Navigating Car Accident Claims in El Paso, Texas: Pre-Existing Conditions, the Eggshell Skull Rule, and Care at El Paso Back Clinic
The doctor explains an X-ray to the patient and points at the computer screen. The patient wears a cervical collar
Car accidents are common in El Paso, Texas. They can cause new injuries or worsen existing ones. People often wonder if a past health issue, like back pain or arthritis, will block them from getting help after a crash. Texas law offers protection. You can still claim money for injuries even with prior conditions. This article covers the rules, what you can get paid for, and the steps to follow. It highlights the “eggshell skull rule” and why quick medical care is key. In El Paso, El Paso Back Clinic stands out for expert care for auto accidents and worsening conditions.
Understanding the Eggshell Skull Rule
The eggshell skull rule is an important legal concept. It means that if someone causes an accident, they must pay for all resulting damage. This applies even if the injured person had a weakness from a prior condition. It’s like breaking a fragile egg—you can’t blame the thin shell. The rule is also known as the “thin skull rule” or “take your victim as you find them” (Amtz Law, n.d.).
Simply put, the at-fault person takes full responsibility. They can’t use your old health problems to avoid paying. However, the accident must cause new damage or aggravate the existing issue. If your condition had worsened on its own, that might not be covered (Gutierrez Law Firm, n.d.a). For instance, if you had mild back arthritis and the crash resulted in severe pain that required therapy, the at-fault driver is responsible for covering that additional harm.
This rule originated in prior legal cases. It safeguards those who are more vulnerable. In Texas, it’s used in car accident lawsuits to ensure fair compensation (Reyes Law, n.d.).
Applying the Eggshell Skull Rule in Texas and El Paso
Texas fully supports the eggshell skull rule. In El Paso, if a car accident aggravates your pre-existing condition, you can pursue a claim. The law holds the at-fault party liable for all injuries resulting from the crash, including those amplified by prior issues (GDL Firm, n.d.).
El Paso has busy highways, such as I-10, which leads to frequent accidents. Local laws follow Texas standards. For example, if you had an old neck injury and a collision causes whiplash on top of it, the rule helps you recover costs. Insurance companies may argue that your pain stems solely from the prior condition to reduce payments (BHW Law Firm, n.d.). Strong evidence can counter this.
You have two years from the accident date to file in El Paso under the statute of limitations (No Bull Law, n.d.). Act fast to avoid missing out.
Typical Pre-Existing Conditions Impacted: Chronic back pain, sciatica, herniated discs, fibromyalgia, or degenerative disc disease.
Signs of Aggravation: Increased pain, new movement limitations, or the need for additional medical treatment.
El Paso-Specific Risks: Border traffic and dust storms increase crash chances, often affecting backs and necks.
Compensation Options for Aggravated Conditions
When an accident worsens your condition, Texas allows claims for various damages. The eggshell skull rule ensures coverage for the full extent of harm (Siegfried & Jensen, n.d.). This includes bills, lost income, and emotional distress.
Possible compensations include:
Medical Expenses: Costs for new therapies, adjustments, or surgeries due to the aggravation, plus future care.
Wage Loss: Earnings missed from work because of heightened symptoms.
Pain and Suffering: Payment for added physical discomfort and mental strain, such as stress from chronic pain.
Reduced Quality of Life: If daily activities or hobbies become harder.
Long-Term Disability: For permanent worsening, like ongoing sciatica.
Amounts depend on severity. Minor aggravations may yield smaller settlements, while persistent issues, such as the need for regular chiropractic care, may increase them (Reyes Law, n.d.). Age factors in—younger victims may experience greater impacts over time.
In El Paso, solid documentation boosts settlements (Abraham Watkins, n.d.).
Proving Your Case for Compensation
To win, show that the accident directly worsened your condition. Use medical records from before and after to illustrate changes (St. Louis Injury Law, n.d.). This “before-and-after” approach is crucial.
Key steps:
Seek Immediate Care: Visit a doctor soon after. Discuss your history and new symptoms.
Maintain Documentation: Collect bills, notes, and X-ray scans.
Log Daily Effects: Journal pain levels and activity changes.
Expert Testimony: Have a physician explain the connection.
Accident Evidence: Include reports, photos, and statements.
Honesty about your past is vital—concealing it can weaken your claim (Gage Mathers, n.d.). Courts assess if the aggravation ties to the crash or is a natural progression.
Handling Insurance Challenges
Insurers aim to minimize payouts. They may blame your pre-existing condition entirely. They could demand full records to deny claims (Romanow Law Group, n.d.). Avoid broad agreements without advice.
Strategies:
Use Legal Support: Have an attorney negotiate on your behalf.
Reject Low Offers: Initial proposals are often insufficient.
Challenge Rejections: Present evidence linking to the accident.
Recognize Strategies: Beware of their experts minimizing damage.
El Paso attorneys familiar with local rules can help (Ellis & Thomas, n.d.).
Benefits of Specialized Auto Accident Clinics in El Paso
Post-accident, choose a clinic expert in auto injuries. This ensures proper documentation and healing. El Paso Back Clinic excels in this, offering chiropractic care for whiplash, back pain, and aggravated conditions (El Paso Back Clinic, n.d.).
Their approach includes:
Chiropractic Adjustments: To align the spine and ease nerve pressure.
Physical Therapy: To rebuild strength and mobility.
Spinal Decompression: For herniated discs and sciatica.
Functional Medicine: Addressing root causes with nutrition and lifestyle.
Seeing them early helps record aggravations, aiding claims (Your Back in Line Now, n.d.). They coordinate with attorneys for seamless support.
Insights from Dr. Alexander Jimenez at El Paso Back Clinic
Dr. Alexander Jimenez, DC, APRN, FNP-BC, leads El Paso Back Clinic. With dual expertise in chiropractic and nursing, he treats complex cases like auto-aggravated back issues (El Paso Back Clinic, n.d.).
He observes that crashes often intensify conditions like degenerative discs or fibromyalgia. Treatments blend adjustments, acupuncture, and rehab. He emphasizes non-invasive methods, using diagnostic tools such as X-rays to establish links.
Patients praise quick relief. For example, Gale Grijalva recovered from accident-related back pain, resuming activities. Dr. Jimenez’s team offers personalized plans to prevent surgery.
The clinic’s 30,000+ sq ft facility includes gyms and meal prep, supporting full recovery.
Wrapping Up
Dealing with car accidents in El Paso is challenging, especially with pre-existing conditions. Texas’s eggshell skull rule allows compensation for aggravations with proper proof. Seek prompt medical attention, document everything, and consult legal counsel. El Paso Back Clinic, led by Dr. Jimenez, provides top chiropractic and rehab for healing and claims. Contact them at +1-915-850-0900 or visit https://elpasobackclinic.com/ for help.
References
Abraham Watkins. (n.d.). Do Pre-Existing Conditions Disqualify Me From Damages in a Personal Injury Case?Abraham Watkins.
Amtz Law. (n.d.). How Pre-Existing Conditions Affect Your Personal Injury Claim.Amtz Law.
BHW Law Firm. (n.d.). Pre-Existing Injury and Accident in Texas.BHW Law Firm.
Common Motor Vehicle Accidents in El Paso: Recovery and Healing at El Paso Back Clinic®
An injured woman in a stretcher after a car accident, covered by a thermal blanket.
Motor vehicle accidents, or MVAs, are a big issue in El Paso. This city sits on the border, with lots of trucks and cars zooming on roads like I-10 and Loop 375. Accidents often result from drivers not paying attention, drinking, or speeding. They can lead to injuries like neck pain or broken bones. At El Paso Back Clinic®, we help people heal from these injuries. Our team, led by Dr. Alexander Jimenez, uses integrative chiropractic care. This mixes spine fixes with massage, exercise, and healthy eating tips. It treats the whole body and mind. In this article, we discuss common crashes in El Paso, the harm they cause, and how our clinic supports recovery. We draw on Dr. Jimenez’s expertise at our locations in El Paso, TX.
El Paso has many crashes each year. Recent data shows thousands of wrecks, with injuries and even deaths. The border sees heavy truck traffic, upping the risks. Dust storms or rain-slick roads. Work zones add hazards. Knowing this helps folks drive safely. At El Paso Back Clinic®, we see many patients from these events. Our care focuses on pain relief and full health.
Common Types of Motor Vehicle Accidents in El Paso
El Paso’s roads mix locals, visitors, and cross-border traffic. This leads to jam-ups and crashes. Here are the key types:
Distracted Driving Accidents: Phones or snacks pull drivers’ eyes from the road. In El Paso, this sparks many wrecks. Texting hits hard at spots like Mesa and Stanton streets. Texas-wide, it caused over 84,000 crashes in one year.
Drunk or Impaired Driving: Booze or drugs slow folks down. Crashes spike nights and weekends. It’s a top cause in Texas spots like El Paso. They pop up near fun zones like Cincinnati Avenue.
Speeding-Related Crashes: Too fast means tough stops. It makes up 30% of Texas wrecks. On I-10 and Loop 375, speed leads to bad hits. Winds make it worse.
Rear-End Collisions: Cars bump backs from close follows or late brakes. Common on Loop 375 in traffic or near shops like Cielo Vista. Distractions or weather help cause them.
Intersection Crashes: Red-light runs or no yields cause side smacks. Over half happen at crossings like Montana or Zaragoza. The Spaghetti Bowl adds mess. Stop sign skips are big faults.
Pedestrian Incidents: Walkers get struck when drivers miss spots or speed. Downtown, schools, or UTEP see many. Poor walks led to many deaths lately.
Truck Accidents: Border hauls mean big trucks everywhere. Thousands cross yearly. Recent counts show many truck wrecks with injuries. Tired drivers, heavy loads, or blind areas cause them. Spots like I-10, US-54, and Loop 375 are hot.
Pile-ups hit in storms on I-10. Lane changes in builds confuse. Hit-runs occur in town. Stay alert, slow down, and watch out for trucks to avoid.
At El Paso Back Clinic®, we treat folks from all these. Our team knows border traffic woes. We offer care plans for quick heals.
Common Injuries Sustained in Motor Vehicle Accidents
MVAs jolt bodies hard. Sudden moves cause hidden hurts. Here are the usual ones:
Whiplash: Neck snaps cause pain, stiffness, headaches, and dizziness. Top in rear-ends.
Neck and Back Sprains: Pulls or tears cause pain and reduced movement. Low back twists.
Soft Tissue Damage: Bruises, rips in muscles. Swell, stiff. Deep ones last.
Fractures: Breaks from hits. Ribs puncture lungs. Bad ones need ops. Limbs, spine too.
Traumatic Brain Injuries (TBIs): Head knocks cause mix-ups, forgetfulness, and eye issues. Change lives, cost lots.
Shoulders, knees, and inside bleed too. Burns and scars are possible. Trucks crush more. Walkers break bones, heads. Minor ones spark worry or PTSD.
At our clinic, we spot these early. Dr. Jimenez’s team uses checks to plan care.
How These Injuries Occur
Crashes stop or hit fast. Bodies fly in cars. Belts save, but force hurts. Rear-ends jerk heads, stretch necks for whiplash. Sides twist spines for sprains, disc slips. Heads hit for TBIs. Knees dash-bang for sprains. Moves inflame tissues. Trucks smash small cars, break bones. Walkers fly, land hard. Signs may be delayed, so check soon.
We urge quick visits. Our El Paso spots offer fast help.
Integrative Chiropractic Care at El Paso Back Clinic® for MVA Recovery
Our integrative care treats all of you. We fix spines hands-on, easing pain without pills or cuts first. Mixes old ways with massage, PT, and nutrition. Speeds heal, drops swell. Here’s our approach:
Spinal Adjustments: Move bones right, cut nerve pinch, up move. Great for whiplash, back.
Physical Therapy: Builds strong, flexible. Restores after sprains and breaks.
Nutritional Support: Food advice; adds fight-swell, up mood.
Other Therapies: Needle work or disc pull. Ease pain, stress.
We speed recovery, hit the body and feelings. Start in 72 hours, best. Stops long pain. Our functional medicine finds roots.
Insights from Dr. Alexander Jimenez and El Paso Back Clinic®
Dr. Alexander Jimenez, DC, APRN, FNP-BC, has headed El Paso Back Clinic® for 30+ years. He excels in MVA, which includes injuries like whiplash and TBIs. We use functional medicine, nutrition, and rehab. Holistic care heals body and mind from trauma. Cases show fast recovery from car and truck hits. Border traffic brings many to us. Our spots at 11860 Vista Del Sol and 6440 Gateway East offer full care. Call 915-850-0900 for help.
Conclusion
El Paso MVAs from busy roads hurt many. From whiplash to TBIs, harms vary. El Paso Back Clinic® gives natural healing. We cut pain, restore movement. See us after crashes. Safe drives prevent woes. Visit elpasobackclinic.com or call for wellness.
Introduction: My Personal Commitment to the Medico-Legal World—Bridging the Gap Between Clinical Science and Courtroom Proof
By Dr. Alex Jimenez, DC, APRN, FNP-BC | Board-Certified Nurse Practitioner & Chiropractor
Injury Medical Clinic PA, El Paso, Texas
The answer to the crucial question of whether the injury can be conclusively proven, dated, and causally connected to the traumatic event frequently determines the outcome of the high-stakes world of personal injury litigation.
My life’s work at Injury Medical Clinic PA is dedicated to answering this question with an unassailable “Yes.” I have spent decades developing a diagnostic and documentation protocol that transcends the limitations of standard clinical practice. For me, a patient is not just a set of symptoms; they are a complex medico-legal case requiring forensic-level analysis. I recognized early on that El Paso attorneys needed more than a standard radiologist’s report or a simple chiropractor’s diagnosis—they needed a comprehensive, integrated expert who could seamlessly bridge advanced musculoskeletal biomechanics (my foundation as a Chiropractic Physician, DC) with the rigorous standards of comprehensive medical management and documentation (my expertise as a Board-Certified Nurse Practitioner, APRN, FNP-BC).
This unique duality is the engine of our practice. I am not just treating the patient; I am building the legal case. My goal for every personal injury client referred to me is to deliver definitive diagnostic proof that withstands the most rigorous cross-examination, establishes clear causality using objective biomechanical markers, and determines a scientifically validated timeline for the injury—what I call injury dating.
This lengthy post serves as my own, in-depth guide to legal counsel, shedding light on the extent of my involvement in the evaluation of injuries. I meticulously examine the procedures that I use to assess patient cases. These procedures are indispensable for determining the root cause of an illness and for shedding light on the actual degree of disability and impairment that has resulted from traumatic events. I take great pride in my role as a professional in that I am committed to the idea that when a clinical case is brought before a jury, the attorneys representing the plaintiff have complete confidence in the credibility and scientific basis of the expert testimony that I provide.
Dr. Alex Jimenez, DC, APRN, FNP-BC
I will deeply discuss, from my personal experience:
The Diagnostic Imperative: My sophisticated capability to personally stage and interpret complex Magnetic Resonance Imaging (MRI) findings, distinguishing acute trauma from pre-existing conditions using forensic principles.
Causality and Timing: My systematic, proprietary methodology for establishing causality and determining the precise timing (injury dating) of trauma using advanced biomechanical and physiological markers like Modic changes and Wolff’s Law.
The Dual-Licensed Advantage: The justification and profound benefit of treatment and testimony provided by me, a dual-licensed professional, within the El Paso legal community.
Expert Credibility: How attorneys frequently utilize my expert testimony as the credible, objective voice regarding injury dating, impairment, and functional loss, ensuring my documented assessments and evaluations meet the stringent Daubert Standard.
1.0 The Diagnostic Imperative: Personally Staging and Interpreting Complex MRI Findings—Going Beyond the Radiologist’s Report
In my experience, the Magnetic Resonance Imaging (MRI) scan is the single most crucial piece of objective evidence in spinal injury litigation. However, I’ve found that a standard radiologist report often focuses primarily on morphology—describing what is seen—but fails to provide the critical context of causality and chronicity necessary for a successful legal claim.
At Injury Medical Clinic PA, I do not simply accept the outside read; I forensically interpret the physiological, mechanical, and temporal signatures embedded within the MRI data myself. I personally review every single slice and sequence because my ultimate testimony depends on my deep understanding of the images.
1.1 Meeting the Daubert Standard: My Personal Protocols for Scientific Admissibility
In the medico-legal domain, any scientific evidence I present, especially complex imaging findings, must adhere to the Daubert Standard. This requires my expert testimony to be grounded in the methods and procedures of science and supported by appropriate validation (Spinal Diagnostics, n.d.). My entire documentation protocol is built around this necessity.
I personally ensure my findings are admissible by:
Employing Validated Methodology: I utilize diagnostic criteria and staging methods that are thoroughly established in peer-reviewed orthopedic and radiological literature, such as the classification of disc pathology and the chronology of vertebral changes (Wang et al., 2017).
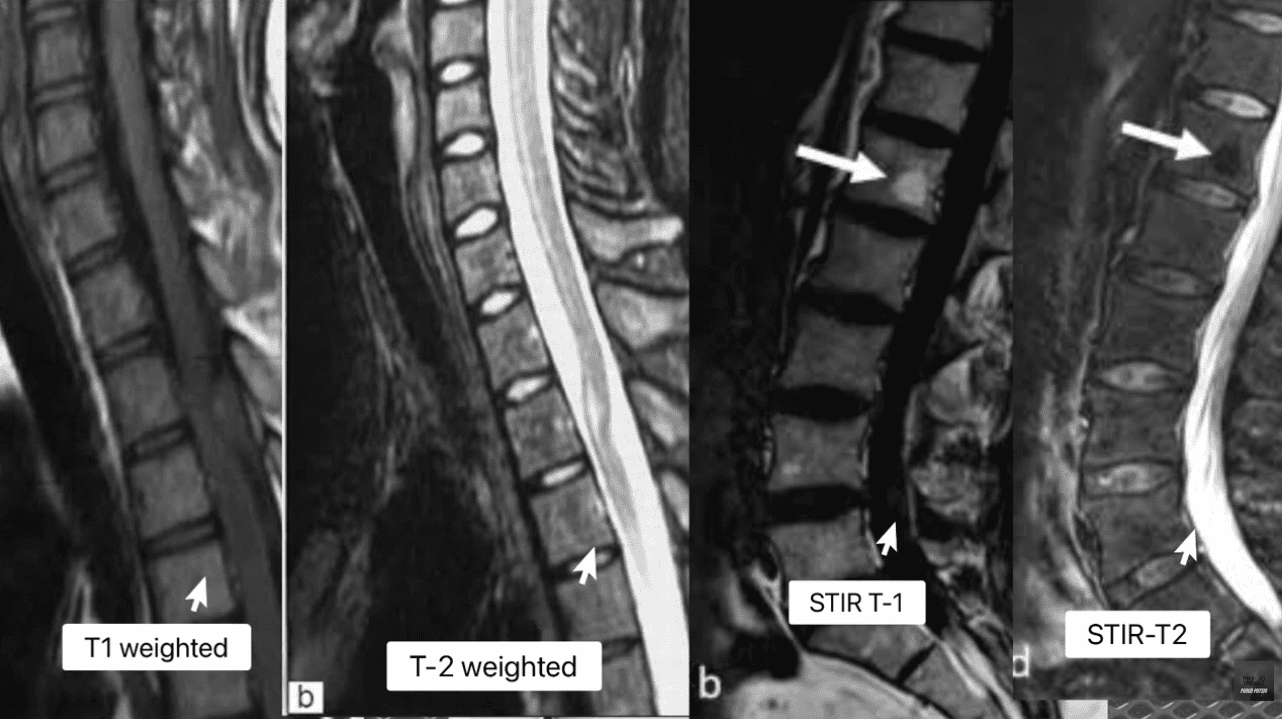
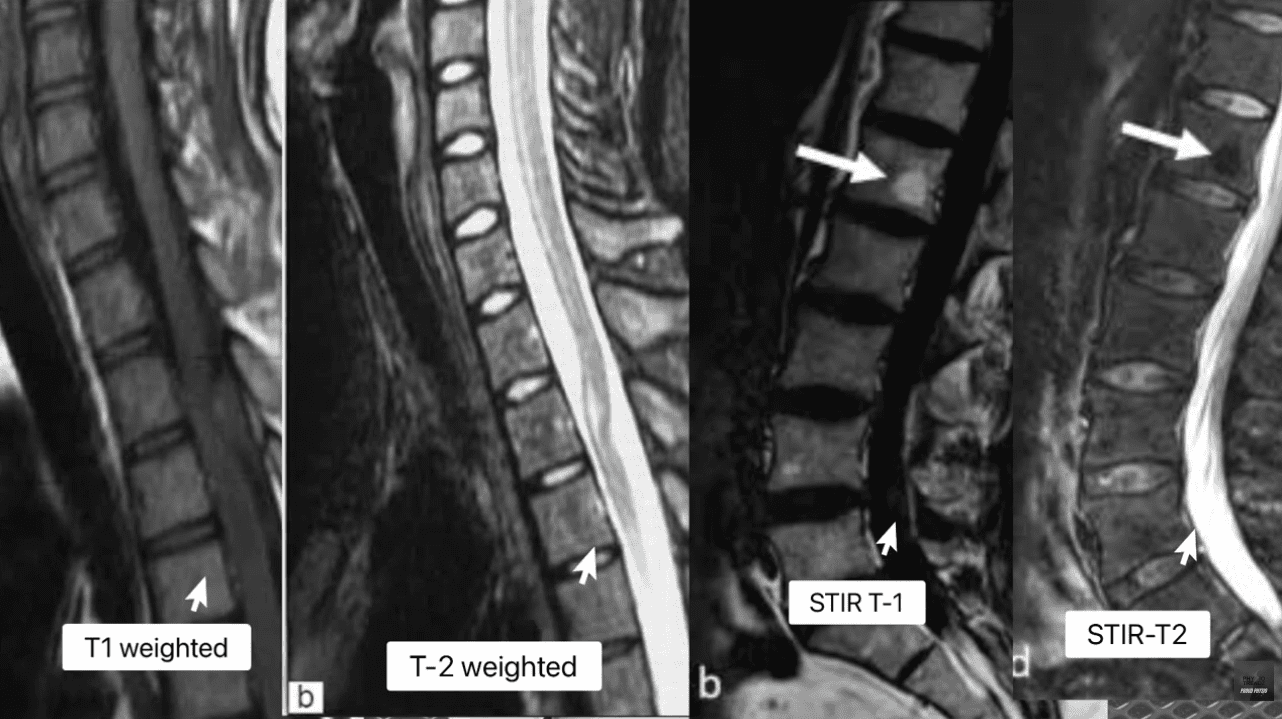
Focusing on Objectivity: My reports meticulously cite the specific MRI pulse sequences (T1, T2, STIR) and image numbers where the pathology is visualized, allowing opposing counsel and the court to verify the data. This objectivity mirrors the rigor seen in advanced quantitative neuroimaging tools like NeuroQuant®, which are successfully used to meet the Daubert standard in TBI cases (National Institutes of Health, 2022).
Simplifying Complex Science: When I testify, my goal is to translate complex terms into easily digestible concepts for the jury. I do not just state a Modic 1 change is present; I explain why it’s a marker of acute trauma, making the science reliable and understandable. This is a crucial skill that attorneys rely on me for.
1.2 Decoding the Spinal Pathologies: My Forensic Review of T1, T2, and STIR Sequences
My method for forensic MRI interpretation depends on a nuanced understanding of various pulse sequences and their physiological meaning (Advanced MRI Interpretation, n.d.). I meticulously review the T1-weighted, T2-weighted, and Short Tau Inversion Recovery (STIR) sequences because they tell different stories about the underlying tissue pathology.
MRI Staging Acute Vs Chronic Injuries
MRI Sequence
Primary Signal (Bright)
Primary Signal (Dark)
Pathological Significance
T1-Weighted
Fat (Marrow), Contrast (Gadolinium)
Water (Edema, CSF), Cortical Bone
Anatomy: Excellent for visualizing fatty infiltration (chronic muscle atrophy, Modic 2) and overall anatomical structure.
T2-Weighted
Water (Edema, CSF), Degenerated Disc
Fat (Marron), Cortical Bone
Pathology: Crucial for identifying water, making it the primary sequence for acute inflammation, disc herniation (fluid), and spinal cord changes.
STIR (Fat-Suppressed)
Water (Edema, CSF, Inflammation)
Fat (Marrow)
Acuity: The definitive sequence for acute trauma. By suppressing fat signal, any remaining bright signal is unequivocally edema, confirming acute inflammation in bone or soft tissue.
The presence of edema (abnormal fluid accumulation) in the bone marrow or soft tissues surrounding the spine is, in my professional opinion, the most powerful, objective indicator of acute trauma. This edema is the body’s immediate inflammatory response to injury and provides the temporal signature required for my precise injury dating.
1.3 Injury Dating: My Systematic Methodology for Establishing a Timeline of Trauma
The ability to accurately date an injury—to definitively state that a spinal pathology is new or acute, rather than chronic and pre-existing—is, without question, the cornerstone of a successful personal injury claim. My clinic utilizes physiological and biomechanical principles to establish this timeline with forensic precision.
1.3.1 Modic Changes: The Gold Standard for Vertebral Endplate Chronology
Modic changes are alterations in the vertebral body endplates and adjacent bone marrow, visible on MRI, that reflect different stages of pathological response. I rely on them heavily because they provide an objective and scientifically validated marker for estimating the age of an injury (Wang et al., 2017; Spinal Diagnostics, n.d.).
Determining Age of Injury Via MRI Staging
Modic Type 1 (MC1) – The Acute Signature: MC1 represents the acute inflammatory stage characterized by bone marrow edema. When I see this, I know I’m looking at an injury that is active and recent.
My Staging: I stage this based on the specific signal patterns: Dark on T1 and Bright on T2/STIR (Spinal Diagnostics, n.d.). The persistent bright signal on STIR is the definitive confirmation of active, acute inflammation.
My Testimony: I explain to attorneys that MC1 changes typically resolve or transition to the fatty Type 2 changes within approximately 6 to 8 weeks (Spinal Diagnostics, n.d.). Therefore, the presence of MC1 is a powerful, objective sign of recent trauma, often correlating directly with the patient’s reported high pain scores (Jensen et al., 2024). When a defense expert attempts to argue degeneration, my documentation of MC1 provides the irrefutable evidence of a specific, new acute event.
Modic Type 2 (MC2) – The Chronic Transition: MC2 represents the replacement of normal bone marrow with fatty tissue (Wang et al., 2017). This is a marker of a more subacute or chronic condition.
My Staging: I stage this based on the characteristic Bright on T1/T2 but crucially, Dark on STIR (fat-suppressed) sequence (Spinal Diagnostics, n.d.).
My Testimony: I use MC2 to show pre-existing degeneration, which ironically, strengthens my credibility. By acknowledging a chronic condition at one level (MC2) while simultaneously proving an acute injury at another (MC1), I demonstrate objectivity and isolate the liability to the new, acute trauma.
1.3.2 Wolff’s Law and My Chronological Interpretation of Bone Spurs
Further reinforcing my injury dating is my application of Wolff’s Law, a fundamental biomechanical principle that bone tissue adapts to the loads placed upon it (Spinal Diagnostics, n.d.). Chronic instability leads to the formation of osteophytes (bone spurs) as the body attempts to stabilize the segment through the piezoelectric effect (Spinal Diagnostics, n.d.).
The Biomechanical Timeline: I rely on scientific research confirming that it takes approximately six months for a bone spur to become radiographically visible or significant (Spinal Diagnostics, n.d.).
My Medico-Legal Implication: When I review a patient’s initial X-rays or CT scans following an MVA, and I find a complete absence of chronic osteophyte formation in the affected segment (e.g., C5-C6), yet the MRI shows an acute disc herniation, I have created an unassailable timeline. The absence of the six-month marker (the bone spur) provides strong supporting evidence that the soft-tissue injury is acute and causally related to the recent collision.
1.4 The Crucial Differential Diagnosis: My Approach to Acute Trauma vs. Chronic Degeneration
Distinguishing new trauma from old, asymptomatic degeneration is essential for proving the extent of damage. I use specific MRI markers to draw this clear line, transforming a murky diagnosis into legal certainty.
Many accident victims have some degree of pre-existing, asymptomatic degeneration. The defense always targets this reality. My expertise lies in identifying and quantifying the acute-on-chronic injury (Spinal Diagnostics, n.d.).
The tell-tale radiological sign I look for is the clear observation of newly extruded disc material extending beyond the border of a mature, pre-existing osteophyte (Spinal Diagnostics, n.d.). The osteophyte, being a chronic boney change, acts as an anatomical baseline for pre-injury status. Any disc material that has been forcefully extruded beyond this chronic bony landmark is, by definition, new trauma and directly quantifiable aggravation. I personally measure this new extrusion and document its displacement in my reports.
1.4.2 The Vacuum Disc Phenomenon: The Irrefutable Marker of Old Pathology
I use the Vacuum Disc Phenomenon as another definitive marker of a chronic, old condition. This finding—nitrogen gas (a distinct signal void, appearing black) within the center of the disc on all MRI sequences (T1, T2, and STIR)—is a reliable sign of old, irreversible degenerative changes and instability (Spinal Diagnostics, n.d.; Advanced MRI Interpretation, n.d.).
When I find a vacuum disc at one level, I include it in my report. This establishes my objectivity, allowing me to state confidently that while one level is chronic, the adjacent, non-vacuum level that displays Modic 1 changes is acute and causally related to the MVA. This approach prevents the defense from collapsing the entire spine into a single, pre-existing condition.
1.5 Analysis of Complex Non-Disc Spinal Pathologies: The Hidden Injuries
Beyond disc herniation, I specialize in the advanced interpretation of other complex spinal pathologies frequently misunderstood or missed by general practitioners, yet vital for proving injury.
1.5.1 The Spinal Epidural Venous Plexus (Batson’s Plexus): Dural Tenting
The Spinal Epidural Venous Plexus (Batson’s Plexus) is a valveless network highly susceptible to sudden pressure changes (Advanced MRI Interpretation, n.d.). In court, I must distinguish between normal physiological changes and pathological ones.
My Differential Diagnosis: Trauma can cause a physiological venous dilation because a disc extrusion can push on the thecal sac—a phenomenon known as dural tenting. This must be carefully distinguished from a pathological Epidural Varix (a symptomatic dilation that causes neural compression) (Advanced MRI Interpretation, n.d.). I rely on sequences like contrast-enhanced MRI (when medically necessary) and non-contrast flow-sensitive sequences to confirm the difference. Incorrectly diagnosing normal venous dilation as a compressive pathology can undermine an entire claim, and my careful distinction preserves my credibility.
1.5.2 Post-Traumatic Muscle Changes: Fatty Infiltration of the Multifidus
The deep lumbar muscles, particularly the multifidus, are essential stabilizers. I have seen time and again how pain-induced inhibition leads to rapid structural changes in this muscle.
My Injury Dating and Causality: This muscle transformation begins to appear on imaging as early as 2 to 12 weeks post-injury (Spinal Diagnostics, n.d.; Central Ohio Spine and Joint, n.d.). Fatty infiltration (visible as a bright signal on T1-weighted images) is highly associated with chronic pain and instability. The degree of infiltration is a crucial prognostic indicator, correlating negatively with functional improvement (Xu et al., 2024). The presence and severity of multifidus fatty infiltration provide powerful objective evidence of chronic functional impairment and instability directly resulting from the traumatic event. I use this finding to prove permanent injury to the core stabilizing system, which is critical for future medical damages.
2.0 Establishing Causality: My Biomechanical and Legal Framework
The defense is designed to argue that a plaintiff’s pain is due to aging or unrelated issues. My documentation provides the scientific and legal rebuttals necessary to establish clear causation—a process I personally manage from the moment the patient walks through my door.
2.1 The “Eggshell Plaintiff” Doctrine: My Documentation Strategy
A foundational principle in personal injury law is the “Eggshell Plaintiff” Rule: a defendant must take the victim as they find them (Cornell Law School, n.d.). This means the defendant is fully liable for the plaintiff’s injuries, even if those injuries are more severe than they would have been in an average person due to an existing, pre-disposed condition (Rafi Law Firm, n.d.).
My Personal Role: Successfully applying this doctrine in court requires meticulous documentation, which I provide by:
Defining the Baseline: Precisely evaluating the pre-accident state (using the Vacuum Disc, Modic 2/3, and chronic osteophyte timelines). I acknowledge the pre-existing state without minimizing the new trauma.
Quantifying the Acute Change: Using Modic Type 1 and Acute-on-Chronic findings to objectively demonstrate the new, causally related injury (Spinal Diagnostics, n.d.).
Proving Exacerbation: Establishing that the traumatic event (MVA) directly aggravated the pre-existing condition, resulting in new symptoms, functional loss, and permanent impairment. My reports meticulously connect the mechanism of injury to the exacerbation, ensuring the court grasps the full scope of liability.
2.2 The Biomechanical Signatures of Soft Tissue and Ligamentous Injury (Whiplash)
Soft tissue injuries, or whiplash-associated disorders (WAD), are commonly challenged as subjective. My examination protocol goes beyond standard range of motion checks to confirm structural injury.
Occult Ligamentous Injury: I utilize the MRI’s fluid-sensitive sequences (STIR) to search for occult tears and sprains. I look for the hyperintense (bright) signal in the interspinous and supraspinous ligaments (Spinal Diagnostics, n.d.), which represents edema and tearing. This finding transforms a subjective “sprain/strain” into an objective, structural instability.
Facet Capsular Edema: The facet joints are often injured during MVA hyperflexion/hyperextension. I meticulously look for capsular edema or effusion (bright signal around the joint) on T2/STIR images. This is a highly specific finding for acute trauma to the joint capsule, which often correlates to localized, severe pain.
The Biomechanical Correlation: I thoroughly document the mechanism of injury (e.g., rear-end collision, specific speed data if available) and link the vector of force to the specific pathology found (e.g., a rear-end vector causing anterior compression and posterior ligamentous tearing) (NCBI, 2023). This correlation is crucial in court to overcome defense arguments that the forces were insufficient to cause the documented injury.
3.0 The Dual-Licensed Advantage: My DC & APRN/FNP-BC Model in El Paso
The most compelling aspect of the Injury Medical Clinic PA model, and the primary reason for my success in the medico-legal field, is my unique qualification as a dual-licensed professional. The integration of the Doctor of Chiropractic (DC) and the Advanced Practice Registered Nurse/Family Nurse Practitioner (APRN/FNP-BC) licenses creates a holistic, comprehensive, and legally powerful care model that is unmatched in the El Paso area.
3.1 Comprehensive Care Models: My Integrated Approach
I bring together the best of both worlds, creating a single source of expertise that satisfies both the clinical and legal standards of care:
My Role as a Chiropractic Physician (DC): I provide unparalleled expertise in spinal biomechanics, functional assessment, manual therapy, and the non-surgical management of complex musculoskeletal injuries. The DC perspective is critical for evaluating the long-term functional impairment caused by disc, facet, and ligament pathology.
My Role as a Nurse Practitioner (APRN/FNP-BC): I provide the essential medical framework, including the ability to prescribe medication (e.g., muscle relaxants, neuropathic agents), order and manage advanced diagnostic testing (e.g., specific, medically-prescribed MRI protocols, nerve conduction studies), manage co-morbidities, and, most crucially, write comprehensive, authoritative medical-legal reports and provide expert testimony that carries the weight of a board-certified medical professional, satisfying the standard medical scrutiny of the court.
This integration ensures the patient receives optimal physical rehabilitation alongside rigorous medical documentation, all under one practice. My reports are medical documents authored by an APRN/FNP-BC, while the therapeutic details reflect the specialized biomechanical insight of a DC. This synergy is invaluable to attorneys.
3.2 Justification for Dual-Licensed Intervention: Case Archetypes in My Practice
I manage these three case archetypes every day, and they demonstrate why my dual-licensed approach is often medically and legally necessary:
Case Archetype
Clinical Presentation in My Clinic
My Dual-Licensed Treatment Rationale
Medico-Legal Value in My Reports
Type 1: Complex Cervical WAD with Radiculopathy.
Patient presents with neck pain, headaches, and confirmed numbness/tingling in the arm. MRI shows a C5-C6 disc bulge impinging on the nerve root.
My DC Expertise: Focus on specific spinal mobilization to reduce segmental dysfunction and restore cervical curve stability. My APRN Expertise: Prescribe gabapentin or NSAIDs for nerve pain, order Electromyography/Nerve Conduction Velocity (EMG/NCV) studies, and administer facet or trigger point injections if necessary (Mayo Clinic, 2024).
Causality: The combined finding of clinical radiculopathy (confirmed by NCV—a medical test I ordered) and the biomechanical trauma (my DC diagnosis) is documented under a single, authoritative medical record (my APRN report). I can objectively testify to the severity of the neurological deficit.
Type 2: Acute Lumbar Disc Extrusion with Failed Conservative Care.
Patient suffers acute L5-S1 disc extrusion causing severe, debilitating sciatica that is not responding to basic care.
My DC Expertise: Implement specialized non-surgical spinal decompression protocols and advanced core stabilization exercises. My APRN Expertise: Medically evaluate the patient’s pain using objective outcome measures (Oswestry Disability Index), rule out Red Flags (Cauda Equina), manage opioid/non-opioid medication, and critically, document the failure of conservative care, which justifies the trajectory toward advanced interventions or surgical consultation.
Damages & Prognosis: My comprehensive documentation of conservative care failure establishes the persistent, debilitating nature of the injury. This robust history is essential for the attorney to justify the valuation of both past and high-value future medical costs in front of a jury.
Type 3: Acute-on-Chronic Spinal Instability.
Patient has pre-existing, asymptomatic spinal stenosis (Modic Type 2 changes), but the MVA results in new symptoms and a new Modic Type 1 change at the adjacent level.
My DC Expertise: Focus on restoring segmental stability to the traumatized level while protecting the degenerated level. My APRN Expertise: Personally interpret the complex MRI (Modic 1 vs. Modic 2) to clearly delineate the acute injury (liability) from the pre-existing condition (eggshell) (Spinal Diagnostics, n.d.).
Defeating the Defense: My precise diagnostic report legally isolates the acute trauma (Modic 1) from the chronic degeneration (Modic 2/Vacuum Disc), providing the attorney with clear, objective evidence to apply the Eggshell Plaintiff doctrine and secure recovery for the aggravation and new injury.
4.0 My Credible Expert Witness Testimony: Illuminating Disability and Driving Monetary Recoveries
My ultimate function for the legal community is to serve as the credible, objective voice that clarifies the patient’s impairment for the jury. My testimony is built upon the synthesis of advanced clinical diagnostics and established medico-legal principles that I personally adhere to.
4.1 The Credibility Foundation: My Daubert-Compliant Testimony
Attorneys frequently utilize my expertise because my methodology is rooted in the scientific method, ensuring my opinions are admissible under the Daubert Standard. My expert testimony is not merely anecdotal; it is a direct presentation of verifiable scientific data:
Measurable Markers: When I testify, I don’t just state an opinion. I point to the imaging and explain that the Modic Type 1 change is not random, but an established scientific finding with a specific 6-8 week timeline, proving the freshness of the bone trauma (Wang et al., 2017). I use analogies, like comparing the Modic 1 change to a fresh bruise on the bone, which makes the complex science undeniable to a layperson jury.
Biomechanically Sound Conclusions: I personally explain how the physics of the impact (the vector, the forces) translates into the specific, demonstrable injury, such as the mechanism by which a sudden flexion-extension event causes an annular tear (Paredes et al., 2023). This link between physics and physiology is critical for proving causation.
The Power of the Dual Role: When I stand before the court, my opinion integrates the highest standard of musculoskeletal diagnosis (DC) with the authority of advanced medical management (APRN). I am uniquely positioned to counter both the defense’s biomechanics expert and their medical expert.
4.2 My Method for Translating Pathology into Permanent Impairment and Disability
The value of a personal injury case is directly linked to the demonstrability and permanency of the injury. My detailed reports translate abstract medical findings into tangible, compelling evidence of long-term disability for the jury.
4.2.1 Quantifying Functional Loss: From Imaging to Activities of Daily Living (ADLs)
I shift the focus from what the injury looks like on an MRI to how it permanently impairs the patient’s life:
Multifidus Fatty Infiltration: I explain to the jury that the increased bright signal on the patient’s T1 MRI is not simply “fat,” but the objective, measurable sign of a permanent loss of spinal stability (Central Ohio Spine and Joint, n.d.). I elaborate that the muscle is no longer functional, leading to chronic instability, increased risk of re-injury, and an inability to perform basic ADLs like prolonged sitting, standing, or lifting—directly correlating to a lower quality of life and permanent functional loss.
Irreversible Cord Damage (Myelomalacia): If I identify Myelomalacia (softening, necrosis, and scarring of the spinal cord tissue) on a T2 image (hyperintensity within the cord), I use this to establish a definitive, catastrophic, permanent neurological injury (Spinal Diagnostics, n.d.). This finding is irreversible and dictates a life of permanent neurological deficits, which is irrefutable evidence of severe disability that warrants significant monetary recovery.
4.2.2 Linking Causality to Prognosis and Future Medical Costs
My reports connect the initial traumatic event to the long-term cost of care. This is vital for the attorney’s calculation of future medical damages.
Permanent Impairment Rating (PIR): I use objective prognostic indicators—such as the severity of multifidus infiltration (Xu et al., 2024), the persistence of Modic 1 changes, or the presence of irreversible ligament instability—to generate a scientifically grounded Permanent Impairment Rating (PIR) using the AMA Guides to the Evaluation of Permanent Impairment.
Future Medical Requirements: The report then outlines the need for future care (e.g., ongoing chiropractic maintenance, periodic APRN follow-ups, medication management, or potential injections/surgical consultations) directly necessitated by the MVA. This robust justification of future needs is critical for maximizing the final settlement or jury award.
By establishing causation, chronicity, and prognosis through my rigorous, peer-reviewed methodology, I provide the unassailable evidence necessary to maximize the plaintiff’s recovery and to position legal counsel to confidently present even the most complex clinical cases before a jury. My role is to ensure that the injury is not only treated effectively but also documented exhaustively, establishing Injury Medical Clinic PA as the premier clinic for injuries resulting from accidents in the El Paso area.
National Institutes of Health (NIH). (2022). Updated Review of the Evidence Supporting the Medical and Legal Use of NeuroQuant® and NeuroGage® in Patients With Traumatic Brain Injury. PMC – PubMed Central. https://pmc.ncbi.nlm.nih.gov/articles/PMC9027332/
T-bone accidents/collisions, also known as side-impact or broadside collisions where the front end of one car slams into the side of another, can result in severe injuries and tend to have a more devastating effect on the body. Side impact collisions account for 24% of driver or passenger deaths; even at 30 mph, side-impacts regularly cause injuries to the occupants of the struck car. Modern vehicles have many safety features, including safety belt features, airbags, and collision avoidance systems that protect drivers and passengers from front and rear collisions; however, when it comes to side-impact, occupants tend to remain unprotected.
T-Bone Side Collision Causes
T-bone accidents usually happen at intersections. Usual Causes of T-bone accidents involve someone failing to yield the right of way. The most common causes include:
A driver makes a risky left turn at an intersection, believing the other car/s will stop.
A driver decides to run a red light crashing into a vehicle making a left turn.
A driver runs through a stop sign, slams into a vehicle, or gets slammed.
Back injuries can damage the spinal cord causing herniated discs, sciatica, and chronic pain that can radiate to the rest of the body.
Treatment and Recovery
Individuals have different recovery times and depend on the severity of the injury and on any pre-existing conditions. Brain injuries and spinal issues can take months to recover fully. Fractures placed in a hard or soft cast to heal for weeks or months can lead to muscle atrophy. Chiropractic therapeutic massage and decompression strengthens muscle weakness, resets and realigns the spinal column, improves range of motion/movement, strengthens grip, and relieves pain.
Neurosurgeon Explains DRX9000
References
Gierczycka, Donata, and Duane Cronin. “Importance of impact boundary conditions and pre-crash arm position for the prediction of thoracic response to pendulum, side sled, and near side vehicle impacts.” Computer methods in biomechanics and biomedical engineering vol. 24,14 (2021): 1531-1544. doi:10.1080/10255842.2021.1900132
Hu, JunMei, et al. “Chronic widespread pain after motor vehicle collision typically occurs through immediate development and nonrecovery: results of an emergency department-based cohort study.” Pain vol. 157,2 (2016): 438-444. doi:10.1097/j.pain.0000000000000388
Lidbe, Abhay, et al. “Do NHTSA vehicle safety ratings affect side impact crash outcomes?.” Journal of safety research vol. 73 (2020): 1-7. doi:10.1016/j.jsr.2020.02.001
Mikhail, J N. “Side impact motor vehicular crashes: patterns of injury.” International journal of trauma nursing vol. 1,3 (1995): 64-9. doi:10.1016/s1075-4210(05)80041-0
Shaw, Greg et al. “Side impact PMHS thoracic response with a large-volume airbag.” Traffic injury prevention vol. 15,1 (2014): 40-7. doi:10.1080/15389588.2013.792109
The gut microbiome is “the second brain” in the body as it helps regulate homeostasis and metabolize the immune system for functionality and to keep the body in motion. The brain is part of the nervous system, providing neuron signals constantly traveling all over the body. The brain and the gut have a communication partnership where they send information back and forth for the body to function normally. When the body gets injured, either the brain, the gut, or both can be affected, causing dysfunction and unwanted symptoms that can cause other issues to affect the other systems in the body. One of these injuries can affect the brain in a traumatic way, which can disturb the signaling to the gut microbiota and affect an individual’s quality of life. Today’s article looks at a traumatic brain injury known as a concussion, its symptoms, and how it affects the gut-brain axis in the body. Refer patients to certified, skilled providers specializing in gut treatments for individuals that suffered from concussions. We guide our patients by referring to our associated medical providers based on their examination when it’s appropriate. We find that education is critical for asking insightful questions to our providers. Dr. Alex Jimenez DC provides this information as an educational service only. Disclaimer
Can my insurance cover it? Yes, it may. If you are uncertain, here is the link to all the insurance providers we cover. If you have any questions or concerns, please call Dr. Jimenez at 915-850-0900.
What Is A Concussion?
Have you been headaches that pop out of nowhere and affect you daily? Have you been experiencing leaky gut or other gut disorder issues causing problems? Do you have trouble concentrating on the simple tasks at hand? Many of these symptoms are signs that you might be suffering from a concussion. Research studies have defined a concussion as a transient disturbance that traumatically induces brain function in the body. Concussions can vary depending on the severity of the injury. When a person suffers from a concussion, the neurotransmitters get disrupted as the brain’s electrolytes go through neurological dysfunction, and blood glucose metabolism decreases cerebral blood flow. Other research studies have found that a concussion does an axial rotation to the brain, which results in the brain jiggling and causes whiplash to the neck. This disruption will cause a biochemical injury that either alters the blood glucose metabolism or can cause derangement of the adenine nucleotides of the nervous system.
Its Symptoms
Research studies have found that when a person suffers from a concussion, the symptoms in its acute phase can drastically change and evolve into a chronic situation over time. Concussions usually occur in individuals that play a contact sport, where they bump each other in the heads, auto accidents that causes severe injuries that affect the neck and brain, or even a simple blow to the head. Other research studies have stated that the symptoms of a concussion can include:
Blurry vision
Headaches
Dizzyness
Mood changes
Light sensitivity
Concentration and memory complications
Additional research studies have mentioned that neuronal dysfunction can occur when a person suffers from a concussion as there are ionic shifts, impaired connectivity to the brain, and changes in the neurotransmitters from completing their jobs to provide sensory-motor functions to the entire body. When this happens, not only does the nervous system gets affected, but the gut system gets affected as well.
An Overview Of Leaky Gut & Concussions-Video
Do gut disorder symptoms seem to be affecting your quality of life? Have you become sensitive to light? Have you felt muscle stiffness in your neck? Or have you been suffering from frequent headaches? If you are experiencing any of these symptoms, it might be due to a concussion affecting your gut microbiota. The video above explains how a concussion and a leaky gut are linked. In an average functioning body, the gut and the brain have a bi-directional connection as they help send the neuron signals to each of the body systems and muscle tissues that make the body move. When traumatic forces like a concussion affect the brain, it can disrupt and change the neurotransmitters signals that can cause gut disorders in the microbiota. When gut disorders affect the gut microbiota, it can cascade a series of inflammatory effects that can affect the body’s homeostasis and immune function. Experiencing these symptoms in the body can drastically affect a person’s mood and quality of life if it is not taken care of immediately.
How The Gut-Brain Axis Is Affected By A Concussion?
Since the gut-brain axis has a communication partnership, this axis helps the body’s immunity, homeostasis, and metabolism function. When a concussion starts to affect the gut-brain axis, research studies have shown that the communication pathways are affected in the gut-brain axis as tit incorporates the afferent and efferent signals. The signals involved in the gut-brain axis include the hormones, neurons, and immune pathways that can result in chronic gastrointestinal dysfunction and disability to the body. Since the gut helps keep the body functional through homeostasis, the brain helps the neuron signals provide sensory functions. With a concussion, these signals are disrupted, affecting the body’s functionality and causing a change in a person’s mood.
Conclusion
Overall the gut-brain axis provides functionality to the body by maintaining the homeostasis and metabolism of the immune system. A person’s involvement in a traumatic accident can lead to brain injuries like a concussion that can impair the gut and brain relationship. A concussion can become severe when it is not treated right away and can affect a person’s quality of life in their health and wellness journey.
Giza, Christopher C., and David A. Hovda. “The Neurometabolic Cascade of Concussion.” Journal of Athletic Training, National Athletic Trainers’ Association, Inc., Sept. 2001, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC155411/.
Mann, Aneetinder, et al. “Concussion Diagnosis and Management: Knowledge and Attitudes of Family Medicine Residents.” Canadian Family Physician Medecin De Famille Canadien, College of Family Physicians of Canada, June 2017, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5471087/.
Staff, Mayo Clinic. “Concussion.” Mayo Clinic, Mayo Foundation for Medical Education and Research, 17 Feb. 2022, https://www.mayoclinic.org/diseases-conditions/concussion/symptoms-causes/syc-20355594.
Tator, Charles H. “Concussions and Their Consequences: Current Diagnosis, Management and Prevention.” CMAJ : Canadian Medical Association Journal = Journal De L’Association Medicale Canadienne, Canadian Medical Association, 6 Aug. 2013, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3735746/.
Zhu, Caroline S, et al. “A Review of Traumatic Brain Injury and the Gut Microbiome: Insights into Novel Mechanisms of Secondary Brain Injury and Promising Targets for Neuroprotection.” Brain Sciences, MDPI, 19 June 2018, https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6025245/.
In the prior composing we created the foundation of the significance of tire pressures. Specifically, we demonstrated that a third of the vehicles on the street and additional only a third of those vehicles have an underinflated tire and a warning light, respectively.
We also know a 20% decrease in pressure results in substandard performance, these are the factors we’re likely to explore.
Underinflated tires have a different profile and contact patch with the road.
Where the tire meets the roadway is known as the contact patch. Maximizing the touch patch affords the motorist the most performance, specifically steering and braking. What happens if we reduce the contact patch? Under inflation does that.
The contact patch is what connects the vehicle to street, when a tire is properly inflated ( other variables being ignored), the scooter can provide 100 percent of the contact patch (and also the friction between the tire and the roadway) to steering, braking or a combination of both. If the pressure drops performance is also reduced and the contact patch is reduced – but by how much? There are schools of thought on this and a ton of research, for our argument we’ll say tires will have a reduction in performance.
Analyzing an Automobile Accident
But what does this actually mean in the real world? Let say a car traveling at 20 miles with tires was successful and needed to swerve to prevent a collision. The same vehicle with underinflated tires could successfully avoid the same collision at no longer than 17 mph. Let us increase the rates, 55 mph properly inflated collision avoidance becomes collision avoidance.
How about braking? If a vehicle with properly inflated tires could stop in 200 feet (roughly 70 mph), then the identical vehicle with under inflated tires will require 230 feet.
Rollovers turned into another related concern. Aside from the contact patch, appropriate inflation also affects rigidity and stability. In simple terms as a bicycle is asked to alter direction (steer), then an underinflated tire will bend enough to allow the sidewall touch the roadway surface and lift the touch patch from the roadway. In extreme instances, the tire will separate out of the rim allowing the rim to dig in the roadway surface. The photo below depicts a sidewall that is currently experiencing this condition.
The tires in this photo are still able to perform well, in part due to the very little side wall and lack of extreme under pressures. Increasing the sidewall, very similar to SUV or a truck, magnifies the bend and distortion.
The last thing to touch on is that the increase of blowouts. Underinflated tires put pressure inside the tire on the tire structure and boost heat. These variables can, and do, raise the probability of a tire failure by causing or exacerbating the layers of material inside the tire.
Proper tire inflation is among the single most significant routine maintenance activity, and ironically, one of the most ignored tasks and when contemplating causality, the tire pressure ought to be assessed to help rebuild the whole picture of this accident. Tire pressure should be taken into consideration when determining is the arbiter of the culpable party and slide and distances marks.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .�
Additional Topics: Auto Injuries
Whiplash is a commonly reported injury after an individual has been involved in an automobile accident. During an auto accident, the sheer force of the impact often causes the head and neck of the victim to jerk abruptly, back-and-forth, causing damage to the complex structures surrounding the cervical spine. Chiropractic care is a safe and effective, alternative treatment option utilized to help decrease the symptoms of whiplash.
There’s a lot of information about tires, far beyond the reviews and recommendations on a variety of websites. Here we’ll talk about, from a post-collision perspective, car specifications, standard tire information, and how tire pressure monitoring systems (TPMS) work. We will then analyze how tire pressures relate to automotive collisions.
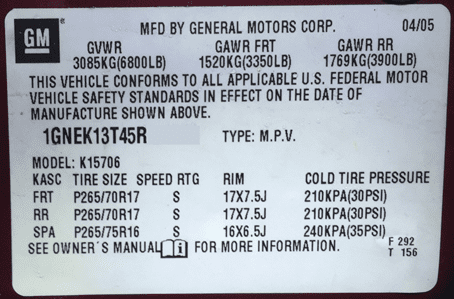
Vehicle Specifications
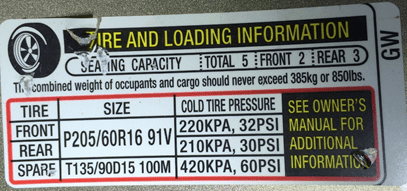
Vehicles offered in the United States have a placard in the driver’s door jamb or internal door. This placard contains some advice we need to explore the tires including the vehicle manufacturer recommended load rating tire size, and tire pressure. Here’s an example:
(there’s a second placard particularly for tires but this should be supported contrary to the above mentioned placard as the next one does not include any vehicle identifying information such as a VIN. In this picture the last six digits of the VIN have been omitted.)
Tire Size
The majority of modern tires have writing on the sidewall which explains the tires measurements as well as other critical characteristics. What does it imply? Sizes for front and back are recorded. The 265 is the width, in millimeters, of the face. The next number, 70, is that the height of the tire sidewall for a percentage of the tread face (in this instance 70 percent of those 265). The “R” creates the tire structure a radial. Finally, the 17 is sized diameter in inches.
Tire Pressure
Notice that the listed tire pressure is assumed to be chilly. Tires have to sit at least eight hours from direct sunlight before they are deemed enough. Gases expand as they are heated and also the minimal cold pressure is put so that the scooter will be at the optimal pressure once at operating temperature; accordingly, if a bicycle is at or below the minimum and is at operating temperature, the strain was lower when the tire was cold.
Tire Pressure Monitoring System (TPMS)
The TPMS became a mandated normal after the fallout of the Ford Explorer & Firestone bicycle event. The federal government needed a system that would alert drivers to “non” tire pressure(s). There are two types of systems. The first type is called “direct measurement” and it uses a detector inside each tire which relays the strain. The second kind is known as “indirect dimension” and it utilizes the anti-lock brake method to determine if a tire is spinning faster than others. A bicycle with air pressure that is less will have a diameter that is smaller and will spin faster; this difference can be calculated by the brake system.
The gap in either system comes when we examine how this system decides to warn the motorist. Because the pressures at a tire can differ for a few reasons (we only discussed how temperature is one of these) that the TPMS doesn’t search for a single pressure, but rather an array or minimum strain. The setup within the computer of the vehicle only illuminates the warning light when a tire’s pressure is outside the specifications that are preselected.
Many studies by the national authorities, independent organizations, and tire producers all support substandard performance of tires where the tires are below the recommended pressure. The research have three points of discussion.
71 percent of drivers check tire pressure less than a month.
More than 1/3 of passenger cars surveyed had at least one tire at or below 20 percent of their placard.
Only 36 percent of vehicles tested would find a warning light at 20 percent or more below the placard.
The first point is not a surprise. The absence of frequent tire pressure maintenance is part of why the federal government mandated the TPMS system. The next point is also not surprising. If the majority (71\%) does not regularly check tire pressure, it should be anticipated tires are below the recommended pressure. The point is that the one we want to concentrate on. We want to focus on this fact since the majority of passenger car worries are 30 PSI; 20 percent less is 24 PSI.
If 100 passenger vehicles were on the road, 36 of these would have a minumum of one tire at 20\% below the placard pressure. Of those 36 vehicles, just 13 of them would have a warning light. (For the record it’s not much better for your light truck / SUV category.)
So now we know a third of those vehicles on the street have an underinflated tire and additional only a third of those vehicles have a warning light. The question is does 6 PSI thing? Yes, it does. Testing done by Goodyear and the NHTSA supported decrease in managing a reduction in pressure results in greater stopping distances, increase in blowouts, lower fuel economy, and tire wear.
Putting it All Together
The National Highway Transportation Safety Administration (NHTSA) also regularly studies tire related accidents. 1 study found approximately 9 percent of all collisions are tire related. In 2012, out of the 5.6 million authorities reported accidents, 504,000 were related.
For simplicity, we will assume each the accidents involved one car making the total 5.6 million. 725,000 would possess the warning lighting if we utilize the proportions more than 2 million would have at least one tire that is underinflated, in the table. Increasing the amount of vehicles only increases the statistics.
When deciding causality, you will find 504,000 tire related collisions as reported previously and also this misunderstood and often overlooked fact is omitted when attempting to determine the culpable party. It’s because of this that upkeep that tire pressures should be ascertained immediately post-accident rather than only focus on skid marks (though they are equally important in the equation important) because demonstrative evidence when trying to reconstruct accidents in the pursuit of discovering causality.
In Part 2 we will discuss how these variables affect tire performance that further provides demonstrative evidence to the accident reconstructionist, accident investigator and lawyer.
The scope of our information is limited to chiropractic and spinal injuries and conditions. To discuss options on the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
References
National Highway Transportation Safety Administration. (2012). Traffic Safety Facts 2012. Retrieved from http://www-nrd.nhtsa.dot.gov/Pubs/812032.pdf
National Highway Transportation Safety Administration. (2013, june 28). SAFETY ADVISORY: NHTSA Urges Drivers to Check Tires During Hot Weather. Retrieved from http://www.nhtsa.gov/About+NHTSA/Press+Releases/SAFETY+ADVISORY:+NHTSA+Urges+Drivers+to+Check+Tires+During+Hot+Weather
National Highway Transportation Safety Administration. (2013, June). The Problem. Retrieved from http://www.nhtsa.gov/nhtsa/Safety1nNum3ers/june2013/theProblemJune2013.html
National Highway Transportation Safety Administration. (n.d.). TIRE PRESSURE SURVEY AND TEST RESULTS. Retrieved from http://www.nhtsa.gov/cars/rules/rulings/TirePressure/LTPW3.html
National Highway Transportation Safety Administration. (n.d.). Tire Pressure Final. Retrieved from http://www.nhtsa.gov/cars/rules/rulings/tirepresfinal/safetypr.html
Additional Topics: Auto Injury Playlist
Whiplash is a commonly reported injury after an individual has been involved in an automobile accident. During an auto accident, the sheer force of the impact often causes the head and neck of the victim to jerk abruptly, back-and-forth, causing damage to the complex structures surrounding the cervical spine. Chiropractic care is a safe and effective, alternative treatment option utilized to help decrease the symptoms of whiplash.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine