One of the most difficult medical conditions to spell is also one of the most common. Plantar fasciitis is the most common cause of heel pain. A person is afflicted with this medical condition when the tissue tears in the long ligament that runs along the bottom of the foot, called the plantar fascia ligament. The resulting symptoms include pain and inflammation that can be acute and often ongoing.
Plantar Fasciitis
It’s estimated that 2 million Americans suffer from plantar fasciitis. However, many different factors cause the condition.
A foot trauma from an injury such as a fall can bring about the condition. Other causes are wearing ill-fitting or non-supporting footwear, prolonged standing, and arthritis. Once afflicted with plantar fasciitis, the sufferer often changes their gait to avoid foot pain, bringing on secondary issues such as misalignment and joint stress.
While there are several modes of treatment options, chiropractic care offers multiple unique benefits to those who suffer from plantar fasciitis. Here are four specific ways chiropractic care effectively treats plantar fasciitis.
Chiropractic Adjustments Can Reduce Stress In The Plantar fascia
When the ligament is stressed, it can cause tiny tears that brings on plantar fasciitis. Sufferers who don’t take measures to repair this damage often experience ongoing pain and inflammation. A chiropractor, over a series of visits, is able to adjust the foot and heel so the ligament starts to relax, which in return, promotes healing and diminishes the instances of dealing with the condition again down the road.
Chiropractic Care Helps Minimize Secondary Bodily Injury Due To Compensation
As mentioned above, individuals dealing with the pain of plantar fasciitis frequently adapt their gait to avoid painful steps, causing stress and weight to fall on other parts of the feet, ankles, and joints. This may eventually cause issues with strained muscles and sore joints.
Chiropractic treatment not only deals with the symptoms, but treats the root of the problem. Patients who commit to chiropractic care see the plantar fasciitis decrease in severity. In addition, the chiropractor helps re-train them to walk and stand correctly, taking care of the secondary issues.
Additional At Home Exercises Promote Healing
Patients can help their situations in addition to visiting their chiropractor by taking advantage of regular home therapy exercises. Part of chiropractic care for plantar fasciitis includes a regular recommendation of exercises that stretches and heals the plantar fascia as well as secondary affected areas. For maximum results, patients need to make sure they perform the exercises correctly and diligently stick to the rehabilitation plan.
Chiropractic Works Well In Conjunction With Other Treatments
Chiropractic treatment for plantar fasciitis complements other treatments. Chiropractic visits paired with massage, physical therapy, and more invasive treatment such as injections to offer pain management, increased mobility, and faster healing. Talk with your chiropractor to see what other treatments may complement your current care.
The not so great news is plantar fasciitis’s typical recovery time is several months. The great news is that committing to a combination of chiropractic visits and therapy exercises heals 9 out of 10 cases.
Plantar fasciitis is a common issue that millions of people face, but it doesn’t have to control your activity level or hinder your lifestyle. Consult a chiropractor and work together to lay out a plan of chiropractic adjustments, at-home rehab, and possibly other complementary forms of treatments. It may take time, but plantar fasciitis sufferers can eventually reach a point where they are pain free and their mobility is unhindered!
Why Chiropractic Works:�PUSH-as-Rx ��: 915-203-8122 | Dr. Alex Jimenez � Chiropractor: 915-850-0900
PUSH-as-Rx �� & Chiropractor Dr. Alex Jimenez are leading the field with laser focus supporting our youth sport programs.� The�PUSH-as-Rx ���System is a sport specific athletic program designed by a strength-agility coach and physiology doctor with a combined 40 years of experience working with extreme athletes. At its core, the program is the multidisciplinary study of reactive agility, body mechanics and extreme motion dynamics. Through continuous and detailed assessments of the athletes in motion and while under direct supervised stress loads, a clear quantitative picture of body dynamics emerges. Exposure to the biomechanical vulnerabilities are presented to our team. �Immediately,�we adjust our methods for our athletes in order to optimize performance.� This highly adaptive system with continual�dynamic adjustments has helped many of our athletes come back faster, stronger, and ready post injury while safely minimizing recovery times. Results demonstrate clear improved agility, speed, decreased reaction time with greatly improved postural-torque mechanics.��PUSH-as-Rx ���offers specialized extreme performance enhancements to our athletes no matter the age.
Why Chiropractic Works
We Welcome You ??. Purpose & Passions: I am a Doctor of Chiropractic specializing in progressive cutting-edge therapies and functional rehabilitation procedures focused on clinical physiology, total health, functional strength training and complete conditioning. We focus on restoring normal body functions after neck, back, spinal and soft tissue injuries. We use Specialized Chiropractic Protocols, Wellness Programs, Functional & Integrative Nutrition, Agility & Mobility Fitness Training and Cross-Fit Rehabilitation Systems for all ages. As an extension to dynamic rehabilitation, we too offer our patients, disabled veterans, athletes, young and elder a diverse portfolio of strength equipment, high performance exercises and advanced agility treatment options. We have teamed up with the cities premier doctors, therapist and trainers in order to provide high level competitive athletes the options to push themselves to their highest abilities within our facilities. We’ve been blessed to use our methods with thousand of El Pasoan’s over the last 3 decades allowing us to restore our patients health and fitness while implementing researched non-surgical methods and functional wellness programs. Our programs are natural and use the body’s ability to achieve specific measured goals, rather than introducing harmful chemicals, controversial hormone replacement, un-wanted surgeries, or addictive drugs. We want you to live a functional life that is fulfilled with more energy, positive attitude, better sleep, and less pain. Our goal is to ultimately empower our patients to maintain the healthiest way of living. With a bit of work, we can achieve optimal health together, no matter the age or disability. Join us in improving your health for you and your family. Its all about: LIVING, LOVING & MATTERING! �And this is why chiropractic works!�?
Chiropractic Relieves: How can a body part you have probably never heard of hurt so BAD? This is a common question we hear from individuals suffering from sacroiliac joint pain.
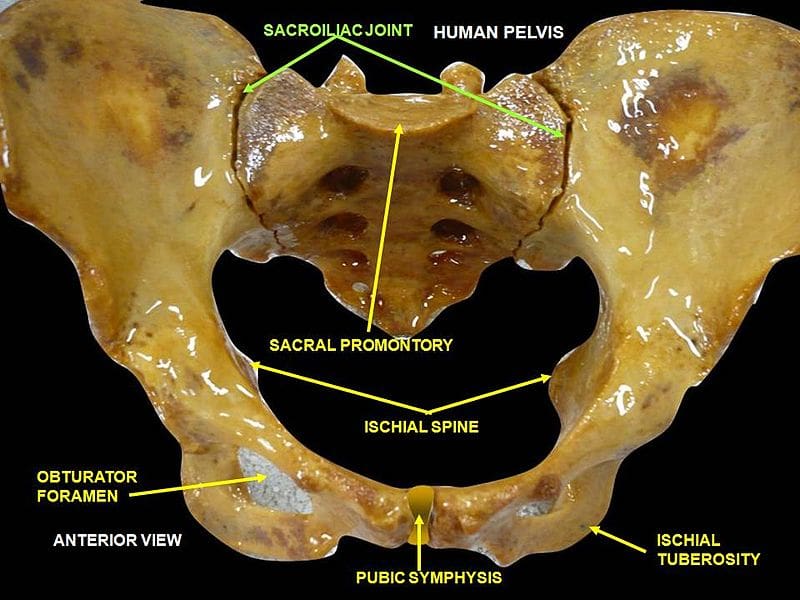
The sacroiliac�joint is formed by the sacrum and the ilium where they meet on either side of the lower back, with the purpose of connecting the spine to the pelvis. This small joint is one of the most durable parts of the human body, and it is responsible for a big job.
The unassuming little sacroiliac joint withstands the pressure of the upper body’s weight pushing down on it, as well as pressure from the pelvis. It’s basically the cushion between the torso and the legs. As such, it handles force from pretty much every angle.
While immensely strong and durable, this joint is not indestructible. Sacroiliac joint pain usually crops up as lower back pain, or pain in the legs or buttocks.
Weakness in these areas may also be present. The typical culprits in causing the sacroiliac joint to exhibit pain are traumatic injuries to the lower back, but more frequently develops over a longer period of time.
Sacroiliac joint pain is often misdiagnosed as soft tissue issues instead of the joint itself. Doctors may rule out other medical conditions before settling on a diagnosis that includes a sacroiliac joint problem.
If you have suffered an injury, a degenerative disease, or otherwise damaged the sacroiliac joint, there are treatments available to help manage pain, promote healing, and lessen the chances of recurrence. Here are a four helpful guidelines to assist in effectively handling sacroiliac joint pain.
Chiropractic Relieves:
First, rest and ice the area. Avoid exaggerated movements of your lower back in order to relieve some of the body’s pressure on the sacroiliac joint. Also apply ice wrapped in a towel periodically to soothe the area and minimize the pain.
A second way to handle sacroiliac pain is with therapeutic massage. Tightness around the joint is a common cause of discomfort and pain. Professional massage serves to loosen and relax the lower back, buttocks, and leg areas, offering relief from pain.
Third, consider chiropractic and seeing a chiropractor. Chiropractic relieves pain, treatment known as adjustments, not only provides great options for pain relief but also helps promote the healing process of this joint.
A chiropractor is specifically trained to guide you through several phases of care. They don�t focus just on pain relief but are primarily interested in helping you fix the problem.
They�re also very well trained in rehabilitation of the spine. This approach will help loosen the muscles surrounding the joint as well as strengthen them. This will decrease the risk of pain returning down the road.
Finally, in very rare cases, doctors will choose to apply an injection to the area to alleviate pain and inflamed tissue. Obviously, the injection won�t fix the problem but may give the patient relief temporarily. Surgery is rarely a viable option.
If you show symptoms of sacroiliac pain, it’s important to see a Doctor of Chiropractic so he or she can perform tests to correctly diagnose your condition. It could very well be another type of lower back problem. Remember chiropractic relieves, so quit suffering and give us a call!
These assessment and treatment recommendations represent a synthesis of information derived from personal clinical experience and from the numerous sources which are cited, or are based on the work of researchers, clinicians and therapists who are named (Basmajian 1974, Cailliet 1962, Dvorak & Dvorak 1984, Fryette 1954, Greenman 1989, 1996, Janda 1983, Lewit 1992, 1999, Mennell 1964, Rolf 1977, Williams 1965).
Clinical Application of Neuromuscular Techniques: Levator Scapulae (As Seen on Fig. 4.36 Below)
Assessment of the Levator Scapulae
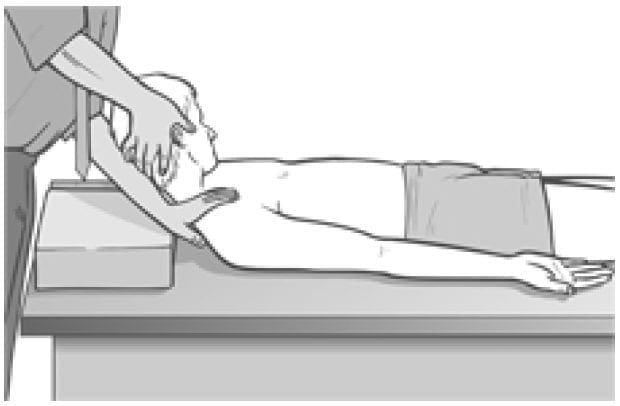
Levator scapula �springing� test (a) The patient lies supine with the arm of the side to be tested stretched out with the supinated hand and lower arm tucked under the buttocks, to help restrain movement of the shoulder/scapula. The practitioner�s contralateral arm is passed across and under the neck to cup the shoulder of the side to be tested, with the forearm supporting the neck. 11 The practitioner�s other hand supports the head. The forearm is used to lift the neck into full pain-free flexion (aided by the other hand). The head is placed fully towards side-flexion and rotation, away from the side being treated.
Figure 4.36 MET test (a) and treatment position for levator scapula (right side).
With the shoulder held caudally and the head/ neck in the position described (each at its resistance barrier) stretch is being placed on levator from both ends.
If dysfunction exists and/or levator scapula is short, there will be discomfort reported at the attachment on the upper medial border of the scapula and/or pain reported near the levator attachment on the spinous process of C2.
The hand on the shoulder gently �springs� it caudally.
If levator is short there will be a harsh, wooden feel to this action. If it is normal there will be a soft feel to the springing pressure.
Levator scapula observation test (b) A functional assessment involves applying the evidence we have seen (see Ch. 2) of the imbalances which commonly occur between the upper and lower stabilisers of the scapula. In this process shortness is noted in pectoralis minor, levator scapulae and upper trapezius (as well as SCM), while weakness develops in serratus anterior, rhomboids, middle and lower trapezius � as well as the deep neck flexors.
Observation of the patient from behind will often show a �hollow� area between the shoulder blades, where interscapular weakness has occurred, as well as an increased (over normal) distance between the medial borders of the scapulae and the thoracic spine, as the scapulae will have �winged� away from it.
Levator scapula test (c) To see the imbalance described in test (b) in action, Janda (1996) has the patient in the press-up position (see Fig. 5.15). On very slow lowering of the chest towards the floor from a maximum push-up position, the scapula(e) on the side(s) where stabilisation has been compromised will move outwards, laterally and upwards � often into a winged position � rather than towards the spine.
This is diagnostic of weak lower stabilisers, which implicates tight upper stabilisers, including levator scapulae, as inhibiting them.
MET Treatment of Levator Scapula (Fig. 4.36)
Treatment of levator scapulae using MET enhances the lengthening of the extensor muscles attaching to the occiput and upper cervical spine. The position described below is used for treatment, either at the limit of easily reached range of motion, or a little short of this, depending upon the degree of acuteness or chronicity of the dysfunction.
The patient lies supine with the arm of the side to be tested stretched out alongside the trunk with the hand supinated. The practitioner, standing at the head of the table, passes his contralateral arm under the neck to rest on the patient�s shoulder on the side to be treated, so that the practitioner�s forearm supports the patient�s neck. The practitioner�s other hand supports and directs the head into subsequent movement (below).
The practitioner�s forearm lifts the neck into full flexion (aided by the other hand). The head is turned fully into side-flexion and rotation away from the side being treated.
With the shoulder held caudally by the practitioner�s hand, and the head/neck in full flexion, sideflexion and rotation (each at its resistance barrier), stretch is being placed on levator from both ends.
The patient is asked to take the head backwards towards the table, and slightly to the side from which it was turned, against the practitioner�s unmoving resistance, while at the same time a slight (20% of available strength) shoulder shrug is also asked for and resisted.
Following the 7�10 second isometric contraction and complete relaxation of all elements of this combined contraction, the neck is taken to further flexion, sidebending and rotation, where it is maintained as the shoulder is depressed caudally with the patient�s assistance (�as you breathe out, slide your hand towards your feet�). The stretch is held for 20�30 seconds.
The process is repeated at least once.
CAUTION: Avoid overstretching this sensitive area.
Facilitation of Tone in Lower Shoulder Fixators Using Pulsed MET (Ruddy 1962)
In order to commence rehabilitation and proprioceptive re-education of a weak serratus anterior:
The practitioner places a single digit contact very lightly against the lower medial scapula border, on the side of the treated upper trapezius of the seated or standing patient. The patient is asked to attempt to ease the scapula, at the point of digital contact, towards the spine (�press against my finger with your shoulder blade, towards your spine, just as hard [i.e. very lightly] as I am pressing against your shoulder blade, for less than a second�).
Once the patient has learned to establish control over the particular muscular action required to achieve this subtle movement (which can take a significant number of attempts), and can do so for 1 second at a time, repetitively, they are ready to begin the sequence based on Ruddy�s methodology (see Ch. 10, p. 75).
The patient is told something such as �now that you know how to activate the muscles which push your shoulder blade lightly against my finger, I want you to try do this 20 times in 10 seconds, starting and stopping, so that no actual movement takes place, just a contraction and a stopping, repetitively�.
This repetitive contraction will activate the rhomboids, middle and lower trapezii and serratus anterior � all of which are probably inhibited if upper trapezius is hypertonic. The repetitive contractions also produce an automatic reciprocal inhibition of upper trapezius, and levator scapula.
The patient can be taught to place a light finger or thumb contact against their own medial scapula (opposite arm behind back) so that home application of this method can be performed several times daily.
Treatment for Eye Muscles (Ruddy 1962)
Ruddy�s treatment method for the muscles of the eye is outlined in the notes below.
Ruddy�s Treatment for the Muscles of the Eye (Ruddy 1962)
Osteopathic eye specialist Dr T. Ruddy described a practical treatment method for application of MET principles to the muscles of the eye:
The pads of the practitioner�s index, middle and ring finger and the thumb are placed together to form four contacts into which the eyeball (eye closed) can rest (middle finger is above the cornea and the thumb pad below it).
These contacts resist the attempts the patient is asked to make to move the eyes downwards, laterally, medially and upwards � as well as obliquely between these compass points � up and half medial, down and half medial, up and half lateral, down and half lateral, etc.
The fingers resist and obstruct the intended path of eye motion.
Each movement should last for a count �one� and then rest between efforts for a similar count, and in each position there should be 10 repetitions before moving on around the circuit. Ruddy maintained the method released muscle tension, permitted better circulation, and enhanced drainage. He applied the method as part of treatment of many eye problems.
Dr. Alex Jimenez offers an additional assessment and treatment of the hip flexors as a part of a referenced clinical application of neuromuscular techniques by Leon Chaitow and Judith Walker DeLany. The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
By Dr. Alex Jimenez
Additional Topics: Wellness
Overall health and wellness are essential towards maintaining the proper mental and physical balance in the body. From eating a balanced nutrition as well as exercising and participating in physical activities, to sleeping a healthy amount of time on a regular basis, following the best health and wellness tips can ultimately help maintain overall well-being. Eating plenty of fruits and vegetables can go a long way towards helping people become healthy.
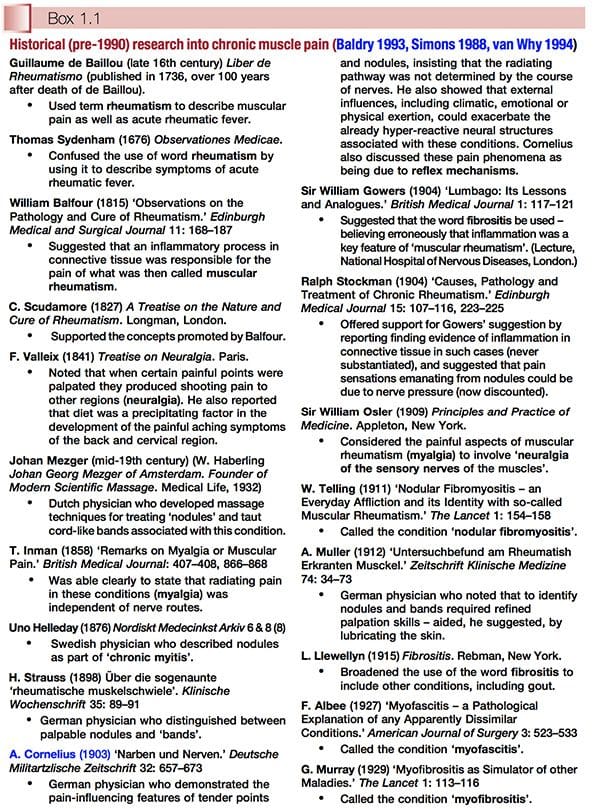
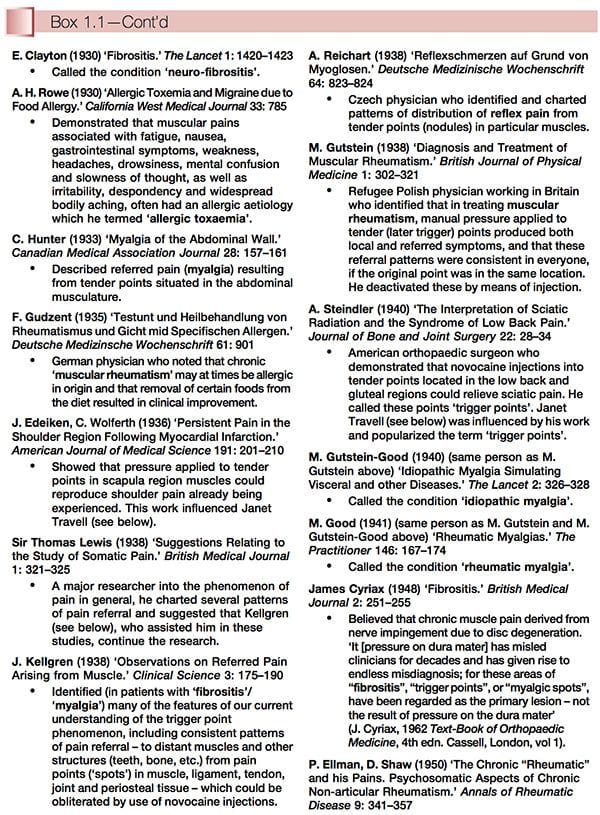
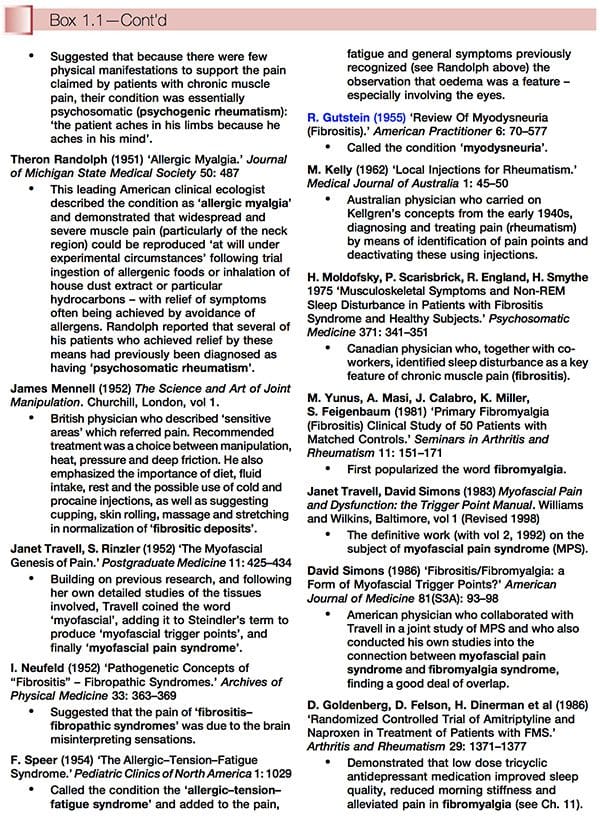
Fibromyalgia History: Historically, fibromyalgia � or conditions very like it � have been reported for hundreds of years, under many names, including the most unsatisfactory term �fibrositis�. The fascinating history of what we now call fibromyalgia syndrome (FMS) and myofascial pain syndrome (MPS) has been catalogued by several modern clinicians working in the sphere of chronic muscle pain, from whose work the material summarized in Box 1.1 has been compiled. Thanks are due to these individuals (Peter Baldry, David Simons and Richard van Why in particular) for revealing so much about past studies into the phenomenon of chronic muscle pain. What we can learn from this information is just how long ago (well over 150 years) particular features were recognized, for example pain referral patterns and characteristics such as taut bands and �nodules�, as well as insights from many astute researchers and clinicians into the pathophysiology of these conditions.
American College Of Rheumatology Definition
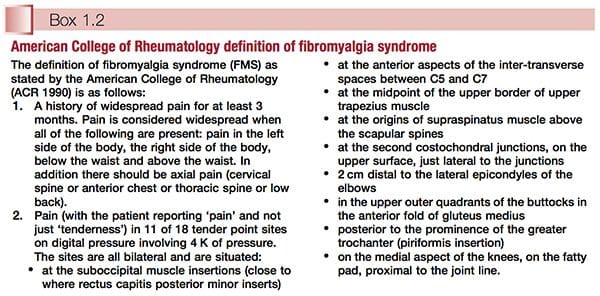
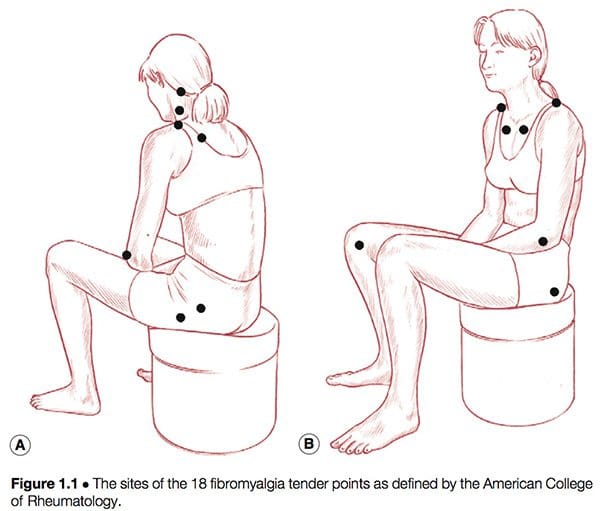
Simply defined, fibromyalgia syndrome (FMS) can be said to be a debilitating illness, characterized primarily by musculoskeletal pain, fatigue, sleep disturbances, depression and stiffness (Yunus & Inanici 2002). It was not until the 1980s that a redefining took place of what was by then a confused � and confusing � picture of a common condition. In 1987, the American Medical Association recognized fibromyalgia as a distinct syndrome (Starlanyl & Copeland 1996), although at that time detailed knowledge of what the syndrome comprised was not as clear as the current, generally accepted American College of Rheumatology (ACR) definition, which was produced in 1990 (see Box 1.2 and Fig. 1.1). Russell (in Mense & Simons 2001) notes that defining the condition had profound effects on the scientific and medical communities:
In the wake of successful classification criteria, a surge of investigative energy in the early 1990s led to a number of important new observations. FMS was found to be universally common. It was present in approximately 2% of the adult population of the USA and exhibited a similar distribution in most other countries where valid epidemiological studies had been conducted. Adult women were affected five to seven times more commonly than were men. In children the gender distribution was about equal for boys or girls.
When psychosocial and physical/functional factors of people with FMS were compared with those six different, predominantly chronic pain syndromes (upper extremity pain, cervical pain, thoracic pain, lumbar pain, lower extremity pain and headache), it was found that the fibromyalgia group experienced the most difficulties, by a significant margin. In regard to gender distribution of these seven chronic pain conditions, it was noted that fibromyalgia (and headache) are experienced by more females than males (Porter-Mofitt et al 2006).
What can be said with certainty about fibromyalgia syndrome is that:
� It is a non-deforming rheumatic condition, and, indeed, one of the commonest such conditions.
� It is an ancient condition, newly defined (controversially � see below) as a disease complex or syndrome.
� There is no single cause, or cure, for its widespread and persistent symptoms (however, as will become clear, there do seem to exist distinct subsets of individuals with different aetiologies to their conditions, such as thyroid imbalance and whiplash injuries).
� Its complex causation often seems to require more than one essential aetiological factor to be operating, and there are numerous theories as to what these might be (see Ch. 4).
� There has been an explosion of research into the subject over the past decade (one data search on the internet revealed over 20 000 papers which mention fibromyalgia as a key word).
Despite its earlier medical meaning, which suggested involvement of both articular and non-articular structures, the word rheumatic has, through common usage, come to mean �a painful but nondeforming soft tissue musculoskeletal condition�, as distinct from the word arthritic which suggests articular and/or deforming features (Block 1993).
The Fibromyalgia Controversy
For the purposes of practicality this book accepts that the current widely used ACR definition is a hypothesis that is evolving, but that it may be flawed (see below). The definition as presented in Box 1.2 allows for the categorization of individuals with chronic pain and associated symptoms into subgroups, and offers clinicians a chance to begin to decipher the confusing patterns of symptoms displayed and reported by people who have been so labelled. However, not all experts, including many of the contributors to this text, accept the ACR definition. Nevertheless, since it forms the foundation for much of the research reported on in the book, the current definition needs to be given due consideration.
What Are The Arguments Against The ACR Definition?
Schneider et al (2006) sum up one major alternative view:
Recent data tend to support the notion that FMS is a disorder of the central nervous system pain processing pathways, and not some type of primary auto-immune disorder of the peripheral tissues. It is quite possible that the term FMS is a poor choice of words, for it implies that patients with a variable symptom complex all have the same singular disease or disorder.
As will be clear in subsequent chapters, this is precisely the message that this book will promote � that there are numerous aetiological influences relating to the symptom cluster represented by people with a diagnosis of FMS, and that within that population subgroups can be identified that demand quite distinctive therapeutic handling, compared with other subgroup cohorts. A logical extension of this multicausal scenario is a model that offers a variety of potential therapeutic interventions, none of which would have universal applicability, and most of which would be most usefully employed in treatment of specific subgroups within the overall diagnosis of FMS. The chapters in this book that reflect a variety of therapeutic approaches include those that evaluate and explain the use of acupuncture, endocrine issues, psychological influences, myofascial trigger points/ dry needling, use of microcurrent, hydrotherapy, therapeutic touch, manipulation, massage, exercise, nutrition and various other clinical methods. The issues surrounding FMS subsets, and of possible over(or mis-)diagnosis of FMS, are explored more fully in Chapters 3, 4 and 5.
Problems Arising From The ACR Definition
Useful as the defining of this condition has been, there are distinct and obvious problems with a definition as precise as that offered by the ACR:
� If pressure varies only slightly, so that on a �good day� a patient may report sensitivity and tenderness rather than �pain� when tender points are being tested, the patient may therefore not �qualify�; this could have very real insurance benefit implications, as well as leaving distressed individuals still seeking a diagnosis which might help them understand their suffering.
� If all other criteria are present, and fewer than 11 of the 18 possible sites are reported as �painful� (say only 9 or 10), what diagnosis is appropriate?
� If there are 11 painful sites but the �widespread� nature of the pain is missing (as per the definition in Box 1.2), what diagnosis is appropriate? Clearly, what is being observed in people with widespread pain and who also demonstrate at least 11 of the 18 test points as being painful is a situation which represents the distant end of a spectrum of dysfunction. Others who do not quite meet the required (for a diagnosis of FMS) number of tender points may well be progressing towards that unhappy state.
As reported earlier, approximately 2% of the population meet all the ACR criteria (Wolfe et al 1993). A great many more people, however, are advancing in that direction, according to both British and American research, which shows that about 20% of the population suffer �widespread� pain that matches the ACR definition, with almost the same number, but not necessarily the same people, demonstrating 11 of the specified 18 tender points as being painful on appropriate testing, also in accordance with the ACR definition. Some people have the widespread pain and not enough painful points, while others have the points but their generalized pain distribution is not sufficiently widespread.
What Condition Do They Have If It Is Not FMS (Croft et al 1992)?
If all the criteria are not fully met, and people with, say, 9 or 10 points (rather than the 11 needed) are offered a diagnosis of FMS (and therefore become eligible for insurance reimbursement or disability benefits, or suitable for inclusion in research projects), what of the person with only 8 painful points who meets all the other criteria?
In human terms this is all far from an academic exercise, for pain of this degree is distressing and possibly disabling, whether or not 11 (or more) points are painful. Clinically, such patients should receive the same attention, wherever they happen to be in the spectrum of disability, and whatever the tender point score, if their pain is sufficient to require professional attention.
As will become clear as examination of FMS unfolds in this and subsequent chapters, the frustration of the patient is matched in large degree by that of health care providers attempting to understand and offer treatment for the patient with FMS. This is largely because no single aetiological pattern has emerged from research efforts to date. Russell (in Mense & Simons 2001) sums it up as follows:
The cause of FMS is unknown, but growing evidence indicates that its pathogenesis involves aberrant neurochemical processing of sensory�signals in the CNS. The symptomatic result is lowering of the pain thresholds and an amplification of normal sensory signals until the patient experiences near constant pain.
As will also become clear, the components of the pathogenesis of the condition commonly include biochemical, psychological and biomechanical features. Somewhere in the combination of causal elements and unique characteristics of the individual may lie opportunities for functional improvement and the easing of the often intractable pain and other symptoms associated with FMS.
Symptoms Other Than Pain
In 1992, at the Second World Congress on Myofascial Pain and Fibromyalgia in Copenhagen, a consensus document on fibromyalgia was produced and later published in The Lancet (Copenhagen Declaration 1992). This declaration accepted the ACR fibromyalgia definition as the basis for a diagnosis, and added a number of symptoms to that definition (apart from widespread pain and multiple tender points), including persistent fatigue, generalized morning stiffness and non-refreshing sleep.
The Copenhagen document recognized that people with FMS may indeed at times present with fewer than 11 painful points � which is clearly important if most of the other criteria for the diagnosis are met. In such a case, a diagnosis of �possible FMS� is thought appropriate, with a follow-up examination suggested to reassess the condition.
There are practical implications for a cut-off point (of symptoms or tender point numbers, for example) in making such a diagnosis: these relate directly to insurance reimbursement and/or disability benefits, as well as, possibly, to differential diagnosis.
The Copenhagen document adds that FMS is seen to be a part of a larger complex which includes symptoms such as headache, irritable bladder, dysmenorrhoea, extreme sensitivity to cold, restless legs, odd patterns of numbness and tingling, intolerance to exercise, and other symptoms.
Mind Issues
The Copenhagen Declaration (1992) of the symptoms associated with FMS (over and above pain, which is clearly the defining feature) also addresses the psychological patterns often related to FMS, namely anxiety and/or depression.
The possible psychological component in FMS is an area of study fraught with entrenched beliefs and defensive responses. A large body of medical opinion assigns the entire FMS phenomenon � as well as chronic fatigue syndrome (CFS) � to the arena of psychosomatic/psychosocial illness. An equally well-defined position, occupied by many health care professionals as well as most patients, holds that anxiety and depression symptoms are more commonly a result, rather than a cause, of the pain and disability being experienced in FMS (McIntyre 1993a).
A 1994 review paper analysed all British medical publications on the topic of CFS from 1980 onwards and found that 49% favoured a non-organic cause while only 31% favoured an organic cause. When the popular press was examined in the same way, between 70% (newspapers) and 80% (women�s magazines) favoured an organic explanation (McClean & Wesseley 1994).
Typical of the perspective which holds to a largely �psychological� aetiology is a multicentre study by Epstein and colleagues, which was published in 1999. It concluded: �In this multicenter study, the persons with FMS exhibited marked functional impairment, high levels of some lifetime and current psychiatric disorders, and significant current psychological distress.� The most common disorders noted were major depression, dysthymia, panic disorder and simple phobia.
Many leading researchers into FMS who hold to an organic � biochemical � neurological explanation for the main symptoms are, however, dismissive of psychological explanations for the condition. Dr Jay Goldstein, whose detailed and important research and clinical insights into the care of patients with CFS and FMS will be outlined later in this book, uses the term �neurosomatic� to describe what he sees as a disorder of central information processing. He makes clear his position regarding the non-organic, psychosocial school of thought (Goldstein 1996):
Many of the illnesses [CFS, FMS] treated using this model [neurosomatic] are still termed �psychosomatic� by the medical community and are treated psychodynamically by psychiatrists, neurologists and general physicians. Social anthropologists also have their theories describing CFS as the �neurasthenia� of the 1990s, and a �culture bound syndrome� that�displaces the repressed conflicts of patients unable to express their emotions (�alexithymics�) into a culturally acceptable viral illness or immune dysfunction. Cognitive�behavioural therapy is perhaps more appropriate, since coping with the vicissitudes of their illnesses, which wax and wane unpredictably, is a major problem for most of those afflicted. Few investigators in psychosomatic illness (except those researching panic disorders) have concerned themselves about the pathophysiology of the patients they study, seeming content to define this population in psychosocial phenomenological terms. This position becomes increasingly untenable as the mind�body duality disappears.
Goldstein says that he only refers patients for psychotherapy if they are suicidally depressed. He emphasizes the normalization (using a variety of medications) of the biochemical basis for neural network dysfunction, which he has satisfied himself is the underlying cause of these (and many other) conditions.
When Is A Cause Not A Cause?
Goldstein�s methods will be examined in later chapters; however, it might prove useful at this stage to make a slight diversion in order to clarify the importance of looking beyond apparent causes to attempt to uncover their origins.
As we progress through the saga which is FMS (and CFS) we will come across a number of welldefined positions which maintain that the dominant cause is X or Y � or more usually a combination of X and Y (and possibly others). The truth is that in some important instances these �causes� themselves have underlying causes, which might usefully be therapeutically addressed.
An example � which will emerge in more detail later � is the suggestion that many of the problems associated with FMS (and CFS) are allergy related (Tuncer 1997). This may well be so in the sense that particular foods or substances can be shown, in given cases, to provoke or exacerbate symptoms of pain and fatigue. But what produces this increased reactivity/sensitivity? Are there identifiable causes of the (usually food) intolerances (Ventura et al 2006)?
In some cases this can be shown to result from malabsorption of large molecules through the intestinal wall, possibly due to damage to the mucosal surfaces of the gut (Tagesson 1983, Zar 2005). In some cases the mucosal damage itself can be shown to have resulted from abnormal yeast or bacterial overgrowth, resulting from prior (possibly inappropriate) use of antibiotics and consequent disturbance of the normal flora, and their control over opportunistic organisms (Crissinger 1990). Or the disturbed gut mucosa may be associated with endotoxaemia involving disturbed beneficial bacteria status (McNaught et al 2005).
The layers of the onion can be peeled away one by one, revealing causes which lie ever further from the obvious. The pain is aggravated by allergy, which results from bowel mucosa damage, which results from yeast overgrowth, which results from excessive or inappropriate use of antibiotics… and so on. The allergy in this example is not a cause per se but an exacerbating factor, a link in a chain, and while treating it might satisfactorily reduce symptoms, it would not necessarily deal with causes. Neither would treating the bacterial or yeast overgrowth, although this too might well assist in reducing overall symptom distress.
Where does the cause lie in this particular individual�s FMS? Probably in a complex array of interlocking (often historical) features, which may be impossible to untangle. Therefore, approaches such as those which direct themselves at the allergy or at the increased permeability, while possibly (in this instance) valid and helpful, are not necessarily dealing with fundamental causes.
Does this matter? In Goldstein�s model of FMS and CFS aetiology we are faced with a neural network which is dysfunctional. He acknowledges that the evolution of such a state requires several interacting elements:
� a basic susceptibility which is probably genetically induced
� some developmental factors in childhood (physical, chemical or psychological abuse/ trauma, for example)
� probably a degree of viral encephalopathy (influenced by �situational perturbations of the immune response�)
� increased susceptibility to environmental stressors resulting from reduction in neural plasticity.
The possibility that early developmental trauma or abuse is a feature is supported by research. For example, Weissbecker et al (2006) report that:
Adults with fibromyalgia syndrome report high rates of childhood trauma. Neuroendocrine abnormalities have also been noted in this population. Findings suggest that severe traumatic experiences in childhood may be a factor of adult neuroendocrine dysregulation among fibromyalgia sufferers. Trauma history should be evaluated and psychosocial intervention may be indicated as a component of treatment for fibromyalgia.
The �causes� within this model can be seen to be widely spread. Goldstein�s (apparently successful) interventions deal with what is happening at the end of this complex sweep of events when the neural network has, as a result, become dysfunctional. By manipulating the biochemistry of that end-state, many (Goldstein says most) of his patients� symptoms apparently improve dramatically and rapidly.
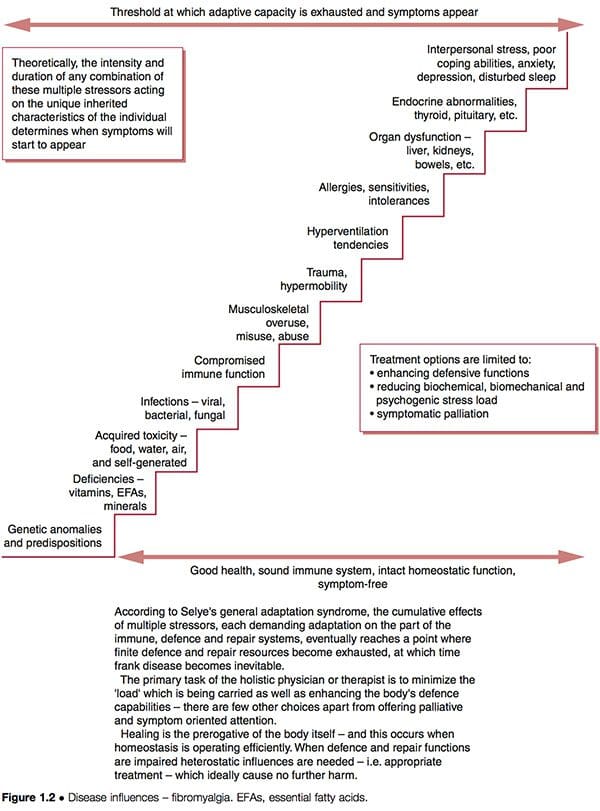
Such improvement does not necessarily indicate that underlying causes have been addressed; if these are still operating, future health problems may be expected to eventually emerge. The schematic representation of a �stairway to ill-health� (Fig. 1.2) indicates some of the possible features ongoing in complicated dysfunctional patterns such as FMS, where adaptive resources have been stretched to their limits, and the �stage of exhaustion� in Selye�s general adaptation syndrome has been reached (Selye 1952). See also the discussion of allostasis in Chapter 3, particularly Table 3.2.
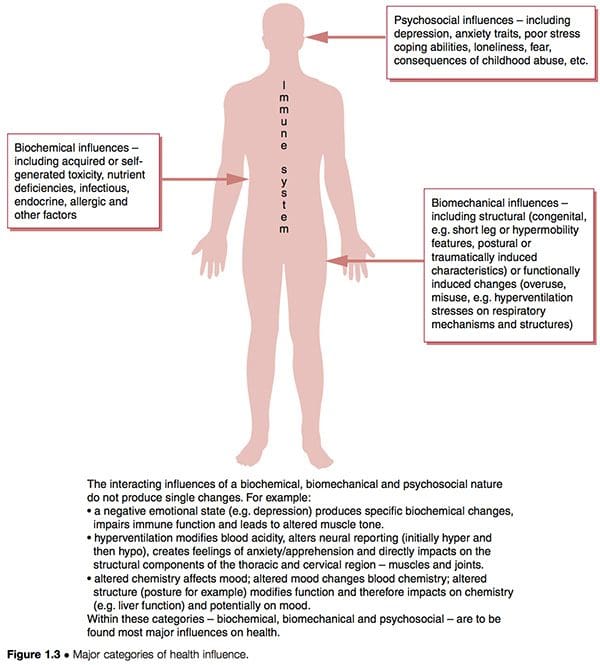
Dysfunctional patterns such as CFS and FMS seem to have three overlapping aetiological features interacting with the unique inborn and subsequently acquired characteristics of individuals to determine their particular degree of vulnerability and susceptibility (Fig. 1.3):
1. Biochemical factors. These can include toxicity, deficiency, infectious, endocrine, allergic and other characteristics (Wood 2006).
2. Biomechanical factors. These might include:
a. structural (congenital � i.e. short leg or hypermobility features � postural or traumatically induced characteristics) (Gedalia et al 1993, Goldman 1991)
b. functional (overuse patterns, hyperventilation stresses on respiratory mechanisms, etc.)
c. neurological (sensitization, hypersensitivity � �wind-up�) (Staud et al 2005).
3. Psychosocial factors. These might include depression and/or anxiety traits, poor stress coping abilities, post-traumatic stress disorders, etc. (Arguellesa et al 2006).
Let us briefly consider Dr Goldstein�s model of dysfunction, which suggests neural network dysfunction as the �cause� of FMS, itself being a result of a combination of features as outlined above (Goldstein 1996). If we utilize the clinical options suggested in Figure 1.2, we can see that it is possible to attempt to:
1. reduce the biochemical, biomechanical or psychogenic �stress� burden to which the person is responding
2. enhance the defense, repair, immune functions of the person so that they can handle these stressors more effectively
3. palliate the symptoms, hopefully without producing any increase in adaptive demands on an already overloaded system.
Which of these tactics are being employed in Goldstein�s treatment approach in which drug-induced biochemical manipulation is being carried out, and does this address causes or symptoms, and does this matter, as long as there is overall improvement?
The particular philosophical perspective adopted by the practitioner/therapist will determine his judgement on this question. Some may see the rapid symptom relief claimed for the majority of these patients as justifying Goldstein�s particular therapeutic approach. Others might see this as offering short term benefits, not addressing underlying causes, and leaving the likelihood of a return of the original symptoms, or of others evolving, a probability. These issues will be explored in relation to this and other approaches to treatment of FMS in later chapters.
Associated Conditions
A number of other complex conditions exist which have symptom patterns which mimic many of those observed in FMS, in particular:
� chronic myofascial pain syndrome (MPS) involving multiple active myofascial trigger points and their painful repercussions
� chronic fatigue syndrome (CFS) which has among its assortment of symptoms almost all those ascribed to FMS, with greater emphasis on the fatigue elements, rather than the pain ones
� multiple chemical sensitivity (MCS)
� post-traumatic stress disorder (PTSD). MPS, FMS, MCS (for example, in relation to what has become known as Gulf War syndrome) and CFS � their similarities, and the sometimes great degree of overlap in their symptom presentation, as well as their differences � will be examined in later chapters. One feature of all of these conditions which has been highlighted is based on a toxic/biochemical hypothesis, involving �elevated levels of nitric oxide and its potent oxidant product, peroxynitrite� (Pall 2001).
Other Theories Of Causation
A variety of theories as to the causation of FMS have emerged, with many of these overlapping and some being essentially the same as others, with only slight differences in emphasis as to aetiology, cause and effect. FMS is variously thought to involve any of a combination of the following (as well as other) causative features, each of which raises questions as well as suggesting answers and therapeutic possibilities:
� FMS could be a neuroendocrine disturbance, particularly involving thyroid hormone imbalances (see Ch. 10) (Garrison & Breeding 2003, Honeyman 1997, Lowe 1997, Lowe & Honeyman-Lowe 2006) and/or hypophyseal growth hormone imbalances (possibly as a direct result of sleep disturbance � a key feature of FMS, and/or lack of physical exercise) (Moldofsky 1993). The question which then needs to be asked is, what produces the endocrine disturbance? Is it genetically determined as some believe, or is it the result of deficiency, toxicity, allergy, an autoimmune condition or infection?
� Duna & Wilke (1993) propose that disordered sleep leads to reduced serotonin production, and consequent reduction in the pain-modulating effects of endorphins and increased �substance P� levels, combined with sympathetic nervous system changes resulting in muscle ischaemia and increased sensitivity to pain (Duna & Wilke 1993). This hypothesis starts with a symptom, sleep disturbance, and the logical question is, what produces this?
� Dysautonomia, autonomic imbalance or dysfunction, characterized by �relentless sympathetic hyperactivity�, more prominent at night (Martinez-Lavin & Hermosillo 2005), have been proposed as foundational causes in a subgroup of individuals with FMS (and CFS). Many such patients have also been labelled with Gulf War-related illness (Geisser et al 2006, Haley et al 2004, van der Borne 2004).
� Muscle microtrauma may be the cause, possibly due to genetic predisposition (and/or growth hormone dysfunction), leading to calcium leakage, and so increasing muscle contraction and reducing oxygen supply. An associated decrease in mitochondrial energy production would lead to local fatigue and an inability for excess calcium to be pumped out of the cells, resulting in local hypertonia and pain (Wolfe et al 1992). The question as to why muscle microtrauma occurs more in some people than in others, or why repair is slower, requires investigation.
� FMS may be a pain modulation disorder resulting at least in part from brain (limbic system) dysfunction and involving mistranslation of sensory signals and consequent misreporting (Goldstein 1996). Why and how the limbic system and neural networks become dysfunctional is the key to this hypothesis (promoted by Goldstein, as discussed above).
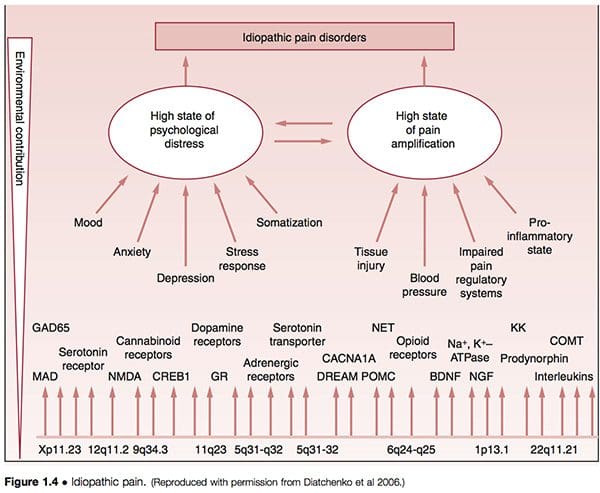
� It has been suggested that what are termed idiopathic pain disorders (IPD) � such as temporomandibular joint disorders (TMJD), fibromyalgia syndrome (FMS), irritable bowel syndrome (IBS), chronic headaches, interstitial cystitis, chronic pelvic pain, chronic tinnitus, whiplash-associated disorders and vulvar vestibulitis (VVS) � are mediated by an individual�s genetic variability, as well as by exposure to environmental events. The primary pathways of vulnerability that underlie the development of such conditions are seen to involve pain amplification and psychological distress, modified by gender and ethnicity (Diatchenko et al 2006) (Fig. 1.4).
� FMS may be a congenitally acquired disorder, possibly related to inadequate thyroid regulation of gene transcription, with an autosomal dominant feature (Lowe et al 1997, Pellegrino et al 1989). As will be outlined, some research studies have found evidence of a genetically linked predisposition towards FMS. Congenital structural abnormalities, such as extreme ligamentous laxity (i.e. hypermobility (Karaaslan et al 2000)), and Chiari malformations (see further discussion of this in Ch. 3 (Kesler & Mandizabal 1999, Thimineur et al 2002)), certainly seem to predispose toward FMS. The questions this raises include: which factors exacerbate these predispositions, and can anything be done about them?
� Hudson et al (2004) have proposed that fibromyalgia is one member of a group of 14 psychiatric and medical disorders (attentiondeficit/hyperactivity disorder, bulimia nervosa, dysthymic disorder, generalized anxiety disorder, major depressive disorder, obsessive-compulsive disorder, panic disorder, post-traumatic stress�disorder, premenstrual dysphoric disorder and social phobia � plus four medical conditions: fibromyalgia, irritable bowel syndrome, migraine, and cataplexy), collectively termed affective spectrum disorder (ASD), hypothesized to share possibly heritable pathophysiological features. Following detailed analysis of data from 800 individuals with and without fibromyalgia (and the additional conditions under assessment), Hudson et al concluded that the present information added to evidence that the psychiatric and medical disorders, grouped under the term ASD, run together in families, raising the possibility that these disorders might share a heritable physiological abnormality.
� The underlying cause of FMS is seen by some to result from the (often combined) involvement of allergy, infection, toxicity and nutritional deficiency factors which themselves produce the major symptoms of FMS (and CFS), such as fatigue and pain, or which are associated with endocrine imbalances and the various consequences outlined above, such as thyroid hormone dysfunction and/or sleep disturbance (Abraham & Lubran 1981, Bland 1995, Cleveland et al 1992, Fibromyalgia Network Newsletters 1990�94, Pall 2001, Robinson 1981, Vorberg 1985). The list of possible interacting features such as these, which frequently seem to coexist in someone with FMS, offers the possibility of intervention strategies which seem to focus on causes rather than effects. For example, specific �excitotoxins� such as monosodium glutamate (MSG) have been identified as triggering FMS symptoms (Smith et al 2001). These and other examples will be examined in later chapters.
� A central sensitization hypothesis suggests that central mechanisms of FMS pain are dependent on abnormal peripheral input(s) for development�and maintenance of the condition (Vierck 2006). A substantial literature defines peripheral�CNS� peripheral interactions that seem integral to fibromyalgia pain. The generalized hypersensitivity associated with the condition has focused interest on central (CNS) mechanisms for the disorder. These include central sensitization, central disinhibition and a dysfunctional hypothalamic�pituitary�adrenal (HPA) axis. However, it is asserted that the central effects associated with fibromyalgia can be produced by peripheral sources of pain. In this model, chronic nociceptive input induces central sensitization, magnifying pain and activating the HPA axis and the sympathetic nervous system. Chronic sympathetic activation then indirectly sensitizes peripheral nociceptors, and sets up a vicious cycle. (See also notes on facilitation later in this chapter, as well as further discussion of central and peripheral sensitization in Ch. 4.)
� Use of MRI and other scanning/imaging technology suggests that the central sensitization concept has objective evidence to support it. This subject is discussed further in Chapter 3 (see �The polysymptomatic patient�) and Chapter 4 (see �Central sensitization hypothesis� and Fig. 3.1). Two examples of imaging evidence, relating to altered brain morphology and/or behaviour in relation to FMS, are summarized in Box 1.3.
� Within the framework of �allergy� and �intolerance� as triggers to FMS symptoms lies a hypothesis which remains controversial, but worthy of discussion. This relates to the concept of blood-type specific intolerances resulting from an interaction between food-derived lectins (protein molecules) and specific tissue markers related to the individual�s blood type. D�Adamo (2002), who has done most to promote this concept, states (in relation to FMS sufferers who happen to be type O):
It has become obvious that those who are type O and suffering from fibromyalgia can see quite dramatic responses if they can stick to the wheat-free component of the diet for a long enough duration. A recent study indicates that dietary lectins interacting with enterocytes (cells lining�the intestines) and lymphocytes may facilitate the transportation of both dietary and gutderived pathogenic antigens to peripheral tissues, which in turn causes persistent immune stimulation at the periphery of the body, such as the joints and muscles (Cordain et al 2000). This, despite the fact that many nutrition �authorities� still question whether lectins even get into the systemic circulation! In genetically susceptible individuals, this lectin stimulation may ultimately result in the expression of disorders like rheumatoid arthritis and fibromyalgia via molecular mimicry, a process whereby foreign peptides, similar in structure to endogenous peptides, may cause antibodies or T-lymphocytes to cross-react and thereby break immunological tolerance. Thus by removing the general and type O specific lectins from the diet, we allow for the immune system to redevelop tolerance, the inflammation begins to ebb, and healing can begin.
� Many FMS patients demonstrate low carbon dioxide levels when resting � an indication of possible hyperventilation involvement. The symptoms of hyperventilation closely mirror those of FMS and CFS, and the pattern of upper chest breathing which it involves severely stresses the muscles of the upper body which are most affected in FMS, as well as producing major oxygen deficits in the brain and so influencing its processing of information such as messages received from pain receptors (Chaitow et al 2002, Janda 1988, King 1988, Lum 1981). When hyperventilation tendencies are present, they can be seen in some instances to be a response to elevated acid levels (because of organ dysfunction perhaps) or they can be the result of pure habit. Breathing retraining can, in some FMS patients, offer a means of modifying symptoms rapidly (Readhead 1984).
� Psychogenic (or psychosomatic) rheumatism is the name ascribed to FMS (and other nonspecific chronic muscle pain problems) by those who are reluctant to see an organic origin for the syndrome. Until the 1960s it was suggested that such conditions be treated as �psychoneurosis� (Warner 1964). In FMS, as in all chronic forms of ill-health, there are undoubtedly elements of emotional involvement, whether as a cause or as an effect. These impact directly on pain perception and immune function, and, whether causative or not, benefit from appropriate attention, assisting both in recovery and rehabilitation (Melzack & Wall 1988, Solomon 1981).
� FMS is seen by some to be an extreme of the myofascial pain syndrome (MPS), where numerous active myofascial triggers produce pain both locally and at a distance (Thompson 1990). Others see FMS and MPS as distinctive, but recognize that �it is not uncommon for a patient with myofascial pain syndrome to progress with time to a clinical picture identical to that of FMS� (Bennett 1986a). Among the most important practical pain-relieving approaches to FMS will be the need to identify and deactivate myofascial trigger points which may be influencing the overall pain burden. A number of different approaches, ranging from electroacupuncture to manual methods, will be detailed (see Chs 6, 8 and 9 in particular).
� Trauma (e.g. whiplash) seems to be a key feature of the onset in many cases of FMS, and especially cervical injuries, particularly those involving the suboccipital musculature (Bennett 1986b, Curatolo et al 2001, Hallgren et al 1993). Recognition of mechanical, structural factors allows for interventions which address their repercussions, as well as the psychological effects of trauma. In Chapter 9 Carolyn McMakin presents compelling evidence for the use of microcurrents in treatment of FMS of traumatic (especially of the cervical region) origin.
� There is an �immune dysfunction� model for myalgic encephalomyelitis (ME) � that uniquely British name for what appears to be an amalgam of chronic fatigue syndrome and fibromyalgia. This proposes a viral or other (vaccination, trauma, etc.) initial trigger which may lead to persistent overactivity of the immune system (overproduction of cytokines). Associated with this there may be chemical and/or food allergies, hypothalamic disturbance, hormonal imbalance and specific areas of the brain (e.g. limbic system) �malfunctioning�. The primary feature of this model is the overactive immune function, with many of the other features, such as endocrine imbalance and brain dysfunction, secondary to this (Macintyre 1993b). In recent research, the presence of systemic bacterial, mycoplasmal and viral coinfections in many�patients with CFS and FMS has been a feature (Nicolson et al 2002).
