Rheumatoid arthritis, or RA, is a chronic health issue which affects approximately 1 percent of the population in the United States. RA is an autoimmune disorder that causes the inflammation and degeneration of the synovial tissue, specific cells and tissue which form the lining of the joints within the human body. Rheumatoid arthritis may and generally does affect every joint in the body, especially as people get older. RA commonly develops in the joints of the hands and feet, severely restricting an individual’s ability to move, however, those with significant disease in the spine are at risk of damage like paraplegia. Rheumatoid arthritis of the spine is frequent in three areas, causing different clinical problems.
The first is basilar invagination, also referred to as cranial settling or superior migration of the odontoid, a health issue where degeneration from rheumatoid arthritis at the base of the skull causes the it to “settle” into the spinal column, causing the compression or impingement of the spinal cord between the skull and the 1st cervical nerves. The second health issue, and also the most frequent, is atlanto-axial instability. A synovitis and erosion of the ligaments and joints connecting the 1st (atlas) and the 2nd (axis) cervical vertebrae causes instability of the joint, which may ultimately result in dislocation and spinal cord compression. In addition, a pannus, or localized mass/swelling of rheumatoid synovial tissue, can also form in this region, causing further spinal cord compression. The third health issues is a subaxial subluxation which causes the degeneration of the cervical vertebrae (C3-C7) and often results in other problems like spinal stenosis.
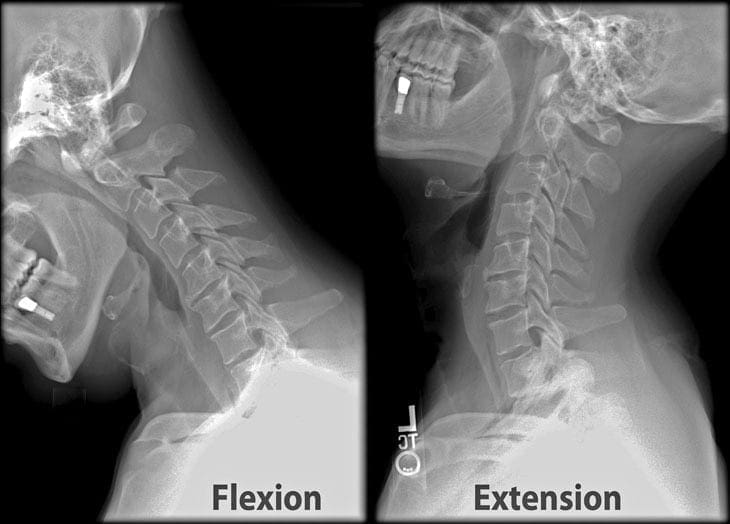
Imaging studies are crucial to properly diagnose patients with rheumatoid arthritis of the cervical spine. X-rays will demonstrate the alignment of the spine, and if there is obvious cranial settling or instability. It can also be difficult to demonstrate the anatomy at the bottom of the skull, therefore, computed tomography scanning, or CT scan, with an injection of dye within the thecal sac is arranged. Magnetic resonance imaging, or MRI, is beneficial to assess the severity of nerve compression or spinal cord injury, and allows visualization of structures, including the nerves, muscles, and soft tissues. Flexion/extension x-rays of the cervical spine are usually obtained to evaluate for signs of ligamentous instability. These imaging studies entails a plain lateral x-ray being taken with the patient bending forward and the other lateral x-ray being taken with the individual extending the neck backwards.�The scope of our information is limited to chiropractic, spinal injuries, and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Neck Pain and Auto Injury
Whiplash is one of the most common causes of neck pain after an automobile accident. A whiplash-associated disorder occurs when a person’s head and neck moves abruptly back-and-forth, in any direction, due to the force of an impact. Although whiplash most commonly occurs following a rear-end car crash, it can also result from sports injuries. During an auto accident, the sudden motion of the human body can cause the muscles, ligaments, and other soft tissues of the neck to extend beyond their natural range of motion, causing damage or injury to the complex structures surrounding the cervical spine. While whiplash-associated disorders are considered to be relatively mild health issues, these can cause long-term pain and discomfort if left untreated. Diagnosis is essential.
A teardrop fracture is caused when the anteroinferior aspect of a cervical vertebral body is damaged due to flexion of the spine together with vertical compression. The fracture throughout the body is also associated with deformity of the human body and subluxation or dislocation of the facet joints. A teardrop fracture is generally associated with a spinal cord injury due to the displacement of the anterior portion of the body into the spine.
The flexion teardrop fracture shouldn’t be confused with a similar-looking vertebral fracture called “expansion teardrop fracture”. Both usually happen in the cervical spine, but as their names indicate, they result from other mechanisms (flexion-compression vs. hyperextension). Both are linked to a small fragment being broken apart from the anteroinferior corner of the affected vertebra. Flexion teardrop fractures normally involve instability in most elements of the backbone, commonly occur at the C4-C7 vertebra, and have a higher association with spinal cord injury (specifically anterior cord syndrome). In contrast, the extension-type fracture happens more commonly in C2 or C3, causes significantly less if any disturbance to the middle and posterior elements, and does not normally result in spinal cord injury (but it may co-occur with more harmful spinal injuries).
A flexion teardrop fracture is a common injury of the cervical spine,�or neck, which can be severe in nature. Its name�is characterized by the triangle-shaped fragment which typically fractures from the anteroinferior corner of�the vertebral body and that resembles a drop of water dripping from the vertebral body. The scope of our information is limited to chiropractic, spinal injuries, and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Acute Back Pain
Back pain�is one of the most prevalent causes of disability and missed days at work. Back pain attributes to the most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
A vertebral fracture is a common health issue which can often cause bone fragments to damage the spinal chord and nerve roots. Broken bones can occur due to trauma or injury from automobile accidents, slip-and-fall accidents, or sports injuries, among other causes. Depending on how severe the vertebral fracture is, individuals may have difficulty performing everyday activities. The purpose of the article below is to demonstrate and discuss vertebral fracture diagnosis imaging studies and their results.
Practice Essentials
Vertebral fractures of the thoracic and lumbar spine are usually associated with major trauma and can cause spinal cord damage that results in neural deficits. Each vertebral region has unique anatomical and functional features that result in specific injuries. See the image below.
Figure 1: Anteroposterior and lateral radiographs of an L1 osteoporotic wedge compression fracture.
Signs and Symptoms
Symptoms of vertebral fracture can include pain or the development of neural deficits such as the following:
Weakness
Numbness
Tingling
Neurogenic shock – In this, hypotension is associated with relative bradycardia as a result of autonomic hyporeflexia
Spinal shock – The temporary loss of spinal reflex activity that occurs below a total or near-total spinal cord injury; initially results in hyporeflexia and flaccid paralysis; with time, the descending inhibitory influence is removed and hyperreflexive arches, even spasticity, may occur
An injury to the thoracic or lumbosacral cord would likely result in neural deficits at the trunk, genital area, and lower extremities. Specific syndromes, such as Brown-S�quard syndrome and anterior cord syndrome, may affect a compression part of the spinal cord.
See Overview for more detail.
Diagnosis
Laboratory Studies
Patients with vertebral or pelvic fractures resulting from a major trauma require serial hemoglobin determinations as an indicator of hemodynamic stability.
Other laboratory studies, including the following, aid in the evaluation of associated organ damage in patients with vertebral fracture:
Urinalysis or urine dip for blood – Can help to rule out associated kidney injury
Amylase and lipase levels – Elevated level of amylase or lipase may suggest pancreatic injury
Cardiac-marker levels – Elevated levels in the setting of chest trauma may indicate a cardiac contusion
Urine myoglobin and serum creatine kinase levels – Elevated level of urine myoglobin or serum creatine kinase in the context of a crush injury may indicate evolving rhabdomyolysis
Serum calcium level – In patients with metastatic disease to the bone and resultant pathologic fractures, a serum calcium determination is necessary; these patients may have hypercalcemia that requires medical attention
Pregnancy test – Should be obtained in females of childbearing age
Imaging Studies
Radiography – Plain radiographs are helpful in screening for fractures, but hairline fractures or nondisplaced fractures may be difficult to detect
Computed tomography (CT) scanning – CT scans can readily detect bony fractures and help with the assessment of the extent of fractures
Magnetic resonance imaging (MRI) – This is usually the study of choice for determining the extent of damage to the spinal cord; MRI is the most sensitive tool for detecting lesions of neural tissue and bone
See Workup for more detail.
Management
Nonsurgical Fracture Management
Minor fractures or those with column stability are treated without surgery. Nonoperative management of unstable spinal fractures involves the use of a spinal orthotic vest or brace to prevent rotational movement and bending.
Consideration should be given to the stabilization of patients with spinal cord injuries and paraplegia. These patients need to be stabilized sufficiently so that their upper body and axial skeleton are appropriately supported, which allows for effective rehabilitation.
Surgical Fracture Management
The goals of operative treatment are decompression of the spinal cord canal and stabilization of the disrupted vertebral column. The following basic approaches are used for surgical management of the thoracolumbar spine:
Posterior approach – Useful for stabilization procedures that involve fixation of the posterior bony elements; the posterior approach is used when early mobilization is considered and decompression of the spinal canal is not a major consideration
Posterolateral approach – Often used for high thoracic fractures such as T1 through T4; it may be combined with a posterior stabilization procedure when limited ventral exposure is needed
Anterior approach – Allows access to the vertebral bodies at multiple levels; the anterior approach is most useful for decompression of injuries and spinal canal compromise caused by vertebral body fractures
The 4 basic types of stabilization procedures are as follows:
Posterior lumbar interspinous fusion – Least-invasive method; involves the use of screws to achieve stability and promote fusion
Posterior rods – Effective in stabilizing multiple fractures or unstable fractures
Z-plate anterior thoracolumbar plating system – Has been used for the treatment of burst fractures
Cage
See Treatment for more detail.
While automobile accidents, slip-and-fall accidents, and sports injuries can cause spinal injuries, osteoporosis has been described as the leading cause of non-traumatic vertebral fracture. Vertebral fractures can generally be overlooked due to non-specific presentation. Imaging diagnostics are essential in the case of trauma or injury to determine the presence of broken bones in the spine, among other health issues.
Dr. Alex Jimenez D.C., C.C.S.T.
�
Background
Vertebral fractures of the thoracic and lumbar spine are usually associated with major trauma and can cause spinal cord damage that results in neural deficits. Each vertebral region has unique anatomical and functional features that result in specific injuries. See Figure 1 above.
This article reviews the mechanisms and management of individual injuries in the thoracic and lumbar regions of the spine; information on cervical spine fractures is presented in Fracture, Cervical Spine.
For patient education resources, see the patient education article Vertebral Compression Fracture.
Epidemiology
Approximately 11,000 new spinal cord injuries occur each year, and approximately 250,000 people in the United States have a spinal cord injury. Approximately half the injuries occur in the thoracic, lumbar, and sacral areas; the other half occur in the cervical spine. The average age at injury is 32 years, and 55% of those injured are aged 16-30 years. Approximately 80% of patients in the US national database are male.
In a retrospective analysis of patients 55 years or older who had traumatic fracture to the lumbar spine, age 70 years or older was an independent predictor of mortality, whereas instrumented surgery and vertebroplasty or kyphoplasty were associated with decreased odds of death. [1]
Vehicular accidents account for approximately one third of reported cases, and approximately 25% of cases are due to violence. Other injuries are typically the result of falls or recreational sporting activities. The incidence of injuries due to violence has been increasing, while the incidence of injuries due to vehicular accidents has been declining.
The cost of a spinal cord injury that causes paraplegia is approximately $200,000 for the first year and $21,000 annually thereafter. The average lifetime cost of treating a patient with paraplegia is $730,000 for those injured at age 25 years and approximately $500,000 for those injured at age 50 years. The life expectancy for subjects with spinal cord injuries is shortened by 15-20 years compared with uninjured control subjects. The major causes of death are pneumonia, pulmonary embolism, and sepsis.
Etiology
Certain risk factors predispose the thoracic spinal cord to injury. The thoracic cord is the longest component of the spinal cord (12 segments), which results in an increased probability of injury compared to other spinal areas. The spinal canal and vertebral bodies are proportionately smaller than those of the lumbar region. Finally, the vascular supply is more tentative, with few collateral vessels, small anterior spinal arteries, and small radicular arteries. All of these factors make the thoracic cord more vulnerable to injury.
By comparison, the lumbar cord has a better vascular supply, including the large radicular vessel (usually at L2) known as the artery of Adamkiewicz. The lumbosacral enlargement is rather compact (5 lumbar spinal segments) and terminates in the conus medullaris. With a proportionately more generous spinal canal, the lumbar cord is less susceptible to direct traumatic injury or vascular insult.
Pathophysiology
Fractures of the thoracolumbar spine can be classified into 4 groups based on the mechanism of injury. The mechanism of injury is used interchangeably with the name of the fracture. These major fractures are presented in escalating order of severity.
Flexion-Compression Mechanism (Wedge or Compression Fracture)
This mechanism usually results in an anterior wedge compression fracture. As the name implies, the anterior column is compressed, with varying degrees of middle and posterior column insult. See Figure 1 above.
Ferguson and Allen have proposed a classification scheme that characterizes 3 distinct patterns of injury, as follows:
The first pattern involves anterior column failure while the middle and posterior columns remain intact. Imaging studies demonstrate wedging of the anterior component of the vertebral bodies. Loss of anterior vertebral body height is usually less than 50%. This is a stable fracture.
The second pattern involves both anterior column failure and posterior column ligamentous failure. Imaging studies demonstrate anterior wedging and may indicate increased interspinous distance. Anterior wedging can produce a loss of vertebral body height greater than 50%. This has an increased possibility of being an unstable injury.
The third pattern involves failure of all 3 columns. Imaging studies demonstrate not only anterior wedging, but also varying degrees of posterior vertebral body disruption. This is an unstable fracture. Additionally, the possibility exists for cord, nerve root, or vascular injury from free-floating fracture fragments dislodged in the spinal canal.
Axial-Compression Mechanism
This mechanism results in an injury called a burst fracture, and the pattern involves failure of both the anterior and middle columns. Both columns are compressed, and the result is loss of height of the vertebral body. Five subtypes are described, and each is dependent on concomitant, namely rotation, extension, and flexion. The 5 subtypes are (1) fracture of both endplates, (2) fracture of the superior endplate (most common), (3) fracture of the inferior endplate, (4) burst rotation fracture, and (5) burst lateral flexion fracture. [2]
McAfee classified burst fractures based on the constitution of the posterior column (stable or unstable). [3] In stable burst fractures, the posterior column is intact; in unstable burst fractures, the posterior column has sustained significant insult. Imaging studies of both stable and unstable burst fractures demonstrate loss of vertebral body height. Additionally, unstable fractures may have posterior element displacement and/or vertebral body or facet dislocation or subluxation. As with a severe wedge fracture, the possibility exists for a cord, nerve root, or vascular injury from posterior displacement of fracture fragments into the canal. Denis showed that the frequency rate of neurologic sequelae could be as high as 50%. [4] Current recommendations call for more detailed imaging studies to identify the possibility of canal impingement, which requires decompressive surgery.
Flexion-Distraction Mechanism
This mechanism results in an injury called a Chance (or seatbelt) fracture. This pattern involves failure of the posterior column with injury to ligamentous components, bony components, or both. The pathophysiology of this injury pattern is dependent on the axis of flexion. Several subtypes exist, and each is dependent on the axis of flexion and on the number and degree of column failure.
The classic Chance fracture has its axis of flexion anterior to the anterior longitudinal ligament; this results in a horizontal fracture through the posterior and middle column bony elements along with disruption of the supraspinous ligament. This is considered a stable fracture. Imaging studies show an increase in the interspinous distance and possible horizontal fracture lines through the pedicles, transverse processes, and pars interarticularis.
The flexion-distraction subtype has its axis of flexion posterior to the anterior longitudinal ligament. In addition to the previously mentioned radiographic findings, this type of injury also has an anterior wedge fracture. Because all 3 columns are involved, this is considered an unstable injury.
If the pars interarticularis is disrupted in either type of fracture, then the instability of the injury is increased, which may be radiographically demonstrated by significant subluxation. Neurologic sequelae, if they occur, appear to be related to the degree of subluxation.
Rotational Fracture-Dislocation Mechanism
The precise mechanism of this fracture is a combination of lateral flexion and rotation with or without a component of posterior-anteriorly directed force. The resultant injury pattern is failure of both the posterior and middle columns with varying degrees of anterior column insult. The rotational force is responsible for disruption of the posterior ligaments and articular facet. With sufficient rotational force, the upper vertebral body rotates and carries the superior portion of the lower vertebral body along with it. This causes the radiographic “slice” appearance sometimes seen with these types of injuries.
Denis subtyped fracture-dislocations into flexion-rotation, flexion-distraction, and shear injuries. [4] The flexion-rotation injury pattern results in failure of both the middle and posterior columns along with compression of the anterior column. Imaging studies may demonstrate vertebral body subluxation or dislocation, increased interspinous distance, and an anterior wedge fracture.
The flexion-distraction injury pattern represents failure of both the posterior and middle columns. The pars interarticularis is also disrupted. Imaging studies demonstrate an increased interspinous distance and fracture line(s) through the pedicles and transverse processes, with extension into the pars interarticularis and subsequent subluxation.
The shear (sagittal slice) injury pattern results in a 3-column failure. The combined rotational and posterior-to-anterior force vectors result in vertebral body rotation and annexation of the superior portion of the adjacent and more caudal vertebral body. Imaging studies demonstrate both the nature of the fracture and dislocation.
Each of these fractures is considered unstable. Neurologic sequelae are common.
Minor Fractures
Minor fractures include fractures of the transverse processes of the vertebrae, spinous processes, and pars interarticularis. Minor fractures do not usually result in associated neurologic compromise and are considered mechanically stable. However, because of the large forces required to cause these fractures, associated abdominal injuries may occur. In this context, the index of suspicion for associated injuries should increase and the physician should examine the patient for associated injuries.
Fractures Secondary to Osteoporosis
Osteoporosis causes fractures of the vertebrae and fractures of other bones such as the proximal humerus, distal forearm, proximal femur (hip), and pelvis (see Osteoporosis). Women are at greatest risk. The prevalence rate for these fractures increases steadily with age, ranging from 20% for 50-year-old women to 65% for older women. Most vertebral fractures are not associated with severe trauma. Many patients remain undiagnosed and present with symptoms such as back pain and increased kyphosis. The presence of a significant vertebral fracture is associated with increased mortality. Patients with these fractures have a relative risk of death that is 9 times greater than healthy counterparts. Approximately 20% of women with vertebral fractures have another fracture of a different bone within a year. [5]
Efforts are currently underway to reliably predict who is at risk for these fractures. Bone densitometry is used to assess relative bone strength and fracture risk. Risk factors for osteoporosis fractures include postmenopausal age, white race, and low bone density prior to menopause. Predicting which patients are at risk using risk factor analysis or bone imaging allows for the administration of specific treatments that promote bone deposition or delay resorption. Prevention of fractures is critical and should include exogenous calcium and an appropriate exercise regimen. Many hormonal therapies are also available, including raloxifene (Evista) and calcitonin (Miacalcin).
In 2008, the American College of Physicians developed a guideline for the pharmacologic treatment of low bone density or osteoporosis to prevent fractures. [6]
Pathologic Fractures
Pathologic fractures are the result of metastatic disease of primary cancers affecting the lung, prostate, and breast. Kaposi sarcoma can also result in vertebral body fractures. Occasionally, cancer affects the spine itself or is the result of meningeal neoplasia. Pathologic fractures tend to affect the vertebral body at both the thoracic and lumbar levels. They cause kyphotic deformity and may result in compression of the cord or cauda equina. If the patient has neurologic deficits, consider emergent radiotherapy, steroid use, and surgical decompression and stabilization. See the image below.
Figure 2: Fluoroscopic view of a kyphoplasty procedure.
Fractures Secondary to Infection
Pott disease (tuberculosis spondylitis) results from the hematogenous spread of microbacteria to the spine (see Pott Disease (Tuberculous Spondylitis)). Other bacteria can be spread to the spine and cause osteomyelitis. As bacteria proliferate, vertebral damage occurs and primarily affects the vertebral bodies. As in the case of pathologic fractures, associated fractures and an increase in kyphotic deformity may be present. Treatment includes antibiotics. The presence of a neurologic deficit may prompt instrumentation and stabilization of the spine.
Patients with Special Considerations
Elderly patients usually have significant osteoporotic disease and degenerative bone disease. These patients may experience a significant fracture even from a relatively minor, low-energy mechanism of injury. Compression fractures in both the thoracic and lumbar regions are common. These patients also may have pathological fractures. Central cord syndrome is common for patients who develop neurologic deficits. For elderly patients with stable fractures, early mobilization is important to decrease morbidity and mortality.
Special consideration should be given to pediatric patients with significant trauma to the thoracic or lumbar spine. Because the skeleton is immature and the ligaments are elastic, significant force must be generated to cause a fracture, especially those associated with neurologic deficits. One entity that occurs in pediatric patients is spinal cord injury without radiographic abnormality. If injury and neurologic deficits are strongly considered, perform imaging studies such as computed tomography (CT) or magnetic resonance imaging (MRI) scans. If the mechanism or circumstances are not consistent with the injury, consider abuse or neglect. Pediatric patients should be examined for additional injuries and bruises.
Patients in altered mental states pose a diagnostic challenge. In the absence of a reliable history and review of systems, findings from the physical examination and radiographic studies can help the physician assess vertebral injuries. In altered or intubated patients with other significant fractures such as pelvic fractures, multiple rib fractures, or scapular fractures, the physician should have a heightened index of suspicion for vertebral fractures. Once these patients have been stabilized, abdominal and chest radiographs may be supplemented with lateral views to reduce the likelihood of a missed vertebral fracture.
Diagnosis is essential in order for the healthcare professional to determine the best treatment approach for the patient’s vertebral fracture. Spinal injuries which go undiagnosed and are therefore left untreated can have an increased chance of fracture in another vertebra and it may subsequently heighten the risk of hip fracture. Early detection of vertebral fractures can further improve quality of life.
Dr. Alex Jimenez D.C., C.C.S.T.
�
Presentation
Patient History
Details of the injury and mechanism of trauma are helpful in understanding the forces involved and the possible injury. Back pain in the setting of a major accident or a fall from a significant height (>10-15 ft) may increase the index of suspicion. The threshold for obtaining radiographic studies under these circumstances is lowered, and attention to spinal precautions and logrolling is increased. The concern is to not have iatrogenically induced deterioration of neurologic function or worsening of symptoms.
A major accident may involve significant vehicular damage, a head-on collision at high speed, vehicular rollover, or death at the scene. Accidents in which extrication, damage to the steering wheel or windshield, or passenger space intrusion occurred may produce spine injuries. Vehicular accidents involving motorcycles, bicycles, or pedestrians have a higher propensity for spine injuries. Questions about seatbelt use and airbag deployment are helpful in developing a high index of suspicion for vertebral injuries.
Symptoms include pain or the development of neural deficits such as weakness, numbness, and tingling. Even transient symptoms should be investigated. The morbidity of a spinal cord injury is so significant that even minor symptoms should be investigated.
Physical Examination
Patients with vertebral fractures secondary to trauma should be evaluated and treated in a systematic fashion as outlined by advanced trauma life-support protocols. At first, attention should be directed toward the patient’s airway, breathing, and circulation (ABC). Clinicians should adhere to cervical spine precautions. The patient can be logrolled off the spinal cord while radiographs are performed.
A neurologic examination should be performed as part of the expanded primary survey or secondary survey. The neurologic examination should include the cranial nerves, motor and sensory components, coordination, and reflexes. The physician should examine the pelvic areas, perineal areas, and extremities. A rectal examination is indicated, especially if the patient has weakness in the extremities. An injury to the thoracic or lumbosacral cord would likely result in neural deficits at the trunk, genital area, and lower extremities. Specific syndromes, such as Brown-S�quard syndrome and anterior cord syndrome, may affect a major part of the spinal cord (see Brown-S�quard Syndrome).
Associated Injuries
Patients with vertebral fractures typically experience significant force as the cause of injury. As such, they are likely to have associated injuries. Almost any organ can be affected, and the secondary survey should address these issues.
An altered patient may have an intercranial injury. Chest deformity, decreased breath sounds, low oximetry readings, or poor oxygen saturation are commonly associated with pulmonary injury. Consider cardiac injury if the patient has muffled heart tones, rhythm disturbances, or hemodynamic instability. Blunt or penetrating abdominal injury may be associated with spinal fractures; in these situations, conducting a neurologic examination and instituting spinal precautions is important until a spinal cord injury has been excluded. Orthopedic injuries require a significant force to fracture the bone and thus may be associated with vertebral fractures.
A correlation exists between fracture of the transverse process of L1 and same-side renal injury. Patients with calcareous injuries have approximately a 10% chance of associated lumbar vertebral injury. Patients involved in a motor vehicle accident while wearing a lap belt who sustained lumbar fractures are at significant risk for concomitant intra-abdominal injuries (eg, diaphragmatic, hollow viscus, or solid organ injuries).
Hemodynamic Instability
In the setting of a spinal cord injury with a neurologic deficit, close attention should be paid to the hemodynamic status of the patient. In the case of neurogenic shock, hypotension is associated with relative bradycardia as a result of autonomic hyporeflexia. The thoracic sympathetic chain is disrupted, which removes sympathetic tone and leaves unopposed vagal tone. This should be distinguished from hemorrhagic shock, in which a patient is tachycardic, hypotensive, and similarly unresponsive and flaccid. Thus, attention to the heart rate and a mechanism for exsanguination may help differentiate between these forms of shock.
Patients who are on beta-blockers may remain bradycardic despite being in hemorrhagic shock. A bedside ultrasound evaluation is a noninvasive screen for free fluid in the peritoneum. The more invasive peritoneal tap and lavage is the classic method of assessment for free fluid. Both types of shock require aggressive fluid and hemodynamic resuscitation.
Spinal shock refers to the temporary loss of spinal reflex activity that occurs below a total or near-total spinal cord injury. It initially results in hyporeflexia and flaccid paralysis. With time, the descending inhibitory influence is removed and hyperreflexive arches�even spasticity may occur. For patients with spinal shock, pressures may be used after obtaining the proper fluid balance.
Indications
Patients with vertebral fractures who are neurologically intact should be assessed for the need for emergent decompressive surgery. Once the patient is hemodynamically stable and life-threatening injuries have been controlled, attention should be directed to neurologic injuries. The second consideration is obtaining a mechanically stable weight-bearing construct that allows for mechanical stability. This facilitates future ambulation and rehabilitation.
Patients with incomplete neurologic injuries need to be assessed for emergent decompressive surgery. For these patients, surgery may help maximize salvage of neurologic function. The surgeon can combine decompressive and stabilization procedures of the spine.
A study by Baldwin et al assessed conservative treatment of thoracolumbar spinal fractures. [7] Given the shortage of neurosurgeons at many trauma centers in the United States, Baldwin et al designed a treatment protocol that used radiologic criteria to screen for potentially stable fractures and to guide treatment without spinal consultation. Using both prospective and retrospective evaluation, the study determined that use of a treatment protocol for stable thoracolumbar fractures appeared safe and could help conserve resources.
Surgery for patients with complete neurologic deficit and paraplegia for more than 2-3 days is controversial. Decompressive procedures have little merit. Spinal stabilization is helpful in achieving mechanical stability and allows for more effective rehabilitation.
Relevant Anatomy
Basic Vertebral Anatomy
The vertebral column has 2 major roles: (1) a structural, weight-bearing role as the centerpiece of the axial skeleton and (2) a role as the conduit for the spinal cord. The vertebral column has 31 vertebrae. The typical vertebral body consists of a ventral segment, the body, and a dorsal part, the vertebral arch. The vertebral arch consists of a pair of pedicles and laminae and encloses the vertebral foramen. The intervertebral disks form the fibrocartilaginous articulation of the vertebral bodies. The vertebral bodies are stabilized anteriorly by the anterior longitudinal ligament and posteriorly by the posterior longitudinal ligament. The spinal canal is formed by the longitudinal apposition of the vertebral bodies, arches, disks, and ligaments. The spinal cord, meninges, and nerve roots course in the spinal canal.
Thoracic Region
The thoracic region of the spine has a relatively high stability because of the stabilizing effects of the ribs and the rib cage. This region extends from the first thoracic vertebra (T1) down to the level of tenth thoracic vertebra (T10). Additional stabilizing effects are provided by the almost-vertical orientation of the articulating processes and the shinglelike oblique arrangement of the spinal processes. A significant force is required to cause a fracture or dislocation in this region. The low thoracic region has false ribs at levels T11 and T12; thus, this region of the spine is less stable. This region can be considered the transition zone between the thoracic and lumbar regions because it resembles the lumbar region in stability and mechanisms of injury.
Lumbar and Low Thoracic Regions
The lumbar and low thoracic vertebrae are larger and wider, which is an adaptation required for their weight-bearing role as supports for the upper body and axial skeleton. In contrast to the mid and upper thoracic regions, the lumbar and low thoracic areas lack the stabilizing effect of the rib cage. The spinous processes are more horizontal, which provides increased mobility but less mechanical stability. The lumbar and low thoracic areas have greater mobility, which allows for flexion, extension, and rotation of the upper skeleton in relation to the pelvis and lower extremities.
As a result of increased mobility, the low thoracic and lumbar regions are more susceptible to injury. The transition area between the low-mobility thoracic region (T1 through T10) and the highly mobile lumbar area (approximately T11 through L2) is susceptible to injury. In adults, the spinal cord ends at the lumbosacral enlargement and conus medullaris at approximately the vertebral level of L1. Consequently, injuries to the low thoracic spine and L1 can result in significant paralysis and paraplegia of the lower body because they injure the lumbosacral enlargement of the spinal cord. In contrast, the mid and low lumbar regions are more forgiving because the individual nerve roots of the cauda equina course in this region and they are smaller, more flexible, and more resistant to injury compared with the lumbosacral enlargement.
Three-Column Model of the Spine
In 1983, Denis proposed the 3-column model of the spine, which described both the functional units that contribute to the stability of the spine and the destabilizing effect of injuries to the various columns. Denis defines the anterior column as containing the anterior longitudinal ligament, the anterior half of the vertebral body, and the related portion of the intervertebral disk and its annulus fibrosus. The middle column contains the posterior longitudinal ligament, the posterior half of the vertebral body, and the intervertebral disk and its annulus. The posterior column contains the bony elements of the posterior neural arch and the ligamental elements, which include the ligamentum flavum, the interspinous ligaments, and the supraspinous ligaments. The joint capsule of the intervertebral articulations is also part of the posterior column. Disruption of 2 or more columns results in an unstable configuration.
Contraindications
Hemodynamically unstable patients should not be taken for operative treatment of vertebral fractures until their condition has stabilized. Patients with advanced age and those with significant comorbid conditions (eg, significant coronary artery disease, peripheral vascular disease, advanced pulmonary disease) are poor candidates for any surgery, including vertebral fracture stabilization surgery. Patients with stable fractures can be observed for the development of deformity and then assessed for surgical treatment.
In conclusion, a vertebral fracture can differ tremendously from a broken arm or leg. Because a fracture in the vertebra can cause bone fragments to damage the spinal chord or nerve roots, it’s essential to receive a proper diagnosis of the extent of the spinal injury. Imaging diagnostics can help doctors determine the health issues. The scope of our information is limited to chiropractic, spinal injuries, and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Acute Back Pain
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
Fitness is loved by April Hermosillo. She enjoys exercising and eating foods that are healthful. As an athlete since age 14, her neck and lower back pain induced her to experience foot cramps. April Hermosillo tries not to allow her symptoms to change her life. April expresses just how much pain relief Dr. Alex Jimenez has provided her and how thankful she is for trusting chiropractic care with her health problems. Dr. Jimenez is highly recommended by her as the selection for pain.
Lower Back Pain Chiropractic Treatment
Eight out of 10 adults experience debilitating neck or back pain at some time in their lives. Back pain is the second most frequent cause of missed workdays because of illness, and also the most frequent cause of disability in the United States. The goal of chiropractic care is to provide safe and effective treatment which allows patients to come back to a busy lifestyle as soon as possible. Spine specialists can ascertain which treatment strategies are best for each health issue. Non-surgical treatments are the most suitable treatments for neck and back pain.
We are blessed to present to you�El Paso�s Premier Wellness & Injury Care Clinic.
As El Paso�s Chiropractic Rehabilitation Clinic & Integrated Medicine Center,�we passionately are focused on treating patients after frustrating injuries and chronic pain syndromes. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.
If you have enjoyed this video and we have helped you in any way, please feel free to subscribe and recommend�us.
Imaging diagnostics are an essential element in the evaluation of spine trauma. Over the last few decades, the rapid evolution of imaging technology has tremendously changed the assessment and treatment of spinal injuries. Imaging diagnostics utilizing CT and MRI, among others, are helpful in the acute and the chronic settings. Spinal cord and soft-tissue injuries are best evaluated by magnetic resonance imaging, or MRI, whereas computed tomography scanning, or CT scans, best evaluate spinal trauma or spine fracture. The purpose of the article below is to demonstrate the significance of imaging diagnostics in spine trauma.
Cervical Spine Fracture Evaluation
Practice Essentials
Approximately 5-10% of unconscious patients who present to the ED as the result of a motor vehicle accident or fall have a major injury to the cervical spine. Most cervical spine fractures occur predominantly at two levels: one-third of injuries occur at the level of C2, and one-half of injuries occur at the level of C6 or C7. Most fatal cervical spine injuries occur in upper cervical levels, either at craniocervical junction C1 or C2. [1, 2, 3, 4, 5, 6, 7, 8]
Anatomy
The normal anatomy of the cervical spine consists of 7 cervical vertebrae separated by intervertebral disks and joined by a complex network of ligaments. These ligaments keep individual bony elements behaving as a single unit. [7]
View the cervical spine as three distinct columns: anterior, middle, and posterior. The anterior column is composed of the anterior longitudinal ligament and the anterior two-thirds of the vertebral bodies, the annulus fibrosus and the intervertebral disks. The middle column is composed of the posterior longitudinal ligament and the posterior one-third of the vertebral bodies, the annulus, and intervertebral discs. The posterior column contains all of the bony elements formed by the pedicles, transverse processes, articulating facets, laminae, and spinous processes.
The anterior and posterior longitudinal ligaments maintain the structural integrity of the anterior and middle columns. The posterior column is held in alignment by a complex ligamentous system, including the nuchal ligament complex, capsular ligaments, and the ligamenta flava.
If one column is disrupted, other columns may provide sufficient stability to prevent spinal cord injury. If two columns are disrupted, the spine may move as two separate units, increasing the likelihood of spinal cord injury.
The atlas (C1) and the axis (C2) differ markedly from other cervical vertebrae. The atlas has no vertebral body; however, it is composed of a thick anterior arch with two prominent lateral masses and a thin posterior arch. The axis contains the odontoid process that represents fused remnants of the atlas body. The odontoid process is held in tight approximation to the posterior aspect of the anterior arch of C1 by the transverse ligament, which stabilizes the atlantoaxial joint. [9, 7]
Apical, alar and transverse ligaments provide further stabilization by allowing spinal column rotation; this prevents posterior displacement of the dens in relation to the atlas.
In pediatric patients, the spine is more flexible, and therefore, neural damage occurs much earlier than musculoskeletal injury in young patients. Because of this high flexibility, fatal consequences can occur with sometimes even minimal structural damage. Compared to adults, children have a different fulcrum because of a relatively large head, the vertebrae are not completely ossified, and the ligaments are firmly attached to articular bone surfaces that are more horizontal, making the pathophysiology of injury in children different from that in adults. [6, 10]
�
The neck consists of seven bones, or the cervical vertebrae, which support the head and connect it the body. A cervical fracture is commonly referred to as a broken neck. Cervical spine fractures often occur due to trauma or injury, such as from automobile accidents or slip-and-fall accidents. Imaging diagnostics have advanced to be able to help healthcare professionals diagnose cervical spine health issues.
Dr. Alex Jimenez D.C., C.C.S.T.
�
Evaluation of injury
When a cervical spine injury is suspected, neck movement should be minimized during transport to the treating facility. Ideally, the patients should be transported on a backboard with a semirigid collar, with the neck stabilized on the sides of the head with sandbags or foam blocks taped from side to side (of the board), across the forehead.
If spinal malalignment is identified, place the patient in skeletal traction with tongs as soon as possible (with very few exceptions), even if no evidence of neurologic deficit exists. The specific injury involved and capabilities of the consulting staff guide further management.
Place tongs one finger width above the earlobes in alignment with the external auditory canal. The consultant applies the tongs for traction under close neurologic and radiograph surveillance. Care must be taken while managing the airway in patients with potential cervical spine injuries. Video-assisted intubation should be considered to limit cervical spine motion during the process of securing the airway. [11, 12, 13, 1]
Cervical spine injuries are best classified according to several mechanisms of injury. These include flexion, flexion-rotation, extension, extension-rotation, vertical compression, lateral flexion, and imprecisely understood mechanisms that may result in odontoid fractures and atlanto-occipital dislocation. [1, 14, 4, 5, 15, 7, 16]
Radiographic evaluation is indicated in the following: [2, 2, 17, 18, 15, 19, 20]
Patients who exhibit neurologic deficits consistent with a cord lesion
Patients with an altered sensorium from head injury or intoxication
Patients who complain about neck pain or tenderness
Patients who do not complain about neck pain or tenderness but have significant distracting injuries
A standard trauma series is composed of 5 views: cross-table lateral, swimmer’s, oblique, odontoid, and anteroposterior. Approximately 85-90% of cervical spine injuries are evident in the lateral view, making it the most useful view from a clinical standpoint.
The advent of readily available multidetector computed tomography has supplanted the use of plain radiography at many centers. Recent literature supports CT as more sensitive with lower rates of missed primary and secondary injury. [14]
Thoracic Spinal Trauma Imaging
Computed Tomography
Findings
Thin-section axial CT performed by using a bone algorithm is the single most sensitive means by which to diagnose fractures of the thoracic spine. Routine helical CT scans of the thoracic spine are valuable because multisection CT scanners can generate high-resolution spinal images, even during a primary multisystemic trauma evaluation. [21, 22, 28, 29]
The CT images below display various thoracic spinal traumatic injuries.
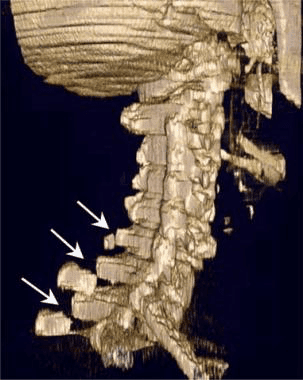
Figure 1: Lateral 3-dimensional maximum intensity projection CT scan of multiple upper thoracic and lower cervical spinous process fractures. The force necessary to fracture the spinous processes of the upper thoracic spine may also involve the lower cervical spine.
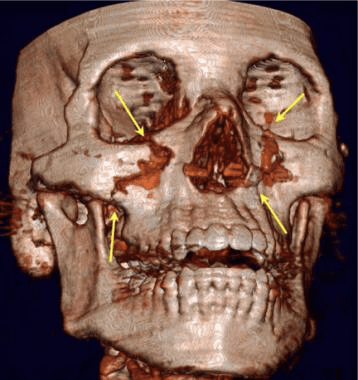
Figure 2:�Three-dimensional CT scan of complex mid-face fractures including a Le Fort I injury in a patient who had fractures of the upper thoracic and lower cervical spinous processes. Sudden deceleration of the face and skull resulted in severe stress forces on the spinous processes.
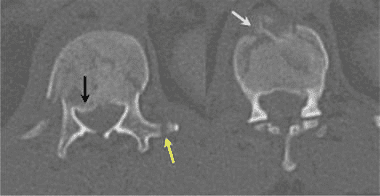
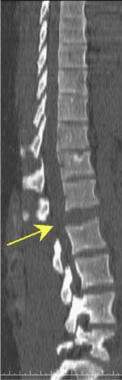
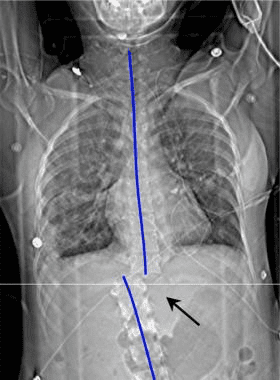
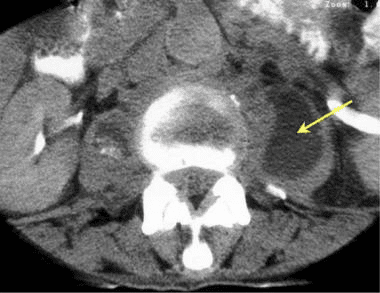
Figure 3:�Axial CT scan of a T12 compression fracture demonstrates a fracture line through the anterior body of the T12 (white arrow), posterior displacement of the T12 vertebral endplate (black arrow) into the spinal canal, and a fracture of the left transverse spinous process.
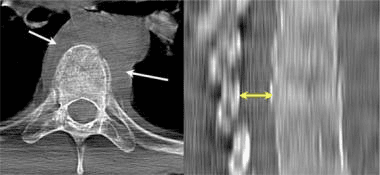
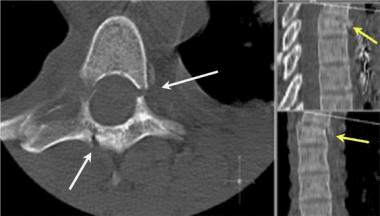
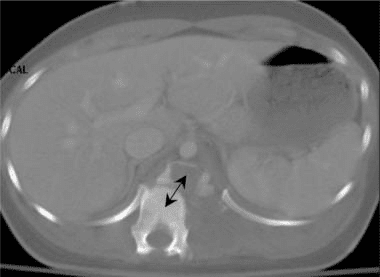
Figure 4:�Axial and sagittal CT images of an acute lower thoracic spine compression fracture. Note the paraspinal hematoma (white arrows) and the slight narrowing of the spinal canal at the level of the compression fracture (double yellow arrows).
Figure 5:�Three-dimensional CT scan of the thoracic spine demonstrates a compression fracture.
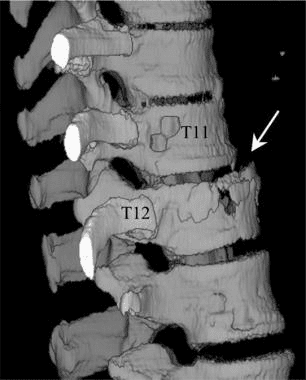
Figure 6:�Sagittal CT scan of the thoracic and lumbar spine demonstrates a complete distraction fracture at the L1-2 interspace (arrow).
Figure 7:�Axial CT image of an unstable fracture of the thoracic spine. Note the association of compression of the vertebral body with laminar and pedicle fractures. Injury to the anterior, middle and posterior columns results in an unstable fracture.
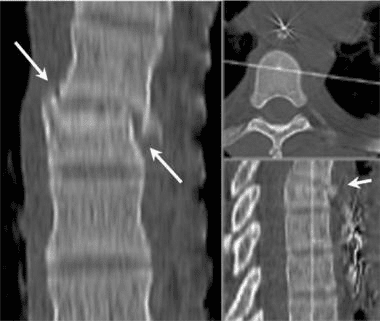
Figure 8:�Coronal multiplanar reformatted CT images of an unstable thoracic spinal fracture. The association of both anterior compression and lateral subluxation (arrows) indicates instability.
Figure 9:�Volume maximum intensity projection CT image of the entire thoracic spine demonstrates spinous process fractures of the C7 through T7 vertebra. Although spinous process fractures of the T1 may occur in a manner similar to a clay shoveler’s fracture of the C6 or C7, middle and lower thoracic spinous process fractures most likely occur due to a combination of forward flexion and axial rotation. Note the lack of findings of compression vertebral body fractures.
Figure 10:�Three-dimensional surface CT image of the cervical spine. Note the spinous process fractures of the C6, C7, and T1. CT examination of both the cervical and the thoracic spine was obtained as a single study using a multisection CT scanner. All images were obtained by using a 3-mm reconstruction with 1.5-mm collimation. Scanning times were 0.5 seconds per rotation. These 3-dimensional images were reconstructed by using an independent imaging workstation. In complex cases, reconstructed images are very useful in consultation with treating physicians.
Figure 11:�Scout view image from a spiral CT scan shows a complete subluxation fracture (curved blue lines) of the lower thoracic spine. Such an injury combines lateral displacement with rotational injury (arrow).
Figure 12: Fracture dislocation of the lower thoracic spine. Axial CT image demonstrates the large distance that the lower thoracic spine has been displaced.
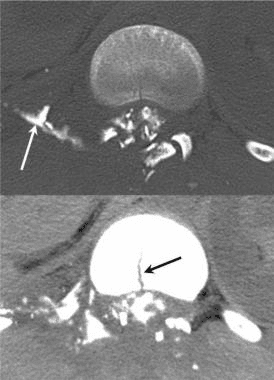
Figure 13:�Axial CT myelogram in a patient with a gunshot wound to the thoracic spine. While a fracture is obvious, the injury also resulted in a dural tear with a freely leaking cerebrospinal fluid space (white arrow). The midline fracture of the vertebral body is noted in the lower image (black arrow).
Figure 14:�Axial CT image demonstrates a complex fracture of the T12 with rotation subluxation. Air was introduced into the epidural space during the injury.
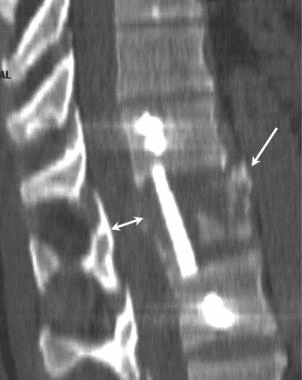
Figure 15:�Sagittal multi-planar CT image of a burst fracture following fixation. The image has been cut in the sagittal plane. Surgical repair of unstable thoracic spine fractures, such as this burst fracture, usually involves placement of an interposition graft (double black arrow) together with a lateral plate held in position by screws placed into the vertebral body above and below the injury. A residual fragment of the burst fracture is seen anteriorly (white arrow). The double white arrow illustrates the restored spinal canal.
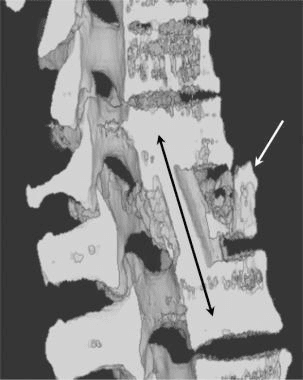
Figure 16:�Shaded-surface 3-dimensional CT image of a burst fracture following fixation. The image has been cut in the sagittal plane. Surgical repair of unstable thoracic spine fractures, such as this burst fracture, usually involves placement of an interposition graft (double black arrow) together with a lateral plate held in position by screws placed into the vertebral body above and below the injury. A residual fragment of the burst fracture is seen anteriorly (white arrow).
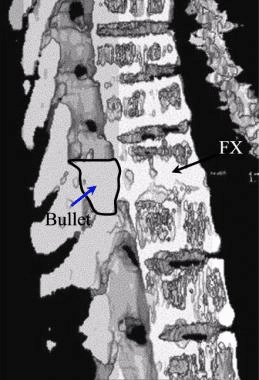
Figure 17: Shaded-surface 3-dimensional CT image of a gunshot wound to the thoracic spine. Although the bullet passed into the interspace, causing a fracture of the vertebral body, the bullet stopped within the spinal canal. Note the outline drawn around the bullet (arrow).
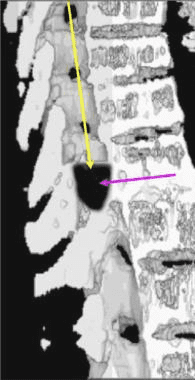
Figure 18:�Shaded-surface 3-dimensional CT scan of a gunshot wound to the thoracic spine. In other cases, the bullet may enter the spinal canal superior to the final position in the canal. The passage of the bullet within the spinal canal (yellow arrow) destroys the spinal cord and also may result in a fracture of the vertebral body. Note that the bullet has been darkened (blue arrow).
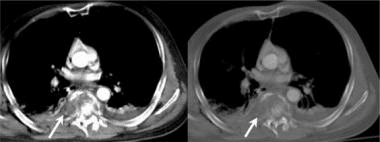
Figure 19:�Axial CT image in a man with known pulmonary tuberculosis and back pain. Note the left-sided paraspinal abscess (arrow).
Figure 20:�Sagittal shaded-surface 3-dimensional reconstruction CT scan of the lower thoracic spine. The spinal image has been cut in the midsagittal plane to demonstrate posterior displacement of the thoracic spinal vertebral body (arrow) and downward displacement of the superior endplate. Note the general wedge shape of the vertebral body.
Because of its superior contrast definition and the absence of superimposed structures, good-quality CT imaging depicts more thoracic spinal injuries than do conventional radiographic studies. However, the percentage of clinically important fractures that are seen on CT scans but not on radiographs is lower with thoracic than with cervical spinal fractures. Most of the fractures missed on radiographs were spinous process fractures, transverse processes fractures, and fractures in large patients. Because axial CT is performed with patients in a neutral position, bony distraction of the fracture fragments and subluxations of the spinal articulations may not be as significant on CT images as on they are on acute trauma-series radiographs. [22, 25, 28, 29, 30, 31, 32]
The level of a burst fracture and the percentage of spinal canal stenosis have been correlated with associated neurologic deficits. A significant correlation exists between neurologic deficit and the percentage of spinal canal stenosis. The higher the level of injury, the greater the probability of neurologic deficit. This association may be related to the smaller canal diameter in the upper thoracic spine. The severity of neurologic deficit cannot be predicted.
In patients with Chance-type fractures, CT scans often show a burst-type fracture with posterior cortex buckling or retropulsion, and serial transaxial CT images often show a gradual loss of definition of the pedicles. [23]
The thoracic spine, located between the cervical and lumbar vertebrae, consists of 12 vertebrae levels. Thoracic spinal trauma, including spinal cord injuries along the middle of the spine, can generally be severe, however, with early treatment, long-term prognosis is good. Therefore, imaging diagnostics for thoracic spinal trauma are essential. Many healthcare professionals can provide patients with these services.
Dr. Alex Jimenez D.C., C.C.S.T.
�
Degree of Confidence
The confidence level for the diagnosis of a thoracic spinal fracture with 2-mm axial sections (possible with a multisection CT unit) is greater than 98% and reportedly 99%.
Because axial CT is performed with the patient in a neutral position, a bony distraction of the fracture fragments and subluxations of the spinal articulations may not be as significant on CT images as on acute trauma-series radiographs.
False Positives/Negatives
False-positive results may occur in patients with a Schmorl node, which is a chronic internal herniation of the vertebral disk into the thoracic vertebral body endplate and failure of the fusion of the anterior vertebral endplate epiphysis, resulting in a limbus vertebra. False-negative CT studies may occur in chronic stress injuries and severe generalized osteoporotic endplate fractures.
It has been reported that among trauma patients who had a chest and/or abdominal CT, fractures of the thoracic spine are frequently underreported. Sagittal reformats of the spine obtained from thin sections, and morphometric analysis using electronic calipers help to identify fractures that might otherwise not be identified. [25]
In conclusion, imaging diagnostics of�spinal trauma or spine fracture are essential towards the assessment and treatment of patients. Magnetic resonance imaging, or MRI, is helpful in the evaluation of spinal cord and soft-tissue injuries whereas computed tomography scanning, or CT scans, is helpful in the evaluation of spinal trauma or spine fracture. The understanding of imaging technology has tremendously enhanced advances in treatment.� The scope of our information is limited to chiropractic, spinal injuries, and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Acute Back Pain
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
Imaging diagnostics of the spine consist from radiographies to computed tomography scanning, or CT scans, in which CT is utilized in conjunction with myelography and most recently with magnetic resonance imaging, or MRI. These imaging diagnostics are being used to determine the presence of abnormalities of the spine, scoliosis, spondylolysis and spondylolisthesis. The following article describes various imaging modalities and their application in the evaluation of common spinal disorders described.
Achondroplasia
Achondroplasia is the most common cause of rhizomelic (root/proximal) short-limb dwarfism. Patients are of normal intelligence.�
It shows multiple distinct radiographic abnormalities affecting long bones, pelvis, skull, and hands.
Vertebral column changes may present with significant clinical and neurological abnormalities.�
Achondroplasia is an autosomal dominant disorder with about 80% of cases from a random new mutation. Advanced paternal age is often linked. Achondroplasia results from a mutation in the fibroblast growth factor gene (FGFR3) which causes abnormal cartilage formation.
All bones formed by endochondral ossification are affected.
Bones that form by intra-membranous ossification are not normal.
Thus, skull vault, iliac wings develop normally vs. the base of the skull, some facial bones, vertebral column, and most tubular bones are abnormal.
�
Dx: is usually made at birth with many features becoming apparent during the first few years of life.
Radiography plays an important part of clinical diagnosis.
Typical features include: shortening and widening of tubular bones, metaphyseal flaring, Trident hand with short, broad metacarpals and proximal and middle phalanges. Longer Fibular, Tibial bowing, markedly short humeri often with dislocated Radial head and elbow flexion deformity.
Spine: characteristic narrowing of L1-L5 interpedicular distance on AP views. Lateral view shows shortening of pedicles and vertebral bodies, �bullet shaped vertebrae� can be a characteristic feature. Early degenerative changes and canal narrowing occur. The horizontal sacral inclination is an important feature.
Pelvis is broad and short with characteristic �champagne glass� pelvis appearance.
Femoral heads are hypoplastic, but hip arthrosis is normally not observed even in older patients likely due to reduced leverage and lightweight (50kg) of patients.
Management of Achondroplasia
Recombinant human growth hormone (GH)�is currently being used to augment the height of patients with achondroplasia.
Most complications of Achondroplasia are related to the spine: vertebral canal stenosis, thoracolumbar kyphosis, narrowed foramen magnum and others.
Laminectomy extending to pedicles/lateral recess with foraminotomies and discectomies can be performed.
Cervical manipulations are contraindicated.
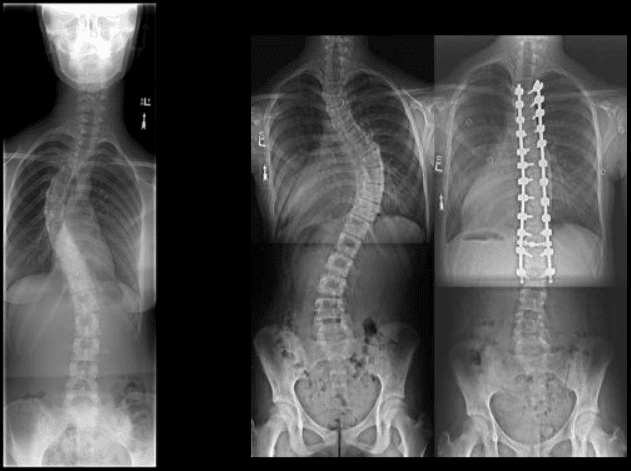
Imaging diagnostics play a fundamental role in the diagnosis the of scoliosis, an abnormality of the spine which is believed to occur due to an underlying health issue, although most cases of scoliosis are idiopathic. More over, radiographies, CT scans, and MRI, among others, can help monitor the changes of the deformity of the spine associated with this spinal manifestation. Chiropractors can provide imaging diagnostics to patients with scoliosis before proceeding with treatment.�
Dr. Alex Jimenez D.C., C.C.S.T.
�
Scoliosis
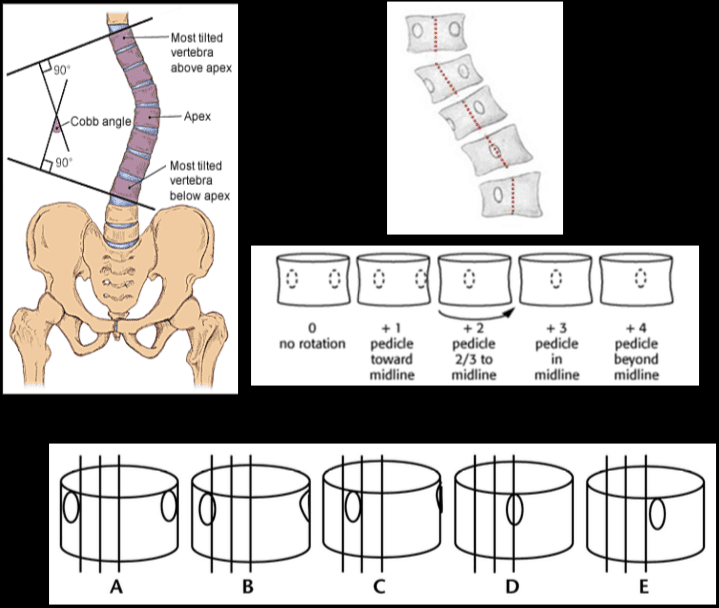
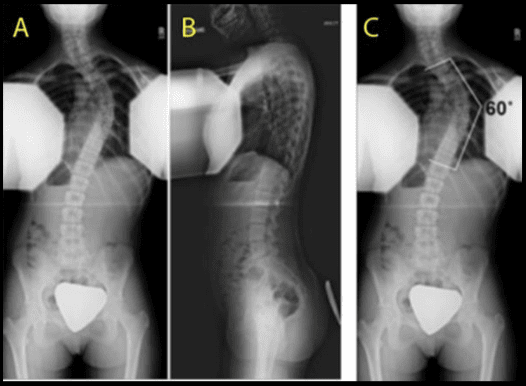
Scoliosis is defined as the abnormal lateral curvature of the spine >10-degree when examined by Cobb�s method of mensuration.
Scoliosis can be described as postural and structural.
Postural scoliosis is not fixed and can be improved by lateral flexion to the side of the convexity.
Structural scoliosis has multiple causes ranging from: ? Idiopathic (>80%) ? Congenital (wedge or hemivertebra, blocked vertebra, Marfan syndrome, skeletal dysplasias) ? Neuropathic (neurofibromatosis, neurological conditions like tethered cord, spinal dysraphism, etc.) ? Scoliosis d/t Spinal neoplasms ? Post-traumatic etc.
Idiopathic scoliosis is the most common type (>80%).
Idiopathic scoliosis can be of 3-types ( infantile, juvenile, adolescent).
Idiopathic adolescent scoliosis if patients >10y.o.
Infantile scoliosis if <3 y.o. M>F.
Juvenile scoliosis if >3 but <10-y.o.
Idiopathic Adolescent scoliosis is the most common with F:M 7:1 (adolescent girls are at particular risk).
Etiology: unknown thought to be the result of some disturbance of proprioceptive control of the spine and spinal musculature, other hypotheses exist.
Most seen in the thoracic region and most commonly convex to the right.
Dx: full spine radiography with gonadal and breast shielding (preferably PA views to protect breast tissue).
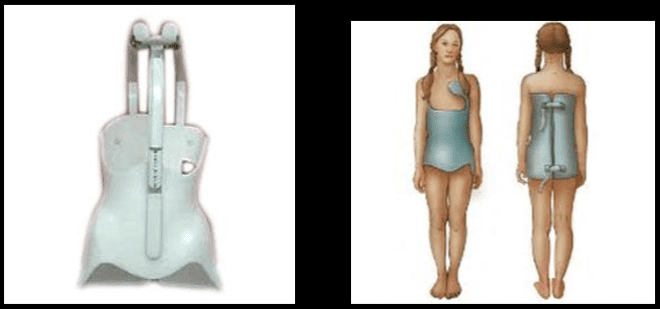
� Curves that are 50-degrees or greater and rapidly progressing will require operative intervention to prevent severe deformity of the thorax & ribs leading to cardiopulmonary abnormalities. � �? If curvature is < 20-degree, no treatment is required (observation). � �? For curves that are >20-40-degrees bracing may be used (orthosis).
Milwaukee (metal) brace (left).
Boston brace polypropylene lined with polyethylene (right) often preferred because it can be worn under clothing.
Bracing wearing is required for 24-hours for the duration of the treatment.
Note Cobb�s method of mensuration to record spinal curvature. It has some limitations: 2D imaging, not able to estimate rotation, etc.
Cobb�s method is still a standard evaluation performed in Scoliosis studies.
Nash-Moe method: determines pedicle rotation in scoliosis.
Risser index is used to estimate spinal skeletal maturity.
Iliac growth apophysis appears at ASIS (F- 14, M-16) and progresses medially and expected to be closed in 2-3-years (Risser 5).
Scoliosis progression ends at Risser 4 in females & Risser 5 in males.
During radiographic evaluation of scoliosis, it is crucial to report if Risser growth apophysis remains open or closed.
Spondylolysis and spondylolisthesis are health issues which can result in back pain. Spondylolysis is believed to be caused by repeated microtrauma leading to stress fractures in the pars interarticularis. Patients with bilateral pars defects can develop spondylolisthesis, where the degree of slippage of the adjacent vertebrae can progress gradually over time. Patients with suspected spondylolysis and spondylolisthesis may initially be evaluated with pain radiography. Chiropractic care can also help provide imaging diagnostics for these health issues.
Dr. Alex Jimenez D.C., C.C.S.T.
�
Spondylolysis & Spondylolisthesis
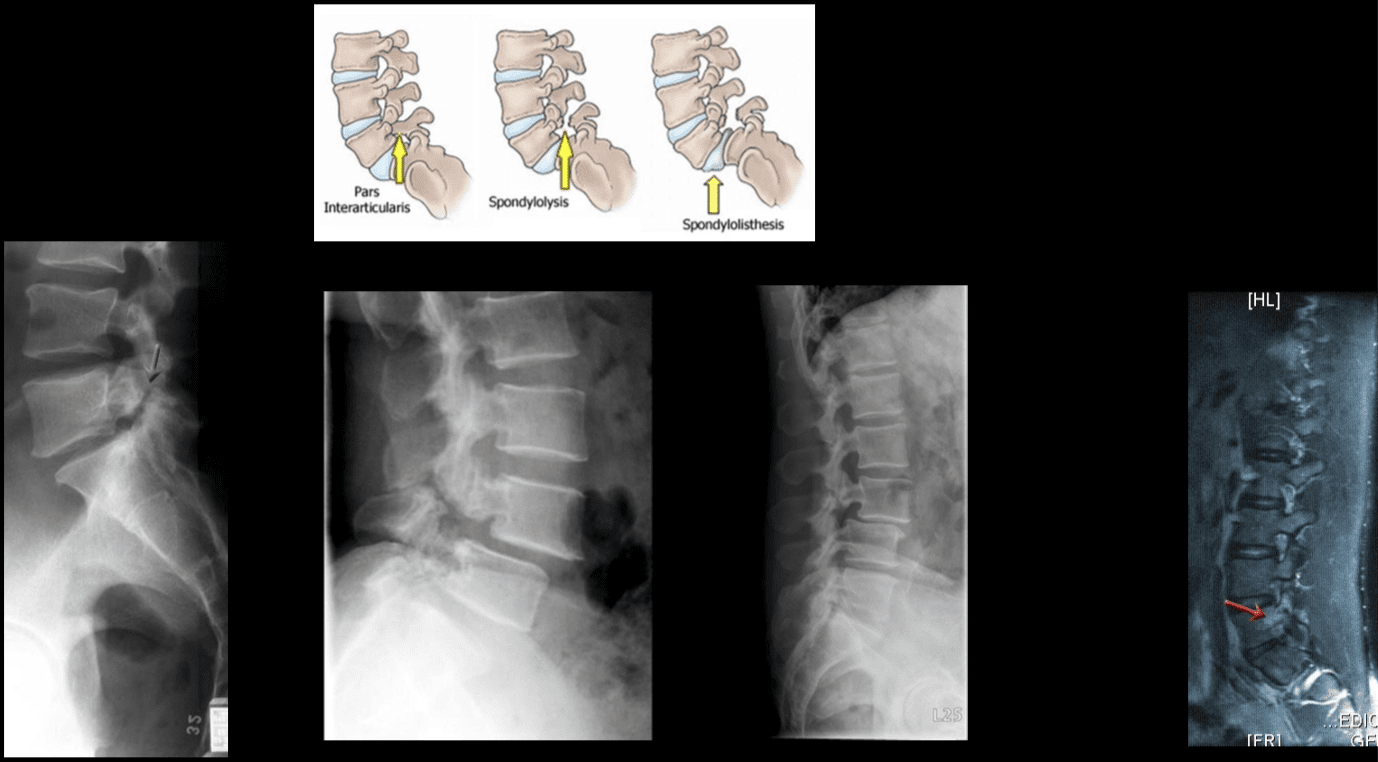
Spondylolysis defect in pars interarticularis or osseous bridge between superior and inferior articular processes.
Pathology stress fracture of the pars, believed to be after repeated microtrauma on extensions Men > Women, affects 5% of the general population especially in athletic adolescents.
Clinically postulated that adolescent back pain cases may be related to this process.
Typically spondylolysis remains asymptomatic.
Spondylolysis can be present with or w/o spondylolisthesis.
Spondylolysis is found in 90% at L5 with the remaining 10% in L4.
Can be uni or bilateral.
In 65%�of�cases, spondylolysis is associated with spondylolisthesis.
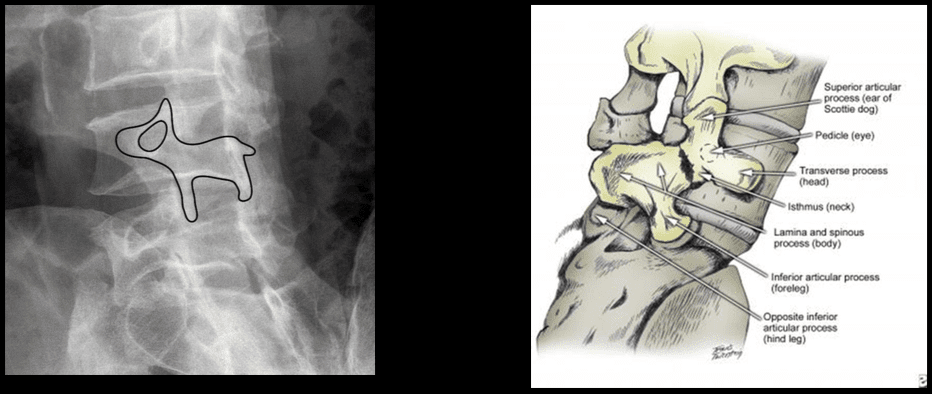
Radiographic Features: break in the Scotty dog collar around the neck on oblique lumbar views.
Radiography has low sensitivity compared to SPECT. SPECT is associated with ionizing radiation, and MRI is currently a preferred method of imaging diagnosis.
MRI can help to show reactive marrow edema next to pars defect or w/o defect so-called pending or potential to develop spondylolysis.
Types of Spondylolisthesis
Type 1 – Dysplastic, rare and found in congenital dysplastic malformation of the sacrum allowing anterior displacement of L5 on S1. Often no pars defect.
Type 2 – Isthmic, most common, often the result of a stress fracture.
Type 3 – Degenerative from the remodeling of articular processes.
Type 4 – Traumatic in an acute posterior arch fracture.
Type 5 – Pathologic due to bone disease locally or generalized.
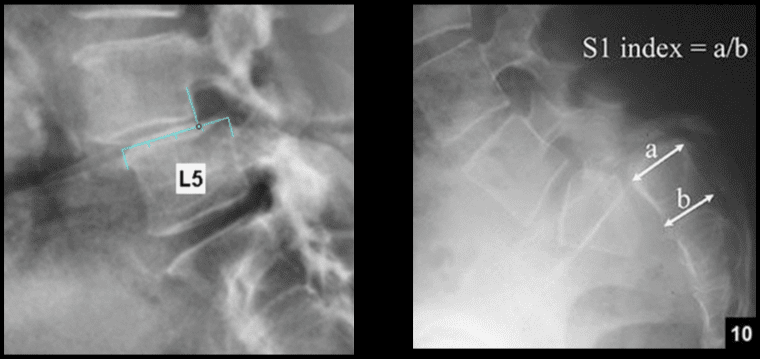
Grading of spondylolisthesis is based on the Myereding Classification. This classification refers to the overhanging part of the superior body in relation to anterior-posterior part of the inferior body.
Grade 1 – 0-25% anterior slip
Grade 2 – 26-50%
Grade 3 – 51%-75%
Grade 4 – 76-100%
Grade 5 – >100% spondyloptosis
Note degenerative spondylolisthesis at L4 and retrolisthesis at L2, L3.
This abnormality develops due to degeneration of facets and disc with decreased local stability.
Rarely progresses beyond Grade 2.
Must be recognized in the imaging report.
Contributes to vertebral canal stenosis.
Canal stenosis is better delineated by cross-sectional imaging.
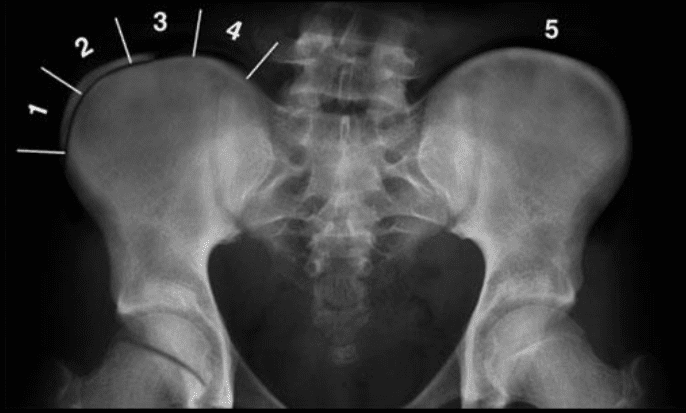
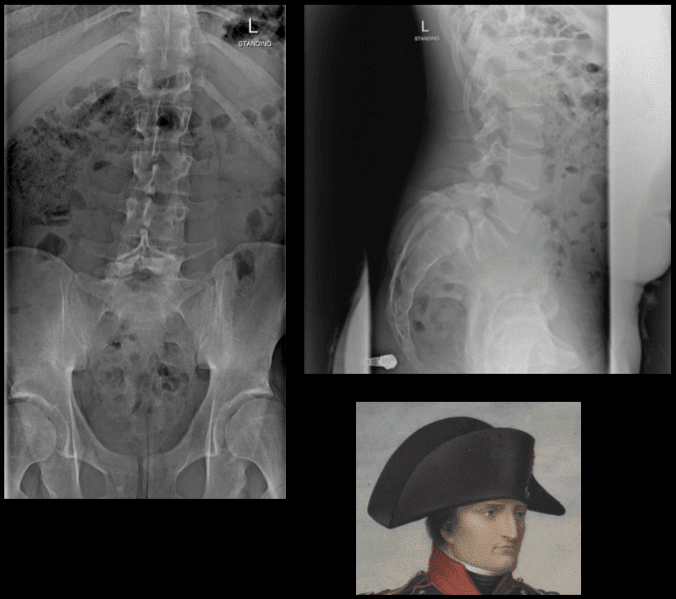
The inverted Napoleon hat sign -�seen on the frontal lumbar/pelvic radiographs at L5-S1.
Represents bilateral spondylolysis with marked anterolisthesis of L5 on S1 often with spondyloptosis and marked exaggeration of the normal lordosis.
Spondylolysis resulting in this degree of spondylolisthesis is more often congenital and/or traumatic in origin and less often degenerative.
The “brim” of the hat is formed by the downward rotation of the transverse processes, and the “dome” of the hat is formed by the body of L5.
In conclusion,�imaging diagnostics for the spine are recommended for patients with specific abnormalities of the spine, however, their increased use can help determine�their best treatment option. Understanding the abnormalities of the spine described above can help healthcare professionals and patients create a treatment program to improve their symptoms. The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Acute Back Pain
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
While computed tomography scanning, or CT scans, of the cervical spine are frequently utilized to help diagnose neck injuries, simple radiographs are still commonly performed for patients who have experienced minor cervical spine injuries with moderate neck pain, such as those who have suffered a slip-and-fall accident. Imaging diagnostic assessments may reveal underlying injuries and/or aggravated conditions to be more severe than the nature of the trauma. The purpose of the article is to demonstrate the significance of cervical spine radiographs in the trauma patient.�
Abstract
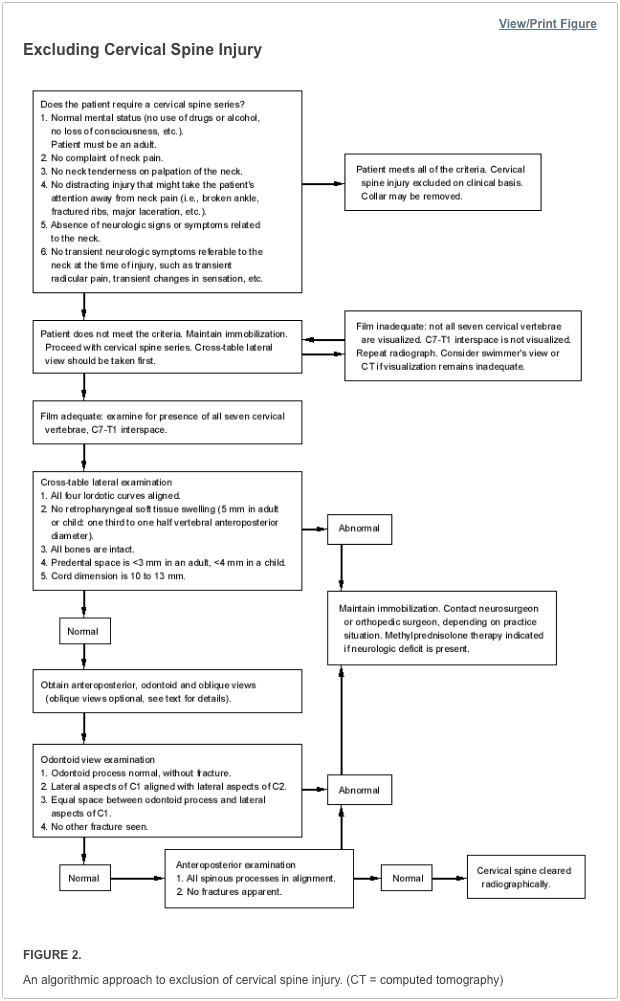
Significant cervical spine injury is very unlikely in a case of trauma if the patient has normal mental status (including no drug or alcohol use) and no neck pain, no tenderness on neck palpation, no neurologic signs or symptoms referable to the neck (such as numbness or weakness in the extremities), no other distracting injury and no history of loss of consciousness. Views required to radiographically exclude a cervical spine fracture include a posteroanterior view, a lateral view and an odontoid view. The lateral view must include all seven cervical vertebrae as well as the C7-T1 interspace, allowing visualization of the alignment of C7 and T1. The most common reason for a missed cervical spine injury is a cervical spine radiographic series that is technically inadequate. The �SCIWORA� syndrome (spinal cord injury without radiographic abnormality) is common in children. Once an injury to the spinal cord is diagnosed, methylprednisolone should be administered as soon as possible in an attempt to limit neurologic injury.
Radiographs continue to be used as a first-line imaging diagnostic assessment modality in the evaluation of patients with suspected cervical spine injuries. The aim of cervical spine radiographs is to confirm the presence of a health issue in the complex structures of the neck and define its extent, particularly with respect to instability. Multiple views may generally be necessary to provide optimal visualization.
Dr. Alex Jimenez D.C., C.C.S.T.
Introduction
Although cervical spine radiographs are almost routine in many emergency departments, not all trauma patients with a significant injury must have radiographs, even if they arrive at the emergency department on a backboard and wearing a cervical collar. This article reviews the proper use of cervical spine radiographs in the trauma patient.
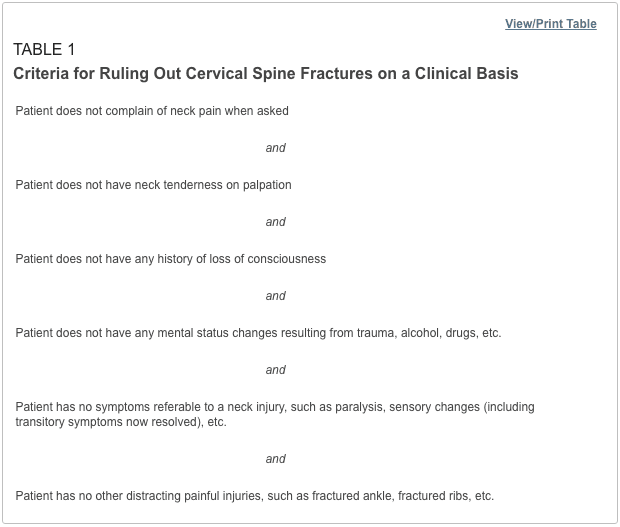
Low-risk criteria have been defined that can be used to exclude cervical spine fractures, based on the patient’s history and physical examination.1�6 Patients who meet these criteria (Table 1) do not require radiographs to rule out cervical fractures. However, the criteria apply only to adults and to patients without mental status changes, including drug or alcohol intoxication. Although studies suggest that these criteria may also be used in the management of verbal children,7�9 caution is in order, since the study series are small, and the ability of children to complain about pain or sensory changes is variable. An 18-year-old patient can give a more reliable history than a five-year-old child.
Some concern has been expressed about case reports suggesting that �occult� cervical spine fractures will be missed if asymptomatic trauma patients do not undergo radiography of the cervical spine.10 On review, however, most of the reported cases did not meet the low-risk criteria in Table 1. Attention to these criteria can substantially reduce the use of cervical spine radiographs.
Cervical Spine Series and Computed Tomography
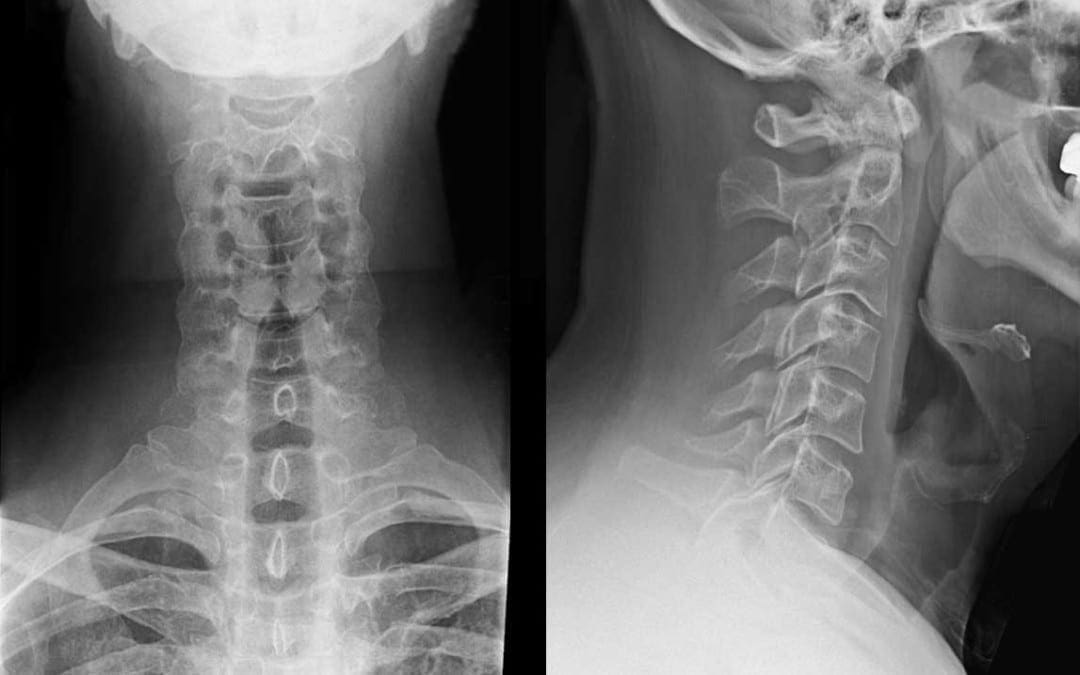
Once the decision is made to proceed with a radiographic evaluation, the proper views must be obtained. The single portable cross-table lateral radiograph, which is sometimes obtained in the trauma room, should be abandoned. This view is insufficient to exclude a cervical spine fracture and frequently must be repeated in the radiographic department.11,12 The patient’s neck should remain immobilized until a full cervical spine series can be obtained in the radiographic department. Initial films may be taken through the cervical collar, which is generally radiolucent. An adequate cervical spine series includes three views: a true lateral view, which must include all seven cervical vertebrae as well as the C7-T1 junction, an anteroposterior view and an open-mouth odontoid view.13
If no arm injury is present, traction on the arms may facilitate visualization of all seven cervical vertebrae on the lateral film. If all seven vertebrae and the C7-T1 junction are not visible, a swimmer’s view, taken with one arm extended over the head, may allow adequate visualization of the cervical spine. Any film series that does not include these three views and that does not visualize all seven cervical vertebrae and the junction of C7-T1 is inadequate. The patient should be maintained in cervical immobilization, and plain films should be repeated or computed tomographic (CT) scans obtained until all vertebrae are clearly visible. The importance of obtaining all of these views and visualizing all of the vertebrae cannot be overemphasized. While some missed cervical fractures, subluxations and dislocations are the result of film misinterpretation, the most frequent cause of overlooked injury is an inadequate film series.14,15
In addition to the views listed above, some authors suggest adding two lateral oblique views.16,17 Others would obtain these views only if there is a question of a fracture on the other three films or if the films are inadequate because the cervicothoracic junction is not visualized.18 The decision to take oblique views is best made by the clinician and the radiologist who will be reviewing the films.
Besides identifying fractures, plain radiographs can also be useful in identifying ligamentous injuries. These injuries frequently present as a malalignment of the cervical vertebrae on lateral views. Unfortunately, not all ligamentous injuries are obvious. If there is a question of ligamentous injury (focal neck pain and minimal malalignment of the lateral cervical x-ray [meeting the criteria in Table 2]) and the cervical films show no evidence of instability or fracture, flexion-extension views should be obtained.17,19 These radiographs should only be obtained in conscious patients who are able to cooperate. Only active motion should be allowed, with the patient limiting the motion of the neck based on the occurrence of pain. Under no circumstance should cervical spine flexion and extension be forced, since force may result in cord injury.
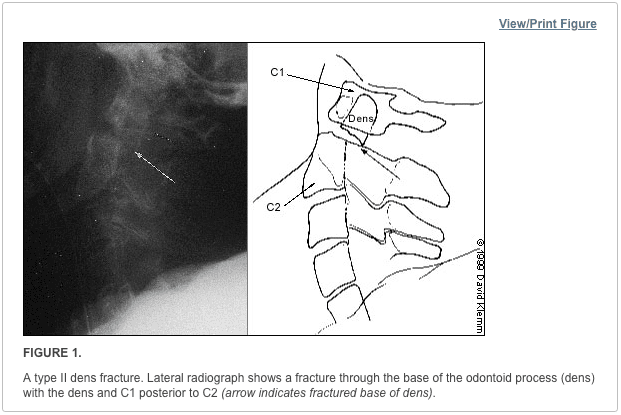
Although they may be considered adequate to rule out a fracture, cervical spine radiographs have limitations. Up to 20 percent11,20,21 of fractures are missed on plain radiographs. If there is any question of an abnormality on the plain radiograph or if the patient has neck pain that seems to be disproportionate to the findings on plain films, a CT scan of the area in question should be obtained. The CT is excellent for identifying fractures, but its ability to show ligamentous injuries is limited.22 Occasionally, plain film tomography may be in order if there is a concern about a type II dens fracture (Figure 1).
While some studies have used magnetic resonance imaging (MRI) as an adjunct to plain films and CT scanning,23,24 the lack of wide availability and the relatively prolonged time required for MRI scanning limits its usefulness in the acute setting. Another constraint is that resuscitation equipment with metal parts may not be able to function properly within the magnetic field generated by the MRI.
Cervical Spine Radiography
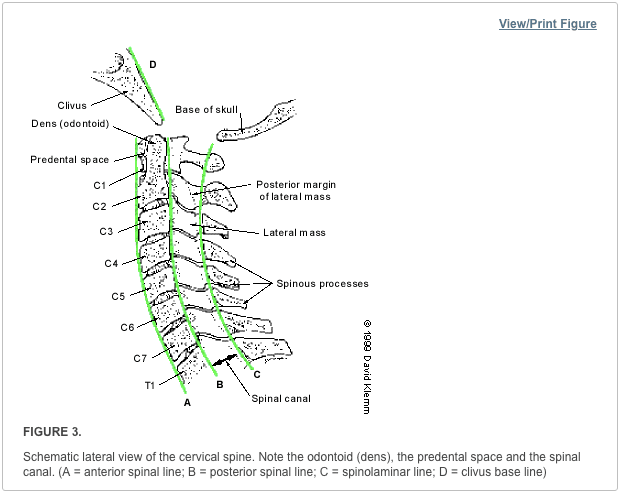
Figure 2 summarizes the approach to reading cervical spine radiographs.
Lateral View
Alignment of the vertebrae on the lateral film is the first aspect to note (Figure 3). The anterior margin of the vertebral bodies, the posterior margin of the vertebral bodies, the spinolaminar line and the tips of the spinous processes (C2-C7) should all be aligned. Any malalignment (Figures 4 and 5) should be considered evidence of ligamentous injury or occult fracture, and cervical spine immobilization should be maintained until a definitive diagnosis is made.
Confusion can sometimes result from pseudosubluxation, a physiologic misalignment that is due to ligamentous laxity, which can occur at the C2-C3 level and, less commonly, at the C3-C4 level. While pseudosubluxation usually occurs in children, it also may occur in adults. If the degree of subluxation is within the normal limits listed in Table 2 and the neck is not tender at that level, flexion-extension views may clarify the situation. Pseudosubluxation should disappear with an extension view. However, flexion-extension views should not be obtained until the entire cervical spine is otherwise cleared radiographically.
After ensuring that the alignment is correct, the spinous processes are examined to be sure that there is no widening of the space between them. If widening is present, a ligamentous injury or fracture should be considered. In addition, if angulation is more than 11 degrees at any level of the cervical spine, a ligamentous injury or fracture should be assumed. The spinal canal (Figure 2) should be more than 13 mm wide on the lateral view. Anything less than this suggests that spinal cord compromise may be impending.
Next, the predental space�the space between the odontoid process and the anterior portion of the ring of C1 (Figure 2)�is examined. This space should be less than 3 mm in adults and less than 4 mm in children (Table 2). An increase in this space is presumptive evidence of a fracture of C1 or of the odontoid process, although it may also represent ligamentous injury at this level. If a fracture is not found on plain radiographs, a CT scan should be obtained for further investigation. The bony structures of the neck should be examined, with particular attention to the vertebral bodies and spinous processes.
The retropharyngeal space (Figure 2) is now examined. The classic advice is that an enlarged retropharyngeal space (Table 2) indicates a spinous fracture. However, the normal and abnormal ranges overlap significantly.25 Retropharyngeal soft tissue swelling (more than 6 mm at C2, more than 22 mm at C6) is highly specific for a fracture but is not very sensitive.26 Soft tissue swelling in symptomatic patients should be considered an indication for further radiographic evaluation. Finally, the craniocervical relationship is checked.
Odontoid View
The dens is next examined for fractures. Artifacts may give the appearance of a fracture (either longitudinal or horizontal) through the dens. These artifacts are often radiographic lines caused by the teeth overlying the dens. However, fractures of the dens are unlikely to be longitudinally oriented. If there is any question of a fracture, the view should be repeated to try to get the teeth out of the field. If it is not possible to exclude a fracture of the dens, thin-section CT scans or plain film tomography is indicated.
Next, the lateral aspects of C1 are examined. These aspects should be symmetric, with an equal amount of space on each side of the dens. Any asymmetry is suggestive of a fracture. Finally, the lateral aspects of C1 should line up with the lateral aspects of C2. If they do not line up, there may be a fracture of C1. Figure 6 demonstrates asymmetry in the space between the dens and C1, as well as displacement of the lateral aspects of C1 laterally.
Anteroposterior View
The height of the cervical spines should be approximately equal on the anteroposterior view. The spinous processes should be in midline and in good alignment. If one of the spinous processes is off to one side, a facet dislocation may be present.
Common Cervical Abnormalities
The most common types of cervical abnormalities and their radiographic findings are listed in Table 3. Except for the clay shoveler’s fracture, they should be assumed to be unstable and warrant continued immobilization until definitive therapy can be arranged. Any patient found to have one spinal fracture should have an entire spine series, including views of the cervical spine, the thoracic spine and the lumbosacral spine. The incidence of noncontiguous spine fractures ranges up to 17 percent.27,28 Figures 7 through 9 demonstrate aspects of common cervical spine fractures.
Initial Treatment of Cervical Spine and Cord
If a cervical fracture or dislocation is found, orthopedic or neurosurgical consultation should be obtained immediately. Any patient with a spinal cord injury should begin therapy with methylprednisolone within the first eight hours after the injury, with continued administration for up to 24 hours. Patients should receive methylprednisolone in a dosage of 30 mg per kg given intravenously over one hour. Over the next 23 hours, intravenous methylprednisolone in a dosage of 5.4 mg per kg per hour should be administered. This therapy has been shown to improve outcomes and minimize cord injury,29 although it is not without its problems. The incidence of pneumonia is increased in patients treated with high dosages of methylprednisolone.30
�Sciwora� Syndrome: Unique in Children
A special situation involving children deserves mention. In children, it is not uncommon for a spinal cord injury to show no radiographic abnormalities. This situation has been named �SCIWORA� (spinal cord injury without radiographic abnormality) syndrome. SCIWORA syndrome occurs when the elastic ligaments of a child’s neck stretch during trauma. As a result, the spinal cord also undergoes stretching, leading to neuronal injury or, in some cases, complete severing of the cord.31 This situation may account for up to 70 percent of spinal cord injuries in children and is most common in children younger than eight years. Paralysis may be present on the patient’s arrival in the emergency department. However, up to 30 percent of patients have a delayed onset of neurologic abnormalities, which may not occur until up to four or five days after the injury. In patients with delayed symptoms, many have neurologic symptoms at the time of the injury, such as paresthesias or weakness, that have subsequently resolved.32
It is important to inform the parents of young patients with neck trauma about this possibility so that they will be alert for any developing symptoms or signs. Fortunately, most children with SCIWORA syndrome have a complete recovery, especially if the onset is delayed.33 It is possible to evaluate these injuries with MRI, which will show the abnormality and help determine the prognosis: a patient with complete cord transection is unlikely to recover.3
The treatment of SCIWORA syndrome has not been well studied. However, the general consensus is that steroid therapy should be used.34 In addition, any child who has sustained a significant degree of trauma but has recovered completely should be restricted from physical activities for several weeks.34
Cervical spine radiographs include three standard views, such as the coned odontoid peg view, the anteroposterior view of the entire cervical spine, and the lateral view of the entire cervical spine. Most qualified and experienced healthcare professionals, including chiropractors, offer additional views to visualize the cervicothoracic junction as well as to evaluate the proper alignment of the spine in all patients.�
Dr. Alex Jimenez D.C., C.C.S.T.
About the Authors
MARK A. GRABER, M.D., is associate professor of clinical family medicine and surgery (emergency medicine) at the University of Iowa Hospitals and Clinics, Iowa City. He received his medical degree from Eastern Virginia Medical School, Norfolk, and served a residency in family medicine at the University of Iowa College of Medicine, Iowa City.
MARY KATHOL, M.D., is associate professor of radiology at the University of Iowa Hospitals and Clinics. She is also head of the musculoskeletal radiology section. She received her medical degree from the University of Kansas School of Medicine, Kansas City, Kan., and served a residency in radiology at the University of Iowa College of Medicine.
Address correspondence to Mark A. Graber, M.D., Department of Family Medicine, Steindler Bldg., University of Iowa Hospitals and Clinics, Iowa City, Iowa 52242. Reprints are not available from the authors.
In conclusion,�it is essential to evaluate all views of the cervical spine through imaging diagnostic assessments. While cervical spine radiographs can reveal injuries and conditions, not all neck injuries are detected through radiography. Computed tomography, or CT, scans of the cervical spine are highly accurate in the diagnosis of neck fractures which can help with treatment. The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at�915-850-0900�.
Curated by Dr. Alex Jimenez
Additional Topics: Acute Back Pain
Back pain�is one of the most prevalent causes of disability and missed days at work worldwide. Back pain attributes to the second most common reason for doctor office visits, outnumbered only by upper-respiratory infections. Approximately 80 percent of the population will experience back pain at least once throughout their life. The spine is a complex structure made up of bones, joints, ligaments, and muscles, among other soft tissues. Because of this, injuries and/or aggravated conditions, such as�herniated discs, can eventually lead to symptoms of back pain. Sports injuries or automobile accident injuries are often the most frequent cause of back pain, however, sometimes the simplest of movements can have painful results. Fortunately, alternative treatment options, such as chiropractic care, can help ease back pain through the use of spinal adjustments and manual manipulations, ultimately improving pain relief.
1.�Kreipke DL, Gillespie KR, McCarthy MC, Mail JT, Lappas JC, Broadie TA. Reliability of indications for cervical spine films in trauma patients.�J Trauma. 1989;29:1438�9.
2.�Ringenberg BJ, Fisher AK, Urdaneta LF, Midthun MA. Rational ordering of cervical spine radiographs following trauma.�Ann Emerg Med. 1988;17:792�6.
3.�Bachulis BL, Long WB, Hynes GD, Johnson MC. Clinical indications for cervical spine radiographs in the traumatized patient.�Am J Surg. 1987;153:473�8.
4.�Hoffman JR, Schriger DL, Mower W, Luo JS, Zucker M. Low-risk criteria for cervical-spine radiography in blunt trauma: a prospective study.�Ann Emerg Med. 1992;21:1454�60.
5.�Saddison D, Vanek VW, Racanelli JL. Clinical indications for cervical spine radiographs in alert trauma patients.�Am Surg. 1991;57:366�9.
6.�Kathol MH, El-Khoury GY. Diagnostic imaging of cervical spine injuries.�Seminars in Spine Surgery. 1996;8(1):2�18.
7.�Lally KP, Senac M, Hardin WD Jr, Haftel A, Kaehler M, Mahour GH. Utility of the cervical spine radiograph in pediatric trauma.�Am J Surg. 1989;158:540�1.
8.�Rachesky I, Boyce WT, Duncan B, Bjelland J, Sibley B. Clinical prediction of cervical spine injuries in children. Radiographic abnormalities.�Am J Dis Child. 1987;141:199�201.
9.�Laham JL, Cotcamp DH, Gibbons PA, Kahana MD, Crone KR. Isolated head injuries versus multiple trauma in pediatric patients: do the same indications for cervical spine evaluation apply?�Pediatr Neurosurg. 1994;21:221�6.
10.�McKee TR, Tinkoff G, Rhodes M. Asymptomatic occult cervical spine fracture: case report and review of the literature.�J Trauma. 1990;30:623�6.
11.�Woodring JH, Lee C. Limitations of cervical radiography in the evaluation of acute cervical trauma.�J Trauma. 1993;34:32�9.
12.�Spain DA, Trooskin SZ, Flancbaum L, Boyarsky AH, Nosher JL. The adequacy and cost effectiveness of routine resuscitation-area cervical-spine radiographs.�Ann Emerg Med. 1990;19:276�8.
13.�Tintinalli JE, Ruiz E, Krome RL, ed. Emergency medicine: a comprehensive study guide. 4th ed. New York: McGraw-Hill, 1996.
15.�Davis JW, Phreaner DL, Hoyt DB, Mackersie RC. The etiology of missed cervical spine injuries.�J Trauma. 1993;34:342�6.
16.�Apple JS, Kirks DR, Merten DF, Martinez S. Cervical spine fractures and dislocations in children.�Pediatr Radiol. 1987;17:45�9.
17.�Turetsky DB, Vines FS, Clayman DA, Northup HM. Technique and use of supine oblique views in acute cervical spine trauma.�Ann Emerg Med. 1993;22:685�9.
18.�Freemyer B, Knopp R, Piche J, Wales L, Williams J. Comparison of five-view and three-view cervical spine series in the evaluation of patients with cervical trauma.�Ann Emerg Med. 1989;18:818�21.
19.�Lewis LM, Docherty M, Ruoff BE, Fortney JP, Keltner RA Jr, Britton P. Flexion-extension views in the evaluation of cervical-spine injuries.�Ann Emerg Med. 1991;20:117�21.
20.�Mace SE. Emergency evaluation of cervical spine injuries: CT versus plain radiographs.�Ann Emerg Med. 1985;14:973�5.
21.�Kirshenbaum KJ, Nadimpalli SR, Fantus R, Cavallino RP. Unsuspected upper cervical spine fractures associated with significant head trauma: role of CT.�J Emerg Med. 1990;8:183�98.
22.�Woodring JH, Lee C. The role and limitations of computed tomographic scanning in the evaluation of cervical trauma.�J Trauma. 1992;33:698�708.
23.�Schaefer DM, Flanders A, Northrup BE, Doan HT, Osterholm JL. Magnetic resonance imaging of acute cervical spine trauma. Correlation with severity of neurologic injury.�Spine. 1989;14:1090�5.
24.�Levitt MA, Flanders AE. Diagnostic capabilities of magnetic resonance imaging and computed tomography in acute cervical spinal column injury.�Am J Emerg Med. 1991;9:131�5.
25.�Templeton PA, Young JW, Mirvis SE, Buddemeyer EU. The value of retropharyngeal soft tissue measurements in trauma of the adult cervical spine. Cervical spine soft tissue measurements.�Skeletal Radiol. 1987;16:98�104.
26.�DeBehnke DJ, Havel CJ. Utility of prevertebral soft tissue measurements in identifying patients with cervical spine fractures.�Ann Emerg Med. 1994;24:1119�24.
29.�Bracken MB, Shepard MJ, Collins WF Jr, Holford TR, Baskin DS, Eisenberg HM, et al. Methylprednisolone or naloxone treatment after acute spinal cord injury: 1-year follow-up data. Results of the second National Acute Spinal Cord Injury Study.�J Neurosurg. 1992;76:23�31.
30.�Galandiuk S, Raque G, Appel S, Polk HC Jr. The two-edged sword of large-dose steroids for spinal cord trauma.�Ann Surg. 1993;218:419�25.
31.�Grabb PA, Pang D. Magnetic resonance imaging in the evaluation of spinal cord injury without radiographic abnormality in children.�Neurosurgery. 1994;35:406�14.
32.�Pang D, Pollack IF. Spinal cord injury without radiographic abnormality in children�the SCIWORA syndrome.�J Trauma. 1989;29:654�64.
33.�Hadley MN, Zabramski JM, Browner CM, Rekate H, Sonntag VK. Pediatric spinal trauma. Review of 122 cases of spinal cord and vertebral column injuries.�J Neurosurg. 1988;68:18�24.
34.�Kriss VM, Kriss TC. SCIWORA (spinal cord injury without radiographic abnormality) in infants and children.�Clin Pediatr. 1996;35:119�24.
The editors of AFP welcome the submission of manuscripts for the Radiologic Decision-Making series. Send submissions to Jay Siwek, M.D., following the guidelines provided in �Information for Authors.�
Coordinators of this series are Thomas J. Barloon, M.D., associate professor of radiology and George R. Bergus, M.D., assistant professor of family practice, both at the University of Iowa College of Medicine, Iowa City.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine