) [156] and decreasing the expression of adhesion proteins such as ICAM-1 and VCAM-1 [152].
Finally, it has been described that resveratrol may have a role in preventing obesity as it has been related with energy metabolism improvement, increasing lipolysis and reducing lipogenesis [157]. However, more studies are needed in order to corroborate these findings.
3.5. Tocopherol
Tocopherols, also known as vitamin E, are a family of eight fat-soluble phenolic compounds whose main dietary sources are vegetable oils, nuts and seeds [130,158].
For a long time, it has been suggested that vitamin E could prevent different metabolic diseases as a potent antioxidant, acting as scavenger of lipid peroxyl radicals by hydrogen donating [159]. In this sense, it was described that tocopherols inhibit peroxidation of membrane phospholipids and prevent generation of free radicals in cell membranes [160].
Moreover, it has been shown that supplementation with ?-tocopherol or ?-tocopherol, two of the different isoforms of vitamin E, could have an effect on inflammation status by reducing CRP levels [161]. Additionally, inhibition of COX and protein kinase C (PKC) and reduction of cytokines�such as IL-8 or plasminogen activator inhibitor-1 (PAI-1) are other mechanisms that may contribute to these anti-inflammatory effects [162,163].
However, the beneficial effects attributed to this vitamin previously have lately became controversial as different clinical trials have not come across such benefits, but ineffective or even harmful effects have been observed [164]. It has been recently suggested that this may be explained by the fact that vitamin E may lose most of the antioxidant capacity when ingested by human beings through different mechanisms [162].
3.6. Anthocyanins
Anthocyanins are water-soluble polyphenolic compounds responsible for the red, blue and purple colors of berries, black currants, black grapes, peaches, cherries, plums, pomegranate, eggplant, black beans, red radishes, red onions, red cabbage, purple corn or purple sweet potatoes [165�167]. Actually, they are the most abundant polyphenols in fruits and vegetables [167]. Moreover, they can also be found in teas, honey, nuts, olive oil, cocoa, and cereals [168].
These compounds have high antioxidant capacity inhibiting or decreasing free radicals by donating or transferring electrons from hydrogen atoms [167].
Regarding clinical studies, it has been shown that these bioactive compounds may prevent type 2 diabetes development by improving insulin sensitivity [169]. The exact mechanisms by which anthocyanins exert their antidiabetic effect are not yet clear, but an enhancement of the glucose uptake by muscle and adipocyte cells in an insulin-independent manner has been suggested [169].
Moreover, it has been shown that anthocyanins may have the capacity to prevent CVD development by improving endothelial function via increasing brachial artery flow-mediated dilation and HDL-c, and decreasing serum VCAM-1 and LDL-c concentrations [170�173].
Finally, these polyphenolic compounds may exert anti-inflamatory effects via reducing proinflamatory molecules such as IL-8, IL-1? or CRP [172,174].
However, most studies have used anthocyanin-rich extracts instead of purified anthocyanins; thus, a synergic effect with other polyphenols cannot be discarded.
3.7. Catechins
Catechins are polyphenols that can be found in a variety of foods including fruits, vegetables, chocolate, wine, and tea [175]. The epigallocatechin 3-gallate present in tea leaves is the catechin class most studied [176].
Anti-obesity effects have been attributed to these polyphenols in different studies [176]. The mechanisms of action suggested to explain these beneficial effects on body weight are: increasing energy expenditure and fat oxidation, and reducing fat absorption [177]. It is thought that energy expenditure is enhanced by catechol-O-methyltransferase and phosphodiesterase inhibition, which stimulates the sympathetic nervous system causing an activation of the brown adipose tissue [178]. Fat oxidation is mediated by upregulation of acyl-CoA dehydrogenase and peroxisomal b-oxidation enzymes [178,179].
Moreover, catechin intake has also been associated with lower risk of CVD development by improving lipid biomarkers. Thus, it has been reported that consumption of this kind of polyphenols may increase HDL-c and decrease LDL-c and total cholesterol [180].
Finally, and antidiabetic effect has also been related to catechin comsumption, lowering fasting glucose levels [175] and improving insulin sensitivity [178].
4. Conclusions
As the prevalence of MetS reaches epidemic rates, the finding of an effective and easy-to-follow dietary strategy to combat this heterogenic disease is still a pending subject. This work recompiled different dietary nutrients and nutritional patterns with potential benefits in the prevention and�treatment of MetS and related comorbidities (Figure 1) with the aim of facilitating future clinical�studies in this area. The challenge now is to introduce precision bioactive compounds in personalized�nutritional patterns in order to gain the most benefits for prevention and treatment of this disease�through nutrition.
Conflicts of Interest: The authors declare no conflict of interest.
blank
References:
1. Sarafidis, P.A.; Nilsson, P.M. The metabolic syndrome: A glance at its history. J. Hypertens. 2006, 24, 621�626.
[CrossRef] [PubMed]
2. Alberti, K.G.; Zimmet, P.Z. Definition, diagnosis and classification of diabetes mellitus and its complications.
Part 1: Diagnosis and classification of diabetes mellitus provisional report of a WHO consultation.
Diabet. Med. 1998, 15, 539�553. [CrossRef]
3. Balkau, B.; Charles, M.A. Comment on the provisional report from the WHO consultation. European Group
for the Study of Insulin Resistance (EGIR). Diabet. Med. 1999, 16, 442�423. [PubMed]
4. Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive
Summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on
Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA
2001, 285, 2486�2497.
5. Grundy, S.M.; Cleeman, J.I.; Daniels, S.R.; Donato, K.A.; Eckel, R.H.; Franklin, B.A.; Gordon, D.J.;
Krauss, R.M.; Savage, P.J.; Smith, S.C., Jr.; et al. Diagnosis and management of the metabolic syndrome:
An American Heart Association/National Heart, Lung, and Blood Institute Scientific Statement. Circulation
2005, 112, 2735�2752. [CrossRef] [PubMed]
6. Alberti, K.G.; Zimmet, P.; Shaw, J. The metabolic syndrome�A new worldwide definition. Lancet 2005, 366,
1059�1062. [CrossRef]
7. Selassie, M.; Sinha, A.C. The epidemiology and aetiology of obesity: A global challenge. Best Pract. Res.
Clin. Anaesthesiol. 2011, 25, 1�9. [CrossRef] [PubMed]
8. WHO, W.H.O. Available online: http://www.who.int/mediacentre/factsheets/fs311/es/ (accessed on
4 June 2016).
9. Shimano, H. Novel qualitative aspects of tissue fatty acids related to metabolic regulation: Lessons from
Elovl6 knockout. Prog. Lipid Res. 2012, 51, 267�271. [CrossRef] [PubMed]
10. Bosomworth, N.J. Approach to identifying and managing atherogenic dyslipidemia: A metabolic
consequence of obesity and diabetes. Can. Fam. Phys. 2013, 59, 1169�1180.
11. Vidal-Puig, A. The Metabolic Syndrome and its Complex Pathophysiology. In A Systems Biology Approach to
Study Metabolic Syndrome; Oresic, M., Ed.; Springer: New York, NY, USA, 2014; pp. 3�16.
12. Poitout, V.; Robertson, R.P. Glucolipotoxicity: Fuel excess and beta-cell dysfunction. Endocr. Rev. 2008, 29,
351�366. [CrossRef] [PubMed]
13. Rizza, W.; Veronese, N.; Fontana, L. What are the roles of calorie restriction and diet quality in promoting
healthy longevity? Ageing Res. Rev. 2014, 13, 38�45. [CrossRef] [PubMed]
14. Lloyd-Jones, D.M.; Levy, D. Epidemiology of Hypertension. In Hypertension: A Companion to Braunwald�s
Heart Disease; Black, H.R., Elliott, W.J., Eds.; Elsevier: Philadephia, PA, USA, 2013; pp. 1�11.
15. Zanchetti, A. Challenges in hypertension: Prevalence, definition, mechanisms and management. J. Hypertens.
2014, 32, 451�453. [CrossRef] [PubMed]
16. Thomas, G.; Shishehbor, M.; Brill, D.; Nally, J.V., Jr. New hypertension guidelines: One size fits most?
Clevel. Clin. J. Med. 2014, 81, 178�188. [CrossRef] [PubMed]
17. James, P.A.; Oparil, S.; Carter, B.L.; Cushman, W.C.; Dennison-Himmelfarb, C.; Handler, J.; Lackland, D.T.;
LeFevre, M.L.; MacKenzie, T.D.; Ogedegbe, O.; et al. 2014 evidence-based guideline for the management
of high blood pressure in adults: Report from the panel members appointed to the Eighth Joint National
Committee (JNC 8). JAMA 2014, 311, 507�520. [CrossRef] [PubMed]
18. Klandorf, H.; Chirra, A.R.; DeGruccio, A.; Girman, D.J. Dimethyl sulfoxide modulation of diabetes onset in
NOD mice. Diabetes 1989, 38, 194�197. [CrossRef] [PubMed]
19. Ballard, K.D.; Mah, E.; Guo, Y.; Pei, R.; Volek, J.S.; Bruno, R.S. Low-fat milk ingestion prevents postprandial
hyperglycemia-mediated impairments in vascular endothelial function in obese individuals with metabolic
syndrome. J. Nutr. 2013, 143, 1602�1610. [CrossRef] [PubMed]
20. Pugliese, G.; Solini, A.; Bonora, E.; Orsi, E.; Zerbini, G.; Fondelli, C.; Gruden, G.; Cavalot, F.; Lamacchia, O.;
Trevisan, R.; et al. Distribution of cardiovascular disease and retinopathy in patients with type 2 diabetes
according to different classification systems for chronic kidney disease: A cross-sectional analysis of the
renal insufficiency and cardiovascular events (RIACE) Italian multicenter study. Cardiovasc. Diabetol. 2014,
13, 59. [PubMed]
21. Asif, M. The prevention and control the type-2 diabetes by changing lifestyle and dietary pattern. J. Educ.
Health Promot. 2014, 3, 1. [CrossRef] [PubMed]
22. Russell, W.R.; Baka, A.; Bjorck, I.; Delzenne, N.; Gao, D.; Griffiths, H.R.; Hadjilucas, E.; Juvonen, K.;
Lahtinen, S.; Lansink, M.; et al. Impact of Diet Composition on Blood Glucose Regulation. Crit. Rev. Food
Sci. Nutr. 2016, 56, 541�590. [CrossRef] [PubMed]
23. Soares, R.; Costa, C. Oxidative Stress, Inflammation and Angiogenesis in the Metabolic Syndrome; Springer:
Heidelberg, Germany, 2009.
24. Rahal, A.; Kumar, A.; Singh, V.; Yadav, B.; Tiwari, R.; Chakraborty, S.; Dhama, K. Oxidative Stress,
Prooxidants, and Antioxidants: The Interplay. BioMed Res. Int. 2014, 2014, 761264. [CrossRef] [PubMed]
25. Parthasarathy, S.; Litvinov, D.; Selvarajan, K.; Garelnabi, M. Lipid peroxidation and decomposition�Conflicting
roles in plaque vulnerability and stability. Biochim. Biophys. Acta 2008, 1781, 221�231. [CrossRef] [PubMed]
26. McGrowder, D.; Riley, C.; Morrison, E.Y.; Gordon, L. The role of high-density lipoproteins in reducing the
risk of vascular diseases, neurogenerative disorders, and cancer. Cholesterol 2011, 2011, 496925. [CrossRef]
[PubMed]
27. Ferri, N.; Ruscica, M. Proprotein convertase subtilisin/kexin type 9 (PCSK9) and metabolic syndrome:
Insights on insulin resistance, inflammation, and atherogenic dyslipidemia. Endocrine 2016. [CrossRef]
28. Oresic, M.; Vidal-Puig, A. A Systems Biology Approach to Study Metabolic Syndrome; Springer: Heidelberg,
Germany, 2014.
29. Lee, E.G.; Choi, J.H.; Kim, K.E.; Kim, J.H. Effects of a Walking Program on Self-management and Risk Factors
of Metabolic Syndrome in Older Korean Adults. J. Phys. Ther. Sci. 2014, 26, 105�109. [CrossRef] [PubMed]
30. Bernabe, G.J.; Zafrilla, R.P.; Mulero, C.J.; Gomez, J.P.; Leal, H.M.; Abellan, A.J. Biochemical and nutritional
markers and antioxidant activity in metabolic syndrome. Endocrinol. Nutr. 2013, 61, 302�308.
31. Bales, C.W.; Kraus, W.E. Caloric restriction: Implications for human cardiometabolic health. J. Cardiopulm.
Rehabil. Prev. 2013, 33, 201�208. [CrossRef] [PubMed]
32. Grams, J.; Garvey, W.T. Weight Loss and the Prevention and Treatment of Type 2 Diabetes Using Lifestyle
Therapy, Pharmacotherapy, and Bariatric Surgery: Mechanisms of Action. Curr. Obes. Rep. 2015, 4, 287�302.
[CrossRef] [PubMed]
33. Lazo, M.; Solga, S.F.; Horska, A.; Bonekamp, S.; Diehl, A.M.; Brancati, F.L.; Wagenknecht, L.E.; Pi-Sunyer, F.X.;
Kahn, S.E.; Clark, J.M. Effect of a 12-month intensive lifestyle intervention on hepatic steatosis in adults with
type 2 diabetes. Diabetes Care 2010, 33, 2156�2163. [CrossRef] [PubMed]
34. Rossmeislova, L.; Malisova, L.; Kracmerova, J.; Stich, V. Adaptation of human adipose tissue to hypocaloric
diet. Int. J. Obes. 2013, 37, 640�650. [CrossRef] [PubMed]
35. Wing, R.R.; Lang, W.; Wadden, T.A.; Safford, M.; Knowler, W.C.; Bertoni, A.G.; Hill, J.O.; Brancati, F.L.;
Peters, A.; Wagenknecht, L. Benefits of modest weight loss in improving cardiovascular risk factors in
overweight and obese individuals with type 2 diabetes. Diabetes Care 2011, 34, 1481�1486. [CrossRef]
[PubMed]
36. Golay, A.; Brock, E.; Gabriel, R.; Konrad, T.; Lalic, N.; Laville, M.; Mingrone, G.; Petrie, J.; Phan, T.M.;
Pietilainen, K.H.; et al. Taking small steps towards targets�Perspectives for clinical practice in diabetes,
cardiometabolic disorders and beyond. Int. J. Clin. Pract. 2013, 67, 322�332. [CrossRef] [PubMed]
37. Fock, K.M.; Khoo, J. Diet and exercise in management of obesity and overweight. J. Gastroenterol. Hepatol.
2013, 28, 59�63. [CrossRef] [PubMed]
38. Abete, I.; Parra, D.; Martinez, J.A. Energy-restricted diets based on a distinct food selection affecting the
glycemic index induce different weight loss and oxidative response. Clin. Nutr. 2008, 27, 545�551. [CrossRef]
[PubMed]
39. Alberti, K.G.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.C.; James, W.P.;
Loria, C.M.; Smith, S.C., Jr. Harmonizing the metabolic syndrome: A joint interim statement of the
International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung,
and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis
Society; and International Association for the Study of Obesity. Circulation 2009, 120, 1640�1645. [PubMed]
40. Fleming, J.A.; Kris-Etherton, P.M. The evidence for alpha-linolenic acid and cardiovascular disease benefits:
Comparisons with eicosapentaenoic acid and docosahexaenoic acid. Adv. Nutr. 2014, 5, 863S�876S. [CrossRef]
[PubMed]
41. Gray, B.; Steyn, F.; Davies, P.S.; Vitetta, L. Omega-3 fatty acids: A review of the effects on adiponectin and
leptin and potential implications for obesity management. Eur. J. Clin. Nutr. 2013, 67, 1234�1242. [CrossRef]
[PubMed]
42. Wen, Y.T.; Dai, J.H.; Gao, Q. Effects of Omega-3 fatty acid on major cardiovascular events and mortality
in patients with coronary heart disease: A meta-analysis of randomized controlled trials. Nutr. Metab.
Cardiovasc. Dis. 2014, 24, 470�475. [CrossRef] [PubMed]
43. Lopez-Huertas, E. The effect of EPA and DHA on metabolic syndrome patients: A systematic review of
randomised controlled trials. Br. J. Nutr. 2012, 107, 185�194. [CrossRef] [PubMed]
44. Maiorino, M.I.; Chiodini, P.; Bellastella, G.; Giugliano, D.; Esposito, K. Sexual dysfunction in women with
cancer: A systematic review with meta-analysis of studies using the Female Sexual Function Index. Endocrine
2016, 54, 329�341. [CrossRef] [PubMed]
45. EFSA NDA Panel (EFSA Panel on Dietetic Products, Nutrition and Allergies). Scientific Opinion on Dietary
Reference Values for fats, including saturated fatty acids, polyunsaturated fatty acids, monounsaturated
fatty acids, trans fatty acids, and cholesterol1. EFSA J. 2010, 8, 1461�1566.
46. Bellastella, G.; Bizzarro, A.; Aitella, E.; Barrasso, M.; Cozzolino, D.; di Martino, S.; Esposito, K.; de Bellis, A.
Pregnancy may favour the development of severe autoimmune central diabetes insipidus in women with
vasopressin cell antibodies: Description of two cases. Eur. J. Endocrinol. 2015, 172, K11�K17. [CrossRef]
[PubMed]
47. Sun, F.H.; Li, C.; Zhang, Y.J.; Wong, S.H.; Wang, L. Effect of Glycemic Index of Breakfast on Energy Intake at
Subsequent Meal among Healthy People: A Meta-Analysis. Nutrients 2016, 8, 37. [CrossRef] [PubMed]
48. Barclay, A.W.; Brand-Miller, J.C.; Wolever, T.M. Glycemic index, glycemic load, and glycemic response are
not the same. Diabetes Care 2005, 28, 1839�1840. [CrossRef] [PubMed]
49. Nakagawa, T.; Hu, H.; Zharikov, S.; Tuttle, K.R.; Short, R.A.; Glushakova, O.; Ouyang, X.; Feig, D.I.;
Block, E.R.; Herrera-Acosta, J.; et al. A causal role for uric acid in fructose-induced metabolic syndrome.
Am. J. Physiol. Ren. Physiol. 2006, 290, F625�F631. [CrossRef] [PubMed]
50. Symons Downs, D.; Hausenblas, H.A. Women�s exercise beliefs and behaviors during their pregnancy and
postpartum. J. Midwifery Women Health 2004, 49, 138�144.
51. Brand-Miller, J.; McMillan-Price, J.; Steinbeck, K.; Caterson, I. Dietary glycemic index: Health implications.
J. Am. Coll. Nutr. 2009, 28, 446S�449S. [CrossRef] [PubMed]
52. Thomas, D.; Elliott, E.J. Low glycaemic index, or low glycaemic load, diets for diabetes mellitus.
Cochrane Database Syst. Rev. 2009. [CrossRef]
53. Barrea, L.; Balato, N.; di Somma, C.; Macchia, P.E.; Napolitano, M.; Savanelli, M.C.; Esposito, K.; Colao, A.;
Savastano, S. Nutrition and psoriasis: Is there any association between the severity of the disease and
adherence to the Mediterranean diet? J. Transl. Med. 2015, 13, 18. [CrossRef] [PubMed]
54. Mathias, K.C.; Ng, S.W.; Popkin, B. Monitoring changes in the nutritional content of ready-to-eat grain-based
dessert products manufactured and purchased between 2005 and 2012. J. Acad. Nutr. Diet. 2015, 115, 360�368.
[CrossRef] [PubMed]
55. Serafini, M.; del Rio, D. Understanding the association between dietary antioxidants, redox status and
disease: Is the Total Antioxidant Capacity the right tool? Redox Rep. 2004, 9, 145�152. [CrossRef] [PubMed]
56. Bellastella, G.; Maiorino, M.I.; Olita, L.; della Volpe, E.; Giugliano, D.; Esposito, K. Premature ejaculation is
associated with glycemic control in Type 1 diabetes. J. Sex. Med. 2015, 12, 93�99. [CrossRef] [PubMed]
57. Zulet, M.A.; Moreno-Aliaga, M.J.; Martinez, J.A. Dietary Determinants of Fat Mass and Body Composition.
In Adipose Tissue Biology; Symonds, M.E., Ed.; Springer: New York, NY, USA, 2012; pp. 271�315.
58. Carlsen, M.H.; Halvorsen, B.L.; Holte, K.; Bohn, S.K.; Dragland, S.; Sampson, L.; Willey, C.; Senoo, H.;
Umezono, Y.; Sanada, C.; et al. The total antioxidant content of more than 3100 foods, beverages, spices,
herbs and supplements used worldwide. Nutr. J. 2010, 9, 3. [CrossRef] [PubMed]
59. Harasym, J.; Oledzki, R. Effect of fruit and vegetable antioxidants on total antioxidant capacity of blood
plasma. Nutrition 2014, 30, 511�517. [CrossRef] [PubMed]
60. Maiorino, M.I.; Bellastella, G.; Petrizzo, M.; della Volpe, E.; Orlando, R.; Giugliano, D.; Esposito, K. Circulating
endothelial progenitor cells in type 1 diabetic patients with erectile dysfunction. Endocrine 2015, 49, 415�421.
[CrossRef] [PubMed]
61. Bahadoran, Z.; Golzarand, M.; Mirmiran, P.; Shiva, N.; Azizi, F. Dietary total antioxidant capacity and the
occurrence of metabolic syndrome and its components after a 3-year follow-up in adults: Tehran Lipid and
Glucose Study. Nutr. Metab. 2012, 9, 70. [CrossRef] [PubMed]
62. Chrysohoou, C.; Esposito, K.; Giugliano, D.; Panagiotakos, D.B. Peripheral Arterial Disease and
Cardiovascular Risk: The Role of Mediterranean Diet. Angiology 2015, 66, 708�710. [CrossRef] [PubMed]
63. De la Iglesia, R.; Lopez-Legarrea, P.; Celada, P.; Sanchez-Muniz, F.J.; Martinez, J.A.; Zulet, M.A. Beneficial
effects of the RESMENA dietary pattern on oxidative stress in patients suffering from metabolic syndrome
with hyperglycemia are associated to dietary TAC and fruit consumption. Int. J. Mol. Sci. 2013, 14, 6903�6919.
[CrossRef] [PubMed]
64. Lopez-Legarrea, P.; de la Iglesia, R.; Abete, I.; Bondia-Pons, I.; Navas-Carretero, S.; Forga, L.; Martinez, J.A.;
Zulet, M.A. Short-term role of the dietary total antioxidant capacity in two hypocaloric regimes on obese
with metabolic syndrome symptoms: The RESMENA randomized controlled trial. Nutr. Metab. 2013, 10, 22.
[CrossRef] [PubMed]
65. Puchau, B.; Zulet, M.A.; de Echavarri, A.G.; Hermsdorff, H.H.; Martinez, J.A. Dietary total antioxidant
capacity is negatively associated with some metabolic syndrome features in healthy young adults. Nutrition
2010, 26, 534�541. [CrossRef] [PubMed]
66. World Health Organization. Obesity: Preventing and Managing the Global Epidemic; Report of a WHO
Consultation; World Health Organization Technical Report Series; WHO: Geneva, Switzerland, 2000.
67. Tapsell, L.C.; Hemphill, I.; Cobiac, L.; Patch, C.S.; Sullivan, D.R.; Fenech, M.; Roodenrys, S.; Keogh, J.B.;
Clifton, P.M.; Williams, P.G.; et al. Health benefits of herbs and spices: The past, the present, the future.
Med. J. Aust. 2006, 185, S4�S24. [PubMed]
68. Abete, I.; Astrup, A.; Martinez, J.A.; Thorsdottir, I.; Zulet, M.A. Obesity and the metabolic syndrome: Role of
different dietary macronutrient distribution patterns and specific nutritional components on weight loss and
maintenance. Nutr. Rev. 2010, 68, 214�231. [CrossRef] [PubMed]
69. Ebbeling, C.B.; Swain, J.F.; Feldman, H.A.; Wong, W.W.; Hachey, D.L.; Garcia-Lago, E.; Ludwig, D.S. Effects
of dietary composition on energy expenditure during weight-loss maintenance. JAMA 2012, 307, 2627�2634.
[CrossRef] [PubMed]
70. Abete, I.; Goyenechea, E.; Zulet, M.A.; Martinez, J.A. Obesity and metabolic syndrome: Potential benefit
from specific nutritional components. Nutr. Metab. Cardiovasc. Dis. 2011, 21, B1�B15. [CrossRef] [PubMed]
71. Arciero, P.J.; Ormsbee, M.J.; Gentile, C.L.; Nindl, B.C.; Brestoff, J.R.; Ruby, M. Increased protein intake and
meal frequency reduces abdominal fat during energy balance and energy deficit. Obesity 2013, 21, 1357�1366.
[CrossRef] [PubMed]
72. Wikarek, T.; Chudek, J.; Owczarek, A.; Olszanecka-Glinianowicz, M. Effect of dietary macronutrients on
postprandial incretin hormone release and satiety in obese and normal-weight women. Br. J. Nutr. 2014, 111,
236�246. [CrossRef] [PubMed]
73. Bray, G.A.; Smith, S.R.; de Jonge, L.; Xie, H.; Rood, J.; Martin, C.K.; Most, M.; Brock, C.; Mancuso, S.;
Redman, L.M. Effect of dietary protein content on weight gain, energy expenditure, and body composition
during overeating: A randomized controlled trial. JAMA 2012, 307, 47�55. [CrossRef] [PubMed]
74. Westerterp-Plantenga, M.S.; Nieuwenhuizen, A.; Tome, D.; Soenen, S.; Westerterp, K.R. Dietary protein,
weight loss, and weight maintenance. Annu. Rev. Nutr. 2009, 29, 21�41. [CrossRef] [PubMed]
75. Koppes, L.L.; Boon, N.; Nooyens, A.C.; van Mechelen, W.; Saris, W.H. Macronutrient distribution over
a period of 23 years in relation to energy intake and body fatness. Br. J. Nutr. 2009, 101, 108�115. [CrossRef]
[PubMed]
76. De Jonge, L.; Bray, G.A.; Smith, S.R.; Ryan, D.H.; de Souza, R.J.; Loria, C.M.; Champagne, C.M.;
Williamson, D.A.; Sacks, F.M. Effect of diet composition and weight loss on resting energy expenditure in
the POUNDS LOST study. Obesity 2012, 20, 2384�2389. [CrossRef] [PubMed]
77. Stocks, T.; Angquist, L.; Hager, J.; Charon, C.; Holst, C.; Martinez, J.A.; Saris, W.H.; Astrup, A.; Sorensen, T.I.;
Larsen, L.H. TFAP2B-dietary protein and glycemic index interactions and weight maintenance after weight
loss in the DiOGenes trial. Hum. Hered. 2013, 75, 213�219. [CrossRef] [PubMed]
78. Giugliano, D.; Maiorino, M.I.; Esposito, K. Linking prediabetes and cancer: A complex issue. Diabetologia
2015, 58, 201�202. [CrossRef] [PubMed]
79. Bendtsen, L.Q.; Lorenzen, J.K.; Bendsen, N.T.; Rasmussen, C.; Astrup, A. Effect of dairy proteins on appetite,
energy expenditure, body weight, and composition: A review of the evidence from controlled clinical trials.
Adv. Nutr. 2013, 4, 418�438. [CrossRef] [PubMed]
80. Heer, M.; Egert, S. Nutrients other than carbohydrates: Their effects on glucose homeostasis in humans.
Diabetes Metab. Res. Rev. 2015, 31, 14�35. [CrossRef] [PubMed]
81. Layman, D.K.; Evans, E.M.; Erickson, D.; Seyler, J.; Weber, J.; Bagshaw, D.; Griel, A.; Psota, T.; Kris-Etherton, P.
A moderate-protein diet produces sustained weight loss and long-term changes in body composition and
blood lipids in obese adults. J. Nutr. 2009, 139, 514�521. [CrossRef] [PubMed]
82. Pedersen, A.N.; Kondrup, J.; Borsheim, E. Health effects of protein intake in healthy adults: A systematic
literature review. Food Nutr. Res. 2013, 57, 21245. [CrossRef] [PubMed]
83. Daly, R.M.; O�Connell, S.L.; Mundell, N.L.; Grimes, C.A.; Dunstan, D.W.; Nowson, C.A. Protein-enriched
diet, with the use of lean red meat, combined with progressive resistance training enhances lean tissue mass
and muscle strength and reduces circulating IL-6 concentrations in elderly women: A cluster randomized
controlled trial. Am. J. Clin. Nutr. 2014, 99, 899�910. [CrossRef] [PubMed]
84. Arciero, P.J.; Gentile, C.L.; Pressman, R.; Everett, M.; Ormsbee, M.J.; Martin, J.; Santamore, J.; Gorman, L.;
Fehling, P.C.; Vukovich, M.D.; et al. Moderate protein intake improves total and regional body composition
and insulin sensitivity in overweight adults. Metab. Clin. Exp. 2008, 57, 757�765. [CrossRef] [PubMed]
85. Gregory, S.M.; Headley, S.A.; Wood, R.J. Effects of dietary macronutrient distribution on vascular integrity in
obesity and metabolic syndrome. Nutr. Rev. 2011, 69, 509�519. [CrossRef] [PubMed]
86. Consenso FESNAD-SEEDO. Recomendaciones nutricionales basadas en la evidencia para la prevenci�n y el
tratamiento del sobrepeso y la obesidad en adultos (Consenso FESNAD-SEEDO). Rev. Esp. Obes. 2011, 10, 36.
87. Jakubowicz, D.; Froy, O.; Wainstein, J.; Boaz, M. Meal timing and composition influence ghrelin levels,
appetite scores and weight loss maintenance in overweight and obese adults. Steroids 2012, 77, 323�331.
[CrossRef] [PubMed]
88. Schwarz, N.A.; Rigby, B.R.; La Bounty, P.; Shelmadine, B.; Bowden, R.G. A review of weight control strategies
and their effects on the regulation of hormonal balance. J. Nutr. Metab. 2011, 2011, 237932. [CrossRef]
[PubMed]
89. Ohkawara, K.; Cornier, M.A.; Kohrt, W.M.; Melanson, E.L. Effects of increased meal frequency on fat
oxidation and perceived hunger. Obesity 2013, 21, 336�343. [CrossRef] [PubMed]
90. Ekmekcioglu, C.; Touitou, Y. Chronobiological aspects of food intake and metabolism and their relevance on
energy balance and weight regulation. Obes. Rev. 2011, 12, 14�25. [CrossRef] [PubMed]
91. Lioret, S.; Touvier, M.; Lafay, L.; Volatier, J.L.; Maire, B. Are eating occasions and their energy content related
to child overweight and socioeconomic status? Obesity 2008, 16, 2518�2523. [CrossRef] [PubMed]
92. Bhutani, S.; Varady, K.A. Nibbling versus feasting: Which meal pattern is better for heart disease prevention?
Nutr. Rev. 2009, 67, 591�598. [CrossRef] [PubMed]
93. Leidy, H.J.; Tang, M.; Armstrong, C.L.; Martin, C.B.; Campbell, W.W. The effects of consuming frequent,
higher protein meals on appetite and satiety during weight loss in overweight/obese men. Obesity 2011, 19,
818�824. [CrossRef] [PubMed]
94. Mills, J.P.; Perry, C.D.; Reicks, M. Eating frequency is associated with energy intake but not obesity in midlife
women. Obesity 2011, 19, 552�559. [CrossRef] [PubMed]
95. Cameron, J.D.; Cyr, M.J.; Doucet, E. Increased meal frequency does not promote greater weight loss in subjects
who were prescribed an 8-week equi-energetic energy-restricted diet. Br. J. Nutr. 2010, 103, 1098�1101.
[CrossRef] [PubMed]
96. Smeets, A.J.; Lejeune, M.P.; Westerterp-Plantenga, M.S. Effects of oral fat perception by modified sham
feeding on energy expenditure, hormones and appetite profile in the postprandial state. Br. J. Nutr. 2009,
101, 1360�1368. [CrossRef] [PubMed]
97. Taylor, M.A.; Garrow, J.S. Compared with nibbling, neither gorging nor a morning fast affect short-term
energy balance in obese patients in a chamber calorimeter. Int. J. Obes. Relat. Metab. Disord. 2001, 25, 519�528.
[CrossRef] [PubMed]
98. Smeets, A.J.; Westerterp-Plantenga, M.S. Acute effects on metabolism and appetite profile of one meal
difference in the lower range of meal frequency. Br. J. Nutr. 2008, 99, 1316�1321. [CrossRef] [PubMed]
99. Heden, T.D.; LeCheminant, J.D.; Smith, J.D. Influence of weight classification on walking and jogging energy
expenditure prediction in women. Res. Q. Exerc. Sport 2012, 83, 391�399. [CrossRef] [PubMed]
100. Bachman, J.L.; Raynor, H.A. Effects of manipulating eating frequency during a behavioral weight loss
intervention: A pilot randomized controlled trial. Obesity 2012, 20, 985�992. [CrossRef] [PubMed]
101. Perrigue, M.M.; Drewnowski, A.; Wang, C.Y.; Neuhouser, M.L. Higher Eating Frequency Does Not Decrease
Appetite in Healthy Adults. J. Nutr. 2016, 146, 59�64. [CrossRef] [PubMed]
102. Keys, A. Coronary heart disease in seven countries. 1970. Nutrition 1997, 13, 249�253. [CrossRef]
103. Keys, A.; Menotti, A.; Aravanis, C.; Blackburn, H.; Djordevic, B.S.; Buzina, R.; Dontas, A.S.; Fidanza, F.;
Karvonen, M.J.; Kimura, N.; et al. The seven countries study: 2289 deaths in 15 years. Prev. Med. 1984, 13,
141�154. [CrossRef]
104. Davis, C.; Bryan, J.; Hodgson, J.; Murphy, K. Definition of the Mediterranean Diet; a Literature Review.
Nutrients 2015, 7, 9139�9153. [CrossRef] [PubMed]
105. Sofi, F.; Macchi, C.; Abbate, R.; Gensini, G.F.; Casini, A. Mediterranean diet and health status: An updated
meta-analysis and a proposal for a literature-based adherence score. Public Health Nutr. 2014, 17, 2769�2782.
[CrossRef] [PubMed]
106. Mayneris-Perxachs, J.; Sala-Vila, A.; Chisaguano, M.; Castellote, A.I.; Estruch, R.; Covas, M.I.; Fito, M.;
Salas-Salvado, J.; Martinez-Gonzalez, M.A.; Lamuela-Raventos, R.; et al. Effects of 1-year intervention with
a Mediterranean diet on plasma fatty acid composition and metabolic syndrome in a population at high
cardiovascular risk. PLoS ONE 2014, 9, e85202. [CrossRef] [PubMed]
107. Esposito, K.; Maiorino, M.I.; Bellastella, G.; Chiodini, P.; Panagiotakos, D.; Giugliano, D. A journey
into a Mediterranean diet and type 2 diabetes: A systematic review with meta-analyses. BMJ Open
2015, 5, e008222. [CrossRef] [PubMed]
108. Kastorini, C.M.; Milionis, H.J.; Esposito, K.; Giugliano, D.; Goudevenos, J.A.; Panagiotakos, D.B. The effect of
Mediterranean diet on metabolic syndrome and its components: A meta-analysis of 50 studies and 534,906
individuals. J. Am. Coll. Cardiol. 2011, 57, 1299�1313. [CrossRef] [PubMed]
109. Schwingshackl, L.; Missbach, B.; Konig, J.; Hoffmann, G. Adherence to a Mediterranean diet and risk of
diabetes: A systematic review and meta-analysis. Public Health Nutr. 2015, 18, 1292�1299. [CrossRef]
[PubMed]
110. Koloverou, E.; Esposito, K.; Giugliano, D.; Panagiotakos, D. The effect of Mediterranean diet on the
development of type 2 diabetes mellitus: A meta-analysis of 10 prospective studies and 136,846 participants.
Metab. Clin. Exp. 2014, 63, 903�911. [CrossRef] [PubMed]
111. Salas-Salvado, J.; Garcia-Arellano, A.; Estruch, R.; Marquez-Sandoval, F.; Corella, D.; Fiol, M.;
Gomez-Gracia, E.; Vinoles, E.; Aros, F.; Herrera, C.; et al. Components of the Mediterranean-type food
pattern and serum inflammatory markers among patients at high risk for cardiovascular disease. Eur. J.
Clin. Nutr. 2008, 62, 651�659. [CrossRef] [PubMed]
112. Martinez-Gonzalez, M.A.; Garcia-Lopez, M.; Bes-Rastrollo, M.; Toledo, E.; Martinez-Lapiscina, E.H.;
Delgado-Rodriguez, M.; Vazquez, Z.; Benito, S.; Beunza, J.J. Mediterranean diet and the incidence of
cardiovascular disease: A Spanish cohort. Nutr. Metab. Cardiovasc. Dis. 2011, 21, 237�244. [CrossRef]
[PubMed]
113. Fito, M.; Estruch, R.; Salas-Salvado, J.; Martinez-Gonzalez, M.A.; Aros, F.; Vila, J.; Corella, D.; Diaz, O.;
Saez, G.; de la Torre, R.; et al. Effect of the Mediterranean diet on heart failure biomarkers: A randomized
sample from the PREDIMED trial. Eur. J. Heart Fail. 2014, 16, 543�550. [CrossRef] [PubMed]
114. Estruch, R.; Ros, E.; Salas-Salvado, J.; Covas, M.I.; Corella, D.; Aros, F.; Gomez-Gracia, E.; Ruiz-Gutierrez, V.;
Fiol, M.; Lapetra, J.; et al. Primary prevention of cardiovascular disease with a Mediterranean diet. N. Engl.
J. Med. 2013, 368, 1279�1290. [CrossRef] [PubMed]
115. Serra-Majem, L.; Roman, B.; Estruch, R. Scientific evidence of interventions using the Mediterranean diet:
A systematic review. Nutr. Rev. 2006, 64, S27�S47. [CrossRef] [PubMed]
116. Esposito, K.; Kastorini, C.M.; Panagiotakos, D.B.; Giugliano, D. Mediterranean diet and weight loss:
Meta-analysis of randomized controlled trials. Metab. Syndr. Relat. Disord. 2011, 9, 1�12. [CrossRef]
[PubMed]
117. Razquin, C.; Martinez, J.A.; Martinez-Gonzalez, M.A.; Mitjavila, M.T.; Estruch, R.; Marti, A. A 3 years
follow-up of a Mediterranean diet rich in virgin olive oil is associated with high plasma antioxidant capacity
and reduced body weight gain. Eur. J. Clin. Nutr. 2009, 63, 1387�1393. [CrossRef] [PubMed]
118. Bertoli, S.; Spadafranca, A.; Bes-Rastrollo, M.; Martinez-Gonzalez, M.A.; Ponissi, V.; Beggio, V.; Leone, A.;
Battezzati, A. Adherence to the Mediterranean diet is inversely related to binge eating disorder in patients
seeking a weight loss program. Clin. Nutr. 2015, 34, 107�114. [CrossRef] [PubMed]
119. Rios-Hoyo, A.; Cortes, M.J.; Rios-Ontiveros, H.; Meaney, E.; Ceballos, G.; Gutierrez-Salmean, G. Obesity,
Metabolic Syndrome, and Dietary Therapeutical Approaches with a Special Focus on Nutraceuticals
(Polyphenols): A Mini-Review. Int. J. Vitam. Nutr. Res. 2014, 84, 113�123. [CrossRef] [PubMed]
120. Juraschek, S.P.; Guallar, E.; Appel, L.J.; Miller, E.R., 3rd. Effects of vitamin C supplementation on blood
pressure: A meta-analysis of randomized controlled trials. Am. J. Clin. Nutr. 2012, 95, 1079�1088. [CrossRef]
[PubMed]
121. Michels, A.J.; Frei, B. Myths, artifacts, and fatal flaws: Identifying limitations and opportunities in vitamin C
research. Nutrients 2013, 5, 5161�5192. [CrossRef] [PubMed]
122. Frei, B.; Birlouez-Aragon, I.; Lykkesfeldt, J. Authors� perspective: What is the optimum intake of vitamin C
in humans? Crit. Rev. Food Sci. Nutr. 2012, 52, 815�829. [CrossRef] [PubMed]
123. Mason, S.A.; della Gatta, P.A.; Snow, R.J.; Russell, A.P.; Wadley, G.D. Ascorbic acid supplementation
improves skeletal muscle oxidative stress and insulin sensitivity in people with type 2 diabetes: Findings of
a randomized controlled study. Free Radic. Biol. Med. 2016, 93, 227�238. [CrossRef] [PubMed]
124. Chambial, S.; Dwivedi, S.; Shukla, K.K.; John, P.J.; Sharma, P. Vitamin C in Disease Prevention and Cure:
An Overview. Indian J. Clin. Biochem. 2013, 28, 314�328. [CrossRef] [PubMed]
125. Block, G.; Jensen, C.D.; Dalvi, T.B.; Norkus, E.P.; Hudes, M.; Crawford, P.B.; Holland, N.; Fung, E.B.;
Schumacher, L.; Harmatz, P. Vitamin C treatment reduces elevated C-reactive protein. Free Radic. Biol. Med.
2009, 46, 70�77. [CrossRef] [PubMed]
126. Ashor, A.W.; Siervo, M.; Lara, J.; Oggioni, C.; Afshar, S.; Mathers, J.C. Effect of vitamin C and vitamin E
supplementation on endothelial function: A systematic review and meta-analysis of randomised controlled
trials. Br. J. Nutr. 2015, 113, 1182�1194. [CrossRef] [PubMed]
127. Kim, S.M.; Lim, S.M.; Yoo, J.A.; Woo, M.J.; Cho, K.H. Consumption of high-dose vitamin C (1250 mg
per day) enhances functional and structural properties of serum lipoprotein to improve anti-oxidant,
anti-atherosclerotic, and anti-aging effects via regulation of anti-inflammatory microRNA. Food Funct.
2015, 6, 3604�3612. [CrossRef] [PubMed]
128. Monfared, S.; Larijani, B.; Abdollahi, M. Islet transplantation and antioxidant management: A comprehensive
review. World J. Gastroenterol. 2009, 15, 1153�1161. [CrossRef]
129. German Nutrition Society (DGE). New Reference Values for Vitamin C Intake. Ann. Nutr. Metab. 2015,
67, 13�20.
130. Mamede, A.C.; Tavares, S.D.; Abrantes, A.M.; Trindade, J.; Maia, J.M.; Botelho, M.F. The role of vitamins in
cancer: A review. Nutr. Cancer 2011, 63, 479�494. [CrossRef] [PubMed]
131. Moser, M.A.; Chun, O.K. Vitamin C and Heart Health: A Review Based on Findings from Epidemiologic
Studies. Int. J. Mol. Sci. 2016, 17, 1328. [CrossRef] [PubMed]
132. Vilaplana-Perez, C.; Aunon, D.; Garcia-Flores, L.A.; Gil-Izquierdo, A. Hydroxytyrosol and potential uses in
cardiovascular diseases, cancer, and AIDS. Front. Nutr. 2014, 1, 18. [PubMed]
133. Achmon, Y.; Fishman, A. The antioxidant hydroxytyrosol: Biotechnological production challenges and
opportunities. Appl. Microbiol. Biotechnol. 2015, 99, 1119�1130. [CrossRef] [PubMed]
134. Bulotta, S.; Celano, M.; Lepore, S.M.; Montalcini, T.; Pujia, A.; Russo, D. Beneficial effects of the olive
oil phenolic components oleuropein and hydroxytyrosol: Focus on protection against cardiovascular and
metabolic diseases. J. Transl. Med. 2014, 12, 219. [CrossRef] [PubMed]
135. EFSA NDA Panel (EFSA Panel on Dietetic Products, Nutrition and Allergies). Scientific Opinion on the
substantiation of health claims related to polyphenols in olive and protection of LDL particles from oxidative
damage (ID 1333, 1638, 1639, 1696, 2865), maintenance of normal blood HDL cholesterol concentrations
(ID 1639). EFSA J. 2011, 9, 2033�2058.
136. Scoditti, E.; Nestola, A.; Massaro, M.; Calabriso, N.; Storelli, C.; De Caterina, R.; Carluccio, M.A.
Hydroxytyrosol suppresses MMP-9 and COX-2 activity and expression in activated human monocytes
via PKCalpha and PKCbeta1 inhibition. Atherosclerosis 2014, 232, 17�24. [CrossRef] [PubMed]
137. Giordano, E.; Dangles, O.; Rakotomanomana, N.; Baracchini, S.; Visioli, F. 3-O-Hydroxytyrosol glucuronide
and 4-O-hydroxytyrosol glucuronide reduce endoplasmic reticulum stress in vitro. Food Funct. 2015, 6,
3275�3281. [CrossRef] [PubMed]
138. Granados-Principal, S.; Quiles, J.L.; Ramirez-Tortosa, C.L.; Sanchez-Rovira, P.; Ramirez-Tortosa, M.C.
Hydroxytyrosol: From laboratory investigations to future clinical trials. Nutr. Rev. 2010, 68, 191�206.
[CrossRef] [PubMed]
139. Carluccio, M.A.; Siculella, L.; Ancora, M.A.; Massaro, M.; Scoditti, E.; Storelli, C.; Visioli, F.;
Distante, A.; De Caterina, R. Olive oil and red wine antioxidant polyphenols inhibit endothelial activation:
Antiatherogenic properties of Mediterranean diet phytochemicals. Arterioscler. Thromb. Vasc. Biol. 2003, 23,
622�629. [CrossRef] [PubMed]
140. Visioli, F.; Bernardini, E. Extra virgin olive oil�s polyphenols: Biological activities. Curr. Pharm. Des. 2011, 17,
786�804. [CrossRef] [PubMed]
141. Nabavi, S.F.; Russo, G.L.; Daglia, M.; Nabavi, S.M. Role of quercetin as an alternative for obesity treatment:
You are what you eat! Food Chem. 2015, 179, 305�310. [CrossRef] [PubMed]
142. Vinayagam, R.; Xu, B. Antidiabetic properties of dietary flavonoids: A cellular mechanism review.
Nutr. Metab. 2015, 12, 60. [CrossRef] [PubMed]
143. Shibata, T.; Nakashima, F.; Honda, K.; Lu, Y.J.; Kondo, T.; Ushida, Y.; Aizawa, K.; Suganuma, H.; Oe, S.;
Tanaka, H.; et al. Toll-like receptors as a target of food-derived anti-inflammatory compounds. J. Biol. Chem.
2014, 289, 32757�32772. [CrossRef] [PubMed]
144. Ahn, J.; Lee, H.; Kim, S.; Park, J.; Ha, T. The anti-obesity effect of quercetin is mediated by the AMPK and
MAPK signaling pathways. Biochem. Biophys. Res. Commun. 2008, 373, 545�549. [CrossRef] [PubMed]
145. Fang, X.K.; Gao, J.; Zhu, D.N. Kaempferol and quercetin isolated from Euonymus alatus improve glucose
uptake of 3T3-L1 cells without adipogenesis activity. Life Sci. 2008, 82, 615�622. [CrossRef] [PubMed]
146. Clark, J.L.; Zahradka, P.; Taylor, C.G. Efficacy of flavonoids in the management of high blood pressure.
Nutr. Rev. 2015, 73, 799�822. [CrossRef] [PubMed]
147. D�Andrea, G. Quercetin: A flavonol with multifaceted therapeutic applications? Fitoterapia 2015, 106, 256�271.
[CrossRef] [PubMed]
148. Larson, A.; Witman, M.A.; Guo, Y.; Ives, S.; Richardson, R.S.; Bruno, R.S.; Jalili, T.; Symons, J.D. Acute,
quercetin-induced reductions in blood pressure in hypertensive individuals are not secondary to lower
plasma angiotensin-converting enzyme activity or endothelin-1: Nitric oxide. Nutr. Res. 2012, 32, 557�564.
[CrossRef] [PubMed]
149. Tome-Carneiro, J.; Gonzalvez, M.; Larrosa, M.; Yanez-Gascon, M.J.; Garcia-Almagro, F.J.; Ruiz-Ros, J.A.;
Tomas-Barberan, F.A.; Garcia-Conesa, M.T.; Espin, J.C. Resveratrol in primary and secondary prevention of
cardiovascular disease: A dietary and clinical perspective. Ann. N. Y. Acad. Sci. 2013, 1290, 37�51. [CrossRef]
[PubMed]
150. Leonard, S.S.; Xia, C.; Jiang, B.H.; Stinefelt, B.; Klandorf, H.; Harris, G.K.; Shi, X. Resveratrol scavenges
reactive oxygen species and effects radical-induced cellular responses. Biochem. Biophys. Res. Commun. 2003,
309, 1017�1026. [CrossRef] [PubMed]
151. Ren, Z.; Wang, L.; Cui, J.; Huoc, Z.; Xue, J.; Cui, H.; Mao, Q.; Yang, R. Resveratrol inhibits NF-?B signaling
through suppression of p65 and I?B kinase activities. Die Pharm. 2013, 68, 689�694.
152. Latruffe, N.; Lancon, A.; Frazzi, R.; Aires, V.; Delmas, D.; Michaille, J.J.; Djouadi, F.; Bastin, J.;
Cherkaoui-Malki, M. Exploring new ways of regulation by resveratrol involving miRNAs, with emphasis on
inflammation. Ann. N. Y. Acad. Sci. 2015, 1348, 97�106. [CrossRef] [PubMed]
153. Hausenblas, H.A.; Schoulda, J.A.; Smoliga, J.M. Resveratrol treatment as an adjunct to pharmacological
management in type 2 diabetes mellitus�Systematic review and meta-analysis. Mol. Nutr. Food Res. 2015,
59, 147�159. [CrossRef] [PubMed]
154. Liu, K.; Zhou, R.; Wang, B.; Mi, M.T. Effect of resveratrol on glucose control and insulin sensitivity:
A meta-analysis of 11 randomized controlled trials. Am. J. Clin. Nutr. 2014, 99, 1510�1519. [CrossRef]
[PubMed]
155. Bitterman, J.L.; Chung, J.H. Metabolic effects of resveratrol: Addressing the controversies. Cell. Mol. Life Sci.
2015, 72, 1473�1488. [CrossRef] [PubMed]
156. Han, S.; Park, J.S.; Lee, S.; Jeong, A.L.; Oh, K.S.; Ka, H.I.; Choi, H.J.; Son, W.C.; Lee, W.Y.; Oh, S.J.; et al.
CTRP1 protects against diet-induced hyperglycemia by enhancing glycolysis and fatty acid oxidation.
J. Nutr. Biochem. 2016, 27, 43�52. [CrossRef] [PubMed]
157. Gambini, J.; Ingles, M.; Olaso, G.; Lopez-Grueso, R.; Bonet-Costa, V.; Gimeno-Mallench, L.; Mas-Bargues, C.;
Abdelaziz, K.M.; Gomez-Cabrera, M.C.; Vina, J.; et al. Properties of Resveratrol: In Vitro and In Vivo
Studies about Metabolism, Bioavailability, and Biological Effects in Animal Models and Humans. Oxid. Med.
Cell. Longev. 2015, 2015, 837042. [CrossRef] [PubMed]
158. Yang, C.S.; Suh, N. Cancer prevention by different forms of tocopherols. Top. Curr. Chem. 2013, 329, 21�33.
[PubMed]
159. Jiang, Q. Natural forms of vitamin E: Metabolism, antioxidant, and anti-inflammatory activities and their
role in disease prevention and therapy. Free Radic. Biol. Med. 2014, 72, 76�90. [CrossRef] [PubMed]
160. Witting, P.K.; Upston, J.M.; Stocker, R. The molecular action of alpha-tocopherol in lipoprotein lipid
peroxidation. Pro- and antioxidant activity of vitamin E in complex heterogeneous lipid emulsions.
In Fat-Soluble Vitamins; Quinn, P.J., Kagan, V.E., Eds.; Springer: New York, NY, USA; pp. 345�390.
161. Saboori, S.; Shab-Bidar, S.; Speakman, J.R.; Yousefi Rad, E.; Djafarian, K. Effect of vitamin E supplementation
on serum C-reactive protein level: A meta-analysis of randomized controlled trials. Eur. J. Clin. Nutr. 2015,
69, 867�873. [CrossRef] [PubMed]
162. Azzi, A.; Meydani, S.N.; Meydani, M.; Zingg, J.M. The rise, the fall and the renaissance of vitamin E.
Arch. Biochem. Biophys. 2016, 595, 100�108. [CrossRef] [PubMed]
163. Raederstorff, D.; Wyss, A.; Calder, P.C.; Weber, P.; Eggersdorfer, M. Vitamin E function and requirements in
relation to PUFA. Br. J. Nutr. 2015, 114, 1113�1122. [CrossRef] [PubMed]
164. Loffredo, L.; Perri, L.; Di Castelnuovo, A.; Iacoviello, L.; De Gaetano, G.; Violi, F. Supplementation
with vitamin E alone is associated with reduced myocardial infarction: A meta-analysis. Nutr. Metab.
Cardiovasc. Dis. 2015, 25, 354�363. [CrossRef] [PubMed]
165. Giampieri, F.; Tulipani, S.; Alvarez-Suarez, J.M.; Quiles, J.L.; Mezzetti, B.; Battino, M. The strawberry:
Composition, nutritional quality, and impact on human health. Nutrition 2012, 28, 9�19. [CrossRef] [PubMed]
166. Amiot, M.J.; Riva, C.; Vinet, A. Effects of dietary polyphenols on metabolic syndrome features in humans:
A systematic review. Obes. Rev. 2016, 17, 573�586. [CrossRef] [PubMed]
167. Smeriglio, A.; Barreca, D.; Bellocco, E.; Trombetta, D. Chemistry, Pharmacology and Health Benefits of
Anthocyanins. Phytother. Res. 2016, 30, 1265�1286. [CrossRef] [PubMed]
168. Lila, M.A. Anthocyanins and Human Health: An In Vitro Investigative Approach. J. Biomed. Biotechnol. 2004,
2004, 306�313. [CrossRef] [PubMed]
169. Stull, A.J.; Cash, K.C.; Johnson, W.D.; Champagne, C.M.; Cefalu, W.T. Bioactives in blueberries improve
insulin sensitivity in obese, insulin-resistant men and women. J. Nutr. 2010, 140, 1764�1768. [CrossRef]
[PubMed]
170. Zhu, Y.; Xia, M.; Yang, Y.; Liu, F.; Li, Z.; Hao, Y.; Mi, M.; Jin, T.; Ling, W. Purified anthocyanin supplementation
improves endothelial function via NO-cGMP activation in hypercholesterolemic individuals. Clin. Chem.
2011, 57, 1524�1533. [CrossRef] [PubMed]
171. Qin, Y.; Xia, M.; Ma, J.; Hao, Y.; Liu, J.; Mou, H.; Cao, L.; Ling, W. Anthocyanin supplementation improves
serum LDL- and HDL-cholesterol concentrations associated with the inhibition of cholesteryl ester transfer
protein in dyslipidemic subjects. Am. J. Clin. Nutr. 2009, 90, 485�492. [CrossRef] [PubMed]
172. Zhu, Y.; Ling, W.; Guo, H.; Song, F.; Ye, Q.; Zou, T.; Li, D.; Zhang, Y.; Li, G.; Xiao, Y.; et al. Anti-inflammatory
effect of purified dietary anthocyanin in adults with hypercholesterolemia: A randomized controlled trial.
Nutr. Metab. Cardiovasc. Dis. 2013, 23, 843�849. [CrossRef] [PubMed]
173. Zhu, Y.; Huang, X.; Zhang, Y.; Wang, Y.; Liu, Y.; Sun, R.; Xia, M. Anthocyanin supplementation
improves HDL-associated paraoxonase 1 activity and enhances cholesterol efflux capacity in subjects
with hypercholesterolemia. J. Clin. Endocrinol. Metab. 2014, 99, 561�569. [CrossRef] [PubMed]
174. Karlsen, A.; Retterstol, L.; Laake, P.; Paur, I.; Bohn, S.K.; Sandvik, L.; Blomhoff, R. Anthocyanins inhibit
nuclear factor-kappaB activation in monocytes and reduce plasma concentrations of pro-inflammatory
mediators in healthy adults. J. Nutr. 2007, 137, 1951�1954. [PubMed]
175. Keske, M.A.; Ng, H.L.; Premilovac, D.; Rattigan, S.; Kim, J.A.; Munir, K.; Yang, P.; Quon, M.J. Vascular and
metabolic actions of the green tea polyphenol epigallocatechin gallate. Curr. Med. Chem. 2015, 22, 59�69.
[CrossRef] [PubMed]
176. Johnson, R.; Bryant, S.; Huntley, A.L. Green tea and green tea catechin extracts: An overview of the clinical
evidence. Maturitas 2012, 73, 280�287. [CrossRef] [PubMed]
177. Huang, J.; Wang, Y.; Xie, Z.; Zhou, Y.; Zhang, Y.; Wan, X. The anti-obesity effects of green tea in human
intervention and basic molecular studies. Eur. J. Clin. Nutr. 2014, 68, 1075�1087. [CrossRef] [PubMed]
178. Hursel, R.; Westerterp-Plantenga, M.S. Catechin- and caffeine-rich teas for control of body weight in humans.
Am. J. Clin. Nutr. 2013, 98, 1682S�1693S. [CrossRef] [PubMed]
179. Gutierrez-Salmean, G.; Ortiz-Vilchis, P.; Vacaseydel, C.M.; Rubio-Gayosso, I.; Meaney, E.; Villarreal, F.;
Ramirez-Sanchez, I.; Ceballos, G. Acute effects of an oral supplement of (?)-epicatechin on postprandial fat
and carbohydrate metabolism in normal and overweight subjects. Food Funct. 2014, 5, 521�527. [CrossRef]
[PubMed]
180. Khalesi, S.; Sun, J.; Buys, N.; Jamshidi, A.; Nikbakht-Nasrabadi, E.; Khosravi-Boroujeni, H. Green tea
catechins and blood pressure: A systematic review and meta-analysis of randomised controlled trials.
Eur. J. Nutr. 2014, 53, 1299�1311. [CrossRef] [PubMed]
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine










 We usually talk of energy in general terms, as in �I don�t have a lot of energy today� or �You can feel the energy in the room.� But what really is energy? Where do we get the energy to move? How do we use it? How do we get more of it? Ultimately, what controls our movements? The three metabolic energy pathways are the�phosphagen system, glycolysis�and the�aerobic system.�How do they work, and what is their effect?
We usually talk of energy in general terms, as in �I don�t have a lot of energy today� or �You can feel the energy in the room.� But what really is energy? Where do we get the energy to move? How do we use it? How do we get more of it? Ultimately, what controls our movements? The three metabolic energy pathways are the�phosphagen system, glycolysis�and the�aerobic system.�How do they work, and what is their effect?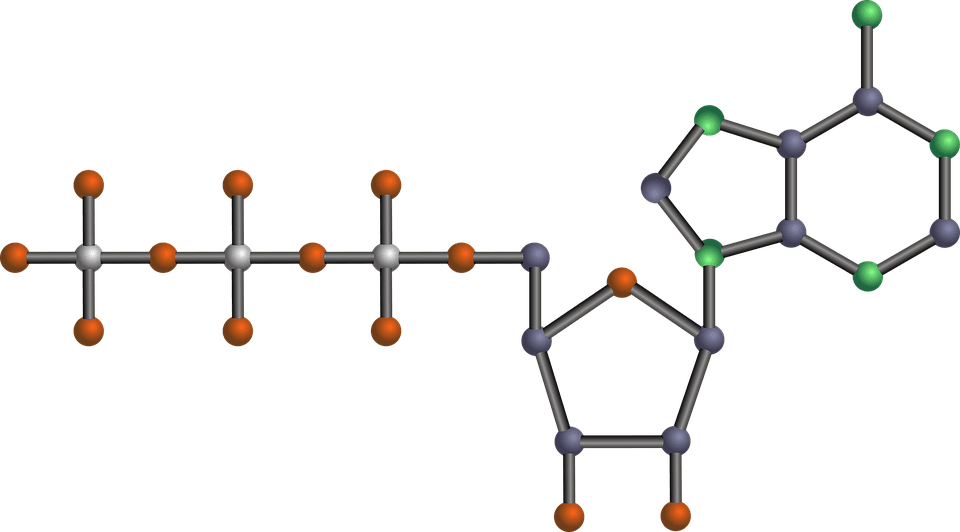 The energy for all physical activity comes from the conversion of high-energy phosphates (adenosine�triphosphate�ATP) to lower-energy phosphates (adenosine�diphosphate�ADP; adenosine�monophosphate�AMP; and inorganic phosphate, Pi). During this breakdown (hydrolysis) of ATP, which is a water-requiring process, a proton, energy and heat are produced: ATP + H2O ���ADP + Pi�+ H+�+ energy + heat. Since our muscles don�t store much ATP, we must constantly resynthesize it. The hydrolysis and resynthesis of ATP is thus a circular process�ATP is hydrolyzed into ADP and Pi, and then ADP and Pi�combine to resynthesize ATP. Alternatively, two ADP molecules can combine to produce ATP and AMP: ADP + ADP ���ATP + AMP.
The energy for all physical activity comes from the conversion of high-energy phosphates (adenosine�triphosphate�ATP) to lower-energy phosphates (adenosine�diphosphate�ADP; adenosine�monophosphate�AMP; and inorganic phosphate, Pi). During this breakdown (hydrolysis) of ATP, which is a water-requiring process, a proton, energy and heat are produced: ATP + H2O ���ADP + Pi�+ H+�+ energy + heat. Since our muscles don�t store much ATP, we must constantly resynthesize it. The hydrolysis and resynthesis of ATP is thus a circular process�ATP is hydrolyzed into ADP and Pi, and then ADP and Pi�combine to resynthesize ATP. Alternatively, two ADP molecules can combine to produce ATP and AMP: ADP + ADP ���ATP + AMP. During short-term, intense activities, a large amount of power needs to be produced by the muscles, creating a high demand for ATP. The phosphagen system (also called the ATP-CP system) is the quickest way to resynthesize ATP (Robergs & Roberts 1997). Creatine phosphate (CP), which is stored in skeletal muscles, donates a phosphate to ADP to produce ATP: ADP + CP ���ATP + C. No carbohydrate or fat is used in this process; the regeneration of ATP comes solely from stored CP. Since this process does not need oxygen to resynthesize ATP, it is anaerobic, or oxygen-independent. As the fastest way to resynthesize ATP, the phosphagen system is the predominant energy system used for all-out exercise lasting up to about 10 seconds. However, since there is a limited amount of stored CP and ATP in skeletal muscles, fatigue occurs rapidly.
During short-term, intense activities, a large amount of power needs to be produced by the muscles, creating a high demand for ATP. The phosphagen system (also called the ATP-CP system) is the quickest way to resynthesize ATP (Robergs & Roberts 1997). Creatine phosphate (CP), which is stored in skeletal muscles, donates a phosphate to ADP to produce ATP: ADP + CP ���ATP + C. No carbohydrate or fat is used in this process; the regeneration of ATP comes solely from stored CP. Since this process does not need oxygen to resynthesize ATP, it is anaerobic, or oxygen-independent. As the fastest way to resynthesize ATP, the phosphagen system is the predominant energy system used for all-out exercise lasting up to about 10 seconds. However, since there is a limited amount of stored CP and ATP in skeletal muscles, fatigue occurs rapidly.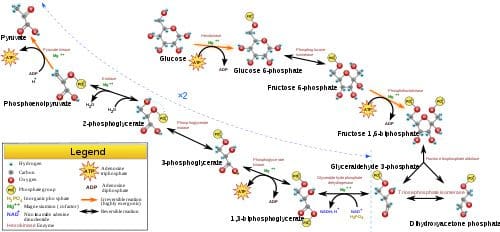 Glycolysis is the predominant energy system used for all-out
Glycolysis is the predominant energy system used for all-out  Since humans evolved for aerobic activities (Hochachka, Gunga & Kirsch 1998; Hochachka & Monge 2000), it�s not surprising that the aerobic system, which is dependent on oxygen, is the most complex of the three energy systems. The metabolic reactions that take place in the presence of oxygen are responsible for most of the cellular energy produced by the body. However, aerobic metabolism is the slowest way to resynthesize ATP. Oxygen, as the patriarch of metabolism, knows that it is worth the wait, as it controls the fate of endurance and is the sustenance of life. �I�m oxygen,� it says to the muscle, with more than a hint of superiority. �I can give you a lot of ATP, but you will have to wait for it.�
Since humans evolved for aerobic activities (Hochachka, Gunga & Kirsch 1998; Hochachka & Monge 2000), it�s not surprising that the aerobic system, which is dependent on oxygen, is the most complex of the three energy systems. The metabolic reactions that take place in the presence of oxygen are responsible for most of the cellular energy produced by the body. However, aerobic metabolism is the slowest way to resynthesize ATP. Oxygen, as the patriarch of metabolism, knows that it is worth the wait, as it controls the fate of endurance and is the sustenance of life. �I�m oxygen,� it says to the muscle, with more than a hint of superiority. �I can give you a lot of ATP, but you will have to wait for it.�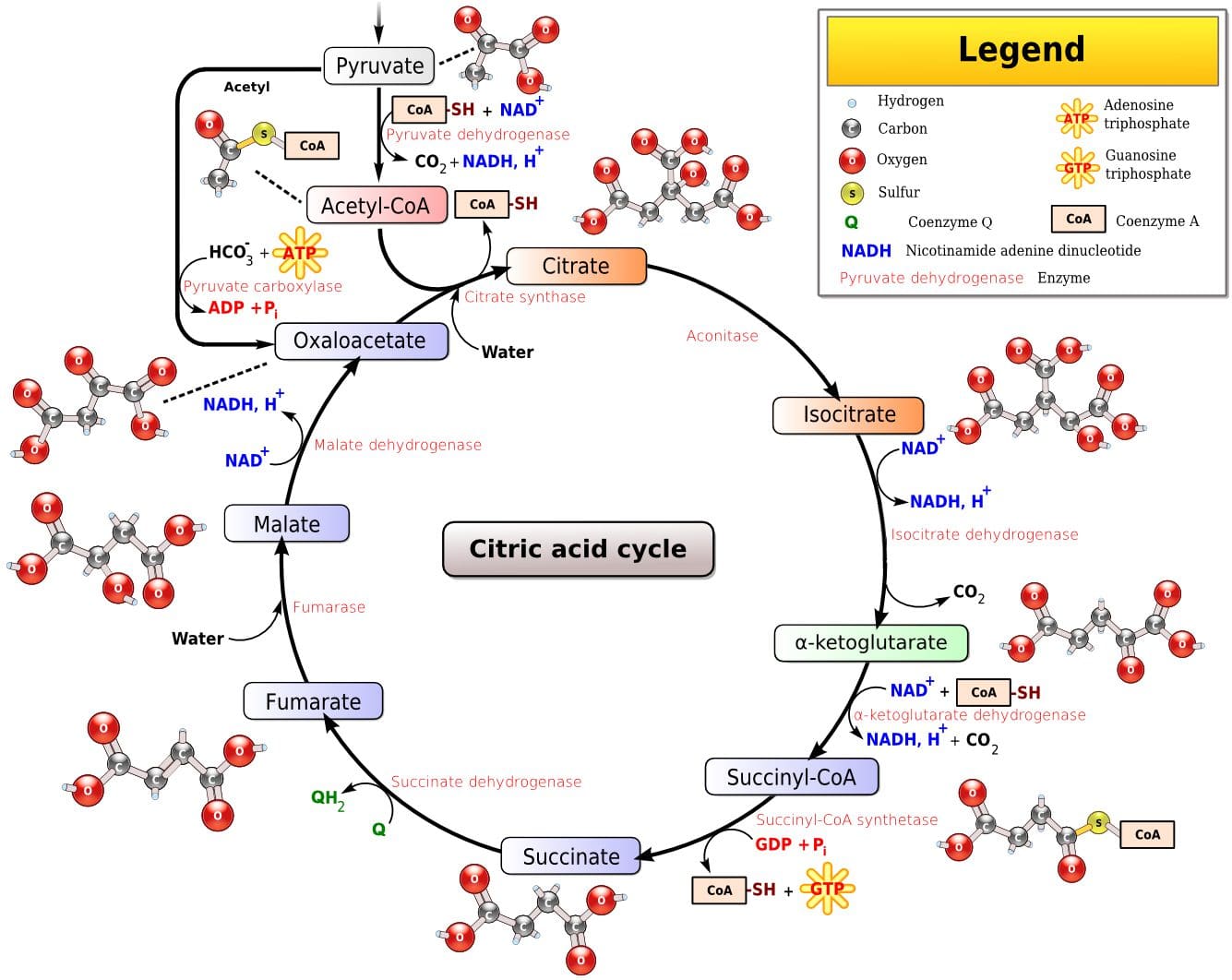 Fat, which is stored as triglyceride in adipose tissue underneath the skin and within skeletal muscles (called�intramuscular triglyceride), is the other major fuel for the aerobic system, and is the largest store of energy in the body. When using fat, triglycerides are first broken down into free fatty acids and glycerol (a process called�lipolysis). The free fatty acids, which are composed of a long chain of carbon atoms, are transported to the muscle mitochondria, where the carbon atoms are used to produce acetyl-CoA (a process called�beta-oxidation).
Fat, which is stored as triglyceride in adipose tissue underneath the skin and within skeletal muscles (called�intramuscular triglyceride), is the other major fuel for the aerobic system, and is the largest store of energy in the body. When using fat, triglycerides are first broken down into free fatty acids and glycerol (a process called�lipolysis). The free fatty acids, which are composed of a long chain of carbon atoms, are transported to the muscle mitochondria, where the carbon atoms are used to produce acetyl-CoA (a process called�beta-oxidation).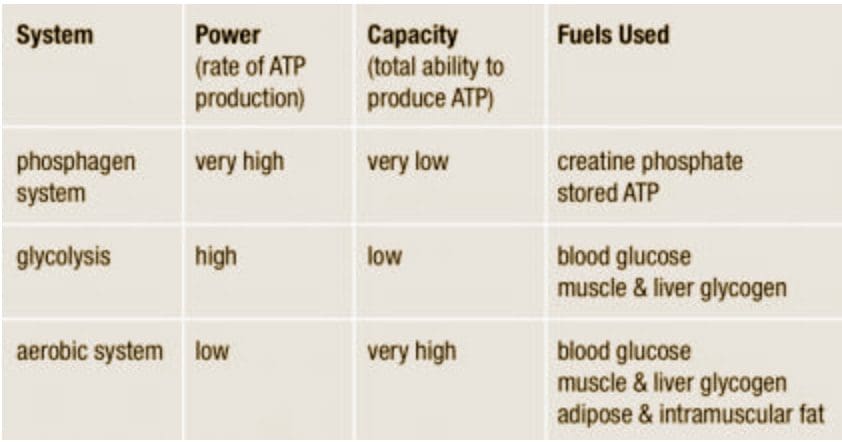
 It was during the period between 1910 and 1920 when it was suggested for the first time that a cluster of associated metabolic disturbances tended to coexist together [1]. Since then, different health organisms have suggested diverse definitions for metabolic syndrome (MetS) but there has not yet been a well-established consensus. The most common definitions are summarized in Table 1. What is clear for all of these is that the MetS is a clinical entity of substantial heterogeneity, commonly represented by the combination of obesity (especially abdominal obesity), hyperglycemia, dyslipidemia and/or hypertension [2�6].
It was during the period between 1910 and 1920 when it was suggested for the first time that a cluster of associated metabolic disturbances tended to coexist together [1]. Since then, different health organisms have suggested diverse definitions for metabolic syndrome (MetS) but there has not yet been a well-established consensus. The most common definitions are summarized in Table 1. What is clear for all of these is that the MetS is a clinical entity of substantial heterogeneity, commonly represented by the combination of obesity (especially abdominal obesity), hyperglycemia, dyslipidemia and/or hypertension [2�6].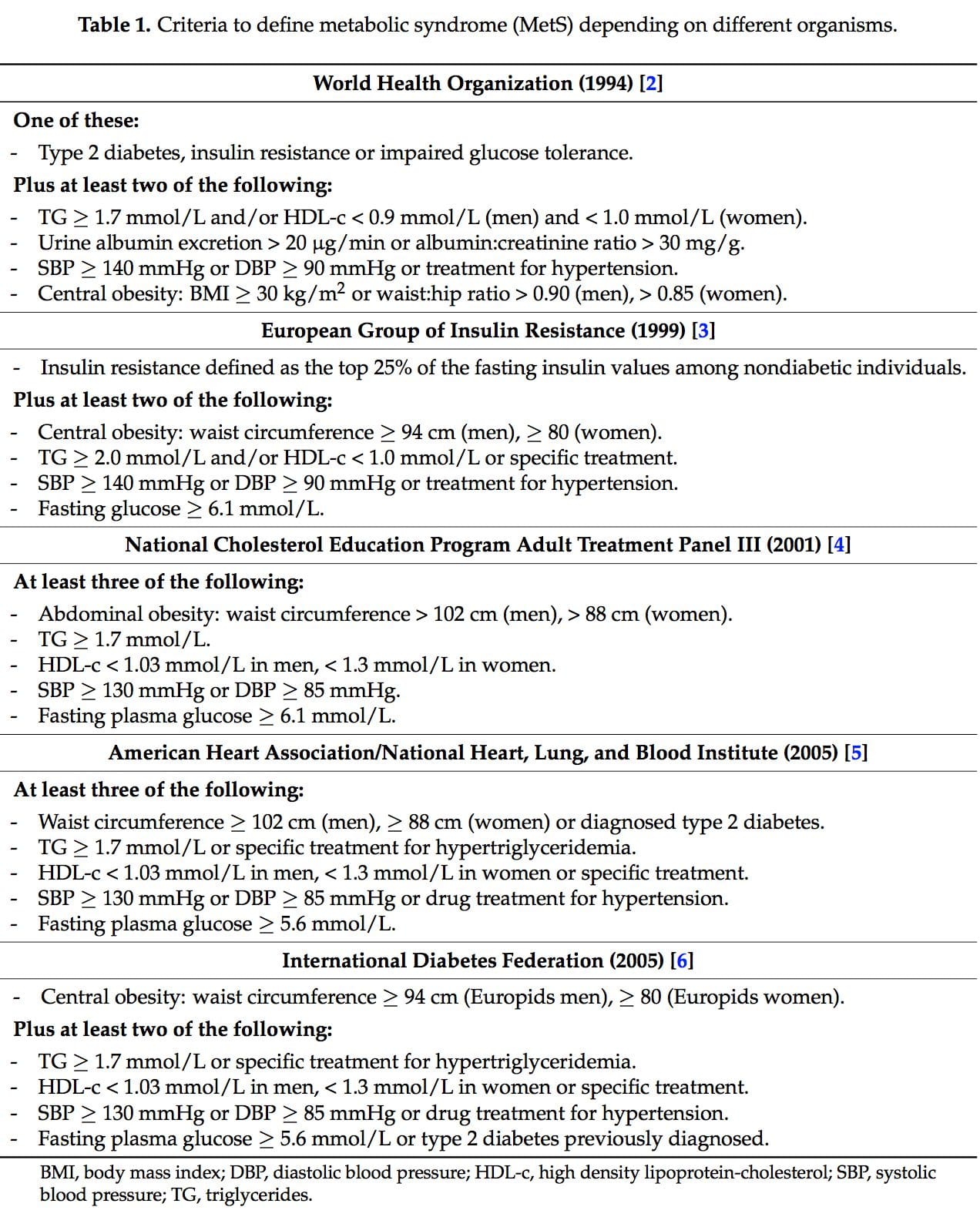
 Several dietary strategies and their potential positive effects on the prevention and treatment of the different metabolic complications associated to the MetS, are described below and summarized in Table 2.
Several dietary strategies and their potential positive effects on the prevention and treatment of the different metabolic complications associated to the MetS, are described below and summarized in Table 2.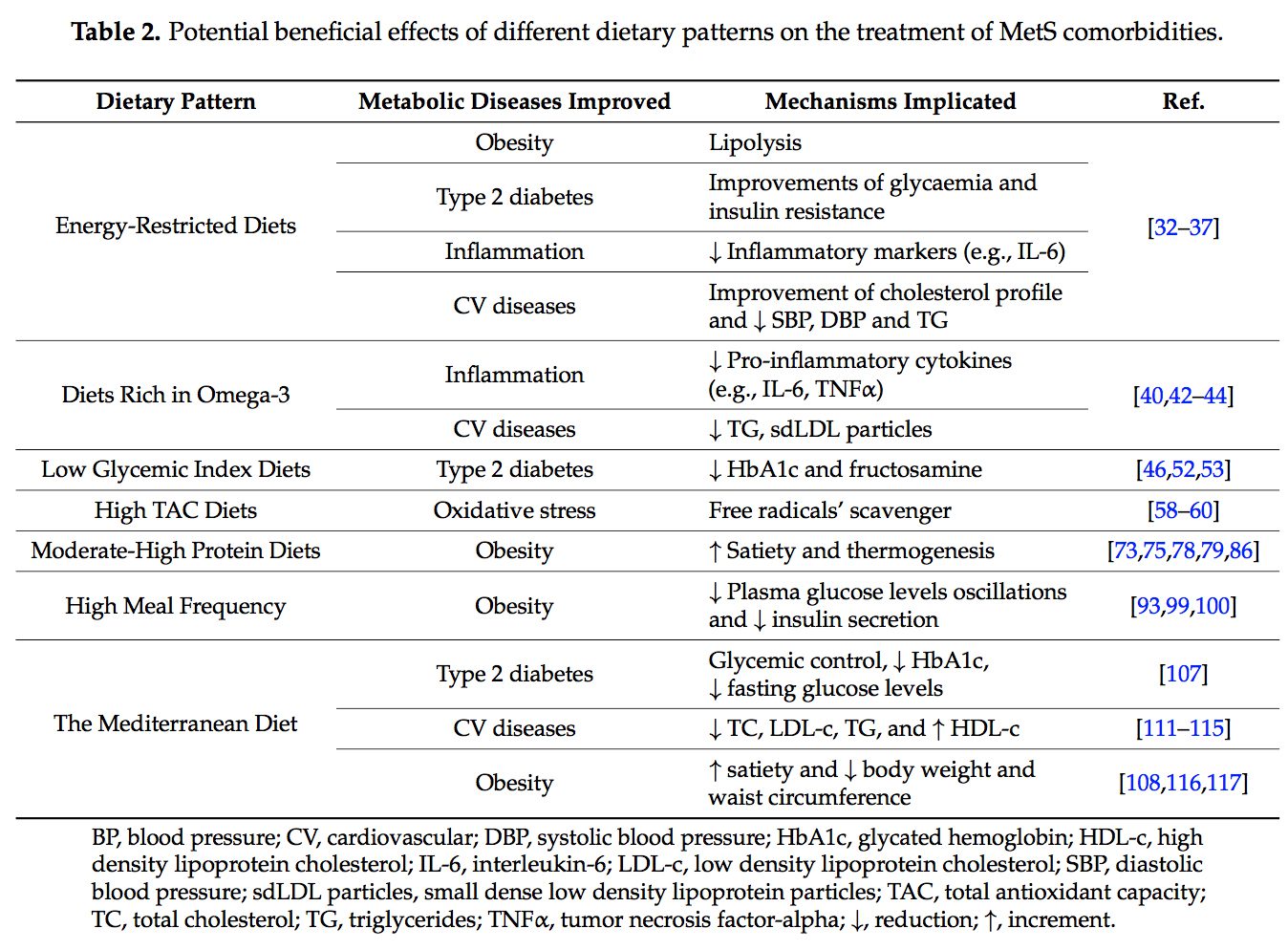 2.1. Energy-Restricted Diet Strategies
2.1. Energy-Restricted Diet Strategies
 The very long-chain eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) are essential omega-3 polyunsaturated fatty acids (n-3 PUFAs) for human physiology. Their main dietary sources are fish and algal oils and fatty fish, but they can also be synthesized by humans from ?-linolenic acid [40].
The very long-chain eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) are essential omega-3 polyunsaturated fatty acids (n-3 PUFAs) for human physiology. Their main dietary sources are fish and algal oils and fatty fish, but they can also be synthesized by humans from ?-linolenic acid [40]. Over the last ten years, the concern about the quality of the carbohydrates (CHO) consumed has risen [46]. In this context, the glycemic index (GI) is used as a CHO quality measure. It consists in a ranking on a scale from 0 to 100 that classifies carbohydrate-containing foods according to the postprandial glucose response [47]. The higher the index, the more promptly the postprandial serum glucose rises and the more rapid the insulin response. A quick insulin response leads to rapid hypoglycemia, which is suggested to be associated with an increment of the feeling of hunger and to a subsequent higher caloric intake [47]. The glycemic load (GL) is equal to the GI multiplied by the number of grams of CHO in a serving [48].
Over the last ten years, the concern about the quality of the carbohydrates (CHO) consumed has risen [46]. In this context, the glycemic index (GI) is used as a CHO quality measure. It consists in a ranking on a scale from 0 to 100 that classifies carbohydrate-containing foods according to the postprandial glucose response [47]. The higher the index, the more promptly the postprandial serum glucose rises and the more rapid the insulin response. A quick insulin response leads to rapid hypoglycemia, which is suggested to be associated with an increment of the feeling of hunger and to a subsequent higher caloric intake [47]. The glycemic load (GL) is equal to the GI multiplied by the number of grams of CHO in a serving [48]. Dietary total antioxidant capacity (TAC) is an indicator of diet quality defined as the sum of antioxidant activities of the pool of antioxidants present in a food [55]. These antioxidants have the capacity to act as scavengers of free radicals and other reactive species produced in the organisms [56]. Taking into account that oxidative stress is one of the remarkable unfortunate physiological states of MetS, dietary antioxidants are of main interest in the prevention and treatment of this multifactorial disorder [57]. Accordingly, it is well-accepted that diets with a high content of spices, herbs, fruits, vegetables, nuts and chocolate, are associated with a decreased risk of oxidative stress-related diseases development [58�60]. Moreover, several studies have analyzed the effects of dietary TAC in individuals suffering from MetS or related diseases [61,62]. In the Tehran Lipid and Glucose Study it was demonstrated that a high TAC has beneficial effects on metabolic disorders and especially prevents weight and abdominal fat gain [61]. In the same line, research conducted in our institutions also evidenced that beneficial effects on body weight, oxidative stress biomarkers and other MetS features were positively related with higher TAC consumption in patients suffering from MetS [63�65].
Dietary total antioxidant capacity (TAC) is an indicator of diet quality defined as the sum of antioxidant activities of the pool of antioxidants present in a food [55]. These antioxidants have the capacity to act as scavengers of free radicals and other reactive species produced in the organisms [56]. Taking into account that oxidative stress is one of the remarkable unfortunate physiological states of MetS, dietary antioxidants are of main interest in the prevention and treatment of this multifactorial disorder [57]. Accordingly, it is well-accepted that diets with a high content of spices, herbs, fruits, vegetables, nuts and chocolate, are associated with a decreased risk of oxidative stress-related diseases development [58�60]. Moreover, several studies have analyzed the effects of dietary TAC in individuals suffering from MetS or related diseases [61,62]. In the Tehran Lipid and Glucose Study it was demonstrated that a high TAC has beneficial effects on metabolic disorders and especially prevents weight and abdominal fat gain [61]. In the same line, research conducted in our institutions also evidenced that beneficial effects on body weight, oxidative stress biomarkers and other MetS features were positively related with higher TAC consumption in patients suffering from MetS [63�65]. The macronutrient distribution set in a weight loss dietary plan has commonly been 50%�55% total caloric value from CHO, 15% from proteins and 30% from lipids [57,68]. However, as most people have difficulty in maintaining weight loss achievements over time [69,70], research on increment of protein intake (>20%) at the expense of CHO was carried out [71�77].
The macronutrient distribution set in a weight loss dietary plan has commonly been 50%�55% total caloric value from CHO, 15% from proteins and 30% from lipids [57,68]. However, as most people have difficulty in maintaining weight loss achievements over time [69,70], research on increment of protein intake (>20%) at the expense of CHO was carried out [71�77].
 The concept of the
The concept of the 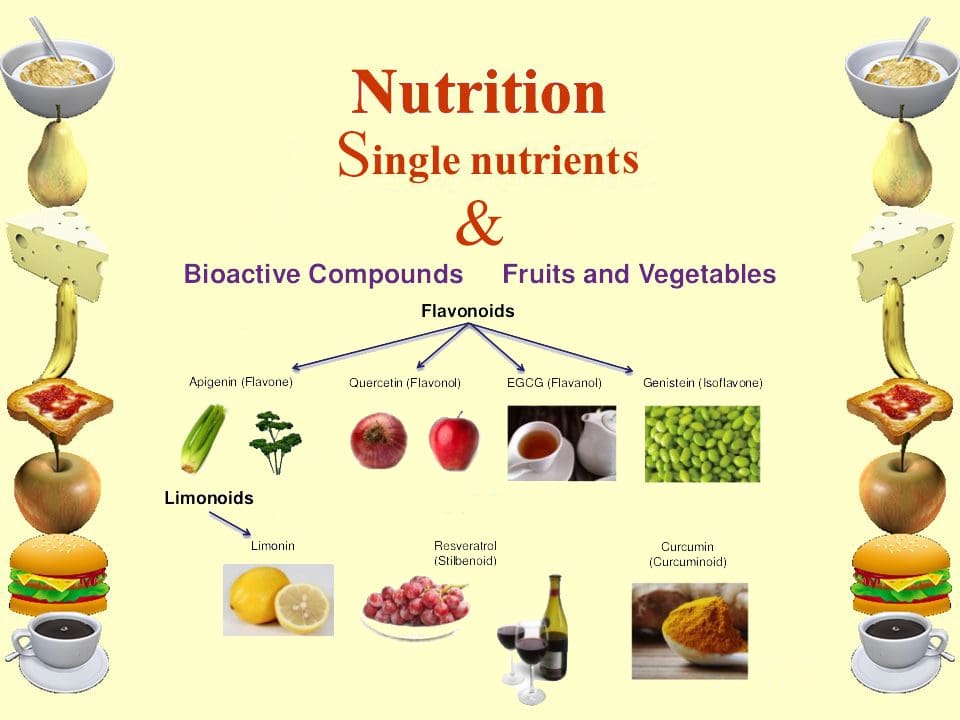 New studies focused on the molecular action of nutritional bioactive compounds with positive effects on MetS are currently an objective of scientific research worldwide with the aim of designing more personalized strategies in the framework of molecular nutrition. Among them, flavonoids and antioxidant vitamins are some of the most studied compounds with different potential benefits such as antioxidant, vasodilatory, anti-atherogenic, antithrombotic, and anti-inflammatory effects [119]. Table 3 summarizes different nutritional bioactive compounds with potential positive effects on MetS, including the possible molecular mechanism of action involved.
New studies focused on the molecular action of nutritional bioactive compounds with positive effects on MetS are currently an objective of scientific research worldwide with the aim of designing more personalized strategies in the framework of molecular nutrition. Among them, flavonoids and antioxidant vitamins are some of the most studied compounds with different potential benefits such as antioxidant, vasodilatory, anti-atherogenic, antithrombotic, and anti-inflammatory effects [119]. Table 3 summarizes different nutritional bioactive compounds with potential positive effects on MetS, including the possible molecular mechanism of action involved.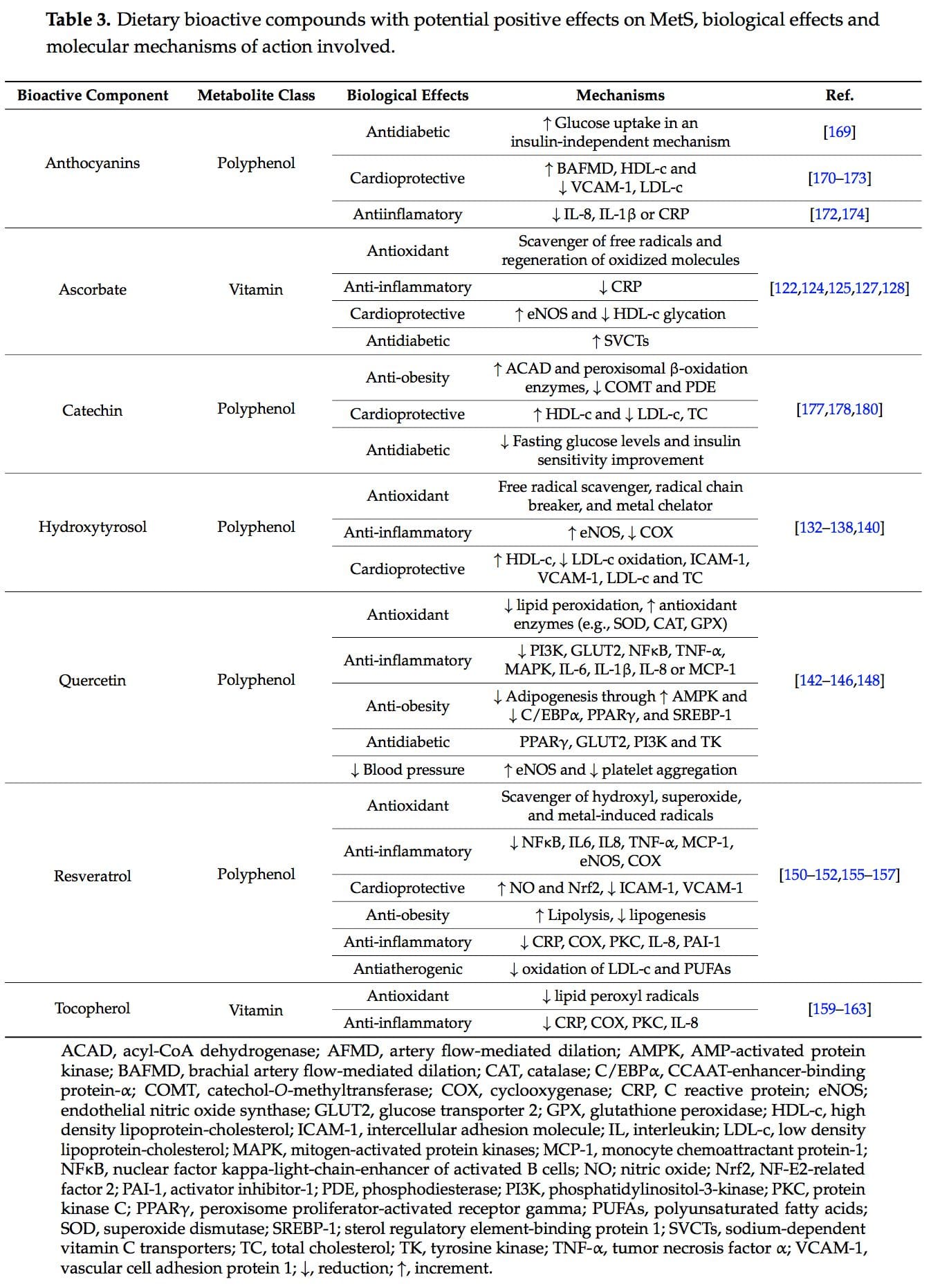
 Vitamin C, ascorbic acid or ascorbate is an essential nutrient as human beings cannot synthesize it. It is a water-soluble antioxidant mainly found in fruits, especially citrus (lemon, orange), and vegetables (pepper, kale) [120]. Several beneficial effects have been associated to this vitamin such as antioxidant and anti-inflammatory properties and prevention or treatment of CVD and type 2 diabetes [121�123].
Vitamin C, ascorbic acid or ascorbate is an essential nutrient as human beings cannot synthesize it. It is a water-soluble antioxidant mainly found in fruits, especially citrus (lemon, orange), and vegetables (pepper, kale) [120]. Several beneficial effects have been associated to this vitamin such as antioxidant and anti-inflammatory properties and prevention or treatment of CVD and type 2 diabetes [121�123]. Hydroxytyrosol (3,4-dihydroxyphenylethanol) is a phenolic compound mainly found in olives [132].
Hydroxytyrosol (3,4-dihydroxyphenylethanol) is a phenolic compound mainly found in olives [132]. Quercetin is a predominant flavanol naturally present in vegetables, fruits, green tea or red wine. It is commonly found as glycoside forms, where rutin is the most common and important structure found in nature [141].
Quercetin is a predominant flavanol naturally present in vegetables, fruits, green tea or red wine. It is commonly found as glycoside forms, where rutin is the most common and important structure found in nature [141].
 Tocopherols, also known as vitamin E, are a family of eight fat-soluble phenolic compounds whose main dietary sources are vegetable oils, nuts and seeds [130,158].
Tocopherols, also known as vitamin E, are a family of eight fat-soluble phenolic compounds whose main dietary sources are vegetable oils, nuts and seeds [130,158].
 Catechins are polyphenols that can be found in a variety of foods including fruits, vegetables, chocolate, wine, and tea [175]. The epigallocatechin 3-gallate present in tea leaves is the catechin class most studied [176].
Catechins are polyphenols that can be found in a variety of foods including fruits, vegetables, chocolate, wine, and tea [175]. The epigallocatechin 3-gallate present in tea leaves is the catechin class most studied [176].