The Musculoskeletal Terrain Of FMS
Current research and clinical consensus seem to indicate that FMS is not primarily a musculoskeletal problem, although it is in the tissues of this system that its major symptoms manifest: �Fibromyalgia is a chronic, painful, musculo-skeletal condition characterised by widespread aching and points of tenderness associated with: 1) changed perception of pain, abnormal sleep patterns and reduced brain serotonin; and 2) abnormalities of microcirculation and energy metabolism in muscle� (Eisinger et al 1994).
These characteristics, involving abnormal microcirculation and energy deficits, are the prerequisites for the evolution of localized areas of myofascial distress and neural hyper-reactivity (i.e. trigger points). As indicated, one of the key questions to be answered in any given case is the degree to which the person�s pain is deriving from myofascial trigger points, or other musculoskeletal sources, since these may well be more easily modified than the complex underlying imbalances which are producing, contributing to, or maintaining the primary FMS condition.
Fibromyalgia History: Early Research
A great deal of research into FMS (under different names � see Box 1.1), and of the physiological mechanisms that increase our understanding of the FMS phenomenon, has been conducted over the past century (and earlier) and is worthy of review. Additional research in parallel with that focused on chronic muscular pain may clarify processes at work in this complex condition.
Korr�s Work On Facilitation
Among the most important researchers in the area of musculoskeletal dysfunction and pain over the past half century has been Professor Irwin Korr, whose work in explaining the facilitation phenomenon offers important insights into some of the events occurring in FMS and, more specifically, in myofascial pain settings. Needless to say, these often overlap. As suggested above, in a clinical context it is vital to know what degree of the pain being experienced in FMS is the result of myofascial pain, since this part of the pain package can relatively easily be modified or eliminated (see Chs 8 and 9).
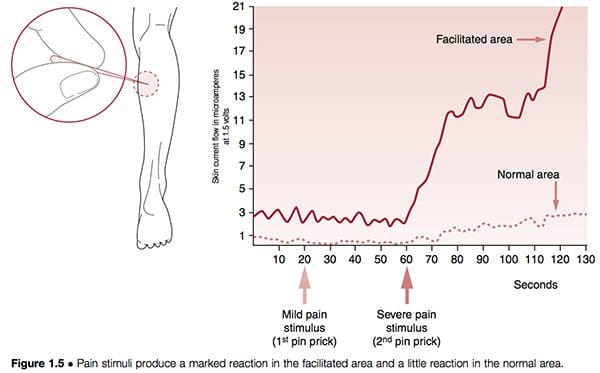
Neural structures can become hyper-reactive in either spinal and paraspinal tissues or almost any other soft tissue. When they are found close to the spine the phenomenon is known as segmental facilitation. When such changes occur in ligaments, tendons or periosteal tissues, they are called trigger points; if situated in muscles or in fascia they are termed �myofascial� trigger points. In early studies by the most important researcher into facilitation, Irwin Korr (1970, 1976), he demonstrated that a feature of unilateral segmental facilitation was that one side would test as having normal skin resistance to electricity compared with the contralateral side, the facilitated area, where a marked reduction in resistance was present. When �stress� � in the form of needling or heat � was applied elsewhere in the body, and the two areas of the spine were monitored, the area of facilitation showed a dramatic rise in electrical (i.e. neurological) activity. In one experiment volunteers had pins inserted into a calf muscle in order to gauge the effect on the paraspinal muscles, which were monitored for electrical activity. While almost no increase occurred in the normal region, the facilitated area showed greatly increased neurological activity after 60 seconds (Korr 1977) (Fig. 1.5). This and numerous similar studies have confirmed that any form of stress impacting the individual � be it climatic, toxic, emotional, physical or anything else � will produce an increase in neurological output from facilitated areas.
In Chapter 9, Carolyn McMakin describes how some forms of trauma, particularly those affecting cervical structures, can lead to chronic local facilitation, resulting in FMS-like pain. She reports that treatment utilizing microcurrent, manual modalities and nutritional support can frequently ease, or even remove, such symptoms.
Professor Michael Patterson (1976) explains the concept of segmental (spinal) facilitation as follows:
The concept of the facilitated segment states that because of abnormal afferent or sensory inputs to a particular area of the spinal cord, that area is kept in a state of constant increased excitation. This facilitation allows normally ineffectual or subliminal stimuli to become effective in producing efferent output from the facilitated segment, causing both skeletal and visceral organs innervated by the affected segment to be maintained in a state of�overactivity. It is probable that the somatic dysfunction with which a facilitated segment is associated, is the direct result of the abnormal segmental activity as well as being partially responsible for the facilitation.
Wind-Up And Facilitation
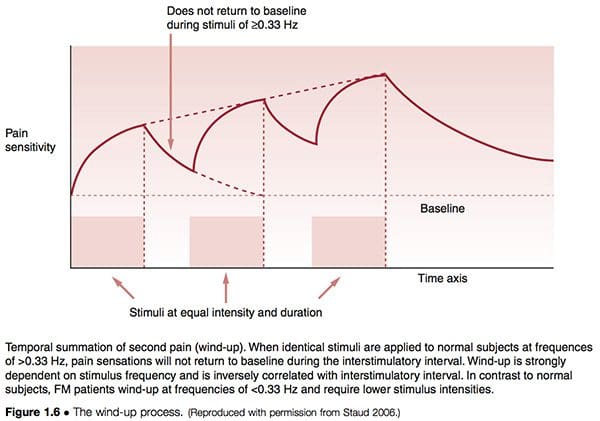
The process known as wind-up (Fig. 1.6) supports the concepts of facilitation, in different terms. Staud (2006) has described the relationship between peripheral pain impulses that lead to central sensitization as follows:
Increasing evidence points towards peripheral tissues as relevant contributors of painful impulse input that might either initiate or maintain central sensitization, or both. It is well known that persistent or intense nociception can lead to neuroplastic changes in the spinal cord and brain, resulting in central sensitization and pain. This mechanism represents a hallmark of FM and many other chronic pain syndromes, including irritable bowel syndrome, temporomandibular disorder, migraine, and low back pain. Importantly, after central sensitization has been established only minimal nociceptive input is required for the maintenance of the chronic pain state. Additional factors, including pain related negative affect and poor sleep have been shown to significantly contribute to clinical FM pain.
The similarities between modern neurological observations and Korr�s original work are clear.
Arousal And Facilitation
Emotional arousal is also able to affect the susceptibility of neural pathways to sensitization. The increase in descending influences from the emotionally aroused subject would result in an increase in toxic excitement in the pathways and allow additional inputs to produce sensitization at lower intensities. This implies that highly emotional people, or those in a highly emotional situation, would be expected to show a higher incidence of facilitation of spinal pathways or local areas of myofascial distress (Baldry 1993).
This has a particular relevance to fibromyalgia, where heightened arousal (for a variety of possible�reasons, as will become clear), in addition to possible limbic system dysfunction, leads to major influences from the higher centers (Goldstein 1996). Since the higher brain centers do influence the tonic levels of the spinal paths, it might be expected that physical training and mental attitudes would also tend to alter the tonic excitability, reducing the person�s susceptibility to sensitization from everyday stress. Thus the athlete would be expected to withstand a comparatively high level of afferent input prior to experiencing the self-perpetuating results of sensitization. This, too, has a relevance to fibromyalgia, where there exists ample evidence of beneficial influences of aerobic training programs (McCain 1986, Richards & Scott 2002).
Selective Motor Unit Recruitment
Researchers have shown that a small number of motor units, located in particular muscles, may display almost constant or repeated activity when influenced psychogenically. Low amplitude activity (using surface EMG) was evident even when the muscle was not being employed, if there was any degree of emotional arousal. �A small pool of lowthreshold motor units may be under considerable load for prolonged periods of time … motor units with Type 1 [postural] fibers are predominant among these. If the subject repeatedly recruits the same motor units, the overload may result in a metabolic crisis.� (Waersted et al 1993). The implications of this research are profound for they link even low grade degrees of emotional distress with almost constant sensitization of specific myofascial structures, with the implications associated with facilitation and pain generation. This aetiology parallels the proposed evolution of myofascial trigger points, as suggested by Simons et al (1999).
Not Only Myelinated Fibres
Research by Ronald Kramis has shown that, in chronic pain settings, non-nociceptive neurons can become sensitized to carry pain impulses (Kramis 1996). Hypersensitization of spinal neurons may actually involve non-nociceptive neurons altering their phenotype so that they commence releasing substance P. This, it is thought, may play a significant part in FMS pain perception, as increased levels of substance P in�the cerebrospinal fluid maintain heightened amplification of what would normally be registered as benign impulses. The research suggests that impulses from associated conditions such as ongoing viral activity, �muscular distress� or irritable bowel may be adequate to maintain the central pain perception.
Local Facilitation
Apart from paraspinal tissues, where segmental facilitation, as described above, manifests, localized areas of neural facilitation can occur in almost all soft tissues: these are called myofascial trigger points.
Much of the basic research and clinical work into this aspect of facilitation has been undertaken by doctors Janet Travell and David Simons (Simons et al 1999; Travell 1957; Travell & Simons 1986, 1992; see also Chs 6 and 8). Travell and Simons are on record as stating that if a pain is severe enough to cause a patient to seek professional advice (in the absence of organic disease), it usually involves referred pain, and therefore a trigger area is probably a factor. They remind us that patterns of referred pain are constant in distribution in all people, and that only the intensity of referred symptoms/pain will vary.
The implication for the fibromyalgia patient is the possibility (according to Travell and Simons this is a veritable certainty) that their pain has as part of its make-up the involvement of myofascial trigger points, which are themselves areas of facilitation (see Ch. 8 by Dommerholt & Issa). This suggests that trigger points, and the pain (and tingling, numbness, etc.) which they produce, will be exaggerated by all forms of stress influencing that individual patient. Travell has confirmed that her research indicates that the following factors can all help to maintain and enhance myofascial trigger point activity:
� nutritional deficiencies (especially vitamins C and B complex, and iron)
� low oxygenation of tissues (aggravated by tension, stress, inactivity, poor respiration) (Simons et al 1999, Travell & Simons 1986, 1992).
This list corresponds closely with factors that are key aggravating agents for many (most) people with fibromyalgia, suggesting that the connection between facilitation (trigger point activity) and FMS is close (Starlanyl & Copeland 1996). Myofascial trigger points are, however, not the cause of fibromyalgia, and myofascial pain syndrome is not FMS, although they may coexist in the same person at the same time. Myofascial trigger points do undoubtedly frequently contribute to the painful aspect of FMS, and as such are deserving of special attention.
As will be explained in later chapters, there are a number of ways in which deactivation or modulation of myofascial trigger points can be achieved. Some practitioners opt for approaches that deal with them manually, while others prefer microcurrents or electro-acupuncture methods or variations on these themes, with yet others suggesting that reduction in the number and intensity of stress factors � of whatever type � offers a safer approach to reducing the influence of facilitation on pain.
Following this introduction to the concept of hyper-reactive, sensitized (facilitated) neural structures, it would be justifiable to enquire as to whether or not what is happening in the brain and in the neural network, as described by Goldstein, is not simply facilitation on a grand scale. The outline of some of the leading current hypotheses as to the aetiology of FMA in Chapter 4 may shed light on this possibility.
Additional Early Research Into FMS
Early FMS research has been presented in summary form in Box 1.1. Aspects of that research, and how some of it correlates with more recent findings, are outlined below.
R. Gutstein, a Polish physician who emigrated to the UK prior to the Second World War, was a remarkable researcher who published papers under different names (M. G. Good, for example) before, during and following the war. In them he clearly described the myofascial trigger point phenomenon, as well as what is now known as fibromyalgia, along with a great many of its predisposing and maintaining features.
Gutstein (1956) showed that conditions such as ametropia (an error in the eye�s refractive power occurring in myopia, hypermetropia and astigmatism) may result from changes in the neuromuscular component of the craniocervical area, as well as more distant conditions involving the pelvis or shoulder girdle. He stated: �Myopia is the long-term effect of pressure of extra-ocular muscles in the convergence effort of accommodation involving spasm of the ciliary muscles, with resultant elongation of the eyeball. A sequential relationship has been shown between such a condition and muscular spasm of the neck.�
Gutstein termed reflex areas he identified �myodysneuria� and suggested that the reference phenomena of such spots or �triggers� would include pain, modifications of pain, itching, hypersensitivity to physiological stimuli, spasm, twitching, weakness and trembling of striated muscles, hyper- or hypotonus of smooth muscle of blood vessels and of internal organs, and/or hyper- or hyposecretion of visceral, sebaceous and sudatory glands. Somatic manifestations were also said to occur in response to visceral stimuli of corresponding spinal levels (Gutstein 1944). In all of these suggestions Gutstein seems to have been in parallel with the work of Korr.
Gutstein/Good�s method of treatment involved the injection of an anaesthetic solution into the trigger area. He indicated, however, that where accessible (e.g. muscular insertions in the cervical area) the chilling of these areas combined with pressure would yield good results.
In this and much of what he reported in the 1940s and 1950s Gutstein was largely in agreement with the research findings of John Mennell (1952) as well as with Travell & Simons, as expressed in their major texts on the subject (Travell & Simons 1986, 1992). He reported that obliteration of overt and latent triggers in the occipital, cervical, interscapular, sternal and epigastric regions was accompanied by years of alleviation of premenopausal, menopausal and late menopausal symptoms (Good 1951). He quotes a number of practitioners who had achieved success in treating gastrointestinal dysfunctions by deactivating trigger areas. Some of these were treated by procainization, others by pressure techniques and massage (Cornelius 1903). He also reported the wide range of classic fibromyalgia symptoms and features, suggesting the name myodysneuria for this syndrome, which he also termed �nonarticular rheumatism� (Gutstein 1955). In describing myodysneuria (FMS), Gutstein demonstrated localized functional sensory and/or motor abnormalities of musculoskeletal tissues and saw the causes of such changes as multiple (Gutstein 1955). Most of these findings have been validated subsequently, in particular by the work of Travell and Simons. They include:
� acute and chronic infections, which he postulated stimulated sympathetic nerve activity via their toxins
� excessive heat or cold, changes in atmospheric pressure and draughts
� mechanical injuries, both major and repeated minor microtraumas � now validated by the recent research of Professor Philip Greenman of Michigan State University (Hallgren et al 1993)
� postural strains, unaccustomed exercise, etc., which could predispose towards future changes by lowering the threshold for future stimuli (in this he was agreeing with facilitation mechanisms as described above)
� allergic and/or endocrine factors which could cause imbalances in the autonomic nervous system
� congenital factors which make adaptation to environmental stressors difficult
� arthritic changes which could impose particular demands on the musculoskeletal system�s adaptive capacity
� visceral diseases which could intensify and precipitate somatic symptoms in the distribution of their spinal and adjacent segments.
We can see from these examples of Gutstein�s thinking strong echoes of the facilitation hypothesis in osteopathic medicine.
Gutstein�s diagnosis of myodysneuria was made according to some of the following criteria:
� a varying degree of muscular tension and contraction is usually present, although sometimes adjacent, apparently unaffected tissue is more painful
� sensitivity to pressure or palpation of affected muscles and their adjuncts
� marked hypertonicity may require the application of deep pressure to demonstrate pain.
In 1947 Travell & Bigelow produced evidence supporting much of what Gutstein (1944) had reported. They indicated that high intensity stimuli from active trigger areas produce, by reflex, prolonged vasoconstriction with partial ischaemia in localized areas of the brain, spinal cord, or peripheral nerve structures.
A widespread pattern of dysfunction might then result, affecting almost any organ of the body. These�early research findings correlate well with modern fibromyalgia and chronic fatigue research and the hypothesis of �neural network disorders� as described by Goldstein (1996), and in British and American research utilizing SPECT scans, which show clearly that severe circulatory deficits occur in the brainstem and in other areas of the brain of most people with CFS and FMS (Costa 1992).
Gutstein�s Suggested Pathophysiology Of Fibromyalgia/ Fibrositis/Myodysneuria
The changes which occur in tissue involved in the onset of myodysneuria/fibromyalgia, according to Gutstein, are thought to be initiated by localized sympathetic predominance, associated with changes in the hydrogen ion concentration and calcium and sodium balance in the tissue fluids (Petersen 1934). This is associated with vasoconstriction and hypoxia/ischaemia. Pain resulted, he thought, by these alterations affecting the pain sensors and proprioceptors.
Muscle spasm and hard, nodular, localized tetanic contractions of muscle bundles, together with vasomotor and musculomotor stimulation, intensified each other, creating a vicious cycle of self-perpetuating impulses (Bayer 1950). Varied and complex patterns of referred symptoms might then result from such �trigger� areas, as well as local pain and minor disturbances. Sensations such as aching, soreness, tenderness, heaviness and tiredness may all be manifest, as may modification of muscular activity due to contraction, resulting in tightness, stiffness, swelling and so on.
It is clear from this summary of his work that Gutstein was describing fibromyalgia, and many of its possible causative features.
Chapter 2 examines what FMS is, as well as what it is not, with suggestions for differential diagnosis.
blank
References:
Abraham G, Lubran M M 1981 Serum
and red cell magnesium levels in
patients with PMT. American
Journal of Clinical Nutrition 34(11):
2364�2366
American College of Rheumatology
1990 Criteria for the classification of
fibromyalgia. Arthritis and
Rheumatism 33: 160�172
Arguellesa L, Afarib N, Buchwald D et al
2006 A twin study of posttraumatic
stress disorder symptoms and
chronic widespread pain. Pain 124
(1�2): 150�157
Baldry P 1993 Acupuncture trigger
points and musculoskeletal pain.
Churchill Livingstone, London
Bayer H 1950 Pathophysiology of
muscular rheumatism. Zeitschrift fur
Rheumaforschung 9: 210
Bennett R 1986a Fibrositis: evolution of
an enigma. Journal of Rheumatology
13(4): 676�678
Bennett R 1986b Current issues
concerning management of the
fibrositis/fibromyalgia syndrome.
American Journal of Medicine
81(S3A): 15�18
Bland J 1995 A medical food
supplemented detoxification
programme in the management of
chronic health problems. Alternative
Therapies 1: 62�71
Block S 1993 Fibromyalgia and the
rheumatisms. Controversies in
Rheumatology 19(1): 61�78
Chaitow L, Bradley D, Gilbert C 2002
Multidisciplinary approaches to
breathing pattern disorders.
Churchill Livingstone, Edinburgh
Cleveland C H Jr, Fisher R H, Brestel
E P et al 1992 Chronic rhinitis: an
underrecognized association with
fibromyalgia. Allergy Proceedings 13
(5): 263�267
Copenhagen Declaration 1992
Consensus document on FMS: the
Copenhagen declaration. Lancet 340
(September 12)
Cordain L, Toohey L, Smith M J,
Hickey M S 2000 Modulation of
immune function by dietary lectins in
rheumatoid arthritis. British Journal
of Nutrition 83(3): 207�217
Cornelius A 1903 Die Neurenpunkt
Lehre. George Thiem, Leipzig, vol 2
Costa D 1992 Report. European Journal
of Nuclear Medicine 19(8): 733
Crissinger K 1990 Pathophysiology of
gastrointestinal mucosal
permeability. Journal of Internal
Medicine 228: 145�154
Croft P, Cooper C, Wickham C,
Coggon D 1992 Is the hip involved in
generalized osteoarthritis? British
Journal of Rheumatology 31:
325�328
Curatolo M, Petersen-Felix S, ArendtNielsen
L et al 2001 Central
hypersensitivity in chronic pain after
whiplash injury. Clinical Journal of
Pain 17(4): 306�315
D�Adamo P 2002 <http://www.
dadamo.com>
Diatchenko L, Nackleya A, Slade G
2006 Idiopathic pain disorders �
pathways of vulnerability. Pain 123
(3): 226�230
Duna G, Wilke W 1993 Diagnosis,
etiology and therapy of fibromyalgia.
Comprehensive Therapy 19(2):
60�63
Eisinger J, Plantamura A, Ayavou T 1994
Glycolysis abnormalities in
fibromyalgia. Journal of the
American College of Nutrition 13(2):
144�148
Epstein S, Kay G, Clauw D 1999
Psychiatric disorders in patients with
fibromyalgia: a multicenter
investigation. Psychosomatics 40:
57�63
Fibromyalgia Network Newsletters
1990�94 Reports on nutritional
influences: October 1990�January
1992, Compendium No. 2, January
1993, May 1993 Compendium,
January 1994, July 1994 (Back issues
are available from the Network at PO
Box 31750, Tucson, Arizona
85761�1750)
Garrison R, Breeding P 2003 A
metabolic basis for fibromyalgia and
its related disorders: the possible role
of resistance to thyroid hormone.
Medical Hypotheses 61(2): 182�189
Gedalia A, Press J, Klein M, Buskila D
1993 Joint hypermobility and
fibromyalgia in schoolchildren.
Annals of the Rheumatic Diseases
52(7): 494�496
Geisser M, Williams D, Clauw D 2006
Impact of co-morbid somatic
symptoms above and beyond that of
pain in patients with fibromyalgia
and gulf war illnesses. Journal of Pain
7(4 Suppl 1): S28
Goldman J 1991 Hypermobility and
deconditioning: important links to
fibromyalgia. Southern Medical
Journal 84: 1192�1196
Goldstein J 1996 Betrayal by the brain:
the neurological basis of CFS and
FMS and related neural network
disorders. Haworth Medical Press,
New York
Good M G 1951 Objective diagnosis
and curability of non-articular
rheumatism. British Journal of
Physical Medicine and Industrial
Hygiene 14: 1�7
Gutstein R 1944 The role of abdominal
fibrositis in functional indigestion.
Mississippi Valley Medical Journal
66: 114�124
Gutstein R 1955 A review of
myodysneuria (fibrositis). American
Practitioner and Digest of
Treatments 6(4)
Gutstein R 1956 The role of
craniocervical myodysneuria in
functional ocular disorders. American
Practitioner�s Digest of Treatments
(November)
Haley R, Vongpatanasin W, Wolfe G
et al 2004 Blunted circadian variation
in autonomic regulation of sinus node
function in veterans with Gulf War
syndrome. American Journal of
Medicine 117(7): 469�478
Hallgren R, Greenman P, Rechtien J
1993 MRI of normal and atrophic
muscles of the upper cervical spine.
Journal of Clinical Engineering 18(5):
433�439
Honeyman G 1997 Metabolic therapy
for hypothyroid and euthyroid
fibromyalgia: two case reports.
Clinical Bulletin of Myofascial
Therapy 2(4): 19�49
Hudson J I, Arnold L M, Keck P E et al
2004 Family study of fibromyalgia
and affective spectrum disorder.
Biological Psychiatry 56(11):
884�891
Janda V 1988 Muscles and cervicogenic
pain and syndromes. In: Grant R (ed)
Physical therapy of the cervical and
thoracic spine. Churchill Livingstone,
London, pp 153�166
Karaaslan Y, Haznedaroglu S, Ozturk M
2000 Joint hypermobility and
primary fibromyalgia. Journal of
Rheumatology 27: 1774�1776
Kesler R, Mandizabal J 1999 Headache
in Chiari malformation. Journal of
the American Osteopathic
Association 99(3): 153�156
King J 1988 Hyperventilation � a
therapist�s point of view. Journal of
the Royal Society of Medicine 81
(September): 532�536
Korr I 1970 Physiological basis of
osteopathic medicine. Postgraduate
Institute of Osteopathic Medicine
and Surgery, New York
Korr I 1976 Spinal cord as organiser of
disease process. Academy of Applied
Osteopathy Yearbook 1976, Carmel
Korr I (ed) 1977 Neurobiological
mechanisms in manipulation. Plenum
Press, New York
Kramis R 1996 Non-nociceptive aspects
of musculoskeletal pain. Journal of
Orthopaedic and Sports Physical
Therapy 24(4): 255�267
Lowe J 1997 Results of open trial of T3
therapy with 77 euthyroid female
FMS patients. Clinical Bulletin of
Myofascial Therapy 2(1): 35�37
Lowe J, Honeyman-Lowe B 2006
Female fibromyalgia patients: lower
resting metabolic rates than matched
healthy controls. Medical Science
Monitor 12(7): 282�289
Lowe J, Cullum M, Graf L, Yellin J
1997 Mutations in the c-erb-Ab1
gene: do they underlie euthyroid
fibromyalgia? Medical Hypotheses 48
(2): 125�135
Lum L 1981 Hyperventilation and
anxiety state. Journal of the Royal
Society of Medicine 74(January): 1�4
McCain G A 1986 Role of physical
fitness training in fibrositis/
fibromyalgia syndrome. American
Journal of Medicine 81(S3A): 73�77
McClean G, Wesseley S 1994
Professional and popular view of
CFS. British Medical Journal 308:
776�777
Macintyre A 1993a What causes ME?
Journal of Action for ME 14: 24�25
Macintyre A 1993b The immune
dysfunction hypothesis. Journal of
Action for ME 14: 24�25
McNaught C E, Woodcock N P,
Anderson A D, MacFie J 2005 A
prospective randomised trial of
probiotics in critically ill patients.
Clinical Nutrition 24(2): 211�219
Martinez-Lavin M, Hermosillo A 2005
Dysautonomia in Gulf War
syndrome and in fibromyalgia.
American Journal of Medicine
118(4): 446
Melzack R, Wall P 1988 The challenge
of pain. Penguin, New York
Mennell J 1952 The science and art of
manipulation. Churchill Livingstone,
London
Mense S, Simons D 2001 Muscle pain.
Lippincott/Williams and Wilkins,
Philadelphia
Moldofsky H L 1993 Fibromyalgia, sleep
disorder and chronic fatigue
syndrome. CIBA Symposium 173:
262�279
Nicolson G, Nasralla M, De Meirleir K
2002 Bacterial and viral co-infections
in chronic fatigue syndrome patients.
This article is available from: http://
www.prohealth.com/library/
showarticle.cfm?
id�3635&t�CFIDS_FM.
8 December 2008
Pall M L 2001 Common etiology of
posttraumatic stress disorder,
fibromyalgia, chronic fatigue
syndrome and multiple chemical
sensitivity via elevated nitric oxide/
peroxynitrite. Medical Hypotheses
57(2): 139�145
Patterson M 1976 Model mechanism for
spinal segmental facilitation.
Academy of Applied Osteopathy
Yearbook 1976, Carmel
Pellegrino M J, Waylonis G W, Sommer
A 1989 Familial occurrence of
primary fibromyalgia. Archives of
Physical Medicine and Rehabilitation
70(1): 61�63
Petersen W 1934 The patient and the
weather: autonomic disintegration.
Edward Brothers, Ann Arbor,
Michigan
Porter-Moffitt S, Gatchel R, Robinson R
et al 2006 Biopsychosocial profiles of
different pain diagnostic groups.
Journal of Pain 7(5):
308�318
Readhead C 1984 Enhanced adaptive
behavioural response in patients
pretreated by breathing retraining.
Lancet 22(September): 665�668
Richards S, Scott D 2002 Prescribed
exercise in people with fibromyalgia:
parallel group randomised controlled
trial. British Medical Journal 325:
185
Robinson M 1981 Effect of daily
supplements of selenium on patients
with muscular complaints. New
Zealand Medical Journal 93:
289�292
Schmidt-Wilcke T, Luerding R,
Weigand T 2007 Striatal grey matter
increase in patients suffering from
fibromyalgia � a voxel-based
morphometry study. Pain 132:
S109�S116
Schneider M J, Brady D M, Perle S M
2006 Commentary: differential
diagnosis of fibromyalgia syndrome:
proposal of a model and algorithm for
patients presenting with the primary
symptom of chronic widespread
pain. Journal of Manipulative and
Physiological Therapeutics 29:
493�501
Selye H 1952 The story of the
adaptation syndrome. ACTA,
Montreal, Canada
Simons D 1988 Myofascial pain
syndromes: where are we? Where are
we going? Archives of Physical
Medicine and Rehabilitation 69:
207�211
Simons D, Travell J, Simons L 1999
Myofascial pain and dysfunction: the
trigger point manual. Vol 1. Upper
half of body, 2nd edn. Williams and
Wilkins, Baltimore
Smith J D, Terpening C M, Schmidt S
O, Gums J G 2001 Relief of
fibromyalgia symptoms following
discontinuation of dietary
excitotoxins. Annals of
Pharmacotherapy 35(6):
702�706
Solomon G 1981
Psychoneuroimmunology. Academic
Press, New York
Starlanyl D, Copeland M E 1996
Fibromyalgia and chronic myofascial
pain syndrome. New Harbinger
Publications, Oakland, California
Staud R 2006 Biology and therapy of
fibromyalgia: pain in fibromyalgia
syndrome. Arthritis Research and
Therapy 8: 208
Staud R, Robinson M, Price D 2005
New evidence for central
sensitization of fibromyalgia patients:
Windup maintenance is abnormal.
Journal of Pain 6(3): S6
Sundgren P, Petrou P, Harris R 2007
Diffusion-weighted and diffusion
tensor imaging in fibromyalgia
patients: a prospective study of
whole brain diffusivity, apparent
diffusion coefficient, and fraction
anisotropy in different regions of the
brain and correlation with symptom
severity. Academic Radiology 14:
839�846
Tagesson C 1983 Passage of molecules
through the wall of the intestinal
tract. Scandinavian Journal of
Gastroenterology 18: 481�486
Thimineur M, Kitaj M, Kravitz E,
Kalizewski T, Sood P 2002
Functional abnormalities of the
cervical cord and lower medulla and
their effect on pain. Clinical Journal
of Pain 18(3): 171�179
Thompson J 1990 Tension myalgia as a
diagnosis at the Mayo Clinic and its
relationship to fibrositis, fibromyalgia
and myofascial pain syndrome. Mayo
Clinic Proceedings 65: 1237�1248
Travell J 1957 Symposium on
mechanism and management of pain
syndromes. Proceedings of the
Rudolph Virchow Medical Society
Travell J, Bigelow N 1947 Role of
somatic trigger areas in the patterns
of hysteria. Psychosomatic Medicine
9(6): 353�363
Travell J, Simons D 1986 Myofascial
pain and dysfunction. Williams and
Wilkins, Baltimore, vol 1
Travell J, Simons D 1992 Myofascial
pain and dysfunction. Williams and
Wilkins, Baltimore, vol 2
Tuncer T 1997 Primary FMS and allergy.
Clinical Rheumatology 16(1): 9�12
van de Borne P 2004 Cardiac autonomic
dysfunction in Gulf War syndrome:
veterans� hearts don�t rest at night.
American Journal of Medicine 117
(7): 531�532
van Why R 1994 FMS and massage
therapy. Self published
Ventura M T, Polimeno L, Amoruso A C
et al 2006 Intestinal permeability in
patients with adverse reactions to
food. Digestive and Liver Disease 38
(10): 732�736
Vierck C Jr 2006 Mechanisms
underlying development of spatially
distributed chronic pain
(fibromyalgia). Pain 124(3):
242�263
Vorberg G 1985 Ginko extract � a longterm
study of chronic cerebral
insufficiency. Clinical Trials Journal
22: 149�157
Waersted M, Eken T, Westgaard R 1993
Psychogenic motor unit activity � a
possible muscle injury mechanism
studied in a healthy subject. Journal
of Musculoskeletal Pain 1(3/4):
185�190
Warner E (ed) 1964 Saville�s system of
clinical medicine, 14th edn. Edward
Arnold, London, p 918
Weissbecker I, Floyd A, Dedert E et al
2006 Childhood trauma and diurnal
cortisol disruption in fibromyalgia
syndrome.
Psychoneuroendocrinology 31(3):
312�324
Wolfe F, Simons D G, Fricton J et al
1992 The fibromyalgia and
myofascial pain syndromes: a
preliminary study of tender points
and trigger points. Journal of
Rheumatology 19(6): 944�951
Wolfe F, Anderson J, Ross K, Russel I
1993 Prevalence of characteristics of
fibromyalgia in the general
population. Arthritis and
Rheumatism 36: S48 (abstract)
Wood P 2006 A reconsideration of the
relevance of systemic low-dose
ketamine to the pathophysiology of
fibromyalgia. Journal of Pain 7(9):
611�614
Yunus M, Inanici F 2002 Fibromyalgia
syndrome: clinical features,
diagnosis, and biopathophysiologic
mechanisms. In: Yunus M B, Yunus I
(eds) Myofascial pain and
fibromyalgia. Mosby, St Louis
Zar S 2005 Food-specific serum IgG4
and IgE titers to common food
antigens in irritable bowel syndrome.
American Journal of
Gastroenterology 100: 1550�1557
Headaches can be a real aggravating issue, especially if these begin to occur more frequently. Even more so, headaches can become a bigger problem when the common type of head pain becomes a migraine. Head pain is often a symptom resulting from an underlying injury and/or condition along the cervical spine, or upper back and neck. Fortunately, a variety of treatment methods are available to help treat headaches. Chiropractic care is a well-known alternative treatment option which is commonly recommended for neck pain, headaches and migraines. The purpose of the following research study is to determine the effectiveness of chiropractic spinal manipulative therapy for migraine.
Chiropractic Spinal Manipulative Therapy for Migraine: a Study Protocol of a Single-Blinded Placebo-Controlled Randomised Clinical Trial
Abstract
Introduction
Migraine affects 15% of the population, and has substantial health and socioeconomic costs. Pharmacological management is first-line treatment. However, acute and/or prophylactic medicine might not be tolerated due to side effects or contraindications. Thus, we aim to assess the efficacy of chiropractic spinal manipulative therapy (CSMT) for migraineurs in a single-blinded placebo-controlled randomised clinical trial (RCT).
Method and Analysis
According to the power calculations, 90 participants are needed in the RCT. Participants will be randomised into one of three groups: CSMT, placebo (sham manipulation) and control (usual non-manual management). The RCT consists of three stages: 1?month run-in, 3?months intervention and follow-up analyses at the end of the intervention and 3, 6 and 12?months. The primary end point is migraine frequency, while migraine duration, migraine intensity, headache index (frequency x duration x intensity) and medicine consumption are secondary end points. Primary analysis will assess a change in migraine frequency from baseline to the end of the intervention and follow-up, where the groups CSMT and placebo and CSMT and control will be compared. Owing to two group comparisons, p values below 0.025 will be considered statistically significant. For all secondary end points and analyses, a p value below 0.05 will be used. The results will be presented with the corresponding p values and 95% CIs.
Ethics and Dissemination
The RCT will follow the clinical trial guidelines from the International Headache Society. The Norwegian Regional Committee for Medical Research Ethics and the Norwegian Social Science Data Services have approved the project. Procedure will be conducted according to the declaration of Helsinki. The results will be published at scientific meetings and in peer-reviewed journals.
Trial Registration Number
NCT01741714.
Keywords:Statistics & Research Methods
Strengths and Limitations of this Study
The study will be the first three-armed manual therapy randomised clinical trial (RCT) assessing the efficacy of chiropractic spinal manipulative therapy versus placebo (sham manipulation) and control (continue usual pharmacological management without receiving manual intervention) for migraineurs.
Strong internal validity, since a single chiropractor will conduct all interventions.
The RCT has the potential to provide a non-pharmacological treatment option for migraineurs.
Risk for dropouts is increased due to strict exclusion criteria and 17?months duration of the RCT.
A generally accepted placebo has not been established for manual therapy; thus, there is a risk for unsuccessful blinding, while the investigator who provides the interventions cannot be blinded for obvious reasons.
Background
Migraine is a common health problem with substantial health and socioeconomic costs. On the recent Global Burden of Disease study, migraine was ranked as the third most common condition.[1]
About 15% of the general population have migraine.[2, 3] Migraine is usually unilateral with pulsating and moderate/severe headache which is aggravated by routine physical activity, and is accompanied by photophobia and phonophobia, nausea and sometimes vomiting.[4] Migraine exists in two major forms, migraine without aura and migraine with aura (below). Aura is reversible neurological disturbances of the vision, sensory and/or speech function, occurring prior to the headache. However, intraindividual variations from attack to attack are common.[5, 6] The origin of migraine is debated. The painful impulses may originate from the trigeminal nerve, central and/or peripheral mechanisms.[7, 8] Extracranial pain sensitive structures include the skin, muscles, arteries, periosteum and joints. The skin is sensitive to all usual forms of pain stimuli, while temporal and neck muscles may especially be sources for pain and tenderness in migraine.[9�11] Similarly, the frontal supraorbital, superficial temporal, posterior and occipital arteries are sensitive to pain.[9, 12]
Notes
The International Classification of Headache Disorders-II Diagnostic Criteria for Migraine
Migraine without Aura
A. At least five attacks fulfilling criteria B�D
B. Headache attacks lasting 4�72?h (untreated or unsuccessfully treated)
C. Headache has at least two of the following characteristics:
1. Unilateral location
2. Pulsating quality
3. Moderate or severe pain intensity
4. Aggravated by or causing avoidance of routine physical activity
D. During headache at least one of the following:
1. Nausea and/or vomiting
2. Photophobia and phonophobia
E. Not attributed to another disorder
Migraine with aura
A. At least two attacks fulfilling criteria B�D
B. Aura consisting of at least one of the following, but no motor weakness:
1. Fully reversible visual symptoms including positive features (ie, flickering lights, spots or lines) and/or negative features (ie, loss of vision). Moderate or severe pain intensity
2. Fully reversible sensory symptoms including positive features (ie, pins and needles) and/or negative features (ie, numbness)
2. At least one aura symptom develops gradually over ?5?min and/or different aura symptoms occur in succession over ?5?min
3. Each symptom lasts ?5 and ?60?min
D. Headache fulfilling criteria B-D for 1.1 Migraine without aura begins during the aura or follows the aura within 60?min
E. Not attributed to another disorder
Pharmacological management is the first treatment option for migraineurs. However, some patients do not tolerate acute and/or prophylactic medicine due to side effects or contraindications due to comorbidity of other diseases or due to a wish to avoid medication for other reasons. The risk of medication overuse due to frequent migraine attacks represents a major health hazard with direct and indirect cost concerns. The prevalence of medication overuse headache (MOH) is 1�2% in the general population,[13�15] that is, about half the population suffering chronic headache (15 headache days or more per month) have MOH.[16] Migraine causes loss of 270 workdays per year per 1000 persons from the general population.[17] This corresponds to about 3700 work years lost per year in Norway due to migraine. The economic cost per migraineur was estimated to be $655 in USA and �579 in Europe per year.[18, 19] Owing to the high prevalence of migraine, the total cost per year was estimated to be $14.4 billion in the USA and �27 billion in the EU countries, Iceland, Norway and Switzerland at that time. Migraine costs more than neurological disorders such as dementia, multiple sclerosis, Parkinson’s disease and stroke.[20] Thus, non-pharmacological treatment options are warranted.
The Diversified technique and the Gonstead method are the two most commonly used chiropractic manipulative treatment modalities in the profession, used by 91% and 59%, respectively,[21, 22] along with other manual and non-manual interventions, that is, soft tissue techniques, spinal and peripheral mobilisation, rehabilitation, postural corrections and exercises as well as general nutrition and dietetic advice.
A few spinal manipulative therapy (SMT) randomised controlled trials (RCTs) using the Diversified technique have been conducted for migraine, suggesting an effect on migraine frequency, migraine duration, migraine intensity and medicine consumption.[23�26] However, common for previous RCTs are the methodological shortcomings such as inaccurate headache diagnosis, that is, questionnaire diagnoses used are imprecise,[27] inadequate or no randomisation procedure, lack of placebo group, and primary and secondary end points not prespecified.[28�31] In addition, previous RCTs did not consequently adhere to the recommended clinical guidelines from the International Headache Society (IHS).[32, 33] At present, no RCTs have applied the Gonstead chiropractic SMT (CSMT) method. Thus, considering the methodological shortcomings in previous RCTs, a clinical placebo-controlled RCT with improved methodological quality remains to be conducted for migraine.
The SMT mechanism of action on migraine is unknown. It is argued that migraine might originate from a complexity of nociceptive afferent responses involving the upper cervical spine (C1, C2 and C3), leading to a hypersensitivity state of the trigeminal pathway conveying sensory information for the face and much of the head.[34, 35] Research has thus suggested that SMT may stimulate neural inhibitory systems at different spinal cord levels, and might activate various central descending inhibitory pathways.[36�40] However, although the proposed physiological mechanisms are not fully understood, there are most likely additional unexplored mechanisms which could explain the effect SMT has on mechanical pain sensitisation.
The objective of this study is to assess the efficacy of CSMT versus placebo (sham manipulation) and controls (continue usual pharmacological management without receiving manual intervention) for migraineurs in an RCT.
Method and Design
This is a single-blinded placebo-controlled RCT with three parallel groups (CSMT, placebo and control). Our primary hypothesis is that CSMT gives at least 25% reduction in the average number of migraine days per month (30?days/month) as compared to placebo and control from baseline to the end of intervention, and we expect the same reduction to be maintained at 3, 6 and 12?months follow-up. If the CSMT treatment is effective, it will be offered to participants who received placebo or control after study completion, that is, after 12?months follow-up. The study will adhere to the recommended clinical trial guidelines from the IHS,32 33 and the methodological CONSORT and SPIRIT guidelines.[41, 42]
Patient Population
Participants will be recruited in the period January to September 2013 through the Akershus University Hospital, through general practitioners and media advertisement, that is, posters with general information will be put up at general practitioners� offices along with oral information in the Akershus and Oslo counties, Norway. Participants will receive posted information about the project followed by a short telephone interview. Those recruited from the general practitioners� offices will have to contact the clinical investigator whose contact details have been provided on the posters in order to obtain extensive information about the study.
Eligible participants are between 18 and 70?years of age and have at least one migraine attack per month. Participants are diagnosed according to the diagnostic criteria of the International Classification of Headache Disorders (ICHD-II) by a neurologist at the Akershus University Hospital.[43] They are only allowed to have co-occurrence of tension-type headache and not other primary headaches.
Exclusion criteria are contraindication to SMT, spinal radiculopathy, pregnancy, depression and CSMT within the previous 12?months. Participants whom during the RCT receive any manual interventions by physiotherapists, chiropractors, osteopaths or other health professionals to treat musculoskeletal pain and disability, including massage therapy, joint mobilisation and manipulation,[44] changed their prophylactic headache medicine or pregnancy will be withdrawn from the study at that time and be regarded as dropouts. They are allowed to continue and change their usual acute migraine medication throughout the trial.
In response to initial contact, participants fulfilling the inclusion criteria will be invited to further assessment by the chiropractic investigator. The assessment includes an interview and a physical examination with special emphasis on the whole spinal column. Oral and written information about the project will be provided in advance and oral and written consent will be obtained from all accepted participants during the interview and by the clinical investigator. In accordance with good clinical practice, all patients will be informed about the harms and benefits as well as possible adverse reactions of the intervention primarily including local tenderness and tiredness on the treatment day. No serious adverse events have been reported for the chiropractic Gonstead method.[45, 46] Participants randomised into active or placebo interventions will undergo a full spine radiographic examination and be scheduled for 12 intervention sessions. The control group will not be exposed to this assessment.
Clinical RCT
The clinical RCT consists of a 1?month run-in and 3?months intervention. Time profile will be assessed from baseline to the end of follow-up for all end points (Figure 1).
The participants will fill in a validated diagnostic paper headache diary 1?month prior to intervention which will be used as baseline data for all participants.[47, 48] The validated diary includes questions directly related to the primary and secondary end points. X-rays will be taken in standing position in the anterioposterior and lateral planes of the entire spine. The X-rays will be assessed by the chiropractic investigator.
Randomisation
Prepared sealed lots with the three interventions, that is, active treatment, placebo and the control group, will be subdivided into four subgroups by age and gender, that is, 18�39 and 40�70?years of age and men and women, respectively. Participants will be equally allocated to the three groups by allowing the participant to draw one lot only. The block randomisation will be administrated by an external trained party with no involvement from the clinical investigator.
Intervention
Active treatment consists of CSMT using the Gonstead method,[21] that is, a specific contact, high-velocity, low-amplitude, short-lever spinal with no postadjustment recoil directed to spinal biomechanical dysfunction (full spine approach) as diagnosed by standard chiropractic tests.
The placebo intervention consists of sham manipulation, that is, a broad non-specific contact, low-velocity, low-amplitude sham push manoeuvre in a non-intentional and non-therapeutic directional line. All the non-therapeutic contacts will be performed outside the spinal column with adequate joint slack and without soft tissue pretension so that no joint cavitations occur. In some sessions, the participant lay either prone on a Zenith 2010 HYLO bench with the investigator standing at the participant’s right side with his left palm placed on the participant’s right lateral scapular edge with the other hand reinforcing. In other sessions, the investigator will stand at the participant’s left side and place his right palm over the participant’s left scapular edge with the left hand reinforcing, delivering a non-intentional lateral push manoeuvre. Alternatively, the participant lay in the same side posture position as the active treatment group with the bottom leg straight and the top leg flexed with the top leg’s ankle resting on the bottom leg’s knee fold, in preparation for a side posture push move, which will be delivered as a non-intentional push in the gluteal region. The sham manipulation alternatives will be equally interchanged among the placebo participants according to protocol during the 12-week treatment period to strengthen the study validity. The active and the placebo groups will receive the same structural and motion assessment prior to and after each intervention. No additional cointerventions or advice will be given to participants during the trial period. The treatment period will include 12 consultations, that is, twice per week in the first 3?weeks followed by once a week in the next 2?weeks and once every second week until 12?weeks are reached. Fifteen minutes will be allocated per consultation for each participant. All interventions will be conducted at the Akershus University Hospital and administered by an experienced chiropractor (AC).
The control group will continue usual care, that is, pharmacological management without receiving manual intervention by the clinical investigator. The same exclusion criteria apply for the control group during the whole study period.
Blinding
After each treatment session, the participants who receive active or placebo intervention will complete a de-blinding questionnaire administrated by an external trained independent party with no involvement from the clinical investigator, that is, providing a dichotomous �yes� or �no� answer as to whether active treatment was received. This response was followed by a second question regarding how certain they were that active treatment was received on a 0�10 numeric rating scale (NRS), where 0 represents absolutely uncertain and 10 represents absolutely certainty. The control group and the clinical investigator can for obvious reasons not be blinded.[49, 50]
Follow-Up
Follow-up analysis will be conducted on the end points measured after the end of intervention and at 3, 6 and 12?months follow-up. During this period, all participants will continue to fill in a diagnostic paper headache diary and return it on a monthly basis. In the case of unreturned diary or missing values in the diary, the participants will be contacted immediately on detection to minimise recall bias. Participants will be contacted by phone to secure compliance.
Primary and Secondary End Points
The primary and secondary end points are listed below. The end points adhere to the recommended IHS clinical trial guidelines.[32, 33] We define number of migraine days as the primary end point and expect at least a 25% reduction in average number of days from baseline to the end of intervention, with the same level of reduction being maintained at follow-up. On the basis of previous reviews on migraine, a 25% reduction is considered to be a conservative estimate.[30] A 25% reduction is also expected in secondary end points from baseline to the end of intervention, retaining at follow-up for migraine duration, migraine intensity and headache index, where the index is calculated as number of migraine days (30?days)�average migraine duration (hours per day)�average intensity (0�10 NRS). A 50% reduction in medication consumption from baseline to the end of intervention and to follow-up is expected.
Notes
Primary and Secondary End Points
Primary End Points
1. Number of migraine days in active treatment versus placebo group.
2. Number of migraine days in active treatment versus control group.
Secondary End Points
3. Migraine duration in hours in active treatment versus placebo group.
4. Migraine duration in hours in active treatment versus control group.
5. Self-reported VAS in active treatment versus placebo group.
6. Self-reported VAS in active treatment versus control group.
7. Headache index (frequency x duration x intensity) in active treatment versus placebo group.
8. Headache index in active treatment versus control group.
9. Headache medication dosage in active treatment versus placebo group.
10. Headache medication dosage in active treatment versus control group.
*The data analysis is based on the run-in period versus end of intervention. Point 11�40 will be duplicate of point 1�10 above at 3, 6 and 12?months follow-up, respectively.
Data Processing
A flow chart of the participants is shown in Figure 2. Baseline demographic and clinical characteristics will be tabulated as means and SDs for continuous variables and proportions and percentages for categorical variables. Each of three groups will be described separately. Primary and secondary end points will be presented by suitable descriptive statistics in each group and for each time point. Normality of end points will be assessed graphically and transformation will be considered if necessary.
Change in primary and secondary end points from baseline to the end of intervention and to follow-up will be compared between the active and placebo groups and the active and control groups. The null hypothesis states that there is no significant difference between the groups in average change, while the alternative hypothesis states that a difference of at least 25% exists.
Owing to the follow-up period, repeated recordings of primary and secondary end points will be available, and analyses of trend in primary and secondary end points will be of main interest. Intra-individual correlations (cluster effect) are likely to be present in data with repeated measurements. Cluster effect will thus be assessed by calculating intraclass correlation coefficient quantifying the proportion of total variation attributable to the intraindividual variations. The trend in end points will be assessed by a linear regression model for longitudinal data (linear mixed model) to correctly account for the possible cluster effect. The linear mixed model handles unbalanced data, enabling all available information from randomised patients to be included, as well as from dropouts. Regression models with fixed effects for time component and group allocation as well as the interaction between the two will be estimated. The interaction will quantify possible differences between groups regarding time trend in the end points and serve as an omnibus test. Random effects for patients will be included to adjust the estimates for intraindividual correlations. Random slopes will be considered. The linear mixed models will be estimated by the SAS PROC MIXED procedure. The two pairwise comparisons will be performed by deriving individual time point contrasts within each group with the corresponding p values and 95% CIs.
Both per-protocol and intention-to-treat analyses will be conducted if relevant. All analyses will be performed by a statistician, blinded for group allocation and participants. All adverse effects will also be registered and presented. Participants who experience any sort of adverse effects during the trial period will be entitled to call the clinical investigator on the project cell phone. The data will be analysed with SPSS V.22 and SAS V.9.3. Owing to two group comparisons in the primary end point, p values below 0.025 will be considered statistically significant. For all secondary end points and analyses, a significance level of 0.05 will be used. Missing values might appear in incomplete interview questionnaires, incomplete headache diaries, missed intervention sessions and/or due to dropouts. The pattern of missingness will be assessed and missing values handled adequately.
Power Calculation
Sample size calculations are based on the results in a recently published group comparison study on topiramate.[51] We hypothesise that the average difference in reduction of number of days with migraine per month between the active and the placebo groups is 2.5?days. The same difference is assumed between the active and control groups. SD for reduction in each group is assumed to be equal to 2.5. Under the assumption of, on average, 10 migraine days per month at baseline in each group and no change in the placebo or control group during the study, 2.5?days reduction corresponds to a reduction by 25%. Since primary analysis includes two group comparisons, we set a significance level at 0.025. A sample size of 20 patients is required in each group to detect a statistically significant average difference in reduction of 25% with 80% power. To allow for dropouts, the investigators plan to recruit 120 participants.
Dr. Alex Jimenez’s Insight
“I’ve been recommended to seek chiropractic care for my migraine-type headaches. Is chiropractic spinal manipulative therapy effective for migraine?”�Many different types of treatment options can be utilized to effectively treat migraine, however, chiropractic care is one of the most popular treatment approaches for naturally treating migraine. Chiropractic spinal manipulative therapy�is the traditional high-velocity low-amplitude (HVLA) thrust. Also known as spinal manipulation, a chiropractor performs this chiropractic technique by applying a controlled sudden force to a joint while the body is positioned in a specific way. According to the following article, chiropractic spinal manipulative therapy can effectively help treat migraine.
Discussion
Methodological Considerations
Current SMT RCTs on migraine suggest treatment efficacy regarding migraine frequency, duration and intensity. However, a firm conclusion requires clinical single-blinded placebo-controlled RCTs with few methodological shortcomings.[30] Such studies should adhere to the recommended IHS clinical trial guidelines with migraine frequency as the primary end point and migraine duration, migraine intensity, headache index and medication consumption as secondary end points.[32, 33] The headache index, as well as a combination of frequency, duration and intensity, gives an indication of the total level of suffering. Despite the lack of consensus, the headache index has been recommended as an accepted standard secondary end point.[33, 52, 53] The primary and secondary end points will be collected prospectively in a validated diagnostic headache diary for all participants in order to minimise recall bias.[47, 48] To the best of our knowledge, this is the first prospective manual therapy in a three-armed single-blinded placebo-controlled RCT to be conducted for migraine. The study design adheres to the recommendations for pharmacological RCTs as far as possible. RCTs that include a placebo group and a control group are advantageous to pragmatic RCTs that compare two active treatment arms. RCTs also provide the best approach for producing safety as well as efficacy data.
Unsuccessful blinding is a possible risk to the RCT. Blinding is often difficult as there is no single validated standardised chiropractic sham intervention which can be used as a control group for this date. It is, however, necessary to include a placebo group in order to produce a true net effect of the active intervention. Consensus about an appropriate placebo for a clinical trial of SMT among experts representing clinicians and academics has, however, not been reached.[54] No previous studies have, to the best of our knowledge, validated a successful blinding of a CSMT clinical trial with multiple treatment sessions. We intend to minimise this risk by following the proposed protocol for the placebo group.
The placebo response is furthermore high in pharmacological and assumed similarly high for non-pharmacological clinical studies; however, it might even be higher in manual therapy RCTs were attention and physical contact is involved.[55] Similarly, a natural concern with regard to attention bias will be involved for the control group as it is not being seen by anyone or not seen as much by the clinical investigator as the other two groups.
There are always risks for dropouts due to various reasons. Since the trial duration is 17?months with a 12?month follow-up period, the risk for loss to follow-up is thus enhanced. Co-occurrence of other manual intervention during the trial period is another possible risk, as those who receive manipulation or other manual physical treatments elsewhere during the trial period will be withdrawn from the study and regarded as dropouts at the time of violation.
The external validity of the RCT might be a weakness as there is only one investigator. However, we found that advantageous to multiple investigators, in order to provide similar information to participants in all three groups and manual intervention in the CSMT and the placebo groups. Thus, we intend to eliminate inter-investigator variability which might be present if there are two or more investigators. Although the Gonstead method is the second most commonly used technique among chiropractors, we do not see an issue of concern when it comes to generalisability and external validity. Furthermore, the block randomisation procedure will provide a homogeneous sample across the three groups.
The internal validity is, however, strong by having one treating clinician. It reduces the risk of potential selection, information and experimental biases. Furthermore, the diagnosis of all participants is performed by experienced neurologists and not by questionnaires. A direct interview has higher sensitivity and specificity as compared to a questionnaire.[27] Individual motivational factors which can influence a participant’s perception and personal preferences when treating are both reduced by having one investigator. In addition, the internal validity is further strengthened by a concealed validated randomisation procedure. Since age and genders may play a role in migraine, block randomisation was found necessary to balance arms by age and gender in order to reduce possible age-related and/or gender-related bias.
X-rays demonstrating loss of cervical lordosis as a possible cause for migraine.
Conducting X-rays prior to the active and placebo interventions was found to be applicable in order to visualise posture, joint and disc integrity.[56, 57] Since the total X-ray radiation dose varies from 0.2�0.8?mSv, the radiation exposure was considered low.[58, 59] X-ray assessments were also found to be necessary in order to determine if full spine X-rays are useful in future studies or not.
Since we are unaware of the mechanisms of possible efficacy, and both spinal cord and central descending inhibitory pathways have been postulated, we see no reasons to exclude a full spine treatment approach for the intervention group. It has furthermore been postulated that pain in different spinal regions should not be regarded as separate disorders but rather as a single entity.[60] Similarly, including a full spine approach limits the differentiations between the CSMT and the placebo groups. Thus, it might strengthen the likelihood of successful blinding in the placebo group being achieved. In addition, all the placebo contacts will be performed outside the spinal column, thus minimising a possible spinal cord afferent input.
Innovative and Scientific Value
This RCT will highlight and validate the Gonstead CSMT for migraineurs, which has not previously been studied. If CSMT proves to be effective, it will provide a non-pharmacological treatment option. This is especially important as some migraineurs do not have efficacy of prescript acute and/or prophylactic medications, while others have non-tolerable side effects or comorbidity of other diseases that contradict medication while others wish to avoid medication for various reasons. Thus, if CSMT works, it can really have an impact on migraine treatment. The study also bridges cooperation between chiropractors and physicians, which is important in order to make healthcare more efficient. Finally, our method might be applied in future chiropractic and other manual therapy RCTs on headache.
Ethics and Dissemination
Ethics
The study has been approved by the Norwegian Regional Committee for Medical Research Ethics (REK) (2010/1639/REK) and the Norwegian Social Science Data Services (11�77). The declaration of Helsinki is otherwise followed. All data will be anonymised while participants must give oral and written informed consent. Insurance is provided through �The Norwegian System of Compensation to Patients� (NPE), which is an independent national body set up to process compensation claims from patients who have suffered an injury as a result of treatment under the Norwegian health service. A stopping rule was defined for withdrawing participants from this study in accordance with recommendations in the CONSORT extension for Better Reporting of Harms.[61] If a participant reports to their chiropractor or research staff a severe adverse event, he or she will be withdrawn from the study and referred to their general practitioner or hospital emergency department depending on the nature of the event. The final data set will be available to the clinical investigator (AC), the independent and blinded statistician (JSB) and Study Director (MBR). Data will be stored in a locked cabinet at the Research Centre, Akershus University Hospital, Norway, for 5?years.
Dissemination
This project is due for completion 3?years after the start. Results will be published in peer-reviewed international scientific journals in accordance with the CONSORT 2010 Statement. Positive, negative, as well as inconclusive results will be published. In addition, a written lay summary of the results will be available to study participants on request. All authors should qualify for authorship according to the International Committee of Medical Journal Editors, 1997. Each author should have participated sufficiently in the work to take public responsibility for the content. The final decision on the order of authorship will be decided when the project has been finalised. The results from the study may, moreover, be presented as posters or oral presentations at national and/or international conferences.
Acknowledgments
Akershus University Hospital kindly provided research facilities. Chiropractor Clinic1, Oslo, Norway, performed X-ray assessments.
Footnotes
Contributors: AC and PJT had the original idea for the study. AC and MBR obtained funding. MBR planned the overall design. AC prepared the initial draft and PJT commented on the final version of the research protocol. JSB performed all the statistical analyses. AC, JSB, PJT and MBR were involved in the interpretation and assisted in the revision and preparation of the manuscript. All authors have read and approved the final manuscript.
Funding: The study has received funding from Extrastiftelsen (grant number: 2829002), the Norwegian Chiropractic Association (grant number: 2829001), Akershus University Hospital (grant number: N/A) and University of Oslo in Norway (grant number: N/A).
Competing interests: None declared.
Patient consent: Obtained.
Ethics approval: The Norwegian Regional Committee for Medical Research Ethics approved the project (ID of the approval: 2010/1639/REK).
Provenance and peer review: Not commissioned; externally peer reviewed.
A Randomized Controlled Trial of Chiropractic Spinal Manipulative Therapy for Migraine
Abstract
Objective: To assess the efficacy of chiropractic spinal manipulative therapy (SMT) in the treatment of migraine.
Design: A randomized controlled trial of 6 months’ duration. The trial consisted of 3 stages: 2 months of data collection (before treatment), 2 months of treatment, and a further 2 months of data collection (after treatment). Comparison of outcomes to the initial baseline factors was made at the end of the 6 months for both an SMT group and a control group.
Setting: Chiropractic Research Center of Macquarie University.
Participants: One hundred twenty-seven volunteers between the ages of 10 and 70 years were recruited through media advertising. The diagnosis of migraine was made on the basis of the International Headache Society standard, with a minimum of at least one migraine per month.
Interventions: Two months of chiropractic SMT (diversified technique) at vertebral fixations determined by the practitioner (maximum of 16 treatments).
Main Outcome Measures: Participants completed standard headache diaries during the entire trial noting the frequency, intensity (visual analogue score), duration, disability, associated symptoms, and use of medication for each migraine episode.
Results: The average response of the treatment group (n = 83) showed statistically significant improvement in migraine frequency (P < .005), duration (P < .01), disability (P < .05), and medication use (P< .001) when compared with the control group (n = 40). Four persons failed to complete the trial because of a variety of causes, including change in residence, a motor vehicle accident, and increased migraine frequency. Expressed in other terms, 22% of participants reported more than a 90% reduction of migraines as a consequence of the 2 months of SMT. Approximately 50% more participants reported significant improvement in the morbidity of each episode.
Conclusion: The results of this study support previous results showing that some people report significant improvement in migraines after chiropractic SMT. A high percentage (>80%) of participants reported stress as a major factor for their migraines. It appears probable that chiropractic care has an effect on the physical conditions related to stress and that in these people the effects of the migraine are reduced.
In conclusion, chiropractic spinal manipulative therapy can be used effectively to help treat migraine, according to the research study. Furthermore, chiropractic care improved the individual’s overall health and wellness. The well-being of the human body as a whole is believed to be one of the biggest factors as to why chiropractic care is effective for migraine. Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Neck Pain
Neck pain is a common complaint which can result due to a variety of injuries and/or conditions. According to statistics, automobile accident injuries and whiplash injuries are some of the most prevalent causes for neck pain among the general population. During an auto accident, the sudden impact from the incident can cause the head and neck to jolt abruptly back-and-forth in any direction, damaging the complex structures surrounding the cervical spine. Trauma to the tendons and ligaments, as well as that of other tissues in the neck, can cause neck pain and radiating symptoms throughout the human body.
1. Vos T, Flaxman AD, Naghavi M et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990�2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012;380:2163�96. doi:10.1016/S0140-6736(12)61729-2[PubMed]
2. Russell MB, Kristiansen HA, Saltyte-Benth J et al. A cross-sectional population-based survey of migraine and headache in 21,177 Norwegians: the Akershus sleep apnea project. J Headache Pain 2008;9:339�47. doi:10.1007/s10194-008-0077-z[PMC free article][PubMed]
3. Steiner TJ, Stovner LJ, Katsarava Z et al. The impact of headache in Europe: principal results of the Eurolight project. J Headache Pain 2014;15:31 doi:10.1186/1129-2377-15-31[PMC free article][PubMed]
4. Headache Classification Subcommittee of the International Headache Society. The International Classification of Headache Disorders, 3rd edition (beta version). Cephalalgia 2013;33:629�808. doi:10.1177/0333102413485658[PubMed]
5. Russell MB, Iversen HK, Olesen J. Improved description of the migraine aura by a diagnostic aura diary. Cephalalgia 1994;14:107�17. doi:10.1046/j.1468-2982.1994.1402107.x[PubMed]
6. Russell MB, Olesen J. A nosographic analysis of the migraine aura in a general population. Brain 1996;119(Pt 2):355�61. doi:10.1093/brain/119.2.355[PubMed]
7. Olesen J, Burstein R, Ashina M et al. Origin of pain in migraine: evidence for peripheral sensitisation. Lancet Neurol 2009;8:679�90. doi:10.1016/S1474-4422(09)70090-0[PubMed]
8. Amin FM, Asghar MS, Hougaard A et al. Magnetic resonance angiography of intracranial and extracranial arteries in patients with spontaneous migraine without aura: a cross-sectional study. Lancet Neurol 2013;12:454�61. doi:10.1016/S1474-4422(13)70067-X[PubMed]
9. Wolff HGF. Headache and other head pain. 2nd edn Oxford: Oxford University Press, 1963.
10. Jensen K. Extracranial blood flow, pain and tenderness in migraine. Clinical and experimental studies. Acta Neurol Scand Suppl 1993;147:1�8. doi:10.1111/j.1748-1716.1993.tb09466.x[PubMed]
11. Svensson P, Ashina M. Human studies of experimental pain from muscles. In: Olesen J, Tfelt-Hansen P, Welch KMA et al., eds Headache. 3rd edn Lippincott Williams & Wilkins, 2006:627�35.
12. Ray BS, Wolff HG. Experimental studies on headache. Pain sensitive structures of the head and their significance in headache. Arch Surg 1940;41:813�56. doi:10.1001/archsurg.1940.01210040002001
13. Grande RB, Aaseth K, Gulbrandsen P et al. Prevalence of primary chronic headache in a population-based sample of 30- to 44-year-old persons. The Akershus study of chronic headache. Neuroepidemiology 2008;30:76�83. doi:10.1159/000116244[PubMed]
14. Aaseth K, Grande RB, Kvaerner KJ et al. Prevalence of secondary chronic headaches in a population-based sample of 30�44-year-old persons. The Akershus study of chronic headache. Cephalalgia 2008;28:705�13. doi:10.1111/j.1468-2982.2008.01577.x[PubMed]
16. Lundqvist C, Grande RB, Aaseth K et al. Dependence scores predict prognosis of medication overuse headache: a prospective cohort from the Akershus study of chronic headache. Pain 2012;153:682�6. doi:10.1016/j.pain.2011.12.008[PubMed]
17. Rasmussen BK, Jensen R, Olesen J. Impact of headache on sickness absence and utilisation of medical services: a Danish population study. J Epidemiol Community Health 1992;46:443�6. doi:10.1136/jech.46.4.443[PMC free article][PubMed]
18. Hu XH, Markson LE, Lipton RB et al. Burden of migraine in the United States: disability and economic costs. Arch Intern Med 1999;159:813�18. doi:10.1001/archinte.159.8.813[PubMed]
20. Andlin-Sobocki P, Jonsson B, Wittchen HU et al. Cost of disorders of the brain in Europe. Eur J Neurol 2005;12(Suppl 1):1�27. doi:10.1111/j.1468-1331.2005.01202.x[PubMed]
24. Parker GB, Pryor DS, Tupling H. Why does migraine improve during a clinical trial? Further results from a trial of cervical manipulation for migraine. Aust NZ J Med 1980;10:192�8. doi:10.1111/j.1445-5994.1980.tb03712.x[PubMed]
25. Nelson CF, Bronfort G, Evans R et al. The efficacy of spinal manipulation, amitriptyline and the combination of both therapies for the prophylaxis of migraine headache. J Manipulative Physiol Ther 1998;21:511�19. [PubMed]
26. Tuchin PJ, Pollard H, Bonello R. A randomized controlled trial of chiropractic spinal manipulative therapy for migraine. J Manipulative Physiol Ther 2000;23:91�5. doi:10.1016/S0161-4754(00)90073-3[PubMed]
28. Vernon HT. The effectiveness of chiropractic manipulation in the treatment of headache: an exploration in the literature. J Manipulative Physiol Ther 1995;18:611�17. [PubMed]
29. Fernandez-de-las-Penas C, Alonso-Blanco C, San-Roman J et al. Methodological quality of randomized controlled trials of spinal manipulation and mobilization in tension-type headache, migraine, and cervicogenic headache. J Orthop Sports Phys Ther 2006;36:160�9. doi:10.2519/jospt.2006.36.3.160[PubMed]
31. Chaibi A, Russell MB. Manual therapies for primary chronic headaches: a systematic review of randomized controlled trials. J Headache Pain 2014;15:67 doi:10.1186/1129-2377-15-67[PMC free article][PubMed]
32. Tfelt-Hansen P, Block G, Dahlof C et al. International Headache Society Clinical Trial Subcommittee. Guidelines for controlled trials of drugs in migraine: second edition. Cephalalgia 2000;20:765�86. doi:10.1046/j.1468-2982.2000.00117.x[PubMed]
33. Silberstein S, Tfelt-Hansen P, Dodick DW et al. , Task Force of the International Headache Society Clinical Trial Subcommittee . Guidelines for controlled trials of prophylactic treatment of chronic migraine in adults. Cephalalgia 2008;28:484�95. doi:10.1111/j.1468-2982.2008.01555.x[PubMed]
34. Kerr FW. Central relationships of trigeminal and cervical primary afferents in the spinal cord and medulla. Brain Res 1972;43:561�72. doi:10.1016/0006-8993(72)90408-8[PubMed]
36. McLain RF, Pickar JG. Mechanoreceptor endings in human thoracic and lumbar facet joints. Spine (Phila Pa 1976) 1998;23:168�73. doi:10.1097/00007632-199801150-00004[PubMed]
37. Vernon H. Qualitative review of studies of manipulation-induced hypoalgesia. J Manipulative Physiol Ther 2000;23:134�8. doi:10.1016/S0161-4754(00)90084-8[PubMed]
38. Vicenzino B, Paungmali A, Buratowski S et al. Specific manipulative therapy treatment for chronic lateral epicondylalgia produces uniquely characteristic hypoalgesia. Man Ther 2001;6:205�12. doi:10.1054/math.2001.0411[PubMed]
39. Boal RW, Gillette RG. Central neuronal plasticity, low back pain and spinal manipulative therapy. J Manipulative Physiol Ther 2004;27:314�26. doi:10.1016/j.jmpt.2004.04.005[PubMed]
40. De Camargo VM, Alburquerque-Sendin F, Berzin F et al. Immediate effects on electromyographic activity and pressure pain thresholds after a cervical manipulation in mechanical neck pain: a randomized controlled trial. J Manipulative Physiol Ther 2011;34:211�20. doi:10.1016/j.jmpt.2011.02.002[PubMed]
41. Moher D, Hopewell S, Schulz KF et al. CONSORT 2010 explanation and elaboration: updated guidelines for reporting parallel group randomised trials. BMJ 2010;340:c869 doi:10.1136/bmj.c869[PMC free article][PubMed]
42. Hoffmann TC, Glasziou PP, Boutron I et al. Better reporting of interventions: template for intervention description and replication (TIDieR) checklist and guide. BMJ 2014;348:g1687 doi:10.1136/bmj.g1687[PubMed]
43. Headache Classification Subcommittee of the International Headache Society. The International Classification of Headache Disorders: 2nd edition. Cephalalgia 2004;24(Suppl 1):9�10. doi:10.1111/j.1468-2982.2003.00824.x[PubMed]
44. French HP, Brennan A, White B et al. Manual therapy for osteoarthritis of the hip or knee – a systematic review. Man Ther 2011;16:109�17. doi:10.1016/j.math.2010.10.011[PubMed]
45. Cassidy JD, Boyle E, Cote P et al. Risk of vertebrobasilar stroke and chiropractic care: results of a population-based case-control and case-crossover study. Spine (Phila Pa 1976) 2008;33(4Suppl):S176�S83. doi:10.1097/BRS.0b013e3181644600[PubMed]
47. Russell MB, Rasmussen BK, Brennum J et al. Presentation of a new instrument: the diagnostic headache diary. Cephalalgia 1992;12:369�74. doi:10.1111/j.1468-2982.1992.00369.x[PubMed]
48. Lundqvist C, Benth JS, Grande RB et al. A vertical VAS is a valid instrument for monitoring headache pain intensity. Cephalalgia 2009;29:1034�41. doi:10.1111/j.1468-2982.2008.01833.x[PubMed]
49. Bang H, Ni L, Davis CE. Assessment of blinding in clinical trials. Control Clin Trials 2004;25:143�56. doi:10.1016/j.cct.2003.10.016[PubMed]
51. Silberstein SD, Neto W, Schmitt J et al. Topiramate in migraine prevention: results of a large controlled trial. Arch Neurol 2004;61:490�5. doi:10.1001/archneur.61.4.490[PubMed]
52. Bendtsen L, Jensen R, Olesen J. A non-selective (amitriptyline), but not a selective (citalopram), serotonin reuptake inhibitor is effective in the prophylactic treatment of chronic tension-type headache. J Neurol Neurosurg Psychiatry 1996;61:285�90. doi:10.1136/jnnp.61.3.285[PMC free article][PubMed]
53. Hagen K, Albretsen C, Vilming ST et al. Management of medication overuse headache: 1-year randomized multicentre open-label trial. Cephalalgia 2009;29:221�32. doi:10.1111/j.1468-2982.2008.01711.x[PubMed]
54. Hancock MJ, Maher CG, Latimer J et al. Selecting an appropriate placebo for a trial of spinal manipulative therapy. Aust J Physiother 2006;52:135�8. doi:10.1016/S0004-9514(06)70049-6[PubMed]
55. Meissner K, Fassler M, Rucker G et al. Differential Effectiveness of Placebo Treatments: A Systematic Review of Migraine Prophylaxis. JAMA Inter Med 2013;173:1941�51. doi:10.1001/jamainternmed.2013.10391[PubMed]
56. Taylor JA. Full-spine radiography: a review. J Manipulative Physiol Ther 1993;16:460�74. [PubMed]
57. International Chiropractic Assocoation Practicing Chiropractors� Committee on Radiology Protocols (PCCRP) for biomechanical assessment of spinal subluxation in chiropractic clinical practice. Secondary International Chiropractic Assocoation Practicing Chiropractors� Committee on Radiology Protocols (PCCRP) for biomechanical assessment of spinal subluxation in chiropractic clinical practice 2009. http://www.pccrp.org/
58. Cracknell DM, Bull PW. Organ dosimetry in spinal radiography: a comparison of 3-region sectional and full-spine techniques. Chiropr J Austr 2006;36:33�9.
59. Borretzen I, Lysdahl KB, Olerud HM. Diagnostic radiology in Norway trends in examination frequency and collective effective dose. Radiat Prot Dosimetry 2007;124:339�47. doi:10.1093/rpd/ncm204[PubMed]
60. Leboeuf-Yde C, Fejer R, Nielsen J et al. Pain in the three spinal regions: the same disorder? Data from a population-based sample of 34,902 Danish adults. Chiropr Man Ther 2012;20:11 doi:10.1186/2045-709X-20-11[PMC free article][PubMed]
61. Ioannidis JP, Evans SJ, Gotzsche PC et al. Better reporting of harms in randomized trials: an extension of the CONSORT statement. Ann Intern Med 2004;141:781�8. doi:10.7326/0003-4819-141-10-200411160-00009[PubMed]
Being involved in an automobile accident can cause damage or injury to the complex structures of the cervical spine which can go unnoticed for months if left untreated. Medically referred to as whiplash-associated disorders, or whiplash, symptoms resulting after an auto accident can often take days to even weeks or months to manifest. Persistent neck pain that lasts for more than 3 months then becomes chronic neck pain, an issue which can be difficult to manage if not treated accordingly. Chronic neck pain may also result due to other underlying issues. The following article demonstrates which types of treatment methods can help relieve chronic neck pain symptoms and its associated complications, including capsular ligament laxity and cervical instability.
Chronic Neck Pain: Making the Connection Between Capsular Ligament Laxity and Cervical Instability
Abstract
The use of conventional modalities for chronic neck pain remains debatable, primarily because most treatments have had limited success. We conducted a review of the literature published up to December 2013 on the diagnostic and treatment modalities of disorders related to chronic neck pain and concluded that, despite providing temporary relief of symptoms, these treatments do not address the specific problems of healing and are not likely to offer long-term cures. The objectives of this narrative review are to provide an overview of chronic neck pain as it relates to cervical instability, to describe the anatomical features of the cervical spine and the impact of capsular ligament laxity, to discuss the disorders causing chronic neck pain and their current treatments, and lastly, to present prolotherapy as a viable treatment option that heals injured ligaments, restores stability to the spine, and resolves chronic neck pain.
The capsular ligaments are the main stabilizing structures of the facet joints in the cervical spine and have been implicated as a major source of chronic neck pain. Chronic neck pain often reflects a state of instability in the cervical spine and is a symptom common to a number of conditions described herein, including disc herniation, cervical spondylosis, whiplash injury and whiplash associated disorder, postconcussion syndrome, vertebrobasilar insufficiency, and Barr�-Li�ou syndrome.
When the capsular ligaments are injured, they become elongated and exhibit laxity, which causes excessive movement of the cervical vertebrae. In the upper cervical spine (C0-C2), this can cause a number of other symptoms including, but not limited to, nerve irritation and vertebrobasilar insufficiency with associated vertigo, tinnitus, dizziness, facial pain, arm pain, and migraine headaches. In the lower cervical spine (C3-C7), this can cause muscle spasms, crepitation, and/or paresthesia in addition to chronic neck pain. In either case, the presence of excessive motion between two adjacent cervical vertebrae and these associated symptoms is described as cervical instability.
Therefore, we propose that in many cases of chronic neck pain, the cause may be underlying joint instability due to capsular ligament laxity. Currently, curative treatment options for this type of cervical instability are inconclusive and inadequate. Based on clinical studies and experience with patients who have visited our chronic pain clinic with complaints of chronic neck pain, we contend that prolotherapy offers a potentially curative treatment option for chronic neck pain related to capsular ligament laxity and underlying cervical instability.
In the realm of pain management, an ever-growing number of treatment-resistant patients are being left with relatively few conventional treatment options that effectively and permanently relieve their chronic pain symptoms. Chronic cervical spine pain is particularly challenging to treat, and data regarding the long-term efficacy of traditional therapies has been extremely discouraging [1]. The prevalence of neck pain in the general population has been reported to range between 30% and 50%, with women over 50 making up the larger portion [1-3]. Although many of these cases resolve with time and require minimal intervention, the recurrence rate of neck pain is high, and about one-third of people will suffer from chronic neck pain (defined as pain that persists longer than 6 months), and 5% will develop significant disability and reduction in quality of life [2, 4]. For this group of chronic pain patients, modern medicine offers few options for long-term recovery.
Treatment protocols for acute and sub-acute neck pain are standard and widely agreed upon [1, 2]. However, conventional treatments for chronic neck pain remain debatable and include interventions such as use of nonsteroidal anti-inflammatory drugs (NSAIDs) and narcotics for pain management, cervical collars, rest, physiotherapy, manual therapy, strengthening exercises, and nerve blocks. Furthermore, the literature on long-term treatment outcomes has been inconclusive at best [5-9]. Chronic neck pain due to whiplash injury or whiplash associated disorder (WAD) is particularly resistant to long-term treatment; conventional treatment for these conditions may give temporary relief but long-term outcomes have been disappointing [10].
In light of the poor treatment options and outcomes for chronic neck pain, we propose that in many of these cases, the underlying condition may be related to capsular ligament laxity and subsequent joint instability of the cervical spine. Should this be the case and joint instability is the fundamental problem causing chronic neck pain, a new treatment approach may be warranted.
The diagnosis of chronic neck pain due to cervical instability is particularly challenging. In most cases, diagnostic tools for detecting cervical instability have been inconsistent and lack specificity [11-15], and are therefore inadequate. A better understanding of the pathogenesis of cervical instability may better enable practitioners to recognize and treat the condition more effectively. For instance, when cervical instability is related to injury of soft tissue (eg, ligaments) alone and not fracture, the treatment modality should be one that stimulates the involved soft tissue to regenerate and repair itself.
In that context, comprehensive dextrose prolotherapy offers a promising treatment option for resolving cervical instability and the subsequent pain and disability it causes. The distinct anatomy of the cervical spine and the pathology of cervical instability described herein underlie the rationale for treating the condition with prolotherapy.
Anatomy
The cervical spine consists of the first seven vertebrae in the spinal column and is divided into two segments, the upper cervical (C0-C2) and lower cervical (C3-C7) regions. Despite having the smallest vertebral bodies, the cervical spine is the most mobile segment of the entire spine and must support a high degree of movement. Consequently, it is highly reliant on ligamentous tissue for stabilizing the neck and spinal column, as well as for controlling normal joint motion; as a result, the cervical spine is highly susceptible to injury.
The upper cervical spine consists of C0, called the occiput, and the first two cervical vertebrae, C1 and C2, or atlas and axis, respectively. C1 and C2 are more specialized than the rest of the cervical vertebrae. C1 is ring-shaped and lacks a vertebral body. C2 has a prominent vertebral body called the odontoid process or dens which acts as a pivot point for the C1 ring [16]. This pivoting motion (Fig. ?1), coupled with the lack of intervertebral discs in the upper cervical spine, allows for more movement and rotation of the joint, thus facilitating mobility rather than stability [17]. Collectively, the upper cervical spine is responsible for 50% of total neck flexion and extension at the atlanto-occipital (C0-C1) joint, as well as 50% of total neck rotation that occurs at the atlanto-axial joint (C1-C2) [16]. This motion is possible because the atlas (C1) rotates around the axis (C2) via the dens and the anterior arch of the atlas.
Figure 1: Atlanto-axial rotational instability. The atlas is shown in the rotated position on the axis. The pivot is the eccentrically placed odontoid process. In rotation, the wall of the vertebral foramen of Cl decreases the opening of the spinal canal between Cl and C2. This can potentially cause migraine headaches, C2 nerve root impingement, dizziness, vertebrobasilar insufficiency, ‘drop attacks; neck-tongue syndrome, Barr�-Li�ou syndrome, severe neck pain, and tinnitus.
The intrinsic, passive stability of the spine is provided by the intervertebral discs and surrounding ligamentous structures. The upper cervical spine is stabilized solely by ligaments, including the transverse, alar, and capsular ligaments. The transverse ligament runs behind the dens, originating on a small tubercle on the medial side of a lateral mass of the atlas and inserting onto the identical tubercle on the other side. Thus, the transverse ligament restricts flexion of the head and anterior displacement of the atlas. The left and right alar ligaments originate from the posterior dens and attach to the medial occipital condyles on the ipsilateral sides. They work to limit axial rotation and are under the greatest tension in rotation and flexion. By holding C1 and C2 in proper position, the transverse and alar ligaments help to protect the spinal cord, brain stem, and nervous system from excess movement in the upper cervical spine [18].
The lower cervical spine, while less specialized, allows for the remaining 50% of neck flexion, extension, and rotation. Each vertebra in this region (C3-C7) has a vertebral body, in between which lies an intervertebral disc, the largest avascular structure of the body. This disc is a piece of fibrocartilage that helps cushion the joints and allows for more stability and is comprised of an inner gelatinous nucleus pulposus, which is surrounded by an outer, fibrous annulus fibrosus. The nucleus pulposus is designed to sustain compression loads and the annulus fibrosus, to resist tension, shear and torsion [19]. The annulus fibrosus is thought to determine the proper functioning of the entire intervertebral disc [20] and has been described as a lamellar structure consisting of 15-26 distinct concentric fibrocartilage layers that constitute a criss-crossing fiber matrix [19]. However, the form of this structure has been disputed. A microdissection study using cadavers reported that the cervical annulus fibrosus does not consist of concentric laminae of collagen fibers as it does in lumbar discs. Instead, the authors contend that the three-dimensional architecture of the cervical annulus fibrosus is more like that of a crescentic anterior interosseous ligament surrounding the nucleus pulposus [21].
In addition to the discs, multiple ligaments and the two synovial joints on each pair of adjacent vertebrae (facet joints) allow for controlled, fully three dimensional motions. Capsular ligaments wrap around each facet joint, which help to maintain stability during neck rotation. Each vertebra in the lower cervical spine (in addition to C2) contains a spinous process that serves as an attachment site for the interspinal ligaments. These tissues connect adjacent spinous processes and limit flexion of the cervical spine. Anteriorly, they meet with the ligamentum flavum.
Three other ligaments, the ligamentum flavum, anterior longitudinal ligament (ALL), and posterior longitudinal ligament (PLL), help to stabilize the cervical spine during motion and protect against excess flexion and extension of the cervical vertebrae. From C1-C2 to the sacrum, the ligamentum flava run down the posterior aspect of the spinal canal and join the laminae of adjacent vertebrae while helping to maintain proper neck posture. The ALL and PLL both run alongside the vertebral bodies. The ALL begins at the occiput and runs anteriorly to the anterior sacrum, helping to stabilize the vertebrae and intervertebral discs and limit spinal extension. The PLL also helps to stabilize the vertebrae and intervertebral discs, as well as limit spinal flexion. It extends from the body of the axis to the posterior sacrum and runs within the anterior aspect of the spinal canal across from the ligamentum flava.
A spinous process and two transverse processes emanate off the neural arch (or vertebral arch) which lies at the posterior aspect of the cervical vertebral column. The transverse processes are bony prominences that protrude postero-laterally and serve as attachment sites for various muscles and ligaments. With the exception of C7, each of these processes has a foramen which allows for passage of the vertebral artery towards the brain; the C7 transverse process has foramina which allow for passage of the vertebral vein and sympathetic nerves [22]. The transverse processes of the cervical vertebrae are connected via the intertransverse ligaments; each attaches a transverse process to the one below and helps to limit lateral flexion of the cervical spine.
Facet Joints
The inferior articular process of the superior cervical vertebra, except for C0-C1, and the superior articular process of the inferior cervical vertebra join to form the facet joints of the cervical spine; in the case of C0-C1, the inferior articular process of C1 joins the occipital condyles. Also referred to as zygapophyseal joints (Fig. ?2), the facet joints are diarrthrodial, meaning they function similar to the knee joint in that they contain synovial cells and joint fluid and are surrounded by a capsule. They also contain a meniscus which helps to further cushion the joint, and like the knee, are lined by articular cartilage and surrounded by capsular ligaments, which stabilize the joint. These capsular ligaments hold adjacent vertebrae to one another, and the articular cartilage therein is aligned such that its opposing tissue surfaces provide for a low-friction environment [23].
Figure 2: Typical Z (zygapophyseal/ facet) joint. Each facet joint has articular cartilage, the synovium where synovial fluid is produced, and a meniscus.
There is some dissimilarity in facet joint anatomy between the upper and lower cervical spine. Even in the upper cervical region, C0-C1 and C1-C2 facet joints differ anatomically. At C0-C1, the convex shape of the occipital condyles enables them to fit into the concave surface of the inferior articular process. The C1-C2 facet joints are oriented cranio-caudally, meaning they run more parallel to their transverse processes. As such, their capsular ligaments are normally relatively lax, and thus, are inherently less stable and meant to facilitate mobility (i.e., rotation) [23, 24].
In contrast, the facet joints of the lower cervical spine are positioned at more of an angle. In the transverse plane, the angles of the right and left C2-C3 facet joints are estimated to be 32� to 65� and 32� to 60�, respectively, while those of the C6-C7 facet joints are typically steeper at 45� to 75� and 50� to 78� [25]. As the cervical spine extends downward, the angle of the facet joint becomes bigger such that the joint slopes backwards and downwards. Thus, the facet joints of the lower cervical spine have progressively less rotation than those of the upper cervical spine. Furthermore, the presence of intervertebral discs helps give the lower cervical spine more stability.
Nevertheless, injury to any of the facet joints can cause instability to the cervical spine. Researchers have found there is a continuum between the amount of trauma and degree of instability to the cervical facets, with greater trauma causing a higher degree of facet instability [26-28].
Cervical Capsular Ligaments
The capsular ligaments are extremely strong and serve as the main stabilizing tissue in the spinal column. They lie close to the intervertebral centers of rotation and provide significant stability in the neck, especially during axial rotation [29]; consequently, they serve as essential components for ensuring neck stability with movement. The capsular ligaments have a high peak force and elongation potential, meaning they can withstand large forces before rupturing. This was demonstrated in a dynamic mechanical study in which the capsular ligaments and ligamentum flavum were shown to have the highest average peak force, up to 220 N and 244 N, respectively [30]. This was reported as considerably greater than the force shown in the anterior longitudinal ligament and middle third disc.
While much has been reported about the strength of the capsular ligaments as related to cervical stability, when damaged, these ligaments lose their strength and are unable to support the cervical spine properly. For instance, in an animal study, it was shown that sequential removal of sheep capsular ligaments and cervical facets caused an undue increase in range of motion, especially in axial rotation, flexion and extension with caudal progression [31]. Human cadaver studies have also indicated that transection or injury of joint capsular ligaments significantly increases axial rotation and lateral flexion [32, 33]. Specifically, the largest increase in axial rotation with damage to a unilateral facet joint was 294% [33].
Capsular ligament laxity can occur instantaneously as a single macrotrauma, such as a whiplash injury, or can develop slowly as cumulative microtraumas, such as those from repetitive forward or bent head postures. In either case, the cause of injury occurs through similar mechanisms, leading to capsular ligament laxity and excess motion of the facet joints, which often results in cervical instability. When ligament laxity develops over time, it is defined as �creep� (Fig. ?3) and refers to the elongation of a ligament under a constant or repetitive stress [34]. While this constitutes low-level subfailure ligament injuries, it may represent the vast majority of cervical instability cases and can potentially incapacitate people due to disabling pain, vertigo, tinnitus or other concomitant symptoms of cervical instability. Such symptoms can be caused by elongation-induced strains of the capsular ligaments; these strains can progress to subsequent subfailure tears in the ligament fibers or to laxity in the capsular ligaments, leading to instability at the level of the cervical facet joints [35]. This is most evident when the neck is rotated (ie, looking to the left or right) and that movement�causes a �cracking� or �popping� sound. Clinical instability indicates that the spine is unable to maintain normal motion and function between vertebrae under normal physiological loads, inducing irritation to nerves, possible structural deformation, and/or incapacitating pain.
Figure 3: Ligament laxity and creep. When ligaments are under a constant stress, they display creep behavior. Creep refers to a time-dependent increase in strain and causes ligaments to “stretch out” over time.
Furthermore, the capsular ligaments surrounding the facet joints are highly innervated by mechanoreceptive and nociceptive free nerve endings. Hence, the facet joint has long been considered the primary source of chronic spinal pain [36-38]. Additionally, injury to these nerves has been shown to affect the overall joint function of the facet joints [39]. Therefore, injury to the capsular ligaments and subsequent nerve endings could explain the prevalence of chronic pain and joint instability in the facet joints of the cervical spine.
Cervical Instability
Clinical instability is not to be confused with hypermobility. In general, instability implies a pathological condition with resultant symptoms, whereas joint hypermobility alone does not (Fig. ?4). Clinical instability refers to a loss of motion stiffness in a particular spinal segment when the application of force to it produces greater displacement(s) than would otherwise be seen in a normal structure. In clinical instability, symptoms such as pain and muscle spasms can thus be experienced within a person�s range of motion, not just at its furthest extension point. These muscle spasms can cause intense pain and are the body�s response to cervical instability in that the ligaments act as sensory organs involved in ligamento-muscular reflexes. The ligamento-muscular reflex is a protective reflex emanating from mechanoreceptors (ie, pacinian corpuscles, golgi tendon organs, and ruffini endings) in the ligaments and transmitted to the muscles. Subsequent activation of these muscles helps to preserve joint stability, either directly by muscles crossing the joint or indirectly by muscles that do not cross the joint but limit joint motion [40].
Figure 4: Cervical spinal motion continuum and role of prolotherapy. When minor or moderate spinal instability occurs, treatment with prolotherapy may be of benefit in alleviating symptoms and restoring normal cervical joint function.
In a clinically unstable joint where neurologic insult is present, it is presumed that the joint has undergone more severe damage in its stabilizing structures, which may include the vertebrae themselves. In contrast, joints that are hypermobile demonstrate increased segmental mobility but are able to maintain their stability and function normally under physiological loads [41].
Clinical instability can be classified as mild, moderate or severe, with the later being associated with catastrophic injury. Minor injuries of the cervical spine are those involving soft tissues alone without evidence of fracture and are the most common causes of cervical instability. Mild or moderate clinical instability is that which is without neurologic (somatic) injury and is typically due to cumulative micro-traumas.
Diagnosis of Cervical Instability
Cervical instability is a diagnosis based primarily on a patient�s history (ie, symptoms) and physical examination because there is yet to be standardized functional X-rays or imaging able to diagnose cervical instability or detect ruptured ligamentous tissue without the presence of bony lesions [24]. For example, in one autopsy study of cryosection samples of the cervical spine, [42] only one out of ten gross ligamentous disruptions was evident on x-ray. Furthermore, there is often little correlation between the degree of instability or hypermobility shown on radiographic studies and clinical symptoms [43-45]. Even after severe whiplash injuries, plain radiographs are usually normal despite clinical findings indicating the presence of soft tissue damage.
However, functional computerized tomography (fCT) and magnetic resonance imaging (fMRI) scans and digital motion x-ray (DMX) are able to adequately depict cervical instability pathology [46, 47]. Studies using fCT for diagnosing soft tissue ligament or post-whiplash injuries have demonstrated the ability of this technique to show excess atlanto-occipital or atlanto-axial movement during axial rotation [48, 49]. This is especially pertinent when patients have signs and symptoms of cervical instability, yet have normal MRIs in a neutral position.
Functional imaging technology, as opposed to static standard films, is necessary for adequate radiologic depiction of instability in the cervical spine because they provide dynamic imaging of the neck during movement and are helpful for evaluating the presence and degree of cervical instability (Fig. ?5). There are also specialized physical examination tests specific for upper cervical instability, such as the Sharp-Purser test, upper cervical flexion test, and cervical flexion-rotation test.
Figure 5: 3D CT scan of upper cervical spine. C1-C2 instability can easily be seen in the patient, as 70% of C1 articular facet is subluxed posteriorly (arrow) on C2 facet when the patient rotates his head (turns head to the left then the right).
Upper Cervical Pathology and Instability
Although not usually apparent radiographically, injury to the ligaments and soft tissues of C0-C2 from head or neck trauma is more likely than are cervical fractures or subluxation of bones [50, 51]. Ligament laxity across the C0-C1-C2 complex is primarily caused by rotational movements, especially those involving lateral bending and axial rotation [52-54]. With severe neck traumas, especially those with rotation, up to 25% of total lesions can be attributed to ligament injuries of C0-C2 alone. Although some ligament injuries in the C0-C2 region can cause severe neurological impairment, the majority involve sub-failure loads to the facet joints and capsular ligaments, which are the primary source of most chronic pain in post-neck trauma [26, 55].
Due to its lack of osseous stability, the upper cervical spine is also vulnerable to injury by high velocity manipulation. The capsular ligaments of the atlanto-axial joint are especially susceptible to injury from rotational thrusts, and thus, may be at risk during mechanically mediated manipulation. The capsular ligaments in the occipto-atlantal joint function as joint stabilizers and can also become injured due to excessive or abnormal forces [46].
Excessive tension on the capsular ligaments can cause upper cervical instability and related neck pain [56]. Capsular ligament tension is increased during abnormal postures, causing elongation of the capsular ligaments, with magnitudes increased by up to 70% of normal [57]. Such excessive ligament elongation induces laxity to the facet joints, which puts the cervical spine more at risk for further degenerative changes and instability. Therefore, capsular ligament injury appears to cause upper cervical instability because of laxity in the stabilizing structure of the facet joints [58].
Cervical Pain Versus Cervical Radiculopathy
According to the International Association for the Study of Pain (IASP), cervical spinal pain is pain perceived as anywhere in the posterior region of the cervical spine, defining it further as pain that is �perceived as arising from anywhere within the region bounded superiorly by the superior nuchal line, inferiorly by an imaginary transverse line through the tip of the first thoracic spinous process, and laterally by sagittal planes tangential to the lateral borders of the neck� [59]. Similarly, cervical pain is divided equally by an imaginary transverse plane into upper cervical pain and lower cervical pain. Suboccipital pain is that pain located between superior nuchal line and an imaginary transverse line through the tip of the second cervical spinous process. Likewise, cervico-occipital pain is perceived as arising in the cervical region and extending over the occipital region of the skull. These sources of pain could be a result of underlying cervical instability.
The IASP defines radicular pain as that arising in a limb or the trunk wall, caused either by ectopic activation of nociceptive afferent fibers in a spinal nerve or its roots or by other neuropathic mechanisms, and may be episodic, recurrent, or sudden [59]. Clinically, there is a 30% rate of radicular symptoms during axial rotation in those with rotator instabilities [60]. Thus, radicular pain may also be a result of underlying cervical instability.
With capsular ligament laxity, hypertrophic facet joint changes occur (including osteophytosis) as cervical degeneration progresses, causing encroachment on cervical nerve roots as they exit the spine through the neural foramina. This condition is called cervical radiculopathy and manifests as stabbing pain, numbness, and/or tingling down the upper extremity in the area of the affected nerve root.
The neural foramina lie between the intervertebral disc and the joints of Luschka (uncovertebral joints) anteriorly and the facet joint posteriorly. Their superior and inferior borders are the pedicles of adjacent vertebral bodies. Cervical nerve roots there are vulnerable to compression or injury by the facet joints posteriorly or by the joints of Luschka and the intervertebral disc anteriorly.
Cadaver studies have demonstrated that cervical nerve roots take up as much as 72% of the space in the neural foramina [61]. Normally, this provides ample room for the nerves to function optimally. However, if the cervical spine and capsular ligaments are injured, facet joint hypertrophy and degeneration of the cervical discs can occur. Over time, this causes narrowing of the neural foramina (Fig. ?6) and a decrease in space for the nerve root. In the event of another ligament injury, instability of the hypertrophied bones can occur and further reduce the patency of the neural foramen.
Figure 6: Digital motion X-ray demonstrating multi-level cervical instability. Neural foraminal narrowing is shown at two levels during lateral extension versus lateral flexion.
Cervical radiculopathy from a capsular ligament injury typically produces intermittent radicular symptoms which become more noticeable when the neck is moved in a certain direction, such as during rotation, flexion or extension. These movements can cause encroachment on cervical nerve roots and subsequent paresthesia along the pathway therein of the affected nerve and may be why evidence of cervical radiculopathy does not show up on standard MRI or CT scans.
When disc herniation is the cause of cervical radiculopathy, it typically presents with acute onset of severe neck and arm pain unrelieved by any position and often results in encroachment on a cervical nerve root. While disc herniation can easily be seen on routine (non-functional) MRI or CT scans, evidence of radiculopathy from cervical instability cannot. Most cases of acute radiculopathy due to disc herniation resolve with non-surgical active or passive therapies, but some patients continue to have clinically significant symptoms, in which case surgical treatments such as anterior cervical decompression with fusion or posterior cervical laminoforaminotomy can be performed [62]. Cervical radiculopathy is also strongly associated with spondylosis, a disease generally attributed to aging that involves an overall degeneration of the cervical spine. The disorder is characterized by degenerative changes in the intervertebral disc, osteophytosis of the vertebral bodies, and hypertrophy of the facet joints and laminar arches. Since more than one cervical spine segment is usually affected in spondylosis, the symptoms of radiculopathy are more diffuse than those typical of unilateral soft disc herniation and present as neck, mid-upper back, and arm pain with paresthesia.
Dr. Alex Jimenez’s Insight
“I was involved in an automobile accident that left me with chronic neck pain. What could be causing my painful and persistent neck pain symptoms?”�Being involved in an automobile accident can be a traumatic experience, resulting in both mental and physical harm. Whiplash-associated injuries are some of the most common diagnosis behind reported cases of chronic neck pain after an auto accident. During a car crash, the force of the impact can abruptly jerk the head back-and-forth, stretching the complex structures around the cervical spine beyond their natural range, causing damage or injury.The following article provides an overview of chronic neck pain, its mechanism of injury and effective treatment methods for neck pain.
Cervical Spondylosis: the Instability Connection
Spondylosis has previously been described as occurring in three stages: the dysfunctional stage, the unstable stage, and the stabilization stage (Fig. ?7) [63]. Spondylosis begins with repetitive trauma, such as rotational strains or compressive forces to the spine. This causes injury to the facet joints which can compromise the capsular ligaments. The dysfunctional phase is characterized by capsular ligament injuries and subsequent cartilage degeneration and synovitis, ultimately leading to abnormal motion in the cervical spine. Over time, facet joint dysfunction intensifies as capsular laxity occurs. This stretching response can cause cervical instability, marking the unstable stage. During this progression, ongoing degeneration is occurring in the intervertebral discs, along with other parts of the cervical spine. Ankylosis (stiffening of the joints) can also occur at the unstable cervical spine segment, and rarely, causes entrapment of nearby spinal nerves. The stabilization phase occurs with the formation of marginal osteophytes as the body tries to heal the spine. These bridging bony deposits can lead to a natural fusion of the affected vertebrae [64].
Figure 7: Cervical OA: The 3 phases of the degenerative cascade. Used with permission from: Kramer WC, et al. Pathogenetic mechanisms of posttraumatic osteoarthritis: opportunities for early intervention. Int J Clin Exp Me d. 2011; 4(4): 285-298.
The degenerative cascade, however, begins long before symptoms become evident. Initially, spondylosis develops silently and is asymptomatic [65]. When symptoms of cervical spondylosis do develop, they are generally nonspecific and include neck pain and stiffness [66]. Only rarely do neurologic symptoms develop (ie, radiculopathy or myelopathy), and most often they occur in people with congenitally narrowed spinal canals [67]. Physical exam findings are often limited to restricted range of neck motion and poorly localized tenderness. Clinical symptoms commonly manifest when a new cervical ligament injury is superimposed on the underlying degeneration. In patients with spondylosis and underlying capsular ligament laxity, cervical radiculopathy is more likely to occur because the neural foramina may already be narrowed from facet joint hypertrophy and disc degeneration, enabling any new injury to more readily pinch on an exiting nerve root.
Thus, there are compelling reasons to believe that facet joint/capsular ligament injuries in the cervical spine may be an etiological basis for the degenerative cascade in cervical spondylosis and may be responsible for the attendant cervical instability. Animal models used for initiating disc degeneration in research studies have shown the induction of spinal instability through injury of the facet joints [68, 69]. In similar models, capsular ligament injuries of the facet joints caused multidirectional instability of the cervical spine, greatly increasing axial rotation motion correlating with cervical disc injuries [31, 28, 70, 71]. Using human specimens, surgical procedures such as discectomy have been shown to cause an immediate increase in motion of the segments involved [72]. Stabilization procedures such as neck fusion have been known to create increased pressure on the adjacent cervical spinal segments; this is referred to as adjacent segment disease. This can develop when the loss of motion from cervical fusion causes greater shearing and increased rotation and traction stress on adjacent vertebrae at the facet joints [73-75]. Thus, instability can �travel� up or down from the fused segment, furthering disc degeneration. These findings support the theory that iatrogenic-introduced stress and instability at adjacent spinal segments contribute to the pathogenesis of cervical spondylosis [74].
Whiplash Trauma
Damage to cervical ligaments from whiplash trauma has been well studied, yet these injuries are still often difficult to diagnose and treat. Standard x-rays often do not reveal present injury to the cervical spine and as a consequence, these injuries go unreported and patients are left without proper treatment for their condition [76]. Part of the difficulty lies in the fact that major injury to the cervical spine may only produce minor symptoms in some patients, whereas minor injury may produce more severe symptoms in others [77]. These symptoms include acute and/or chronic neck pain, headache, dizziness, vertigo and paresthesia in the upper extremities [78, 79].
MRI and autopsy studies have both shown an association between chronic symptoms in whiplash patients and injuries to the cervical discs, ligaments and facet joints [42, 80]. Success in relieving neck pain in whiplash patients has been documented by numerous clinical studies using nerve block and radiofrequency ablation of facet joint afferents, including capsular ligament nerves, such that increased interest has developed regarding the relationships between injury to the facet joints and capsular ligaments and post-whiplash dysfunction and related symptoms [36, 81].
Multiple studies have implicated the cervical facet joint and its capsule as a primary anatomical site of injury during whiplash exposure to the neck [55, 57, 82, 83]. Others have shown that injury to the cervical facet joints and capsular ligaments are the most common cause of pain in post-whiplash patients [84-86]. Cinephotographic and cineradiographic studies of both cadavers and human subjects show that under the conditions of whiplash, a resultant high impact force occurs in the cervical facet joints, leading to their injury and the possibility of cervical spine instability [84].
In whiplash trauma, up to 10 times more force is absorbed in the capsular ligaments versus the intervertebral disc [30]. Unlike the disc, the facet joint has a much smaller area in which to disperse this force. Ultimately, the capsular ligaments become elongated, resulting in abnormal motions in the spinal segments affected [30, 87]. This sequence has been documented with both in vitro and in vivo studies of segmental motion characteristics after torsional loads and resultant disc degeneration [88-90].
Injury to the facet joints and capsular ligaments has been further confirmed during simulated whiplash traumas [91]. Maximum capsular ligament strains occur during shear forces, such as when a force is applied while the head is rotated (axial rotation). While capsular ligament injury in the upper cervical spinal region can occur from compressive forces alone, exertion from a combination of shear, compression and bending forces is more likely and usually involves much lower loads to cause injury [92]. However, if the head is turned during whiplash trauma, the peak strain on the cervical facet joints and capsular ligaments can increase by 34% [93]. In one study reporting on an automobile rear-impact simulation, the magnitude of the joint capsule strain was 47% to 196% higher in instances when the head was rotated 60� during impact, compared with those when the head was forward facing [94]. The impact was greatest in the ipsilateral facet joints, such that head rotation to the left caused higher ligament strain at the left facet joint capsule.
In other simulations, whiplash trauma has been shown to reduce cervical ligament strength (ie, failure force and average energy absorption capacity) compared with controls or computational models [30, 87]; this is especially true in the case of capsular ligaments, since such trauma causes capsular ligament laxity. One study conclusively demonstrated that whiplash injury to the capsular ligaments resulted in an 85% to 275% increase in ligament elongation (ie, laxity) compared to that of controls [30]. The study also reported evidence that tension of the capsular ligaments is requisite for producing pain from the facet joint.
Post-Concussion Syndrome
Each year in the United States, approximately 1.7 million people are diagnosed with traumatic brain injury (TBI), although many more go undiagnosed because they do not seek out medical care [95]. Of these, approximately 75% – 90% are diagnosed as having a concussion. A concussion is considered a mild TBI and is defined as any transient neurologic dysfunction resulting from a biomechanical force, usually a sudden or forceful blow to the head which may or may not cause a loss of consciousness. Concussion induces a barrage of ionic, metabolic, and physiologic events [96] and manifests in a composite of symptoms affecting a patient�s physical, cognitive, and emotional states, and his or her sleep cycle, any one of which can be fleeting or long-term in duration [97]. The diagnosis of concussion is made by the presence of any one of the following: (1) any loss of consciousness; (2) any loss of memory for events immediately before or after the injury; (3) any alteration in mental status at the time of the accident; (4) focal neurological deficits that may or may not be transient [98].
While most individuals recover from a single concussion, up to one-third of those will continue to suffer from residual effects such as headache, neck pain, dizziness and memory problems one year after injury [99]. Such symptoms characterize a disorder known as post-concussion syndrome (PCS) and are much like those of WAD; both disorders are likely due to cervical instability. According to the International Classification of Diseases, 10th Revision (ICD-10), the diagnosis of PCS is made when a person has had a head injury sufficient enough to result in loss of consciousness and develops at least three of eight of the following symptoms within four weeks: headache, dizziness, fatigue, irritability, sleep problems, concentration difficulties, memory issues, and problems tolerating stress [100, 101]. Of those treated for PCS who had mild head injury, 80% report having chronic daily headaches; surprisingly, of those with moderate to severe head injury, only 27% reported having chronic daily headaches [102]. The impact of the brain on the skull is believed to be the cause of the symptoms of both concussion and PCS, although the specific mechanisms underlying neural tissue damage are still being investigated.
PCS-associated symptoms also overlap with many symptoms common to WAD. This overlap in symptomology may be due to a common etiology of underlying cervical instability that affects the cervical spine near the neck. Data has revealed that over half of patients with damage to the upper cervical spine from whiplash injury had evidence of concurrent head trauma [103]. It was shown that whiplash can cause minor brain injuries similar to that of concussion if it occurs with such rapid neck movement that there is a collision between the brain and skull. Thus, one may conjecture that concussion involves a whiplash-type injury to the neck.
Despite unique differences in the biomechanics of concussion and whiplash, both types of trauma involve an acceleration-deceleration of the head and neck. This impact to the head can not only cause injury to the brain and skull, but can also damage surrounding ligaments of the neck since these tissues undergo the same accelerating-decelerating force. The acceleration-deceleration forces which occur during whiplash injury are staggering. Direct head trauma has been shown to produce forces between 10,000 and 15,000 N on the head and between 1,000 and 1,500 N on the neck, depending on the angle at which the object hits the head [104, 105]. Cervical capsular ligaments can become lax with as little as 5 N of force, although most studies report cervical ligament failure at around 100 N [30, 55, 91, 106]. Even low speed rear impact collisions at as little as 7 mph to 8 mph can cause the head to move roughly 18 inches at a force as great as 7 G in less than a quarter of a second [107]. Numerous experimental studies have suggested that certain features of injury mechanisms including direction and degree of acceleration and deceleration, translation and rotation forces, position and posture of head and neck, and even seat construction may be linked to the extent of cervical spine damage and to the actual structures damaged [23, 27, 35, 50, 61].
Debate over the veracity of PCS or WAD symptomology has persisted; however, there is no single explanation for the etiology of these disorders, especially since the onset and duration of symptoms can vary greatly among individuals. Many of the symptoms of PCS and WAD tend to increase over time, especially when those affected are engaged in physical or cognitive activity. Chronic neck pain is often described as a long-term result of both concussion and whiplash, indicating that the most likely structures to become injured during these traumas are the capsular ligaments of the cervical facet joints. In light of this, we propose that the best scientific anatomical explanation is cervical instability in the upper cervical spine, resulting from ligament injury (laxity).
Vertebrobasilar Insufficiency
The occipito-atlanto-axial complex has a unique anatomical relationship with the vertebral arteries. In the lower cervical spine, the vertebral arteries lie in a relatively straight-forward course as they travel through the transverse foramina from C3-C6. However, in the upper cervical spine the arteries assume a more serpentine-like course. The vertebral artery emerges from the transverse process of C2 and sweeps laterally to pass through the transverse foramen of C1 (atlas). From there it passes around the posterior border of the lateral mass of C1, at which point it is farthest from the midline plane at the level of C1 [108, 109]. This pathway creates extra space which allows for normal head rotation without compromising vertebral artery blood flow.
Considering the position of the vertebral arteries in the canals of the transverse processes in the cervical vertebrae, it is possible to see how head positioning can alter vertebral arterial flow. Even normal physiological neck movements (ie, neck rotation) have been shown to cause partial occlusion of up to 20% or 30% in at least one vertebral artery [110]. Studies have shown that contralateral neck rotation is associated with vertebral artery blood flow changes, primarily between the atlas and axis; such changes can also occur when osteophytes are present in the cervical spine [111, 112].
Proper blood flow in the vertebral arteries is crucial because these arteries travel up to form the basilar artery at the brainstem and provide circulation to the posterior half of the brain. When this blood supply is insufficient, vertebrobasilar insufficiency (VBI) can develop and cause symptoms, such as neck pain, headaches/migraines, dizziness, drop attacks, vertigo, difficulty swallowing and/or speaking, and auditory and visual disturbances. VBI usually occurs in the presence of atherosclerosis or cervical spondylosis, but symptoms can also arise when there is intermittent vertebral artery occlusion induced by extreme rotation or extension of the head [113, 114]. This mechanical compression of the vertebral arteries can occur along with other anomalies, including cervical osteophytes, fibrous bands, and osseous prominences [115, 116] These anomalies were seen in about half of the cases of vertebral artery injury after cervical manipulation, as reported in a recent review [117].
Whiplash injury itself has been shown to reduce vertebral artery blood flow and elicit symptoms of VBI [118, 119]. In one study, the authors concluded that patients with persistent vertigo or dizziness after whiplash injury are likely to have VBI if the injury was traumatic enough to cause a circulation disorder in the vertebrobasilar arterial system [118]. Other researchers have surmised that excessive cervical instability, especially of the upper cervical spine, can cause obstruction of the vertebral artery during neck rotation, thus compromising blood flow and triggering symptoms [120-122].
Barr�-Li�ou Syndrome
A lesser known, yet relatively common, cause of neck pain is Barr�-Li�ou syndrome. In 1925, Jean Alexandre Barr�, and in 1928, Yong Choen Li�ou, each independently described a syndrome presenting with headache, orbital pressure/pain, vertigo, and vasomotor disturbances and proposed that these symptoms were related to alterations in the posterior cervical sympathetic chain and vertebral artery blood flow in patients who had cervical spine arthritis or other arthritic disorders [123, 124]. Barr�-Li�ou syndrome is also referred to as posterior cervical syndrome or posterior cervical sympathetic syndrome because the condition is now presumed to develop more from disruption of the posterior cervical sympathetic nervous system, which consists of the vertebral nerve and the sympathetic nerve network surrounding it. Symptoms include neck pain, headaches, dizziness, vertigo, visual and auditory disturbances, memory and cognitive impairment, and migraines. It has been surmised that cervical arthritis or injury provokes an irritation of both the vertebral and sympathetic nerves. As a result, current treatment now centers on resolution of cervical instability and its effects on the posterior sympathetic nerves [124]. Other research has found an association between the sympathetic symptoms of Barr�-Li�ou and cervical instability and has documented successful outcomes in case reports when the instability was addressed by various means including prolotherapy [125].
Symptoms of Barr�-Li�ou syndrome also appear to develop after trauma. In one study, 87% of patients with a diagnosis of Barr�-Li�ou syndrome reported that they began experiencing symptoms after suffering a cervical injury, primarily in the mid-cervical region [126]; in a related study, this same region was found to exhibit more instability than other spinal segments [127] The various symptoms that characterize Barr�-Li�ou syndrome can also mimic symptoms of PCS or WAD, [128] which can pose a challenge for practitioners in making a definitive diagnosis (Fig. ?8). The diagnosis of Barr�-Li�ou syndrome is made on clinical grounds, as there is yet to be a definitive test to document irritation of the sympathetic nervous system.
Figure 8: Overlap in chronic symptomology between atlanto-axial instability, whiplash associated disorder, post-concussion syndrome, vertebrobasilar insufficiency, and Barr�-Li�ou syndrome. There is considerable overlap in symptoms amongst these conditions, possibly because they all appear to be due to cervical instability.
Other Sources of Cervical Pain
Various tensile forces place strains with differing deformations on a variety of viscoelastic spinal structures, including the ligaments, the annulus and nucleus of the intervertebral disc, and the spinal cord. Further to this, cadaver experiments have shown that the spinal cord and the intervertebral disc components carry considerably lower tensile forces than the spinal ligament column [129, 130]. Encapsulated mechanoreceptors and free nerve endings have been identified in the periarticular tissues of all major joints of the body including those in the spine, and in every articular tissue except cartilage [131]. Any innervated structure that has been injured by trauma is a potential chronic pain generator; this includes the intervertebral discs, facet joints, spinal muscles, tendons and ligaments [132-134].
The posterior ligamentous structures of the human spine are innervated by four types of nerve endings: pacinian corpuscles, golgi tendon organs, and ruffini and free nerve endings [40]. These receptors monitor joint excursion and capsular tension, and may initiate protective muscular reflexes that prevent joint degeneration and instability, especially when ligaments, such as the anterior and posterior longitudinal, ligamentum flavum, capsular, interspinous and supraspinous, are under too much tension [131, 135]. Collectively, the cervical region of the spinal column is at risk to sustain deformations at all levels and in all components, and when the threshold crosses a particular level at a particular component, injury is imminent owing to the relative increased flexibility or joint laxity.
Other Sources of Trauma
As described earlier, the nucleus pulposus is designed to sustain compression loads and the annulus fibrosus that surrounds it, to resist tension, shear and torsion. The stress in the annulus fibers is approximately 4-5 times the applied stress in the nucleus [136, 137]. In addition, annulus fibers elongate by up to 9% during torsional loading, but this is still well below the ultimate elongation at failure of over 25% [138]. Pressure within the nucleus is approximately 1.5 times the externally applied load per unit of disc area. As such, the nucleus is relatively incompressible, which causes the intervertebral disc to be susceptible to injury in that it bulges under loads – approximately 1 mm per physiological load [139]. As the disc degenerates on bulging (herniates), it looses elasticity, further compromising its ability to compress. Shock absorption is no longer spread or absorbed evenly by the surrounding annulus, leading to greater shearing, rotation, and traction stress on the disc and adjacent vertebrae. The severity of disc herniation can range from protrusion and bulging of the disc without rupture of the annulus fibrosus to disc extrusion, in which case, the annulus is perforated, leading to tearing of the structure.
Dr. Alex Jimenez’s Insight
“What type of treatment methods can provide effective relief from my chronic neck pain symptoms?”�The symptoms of chronic neck pain can be debilitating and can ultimately affect any individual’s ability to carry on with their everyday activities. While neck pain is a common symptom in a variety of injuries and/or conditions affecting the cervical spine, there are also a number of treatment methods available to help improve neck pain. However, some treatments also address stabilizing the cervical spine as well as healing damaged or injured tissues. Chiropractic care is a well-known alternative treatment option which has been demonstrated to help cure symptoms of neck pain at the source, according to several research studies.
Treatment Options
There are a number of treatment modalities for the management of chronic neck pain and cervical instability, including injection therapy, nerve blocks, mobilization, manipulation, alternative medicine, behavioral therapy, fusion, and pharmacologic agents such as NSAIDS and opiates. However, these treatments do not address stabilizing the cervical spine or healing ligament injuries, and thus, do not offer long-term curative options. In fact, cortisone injections are known to inhibit, rather than promote healing. As mentioned earlier in this paper, most treatments have shown limited evidence in their efficacy or are inconsistent in their results. In a systematic review of the literature from January 2000 to July 2012 on physical modalities for acute to chronic neck pain, acupuncture, laser therapy, and intermittent traction were found to provide moderate benefits [5].
The literature contains many reports on injection therapy for the treatment of chronic neck pain. Cervical interlaminar epidural injections with or without steroids may provide significant improvement in pain and function for patients with cervical disc herniation and radiculitis [140]. As a follow-up to its one-year results, a randomized, double-blind controlled trial found that the clinical effectiveness of therapeutic cervical medial branch blocks with or without steroids in managing chronic neck pain of facet joint origin provided significant improvement over a period of 2 years [141].
However, many other studies have had more nebulous results. In a systematic review of therapeutic cervical facet joint interventions, the evidence for both cervical radiofrequency neurotomy and cervical medial branch blocks is fair, and for cervical intra-articular injections with local anesthetic and steroids, the evidence is limited [142]. In a later corresponding systematic review, the same group of authors concluded that the strength of evidence for diagnostic facet joint nerve blocks is good (?75% pain relief), but stated the evidence is limited for dual blocks (50% to 74% pain relief), as well as for single blocks (50% to 74% pain relief) and (?75% pain relief.) [6]. In another systematic review evaluating cervical interlaminar epidural injections, the evidence indicated that the injection therapy showed significant effects in relieving chronic intractable pain of cervical origin; specific to long-term relief the indicated level of evidence was Level II-1 [143].
In the case of manipulative therapy, the results of a randomized trial disputed the hypothesis that supervised home exercises, combined or not with manual therapy, can be of benefit in treating non-specific chronic neck pain, as compared to no treatment [7]. The study found that there were no differences in primary or secondary outcomes among the three groups and that no significant change in health-related quality of life was associated with the preventive phase. Participants in the combined intervention group did not have less pain or disability and fared no better functionally than participants from the two other groups during the preventive phase of the trial. Another randomized clinical trial comparing the effects of applying joint mobilization at symptomatic and asymptomatic cervical levels in patients with chronic nonspecific neck pain was inconclusive in that there was no significant difference in pain intensity immediately after treatment between groups during resting position, painful active movement, or vertebral palpation [8]. Massage therapy had similar inconclusive results. Evidence was reported as �not strong� [144] in one randomized trial comparing groups receiving massage treatment for neck pain versus those reading a self-care book, while another found that cupping massage was no more effective than progressive muscle relaxation in reducing chronic non-specific neck pain [9]. Acupuncture appears to have better results in relieving neck pain but leaves questions as to the effects on the autonomic nervous system, suggesting that acupuncture points per se have different physical effects according to location [145].
Cervical disc herniation is a major source of chronic neck and spinal pain and is generally treated by either surgery or epidural injections, but their effectiveness continues to be debatable. In a randomized, double-blind, controlled clinical trial assigning patients to treatment with epidural injections with lidocaine or lidocaine mixed with betamethasone, 72% of patients in the local anesthetic group and 68% of patients in the local anesthetic with steroid group had at least a 50% improvement in pain and disability at 2 years, indicating that either protocol may be beneficial in alleviating chronic pain from cervical disc herniation [146].
In a systematic review of pharmacological interventions for neck pain, Peloso, et al. [147] reported that, aside from evidence in one study of a small immediate benefit for the psychotropic agent eperison hydrochloride (a muscle relaxant), most studies had low to very low quality methodologic evidence. Furthermore, they found evidence against a long-term benefit for medial branch block of facet joints with steroids and against a short-term benefit for botulinum toxin-A compared to saline, concluding that there is a lack of evidence for most pharmacological interventions.
Collectively, these interventions for the treatment of chronic neck pain may each offer temporary relief, but many fall short of a cure. Aside from these conventional treatment options, there are pain medications and pain patches, but their use is controversial because they offer little restorative value and often lead to dependence. If joint instability is the fundamental problem causing chronic neck pain and its associated autonomic symptoms, prolotherapy may be a treatment approach that meets this challenge.
Prolotherapy for Cervical Instability
To date, there is no consensus on the diagnosis of cervical spine instability or on traditional treatments that relieve chronic neck pain. In such cases, patients often seek out alternative treatments for pain and symptom relief. Prolotherapy is one such treatment which is intended for acute and chronic musculoskeletal injuries, including those causing chronic neck pain related to underlying joint instability and ligament laxity (Fig. ?9).
Figure 9: Stress-strain curve for ligaments and tendons. Ligaments can withstand forces and revert back to their original position up to Point C. At this point, prolotherapy treatment may succeed in tightening the tissue. Once the force continues past Point C. the ligament becomes permanently elongated or stressed.
Chronic neck pain and cervical instability are particularly difficult to treat when capsular ligament laxity is the cause because ligament cartilage is notoriously slow in healing due to a lack of blood supply. Most treatment options do not address this specific problem, and therefore, have limited success in providing a long-term cure.
Whiplash is a prime example because it often results in ligament laxity. In a five-part series evaluating the strength of evidence supporting WAD therapies, Teasell, et al. [10, 148-151] report that there is insufficient evidence to support any treatment for subacute WAD, stating that radiofrequency neurotomy may be the most effective treatment for chronic WAD. Furthermore, they state that immobilization with a soft collar is ineffective to the point of impeding recovery, saying that activation-based therapy is recommended instead, a conclusion similar to that of Hauser et al. [40] For chronic WAD, exercise programs were the most effective noninvasive treatment and radiofrequency neurotomy, the most effective of surgical or injection-based interventions, although evidence was not strong enough to establish the efficacy of any one treatment [10].
Prolotherapy is referred to as a regenerative injection technique (RIT) because it is based on the premise that the regenerative/reparative healing process consists of three overlapping phases: inflammatory, proliferative with granulation, and remodeling with contraction (Fig. ?10) [152]. The prolotherapy technique involves injecting an irritating solution (usually a dextrose/sugar solution) at painful ligament and tendon attachment sites to produce a mild inflammatory response. Such a response initiates a healing cascade that duplicates the natural healing process of poorly vascularized tissue (ligaments, tendons, and cartilage) [40, 153]. In doing so, tensile strength, elasticity, mass and load-bearing capacity of collagenous connective tissues become increased [152]. This occurs because the increased glucose concentration causes increases in cell protein synthesis, DNA synthesis, cell volume, and proliferation, all of which stimulate ligament size and mass and ligament-bone junction strength, as well as the production of growth factors, which are essential for ligament repair and growth [154].
Figure 10: The biology of prolotherapy.
While the most studied type of prolotherapy is the Hackett-Hemwall procedure which uses dextrose as the proliferant, there are multiple other choices that are suitable, such as polidocanol, manganese, human growth hormone, and zinc. In addition to the Hackett-Hemwall procedure, there is another procedure called cellular prolotherapy, which involves the use of a patient�s own cells from blood, bone marrow, or adipose tissue as the proliferant to generate healing.
It is important to note that prolotherapy not only involves the treatment of joints, but also the associated tendon and ligament attachments surrounding them; hence, it is a comprehensive and highly effective means of wound healing and pain resolution. The Hackett-Hemwall prolotherapy technique was developed in the 1950s and is being transitioned into mainstream medicine due to an increasing number of studies reporting positive outcomes [155-158].
Prolotherapy has a long history of being used for whiplash-type soft tissue injuries of the neck. In separate studies, Hackett and his colleagues early on had remarkably successful outcomes in treating ligament injuries; more than 85% of patients with cervical ligament injury-related symptoms, including those with headache or WAD, reported they had minor to no residual pain or related symptoms after prolotherapy [125, 159, 160]. Similar favorable outcomes for resolving neck pain were reported recently by Hauser, et al. [161]. Hooper, et al. also reported on a case series [162] in which patients with whiplash received intra-articular injections (prolotherapy) into each zygapophysial (facet)
joint and attained consistently improved scores in the Neck Disability Index (NDI) at 2, 6 and 12 months post treatment; average change in Neck Disability Index (NDI) was significant (13.77; p < 0.001) at baseline versus 12 months. Specific to cervical instability, Centeno, et al. [163] performed fluoro-scopically guided prolotherapy and reported that stabilization of the cervical spine with prolotherapy correlated with symptom relief, as depicted in blinded pre and post radiographic readings. Prolotherapy has also been found effective for other ligament injuries, including the lower back, [164-166] knee, [167-169] and other peripheral joints, [170-172] as well as congenital systemic ligament laxity conditions [173].
Evidence that prolotherapy induces the repair of ligaments and other soft tissue structures has been reported in both animal and human studies. Animal research conducted by Hackett [174] demonstrated that proliferation and strengthening of tendons occurred, while Liu and associates [175] found that prolotherapy injections to rabbit ligaments increased ligamentous mass (44%), thickness (27%), as well as ligament-bone junction strength (28%) over a six-week period. In a study on human subjects, Klein et al. [176] used electron microscopy and found an average increase in ligament diameter from 0.055 �m to 0.087 �m after prolotherapy, as shown in biopsies of posterior sacroi-liac ligaments. They also found a linear ligament orientation similar to what is found in normal ligaments. In a case study, Auburn, et al. [177] documented a 27% increase in iliolum-bar ligament size after prolotherapy, via ultrasound.
Studies have also been published on the use of prolotherapy for resolving chronic pain, [152, 178, 179] as well as for conditions specifically related to joint instability in the cervical spine [163, 180] In our own pain clinic, we have used prolotherapy successfully on patients who had chronic pain in the shoulder, elbow, low back, hip, and knee [181-186].
Conclusion
The capsular ligaments are the main stabilizing structures of the facet joints in the cervical spine and have been implicated as a major source of chronic neck pain. Such pain often reflects a state of instability in the cervical spine and is a symptom common to a number of conditions such as disc herniation, cervical spondylosis, whiplash injury and whiplash associated disorder, postconcussion syndrome, vertebrobasilar insufficiency, and Barr�-Li�ou syndrome.
When the capsular ligaments are injured, they become elongated and exhibit laxity, which causes excessive movement of the cervical vertebrae. In the upper cervical spine (C0-C2), this can cause symptoms such as nerve irritation and vertebrobasilar insufficiency with associated vertigo, tinnitus, dizziness, facial pain, arm pain, and migraine headaches. In the lower cervical spine (C3-C7), this can cause muscle spasms, crepitation, and/or paresthesia in addition to chronic neck pain. In either case, the presence of excessive motion between two adjacent cervical vertebrae and these associated symptoms is described as cervical instability.
Therefore, we propose that in many cases of chronic neck pain, the cause may be underlying joint instability due to capsular ligament laxity. Furthermore, we contend that the use of comprehensive Hackett-Hemwall prolotherapy appears to be an effective treatment for chronic neck pain and cervical instability, especially when due to ligament laxity. The technique is safe and relatively non-invasive as well as efficacious in relieving chronic neck pain and its associated symptoms. Additional randomized clinical trials and more research into its use will be needed to verify its potential to reverse ligament laxity and correct the attendant cervical instability.
Acknowledgements
Declared none.
Conflict of Interest
Ms. Woldin and Ms. Sawyer have nothing to declare. Dr. Hauser and Ms. Steilen declare that they perform prolotherapy at Caring Medical Rehabilitation Services.
Dr. Alex Jimenez’s Insight
“I was diagnosed with a whiplash-associated disorder after reporting chronic neck pain symptoms following an automobile accident. What form of care can help me manage the persistent symptoms?”�In order to manage chronic neck pain symptoms, not only is it essential for you to seek immediate medical attention from the proper healthcare professional, its also important to understand the mechanism of injury behind your persistent symptoms. Tendons, ligaments and other structures surrounding the cervical spine, such as the facet joints, can become damaged or injured during an auto accident and their care must be consistent to achieve overall recovery. Many healthcare professionals can provide patients with individualized guidelines on the management of their whiplash-associated disorders and chronic neck pain.
Facet Joint Kinematics and Injury Mechanisms During Simulated Whiplash
Abstract
Study Design: Facet joint kinematics and capsular ligament strains were evaluated during simulated whiplash of whole cervical spine specimens with muscle force replication.
Objectives: To describe facet joint kinematics, including facet joint compression and facet joint sliding, and quantify peak capsular ligament strain during simulated whiplash.
Summary of Background Data: Clinical studies have implicated the facet joint as a source of chronic neck pain in whiplash patients. Prior in vivo and in vitro biomechanical studies have evaluated facet joint compression and excessive capsular ligament strain as potential injury mechanisms. No study has comprehensively evaluated facet joint compression, facet joint sliding, and capsular ligament strain at all cervical levels during multiple whiplash simulation accelerations.
Methods: The whole cervical spine specimens with muscle force replication model and a bench-top trauma sled were used in an incremental trauma protocol to simulate whiplash of increasing severity. Peak facet joint compression (displacement of the upper facet surface towards the lower facet surface), facet joint sliding (displacement of the upper facet surface along the lower facet surface), and capsular ligament strains were calculated and compared to the physiologic limits determined during intact flexibility testing.
Results: Peak facet joint compression was greatest at C4-C5, reaching a maximum of 2.6 mm during the 5 g simulation. Increases over physiologic limits (P < 0.05) were initially observed during the 3.5 g simulation. In general, peak facet joint sliding and capsular ligament strains were largest in the lower cervical spine and increased with impact acceleration. Capsular ligament strain reached a maximum of 39.9% at C6-C7 during the 8 g simulation.
Conclusions: Facet joint components may be at risk for injury due to facet joint compression during rear-impact accelerations of 3.5 g and above. Capsular ligaments are at risk for injury at higher accelerations.
The Treatment of Neck Pain-Associated Disorders and Whiplash-Associated Disorders: A Clinical Practice Guideline
Abstract
Objective: The objective was to develop a clinical practice guideline on the management of neck pain-associated disorders (NADs) and whiplash-associated disorders (WADs). This guideline replaces 2 prior chiropractic guidelines on NADs and WADs.
Methods: Pertinent systematic reviews on 6 topic areas (education, multimodal care, exercise, work disability, manual therapy, passive modalities) were assessed using A Measurement Tool to Assess Systematic Reviews (AMSTAR) and data extracted from admissible randomized controlled trials. We incorporated risk of bias scores in the Grading of Recommendations Assessment, Development, and Evaluation. Evidence profiles were used to summarize judgments of the evidence quality, detail relative and absolute effects, and link recommendations to the supporting evidence. The guideline panel considered the balance of desirable and undesirable consequences. Consensus was achieved using a modified Delphi. The guideline was peer reviewed by a 10-member multidisciplinary (medical and chiropractic) external committee.
Results: For recent-onset (0-3 months) neck pain, we suggest offering multimodal care; manipulation or mobilization; range-of-motion home exercise, or multimodal manual therapy (for grades I-II NAD); supervised graded strengthening exercise (grade III NAD); and multimodal care (grade III WAD). For persistent (>3 months) neck pain, we suggest offering multimodal care or stress self-management; manipulation with soft tissue therapy; high-dose massage; supervised group exercise; supervised yoga; supervised strengthening exercises or home exercises (grades I-II NAD); multimodal care or practitioner’s advice (grades I-III NAD); and supervised exercise with advice or advice alone (grades I-II WAD). For workers with persistent neck and shoulder pain, evidence supports mixed supervised and unsupervised high-intensity strength training or advice alone (grades I-III NAD).
Conclusions:�A multimodal approach including manual therapy, self-management advice, and exercise is an effective treatment strategy for both recent-onset and persistent neck pain.
In conclusion, chronic neck pain, particularly that resulting from whiplash-associated disorders, can be treated using treatment methods which focus on the rehabilitation of the complex structures surrounding the cervical spine. Furthermore, by understanding chronic neck pain as it relates to cervical instability as well as its impact on capsular ligament laxity, patients can seek the proper treatment for their type of chronic neck pain, including whiplash. Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Neck Pain
Neck pain is a common complaint which can result due to a variety of injuries and/or conditions. According to statistics, automobile accident injuries and whiplash injuries are some of the most prevalent causes for neck pain among the general population. During an auto accident, the sudden impact from the incident can cause the head and neck to jolt abruptly back-and-forth in any direction, damaging the complex structures surrounding the cervical spine. Trauma to the tendons and ligaments, as well as that of other tissues in the neck, can cause neck pain and radiating symptoms throughout the human body.
1. Childs J, Cleland J, Elliott J , et al. Neck pain clinical practice guidelines linked to the international classification of functioning, disability, and health from the orthopaedic section of the American Physical Therapy Association. J Orthop Sports Phys Ther. 2008;38(9): A1�34. [PubMed]
2. C�t� P, Cassidy JD, Carroll LJ, Kristman V. The annual incidence and course of neck pain in the general population a population based cohort study. Pain. 2004;112(3): 267�73. [PubMed]
3. Hogg-Johnson S, van der Velde G, Carroll LJ , et al. The burden and determinants of neck pain in the general population. Eur Spine J. 2008;17(Suppl 1 ): 39�51.
4. Childs JD, Fritz JM, Flynn TW , et al. A clinical prediction rule to identify patients with low back pain most likely to benefit from spinal manipulation a validation study. Ann Intern Med. 2004;141(12): 920�8. [PubMed]
5. Graham N, Gross AR, Carlesso LC , et al. ICON. An ICON overview on physical modalities for neck pain and associated disorders. Open Orthop J. 2013;7(Suppl 4 ): 440�60. [PMC free article][PubMed]
6. Onyewu O, Manchikanti L, Falco FJE , et al. An update of the appraisal of the accuracy and utility of cervical discography in chronic neck pain. Pain Physician. 2012;15: E777�806. [PubMed]
7. Martel J, Dugas C, Dubois JD, Descarreaux M. A randomised controlled trial of preventive spinal manipulation with and without a home exercise program for patients with chronic neck pain. BMC Musculoskelet Disord. 2011;12: 41. [PMC free article][PubMed]
8. Aquino RL, Caires PM, Furtado FC, Loureiro AV, Ferreira PH, Ferreira ML. Applying joint mobilization at different cervical vertebral levels does not influence immediate pain reduction in patients with chronic neck pain a randomized clinical trial. J Manual Manipulative Ther. 2009;17(2): 95�100. [PMC free article][PubMed]
9. Lauche R, Materdey S, Cramer H , et al. Effectiveness of home-based cupping massage compared to progressive muscle relaxation in patients with chronic neck pain-a randomized controlled trial. PLoS ONE. 2013;8(6): e65378. [PMC free article][PubMed]
10. Teasell RW, McClure JA, Walton D , et al. A research synthesis of therapeutic interventions for whiplash-associated disorder (WAD): part 1 – overview and summary. Pain Res Manage. 2010;15(5): 287�94. [PMC free article][PubMed]
11. Murphy DR, Hurwitz EL. Application of a diagnosis-based clinical decision guide in patients with neck pain. Chiropr Manual Ther. 2011;19: 19. [PMC free article][PubMed]
12. Suzuki F, Fukami T, Tsuji A, Takagi K, Matsuda M. Discrepancies of MRI findings between recumbent and upright positions in atlantoaxial lesion. Report of two cases. Eur Spine J. 2008;17(Suppl 2 ): S304�7. [PMC free article][PubMed]
13. R�ijezon U, Djupsj�backa M, Bj�rklund M, H�ger-Ross C, Grip H, Liebermann DG. Kinematics of fast cervical rotations in persons with chronic neck pain a cross-sectional and reliability study. BMC Musculoskelet Disord. 2010;11: 22. [PMC free article][PubMed]
14. Gelalis ID, Christoforou G, Arnaoutoglou CM, Politis AN, Manoudis G, Xenakis TA. Misdiagnosed bilateral C5-C6 dislocation causing cervical spine instability a case report. Cases J. 2009;2: 6149. [PMC free article][PubMed]
15. Taylor M, Hipp JA, Gertzbein SD, Gopinath S, Reitman CA. Observer agreement in assessing flexion-extension X-rays of the cervical spine, with and without the use of quantitative measurements of intervertebral motion. Spine J. 2007;7(6): 654�8. [PMC free article][PubMed]
17. Driscoll DR. Anatomical and biomechanical characteristics of upper cervical ligamentous structures a review. J Manipulative and Physiol Ther. 1987;10(3): 107�10. [PubMed]
18. Cusick JF, Yoganandan N. Biomechanics of the cervical spine part 4: major injuries. Clin Biomech. 2002;17(1): 1�20. [PubMed]
19. Nachemson A. The influence of spinal movements of the lumbar intradiscal pressure on the tensile stresses in the annulus fibrosus. Acta Orthop Scan. 1963;33: 183�207. [PubMed]
20. Zak M, Pezowicz C. Spinal sections and regional variations in the mechanical properties of the annulus fibrosus subjected to tensile loading. Acta Bioeng Biomech. 2013;15(1): 51�9. [PubMed]
21. Mercer S, Bogduk N. The ligaments and annulus fibrosus of human adult cervical intervertebral discs. Spine (Phila Pa 1976). 1999;24(7): 619�28. [PubMed]
22. Kuri J, Stapleton E. The spine at trial practical medicolegal concepts about the spine. http: //books.google.com/books?id=Gi6w jdftC7cC&pg=PA12&lpg=PA12&dq=cervical+spine+transverse+processes&source=bl&ots=tboGEQAnuB&sig=Vi4bIDA24bLxGWWEivgAmmlETFo&hl=en&sa=X&ei=YETZUteXHMTAyAGNkICIBQ&ved=0CDYQ6AEwAjgK#v=onepage&q=cervical%20spine%20transverse%20processes&f=false [Accessed April 14. 2014.
23. Jaumard N, Welch WC, Winkelstein BA. Spinal facet joint biomechanics and mechanotransduction in normal, injury, and degenerative conditions. J Biomech Eng. 2011;133(7): 071010. [PMC free article][PubMed]
24. Volle E. Functional magnetic resonance imaging video diagnosis of soft-tissue trauma to the craniocervical joints and ligaments. Int Tinnitus J. 2000;6(2): 134�9. [PubMed]
25. Pal GP, Routal RV, Saggu KG. The orientation of the articular facets of the zygapophyseal joints at the cervical and upper thoracic region. J Anat. 2001;198(Pt 4): 431�41. [PMC free article][PubMed]
26. Quinn KP, Lee KE, Ahaghotu CC, Winkelstein BA. Structural changes in the cervical facet capsular ligament potential contributions to pain following subfailure loading. Stapp Car Crash J. 2007;51: 169�87. [PubMed]
27. Panjabi MM, Bibu K, Cholewicki J. Whiplash injuries and the potential for mechanical instability. Eur Spine J. 1998;7: 484�92. [PMC free article][PubMed]
28. Zdeblick TA, Abitbol JJ, Kunz DN, McCabe RP, Garfin S. Cervical stability after sequential capsule resection. Spine (Phila Pa 1976). 1993;18: 2005�8. [PubMed]
29. Rasoulinejad P, McLachlin SD, Bailey SI, Gurr KR, Bailey CS, Dunning CE. The importance of the posterior osteoligamentous complex to subaxial cervical spine stability in relation to a unilateral facet injury. Spine J. 2012;12(7): 590�5. [PubMed]
30. Ivancic PC, Coe MP, Ndu AB , et al. Dynamic mechanical properties of intact human cervical spine ligaments. Spine J. 2007;7(6): 659�65. [PMC free article][PubMed]
31. DeVries NA, Gandhi AA, Fredericks DC, Grosland NM, Smucker JD. Biomechanical analysis of the intact and destabilized sheep cervical spine. Spine (Phila Pa 1976). 2012;37(16): E957�63. [PubMed]
32. Crisco JJ, 3rd, Oda T, Panjabi MM, Bueff HU, Dvor�k J, Grob D. Transections of the C1-C2 joint capsular ligaments in the cadaveric spine. Spine (Phila Pa 1976). 1991;16: S474�9. [PubMed]
33. Nadeau M, McLachlin SD, Bailey SI, Gurr KR, Dunning CE, Bailey CS. A biomechanical assessment of soft-tissue damage in the cervical spine following a unilateral facet injury. J Bone Joint Surg. 2012;94(21): e156. [PubMed]
34. Frank CB. Ligament structure, physiology, and function. J Musculoskelet Neuronal Interact. 2004;4(2): 199�201. [PubMed]
35. Chen HB, Yang KH, Wang ZG. Biomechanics of whiplash injury. Chin J Traumatol. 2009;12(5): 305�14. [PubMed]
36. Boswell MV, Colson JD, Sehgal N, Dunbar EE, Epter R. A systematic review of therapeutic facet joint interventions in chronic spinal pain. Pain Physician. 2007;10(1): 229�53. [PubMed]
37. Aprill C, Bogduk N. The prevalence of cervical zygapophyseal joint pain a first approximation. Spine (Phila Pa 1976). 1992;17: 744�7. [PubMed]
38. Barnsley L, Lord SM, Wallis BJ, Bogduk N. The prevalence of cervical zygapophaseal joint pain after whiplash. Spine (Phila Pa 1976). 1995;20: 20�5. [PubMed]
39. McLain RF. Mechanoreceptor endings in human cervical facet joints. Iowa Orthop J. 1993;13: 149�54. [PMC free article][PubMed]
40. Hauser RA, Dolan EE, Phillips HJ, Newlin AC, Moore RE Woldin BA. Ligament injury and healing a review of current clinical diagnostics and therapeutics. Open Rehabil J. 2013;6: 1�20.
41. Bergmann TF, Peterson DH. Chiropractic technique principles and procedures, 3rd ed. New York Mobby Inc. 1993
42. J�nsson H , Jr, Bring G, Rauschning W, Sahlstedt B. Hidden cervical spine injuries in traffic accident victims with skull fractures. J Spinal Disord. 1991;4(3): 251�63. [PubMed]
43. van Mameren H, Drukker J, Sanches H, Beursgens J. Cervical spine motion in the sagittal plane (I) range of motion of actually performed movements, an x-ray cinematographic study. Eur J Morphol. 1990;28(1): 47�68. [PubMed]
44. van Mameren H, Sanches H, Beursgens J, Drukker J. Cervical spine motion in the sagittal plane II positions of segmental averaged instantaneous centers of rotation-a cineradiographic study. Spine (Phila Pa 1976). 1992;17(5): 467�74. [PubMed]
45. Bogduk N, Mercer S. Biomechanics of the cervical spine 1: normal kinematics. Clin Biomech. 2000;15(9): 633�48. [PubMed]
46. Radcliff K, Kepler C, Reitman C, Harrop J, Vaccaro A. CT and MRI-based diagnosis of craniocervical dislocations the role of the occipitoatlantal ligament. Clin Orthop Rel Res. 2012;70(6): 1602�13. [PMC free article][PubMed]
47. Hino H, Abumi K, Kanayama M, Kaneda K. Dynamic motion analysis of normal and unstable cervical spines using cineradiography.an in vivo study. Spine (Phila Pa 1976). 1999;24(2): 163�8. [PubMed]
48. Dvorak J, Penning L, Hayek J, Panjabi MM, Grob D, Zehnder R. Functional diagnostics of the cervical spine using computer tomography. Neuroradiology. 1988;30: 132�7. [PubMed]
49. Antinnes J, Dvorak J, Hayek J, Panjabi MM, Grob D. The value of functional computed tomography in the evaluation of soft-tissue injury in the upper cervical spine. Eur Spine J. 1994;3: 98�101. [PubMed]
51. Levine A, Edwards CC. Traumatic lesions of the occipitoatlantoaxial complex. Clin Orthop Rel Res. 1989;239: 53�68. [PubMed]
52. Chang H, Gilbertson LG, Goel VK, Winterbottom JM, Clark CR, Patwardhan A. Dynamic response of the occipito-atlanto-axial (C0-C1-C2):complex in right axial rotation. J Orthop Res. 1992;10(3): 446�53. [PubMed]
53. Goel VK, Winterbottom JM, Schulte KR, Chang H , et al. Ligamentous laxity across C0-C1-C2 complex.Axial torque-rotation characteristics until failure. Spine (Phila Pa 1976). 1990;5(10): 990�6. [PubMed]
54. Goel VK, Clark CR, Gallaes K, Liu YK. Moment-rotation relationships of the ligamentous occipito-atlanto-axial complex. J Biomech. 1988;21(8): 673�80. [PubMed]
55. Quinn KP, Winkelstein BA. Cervical facet capsular ligament yield defines the threshold for injury and persistent joint-mediated neck pain. J Biomech. 2007;40(10): 2299�306. [PubMed]
56. Winkelstein BA, Santos DG. An intact facet capsular ligament modulates behavioral sensitivity and spinal glial activation produced by cervical facet joint tension. Spine (Phila Pa 1976). 2008;33(8): 856�62. [PubMed]
57. Stemper BD, Yoganandan N, Pintar FA. Effects of abnormal posture on capsular ligament elongations in a computational model subjected to whiplash loading. J Biomech Eng. 2005;38(6): 1313�23. [PubMed]
58. Ivancic PC, Ito S, Tominaga Y , et al. Whiplash causes increased laxity of cervical capsular ligament. Clin Biomech. 2008;23(2): 159�65. [PMC free article][PubMed]
59. IASP Spinal pain, section 1: spinal and radicular pain syndromes. http: //www.iasp-pain.org/AM/Template.cfm?Section=Classification _of_Chronic_Pain&Template=/CM/ContentDisplay.cfm&ContentID=16268. Accessed Nov 25. 2013.
60. Argenson C, Lovet J, Sanouiller JL, de Peretti F. Traumatic rotatory displacement of the lower cervical spine. Spine (Phila Pa 1976). 1988;3(7): 767�73. [PubMed]
61. Tominaga Y, Maak TG, Ivancic PC, Panjabi MM, Cunningham BW. Head-turned rear impact causing dynamic cervical intervertebral foraminal narrowing implications for ganglion and nerve root injury. J Neurosurg Spine. 2006;4: 380�7. [PubMed]
62. Caridi JM, Pumberger M, Hughes AP. Cervical radiculopathy a review. HSS J. 2011;7(3): 265�72. [PMC free article][PubMed]
63. Kirkaldy-Willis HF, Farfan HF. Instability of the lumbar spine. Clin Orthop Rel Res. 1982;(165): 110�23. [PubMed]
64. Voorhies RM. Cervical spondylosis recognition, differential diagnosis, and management. Ochsner J. 2001;3(2): 78�84. [PMC free article][PubMed]
66. Aker PD, Gross AR, Goldsmith CH, Peloso P. Conservative management of mechanical neck pain systematic overview and meta-analysis. BMJ. 1996;313: 1291�6. [PMC free article][PubMed]
67. McCormack BM, Weinstein PR. Cervical spondylosis an update. West J Med. 1996;165: 43�51. [PMC free article][PubMed]
68. Peng BG, Hou SX, Shi Q, Jia LS. The relationship between cartilage end-plate calcification and disc degeneration an experimental study. Chin Med J. 2001;114: 308�12. [PubMed]
69. Mauro A, Eisenstein SM, Little C , et al. Are animal models useful for studying human disc disorders/degeneration?. Eur Spine J. 2008;17: 2�19. [PMC free article][PubMed]
70. Oxland TR, Panjabi MM, Southern EP, Duranceau JS. An anatomic basis for spinal instability a porcine trauma model. J Orthop Res. 1991;9(3): 452�62. [PubMed]
71. Wang JY, Shi Q, Lu WW , et al. Cervical intervertebral disc degeneration induced by unbalanced dynamic and static forces a novel in vivo rat model. Spine (Phila Pa 1976) 2006;Jun 15; 31: 1532�38. [PubMed]
72. Schulte K, Clark CR, Goel VK. Kinematics of the cervical spine following discectomy and stabilization. Spine (Phila Pa 1976). 1989;(10): 1116�21. [PubMed]
73. Kelly MP, Mok JM, Frisch RF, Tay BK. Adjacent segment motion after anterior cervical discectomy and fusion versus prodisc-c cervical total disk arthroplasty analysis from a randomized, controlled trial. Spine (Phila Pa 1976) 2011; 36(15): 1171�9. [PubMed]
74. Bydon M, Xu R, Macki M , et al. Adjacent segment disease after anterior cervical discectomy and fusion in a large series. Neurosurgery. 2014;74: 139�46. [PubMed]
75. Song JS, Choi BW, Song KJ. Risk factors for the development of adjacent segment disease following anterior cervical arthrodesis for degenerative cervical disease comparison between fusion methods. J Clin Neurosci. 2014;21(5): 794�8. [PubMed]
76. Johansson BH. Whiplash injuries can be visible by functional magnetic resonance imaging. Pain Res Manage. 2006;11(3): 197�9. [PMC free article][PubMed]
78. Barnsley L, Lord S, Bogduk N. Whiplash injury. Pain. 1994;58: 283�307. [PubMed]
79. Spitzer WO, Skovron ML, Salmi LR , et al. Scientific monograph of the Quebec task force on whiplash-associated disorders redefining “whiplash” and its management. Spine (Phila Pa 1976). 1995;20(8) Suppl : 1S�73. [PubMed]
80. Kaale BR, Krakenes J, Albrektsen G, Wester K. Head position and impact direction in whiplash injuries associations with MRI-verified lesions of ligaments and membranes in the upper cervical spine. J Neurotrauma. 2005;22(11): 1294�302. [PubMed]
81. Falco FJ, Erhart S, Wargo BW , et al. Systematic review of diagnostic utility and therapeutic effectiveness of cervical facet joint interventions. Pain Physician. 2009;12(2): 323�44. [PubMed]
82. Winkelstein BA, Nightingale RW, Richardson WJ, Myers BS, editors. Proceedings of the 43rd Stapp Car Crash Conference. Saniego CA.: 1999. Cervical facet joint mechanics its application to whiplash injury.
83. Lee DJ, Winkelstein BA. The failure response of the human cervical facet capsular ligament during facet joint retraction. J Biomech. 2012;45(14): 2325�9. [PubMed]
84. Bogduk N, Yoganandan N. Biomechanics of the cervical spine part 3: minor injuries. Clin Biomech. 2001;16(4): 267�75. [PubMed]
85. Lord SM, Barnsley L, Wallis BJ, Bogduk N. The prevalence of chronic cervical zygapophysial joint pain after whiplash. Spine (Phila Pa 1976). 1995;20(1): 20�5. [PubMed]
86. Lee KE, Davis MB, Mejilla RM, Winkelstein BA. In vivo cervical facet capsule distraction mechanical implications for whiplash and neck pain. Stapp Car Crash J. 2004;48: 373�95. [PubMed]
87. Tominaga Y, Ndu AB, Coe MP , et al. Neck ligament strength is decreased following whiplash trauma. BMC Musculoskelet Disord. 2006;7: 103. [PMC free article][PubMed]
88. Stokes IA, Frymoyer JW. Segmental motion and instability. Spine (Phila Pa 1976). 1987;7: 688�91. [PubMed]
89. Stokes IA, Iatridis JC. Mechanical conditions that accelerate intervertebral disc degeneration overload versus immobilization. Spine (Phila Pa 1976). 2004;29: 2724�32. [PubMed]
90. Veres SP, Robertson PA, Broom ND. The influence of torsion on disc herniation when combined with flexion. Eur Spine J. 2010;19: 1468�78. [PMC free article][PubMed]
91. Winkelstein BA, Nightingale RW, Richardson WJ, Myers BS. The cervical facet capsule and its role in whiplash injury a biomechanical investigation. Spine (Phila Pa 1976). 2000;25(10): 1238�46. [PubMed]
92. Siegmund GP, Myers BS, Davis MB, Bohnet HF, Winkelstein BA. Mechanical evidence of cervical facet capsule injury during whiplash a cadaveric study using combined shear, compression, and extension loading. Spine (Phila Pa 1976). 2001;26(19): 2095�101. [PubMed]
93. Siegmund GP, Davis MB, Quinn KP , et al. Head-turned postures increase the risk of cervical facet capsule injury during whiplash. Spine (Phila PA 1976). 2008;33(15): 1643�9. [PubMed]
94. Storvik SG, Stemper BD. Axial head rotation increases facet joint capsular ligament strains in automotive rear impact. Med Bio Eng Comput. 2011;49(2): 153�61. [PubMed]
95. Centers for Disease Control Injury prevention & control traumatic brain injury. http: //www.cdc.gov/TraumaticBrainInjury/statistics. html [Accessed March 4. 2014.
96. Centers for Disease Control Concussion.facts for physicians booklet. http: //www.cdc.gov/concussion/HeadsUp/physicians_too l_kit.html [Accessed March 4. 2014.
97. Giza C, Hovda D. The neurometabolic cascade of concussion. J Athl Train. 2001;36: 228�35. [PMC free article][PubMed]
98. Cuccurullo S, Elovic E, Baerga E, Cuccurullo S, editors. Demos Medical Publishing: New York; 2004. Mild traumatic brain injury and postconcussive syndrome Physical medicine and rehabilitation board review.
99. Leddy J, Sandhu H, Sodhi V, Baker J, Willer B. Rehabilitation of concussion and post-concussion syndrome. Sports Health. 2012;4(2): 147�54. [PMC free article][PubMed]
100. ICD-10, International statistical classification of diseases and related health problems 10th revision. World Health Organization. [PubMed]
101. Boake C, McCauley SR, Levin HS , et al. Diagnostic criteria for postconcussional syndrome after mild to moderate traumatic brain injury. J Neuropsych Clin Neurosci. 2005;17: 350�6. [PubMed]
102. Couch Jr, Bears C. Chronic daily headache in the posttrauma syndrome relation to extent of head injury. Headache. 2001;41: 559�64. [PubMed]
103. Barkhoudarian G, Hovda DA, Giza CC. The molecular pathophysiology of concussive brain injury. Clin Sports Med. 2011;30: 33�48. [PubMed]
104. Saari A, Dennison CR, Zhu Q , et al. Compressive follower load influences cervical spine kinematics and kinetics during simulated head-first impact in an in vitro model. J Biomech Eng. 2013;135(11): 111003. [PubMed]
105. Zhou S-W, Guo L-X, Zhang S-Q, Tang C-Y. Study on cervical spine injuries in vehicle side impact. Open Mech Eng J. 2010;4: 29�35.
106. Yoganandan N, Kumaresan S, Pintar FA. Geometric and mechanical properties of human cervical spine ligaments. J Biomech Invest. 2000;122: 623�9. [PubMed]
107. Radanov BP, Sturzenegger M, Distefano G, Schnidrig A, Aljinovic M. Factors influencing recovery from headache after common whiplash. BMJ. 1993;307: 652�5. [PMC free article][PubMed]
108. Martins J, Pratesi R, Bezerra A. Anatomical relationship between vertebral arteries and cervical vertebrae a computerized tomography study. Int J Morph. 2003;21: 123�9.
109. Cacciola F, Phalke U, Goel A. Vertebral artery in relationship to C1-C2 vertebrae an anatomical study. Neurology India. 2004;52: 178�84. [PubMed]
110. Mitchell JA. Changes in vertebral artery blood flow following normal rotation of the cervical spine. J Manip Physiol Ther. 2003;26: 347�51. [PubMed]
111. Mitchell J. Vertebral artery blood flow velocity changes associated with cervical spine rotation a meta-analysis of the evidence with implications for professional practice. J Man Manip Ther. 2009;17: 46�57. [PMC free article][PubMed]
112. Haynes M, Hart R, McGeachie J. Vertebral arteries and neck rotation doppler velocimeter interexaminer reliability. Ultrasound Med Biol. 2000;26: 57�62. [PubMed]
113. Kuether TA, Nesbit GM, Clark VM, Barnwell SL. Rotational vertebral artery occlusion a mechanism of vertebrobasilar insufficiency. Neurosurgery. 1997;41: 427�32. [PubMed]
114. Yang PJ, Latack JT, Gabrielsen TO, Knake JE, Gebarski SS, Chandler WF. Rotational vertebral artery occlusion at C1-C2. Am J Neuroradiol. 1985;6: 96�100. [PubMed]
115. Cape RT, Hogan DB. Vertebral-basilar insufficiency. Can Family Physician. 1983;29: 305�8. [PMC free article][PubMed]
116. Go G, Soon-Hyun H, Park IS, Park H. Rotational vertebral artery compression bow hunter’s syndrome. J Korean Neurosurg Soc. 2013;54: 243�5. [PMC free article][PubMed]
117. Gordin K, Hauser R. The case for utilizing prolotherapy as a promising stand-alone or adjunctive treatment for over-manipulation syndrome. J Applied Res. 2013;13: 1�28.
118. Endo K, Ichimaru K, Komagata M, Yamamoto K. Cervical vertigo and dizziness after whiplash injury. Eur Spine J. 2006;15: 886�90. [PMC free article][PubMed]
119. Creighton D, Kondratek M, Krauss J, Huijbregts P, Qu H. Ultrasound analysis of the vertebral artery during non-thrust cervical translatoric spinal manipulation. J Man Manip Ther. 2011;19: 84�90. [PMC free article][PubMed]
120. Inamasu J, Nakatsukasa M. Rotational vertebral artery occlusion associated with occipitoatlantal assimilation, atlantoaxial subluxation and basilar impression. Clin Neurol Neurosurg. 2013;115: 1520�3. [PubMed]
121. Kim HA, Yi HA, Lee CY, Lee H. Origin of isolated vertigo in rotational vertebral artery syndrome. Neuro Sci. 2011;32: 1203�7. [PubMed]
122. Yacovino DA1, Hain TC. Clinical characteristics of cervicogenic related dizziness and vertigo. Sem Neurol. 2013;33: 244�55. [PubMed]
123. Limousin CA. Foramen arcuale and syndrome of Barr�-Li�ou. Int Orthop. 1980;4(1): 19�23. [PubMed]
125. Hackett GS, Huang TC, Raferty A. Prolotherapy for headache; pain in the head and neck, and neuritis. Headache. 1962:3�11. [PubMed]
126. Tamura T. Cranial symptoms after cervical injury.Aetiology and treatment of the Barr -Li ou syndrome. J Bone Joint Surg Br. 1989;71B:282�7. [PubMed]
127. Qian J, Tian Y, Qiu GX, Hu JH. Dynamic radiographic analysis of sympathetic cervical spondylosis instability. Chin Med Sci J. 2009;24: 46�9. [PubMed]
128. Humphreys BK, Peterson C. Comparison of outcomes in neck pain patients with and without dizziness undergoing chiropractic treatment a prospective cohort study with 6 month follow-up. Chiropr Man Ther. 2013;21(1): 3. [PMC free article][PubMed]
129. Pintar FA, Yoganandan N, Myers T, Elhagediab A, Sances A ., Jr Biomechanical properties of human lumbar spine ligaments. J Biomech. 1992;25: 1351�6. [PubMed]
130. Yoganandan N, Pintar D, Maiman J, Cusick JF, Sances A , Jr, Walsh PR. Human head-neck biomechanics under axial tension. Med Eng Phys. 1996;18: 289�94. [PubMed]
131. Mc Lain R. Mechanoreceptors endings in human cervical facet joints. Iowa Orthop J. 1993;13: 149�54. [PMC free article][PubMed]
132. Steindler A, Luck J. Differential diagnosis of pain low in the back allocation of the source of pain by the procaine hydrochloride method. JAMA. 1938;110: 106�13.
133. Donelson R, Aprill C, Medcalf R, Grant W. A prospective study of centralization of lumbar and referred pain a predictor of symptomatic discs and anular competence. Diagn Ther. 1997;22: 1115�22. [PubMed]
134. Meleger AL, Krivickas LS. Neck and back pain musculoskeletal disorders. Neurol Clin. 2007;25: 419�38. [PubMed]
135. Silver P. Direct observation of changes in tension in the supraspinous and interspinous ligaments during flexion and extension of the vertebral column in man. J Anat. 1954:550�1.
136. Nachemson A. Lumbar intradiscal pressure.Experimental studies on post-mortem material. Acta Orthop Scand. 1960;43S:1�104. [PubMed]
137. Galante J. Tensile properties of the human lumbar annulus fibrosus. Acta Orthop Scand. 1967;100S:1�91. [PubMed]
138. Stokes IA. Surface strain on human intervertebral discs. J Orthop Res. 1987;5: 348�55. [PubMed]
139. Stokes IA. Bulging of the lumbar intervertebral discs non-contacting measurements of anatomical specimens. J Spinal Disord. 1988;1: 189�93. [PubMed]
140. Manchikanti L, Malla Y, Cash KA, McManus CD, Pampati V. Fluoroscopic cervical interlaminar epidural injections in managing chronic pain of cervical postsurgery syndrome preliminary results of a randomized, double-blind, active control trial. Pain Physician. 2012;15: 13�26. [PubMed]
141. Manchikanti L, Singh V, Falco FJE, Cash KA, Fellows B. Comparative outcomes of a 2-year follow-up of cervical medial branch blocks in management of chronic neck pain a randomized, double-blind controlled trial. Pain Physician. 2010;13: 437�50. [PubMed]
142. Falco FJE, Manchikanti L, Datta S , et al. Systematic review of the therapeutic effectiveness of cervical facet joint interventions an update. Pain Physician. 2012;15: E839�68. [PubMed]
143. Benyamin R, Singh V, Parr AT, Conn A, Diwan S, Abdi S. Systematic review of the effectiveness of cervical epidurals in the management of chronic neck pain. Pain Physician. 2009;12: 137�57. [PubMed]
145. Matsubara T, Arai Y-CP, Shiro Y , et al. Comparative effects of acupressure at local and distal acupuncture points on pain conditions and autonomic function in females with chronic neck pain. Evidence-Based Complementary Alternative Med. 2011; 2011: 543921. [PMC free article][PubMed]
146. Manchikanti L, Cash KA, Pampati V, Wargo BW, Malla Y. A randomized, double-blind, active control trial of fluoroscopic cervical interlaminar epidural injections in chronic pain of cervical disc herniation results of a 2-year follow-up. Pain Physician. 2013;16: 465�78. [PubMed]
147. Peloso PM, Khan M, Gross AR , et al. Pharmacological interventions including medical injections for neck pain an overview as part of the ICON project. Open Orthop J. 2013;7(Suppl 4 M8 ): 473�93. [PMC free article][PubMed]
148. Teasell RW, McClure JA, Walton D, Pretty J , et al. A research synthesis of therapeutic interventions for whiplash-associated disorder (WAD): part 2 – interventions for acute WAD. Pain Res Manage. 2010;15(5): 295�304. [PMC free article][PubMed]
149. Teasell RW, McClure JA, Walton D , et al. A research synthesis of therapeutic interventions for whiplash-associated disorder (WAD): part 3 – interventions for subacute WAD. Pain Res Manag. 2010;15(5): 305�12. [PMC free article][PubMed]
150. Teasell RW, McClure JA, Walton D , et al. A research synthesis of therapeutic interventions for whiplash-associated disorder (WAD): part 4 -noninvasive interventions for chronic WAD. Pain Res Manag. 2010;15(5): 313�22. [PMC free article][PubMed]
151. Teasell RW, McClure JA, Walton D , et al. A research synthesis of therapeutic interventions for whiplash-associated disorder (WAD): part 5 – surgical and injection-based interventions for chronic WAD. Pain Res Manag. 2010;15(5): 323�34. [PMC free article][PubMed]
152. Linetsky FS, Manchikanti L. Regenerative injection therapy for axial pain. Tech Reg Anaesh Pain Manag. 2005;9: 40�9.
153. Hackett G, editor. Oak Park IL. 5th ed. 1993. Ligament and tendon relaxation treated by prolotherapy ; pp. 94�6.
154. Goswami A. Prolotherapy. J Pain Palliative Care Pharmacother. 2012;26: 376�8. [PubMed]
155. Hauser RA, Maddela HS, Alderman D , et al. Journal of Prolotherapy international medical editorial board consensus statement on the use of prolotherapy for musculoskeletal pain. J Prolotherapy. 2011;3: 744�6.
156. Kim J. The effect of prolotherapy for osteoarthritis of the knee. J Korean Ac Rehab Med. 2002;26: 445�8.
157. Rabago D, Slattengren A, Zgierska A. Prolotherapy in primary care practice. Primary Care. 2010;37: 65�80. [PMC free article][PubMed]
158. Distel LM, Best TM. Prolotherapy a clinical review of its role in treating chronic musculoskeletal pain. PMR. 2011;3(6) Suppl1 : S78�81. [PubMed]
159. Hackett G. Prolotherapy in whiplash and low back pain. Postgrad Med. 1960:214�9. [PubMed]
160. Kafetz D. Whiplash injury and other ligamentous headache – its management with prolotherapy. Headache. 1963;3: 21�8. [PubMed]
161. Hauser RA, Hauser MA. Dextrose prolotherapy for unresolved neck pain an observational study of patients with unresolved neck pain who were treated with dextrose prolotherapy at an outpatient charity clinic in rural Illinois. Pract Pain Manage. 2007;10: 56�69.
162. Hooper RA, Frizzell JB, Faris P. Case series on chronic whiplash related neck pain treated with intraarticular zygapophysial joint regeneration injection therapy. Pain Physician. 2007;10: 313�8. [PubMed]
163. Centeno CJ, Elliott J, Elkins WL, Freeman M. Fluoroscopically guided cervical prolotherapy for instability with blinded pre and post radiographic reading. Pain Physician. 2005;8(1): 67�72. [PubMed]
164. Lee J, Lee HG, Jeong CW, Kim CM, Yoon MH. Effects of intraarticular prolotherapy on sacroiliac joint pain. Korean J Pain. 2009:229�33.
165. Cusi M, Saunders J, Hungerford B, Wisbey-Roth T, Lucas P, Wilson S. The use of prolotherapy in the sacroiliac joint. Brit J Sports Med. 2010;44: 100�4. [PubMed]
166. Naeim F, Froetscher L, Hirschberg GG. Treatment of chronic iliolumbar syndrome by infiltration of the iliolumbar ligament. West J Med. 1982;136: 372�4. [PMC free article][PubMed]
167. Kim J. Effects of prolotherapy on knee joint pain due to ligament laxity. J Korean Pain Soc. 2004;17: 47�5.
168. Reeves K, Hassanein KM. Long-term effects of dextrose prolotherapy for anterior cruciate laxity. Alternative Ther. 2003;9: 58�62. [PubMed]
169. Jo D. Effects of prolotherapy on knee joint pain due to ligament laxity. J Korean Pain Soc. 2004;17: 47�50.
170. Kim S. Effects of prolotherapy on chronic musculoskeletal disease. Korean J Pain. 2002;15: 121�5.
171. Wheaton MT, Jensen N. The ligament injury-osteoarthritis connection the role of prolotherapy in ligament repair and the prevention of osteoarthritis. J Prolotherapy. 2011;3: 790�812.
172. Refai H, Altahhan O, Elsharkawy R. The efficacy of dextrose prolotherapy for temporomandibular joint hypermobility a preliminary prospective, randomized double-blind, placebo-controlled clinical trial. J Oral Maxillofac Surg. 2011;69(12): 2962�70. [PubMed]
173. Hauser R, Phillips HJ. Treatment of joint hypermobility syndrome, including Ehlers-Danlos syndrome, with Hackett-Hemwall prolotherapy. J Prolotherapy. 2011;3: 612�29.
174. Hackett G. Joint stabilization an experimental, histologic study with comments on the clinical application in ligament proliferation. Am J Surg. 1955;89: 967�73. [PubMed]
175. Liu Y, Tipton C, Matthes R, Bedford TG, Maynard JA, Walmer HC. An in situ study of the influence of a sclerosing solution in rabbit medial collateral ligaments and its junction strength. Connect Tissue Res. 1983;11: 95�102. [PubMed]
176. Klein R, Dorman T, Johnson C. Proliferant injections for low back pain histologic changes of injected ligaments and objective measurements of lumbar spine mobility before and after treatment. J Neuro Ortho Med Surg. 1989;10: 123�6.
177. Auburn A, Benjamin S, Bechtel R, Matthews S. Increase in cross sectional area of the iliolumbar ligament using prolotherapy agents an ultrasonic case study. J Prolotherapy. 1999;1: 156�62.
178. Linetsky FS, Miguel R, Torres F. Treatment of cervicothoracic pain and cervicogenic headaches with regenerative injection therapy. Curr Pain Headache Rep. 2004;8(1): 41�8. [PubMed]
179. Alderman D. Prolotherapy for knee pain. Pract Pain Manage. 2007;7(6): 70�9.
180. Hooper RA, Yelland M, Fonstad P, Southern D. Prospective case series of litigants and non-litigants with chronic spinal pain treated with dextrose prolotherapy. Int Musculoskelet Med. 2011;33: 15�20.
181. Hauser RA. A retrospective study on Hackett-Hemwall dextrose prolotherapy for chronic shoulder pain at an outpatient charity clinic in rural Illinois. J Prolotherapy. 2009;4: 205�16.
182. Hauser RA, Hauser MA, Holian P. Hackett-Hemwall dextrose prolotherapy for unresolved elbow pain. Pract Pain Manage. 2009:14�26.
183. Hauser RA. Dextrose prolotherapy for unresolved low back pain a retrospective case series study. J Prolotherapy. 2009;3: 145�55.
184. Hauser RA. A retrospective study on Hackett-Hemwall dextrose prolotherapy for chronic hip pain at an outpatient charity clinic in rural Illinois. J Prolotherapy. 2009;(2): 76�88.
185. Hauser RA. A retrospective study on dextrose prolotherapy for unresolved knee pain at an outpatient charity clinic in rural Illinois. J Prolotherapy. 2009;(1): 11�21.
186. Hauser R, Woldin B. Treating osteoarthritic joints using dextrose prolotherapy and direct bone marrow aspirate injection therapy. Open Arthritis J. 2014;7: 1�9.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine