Baseball Injuries: The crack of a ball against your bat, good! The crack of a back or shoulder, bad!
Baseball, the nationwide pass time, heats up in summer. From little league on up, individuals enjoy swinging the bat and running the bases. Unfortunately, the movements baseball requires can wreak havoc on a person’s body, leaving them with strained backs, hurt shoulders, and pulled muscles. According to Livestrong, there are over 600,000 injuries from playing baseball per year, and 5-14 year olds suffer from 117,000 of them.
The aspects of the game � running, sliding, twisting, and jumping � cause the body to maneuver into awkward positions. If you or a loved one has slid into first and felt a pop, or twisted to catch a fly ball and felt a snap, chiropractic care offers several ways to help put you on the road to a complete recovery.
Baseball Injuries: Manage Pain
Baseball injuries frequently involve large muscles, resulting in a high degree of pain. Chiropractic treatment offers relief from severe pain of many injuries involving the spine, muscles, and joints.
Using spinal adjustments, a chiropractor is able to help the body align itself properly, and sooth the injured area. Once the body functions normally, pain is diminished. Sometimes this can be accomplished in one visit, while other injuries require a few sessions before pain diminishes.
Increase Mobility
A strained neck, pulled back, or overextended knee may cause the individual serious issues in being able to move. Limping around slowly is nobody’s idea of fun!
Chiropractic adjustments are proven to help reduce inflammation and improve mobility in many injury cases. If that last baseball game has you unable to put weight on your knee, your neck won’t twist without pain, or your shoulder won’t lift your arm, it may be time to visit a chiropractor for evaluation.
Promote Healing
The premise of chiropractic care is to treat the entire body as a whole, not just the injured part. As the body becomes better aligned, it functions at a higher capacity, and begins to heal itself.
Most injuries resulting from playing baseball, such as tendonitis, strained muscles, torn rotator cuffs, and the like, heal faster with chiropractic care. Increased blood flow to the injured area, and less pressure on the body part (usually due to misalignment of the spine) allow the injured area to regenerate, and a greater chance to begin healing faster than without chiropractic care.
Avoid Medication
Even over-the-counter pain and anti-inflammatory drugs cause side effects in certain individuals. Allergies, stomach issues, and other reasons result in many injured people steering clear of medication to relieve pain and inflammation.
Chiropractic care provides these individuals a drug-free, less invasive way to help manage the pain and promote healing. More people every year are choosing to visit a chiropractor for pain relief instead of popping pain medicine.
Before jumping into a baseball game, or even if you or your children play regularly, remember that prevention is worth its weight in gold. Take care of your body by stretching beforehand, being aware of your physical limits, maintaining proper posture, and staying hydrated during the game. With a little extra effort, the chance of a baseball injury can be dramatically decreased.
Summer fun often includes activities such as baseball, whether in a league or in your back yard with your family. Avoid suffering from an injury as best you can, and, if you or your child end up with an achy knee, twisted elbow, or smarting shoulder, call you chiropractor to schedule a thorough evaluation as quickly as possible.
Prevention, Recognition & Management Of Youth Sports Injuries
This article is copyrighted by Blogging Chiros LLC for its Doctor of Chiropractic members and may not be copied or duplicated in any manner including printed or electronic media, regardless of whether for a fee or gratis without the prior written permission of Blogging Chiros, LLC.
El Paso, TX. Chiropractor, Dr. Jimenez takes a look at top running shoes that are great for knee pain and Iliotibial (IT) Band Syndrome.
Running Shoes: Knee pain is one of the common problems with most active people. It could get worse for those who love running, especially the athletes. A majority of them suffer from knee pains each year. This pain hinders you from enjoying your daily sports activities and might even become worse with time if not treated correctly. There are causes and cures for such pains that this article is going to look at, but the main focus is on the best shoes for knee pain, also referred to as Iliotibial (IT) Band Syndrome.
This can happen due to various causes like overtraining, running many hills, and wrong running form, among others. These injuries are very frustrating as they can take up to months to go away. This is the reason different companies have designed shoes that will offer you support for any knee problem.
What Goes Wrong
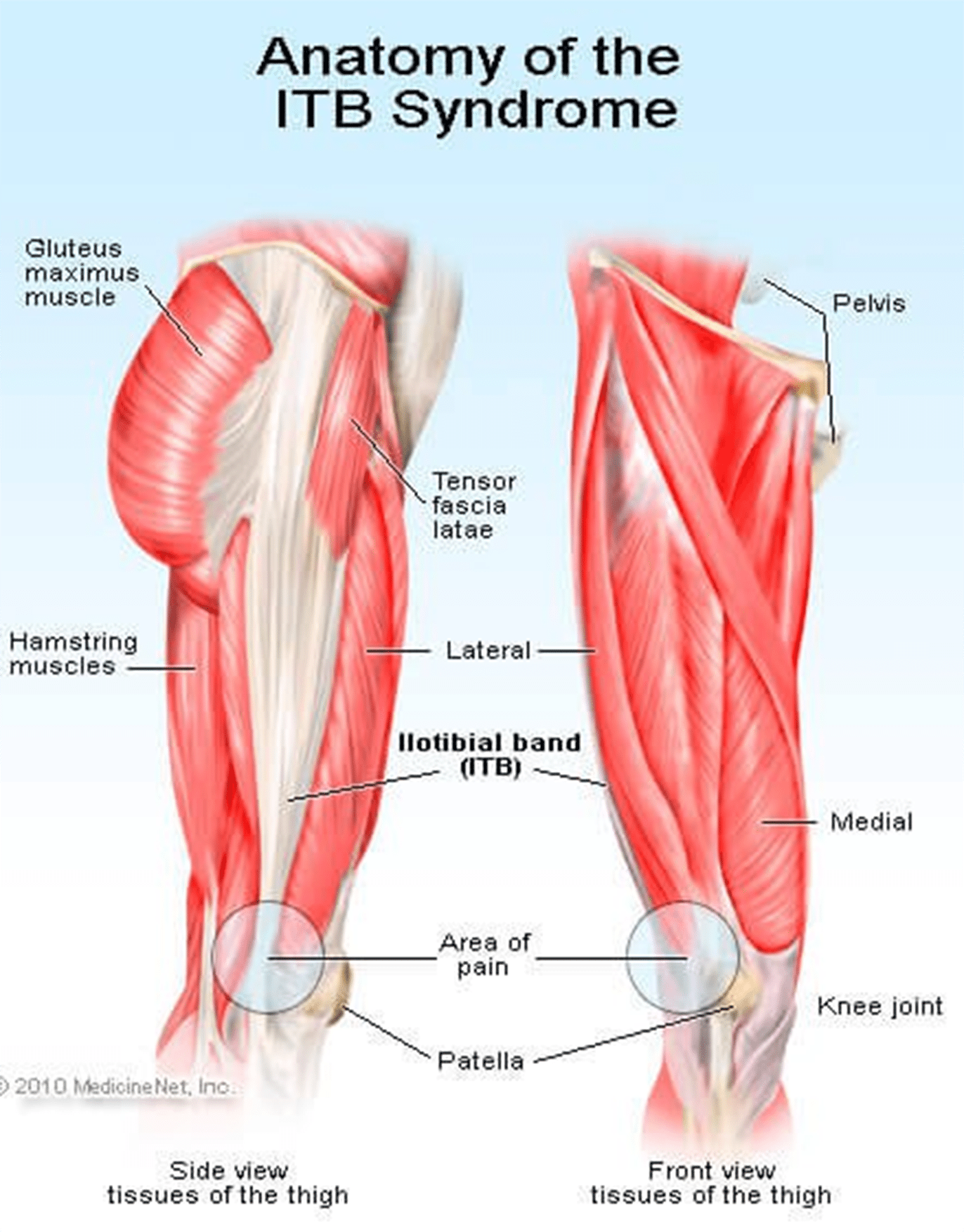
The iliotibial band (ITB) is usually a structure whose job is to provide leg stability whenever you take a step. It works with the hip muscles in a thigh’s outward movement and also helps counter the movements within the knee joint. This band starts in the hip and ends just under the knee joint.
Repeated use of the ITB leads to stress, causing knee pain. You will also notice clicking sensations from the joint as ITB snaps across it. This pain is always experienced when the heel comes into contact with the ground; running slowly or downhill tends to make the symptoms worse.
ITBS will usually start as tightness while running but continues to a point where the pain is severe and unbearable. Although ITB continues to tighten when overstressed or injured from training, this is not the main problem. What causes the injury is how the ITB functions and the weakness around it.
The ITB is generally a weak structure and any weakness around it will lead to injury. Most runners have weak core muscles due to the fact that they don’t do strength training or have never been in any sports with side-to-side movement.
Signs Of IT Band Syndrome
If you are a runner, you will be able to distinguish ITBS by:
A swelling
A cracking feeling when stretching the knee
A feeling of burning, stinging and aching on the outer side of the knee that might migrate to the thigh. You will notice these discomforts especially, on your second half of the run.
Bending the knee at 45 degrees causes severe external knee pain
Criteria You Should Follow When Selecting The Best Running Shoes for ITBS
?There are various things that you should always consider when buying running shoes. Since most runners experience knee pain, it is wise to look for shoes that will help alleviate this pain without slowing them down. Below are some of the features to look out for in running shoes:
Stability/ Support
Since it is common to have knee pains due to lack of motion control and lack of stability, it is good to choose shoes that will offer you the support you need while running. If your running shoes don’t have any stability, you will end up stressing out your knee, which will result in pain and discomfort while running.
Fit
If you want to do away with pain, you might consider looking for a fit pair of shoes as they will reduce any pain, causing issues in the long run. Pay attention to small specifics like shoes that offer enough heel space, sufficient toe box room, and enough space for wide feet. Your toes should be able to move freely without being constricted.
If your foot cannot move freely and the toes are restricted from spreading, it could lead to painful issues in your feet, legs, and knees.
Motion control footwear is not the whole solution; you need to ensure your feet can still function naturally as they are supposed to.
Comfort
No one wants to wear uncomfortable shoes! Each of these selected best shoes come with upper and underfoot comforts to ensure you get to enjoy your run.
Most of these shoes are made with DNA technology, Gel cushioning, and REVlite midsole for ultimate comfort.
Durability
Your running shoes should run their course without falling apart as this will cause you pain in the long-run. If they promise to offer you support, they should do just that and not start peeling off and tearing when you are on the run.
The ??below 5 shoes have passed the durability test to ensure they give you maximum performance.
Breathability
Although this has nothing to do with knees, it is paramount that your running shoes have enough breathing space to avoid accumulating excess moisture, which might bring discomfort and other feet related problems.
There is no magical cure for knee pain and you should always know the root cause. This way, you will be able to come up with the best solution of minimizing or even eliminating the pain entirely. Although there are various causes of knee pain, this article is focusing on ITB syndrome which happens to be one of the causes.
Reviews Of The Top 5 Shoes
These shoes have been selected with the runner’s welfare in mind. They will help deal with the ITBS, which is a problem for most of them. Since one way of dealing with this condition is getting good running shoes, here is a review of such products.
Asics Gel Kayano 23
This upgraded version is lightweight to help with any knee problems. It offers you comfort through cushioning that help absorb shock as you run as well as other features like grip, fit, and durability. The shoe has an added outer sole to ensure it lasts you as long as possible.
PROS
?Gel cushioning will act as a shock absorber for more comfort
?Has superb breathability feature
?Is ideal for overpronation and knee pain
?The outsole’s traction will offer the intended support on various surfaces
CONS
?It is a bit pricey
New Balance 890v5
It tops the list of 5 best running shoes. Also, it has remained the first choice for most runners with knee pain issues. This pair offers all the above functionalities too, making it your best choice.
PROS
?It comes with one of a kind breathability and fit due to its great FantomFit design
?Its smooth upper construction will ensure no irritation occurs
?The REVlite midsole will give you much needed cushioning
CONS
?It has a narrow toe box and might not fit a person with a wide foot
?Puma Faas 600 V3
Puma models have never disappointed, and this one is no exception. Puma Faas 600 is the solution to your knee pain. It is also an affordable option for the short-handed.
PROS
?Great breathability
?Comes at a reasonable price
?It’s lacing system and fit offers you a secure and comfortable run
?It is designed to fit perfectly
CONS
?There have been reported concerns about the outsole’s durability
New Balance 1080v7
This is another great choice on the list. It is one of the New Balance Fresh Foam Series. Its midsole offers you the required support coupled with comfort to eliminate knee pains.
PROS
?Very durable
?Enough breathability for long runs
?Good amount of cushioning and support from the Fresh Foam midsole
?It fits like a sock giving you a confident use
CONS
?The upper design is not seamless
?Can be stiff
Saucony Hurricane 16
This is the 16th edition of the Saucony Hurricane, which offers a combination of steadiness and protection. Those with knee pain have agreed with the stability offered by this shoe. It is also cushioned to help you go for long runs without any pain or injury. It is perfect for heavy runners and those who are out of shape due to inactivity.
PROS
?Superb stability
?Lightweight rubber offers protection and cushioning
?Great ground contact
?Reflective parts allow you to have a safe run
?Comes with Sauc-Fit Technology that enhances its comfortability
CONS
?It is a bit narrow
?Limited colors to choose from
?Might be heavy for fast runners
If you are a long-distance runner, it is good to know that your shoes cushioning will wear out quite easily and you might be tempted to continue using them since they look good on the outside. This is a big mistake. The following will help you prevent any more ITBS recurrences:
Replace running shoes frequently to avoid wearing those with worn out inner cushioning
Always give your shoes time to rest so that the cushioning can get restored; it would be wise to have two pairs of running shoes.
Although shoes can offer you relief from ITBS, it is better to look out for other ways of helping you cope with or eliminate the pain entirely. Also, know what triggers the problem and avoid it at all costs.
These shoes have been tried and tested and found to offer support and help in managing the iliotibial band syndrome. Asics takes the lead on these best shoes. It comes with gel cushioning that will offer you the best shock absorption and maximum comfort as seen above. Its sole is also made to help you tackle any terrain and you can be assured that your knees will thank you later. The only drawback is the price, which is on the upper-side. However, always remember that cheap is expensive.
If you are an active person or an athlete suffering from ITBS, go ahead and get yourself a pair of these shoes as per your preference and choice.
Hey there, I’m Zoey, founder and the main editor of The Babble Out. I know nobody’s life is smooth as they wish, and it�s the same with mine. I had some terrible news a few years ago and running was the way I got through these issues. This has given me enough motivation to create this blog, so that I can give you a helping hand for as many daily problems as I can. If you are curious why “babble out” is the? name of the blog, then check the “About” page and find out more about me.
Return to play describes the stage in recovery from a sports injury when an athlete is able to go back to playing sports or participate in their specific physical activity at a pre-injury level.
Nobody likes to be sidelined with an undesired injury. Among the goals of sports medicine professionals and specialists is to try to restore an athlete back to action. Returning too soon, however before restoration or healing has taken place, can put an athlete at an increased risk for re-injury and down time.
With the ideal treatment and care plan for sport accidents and injury, from early identification and proper treatment to full functional rehabilitation, you can often safely accelerate your return to perform.
Lessons from Professional Athletes
Why does it seem that professional athletes come back to play so much quicker than the normal person or athlete? Professional athletes are often, at the time of injury, in tremendously good physical conditioning. This fitness level helps them in various ways. Various studies have demonstrated that conditioning the body properly can not only prevent injuries, it may also lessen the severity of an injury and speed up recovery.
Professional athletes also get prompt treatment once an injury happens, and this lessens the acute phase of the injury. Treatment and care is required as soon as an injury followed by symptoms such as, stiffness, swelling, and loss of muscle tone manifest. In addition, professional athletes work hard with a physical therapist or certified athletic trainer.
Many professional athletes contribute their healing to exactly what they bring to their game,a positive attitude. You are able to harness the power of a positive mindset to your own benefit, even though you may not have access to the tools that professional athletes possess.
Advice from the Pros to Boost Your Recovery
Maintain balanced physical conditioning
Make Sure injuries are recognized early and treated promptly
Participate in a complete functional rehabilitation program
Stay healthy while injured
Keep a positive, upbeat mental attitude
Proper Athletic Treatment Recovery Plan
Phases of Care
Recovery from an injury involves a set of logical steps from the time of the injury until you are able to return on the field or court. Every step should be summarized and monitored by your physician and therapist.
During the acute phase of injury, the focus should be on minimizing swelling. This entails the RICE formula (Rest, Ice, Compression, and Elevation), Together with a limitation of actions. Based on the type and severity of your injury, treatment may involve casting, or bracing and surgery in more serious cases.
During the acute period, it’s extremely important to keep overall conditioning while the injury heals. Creative techniques may be used to safely work around the injury. As an example, a runner with a leg injury may often run in plain water or use a bicycle to keep conditioning. By doing exercises if one leg is in a cast, the remainder of the human body can be exercised. Don’t wait till your injury is treated to get back into shape.
In another phase of recovery, you should focus on regaining full motion and strength of the injured limb or joint. Your doctor, physical therapist or certified athletic trainer will help outline an exact treatment plan. For injuries, gentle protective exercises can be started almost immediately. Muscle tone may be preserved by means of strengthening exercises or electric stimulation.
When strength returns to normal, functional drills could be started. For lower extremity injuries, this may include brisk walking, jumping rope, hopping, or light jogging. For upper extremity injuries, effortless ground strokes or light throwing could be carried out. The coordination that might have been lost in the injury can be brought back by specific exercises for agility and balance.
Once you have progressed with mobility, endurance, strength, and agility, and are tolerating functional exercises, you can try higher levels of sport-specific movement routines. Your physical therapist or certified athletic trainer monitors this. You could find that tape, braces, or supports help in this transition time.
Only when you are practicing hard without significant problem, and the healing has progressed to the point at which the probability of injury or harm is reduced, are you ready to return to play. During these phases of recovery, you ought to be carefully monitored. Special attention ought to be given to sufficient warm up following the activity prior to the activity and icing after engaging in the specific sport or physical activity.
Note Of Caution
The rational progression of recovery not only reduces the chance of re-injury but also assures that you will be able to perform at your best when you return to play. Frequently, athletes believe they are all set to return as soon as the limp or even the swelling subsides. They might feel good, but they are probably just 70 to 75% recovered. This invites re-injury.
Sports medicine experts are working on approaches to assist athletes to achieve near 100% healing as fast as the proper cautionary measures allows. The athlete’s health and safety has to be put over all other concerns, although there is enormous pressure to get the athlete back whenever possible.
A systematic recovery program has been successfully utilized every day, at all levels of play, from the recreational athlete to the elite professional or Olympic athlete, by a variety of specialized healthcare professionals. As with any type of sports injury, seek immediate medical attention from a qualified specialist to begin the rehabilitation process.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
By Dr. Alex Jimenez
Additional Topics: Sports Care
Athletes engage in a series of stretches and exercises on a daily basis in order to prevent damage or injury from their specific sports or physical activities as well as to promote and maintain strength, mobility and flexibility. However, when injuries or conditions occur as a result of an accident or due to repetitive degeneration, getting the proper care and treatment can change an athlete’s ability to return to play as soon as possible and restore their original health.
With the presence of blood flow restriction training in discussions surrounding intensity coaches and physiotherapists, people are beginning to seek out programs for the best training procedure which might help them reach new levels of athletic performance.
In arenas that were competitive; an athlete’s practice volume is often restricted by their capacity, not their desire to keep training. With elite athletes there are a handful of variables that influence recovery; sleep, nourishment, training volume, the modality of training, body work…etc.. Athletes are looking for everything they can to be able to recuperate faster so they can train harder. Blood flow restriction training is an alternative and should be included in the dialogue of methods which help you recover.
What is Blood Flow Restriction Training (BFR)?
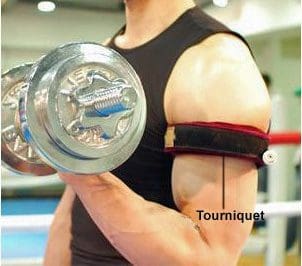
In brief, it is when you use a tourniquet device to restrict blood flow to your extremities while exercising. Faster recovery, and amount of superior training, equals gains.
BFR and Recovery
First let us begin with the thought that BFR does not cause muscle damage. This is an extremely important aspect of BFR training. If we’re currently performing a modality to boost recovery, then we do not want to break down muscle fibers in the procedure.
Think of muscle recovery as an equation of protein balance. Net protein equilibrium muscle protein breakdown. We would like our web protein balance to be over 0 (in the favorable). A positive protein balance suggests we are building muscle, not breaking it down.
There are different markers used in study to quantify muscle breakdown such as CK degrees and myoglobin levels. Delayed onset muscle soreness (DOMS) has also been measured in areas after BFR. The subject revealed no increase in DOMS after blood flow restriction. There seems to be no indirect or direct measures of muscular damage related to BFR when looking at the study. So we can conclude that using BFR will not increase muscle dysfunction following an athlete’s training session.
Process of Recovery with BFR
The very first thing we will look at is the greater release of growth hormone. Studies have shown there to be up to some 290% boost in growth hormone following BFR. Growth hormone is an integral component in collagen synthesis. Collagen synthesis enables the body to restore ligaments and tendons, which are reliant on hydration for strength and their structure.
Tendons, exactly like muscles, are subject to damage following training. When we’ve got higher tendon (collagen) breakdown when compared to tendon (hydration) synthesis we can ultimately wind up with bothersome limb injuries (tendonopathy, tendonitis, tendonosis). Various studies have shown there to be increased cross sectional area and tendon stiffness that was enhanced when comparing raised GH to a control group that was normal without GH.
What exactly does this mean to the athlete? The Growth hormone reaction with blood flow restriction training can lead to tendon strength and durability, thus allowing them to train longer without harm.
Growth hormone can also be correlated with greater healing in bone (thanks to the higher collagen synthesis). A frequent type of sport injury includes stress fractures. A stress fracture is when there’s more collagen breakdown when compared to collagen synthesis. BFR may play a role in helping to stop or limit stress fractures in athletes.
Next let us look at IGF-1. Insulin like growth factor -1 (IGF-1) is ultimately a protein that is connected to muscle growth. When we examine what is needed for muscle development, we could refer back to this equation cited before protein equilibrium muscle protein breakdown. If you have a favorable protein balance we could conclude that muscle development will be achieved by utilizing BFR therapy. More muscle being assembled compared to muscle being destroyed equals more muscle development. If we’re currently attaining a positive protein balance, we could conclude that our muscle fibers are recovering like they ought to be. When comparing to controls, when using BFR training various studies have shown there to be an increased number of IGF-1.
BFR Into Practice
The BFR would take place as the last thing you did before leaving the gym. You can do upper or lower body, however if your goal is strictly muscle recovery, I�d recommend doing the lower extremity. The lower extremity has muscle mass which will create a higher reaction. Since HGH and IGF-1 are carried throughout the blood flow, the result is systemic (whole body). You would be fine doing either the lower or upper extremities. BFR is safe to use on a daily basis, therefore its recommended to switc pper body on your primarily upper body dominant days and the lower body on primarily your lower body dominant days.
The exercise of choice for the lower extremity are some kind of deadlift or squat done at 20 to 30% of your 1RM. The exercise of choice for the upper body would be some kind of push up, row, or press. Once again you are currently aiming for 20-30 percent 1RM. You desire the exercises to be easy. It is not a wonderful notion when performing muscle ups or handstand pushups to perform BFR. That’s a recipe for failure.
The method would be to use 4 sets of 30/15/15/15 reps with a 30 second break between sets and a 2-second concentric and two- second eccentric contraction to get a metabolic reaction. The protocol would be complete in approximately 4-5 minutes.
The placement of the cuffs will be at the peak of your arm, the most proximal segment just before the shoulder, or the top of your leg, the most proximal segment below your hip. We want the limb occlusion pressure to be 80 percent for the lower extremities and 50% to the upper extremities. If you experience numbing and tingling sensations, you’ve constricted too much. It will be uncomfortable, and will be the greatest “pump” and “burn” you’ve ever encounter. There ought to be zero numbness or tingling when performing BFR.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
By Dr. Alex Jimenez
Additional Topics: Sports Care
Athletes engage in a series of stretches and exercises on a daily basis in order to prevent damage or injury from their specific sports or physical activities as well as to promote and maintain strength, mobility and flexibility. However, when injuries or conditions occur as a result of an accident or due to repetitive degeneration, getting the proper care and treatment can change an athlete’s ability to return to play as soon as possible and restore their original health.
BFR or blood flow restriction therapy has been around for a long time, but recently, the evidence for its use in the world that is rehabilitation has begun to emerge. The principle is very simple: that the circulation of blood flow is confined to the area of the human body that’s being trained or undergoing rehabilitation in a certain manner to boost the impacts of the training via lower load (less stress).
Is Blood Flow Restriction Effective?
According to the American College of Sports Medicine, to achieve an increase in muscle size and strength, you want to do 8 to 10 repetitions of an exercise. A moderate to high intensity is deemed to be 65 to 80 percent of their patient’s one rep maximum (the maximum amount of weight a person can lift 1 time). However, the majority of patients that are injured can’t deal with this kind of load, consequently restricting their capacity.
So again we’re faced with the question: Just how can we achieve hypertrophy and gain muscle strength without using heavy loads? The solution involves using a tourniquet to restrict blood flow into a muscle. This technique is known as blood flow restriction training (BFR).
According to the most recent research in the event the appropriate blood flow restriction therapy protocols are utilized, the benefits of the training are equal to those found when using 70 percent of an individual’s maximal load, while using as little as 20 to 30 percent of somebody’s maximum load. The secret is that restricted blood flow training allows healthcare professionals, such as physical therapists, to make a localized region of exercise that is anaerobic.
BFR is a tool that uses a doppler and tourniquet system placed on either thigh or the upper arm to limit blood circulation. After this, it begins to create lactate and hydrogen ions and denies the muscle oxygen. This is what causes the “burning” feeling when we lift heavy weights. The burn is simply the response to being in an active environment of the body. During heavy lifting (65-85%), we create small microtraumas in the muscle that the body then repairs by building more muscle. Together with BFR, we are not generating microtraumas at the muscle, so our body does not have to devote the energy to repair the muscle; rather our bodies just focus on creating the muscle.
Second, soreness is not experienced by us as we would when we were lifting weights. This means we can now lift at low loads (15-30%) and basically gain more muscle strength and size, at a quicker manner, as if we were lifting a more heavier load.
As soon as we create lactate, we activate growth hormone release. The release of IGF-1 subsequently stimulates once growth hormone is released. Such enables your muscles ability to activate; this in turn increases muscle protein synthesis, or our stem cells to the muscle. As previously mentioned, if we were to have muscle breakdown, these stem cells could have to concentrate on repairing muscles building. With blood flow restriction therapy or training, we skip the muscle repair and focus on muscle building. This result is not concentrated throughout the exercise, but impacts the tissues and muscles to create the greater benefit of BFR. BFR has shown to have the ability to help in endurance training and coaching, tendon healing and bone recovery.
All of our muscles are produced from other kinds of fibers, including type 1 which are slow to twitch and rely on oxygen and type 2, which are those we’re currently attempting to build with BFR training and fast-twitch fibers. By limiting the blood flow, we create an environment at the muscle group that compels the increase of more fibers that are type 2. Higher strength gains are the outcome because these type 2 fibers normally can produce more force. Another effect of blood flow restriction is that is allows for a synthesis of proteins needed to build and repair muscles and tissues.
In a treatment setting, this helps us achieve the outcomes for patients faster, and in sports it enables the gains to be attained with less strength and less damage to the muscle. That is why pro and college teams are currently turning to BFR as a training principle. In sports, athletes are attempting to come back to the field quicker after suffering trauma or injury from an accident. Some athletes re-injure themselves by lifting. That is really where BFR can come by lifting loads that are lower and receiving the same, or even much better profits. Healthcare specialists will tend to eliminate strength immediately following a sports injury, but they can not exercise at elevated levels. In this manner, they can not only keep the power but build strength in the process although together with blood flow restriction training.
Is Blood Flow Restriction Safe?
You might be thinking that its effects sounds fantastic, but is it safe? The brief answer is yes, but as with any rehab technique, there are precautions which should be taken and it’s recommended to first seek medical attention from a healthcare professional to discuss the option of BFR therapy for you. We certainly don’t recommend that individuals do this by themselves and tie bands around their limbs. In the practice, specialists can track it as you train and use special devices to know exactly how much you need to train to experience its benefits.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
By Dr. Alex Jimenez
Additional Topics: Sports Care
Athletes engage in a series of stretches and exercises on a daily basis in order to prevent damage or injury from their specific sports or physical activities as well as to promote and maintain strength, mobility and flexibility. However, when injuries or conditions occur as a result of an accident or due to repetitive degeneration, getting the proper care and treatment can change an athlete’s ability to return to play as soon as possible and restore their original health.
Imagine you trained well for a significant race, got yourself into form and cruised through the first half of the course without any issues, and were on pace for a nice PR. All of a sudden, you started to notice tightness in one of your hamstrings. In the beginning, it was a hindrance that could be ignored, but the tightness got steadily worse until your hamstring was a stiff, painful mass of tissue which cried out to cease.
You slowed down, you ceased to stretch, massaged it, but nothing helped. Realizing that this was the conclusion of your race, you limped to the end, disappointed and frustrated that after six months of attentive, time-consuming preparations, some strips of muscular tissue in the back of your thigh had prevented you from attaining your goal. Does this situation sound familiar to someone or has this happened to someone you know?
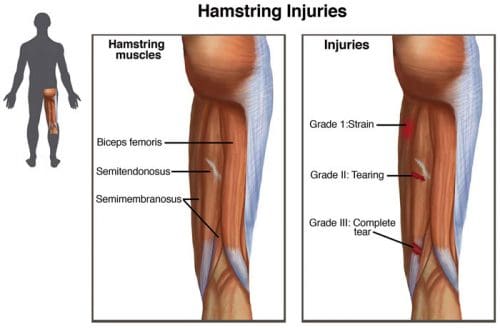
Hamstring Injury Issues
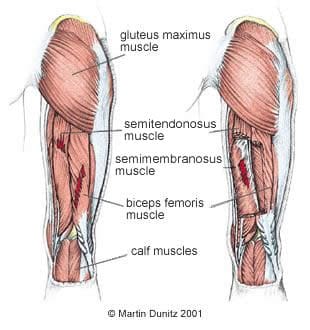
Hamstring difficulties are common among runners, with strains, pulls, tendinitis and tears being the most commonly reported damage or injury to the hamstring muscles. Are hamstring issues common? Most distance runners have developed a scenario called “quad dominance,” a scenario that takes place when the quad muscles overpower the action of the hamstrings at the movement of the leg through a running stride.
Logging a great deal of miles on the streets can put repetitive functional overload on the quadriceps, which makes them powerful, strong and dominant. When the quadriceps contract as you land, the hamstrings, the opposite muscles, act as brakes for your knee to stop against hyperextending in the conclusion motion of a stride.
The quad functions when the knee is locked out in expansion with motion happening in the hip (the forward swing of a stride). The quadriceps work along with the hip flexors to flex the hip as you run. In addition, once the hip is fixated with movement taking place in the knee (when the leg is planted on the floor), the quads function as extensors of the knee.
If your hamstrings are significantly weaker than your quads, due to a continuous loading of the anterior (frontal) chain from jogging or running, particularly seen in athletes, then one of two things will happen: first, your hamstrings will tear as a consequence of not being able to take the load created by the contracting quadriceps and momentum out of hip extension; and two, you will run slower as a consequence of diminished power from the hip flexors and knee extensors since the hamstrings have to contract earlier to have the ability to break the ensuing movement.
Regrettably, once you get yourself into this quad-dominating problem, it’s difficult to undo. Hamstring injuries are rather slow to cure, and athletes regularly spend plenty of time resting before they are able to train without much pain towards carrying out activities. However, like muscle injuries, distress tends to return again and again, particularly because most athletes fail to deal with the root cause of their problems.
When the quadriceps are concentrically contracting (as you land), the hamstrings need to be eccentrically contracting to check the movement. It has been proven for producing activities, that contractions will have limited gains in strength. For this reason, focusing upon loading is critical.
By executing a suitable strengthening program for those hamstrings using a series of specific, isolated, and abnormal exercises, such as those in which muscle fibers lengthen because they contract, you can remove the quad dominance, and keep yourself healthy, powerful and quick. It is possible to begin with the following three simple hamstring exercises below to help treat an athlete’s hamstring injuries, improving strength, flexibility and mobility.
Hamstring Exercises
The exercises here will strengthen the hamstrings while the muscles actively lengthen by mimicking the “grab” of a leg’s swing period whilst jogging. Each of these exercises 8 to 12 times for 3 to 4 sets. On moving from the center, focus, and remember that the emphasis is on the portion of the motion.
Good Morning
A) Start with your thighs locked, arms holding a weight bar on your shoulders with conflicting grasp, back in neutral position and center tight.
B) Slowly bend over at the waist, gently feeling the stretch on down the road. Keep your chest do not hesitate to droop your shoulders toward the floor in an attempt to seem like you are going . Constantly keep the core to support your back.
C) On down the road, maintain the barbell as close to your leg as possible to decrease the pressure on the lower spine. Maintain the back at the neutral position.
D) When you’ve gone as low as possible with your knees locked, start to return up slowly. (Avoid the tendency to jerk upwards or arch your spine. Should you feel inclined to either, use less weight on the bar.)
E) For a sophisticated version, try this exercise one leg at a time by putting the non-exercising leg up on a seat on your side.
Single-Leg Romanian Dead Lift
A) Stand holding a barbell in front of you on your right hand, putting your weight in your right foot. Lean forward 15 degrees or so.
B) Keeping a small bend in your right knee, your back flat and your chest out, lift your left leg straight out behind you as you reduce your body over your right leg. Slide the dumbbell to about mid-shin down your quad and lift your own body back up into an erect posture, keeping your weight onto your right leg. Repeat for 2 to 12 repetitions, then switch hands and legs.
C) To progress this exercise, stand on a barbell or Bosu with the exact same weight, or stay on the floor and increase your weight.
Eccentric Hamstring Curl (with a partner)
A) Kneel on a folded towel or a pile of exercise mats with your toes pulled toward your shins. Keep your hands in front of your chest. Your partner sits behind you, facing your spine, pressing down on your legs with his palms.
B) Keep your core tightup your torso and hips forward so your body forms a straight line from the ears to your knees. As you lower your chest whilst resisting gravity keep this posture. Control the range of motion as far as you can, grab yourself with your hands, then push off the floor in yanking you back up to assist your hamstrings and glutes. (In case you do not have a spouse, you can perform a similar workout on a hamstring washing machine)
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
By Dr. Alex Jimenez
Additional Topics: Sports Care
Athletes engage in a series of stretches and exercises on a daily basis in order to prevent damage or injury from their specific sports or physical activities as well as to promote and maintain strength, mobility and flexibility. However, when injuries or conditions occur as a result of an accident or due to repetitive degeneration, getting the proper care and treatment can change an athlete’s ability to return to play as soon as possible and restore their original health.
Blood Flow Restriction training (BFR) is a style of resistance training that utilizes the custom of wrapping a kind of tourniquet around a limb and training with a relatively light load. It is a practice that has gained quite a bit of popularity in the resistance coaching realm over the last few decades and is something which can benefit training protocols.
If used properly, practical blood flow restriction training (BFR) could help you through hypertrophy plateaus, pack on additional mass and even aid in growth or maintenance of muscle mass during times in which lifting heavy weight is either laborious or impossible. Let’s understand what’s actually going on in the body when it is used by you.
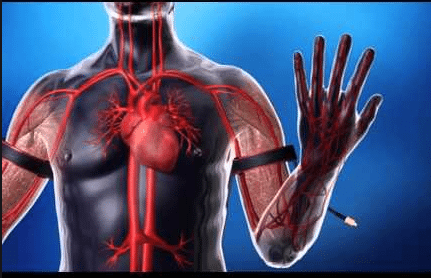
As mentioned prior, BFR demands using some form of tourniquet around a limb so as to inhibit blood flow. However, not all of blood flow is restricted. The purpose of the tourniquet is to prevent what’s known as ‘venous return’ . When you contract a muscle, more blood than ordinary is shuttled to provide the muscle with a myriad of different nutrients, such as oxygen. Typically, if un-wrapped, the blood then returns to the heart through veins so as to rid the muscle of metabolic bi-products like carbon dioxide, lactate, and hydrogen ions (the acidity that makes your muscle “burn off”).
The role of using some form of tourniquet is to inhibit the ‘venous return’ of blood to the heart while still allowing arterial blood circulation to the muscle. By doing this, the blood continues to be shuttled to the muscle and pools without having the ability to escape. It’s believed that the accumulation of blood and bi-products contributes to activation of fast-twitch muscle fibers, which is typically thought to only happen after these are fatigues or due to using fairly heavy loads. By doing this, you increase the potential for the muscle t.
In fact, a recent analysis by suggested that when participants used the same load (40% of 1 RM) and either used a tourniquet or didn’t, the team using BFR observed the same gains in strength and muscle volume as the group that did not. The catch: the BFR team had finished significantly less repeats, and thus less quantity, in addition to less time under pressure. This implies the exact same advantage was observed by them, but achieved in time.
The research appears to indicate that you could complete less work in order to achieve the very same results. Utilizing blood flow restriction training is ideal for times that you are fatigued or simply too sore to execute resistance training that is significant or are just at a time crunch. Additionally, using BFR is a candidate for instances when usage of significant weight is apparently impossible or ill advised, for example post-injury or operation, or being elderly.
Gear
Considering the nature of this kind of training, BFR requires using some form of tourniquet. The easiest and most convenient way to achieve this would be to use some form of strap like an ace bandage or weightlifting knee wraps. If you are able to discover a strap using a comparable elasticity diameter that is smaller, this would be more optimal. When wrapping your limbs, you want to prevent wrap ‘over’ the limb. Otherwise you can risk limiting the muscle’s capacity to contract and your range of movement.
Placement
You will want to put the wrap around the proximal portion of the muscle you’re working. This implies over the muscle and close to the torso. If you are thinking about training forearms and your biceps, you should set the wrap beneath the deltoid. Using this technique for the body requires some careful instructions. Some experts say that when practicing BFR for the body, your leg ought to be wrapped close to the groin area, over the quadriceps. If you’re training calves this would be included. When training BFR for calves, its wise to wrap over the calf and beneath the knee. This is because the common wraps are not really large enough to effectively wrap over the quadriceps.
Wrapping Pressure
When wrapping your muscle, remember to keep in mind that you aren’t attempting to completely restrict blood flow. You still require blood circulation to the muscle. As such, when you wrap, you should try to shoot for wrapping the arm at about a 7 out of 10, with ten being very painful and a complete loss of blood flow. If your arm is totally asleep before you even begin training, the wrap is too tight.�If you complete a set of exercises and your arm is not pumped or fatigued, then you’ve probably not wrapped the bands tight enough.
First and foremost, a majority of experts concur that this kind of training is in fact a safe practice provided that it’s executed properly. To be able to maintain proper safety, ensure that you have not completely restricted blood circulation. Further, as soon as you’ve finished your sets, be certain that you remove the wrap in order to give the muscle blood supply and permit the used blood to be recycled. Should you have them too tight or keep the wraps on too long, you run the danger of inducing tissue and cell death. This isn’t advised. Further, if you have higher blood pressure or heart problems BFR, or blood flow restriction, training is not suggested.
There’s also some evidence to indicate that musculature which isn’t directly occluded, for example chest and shoulders, can experience some benefit from BFR. That is interesting because there was a long belief that advantage would be seen by muscle below the tourniquet. A current meta-analysis indicated that despite evidence, the indirect muscle (chest and shoulders) may see increased benefit in comparison to the same training without a tourniquet. If you are feeling tired, yet still want to get a chest and shoulder pump, then it may help you to wrap your arms.
Finally, BFR shouldn’t be used only in place of different sorts of training. Outcomes like power, power output, hypertrophy and force production rely on coaching specificity and varying immunity (i.e to be able to maximize strength, you need to train with heavier loads to get lower repetitions). The study suggests that blood flow restriction training could be as good as other types of instruction, not exceptional. Therefore, blood flow restriction, or BFR, training may be a useful tool within a resistance-training schedule that is well-rounded.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
By Dr. Alex Jimenez
Additional Topics: Sports Care
Athletes engage in a series of stretches and exercises on a daily basis in order to prevent damage or injury from their specific sports or physical activities as well as to promote and maintain strength, mobility and flexibility. However, when injuries or conditions occur as a result of an accident or due to repetitive degeneration, getting the proper care and treatment can change an athlete’s ability to return to play as soon as possible and restore their original health.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine

 Promote Healing
Promote Healing
 Signs Of IT Band Syndrome
Signs Of IT Band Syndrome If you are a runner, you will be able to distinguish ITBS by:
If you are a runner, you will be able to distinguish ITBS by: If you want to do away with pain, you might consider looking for a fit pair of shoes as they will reduce any pain, causing issues in the long run. Pay attention to small specifics like shoes that offer enough heel space, sufficient toe box room, and enough space for wide feet. Your toes should be able to move freely without being constricted.
If you want to do away with pain, you might consider looking for a fit pair of shoes as they will reduce any pain, causing issues in the long run. Pay attention to small specifics like shoes that offer enough heel space, sufficient toe box room, and enough space for wide feet. Your toes should be able to move freely without being constricted. This upgraded version is lightweight to help with any knee problems. It offers you comfort through cushioning that help absorb shock as you run as well as other features like grip, fit, and durability. The shoe has an added outer sole to ensure it lasts you as long as possible.
This upgraded version is lightweight to help with any knee problems. It offers you comfort through cushioning that help absorb shock as you run as well as other features like grip, fit, and durability. The shoe has an added outer sole to ensure it lasts you as long as possible. It tops the list of 5 best running shoes. Also, it has remained the first choice for most runners with knee pain issues. This pair offers all the above functionalities too, making it your best choice.
It tops the list of 5 best running shoes. Also, it has remained the first choice for most runners with knee pain issues. This pair offers all the above functionalities too, making it your best choice. Puma models have never disappointed, and this one is no exception. Puma Faas 600 is the solution to your knee pain. It is also an affordable option for the short-handed.
Puma models have never disappointed, and this one is no exception. Puma Faas 600 is the solution to your knee pain. It is also an affordable option for the short-handed. This is another great choice on the list. It is one of the New Balance Fresh Foam Series. Its midsole offers you the required support coupled with comfort to eliminate knee pains.
This is another great choice on the list. It is one of the New Balance Fresh Foam Series. Its midsole offers you the required support coupled with comfort to eliminate knee pains. This is the 16th edition of the Saucony Hurricane, which offers a combination of steadiness and protection. Those with knee pain have agreed with the stability offered by this shoe. It is also cushioned to help you go for long runs without any pain or injury. It is perfect for heavy runners and those who are out of shape due to inactivity.
This is the 16th edition of the Saucony Hurricane, which offers a combination of steadiness and protection. Those with knee pain have agreed with the stability offered by this shoe. It is also cushioned to help you go for long runs without any pain or injury. It is perfect for heavy runners and those who are out of shape due to inactivity.