Back pain after eating is often the result of conditions and/or disorders in other areas of the body that radiate to the back. These problems range from unhealthy posture, digestive issues, bowel problems, ulcers, allergies, etc. This is because the nerves of the back and the abdominal area run through areas of the spine. In addition to the classic symptoms like bloating and gas, individuals can develop symptoms beyond the gut, including sleep problems, fatigue, headaches, urinating problems, muscle aches, pelvic discomfort, and back pain. Chiropractic care and functional medicine can realign the body, alleviate symptoms, and restore function.
Back Discomfort
Back pain after eating can be linked to the body’s digestive process.
Individuals in this group can experience inflammation after consuming specific foods.
Inflammation could worsen existing back problems.
Individuals with food intolerance will have uncomfortable but usually not dangerous symptoms.
Individuals with food allergies can experience life-threatening allergic reactions.
Heartburn
Heartburn results from acid reflux, when stomach contents and acid flow back into the esophagus. Heartburn’s key symptom is a burning sensation in the chest. However, heartburn and indigestion do not directly cause back pain. But for individuals with back problems, heartburn can worsen back discomfort.
GERD
Gastroesophageal reflux disease, or GERD, could cause back pain in individuals with more than two weekly heartburn episodes.
The digestive system condition results from the chronic backflow of stomach acid.
Over time, the powerful acid can inflame the esophageal lining.
A stomach or esophageal ulcer can develop if GERD is not managed.
Pain could be felt in the lower to middle back around the stomach and lower intestines.
Ulcers
Ulcers can also result from a bacterial infection of Helicobacter pylori (or H. pylori).
Long-term use of nonsteroidal anti-inflammatory drugs (or NSAIDs) can also enable ulcer formation.
A peptic ulcer (or open sore) can develop on your stomach’s interior lining.
The small intestine’s upper portion can also be affected.
Peptic ulcers cause burning pain in the stomach. These flare-ups can worsen existing back problems and pain. Spicy foods and stress don’t cause peptic ulcers but can worsen their effects. In severe cases, a peptic ulcer can cause referred back pain felt in another location than where the pain originates. This means pain could be felt in the lower to middle back adjacent to the stomach and lower intestines.
Kidney Infection
Back pain could result from a bacterial kidney infection.
Kidney dysfunction infections, kidney stones, and chronic kidney diseases can be mistaken for general back and side pain.
Other symptoms can include chills, fever, nausea, and vomiting.
Pancreatitis
Pancreatitiscan develop if the pancreas becomes inflamed, brought on by excess alcohol consumption or gallstones. This definitely can cause back discomfort and pain.
Pancreatitis is the inflammation of the pancreas.
After eating, individuals can experience worsening abdominal pain that can refer to the back.
The body’s network of interconnecting sensory nerves causes the pain to be felt in other areas.
Most individuals will experience pain in the upper left or middle abdomen.
When individuals with celiac disease consume foods with gluten, the small intestine gets damaged, and their bodies cannot properly absorb the necessary nutrients.
Besides the back discomfort, there could be a burning sensation during urination or other urinary tract symptoms. Stools could be dark or black, a possible ulcer symptom. To reduce the chances of back discomfort after eating, avoid sugary, spicy, fatty foods or anything that triggers heartburn and reduce alcohol consumption. If you are experiencing frequent episodes of back pain after eating or the pain worsens, contact your physician, healthcare provider, or a chiropractor.
Hormonal Dysfunction In Men
References
Celiac Disease Foundation. (n.d.) “What is celiac disease?” https://celiac.org/about-celiac-disease/what-is-celiac-disease/
Mayo Clinic. (n.d.) “Celiac disease.” https://www.mayoclinic.org/diseases-conditions/celiac-disease/symptoms-causes/syc-20352220#:~:text=Celiac%20disease%2C%20sometimes%20called%20celiac,response%20in%20your%20small%20intestine
Pfizer. (April 25, 2022) “Heartburn, acid reflux, or GERD: what’s the difference?” https://www.pfizer.com/news/articles/heartburn_acid_reflux_or_gerd_what_s_the_difference#:~:text=The%20terms%20acid%20reflux%2C%20heartburn,meals%20or%20when%20lying%20down
Prairie Spine & Pain Institute. (n.d.) “What may cause back pain after eating: symptoms & prevention.” https://prairiespine.com/spine-care/5-things-that-may-cause-back-pain-after-eating-symptoms-and prevention/#:~:text=Exercises%20practiced%20in%20yoga%2C%20Pilates,chi%20may%20be%20particularly%20beneficial.&text=If%20a%20doctor%20cannot%20identify,ice%2C%20and%20taking%20pain%20relievers.
The lumbar region of the spine has various muscles and nerve roots that work together with the lower body extremities, like the hips, buttocks, legs, knees, and feet, for mobility and walking function. The various muscles in the buttock region include the gluteal muscles. They have a casual relationship with the hip muscles as they work together for hip mobility and erect good posture in the body. These various muscles and nerves also supply sensory-motor function for the legs to be mobile and provide hip mobility. The piriformis is one of the muscles assisting in the hips and buttock region. When this muscle becomes overused, it can cause mobility issues in the legs and affect a person’s ability to walk. Today’s article looks at the piriformis muscle, how trigger points are associated with piriformis syndrome, and how to manage piriformis syndrome associated with trigger points. We refer patients to certified providers who incorporate multiple methods in the lower body extremities, like sciatic pain and piriformis syndrome treatments related to trigger points, to aid individuals dealing with pain symptoms along the piriformis muscle. We encourage and appreciate patients by referring them to associated medical providers based on their diagnosis, especially when it is appropriate. We understand that education is an excellent solution to asking our providers complex questions at the patient’s request. Dr. Jimenez, D.C., utilizes this information as an educational service only. Disclaimer
What Is The Piriformis Muscle?
Have you been having issues walking from one place to another? Do you feel muscle tightness in your hips or buttock region? Or are you experiencing radiating pain traveling to your knees and feet? These pain symptoms are correlated with trigger points affecting the piriformis muscle. The piriformis is a flat, pear-shaped muscle, one of the six short rotator muscle groups in the gluteal region of the hips and thighs. The rotator muscle groups consist of the following:
Gemelli
Quadratus Femoris
Obturator Internus
Obturator Externus
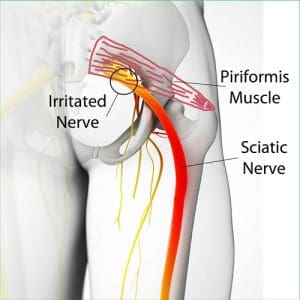
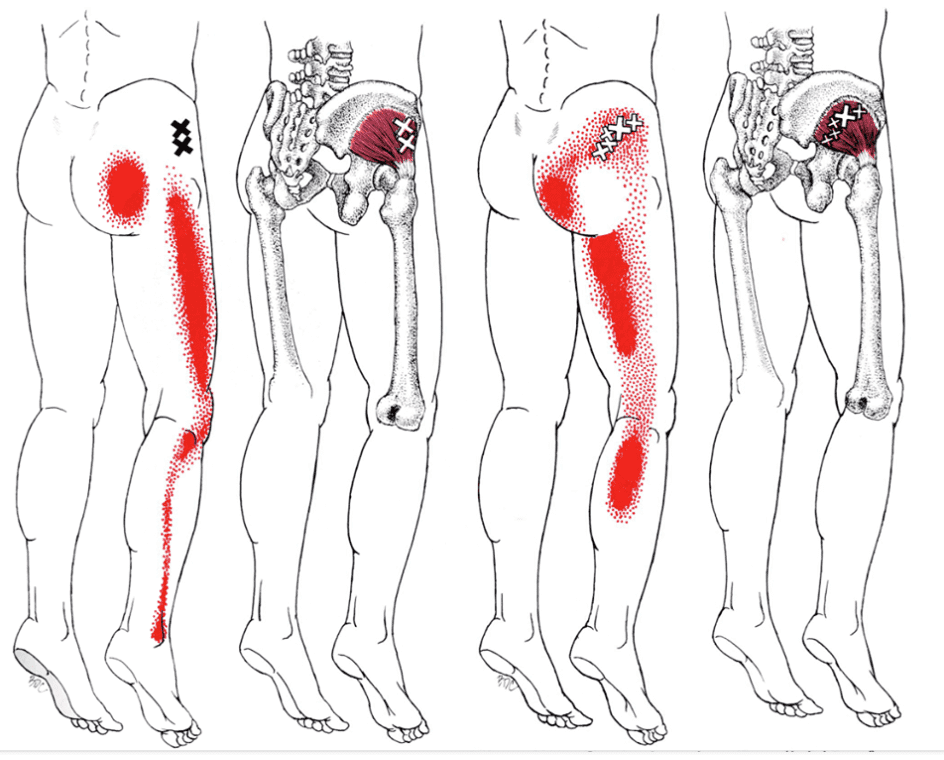
This muscle is parallel to the posterior margins of the gluteus medius and deep into the gluteus maximus. This muscle is very important to the body as it provides lower-body movement by stabilizing the hip joint and can lift and rotate the thighs away from the body. The piriformis muscle also surrounds the sciatic nerve, as this long nerve runs deep beneath the piriformis and enters the gluteal region of the rear. When the piriformis muscle becomes overused or suffers from associated traumatic factors, it can aggravate the sciatic nerve and even develop tiny nodules known as trigger points, causing mobility issues.
Trigger Points Associated With Piriformis Syndrome
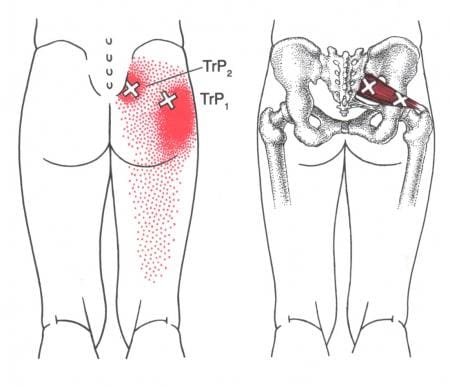
When abnormal factors affect the piriformis muscles, they can develop into trigger points associated with piriformis syndrome and cause issues in the pelvic and hip regions of the body. According to Dr. Janet G. Travell, M.D., “Myofascial Pain and Dysfunction,” trigger points can be activated when repetitive strain affects the piriformis muscle and causes symptoms of muscle weakness and pain in the hips. This causes overlapping issues in the surrounding muscles and the sciatic nerve, making diagnosing tricky for trigger points. Studies reveal that trigger points associated with piriformis syndrome may potentially cause muscle spasms or an inflammatory process to irritate the sciatic nerve that may be presented as identical to lumbar disk syndrome without neurological findings. Trigger points associated with piriformis syndrome may mimic chronic issues like fibromyalgia. Even though trigger points are tricky to pinpoint in a thorough examination, there are various ways to reduce the pain and prevent trigger points from affecting the piriformis muscle causing sciatic nerve pain.
Trigger Point Of The Week: Piriformis Muscle- Video
Have you been dealing with sciatic nerve pain? Have you found it difficult to walk for a short period? Or are you dealing with muscle tenderness or soreness in your buttock or hips? People experiencing these symptoms could be dealing with piriformis syndrome associated with trigger points. The piriformis is a small, fan-shaped muscle, one of the six short rotator muscle groups that help with hip and thigh mobility through stabilization. The piriformis muscles also surround the sciatic nerve and can succumb to injuries. When traumatic forces affect the hips and thighs, the piriformis muscle develops nodules known as trigger points, causing the muscle to irritate the sciatic nerve and cause pain in the legs. The video above shows where the piriformis muscle is located and how trigger points can mimic sciatic nerve pain in the leg without neurological findings. Studies reveal that trigger points could be a rare anatomical variation that can correlate with piriformis syndrome associated with sciatica. However, there is some good news, as there are ways to manage piriformis syndrome associated with trigger points.
Managing Piriformis Syndrome Associated With Trigger Points
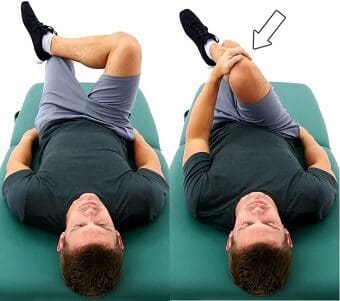
Various techniques can help manage piriformis syndrome associated with trigger points to relieve the piriformis muscle. Studies reveal that Kinesio tape on the piriformis muscle can help reduce pain and improve many individuals’ hip joint range of motion. Other techniques like stretching or deep tissue massage can help loosen up the stiff muscles and relieve trigger points from forming on the piriformis. For sciatica pain associated with trigger points along the piriformis muscle, decompression therapy can help the piriformis muscle lay off pressure on the sciatic nerve and reduce aggravated pain. These techniques can help improve hip joint mobility and increase the range of motion to the hips and lower extremities.
Conclusion
The piriformis is a small muscle that provides hip and thigh mobility. This small muscle surrounds the sciatic nerve, which helps give motor function to the legs. When traumatic factors affect the piriformis muscle, it can develop trigger points and cause sciatic pain in the hips. This causes mobility issues and pain around the hips. Various treatments are provided to help reduce the trigger points along the piriformis muscle and reduce sciatic nerve pain from causing more problems to the hips and legs mobility.
References
Chang, Carol, et al. “Anatomy, Bony Pelvis and Lower Limb, Piriformis Muscle.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 3 Oct. 2022, https://www.ncbi.nlm.nih.gov/books/NBK519497/.
Pfeifer, T, and W F Fitz. “[The Piriformis Syndrome].” Zeitschrift Fur Orthopadie Und Ihre Grenzgebiete, U.S. National Library of Medicine, 1989, https://pubmed.ncbi.nlm.nih.gov/2618150/.
R;, Hashemirad F;Karimi N;Keshavarz. “The Effect of Kinesio Taping Technique on Trigger Points of the Piriformis Muscle.” Journal of Bodywork and Movement Therapies, U.S. National Library of Medicine, 8 Feb. 2016, https://pubmed.ncbi.nlm.nih.gov/27814861/.
Ro, Tae Hoon, and Lance Edmonds. “Diagnosis and Management of Piriformis Syndrome: A Rare Anatomic Variant Analyzed by Magnetic Resonance Imaging.” Journal of Clinical Imaging Science, Medknow Publications & Media Pvt Ltd, 21 Feb. 2018, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5843966/.
Travell, J. G., et al. Myofascial Pain and Dysfunction: The Trigger Point Manual: Vol. 2:the Lower Extremities. Williams & Wilkins, 1999.
The buttock and the lower back have a casual relationship to the body, as the lower back has various muscles and nerves surrounding the spinal column. In contrast, the buttock region has multiple muscles and the sciatic nerve to keep the body upright. The sciatic nerve travels from the lumbar region of the spine across the gluteus muscles and down to the legs. The gluteus muscles include the Maximus, medius, and minimus, and they work with the sciatic nerve regarding good posture. When normal or traumatic factors begin to affect the body, like sciatica or poor posture, it can lead to developing trigger points associated with the gluteus minimus affecting the sciatic nerve. Today’s article examines the gluteus minimus, how trigger points mimic sciatic pain on the gluteus minimus, and various treatments to relieve sciatic nerve pain. We refer patients to certified providers who incorporate multiple methods in the lower body extremities, like sciatic pain treatments related to trigger points, to aid individuals dealing with pain symptoms along the gluteus medius muscles associated with sciatica. We encourage and appreciate patients by referring them to associated medical providers based on their diagnosis, especially when it is appropriate. We understand that education is an excellent solution to asking our providers complex questions at the patient’s request. Dr. Jimenez, D.C., utilizes this information as an educational service only. Disclaimer
What Is The Gluteus Minimus?
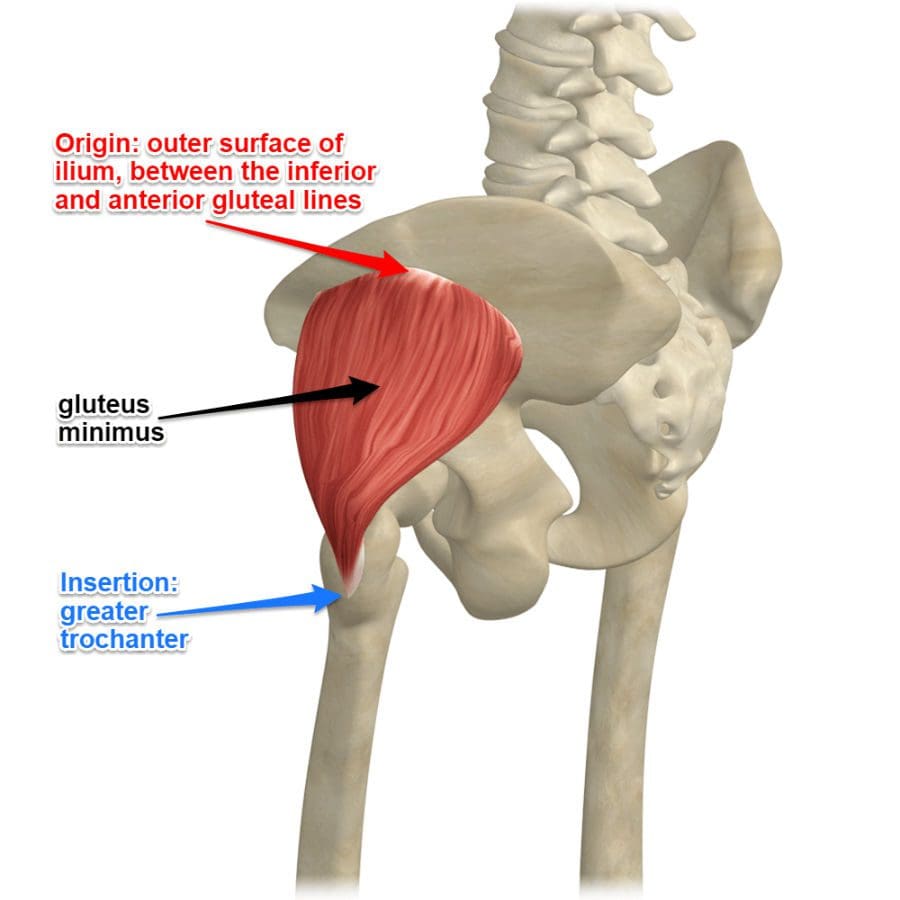
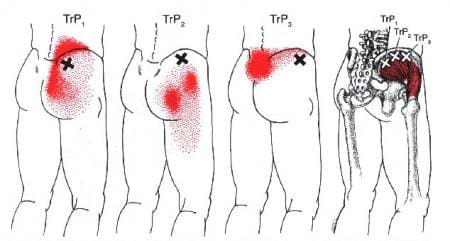
Have you been experiencing radiating pain traveling down to your leg? Do you have difficulty walking or sitting down? Do you feel tenderness or referred pain near your buttock region? Some of the issues correlate with trigger points affecting the gluteus minimus, causing pain in the sciatic nerve. As the smallest muscle in the gluteal region of the buttock, the gluteus minimus shares similar characteristics to the gluteus medius while being located beneath the medius muscle. One of the primary functions of the gluteus minimus is that it predominantly acts as a hip stabilizer and abductor. The nerves from the gluteal muscles include the sciatic nerve, which is on top of the gluteus muscles and the other nerves help supply the muscles to function in the posterior region of the body. Studies reveal that the structural integrity of the gluteus minimus muscles is the key to the lateral hip muscle, which contributes to pelvic stability and lower extremity function. However, when issues affect the gluteal muscles’ posterior region could trigger point pain mimicking sciatica.
How Trigger Points Mimic Sciatic Pain On The Gluteus Minimus?
When the lower body extremities begin to suffer from multiple issues that cause the individual to have mobility dysfunction, various factors could correlate to the dysfunction. When the gluteus minimus muscles have been overused or been through a traumatic experience, they can develop trigger points along the muscle fibers and even cause nerve entrapment along the sciatic nerve. Trigger points along the gluteus minimus can mimic sciatic nerve pain down to the back or even the side of the legs that causes excruciating and deep pain in the posterior region. Studies reveal that pain in the buttock region is a deep gluteal syndrome caused by non-discogenic pain that causes sciatic nerve entrapment.
The book, “Myofascial Pain and Dysfunction,” written by Dr. Janet G. Travell, M.D., states that many patients with active trigger points located in their gluteus minimus would complain about hip pain that could cause them to limp-walk when they are going to places. The pain caused by the active trigger points can make it difficult to stand up from a seated position due to the painful movements. The associated pain that the trigger points are causing to the gluteus minimus can be constant and excruciating; even small stretches can not alleviate the pain. The book also mentioned that trigger points could cause referred pain to the gluteus minimus that can cause various somato-visceral issues to the hips, legs, and knees if the pain worsens.
Sciatic Type Pain: Gluteus Minimus Trigger Points- Video
Are you dealing with pain in your hips, low back, and legs? Do you find it difficult to walk or stand up constantly? Or are you experiencing sciatic nerve pain that is radiating down your leg? All these pain-like symptoms are associated with trigger points along the gluteus minimus affecting the sciatic nerve. The gluteus minimus is the smallest of the gluteal muscles with the same function as the gluteus medius and predominately acts as the hip’s stabilizer and abductor. When the gluteus minimus muscles have been overused from traumatic events or normal factors, they can develop trigger points in the muscle fibers, entrap the sciatic nerve and irritate the nerve causing sciatica. The video above explain where the gluteus minimus is located and pinpoints where the trigger points are in the muscle fibers. Trigger points along the gluteus minimus can mimic sciatica by causing referred pain to travel down the leg. This can cause the individual to be unable to walk or even stand up due to the excruciating pain that they are in. Luckily, trigger points are treatable even though they are tricky to diagnose.
Various Treatments To Release Sciatic Nerve Pain
Even though trigger points along the gluteus minimus are tricky to diagnose, they are treatable through various treatments to alleviate the pain that the person is experiencing and can reduce sciatic nerve pain from causing more issues in the legs. Studies reveal that the effectiveness of active soft tissue release and trigger point block treatments combined can release entrapped nerves from the gluteus minimus and reduce low back and sciatic pain from the lower extremities. Now the treatments alone can only do so much to the individual, as many doctors tell their patients to take corrective actions or techniques to reduce the chances of trigger points from forming again on the gluteus minimus. Techniques like glute stretches, ischemic compressions, or using a foam roller can break the myofascial triggers from the gluteus minimus muscles and reduce the pain in the glutes and legs. This will help bring mobility back to the lower extremities.
Conclusion
As the smallest muscle in the body’s gluteal region, the gluteus minimus is the lower body’s predominant hip stabilizer and abductor. The gluteus minimus contributes to pelvic stability and lower extremity functionality that can be overused and can develop trigger points associated with sciatica. Trigger points along the gluteus minimus can cause referred pain to the legs and lower back while mimicking sciatic nerve pain. Thankfully various treatments and techniques can help reduce the chances of trigger points forming along the gluteus minimus and release nerve entrapment from the aggravated muscles pressing on the sciatic nerve, bringing back lower extremity mobility to the body.
References
Greco, Anthony J, and Renato C Vilella. “Anatomy, Bony Pelvis and Lower Limb, Gluteus Minimus Muscle.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 29 May 2022, https://www.ncbi.nlm.nih.gov/books/NBK556144/.
Kameda, Masahiro, and Hideyuki Tanimae. “Effectiveness of Active Soft Tissue Release and Trigger Point Block for the Diagnosis and Treatment of Low Back and Leg Pain of Predominantly Gluteus Medius Origin: A Report of 115 Cases.” Journal of Physical Therapy Science, The Society of Physical Therapy Science, Feb. 2019, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6382483/.
Martin, Hal David, et al. “Deep Gluteal Syndrome.” Journal of Hip Preservation Surgery, Oxford University Press, July 2015, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4718497/.
Travell, J. G., et al. Myofascial Pain and Dysfunction: The Trigger Point Manual: Vol. 2:the Lower Extremities. Williams & Wilkins, 1999.
Whiler, Lisa, et al. “Gluteus Medius and Minimus Muscle Structure, Strength, and Function in Healthy Adults: Brief Report.” Physiotherapy Canada. Physiotherapie Canada, University of Toronto Press, 2017, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5963550/.
Back discomfort symptoms include stiffness, spasms, tenderness, and headaches often caused by unhealthy posture and overuse muscle strain. Breathing back discomfort can be caused by injuries to the spinal musculoskeletal system, conditions and/or disease in the back, lungs, or heart, and other conditions unrelated to the back. When taking a breath, the intercostal muscles surrounding the rib cage contract, expanding the chest and allowing the lungs to fill with air. These muscles directly affect the spine, which is why back issues can present when breathing. Chiropractic care, decompression, and massage therapy, combined with a functional medicine approach, can realign the spine, release tight muscles, and restore function.
Breathing Back Discomfort
A problem in the back could be a root cause for discomfort and back problems while breathing.
Spinal Conditions
Scoliosis
Scoliosis causes the spine to curve sideways, either in one direction, creating a C shape, or generating an S shape in two directions.
The curvature can be so minimal that it cannot be seen or so severe that it can be life-threatening. Most scoliosis cases fall in between.
Taking deep breaths can cause discomfort and pain because the spine curvature puts extra strain on certain muscles meant to support the body’s weight in tandem with other muscles that have limited function or are no longer functioning.
The condition normally begins in adolescence but can start later in life.
Scoliosis treatment varies depending on the severity.
Monitor
A spinal physician will monitor the individual for mild curvature, as sometimes the process stops before it becomes serious. This is known as the wait-and-see, what-happens approach.
Kyphosis is another curve in the back that is supposed to be there.
Instead of curving like scoliosis, kyphosis causes a curve forward in the thoracic spine/upper back.
Problems arise when the curve is too pronounced.
This curve can come from unhealthy posture, Scheuermann’s disease, or being born with it.
Kyphosis causes breathing back discomfort by straining the muscles in the upper back, which are used for each breath.
Treatment often involves chiropractic and/or physical therapy to restore proper curvature and reduce inflammation.
A back brace could be prescribed if discomfort and pain continue.
Spinal fusion could be recommended for severe cases.
Lungs
The lungs and the spine are close to each other, which is why back discomfort and problems with breathing are connected.
Pneumonia
Pneumonia is an infection in the lungs that causes the tiny sacks known as alveoli to fill with fluid.
This is where the body takes oxygen from the inhaled air to the bloodstream.
The infection causes inflammation and discomfort symptoms in and around the chest and back while taking deep breaths.
Lung Cancer
Lung cancer can cause back issues and pain.
Frequently coughing causes the muscles around the ribs and back to become overused and strained from the jerking and heaving.
The strained muscles cause discomfort and pain when taking a breath.
Tumors can push on sensitive nerves in the back, causing inflammation and pain.
Pleurisy
There is a thin layer of protective tissue surrounding the lungs called pleura.
Pleurisy describes the layer becoming infected and/or inflamed, which causes discomfort symptoms in the back when breathing.
Pleurisy can be caused by injury, infection, or cancer.
Individuals with autoimmune disorders are more at risk of developing the condition.
Pneumothorax
Pneumothorax describes a full or partial lung collapse, usually on one side.
The lung can collapse as a result of severe illness or injury.
The lung collapses because air gets between the pleura and the lung and not allowing the lung to expand.
Pain with breathing is a common indicator of pneumothorax.
Individuals with this condition also experience severe shortness of breath and chest pain on one side.
Pulmonary Embolism
A pulmonary embolism occurs when a blood clot gets stuck in an artery, blocking blood flow to part of the lung.
The lungs will display signs of distress through back pain when trying to take a deep breath.
This is a life-threatening condition that causes chest pain, coughing up blood, a heart rate over 100 beats per minute, dizziness or leg swelling, and painful breathing; get to an emergency room immediately.
Heart
Heart Attack
The nerves associated with pain in the muscles and bones differ from those surrounding the organs, including the heart.
However, a heart attack can cause back pain as the nerves of the heart travel along the same path as spinal nerves, specifically in the upper back.
The brain can misinterpret pain signals from the same roots that supply peripheral nerves in the chest, arm, jaw, and back.
Because they share nerve pathways, the upper back can present with pain during a heart attack.
Aortic Dissection
The largest artery in the body is called the aorta.
It comes off the top of the heart and then drops to supply blood to the rest of the body.
Sometimes, the vessel can get a small tear in the chest area, which grows from the blood circulation pressure.
Aortic dissection can cause intense back pain while breathing.
Chiropractic care, decompression, and massage therapy combined with functional medicine can help realign the spine, stretch and loosen the overused and strained muscles, and provide postural training and nutritional planning to help alleviate symptoms and restore function.
Deep Breathing Back Pain
References
Costumbrado J, Ghassemzadeh S. Spontaneous Pneumothorax. [Updated 2022 Jul 25]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK459302/
Floman, Y., Burnei, G., Gavriliu, S. et al. Surgical management of moderate adolescent idiopathic scoliosis with ApiFix®: a short peri- apical fixation followed by post-operative curve reduction with exercises. Scoliosis 10, 4 (2015). https://doi.org/10.1186/s13013-015-0028-9
Hunter MP, Regunath H. Pleurisy. [Updated 2022 Jul 4]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK558958/
Mansfield JT, Bennett M. Scheuermann Disease. [Updated 2022 Aug 21]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK499966/
Raitio A, Syvänen J, Helenius I. Vertebral Body Tethering: Indications, Surgical Technique, and a Systematic Review of Published Results. Journal of Clinical Medicine. 2022; 11(9):2576. https://doi.org/10.3390/jcm11092576
Many individuals utilize the lower half of their bodies to go to different places and use the various surrounding muscles that provide stability on the hips and low back while supporting the upper body’s weight. Along the lower back is the buttock region, where the gluteal muscles help stabilize the pelvis, extend the hips, and rotate the thighs. The gluteal muscles also help shape and support the spine and have an erect posture in the body. One of the gluteal muscles that support the lower body is the gluteus medius, which can succumb to injuries and strain when overused or strained. This leads to developing trigger points that can cause various issues in the lower extremities and lead to corresponding chronic conditions. Today’s article focuses on the gluteus medius muscles, how the lumbago is associated with gluteus medius trigger pain, and various techniques to manage trigger points along the gluteus medius muscle. We refer patients to certified providers who incorporate multiple methods in the lower body extremities, like butt and low back pain treatments related to trigger points, to aid individuals dealing with pain symptoms along the gluteus medius muscles near and surrounding the body’s lower extremities. We encourage and appreciate patients by referring them to associated medical providers based on their diagnosis, especially when it is appropriate. We understand that education is an excellent solution to asking our providers complex questions at the patient’s request. Dr. Jimenez, D.C., utilizes this information as an educational service only. Disclaimer
What Is The Gluteus Medius?
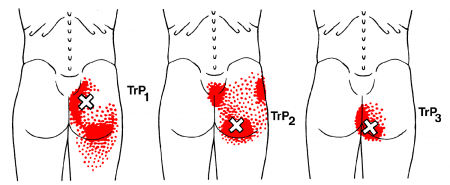
Have you been experiencing pain near your buttock and lower back? Have you been feeling unstable when you are walking? What about feeling pain in your tailbone that makes it unbearable to sit down? Many of these issues are associated with referred pain caused by trigger points affecting the gluteus medius. As part of the gluteal muscle region, the gluteus medius lies between the gluteus maximus and minimus is a flat, triangular muscle and is the primary hip abductor. The gluteus medius and minimus work together for internal rotation for the thighs and lateral rotation for the knees when they are extended. The gluteus medius muscles also help stabilize the pelvis, while the trunk maintains an upright position when the legs are in motion. Studies reveal that the gluteus medius is a key lateral hip muscle that correlates with muscle function with other muscle groups like the quadriceps and abdominal muscles. When injuries or not activating the gluteal muscles often, various muscle issues can cause problems to the gluteus medius muscles.
Lumbago Associated With Gluteus Medius Trigger Pain
Dysfunction in the hips can lead to various issues that can either be acute or chronic, depending on how severely the muscles have been overused or injured. Studies reveal that low back pain has been identified as the leading contributor to disability and when there is dysfunction in the lumbopelvic-hip complex, causing a reduction in gluteus medius strength. When the gluteus medius muscles have become overused or injured through trauma, it can develop trigger points on the muscle causing low back pain issues. When trigger points affect the gluteus medius, additional studies reveal that latent trigger points along the gluteus medius muscles may cause joint movement limitation while causing overload by affecting muscle activation from the hips.
According to Dr. Janet G. Travell, M.D.’s book, “Myofascial Pain and Dysfunction: The Trigger Point Manual,” patients with active trigger points along their gluteus medius complain of pain when they are doing normal actions like walking or sitting. The pressure from the trigger points along the gluteus medius causes the individual to be in a slumped position, causing them to be uncomfortable. This causes instability in the hips and lower body extremities, making many people miserable. The book also explains that the referred pain patterns caused by gluteus medius trigger points can overlap other chronic conditions like sacroiliac joint dysfunction, low back pain, and inflammation of the subgluteus medius bursa.
Trigger Point Of The Week: Gluteus Medius- Video
Have you been dealing with hip pain? Do you feel uncomfortable pain when walking or sitting down? Or Do you feel muscle stiffness or tenderness near your tailbone constantly? If you have been experiencing these painful symptoms constantly in your lower back or your hips, it could be due to your gluteus medius muscles being affected by trigger points. The video above overviews the gluteus medius location and how trigger points or myofascial pain syndrome causes referred pain to the lower back and hips. When trigger points affect the gluteus medius, the referred pain can overlap and correlate to low back and hip pain, thus causing various issues to the muscles surrounding the low back and buttock region. Regarding trigger points affecting the gluteus medius, they can be treatable through multiple techniques specific to the low back, buttocks, and hips.
Various Techniques For Managing Trigger Pain Along The Gluteus Medius
When issues of low back or hip pain begin to cause a problem in the lower extremities, the gluteus muscles can invoke pain-like symptoms in the affected muscle regions, thus developing trigger points. Even though trigger points are tricky to diagnose, they can be treated with various techniques that many people can incorporate into their daily lives. Exercises like resistance training on the gluteus medius can help improve hip abductor functionality and increase the strength of the gluteus medius. To manage trigger points along the gluteus medius, many people must do these corrective actions to reduce the pain that they may be causing to their glutes. When people are putting on pants, it is best to sit down and then put on their pants to prevent muscle strain on their hips and gluteus medius. Another corrective action is to move around after sitting down for a prolonged period to avoid trigger pain from developing. These corrective actions and techniques can help strengthen the lower body extremities and improve hip mobility.
Conclusion
As part of the gluteal muscle region, the gluteus medius lies between the gluteus maximus and minimus by being a primary hip abductor. The gluteus medius helps with pelvic stabilization and helps the trunk maintain an upright position when the legs are in motion. When normal or traumatic factors affect the gluteus medius, it can develop trigger points on the muscle fibers, causing referred pain to the hips and lower back. Trigger points along the gluteus medius are manageable through various techniques that people can use to prevent hip and low back issues. These techniques can minimize the trigger points and strengthen the gluteus medius muscles in the glutes.
References
Bagcier, Fatih, et al. “The Relationship between Gluteus Medius Latent Trigger Point and Muscle Strength in Healthy Subjects.” Journal of Bodywork and Movement Therapies, U.S. National Library of Medicine, Jan. 2022, https://pubmed.ncbi.nlm.nih.gov/35248262/.
Sadler, Sean, et al. “Gluteus Medius Muscle Function in People with and without Low Back Pain: A Systematic Review.” BMC Musculoskeletal Disorders, BioMed Central, 22 Oct. 2019, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6805550/.
Shah, Aashin, and Bruno Bordoni. “Anatomy, Bony Pelvis and Lower Limb, Gluteus Medius Muscle.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 25 Jan. 2022, https://www.ncbi.nlm.nih.gov/books/NBK557509/.
Stastny, Petr, et al. “Strengthening the Gluteus Medius Using Various Bodyweight and Resistance Exercises.” Strength and Conditioning Journal, Strength and Conditioning Journal, June 2016, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4890828/.
Travell, J. G., et al. Myofascial Pain and Dysfunction: The Trigger Point Manual: Vol. 2:the Lower Extremities. Williams & Wilkins, 1999.
Whiler, Lisa, et al. “Gluteus Medius and Minimus Muscle Structure, Strength, and Function in Healthy Adults: Brief Report.” Physiotherapy Canada. Physiotherapie Canada, University of Toronto Press, 2017, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5963550/.
The body’s lower extremities have various muscles that allow the legs and feet to move around from one location to another. The different muscles that make up the lower extremities of the body help stabilize the hips and allow mobility to the legs. The legs and hip muscles have a mutual relationship with one body muscle that helps the lower body, and it’s the glutes, specifically the gluteus maximus. Many individuals must realize that the glutes must be activated when working out. When the glutes are not activated, it can lead to the rest of the lower extremities, like the lower back, hips, and knees, taking most of the loaded weight on the body. This leads to the development of trigger points associated with butt pain along the gluteus maximus, causing referred pain down the legs. Today’s article looks at the gluteus maximus muscles, how trigger points are associated with butt pain, and relieving pain is associated with trigger points along the gluteus maximus. We refer patients to certified providers who incorporate multiple techniques in the lower body extremities, like butt pain treatments related to trigger points, to aid individuals dealing with pain symptoms along the gluteus maximus muscles near and surrounding the body’s lower extremities. We encourage and appreciate patients by referring them to our associated medical providers based on their diagnosis, especially when it is appropriate. We understand that education is an excellent solution to asking our providers complex questions at the patient’s request. Dr. Jimenez, D.C., utilizes this information as an educational service only. Disclaimer
What Is The Gluteus Maximus?
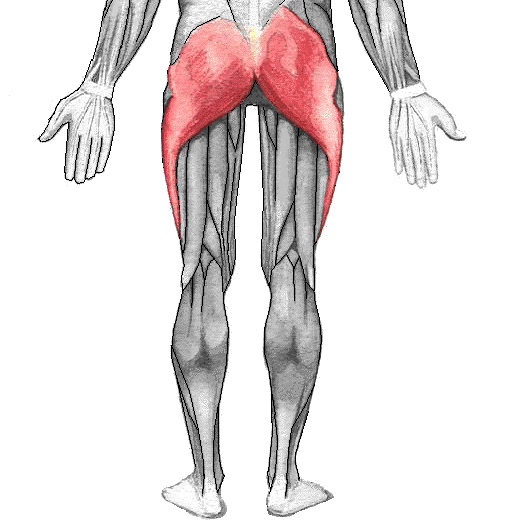
Have you been experiencing pain in your hips, low back, and knees? Are you uncomfortable when you are trying to sit down? Or are you experiencing sciatic pain-like symptoms running from your buttock to your leg? These issues affecting the body’s lower extremities may correlate with trigger points along the gluteus maximus in the buttock. The gluteus maximus is the largest gluteus muscle that makes up the shape and form of the buttock and hip areas of the body. The gluteus maximus can come in different sizes depending on the individual’s body type. This large muscle plays a prominent role in the body as it helps maintain an erect posture for the upper body. Studies reveal that the gluteus maximus is one of the primary hip extensors, and some of its functions include extending and externally rotating the thighs. The gluteus maximus, when trained properly through exercise, can increase in size and strength while supporting the upper body. However, only a few people realize that when their gluteus maximus muscles are not properly trained, it can lead to various issues that can cause trigger points to form along the gluteus maximus.
Trigger Points Associated With Butt Pain
As mentioned earlier, when individuals don’t properly strengthen their gluteus maximus through exercises, it can lead to unwanted pain symptoms affecting the lower back, hips, and knees in the lower body. When the gluteus maximus muscles are not fully activated to their full potential, they can develop into trigger points associated with butt pain. Studies reveal that trigger points or myofascial pain syndrome associated with the gluteus maximus can affect the entry point of the inferior gluteal nerve, causing pain and a limited range of motion to the joints. Dr. Janet G. Travell, M.D., who wrote “Myofascial Pain and Dysfunction,” mentioned that the symptoms caused by active trigger points could make the individual uncomfortable and cause a cramping sensation to the gluteus maximus. At the same time, trigger points along the gluteus maximus can correlate with referred pain that can entrap the sciatic nerve causing sciatica to affect the legs. When this happens, many other issues can pop up and affect the lower extremities, mimicking low back pain.
How To Release Trigger Points On The Gluteus Maximus-Video
Are you experiencing a cramping sensation in your buttock? What about feeling an electric sense running down your leg? Or are you dealing with low back pain? Many of these issues are associated with trigger points affecting the gluteus maximus, causing butt pain. The gluteus maximus is a large, superficial muscle that helps support the hips and ensures that the upper body has an erect posture. When issues affect the gluteus maximus, it can lead to unwanted pain in the lower back, hips, and knees, causing the individual to be in constant pain. This leads to the development of trigger points along the gluteus maximus, thus mimicking sciatica. The video above demonstrates where the trigger points are located in the gluteus maximus and how they can potentially overlap to cause sciatica nerve pain. The video also shows how to use various techniques to relieve the pain from the trigger points and help release the trapped muscle from causing additional pain in the lower body.
Relieving Pain Associated With Trigger Points Along The Gluteus Maximus
Since the gluteus maximus is a large important muscle, it is important to strengthen the glutes to prevent low back pain. When it comes to relieving pain associated with trigger points along the gluteus maximus, there are various techniques that many people can utilize to release the tension from the gluteus maximus and the rest of the lower body. Various glute stretches can help elongate the gluteus maximus muscle after a workout and reduce the chances of triggering points and referred pain re-occurring. Another technique that many people should do is to bend at the knees when lifting heavy objects to reduce overload on the lower back and cause more issues on the gluteus maximus.
Conclusion
The gluteus maximus is a large superficial muscle with a very important function in the body. This muscle helps with extending and externally rotating the thighs and helps keep the posture erect for the upper back. However, the gluteus maximus muscles are not properly trained and can lead to unwanted issues that cause referred pain to the hips, low back, and knees that correlate with triggering points. Luckily though, through proper training and stretching, the lower body can prevent the gluteus maximus from developing trigger points and help improve a person’s posture.
References
Akamatsu, Flavia Emi, et al. “Anatomical Basis of the Myofascial Trigger Points of the Gluteus Maximus Muscle.” BioMed Research International, Hindawi, 2017, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5733974/.
Elzanie, Adel, and Judith Borger. “Anatomy, Bony Pelvis and Lower Limb, Gluteus Maximus Muscle.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 28 Mar. 2022, https://www.ncbi.nlm.nih.gov/books/NBK538193/.
Neto, Walter Krause, et al. “Gluteus Maximus Activation during Common Strength and Hypertrophy Exercises: A Systematic Review.” Journal of Sports Science & Medicine, Uludag University, 24 Feb. 2020, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7039033/.
Travell, J. G., et al. Myofascial Pain and Dysfunction: The Trigger Point Manual: Vol. 2:the Lower Extremities. Williams & Wilkins, 1999.
The posterior section of the lower half of the body consists of the hips, low back, pelvis, legs, and feet, which provide stability to the body while supporting the upper body’s weight. The various muscles surround the lower extremities and make different motions for mobility and functionality by contracting and retracting when the legs and hips are in motion. The various muscles that provide stability to the hips and the legs are the iliopsoas muscles. When normal age or incidents affect the lower body extremities, it can correlate to the development of trigger point pain. Today’s article examines the iliopsoas muscles, how referred trigger pain affects the thighs and low back, and treating trigger point pain on the thighs and low back. We refer patients to certified providers who incorporate multiple techniques in the low back and thigh pain therapies related to trigger points to aid individuals dealing with pain symptoms along the iliopsoas muscle in the lower back, thigh, and near the pelvis. We encourage and appreciate patients by referring them to our associated medical providers based on their diagnosis, especially when it is appropriate. We understand that education is an excellent solution to asking our providers complex questions at the patient’s request. Dr. Jimenez, D.C., utilizes this information as an educational service only. Disclaimer
What Is The Iliopsoas Muscle?
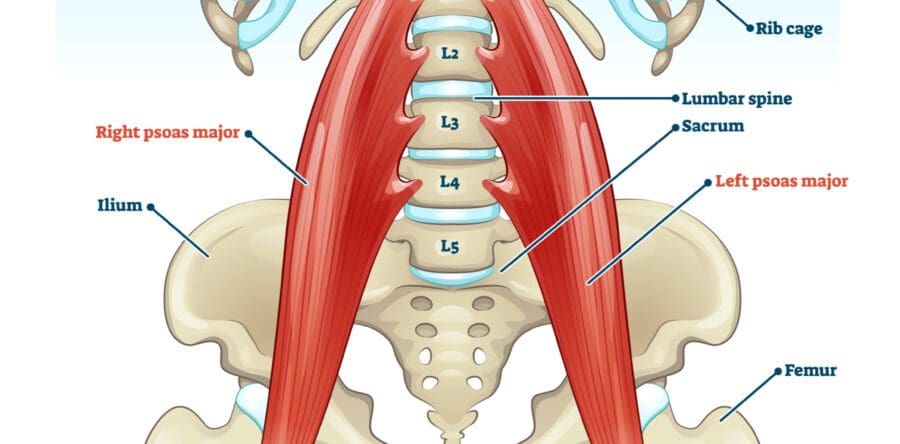
Have you been dealing with muscle cramps in your thighs? What about feeling muscle stiffness in your lower back when you are stretching? Or do you feel your thigh muscles become heavy after a workout? Many of these issues correlate with the iliopsoas muscle becoming overused and developing trigger points, thus affecting the thighs and lower back. In the lower body extremities, the muscles that help provide stability to the hips are the iliopsoas muscles. The iliopsoas muscles consist of three muscles: iliacus, psoas major, and psoas minor, which can work individually or as a unit. When working individually, the iliacus muscle provides stability to the pelvis, the psoas major muscle helps stabilize the lumbar spine when a person is sitting, and the psoas minor helps with flexion of the trunk and stretch the iliac fascia. As a unit, however, these muscles work together to become the primary flexors of the thighs and allow hip flexion.
Studies reveal that the iliopsoas is a deep muscle group that anatomically connects the spine to the body’s lower limbs. The iliopsoas muscles have an important function in the body’s lower limbs as primary hip flexors for daily activities, especially for those in sports. However, many impairments and pathologies affect the iliopsoas, which causes significant limitations and challenges since the symptoms mask the pain, causing individuals to think they are dealing with low back and hip pain.
Referred Trigger Pain On The Thighs & Low Back
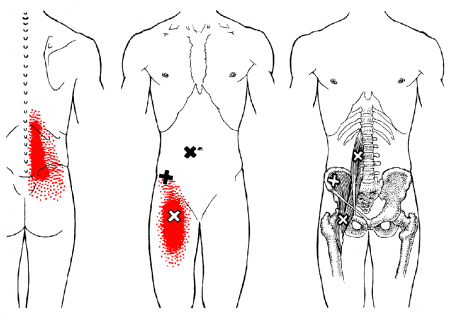
Since the iliopsoas muscles provide hip and thigh flexion to the lower body, many impairments and pathologies can affect this muscle group, causing issues in the hips, thighs, and even the lower back. These impairments can cause the iliopsoas muscles to be overused and overstretched, thus potentially developing trigger points along the iliopsoas muscles, causing referred pain on the thighs and low back. Studies reveal that when the iliopsoas muscle becomes overused or traumatic issues affect it, it can lead to problems in hip flexion and impairment in the lower extremities. In “Myofascial Pain and Disorders: The Trigger Point Manual,” written by Dr. Janet G. Travell, M.D., when trigger points begin to affect the iliopsoas muscles, it is known as the “Hidden Prankster” as normal factors like poor posture can overload the back causing trigger points to form not only on the iliopsoas muscles but the hamstrings, gluteal, thoracolumbar paraspinal, and posterior cervical muscles. Trigger points can mimic other chronic conditions that cause referred pain in different body areas. Trigger point pain in the iliopsoas muscle can lead to back pain, groin pain, snapping hips, and standing up difficult for the individual if it is not treated immediately.
Trigger Point Therapy: Iliopsoas Muscle- Video
Since the iliopsoas muscles provide hip and thigh flexion to the lower body, many impairments and pathologies can affect this muscle group, causing issues in the hips, thighs, and even the lower back. These impairments can cause the iliopsoas muscles to be overused and overstretched, thus potentially developing trigger points along the iliopsoas muscles, causing referred pain in the thighs and low back. Studies reveal that when the iliopsoas muscle becomes overused or traumatic issues affect it, it can lead to problems in hip flexion and impairment in the lower extremities. In “Myofascial Pain and Disorders: The Trigger Point Manual,” written by Dr. Janet G. Travell, M.D., when trigger points begin to affect the iliopsoas muscles, it is known as the “Hidden Prankster” as normal factors like poor posture can overload the back causing trigger points to form not only on the iliopsoas muscles but the hamstrings, gluteal, thoracolumbar paraspinal, and posterior cervical muscles. Trigger points can mimic other chronic conditions that cause referred pain in different body areas. Trigger point pain in the iliopsoas muscle can lead to back pain, groin pain, snapping hips, and standing up difficult for the individual if it is not treated immediately.
Treating Trigger Point Pain On The Thighs & Low Back
When trigger point pain begins to cause issues in the thighs and low back, the iliopsoas muscles will suffer from muscle spasms, stiffness, and difficulty standing. This is due to nerve entrapment from aggravated iliopsoas muscles caused by trigger points. However, various treatments can manage trigger point pain in the thighs, and low back through multiple techniques that pain specialists utilize can help relieve the pain symptoms from the iliopsoas muscle and manage trigger point pain. Studies reveal that combination treatments like soft tissue manipulation and trigger point therapy can help release the tiny nodules from the affected muscle and reduce the symptoms from re-occurring in the body. Other treatments, like correcting one’s posture, strength exercising, and even stretching, can help lengthen the iliopsoas muscles, stretch and strengthen the surrounding muscles, and prevent pain-like symptoms from affecting the thigh and low back muscles again. These various treatments can even improve hip mobility in the lower body extremities.
Conclusion
In the lower body extremities, an iliopsoas is a group of deep muscles that provide stability to the lumbar spine and allow hip and thigh flexion. These groups of deep muscles can work individually or together to enable the individual to sit, stand and move around through physical activities; however, when the iliopsoas muscles become overused or suffer from a traumatic event, they can develop trigger points that can cause mobility issues on the thighs, hips, and lower back. Even though trigger points are difficult to diagnose, they are treatable through various treatments. Various treatments, like soft tissue massages, trigger point therapy, strength exercising, or stretching the iliopsoas muscles, can release trigger points from the affected body part and help bring back mobility function to the hips, thighs, and low back.
References
Bordoni, Bruno, and Matthew Varacallo. “Anatomy, Bony Pelvis and Lower Limb, Iliopsoas Muscle.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 2 Apr. 2022, https://www.ncbi.nlm.nih.gov/books/NBK531508/.
Dydyk, Alexander M, and Amit Sapra. “Psoas Syndrome.” In: StatPearls [Internet]. Treasure Island (FL), StatPearls Publishing, 12 June 2022, https://www.ncbi.nlm.nih.gov/books/NBK551701/.
Kameda, Masahiro, and Hideyuki Tanimae. “Effectiveness of Active Soft Tissue Release and Trigger Point Block for the Diagnosis and Treatment of Low Back and Leg Pain of Predominantly Gluteus Medius Origin: A Report of 115 Cases.” Journal of Physical Therapy Science, The Society of Physical Therapy Science, Feb. 2019, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6382483/.
Lifshitz, Liran, et al. “Iliopsoas the Hidden Muscle: Anatomy, Diagnosis, and Treatment.” Current Sports Medicine Reports, U.S. National Library of Medicine, June 2020, https://pubmed.ncbi.nlm.nih.gov/32516195/.
Travell, J. G., et al. Myofascial Pain and Dysfunction: The Trigger Point Manual: Vol. 2:the Lower Extremities. Williams & Wilkins, 1999.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine