Many individuals have dealt with issues affecting their lives in some way or form. People with autoimmune diseases must learn to manage their immune system from constantly attacking their bodies to function normally. The immune system’s primary function in the body is to attack environmental factors that harm the cells, muscles, and organs. When a person has an autoimmune disease, either from their family history or environmental factors, their immune system will begin to attack the body’s normal cells because it thinks it is a foreign invader to the body. Some common autoimmune disorders that most people have include lupus, ankylosing spondylitis, and rheumatoid arthritis. Most of these common autoimmune disorders correlate to common symptoms that add to other issues that affect the body. Today’s article looks at rheumatoid arthritis, its symptoms, how it relates to fatigue, and how there are available treatments to manage rheumatoid arthritis as well as fatigue. We refer patients to certified providers specializing in musculoskeletal therapies to help those who suffer from rheumatoid arthritis and fatigue. We also guide our patients by referring to our associated medical providers based on their examination when it’s appropriate. We find that education is the solution to asking our providers insightful questions. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
What Is Rheumatoid Arthritis?
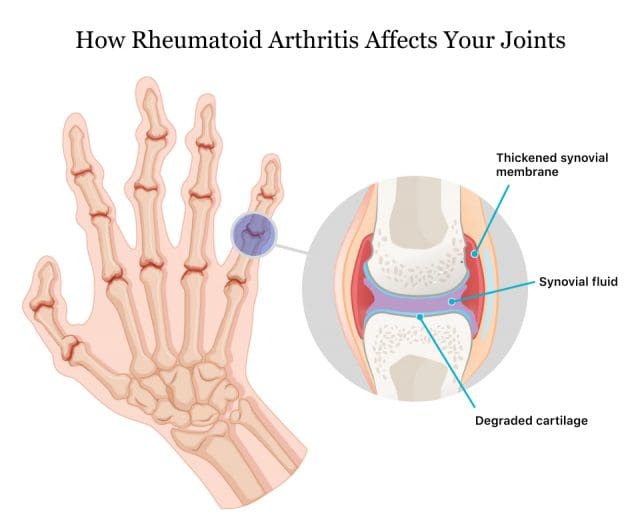
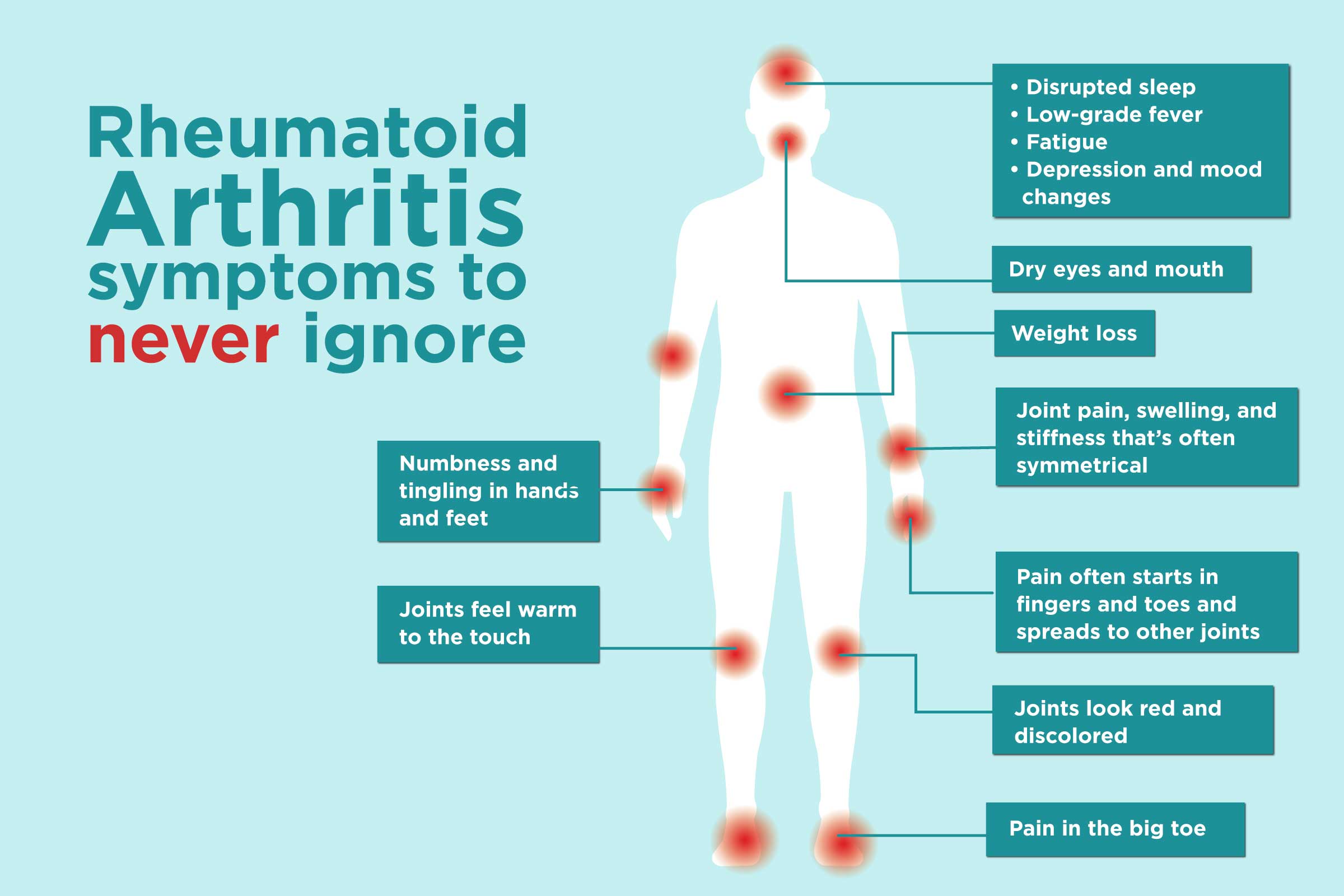
Have you been feeling stiffness and inflammation around your joints? have you experienced gut issues affecting your life? Or do problems of insomnia or fatigue seem to affect your quality of life? Many of these symptoms are associated with rheumatoid arthritis. Rheumatoid arthritis is an autoimmune disease that causes inflammation and swelling in the joints. The video above explains how to manage rheumatoid arthritis and its associated symptoms. Fatigue is one of the symptoms associated with rheumatoid arthritis as the inflammatory cytokines could be a co-morbidity in altering brain function that can lead to an overlap of pain and fatigue in the body, as studies reveal. While there hasn’t been a cure for rheumatoid arthritis, various treatment approaches can help people manage the symptoms of rheumatoid arthritis.
The Symptoms
Some of the most commonly rheumatoid arthritis symptoms do to the body include pain, swelling and inflammation of the joints, joint deformity, and stiffness. Unlike wear and tear damage from different types of common inflammatory issues, rheumatoid arthritis symptoms may come and go that can range from mild, moderate, or even severe. When this happens, rheumatoid arthritis may be the result of making it difficult to perform simple tasks and cause joint alterations. Research shows that rheumatoid arthritis associated with inflammation can damage different body parts like the gut. Gastrointestinal problems like leaky gut, IBS, or SIBO could trigger flare-ups in individuals who have rheumatoid arthritis. This is known as somato-visceral pain, where the muscles affect the vital organs, causing problems for the body.
How Does Fatigue Correlate To RA?
Individuals that have rheumatoid arthritis do suffer from various symptoms that are associated with inflammatory issues. When inflammation begins to affect the body, it can overlap the profiles of fatigue and poorer quality of life in the individual. So how does fatigue correlate to rheumatoid arthritis? Studies reveal that fatigue is considered one of the acute symptoms of rheumatoid arthritis that imposes a burden on individuals, thus being associated with reducing their health and wellness. Fatigue has many dimensions that do impact many individuals. Some people will explain to their primary physicians that they are constantly tired, overworked, and repeatedly stressed from everyday life or disorders affecting their bodies. For rheumatoid arthritis individuals, studies reveal that high inflammatory factors associated with fatigue may cause them to feel exhausted. This is related to individuals who have insomnia from other conditions.
Managing Rheumatoid Arthritis-Video
Have you been feeling stiffness and inflammation around your joints? have you experienced gut issues affecting your life? Or do problems of insomnia or fatigue seem to affect your quality of life? Many of these symptoms are associated with rheumatoid arthritis. Rheumatoid arthritis is a chronic autoimmune disease that causes inflammation and swelling in the joints. The video above explains how to manage rheumatoid arthritis and its associated symptoms. Fatigue is one of the symptoms associated with rheumatoid arthritis as the inflammatory cytokines could be a co-morbidity in altering brain function that can lead to an overlap of pain and fatigue in the body, as studies reveal. While there hasn’t been a cure for rheumatoid arthritis, various treatment approaches can help people manage the symptoms of rheumatoid arthritis.
Treatments For RA & Fatigue
Even though there hasn’t been a cure for rheumatoid arthritis, there are ways to manage the associated symptoms of rheumatoid arthritis. Eating anti-inflammatory riched foods could potentially dampen the effect of inflammation on the joints. One way while exercising can help loosen up stiff joints and bring back muscle strength, thus restoring joint motion. Treatments like chiropractic care can also provide pain relief and management for individuals dealing with rheumatoid arthritis. Chiropractic care comprises passive and active treatment modalities for rheumatoid arthritis and fatigue. Chiropractors utilize spinal adjustments and manual manipulation to reduce misalignment or subluxation of the spine. Chiropractic care may also help with many symptoms like fatigue associated with rheumatoid arthritis without invasive treatments or medication. Chiropractic care could potentially improve the function of the bones, joints, and even the nervous system in the body.
Conclusion
Rheumatoid arthritis is a chronic inflammatory disease that causes joint stiffness and swelling. The causes of this autoimmune disease are unknown. Still, factors like stress, gut issues, and obesity are associated with symptoms like fatigue, leaky gut, muscle stiffness, and poorer quality of life could potentially be involved with rheumatoid arthritis. Treatments like eating anti-inflammatory foods, exercising, and chiropractic care could help manage inflammatory issues triggering rheumatoid arthritis and potentially reduce the effects of fatigue from the body, thus slowing down the progression and bringing back a person’s quality of life.
Korte, S Mechiel, and Rainer H Straub. “Fatigue in Inflammatory Rheumatic Disorders: Pathophysiological Mechanisms.” Rheumatology (Oxford, England), Oxford University Press, 1 Nov. 2019, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6827268/.
Pope, Janet E. “Management of Fatigue in Rheumatoid Arthritis.” RMD Open, BMJ Publishing Group, May 2020, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7299512/.
Santos, Eduardo J F, et al. “The Impact of Fatigue in Rheumatoid Arthritis and the Challenges of Its Assessment.” Rheumatology (Oxford, England), Oxford University Press, 1 Nov. 2019, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6827262/.
Staff, Mayo Clinic. “Rheumatoid Arthritis.” Mayo Clinic, Mayo Foundation for Medical Education and Research, 18 May 2021, https://www.mayoclinic.org/diseases-conditions/rheumatoid-arthritis/symptoms-causes/syc-20353648.
Everyone is trying to find what exercise works for them as they start looking for ways to improve their health and wellness. Many individuals who begin to work out would go with finding a personal trainer or a gym that helps incorporate muscle strength training and cardio training to improve their heart and lung capacity to make the body feel good while strengthening their muscles. One of the unique forms of exercise that involve both the heart and muscles is dancing. Dancing is a great way to not only improve musculoskeletal and cardiovascular health but can help reduce overlapping conditions that a person is dealing with in their bodies. Today’s article looks at how dancing helps with musculoskeletal health, affects the heart and brain, and how chiropractic care goes hand in hand with dancing. We refer patients to certified providers specializing in musculoskeletal and cardiovascular therapies to help those with heart and muscle issues. We also guide our patients by referring to our associated medical providers based on their examination when it’s appropriate. We find that education is the solution to asking our providers insightful questions. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
Dancing For Musculoskeletal Health
Have you ever noticed people take a cardio class with music playing in the background and see them happy afterward? How do athletes incorporate cardio into their exercise regime to improve their mobility and flexibility? Or how do particular video games make you get up and move around? All these scenarios imply that cardio exercises like dancing may help improve musculoskeletal function. Dancing is one of the many aerobic exercises that can help improve a person’s social skills and is something that can be taken up early while providing many beneficial qualities like:
Increase strength
Improve gait and balance
Reduce functional loss
Reducing the risk of falls
Rehabilitating musculoskeletal injuries
Stabilize core muscles
For the musculoskeletal system, dance would be considered an isometric exercise involving different muscle groups like the hips, shoulders, back, and abdominals without using the joints. When a person is dancing, each of the various movements is related to strengthening the core muscles by working thoroughly with the abdominals. Dance can even help improve posture by maintaining strength and enhancing stability in the body. Studies reveal that dance’s impact on individuals with chronic issues like Parkinson’s disease associated with motor and non-motor symptoms can increase their quality of life. So what does that mean? It means that dancing, even for just one song, can help with movement and foster balance, flexibility, and muscle endurance through repeated tasks while associating with accessible, social, and attractive aspects of a person’s physical abilities.
How Does Dancing Affect The Heart and Brain?
Dancing not only helps with musculoskeletal issues, but it can help improve brain and heart function in the body. Studies reveal that moderate-intensity dancing was inversely associated with a reduced risk for cardiovascular disease mortality. What dancing does to the heart is that it makes the body intake more oxygen to the lungs, which relates to the heart beating faster and circulating the blood to be transported throughout the entire body. But how does dancing correlate to brain health? Let’s look at dance fitness classes, like Zumba, and use it as an example. Studies show that dance fitness classes provide several health benefits that could reduce mood disorders like depression and anxiety while improving cognitive skills. This means that dance fitness classes like Zumba do repetitive movements to the beat of the music that engages the individual to repeat the steps while having fun. When the muscles begin to do repetitive movements, this motor function sends the signal to the brain, making the person remember the movements later, known as muscle memory. When an individual suffers from neurological disorders like dementia or Alzheimers, dancing could potentially be involved with music therapy, allowing the individual to reduce the risk of developing neurological disorders from progressing further.
How Does The Body React To Dancing?-Video
Have you felt terrific after listening to a good song? How about feeling like you just had a workout? Or have you noticed certain areas in your body like your abdominals, legs, and back looked more toned? All these are beneficial signs that you should add dancing to your regime. The video explains what happens to the body when people are dancing. Dancing could potentially be a mediator for many athletes that play sports.
An example would be football and ballet. How do football and ballet relate to each other? Football utilizes efficient and precise movements that benefit every position on the field, while ballet requires speed to make them flawless on stage. Combining the two, many football players will increase their speed and agility associated with ballet to avoid tackles, jump higher, catch passes and avoid injuries on the field. Dancing is an excellent way to get some cardio exercises in, and combined with other treatments can make a difference in a person.
Chiropractic Care & Dancing
Like all athletic individuals, professional dancers utilize various treatments to recover and improve their performance. Treatments like chiropractic care are safe, effective, and widely used by young and professional athletes that want to prevent injuries from progressing. Chiropractic care for professional athletes and the general population can help prevent and treat injuries like back and neck pain or aggravating conditions like sciatica through spinal manipulation. Chiropractic care also helps restore an individual’s original well-being while increasing their strength, flexibility, and mobility. By working with an experienced chiropractor, an individual can regain their stamina by adopting new ways to prevent injuries caused by spinal complications from reoccurring in the body.
Conclusion
Dancing for 30 minutes to an hour can be used as part of an exercise regime and could potentially reduce chronic issues that affect the body’s brain, heart, and muscles. Dancing could also enhance a sports athlete’s performance by increasing their agility, endurance, and performance. Combined with chiropractic care, individuals will begin to see improvements in their range of motion, flexibility, and even an increase in their brain function to dance longer and improve their health and wellness. So whether you are a professional or not, dancing is for everyone.
Reference
Barranco-Ruiz, Yaira, et al. “Dance Fitness Classes Improve the Health-Related Quality of Life in Sedentary Women.” International Journal of Environmental Research and Public Health, MDPI, 26 May 2020, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7312518/.
Ferchak, Dawn. “Belly Dance Your Back Pain Away – Spineuniverse.” Spine Universe, 14 Oct. 2020, https://www.spineuniverse.com/wellness/exercise/belly-dance-back-pain.
Gyrling, Therese, et al. “The Impact of Dance Activities on the Health of Persons with Parkinson’s Disease in Sweden.” International Journal of Qualitative Studies on Health and Well-Being, Taylor & Francis, Dec. 2021, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8547839/.
Merom, Dafna, et al. “Dancing Participation and Cardiovascular Disease Mortality: A Pooled Analysis of 11 Population-Based British Cohorts.” American Journal of Preventive Medicine, U.S. National Library of Medicine, June 2016, https://pubmed.ncbi.nlm.nih.gov/26944521/.
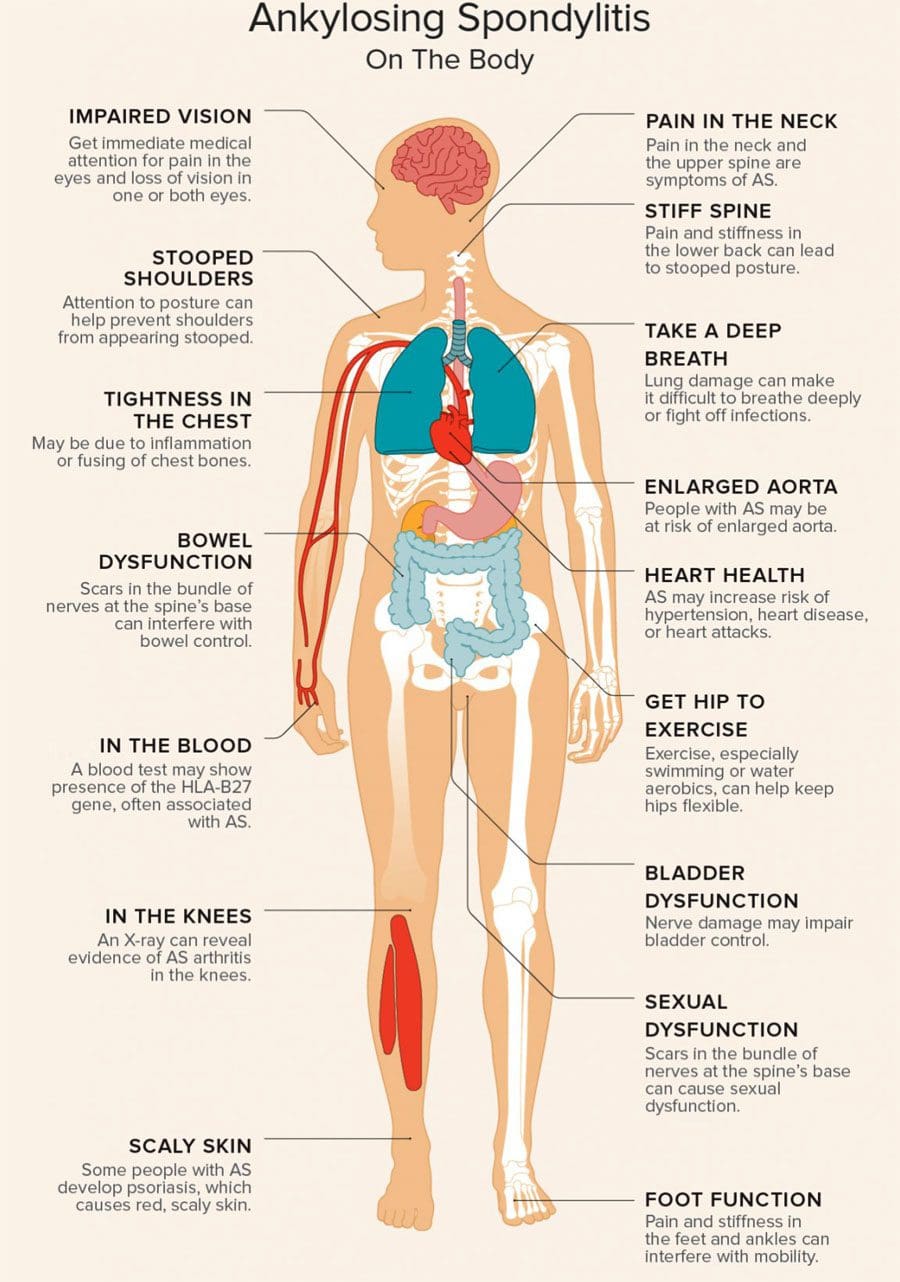
Fatigue Ankylosing Spondylitis: Fatigue is a significant complaint for individuals dealing with ankylosing spondylitis. Ankylosing spondylitis is chronic inflammation of the spine’s joints that can cause them to become fused or locked up. The process can cause the spine to stiffen, limiting movement, reducing flexibility, and generating a severe hunched posture. Symptoms can include back pain, stiffness, and the inability to take a deep breath if the ribs are involved. Fatigue can have a variety of causes, but in ankylosing spondylitis, inflammation and cytokines play a significant role. The underlying cause of ankylosing spondylitis is still being researched, but it currently affects around 300,000 Americans.
Fatigue Ankylosing Spondylitis
Most individuals with ankylosing spondylitis experience pain in the lower back but can also feel pain in their hips and neck, have abdominal pain, or experience problems with vision. Inflammatory back pain is usually strongest in the morning but can also come from inactivity.
Spinal Condition and Extreme Exhaustion
The inability to move along with a decreased spinal range of motion impacts body functionality, sleep quality, and respiratory function affecting energy levels and leading to mild to severe fatigue. Studies have shown that 50% – 85% of individuals with ankylosing spondylitis experience fatigue.
Fatigue is brought on by inflammation, as the body generates the same chemicals when fighting a cold or flu; an individual’s body constantly works to reduce inflammation, leaving them drained and unable to perform ordinary tasks. Inflammatory diseases take a significant toll on the whole body, leading to an increased risk of depression and increased fatigue levels.
Exercise, Massage, and Diet
Many individuals find that their symptoms flare up after long periods of inactivity, like sleeping. This can make wanting to fall and stay asleep complicated, exacerbating fatigue and vice versa, creating a vicious cycle. Even though it can be challenging to move, gentle exercise is recommended. Exercise can help slow the disease progression, build muscle, and improve sleep. It is recommended to speak with a spine specialist, doctor, chiropractor, physical therapist, or exercise trainer about a customized exercise treatment program.
Many individuals with ankylosing spondylitis find therapeutic massage helpful in temporarily relieving pain, and stiffness, reducing stress and improving flexibility from increased blood circulation. A combination of gentle chiropractic massage, exercise, ergonomic adjustments, and rheumatology treatment is recommended for many cases. An anti-inflammatory diet comprised of foods like fatty fish, fruits, nuts, and leafy green vegetables can fight inflammation and decrease fatigue.
AS Causes, Symptoms, Diagnosis, Treatment, and Pathology
References
Cornelson, Stacey M et al. “Chiropractic Care in the Management of Inactive Ankylosing Spondylitis: A Case Series.” Journal of chiropractic medicine vol. 16,4 (2017): 300-307. doi:10.1016/j.jcm.2017.10.002
Li, Ting, et al. “Fatigue in Ankylosing Spondylitis Is Associated With Psychological Factors and Brain Gray Matter.” Frontiers in medicine vol. 6 271. 21 Nov. 2019, doi:10.3389/fmed.2019.00271
Zhang, Jun-Ming, and Jianxiong An. “Cytokines, inflammation, and pain.” International anesthesiology clinics vol. 45,2 (2007): 27-37. doi:10.1097/AIA.0b013e318034194e
Maintaining healthy joints is crucial to preventing injuries from affecting the body. Incorporating physical activities, eating healthy foods, staying hydrated, and getting a routine check-up are ways to ensure that the body is functional, including the joints. The joints in the body act like shock absorbers that soften the impact of any injuries that the body has sustained. However, as the body ages, so do the joints, causing them to become hardened and cause problems in the body. In today’s article, we will look at sacroiliac dysfunction, what issues it affects besides back pain, and how chiropractic care manages sacroiliac dysfunction. We refer patients to certified providers specializing in musculoskeletal therapies to help those with sacroiliac dysfunction. We also guide our patients by referring to our associated medical providers based on their examination when it’s appropriate. We find that education is the solution to asking our providers insightful questions. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
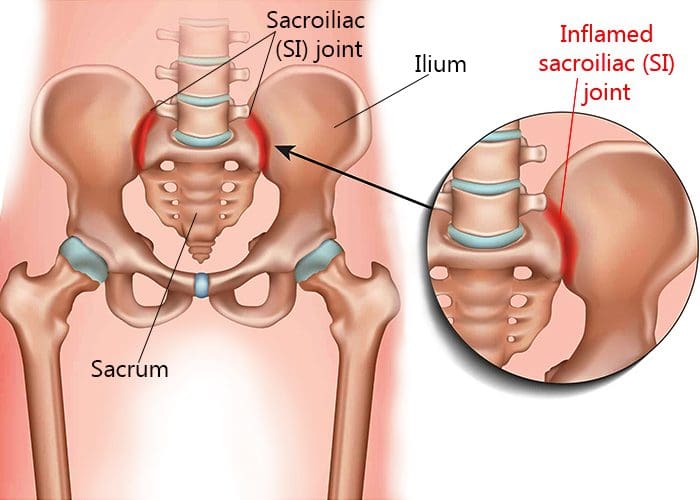
What Is Sacroiliac Dysfunction?
Are you experiencing pain in the pelvis? Do your hips seem tighter than usual? Do you feel muscle stiffness when you twist from side to side? Some of these issues are signs that you might be experiencing sacroiliac dysfunction. Around the pelvic region lies the sacroiliac joint, a weight-bearing solid joint connecting the pelvis to the sacrum. It is surrounded by tough ligaments that support the body as it distributes the weight from the upper body to the lower body. However, like all the other joints in the body, any injury or condition can cause this joint to be unstable and succumb to the pain, causing sacroiliac dysfunction. Sacroiliac dysfunction or sacroiliac joint pain is defined as one of the potential causes of axial low back pain. When there are issues affecting the sacroiliac joints, it’s associated with about a quarter of most low back pain cases. This is due to the problems that overlap with pain associated with the low back. Studies reveal that dysfunction in the sacroiliac joint can relate to leg or back pain, making diagnosing the problem difficult. Back pain associated with sacroiliac dysfunction causes the pelvis to be hypermobile, causing the risk of developing radiating groin pain. Leg pain associated with sacroiliac dysfunction causes muscle tension and stiffness to the low back, legs, or buttock region, mimicking sciatica-like symptoms.
What Other Issues Does It Affect?
Many individuals may not realize that when they are experiencing sacroiliac dysfunction, symptoms show that they overlap with lumbar spine pathologies. However, sacroiliac dysfunction can also affect the pelvic region of the body. Studies reveal that when the muscles around the body’s pelvic area become inflamed or irritated, it can cause stiffness in the sacroiliac joints, thus developing the risk of pelvic pain. Pelvic pain is usually defined as non-menstrual pain that causes functional disability to the lower extremities. Around the pelvic region, the lower sacral nerves provide extensive neurologic connections to the structures throughout the pelvic area that maintain normal pelvic organ function. When issues like sacroiliac dysfunction become the risk of pelvic pain, it may potentially involve pelvic symptoms like constipation. Studies reveal that constipation is significantly associated with a high prevalence of pelvic organ prolapse and low urinary tract symptoms. Other issues that sacroiliac dysfunction correlates with are:
Ankylosing spondylitis
Rheumatoid arthritis
Inflammatory issues
Hip pain
Pelvic pain
Low back pain
Piriformis syndrome
An Overview Of Sacroiliac Joint Pain- Video
Are you experiencing radiating from your lower back down to your leg? How about stiffness in your hips? Are you feeling constipated or have a sense of fullness in your bladder? You may suffer from sacroiliac dysfunction in your pelvic region if you notice these symptoms. The video above explains how to understand sacroiliac joint pain. The sacroiliac joint connects the pelvis and sacrum, surrounded by tough ligaments and muscles that help support the body by distributing weight from the upper body to the lower body. When issues affect the sacroiliac joints can overlap other risk profiles like low back pain, leg pain, and pelvic pain. This can make diagnosing sacroiliac dysfunction difficult because the symptoms are similar to other issues. For example, hip pain is associated with piriformis syndrome while potentially being involved with sciatica. How would hip pain be correlated with piriformis syndrome? The piriformis muscle can become overused and injured and can entrap the sciatic nerve (which runs from the lumbar spine, through the hips, and down to the leg), causing radiating, throbbing pain. Other times referred pain in the low back can affect different areas in the body due to sacroiliac dysfunction. Luckily, there are treatments available to manage sacroiliac dysfunction.
How Chiropractic Care Manages Sacroiliac Dysfunction
When issues of sacroiliac dysfunction become associated with leg or back pain, physicians often misdiagnose it as a soft tissue issue rather than a joint issue. Many doctors might rule out various medical conditions before including sacroiliac dysfunction as part of the diagnosis. Some treatments like massage therapy can help loosen up the tight muscles surrounding the joints relieving the pain and discomfort. At the same time, chiropractic care utilizes spinal manipulation and mobilization to the affected spinal area. Since the sacroiliac joint is an essential part of the musculoskeletal system, chiropractors specialize in this area. Through practical, non-invasive methods, chiropractic care has proven to not only relieve pain in the spine but can also help rehabilitate the spine. Chiropractors are specially trained to guide the individual through several phases of care that help loosen the stiff muscles and strengthen the joints. Chiropractic care will help decrease the pain from returning to the body and let the individual return to their health and wellness journey.
Conclusion
Maintaining healthy joints is crucial to prevent injuries from affecting the body. The sacroiliac joints are part of the musculoskeletal system that connects the pelvic bone to the sacrum. This joint is surrounded by tough ligaments and muscles that support the upper and lower half of the body through weight distribution. When the sacroiliac joint becomes unstable, it can succumb to pain, thus becoming sacroiliac dysfunction. Sacroiliac dysfunction sometimes mimics low back and leg pain, making it difficult to diagnose. Co-morbidities like pelvic pain correlate to sacroiliac dysfunction, causing somato-visceral pain in different body areas. Treatments like chiropractic care can help strengthen the stiff muscles and joints in the body through spinal manipulation and mobilization in practical, non-invasive treatment. Chiropractic care can help rehabilitate the spine while decreasing the pain from returning to the body.
References
Jonely, Holly, et al. “Chronic Sacroiliac Joint and Pelvic Girdle Dysfunction in a 35-Year-Old Nulliparous Woman Successfully Managed with Multimodal and Multidisciplinary Approach.” The Journal of Manual & Manipulative Therapy, Maney Publishing, Feb. 2015, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4459139/.
Raj, Marc A, et al. “Sacroiliac Joint Pain.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 12 Feb. 2022, https://www.ncbi.nlm.nih.gov/books/NBK470299/.
Singh, Prashant, et al. “Pelvic Floor Symptom Related Distress in Chronic Constipation Correlates with a Diagnosis of Irritable Bowel Syndrome with Constipation and Constipation Severity but Not Pelvic Floor Dyssynergia.” Journal of Neurogastroenterology and Motility, Korean Society of Neurogastroenterology and Motility, 31 Jan. 2019, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6326213/.
Everyone has dealt with acute or chronic pain at some point in their lives. The body’s response tells many of us where the pain is located and can leave the body sore as the immune system begins to heal the affected area. When disorders like autoimmune diseases start to attack the body for no reason, then that is when chronic issues and disorders begin to overlap in risk profiles on other various problems that affect both the muscles and organs. Autoimmune diseases like fibromyalgia can affect a person’s body; however, they could be associated with different issues affecting the body. Today’s article looks at fibromyalgia, how it affects the musculoskeletal system, and how chiropractic care helps manage fibromyalgia in the body. We refer patients to certified providers specializing in musculoskeletal treatments to help those with fibromyalgia. We also guide our patients by referring to our associated medical providers based on their examination when it’s appropriate. We find that education is the solution to asking our providers insightful questions. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
What Is Fibromyalgia?
Have you experienced excruciating pain that is spread all over your body? Do you have trouble sleeping and feel exhausted every day? Do you experience brain fog or other cognitive disturbances? Many of these issues are signs and conditions of fibromyalgia. Fibromyalgia is defined as a chronic condition that is characterized by widespread musculoskeletal pain. Symptoms like fatigue, cognitive disturbances, and multiple somatic symptoms often overlap and accompany this disorder. Around two to eight percent of the world population suffers from fibromyalgia, and it affects women more than men. Sadly though, fibromyalgia is a challenge to diagnose, and the pain can last several months to years. Some of the main symptoms that fibromyalgia does to the body include:
Muscle and joint stiffness
General sensitivity
Insomnia
Cognitive dysfunction
Mood disorders
Fibromyalgia could also potentially be associated with specific diseases like diabetes, lupus, rheumatic diseases, and musculoskeletal disorders.
How Does It Affect The Musculoskeletal System?
The musculoskeletal system in the body has three muscle groups: skeletal, cardiac, and smooth muscles that provide different functions correlating how the body moves. Individuals with fibromyalgia will experience amplified painful sensations affecting their brain and spinal cord to process pain and nonpainful signals potentially associated with musculoskeletal disorders. The neural structures from the brain become hyper-reactive to any soft tissues close to the spine, known as segmental facilitation. These changes that occur to the soft tissues are called trigger points, and if situated in the muscles, they are referred to as “myofascial” trigger points. Studies reveal that the pathophysiology of musculoskeletal dysfunction can be considered secondary to central abnormalities of pain modulation associated with fibromyalgia.
An Overview Of Fibromyalgia-Video
Have you been experiencing excruciating pain in different areas of your body? Have you been constantly tired throughout the entire day? Or has your mood been dampened all of a sudden? These are the signs that you have fibromyalgia, and the video above gives an overview of what fibromyalgia is. Fibromyalgia is defined as a chronic disorder that is difficult to diagnose. Studies reveal that fibromyalgia is possible to be described as a cognitive disorder that triggers painful amplifications and sensory nociceptors that become hypersensitive. So what does this mean, and how is the nervous system affected by fibromyalgia? The nervous system has the central and peripheral systems. The peripheral system has a component known as the autonomic nervous system that regulates involuntary bodily functions. The autonomic system consists of two subsystems: the sympathetic and parasympathetic systems. For individuals with fibromyalgia, the sympathetic nervous system, which provides the “fight or flight” response, is constantly active, causing the parasympathetic nervous system, which provides the “rest and digest” response, to be inactive in the body. The good news is that individuals with fibromyalgia and its associated symptoms can find relief through treatment.
Chiropractic Care & Fibromyalgia
Even though there hasn’t been a cure for fibromyalgia yet, treatments are available to manage and improve the symptoms associated with fibromyalgia with chiropractic care. Chiropractic care can help relieve fibromyalgia pain by carefully correcting spinal misalignments or subluxations through spinal adjustments and manual manipulations of the body. Studies reveal that the effectiveness of chiropractic care for fibromyalgia patients helps improve their range of motion to the cervical and lumbar areas of the spine. Chiropractic care can help improve their flexibility, decrease their pain levels, and have better sleep quality. People diagnosed with fibromyalgia need to understand that many options for pain management don’t rely on medicines. Chiropractic care is gentle and non-invasive. It can be helpful for individuals that want to take control of their circumstances and have chiropractic therapy as a vital part of managing their well-being.
Conclusion
Fibromyalgia is a chronic disorder that affects the musculoskeletal system by causing stiffness in the muscles and joints, general sensitivity, and other chronic issues associated with this disorder. Individuals with fibromyalgia will describe their pain as unbearable due to the nerves in the sympathetic system being hyperactive and tender to the touch. Fortunately, treatments like chiropractic care can help relieve fibromyalgia pain through spinal adjustments and manual manipulations. Chiropractic care for individuals with fibromyalgia can help improve their range of motion and flexibility and decrease their pain levels without using medicines. Incorporating chiropractic care as a treatment for fibromyalgia can be vital in managing a person’s well-being.
References
Bhargava, Juhi, and John A Hurley. “Fibromyalgia – Statpearls – NCBI Bookshelf.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 1 May 2022, https://www.ncbi.nlm.nih.gov/books/NBK540974/.
Blunt, K L, et al. “The Effectiveness of Chiropractic Management of Fibromyalgia Patients: A Pilot Study.” Journal of Manipulative and Physiological Therapeutics, U.S. National Library of Medicine, 1997, https://pubmed.ncbi.nlm.nih.gov/9272472/.
Geel, S E. “The Fibromyalgia Syndrome: Musculoskeletal Pathophysiology.” Seminars in Arthritis and Rheumatism, U.S. National Library of Medicine, Apr. 1994, https://pubmed.ncbi.nlm.nih.gov/8036524/.
Maugars, Yves, et al. “Fibromyalgia and Associated Disorders: From Pain to Chronic Suffering, from Subjective Hypersensitivity to Hypersensitivity Syndrome.” Frontiers, Frontiers, 1 July 2021, https://www.frontiersin.org/articles/10.3389/fmed.2021.666914/full.
Siracusa, Rosalba, et al. “Fibromyalgia: Pathogenesis, Mechanisms, Diagnosis and Treatment Options Update.” International Journal of Molecular Sciences, MDPI, 9 Apr. 2021, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8068842/.
When the weather becomes hot, and everyone begins to plan fun activities to enjoy, one of the many activities that come to mind is hanging out in the pool. Swimming is an excellent way to combat the summer heat, but it can provide much more for the body. For athletes, it provides another form of cardio exercise to improve their quality performance when they are competing. While for individuals looking for an affordable exercise regimeor just some fun activity to do, swimming can become a form of therapy and be beneficial for them if they were previously injured. Today’s article looks at how swimming causes an impact on the musculoskeletal system, its beneficial properties to the heart, and how aqua therapy combined with chiropractic care helps optimize full-body health. We refer patients to certified providers specializing in musculoskeletal treatments and hydrotherapy to help those with musculoskeletal disorders. We also guide our patients by referring to our associated medical providers based on their examination when it’s appropriate. We find that education is the solution to asking our providers insightful questions. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
Swimming & Its Impact On The Musculoskeletal System
Water exercises or swimming can benefit those looking for different cardio exercises to build muscle endurance or have a clear sense of mind. Swimming is fantastic for all body sizes, and when it is done correctly, it can be highly recognized as a form of rehabilitation and injury recovery known as aquatic therapy. Research studies reveal that aquatic treatments and exercises can significantly reduce pain in individuals that suffer from low back pain while increasing physical function. Some of the impacts that swimming/aquatic therapy provides on the musculoskeletal system include:
Builds muscle strength
Improves endurance
Stabilizes joints
Improves poor posture
Swimming/ hydrotherapy is an excellent low-impact exercise that is easy on the back and spine, especially for individuals suffering from low back pain or spinal misalignments. Studies reveal that the efficacy of aquatic activities helps strengthen the abdominals and legs and stretch the back while managing musculoskeletal issues.
When individuals suffer from back pain associated with chronic issues can become concerning for the vital organs that have a causal relationship with the muscle as they are affected as well. When spinal joints and muscles begin to suffer from abnormal weight increases, the muscles and ligaments become misaligned. Misalignment or subluxation is defined as spinal vertebrates that are out of place and cause pressure on the surrounding nerves exiting the spinal cord. These spinal issues then become a risk of developing musculoskeletal disorders in the body. Unlike many aerobic exercises like running or cycling that may be hard on the spine, swimming has little to no impact on the spinal structures. So when individuals begin to take up swimming, they realize that the water buoyancy helps support their body weight while relieving stress on all joints and decompressing the spine. This gives the individual a greater range of motion, while the water gives off a sense of purification as it helps the body relax. Hence, hydrotherapy helps relax people who suffer from obesity or muscle injuries associated with muscle and joint pain as the water provides gentle resistance while relaxing the muscles to promote longer exercise sessions.
The Benefits Of Swimming For The Heart
Swimming or any form of water aerobics is not only beneficial to the musculoskeletal system but can help improve cardiac function in the heart and even the lungs. Studies reveal that swimming is an effective option for maintaining and enhancing cardiovascular fitness. Some of the benefits swimming provides for the cardiovascular system include:
Lowers blood pressure
Improve circulation
Reduces heart rate
But how does swimming improve cardiovascular function in the body? Individuals submerge themselves underwater; they hold their breath until the air is needed. Being submerged underwater may help lung capacity while gaining control of how a person breathes. Breathing exercises associated with aqua therapy help promote stronger lungs and heart while increasing their capacity for blood and airflow to the heart and lungs. Say, for example, a person is having trouble breathing due to restrictive blood and air flow associated with cardiopulmonary issues, which potentially be involved in experiencing an asthma attack associated with obesity.
The Benefits Of Swimming-Video
Have you wanted to try a different form of cardio exercise? Have you been experiencing a limited range of motion in your arms, shoulders, back, and neck? Do you feel tightness across your chest? The video above gives an overview explanation of the health benefits of swimming. Swimming or aquatic therapy allows the individual experiencing chronic pain issues to do cardio activities without increasing or worsening pain, which is very therapeutic for the body. Many people are either training for an athletic event or finding a leisure activity that will benefit them in the long run. Swimming is considered an important factor in a person’s quality of life as it helps them become motivated to make small changes to better their health. Additionally, regular cardiovascular exercises/activities like swimming benefit pain reduction in a therapeutic sense. When individuals are trying to figure out and determine the proper training or therapy that can help alleviate their specific ailments, their goal is to see how those exercises should be done in a certain amount of time without causing fatigue or increased pain as the primary objective.
Aqua Therapy & Chiropractic Care
When looking for the proper exercise regime or treatment for pain issues, it can be challenging to see what works and doesn’t. For those with musculoskeletal disorders related to chronic issues, aqua therapy and chiropractic care go hand in hand in alleviating pain. Aqua therapy exercises can range from simple routines in shallow waters to high-tech equipment like underwater treadmills for muscle conditioning. Active water therapy exercises that are diverse in relieving musculoskeletal pain should be tailored to the person and the specific conditions that are ailing them.
But how does chiropractic care work hand in hand with aqua therapy? Well, chiropractic care and exercise have a casual relationship when it comes to treating musculoskeletal disorders. Many individuals do suffer from spinal misalignment, which becomes a risk of developing musculoskeletal issues that cause discomfort. Since many individuals associate chiropractic care with back issues, the reality shows that chiropractic care not only helps with back issues but various issues that affect the muscles, joints, and organs related to each other. An example would be an individual with low back problems who cannot do any activities for long periods while triggering gut issues. This is defined as somato-visceral pain where affected muscles associated with internal organs trigger pain. So for a chiropractor to adjust an individual dealing with back pain associated with gut or heart issues can slowly restore the person’s natural alignment by reducing the irritated nerve roots between the vertebrae and strengthening the surrounding muscles and tissues. Afterward, a chiropractor may recommend exercises like aquatic therapy to speed up the rehabilitation process, as studies reveal that physical activities are perceived to have a positive impact on health while being associated with perceived symptom reductions in musculoskeletal and injuries, as well as cardiovascular and blood conditions. Once a chiropractic regimen and exercise routine are in place, injury prevention kicks in, keeping the individual moving pain-free.
Conclusion
Whether it is having fun in the sun or finding a new exercise, swimming is not only for just playing but can be therapeutic for individuals dealing with chronic issues. Any aquatic exercise provides little to no impact on the body as it helps strengthen the musculoskeletal and cardiovascular systems with gentle force. Combined with chiropractic care, many individuals that are dealing with musculoskeletal issues associated with chronic organ issues will begin to become motivated to better themselves in the long run.
References
Ariyoshi, Mamoru, et al. “Efficacy of Aquatic Exercises for Patients with Low-Back Pain.” The Kurume Medical Journal, Kurume University School of Medicine, 11 Aug. 2009, https://www.jstage.jst.go.jp/article/kurumemedj1954/46/2/46_2_91/_article.
Lazar, Jason M, et al. “Swimming and the Heart.” International Journal of Cardiology, U.S. National Library of Medicine, 18 Apr. 2013, https://pubmed.ncbi.nlm.nih.gov/23602872/.
Massey, Heather, et al. “Perceived Impact of Outdoor Swimming on Health: Web-Based Survey.” Interactive Journal of Medical Research, JMIR Publications, 4 Jan. 2022, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8767464/.
Shi, Zhongju, et al. “Aquatic Exercises in the Treatment of Low Back Pain: A Systematic Review of the Literature and Meta-Analysis of Eight Studies.” American Journal of Physical Medicine & Rehabilitation, U.S. National Library of Medicine, Feb. 2018, https://pubmed.ncbi.nlm.nih.gov/28759476/.
Everyone wants to be healthier at some point in their lives. Some individuals train to be athletes and must follow procedures to maintain their health. In comparison, others want to get healthier by eating the right food, exercising for at least 30 minutes to an hour, meditating or doing yoga to relieve stress, and maintaining a healthy weight. However, many environmental factors do affect the human body. They can alter how a person looks, weight, levels of physical activity, and how different foods affect the body’s metabolism. When environmental factors start to take hold of a person’s health, it can trigger unwanted issues that affect not only the muscles in the body but the associated internal organs that help provide the functionality to the body. Today’s article focuses on the musculoskeletal system, how different issues affect the musculoskeletal system and associate with other problems in the body, and various treatments to improve musculoskeletal health. We refer patients to certified providers specializing in musculoskeletal therapies that help those with musculoskeletal disorders. We also guide our patients by referring to our associated medical providers based on their examination when it’s appropriate. We find that education is the solution to asking our providers insightful questions. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
The Musculoskeletal System & Its Function
How does the musculoskeletal system play its role in the human body? The body is considered a complex being that consists of various organs, muscles, tissues, ligaments, and joints that help move a person from one place to another, resting while needed, and doing multiple activities in a casual relationship. Studies reveal that the musculoskeletal system is controlled by the central nervous system that interconnects the motor-sensory function for the body’s ability to move and rest.
The three main muscle groups that make up the musculoskeletal system are:
Skeletal muscle- Muscle tendons that are connected to the bones
Cardiac muscle- Muscles associated with the heart
Smooth muscle- Muscles that line with blood vessels and specific organs (ex. intestines)
Each muscle group provides different functions that correlate to how the body moves. Skeletal muscles make the legs and arms move. Cardiac muscles help the heart pump blood to the various muscles, organs, and tissues. Smooth muscles help specific organs (intestines, stomach, and urinary tract) digest, collect nutrients, and eliminate toxins in the body.
Issues That Affect The Musculoskeletal System
These factors are related to different issues that can not only disrupt the musculoskeletal system but can be an overlap of profiles affecting the cardiovascular system, spinal health, and gut system. The different factors that are associated with the musculoskeletal system are:
Obesity
Lack of physical activity
Poor Posture
Inflammation
Unhealthy Diet
How would various factors implicate musculoskeletal issues while triggering different bodily problems? Well, let’s use obesity as an example. Obesity is associated with issues like back and joint pain as studies reveal that these musculoskeletal issues make up pain and disability as a dominant source. A poor diet of processed foods high in fats and sugars can be associated with the risk of developing obesity.
Not only that, but obesity could potentially be involved in the thoracic spine and upper back pain due to the result of physical inactivity and poor dieting. The weight on the body can strain the muscles and ligaments in the back, causing the spinal vertebrae to become misaligned and pressure the nerves exiting the spinal cord. The misalignment of the vertebrae is called a subluxation. When a person is suffering from upper back pain, it can overlap with chest pain, which can be a concerning issue to vital organs like the heart, which potentially involved in the risk of cardiovascular disease. It is related to subluxation that may affect the heart contraction rate, rhythm, and power through the sympathetic efferent pathways originating from the thoracic region.
An Overview Of The Musculoskeletal System-Video
Are you experiencing pain in your upper back or chest? How about cardiac issues associated with shouldering and arming pain? Many of these issues are related to factors that affect the musculoskeletal system that might potentially be involved with chronic issues. The video above summarizes the musculoskeletal system’s role in the body. When environmental factors become a risk of developing musculoskeletal disorders that can potentially be involved in different bodily problems, studies reveal that musculoskeletal disorders associated with abnormal functions may cause a significant impact on regular performances. An example would be a person dealing with bad hip pain and cannot do any exercises triggering heart issues. This is defined as somato-visceral pain where the affected muscle is associated with an internal organ being a pain mediator.
Treatments For Improving Musculoskeletal System
In most treatments, many individuals utilize the following to improve not only the musculoskeletal system but other issues that affect the body:
Exercise
Healthy Diet
Stress Management Treatments
Chiropractic Therapy
No matter what affliction or health problem a person is dealing with, having the best treatment solution possible is a start on a person’s health and wellness journey. The first step is to have a precise diagnosis to the doctor while giving as much information as possible is critical. Providing them with a complete health history is an essential first step. After a manual examination of the issues causing them pain, the primary physician could refer the individual for chiropractic care to relieve issues affecting their musculoskeletal system.
Many people usually only associate chiropractic care with back problems. Still, the reality is that chiropractic therapy can be helpful for the musculoskeletal system and various issues related to the muscles and organs. A chiropractor can provide therapeutic stretches and recommend exercises to individuals to help them avoid the same problems later on. Many chiropractors offer recommendations and nutrition that individuals can utilize to help improve their condition. For the musculoskeletal system, a healthy diet may help achieve and maintain a healthy body weight while reducing the risk of chronic disease. Eating the right amount of healthy greens, fruits, beneficial carbs, and healthy fats can help reduce the risk of developing chronic issues in the body like cardiovascular diseases. However, if primary cardiac problems affect the body, it is best to seek medical attention as soon as possible.
Conclusion
The body is considered a complex being that consists of various organs, muscles, tissues, ligaments, and joints that provide various activities to the host. The musculoskeletal system has three muscle groups: skeletal, cardiac, and smooth muscles provide different functions that correlate to how the body moves. When various factors begin to cause issues to the musculoskeletal system, they can potentially be involved with pain issues that affect more than the body. Treatments like chiropractic care, a healthy diet, exercise, and stress management may be the stepping stones to alleviating various issues that are affecting the musculoskeletal system and a great start in achieving health and wellness.
References
Kennel, Peter J, et al. “Skeletal Muscle Changes in Chronic Cardiac Disease and Failure.” Comprehensive Physiology, U.S. National Library of Medicine, 20 Sept. 2015, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6752037/.
Malik, Khalid M, et al. “Musculoskeletal Disorders a Universal Source of Pain and Disability Misunderstood and Mismanaged: A Critical Analysis Based on the U.S. Model of Care.” Anesthesiology and Pain Medicine, Kowsar, 15 Dec. 2018, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6348332/.
Murphy, Andrew C, et al. “Structure, Function, and Control of the Human Musculoskeletal Network.” PLoS Biology, Public Library of Science, 18 Jan. 2018, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5773011/.
Stochkendahl, Mette J, et al. “Diagnosis and Treatment of Musculoskeletal Chest Pain: Design of a Multi-Purpose Trial.” BMC Musculoskeletal Disorders, BioMed Central, 31 Mar. 2008, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2315652/.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine