Leg Length: One side of the human body doesn’t necessarily match the other perfectly. In fact, there is almost always a tiny disparity of size and length in a person’s hands, feet, arms, and legs.
Think about it, a ring may fit on one hand but be tight on the other, a shoe may feel loose on one foot but be comfortably worn on the other. Most of the time these slight discrepancies in size are normal and have no bearing on an individual’s well-being.
Leg Length Inequality, Unfortunately, Is The Exception
According to the American Chiropractic Association, a study found 75% of subjects who suffered from lower back pain had legs that were slightly different lengths (5 millimeters or more). This condition is called Short Leg Syndrome, and causes a variety of issues for its sufferers. The symptoms can be quite severe, depending on the degree of difference in the leg length.
The premise of this condition is that the leg length inequality disrupts the body’s entire balance, possibly resulting in issues in the knees, hips, and back. The spinal system is designed to bear weight evenly, and, when one leg is shorter than the other, this places additional weight and stress on one side.
According to The Back Pain Authority, common causes of Short Leg Syndrome are a past history of fractures, hip or knee issues, or the individual was simply born that way.
Unfortunately, the condition often brings about recurring and sometimes intense spells of lower back pain and mobility issues for the patient. The good news is that once it’s diagnosed, the patient who commits to consistent treatment measures can manage the condition and resulting lower back pain.
Patients can choose two vital options that help control and manage Short Leg Syndrome’s symptoms:
Chiropractic Care
Visiting an experienced chiropractor and mapping out a treatment plan for lower back pain caused by Short Leg Syndrome is a smart first step. Leg length inequality results in pain because it puts excess pressure and weight on one side of the body. Over time, this creates misalignment in the spine and stiff muscles and joints.
Chiropractic care including spinal adjustments re-align the spine, loosens up the body’s muscles and joints, and promotes healing. A series of visits helps the body gain its balance, and pain hopefully begins decreasing during this period.
However, depending on the degree of leg length inequality, chiropractic treatment alone may not be enough to manage the symptoms long-term. That’s where the second step presents itself as valuable.
Orthotic Heel Lifts
Chiropractic care does wonders for helping individuals regain their spinal alignment and loosen the joints and muscles affected by leg length inequality, but the underlying issue of Short Leg Syndrome remains. The goal of an orthotic heel lift is to balance out the legs, which in turn balances the hips and pelvis.
An orthotic equals out the weight, helping reduce the condition’s symptoms and resulting pain. A treatment of chiropractic care and orthotics gain great advantages over Short Leg Syndrome, and, when used together consistently, offer less pain and fewer recurrences.
An individual who suffers from recurring lower back pain should visit a chiropractor to pursue a diagnosis. If leg length inequality is the cause, patients must rest assured it is manageable in most cases.
Talk with your chiropractor about the recommended regimen of chiropractic adjustments, and the possibility of utilizing an orthotic heel lift. Together, these two steps can decrease pain and the chances of recurrence, and increase overall mobility.
If you or a loved one is suffering from this condition, please give us a call. Our Doctor of Chiropractic is here to help!
18 Wheeler Accident: Jesus Rabelo earns a living as a truck driver in El Paso, TX. After being involved in an accident, however, Mr. Rabelo sufferered from shoulder and back pain which affected his personal life and work, forcing him to have to start over again. In regards to a highly valued recommendation, Jesus Rabelo found Dr. Alex Jimenez, chiropractor in El Paso, TX. Mr. Rabelo describes receiving excellent service from the staff and he highly recommends Dr. Alex Jimenez.
In 2013, 54 million people sustained injuries from traffic collisions. This resulted in 1.4 million deaths in 2013, up from 1.1 million deaths in 1990. Auto accidents can be classified into different types, including head-on, road departure, rear-end, side collisions, and rollovers. Psychological issues may occur due to automobile accidents. A range of injuries and conditions can result from the blunt force trauma caused by a collision, including whiplash and back pain.
Please Recommend Us: If you have enjoyed this video and/or we have helped you in any way please feel free to recommend us. Thank You.
Araceli Norte used to teach physical therapy at the technician level before she suffered a slip and fall accident. When she was recommended to see an excellent doctor who genuinely cared about his patients, Mrs. Norte didn’t hesitate to visit Dr. Alex Jimenez to receive slip and fall injury treatment. Before treatment, Araceli Norte experienced chronic pain on the left side of her body as well as radiating pain down her left leg and foot, ultimately affecting her quality of life. Araceli Norte emphasizes how much relief she’s found with Dr. Alex Jimenez and how much he cares about his patients.
Slip and fall injuries can occur for a variety of reasons. There is an assortment of conditions both indoors and outdoors that can make a slip and fall injury prone. Some common causes of a slip and fall accident inside are because the floor is wet, improperly waxed, or when carpeting is torn or bulging. Normally, liability of the proprietor will be dependent on whether he or she did not take the right action to fix the problem or at least remind people of the issue.
Please Recommend Us: If you have enjoyed this video and/or we have helped you in any way please feel free to recommend us. Thank You.
Cost Effectiveness: There are tons of reasons why a person would answer “yes.” From overall general health to specific aches and pains, to an injury, millions of folks turn to chiropractors for pain relief, increased movement and strength, and overall healing.
For some individuals, the price tag seems to hinder their decision to seek chiropractic treatment. Lack of insurance coverage, or a recommended ongoing treatment regimen (because it usually takes more than one treatment) are two of the most common reasons patients deem it too expensive.
When looking at the big picture, however, patients see and understand the cost of NOT pursuing the care of a chiropractor, and these costs end up being more than simply dollars.
Let’s look at three reasons an individual would visit a chiropractor, and the cost effective savings each scenario provides.
The Cost Effectiveness Of Chiropractic Treatment
An Ounce Of Prevention Is Worth A Pound Of Cure.
Choosing to see a chiropractor to promote and sustain good health is a forward thinking idea that is increasingly attractive to those striving to stay younger, longer. Chiropractic care promotes healing through the body as a whole.
Spinal adjustments and joint manipulations help increase mobility and maximize the entire body’s performance. In addition, they offer a wide variety of health benefits, from decreasing blood pressure to lowering the chance of headaches. Avoiding these health issues potentially save tens of thousands of dollars in future doctor bills!
Regular visits to a professional chiropractor enable a person to stay healthy and enjoy a more active life with a healthy back, bones, and joints.
Oops! I Strained It Again!
Millions of unfortunate souls injure their bodies in a variety of mishaps. From sports injuries to car accidents, to erroneously thinking you really can walk in those four inch heels, our backs, ankles, and hips take a beating.
Choosing chiropractic care for an injury is a smart decision. In many cases, a chiropractor is able to promote healing, decrease a patient’s dependence on drugs for pain management, and minimize the chance of a recurrence.
Chiropractic care treats the body as a whole, so a patient’s visits help strengthen other parts of the surrounding area of the body, not just the injured area. The cost effectiveness of chiropractic care for treating injuries, decreases the money spent on costly medicine and reduces time off work. It also helps people stay married, because most individuals are hateful when they are in pain. (Ok, we made that last point up).
Chronic Medical Conditions.
Many types of medical conditions are ongoing, with no definitive cure. These can be devastating to a person’s quality of life. Daily pain, and loss of strength and mobility are difficult to manage, and sometimes medicine is the chosen option. Numerous times, chiropractic care can work wonders in these situations.
A chiropractor who is experienced in treating the specific type of medical condition can build a treatment plan to help manage the symptoms of the condition, including drug-free pain management. With adjustments to the afflicted area, along with an at-home routine of recommended exercise, the patient frequently experiences a reduction in pain and symptoms, and an increase in mobility. In the best situation, his or her quality of life is positively affected, and relapses are avoided.
Chiropractic care is a productive treatment for a variety of injuries and medical conditions, as well as a preventive therapy to maintain and prolong wellness. The up front cost is paltry when measured against the rewards of increased mobility, decreased pain, and a greater quality of life.
There was a time when Attention Deficit Hyperactivity Disorder, or ADHD, was laughed off as �kids being kids.� Research has shown, however, that ADHD is a neuro behavioral disorder that is often diagnosed in children. In fact, 1 in 10 children receives a diagnosis of ADHD and experts are taking notice of the condition�s impact in learning and even daily living.
ADHD Drugs – Dangerous Game
Traditional treatments for ADHD are often heavily dependent upon medication, particularly stimulants like Ritalin. This drug has long been the standard for treating children diagnosed with ADHD and it, along with other similar drugs, have been shown to be somewhat effective in treating the symptoms of the condition in many patients. Unfortunately, that is not all that these drugs do.
Several of the drugs marketed specifically for ADHD are schedule II controlled substances and act very similar to amphetamines. Drugs including Ritalin have effects that closely mimic those of cocaine. Several of these drugs have been linked to cardiovascular problems in children and teens. Many of them are highly addictive.
Drugs like Adderall have become street drugs abused by teens and college students who enjoy its �speed� effects or who use it to stay awake so they can study. Some young women are abusing the drug by taking it as a diet aid.
Aside from all of this, though, are the effects a child�s brain and body undergo when they take the medication as prescribed. There is usually a distinct behavioral and personality change which often presents as a �dulling� or �stoned� reaction.
There are also great concerns that too little is known about the long term effects of taking ADHD drugs. It is a dangerous game to play with a child�s life.
Studies & Research
Several studies have been conducted to determine the effectiveness of chiropractic treatments as a viable therapy for ADHD. A study published in the Journal of Manipulative and Physiological Therapeutics in 1989 was one of the early studies to explore this. The conclusion of the study was �impressive evidence� that the majority of the subjects did improve while using specific chiropractic care.
It also called for more studies to be conducted to further explore the possibilities that chiropractic care offers. Another study published in Explore (NY) in 2010 also provided strong evidence that chiropractic spinal manipulation has significant benefits for patients with ADHD.
Chiropractic For ADHD
Chiropractic is steadily gaining ground as a viable, effective, non-drug treatment for ADHD patients. Doctors of Chiropractic are teaming up with chiropractic neurologists to help move children away from the drugs. As they create chiropractic based ADHD treatments they not only free children from the unpleasant side effects of the medication, they also introduce them to a healthier lifestyle.
The patient is put through a variety of tests including a brain function exam. Their auditory and visual reflexes are tested as well as other assessments to determine not only the problem, but the specific manifestations of the problem as they relate to the patient. This results in a very individualized treatment plan that is tailored specifically to the patient�s needs, unlike �one size fits all� approach of drug therapy.
Through these individualized programs, data on the patient�s progress is constantly being gathered and compiled by the chiropractic neurologist. Often, children who go through such programs not only experience a significant grade improvement in the first three months, they also experience improvement in their academic performance even after the program is complete.
Improvements in patients who use drug therapy only experience the improvements as long as they are taking the drugs. Chiropractic neurology changes the brain function of the patient so that they enjoy its effects and benefits for life.
If you or a loved one is suffering from this condition, give us a call. Our Doctor of Chiropractic is here to help!
If you’ve experienced a headache, you’re not alone. Approximately 9 out of 10 individuals in the United States suffer from headaches. While some are intermittent, some frequent, some are dull and throbbing, and some cause debilitating pain and nausea, getting rid of the head pain is an immediate response for many. But, how can you most effectively relieve a headache?
Research studies have demonstrated that chiropractic care is an effective alternative treatment option for many types of headaches. A 2014 report in the Journal of Manipulative and Physiological Therapeutics (JMPT) discovered that spinal adjustments and manual manipulations used in chiropractic care improved outcome measures for the treatment of chronic and acute neck pain as well as improved the benefits of a variety of treatment approaches for neck pain. Furthermore, a 2011 JMPT study found that chiropractic care can improve and reduce the frequency of migraine and cervicogenic headaches.
How Does Chiropractic Care Treat Headaches?
Chiropractic care focuses on the treatment of a variety of injuries and/or conditions of the musculoskeletal and nervous system, including headache. A chiropractor utilizes spinal adjustments and manual manipulations to carefully correct the alignment of the spine. A subluxation, or a spinal misalignment, has been demonstrated to cause symptoms, such as neck and back pain, and headache and migraine. A balanced spine can improve spine function as well as alleviate structural stress. In addition, a doctor of chiropractic can help treat headaches and other painful symptoms by supplying nutritional advice, offering posture and ergonomics advice and recommending stress management and exercise advice. Chiropractic care can ultimately ease muscle tension along the surrounding structures of the spine, restoring the spine’s original function.
Furthermore, chiropractic care can safely and effectively treat other spinal health issues, including symptoms of neck and lower back pain due to cervical and lumbar herniated discs, among other injuries and/or conditions. A chiropractor understands how a spinal misalignment, or subluxation, can affect different areas of the body and they will treat the body as a whole rather than focusing on the symptom alone. Chiropractic treatment can help the human body naturally restore its original health and wellness.
It is well-known that chiropractic care is effective for a variety of injuries and/or conditions, however, over the last few years, research studies have found that chiropractic can enhance our well-being by managing our stress. A number of these recent research studies demonstrated that chiropractic care can alter immune function, affect heart rate, and also reduce blood pressure. A 2011 research from Japan indicated that chiropractic may have a much bigger influence on your body than you believe.
Stress is an essential indicator of health, and chronic pain symptoms can tremendously affect wellness. Researchers in Japan sought to check whether chiropractic could alter stress levels in 12 men and women with neck pain and headache. But scientists at Japan wanted to find a more objective picture of how chiropractic spinal adjustments and manual manipulations affect the nervous system, so they used PET scans to monitor brain activity and salvia trials to monitor hormone changes.
After chiropractic care, patients had altered brain activity in the areas of the brain responsible for pain processing and stress reactions. They also had significantly reduced cortisol levels, indicating decreased stress. Participants also reported lower pain scores and a greater quality of life after treatment. Mindfulness interventions, such as chiropractic care, are fundamental stress management methods and techniques. Chronic stress can lead to a variety of health issues, including neck and back pain as well as headache and migraine. Other mindfulness interventions can also safely and effectively help improve symptoms. The purpose of the following article is to demonstrate the effectiveness of another mindfulness intervention, known as mindfulness-based stress reduction, on perceived pain intensity and quality of life in patients previously diagnosed with chronic headache.
The Effectiveness of Mindfulness-Based Stress Reduction on Perceived Pain Intensity and Quality of Life in Patients With Chronic Headache
Abstract
The aim of this study was to determine the effectiveness of Mindfulness-Based Stress reduction (MBSR) on perceived pain intensity and quality of life in patients with chronic headache. Thus, forty patients based on the diagnosis of a neurologist and diagnostic criteria of the International Headache Society (IHS) for migraine and chronic tension-type headache were selected and randomly assigned to the intervention group and control group, respectively. The participants completed the Pain and quality of life (SF-36) questionnaire. The intervention group enrolled in an eight-week MBSR program that incorporated meditation and daily home practice, per week, session of 90-minutes. Results of covariance analysis with the elimination of the pre-test showed significantly improvement of pain and quality of life in the intervention group compared with the control group. The findings from this study revealed that MBSR can be used non-pharmacological intervention for improvement the quality of life and development of strategies to cope with pain in patients with chronic headache. And can be used in combination with other therapies such as pharmacotherapy.
Keywords:chronic pain, migraine headache, mindfulness, quality of life, tension headache
Dr. Alex Jimenez’s Insight
Chronic headache is a debilitating symptoms which affects many people. There are many different types of headaches, however, a majority of them often share a common trigger. Chronic stress can cause a variety of health issues of not properly managed, including muscle tension, which may lead to spinal misalignment, or subluxation, as well as other symptoms, such as neck and back pain, headaches and migraines. Stress management methods and techniques can ultimately help improve and manage stress associated symptoms. Mindfulness interventions like chiropractic care and mindfulness-based stress reduction have been determined to effectively help reduce stress and alleviate chronic headache symptoms.
Introduction
Headache is one of the most common complaints investigated in adult and pediatric neurological clinics. The vast majority of these headaches are migraine and tension-type headaches (Kurt & Kaplan, 2008). Headaches are classified into two categories of main or primary and secondary headaches. Ninety percent of headaches are primary headaches, among which migraine and tension headaches are the most common types (International Headache Society [IHS], 2013). According to the definition, migraine headache is usually unilateral and pulsating in nature and lasts from 4 to 72 hours. The associated symptoms include nausea, vomiting, increased sensitivity to light, sound and pain, and it generally increases with increasing physical activity. Also, tension headache is characterized by bilateral, non-pulsating pain, pressure or tightness, blunt pain, like a bandage or a hat, and a continuum of mild to moderate pain, preventing daily life activities (IHS, 2013).
Stovner et al. (2007) using the IHS diagnostic criteria, estimated the percentages of the adult population with an active headache disorder about 46% for headache in general, 42% for tension-type headache. This suggests that the incidence and the prevalence of tension-type headache are much higher than it was predicted. It is estimated that about 12 to 18 percent of the people have migraines (Stovner & Andree, 2010). Women are more likely to experience migraines compared to men, migraine prevalence is about 6% for men and 18% for women (Tozer et al., 2006).
Migraine and tension-type headaches are common and well-documented responses to psychological and physiological stressors (Menken, Munsat, & Toole, 2000). Migraine is a periodic and debilitating chronic pain and has a negative impact on quality of life, relationships and productivity. The World Health Organization (WHO) has announced the severe migraine as one of the most debilitating diseases with the nineteenth rank (IHS, 2013; Menken et al., 2000).
Despite the development of many medications for treatment and prevention of migraine attacks, a number of patients find them ineffective and some other find them inappropriate because of their side effects and side-effects often times lead to early discontinuation of treatment. As a result, a great interest in the development of non-pharmacologic treatments can be observed (Mulleners, Haan, Dekker, & Ferrari, 2010).
Biological factors alone cannot explain vulnerability to the experience of the headache, the onset of the attack and its course, intensified attacks of headache, headache-related disability and also the quality of life in patients with chronic headache. Negative life events are (as psychosocial factor) often known as a key factor in the development and exacerbation of headache (Nash & Thebarge, 2006).
The program of Mindfulness-Based Stress reduction (MBSR) is among the treatments, which have been studied in the past two decades on a variety of chronic pain. MBSR developed by Kabat-Zinn and used in a wide range of population with stress-related disorders and chronic pain (Kabat-Zinn, 1990). Especially in recent years, many studies have been conducted to examine the therapeutic effects of MBSR. Most studies have shown the significant effects of MBSR on different psychological conditions including the reduction of psychological symptoms of distress, anxiety, rumination, anxiety and depression (Bohlmeijer, Prenger, Taal, & Cuijpers, 2010; Carlson, Speca, Patel, & Goodey, 2003; Grossman, Niemann, Schmidt, & Walach, 2004; Jain et al., 2007; Kabat-Zinn, 1982; Kabat-Zinn, Lipworth, & Burney, 1985; Kabat-Zinn et al., 1992; Teasdale et al., 2002), pain (Flugel et al., 2010; Kabat-Zinn, 1982; Kabat-Zinn et al., 1985; La Cour & Petersen, 2015; Rosenzweig et al., 2010; Zeidan, Gordon, Merchant, & Goolkasian, 2010) and quality of life (Brown & Ryan, 2003; Carlson et al., 2003; Flugel et al., 2010; Kabat-Zinn, 1982; La Cour & Petersen, 2015; Morgan, Ransford, Morgan, Driban, & Wang, 2013; Rosenzweig et al., 2010).
Bohlmeijer et al. (2010) conducted a meta-analysis of eight randomized controlled studies on the effects of MBSR program, concluded that MBSR has small effects on depression, anxiety and psychological distress in people with chronic medical diseases. Also Grossman et al. (2004) in a meta-analysis of 20 controlled and uncontrolled studies on the effects of the MBSR program on physical and mental health of medical and non-medical samples, found an effect size of moderate for controlled studies on mental health. No effect sizes for specific symptoms such as depression and anxiety were reported. The most recent review includes 16 studies controlled and uncontrolled, This review reports that MBSR intervention decrease pain intensity, and most controlled trial studies (6 of 8) show higher reductions in pain intensity for intervention group compared with control group (Reiner, Tibi, & Lipsitz, 2013).
In another study, researchers found significant effect sizes for some subscales of quality of life for example vitality scale and bodily pain, nonsignificant effect sizes for pain and significant medium to large size effects for lower general anxiety and depression (La Cour & Petersen, 2015). Also in a study by Rosenzweig et al. (2010) on patients with chronic pain including those suffering from migraine, there were significant differences in pain intensity, pain-related functional limitations between patients. However, those suffering from migraine experienced the lowest improvement in pain and different aspects of quality of life. In general, different groups of chronic pain showed significant improvements in pain intensity and pain-related functional limitations in this study. Two other studies were conducted by Kabat-Zinn and using MBSR methods for treating patients with chronic pain, including a number of patients with chronic headaches. Statistical analysis showed a significant reduction in pain, pain interference with daily activities, medical and psychiatric signs and symptoms, anxiety and depression, negative body image, pain interference with daily activities, use of the drug and also increase in confidence (Kabat-Zinn, 1982; Kabat-Zinn et al., 1985).
Due to pain and loss of function and reduced work productivity and increased use of health care, chronic headache impose costs on individual and society, it seems that the chronic headache is a major health problem and finding ways to control and treat this problem could be of great importance. The main objective of this study was to evaluate the effectiveness of MBSR in addition to conventional pharmacotherapy in a clinical population sample of patients with chronic headache to show the effectiveness of this technique as a method of pain management and enhancement of the quality of life in patients with chronic headaches.
Methods
Participants and Procedure
This is a randomized controlled trial two- group �pretest-posttest� study design. Also an approval was obtained from the Ethics Committee of Zahedan University of Medical Sciences. The participants selected through convenience sampling method from patients with chronic migraine and tension-type headache, diagnosed by a neurologist and a psychiatrist using IHS diagnostic criteria-referred to university hospitals of Zahedan University of Medical Sciences, Zahedan-Iran.
After evaluating each patient for meeting the inclusion and exclusion criteria and taking an initial interview, 40 out of eighty-seven primary patients with chronic headache were selected and randomly assigned into two equal groups of intervention and control. Both the control and intervention groups received common pharmacotherapy under the supervision of the neurologist. During therapy sessions three subjects, due to the lack of a regular presence or exclusion criteria, opted out or were excluded from the study.
Inclusion Criteria
(1) Informed consent to participate in the sessions.
(2) Minimum age of 18 years.
(3) Minimum educational qualification of middle-school degree.
(4) The diagnosis of chronic headache (primary chronic migraine and tension-type headache) by the neurologist and according to IHS diagnostic criteria.
(5) 15 or more days per month for more than 3 months and least six months history of migraines and tension-type headache
Exclusion Criteria
(1) Subjects who were not willing to continue the participation in the study or leave the study for any reason.
(2) Other chronic pain problems.
(3) Psychosis, delirium and cognitive disorders.
(4) Cases of interpersonal difficulties interfering with teamwork.
(5) Drug and substance abuse.
(6) Mood disorder
Intervention Groups
Therapy sessions (MBSR) were held for 1.5 to 2 hours a week for the members of the intervention group (drug plus MBSR); While no MBSR was performed for the control group (only common drugs used) until the end of the research. The MBSR was carried out for 8 weeks. In this study, the 8-session MBSR program (Chaskalon, 2011) has been used. To do the meditation homework while training participants in sessions, the necessary measures have been provided in a CD and a booklet. If any one of subjects did not participate in a session or sessions, at the beginning of the next session the therapist would provide written notes of the sessions to the subjects, in addition to repeat the previous session summaries. MBSR program and discussions were presented to the patients in the eight sessions including: understanding pain and its aetiology, discuss about relationship stress, anger and emotion with pain, Understanding negative automatic thoughts, identyfying thoughts and feelings, introducing the concept of Acceptance, breathing space, three-minute breathing space, breath focus exercise, pleasant and unpleasant events daily, behavioral activation, mindfulness of routine activity, body scan practice, Seeing and hearing exercise, sitting meditation, mindful walking, reading poems related to mindfulness and also discuss how to keep up what has been developed over the whole course, discuss plans and positive reasons for maintaining the practice. Patients also received information about learning how to detect any future relapses as well as strategies and plans on which to base early detection of symptom pain attacks and for being self-directed towards new situations.
Control Group
Patients who were randomized in the control group were continuing usual pharmacotherapy(including specific and nonspecific drugs) by their neurologist until the end of the research.
Instruments
Two main tools were used in the pre-test and post-test to collect data, in addition to demographic data form. Headache log was used to determine the perceived intensity of pain using three parts: (1) 10-point likert-scale ratings, (2) the number of hours of pain per day and (3) pain frequency during the month. Each part is scored from 0 to 100, the highest level being 100. Since each patient rates their perceived pain intensity in the questionnaire, validity and reliability are not considered. And the other was a short-form 36 questionnaire (SF-36). The questionnaire is applicable in the various age groups and different diseases. The reliability and validity of the questionnaire was approved by Ware et al (Ware, Osinski, Dewey, & Gandek, 2000). The SF-36 assesses the perception of the quality of life in 8 subscales include: physical functioning (PF), role limitations due to physical health (RP), bodily pain (PB), general health (GH), energy and vitality (VT), social functioning (SF), role limitations due to emotional problems (RE) and affect health (AH). The tool has also two summary scales for Physical Component Summary (PCS) and Mental Component Summary (MCS) scores. Each scale is scored from 0 to 100, the highest functional status level being 100. The validity and reliability of the SF-36 were examined in an Iranian population. Internal consistency coefficients were between 0.70 and 0.85 for the 8 subscales and test-retest coefficients were between 0.49 and 0.79 with an interval of one week (Montazeri, Goshtasebi, Vahdaninia, & Gandek, 2005).
Data Analysis
For analyzing the data, in addition to the use of descriptive indicators, to compare the results of the intervention and control groups, the analysis of covariance was used to determine the effectiveness and the removal of the pre-test results at 95% confidence level.
Drop-Out
During therapy sessions three subjects, due to the lack of a regular presence or exclusion criteria, opted out or were excluded from the study. Thirty-seven out of 40 patients completed current study and the gathered data were then analyzed.
Results
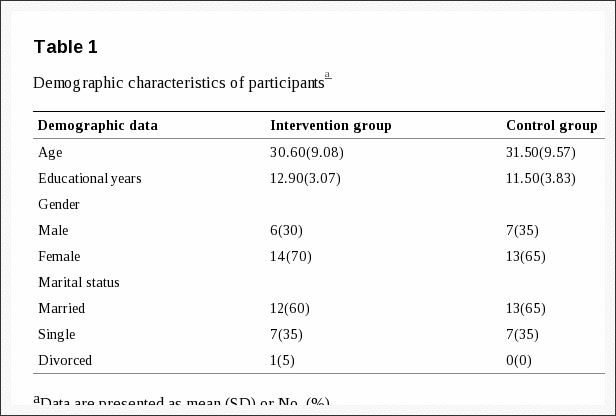
Analysis for comparison of demographic distribution between the two groups was performed using chi-square and independent t-test. Demographic data of both groups are shown in Table 1. Distribution of age, educational years, gender and marital status were the same in each group.
Table 1: Demographic characteristics of participants.
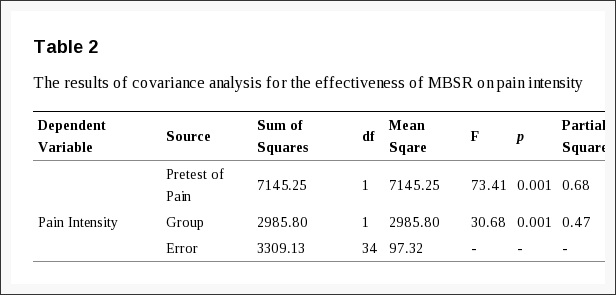
Table 2 shows the results of analysis of covariance (ANCOVA). Levene�s test was non-significant, F (1, 35) = 2.78, P = 0.105, indicating that the assumption of homogeneity of variance had been approved. This finding shows that the variances across groups are equal and no difference was observed between two groups.
Table 2: The results of covariance analysis for the effectiveness of MBSR on pain intensity.
The main effect of MBSR intervention was significant, F (1, 34) = 30.68, P = 0.001, partial ?2 = 0.47, indicating that the pain intensity was lower after MBSR intervention (Mean = 53.89, SD.E = 2.40) than control group (Mean = 71.94, SD.E = 2.20). The covariate (pre-test of pain) was also significant, F (1, 34) = 73.41, P = 0.001, partial ?2 = 0.68, indicating that level of pain intensity before MBSR intervention had a significant effect on level of pain intensity. In other words, there was a positive relationship in the pain scores between pre-test and post-test. Therefore, the first research hypothesis is confirmed and MBSR treatment on perceived intensity was effective in patients with chronic headache and could reduce the intensity of perceived pain in these patients. All significant values are reported at p<0.05.
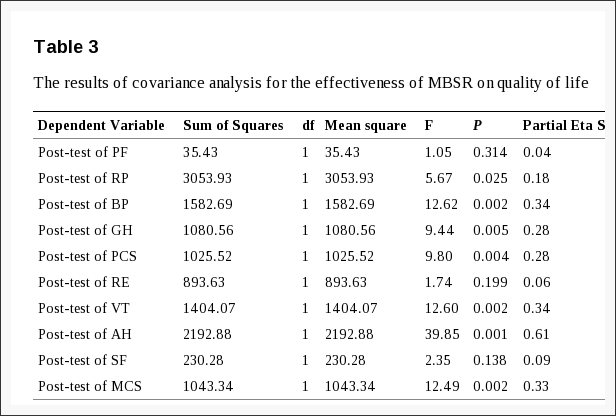
The second hypothesis of this study is the effectiveness of MBSR technique on quality of life in patients with chronic headache. To evaluate the effectiveness of MBSR technique on quality of life in patients with chronic headaches and eliminating the confounding variables and the effect of pre-test, for the analysis of data, multivariate covariance analysis (MANCOVA) of the dimensions of quality of life is used that Table 3 shows the results of analysis in the intervention group.
Table 3: The results of covariance analysis for the effectiveness of MBSR on quality of life.
The Table 3 shows the results of analysis of covariance (MANCOVA). The following information is needed to understand the results presented in Table 3.
The box�s test was non- significant, F = 1.08, P = 0.320, indicating that the variance�covariance matrices are the same in two groups and therefore the assumption of homogeneity is met. Also F (10, 16) = 3.153, P = 0.020, Wilks� Lambda = 0.33, partial ?2 = 0.66, indicating was a significant difference between the pre-test of the groups in the dependent variables.
Levene�s test was non-significant in some of dependent variables including [PF: F (1, 35) = 3.19, P = 0.083; RF: F (1, 35) = 1.92, P = 0.174; BP: F (1, 35) = 0.784, P = 0.382; GH: F (1, 35) = 0.659, P = 0.422; PCS: F (1, 35) = 2.371, P = 0.133; VT: F (1, 35) = 4.52, P = 0.141; AH: F (1, 35) = 1.03, P = 0.318], indicating that the assumption of homogeneity of variance had been approved in subscales of quality of life and Levene�s test was significant in some of dependent variables including [RE: F (1, 35) = 4.27, P = 0.046; SF: F (1, 35) = 4.82, P = 0.035; MCS: F (1, 35) = 11.69, P = 0.002], showing that the assumption of homogeneity of variance had been broken in subscales of quality of life.
The main effect of MBSR intervention was significant for some of dependent variables including [RP: F (1, 25) = 5.67, P = 0.025, partial ?2 = 0.18; BP: F (1, 25) = 12.62, P = 0.002, partial ?2 = 0.34; GH: F (1, 25) = 9.44, P = 0.005, partial ?2 = 0.28; PCS: F (1, 25) = 9.80, P = 0.004, partial ?2 = 0.28; VT: F (1, 25) = 12.60, P = 0.002, partial ?2 = 0.34; AH: F (1, 25) = 39.85, P = 0.001, partial ?2 = 0.61; MCS: F (1, 25) = 12.49, P = 0.002, partial ?2 = 0.33], these results indicating that subscales of RP, BP, GH, PCS, VT, AH, and MCS were higher after MBSR intervention [RP: Mean = 61.62, SD.E = 6.18; BP: Mean = 48.97, SD.E = 2.98; GH: Mean = 48.77, SD.E = 2.85; PCS: Mean = 58.52, SD.E = 2.72; VT: Mean = 44.99, SD.E = 2.81; AH: Mean = 52.60, SD.E = 1.97; MCS: Mean = 44.82, SD.E = 2.43] than control group [RP: Mean = 40.24, SD.E = 5.62; BP: Mean = 33.58, SD.E = 2.71; GH: Mean = 36.05, SD.E = 2.59; PCS: Mean = 46.13, SD.E = 2.48; VT: Mean = 30.50, SD.E = 2.56; AH: Mean = 34.49, SD.E = 1.80; MCS: Mean = 32.32, SD.E = 2.21].
Nonetheless, the main effect of MBSR intervention was non-significant for some of dependent variables including [PF: F (1, 25) = 1.05, P = 0.314, partial ?2 = 0.04; RE: F (1, 25) = 1.74, P = 0.199, partial ?2 = 0.06; SF: F (1, 25) = 2.35, P = 0.138, partial ?2 = 0.09]. These results indicating, although the means in these subscales of quality of life were higher [PF: Mean = 75.43, SD.E = 1.54; RE: Mean = 29.65, SD.E = 6.02; SF: Mean = 51.96, SD.E = 2.63] than the control group [PF: Mean = 73.43, SD.E = 1.40; RE: Mean = 18.08, SD.E = 5.48; SF: Mean = 46.09, SD.E = 2.40], But Mean difference was non-significant.
In summary, Covariance analysis (MANCOVA) results in Table 3 indicate a statistically significant difference in the scores of subscales of role limitation due to physical health (RP), bodily pain (BP), general health (GH), energy and vitality (VT), Affect health (AH) and sum of physical health dimensions (PCS) and mental health (MCS). And also indicates that there was not a statistically significant difference in subscale scores of physical functioning (PF), role limitations due to emotional problems (RE) and social functioning (SF) in the intervention group. All significant values are reported at p<0.05.
Discussion
This study aimed to evaluate the effectiveness of MBSR on perceived pain intensity and quality of life in patients with chronic headache. The results showed that MBSR treatment was significantly effective on reduction of pain intensity perception. The results of current study are consistent with the results of other researchers who had used the same method for chronic pain (e.g. Flugel et al., 2010; Kabat-Zinn, 1982; Kabat-Zinn et al., 1985; La Cour & Petersen, 2015; Reibel, Greeson, Brainard, & Rosenzweig, 2001; Reiner et al., 2013; Rosenzweig et al., 2010; zeidan et al., 2010). For example, in two studies conducted by Kabat-Zinn, where the MBSR program was used for treating patients with chronic pain by physicians, a number of patients with chronic headache were also included. The first study of the two studies, showed a significant reduction in pain, pain interference with daily activities, medical signs and psychiatric disorders, including anxiety and depression (Kabat-Zinn, 1982). The results of second study showed significant reduction in pain, negative body image, anxiety, depression, pain interference with daily activities, medical symptoms, medication use, and also showed an increase in self-confidence (Kabat-Zinn et al., 1985).
Also, the findings of the current study are consistent with the results of Rosenzweig et al. (2010), their results suggest that MBSR program is effective for reduction, physical pain, quality of life and psychological well-being of patients with various chronic pains and mindfulness is effective on emotional and sensory components of pain perception by self-regulation of attention through meditation activities. Although the results of Rosenzweig et al. (2010) showed that among patients with chronic pain the minimal impact on the reduction in bodily pain and improvement in quality of life was related to patients with fibromyalgia, chronic headache. In another study conducted by Flugel et al. (2010), although positive changes were observed in the frequency and the intensity of pain, the pain reduction was not statistically significant.
In another study, pain severity significantly reduced after the intervention in patients with tension headache. In addition, the MBSR group showed higher scores in mindful awareness in comparison with the control group (Omidi & Zargar, 2014). In a pilot study by Wells et al. (2014), their results showed that MBSR with pharmacological treatment was possible for patients with migraines. Although the small sample size of this pilot study did not provide power to detect a significant difference in the pain severity and migraine frequency, results demonstrated this intervention had a beneficial effect on headache duration, disability, self-efficacy.
In explaining the results of the effectiveness of mindfulness based therapies for pain it can be said, psychological models of chronic pain such as fear-avoidance model showed that the ways by which people interpret their feelings of pain and respond to them are important determinants in the experience of pain (Schutze, Rees, Preece, & Schutze, 2010). Pain catastrophizing is significantly associated with fear and anxiety caused by pain, the cognitive paths through which the fear of pain can be caused and also the pain-related disability is associated and also because the negative cognitive assessment of pain explains 7 to 31% of the variance of the pain intensity. Therefore, any mechanism that can reduce pain catastrophizing or make changes in its process can reduce the perception of pain intensity and the disability caused by that. Schutz et al. (2010) argue that the little mindfulness is the primer of pain catastrophizing. In fact, it seems that the tendency of the individual to engage in the automatic processing processes rather than knowledge-based processes with attention of insufficient flexibility, and lack of awareness of the present moment (Kabat-Zinn, 1990), will cause people to think more about the pain and thus overestimate the resulting risk of it. Thus, little mindfulness allows for the development of negative cognitive evaluation of the pain (Kabat-Zinn, 1990).
Another possible reason may be that the pain acceptance and readiness for change increase positive emotions, leading to a reduction in pain intensity through effects on the endocrine system and the production of endogenous opioids and reduction in pain-related disability or preparing individuals for the use of effective strategies to deal with pain (Kratz, Davis, & Zautra, 2007). Another possible reason to explain the results of the present study in its effectiveness on pain reduction can be the fact that chronic pain is developed due to an overactive stress response system (Chrousos & Gold, 1992). The result is the disturbing of the physical and mental processes. Mindfulness can allow for the access to the frontal cortex and improve it, brain areas that integrate physical and mental functions (Shapiro et al., 1995). The result is the creation of a little stimulation that reduces the intensity and the experience of physical and mental pain. Thus, pain impulses are experienced as feeling of the real pain rather than a negative recognition. The result is the closing of the pain channels that can reduce pain (Astin, 2004).
Mindfulness meditation Reduces Pain Through several Brain Mechanisms and various pathways such as changing of attention in meditation practices might impress both sensory and affective components of pain perception. On the other hand, mindfulness reduces the reactivity to distressing thoughts and feelings that accompany pain perception and strengthen the pain. Also, mindfulness reduces psychological symptoms such as comorbid anxiety and depression and increases parasympathetic activity, which can promote deep muscle relaxation that may reduce pain. Finally, mindfulness may decrease stress and mood dysfunction-related psychophysiologic activation by strengthening reframing negative situation and self-regulation skills. Higher level of mindfulness predicted lower levels of anxiety, depression, catastrophic thinking and disability. Other research has showed that mindfulness has an important role in cognitive and emotional control, and may be useful in reframing negative situations (Zeidan et al., 2011; Zeidan, Grant, Brown, McHaffie, & Coghill, 2012).
The second aim of this study was to determine the effectiveness of the MBSR program on quality of life in patients with chronic headache. This study showed that this treatment was significantly effective on quality of life dimensions, including role limitations due to health status, bodily pain, general health, energy and vitality, emotional health and overall physical and mental health scales. However, the MBSR program could not significantly increase the quality of life in physical functioning, role limitations due to emotional problems and social functioning. It seems apparent from previous and current studies and as well as from the present study that MBSR no effect on physical and social functions. This is likely because that the effects on pain levels in patients with headache are small, and that change is slow. On the other hand, patients with chronic pain have often learned to ignore pain in order to function normally (La Cour & Petersen, 2015). Although, the changes have been in the desired direction and increased the mean scores of the intervention group compared with the control group. These findings are consistent with previous findings (Brown & Ryan, 2003; Carlson et al., 2003; Flugel et al., 2010; Kabat-Zinn, 1982; La Cour & Petersen, 2015; Morgan et al., 2013; Reibel et al., 2001; Rosenzweig et al., 2010).
With regard to the content of the MBSR sessions, this program emphasizes the application of techniques to reduce stress, deal with pain and the awareness of the situation. Giving up the fight and accepting the present situation, without judgment, is the main concept of the program (Flugel et al., 2010). In fact, changes in acceptance without judgment are associated with improvement in quality of life (Rosenzweig et al., 2010). MBSR is aimed to increase awareness of the present moment. The treatment plan is a new and personal way to deal with stress to the individual. External stressors are part of life and cannot be changed, but coping skills and how to respond to the stress can be changed (Flugel et al., 2010). McCracken and velleman (2010) showed that cognitive flexibility and higher mindfulness is associated with less suffering and disability in patients. Patients with chronic pain with higher levels of mindfulness reported less depression, stress, anxiety and pain and also improvement in the self-efficacy and quality of life. Morgan et al. (2013) studying arthritis patients achieved similar results, so that patients with higher levels of mindfulness reported lower stress, depression and higher self-efficacy and quality of life. As noted above it was expected that pain reduction in patients leads to reduced fear and anxiety associated with pain and thereby reduces the resulting functioning limitations. Also, the results of the several studies (Cho, Heiby, McCracken, Lee, & Moon, 2010; McCracken, Gauntlett-Gilbert, & Vowles, 2007; Rosenzweig et al., 2010; Schutz et al., 2010) confirm this finding.
Several studies have been done to evaluate the effectiveness of different types of mindfulness-based treatments on chronic pain, including patients with headache. Unlike other research that examined heterogeneous sets of patients with chronic pain, the advantage of this study is that, it has been only performed on patients with chronic headache.
In the end, it should be acknowledged that there are some limitations in this study such as small sample size, lack of a long-term follow-up program, participants� medication use and arbitrary treatments; and despite the efforts of researchers, the lack of fully similar pharmacotherapy for all participants can confound the test results and make it difficult to generalize the results. Since the present study is the first of its type in patients with chronic headache in Iran, it is suggested that similar studies should be carry out in this field, with larger sample sizes as possible. And further studies investigate the stability of the treatment results in long-term follow-up periods of time.
Conclusion
According to the findings of this study it can be concluded that MBSR methods generally are effective on perceived pain intensity and quality of life of patients with chronic headache. Although there was no statistically significant difference in some aspects of quality of life, such as physical functioning, role limitations due to emotional problems and social functioning, but overall changes in mean were desired to the study. Thus the integrating of MBSR treatment with conventional medical therapy in the treatment protocol for patients with chronic headache can be advised. The researcher also believes that despite the shortcomings and deficiencies of current research, this study could be a new approach to the treatment of chronic headache and could provide a new horizon in this field of treatment.
Acknowledgements
This research was supported (as a thesis) in part by Zahedan University of Medical Sciences. We would like to thank all participants in the study, local healers, the staff of hospitals- Ali -ebn-abitaleb, Khatam-al-anbia and Ali asghar- for their support and help.
In conclusion,�chiropractic care is a safe and effective alternative treatment option utilized to help improve as well as manage chronic headache symptoms by carefully and gently realigning the spine as well as providing stress management methods and techniques. Because stress has been associated with a variety of health issues, including subluxation, or misalignment of the spine, and chronic headache, mindfulness interventions like chiropractic care and mindfulness-based stress reduction (MBSR) are fundamental towards chronic headache. Finally, the article above demonstrated that MBSR can be effectively used as a mindfulness intervention for chronic headache and to improve overall health and wellness. Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Back Pain
According to statistics, approximately 80% of people will experience symptoms of back pain at least once throughout their lifetimes. Back pain is a common complaint which can result due to a variety of injuries and/or conditions. Often times, the natural degeneration of the spine with age can cause back pain. Herniated discs occur when the soft, gel-like center of an intervertebral disc pushes through a tear in its surrounding, outer ring of cartilage, compressing and irritating the nerve roots. Disc herniations most commonly occur along the lower back, or lumbar spine, but they may also occur along the cervical spine, or neck. The impingement of the nerves found in the low back due to injury and/or an aggravated condition can lead to symptoms of sciatica.
1. Astin J A. Health psychology therapies for the management of pain. Clinical Journal of Pain. 2004;20:27�32. http://dx.doi.org/10.1097/00002508-200401000-00006 . [PubMed]
2. Bohlmeijer E, Prenger R, Taal E, Cuijpers P. The effects of mindfulness-based stress reduction therapy on mental health of adults with a chronic medical disease: a meta-analysis. J Psychosom Res. 2010;68(6):539�544. http://dx.doi.org/10.1016/j.jpsychores.2009.10.005 . [PubMed]
3. Brown K. W, Ryan R. M. The benefits of being present: mindfulness and its role in psychological well-being. J Pers Soc Psychol. 2003;84(4):822�848. http://dx.doi.org/10.1037/0022-3514.84.4.822 . [PubMed]
4. Carlson L. E, Speca M, Patel K. D, Goodey E. Mindfulness-based stress reduction in relation to quality of life, mood, symptoms of stress, and immune parameters in breast and prostate cancer outpatients. Psychosom Med. 2003;65(4):571�581. [PubMed]
5. Chaskalson M. The mindful workplace: developing resilient individuals and resonant organizations with MBSR. John Wiley & Sons; 2011.
6. Cho S, Heiby E. M, McCracken L. M, Lee S. M, Moon D. E. Pain-related anxiety as a mediator of the effects of mindfulness on physical and psychosocial functioning in chronic pain patients in Korea. J Pain. 2010;11(8):789�797. http://dx.doi.org/10.1016/j.jpain.2009.12.006 . [PubMed]
7. Chrousos G. P, Gold P. W. The concepts of stress and stress system disorders. Overview of physical and behavioral homeostasis. JAMA. 1992;267(9):1244�1252. http://dx.doi.org/10.1001/jama.1992.03480090092034 . [PubMed]
8. Flugel Colle K. F, Vincent A, Cha S. S, Loehrer L. L, Bauer B. A, Wahner-Roedler D. L. Measurement of quality of life and participant experience with the mindfulness-based stress reduction program. Complement Ther Clin Pract. 2010;16(1):36�40. http://dx.doi.org/10.1016/j.ctcp.2009.06.008 . [PubMed]
9. Grossman P, Niemann L, Schmidt S, Walach H. Mindfulness-based stress reduction and health benefits. A meta-analysis. J Psychosom Res. 2004;57(1):35�43. http://dx.doi.org/10.1016/S0022-3999(03)00573-7 . [PubMed]
10. Headache Classification Committee of the International Headache, Society. The International Classification of Headache Disorders, 3rd edition (beta version) Cephalalgia. 2013;33(9):629�808. http://dx.doi.org/10.1177/0333102413485658 . [PubMed]
11. Jain S, Shapiro S. L, Swanick S, Roesch S. C, Mills P. J, Bell I, Schwartz G. E. A randomized controlled trial of mindfulness meditation versus relaxation training: effects on distress, positive states of mind, rumination, and distraction. Ann Behav Med. 2007;33(1):11�21. http://dx.doi.org/10.1207/s15324796abm3301_2 . [PubMed]
12. Kabat-Zinn J. An outpatient program in behavioral medicine for chronic pain patients based on the practice of mindfulness meditation: theoretical considerations and preliminary results. Gen Hosp Psychiatry. 1982;4(1):33�47. [PubMed]
13. Kabat-Zinn Jon, University of Massachusetts Medical Center/Worcester . Stress Reduction Clinic. Full catastrophe living: using the wisdom of your body and mind to face stress, pain, and illness. New York, N.Y: Delacorte Press; 1990.
14. Kabat-Zinn J, Lipworth L, Burney R. The clinical use of mindfulness meditation for the self-regulation of chronic pain. J Behav Med. 1985;8(2):163�190. http://dx.doi.org/10.1007/BF00845519 . [PubMed]
15. Kabat-Zinn J, Massion A. O, Kristeller J, Peterson L. G, Fletcher K. E, Pbert L, Santorelli S. F. Effectiveness of a meditation-based stress reduction program in the treatment of anxiety disorders. Am J Psychiatry. 1992;149(7):936�943. http://dx.doi.org/10.1176/ajp.149.7.936 . [PubMed]
16. Kratz A. L, Davis M. C, Zautra A. J. Pain acceptance moderates the relation between pain and negative affect in female osteoarthritis and fibromyalgia patients. Ann Behav Med. 2007;33(3):291�301. http://dx.doi.org/10.1080/08836610701359860 . [PMC free article] [PubMed]
17. Kurt S, Kaplan Y. Epidemiological and clinical characteristics of headache in university students. Clin Neurol Neurosurg. 2008;110(1):46�50. http://dx.doi.org/10.1016/j.clineuro.2007.09.001 . [PubMed]
18. La Cour P, Petersen M. Effects of mindfulness meditation on chronic pain: a randomized controlled trial. Pain Med. 2015;16(4):641�652. http://dx.doi.org/10.1111/pme.12605 . [PubMed]
19. McCracken L. M, Gauntlett-Gilbert J, Vowles K. E. The role of mindfulness in a contextual cognitive-behavioral analysis of chronic pain-related suffering and disability. Pain. 2007;131(1-2):63�69. http://dx.doi.org/10.1016/j.pain.2006.12.013 . [PubMed]
20. McCracken L. M, Velleman S. C. Psychological flexibility in adults with chronic pain: a study of acceptance, mindfulness, and values-based action in primary care. Pain. 2010;148(1):141�147. http://dx.doi.org/10.1016/j.pain.2009.10.034 . [PubMed]
21. Menken M, Munsat T. L, Toole J. F. The global burden of disease study: implications for neurology. Arch Neurol. 2000;57(3):418�420. http://dx.doi.org/10.1001/archneur.57.3.418 . [PubMed]
22. Montazeri A, Goshtasebi A, Vahdaninia M, Gandek B. The Short Form Health Survey (SF-36): translation and validation study of the Iranian version. Qual Life Res. 2005;14(3):875�882. http://dx.doi.org/10.1007/s11136-004-1014-5 . [PubMed]
23. Morgan N. L, Ransford G. L, Morgan L. P, Driban J. B, Wang C. Mindfulness is associated with psychological symptoms, self-efficacy, and quality of life among patients with symptomatic knee osteoarthritis. Osteoarthritis and Cartilage. 2013;21(Supplement):S257�S258. http://dx.doi.org/10.1016/j.joca.2013.02.535 .
24. Mulleners W. M, Haan J, Dekker F, Ferrari M. D. Preventive treatment for migraine. Ned Tijdschr Geneeskd. 2010;154:A1512. [PubMed]
25. Nash J. M, Thebarge R. W. Understanding psychological stress, its biological processes, and impact on primary headache. Headache. 2006;46(9):1377�1386. http://dx.doi.org/10.1111/j.1526-4610.2006.00580.x . [PubMed]
26. Omidi A, Zargar F. Effect of mindfulness-based stress reduction on pain severity and mindful awareness in patients with tension headache: a randomized controlled clinical trial. Nurs Midwifery Stud. 2014;3(3):e21136. [PMC free article] [PubMed]
27. Reibel D. K, Greeson J. M, Brainard G. C, Rosenzweig S. Mindfulness-based stress reduction and health-related quality of life in a heterogeneous patient population. Gen Hosp Psychiatry. 2001;23(4):183�192. http://dx.doi.org/10.1016/S0163-8343(01)00149-9 . [PubMed]
28. Reiner K, Tibi L, Lipsitz J. D. Do mindfulness-based interventions reduce pain intensity? A critical review of the literature. Pain Med. 2013;14(2):230�242. http://dx.doi.org/10.1111/pme.12006 . [PubMed]
29. Rosenzweig S, Greeson J. M, Reibel D. K, Green J. S, Jasser S. A, Beasley D. Mindfulness-based stress reduction for chronic pain conditions: variation in treatment outcomes and role of home meditation practice. J Psychosom Res. 2010;68(1):29�36. http://dx.doi.org/10.1016/j.jpsychores.2009.03.010 . [PubMed]
30. Schutze R, Rees C, Preece M, Schutze M. Low mindfulness predicts pain catastrophizing in a fear-avoidance model of chronic pain. Pain. 2010;148(1):120�127. http://dx.doi.org/10.1016/j.pain.2009.10.030 . [PubMed]
31. Shapiro D. H, Wu J, Hong C, Buchsbaum M. S, Gottschalk L, Thompson V. E, Hillyard D, Hetu M, Friedman G. Exploring the relationship between having control and losing control to functional neuroanatomy within the sleeping state. Psychologia. 1995;38:133�145.
32. Stovner L, Hagen K, Jensen R, Katsarava Z, Lipton R, Scher A, Zwart J. A. The global burden of headache: a documentation of headache prevalence and disability worldwide. Cephalalgia. 2007;27(3):193�210. http://dx.doi.org/10.1111/j.1468-2982.2007.01288.x . [PubMed]
33. Stovner L. J, Andree C. Prevalence of headache in Europe: a review for the Eurolight project. J Headache Pain. 2010;11(4):289�299. http://dx.doi.org/10.1007/s10194-010-0217-0 . [PMC free article] [PubMed]
34. Teasdale J. D, Moore R. G, Hayhurst H, Pope M, Williams S, Segal Z. V. Metacognitive awareness and prevention of relapse in depression: empirical evidence. J Consult Clin Psychol. 2002;70(2):275�287. http://dx.doi.org/10.1037/0022-006X.70.2.275 . [PubMed]
35. Tozer B. S, Boatwright E. A, David P. S, Verma D. P, Blair J. E, Mayer A. P, Files J. A. Prevention of migraine in women throughout the life span. Mayo Clin Proc. 2006;81(8):1086�1091. quiz 1092. http://dx.doi.org/10.4065/81.8.1086 . [PubMed]
36. Ware J. E, Kosinski M, Dewey J. E, Gandek B. SF-36 health survey: manual and interpretation guide. Quality Metric Inc; 2000.
37. Wells R. E, Burch R, Paulsen R. H, Wayne P. M, Houle T. T, Loder E. Meditation for migraines: a pilot randomized controlled trial. Headache. 2014;54(9):1484�1495. http://dx.doi.org/10.1111/head.12420 . [PubMed]
38. Zeidan F, Gordon N. S, Merchant J, Goolkasian P. The effects of brief mindfulness meditation training on experimentally induced pain. J Pain. 2010;11(3):199�209. http://dx.doi.org/10.1016/j.jpain.2009.07.015 . [PubMed]
39. Zeidan F, Grant J. A, Brown C. A, McHaffie J. G, Coghill R. C. Mindfulness meditation-related pain relief: evidence for unique brain mechanisms in the regulation of pain. Neurosci Lett. 2012;520(2):165�173. http://dx.doi.org/10.1016/j.neulet.2012.03.082 . [PMC free article] [PubMed]
40. Zeidan F, Martucci K. T, Kraft R. A, Gordon N. S, McHaffie J. G, Coghill R. C. Brain mechanisms supporting the modulation of pain by mindfulness meditation. The Journal of Neuroscience. 2011;31(14):5540�5548. http://dx.doi.org/10.1523/JNEUROSCI.5791-10.2011 . [PMC free article] [PubMed]
Stress is a result of the human body’s “fight or flight” response, a prehistoric defense mechanism triggered by the sympathetic nervous system (SNS). Stress is an essential component of survival. When stressors activate the fight or flight response, a mixture of chemicals and hormones are secreted into the blood flow, which prepare the body for perceived danger. Although short-term stress is helpful, however, long-term stress can lead to a variety of health issues. Furthermore, stressors in modern society have changed and it’s become more difficult for people to manage their stress and maintain mindfulness.
How Does Stress Affect the Body?
Stress can be experienced through three different channels: emotion; body and environment. Emotional stress involves adverse situations which affect our mind and decision making. Bodily stress includes improper nutrition and a lack of sleep. And finally, environmental stress occurs based on external experiences. When you experience any of these types of stressors, the sympathetic nervous system will trigger the “fight or flight” response, releasing adrenaline and cortisol to increase heart rate and heighten our senses to make us more alert in order to face the situation ahead of us.
However, if perceived stressors are always present, the SNS’s fight or flight response can remain active. Chronic stress can then lead to a variety of health issues, such as anxiety, depression, muscle tension, neck and back pain, digestive problems, weight gain and sleep problems as well as impaired memory and concentration. In addition, muscle tension along the spine due to stress can cause a spinal misalignment, or subluxation, which may in turn lead to disc herniation.
Headache and Disc Herniation from Stress
A herniated disc occurs when the soft, gel-like center of an intervertebral disc pushes through a tear in its outer, cartilage ring, irritating and compressing the spinal cord and/or the nerve roots. Disc herniation commonly occurs in the cervical spine, or neck, and in the lumbar spine, or low back. Symptoms of herniated discs depend on the location of the compression along the spine. Neck pain and back pain accompanied by numbness, tingling sensations and weakness along the upper and lower extremities are some of the most common symptoms associated with disc herniation. Headache and migraine are also common symptoms associated with stress and herniated discs along the cervical spine, as a result of muscle tension and spinal misalignment.
Mindfulness Interventions for Stress Management
Stress management is essential towards improving as well as maintaining overall health and wellness. According to research studies, mindfulness interventions, such as chiropractic care and mindfulness-based stress reduction (MBSR), among others, can safely and effectively help reduce stress. Chiropractic care utilizes spinal adjustments and manual manipulations to carefully restore the original alignment of the spine, relieving pain and discomfort as well as easing muscle tension. Additionally, a chiropractor may include lifestyle modifications to help further improve symptoms of stress.�A balanced spine can help the nervous system respond to stress more effectively. MBSR can also help reduce stress, anxiety and depression.
Contact Us Today
If you are experiencing symptoms of stress with headache or migraine as well as neck and back pain associated with disc herniation, mindfulness interventions such as chiropractic care can be a safe and effective treatment for your stress. Dr. Alex Jimenez’s stress management services can help you achieve overall health and wellness. Seeking the proper mindfulness interventions can get you the relief you deserve. The purpose of the following article is to demonstrate the effects of mindfulness-based stress reduction in patients with tension headache. Don’t just treat the symptoms, get to the source of the issue.
Effects of Mindfulness-Based Stress Reduction on Perceived Stress and Psychological Health in Patients with Tension Headache
Abstract
Background: Programs for improving health status of patients with illness related to pain, such as headache, are often still in their infancy. Mindfulness-based stress reduction (MBSR) is a new psychotherapy that appears to be effective in treating chronic pain and stress. This study evaluated efficacy of MBSR in treatment of perceived stress and mental health of client who has tension headache.
Materials and Methods: This study is a randomized clinical trial. Sixty patients with tension type headache according to the International Headache Classification Subcommittee were randomly assigned to the Treatment As Usual (TAU) group or experimental group (MBSR). The MBSR group received eight weekly classmates with 12-min sessions. The sessions were based on MBSR protocol. The Brief Symptom Inventory (BSI) and Perceived Stress Scale (PSS) were administered in the pre- and posttreatment period and at 3 months follow-up for both the groups.
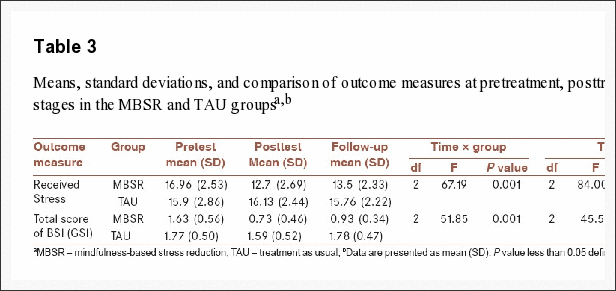
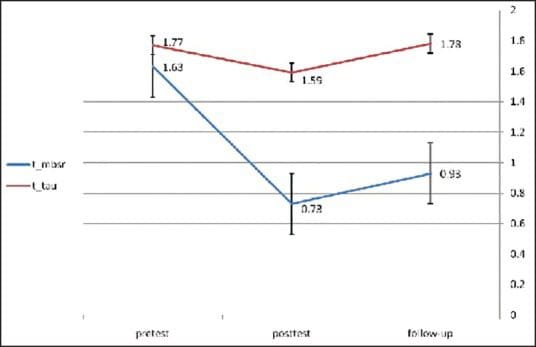
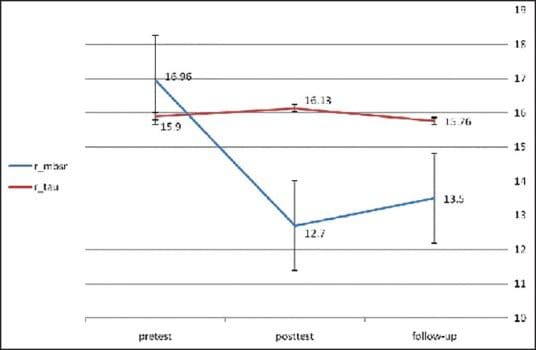
Results: The mean of total score of the BSI (global severity index; GSI) in MBSR group was 1.63 � 0.56 before the intervention that was significantly reduced to 0.73 � 0.46 and 0.93 � 0.34 after the intervention and at the follow-up sessions, respectively (P < 0.001). In addition, the MBSR group showed lower scores in perceived stress in comparison with the control group at posttest evaluation. The mean of perceived stress before the intervention was 16.96 � 2.53 and was changed to 12.7 � 2.69 and 13.5 � 2.33 after the intervention and at the follow-up sessions, respectively (P < 0.001). On the other hand, the mean of GSI in the TAU group was 1.77 � 0.50 at pretest that was significantly reduced to 1.59 � 0.52 and 1.78 � 0.47 at posttest and follow-up, respectively (P < 0.001). Also, the mean of perceived stress in the TAU group at pretest was 15.9 � 2.86 and that was changed to 16.13 � 2.44 and 15.76 � 2.22 at posttest and follow-up, respectively (P < 0.001).
Conclusion: MBSR could reduce stress and improve general mental health in patients with tension headache.
Chiropractic care is an effective stress management treatment because it focuses on the spine, which is the base of the nervous system. Chiropractic utilizes spinal adjustments and manual manipulations to carefully restore the alignment of the spine in order to allow the body to naturally heal itself. A spinal misalignment, or subluxation, can create muscle tension along the spine and lead to a variety of health issues, including headache and migraine, as well as disc herniation and sciatica. Chiropractic care can also include lifestyle modifications, such as nutritional advice and exercise recommendations, to further enhance its effects. Mindfulness-based stress reduction can also effectively help with stress management and symptoms.
Introduction
Tension headache constitutes 90% of total headaches. About 3% of the population are suffering from chronic tension headache.[1] Tension headaches are often associated with lower quality of life and high levels of psychological discomforts.[2] In recent years, several meta-analyses evaluating the established pain treatments used today have shown that medical treatments, which may be effective in acute pain, are not effective with chronic pain and may, in fact, be causing further problems. Most of the pain treatments are designed for and useful for acute pain but if used in the long run may create more problems such as substance abuse and avoidance of important activities.[3] A common element in most of the pain treatments is that they emphasize on either avoiding pain or fighting to reduce pain. The pain in tension headache can be intolerable. Painkillers and pain management strategies can increase intolerance and sensitivity to pain. Therefore, the treatments that increase acceptance and tolerance to pain, especially chronic pain, are effective. Mindfulness-based stress reduction (MBSR) is a new psychotherapy that appears to be effective in improving physical performance and psychological well-being in patients with chronic pain.[4,5,6,7,8] In the past two decades, Kabat-Zinn et al. in the US successfully used mindfulness for the relief of pain and illness related to pain.[9] Recent studies on acceptance-based methods, such as mindfulness, show improved performance in patients with chronic pain. Mindfulness modulates the pain using nonelaborative awareness of thoughts, feelings and sensations, and an emotionally distanced relationship with internal and external experience.[10] Studies found that MBSR program can significantly alleviate medical illness related to chronic pains such as fibromyalgia, rheumatoid arthritis, chronic musculoskeletal pain, chronic low back pain, and multiple sclerosis.[7,11,12,13] MBSR has significant changes in pain intensity, anxiety, depression, somatic complaints, well-being, adaptation, quality of sleep, fatigue, and physical functioning.[6,14,15,16,17] But the programs for improving health status of patients with illness related to pain, such as tension headache, are often still in their infancy. Therefore, the study was conducted to assess the effects of MBSR on perceived stress and general mental health in patients with tension headache.
Materials and Methods
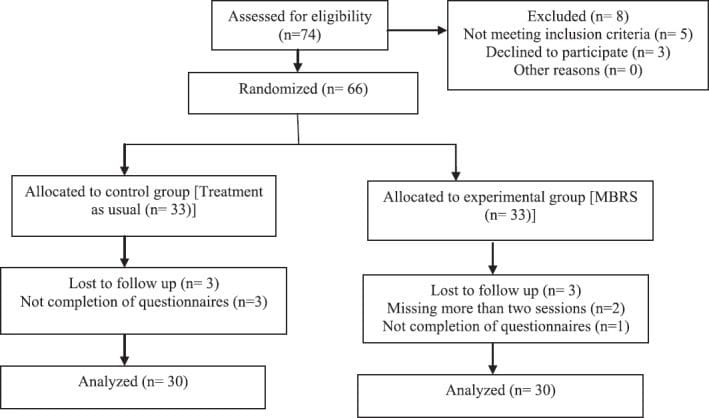
This randomized controlled clinical trial was performed in 2012 in Shahid Beheshti Hospital in Kashan City. The Research Ethics Committee of the Kashan University of Medical Sciences approved this study (IRCT No: 2014061618106N1). The participants of the study included adults with tension headache who were referred by the psychiatrists and neurologists in Kashan. The inclusion criteria were as follows: Having tension headache according to the International Headache Classification Subcommittee, willing to participate in the study, not having a medical diagnosis of organic brain disorder or psychotic disorder, and not having a history of psychological treatment during the preceding 6 months. The patients who did not complete the intervention and missed more than two sessions were excluded from the study. The participants, who signed an informed consent form, completed the measures as a pretest. For estimating the sample size, we referred to another study in which changes in mean of scores of fatigue was 62 � 9.5 in the pretreatment period and 54.5 � 11.5 in the posttreatment period.[18] Then, by utilizing the sample size calculation, 33 participants (with attrition risk) in each group with ? = 0.95 and 1 � ? = 0.9 were segregated. After sample size calculation, 66 patients with tension headache were selected via convenient sampling according to the inclusion criteria. Then, the patients were called and invited to participate in the study. If a patient agreed to participate, then he/she was invited to attend the study-briefing session and if not another patient was selected similarly. Then using a random number table, they were assigned either to the experimental group (MBSR) or to the control group that treated as usual. Finally, 3 patients were excluded from each group and 60 patients were included (30 patients in each group). The TAU group was treated only by antidepressant medication and clinical management. The MBSR group received MBSR training in addition to TAU. The patients in MBSR group were trained for 8 weeks by a clinical psychologist with PhD degree. The Brief Symptom Inventory (BSI) and Perceived Stress Scale (PSS) were administered before the first treatment session in the MBSR group, after the eighth session (posttest), and 3 months after the test (follow-up) in both groups. The TAU group was invited to Shahid Beheshti Hospital to fill out the questionnaires. Figure 1 shows a Consolidated Standards of Reporting Trials (CONSORT) diagram depicting the flow of study participants.
Figure 1: CONSORT diagram depicting flow of study participants.
Intervention
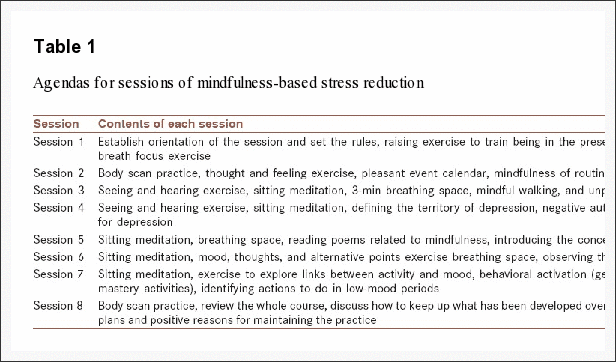
The intervention group (MBSR) was trained in Shahid Beheshti Hospital. The eight weekly sessions (120 min) were held according to the standard MBSR protocol as developed by Kabat-Zinn.[11] Additional sessions were held for the participants who had missed one or two sessions. At the end of the training and 3 months later (follow-up), both MBSR and TAU groups were invited to Shahid Beheshti Hospital (the place of MBSR trial) and were instructed to complete the questionnaires. During the MBSR sessions, the participants were trained to be aware of their thoughts, feelings, and physical sensations nonjudgmentally. Mindfulness exercises are taught as two forms of meditation practices � formal and informal. Formal type exercises include trained sitting meditation, body scan, and mindful yoga. In informal meditation, attention and awareness are focused not only on daily activities, but also on thoughts, feelings, and physical sensation even they are problematic and painful. The overall content of the sessions were mentioned in Table 1.
Table 1: Agendas for sessions of mindfulness-based stress reduction.
Measurement Tools
International Headache Classification Subcommittee Diary Scale for Headache
Headache was measured by diary scale for headache.[19] The patients were asked to record the pain severity diary on a 0-10 rating scale. Absence of pain and the most intense disabling headache were characterized by 0 and 10, respectively. The mean of headache severity in a week was calculated by dividing the sum of the severity scores by 7. Moreover, the mean of headache severity in a month was calculated by dividing the sum of the severity scores by 30. The minimum and maximum scores of headache severity were 0 and 10, respectively. Headache diary was given to five patients and a neurologist and a psychiatrist confirmed the content validity of the instrument.[20] The reliability coefficient of Persian version of this scale was calculated as 0.88.[20]
Brief symptom Inventory (BSI)
Psychological symptoms were assessed with the BSI.[21] The inventory consist 53 items and 9 subscales that assess psychological symptoms. Each item scores between 0 and 4 (for example: I have nausea or upset in my stomach). BSI has a global severity index (GSI) achieved a total score of 53 items. The reliability of the test has reported a score of 0.89.[22] In our study, GSI test�retest estimate was .90 based on a sample of 60 patients with tension headache who completed the BSI.
Perceived Stress Scale (PSS)
Perceived stress was assessed using the PSS,[21,23] a 10-item scale that assesses the degree of uncontrollable and unpredictable situations of life during the past month (for example: Felt that you were unable to control the important things in your life?). Respondents report the prevalence of an item within the last month on a 5-point scale, ranging from 0 (never) to 4 (very often). Scoring is completed by reverse scoring of four positively worded items[4,5,7,8] and summing all item scores. The scale scores range from 0-40. Higher scores indicate higher levels of stress. It assumes that people depending on their coping resources evaluate level of threatening or challenging events. A higher score indicates a greater degree of perceived stress. Adequate test�retest reliability and convergent and discriminate validity have also been reported.[19] In our study, Cronbach’s alpha coefficients for assessing internal consistency of this scale were calculated to be 0.88.
The repeated measures analysis of variance was performed to compare the MBSR and TAU groups on measures of perceived stress and GSI at pretreatment, posttreatment, and 3-month follow-up. Also, Chi-square test was used to compare the demographics in the two groups. P value less than 0.05 was considered significant in all tests.
Results
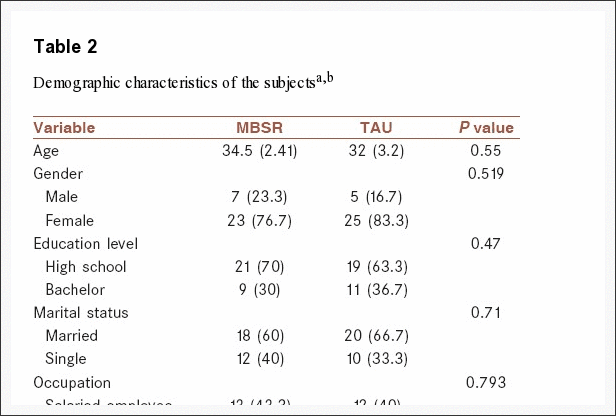
Among 66 subjects, 2 participants from the MBSR group were excluded because of missing more than 2 sessions. Also, three participants were excluded because of did not complete the questionnaires in post-test or follow-up who one of them were from MBSR group and three participants from TAU group. Table 2 showed demographic characteristics of the subjects and results of the randomization check. The results of t-test for differences between the MBSR and TAU groups in age variable and Chi-square test in other variables showed that there was no significant difference between demographic variables in two groups and the subjects were randomly assigned to two groups.
Table 2: Demographic characteristics of the subjects a,b.
Table 3 provides the mean scores and standard deviations of the dependent variables (perceived stress and GSI) and comparison of outcome measures at pretreatment period, post-treatment period, and 3-month follow-up.
Table 3: Means, standard deviations, and comparison of outcome measures at pretreatment, posttreatment, and follow-up stages in the MBSR and TAU groups a,b.
Table 3 shows the more reduction in received stress and GSI in the intervention group (MBSR) compared to TAU group, while the reduction in received stress and GSI were not observed in the TAU group. The results revealed the significant effect of time and interaction between time and type of treatment on the changes of scores (P < 0.001).
Figures ?2 and ?3 present mean received stress and GSI scores for MBSR and TAU groups at posttest and follow-up stages.
Figure 2: CONSORT diagram depicting flow of study participants.
Figure 3: Mean of perceived stress in MBSR and control groups in pretest, posttest, and follow-up.
Discussion
This study compared efficacy of MBSR and Treatment As Usual (TAU) in perceived stress and mental health of patients with tension headache. Although MBSR is recognized as an effective treatment for stress symptoms and pain, there is a need to examine its efficacy for the treatment of mental health problems in patients with tension headache, which is one of the common complaints in the population.
The findings of our study demonstrate enhanced general mental health in the GSI index of BSI. In some study, significant improvements by MBSR intervention were reported on all indexes of the 36-item Short Form Health Survey (SF-36).[20,24] Studies showed significant reduction in psychological problems in the Symptom Checklist-90-Revised (SCL-90-R) subscale such as anxiety and depression by MBSR after intervention and 1-year follow-up.[5] Reibel et al. showed MBSR in patients with chronic pain reported a decrease in medical symptoms such as anxiety, depression, and pain.[5] It has been shown that tension headache and anxiety are accompanied with deficits in controlled cognitive processing such as sustained attention and working memory.[25] Negative emotions may amplify suffering associated with pain perception.
MBSR implements the following mechanisms to improve the patient’s mental status: First, mindfulness leads to increased awareness for what is happening in each moment, with an accepting attitude, without getting caught up in habitual thoughts, emotions, and behavior patterns. The increased awareness then gives rise to new ways to respond and cope in relation to oneself and the world around.[3] Mindfulness establishes a sense of self that is greater than one’s thoughts, feelings, and bodily sensation such as pain. Mindfulness exercises, learned clients develop an �observer�self�. With this ability, they can observe their thoughts and feelings in a nonreactive and nonjudgmental way that previously avoided, that previously avoided thoughts and feelings be observed in a nonreactive and nonjudgmental way. The clients learn to notice thoughts without necessarily acting on them, being controlled by them, or believing them.[3]
Second, mindfulness helps the client develop persistence in taking steps in valued directions that are important to them. Most clients with chronic pain want to become pain free rather than living the vital lives of their choice. But the MBSR program trained them to engage in valued action despite the the pain. Studies have shown attention and emotional reaction to pain has an important role in becoming persistent the pain.[26] Emotional and cognitive components can modulate attention to pain and worry about it that could intensify pain and disrupt the patients activities.[27,28]
Third, findings from some studies indicate that MBSR can alter the function of the brain that is responsible for affect regulation and the areas that govern how we react to stressful impulses, and this in turn may normalize body functions such as breathing, heart rate, and immune function.[29,30] Mindfulness practice reduces reactivity to distressing thoughts and feelings that comorbid and strengthen pain perception.[31] Also mindfulness may lessen psychophysiological activation related to stress and mood dysfunction by strengthening positive reappraisal and emotion regulation skills.[32]
The strength of this study is the use of a new effective psychotherapy in reducing the stress on a complaint that is less studied, but it is a common medical problem. The implications of our study are using a simple psychotherapy that does not make too much cognitive demand and is readily usable as a coping skill for the patient with tension headache. Therefore, the health-care professionals related to this complaint and the patient will be able to use this treatment. Also, MBSR will change the patient’s lifestyle who would be exacerbated by his/her problem. The main limitation of this study was the lack of comparison between MBSR and the gold standard psychotherapies such as cognitive behavior therapy (CBT). It is suggested that future studies need to compare the efficacy of MBSR and other traditional and newer cognitive behavioral therapies in patients with tension headache.
Conclusion
Our study supports the hypothesis that patients suffering from tension headache can enhance their general mental health by participating in the MBSR program. In summary, the results of the present study suggest that MBSR can reduce pain-related anxiety and interference in daily activities in the short term. The unique features of mindfulness exercises are easy training and no need to complex cognitive abilities.
Financial support and sponsorship: Nil.
Conflicts of interest: There are no conflicts of interest.
Author’s Contribution
AO contributed in the conception of the work, conducting the study, and agreed for all aspects of the work. FZ contributed in the conception of the work, revising the draft, approval of the final version of the manuscript and agreed for all aspects of the work.
Acknowledgments
Authors are grateful to the staff of Shahid Beheshti Hospital and participants. Authors also express their gratitude to Kabat-Zinn from the Center for Mindfulness (CFM) at the University of Massachusetts who graciously provided electronic copies of the MBSR guidelines.
In conclusion,�while short-term stress is helpful, long-term stress can eventually lead to a variety of health issues, including anxiety and depression as well as neck and back pain, headache and disc herniation. Fortunately, mindfulness interventions, such as chiropractic care and mindfulness-based stress reduction (MBSR) are safe and effective stress management alternative treatment options. Finally, the article above demonstrated evidence-based results that MBSR could reduce stress and improve general mental health in patients with tension headache. Information referenced from the National Center for Biotechnology Information (NCBI). The scope of our information is limited to chiropractic as well as to spinal injuries and conditions. To discuss the subject matter, please feel free to ask Dr. Jimenez or contact us at 915-850-0900 .
Curated by Dr. Alex Jimenez
Additional Topics: Back Pain
According to statistics, approximately 80% of people will experience symptoms of back pain at least once throughout their lifetimes. Back pain is a common complaint which can result due to a variety of injuries and/or conditions. Often times, the natural degeneration of the spine with age can cause back pain. Herniated discs occur when the soft, gel-like center of an intervertebral disc pushes through a tear in its surrounding, outer ring of cartilage, compressing and irritating the nerve roots. Disc herniations most commonly occur along the lower back, or lumbar spine, but they may also occur along the cervical spine, or neck. The impingement of the nerves found in the low back due to injury and/or an aggravated condition can lead to symptoms of sciatica.
1.�Trkanjec Z, Aleksic-Shihabi A. Tension-type headaches.�Acta Med Croatica.�2008;62:205�10.[PubMed]
2.�Zirke N, Seydel C, Szczepek AJ, Olze H, Haupt H, Mazurek B. Psychological comorbidity in patients with chronic tinnitus: Analysis and comparison with chronic pain, asthma or atopic dermatitis patients.�Qual Life Res.�2013;22:263�72.�[PubMed]
3.�Dionne F, Blais MC, Monestes JL. Acceptance and commitment therapy in the treatment of chronic pain.�Sante Ment Que.�2013;38:131�52.�[PubMed]
4.�Cathcart S, Galatis N, Immink M, Proeve M, Petkov J. Brief mindfulness-based therapy for chronic tension-type headache: A randomized controlled pilot study.�Behav Cogn Psychother.�2013;42:1�15.[PubMed]
5.�Reibel DK, Greeson JM, Brainard GC, Rosenzweig S. Mindfulness-based stress reduction and health-related quality of life in a heterogeneous patient population.�Gen Hosp Psychiatry.�2001;23:183�92.[PubMed]
6.�Grossman P, Niemann L, Schmidt S, Walach H. Mindfulness-based stress reduction and health benefits. A meta-analysis.�J Psychosom Res.�2004;57:35�43.�[PubMed]
7.�Rosenzweig S, Greeson JM, Reibel DK, Green JS, Jasser SA, Beasley D. Mindfulness-based stress reduction for chronic pain conditions: Variation in treatment outcomes and role of home meditation practice.�J Psychosom Res.�2010;68:29�36.�[PubMed]
8.�Kerrigan D, Johnson K, Stewart M, Magyari T, Hutton N, Ellen JM, et al. Perceptions, experiences, and shifts in perspective occurring among urban youth participating in a mindfulness-based stress reduction program.�Complement Ther Clin Pract.�2011;17:96�101.�[PubMed]
9.�Kabat-Zinn J. New York: Dell Publishing; 1990. Full Catastrophe Living; p. 185.
10.�Hayes AM, Feldman G. Clarifying the construct of mindfulness in the context of emotion regulation and the process of change in therapy.�Clin Psychol-Sci Pr.�2004:255�62.
11.�Schmidt S, Grossman P, Schwarzer B, Jena S, Naumann J, Walach H. Treating fibromyalgia with mindfulness-based stress reduction: Results from a 3-armed randomized controlled trial.�Pain.�2011;152:361�9.�[PubMed]
12.�Pradhan EK, Baumgarten M, Langenberg P, Handwerger B, Gilpin AK, Magyari T, et al. Effect of Mindfulness-Based Stress Reduction in rheumatoid arthritis patients.�Arthritis Rheum.�2007;57:1134�42.[PubMed]
13.�Cramer H, Haller H, Lauche R, Dobos G. Mindfulness-based stress reduction for low back pain. A systematic review.�BMC Complement Altern Med.�2012;12:162.�[PMC free article]�[PubMed]
14.�Bazarko D, Cate RA, Azocar F, Kreitzer MJ. The impact of an innovative mindfulness-based stress reduction program on the health and well-being of nurses employed in a corporate setting.�J Workplace Behav Health.�2013;28:107�33.�[PMC free article]�[PubMed]
15.�Carlson LE, Garland SN. Impact of mindfulness-based stress reduction (MBSR) on sleep, mood, stress and fatigue symptoms in cancer outpatients.�Int J Behav Med.�2005;12:278�85.�[PubMed]
16.�Lengacher CA, Kip KE, Barta M, Post-White J, Jacobsen PB, Groer M, et al. A pilot study evaluating the effect of mindfulness-based stress reduction on psychological status, physical status, salivary cortisol, and interleukin-6 among advanced-stage cancer patients and their caregivers.�J Holist Nurs.�2012;30:170�85.�[PubMed]
17.�Simpson J, Mapel T. An investigation into the health benefits of mindfulness-based stress reduction (MBSR) for people living with a range of chronic physical illnesses in New Zealand.�N Z Med J.�2011;124:68�75.�[PubMed]
18.�Omidi A, Mohammadi A, Zargar F, Akbari H. Efficacy of mindfulness-based stress reduction on mood States of veterans with post-traumatic stress disorder.�Arch Trauma Res.�2013;1:151�4.�[PMC free article][PubMed]
19.�Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress.�J Health Soc Behav.�1983;24:385�96.�[PubMed]
20.�Roth B, Robbins D. Mindfulness-based stress reduction and health-related quality of life: Findings from a bilingual inner-city patient population.�Psychosom Med.�2004;66:113�23.�[PubMed]
21.�Brown KW, Ryan RM. The benefits of being present: Mindfulness and its role in psychological well-being.�J Pers Soc Psychol.�2003;84:822�48.�[PubMed]
22.�Astin JA, Shapiro SL, Lee RA, Shapiro DH., Jr The construct of control in mind-body medicine: Implications for healthcare.�Altern Ther Health Med.�1999;5:42�7.�[PubMed]
23.�Cohen S, Williamson G. Perceived stress in a probability sample of the United States. In: Spacapan S, Oskamp S, editors.�The Social Psychology of Health.�Newbury Park, CA: Sage; 1988. p. 185.
24.�Geary C, Rosenthal SL. Sustained impact of MBSR on stress, well-being, and daily spiritual experiences for 1 year in academic health care employees.�J Altern Complement Med.�2011;17:939�44.[PubMed]
25.�Dick BD, Rashiq S, Verrier MJ, Ohinmaa A, Zhang J. Symptom burden, medication detriment, and support for the use of the 15D health-related quality of life instrument in a chronic pain clinic population.�Pain Res Treat 2011.�2011:809071.�[PMC free article]�[PubMed]
26.�McCabe C, Lewis J, Shenker N, Hall J, Cohen H, Blake D. Don�t look now! Pain and attention.�Clin Med.�2005;5:482�6.�[PMC free article]�[PubMed]
27.�Bener A, Verjee M, Dafeeah EE, Falah O, Al-Juhaishi T, Schlogl J, et al. Psychological factors: Anxiety, depression, and somatization symptoms in low back pain patients.�J Pain Res.�2013;6:95�101.[PMC free article]�[PubMed]
28.�Lee JE, Watson D, Frey-Law LA. Psychological factors predict local and referred experimental muscle pain: A cluster analysis in healthy adults.�Eur J Pain.�2013;17:903�15.�[PMC free article]�[PubMed]
29.�Davidson RJ, Kabat-Zinn J, Schumacher J, Rosenkranz M, Muller D, Santorelli SF, et al. Alterations in brain and immune function produced by mindfulness meditation.�Psychosom Med.�2003;65:564�70.[PubMed]
30.�Lazar SW, Kerr CE, Wasserman RH, Gray JR, Greve DN, Treadway MT, et al. Meditation experience is associated with increased cortical thickness.�Neuroreport.�2005;16:1893�7.�[PMC free article]�[PubMed]
31.�McCracken LM, Jones R. Treatment for chronic pain for adults in the seventh and eighth decades of life: A preliminary study of Acceptance and Commitment Therapy (ACT)�Pain Med.�2012;13:860�7.[PubMed]
32.�McCracken LM, Guti�rrez-Mart�nez O. Processes of change in psychological flexibility in an interdisciplinary group-based treatment for chronic pain based on Acceptance and Commitment Therapy.�Behav Res Ther.�2011;49:267�74.�[PubMed]
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine



 Please Recommend Us: If you have enjoyed this video and/or we have helped you in any way please feel free to recommend us. Thank You.
Please Recommend Us: If you have enjoyed this video and/or we have helped you in any way please feel free to recommend us. Thank You.