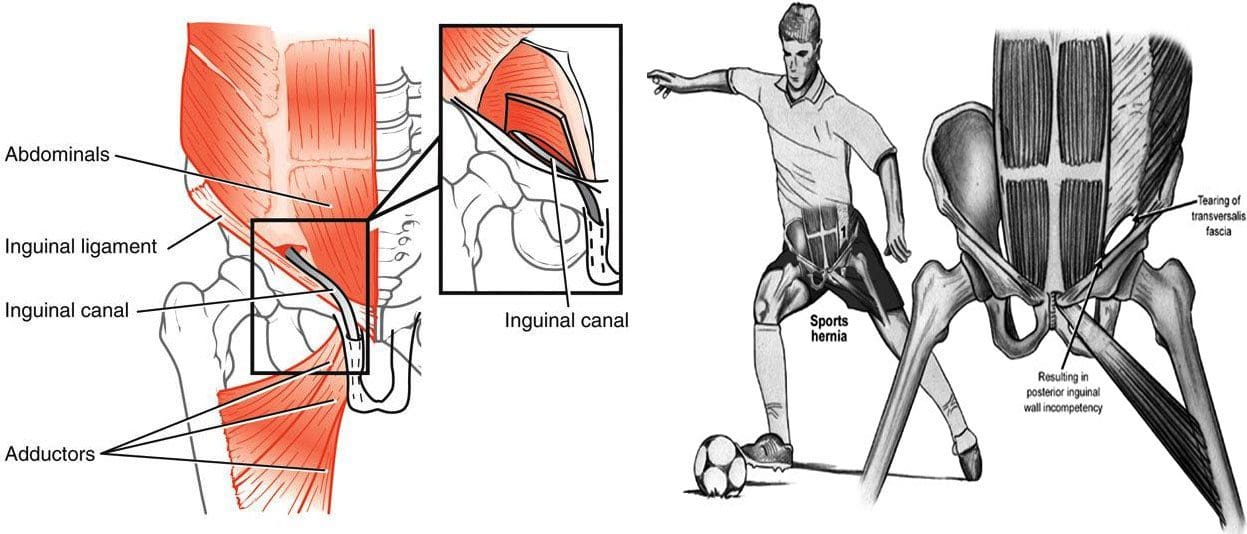
A sports hernia is a soft tissue injury that happens in and around the groin area. It is a strain or tear of any soft-tissue muscles, tendons, or ligaments in the lower abdomen or groin area. It usually happens during physical sports activities that require fast, quick, sudden changes of direction and/or intense twisting movements. Despite its name, a sports hernia is not a hernia in the classic sense. The condition’s proper term is athletic pubalgia. However, a sports hernia can lead to an abdominal hernia. The condition can happen to both men and women.
Anatomy
The soft tissues most affected by sports hernias are the oblique muscles in the lower abdomen, along with the tendons that attach the oblique muscles to the pubic bone, are the most at risk. In many cases, the tendons that attach the thigh muscles to the pubic bone or adductors are also stretched or torn.
Core Muscle Injury
A core muscle injury is when the deep layers of the abdominal wall weaken or tear. This can cause nerve irritation and contribute to uncomfortable symptoms of numbness or tingling. The most common causes include:
Planting the feet and turning or twisting with maximum force.
Constant repetitive hip and pelvic twisting motions.
Imbalances between the hip and abdominal muscles can also, over time, cause overuse injuries.
Weakness in the abdominals and improper or no conditioning can also contribute to injuries.
Chronic groin pain is the primary symptom of a core muscle injury.
Sharp groin pain with exertion.
Basic movements like sitting down or getting out of bed can also present with pain or discomfort.
Pain on one side of the groin.
Pain or numbness that radiates into the inner thigh.
Pain when coughing or sneezing.
Tenderness or pressure on the lower abdominal area.
Pain decreases with rest.
Diagnosis
A doctor will discuss symptoms and how the injury occurred. They will run a series of strength tests like a sit-up or trunk flex against resistance. If it is a sports hernia, there will be tenderness in the groin or above the pubis, along with discomfort and pain. Further tests will include MRI, ultrasound, or X-rays to rule out hip, low back, or pelvis injuries to confirm a core muscle injury.
Non-Surgical Treatment
Rest
In the first 7 to 10 days after the injury resting and icing the area is recommended.
If there is a bulge in the groin, compression or a wrap can help relieve symptoms.
Chiropractic and Physical therapy
Two weeks after the injury, chiropractic adjustments and physical therapy exercises are recommended to improve strength and flexibility in the abdominal and inner thigh muscles.
For most cases, 4 to 6 weeks of chiropractic and physical therapy will resolve any pain and allow the individual to return to their exercise or sports activity.
Anti-inflammatory Medications
A doctor could recommend non-steroidal anti-inflammatory medications to reduce swelling and pain.
If the symptoms persist over a prolonged period, a doctor may suggest a cortisone injection.
If the pain comes back when resuming the physical activities, surgery could be needed to repair the torn tissues.
Surgical Treatment
Repairing the torn tissues can be done with a traditional open procedure that involves one long incision or a minimally invasive endoscopic procedure. In an endoscopy, the surgeon makes smaller incisions and uses a small camera, called an endoscope, to see inside the abdomen. The results of traditional and endoscopic procedures are the same. Most individuals can return to sports and physical activities 6 to 12 weeks after surgery.
Body Composition
Muscle Gain
Individuals can’t lose fat forever. At some point, they need to work on developing muscle or work to preserve the muscle that is already present. This requires a different diet and exercise plan than one designed for fat loss. Instead of getting the body into a catabolic state, the body needs to be in an anabolic state where the body builds tissue instead of breaking it down. To build muscle, the body needs resources meaning proper nutrition and sufficient protein intake to increase muscle mass. Maintaining an energy surplus of around 15% is appropriate for developing musculature, meaning a moderately active individual with a BMR of 1,600 calories would want to their intake to about 2,852 calories a day.
References
Hoffman, Jay R et al. “Effect of protein intake on strength, body composition and endocrine changes in strength/power athletes.” Journal of the International Society of Sports Nutrition vol. 3,2 12-8. 13 Dec. 2006, doi:10.1186/1550-2783-3-2-12
Larson, Christopher M. “Sports hernia/athletic pubalgia: evaluation and management.” Sports health vol. 6,2 (2014): 139-44. doi:10.1177/1941738114523557
Poor, Alexander E et al. “Core Muscle Injuries in Athletes.” Current sports medicine reports vol. 17,2 (2018): 54-58. doi:10.1249/JSR.0000000000000453
Thorborg, Kristian et al. “Clinical Examination, Diagnostic Imaging, and Testing of Athletes With Groin Pain: An Evidence-Based Approach to Effective Management.” The Journal of orthopedic and sports physical therapy vol. 48,4 (2018): 239-249. doi:10.2519/jospt.2018.7850
Tyler, Timothy F et al. “Groin injuries in sports medicine.” Sports health vol. 2,3 (2010): 231-6. doi:10.1177/1941738110366820
Around a half-million high school students in the U.S. play volleyball. Whether the parent of a volleyball player or part of a recreational league, the goal is to be ready for the season, which means preventing and addressing volleyball injuries. It is a highly demanding sport with quick movements, jumping, twisting, diving, spiking, etc. Despite being fit and healthy, extensive training along with match play takes a toll on the body. Chiropractic can benefit volleyball players.
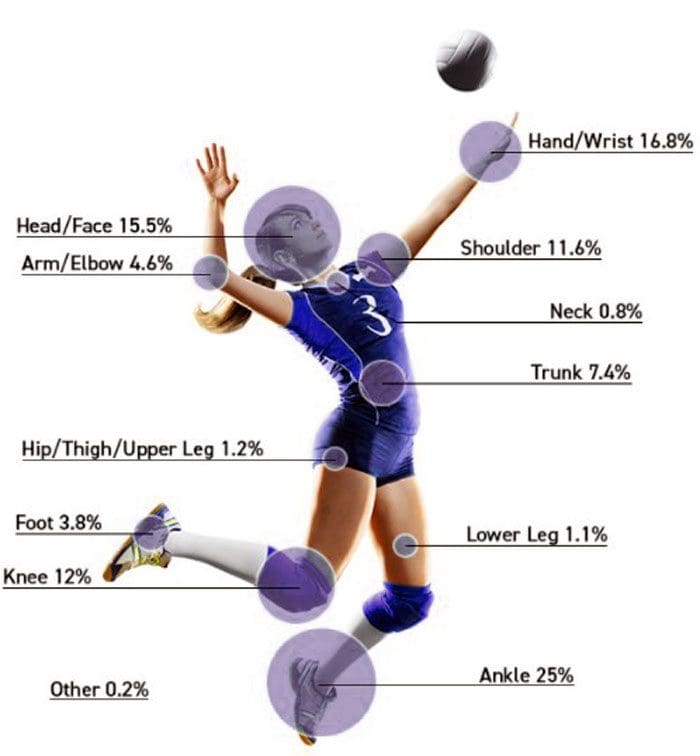
Common Volleyball Injuries
Why Chiropractic Works
Chiropractic treatment and rehabilitation, especially by a sports chiropractor, is recommended for volleyball injuries because it addresses acute and chronic injuries to all areas of the body. Chiropractic treats the entire musculoskeletal system. Proper joint alignment from chiropractic adjustments in the spine and throughout the body maintains the biomechanic integrity. This reduces high-impact forces in the joints. Soft tissue treatments like instrument-assisted soft tissue mobilization can help resolve injuries by providing the tissues with more blood flow into the affected area allowing for faster healing. Most volleyball injuries result from overuse to the joints and muscles, resulting in repetitive strain. In volleyball, repetitive/overuse injuries are common in the knees, ankles, and shoulders. This comes from all the jumping, serving, and spiking.
Player Benefits
Body Soreness Is Reduced/Alleviated
Many athletes, including volleyball players, do not get the proper recovery time from training or playing.
Reduced recovery periods cause body soreness and stiffness that can overlap into an injury.
Chiropractic can reduce and alleviate body soreness.
Chiropractic promotes faster recovery.
Optimal Performance
Studies show that athletes that receive regular chiropractic care found speed and mobility performance enhanced.
Athletes require fast reflexes and optimal hand-eye coordination.
Speed, mobility, reflexes, and coordination depend on a healthy nervous system.
90% of the central nervous system travels through the spine.
Spinal alignment can either allow for proper nerve flow or disrupt nerve flow.
Even when just one spinal segment is misaligned and out of place, the nervous system can impact reflexes, speed, mobility, and hand-eye coordination.
A properly functioning spine and nervous system will ensure the player is at their best.
Faster Injury Recovery Time
Healing the body properly takes time. Just like the body needs sleep/rest to function properly, so it is with injuries.
The issue for athletes is how much time healing takes.
Individual athletes receiving chiropractic care have been shown to heal faster.
Mobility and Strength
A chiropractic doctor can reduce the pressure around the nerve roots that exit the spine, which will help improve player performance. This includes:
Range of motion
Mobility and flexibility
Strength
Endurance
To find out how chiropractic can help, contact Injury Medical Chiropractic and Functional Medicine Clinic. We will perform a thorough musculoskeletal and nervous system examination.
Ankle Sprain Treatment
How Many Calories Over 24 hours
Myths that offer strategies that avoid the hard work and commitment that diet and exercise demand should be avoided. Individuals cannot expect to experience healthy body composition changes by increasing/decreasing meal frequency if they are living a sedentary lifestyle. It is not important how often or what time an individual takes in calories (has a meal). What is important is how many calories an individual has over a 24-hour period. A study looked at healthy individuals that ate one large meal a day for two weeks and then later ate the same meal but spread out over five smaller meals for another two weeks. It was concluded that there was no statistical difference in body weight gain or loss between the two eating methods. 2000 calories over 3 meals is the same 2000 calories consumed over 5 meals. There is no substitute for proper diet and exercise. The focus should be on what and how much you eat.
References
Eerkes, Kevin. “Volleyball injuries.” Current sports medicine reports vol. 11,5 (2012): 251-6. doi:10.1249/JSR.0b013e3182699037
Gouttebarge, Vincent et al. “Preventing musculoskeletal injuries among recreational adult volleyball players: design of a randomized prospective controlled trial.” BMC musculoskeletal disorders vol. 18,1 333. 2 Aug. 2017, doi:10.1186/s12891-017-1699-6
Kilic, O et al. “Incidence, etiology, and prevention of musculoskeletal injuries in volleyball: A systematic review of the literature.” European journal of sports science vol. 17,6 (2017): 765-793. doi:10.1080/17461391.2017.1306114
Seminati, Elena, and Alberto Enrico Minetti. “Overuse in volleyball training/practice: A review on the shoulder and spine-related injuries.” European journal of sports science vol. 13,6 (2013): 732-43. doi:10.1080/17461391.2013.773090
Wolfram, G et al. “Thermogenese des menschen bei unterschiedlicher mahlzeitenhäufigkeit” [Thermogenesis in humans after varying meal time frequency]. Annals of nutrition & metabolism vol. 31,2 (1987): 88-97. doi:10.1159/000177255
Bowling is a fun physical activity that is enjoyable for all ages. Today, there are college bowlers, recreational bowlers, amateur, semiprofessional, professional leagues, and tournaments worldwide. Although it might not be the first sport that comes to mind when thinking of injuries and chronic pain conditions, it can place significant stress on the muscles and tendons of the upper and lower body. It is important to know and understand how to avoid injuries.
How Bowling Injuries Happen
There are two main causes of injuries and chronic pain related to bowling. The first is poor mechanics, and the second is repetitive over-use. Both cause/develop painful symptoms that can turn into injuries that become chronic conditions. Many injuries are caused by:
Slip and fall accidents
Players dropping the ball on their feet
The majority of injuries come from overuse/repetition and improper body mechanics.
Overuse injuries result from repetitive and/or strenuous actions/movements that place profound stress on the body’s musculoskeletal system.
For example, a semi-pro and professional bowler will play fifty or more games a week. This means throwing a sixteen-pound ball for ten frames per game. When consistently repeated over and over, this can cause serious wear and tear to the body. With amateur and recreational bowlers, they don’t play as much, so they don’t experience overuse injury as much, but what they do experience is improper/poor form techniques that shift the body in non-ergonomic ways, wrong equipment like oversized/too-small shoes that can cause awkward postures and body motions, a ball that is too heavy causing an individual to overthrow and strain their arms, backs, hips, and legs. Or a ball with small finger holes that get stuck or too large, causing finger, hand, arm, shoulder pulls strains, and sprains.
Common Bowling Injuries
The most common injuries and conditions associated with bowling include:
Many of the injuries can lead to tendonitis or arthritis later in life.
Trigger/Bowler’s Finger
Symptoms include:
Hand pain after bowling, specifically in the fingers
A clicking or popping when moving the fingers
A finger gets locked in a bent position
Rest, and no bowling is recommended. How long a rest depends on how long the symptoms have been presenting. Physical therapy, along with chiropractic exercises, can help improve finger strength. Splinting the finger could be required to improve the condition. If all fails or does not generate adequate relief, hand surgery could be optioned with a trigger finger release. The surgery allows the finger to move more freely.
Bowler’s Thumb
This usually happens to bowlers that want to generate a lot of spin on the ball. If the thumb’s hole is too tight, it can pinch the ulnar nerve inside the thumb. If the thumb injury is not serious, rest and getting the correct ball size can correct the issue. This is where purchasing a personal bowling ball can help.
Finger Sprain
This is an injury to one or more of the ligaments in the fingers. It most often takes place in the collateral ligaments along the sides of the fingers inside the ball. The ligament/s gets stretched or torn when the finger is forced beyond its normal range of motion. Common symptoms of a finger sprain include swelling, tenderness, stiffness, and pain in the affected finger. This usually occurs from:
The weight of holding the ball with the fingers alone
A poor release
Using a ball that doesn’t properly fit the fingers
A finger sprain falls into grades on the severity of how much the ligament is stretched or torn:
Grade 1
Stretching or microscopic tearing.
Grade 2
Less than 90% of the ligament is torn.
Grade 3
More than 90% of the ligament is torn. Grade three sprains can be accompanied by joint instability and immobility.
Herniated Disc
A herniated disc is when the discs get injured/damaged from overuse, wear, and tear, or a traumatic injury to the spine. The disc can dry out, become less flexible, bulge out, or rupture. Bowlers are constantly:
Bending during the final approach and throw
Carrying a heavy ball
Shifting, twisting, and releasing, increasing the pressure within the discs
In bowling, the majority of herniated discs happen in the low back. The most common symptom is backaches and back pain. Lumbar herniated discs left untreated can cause sciatica.
Avoid and Prevent Injury
The best way to prevent injury is to stay aware of body position, mechanics, equipment, and what the body says.
Stretching
Stretching is one of the best things to avoid injury before practicing, competing, or just playing. Stretching will increase flexibility, especially in the wrist, hand, arm, and low back.
Improving technique
Continually using poor techniques over and over is a perfect set-up for injury. Working with a coach will ensure the proper form. This is important when it comes to generating spin on the ball, as well as, making sure the grip does not place too much strain on the hands.
Using the right ball
The ball being used might not be the right fit for your hand or strength. The holes could be too far apart, causing strain on the fingers. Get as much information as possible and try out different styles and weights to get a comfortable feel for the right ball.
Bowling less
Hard-core bowlers could be overdoing it. Cutting back, and creating a balance will allow the body to recover thoroughly and not cause flare-ups.
Getting in shape
Studies show that individuals who bowl and do not exercise significantly increase the risk of a back injury than those who exercise their back and core. Bowling is not as strenuous as other sports, but it still requires the body to be able to handle the stress.
Body Health
Test Body Composition
Testing body composition regularly is the best way to ensure the body stays healthy. Tracking body composition tracks Lean Mass and Fat Mass gain or loss. The information provided allows the individual to make the necessary changes to ensure they stay fit and healthy.
Diet adjustment
Diet needs to be adjusted to match the individual’s current activity level, or risk running a caloric surplus. A great way to optimize diet is to use Basal Metabolic Rate which will make sure the body is getting enough nutrients to fuel muscle growth, and lose belly fat.
Physical activity that fits the new lifestyle
Increase physical activity levels that work with current lifestyle. This does not mean performing at high levels every day. Be active on a schedule that works for you. Two days of strength training a week offer great physical and mental benefits. The key is to maintain the balance between food consumption and exercise/physical activity that fits your current lifestyle.
References
Almedghio, Sami M et al. “Wii knee revisited: meniscal injury from 10-pin bowling.” BMJ case reports vol. 2009 (2009): bcr11.2008.1189. doi:10.1136/bcr.11.2008.1189
Kerr, Zachary Y et al. “Epidemiology of bowling-related injuries presenting to US emergency departments, 1990-2008.” Clinical pediatrics vol. 50,8 (2011): 738-46. doi:10.1177/0009922811404697
Kisner, W H. “Thumb neuroma: a hazard of ten pin bowling.” British journal of plastic surgery vol. 29,3 (1976): 225-6. doi:10.1016/s0007-1226(76)90060-6
Miller, S, and G M Rayan. “Bowling related injuries of the hand and upper extremity; a review.” The Journal of the Oklahoma State Medical Association vol. 91,5 (1998): 289-91.
Although many soccer injuries involve the legs and lower extremities, other body areas are susceptible to injury/s as well. Acute or cumulative is how soccer injuries are generally described. Acute injuries are traumatic. They are usually caused by a slip, trip, and fall, getting hit, and crashing into other players. Cumulative injuries involve repetitive stress on a muscle, joint, or connective tissue. This triggers progressive aches, pain, and physical impairment that gets worse with time. Understanding how and why they happen is the first step in injury prevention. The more common injuries experienced among soccer athletes include.
Concussion
This is a form of mild traumatic brain injury mTBI caused by a sudden hit/impact to the head. Players are trained to head the ball; however, concussions can happen if not ready for impact or heading at an awkward position.
Ankle Sprains
Ankle sprains are when there is stretching and tearing of ligament/s that surround the ankle joint.
Lateral ankle sprains or outside of the ankle can happen when a player kicks the ball with the top of the foot.
A medial ankle sprain or inside of the ankle can happen when the toes are turned out when the foot is flexed up.
Achilles Tendonitis
This is a chronic injury that occurs from overuse with pain in the back of the ankle. Players are constantly performing repetitive and sudden movements that, over time, can cause this type of injury.
Achilles Tendon Rupture
A rupture involves a partial or complete tear of the Achilles tendon. Often players say with a popping sound. This happens when players perform fast, explosive movements. Rapid stopping, starting, shifting, jumping can all contribute.
Groin Pull/Strain
This is a type of strain that happens when the inner thigh muscles are stretched beyond their limit. As a result, a player can pull the groin when kicking and/or resistance from an opponent trying to take the ball or kick in the opposite direction.
Hamstring Injury
These injuries involve the three back muscles of the thigh and can vary from minor strains to complete ruptures/tears. This comes from running, sprinting, jumping, and stopping, leading to these types of injuries.
Iliotibial Band Syndrome
This is an overuse/repetitive injury that involves a tendon known as the IT band. This is the connective tissue that runs along the outside of the thigh. Constant running can create friction as the band gets pulled along the outside of the knee, which can cause tendonitis.
Plantar Fasciitis
This causes foot pain caused by inflammation of the tissue bands that run from the heel to the toes. Several factors can cause the condition. This could be players using inappropriate or not correctly fitting shoes, shoes that do not provide proper arch support or playing on a hard surface.
Calf Muscle Pull
This is when one of the muscles of the lower leg gets pulled from the Achilles tendon. Again, quick and spontaneous sprinting, running, or jumping is usually the cause.
Knee Injuries
The most common soccer injuries are those that involve the knee. This is because of the stopping and shifting directions quickly and suddenly. The explosive, spontaneous movements place extreme stress on the knees and the supporting ligaments. When the stress goes beyond the ligament’s limits, it can cause a sprain or tear in the joint. When there is an injury to the knee/s, it is diagnosed using a grading scale.
Grade 1 Mild sprain
Grade 2 Partial tear
Grade 3 Complete tear
Runner’s Knee
Patellofemoral pain syndrome, also known as runner’s knee, is a condition where the cartilage under the kneecap gets damaged from an injury or overuse. This happens when there is a misalignment in the knee and/or strained tendons.
ACL Injury
The anterior cruciate ligament or ACL is at the front of the knee. These are the most common knee injuries. This is because the ligaments are less retractable than muscles or tendons. And those in the knees are highly vulnerable to damage.
Cruciate Ligament Injury
This type of injury does not always cause pain but often causes a popping sound when it happens. Pain and swelling develop within 24 hours. This is followed by the loss of range of motion and tenderness around and along the joint.
Meniscus Injury
The Meniscus involves a C-shaped piece of cartilage that cushions the space between the femur and the shin bone. These tears are painful and are often the result of twisting, pivoting, decelerating, or quick/rapid impact.
Shin Splints
The term describes a variety of painful symptoms that develop in the front of the lower leg. This often happens from over/intense training, or the training gets changed. Players can also develop shin splints from training while not using appropriate shoes.
Stress Fractures
These types of fractures are usually the result of overuse or repeated impact on a bone. The result is severe bruising or a slight crack in the bone.
Tendonitis
When tendons get inflamed, it is referred to as tendonitis. This comes with repetitive overuse but can also develop from a traumatic injury that causes micro-tears in the muscle fibers.
Soccer Injuries Prevention
Many of these injuries result from overuse, overtraining, improper conditioning, and/or not warming up properly. Here are few tips to help reduce the risk.
Warm-up for at least 30 minutes before playing
Pay special attention to stretching the:
Groin
Hips
Hamstrings
Achilles’ tendons
Quadriceps
Wear protective gear
This includes:
Mouthguards
Shin guards
Kinesio tape
Ankle supports
Eye protection
Ensure they are correctly sized and maintained.
Check the field
Check for anything that could cause injury/s. This includes:
Holes
Puddles
Broken glass
Stones
Debris
Avoid playing in bad weather
Or immediately after heavy rain when the field is especially slick and muddy.
Allow enough time to heal after an injury.
This also goes for minor soccer injuries. Trying too fast to get back increases the risk of worsening the injury, re-injury, and/or creating new injuries.
Utilize carb-loading to help them increase energy storage for long runs, bike rides, swims, etc. When timed effectively, carb-loading has been shown to increase muscle glycogen, leading to improved performance.
Bodybuilders and fitness athletes
Use carbo-loading to build size and mass before competitions. The timing and efficacy of carb-loading vary from person to person. Make sure to experiment before the next big competition.
References
Fairchild, Timothy J et al. “Rapid carbohydrate loading after a short bout of near maximal-intensity exercise.” Medicine and science in sports and exercise vol. 34,6 (2002): 980-6. doi:10.1097/00005768-200206000-00012
Kilic O, Kemler E, Gouttebarge V. The “sequence of prevention” for musculoskeletal injuries among adult recreational footballers: A systematic review of the scientific literature. Phys Ther Sport. 2018;32:308-322. doi:10.1016/j.ptsp.2018.01.007
Lingsma H, Maas A. Heading in soccer: More than a subconcussive event?. Neurology. 2017;88(9):822-823. doi:10.1212/WNL.0000000000003679
Pfirrmann D, Herbst M, Ingelfinger P, Simon P, Tug S. Analysis of Injury Incidences in Male Professional Adult and Elite Youth Soccer Players: A Systematic Review. J Athl Train. 2016;51(5):410–424. doi:10.4085/1062-6050-51.6.03
Tennis is an intense sport that requires strength, agility, flexibility, stamina, endurance, and conditioning. And it’s a great way to stay in shape. However, with all of this intensity is the risk of injuries. Although they are lower compared to other sports injuries, injuries are more cumulative/repetitive based and wear and tear over time type. Tennis injuries can be painful and impair daily life. They can be treated and prevented with chiropractic medicine and strength training. Chiropractic can help the body heal quicker, and address underlying issues that led to the injury. This will help to worsen and prevent re-injury. The most common tennis injuries include…
Wrist Tendonitis
This is an injury that can happen to beginner players that don’t have a great deal of arm/wrist strength, use a racquet that is too heavy, and begin developing an improper form to compensate. But it can also be caused by repetitive/overusing the wrist instead of the whole arm. Symptoms are chronic stiffness and pain in the area surrounding the wrist joint. Chiropractic sports massage, physical rehabilitation, and learning proper form will help alleviate the pain and prevent worsening or developing new injuries.
Tennis Elbow
Tennis elbow is a condition that is caused by inflammation of the outside muscles in the forearm and tendons. This is usually an overuse injury from all the swinging and hitting, but using the improper technique could also be a cause. Chiropractic adjustments are highly recommended instead of steroid injections and other anti-inflammatories. The adjustments and massage relieve the discomfort and pain by naturally relaxing, stretching, and strengthening the muscles and tendons.
Shoulder Rotator Cuff Tendonitis
The rotator cuff belongs to a group of tendons and muscles that surround the shoulder joint. This allows the shoulder to perform 360-degree arm circles and is what stabilizes the shoulders. Tendonitis happens when the tendons inside the rotator cuff become inflamed. The inflammation causes pain with movement, especially overhead motions decreasing the range of motion in the shoulder. This injury is often caused by serving and hitting overheads with an improper technique. Chiropractic adjusting, heat and ice therapy, and electro-muscular stimulation loosen and stretch the muscles/tendons back to their proper form.
Knee Sprains and Strains
The knee goes through a lot in sports. And tennis is no exception, much like basketball and volleyball with all the jumping, pounding, shifting, twisting,losing balance, or extending beyond the normal range of motion causes injuries that result in:
Pain
Swelling
Bruising
Loss of the ability to move
Chiropractic will help relieve that pain and relax the damaged muscles. It also speeds the healing process by addressing the underlying issues.
Ankle Sprain
An ankle sprain also known as a twisted ankle happens when the ligaments attached to the joint become over-stretched or partially tear. These sprains happen from the:
Quick start and stop movements
Changing direction rapidly
Quick sprints all around the court
Causing the ankle to roll and/or twist.
A chiropractor will realign the ankle and provide physical therapy massage to allow the ligaments to heal properly and faster. Chiropractic treatment will allow the player to return to play quicker and prevent reinjury that if not treated correctly can become chronic. Having the proper personalized treatment plan will ensure the body heals correctly, prevent misalignments, loss of functionality, and/or range of motion.
PUSH Fitness
Aerobic Training
Aerobic exercise is a cornerstone for weight loss. Having the heart rate elevated for a continuous amount of time is the key. This is how calories are burned. Research has found that individuals involved in aerobic training lose more weight overall, including more fat mass than resistance training alone. When combined, aerobic and resistance training individuals gain more fat-free mass, including lean muscle. Aerobics causes the cardiorespiratory system to adapt. Maintaining heart function and health and keeps the body’s energy metabolism system running at optimal levels. Aerobic exercise for fitness and weight loss is a key element of maintaining the body’s health.
Disclaimer
The information herein is not intended to replace a one-on-one relationship with a qualified health care professional, licensed physician, and is not medical advice. We encourage you to make your own health care decisions based on your research and partnership with a qualified health care professional. Our information scope is limited to chiropractic, musculoskeletal, physical medicines, wellness, sensitive health issues, functional medicine articles, topics, and discussions. We provide and present clinical collaboration with specialists from a wide array of disciplines. Each specialist is governed by their professional scope of practice and their jurisdiction of licensure. We use functional health & wellness protocols to treat and support care for the musculoskeletal system’s injuries or disorders. Our videos, posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate to and support, directly or indirectly, our clinical scope of practice.* Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We provide copies of supporting research studies available to regulatory boards and the public upon request. We understand that we cover matters that require an additional explanation of how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900.
Dr. Alex Jimenez DC, MSACP, CCST, IFMCP*, CIFM*, CTG*
email: [email protected]
phone: 915-850-0900
Licensed in Texas & New Mexico
References
Dines, Joshua S et al. “Tennis injuries: epidemiology, pathophysiology, and treatment.” The Journal of the American Academy of Orthopaedic Surgeons vol. 23,3 (2015): 181-9. doi:10.5435/JAAOS-D-13-00148
Minghelli, Beatriz, and Jéssica Cadete. “Epidemiology of musculoskeletal injuries in tennis players: risk factors.” The Journal of sports medicine and physical fitness vol. 59,12 (2019): 2045-2052. doi:10.23736/S0022-4707.19.09842-6
Stuelcken, Max et al. “Wrist Injuries in Tennis Players: A Narrative Review.” Sports medicine (Auckland, N.Z.) vol. 47,5 (2017): 857-868. doi:10.1007/s40279-016-0630-x
Willis, Leslie H et al. “Effects of aerobic and/or resistance training on body mass and fat mass in overweight or obese adults.” Journal of applied physiology (Bethesda, Md.: 1985) vol. 113,12 (2012): 1831-7. doi:10.1152/japplphysiol.01370.2011
The most common causes of golf injuries are playing and practicing too excessively, improper swinging mechanics, and little or no physical conditioning. Pain meds either over-the-counter or prescribed, bracing, and surgical procedures are how symptoms are treated instead of the root cause/s. If the cause/s are addressed then injury prevention comes naturally.
�
Overuse
Driving requires a great deal of effort and power that puts tremendous stress on the body. When done too frequently, injuries can result. The body can take all kinds of forces thrown at it. But there is a limit as to how much it can take before an injury occurs.
Too many swinging reps while playing and practicing could cause trauma to the muscles and connective tissues, which leads to inflammation and pain. Swinging and hitting with bucket after bucket of balls to improve performance will raise the risk of injury. Try practicing swinging without hitting any balls through imagery/imagination. This has become a standard tool utilized by athletes. Practice the perfect swing mentally without the risk/threat of overusing your arms and back.
�
Mechanics
Improper body and swinging mechanics can lead to injury. The constant swinging, bending, squatting, and walking places added stress on muscles that can lead to a shoulder sprain/strain, elbow pain, and rib fractures. Back injuries can happen when bending far too forward while in swinging motion. Common swing mistakes that can contribute to low back pain.
�
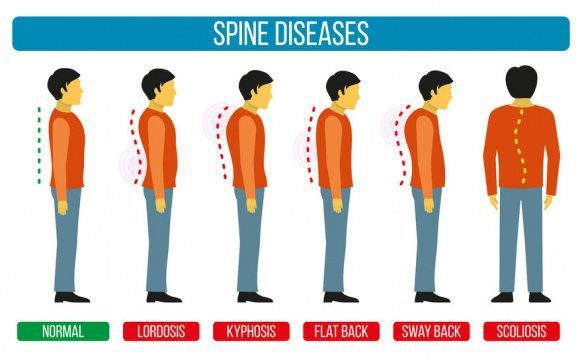
S-Posture
This can happen when golfers are told to stick out their rear but what happens is that they over arch their lower backs which cause hyperlordosis. This is known as an S-Posture and it inhibits the abs and glutes. Or this also happens with a lower crossed syndrome. �
�
Early Extension
This is a term that comes from a forward swinging movement where the lower body does not rotate from the top of the backswing to follow-through. The hips and pelvis do not turn with the body. Spinal posture is extended, the head rises up and the pelvis moves toward the ball’s position. When this happens the spine’s muscles over-activate and force the spine into a fast extension. Forward movement of the lower body toward the golf ball can be a sign of early extension. �
Early Extension
Ideal Position
�
Reverse C
This happens at the swing’s finish being in a full hyperextension position. It places added compression on the lower back right facet joints. �
� Overextending, Flexing, and twistingexcessively, awkwardly, and improperly increases chances of injury. A bit of advice is to have your swing analyzed by a golf pro/instructor to make sure you have proper form and technique. Preventing back injuries can be achieved through proper body mechanics by properly lifting the golf bag and properly teeing the ball.
�
Conditioning
Muscles will be weak and inflexible when there is no conditioning. This causes them to become highly susceptible to injury. The spine is exceptionally vulnerable to increased pressure during a golf swing. This happens from rotating while leaning forward. When the low back and abdominal muscles do not have adequate strength or flexibility the high reps of swinging will eventually cause pain.
With a golf-specific strength and flexibility program, the risk of injury is lessened along with improved performance. Programs like these don’t have to be complicated or take a long time. Stop potential golf injuries from happening by avoiding excessive practice sessions, swinging correctly, and regularly practicing golf-oriented strength and flexibility exercises.
�
Sports Injury Chiropractic Treatment
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
Chiropractic athletics is a natural treatment focused on athletes and sports injuries. It is a non-surgical, non-drug option that can help individual athletes prevent injury/s from happening, maintain optimal athletic performance, and relives sports musculoskeletal injuries.Athletes of all types can benefit from chiropractic athletics.
Sports leagues and professional athletes including Major League Baseball and the National Football League have full-time chiropractors on their teams. Athletes from all over the world utilize chiropractic medicine. With the advancement in sports technology, intense training and superb athleticism come injuries that can turn into game-ending conditions. Because of this, there is a wide variety of treatment needs and is where chiropractic athletics comes in.
�
Commonly athletes are referred to chiropractors for neck, lower back, and extremity conditions. Chiropractic athletics help them get them back into play after an injury faster, with added flexibility and agility. And for those without injuries chiropractic helps athletes prevent injuries by increasing strength and power to help perform at peak level.
Chiropractic sports doctors are highly trained with the tools and skills that will optimize the performance of an athlete’s musculoskeletal and nervous system. This training is what allows these athletic chiropractors to provide sports therapy/s that is focused on maintaining agility, flexibility, strength, and quick rehabilitation after an injury. Why chiropractic athletics should be essential?
�
Chiropractic Athletic Importance
Regular chiropractic improves range of motion. Athletes place intense pressure on their bodies when training, weight-lifting, and playing. This can shift the spine out of alignment affecting movement, along with the rest of the body, generating a high probability of injury.
Athletes have to deal with soreness, stiffness, and pain from their basic training regiment. An injury can easily compound the soreness into something more severe. Spinal alignment problems can cause the range of motion to be hindered and limited, inhibiting overall ability. Chiropractic athletics undoes the damage. Once a chiropractic regiment is in place injury prevention kicks in, all the while keeping the athlete moving pain-free. �
�
Pain Reduction
Anyone especially the strongest athletes can have an episode of back pain, specifically in the low back. A chiropractor promotes proper alignment and movement of the delicate spine. Chiropractors can recommend treatments both professional and self-care that will reduce all types of back pain short and long-term. Research confirms that a manual spine manipulation is an effective form of pain relief.
�
Less Need for Pain Meds
Too often aches and pain are treated with pain meds, cortisone shots, and other drugs that provide short-term relief. Chiropractic is drug-free. This means athletes are not subject to side effects or dependencies that unfortunately arise from prescription med use.
Because of the increasing dependency on opioids, the American College of Physicians has updated their guidelines when it comes to low back pain, a very common reason for opioid prescriptions. Now, those with low back pain are encouraged to utilize various complementary and alternative medicine techniques that include chiropractic spinal manipulation before having to use prescription medication.
�
Non-invasive
Chiropractic is non-surgical and can provide relief from injuries throughout the body. It can even serve as an alternative to surgery/s that would keep athletes on the sidelines because of a long recovery period. Treatments include:
All of these can be used to treat athletic injury.
�
Athletic Benefits
Whether a neighborhood sports league or advanced competitive league athletes need chiropractic specialists for injury treatment to get them back to play. Kids are now traveling at a younger age meaning more practices and tournaments. Kids are also committing to only one sport early on. This is known as specializing. A study by The American Journal of Sports Medicine found that athletes that specialize too early are subject to continued injury/s. �
�
Chiropractic decreases recovery time
Normal wear and tear happens to all of us but can wear down faster especially in an extremely healthy athlete�s body.
A baseball pitcher uses a consistent repetitive throwing motion.
A volleyball player jumps, constantly hitting and blocking.
A skateboarder falls repeatedly, sometimes over one-hundred times trying to land a trick.
At some point and quite often an athlete experiences muscle fatigue and soreness. Practices and games have only a few days between them. Younger athletes and their growing bodies need a lot more than rest to keep them in shape. After practice or a game, a chiropractor can do some soft tissue massage or instrument-assisted soft tissue techniques to make the muscles, tendons, ligaments, and joints flexible, relaxed, with decreased lactic acid, and improved blood circulation.
Physical therapy and the equipment used like ultrasound or cold laser therapy can be used to help with areas that are highly inflamed. This along with adjustments can improve joint mobility. Chiropractic athletics also helps with proper rehydration and customized dietary plans to assist with recovery and maintaining top-level performance. �
Lacrosse players experience knee injuries and muscle strains
Chiropractic adjusting of joint segments, no longer moving, can enhance mechanical motion. Soft tissue techniques improve muscle tone and blood flow to injured areas and decrease tissue buildup around the injured areas. Chiropractic along with the aforementioned treatment options can significantly reduce inflammation and pain.
All of these treatment options can be enhanced with Kinesio Taping. It can add support and various taping techniques can assist in blood circulation to the injured area. A sports chiropractor has a complete understanding of sports injury repair and knows the proper guidelines for safely returning the athlete to their sport. �
�
Health and Wellness
Athletes have to focus on body awareness, health, diet, and optimal function. But they also need to be injury prepared through preventive awareness. Think of it as defensive driving. A chiropractor can assist an athlete with:
Proper training strategies that can become life-long habits
Body mechanic evaluation
Gait analysis
Continually keeping an athlete�s body in top form, allows them to train more efficiently and effectively.
�
A Vital Role
With athletes training year-round and specializing earlier, chiropractic assistance can keep an athlete at a top level of body function. Chiropractic combined with certified athletic trainers can help with muscle development, ligament, and tendon stability. These specialists play a vital role in obtaining and maintaining whole-body wellness.
�
Consider Chiropractic
Chiropractic athletics includes a whole health assessment to ensure there are no underlying issues that could be contributing to an injury, or that could cause future problems. Athletes, consider seeing a chiropractor regularly for those that want to maintain physical strength and range of motion, or if they want to recover from an injury without taking prescription meds and surgery. Sports performance will improve when the body is in alignment and pain-free!
�
Functional Fitness Fellas
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine