A big part of sports is avoiding and preventing injuries, as injury prevention is far better than rehabilitation and recovery. This is where prehabilitation comes in. Prehabilitation is a personalized, constantly evolving, and developing strengthening exercise program. The program aims to provide sports-specific targeted exercises and activities to maintain athletes’ physical abilities and mental preparedness for their sport. The first step is for an athletic trainer, sports chiropractor, and physical therapist to examine the individual.
Prehabilitation
Everybody is different when it comes to developing an effective prehabilitation program. Every individual’s program should be progressive and re-evaluated to adapt and adjust to the athlete’s needs. The first step is learning to prevent injuries and following basic injury prevention protocols. Knowing what to do when the body sustains an injury, like home treatment and when it’s time to see a doctor.
Athletes
Athletes of all levels are recommended to incorporate a prehabilitation program into their training. As athletes engage in their sport, their bodies adjust to the physical demands of practicing, playing, and training. Imbalances can happen naturally with normal activity but become more pronounced with each practice, game, and training session and often are the cause of injury. The repetitive movements and regular stresses can cause neuromusculoskeletal symptoms to present. This includes:
Tightness of muscle groups.
Pain and discomfort symptoms.
Stabilization issues.
Strength imbalances.
Program
A chiropractic therapist will measure the individual’s range of motion and strength, biomechanics, evaluate medical history, and present health status. Individuals with an injury or a condition can also benefit from prehabilitation.
Each program is personalized and will address total body balance, sports-specific needs, and weaknesses.
The exercises will balance strength, coordination, range of motion, and stabilization.
The premise is looking at and comparing movements from left to right, front to back, and upper to lower body.
Activities can be subtle, focused exercises or a complex movement sequence to stabilize or improve a specific skill.
Programs focus on strengthening and stabilizing the core, abdominals, hips, and back.
Instability is common and often presents from a lack of core training, as athletes tend to focus on what parts of the body their specific sport utilizes, leaving the core without a regular training routine.
A prehabilitation program has to be constantly updated to adjust to the individual’s progress.
Tools like foam rollers, balance boards, weights, and exercise balls are used.
Training
Prehabilitation should start before any acute or chronic injury occurs, but often it takes a few injuries for individuals to decide to get into a prehabilitation program. Depending on an athlete’s training cycle, prehabilitation can be incorporated into practice or as an independent workout and become part of an athlete’s training routine. A session can include the following:
Warm-up and cool-down exercises.
Exercises to perform while resting or waiting during practice.
A targeted workout on specific weaknesses.
A complete workout for days off or active rest days.
Mini workouts for when traveling and recovery days.
For athletes, feeling challenged and motivated can be the difference between success and failure. Working with a trainer, sports chiropractor, and therapists who know sports, understand athletic needs, and communicate well, will contribute to a successful prehabilitation program.
Improving Athletic Performance
References
Durrand, James et al. “Prehabilitation.” Clinical medicine (London, England) vol. 19,6 (2019): 458-464. doi:10.7861/clinmed.2019-0257
Giesche, Florian, et al. “Evidence for the effects of prehabilitation before ACL-reconstruction on return to sport-related and self-reported knee function: A systematic review.” PloS one vol. 15,10 e0240192. 28 Oct. 2020, doi:10.1371/journal.pone.0240192
Halloway S, Buchholz SW, Wilbur J, Schoeny ME. Prehabilitation Interventions for Older Adults: An Integrative Review. Western Journal of Nursing Research. 2015;37(1):103-123. doi:10.1177/0193945914551006
Smith-Ryan, Abbie E et al. “Nutritional Considerations and Strategies to Facilitate Injury Recovery and Rehabilitation.” Journal of athletic training vol. 55,9 (2020): 918-930. doi:10.4085/1062-6050-550-19
Vincent, Heather K, and Kevin R Vincent. “Rehabilitation and Prehabilitation for Upper Extremity in Throwing Sports: Emphasis on Lacrosse.” Current sports medicine reports vol. 18,6 (2019): 229-238. doi:10.1249/JSR.0000000000000606
Vincent, Heather K et al. “Injury Prevention, Safe Training Techniques, Rehabilitation, and Return to Sport in Trail Runners.” Arthroscopy, sports medicine, and rehabilitation vol. 4,1 e151-e162. 28 Jan. 2022, doi:10.1016/j.asmr.2021.09.032
Softball and baseball require running, jumping, throwing, and swinging movements. Even for the fittest athletes and weekend warriors, the body and the neuromusculoskeletal system will go through overuse injuries, throwing-related injuries, sliding injuries, falls, collisions, and getting hit by the ball. Chiropractic and physical therapy can assist athletes by integrating strength training, body realignment, and rehabilitation injury recovery.
Softball and Baseball Injuries
Baseball and softball injuries are generally defined as either acute/traumatic or cumulative/overuse injuries. Both types can occur in various body areas, for example, a knee injury caused by a fall or quick repositioning shift.
Acute/Traumatic
Injuries occur from traumatic force or impact.
Overuse/Cumulative
These occur over time from repeated stress on the muscles, joints, and soft tissues.
Often athletes return too soon to play, not giving the injury enough time to heal fully.
They begin as small aches and pains that can progress into chronic conditions if not treated.
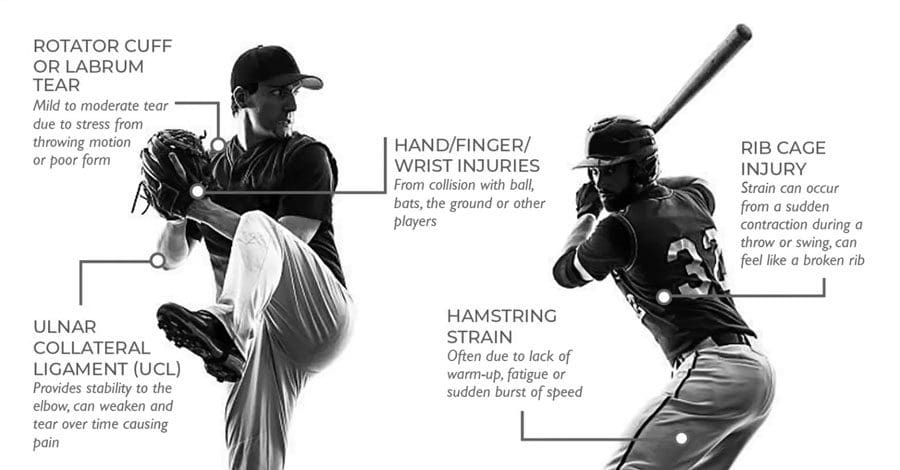
Shoulder
Shoulder overuse injuries are very common. Constantly performing the throwing movements and high-speed throwing strains the joints, muscles, tendons, and ligaments.
In softball, bicep injuries are more common than shoulder injuries.
In baseball, the overhead throwing position leads to shoulder problems.
Frozen Shoulder
Characterized by a restricted range of motion and pain.
Athletes with frequent shoulder injuries have an increased risk.
Shoulder Instability
Softball and baseball players are more susceptible to injury from overhead throwing, which stretches the shoulder capsule and ligaments.
Shoulder instability can lead to loose joints and dislocation.
Shoulder Separation
This is the tearing of the ligaments that connect the shoulder blade to the collarbone.
This is often a traumatic injury that occurs during a collision or fall with outstretched hands.
Shoulder Tendinitis, Bursitis, and Impingement Syndrome
These are overuse injuries in which the shoulder joint becomes inflamed, restricting movement.
This is an injury to the growth plate on the inside of the elbow.
It can be caused by the wrist flexors pulling on the inside.
It is typically attributed to overuse and improper mechanics when throwing.
Tennis Elbow
This overuse injury on the outside of the elbow makes it difficult to lift or grasp objects.
Hand and Wrist
Softball and baseball can cause hand and wrist injuries from catching, colliding, falling, and overuse. Damage to a hand or wrist is typically caused by repetitive stress and/or a sudden impact.
Finger Fractures
These can be caused by impact on the ball or falls.
This can happen during contact with another player or diving for a ball and hitting the ground hard or at an awkward angle.
Sprains
A fall or impact from the ball or another player can cause these.
Tendinitis
This is an overuse injury, often from pitching and/or throwing.
Back
Catchers are especially prone to back injury because of the crouched position and overhead throwing.
Softball pitchers also experience back strain from the windmill pitching action.
Common conditions include chronic muscle strains, herniated discs, low back issues, sciatica symptoms, and pain.
Knee
Softball and baseball players quickly twist or rotate their knees, making them more susceptible to injuries. Sprains, meniscus tears, ACL tears, and hamstring strains are common.
Aggressive twisting and pivoting can cause swelling, stiffness, and pain.
Running and sudden changes in direction can result in acute knee injuries and overuse injuries.
Knee issues require examination for proper diagnosis.
Other common injuries include ankle sprains, stress fractures, and tendonitis in the foot and ankle.
Chiropractic
Chiropractors work with a massage therapy team to treat various musculoskeletal conditions. Chiropractic specializes in spinal adjustments and other treatments, including joint manipulation, myofascial release, MET techniques, trigger point therapy, and electrical stimulation. It encourages expedited recovery for sports-related injuries because instead of focusing on just the injuries, chiropractic assesses the mechanics of the whole body through proper alignment and release of constricted tissues. Adjustments of the spine and extremities allow the body to realign for better overall functionality, reduce pressure, improve blood circulation, and reduce inflammation to promote increased and thorough healing.
Improving Athletic Performance Through Chiropractic
References
Greiner, Justin J et al. “Pitching Behaviors in Youth Fast-Pitched Softball: High Pitching Volumes With Unequal Pitch Counts Among Pitchers are Common.” Journal of pediatric orthopedics vol. 42,7 (2022): e747-e752. doi:10.1097/BPO.0000000000002182
Janda, David H. “The prevention of baseball and softball injuries.” Clinical orthopedics and related research,409 (2003): 20-8. doi:10.1097/01.blo.0000057789.10364.e3
Shanley, Ellen, and Chuck Thigpen. “Throwing injuries in the adolescent athlete.” International Journal of sports physical therapy vol. 8,5 (2013): 630-40.
Shanley, Ellen, et al. “Incidence of injuries in high school softball and baseball players.” Journal of athletic training vol. 46,6 (2011): 648-54. doi:10.4085/1062-6050-46.6.648
Trehan, Samir K, and Andrew J Weiland. “Baseball and softball injuries: elbow, wrist, and hand.” The Journal of hand surgery vol. 40,4 (2015): 826-30. doi:10.1016/j.jhsa.2014.11.024
Wang, Quincy. “Baseball and softball injuries.” Current sports medicine reports vol. 5,3 (2006): 115-9. doi:10.1097/01.csmr.0000306299.95448.cd
Zaremski, Jason L et al. “Sport Specialization and Overuse Injuries in Adolescent Throwing Athletes: A Narrative Review.” Journal of athletic training vol. 54,10 (2019): 1030-1039. doi:10.4085/1062-6050-333-18
Sports exercise headaches are exertion headaches that involve pain during or immediately after sports, exercise, or some physical activity. They come on quickly but can last a few minutes, hours, or days. Activities associated with exercise headaches include running, weightlifting, tennis, swimming, and rowing. Chiropractic, massage, decompression, and traction therapies can realign the body and relax the muscles allowing for optimal circulation and certain strategies to help prevent future episodes. Usually, there is no underlying disease or disorder, but it is recommended to talk to a healthcare provider to make sure.
Sports Exercise Headaches
When individuals exert their bodies intensely, they need added blood and oxygen, particularly with activities that involve tightening/tensing the abdominal muscles or increasing chest pressure. Doctors and scientists believe an exertional headache occurs when intense physical activity causes the veins and arteries to expand to circulate more blood. The expansion and increased blood circulation generate pressure in the skull that can cause pain.
Alternate Triggers
Exercising is not the only cause; other physical activities that can trigger an exertion headache include:
Sneezing
Coughing
Straining to use the bathroom
Sexual intercourse
Lifting or moving a heavy object
Symptoms
Symptoms of a sports exercise headache include:
Neck stiffness or pain
Pain on one or both sides of the head
Pulsating pain discomfort
Throbbing pain discomfort
Shoulder tightness, discomfort, and/or pain
Sometimes individuals report the headache can feel like a migraine that could include:
Vision problems like blind spots
Nausea
Vomiting
Light sensitivity
Most exercise headaches last five to 48 hours and can continue for three to six months.
Diagnosis
An underlying disease or disorder does not cause most exertional headaches. However, individuals experiencing severe or frequent headaches should consult their doctor or a healthcare provider. Tests will be ordered to rule out possible causes that include:
MRI will take computer-generated images of the brain.
A spinal tap/lumbar puncture takes a sample of fluid from the spine for testing.
If there is no underlying cause found, the medical provider can diagnose exertion headaches if there have been at least two headaches that:
Were caused by exercise or physical activity.
Started during or after the physical activity.
Lasted less than 48 hours.
Chiropractic Treatment
According to the American Chiropractic Association, spinal adjustments are an effective headache treatment option. This includes migraines, tension headaches, or sports exercise headaches. Using the targeted approaches, chiropractic restores the body’s natural alignment to improve function and alleviate stress on the nervous system. This allows the body to operate at optimal levels reducing muscle stress and muscle tension.
DOC Decompression Table
References
American Migraine Foundation. Secondary Headaches. (https://americanmigrainefoundation.org/resource-library/secondary-headaches/) Accessed 11/17/2021.
Evans, Randolph W. “Sports and Headaches.” Headache vol. 58,3 (2018): 426-437. doi:10.1111/head.13263
International Headache Society. HIS Classification ICHD-3. (https://ichd-3.org/other-primary-headache-disorders/4-2-primary-exercise-headache/) Accessed 11/17/2021.
McCrory, P. “Headaches and exercise.” Sports medicine (Auckland, N.Z.) vol. 30,3 (2000): 221-9. doi:10.2165/00007256-200030030-00006
National Headache Foundation. Exertional Headaches. (https://headaches.org/2007/10/25/exertional-headaches/) Accessed 11/17/2021.
Ramadan, Nabih M. “Sports-related headache.” Current pain and headache reports vol. 8,4 (2004): 301-5. doi:10.1007/s11916-004-0012-1
Trotta K, Hyde J. Exercise-induced headaches: prevention, management, and treatment. (https://www.uspharmacist.com/article/exerciseinduced-headaches-prevention-management-and-treatment) U.S. Pharm. 2017;42(1):33-36. Accessed 11/17/2021.
The game of baseball takes a toll on the body, especially when players advance from little league to high school, college, minor league, and the pros. The most common baseball injuries can range from mild to severe, from normal wear and tear on the joints and muscles to repetitive stress injuries, collisions with other players, getting hit with the ball, or bodily trauma. A chiropractor can provide ideal treatment for players of all ages and levels with decreased downtime and expedited healing and recovery.
Baseball Injuries
Although there have been a lot of advances in player safety and health, from helmets with face guards to shin and arm padding, the equipment lessens the impact and risks of injury. The game still involves running, sliding, twisting, and jumping, causing the body to maneuver awkwardly. Players often report sliding into first, feeling a pop or twisting to catch a fly ball, and feeling something snap. The most common injuries include:
Torn Labrum
Cartilage surrounding the shoulder joint socket, known as the labrum, often gets torn.
The soft tissue keeps the bones in place and provides stability.
Pitching and throwing motions stress the labrum.
With time, the cartilage begins to overstretch and tear, leading to swelling, shoulder pain, weakness, and overall instability.
Rotator Cuff Tears
The rotator cuff structure involves a complex set of tendons and muscles that stabilize the shoulder.
Pitchers are the most vulnerable, but all players are susceptible.
Cases are caused by not warming up and stretching correctly and repetitive/overuse movements.
Swelling and pain are the most common symptoms.
With a severe tear, a player will lose the ability to rotate the shoulder correctly.
Shoulder Instability or Dead Arm
This is when the shoulder muscles become overly fatigued, and the joint becomes unstable, losing the ability to throw precisely.
The condition is called dead arm by players and trainers.
This type of injury is caused by overuse and repeated stress.
Healing involves letting the shoulder rest for an extended period, but treatment, like chiropractic or physical therapy, could be recommended depending on the severity.
Pitchers Elbow
A pitcher’s elbow injury is caused by overuse and sustained/repeated damage to the tendons that rotate the wrist.
Pain and swelling occur along the inside of the elbow and forearm.
Wrist Tendonitis and Trauma
Wrist Tendonitis or tenosynovitis happens when the ligaments and tendons become tender, swollen, ruptured, or torn.
This causes inflammation, pain, and weakness.
Trauma injuries can result from collisions with another player, the ground, or a ball.
Knee Tears and Trauma
Knee injuries can be caused by normal wear and tear, overuse, or traumatic impact.
The fibrous bands are what stabilize and cushion the knee.
Overuse and any awkward movement can cause the tearing of the various ligaments.
The bands can develop micro-tears or complete ruptures, causing inflammation, pain, and instability.
Chiropractic Care and Rehabilitation
Chiropractic treatment and physical therapy have been found to help athletes maintain flexibility and range of motion, rehabilitate the body after an injury, and prevent new injuries or worsening of current injuries.
Chiropractic helps stretch and flex the muscles to stay limber and less prone to injury.
Chiropractic is a natural pain reliever for sore muscles and joint pain.
Physical therapy can strengthen an injured area during recovery and educate on proper form and techniques.
Taping and strapping can help support the elbows, wrists, ankles, and knees, reducing stress.
A combination of treatment approaches can help decrease recovery time so players can get back on the field.
Shoulder Adjustment Baseball Injuries
References
Bullock, Garrett S et al. “Shoulder Range of Motion and Baseball Arm Injuries: A Systematic Review and Meta-Analysis.” Journal of athletic training vol. 53,12 (2018): 1190-1199. doi:10.4085/1062-6050-439-17
Lyman, Stephen, and Glenn S Fleisig. “Baseball injuries.” Medicine and sport science vol. 49 (2005): 9-30. doi:10.1159/000085340
Matsel, Kyle A et al. “Current Concepts in Arm Care Exercise Programs and Injury Risk Reduction in Adolescent Baseball Players: A Clinical Review.” Sports health vol. 13,3 (2021): 245-250. doi:10.1177/1941738120976384
Shitara, Hitoshi, et al. “Shoulder Stretching Intervention Reduces the Incidence of Shoulder and Elbow Injuries in High School Baseball Players: a Time-to-Event Analysis.” Scientific reports vol. 7 45304. 27 Mar. 2017, doi:10.1038/srep45304
Wilk, Kevin E, and Christopher A Arrigo. “Rehabilitation of Elbow Injuries: Nonoperative and Operative.” Clinics in sports medicine vol. 39,3 (2020): 687-715. doi:10.1016/j.csm.2020.02.010
Whenever stepping out onto a playing field or gym, there is a risk of suffering sports back injuries. Back pulls, strain and sprain injuries are the most common. Low back pain is one of the most prevalent complaints at all levels of competition. 90% of these acute back injuries will heal on their own, usually in about three months. However, sometimes these injuries can be more severe and require professional medical care. Treatment options for different groups of athletes include nonsurgical motorized spinal decompression.
Sports Back Injuries
Injury mechanisms vary from sport to sport, but there are recommendations regarding spinal decompression treatment for these injuries and return to play. Chiropractic healthcare specialists understand the sport-specific injury patterns and treatment guidelines for athletes following a back injury. Spinal decompression treatments are beneficial and result in higher rates of return to play depending on the specific sport of the injured athlete. A chiropractor will create a personalized spinal decompression treatment plan for the sport-specific context to meet the athlete’s short and long-term needs.
An estimated 10–15% of athletes will experience low back pain.
All types of sports place increased stress on the lumbar spine through physically demanding and repetitive movements/motions.
The repetitive shifting, bending, twisting, jumping, flexion, extension, and spinal axial loadingmotions contribute to low back pain even though the athletes are in top shape with increased strength and flexibility.
Injury patterns demonstrate the increased stresses that athletes place on the lumbar spine.
Common Spine Sports Injuries
Cervical Neck Injuries
Stingers are a type of neck injury.
A stinger is also known as a burner is an injury that happens when the head or neck gets hit to one side, causing the shoulder to be pulled in the opposite direction.
These injuries manifest as numbness or tingling in the shoulder from stretching or compressing the cervical nerve roots.
Lumbar Lower Back Sprains and Strains
When trying to lift too much weight or using an improper lifting technique when working out with weights.
Fast running, quick stopping, and shifting can cause the low back and hip muscles to get overly pulled/stretched.
Staying low to the ground and springing/jumping up can cause abnormal stretching or tearing of the muscle fibers.
Fractures and Injuries to the Supporting Spinal Structures
In sports that involve repetitive extension movements, spinal stress fractures are relatively common.
Excessive and repeated strain to the spinal column area leads to low back pain and injury.
Nonsurgical Spinal Decompression
Nonsurgical spinal decompression is motorized traction that is used to relieve compression pressure, restore spinal disc height, and relieve back pain.
Spinal decompression works to gently stretch the spine changing the force and position of the spine.
The gel-like cushions between the vertebrae are pulled to open up the spacing taking pressure off nerves and other structures.
This allows bulging or herniated discs to return to their normal position and promotes optimal circulation of blood, water, oxygen, and nutrient-rich fluids into the discs to heal, as well as, injured or diseased spinal nerve roots.
DRX 9000 Decompression
References
Ball, Jacob R et al. “Lumbar Spine Injuries in Sports: Review of the Literature and Current Treatment Recommendations.” Sports medicine – open vol. 5,1 26. 24 Jun. 2019, doi:10.1186/s40798-019-0199-7
Jonasson, Pall et al. “Prevalence of joint-related pain in the extremities and spine in five groups of top athletes.” Knee surgery, sports traumatology, arthroscopy: official journal of the ESSKA vol. 19,9 (2011): 1540-6. doi:10.1007/s00167-011-1539-4
Lawrence, James P et al. “Back pain in athletes.” The Journal of the American Academy of Orthopaedic Surgeons vol. 14,13 (2006): 726-35. doi:10.5435/00124635-200612000-00004
Petering, Ryan C, and Charles Webb. “Treatment options for low back pain in athletes.” Sports health vol. 3,6 (2011): 550-5. doi:10.1177/1941738111416446
Sanchez, Anthony R 2nd et al. “Field-side and prehospital management of the spine-injured athlete.” Current sports medicine reports vol. 4,1 (2005): 50-5. doi:10.1097/01.csmr.0000306072.44520.22
Squat exercises are highly effective, as they strengthen the back and core muscles, helping the prevention of injury. They can be done anywhere with or without equipment like weights and resistance bands and can be part of an aerobic workout. Squatting requires following proper form and posture. Using the improper form, adding too much weight too soon, overdoing it without enough recovery time can cause soreness, back pain, and injury. Having muscle soreness after performing squats is expected; however, if symptoms like chronic soreness, tingling, numbness, or sharp aches that come and go, begin to appear, it is recommended to consult a medical trainer, chiropractor, doctor, or spine specialist to evaluate the symptoms, and if necessary develop a treatment plan, as well as a prevention plan to continue exercising safely.
Squat Exercises
Squatting is a highly beneficial form of exercise. Athletes, trainers, coaches, and individuals just staying healthy use the technique as a part of their training and workouts. This is because squatting increases core muscle strength, increasing body power. Squat exercises benefits include:
Increased Flexibility
Improved strength and a range of motion allow the body to move flawlessly in various directions with minimal effort.
Increased Core Strength
All major muscles work together during a squat.
This increases muscle stabilization, maintains body balance, increasing core strength.
Injury Prevention
Squats work all leg muscles simultaneously, synchronizing the body.
This increases body stability decreasing the risk of injury.
Back Pain and Potential Injury
The spine is exposed and unprotected during a squat. This is where back pain and injury can happen. Potential causes include:
Priming each muscle is recommended. This could be:
Starting with glute work.
Then planks to activate the core.
Finish off with stretching and range of motion exercises.
A personal trainer can assist in creating a customized workout routine.
Starting Position
The feet should always face forward to protect the hips and knees when beginning a squat.
If the feet face at an angle, the form can be impacted, leading to back pain or collapsing arches.
Spinal Alignment
Maintaining a straight-ahead or upward gaze, which increases center awareness during squat exercises, can prevent the body from leaning forward and placing stress on the spine.
Only squat as far as possible, making sure to feel in control and maintain the form.
Squatting too deep can cause muscle strain leading to pain.
Focus on form, as it is more important than depth.
Joint mobility
Ankle mobility and stability are essential to balance and control.
If the ankle is compromised, the feet could lift off the floor, forcing the body to compensate, leading to strain and potential injuries.
Barbell back squats are more advanced and, if done incorrectly, can cause injury.
A chiropractor or physical therapist will be able to evaluate spinal health, exercise form, and advise if there is an issue.
Body Composition
Achieve Health and Fitness Goals By Doing What You Enjoy
Don’t engage in workouts or fitness programs that make you miserable. Do workouts/activities that you enjoy and have fun doing. Exercise for the love of the body, keeping it healthy and in shape, not because there is a feeling of obligation.
Individuals who don’t like lifting weights try using resistance bands or bodyweight exercises.
The same goes for nutrition. Don’t base diet and supplement choices on misperceptions about health.
References
Calatayud, Joaquín et al. “Tolerability and Muscle Activity of Core Muscle Exercises in Chronic Low-back Pain.” International journal of environmental research and public health vol. 16,19 3509. 20 Sep. 2019, doi:10.3390/ijerph16193509
Clark, Dave R et al. “Muscle activation in the loaded free barbell squat: a brief review.” Journal of strength and conditioning research vol. 26,4 (2012): 1169-78. doi:10.1519/JSC.0b013e31822d533d
Cortell-Tormo, Juan M et al. “Effects of functional resistance training on fitness and quality of life in females with chronic nonspecific low-back pain.” Journal of back and musculoskeletal rehabilitation vol. 31,1 (2018): 95-105. doi:10.3233/BMR-169684
Donnelly, David V et al. “The effect of the direction of gaze on the kinematics of the squat exercise.” Journal of strength and conditioning research vol. 20,1 (2006): 145-50. doi:10.1519/R-16434.1
Zawadka, Magdalena et al. “Altered squat movement pattern in patients with chronic low back pain.” Annals of agricultural and environmental medicine: AAEM vol. 28,1 (2021): 158-162. doi:10.26444/aaem/117708
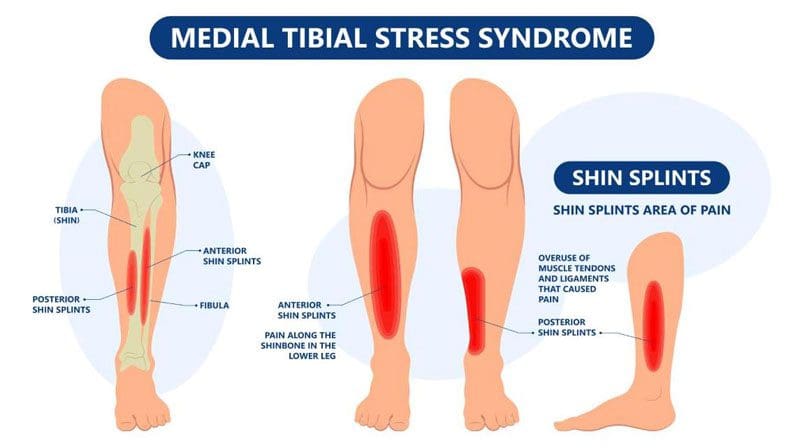
When stress is placed on the shins with physical activity from walking, running, or exercise, the connective tissues attaching the leg muscles to the tibia can become inflamed, causing medial tibial stress syndrome, more commonly known as shin splints. This inflammation is caused by tiny tears in the muscles and tendons of the shin. Chronic shin pain could be related to foot arch problems, underlying issues with the muscles, or shoes that don’t support the feet properly. Although it usually goes away within a few days, it’s important to monitor to ensure that it does not progress into a stress fracture. A chiropractor can offer treatments to relieve the pain and help prevent shin splints from recurring.
Medial Tibial Stress Syndrome
Medial tibial stress syndrome can impact anyone. It can come from walking far distances or in awkward positions like going downstairs with small steps, jumping rope, and playing with the kids on the playground can all cause burning, tightness, and pain in the shins. Shin splints affect individuals differently. For some, the pain recedes when the triggering activity is stopped. For others, the pain can become a chronic condition that results in continuous pain, even when at rest.
The Shin
The shin is a part of the tibia bone in the lower leg.
This bone absorbs the shocks when moving through daily activities.
The muscles that run along the shin support the foot’s arch and raise the toes during movement.
Medial tibial stress syndrome is caused by excessive force on the shinbone and the tissue around it, which causes the muscles to swell and increases pressure around the bone.
If left untreated, small tears in the muscle and the bone can form, leading to chronic pain and stress fractures.
Medial tibial stress syndrome is more likely to happen from:
Not stretching before physical activity or exercise.
Constantly walking or running on hard surfaces.
Wearing the wrong shoes that don’t provide enough cushioning or arch support.
Over-exertion on the body with activity and movement.
The body is not given the proper amount of time to recover.
Athletes often experience shin splints when they’ve intensified their training routine or changed it up.
Symptoms
Pain during exercise or activity.
Pain in the front of the lower leg.
Soreness in the lower leg.
Swelling in the lower leg.
Shin is hot to the touch.
Treatment
Whenever pain is being experienced, some muscles will either get tight or weak in response. By identifying the weak and/or tight muscles, a chiropractor can prescribe stretches and exercises that will help alleviate the pain and prevent it. One of the main principles of chiropractic is to treat the body as an interconnected system. A chiropractor may work on an unrelated part of the body to treat the symptomatic area. For example, they may work to align the spine and pelvis to lessen the impact on the lower legs.
Part of a treatment plan may include:
Soft Tissue Mobilization
A handheld instrument loosens tight tissues during soft tissue mobilization therapy and breaks scar tissue around the tibia.
Massaging tight muscles in the leg keeps them loose and alleviates the pain.
Percussion massage can be added to reduce muscle knots, improve blood flow, and loosen up scar tissue.
The treatment relieves pain and can help avoid shin splints when returning to normal activities.
Ultrasound and Low Laser Therapy
Ultrasound and low laser therapy use heat to warm the deep tissues in the lower leg gently.
The treatment eases pain, reduces inflammation, swelling, and increases blood flow.
Kinesio Taping
Applying flexible Kinesio tape to the foot and lower leg can reduce stress on the shins.
The chiropractor or physical therapist will show how to apply the tape correctly.
Foot Orthotics
Individuals may be more likely to develop shin splints if they have high or low arches or their feet tend to roll inward or outward when walking.
Prescription foot orthotics can be made to keep the feet properly balanced and supported.
Stretching Exercises
Shin splints could be related to tight muscles in the back of the calf and weak muscles in the front of the lower leg.
A chiropractor or physical therapist will show stretching and strengthening exercises to maintain muscle balance.
Body Composition
Retaining Water Due To Salt Intake
Salt/sodium is everywhere and hard to avoid.
It might not be a surprise that a single patty cheeseburger contains over 500 mg of sodium – almost a quarter of the daily recommended level, but it is a surprise to know that the ranch dressing on a salad contains as much as 270 mg or a tablespoon of soy sauce on a healthy, vegetable-only stir-fry has 879 mg of sodium. The Mayo Clinic estimates that the average individual consumes about 3,400 mg of sodium a day: close to double what is recommended. Sodium is linked with water retention, and it is the kidneys’ job to expel unneeded sodium out of the body. Until the kidneys activate, an individual will temporarily be retaining extra water. If daily water and sodium intake habits change daily, this can contribute to water retention, causing fluctuations in daily weight. So, if an individual was on a diet but flooded the body with more salt than usual, expect to see a temporary increase in weight.
References
Bates, P. “Shin splints–a literature review.” British journal of sports medicine vol. 19,3 (1985): 132-7. doi:10.1136/bjsm.19.3.132
Chiropractic Economics: The Science Behind Percussion Massage.
Gross, ML et al. “Effectiveness of orthotic shoe inserts in the long-distance runner.” The American journal of sports medicine vol. 19,4 (1991): 409-12. doi:10.1177/036354659101900416
Heer, Martina et al. “Increasing sodium intake from a previous low or high intake affects water, electrolyte and acid-base balance differently.” The British journal of nutrition vol. 101,9 (2009): 1286-94. doi:10.1017/S0007114508088041
McClure, Charles J. and Robert Oh. “Medial Tibial Stress Syndrome.” StatPearls, StatPearls Publishing, 11 August 2021.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine