The Role of Telemedicine in Integrative Injury Care at El Paso Back Clinic: Providing Full Support for Car Accident, Work, and Sports Injuries in El Paso, TX
A doctor of chiropractic and a nurse practitioner review the MRI of a patient following a motorcycle collision.
In El Paso, TX, getting injured in a car crash, at work, or during sports can be tough. But at El Paso Back Clinic®, a top wellness chiropractic care spot, new tools like telemedicine make getting help simpler. Telemedicine uses video calls and online apps to let health experts care for you from home. This article explores how the clinic’s integrative nurse practitioner (NP) and chiropractor team up with telemedicine to provide comprehensive injury care. This covers virtual check-ups, treatment planning, and long-term help. It’s super useful for folks who can’t easily move or get to the clinic. The team also shares tips on eating, working out, and daily habits to speed up healing. They keep everything organized and documented for the best outcomes.
El Paso Back Clinic® focuses on functional medicine and holistic healing. Led by Dr. Alexander Jimenez, who is both a chiropractor (DC) and a family nurse practitioner (FNP-BC), the clinic combines conventional medicine with natural approaches to treat injuries. Telemedicine here means you can get exams, diagnoses, and follow-ups without leaving home. This is great for busy El Paso residents or for those who are hurting too much to travel. The clinic’s approach considers your whole body, with the NP and chiropractor working together to create plans that fit your life.
What Is Integrative Care at El Paso Back Clinic?
At El Paso Back Clinic®, integrative care means a team of doctors, therapists, and nutritionists working together to fully heal you. For car accident injuries like whiplash or back strains, the chiropractor adjusts your spine while the NP manages pain and checks for deeper issues. They make custom plans using evidence-based methods.
Common Injuries Treated: Neck pain from crashes, work lifts causing strains, or sports-related twists leading to sprains.
Why Choose Integrative?: It targets the cause, not just pain, blending adjustments with lifestyle changes.
Telemedicine’s Role: Allows remote care, so you start healing right away from home.
This method helps with lasting health. For sports fans in El Paso, tips on better nutrition can speed up recovery (Dallas Accident and Injury Rehab, n.d.).
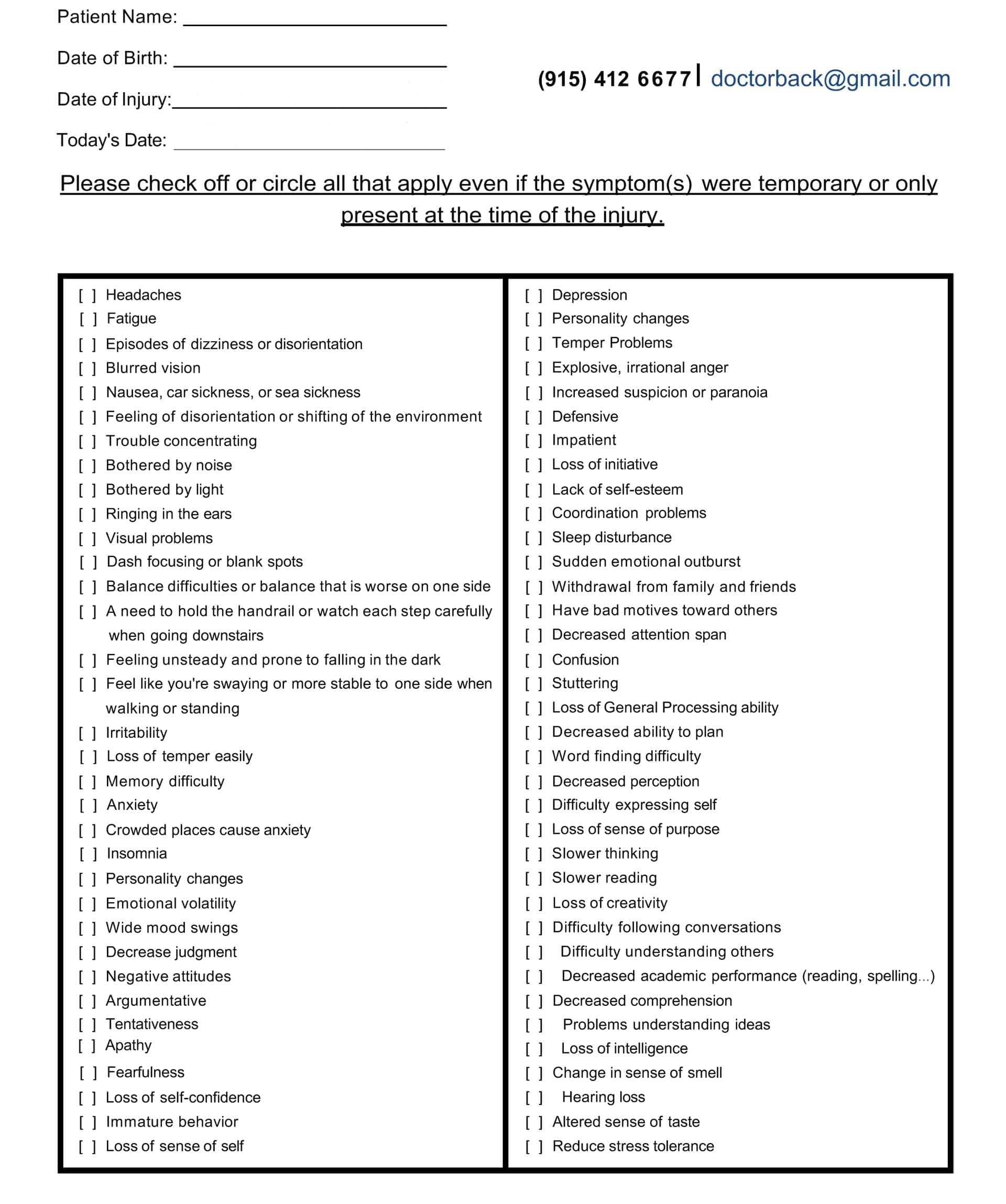
Head Injury/Traumatic Brain Injury Symptom Questionnaire
Virtual Examinations: How El Paso Back Clinic Does It Remotely
Telemedicine at El Paso Back Clinic® starts with virtual exams. You connect via secure video from your phone or computer. Dr. Jimenez or the team talks to you about your injury.
For a car accident, they ask about the crash and pain spots. They watch you move, like bending or walking, to check for swelling or stiffness. Even without hands-on involvement, they spot many problems, such as muscle pulls or nerve issues (Personal Injury Firm, 2025).
Work injuries, like slips, get quick virtual checks to stop things from getting worse. The chiropractor guides home tests, such as balance checks.
Tools in Virtual Exams: Video for movement, apps for sharing photos of injuries, or devices for vital signs.
When It’s Not Enough: Some need in-person touches, so they schedule clinic visits at their El Paso locations.
This remote setup makes getting checked easy, especially in El Paso, where traffic can be a hassle (CK Firm, 2024).
Diagnoses Through Telemedicine at the Clinic
After the exam, the team at El Paso Back Clinic® diagnoses remotely. Common ones from car accidents include whiplash or disc problems. The NP might order X-rays or MRIs, which are performed locally and shared online.
Chiropractors like Dr. Jimenez spot spinal shifts that can cause leg pain, such as sciatica. They explain it clearly on video. The NP assesses whole-body health, including whether swelling worsens.
All sessions are recorded for official documents, insurance keys, or personal injury claims (ChiroMed, n.d.).
Diagnosis Examples: Work-related back pain, sports-related nerve hits, and crash-neck strains.
Team Collaboration: NP handles meds; chiropractor does adjustments.
Tips for Accuracy: Describe pain and show motions well.
This reduces wait times, allowing you to start your El Paso recovery sooner (Complete Care, n.d.).
Managing Treatment Plans Remotely from El Paso Back Clinic
The NP and chiropractor create a treatment plan together, updated via telemedicine. For a sports knee sprain, it might include rest, ice, and shown exercises.
Dr. Jimenez demonstrates stretches on camera. The NP monitors pain and adjusts treatments.
They coordinate to avoid overlaps. For work injuries, plans cover safe job returns. Everything’s online for easy tracking.
Plan Essentials: Pain relief, movement work, and prevention advice.
Integrative Touches: Diet tweaks to cut swelling, like more omega-3 foods.
Telemedicine Updates: Regular video calls to tweak based on progress.
This saves time and money for El Paso patients (Jimenez, n.d.-a).
Ongoing Support and Follow-Up Care at the Clinic
Recovery needs steady help, and El Paso Back Clinic® uses telemedicine for easy follow-ups. Log in to chat about how you’re doing.
For car crash back pain, they check therapy effects and offer encouragement. Support includes mental health tips, as injuries can stress you.
Chiropractors guide home exercises on video. NPs watch for treatment side effects.
Support Types: Mood talks, progress logs, specialist referrals.
How Often: Weekly, early on, then less.
For El Paso Athletes: Safe return-to-play tips, like warm-ups.
This prevents pain from lasting, helping you get back to life fast (Prescient National, n.d.).
Benefits for El Paso Residents with Mobility or Access Issues
Injuries make moving hard, especially in spread-out El Paso. Telemedicine brings care to you.
No travel needed, perfect for remote areas or difficult days. For work injuries, it means less downtime. See pros from home.
Who Gains Most: Those pained by walking, without transport, or packed schedules.
Access Help: Shorter waits than office visits.
Legal Benefits: Docs care for claims without hold-ups.
This makes healing equal for all in El Paso (CK Firm, 2024).
Integrative Advice on Diet, Exercise, and Lifestyle from the Clinic
El Paso Back Clinic® shines with holistic telemedicine tips. They suggest anti-inflammatory foods, such as fruits, to aid healing.
Exercise advice includes easy yoga for pain, demonstrated online. Lifestyle shifts cover better sleep or stress cuts, like apps for calm.
For sports, they teach form to prevent re-injury.
Diet Ideas: Omega-3 for nerves, antioxidants for fixes.
Workout Suggestions: Stretches for range, walks for build-up.
Life Changes: Posture tweaks, drop bad habits.
This addresses root causes for better long-term health (Dallas Accident and Injury Rehab, n.d.).
Coordination and Documentation Between NP and Chiropractor at El Paso Back Clinic
The team shares notes easily on telemedicine platforms. Dr. Jimenez, as both NP and chiropractor, bridges the roles seamlessly.
Records from calls build your file, showing progress for insurance or courts.
Therapies align, like adjustments with rest plans.
Coordination Methods: Shared digital files, joint calls.
Record Value: Shows timely, excellent care.
Your Part: Update honestly for the top plans.
This leads to smooth recoveries in El Paso (Jimenez, n.d.-b).
Insights from Dr. Alexander Jimenez at El Paso Back Clinic
Dr. Alexander Jimenez, DC, APRN, FNP-BC, shares hands-on views from over 30 years at El Paso Back Clinic®. He uses telemedicine for same-day injury exams, like after crashes or sports.
He stresses integrative care for body and mind. For head injuries, he advises sleep, diet, and exercise. His dual license allows him to prescribe medications and adjust spines remotely when possible.
Jimenez highlights tests, such as MRIs, shared online. He combines adjustments in nutrition with other interventions for issues like gut health post-trauma.
Main Observations: Injuries are linked to overall health, like nerves and digestion.
Telemedicine in Practice: Quick virtual help for accidents, with shipped braces.
Tips: Use posture drills and supplements for healing.
His approach shows how the clinic’s NP-chiropractor team excels (Jimenez, n.d.-a; Jimenez, n.d.-b; Jimenez, n.d.-c).
Challenges and Future of Telemedicine at El Paso Back Clinic
Telemedicine has limits, such as the need for touch for some exams. Tech glitches can happen.
But the future is promising. Better apps and AI will improve diagnoses. More insurance covers it.
The clinic trains in remote teamwork.
Fixing Issues: Have in-person backups, help with tech.
Coming Trends: Wearables for live data.
Importance: Makes care more accessible and affordable in El Paso.
Conclusion
At El Paso Back Clinic® in El Paso, TX, telemedicine transforms injury care for car, work, or sports-related injuries. The integrative NP and chiropractor team, led by Dr. Jimenez, offers virtual exams for ongoing support. It includes holistic advice for better living. Ideal for mobility challenges. As Dr. Jimenez proves, this leads to quicker, fuller healing. If injured, reach out to El Paso Back Clinic® for easy, top-notch care at 915-850-0900 or visit their site.
Discover the impact of stress on traumatic brain injury. Insights into coping strategies can enhance recovery and well-being.
Understanding Traumatic Brain Injury: How Stress Impacts the Body and Brain, and How Chiropractic Care Can Help
Traumatic brain injury (TBI) represents one of the most complex medical conditions affecting millions of people each year. While many people think of TBI as simply a physical injury to the head, it actually triggers a complicated chain of events throughout the entire body. Understanding how TBI affects both the brain and body, especially in relation to stress, can help individuals seek appropriate treatment and improve their recovery outcomes. This article explores the relationship between TBI and stress, examines how these conditions affect cognitive function and the body’s autonomic nervous system, and discusses how chiropractic care combined with other integrative treatments can support healing and prevent long-term problems. ninds.nih+1
What Is Traumatic Brain Injury?
A traumatic brain injury occurs when an external force causes the brain to function differently than it should. This injury can happen in several ways, including a bump, blow, or jolt to the head, or when an object penetrates the skull and enters the brain tissue. Not all blows or jolts to the head result in a TBI, but when they do, the consequences can range from temporary disruptions in brain function to severe and permanent disability.cdc+1 TBI can be classified into different types based on how the injury occurs. Penetrating TBI, also called open TBI, happens when an object like a bullet or bone fragment pierces the skull and damages brain tissue. Non-penetrating TBI, also known as closed head injury or blunt TBI, occurs when an external force moves the brain within the skull without breaking through the skull itself. This type of injury commonly results from falls, motor vehicle crashes, sports activities, or physical assaults.ncbi.nlm.nih+2
The severity of TBI ranges from mild to severe. Mild TBI, often called a concussion, may cause temporary changes in how the brain works but typically does not show up on standard brain imaging tests. Moderate and severe TBIs involve more significant damage and usually require immediate medical attention. Falls represent the most common cause of TBI, accounting for nearly half of all TBI-related emergency department visits, particularly among children and older adults. Motor vehicle accidents, sports injuries, and assaults also contribute significantly to TBI statistics. biausa+4 Understanding TBI requires recognizing that the injury occurs in two phases. The primary injury happens at the moment of impact, causing immediate damage to brain tissue, blood vessels, and nerve cells. However, a secondary injury phase follows, during which the brain experiences additional damage from processes triggered by the initial trauma. These secondary injury mechanisms include inflammation, oxidative stress, disruption of the blood-brain barrier, and excitotoxicity. This secondary phase can continue for days, weeks, or even months after the initial injury, making prompt and appropriate treatment essential for preventing long-term complications. frontiersin+4
How TBI Affects Brain Function and Causes Cognitive Problems
One of the most challenging aspects of TBI involves the cognitive changes that can occur. Cognitive function refers to how the brain processes information, encompassing abilities such as attention, memory, learning, reasoning, and problem-solving. When someone experiences a TBI, these cognitive abilities often become impaired, creating significant difficulties in daily life. alz+2 Disturbances in attention, memory, and executive functioning represent the most common cognitive consequences of TBI at all severity levels. Executive functions encompass complex thinking skills, including planning, organizing, decision-making, and problem-solving. Many people with TBI find it harder to focus on tasks, take longer to process thoughts, and struggle to remember new information. These cognitive impairments can persist long after the initial injury and significantly impact a person’s ability to return to work, school, or their previous level of functioning. pubmed.ncbi.nlm.nih+3
The cognitive effects of TBI vary depending on which parts of the brain are damaged and the severity of the injury. Research shows that processing speed becomes the most impacted cognitive domain following moderate to severe TBI, with over forty percent of individuals showing impaired speed with or without other cognitive problems. In contrast, individuals with mild TBI exhibit a more even distribution of impairments across various cognitive domains, including processing speed, memory, and executive function. Slow processing speed can persist for years after moderate to severe TBI and has the strongest relationship with functional outcomes. jamanetwork Memory problems after TBI can take different forms. Some individuals struggle to learn and remember new information, a condition called anterograde amnesia. Others may have difficulty recalling events that happened immediately before or after the injury, known as post-traumatic amnesia. These memory difficulties can significantly impact daily functioning, making it hard to remember appointments, follow instructions, or maintain social relationships. headway+4 The mechanisms behind these cognitive impairments involve damage to specific brain structures and disruption of neural networks. TBI can cause diffuse axonal injury, a condition characterized by widespread damage to the brain’s white matter. White matter contains the nerve fibers that allow different brain regions to communicate with each other. When these connections become damaged, the flow of information throughout the brain becomes disrupted, leading to cognitive difficulties. Additionally, TBI can cause focal injuries to specific brain regions that control particular cognitive functions. ninds.nih+1
The Complex Relationship Between TBI and Stress
The relationship between TBI and stress operates in multiple directions, creating a complicated pattern that affects recovery. First, the event causing a TBI often represents a traumatic experience that triggers significant psychological stress. Second, TBI itself creates physiological stress on the body as it attempts to heal from the injury. Third, dealing with the symptoms and consequences of TBI creates ongoing stress that can interfere with recovery. pmc.ncbi.nlm.nih+2 At the physiological level, stress activates the body’s stress response systems, particularly the hypothalamic-pituitary-adrenal (HPA) axis and the locus coeruleus-norepinephrine system. The HPA axis represents a complex set of interactions between three structures: the hypothalamus in the brain, the pituitary gland, and the adrenal glands. When a person experiences stress, the hypothalamus releases corticotropin-releasing hormone (CRH), which signals the pituitary gland to release adrenocorticotropic hormone (ACTH). This hormone then stimulates the adrenal glands to produce cortisol. Cortisol, often referred to as the stress hormone, helps the body respond to stress by increasing blood sugar levels, suppressing the immune system, and providing energy for the fight-or-flight response. pubmed.ncbi.nlm.nih+4
TBI disrupts the normal functioning of the HPA axis, leading to abnormal stress responses. Research shows that approximately one-quarter of all TBI cases result in adrenal insufficiency due to suppressed HPA axis activation. However, many individuals with TBI actually show elevated cortisol levels, particularly in the acute phase after injury. Studies have found that cortisol remains elevated in people with mild TBI for at least one month after injury. This elevation in cortisol can have significant consequences because chronically high cortisol levels can impede physical and psychological recovery through multiple mechanisms, including altered metabolism, increased neuroinflammation, and activation of pathways linked to psychiatric symptoms. pmc.ncbi.nlm.nih+5 The stress response after TBI becomes particularly problematic because individuals with TBI often suffer from poor stress tolerance. They may have impairments in their ability to evaluate stressors appropriately and difficulty initiating and stopping neuroendocrine stress responses. This dysfunction means that even relatively minor stressors can trigger exaggerated stress responses in people recovering from TBI. The combination of altered stress physiology and reduced stress tolerance creates a situation where stress itself becomes a barrier to recovery. powerofpatients+2 Research on animals and humans demonstrates that stress following TBI can worsen outcomes. In animal studies, rats exposed to social stress immediately before mild TBI showed greater anxiety-like behavior and impaired fear extinction compared to animals that experienced either stress or TBI alone. This finding suggests that stress concurrent with TBI produces more severe psychological outcomes than either insult by itself. The combination of stress and TBI also had greater effects on brain chemistry, particularly affecting serotonin systems associated with anxiety and fear learning. frontiersin
How Stress and TBI Interact to Affect Cognitive Function
The interaction between stress and TBI creates a particularly challenging situation for cognitive function. Both stress and TBI independently impair cognitive abilities, but when they occur together, their effects can compound each other. Understanding these interactions helps explain why some people recover well from TBI while others struggle with persistent cognitive difficulties. pmc.ncbi.nlm.nih+2 Stress affects the brain through multiple mechanisms. Chronic or severe stress reduces levels of brain-derived neurotrophic factor (BDNF), a protein essential for brain health and neuroplasticity. BDNF helps the brain form new neural connections and adapt to challenges. When stress decreases BDNF levels, it impairs the brain’s ability to recover from injury. Stress also increases oxidative stress and inflammation in the brain. Oxidative stress occurs when there are too many reactive oxygen species (ROS) relative to the body’s antioxidant defenses. These reactive molecules can damage brain cells and interfere with normal brain function. pmc.ncbi.nlm.nih+3 TBI similarly increases oxidative stress and inflammation in the brain. The initial mechanical injury damages cells and blood vessels, triggering inflammatory responses that are designed to clear away the damaged tissue. However, when inflammation becomes excessive or prolonged, it can cause additional damage to healthy brain tissue. Studies show that systemic low-grade chronic inflammation can persist for up to one year after mild TBI, much longer than previously recognized. This prolonged inflammation contributes to ongoing cognitive difficulties and other symptoms. journals.plos+5
The combination of stress and TBI creates overlapping pathological processes that intensify cognitive impairment. Both conditions disrupt the balance between excitatory and inhibitory neurons in key brain regions, such as the prefrontal cortex, hippocampus, and amygdala. The prefrontal cortex regulates executive functions, including planning, decision-making, and working memory. The hippocampus plays a crucial role in forming new memories and spatial navigation. The amygdala plays a crucial role in processing emotions, particularly fear and anxiety. When these regions become dysfunctional due to the combined effects of stress and TBI, multiple aspects of cognitive and emotional functioning become impaired. mayoclinic+2 Environmental factors also play an important role in how stress and TBI interact to affect cognitive outcomes. Studies show that environmental enrichment—access to stimulating, complex environments with opportunities for physical activity, cognitive challenge, and social interaction—promotes recovery after TBI. Conversely, lack of environmental enrichment may contribute to cognitive decline in the post-acute phase after TBI. This finding suggests that the environment where a person recovers can significantly influence their outcomes. Barriers such as limited access to resources, inadequate social support, transportation difficulties, and challenging home environments can all impede recovery and contribute to worse outcomes.frontiersin+3
Autonomic Dysfunction After TBI
Beyond cognitive problems, TBI frequently causes autonomic dysfunction, which refers to impaired functioning of the autonomic nervous system (ANS). The ANS controls involuntary bodily functions like heart rate, blood pressure, digestion, breathing, and temperature regulation. It consists of two main branches: the sympathetic nervous system, which activates the body’s “fight or flight” response, and the parasympathetic nervous system, which promotes “rest and digest” functions. pmc.ncbi.nlm.nih+4 The central autonomic network—the brain structures that control the ANS—includes the cerebral cortex (particularly the insular and medial prefrontal regions), amygdala, hypothalamus, and brainstem centers. Because TBI can damage any of these structures, it frequently disrupts normal autonomic function. Studies show that autonomic dysfunction occurs commonly after TBI at all severity levels and contributes significantly to the symptoms people experience. neurologyopen.bmj+3
Signs and symptoms of autonomic dysfunction after TBI are broad and can affect multiple body systems. Common symptoms include headaches, dizziness, balance and coordination problems, nausea, vomiting, sensitivity to light and sound, fatigue, and difficulty concentrating. Autonomic dysfunction can also cause cardiovascular symptoms, such as abnormal heart rate and blood pressure changes, orthostatic intolerance (feeling dizzy or faint when standing up), and exercise intolerance. Gastrointestinal symptoms, including bloating, constipation, diarrhea, and nausea, are also common. Other manifestations include abnormal sweating, dry eyes and mouth, changes in skin color, temperature regulation problems, and visual blurring. concussionalliance+2 Research using heart rate variability (HRV) as a measure of autonomic function shows that both sympathetic and parasympathetic dysfunction occur after TBI. Heart rate variability refers to the variation in time between consecutive heartbeats. Healthy individuals exhibit high HRV, indicating a good balance between sympathetic and parasympathetic activity, as well as the ability to adapt to changing demands. After TBI, many people show decreased HRV, suggesting an autonomic imbalance. This imbalance typically involves increased sympathetic activity and decreased parasympathetic activity, resulting in the body remaining stuck in a heightened state of arousal with difficulty returning to a relaxed state. hellonote+4
The presence of autonomic dysfunction correlates with increased morbidity and mortality in moderate and severe TBI. Autonomic imbalance can lead to cardiac complications, including irregular heart rhythms, sudden cardiac events, and increased blood pressure. Studies show that decreased baroreflex sensitivity—a measure of ANS activity—correlates with increased risk of these cardiac complications. Perturbations of the ANS may result in dangerous heart rhythms and sudden cardiac death. jamanetwork+1 Autonomic dysfunction also affects recovery outcomes more broadly. Research shows that patients with autonomic dysfunction after TBI experience longer periods of post-traumatic amnesia, longer hospital stays, and higher overall healthcare costs. The autonomic symptoms themselves negatively impact quality of life and correlate with other symptoms, such as fatigue, pain, and negative perceptions of health status. Understanding and addressing autonomic dysfunction represents an important but often overlooked aspect of TBI care. pmc.ncbi.nlm.nih+2
Stress, Anxiety, and Reduced Stress Tolerance After TBI
Clinical evidence demonstrates that mild TBI increases the risk for anxiety disorders. Studies show that anxiety symptoms and disorders occur frequently in the first year after mild TBI, with rates significantly higher than in the general population. In military populations, research found that forty-four percent of those with mild TBI screened positive for post-traumatic stress disorder (PTSD), compared to only sixteen percent of those with bodily injuries but no TBI. This elevated risk for anxiety and PTSD after TBI creates significant challenges for recovery. apa+4 The relationship between TBI and PTSD illustrates how these conditions can coexist and interact. TBI and PTSD share overlapping symptoms, making diagnosis complicated. Both conditions can cause problems with memory, concentration, sleep, irritability, and emotional regulation. However, the mechanisms differ: PTSD results from psychological trauma and involves fear conditioning and altered fear responses, while TBI involves physical brain damage that disrupts neural circuits. When both conditions occur together—which happens frequently because brain injuries often result from traumatic events—the symptoms can compound each other and create more severe impairment. pmc.ncbi.nlm.nih+3
Interestingly, research shows that mild TBI actually increases the risk for developing PTSD, a finding that contradicts earlier beliefs that TBI protects against PTSD. Multiple large-scale studies demonstrate that individuals who sustain a mild TBI are significantly more likely to develop PTSD compared to those with no TBI. The mechanisms behind this increased risk remain under investigation, but likely involve altered stress reactivity, enhanced fear conditioning, and dysfunction in brain regions that regulate fear and anxiety. ptsd.va+2 Reduced stress tolerance represents another significant problem after TBI. Individuals with TBI often find that situations that would have been manageable before their injury now feel overwhelming. They may experience heightened emotional reactions to minor stressors and struggle to regulate their stress responses. This reduced stress tolerance stems partly from damage to brain regions involved in emotional regulation and stress appraisal, and partly from the ongoing physiological stress created by the injury itself. abct+1
The chronic activation of stress systems takes a toll on the body. Prolonged elevation of cortisol and sustained sympathetic nervous system activation can lead to multiple adverse effects, including suppressed immune function, increased inflammation, disrupted sleep, mood disturbances, cardiovascular problems, and metabolic dysfunction. These effects create a vicious cycle in which stress impairs recovery, leading to more stress, which in turn further impairs recovery. eihmd+6
The Role of Environmental Factors in TBI Recovery
Environmental factors significantly influence recovery outcomes after TBI. These factors include both the physical environment (such as noise levels, lighting, and crowding) and the social environment (including support systems, access to healthcare, socioeconomic status, and cultural factors). pubmed.ncbi.nlm.nih+4 Research consistently demonstrates that environmental enrichment promotes better outcomes after TBI. Animal studies have shown that housing injured animals in enriched environments—with opportunities for physical activity, cognitive stimulation, and social interaction—leads to improved cognitive function, enhanced neuroplasticity, and better structural recovery of the brain compared to animals housed in standard conditions. Human studies similarly find that greater participation in intellectual and social leisure activities associates with better cognitive outcomes and lower rates of decline. frontiersin
Conversely, lack of environmental enrichment may contribute to post-acute cognitive and neural decline after TBI. Studies document that a significant percentage of TBI survivors experience cognitive decline rather than improvement in the months and years following their injury. This decline may result partly from reduced access to stimulating environments after discharge from intensive rehabilitation services. When people return home from rehabilitation facilities, they may find themselves in environments that are less cognitively and physically stimulating than the structured therapy environment. Additionally, cognitive, physical, or emotional impairments from the TBI may prevent individuals from effectively engaging with potentially enriching environments. frontiersin
Specific environmental barriers commonly reported by TBI survivors include transportation difficulties, challenging physical surroundings (such as poor lighting, excessive noise, or crowding), unsupportive government policies, negative attitudes from others, and challenges posed by the natural environment. These barriers affect multiple aspects of community integration, including employment, social participation, and overall life satisfaction. Addressing these environmental barriers represents an important target for improving outcomes after TBI. biausa+2
Overlapping Risk Profiles: TBI and Comorbid Conditions
TBI creates increased risk for numerous comorbid conditions, creating overlapping risk profiles that complicate treatment and recovery. Research shows that TBI of any severity is associated with increased risk for neurological, psychiatric, cardiovascular, and endocrine conditions. pmc.ncbi.nlm.nih+3 In a large cohort study examining long-term health outcomes after TBI, researchers found that individuals with TBI had a dramatically increased risk for multiple neuropsychiatric conditions. For neurological outcomes, TBI increased the risk of stroke by approximately two-fold, seizure disorders by over three-fold, and dementia by over three-fold. Psychiatric outcomes showed similarly striking increases: depression risk increased by over two-fold, anxiety disorders by over two-fold, sleep disorders by two-fold, suicidality by over two-fold, and substance misuse by over two-fold. Cardiovascular conditions, including hypertension, hyperlipidemia, obesity, and coronary artery disease, all showed increased risk after TBI. Even endocrine conditions like hypothyroidism, diabetes, and hormonal dysfunction occurred more frequently in individuals with a history of TBI. pmc.ncbi.nlm.nih
The relationship between TBI and PTSD represents a particularly important example of overlapping risk profiles. These conditions frequently coexist because brain injuries often occur during traumatic events. The coexistence creates diagnostic challenges due to overlapping symptoms like memory problems, concentration difficulties, sleep disturbances, irritability, and mood changes. Both conditions share certain pathophysiological features, including neuroinflammation, excitotoxicity, and oxidative damage. When TBI and PTSD occur together, they create more complex symptom presentations and greater functional impairment than either condition alone. journals.sagepub+6 Depression represents another common comorbidity after TBI, affecting over half of individuals in some studies. The neuroinflammation and neurochemical changes caused by TBI contribute to the development of depression. Additionally, the functional limitations and life changes resulting from TBI create psychological stress that can trigger or worsen depression. frontiersin+3 Understanding these overlapping risk profiles helps clinicians provide more comprehensive care. Rather than treating TBI in isolation, healthcare providers need to screen for and address comorbid conditions. This comprehensive approach improves overall outcomes and quality of life for TBI survivors. frontiersin+1
Chiropractic Care After Accidents and Injuries-Video
How Chiropractic Care Can Help TBI Recovery
Chiropractic care offers a non-invasive approach to supporting recovery after TBI, particularly when combined with other integrative treatments. While chiropractic care cannot reverse the primary brain injury, it can address many secondary issues that contribute to ongoing symptoms and impaired recovery. pinnaclehealthchiro+6 The foundation of chiropractic care for TBI involves spinal adjustments to restore proper alignment and improve nervous system function. The spine houses the spinal cord, which serves as the primary pathway for communication between the brain and the rest of the body. When vertebrae become misaligned due to trauma—which commonly occurs in accidents that also cause TBI—these misalignments can interfere with nerve signals and contribute to symptoms like pain, headaches, dizziness, and tension. calibrationmansfield+5 Chiropractic adjustments help restore proper spinal alignment, which can relieve pressure on nerves and improve the flow of information throughout the nervous system. This improved communication supports the brain’s healing process and can reduce many TBI-related symptoms. Research shows that chiropractic adjustments can improve overall nervous system function, which proves crucial in the recovery process. neurotraumacenters+5
One important mechanism through which chiropractic care supports recovery from TBI involves restoring cerebrospinal fluid (CSF) flow. Cerebrospinal fluid protects and nourishes the brain, removing waste products and delivering nutrients. After TBI, CSF flow can become disrupted, potentially impeding brain healing. Manual chiropractic adjustments and soft tissue therapy help restore normal CSF flow throughout the brain and spinal cord. This restoration of CSF dynamics represents an essential aspect of brain health and recovery. withinchiro+2 Chiropractic care also addresses musculoskeletal issues that commonly accompany TBI. Many people who sustain a TBI also experience whiplash, neck injuries, or other soft tissue damage. These injuries can cause chronic pain, muscle tension, and reduced mobility, all of which interfere with recovery and quality of life. Chiropractic treatments, including spinal manipulation, soft tissue therapy, myofascial release, and trigger point therapy, help address these musculoskeletal problems. By alleviating physical pain and tension, these treatments support overall healing and enhance the person’s ability to engage in other aspects of recovery. pinnaclehealthchiro+3
Another significant benefit of chiropractic care involves its effects on the autonomic nervous system. As discussed earlier, TBI frequently disrupts autonomic function, resulting in issues with stress regulation, sleep, digestion, cardiovascular function, and other involuntary bodily processes. Chiropractic adjustments help restore balance to the autonomic nervous system by promoting parasympathetic activation. The parasympathetic branch of the ANS controls the body’s rest, digest, and healing responses. By enhancing parasympathetic function, chiropractic care helps shift the body out of the chronic fight-or-flight state that often follows TBI and into a state more conducive to healing. txmac+9 Research demonstrates that chiropractic adjustments can reduce levels of cortisol, the primary stress hormone. Studies have shown that patients receiving chiropractic care experience decreased cortisol levels, along with reduced self-reported stress and improved relaxation. By reducing cortisol and promoting autonomic balance, chiropractic care helps address the stress dysregulation that commonly occurs after TBI. northbayspineandrehab+5 Chiropractic care also improves blood flow, which proves essential for brain healing. Adequate blood circulation delivers oxygen and nutrients to injured brain tissue while removing waste products. Spinal adjustments improve blood flow throughout the body, including to the brain. This enhanced circulation supports the metabolic processes required for tissue repair and neuroplasticity. hmlfunctionalcare+3
Several specialized chiropractic techniques have shown particular promise in treating TBI. Chiropractic neurology focuses on enhancing brain and nervous system function through non-invasive methods, utilizing techniques such as spinal adjustments, sensory therapies, and targeted exercises to stimulate neuroplasticity. This approach addresses conditions like TBI by enhancing neural pathways and brain function. Upper cervical chiropractic techniques, which focus on precise adjustments to the upper neck, can be particularly beneficial for TBI patients as they help optimize brainstem function and reduce pressure on critical neural structures. neurochiro+6
Integrative Approaches: Combining Chiropractic Care with Other Treatments
The most effective approach to TBI recovery typically involves combining chiropractic care with other integrative treatments. This multimodal approach addresses the complex and multifaceted nature of TBI, targeting multiple mechanisms of healing simultaneously. pmc.ncbi.nlm.nih+6 Massage therapy represents an important complementary treatment to chiropractic care for TBI. Massage helps reduce muscle tension, improve circulation, decrease pain, and promote relaxation. After TBI, many individuals experience chronic muscle tension, particularly in the neck and shoulders, which can contribute to headaches and other symptoms. Massage therapy addresses this tension through various techniques, including myofascial release, trigger point therapy, and Swedish massage. Research indicates that massage therapy offers effective short-term relief for chronic pain, enhancing both physical function and quality of life.thinkvida+7 Acupuncture offers another valuable complementary therapy for TBI recovery. This traditional Chinese medicine practice involves inserting thin needles at specific points on the body to restore the flow of energy and promote overall well-being and healing. Scientific research has demonstrated that acupuncture produces measurable physiological effects relevant to TBI recovery. Studies show that acupuncture promotes neurological recovery after TBI by activating the BDNF/TrkB signaling pathway. BDNF represents a crucial protein for brain health, supporting neuronal survival, neuroplasticity, and cognitive function. By enhancing BDNF levels, acupuncture supports the brain’s natural healing processes.pmc.ncbi.nlm.nih+5
Research demonstrates that acupuncture improves multiple aspects of neurological function after TBI, including motor function, sensory abilities, cognitive performance, and synaptic plasticity. In animal studies, acupuncture treatment significantly reduced neurological deficit scores, improved motor coordination, enhanced memory and learning, and increased markers of neuroplasticity compared to control groups. When researchers blocked the BDNF pathway using a specific inhibitor, these beneficial effects of acupuncture disappeared, confirming that the BDNF mechanism underlies acupuncture’s therapeutic effects. pmc.ncbi.nlm.nih Acupuncture also helps reduce neuroinflammation and improve blood flow to affected brain regions. It can alleviate specific TBI-related symptoms such as headaches, dizziness, brain fog, sleep disturbances, and mood problems. Many patients report significant symptom relief and improved quality of life with acupuncture treatment. wildcoasthealth+2
Exercise represents another critical component of comprehensive TBI rehabilitation. Physical activity promotes neuroplasticity, improves cognitive function, enhances mood, and supports overall brain health. Aerobic exercise increases blood flow to the brain, stimulates the release of neurotrophic factors like BDNF, and promotes the growth of new neurons and synapses. Studies show that exercise improves cardiorespiratory fitness, cognitive function, balance, gait, and quality of life in TBI survivors. neuropt+5 However, exercise prescription after TBI requires careful consideration. Research indicates that exercise intensity and timing are significant factors. Exercise that exceeds an individual’s tolerance can activate stress responses and potentially impede recovery. Therefore, exercise programs for TBI should be individualized based on symptom tolerance and gradually progressed as recovery advances. The concept of sub-symptom threshold exercise—activity that does not exacerbate symptoms—has shown particular promise for recovery from TBI. neuliferehab+2
Recommended exercise parameters for TBI recovery include low-resistance, rhythmic, dynamic activities such as walking, jogging, cycling, or using an elliptical machine. Exercise intensity should generally range from 60 to 90 percent of the age-predicted maximum heart rate, with sessions lasting 20 to 40 minutes, performed three to four times per week. These parameters can be adjusted based on individual tolerance and recovery status. neuropt+1 Additional complementary therapies that may benefit TBI recovery include nutritional interventions, stress management techniques, sleep optimization, and cognitive rehabilitation. Nutritional supplementation with vitamins, minerals, omega-3 fatty acids, and antioxidants may support brain healing by reducing inflammation, combating oxidative stress, and providing building blocks for neural repair. Stress management techniques such as meditation, mindfulness practices, breathing exercises, and biofeedback can help address the stress dysregulation common after TBI. Addressing sleep disturbances proves crucial since quality sleep supports brain healing and cognitive recovery. dralexjimenez+9
Dr. Alexander Jimenez’s Integrative Approach to TBI and Injury Care in El Paso
Dr. Alexander Jimenez, DC, APRN, FNP-BC, exemplifies the integrative approach to treating TBI and other injuries at his clinic in El Paso, Texas. His unique dual credentials as both a Doctor of Chiropractic and a board-certified Family Practice Nurse Practitioner enable him to provide comprehensive care that addresses both the biomechanical and medical aspects of injury. dralexjimenez+1 Dr. Jimenez’s clinic specializes in treating various injuries from work accidents, sports activities, personal incidents, and motor vehicle accidents. His practice focuses on evidence-based treatment protocols inspired by principles of integrative medicine, emphasizing the natural restoration of health for patients of all ages. The clinic’s areas of practice include wellness and nutrition, chronic pain management, personal injury care, auto accident rehabilitation, work injuries, back and neck pain, migraine headaches, sports injuries, sciatica, complex herniated discs, stress management, and functional medicine treatments. dralexjimenez+1
A key aspect of Dr. Jimenez’s practice involves correlating patient injuries with dual-scope diagnosis, treatment procedures, diagnostic assessments, and advanced neuromusculoskeletal imaging. This comprehensive approach ensures accurate diagnosis and targeted treatment. Dr. Jimenez utilizes sophisticated diagnostic tools to accurately identify the specific nature and extent of injuries, including those related to TBI complications. dralexjimenez+1 For patients with TBI, Dr. Jimenez’s integrative approach combines multiple treatment modalities to address the complex nature of these injuries. His treatment protocols may include chiropractic adjustments to restore spinal alignment and improve nervous system function, functional medicine interventions to address underlying metabolic and inflammatory issues, acupuncture to promote neurological recovery and reduce symptoms, nutritional support to provide the building blocks for healing, and targeted rehabilitation exercises to restore function and prevent long-term complications. dralexjimenez+1
Dr. Jimenez’s clinic also provides comprehensive support for the legal aspects of injury cases. When patients sustain injuries in motor vehicle accidents or other incidents that may involve legal claims, accurate and thorough medical documentation becomes essential. Dr. Jimenez provides detailed reports that link injuries to the accident, document treatment plans and their necessity, and support compensation claims. His documentation is legally admissible, and he can provide expert testimony to explain his findings clearly to judges, juries, and insurance adjusters.zdfirm+3 The medical evidence Dr. Jimenez provides includes establishing causation—linking the injuries directly to the accident through diagnostic tests and clinical observations. For example, he can demonstrate how the forces involved in a collision cause specific injuries like whiplash, herniated discs, or TBI. His reports detail the severity of injuries, their impact on function and quality of life, and the necessity of ongoing care to achieve optimal recovery. dralexjimenez Dr. Jimenez works closely with personal injury attorneys, providing tailored reports that meet insurance and court standards. His dual licensure enhances his credibility as an expert witness, allowing him to explain both chiropractic and medical aspects of injuries comprehensively. He helps patients navigate insurance claims to ensure their treatments receive proper coverage. This collaboration between medical care and legal support helps ensure that injury victims receive fair compensation for their medical expenses, lost wages, pain and suffering, and long-term care needs. dralexjimenez
The integrative medicine approach used at Dr. Jimenez’s clinic addresses the root causes of symptoms rather than simply masking them with medication. For TBI patients, this means investigating and treating the underlying inflammatory processes, oxidative stress, hormonal imbalances, autonomic dysfunction, and other factors that contribute to persistent symptoms. The clinic uses advanced assessments, including functional medicine health evaluations that examine personal history, nutrition, activity patterns, environmental exposures, and psychological factors. This comprehensive evaluation enables the development of truly personalized treatment plans that address each patient’s unique needs and requirements. wellnesscenterfw+3
An Example of A TBI Symptom Questionnaire
Promoting Natural Healing and Preventing Long-Term Problems
One of the most important goals in TBI treatment involves promoting the brain’s natural healing mechanisms while preventing the development of long-term problems. The brain possesses remarkable plasticity—the ability to reorganize, adapt, and form new neural connections. This neuroplasticity underlies recovery after brain injury. psychiatrictimes+4 Neuroplasticity-based rehabilitation strategies aim to maximize the brain’s reorganization potential. These approaches involve intensive, repetitive practice of functional tasks, which drives the formation of new neural circuits. The principle “neurons that fire together wire together” explains how repeated activation of specific neural pathways strengthens those connections. Through consistent practice and appropriate challenges, new pathways can compensate for damaged brain regions. pmc.ncbi.nlm.nih+2
Effective rehabilitation requires a multidisciplinary approach that integrates physical therapy, occupational therapy, cognitive rehabilitation, speech therapy, psychological support, and complementary treatments. Each discipline targets different aspects of function while working toward common goals. The collaboration between healthcare providers ensures comprehensive care that addresses the complex needs of TBI survivors.p mc.ncbi.nlm.nih+4 Early intervention proves crucial for optimizing outcomes. The brain shows heightened plasticity in the early weeks and months after injury, creating a window of opportunity for rehabilitation. However, neuroplasticity continues throughout life, meaning that improvement remains possible even years after injury with appropriate interventions. The key lies in providing continued stimulation, challenge, and support for neural adaptation. ncbi.nlm.nih+3
Preventing long-term problems requires addressing multiple factors. First, controlling inflammation and oxidative stress helps limit secondary brain damage. Strategies to reduce inflammation include maintaining a healthy diet rich in anti-inflammatory foods, managing stress effectively, ensuring adequate sleep, and potentially using targeted supplements or medications under the guidance of a medical professional. frontiersin+8 Second, maintaining cardiovascular health and metabolic function supports brain healing. Regular exercise, proper nutrition, adequate hydration, and effective management of conditions such as hypertension and diabetes all contribute to optimal brain health. kesslerfoundation+2 Third, addressing psychological health proves essential. The high rates of depression, anxiety, and PTSD after TBI necessitate screening and treatment for these conditions. Psychological interventions, including cognitive behavioral therapy, stress management training, mindfulness practices, and, when appropriate, psychiatric medication, can significantly improve outcomes and quality of life. concussionalliance+6 Fourth, promoting environmental enrichment and social support enhances recovery. Encouraging individuals with TBI to engage in cognitively stimulating activities, maintain social connections, pursue hobbies and interests, and stay physically active promotes continued brain adaptation and prevents decline. pubmed.ncbi.nlm.nih+2 Fifth, monitoring for and treating comorbid conditions prevents complications. Given the increased risk for multiple medical and psychiatric conditions after TBI, regular medical follow-up and comprehensive health management become important. wellnesscenterfw+2
Conclusion
Traumatic brain injury represents a complex medical condition that affects not only the brain but the entire body, particularly through its interactions with stress systems and autonomic function. Understanding TBI requires recognizing both the immediate physical damage and the secondary processes that can continue for months or years after injury. The relationship between TBI and stress operates in multiple directions: TBI disrupts stress regulation systems, stress worsens TBI outcomes, and the experience of living with TBI creates ongoing stress. Cognitive impairments affecting attention, memory, processing speed, and executive function represent common consequences of TBI that significantly impact daily functioning. Autonomic dysfunction creates additional symptoms affecting multiple body systems and interferes with stress regulation. Environmental factors, comorbid conditions, and the quality of rehabilitation and support all influence recovery trajectories. Chiropractic care, particularly when combined with other integrative treatments, offers valuable support for TBI recovery. By addressing spinal alignment, improving nervous system function, restoring cerebrospinal fluid flow, reducing stress hormone levels, promoting autonomic balance, and enhancing blood flow, chiropractic care targets multiple mechanisms relevant to healing. Combined with massage therapy, acupuncture, targeted exercise, nutritional support, and other complementary therapies, this integrative approach provides comprehensive treatment that addresses the multifaceted nature of TBI.
Dr. Alexander Jimenez’s practice in El Paso exemplifies this integrative approach, combining his dual expertise as a chiropractor and nurse practitioner to provide evidence-based care for TBI and other injuries. His comprehensive treatment protocols, advanced diagnostic capabilities, and support for the legal aspects of injury cases ensure that patients receive thorough care addressing both their medical needs and practical concerns. The path to recovery from TBI requires patience, comprehensive care, and attention to multiple aspects of health. By addressing physical injuries, supporting natural healing processes, managing stress and autonomic dysfunction, promoting neuroplasticity through targeted rehabilitation, and preventing long-term complications, individuals with TBI can achieve a meaningful recovery and an improved quality of life. While TBI presents significant challenges, the combination of modern medical understanding, integrative treatment approaches, and the brain’s remarkable capacity for adaptation offers hope for healing and a return to well-being.
References
Alam, M. M., Lee, J., & Lee, S. Y. (2017). Recent progress in the development of THIQ derivatives as neuroprotective agents for the treatment of neurodegenerative diseases. International Journal of Molecular Sciences, 18(8), 1713. https://doi.org/10.3390/ijms18081713
Baguley, I. J., Heriseanu, R. E., Cameron, I. D., Nott, M. T., & Slewa-Younan, S. (2008). A critical review of the pathophysiology of dysautonomia following traumatic brain injury. Neurocritical Care, 8(2), 293-300.
Barlow, K. M. (2016). Traumatic brain injury. Handbook of Clinical Neurology, 136, 883-906.
Bryant, R. A., & Harvey, A. G. (1999). Postconcussive symptoms and posttraumatic stress disorder after mild traumatic brain injury. Journal of Nervous and Mental Disease, 187(5), 302-305.
Chamoun, R., Suki, D., Gopinath, S. P., Goodman, J. C., & Robertson, C. (2010). Role of extracellular glutamate measured by cerebral microdialysis in severe traumatic brain injury. Journal of Neurosurgery, 113(3), 564-570.
Coronado, V. G., Xu, L., Basavaraju, S. V., McGuire, L. C., Wald, M. M., Faul, M. D., Guzman, B. R., & Hemphill, J. D. (2011). Surveillance for traumatic brain injury-related deaths. Morbidity and Mortality Weekly Report Surveillance Summaries, 60(5), 1-32.
Elder, G. A., & Cristian, A. (2009). Blast-related mild traumatic brain injury: Mechanisms of injury and impact on clinical care. Mount Sinai Journal of Medicine, 76(2), 111-118.
Fann, J. R., Burington, B., Leonetti, A., Jaffe, K., Katon, W. J., & Thompson, R. S. (2004). Psychiatric illness following traumatic brain injury in an adult health maintenance organization population. Archives of General Psychiatry, 61(1), 53-61.
Ghajar, J. (2000). Traumatic brain injury. Lancet, 356(9233), 923-929.
Guglielmino, C., & Dean, P. J. (2022). The pathophysiological bases of comorbidity: Traumatic brain injury and post-traumatic stress disorder. Frontiers in Neurology, 12, 654210.
Hoge, C. W., McGurk, D., Thomas, J. L., Cox, A. L., Engel, C. C., & Castro, C. A. (2008). Mild traumatic brain injury in U.S. soldiers returning from Iraq. New England Journal of Medicine, 358(5), 453-463.
Huang, S., Wu, B., Liu, J., Jiang, Q., Wang, Y., Li, M., Zhang, J., Luo, A., Zhou, Y., & Guan, S. (2017). Recent advances in pathophysiology of traumatic brain injury. Translational Neuroscience and Clinics, 3(1), 7-14.
Jamshidi, N., & Cohen, M. M. (2017). The clinical efficacy and safety of tulsi in humans: A systematic review of the literature. Evidence-Based Complementary and Alternative Medicine, 2017, 9217567.
King, C., Robinson, T., Dixon, C. E., Rao, G. R., Larnard, D., & Nemoto, C. E. (2010). Brain temperature profiles during epidural cooling with the ChillerPad in a monkey model of traumatic brain injury. Journal of Neurotrauma, 27(10), 1895-1903.
Kumar, A., & Loane, D. J. (2012). Neuroinflammation after traumatic brain injury: Opportunities for therapeutic intervention. Brain, Behavior, and Immunity, 26(8), 1191-1201.
Leddy, J. J., Haider, M. N., Ellis, M., & Willer, B. S. (2018). Exercise is medicine for concussion. Current Sports Medicine Reports, 17(8), 262-270.
Li, H., Tang, Z., Chu, P., Song, Y., Yang, Y., Sun, B., Niu, Y., Wang, Y., Mao, X., Lin, C., Huang, X., Ma, K., & Bian, J. M. (2014). Neuroprotective effect of phosphocreatine on oxidative stress and mitochondrial dysfunction induced by glutamate in hippocampal HT22 cells. Neurochemical Research, 39(7), 1205-1215.
Logsdon, A. F., Lucke-Wold, B. P., Turner, R. C., Huber, J. D., Rosen, C. L., & Simpkins, J. W. (2018). Role of microvascular disruption in brain damage from traumatic brain injury. Comprehensive Physiology, 8(3), 1147-1169.
Maas, A. I., Stocchetti, N., & Bullock, R. (2008). Moderate and severe traumatic brain injury in adults. Lancet Neurology, 7(8), 728-741.
McAllister, T. W. (2011). Neurobiological consequences of traumatic brain injury. Dialogues in Clinical Neuroscience, 13(3), 287-300.
McKee, A. C., & Daneshvar, D. H. (2015). The neuropathology of traumatic brain injury. Handbook of Clinical Neurology, 127, 45-66.
Meyer, D. L., Davies, D. R., Barr, J. L., Manzerra, P., & Forster, G. L. (2012). Mild traumatic brain injury in the rat alters neuronal number in the limbic system and increases conditioned fear and anxiety-like behaviors. Experimental Neurology, 235(2), 574-587.
Prins, M., Greco, T., Alexander, D., & Giza, C. C. (2013). The pathophysiology of traumatic brain injury at a glance. Disease Models & Mechanisms, 6(6), 1307-1315.
Rabinowitz, A. R., & Levin, H. S. (2014). Cognitive sequelae of traumatic brain injury. Psychiatric Clinics of North America, 37(1), 1-11.
Riggio, S., & Wong, M. (2009). Neurobehavioral sequelae of traumatic brain injury. Mount Sinai Journal of Medicine, 76(2), 163-172.
Risdall, J. E., & Menon, D. K. (2011). Traumatic brain injury. Philosophical Transactions of the Royal Society B: Biological Sciences, 366(1562), 241-250.
Sharp, D. J., Scott, G., & Leech, R. (2014). Network dysfunction after traumatic brain injury. Nature Reviews Neurology, 10(3), 156-166.
Smith, D. H., Johnson, V. E., & Stewart, W. (2013). Chronic neuropathologies of single and repetitive TBI: Substrates of dementia? Nature Reviews Neurology, 9(4), 211-221.
Stern, R. A., Riley, D. O., Daneshvar, D. H., Nowinski, C. J., Cantu, R. C., & McKee, A. C. (2011). Long-term consequences of repetitive brain trauma: Chronic traumatic encephalopathy. PM&R, 3(10 Suppl 2), S460-S467.
Summers, C. R., Ivins, B., & Schwab, K. A. (2009). Traumatic brain injury in the United States: An epidemiologic overview. Mount Sinai Journal of Medicine, 76(2), 105-110.
Taylor, C. A., Bell, J. M., Breiding, M. J., & Xu, L. (2017). Traumatic brain injury-related emergency department visits, hospitalizations, and deaths. Morbidity and Mortality Weekly Report Surveillance Summaries, 66(9), 1-16.
Thurman, D. J., Alverson, C., Dunn, K. A., Guerrero, J., & Sniezek, J. E. (1999). Traumatic brain injury in the United States: A public health perspective. Journal of Head Trauma Rehabilitation, 14(6), 602-615.
Van Reekum, R., Cohen, T., & Wong, J. (2000). Can traumatic brain injury cause psychiatric disorders? Journal of Neuropsychiatry and Clinical Neurosciences, 12(3), 316-327.
Vasterling, J. J., Bryant, R. A., & Keane, T. M. (2012). PTSD and mild traumatic brain injury. Guilford Press.
Wang, M. L., Yu, M. M., Yang, D. X., Liu, Y. L., Wei, X. E., & Li, W. B. (2018). Neurological symptoms and their associations with inflammatory biomarkers following traumatic brain injury. Frontiers in Neurology, 13, 876490.
Werner, C., & Engelhard, K. (2007). Pathophysiology of traumatic brain injury. British Journal of Anaesthesia, 99(1), 4-9.
Xiong, Y., Gu, Q., Peterson, P. L., Muizelaar, J. P., & Lee, C. P. (1997). Mitochondrial dysfunction and calcium perturbation induced by traumatic brain injury. Journal of Neurotrauma, 14(1), 23-34.
Yuh, E. L., Mukherjee, P., Lingsma, H. F., Yue, J. K., Ferguson, A. R., Gordon, W. A., Valadka, A. B., Schnyer, D. M., Okonkwo, D. O., Maas, A. I., Manley, G. T., & TRACK-TBI Investigators. (2013). Magnetic resonance imaging improves 3-month outcome prediction in mild traumatic brain injury. Annals of Neurology, 73(2), 224-235.
Boosting Vitality: Chiropractic and Integrative Care for Optimal Circulation
Introduction
Imagine your body as a network of highways, with blood vessels carrying oxygen and nutrients to every cell, keeping you energized and healthy. This process, known as optimal circulation, ensures the circulatory system efficiently delivers these essentials while removing waste, supporting cell function, and overall vitality (Henry Ford Health, 2025). When circulation falters, you may feel tired, have cold hands, or experience issues such as swelling. Chiropractic care can help by aligning the spine to reduce nerve pressure and improve blood flow naturally. Paired with integrative therapies like massage and exercise, it promotes lasting wellness (Sierra, n.d.). This article examines how these methods enhance circulation, drawing on insights from Dr. Alexander Jimenez at El Paso Back Clinic in El Paso, TX, to demonstrate their role in aiding injury recovery and promoting overall health.
Why Optimal Circulation Matters
Optimal circulation is the body’s way of keeping everything running smoothly. Blood delivers oxygen and nutrients to cells, fueling energy production through ATP and clearing waste, such as carbon dioxide, to prevent fatigue and aches (Elevation Health, n.d.). Good circulation sharpens your mind, strengthens muscles, and speeds up immune responses, helping you fight off illness (Rodgers Stein Chiropractic, n.d.a).
When circulation slows, problems arise—cold feet, leg cramps, or even brain fog can signal trouble. Over time, poor flow increases the risk of conditions such as high blood pressure or slow healing (KC Chiropractic, 2025). Signs of healthy circulation include warm limbs and quick recovery after exercise, while sluggish flow might cause tingling or puffiness (British Heart Foundation, n.d.). Chiropractic care, combined with integrative approaches, keeps these pathways clear, enhancing energy and preventing long-term issues.
The Circulatory System Explained
The circulatory system is your body’s delivery service. The heart pumps approximately 2,000 gallons of blood daily through arteries, veins, and capillaries, delivering oxygen and nutrients while removing waste (Elevation Health, n.d.). Capillaries facilitate the exchange, ensuring that cells receive what they need and toxins are removed to the lungs or kidneys. The nervous system, especially its autonomic part, controls this by adjusting blood vessel size and heart rate, like speeding up for a workout (Sierra, n.d.).
Blockages, such as plaque from unhealthy eating or stress-tightened vessels, disrupt this flow, starving cells of oxygen and slowing waste removal. This can lead to tiredness, weak immunity, or muscle pain (Henry Ford Health, 2025). Maintaining this system supports clear thinking, strong movement, and overall health (Rodgers Stein Chiropractic, n.d.a).
How Chiropractic Care Improves Blood Flow
Chiropractic care focuses on the spine, the central control center of the nervous system. Misaligned vertebrae, or subluxations, can pinch nerves, disrupting signals that regulate blood vessels. Gentle adjustments correct these misalignments, freeing nerves to improve circulation (Sierra, n.d.). Patients often report feeling warmer hands or reduced tingling after sessions, indicating improved blood flow (Chiropractor Lakeworth, n.d.).
These adjustments enhance energy by speeding oxygen delivery to cells and clearing waste, reducing fatigue (LSM Chiropractic, n.d.). Regular care can lower blood pressure, ease heart strain, and improve focus by boosting brain blood flow (Ford Chiropractic, n.d.; Peak Portland, n.d.). Chiropractors may also use tools like ultrasound to warm tissues or suggest foods that support vascular health, helping prevent issues like neuropathy (Chiropractor Lakeworth, n.d.).
Dr. Alexander Jimenez and El Paso Back Clinic’s Approach
At El Paso Back Clinic, Dr. Alexander Jimenez, DC, APRN, FNP-BC, leverages his dual expertise as a chiropractor and nurse practitioner to enhance circulation, particularly after injuries. With over 30 years of experience, his team treats conditions from sports strains to motor vehicle accidents (MVAs), recognizing how trauma can inflame tissues or compress nerves, blocking blood flow (Jimenez, n.d.a). “Injuries create structural imbalances that disrupt circulation,” he notes (Jimenez, n.d.b).
The clinic utilizes advanced diagnostics, combining neuromusculoskeletal imaging, such as X-rays, with blood tests to identify inflammation. For instance, a work-related injury might show nerve pressure affecting leg circulation. Treatments include non-surgical adjustments to restore alignment, ultrasound to reduce swelling, and tailored exercises to strengthen blood vessels (Jimenez, n.d.a). For MVA patients, the clinic provides detailed medical-legal documentation for claims, ensuring seamless care coordination.
Integrative therapies enhance outcomes: massage improves blood flow, acupuncture eases inflammation, and nutrition plans rich in omega-3s promote vascular health. A patient recovering from a fall might regain circulation through adjustments and targeted stretches, avoiding chronic pain (Jimenez, n.d.b). Dr. Jimenez focuses on root causes—like poor posture or old injuries—to foster natural healing and sustained vitality.
Integrative Therapies for Circulation
Integrative care combines natural methods to support the body’s healing abilities. Massage therapy relaxes tight muscles, pushing blood toward the heart and reducing swelling, which boosts energy (Chiropractor Lakeworth, n.d.). The NHS recommends 150 minutes of weekly exercise, such as walking or swimming, to strengthen blood vessels and improve blood flow (British Heart Foundation, n.d.). Chiropractors design specific stretches or yoga poses to enhance spinal alignment and circulation.
Acupuncture targets points to open blood vessels, reducing stress-related constriction (Jimenez, n.d.a). Nutrient-rich foods, such as berries or fish oils, help keep blood fluid and vessels flexible (Kennedy Chiropractic, n.d.). These therapies work together to prevent injury recurrence and maintain energy (University of Minnesota Center for Spirituality & Healing, n.d.). At El Paso Back Clinic, a patient may combine adjustments, massage, and a diet rich in anti-inflammatory foods to restore circulation and alleviate discomfort.
Daily Habits to Support Circulation
Simple habits can enhance professional care. Walk 30 minutes daily to boost heart function and vascular health (British Heart Foundation, n.d.). Avoid smoking to prevent vessel narrowing, and incorporate foods like leafy greens and salmon into your diet for their iron and omega-3 content (Henry Ford Health, 2025; Kennedy Chiropractic, n.d.). Stress-relief practices, such as meditation, relax blood vessels, while elevating legs after long periods of sitting, prevent blood pooling (Rodgers Stein Chiropractic, n.d.a). Drinking water keeps blood flowing smoothly. Regular chiropractic visits amplify these efforts for long-term benefits.
Conclusion
Optimal circulation fuels your body, delivering oxygen and nutrients while clearing waste to sustain energy and health. Chiropractic care at El Paso Back Clinic aligns the spine to free nerves, enhancing blood flow, while integrative therapies, such as massage, exercise, and acupuncture, support natural healing. Dr. Jimenez’s expertise shows how these methods address injury-related circulation issues, promoting recovery and vitality. Begin with a chiropractic consultation, add daily movement, and embrace integrative care to keep your body’s pathways vibrant and strong.
Your Spine, Your Life: An El Paso-Ready Guide to Strong, Flexible, Pain-Resistant Backs
A young woman is performing a spine checkup at a vertebra clinic.
What “spinal health” means (and why it matters here in El Paso)
Spinal health refers to the proper structure, alignment, and function of the spine, enabling it to support the body, facilitate movement, and protect the spinal cord—the pathway for nerve signals between the brain and the body. Good spinal health comes from regular exercise, posture awareness, a nutrient-dense diet, steady hydration, and a healthy weight. Poor spinal health can lead to chronic pain, nerve irritation or damage, and a lower quality of life (Raleigh Orthopaedics, 2024; Orthopedic Specialists of Southwest Florida [OSSWF], 2024; National Spine Health Foundation, 2024).
How a healthy spine supports your whole body
Support & alignment: Your spine acts like a central pillar that shares load with the hips and legs and keeps you upright (Premier Spine & Sports Medicine, n.d.).
Movement & shock absorption: Curves, discs, and joints allow for safe bending and twisting, enabling you to lift, reach, and play (Raleigh Orthopaedics, 2024).
Nerve protection: The spinal column shields the spinal cord and nerve roots, so signals move clearly. Irritation can cause pain, tingling, or weakness (Cary Orthopaedics, 2023).
Quality of life: Ongoing spine issues can lead to fatigue, poor sleep, headaches, and reduced participation in work or sports (Raleigh Orthopaedics, 2024).
Common problems we see—and why early action helps
Strains/sprains and facet irritation from long sitting, poor lifting form, or sudden loads
Disc problems that can press on nearby nerves and create radiating symptoms
Spinal stenosis (narrowing) that pinches nerves
Degenerative changes related to age, low activity, smoking, or extra weight
Most cases respond to conservative care when initiated early, including movement, postural changes, targeted exercises, and load management (OSSWF, 2024).
Red flags—don’t wait: radiating pain, numbness, weakness, headaches, or loss of function. Seek a prompt exam (Cary Orthopaedics, 2023; Suarez Physical Therapy, n.d.).
An El Paso Back Clinic–style plan: simple steps that fit your day
1) Movement you can keep
20–30 minutes of low-impact cardio most days (e.g., walking, cycling, swimming).
Core & hip strength 2–3 days/week: planks, side planks, glute bridges, and bird-dogs.
Mobility after warm-ups: thoracic open-books, hip-flexor, and hamstring stretches (National Spine Health Foundation, 2024; Mobility Project PT, 2024).
2) Posture that holds up at work and home
Sit: feet flat, hips back in the chair, lumbar support, screen at eye level.
Stand: weight balanced, knees soft, ears over shoulders.
Micro-breaks: move every 30–45 minutes (National Spine Health Foundation, 2024).
3) Ergonomics you actually feel
The chair is high enough so the hips are level with or slightly above the knees.
Keyboard and mouse close; forearms supported; shoulders relaxed.
Lift with a hip hinge, keep the load close, and exhale as you stand.
4) Sleep & stress recovery
Neutral neck/back with a supportive mattress and the right pillow height.
Side sleepers: pillow between knees. Back sleepers: pillow under knees.
Use breathing drills, short walks, and stretch breaks to lower tension (Raleigh Orthopaedics, 2024).
5) Hydration & healthy weight
Steady water intake supports disc hydration and tissue recovery (Centeno-Schultz Clinic, n.d.).
A healthy body weight lowers compressive load on joints and discs (Raleigh Orthopaedics, 2024).
Nutrition for a stronger spine (simple and local-friendly)
Protein for muscle and connective-tissue repair
Omega-3s (salmon, trout, walnuts) to help regulate inflammation
Calcium & vitamin D for bone strength
Magnesium for nerve and muscle function
Colorful fruits/vegetables for antioxidants that support recovery
Water for disc hydration and nutrient transport These habits reduce inflammation and support healing (Watkins Family Chiropractic, 2023; OSSWF, 2024).
Four-week “Borderland Back Reset” (minimal gear, steady progress)
Week 1 — Start easy
Daily: 10-minute walk + 5 minutes mobility (open-books, hip-flexor, hamstrings).
Core set (3x/week): plank 20 s, side plank 15 s/side, glute bridge 10 reps.
Posture: Raise the screen and add a small lumbar roll.
Week 2 — Build consistency
Daily: 15–20 minutes walk/cycle + mobility.
Core set (3x/week): plank 25–30 s, side plank 20 s/side, bridge 12 reps; add bird-dog 6/side.
Nutrition: add one serving of leafy greens and one serving of lean protein to each meal (Watkins Family Chiropractic, 2023).
Week 3 — Strength + recovery
Cardio most days: 20–25 minutes.
Light hinge pattern (backpack or kettlebell) 1–2 days/week; focus on form.
Before bed, do slow breathing for 5 minutes.
Week 4 — Re-test & adjust
Compare flexibility, pain, and energy levels with those of Week 1.
Keep what helps; trim what doesn’t.
If numbness, weakness, or radiating pain persists, book an exam (Cary Orthopaedics, 2023; Suarez Physical Therapy, n.d.).
Real-world injuries: work, sports, and motor-vehicle accidents (MVAs)
Work: Desk roles need posture breaks and lumbar support; physical jobs need task rotation, hip-hinge training, and planned recovery.
Sports: Combine mobility, core/hip strength, and gradual return to play.
MVAs: Even “minor” collisions can cause whiplash or soft-tissue injury. A stepwise evaluation, along with imaging when necessary, guides safe return and documentation (OSSWF, 2024).
Inside our integrative approach in El Paso
(Clinical observations from Dr. Alexander Jimenez, DC, APRN, FNP-BC, Nurse Practitioner and Chiropractor)
Dual-scope diagnosis: We blend chiropractic and medical perspectives. Your exam includes a detailed history, movement, and neurological screens, as well as, when necessary, advanced imaging to clarify the problem and rule out potential red flags (Jimenez, n.d.; see Imaging/Diagnostics and Personal-Injury topics).
Evidence-based conservative care:
Chiropractic adjustments to restore motion and reduce joint irritation
Therapeutic exercise to build core/hip strength and mobility
Manual therapy/massage for tight or sensitive tissues
Acupuncture as part of an integrative plan when appropriate
Lifestyle coaching on posture, lifting, sleep, and stress (Prestige Health & Wellness, n.d.; Mobility Project PT, 2024; Raleigh Orthopaedics, 2024)
Documentation & advocacy: For work, sports, personal, and MVA cases, we document the mechanism of injury, exam findings, functional limits, and response to care. When claims or legal issues arise, clear records and appropriate imaging support decision-making (Jimenez, n.d.; Rangeline Chiropractic, n.d.).
Myths vs. facts (short and clear)
Myth: “If my back hurts, I should rest all day.” Fact: Gentle movement and short walks often speed recovery; long bed rest adds stiffness (National Spine Health Foundation, 2024).
Myth: “Only heavy lifting causes back pain.” Fact: Prolonged sitting, poor ergonomics, stress, and sleep problems also drive pain (National Spine Health Foundation, 2024; Raleigh Orthopaedics, 2024).
The El Paso Back Clinic checklist
☐ Break up sitting every 30–45 minutes
☐ Screen at eye level; use lumbar support
☐ 10–15 minutes daily core + mobility
☐ 20–30 minutes low-impact cardio most days
☐ Hydrate across the day
☐ Build meals around protein + produce + healthy fats
☐ Sleep with neutral neck/back alignment
☐ Seek care quickly for red flags or lasting symptoms
Weekend Athletes Injury Solutions: A Simple, Evidence-Based Guide for Safer Play and Faster Recovery
A handsome, muscular man in sportswear is stretching his muscles in a sunny park.
Who this is for: adults who sit most of the week and then go hard on the weekend (a.k.a. “weekend warriors”). What you’ll get: clear reasons these injuries happen, what to do first, how to prevent them, and how integrative chiropractic care—like the approach used in El Paso—helps you recover and return to activity safely.
Weekend warriors 101
A weekend warrior is someone who does most of their intense activity on one or two days after a mostly sedentary week. That pattern can still deliver strong health benefits if you meet weekly exercise targets, but the sudden spike in effort raises the risk of sprains, strains, and overuse problems—especially when you skip warm-ups or jump in too fast (Riverside Health System, 2025; Weill Cornell Medicine, 2024). (riversideonline.com)
Large studies show that “condensed” exercisers can gain health benefits similar to those who spread workouts throughout the week—as long as the total weekly minutes reach the recommended amounts. The catch: your muscles, tendons, and joints still need gradual loading to stay injury-resistant (American Heart Association News, 2024; Shiroma et al., 2019). (www.heart.org)
Why weekend athletes get hurt
Most weekend injuries come down to three drivers:
Overuse: repeating motions your tissues aren’t ready for (long runs, repetitive swings).
Sudden movement: fast cuts, awkward landings, or twisting under load.
Poor preparation: no warm-up, weak stabilizers, and worn-out shoes.
These factors underlie many musculoskeletal problems seen by orthopedic and emergency clinicians (Aligned Orthopedic Partners, 2024; Weill Cornell Medicine, 2024). (Aligned Orthopedic Partners)
What typically gets injured (and what it feels like)
Emergency physicians most often treat injuries to the knees, shoulders, and ankles, with sprains and strains outnumbering fractures (Weill Cornell Medicine, 2024). (weillcornell.org)
Ankle sprain (ligament): twist/roll, swelling, tenderness, sometimes bruising.
Knee sprain/overuse pain: instability, joint-line pain, and pain after cutting or pivoting.
Achilles tendinopathy: stiff, sore area above the heel (often worse in the morning).
Rotator cuff irritation: pain with overhead reach or lying on the shoulder.
Shin splints: aching along the shin after running on hard surfaces (Riverside Health System, 2025). (riversideonline.com)
Sprain vs. strain (plain words): Sprain = ligament (joint stabilizer). Strain = muscle or tendon (mover). Sprains can feel unstable and bruise; strains feel like a pull with spasm or weakness (Aligned Orthopedic Partners, 2024). (Aligned Orthopedic Partners)
Your job habits shape your weekend risk
Repetitive tasks and long sitting can irritate tissues before you ever play. Those weekday loads stack with Saturday’s game and can tip you into pain. Tendinitis, for example, often develops from repeated motions (MyShortlister, 2023). Short micro-breaks, posture changes, and light mid-week movement help. (Shortlister)
First aid: what to do in the first 24–72 hours
For many fresh soft-tissue injuries, start with the PRICE method: Protect, Rest, Ice (20 minutes on), Compress, Elevate. Don’t push through sharp pain. Seek urgent care for a “pop,” severe swelling, numbness/weakness, deformity, or inability to bear weight (Weill Cornell Medicine, 2024). (weillcornell.org)
When imaging is useful (and what usually comes first)
You don’t need an MRI for every sprain. Clinicians begin with a history and examination; an X-ray is often the first test if a fracture is suspected. Musculoskeletal ultrasound or MRI follows when soft-tissue damage is suspected, symptoms persist, or nerve signs appear (Weill Cornell Medicine, 2024). (weillcornell.org)
In work, sport, or motor-vehicle accident (MVA) cases, advanced imaging also supports clear medical-legal documentation—a key part of comprehensive injury care (El Paso Back Clinic; Dr. Jimenez). (elpasobackclinic.com)
Practical prevention that actually works
Warm up and cool down. Do 5–10 minutes of light cardio and dynamic moves (leg swings, lunges, and arm circles). Ease into slow stretches after play (Riverside Health System, 2025; Appleton Chiropractic Center, n.d.). (riversideonline.com)
Build up gradually. Increase time or intensity by ~10% per week. Rotate high- and low-impact days (Center for Orthopedic Surgery & Sports Medicine, n.d.). (COSM)
Use the right gear. Replace worn shoes; match footwear to your sport (Riverside Health System, 2025). (riversideonline.com)
Hydrate, fuel, and sleep. Under-fueling and short sleep increase the risk of cramps and strains (Riverside Health System, 2025). (riversideonline.com)
Add two short mid-week sessions. Even 20–30 minutes of exercise twice a week improves tissue tolerance and reduces the risk of weekend injuries (Mayo Clinic Sports Medicine, n.d.). (sportsmedicine.mayoclinic.org)
Simple self-care roadmaps
Ankle sprain
Days 0–2: PRICE, gentle ankle pumps, compression sleeve.
Days 3–7: pain-free range of motion; start weight bearing as tolerated.
Weeks 2–4: add balance drills and band work.
See a clinician if you can’t bear weight or feel instability (Weill Cornell Medicine, 2024). (weillcornell.org)
Achilles tendinopathy
Reduce jumping/sprinting while painful.
Begin slow calf raises (progress to eccentrics); increase load gradually (Aligned Orthopedic Partners, 2024). (Aligned Orthopedic Partners)
Shoulder soreness (rotator cuff pattern)
Short rest (not total rest), then scapular control and light external-rotation drills; limit overhead volume and improve thoracic mobility (Aligned Orthopedic Partners, 2024). (Aligned Orthopedic Partners)
Low-back strain
After 24–48 hours, try gentle mobility exercises (such as pelvic tilts and cat-camel), followed by core endurance exercises (like planks) and hip-hinge practice. If pain persists or travels below the knee or you notice weakness, seek evaluation (Weill Cornell Medicine, 2024). (weillcornell.org)
2 rounds: push-ups 8–12; band rows 12–15; band “T” raises 10–12
Dead bug 6/side; bird-dog 6/side
3–5 min pec stretch + thoracic rotations
Short “bridge” sessions like these raise tissue tolerance and make weekend play safer (Center for Orthopedic Surgery & Sports Medicine, n.d.). (COSM)
How integrative chiropractic care supports weekend athletes
Integrative chiropractic care blends joint-specific manual therapy with targeted exercise, soft-tissue work, and—when indicated—acupuncture, bracing/taping, and coordinated medical evaluation. The goal is to improve mechanics (how you move) and capacity (what your tissues can handle), so you heal and resist re-injury (Radiant Life Chiropractic, 2024; Aligned Orthopedic Partners, 2024). (Radiant Life Chiropractic)
At El Paso Back Clinic, this approach is paired with a dual-scope model (chiropractic plus nurse practitioner care) for sports, work, personal, and MVA injuries. The team can:
Perform focused orthopedic and neurological exams.
Order X-ray, MRI, CT, or musculoskeletal ultrasound when the exam suggests more than a simple sprain.
Coordinate medical-legal documentation (mechanism, findings, imaging, functional limits, and response to care) for injury cases.
Guide progressive rehab and return-to-play plans based on pain-free motion, strength, and sport-specific tasks (El Paso Back Clinic; Jimenez, 2025). (elpasobackclinic.com)
Local context: Recent clinic articles from El Paso highlight dual-scope evaluation, the role of advanced imaging, and clear documentation for personal-injury cases—useful if your injury involves work or an auto crash (El Paso Back Clinic). (elpasobackclinic.com)
A smarter return-to-play checklist (advance only when all are true)
Daily tasks are pain-free, and you’re sleeping normally.
Full, pain-free range of motion for the injured area.
Strength feels symmetrical from side to side in simple tests.
You can do basic sport drills (jog-cut-jog; easy swings/serves) without symptoms.
If a step hurts, back up, adjust the load, and rebuild capacity (Weill Cornell Medicine, 2024). (weillcornell.org)
Key takeaways
Weekend-only training can be beneficial—the total weekly activity level matters most—but spikes in workload increase the risk of injury (AHA News, 2024; Riverside Health System, 2025). (www.heart.org)
Most common issues include sprains, strains, and overuse injuries in the ankle, knee, and shoulder (Weill Cornell Medicine, 2024). (weillcornell.org)
Warm up, build gradually, and add two short mid-week sessions to cut risk (Riverside Health System, 2025; Center for Orthopedic Surgery & Sports Medicine, n.d.). (riversideonline.com)
Integrative chiropractic care—with exam, imaging when needed, progressive exercise, and thorough documentation—helps you recover and return to play stronger and safer (El Paso Back Clinic; Radiant Life Chiropractic, 2024). (elpasobackclinic.com)
El Paso Back Clinic®: Premier Wellness Chiropractic Care in El Paso, TX
Spine problems are evident in the model. A woman is in consultation with the doctor in the clinic.
At El Paso Back Clinic®, led by Dr. Alexander Jimenez, DC, APRN, FNP-BC, we’re dedicated to transforming lives through advanced chiropractic care and integrative wellness in El Paso, TX. Specializing in recovery from motor vehicle accidents (MVAs), sports injuries, and chronic conditions such as neuropathy, our team utilizes cutting-edge neuromusculoskeletal imaging and dual-scope diagnostics to identify the root causes of injuries. From whiplash to gastrointestinal trauma, we craft personalized plans blending spinal adjustments, nutrition, and therapies like acupuncture to restore mobility and vitality. With a focus on holistic healing and legal support for injury claims, we empower El Pasoans to live pain-free and thrive.
Personal Injuries and Their Impact in El Paso
Living in El Paso’s bustling community means navigating busy roads and an active lifestyle, where accidents—from car crashes to sports mishaps—can disrupt one’s health. MVAs, common on rainy I-10 days, often cause spinal misalignments, leading to sciatica or numbness (Jimenez, 2025a). Sports injuries, like joint strains and workplace falls, add to the toll, risking chronic issues like neuropathy if untreated (Mana.md, n.d.).
At El Paso Back Clinic®, Dr. Jimenez’s chiropractic expertise targets these musculoskeletal and nerve disruptions. Using advanced imaging, we link injuries to symptoms, ensuring precise care. Our integrative approach, which combines adjustments with wellness coaching, helps prevent long-term pain and includes legal documentation to support insurance claims for patients in El Paso.
Nerve Pain and Neuropathy Post-Collision
Car accidents frequently trigger nerve compression, causing tingling, burning, or weakness that mimics peripheral neuropathy. Even minor collisions in El Paso’s unpredictable weather can cause vertebrae to shift, potentially pinching nerves (Jimenez, 2025b). Our clinic employs EMG and dynamic X-rays to map these injuries, correlating crash forces to nerve damage for accurate diagnosis.
We use spinal decompression and laser therapy to relieve pressure and promote healing, with patients often seeing 40-50% symptom improvement in weeks (Miami Chiropractors, n.d.). Detailed biomechanical reports strengthen personal injury claims, ensuring fair compensation for El Paso residents.
Chiropractic Care for Joint and Ligament Injuries
Injuries like ACL tears from sports or MVA dashboard impacts require targeted restoration. At El Paso Back Clinic®, we realign joints, boost circulation, and strengthen muscles to speed recovery without surgery (Jimenez, 2025c). Dr. Jimenez’s functional assessments prevent compensatory patterns, vital for El Paso’s athletes.
We integrate acupuncture and custom orthotics, helping patients resume activities in six months, rather than a year. Nutritional support, like collagen-rich diets, enhances ligament repair, tailored to El Paso’s active community.
Five Musculoskeletal Challenges We Address
Accidents hit muscles and bones hard. Our chiropractic team tackles five common issues:
Neck and Back Pain: Whiplash from MVAs causes stiffness; gentle adjustments restore motion (Jimenez, 2025d).
Sciatica: Pinched nerves from disc issues ease with traction therapy.
Joint Inflammation: Post-injury arthritis responds to ultrasound and anti-inflammatory nutrition.
Sports Strains: Overuse injuries can be effectively treated through myofascial work and gait analysis.
These protocols, customized for El Pasoans, cut recurrence by half, blending wellness education for lasting health.
Spinal Misalignment: Recovery After Crashes
El Paso’s slick roads amplify MVA risks, often misaligning spines and compressing discs, leading to radiating pain (Jimenez, 2025a). We utilize high-velocity adjustments and flexion-distraction techniques to realign the vertebrae, paired with massage to relax the muscles.
Dr. Jimenez’s imaging links crash dynamics to disc damage, guiding non-surgical plans that preserve mobility in 70% of cases (Knecht Chiropractic, n.d.). Legal reports detail injury causation, supporting the claims of El Paso patients.
Reducing Inflammation for Pain Relief
Inflammation fuels post-injury pain. Our chiropractic care enhances lymphatic drainage via soft-tissue therapy and cryotherapy, breaking the cycle (Jimenez, 2025e). Patients adopt home strategies, such as taking turmeric supplements, which can reduce swelling by 40% (Miami Chiropractors, n.d.).
For workers’ compensation cases, we monitor biomarkers, aligning treatments with recovery goals to help El Paso workers return to their feet.
Cyclist Recovery After Bike-MVA Collisions
Biking on El Paso’s scenic trails poses risks from urban traffic, which can lead to fractures or nerve injuries. Our integrative care includes bike-fit corrections and vestibular training for balance (Jimenez, 2025f). Cyclists return to riding in three months, supported by endurance nutrition and legal advocacy.
Massage Therapy for MVA Trauma Healing
MVAs cause soft-tissue damage, from bruises to adhesions. Massage therapy, paired with adjustments, boosts circulation and endorphins, reducing whiplash recovery time by 30% (Jimenez, 2025). We progress from gentle strokes to deep tissue, documenting for El Paso insurance claims.
Spinal Trauma from 18-Wheeler Accidents
Semi-truck crashes deliver intense force, fracturing vertebrae or tearing ligaments. We use dynamic imaging to assess damage, guiding bracing and neuromodulation (Jimenez, 2025h). Legal reports link crash mechanics to injuries, aiding settlements for El Paso patients.
Nutrition for Tissue Repair Post-MVA
Injured tissues require nutrients such as protein and antioxidants. Dr. Jimenez designs diets with salmon and berries, using genetic insights to optimize healing (Jimenez, 2025i). This reduces fibrosis, strengthening tissues for El Paso’s active residents.
Durable Medical Equipment for Recovery
Following a motor vehicle accident (MVA), tools such as TENS units or cervical collars can support healing. We select evidence-based equipment, such as ergonomic chairs, to offload spines (Jimenez, 2025). Tele-rehab ensures compliance, with invoices bolstering El Paso claims.
Comprehensive Musculoskeletal Recovery
MVAs strain muscles and joints, from sprains to dislocations. Our pain mapping and multi-modal care—adjustments, PT, mindfulness—restore 80% function in six weeks (Jimenez, 2025k). Legal narratives ensure fair compensation.
Whiplash-Associated Disorders (WAD) Recovery
WAD from crashes causes neck pain or dizziness. We use Doppler ultrasound for vascular checks and treat with mobilization for 90% relief (Jimenez, 2025). Immediate post-accident icing and evaluations ensure thorough El Paso claims.
Gastrointestinal Injuries from MVAs
Car accidents can disrupt digestion, causing nausea or organ strain. Our integrative care, which includes visceral manipulation and nutrition, restores gut health, backed by legal support for claims (Jimenez, 2025).
Why Choose El Paso Back Clinic®?
Our team, led by Dr. Jimenez, combines chiropractic precision with medical expertise, utilizing tools such as digital motion X-rays. We offer acute-to-chronic care, transparent billing, and testimony for legal cases. Patients reduce their reliance on medication, regaining vitality through holistic plans tailored for El Paso’s vibrant community.
Sciatica Relief for Teachers: El Paso Back Clinic’s Chiropractic Solutions
A teacher helping an elementary school girl using a tablet computer
Introduction: Supporting Teachers’ Health in El Paso
Teaching is a rewarding yet demanding profession, especially in vibrant communities like El Paso, Texas. Teachers spend long hours standing, sitting, and moving in ways that strain their bodies. These daily tasks can lead to sciatica, a painful condition caused by irritation of the sciatic nerve, which runs from the lower back down the legs. Symptoms like sharp leg pain, numbness, or tingling can disrupt lesson plans and classroom energy.
At El Paso Back Clinic®, led by Dr. Alexander Jimenez, DC, APRN, FNP-BC, we understand the unique challenges educators face. Prolonged sitting during grading, standing for lessons, poor posture over desks, and the physical demands of managing classrooms increase sciatica risks. Our clinic specializes in chiropractic care, integrative medicine, and functional rehabilitation to help teachers manage pain and prevent flare-ups. Using manual adjustments, ergonomic advice, and targeted exercises, we aim to restore spinal health and enhance quality of life.
This article examines why teachers are prone to sciatica, how our clinic’s chiropractic and integrative approaches can provide relief, and offers practical steps for achieving lasting wellness. Drawing on Dr. Jimenez’s 30+ years of expertise, we’ll share clinical insights and real-world solutions tailored for El Paso’s educators.
What Is Sciatica and Why Does It Affect Teachers?
Sciatica occurs when the sciatic nerve, the body’s longest nerve, becomes compressed or irritated. This nerve starts in the lower spine, travels through the hips, and extends down each leg. Common symptoms include burning pain, tingling, or weakness in one leg, often worsening with sitting or standing. For teachers, this can mean discomfort during classes or while grading at home.
The teaching environment in El Paso schools, from bustling elementary classrooms to high school lecture halls, creates perfect conditions for sciatica. Standing for long periods during lessons or playground duty fatigues back muscles, pressing on spinal discs (Bomberg Chiropractic, 2023). Sitting at desks or in cramped staff rooms can shorten hip muscles, tilt the pelvis, and pinch the nerve (East Bay Chiropractic Office, 2023). Poor posture, like slouching over lesson plans, further irritates the nerve roots (Scoliosis Center of Utah, n.d.).
Dr. Jimenez sees this often at El Paso Back Clinic. His advanced neuromusculoskeletal imaging, such as X-rays and MRIs, pinpoints disc bulges or muscle imbalances that cause sciatica in teachers. By addressing these root causes, our clinic helps educators stay active without pain.
How Teachers’ Daily Routines Trigger Sciatica
Teachers’ days are a mix of physical and mental demands. Standing to deliver lessons or monitor halls strains the lower back, increasing nerve pressure (Boyne Ergonomics, n.d.). Sitting for hours on outdated chairs compresses the spinal discs, a key factor in triggering sciatica (Bomberg Chiropractic, 2023). Bending to assist students or lifting heavy teaching materials—such as projectors or book boxes—can strain the piriformis muscle, which is located near the sciatic nerve.
Poor posture is a major culprit. Leaning over desks or hunching at computers curves the spine unnaturally, squeezing nerve roots (Scoliosis Center of Utah, n.d.). Stress from managing classrooms or meeting tight deadlines can cause muscle tension, leading to inflammation (Paragon Chiropractic, n.d.). In El Paso, where teachers often juggle bilingual classes and extracurricular duties, these risks accumulate.
Dr. Jimenez’s clinic frequently treats educators with sciatica from these habits. His dual-scope approach—combining chiropractic exams with diagnostic imaging—reveals how daily tasks, such as carrying heavy bags, can lead to spinal misalignment. Our tailored treatments at El Paso Back Clinic, including adjustments and massage, address these issues directly, helping teachers move freely.
The Impact of Prolonged Sitting and Standing
Teachers switch between sitting and standing constantly—standing for morning assemblies, sitting for parent-teacher meetings, then standing again for labs. Prolonged sitting, especially on hard classroom chairs, increases disc pressure by up to 30%, irritating the sciatic nerve (Bomberg Chiropractic, 2023). Standing too long without breaks tightens hip flexors, pulling the spine out of alignment (Boyne Ergonomics, n.d.).
This back-and-forth strains stabilizing muscles, risking micro-tears in discs that pinch nerves. In El Paso’s active school settings, teachers may stand for over four hours daily, increasing the odds of back pain by 50% (Abundant Life Chiropractor, 2023). At El Paso Back Clinic, Dr. Jimenez utilizes advanced imaging to identify these strains, which are often seen in teachers following minor classroom injuries or slips. Our spinal decompression therapy gently stretches the spine, relieving nerve pressure and promoting healing.
Simple fixes can help: switch positions every 20 minutes, use cushioned mats for standing, or adjust your desk height to a comfortable level. These small changes, guided by our clinic’s ergonomic coaching, significantly reduce the risk of sciatica.
Poor Posture: A Hidden Cause of Nerve Pain
Posture shapes spinal health. Teachers often slouch over their desks or lean forward to engage students, curving their spines into a “C” shape. This compresses the lumbar vertebrae, irritating sciatic nerve roots (Scoliosis Center of Utah, n.d.). Low computer screens can cause neck craning, which can lead to lower back strain.
In El Paso classrooms, crouching to help young students or writing on low boards exacerbates this issue. Over time, uneven muscle pull misaligns the spine, trapping the nerve. At El Paso Back Clinic, Dr. Jimenez uses posture assessments to spot these habits early. His chiropractic adjustments realign the vertebrae, while acupuncture relaxes tight muscles, such as the piriformis, easing nerve pressure (Jimenez, n.d.a).
Posture tips: Keep your ears over your shoulders, use a lumbar-support chair, and raise screens to eye level. Our clinic offers workshops for El Paso teachers to build these habits, preventing chronic pain.
Physical Demands: The Active Side of Teaching
Teaching isn’t just standing or sitting—it’s dynamic. Lifting stacks of textbooks, bending to pick up dropped items, or dashing to manage recess chaos strains the back. These motions can herniate discs or inflame muscles near the sciatic nerve (East Bay Chiropractic Office, 2023). In El Paso, where teachers may handle heavy bilingual materials or sports equipment, risks grow.
Sudden twists, such as grabbing a falling projector, mimic sports injuries that Dr. Jimenez treats. His clinic documents these as work-related injuries for insurance purposes, utilizing massage and exercise to aid in tissue healing. Advanced imaging ensures an accurate diagnosis, detecting layered issues such as sprains and nerve compression (Jimenez, n.d.b).
Safe habits reduce risks: Lift with bent knees, use carts for supplies, and stretch before engaging in active duties. El Paso Back Clinic’s tailored plans help teachers stay strong and pain-free.
Chiropractic Care at El Paso Back Clinic: Targeted Relief
Chiropractic care is a cornerstone for sciatica relief. At El Paso Back Clinic, our manual adjustments realign the spine, reducing nerve irritation and inflammation (Active Health Center, n.d.). Teachers notice less leg pain and better mobility after sessions. Our spinal decompression therapy gently stretches the spine, retracting bulging discs that pinch nerves (Bomberg Chiropractic, 2023).
Dr. Jimenez’s expertise shines here. With over 30 years of experience treating patients in El Paso, including educators, Dr. [Last Name] combines chiropractic care with integrative methods, such as acupuncture, to provide natural pain relief. Advanced imaging ensures precise adjustments, targeting the exact cause of sciatica (Jimenez, n.d.a). Regular visits prevent flare-ups, letting teachers focus on students, not pain.
Restoring Spinal Alignment and Nerve Function
Adjustments are quick, targeted thrusts that realign vertebrae, freeing the sciatic nerve. This boosts blood flow and reduces inflammation, key for teachers battling daily strain (AFC Adherence, n.d.). At our clinic, Dr. Jimenez pairs adjustments with soft tissue work to release tight hips, a common issue among educators.
Our approach restores function holistically. Teachers regain flexibility for classroom tasks, and consistent care prevents future issues. Jimenez’s diagnostic tools, such as MRIs, ensure that treatments match each patient’s needs, offering El Paso educators reliable relief (Jimenez, n.d.b).
Reducing Inflammation Naturally
Inflammation fuels sciatica pain and swelling of the tissues around the nerve. Our adjustments improve spinal motion, reducing this swelling (Active Health Center, n.d.). We add ice or heat therapy to speed relief, tailored to each teacher’s symptoms.
Dr. Jimenez enhances this approach with nutrigenomics, recommending anti-inflammatory foods, such as salmon, to support the healing process. For El Paso teachers, this integrative approach means less pain and faster recovery from classroom strains (Jimenez, n.d.a).
Lifestyle Changes: Ergonomics and Exercises for Teachers
El Paso Back Clinic goes beyond adjustments, offering practical advice. Ergonomic tips include adjustable chairs, footrests, and raised monitors to reduce strain (Boyne Ergonomics, n.d.). For teachers, we recommend lumbar pillows and standing desks for grading.
Exercises are key: planks strengthen the core, and piriformis stretches loosen the hips (Alliance Orthopedics, n.d.). Dr. Jimenez designs home routines, such as knee-to-chest stretches, to accommodate busy schedules. Our massage therapy supports recovery, ensuring El Paso educators stay active.
Preventing Flare-Ups: Daily Habits for Long-Term Relief
Preventing sciatica means tracking triggers. Long sits or heavy lifts? Take breaks or use carts. Heat eases tight muscles; cold calms acute pain (Abundant Life Chiropractor, 2023). Weekly core workouts and posture apps help maintain proper alignment.
Dr. Jimenez’s clinic emphasizes prevention. Our exercise plans, paired with stress-reducing yoga, help teachers avoid chronic issues. Legal documentation supports work-injury claims, ensuring access to care (Jimenez, n.d.b).
Integrative Care: A Team Approach at El Paso Back Clinic
We combine chiropractic care with physical therapy, acupuncture, and massage to facilitate a comprehensive recovery. Physical therapy builds strength with moves like bridges (Active Health Center, n.d.). Acupuncture calms the nerves, making it ideal for reducing teachers’ stress (Jimenez, n.d.a). Short movement breaks, such as stretching during class, boost circulation.
Our clinic’s integrative model, led by Dr. Jimenez, treats sciatica holistically, addressing work or personal injuries with detailed records for insurance.
Dr. Alexander Jimenez’s Expertise: A Beacon for El Paso Teachers
Dr. Jimenez, with dual credentials as a chiropractor and nurse practitioner, brings unmatched care to El Paso. His clinic treats sciatica from classroom strains, sports injuries, or accidents, using imaging to diagnose precisely. Treatments such as adjustments, massage, and tailored exercises can help the body heal naturally, thereby preventing long-term issues.
For teachers, Jimenez’s legal documentation supports work claims, ensuring coverage. His functional medicine approach, including nutrition and acupuncture, empowers educators to thrive (Jimenez, n.d.a; Jimenez, n.d.b).
Practical Tips for El Paso Teachers
Morning Stretch: Try cat-cow (10 reps) to loosen the spine.
Classroom Ergonomics: Use lumbar-support chairs; raise boards to waist height.
Breaks: March in place every 30 minutes to ease nerve pressure.
Nutrition: Eat berries and fish to combat inflammation, according to Jimenez’s advice.
Conclusion: Empowering El Paso Educators
Sciatica doesn’t have to slow down El Paso’s teachers. At El Paso Back Clinic, Dr. Jimenez and our team offer chiropractic care, integrative therapies, and practical tips to relieve pain and prevent issues. From adjustments to ergonomic tweaks, we help educators stay healthy and focused on inspiring students.
Visit us at 11860 Vista Del Sol Dr, Suite 128, El Paso, TX, or call 915-850-0900 to start your pain-free journey.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine