Can the effects of electroacupuncture reduce sciatica in individuals dealing with low back pain to restore their mobility?
Introduction
When many people start to overuse their muscles in the lower quadrants, it can lead to numerous issues that cause pain and discomfort. One of the most common pain issues in the lower quadrants of the musculoskeletal system is sciatica, which is associated with low back pain. This pain duo can affect a person’s daily routine and lead them to pain and discomfort. This musculoskeletal condition is common, and when it affects one of the legs and lower back, many people state that it’s a radiating shooting pain that doesn’t go away for a while. Luckily, there are treatments like electroacupuncture to reduce sciatica associated with low back pain. Today’s article looks at the sciatica-low-back connection, how electroacupuncture reduces this pain connection, and how electroacupuncture can restore mobility to the individual. We talk with certified medical providers who consolidate our patients’ information to assess how to reduce the sciatica-low-back connection with electroacupuncture. We also inform and guide patients on how electroacupuncture therapy can be combined with other therapies to restore mobility to the body. We encourage our patients to ask their associated medical providers intricate and important questions about incorporating electroacupuncture therapy as part of their routine to reduce sciatica associated with low back pain. Dr. Jimenez, D.C., includes this information as an academic service. Disclaimer.
The Sciatica & Low Back Connection
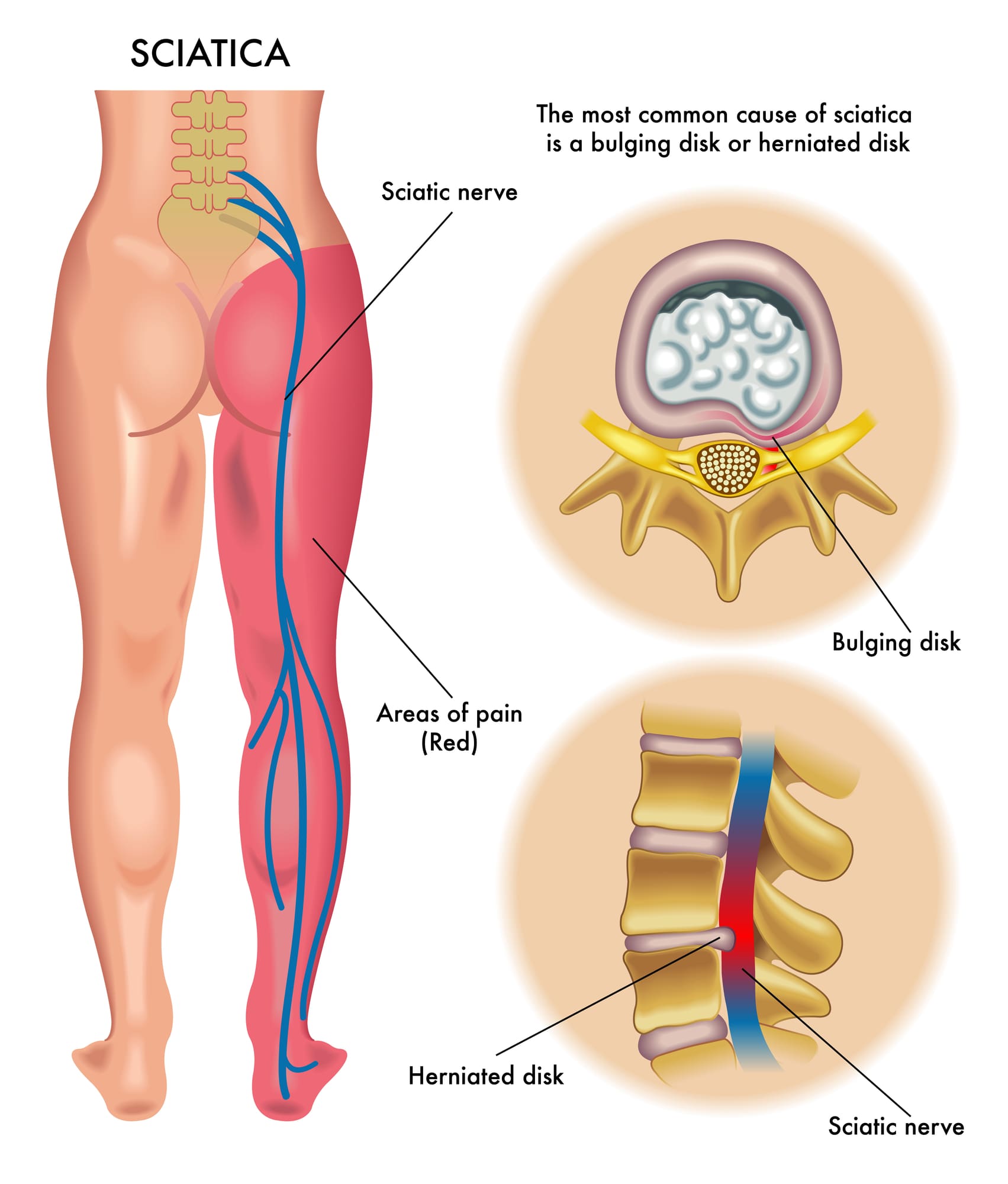
Do you feel muscle aches or pain in your lower back or your legs? Do you experience radiating, throbbing pain in your legs that affects your walking ability? Or have you noticed that your legs and lower back ache more when carrying a heavy object? Many of these scenarios are associated with sciatica, which correlates with lower back pain. Now, sciatica is often characterized by aggravating pain traveling along the sciatic nerve from the lower back region, impairing a person’s quality of life. In the musculoskeletal system, the sciatic nerve plays an important role by providing motor function to the legs. (Davis et al., 2024) Now, when the sciatic nerve, the lumbar region also has a pivotal role. The lumbar region in the musculoskeletal region also has a crucial role in providing support, strength, and flexibility to the body. However, both the sciatic nerve and lumbar spinal region are more prone to stress and injuries from traumatic injuries and environmental factors that can impact the lumbar spinal discs and the sciatic nerve.
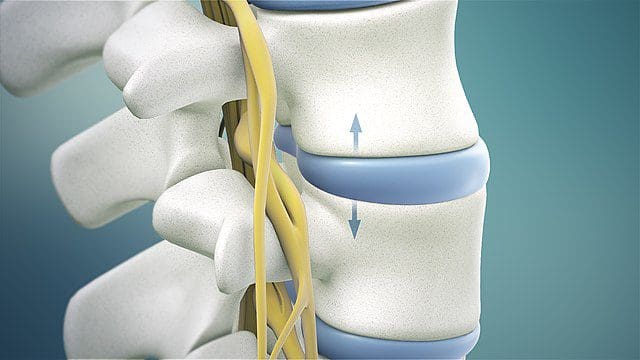
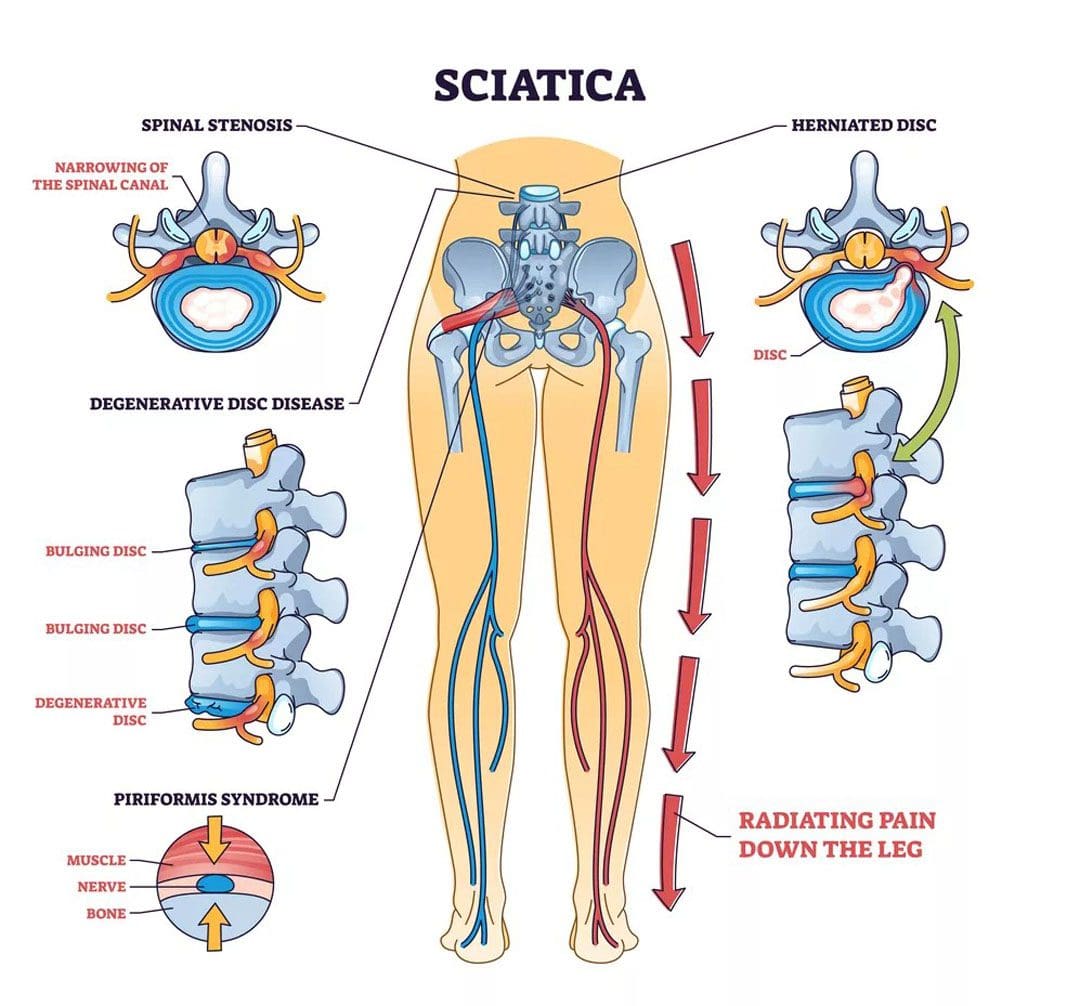
Repetitive motions, obesity, improper lifting, degenerative spinal issues, and musculoskeletal conditions are a few causes and risk factors contributing to the development of sciatica associated with the lower back. What eventually happens is that the water content and the progressive loss of the proteoglycans of the spinal discs break down between the vertebrae and protrude out to press on the sciatic nerve, which then can become irritated and cause referred radiating pain in the legs and lower back. (Zhou et al., 2021) The combination of sciatica and lower back pain can become a socio-economic issue depending on the severity of the pain that the sciatic nerve is causing and can make individuals miss out on any activities they are participating in. (Siddiq et al., 2020) While sciatica pain-like symptoms often correlate with the lumbar region, many individuals can find the relief they are looking for through various treatments.
Sciatica Causes- Video
Electroacupuncture Reducing The Sciatica-Low Back Connection
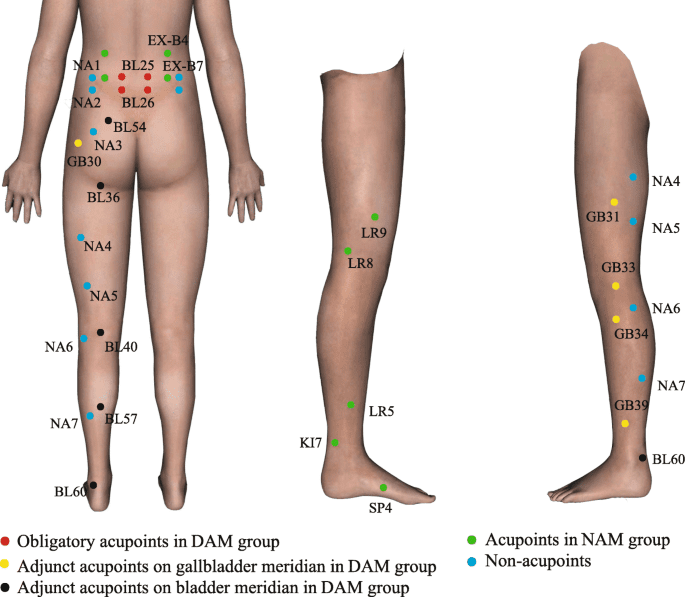
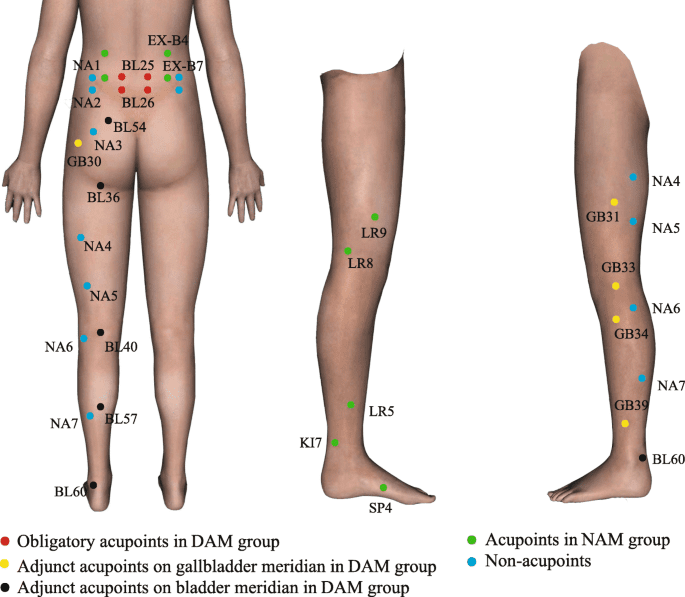
When it comes to reducing the sciatic-low-back connection, many individuals seek out treatment that is affordable and effective in decreasing pain-like issues. Non-surgical treatments like electroacupuncture can be beneficial to many individuals who are experiencing sciatica pain correlated with the lower back. Electroacupuncture is another form of traditional acupuncture therapy that originates in China. Highly trained acupuncturists follow the same acupuncture principles by placing solid thin needles at different acupoints in the body to restore qui or chi (energy flow). Electroacupuncture combines needles and electrostimulation to reduce the central pain-regulatory mechanisms causing low back pain and sciatica by blocking the pain signals and providing pain relief. (Kong, 2020) At the same time, electroacupuncture offers analgesic properties to stimulate endorphins and reduce pain medication for low back pain safely. (Sung et al., 2021)
Electroacupuncture Restoring Mobility
When the lower extremities are experiencing limited mobility due to sciatica associated with low back pain, electroacupuncture can help relax the muscles that are aggravating the sciatic nerve and even help improve blood flow to the lumbar muscles. That is because electroacupuncture can stimulate specific body regions to reduce the somato-vagal-adrenal reflexes to relieve and restore mobility to the lower extremities. (Liu et al., 2021) Additionally, electroacupuncture can be combined with other non-surgical therapies to help strengthen the core and lower back muscles, allowing people to be more mindful of what factors are causing sciatica and lower back pain. By doing this, many people struggling with sciatica associated with low back pain can incorporate electroacupuncture as part of their treatment program combined with holistic approaches to improving their quality of life and providing a pathway to improving their mobility.
Kong, J. T. (2020). Electroacupuncture for Treating Chronic Low-Back Pain: Preliminary Research Results. Med Acupunct, 32(6), 396-397. https://doi.org/10.1089/acu.2020.1495
Liu, S., Wang, Z., Su, Y., Qi, L., Yang, W., Fu, M., Jing, X., Wang, Y., & Ma, Q. (2021). A neuroanatomical basis for electroacupuncture to drive the vagal-adrenal axis. Nature, 598(7882), 641-645. https://doi.org/10.1038/s41586-021-04001-4
Siddiq, M. A. B., Clegg, D., Hasan, S. A., & Rasker, J. J. (2020). Extra-spinal sciatica and sciatica mimics: a scoping review. Korean J Pain, 33(4), 305-317. https://doi.org/10.3344/kjp.2020.33.4.305
Sung, W. S., Park, J. R., Park, K., Youn, I., Yeum, H. W., Kim, S., Choi, J., Cho, Y., Hong, Y., Park, Y., Kim, E. J., & Nam, D. (2021). The effectiveness and safety of electroacupuncture for nonspecific chronic low back pain: A protocol for systematic review and/or meta-analysis. Medicine (Baltimore), 100(4), e24281. https://doi.org/10.1097/MD.0000000000024281
Zhou, J., Mi, J., Peng, Y., Han, H., & Liu, Z. (2021). Causal Associations of Obesity With the Intervertebral Degeneration, Low Back Pain, and Sciatica: A Two-Sample Mendelian Randomization Study. Front Endocrinol (Lausanne), 12, 740200. https://doi.org/10.3389/fendo.2021.740200
Can individuals with piriformis syndrome incorporate acupuncture with various therapies to reduce sciatic nerve pain and other symptoms?
Introduction
As many individuals move around from one location to another thanks to the lower body extremities, the surrounding muscles, ligaments, nerve roots, and tissues help contribute to the sensory-motor function of the hips, legs, buttocks, and feet. All these muscle groups factor in to ensure they can be mobile without the effects of pain or discomfort. However, many factors and issues can cause the surrounding muscles to develop musculoskeletal problems over time, affecting a person’s mobility. One of the muscles that helps share the responsibility for mobility to hips and buttocks is the piriformis muscle, which is often overlooked when various injuries or repetitive motions start to affect a person’s ability to walk. Today’s article examines how piriformis syndrome affects mobility, how sciatic pain correlates with piriformis syndrome, and how therapies like acupuncture can help reduce piriformis syndrome. We talk with certified medical providers who consolidate our patients’ information to provide numerous treatments to minimize piriformis syndrome affecting a person’s mobility. We also inform and guide patients on how treatments like acupuncture can help reduce sciatic nerve pain associated with piriformis syndrome. We encourage our patients to ask their associated medical providers intricated and important questions about the referred pain-like symptoms they are experiencing from piriformis syndrome that is affecting their ability to walk. Dr. Jimenez, D.C., incorporates this information as an academic service. Disclaimer.
Piriformis Syndrome Affecting Mobility
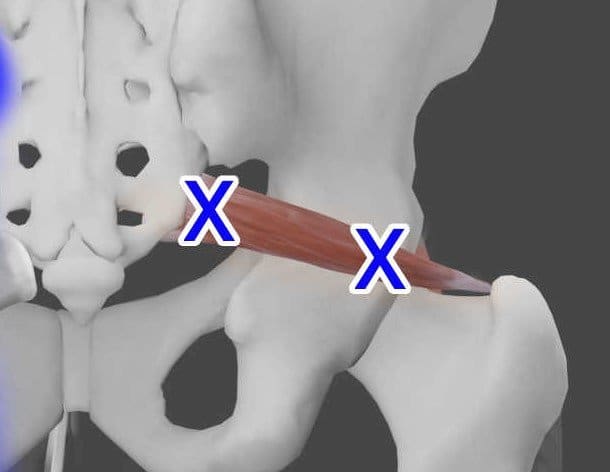
Have you been experiencing muscle tightness in your hips or buttock region, affecting your walking ability? Do you feel sensations of numbness, tingling, or burning pain traveling down to your knees and feet? Or, after a long day of work, do you feel pain when you are sitting down? Most of these symptoms are often correlated with piriformis syndrome. The six surrounding muscles surrounding the gluteal region of the thighs and hips all work together to provide lower body movement while stabilizing the hips and rotating the thighs. The piriformis muscle is a small, flat, pear-shaped muscle that runs on top of the sciatic nerve. Piriformis syndrome is a clinical musculoskeletal condition that causes sciatic nerve entrapment that causes many individuals to report shooting and burning pain down to their buttock region. (Hicks et al., 2024) This causes many people to think they are dealing with low back pain associated with sciatica. When a person is dealing with piriformis syndrome, they will experience limited mobility in their hips, which, over time, if not treated, will affect the thighs and legs.
How Does Sciatic Nerve Pain correlate with Piriformis Syndrome?
Additionally, since piriformis syndrome is correlated with sciatic nerve pain, some clinical findings causing overlapping risk profiles include restricted external hip rotation and muscle tightness of the lumbosacral muscles. Other clinical findings range from palpatory pain over the greater sciatic notch to aggravated pain in a seated position. (Sharma et al., 2023) Since sciatic nerve entrapment is correlated with piriformis syndrome, it is still regarded as the non-discogenic cause of sciatica. (Son & Lee, 2022) When that sciatic nerve gets trapped within the piriformis muscle, many people will experience numbness, tingling sensations, and similar pain patterns in the legs, just like sciatica; however, when individuals are looking for treatments to reduce the sciatic nerve pain and improve the piriformis muscle.
Acupuncture Therapy Reduces Piriformis Syndrome
When people are looking for treatments to reduce their sciatic nerve pain correlated with piriformis syndrome, they are seeking treatments that are affordable and can reduce the pain through consecutive sessions. Acupuncture therapy can help reduce the effects of piriformis syndrome. Acupuncture is a complementary and alternative therapy from China that uses solid, thin needles to be placed on the acupoints in the body. Additionally, highly trained professionals can incorporate various acupuncture methods to treat and reduce the effects of piriformis syndrome. (He et al., 2023) At the same time, when a person is being treated for piriformis syndrome, an acupuncturist uses ultrasound-guided techniques to allow accurate needle placement within the deep muscles to provide an effective treatment response. (Fusco et al., 2018) This allows the affected surrounding muscles to relax and reduce sciatic nerve pain.
Acupuncture Reducing Sciatic Nerve Pain
Since sciatic nerve pain and piriformis syndrome have overlapping risk profiles, they can also be associated with other musculoskeletal pain conditions that can affect a person’s mobility. Acupuncture can help mitigate the pain signals causing motor or sensory disturbances within the pelvic and hip regions. (Kvorning et al., 2004) Acupuncture is one of the oldest forms of non-surgical therapy that can be combined with other various therapies to help remobilize the hips and decompress the pain affecting the sciatic nerve while providing relief. (Vij et al., 2021) By incorporating acupuncture as part of a person’s health and wellness treatment plan, they will begin to gradually manage the associated symptoms and reduce the chances of piriformis syndrome from returning to cause sciatic nerve pain in the lower extremities. This allows people to be more mindful and help restore the body’s natural healing process over time.
Reclaim Your Mobility- Video
References
Fusco, P., Di Carlo, S., Scimia, P., Degan, G., Petrucci, E., & Marinangeli, F. (2018). Ultrasound-guided Dry Needling Treatment of Myofascial Trigger Points for Piriformis Syndrome Management: A Case Series. J Chiropr Med, 17(3), 198-200. https://doi.org/10.1016/j.jcm.2018.04.002
He, Y., Miao, F., Fan, Y., Zhang, F., Yang, P., Zhao, X., Wang, M., He, C., & He, J. (2023). Acupuncture Methods for Piriformis Syndrome: A Protocol for Systematic Review and Network Meta-Analysis. J Pain Res, 16, 2357-2364. https://doi.org/10.2147/JPR.S417211
Kvorning, N., Holmberg, C., Grennert, L., Aberg, A., & Akeson, J. (2004). Acupuncture relieves pelvic and low-back pain in late pregnancy. Acta Obstet Gynecol Scand, 83(3), 246-250. https://doi.org/10.1111/j.0001-6349.2004.0215.x
Sharma, S., Kaur, H., Verma, N., & Adhya, B. (2023). Looking beyond Piriformis Syndrome: Is It Really the Piriformis? Hip Pelvis, 35(1), 1-5. https://doi.org/10.5371/hp.2023.35.1.1
Son, B. C., & Lee, C. (2022). Piriformis Syndrome (Sciatic Nerve Entrapment) Associated With Type C Sciatic Nerve Variation: A Report of Two Cases and Literature Review. Korean J Neurotrauma, 18(2), 434-443. https://doi.org/10.13004/kjnt.2022.18.e29
Vij, N., Kiernan, H., Bisht, R., Singleton, I., Cornett, E. M., Kaye, A. D., Imani, F., Varrassi, G., Pourbahri, M., Viswanath, O., & Urits, I. (2021). Surgical and Non-surgical Treatment Options for Piriformis Syndrome: A Literature Review. Anesth Pain Med, 11(1), e112825. https://doi.org/10.5812/aapm.112825
Can individuals dealing with sciatica pain find the relief they need from acupuncture to restore low back mobility?
Introduction
The body’s lower extremities provide stability and movement to the individual as they are moving from one location to another without pain or discomfort. The lower extremities consist of the hips, lower back, legs, thighs, pelvis, knees, and feet; each has various muscles, nerve roots, and ligaments with a specific job to each muscle quadrant. The spinal column in the musculoskeletal system helps provide proper posture while protecting the spinal cord from injuries. However, more often than not, the lower extremities can succumb to injuries as many individuals incorporate repetitive motions that can compress the nerve roots that are spread out to the lower extremities, which can invoke pain. The most common pain that seems to affect the lower back and legs is sciatica, and when not treated, it can cause overlapping risk profiles to the lower extremities. Today’s article examines how sciatica is correlated with the lower back and how non-surgical treatments can help reduce the effects of sciatic pain. We talk with certified medical providers who consolidate our patients’ information to provide numerous treatments to relieve sciatica pain affecting their lower extremities. We also inform and guide patients on how non-surgical treatments can help reduce sciatica pain from the lower musculoskeletal extremities. We encourage our patients to ask their associated medical providers intricated and important questions about the pain-like symptoms they are experiencing from sciatica that are causing them pain. Dr. Jimenez, D.C., incorporates this information as an academic service. Disclaimer.
How Does Sciatica Correlate With The Lower Back?
Do you often experience numb or tingling sensations running down your leg that cause your leg or foot to lose sensation briefly? Do you feel shooting pain in your lower back after excessive sitting at your desk? Or do you find that stretching your legs or back temporarily relieves the pain, only for it to come back? Many individual who are experiencing shooting pain running down their legs are dealing with sciatica. When it comes to the lower extremities in the musculoskeletal system, many individuals make repetitive motions on their spine that can cause the spinal discs to become compressed and herniated under pressure. When the spinal disc is herniated in the lumbar spine, that disc will start to press on the surrounding nerve roots, thus sending radiating pain down the legs. Sciatica is defined as when individuals are experiencing pain coming from the lumbosacral nerve root and causing either a burning, heaviness, or tightness sensation. (Aguilar-Shea et al., 2022) Sciatica can range from mild to severe, forcing many individuals to think their foot is asleep. However, the sciatic nerve root is compressed, trapped, stuck, or pinched, which causes muscle spasms within the lower back, buttock, or legs. Hence, many individuals will explain that they are experiencing low back or leg pain when it is sciatica.
Since the sciatic nerve is a long, thick nerve in the human body, it travels from the lumbar region down to the knee and connects to other nerves to reach the foot. Sciatica pain can be two conditions with the same pain-like symptom effects known as true or sciatica-like conditions. True sciatica is where an injury is directly affecting the sciatic nerve. This can relate to a slipped disc caused by environmental factors like lifting a heavy object, aggravating the sciatic nerve root, and causing pain that worsens. (Siddiq et al., 2020) For sciatica-like conditions, this is where other musculoskeletal conditions are causing sciatic pain-like symptoms on the lower extremities. Musculoskeletal conditions like piriformis syndrome can cause sciatica pain-like symptoms where the piriformis muscle is irritated or inflamed, pressing on the sciatic nerve, which causes many people to report pain along the gluteal region that may shoot a burning, aching sensations down the back of the legs. (Hicks et al., 2024) However, there are ways to treat sciatica and reduce the pain-like effects causing mobility issues.
Sciatica, Causes, Symptoms and Tips- Video
Non-surgical Treatments For Sciatica
When it comes to reducing sciatica pain, many individuals will seek out treatment that is cost-effective and customized to the person’s pain. Some treatments, like neural mobilization, can apply mechanical forces to the nerve roots to restore healthy movement to the legs and lower extremities. (Peacock et al., 2023) Other treatments, like spinal decompression, use gentle traction on the spinal disc to lay off the pressure on the sciatic nerve to provide relief. Non-surgical treatments are favorable to many people due to how affordable it is and personalized to the person’s pain as they help reduce pain and disability. (Liu et al., 2023) Luckily, a form of non-surgical treatment can help relieve sciatica and its associated pain-like symptoms.
Acupuncture Relieving Sciatic Pain
Acupuncture is one of the oldest forms of non-surgical treatments in which trained professionals use thin, solid needles to be inserted and placed on the affected area, causing pain. Acupuncture can help reduce the distortion of the affected nerve roots, and local inflammatory cytokines correlated with sciatica. (Yu et al., 2021) What this does is that it normalizes the neuron signals to a default mode from aggravating the surrounding muscle fibers and descending the pain. Additionally, acupuncture can help restore the body’s qi or energy by reducing the pain by placing the needles on the acupoint of the vital organs that share a relationship with the sciatic nerve. (Yu et al., 2022) This is known as somato-visceral, where the vital organs could be the affected area, causing overlapping muscle and nerve risk profiles. Acupuncture is an excellent form of non-surgical treatment that can be combined with other various therapies to help restore the body’s natural healing factor and allow people to be more mindful of how to take care of their bodies easily to prevent sciatica pain-like symptoms from arising.
References
Aguilar-Shea, A. L., Gallardo-Mayo, C., Sanz-Gonzalez, R., & Paredes, I. (2022). Sciatica. Management for family physicians. J Family Med Prim Care, 11(8), 4174-4179. https://doi.org/10.4103/jfmpc.jfmpc_1061_21
Liu, C., Ferreira, G. E., Abdel Shaheed, C., Chen, Q., Harris, I. A., Bailey, C. S., Peul, W. C., Koes, B., & Lin, C. C. (2023). Surgical versus non-surgical treatment for sciatica: systematic review and meta-analysis of randomised controlled trials. BMJ, 381, e070730. https://doi.org/10.1136/bmj-2022-070730
Peacock, M., Douglas, S., & Nair, P. (2023). Neural mobilization in low back and radicular pain: a systematic review. J Man Manip Ther, 31(1), 4-12. https://doi.org/10.1080/10669817.2022.2065599
Siddiq, M. A. B., Clegg, D., Hasan, S. A., & Rasker, J. J. (2020). Extra-spinal sciatica and sciatica mimics: a scoping review. Korean J Pain, 33(4), 305-317. https://doi.org/10.3344/kjp.2020.33.4.305
Yu, F. T., Liu, C. Z., Ni, G. X., Cai, G. W., Liu, Z. S., Zhou, X. Q., Ma, C. Y., Meng, X. L., Tu, J. F., Li, H. W., Yang, J. W., Yan, S. Y., Fu, H. Y., Xu, W. T., Li, J., Xiang, H. C., Sun, T. H., Zhang, B., Li, M. H., . . . Wang, L. Q. (2022). Acupuncture for chronic sciatica: protocol for a multicenter randomised controlled trial. BMJ Open, 12(5), e054566. https://doi.org/10.1136/bmjopen-2021-054566
Yu, F. T., Ni, G. X., Cai, G. W., Wan, W. J., Zhou, X. Q., Meng, X. L., Li, J. L., Tu, J. F., Wang, L. Q., Yang, J. W., Fu, H. Y., Zhang, X. C., Li, J., Wang, Y. F., Zhang, B., Zhang, X. H., Zhang, H. L., Shi, G. X., & Liu, C. Z. (2021). Efficacy of acupuncture for sciatica: study protocol for a randomized controlled pilot trial. Trials, 22(1), 34. https://doi.org/10.1186/s13063-020-04961-4
Can individuals dealing with hip pain, find the relief they are looking for from spinal decompression to reduce their sciatica pain?
Introduction
When it comes to individuals doing everyday movements, the body can be in weird positions without pain or discomfort. Hence, people can stand or sit for prolonged periods and feel all right when doing strenuous activities. However, as the body ages, the surrounding muscles and ligaments can become weak and tight, while the spinal joints and discs start to be compressed and wear and tear. This is because many individuals make repetitive motions on their bodies that cause pain-like symptoms in the back, hips, neck, and body extremities, leading to referred pain in different body locations. When individuals are experiencing musculoskeletal pain in their bodies, it can cause overlapping risk profiles that can hinder the individual and cause them to be miserable. Additionally, when people experience musculoskeletal pain in their bodies, many will seek treatment to reduce the referred pain-like symptoms associated with the musculoskeletal pain. Today’s article will examine one type of musculoskeletal pain on the hips, how it can cause sciatica pain-like problems, and how treatments like decompression can reduce the pain-like effects of hip pain correlated with sciatica. We talk with certified medical providers who consolidate our patients’ information to provide numerous treatments to relieve hip pain associated with sciatica. We also inform and guide patients on how decompression can help reduce pain-like symptoms like sciatica and restore hip mobility. We encourage our patients to ask their associated medical providers intricated and important questions about the pain-like symptoms they are experiencing from hip pain. Dr. Jimenez, D.C., incorporates this information as an academic service. Disclaimer.
Hip Pain Associated With Sciatica
Do you often experience stiffness in your lower back and hips after sitting down for an excessive period? How about feeling radiating pain running down from your lower back to your legs? Or do you think your hip and thigh muscles become tight and weak, which is affecting your gait stability? Many individuals experiencing these pain-like issues are experiencing hip pain, and it can be an issue when it is not treated over time. Since hip pain is a common and disabling condition that is challenging to diagnose, many individuals often express localized pain in one of the three anatomic regions: the anterior, posterior, and lateral hip sections. (Wilson & Furukawa, 2014) When individuals are dealing with hip pain, they will also experience referred pain in their lower backs, which causes them to be in distress and miserable. At the same time, simple ordinary movements like sitting or standing can affect the muscles and ligaments surrounding the hips and can be damaging. This can cause hip pain to be referred from the lumbar spine and spine problems, which then cause musculoskeletal issues in the lower extremities. (Lee et al., 2018)
So, how would hip pain be associated with sciatica and causing pain in many lower extremities? The hip areas in the musculoskeletal system have numerous muscles surrounding the pelvic bone area that can become tight and weak, causing referred musculoskeletal pain from intrapelvic and gynecologic issues. (Chamberlain, 2021) This means that musculoskeletal disorders like piriformis syndromes associated with hip pain can lead to sciatica. The sciatic nerve travels down from the lumbar region and the buttocks and behind the leg. When a person is dealing with sciatica and is going to their primary doctor to get treated for the pain, their doctors will do a physical examination to see what factors are causing the pain. Some of the common findings during a physical exam were tenderness and palpation of the greater sciatic notch and the reproduction of pain along the hips. (Son & Lee, 2022) This causes associated symptoms that correlate with sciatica and hip pain, including:
Tingling/numbing sensations
Muscle tenderness
Pain while sitting or standing
Discomfort
Is Motion The Key To Healing- Video
Spinal Decompression Reducing Hip Pain
However, many individuals will find non-surgical treatments to help reduce sciatica associated with hip pain. Non-surgical treatments are customized to a person’s pain and are cost-effective while being gentle on the spine. Spinal decompression can help reduce hip pain associated with sciatica. Decompression on the spine allows gentle traction to stretch out weak muscles along the lower back and hips while the spinal discs are experiencing negative pressure. When a person is dealing with sciatica pain associated with hip pain and trying decompression for the first time, they are provided with the relief they deserve. (Crisp et al., 1955)
Additionally, many individuals who incorporate decompression for their hip pain can begin to feel its effects as it helps improve blood flow circulation back to the hips to start the natural healing process. (Hua et al., 2019) When people begin incorporating decompression for their hip pain, they can relax as they feel all their aches and pain gradually disappear as mobility and rotation are back on the lower extremities.
Crisp, E. J., Cyriax, J. H., & Christie, B. G. (1955). Discussion on the treatment of backache by traction. Proc R Soc Med, 48(10), 805-814. https://www.ncbi.nlm.nih.gov/pubmed/13266831
Hua, K. C., Yang, X. G., Feng, J. T., Wang, F., Yang, L., Zhang, H., & Hu, Y. C. (2019). The efficacy and safety of core decompression for the treatment of femoral head necrosis: a systematic review and meta-analysis. J Orthop Surg Res, 14(1), 306. https://doi.org/10.1186/s13018-019-1359-7
Lee, Y. J., Kim, S. H., Chung, S. W., Lee, Y. K., & Koo, K. H. (2018). Causes of Chronic Hip Pain Undiagnosed or Misdiagnosed by Primary Physicians in Young Adult Patients: a Retrospective Descriptive Study. J Korean Med Sci, 33(52), e339. https://doi.org/10.3346/jkms.2018.33.e339
Son, B. C., & Lee, C. (2022). Piriformis Syndrome (Sciatic Nerve Entrapment) Associated With Type C Sciatic Nerve Variation: A Report of Two Cases and Literature Review. Korean J Neurotrauma, 18(2), 434-443. https://doi.org/10.13004/kjnt.2022.18.e29
For individuals dealing with chronic sciatica, when pain and other symptoms significantly impact daily activities and the ability to walk, can a musculoskeletal healthcare provider help relieve and manage symptoms through a multidisciplinary treatment plan?
Chronic Sciatica
Sciatica is a common condition that results from compression of the sciatic nerve in the lower back or leg. Chronic sciatica occurs when symptoms last for 12 months or longer.
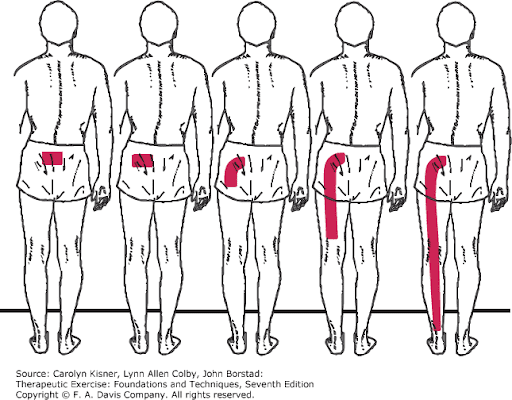
Advanced Sciatica Symptoms
Advanced or chronic sciatica usually produces pain that radiates or travels down the back of the leg. Long-term sciatic nerve compression can result in:
Leg pain
Numbness
Tingling
Electrical or burning sensations
Weakness
Weakness
Instability of the legs, which can impact the ability to walk.
Severe nerve compression can progress to leg paralysis if the nerve is significantly damaged from chronic compression. (Antonio L Aguilar-Shea, et al., 2022)
Sciatica can progress to nerve damage of the smaller nerves and travel into the legs and feet. Nerve damage/neuropathy can result in pain, tingling, and loss of sensation. (Jacob Wycher Bosma, et al., 2014)
Disabling Sciatica Treatment Options
When sciatica becomes disabling, affecting an individual’s ability to walk, more involved treatment is needed to bring relief. Many cases of chronic and disabling sciatica are caused by problems with the lumbar spine. Compression of the nerve roots that form the sciatic nerve can occur from bulging or herniated discs or spinal stenosis. If symptoms of sciatica persist beyond 12 months with little or no relief from physical therapy, non-surgical mechanical decompression, stretches and exercises, or pain management techniques, surgical procedures may be needed. (Lucy Dove, et al., 2023)
Lumbar decompression surgery encompasses several procedures to create more space in the lumbar spine and relieve nerve compression. Lumbar decompression surgery can include: (Mayfield Clinic. 2021)
Discectomy
This procedure removes a portion of a damaged disc between vertebrae to alleviate root compression from a bulging or herniated disc.
Laminectomy
This procedure removes the lamina, a portion of the vertebrae causing nerve compression, especially if there is a bone spur due to arthritic and degenerative changes in the spine.
Foraminotomy
This procedure widens the foramina, the openings in the vertebrae where the nerve roots exit to relieve compression.
Spinal Fusion
This procedure takes two or more vertebrae fusing them together with metal rods and screws for stabilization.
The procedure can be performed if:
An entire disc is removed.
Multiple laminectomies were performed.
One vertebra has slipped forward over another.
Daily Relief Management for Advanced Sciatica
Achieving relief from advanced sciatica symptoms at home can include regularly practicing methods like taking a hot bath or shower massage, and applying a heating pad to the lower back or glutes to relax tight muscles to help release the tightness surrounding the sciatic nerve.
Corrective or therapeutic exercises like sciatic nerve glides can help reduce tension along the nerve while low-back exercises that move the spine into forward or backward bending can reduce compression. (Witold Golonka, et al., 2021)
Medications like nonsteroidal anti-inflammatory drugs/NSAIDs, muscle relaxants, or nerve-pain medications may be recommended. (Antonio L Aguilar-Shea, et al., 2022)
Advanced sciatica may not be as responsive to conservative treatment methods, as the injury has set in and the nerve and surrounding tissues have become significantly restricted.
Sciatica symptoms lasting longer than 12 months require more involved treatment like injections or surgery to address symptoms effectively. (Antonio L Aguilar-Shea, et al., 2022)
Healing Chronic Sciatica
If the underlying cause can be effectively treated then chronic sciatica can be healed. Chronic sciatica often results from spinal conditions like herniated discs or lumbar spinal stenosis. These conditions narrow the space around the nerve roots that exit from the spinal cord and merge to form the sciatica nerve. Surgery is performed to open the space in the spine. (Mayfield Clinic. 2021) Sometimes sciatica is brought on by less common causes like a tumor or a spinal infection. In these cases, symptoms will not resolve until the underlying cause is addressed. Tumors may need to be surgically removed while infections require aggressive antibiotics to prevent spreading to other regions of the body. (Hospital for Special Surgery. 2023)
Pain Specialist Treatment Plan Development
Ongoing pain, numbness, tingling, and weakness are all symptoms that should be addressed with a healthcare provider. A pain specialist can help create a treatment plan that involves: (Hospital for Special Surgery. 2023)
Aguilar-Shea, A. L., Gallardo-Mayo, C., Sanz-González, R., & Paredes, I. (2022). Sciatica. Management for family physicians. Journal of family medicine and primary care, 11(8), 4174–4179. https://doi.org/10.4103/jfmpc.jfmpc_1061_21
Bosma, J. W., Wijntjes, J., Hilgevoord, T. A., & Veenstra, J. (2014). Severe isolated sciatic neuropathy due to a modified lotus position. World journal of clinical cases, 2(2), 39–41. https://doi.org/10.12998/wjcc.v2.i2.39
Dove, L., Jones, G., Kelsey, L. A., Cairns, M. C., & Schmid, A. B. (2023). How effective are physiotherapy interventions in treating people with sciatica? A systematic review and meta-analysis. European spine journal : official publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society, 32(2), 517–533. https://doi.org/10.1007/s00586-022-07356-y
Golonka, W., Raschka, C., Harandi, V. M., Domokos, B., Alfredson, H., Alfen, F. M., & Spang, C. (2021). Isolated Lumbar Extension Resistance Exercise in Limited Range of Motion for Patients with Lumbar Radiculopathy and Disk Herniation-Clinical Outcome and Influencing Factors. Journal of clinical medicine, 10(11), 2430. https://doi.org/10.3390/jcm10112430
Hamstring muscle injuries are common, especially in athletes and individuals with physically demanding jobs. Is there a better chance of full recovery with surgical repair and post-op rehabilitation?
Hamstring Muscle Tear
Most often, hamstring muscle injuries are partial tears of the muscle. These types of injuries are muscle strains that occur when the muscle fibers are stretched beyond their normal limits. Complete tears of the hamstring muscle are unusual, but they do occur in both athletes and non-athletes. Determining the optimal treatment plan depends on:
The severity of the tendon tear
The expectations of the injured individual.
Incomplete tears are when the hamstring muscle is stretched too far, but not completely detached.
Complete tears usually occur at the top of the muscle where the tendon tears away from the pelvis.
A complete tear usually occurs when there is a sudden flexion of the hip and extension of the knee joint – when the muscle contracts in this position, it gets stretched beyond its limits.
Basic hamstring strains can be treated with simple steps – rest, ice, anti-inflammatory medications, and conservative therapies.
Symptoms
Symptoms of a hamstring muscle strain can include pain, bruising, swelling, and movement difficulty. (American Academy of Orthopaedic Surgeons. 2021) Individuals who sustain this injury typically experience sudden sharp pain. Signs of a tear can include:
Sharp pain where the buttock and thigh meet.
Difficulty walking.
Sitting can be difficult as the edge of a chair can place pressure directly on the injury.
Spasms and cramping sensations in the back of the thigh.
Weakness in the leg, specifically when bending the knee or lifting the leg behind the body.
Numbness or burning sensations as a result of sciatic nerve irritation.
Swelling and bruising in the back of the thigh – over time it can travel down to the back of the knee and calf and possibly into the foot.
With a complete hamstring tear, there is usually significant swelling and bruising that develops in the back of the thigh.
Diagnosis
The symptoms can be difficult to spot in the early stages which is why X-rays of the hip or thigh are usually obtained.
In some situations, a fragment of bone can get pulled off the pelvis along with the hamstring muscle attachment. MRI testing can be performed to evaluate the attachment and can define critical features of a complete hamstring muscle tear, including: (American Academy of Orthopaedic Surgeons. 2021)
The number of tendons involved.
Complete versus incomplete tearing.
The amount of retraction – the amount the tendons have pulled back.
This will guide the development of treatment.
Treatment
The treatment of a complete tear will depend on different factors. The other variable is the patient and their expectations.
Treatment is more aggressive in younger individuals like high-level athletes.
Treatment is less aggressive in middle-aged individuals.
Often a single tendon tear can be treated non-surgically.
When one tendon is involved, it is typically not pulled very far from its normal attachment and will develop scar tissue in a positive position.
Conversely, when three tendons have been torn, they usually pull more than a few centimeters away from the bone. These cases have better results with surgical repair. (UW Health. 2017)
Surgeons will use patient characteristics – high-level athletes or less physically active individuals – to guide treatment recommendations.
Rehabilitation
Rehabilitation following surgery can take 3-6 months or longer.
The first six weeks limit weight-bearing with the use of crutches.
Patients may be recommended to wear a brace to reduce tension on the repaired hamstring tendons.
Strengthening does not begin until three months post-op, and even light activities are usually delayed. (UW Health. 2017)
Because this injury can have a long recovery time, some individuals may choose nonsurgical treatment.
Sometimes these individuals experience symptoms of discomfort from sitting and may exhibit long-term weakness of the hamstring muscle.
Full recovery from a complete hamstring muscle injury takes time. Studies have shown high-level athletes are able to resume competitive sports after the repair and rehabilitation of an acute hamstring muscle injury. (Samuel K. Chu, Monica E. Rho. 2016)
Delaying surgical treatment may not always lead to optimal results.
When the tendon is torn away from its normal attachment, it begins to scar around the surrounding soft tissues.
When there is a delay of more than a few weeks following the initial injury, regaining the full length of the tendon and muscle can be challenging.
This could delay the rehabilitation process and may limit the potential for full recovery. (Ho Yoon Kwak, et al., 2011)
With severe injuries, there is a better chance of full recovery with surgical repair but could involve a long recovery and commitment to a post-op rehabilitation plan.
Chu, S. K., & Rho, M. E. (2016). Hamstring Injuries in the Athlete: Diagnosis, Treatment, and Return to Play. Current sports medicine reports, 15(3), 184–190. https://doi.org/10.1249/JSR.0000000000000264
Kwak, H. Y., Bae, S. W., Choi, Y. S., & Jang, M. S. (2011). Early surgical repair of acute complete rupture of the proximal hamstring tendons. Clinics in orthopedic surgery, 3(3), 249–253. https://doi.org/10.4055/cios.2011.3.3.249
Are treatments more successful when patients know key terms that describe their back pain and associated conditions?
Nerve Pain Types
When individuals need to better understand their spine diagnosis, being able to distinguish between key terms can make a significant difference in understanding the development of a personalized treatment plan. Terms that describe back pain and various associated conditions can include:
Sciatica
Radiating and Referred pain
Radiculopathy
Radiculitis
Neuropathy
Neuritis
Causes of Back Pain
Back pain symptoms are most commonly caused by the continued practice of unhealthy/poor posture and overcompensated and weakened muscles. Even for individuals that exercise regularly, the movement choices that are made throughout the day can disrupt the way the muscles, tendons, ligaments, and fascia function to maintain proper body alignment.
Injuries to, and conditions of, the structures of the spinal column like the bones, discs, and nerves, are generally more serious than posture problems and soft tissue-related pain.
Depending on the diagnosis, structural problems can cause symptoms related to nerve compression, irritation, and/or inflammation. (Michigan Medicine, 2022)
Spine and Nervous System
The peripheral nerves extend out to the extremities with sensation and movement capabilities.
Nerve roots exit the spinal canal which is part of the peripheral nervous system.
The branching of nerves from the spinal cord and exit out of the foramina occurs at every level of the spine.
Terms
There are different medical terms when getting a spine diagnosis or going through the treatment process.
Radiculopathy
Radiculopathy is an umbrella term, describing any disease process that affects a spinal nerve root and is something that’s happening to the body.
When a healthcare provider informs you that your pain is due to radiculopathy, a number of more specific diagnoses, clinical signs, and symptoms may be included as part of the description.
Common causes of radiculopathy include herniated disc/s and spinal stenosis.
Less common causes can include a synovial cyst or tumor that presses on the nerve root. (Johns Hopkins Medicine, 2023)
Radiculopathy can occur in the neck, low back, or in the thoracic area.
Often, radiculopathy is brought on by some form of compression of the nerve root.
For example, extruded material from a herniated disc can land on a nerve root, causing pressure to build.
This can cause symptoms associated with radiculopathy, including numbness, weakness, pain, or electrical sensations. (Johns Hopkins Medicine, 2023)
Even though there’s a spinal nerve root on either side of the spinal column, injury, trauma, or issues stemming from degeneration affect the nerves in an asymmetric fashion. Degenerative changes, known as normal wear and tear, typically occur in this fashion. Using the previous herniated disc example, the material that leaks from the disc structure tends to travel in one direction. When this is the case, the symptoms tend to be experienced on the side where the nerve root makes contact with the disc material, but not the other side. (American Association of Neurological Surgeons, 2023)
Radiculitis
Radiculitis is a form of radiculopathy but it is about inflammation and not compression. (Johns Hopkins Medicine, 2023)
Radicu– refers to the spinal nerve root.
The suffix – itis refers to inflammation.
The word refers to a spinal nerve root that is inflamed and/or irritated rather than compressed.
In disc herniations, it is the gel substance that contains various chemicals that is inflammatory.
When the gel substance makes contact with nerve roots, an inflammatory response is triggered. (Rothman SM, Winkelstein BA 2007)
Radiating or Referred Pain
Radiating pain follows the path of one of the peripheral nerves that transmit sensory information like heat, cold, pins and needles, and pain.
Referred pain is experienced in a different area of the body that is away from the pain source which tends to be an organ. (Murray GM., 2009)
It can be brought on by myofascial trigger points or visceral activity.
An example of referred pain is symptoms in the jaw or arm when an individual is having a heart attack. (Murray GM., 2009)
Radicular
The terms radicular pain and radiculopathy tend to get confused.
Radicular pain is a symptom of radiculopathy.
Radicular pain radiates from the spinal nerve root to either part or all the way down the limb/extremity.
However, radicular pain does not represent the complete symptoms of radiculopathy.
Radiculopathy symptoms also include numbness, weakness, or electrical sensations like pins and needles, burning, or shock that travels down the extremity. (Johns Hopkins Medicine, 2023)
Neuropathy
Neuropathy is another umbrella term that refers to any dysfunction or disease that affects the nerves.
It’s usually classified according to the cause, like diabetic neuropathy, or the location.
Neuropathy can occur anywhere in the body – including the peripheral nerves, the autonomic nerves/organ nerves, or nerves that are located inside the skull and innervate the eyes, ears, nose, etc.
Peripheral nerves are the long, thin strands that supply sensation, feeling, and movement impulses to all areas of the body located outside the central nervous system.
Piriformis syndrome is where a tight buttock/piriformis muscle constricts the sciatic nerve, which runs underneath. (Cass SP. 2015)
Chiropractic
Chiropractic adjustments, non-surgical decompression, MET, and various massage therapies can relieve symptoms, release stuck or trapped nerves and restore function. Through the treatments, the chiropractor and therapists will explain what is happening and why they are using a specific technique. Knowing a little about how the neuromusculoskeletal system operates can help the healthcare provider and the patient in developing and adjusting effective treatment strategies.
Sciatica During Pregnancy
References
Michigan Medicine. Upper and Middle Back Pain.
American Academy of Neurological Surgeons. Anatomy of the Spine and Peripheral Nervous System.
Johns Hopkins Medicine. Health Conditions. Radiculopathy.
American Association of Neurological Surgeons. Herniated Disc.
American Academy of Orthopaedic Surgeons. OrthoInfo. Cervical Radiculopathy (Pinched Nerve).
Rothman, S. M., & Winkelstein, B. A. (2007). Chemical and mechanical nerve root insults induce differential behavioral sensitivity and glial activation that are enhanced in combination. Brain Research, 1181, 30–43. https://doi.org/10.1016/j.brainres.2007.08.064
Murray G. M. (2009). Guest Editorial: referred pain. Journal of applied oral science: Revista FOB, 17(6), i. https://doi.org/10.1590/s1678-77572009000600001
American Academy of Orthopaedic Surgeons. OrthoInfo. Carpal Tunnel Syndrome.
Bostelmann, R., Zella, S., Steiger, H. J., & Petridis, A. K. (2016). Could Spinal Canal Compression be a Cause of Polyneuropathy? Clinics and practice, 6(1), 816. https://doi.org/10.4081/cp.2016.816
Cleveland Clinic. Mononeuropathy.
American Association of Neurological Surgeons. Glossary of Neurosurgical Terminology.
National Institutes of Health. U.S. National Library of Medicine. Medline Plus. Peripheral Nerve Disorders.
Cleveland Clinic. Spinal Stenosis.
Cass S. P. (2015). Piriformis syndrome: a cause of non-discogenic sciatica. Current sports medicine reports 14(1), 41–44. https://doi.org/10.1249/JSR.0000000000000110
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine