Can individuals with joint hypermobility find relief through nonsurgical treatments in reducing pain and restoring body mobility?
Introduction
When a person moves their body, the surrounding muscles, joints, and ligaments are incorporated into various tasks that allow them to stretch and be flexible without pain or discomfort. Many repetitive motions enable the individual to continue their routine. However, when the joints, muscles, and ligaments are stretched farther than normal in the upper and lower extremities without pain, it is known as joint hypermobility. This connective tissue disorder can correlate with other symptoms that affect the body and cause many people to seek treatment to manage joint hypermobility symptoms. In today’s article, we will look at joint hypermobility and how various non-surgical treatments can help reduce pain caused by joint hypermobility and restore body mobility. We talk with certified medical providers who consolidate our patients’ information to assess how their pain may be associated with joint hypermobility. We also inform and guide patients on how integrating various non-surgical treatments can help improve joint function while managing the associated symptoms. We encourage our patients to ask their associated medical providers intricate and insightful questions about incorporating non-surgical therapies as part of their routine to reduce pain and discomfort from joint hypermobility. Dr. Jimenez, D.C., includes this information as an academic service. Disclaimer.
What Is Joint Hypermobility?
Do you often feel your joints locked up in your hands, wrists, knees, and elbows? Do you experience pain and fatigue in your joints when your body feels constantly tired? Or when you stretch your extremities, do they extend farther than usual to feel the relief? Many of these various scenarios are often correlated with individuals experiencing joint hypermobility. Joint hypermobility is an inherited disorder with autosomal dominant patterns that characterize joint hyperlaxity and musculoskeletal pain within the body extremities. (Carbonell-Bobadilla et al., 2020) This connective tissue condition is often related to the flexibility of the connected tissues like ligaments and tendons in the body. An example would be if a person’s thumb is touching their inner forearm without feeling pain or discomfort, they have joint hypermobility. Additionally, many individuals dealing with joint hypermobility will often have a difficult diagnosis as they will develop skin and tissue fragility over time, causing musculoskeletal complications. (Tofts et al., 2023)
When individuals deal with joint hypermobility over time, many often have symptomatic joint hypermobility. They will present with musculoskeletal and systemic symptoms that lead to displaying skeletal deformities, tissue and skin fragility, and structural differences in the body’s system. (Nicholson et al., 2022) Some of the symptoms that joint hypermobility are shown in a diagnosis include:
Muscle pain and joint stiffness
Clicking joints
Fatigue
Digestive issues
Balance issues
Luckily, there are various treatments that many people can use to help restrengthen the surrounding muscles around the joints and reduce the correlating symptoms caused by joint hypermobility.
Movement As Medicine-Video
Nonsurgical Treatments For Joint Hypermobility
When dealing with joint hypermobility, many individuals need to seek treatments to reduce the correlating pain-like symptoms of joint hypermobility and help relieve the body’s extremities while restoring mobility. Some excellent treatments for joint hypermobility are non-surgical therapies that are non-invasive, gentle on the joints and muscles, and cost-effective. Various non-surgical treatments can be customized for the individual depending on how severe their joint hypermobility and comorbidities affect the person’s body. Non-surgical treatments can relieve the body from joint hypermobility by treating the causes of the pain through reduction and maximizing functional capacity and restoring a person’s quality of life. (Atwell et al., 2021) The three non-surgical treatments that are excellent for reducing pain from joint hypermobility and helping strengthen the surrounding muscles are below.
Chiropractic Care
Chiropractic care utilizes spinal manipulation and helps restore joint mobility in the body to reduce the effects of joint hypermobility by stabilizing the affected joints from the hypermobile extremities. (Boudreau et al., 2020) Chiropractors incorporate mechanical and manual manipulation and various techniques to help many individuals improve their posture by being more mindful of their bodies and work with multiple other therapies to emphasize controlled movements. With other comorbidities associated with joint hypermobility, like back and neck pain, chiropractic care can reduce these comorbidity symptoms and allow the individual to regain their quality of life.
Acupuncture
Another non-surgical treatment that many individuals can incorporate to reduce joint hypermobility and its comorbidities is acupuncture. Acupuncture utilizes small, thin, solid needles that acupuncturists use to block pain receptors and restore the body’s energy flow. When many individuals are dealing with joint hypermobility, their extremities in the legs, hands, and feet are in pain over time, which can cause the body to be unstable. What acupuncture does is help reduce the pain caused by joint hypermobility associated with the extremities and restore balance and functionality to the body (Luan et al., 2023). This means that if a person is dealing with stiffness and muscle pain from joint hypermobility, acupuncture can help rewire the pain by placing the needles in the body’s acupoints to provide relief.
Physical Therapy
Physical therapy is the last non-surgical treatment many people can incorporate into their daily routine. Physical therapy can help manage joint hypermobility that are tailored to help strengthen weak muscles that are surrounding the affected joints, improving a person’s stability and helping reduce the risk of dislocation. Additionally, many individuals can use low-impact exercise to ensure optimal motor control when doing regular exercises without putting excessive strain on the joints. (Russek et al., 2022)
By incorporating these three non-surgical treatments as part of a customized treatment for joint hypermobility, many individuals will begin to feel a difference in their balance. They will not experience joint pain by being more mindful of the body and incorporating small changes in their routine. Even though living with joint hypermobility can be a challenge for many individuals, by integrating and utilizing the right combination of non-surgical treatments, many can begin to lead active and fulfilling lives.
References
Atwell, K., Michael, W., Dubey, J., James, S., Martonffy, A., Anderson, S., Rudin, N., & Schrager, S. (2021). Diagnosis and Management of Hypermobility Spectrum Disorders in Primary Care. J Am Board Fam Med, 34(4), 838-848. https://doi.org/10.3122/jabfm.2021.04.200374
Boudreau, P. A., Steiman, I., & Mior, S. (2020). Clinical management of benign joint hypermobility syndrome: a case series. J Can Chiropr Assoc, 64(1), 43-54. https://www.ncbi.nlm.nih.gov/pubmed/32476667
Carbonell-Bobadilla, N., Rodriguez-Alvarez, A. A., Rojas-Garcia, G., Barragan-Garfias, J. A., Orrantia-Vertiz, M., & Rodriguez-Romo, R. (2020). [Joint hypermobility syndrome]. Acta Ortop Mex, 34(6), 441-449. https://www.ncbi.nlm.nih.gov/pubmed/34020527 (Sindrome de hipermovilidad articular.)
Luan, L., Zhu, M., Adams, R., Witchalls, J., Pranata, A., & Han, J. (2023). Effects of acupuncture or similar needling therapy on pain, proprioception, balance, and self-reported function in individuals with chronic ankle instability: A systematic review and meta-analysis. Complement Ther Med, 77, 102983. https://doi.org/10.1016/j.ctim.2023.102983
Nicholson, L. L., Simmonds, J., Pacey, V., De Wandele, I., Rombaut, L., Williams, C. M., & Chan, C. (2022). International Perspectives on Joint Hypermobility: A Synthesis of Current Science to Guide Clinical and Research Directions. J Clin Rheumatol, 28(6), 314-320. https://doi.org/10.1097/RHU.0000000000001864
Russek, L. N., Block, N. P., Byrne, E., Chalela, S., Chan, C., Comerford, M., Frost, N., Hennessey, S., McCarthy, A., Nicholson, L. L., Parry, J., Simmonds, J., Stott, P. J., Thomas, L., Treleaven, J., Wagner, W., & Hakim, A. (2022). Presentation and physical therapy management of upper cervical instability in patients with symptomatic generalized joint hypermobility: International expert consensus recommendations. Front Med (Lausanne), 9, 1072764. https://doi.org/10.3389/fmed.2022.1072764
Tofts, L. J., Simmonds, J., Schwartz, S. B., Richheimer, R. M., O’Connor, C., Elias, E., Engelbert, R., Cleary, K., Tinkle, B. T., Kline, A. D., Hakim, A. J., van Rossum, M. A. J., & Pacey, V. (2023). Pediatric joint hypermobility: a diagnostic framework and narrative review. Orphanet J Rare Dis, 18(1), 104. https://doi.org/10.1186/s13023-023-02717-2
Can individuals with herniated discs find the relief they are looking for from traction therapy or decompression to provide pain relief?
Introduction
The spine allows the individual to be mobile and flexible without feeling pain and discomfort when a person is on the move. This is because the spine is part of the musculoskeletal system that consists of muscles, tendons, ligaments, the spinal cord, and spinal discs. These components surround the spine and have three regions to allow the upper and lower extremities to do their jobs. However, the spine also ages when the body starts to age naturally. Many movements or routine actions can cause the body to be stiff and, over time, can cause the spinal disc to herniate. When this happens, a herniated disc can lead to pain and discomfort in the extremities, thus making individuals deal with a reduced quality of life and pain in three spinal regions. Luckily, there are numerous treatments, like traction therapy and decompression, to alleviate the pain and discomfort associated with herniated discs. Today’s article looks at why herniated discs cause issues in the spine and the effects of how these two treatments can help reduce herniated discs. We talk with certified medical providers who consolidate our patients’ information to assess how a herniated disc in the spine may be the issue causing musculoskeletal pain. We also inform and guide patients on how integrating spinal decompression and traction therapy can help realign the spine and reduce disc herniation that is causing spinal issues. We encourage our patients to ask their associated medical providers intricate and important questions about incorporating non-surgical treatments as part of their routine to reduce pain and discomfort in their bodies. Dr. Jimenez, D.C., includes this information as an academic service. Disclaimer.
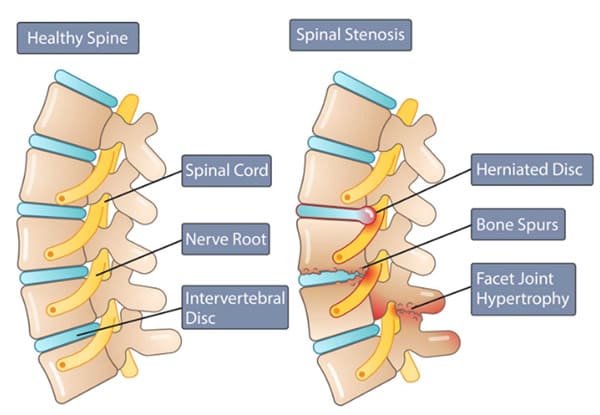
Why Herniated Discs Causes Issues In The Spine?
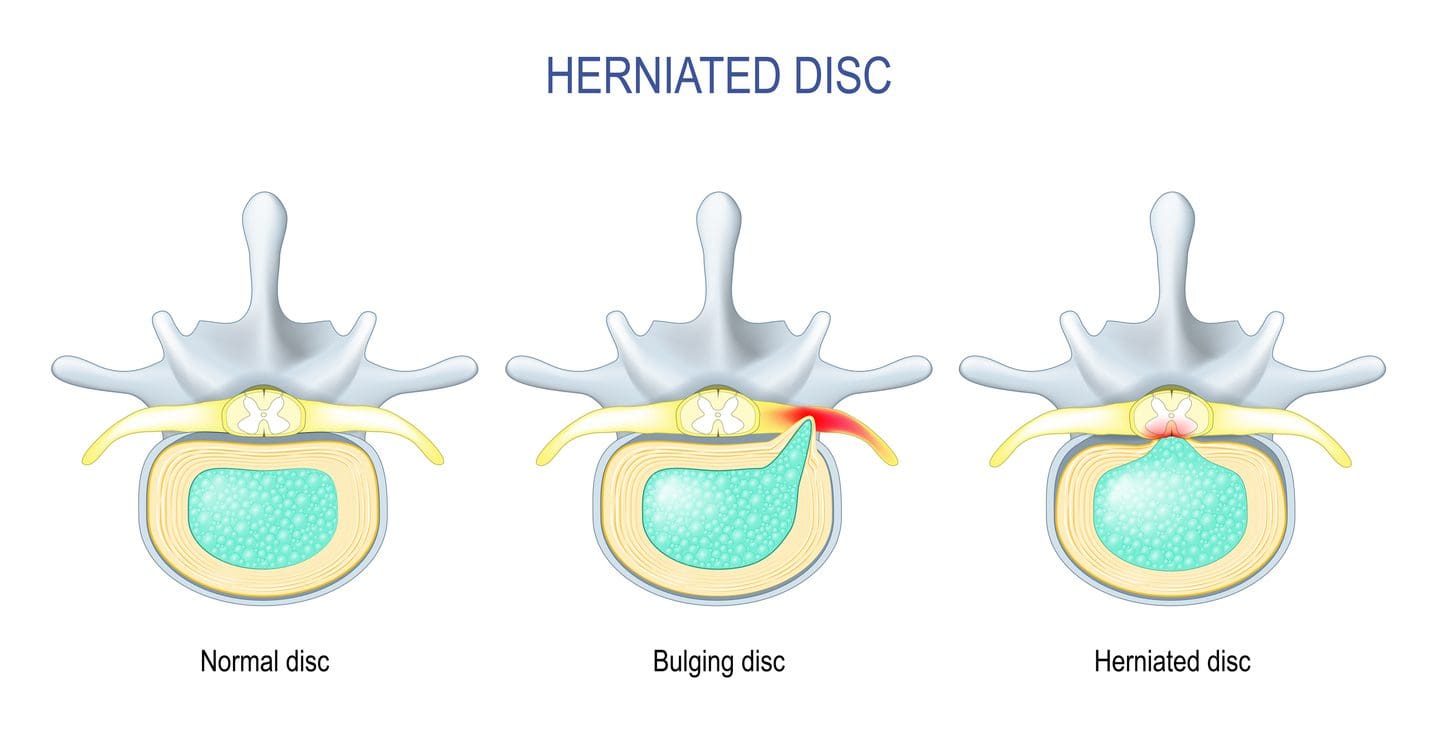
Have you been experiencing constant discomfort in your neck or back that doesn’t allow you to relax? Do you feel tingling sensations in your upper and lower extremities, making grasping objects or walking difficult? Or have you noticed that you are hunching over from your desk or standing and that stretching causes pain? As the spine keeps the body upright, its main components include the moveable vertebrae, the nerve root fibers, and spinal discs to help send neuron signals to the brain to allow movement, cushion the shocked forces on the spine, and be flexible. The spine allows the individual to perform various tasks without pain and discomfort through repetitive movements. However, when the body ages, it can lead to degenerative changes in the spine, causing the spinal disc to herniate over time. A herniated disc is a common degenerative musculoskeletal condition that causes the nucleus pulposus to break through any weak region of the annulus fibrosus and compress the surrounding nerve roots. (Ge et al., 2019) Other times, when repetitive motions start to cause a developing herniated disc, the inner portion of the disc can become desiccated and brittle. In contrast, the outer portion becomes more fibrotic and less elastic, causing the disc to shrink and be narrow. A herniated disc can affect young and old populations as they can have a multifactorial contribution that causes proinflammatory changes to the body. (Wu et al., 2020)
When many people are dealing with pain associated with a herniated disc, the disc itself goes through morphological change through the characterization of the disc being partial damage, which is then followed by the displacement and herniation of the inner disc portion in the vertebral canal to compress the spinal nerve roots. (Diaconu et al., 2021) This causes symptoms of pain, numbness, and weakness in the upper and lower body portions through nerve impingement. Hence why, many individuals are dealing with referred pain symptoms from their arms and legs that are radiating pain. When nerve compression associated with herniated discs starts to cause pain and discomfort, many individuals begin to seek out treatment to reduce the pain that the herniated disc is causing to provide relief for their bodies.
Spinal Decompression In Depth-Video
The Effects Of Traction Therapy In Reducing Herniated Disc
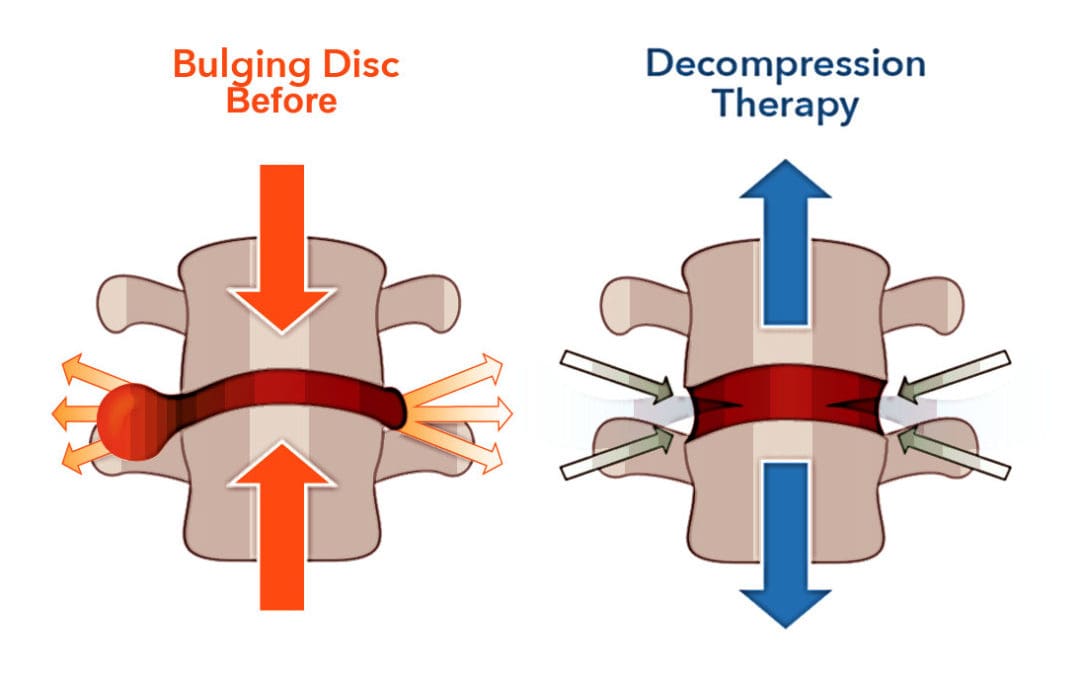
Many people who are suffering from pain that is being affected by herniated discs in their spines can seek out treatments like traction therapy to alleviate pain. Traction therapy is a non-surgical treatment that stretches and mobilizes the spine. Traction therapy can be mechanically or manually done by a pain specialist or with the help of mechanical devices. The effects of traction therapy can reduce the compression force on the spinal disc while reducing nerve root compression by expanding the disc height within the spine. (Wang et al., 2022) This allows the surrounding joints within the spine to be mobile and positively affect the spine. With traction therapy, intermittent or steady tension forces help stretch the spine, reduce pain, and improve functional outcomes. (Kuligowski et al., 2021)
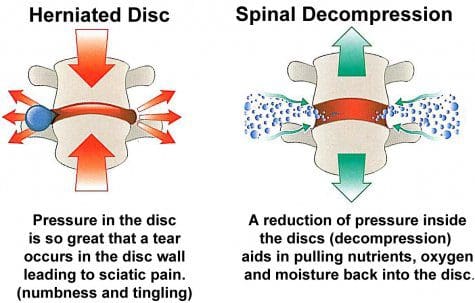
The Effects Of Spinal Decompression In Reducing Herniated Disc
Another form of non-surgical treatment is spinal decompression, a sophisticated version of traction that uses computerized technology to help apply controlled, gentle pulling forces to the spine. Spinal decompression does is that it can help decompress the spinal canal and help pull the herniated disc back to its original position while stabilizing the spine and keeping the vital bones and soft tissues safe. (Zhang et al., 2022) Additionally, spinal decompression can create negative pressure on the spine to allow the flow of nutritional fluids and blood oxygen back to the discs while creating an inverse relationship when tension pressure is introduced. (Ramos & Martin, 1994) Both spinal decompression and traction therapy can offer many therapeutic pathways to provide relief to many individuals dealing with herniated discs. Depending on how severe the herniated disc has caused issues to the person’s spine, many can rely on non-surgical treatments due to its customizable plan that is personalized to the person’s pain and can be combined with other therapies to strengthen the surrounding muscles. By doing so, many people can be pain-free over time while being mindful of their bodies.
References
Diaconu, G. S., Mihalache, C. G., Popescu, G., Man, G. M., Rusu, R. G., Toader, C., Ciucurel, C., Stocheci, C. M., Mitroi, G., & Georgescu, L. I. (2021). Clinical and pathological considerations in lumbar herniated disc associated with inflammatory lesions. Rom J Morphol Embryol, 62(4), 951-960. https://doi.org/10.47162/RJME.62.4.07
Ge, C. Y., Hao, D. J., Yan, L., Shan, L. Q., Zhao, Q. P., He, B. R., & Hui, H. (2019). Intradural Lumbar Disc Herniation: A Case Report and Literature Review. Clin Interv Aging, 14, 2295-2299. https://doi.org/10.2147/CIA.S228717
Kuligowski, T., Skrzek, A., & Cieslik, B. (2021). Manual Therapy in Cervical and Lumbar Radiculopathy: A Systematic Review of the Literature. Int J Environ Res Public Health, 18(11). https://doi.org/10.3390/ijerph18116176
Ramos, G., & Martin, W. (1994). Effects of vertebral axial decompression on intradiscal pressure. J Neurosurg, 81(3), 350-353. https://doi.org/10.3171/jns.1994.81.3.0350
Wang, W., Long, F., Wu, X., Li, S., & Lin, J. (2022). Clinical Efficacy of Mechanical Traction as Physical Therapy for Lumbar Disc Herniation: A Meta-Analysis. Comput Math Methods Med, 2022, 5670303. https://doi.org/10.1155/2022/5670303
Wu, P. H., Kim, H. S., & Jang, I. T. (2020). Intervertebral Disc Diseases PART 2: A Review of the Current Diagnostic and Treatment Strategies for Intervertebral Disc Disease. Int J Mol Sci, 21(6). https://doi.org/10.3390/ijms21062135
Zhang, Y., Wei, F. L., Liu, Z. X., Zhou, C. P., Du, M. R., Quan, J., & Wang, Y. P. (2022). Comparison of posterior decompression techniques and conventional laminectomy for lumbar spinal stenosis. Front Surg, 9, 997973. https://doi.org/10.3389/fsurg.2022.997973
Can individuals with spinal pain in their necks and back utilize decompression therapy to restore spinal disc height and find relief?
Introduction
Many people don’t realize that as the body gets older, so does the spine. The spine is part of the musculoskeletal system that provides structural support to the body by keeping it upright. The surrounding muscles, ligaments, and tissues surrounding the spine help with stability and mobility, while the spinal disc and joints provide shock absorption from the sheer vertical weight. When a person is on the move with their daily activities, the spine can allow the individual to be mobile without pain or discomfort. However, as time passes, the spine goes through degenerative changes that can cause pain and discomfort to the body, thus leaving the individual to deal with overlapping risk profiles that can affect their neck and back. To that point, many people seek out treatments to reduce the pain affecting their spine and restore the disc height in their bodies. Today’s article looks at how spinal pain affects a person’s neck and back and how treatments like spinal decompression can reduce spinal pain and restore disc height. We talk with certified medical providers who consolidate our patients’ information to assess how spinal pain can significantly impact a person’s well-being and quality of life in their bodies. We also inform and guide patients on how integrating spinal decompression can help reduce spinal pain and restore spinal disc height. We encourage our patients to ask their associated medical providers intricate and important questions about incorporating non-surgical treatments into a health and wellness routine to relieve spinal pain and regain their quality of life. Dr. Jimenez, D.C., includes this information as an academic service. Disclaimer.
How Spinal Pain Affects A Person’s Neck & Back
Do you feel constant muscle aches and pains in your neck and back? Have you experienced stiffness and limited mobility when you are twisting and turning? Or do heavy objects cause muscle strain when moving from one location to another? Many individuals will be on the move and be in weird positions without feeling pain and discomfort when it comes to the spine. This is due to the surrounding muscles and tissues being stretched and the spinal discs taking on the vertical pressure on the spine. However, when environmental factors, traumatic injuries, or natural aging start to affect the spine, it can lead to the development of spinal pain. This is because the outer portion of the spinal disc is intact, and the inner portion of the disc is being affected. When abnormal stresses start to reduce the water intake within the disc, it can internally stimulate the pain receptors without nerve root symptoms inside the disc. (Zhang et al., 2009) This causes many individuals to deal with neck and back pain in their bodies and reduces their quality of life.
Spinal pain can lead to overlapping risk profiles that cause many individuals to deal with severe low back pain and neck pain, which then causes the surrounding muscles to become weak, tight, and overstretched. At the same time, the surrounding nerve roots are also affected as the nerve fibers surround the outer and inner parts of the spinal disc, which causes nociceptive pain properties to the neck and back region and leads to discogenic pain. (Coppes et al., 1997) When many individuals are dealing with muscle pain correlated with the spinal discs, it causes a pain-spasm-pain cycle that can affect their bodies due to not moving enough and causing painful muscular activities when trying to be mobile. (Roland, 1986) When a person has limited mobility cause they are experiencing spinal pain, their natural disc height slowly degenerates, causing more issues to their bodies and socioeconomic burdens. Fortunately, when many individuals are dealing with spinal pain, numerous treatments can reduce spinal pain and restore their disc height.
Movement Medicine- Video
How Spinal Decompression Reduces Spinal Pain
When people are seeking treatments for their spinal pain, many will seek surgical treatments to reduce their pain, but it will be a bit pricey. However, many individuals will opt for non-surgical treatments due to their affordability. Non-surgical treatments are cost-effective and customizable to a person’s pain and discomfort. From chiropractic care to acupuncture, depending on the severity of the person’s pain, many will find the relief they seek. One of the most innovative treatments for reducing spinal pain is spinal decompression. Spinal decompression allows the individual to be strapped into a traction table. This is because it gently pulls on the spine to realign the spinal disc by reducing the pressure on the spine to invoke the body’s natural healing process to relieve pain. (Ramos & Martin, 1994) Additionally, when many individuals are using spinal decompression, the gentle traction provides a motorized distraction to the spine that may induce physical changes to the spinal disc and help restore a person’s range of motion, flexibility, and mobility. (Amjad et al., 2022)
Spinal Decompression Restoring Spinal Disc Height
When a person is being strapped into the spinal decompression machine, the gentle traction helps the spinal disc return to the spine, allowing the fluids and nutrients to rehydrate the spine, increasing the spine’s disc height. This is because spinal decompression creates negative pressure on the spine, allowing the spinal disc to return to its original height and providing relief. Plus, the amazing thing that spinal decompression does is that it can be combined with physical therapy to help stretch and strengthen the surrounding muscles near the spine to provide more stability and flexibility. (Vanti et al., 2023) This allows the individual to be more mindful of their bodies and start incorporating small habit changes to reduce the pain from returning. When many people begin to think about their health and wellness by going to treatment, they will regain their quality of life and get back to their daily routine without the issues affecting their spine.
References
Amjad, F., Mohseni-Bandpei, M. A., Gilani, S. A., Ahmad, A., & Hanif, A. (2022). Effects of non-surgical decompression therapy in addition to routine physical therapy on pain, range of motion, endurance, functional disability and quality of life versus routine physical therapy alone in patients with lumbar radiculopathy; a randomized controlled trial. BMC Musculoskelet Disord, 23(1), 255. https://doi.org/10.1186/s12891-022-05196-x
Coppes, M. H., Marani, E., Thomeer, R. T., & Groen, G. J. (1997). Innervation of “painful” lumbar discs. Spine (Phila Pa 1976), 22(20), 2342-2349; discussion 2349-2350. https://doi.org/10.1097/00007632-199710150-00005
Ramos, G., & Martin, W. (1994). Effects of vertebral axial decompression on intradiscal pressure. J Neurosurg, 81(3), 350-353. https://doi.org/10.3171/jns.1994.81.3.0350
Roland, M. O. (1986). A critical review of the evidence for a pain-spasm-pain cycle in spinal disorders. Clin Biomech (Bristol, Avon), 1(2), 102-109. https://doi.org/10.1016/0268-0033(86)90085-9
Vanti, C., Saccardo, K., Panizzolo, A., Turone, L., Guccione, A. A., & Pillastrini, P. (2023). The effects of the addition of mechanical traction to physical therapy on low back pain? A systematic review with meta-analysis. Acta Orthop Traumatol Turc, 57(1), 3-16. https://doi.org/10.5152/j.aott.2023.21323
Zhang, Y. G., Guo, T. M., Guo, X., & Wu, S. X. (2009). Clinical diagnosis for discogenic low back pain. Int J Biol Sci, 5(7), 647-658. https://doi.org/10.7150/ijbs.5.647
Can individuals dealing with muscle pain find relief from acupuncture therapy to get back to their daily activities and well-being?
Introduction
Many people worldwide have dealt with pain in their musculoskeletal system that has affected their daily routine. Some of the most common factors that people have experienced muscle pain include sedentary lifestyles from working at a desk job or physical demands from an active lifestyle. The muscles, tendons, ligaments, and soft tissues can become overstretched and overworked, causing the muscles to become weak. At the same time, visceral somatic issues in the neck, shoulders, and back can affect the upper and lower extremities, leading to a life of disability. Many factors that can contribute to the development of muscle pain can impact a person’s routine and cause them to find various techniques to reduce the muscle pain in their bodies. Since muscle pain can be in acute or chronic form, many individuals who are seeking treatment for their ailments can look into non-surgical therapies like acupuncture to not only reduce muscle pain but also find the relief they are looking for. Today’s article focuses on how muscle pain can affect a person’s well-being, how the essence of acupuncture can be beneficial for muscle pain, and how people can integrate acupuncture therapy as part of a wellness routine. We talk with certified medical providers who consolidate our patients’ information to assess how muscle pain can impact a person’s well-being. We also inform and guide patients on how acupuncture therapy can benefit the body by reducing the effects of muscle pain. We encourage our patients to ask their associated medical providers intricate and important questions about incorporating acupuncture therapy into a wellness routine to reduce muscle pain and its referred symptoms. Dr. Jimenez, D.C., includes this information as an academic service. Disclaimer.
How Muscle Pain Can Affect A Person’s Well-Being
Do you feel the effects of tiredness and weakness in your upper and lower extremity muscles? Have you experienced general soreness or aches in your neck, shoulders, or back? Or does twisting and turning your body cause temporary relief to your body, only for it to be worse throughout the day? When it comes to muscle pain can be a multi-factorial condition where that can involve complex interactions on a person’s structure, physical, social, lifestyle, and comorbid health factors that can come into play as contributing factors for people to experience long-term pain and disability. (Caneiro et al., 2021) As many individuals start to do repetitive motions or stay in sedentary positions, muscle pain can develop when they stretch or try to move their muscles while doing their routine. The burden of muscle pain often correlates with socioeconomic factors that can cause many people, both young and old, to substantially limit their mobility and engagement in their routine, which predisposes increased risk factors to other chronic conditions they may have. (Dzakpasu et al., 2021)
When many individuals are dealing with muscle pain in its acute or chronic form, many often don’t realize that when the affected muscles in the upper and lower body quadrants are coping with pain, there is associated pain and stiffness from how active or inactive the muscles are can affect the soft tissue causing high mechanical stress to the affect the skeletal joints. (Wilke & Behringer, 2021) When this happens, many people will start to experience referred muscle pain in their bodies, causing issues with their mobility, flexibility, and stability. Coincidentally, muscle pain can also be a symptom of many people who have various pains in their bodies that have impacted their lives prior; seeking treatment can reduce the effects of muscle pain and help them take back their routine to lead a healthier lifestyle.
Movement Medicine- Video
The Essence Of Acupuncture For Muscle Pain
When many people are dealing with muscle pain, they are seeking treatments that are not only affordable but also can be effective in reducing the overlapping risk profiles that are affecting the body, causing muscle pain. Many treatments like chiropractic care, decompression, and massage therapy are non-surgical and are effective through consecutive sessions. One of the oldest and most effective treatments that can help reduce muscle pain in the body is acupuncture therapy. Acupuncture is a holistic treatment derived from Traditional Chinese Medicine that utilizes small, solid, thin needles inserted by professional acupuncturists to various acupoints. The main philosophy is that acupuncture provides relief to the body as it helps improve the body’s energy flow while maintaining a person’s overall health and vitality. (Zhang et al., 2022) When a person is dealing with muscle pain, the muscle fibers can develop tiny nodules known as trigger points that can induce pain in the affected muscle quadrants. With acupuncture needles placed in the affected area, local and referred pain is reduced, muscle blood flow and oxygen are returned to the body, and the muscle’s range of motion is improved. (Pourahmadi et al., 2019) Some of the benefits that acupuncture therapy provides include:
Increased circulation
Inflammation reduction
Endorphin release
Relaxing muscle tension
Integrating Acupuncture As Part Of A Wellness Routine
Many individuals who are seeking acupuncture therapy as part of their wellness journey can see the positive benefits of acupuncture and can combine it with other therapies to reduce the chances of muscle pain from returning. While acupuncture can help stimulate the nerves and restore motor function, treatments like joint mobilization can help stretch the affected muscles and joints to improve the body’s range of motion. (Lee et al., 2023) With many individuals seeking acupuncture treatment to reduce muscle pain, many can make small changes in their routine to prevent the pain from causing overlapping risk profiles to their bodies. When addressing the root causes of pain and promoting the body’s innate healing abilities, acupuncture can help restore balance, alleviate discomfort, and enhance overall well-being.
References
Caneiro, J. P., Bunzli, S., & O’Sullivan, P. (2021). Beliefs about the body and pain: the critical role in musculoskeletal pain management. Braz J Phys Ther, 25(1), 17-29. https://doi.org/10.1016/j.bjpt.2020.06.003
Dzakpasu, F. Q. S., Carver, A., Brakenridge, C. J., Cicuttini, F., Urquhart, D. M., Owen, N., & Dunstan, D. W. (2021). Musculoskeletal pain and sedentary behaviour in occupational and non-occupational settings: a systematic review with meta-analysis. Int J Behav Nutr Phys Act, 18(1), 159. https://doi.org/10.1186/s12966-021-01191-y
Lee, J. E., Akimoto, T., Chang, J., & Lee, H. S. (2023). Effects of joint mobilization combined with acupuncture on pain, physical function, and depression in stroke patients with chronic neuropathic pain: A randomized controlled trial. PLOS ONE, 18(8), e0281968. https://doi.org/10.1371/journal.pone.0281968
Pourahmadi, M., Mohseni-Bandpei, M. A., Keshtkar, A., Koes, B. W., Fernandez-de-Las-Penas, C., Dommerholt, J., & Bahramian, M. (2019). Effectiveness of dry needling for improving pain and disability in adults with tension-type, cervicogenic, or migraine headaches: protocol for a systematic review. Chiropr Man Therap, 27, 43. https://doi.org/10.1186/s12998-019-0266-7
Wilke, J., & Behringer, M. (2021). Is “Delayed Onset Muscle Soreness” a False Friend? The Potential Implication of the Fascial Connective Tissue in Post-Exercise Discomfort. Int J Mol Sci, 22(17). https://doi.org/10.3390/ijms22179482
Zhang, B., Shi, H., Cao, S., Xie, L., Ren, P., Wang, J., & Shi, B. (2022). Revealing the magic of acupuncture based on biological mechanisms: A literature review. Biosci Trends, 16(1), 73-90. https://doi.org/10.5582/bst.2022.01039
Can individuals with lumbar spinal stenosis utilize spinal decompression to reduce low back pain and restore mobility?
Introduction
Many individuals worldwide have dealt with low back pain at some point in their lives that has affected their mobility and impacted their routine. Numerous environmental factors can lead to low back pain development, like improper heavy lifting, poor posture, traumatic injuries, and accidents that can affect the surrounding muscles, spinal cord, and nerve roots. When this happens, it can lead to lumbar spinal stenosis and cause overlapping risk profiles that are correlated with low back pain. When people are dealing with lumbar spinal stenosis, they could be thinking that their pain is in the lower extremities. To that point, many individuals seek treatment to not only reduce low back pain but also reduce the effects of lumbar spinal stenosis. Some treatments, like spinal decompression, which is a non-surgical treatment, can help restore mobility to the body. Today’s article looks at how lumbar spinal stenosis affects the lower back and its diagnosis while looking at how spinal decompression can provide relief to the individual and have positive benefits in restoring mobility. We talk with certified medical providers who consolidate our patients’ information to assess how lumbar spinal stenosis correlates with lower back pain, causing mobility issues. We also inform and guide patients on how spinal decompression is an excellent form of treatment that can be combined with other therapies. We encourage our patients to ask their associated medical providers intricate and important questions about incorporating decompression therapy to relieve the pain effects caused by lumbar stenosis while reducing the overlapping pain effects like lower back pain to regain a person’s mobility. Dr. Jimenez, D.C., includes this information as an academic service. Disclaimer.
How Lumbar Spinal Stenosis Affects the Lower Back
Do you feel tingling sensations in the back of your legs affecting your ability to move around? Or does your lower back feel less mobile than it is used to? When many individuals are experiencing low back pain during their lifetime, it can often correlate with lumbar spinal stenosis. Lumbar spinal stenosis usually occurs when the spinal canal in the lower back becomes constricted, leading to degenerative changes. When the spinal canal starts to narrow in the spine, it can cause significant discomfort, interfere with daily activities, and may result in progressive disability for many individuals. (Munakomi et al., 2024) The symptoms caused by lumbar spinal stenosis range from mild to severe, and on which environmental factors correspond to the issue. At the same time, lumbar spinal stenosis is characterized by symptoms like low back pain that can cause spondylotic changes that induce low back pain that can negatively impact a person’s quality of life. (Ogon et al., 2022) This causes many people to go to their primary doctors to get a diagnosis and learn how to manage the pain associated with lumbar spinal stenosis.
The Diagnosis Of Lumbar Spinal Stenosis
When it comes to diagnosing lumbar spinal stenosis, many healthcare providers will incorporate a comprehensive evaluation, which includes a physical examination to see how mobile a person’s back is and imaging testing like MRIs and CT scans to visualize the spinal canal and assess the extent of the narrowing that is causing pain in the lower extremities. This is because when individuals deal with lumbar spinal stenosis, it can manifest with neurogenic claudication in the lower extremities, especially when a person is standing or sitting. The pain is decreased when their position is changed. (Sobanski et al., 2023) Additionally, lumbar spinal stenosis is one of the most commonly diagnosed spinal disorders that many healthcare professionals assess and evaluate. When there is a narrowing in the spinal canal, leading to the development of lumbar spinal, simple motions like walking can exacerbate the symptoms to the lower extremities and increase the oxygen in the spinal nerves, which may exceed the available blood flow to the extremities. (Deer et al., 2019) To that point, treatments like spinal decompression can help reduce lower back pain associated with lumbar spinal stenosis.
The Non-Surgical Approach To Wellness- Video
A Path To Relief Using Spinal Decompression
When it comes to individuals experiencing the pain caused by lumbar spinal stenosis, many individuals can seek out non-surgical treatments like spinal decompression to relieve lower back pain. Spinal decompression has emerged as a non-invasive, effective treatment option for lumbar spinal stenosis. It utilizes gentle mechanical traction on the spine to be stretched, relieving the spinal nerves by creating more space within the spinal canal. Spinal decompression decreases the degenerative process while the surrounding muscles are gently stretched, and the spinal disc height increases due to negative pressure. (Kang et al., 2016)
The Benefits Of Spinal Decompression & Restoring Mobility
Additionally, the gentle traction from spinal decompression helps enhance the production flow of nutrients and oxygen back to the affected spinal discs and spine to foster a better healing environment for the body. Since spinal decompression can be combined with other non-surgical treatments, like physical therapy and spinal manipulation, it can provide long-lasting positive effects for individuals with lumbar spinal stenosis. (Ammendolia et al., 2022) Some of the beneficial results of spinal decompression include:
Pain relief by alleviating pressure off the spinal nerves to reduce pain and discomfort in the lower extremities significantly.
Improved mobility allows the individual to return to their daily activities with ease.
Many people can benefit from spinal decompression to reduce the effects of lumbar spinal stenosis and have their lower extremity mobility restored after consecutive sessions to reduce the chances of the pain from coming back. By thinking more about their health and wellness, many people can make small routine changes in their activities to mitigate the pain and remain mobile throughout their lives. This allows them to have a sense of hope to relieve them from the pain they have been under.
References
Ammendolia, C., Hofkirchner, C., Plener, J., Bussieres, A., Schneider, M. J., Young, J. J., Furlan, A. D., Stuber, K., Ahmed, A., Cancelliere, C., Adeboyejo, A., & Ornelas, J. (2022). Non-operative treatment for lumbar spinal stenosis with neurogenic claudication: an updated systematic review. BMJ Open, 12(1), e057724. https://doi.org/10.1136/bmjopen-2021-057724
Deer, T., Sayed, D., Michels, J., Josephson, Y., Li, S., & Calodney, A. K. (2019). A Review of Lumbar Spinal Stenosis with Intermittent Neurogenic Claudication: Disease and Diagnosis. Pain Med, 20(Suppl 2), S32-S44. https://doi.org/10.1093/pm/pnz161
Kang, J. I., Jeong, D. K., & Choi, H. (2016). Effect of spinal decompression on the lumbar muscle activity and disk height in patients with herniated intervertebral disk. Journal of Physical Therapy Science, 28(11), 3125-3130. https://doi.org/10.1589/jpts.28.3125
Ogon, I., Teramoto, A., Takashima, H., Terashima, Y., Yoshimoto, M., Emori, M., Iba, K., Takebayashi, T., & Yamashita, T. (2022). Factors associated with low back pain in patients with lumbar spinal stenosis: a cross-sectional study. BMC Musculoskelet Disord, 23(1), 552. https://doi.org/10.1186/s12891-022-05483-7
Sobanski, D., Staszkiewicz, R., Stachura, M., Gadzielinski, M., & Grabarek, B. O. (2023). Presentation, Diagnosis, and Management of Lower Back Pain Associated with Spinal Stenosis: A Narrative Review. Med Sci Monit, 29, e939237. https://doi.org/10.12659/MSM.939237
Can individuals dealing with joint pain incorporate acupuncture therapy to manage lupus symptoms and restore body mobility?
Introduction
The immune system is highly important to the body as its main job is to protect vital structures from foreign invaders that can cause pain-like issues and discomfort. The immune system has a healthy relationship with the different body systems, including the musculoskeletal system, as the inflammatory cytokines help heal muscle and tissue damage when the body is injured. Over time, however, when normal environmental and genetic factors start to develop in the body, the immune system will begin to send out these cytokines to healthy, normal cells. To that point, the body starts at risk of developing autoimmune diseases. Now, autoimmune diseases in the body can cause havoc over time when they are not managed, leading to chronic disorders that can cause overlapping symptoms in the musculoskeletal system. One of the most common autoimmune diseases is systemic lupus erythematosus or lupus, and it can cause a person to be in consistent pain and discomfort while correlating with muscle and joint pain. Today’s article looks at the factors and effects of lupus, the burden of joint pain in lupus, and how holistic approaches like acupuncture can help manage lupus while restoring body mobility. We talk with certified medical providers who consolidate our patients’ information to assess how to minimize the pain effects caused by lupus on the joints. We also inform and guide patients on how acupuncture can help manage lupus and combine other therapies to reduce its pain-like symptoms affecting the musculoskeletal system. We encourage our patients to ask their associated medical providers intricate and important questions about incorporating acupuncture therapy to relieve the inflammatory effects of lupus while finding natural ways to restore mobility. Dr. Jimenez, D.C., includes this information as an academic service. Disclaimer.
The Factors & Effects Of Lupus
Have you been experiencing joint pain in your upper or lower extremities, making it difficult to function throughout the day? Have you been feeling the constant effects of fatigue? Many individuals experiencing these pain-like issues could risk developing systemic lupus erythematosus. In this autoimmune disease, the body’s own immune system mistakenly starts to attack its tissues, thus leading to inflammation and a range of pain-like symptoms. Lupis is tricky to diagnose because of its complex immune dysregulation that can lead to an overproduction of cytokines that can affect the body. (Lazar & Kahlenberg, 2023) At the same time, lupus can affect a diverse population, with symptoms and severity varying depending on how mild or severe the factors affect the body. Lupus can impact various body parts, including the joints, skin, kidneys, blood cells, and other vital body parts and organs, as environmental and hormonal factors can influence its development. (Tsang & Bultink, 2021) Additionally, lupus can be closely associated with other comorbidities that are causing overlapping risk profiles with inflammation that can affect the joints in the musculoskeletal system.
The Burden of Joint Pain In Lupus
Lupus is tricky to diagnose since it often mimics other ailments; the most common pain symptom that lupus affects is the joints. Individuals with lupus experience joint pain, which can cause inflammatory effects and structural damage to the joints, tendons, muscles, and bones, causing pathological abnormalities. (Di Matteo et al., 2021) Since lupus causes inflammatory effects in the joints, many individuals will think that they are experiencing inflammatory arthritis, and it can cause overlapping risk profiles as it is accompanied by lupus, thus causing localized pain in the joints regardless of its origin. (Senthelal et al., 2024) Joint pain in lupus individuals can significantly hinder daily activities, reducing mobility and overall quality of life as they are trying to find relief.
Unlocking The Secrets of Inflammation-Video
A Holistic Approach to Managing Lupus
While standard treatments for lupus involve medication and immunosuppressants to reduce the inflammation caused by lupus, many people want to seek out holistic approaches to manage lupus and reduce the inflammatory effects from affecting their joints by making small changes in their lives. Many people incorporate anti-inflammatory foods rich in antioxidants to dampen the inflammatory effects. Various supplements, like vitamin D, calcium, zinc, etc., can help reduce inflammation caused by lupus and strengthen bone health. Additionally, non-surgical treatments can even improve cardiorespiratory capacity and decrease fatigue while improving psychological function, which can help improve a person’s quality of life by managing the symptoms caused by lupus. (Fangtham et al., 2019)
How Acupuncture Could Help Lupus & Restore Mobility
One of the oldest forms of non-surgical and holistic approaches to reducing inflammation and managing lupus is acupuncture. Acupuncture involves solid, thin needles used by highly trained professionals to be inserted into specific body points to balance the body’s qi (energy) by stimulating the nervous system and releasing beneficial chemicals into the affected muscles, spinal cord, and brain. Additionally, acupuncture, with its minimal side effects and holistic approach, can help manage lupus. This is because when acupuncture needles are placed at the acupoints of the body, it can disrupt the pain signals that are causing pain in the affected area and regulate the inflammatory cytokines from lupus to provide relief. (Wang et al., 2023) This is due to its philosophy of addressing not only the physical pain but also the emotional and psychological symptoms of living with a chronic condition like lupus.
Additionally, acupuncture can help restore joint mobility while managing lupus through consecutive treatments, as many people notice that their joint mobility is improved and their pain is diminished. This is because the insertion and manipulation of the needles in the body’s acupoints cause alterations in afferent sensory input to the central nervous system, which increases alpha motoneuron excitability and reduces inflammation. (Kim et al., 2020) When individuals are dealing with lupus and are trying to find alternative holistic methods to relieve inflammation and joint pain caused by lupus, acupuncture, and non-surgical treatments can offer a ray of hope in managing the daily challenges of lupus.
References
Di Matteo, A., Smerilli, G., Cipolletta, E., Salaffi, F., De Angelis, R., Di Carlo, M., Filippucci, E., & Grassi, W. (2021). Imaging of Joint and Soft Tissue Involvement in Systemic Lupus Erythematosus. Curr Rheumatol Rep, 23(9), 73. https://doi.org/10.1007/s11926-021-01040-8
Fangtham, M., Kasturi, S., Bannuru, R. R., Nash, J. L., & Wang, C. (2019). Non-pharmacologic therapies for systemic lupus erythematosus. Lupus, 28(6), 703-712. https://doi.org/10.1177/0961203319841435
Kim, D., Jang, S., & Park, J. (2020). Electroacupuncture and Manual Acupuncture Increase Joint Flexibility but Reduce Muscle Strength. Healthcare (Basel), 8(4). https://doi.org/10.3390/healthcare8040414
Tsang, A. S. M. W. P., & Bultink, I. E. M. (2021). New developments in systemic lupus erythematosus. Rheumatology (Oxford), 60(Suppl 6), vi21-vi28. https://doi.org/10.1093/rheumatology/keab498
Wang, H., Wang, B., Huang, J., Yang, Z., Song, Z., Zhu, Q., Xie, Z., Sun, Q., & Zhao, T. (2023). Efficacy and safety of acupuncture therapy combined with conventional pharmacotherapy in the treatment of systemic lupus erythematosus: A systematic review and meta-analysis. Medicine (Baltimore), 102(40), e35418. https://doi.org/10.1097/MD.0000000000035418
Can individuals with thoracic outlet syndrome incorporate electroacupuncture to reduce neck pain and restore proper posture?
Introduction
More times throughout the world, many individuals have experienced pain around their necks, which can lead to pain and discomfort. Many environmental factors, like being in a hunched position while looking at the computer or phone, traumatic injuries, poor posture, or spinal issues, can cause pain-like symptoms and complications to the body. Since neck pain is a common complaint many people suffer, symptoms like tingling, numbness, or muscle weakness in the upper extremities can lead to comorbidities. When this happens, it can lead to the development of a complex condition known as thoracic outlet syndrome or TOS. Today’s article looks at the link between thoracic outlet syndrome and neck pain, how to manage TOS while alleviating neck pain, and how electroacupuncture can help with TOS. We talk with certified medical providers who consolidate our patients’ information to assess how to minimize the effects of TOS while reducing neck pain. We also inform and guide patients on how electroacupuncture can help manage TOS. We encourage our patients to ask their associated medical providers intricate and important questions about incorporating electroacupuncture to alleviate TOS associated with the neck. Dr. Jimenez, D.C., includes this information as an academic service. Disclaimer.
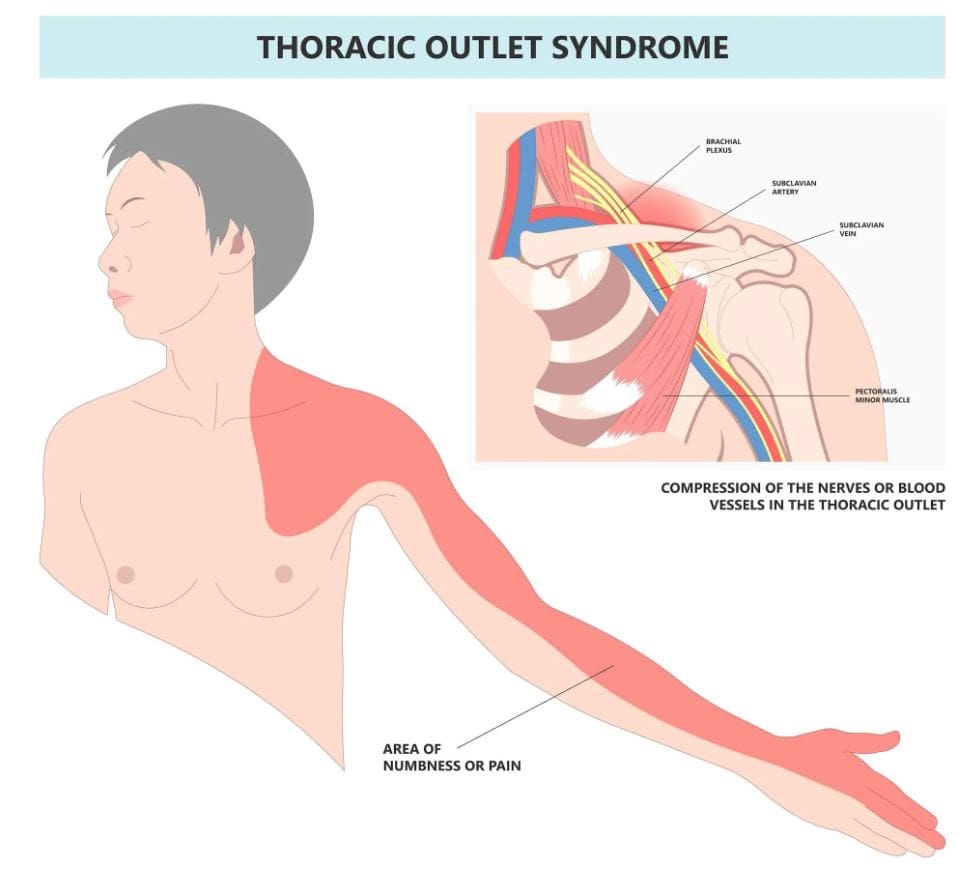
The Link Between Thoracic Outlet Syndrome & Neck Pain
Have you been noticing how you are hunched over more than usual? Do you experience symptoms of tingling or numbness down from your arms to your hands? Or do you feel muscle tension in your neck? Thoracic outlet syndrome, or TOS, is a challenging condition resulting in the compression of neurovascular structures between the clavicle and the first rib. (Masocatto et al., 2019) These neurovascular structures are near the neck and shoulders. When environmental structures affect the upper extremities, it can lead to referred neck pain, which can cause overlapping risk profiles. Some of the factors that TOS can contribute to neck pain include:
Atomical variations
Poor posture
Repetitive motions
Traumatic injuries
At the same time, people with neck pain can develop TOS, as neck pain is a multifactorial musculoskeletal condition that can be associated with overlapping risk profiles that contribute to TOS. (Kazeminasab et al., 2022) As stated earlier, factors like poor posture can overstretch the neck muscles and the neurovascular structures, leading to neuropathic pain symptoms that can cause deep aching referred pain to the neck and muscle weakness. (Childress & Stuek, 2020) When this happens, many people will begin to feel miserable and start to seek treatment to not only reduce TOS but also alleviate neck pain.
What Is Thoracic Outlet Syndrome- Video
Managing TOS & Alleviating Neck Pain
When it comes to treating TOS, especially when neck pain is a significant component, many individuals will try to seek out non-surgical treatments to reduce the symptoms. Many individuals may try physical therapy to stretch and strengthen their shoulder, chest, and neck muscles to relieve compression. Others might try a manual treatment that is joint-oriented for the neck while neural-tissue-oriented for TOS to improve mobilization on the upper extremities and even improve poor posture. (Kuligowski et al., 2021) Additionally, non-surgical treatments can be combined with other therapies to reduce the chances of TOS from returning as they can further increase sensory-motor function back to the neck and upper extremities. (Borrella-Andres et al., 2021)
How Electroacupuncture Can Help With TOS
Electroacupuncture is a modern form of traditional acupuncture that is part of the non-surgical treatments that can help manage TOS while alleviating neck pain. Electroacupuncture is a modification of inserting needles into the body’s acupoints while incorporating electric stimulation to deliver a pulsed electrical current to the affected area gently. (Zhang et al., 2022) Some of the beneficial properties that electrostimulation can provide for TOS include:
Pain reduction by stimulating the release of endorphins to decrease inflammation.
Help relax the affected muscles in the chest and neck to alleviate the pressure on the nerves of the thoracic outlet.
Help enhance the blood flow to reduce vascular compression of TOS.
Help stimulate the nerve pathway to promote healthy nerve function and reduce pain-like symptoms.
By incorporating electroacupuncture and non-surgical treatments to reduce TOS, many individuals can make modifications to their lifestyle habits and prevent issues from affecting their upper body extremities. By utilizing these treatments, many people can listen to their bodies and focus on their health and well-being by addressing the pain-like symptoms they are experiencing from TOS correlating with neck pain. At the same time, they have a positive relationship with their primary doctors to develop a personalized treatment plan that can manage their TOS symptoms to the best outcomes.
References
Borrella-Andres, S., Marques-Garcia, I., Lucha-Lopez, M. O., Fanlo-Mazas, P., Hernandez-Secorun, M., Perez-Bellmunt, A., Tricas-Moreno, J. M., & Hidalgo-Garcia, C. (2021). Manual Therapy as a Management of Cervical Radiculopathy: A Systematic Review. Biomed Res Int, 2021, 9936981. https://doi.org/10.1155/2021/9936981
Kazeminasab, S., Nejadghaderi, S. A., Amiri, P., Pourfathi, H., Araj-Khodaei, M., Sullman, M. J. M., Kolahi, A. A., & Safiri, S. (2022). Neck pain: global epidemiology, trends and risk factors. BMC Musculoskelet Disord, 23(1), 26. https://doi.org/10.1186/s12891-021-04957-4
Kuligowski, T., Skrzek, A., & Cieslik, B. (2021). Manual Therapy in Cervical and Lumbar Radiculopathy: A Systematic Review of the Literature. Int J Environ Res Public Health, 18(11). https://doi.org/10.3390/ijerph18116176
Masocatto, N. O., Da-Matta, T., Prozzo, T. G., Couto, W. J., & Porfirio, G. (2019). Thoracic outlet syndrome: a narrative review. Rev Col Bras Cir, 46(5), e20192243. https://doi.org/10.1590/0100-6991e-20192243 (Sindrome do desfiladeiro toracico: uma revisao narrativa.)
Zhang, B., Shi, H., Cao, S., Xie, L., Ren, P., Wang, J., & Shi, B. (2022). Revealing the magic of acupuncture based on biological mechanisms: A literature review. Biosci Trends, 16(1), 73-90. https://doi.org/10.5582/bst.2022.01039
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine