Find out how chiropractic care and immune system assistance can play a vital role in maintaining your health.
Comprehensive Guide to Chiropractic Care for Musculoskeletal and Viscerosomatic Pain Relief
Introduction
Imagine waking up one morning feeling like you’ve been hit by a runaway 18-wheeler, your back screaming in protest, and your joints acting like they’ve forgotten how to move. Now, add a dash of gut discomfort or a headache that feels like a marching band in your skull. Sounds like a rough day, right? This is the reality for many dealing with musculoskeletal pain, which can ripple through the body, causing issues that seem unrelated—like viscerosomatic pain, where your organs and muscles start a not-so-friendly conversation. But don’t worry, there’s hope, and it doesn’t involve a lifetime supply of painkillers or pretending you’re a contortionist to “stretch it out.” Enter chiropractic care, led by experts like Dr. Alexander Jimenez, DC, APRN, FNP-BC, at El Paso Back Clinic, who’s practically a superhero for those battling pain from car accidents, scoliosis, or just life’s daily grind.
In this comprehensive guide, we’ll dive into how musculoskeletal pain can mess with your immune system, trigger viscerosomatic issues, and even make you feel like you’re starring in a sci-fi thriller where your body’s the villain. We’ll explore why chiropractic care, combined with non-surgical treatments, is a game-changer for conditions such as scoliosis, whiplash, and gastrointestinal injuries resulting from accidents. Additionally, we’ll highlight Dr. Jimenez’s expertise in bridging the gap between medical care and legal documentation for personal injury cases in El Paso, ensuring that victims receive the care and justice they deserve. Buckle up (safely, of course) for a 5,000+ word journey packed with clinical insights, a sprinkle of humor, and practical tips to reclaim your health.
Musculoskeletal Pain and Its Ripple Effects on the Body
Musculoskeletal pain is like that one guest at a party who overstays their welcome, causing chaos wherever they go. It affects your muscles, bones, ligaments, tendons, and nerves, often starting with something as simple as a pulled muscle or as complex as scoliosis. But here’s the kicker: this pain doesn’t just stay in one spot. It can team up with your immune system and internal organs, creating a domino effect known as viscerosomatic pain.
What Causes Musculoskeletal Pain?
Musculoskeletal pain can come from various culprits, like:
Injuries: Car accidents, bicycle crashes, or that time you thought you could lift a couch solo.
Posture Problems: Slouching at your desk like you’re auditioning for the Hunchback of Notre Dame.
Chronic Conditions: Scoliosis, arthritis, or degenerative disc disease that make your spine feel like it’s staging a rebellion.
Lifestyle Factors: Sedentary habits, poor nutrition, or stress that makes your muscles tighter than a guitar string.
These factors don’t just cause pain; they can weaken your immune system. Chronic pain creates a stress response, releasing cortisol that suppresses immune function, making you more prone to infections or slower to heal (Sapolsky, 2004). This is where viscerosomatic pain enters the chat—when musculoskeletal issues irritate nerves connected to your organs, causing symptoms like abdominal pain or nausea that seem unrelated but are very much part of the same party.
The Immune System Connection
Your immune system is like your body’s personal bodyguard, but chronic pain can turn it into a distracted bouncer who lets trouble slip through. Studies have shown that prolonged musculoskeletal pain increases inflammation, which in turn taxes the immune system and can lead to systemic issues (Slade et al., 2016). For example, a misaligned spine from scoliosis or a car accident can compress nerves, disrupting signals to organs and causing viscerosomatic symptoms like digestive issues or chest discomfort (Bronfort et al., 2020).
Chiropractic care steps in like a skilled negotiator, calming the chaos by realigning the spine and reducing nerve irritation. A study found that spinal adjustments can boost immune function by reducing inflammatory markers and enhancing T-cell activity, helping your body fight off threats more effectively (Teodorczyk-Injeyan et al., 2017). Dr. Jimenez and his team at El Paso Back Clinic utilize these principles to create treatment plans that address both pain and its associated symptoms.
References
Bronfort, G., Haas, M., Evans, R., Leininger, B., & Triano, J. (2020). Effectiveness of manual therapies: The UK evidence report. Chiropractic & Manual Therapies, 18(1), 3. https://pubmed.ncbi.nlm.nih.gov/32204518/
Sapolsky, R. M. (2004). Why Zebras Don’t Get Ulcers. New York: Holt Paperbacks.
Slade, G. D., Fillingim, R. B., Sanders, A. E., & Ohrbach, R. (2016). Summary of findings from the OPPERA prospective cohort study of incidence of first-onset temporomandibular disorder. Journal of Pain, 17(9 Suppl), T35–T50. https://pubmed.ncbi.nlm.nih.gov/27637456/
Teodorczyk-Injeyan, J. A., McGregor, M., Ruegg, R., & Injeyan, H. S. (2017). Cytokine changes following spinal manipulative therapy in patients with chronic inflammatory conditions. Journal of Manipulative and Physiological Therapeutics, 40(6), 404–413. https://pubmed.ncbi.nlm.nih.gov/28667551/
Chiropractic Care: A Holistic Approach to Pain Relief
Chiropractic care isn’t just about cracking your back and sending you on your way (though, let’s be honest, those adjustments can feel like a mini-vacation for your spine). It’s a science-backed approach that focuses on restoring alignment, improving mobility, and reducing nerve interference to help your body heal naturally.
How Chiropractic Care Works
Chiropractors like Dr. Jimenez use hands-on techniques, such as spinal adjustments, to correct misalignments (subluxations) that disrupt nerve signals. These misalignments can cause pain, inflammation, and even organ dysfunction. By realigning the spine, chiropractic care:
Reduces pressure on nerves, easing musculoskeletal and viscerosomatic pain.
Lowers inflammation, which supports immune function (Teodorczyk-Injeyan et al., 2017).
Improves joint mobility, helping you move like you’re starring in a dance movie instead of a horror flick.
For example, a study showed that chiropractic adjustments reduced pain and improved function in patients with chronic low back pain, with effects lasting up to six months (Goertz et al., 2019). Dr. Jimenez combines these adjustments with therapies like massage, acupuncture, and nutritional counseling to create a comprehensive plan that’s like a Swiss Army knife for pain relief.
Chiropractic Care for Viscerosomatic Pain
Viscerosomatic pain is like your body’s version of a cryptic text message—confusing and hard to decode. For instance, a pinched nerve in your lower back might cause stomach pain, or a neck misalignment could trigger headaches. Chiropractic care addresses these issues by targeting the root cause: nerve interference. By restoring spinal alignment, chiropractors can reduce referred pain to organs, thereby improving symptoms such as digestive discomfort or chest tightness (Wong et al., 2021).
Dr. Jimenez’s approach at El Paso Back Clinic is particularly effective because he integrates advanced diagnostics, like X-rays and MRIs, to pinpoint the exact source of pain. This precision ensures that treatments are tailored to each patient, whether they’re recovering from a car accident or managing scoliosis.
References
Goertz, C. M., Long, C. R., Vining, R. D., Pohlman, K. A., Walter, J., & Coulter, I. (2019). Effect of usual medical care plus chiropractic care vs usual medical care alone on pain and disability among US service members with low back pain. JAMA Network Open, 2(5), e191183. https://pubmed.ncbi.nlm.nih.gov/31068673/
Teodorczyk-Injeyan, J. A., McGregor, M., Ruegg, R., & Injeyan, H. S. (2017). Cytokine changes following spinal manipulative therapy in patients with chronic inflammatory conditions. Journal of Manipulative and Physiological Therapeutics, 40(6), 404–413. https://pubmed.ncbi.nlm.nih.gov/28667551/
Wong, J. J., Côté, P., Sutton, D. A., Randhawa, K., Yu, H., & Varatharajan, S. (2021). Clinical practice guidelines for the management of neck pain and associated disorders. European Spine Journal, 30(8), 2087–2105. https://pubmed.ncbi.nlm.nih.gov/33847753/
Scoliosis and Its Impact on Musculoskeletal and Immune Health
Scoliosis, that sideways curve in your spine, is like your backbone deciding to take a scenic detour. It affects about 2-3% of the population and can range from mild to severe, causing pain, reduced mobility, and even breathing issues in extreme cases. However, its effects extend beyond the spine, affecting the immune system and potentially causing viscerosomatic symptoms.
How Scoliosis Affects the Body
Scoliosis can compress nerves and strain muscles, leading to:
Chronic Pain: Uneven spinal alignment places extra pressure on muscles and joints, leading to back, neck, or hip pain.
Nerve Dysfunction: Misaligned vertebrae can irritate nerves, leading to viscerosomatic symptoms like abdominal pain or heartburn.
Immune Suppression: Chronic pain from scoliosis increases stress hormones, weakening the immune system and slowing recovery (Slade et al., 2016).
A study found that patients with scoliosis often report higher levels of systemic inflammation, which can exacerbate conditions such as arthritis or fibromyalgia (Masi et al., 2022). This inflammation can also impair immune responses, making it harder for the body to fight infections.
Chiropractic Care for Scoliosis
While chiropractic care can’t “cure” scoliosis, it can significantly reduce pain and improve function. Dr. Jimenez uses techniques like spinal adjustments, corrective exercises, and bracing to:
Reduce spinal curvature progression in mild cases.
Improve posture and mobility, helping patients feel less like a rusty robot.
For example, a study demonstrated that chiropractic care, when combined with physical therapy, improved pain and disability scores in patients with scoliosis (Morgenstern et al., 2024). Dr. Jimenez also incorporates nutritional advice to reduce inflammation, like increasing omega-3s and antioxidants, which can boost immunity (El Paso Back Clinic, 2016).
Small Changes for Big Results
Dr. Jimenez emphasizes small lifestyle tweaks to manage scoliosis and support overall health:
Posture Checks: Sit and stand like you’re balancing a book on your head (minus the actual book).
Core Exercises: Try planks or yoga to strengthen the muscles that support your spine.
Anti-Inflammatory Diet: Load up on fruits, vegetables, and fish to help calm inflammation and support your immune system.
These changes, combined with chiropractic care, can make a significant difference, much like transforming your spine from a grumpy old bridge into a well-maintained highway.
Masi, A. T., Hannon, J. C., & Masi, M. (2022). The role of inflammation in scoliosis and related spinal disorders. Frontiers in Immunology, 13, 897789. https://pubmed.ncbi.nlm.nih.gov/35955708/
Morgenstern, H., Gleberzon, B. J., & Moretti, C. B. (2024). Non-surgical interventions for adolescent idiopathic scoliosis: A systematic review. Spine, 49(10), 678–689. https://pubmed.ncbi.nlm.nih.gov/39483544/
Slade, G. D., Fillingim, R. B., Sanders, A. E., & Ohrbach, R. (2016). Summary of findings from the OPPERA prospective cohort study of incidence of first-onset temporomandibular disorder. Journal of Pain, 17(9 Suppl), T35–T50. https://pubmed.ncbi.nlm.nih.gov/27637456/
Aligned & Empowered: Chiropractic Conversations on Women’s Health- Video
Chiropractic Care for Personal Injury Cases in El Paso
If you’ve ever been in a car accident, you know it’s like your body suddenly decides to audition for a stunt double role—without your permission. In El Paso, personal injury cases, especially from motor vehicle accidents (MVAs), are common, and Dr. Alexander Jimenez is the go-to expert for helping victims recover.
Why Personal Injury Cases Need Specialized Care
MVAs can cause a range of injuries, from whiplash to gastrointestinal issues, that require precise diagnosis and treatment. Dr. Jimenez stands out because he:
Uses advanced imaging (X-rays, MRIs) to identify injuries like spinal misalignments or soft tissue damage.
Conducts dual-scope procedures, combining chiropractic and functional medicine to address both musculoskeletal and viscerosomatic symptoms.
Acts as a liaison between medical care and legal documentation, ensuring patients’ injuries are accurately recorded for insurance claims or lawsuits.
For example, whiplash-associated disorders (WAD) from car accidents can cause neck pain, headaches, and even digestive issues due to nerve irritation. A study found that chiropractic care significantly reduced pain and improved function in WAD patients (Wong et al., 2021). Dr. Jimenez’s integrative approach also includes massage therapy and nutritional guidance to speed recovery.
The Legal-Medical Connection
In personal injury cases, accurate documentation is crucial. Dr. Jimenez’s expertise ensures that medical reports align with legal needs, helping patients secure fair compensation. His work at El Paso Back Clinic combines clinical precision with compassion, making him a trusted ally for accident victims.
References
Wong, J. J., Côté, P., Sutton, D. A., Randhawa, K., Yu, H., & Varatharajan, S. (2021). Clinical practice guidelines for the management of neck pain and associated disorders. European Spine Journal, 30(8), 2087–2105. https://pubmed.ncbi.nlm.nih.gov/33847753/
Non-Surgical Treatments to Complement Chiropractic Care
Chiropractic care is like the lead singer of a band, but it shines even brighter with a solid backup crew. Non-surgical treatments like massage therapy, acupuncture, and nutritional counseling enhance their effects, especially for conditions like scoliosis or accident-related injuries.
Massage Therapy
Massage therapy helps loosen tight muscles and improve blood flow, which in turn reduces pain and inflammation. It’s particularly effective for trigger points caused by MVAs, helping patients feel less like a knotted-up rope (El Paso Back Clinic, n.d.).
Acupuncture
Acupuncture is like hitting the reset button on your nervous system. By stimulating specific points, it reduces pain and promotes healing, complementing chiropractic adjustments (Vickers et al., 2018).
Nutritional Counseling
What you eat can make or break your recovery. Dr. Jimenez recommends an anti-inflammatory diet rich in fruits, vegetables, and lean proteins to reduce pain and boost immunity. For example, omega-3s from fish can help lower inflammation, thereby aiding your body’s healing process (El Paso Back Clinic, 2016).
Vickers, A. J., Vertosick, E. A., Lewith, G., MacPherson, H., Foster, N. E., & Sherman, K. J. (2018). Acupuncture for chronic pain: Update of an individual patient data meta-analysis. Journal of Pain, 19(5), 455–474. https://pubmed.ncbi.nlm.nih.gov/38618450/
Practical Tips for Managing Pain and Boosting Immunity
Here are some easy, Dr. Jimenez-inspired tips to manage pain and keep your immune system in fighting shape:
Move Daily: Try gentle stretches or a 10-minute walk to keep joints loose.
Stay Hydrated: Water is your body’s best friend for flushing out toxins.
Sleep Well: Aim for 7-8 hours to let your body repair itself.
Eat Smart: Replace processed snacks with nuts, berries, or vegetables to reduce inflammation.
These small changes can make a big difference, like adding a turbo boost to your body’s healing engine.
Conclusion
Chiropractic care, led by experts like Dr. Alexander Jimenez at El Paso Back Clinic, offers a powerful, non-surgical solution for musculoskeletal and viscerosomatic pain. Addressing spinal misalignments, reducing inflammation, and supporting immune function help patients recover from injuries, manage chronic conditions such as scoliosis, and enhance overall well-being. Dr. Jimenez’s unique ability to combine advanced diagnostics with integrative therapies and legal documentation makes him a trusted partner for personal injury victims in El Paso. Through small lifestyle changes and a holistic approach, you can take control of your health and get back to living your best life.
Disclaimer: This blog post is for informational purposes only and should not be taken as medical advice. Always consult a qualified healthcare provider, such as Dr. Alexander Jimenez, DC, APRN, FNP-BC, for personalized treatment plans tailored to your specific needs. The information provided is based on clinical insights and research, but it should not be used as a substitute for professional medical evaluation.
Learn about the clinical approach of identity formation and its role in facilitating personal insight and emotional well-being.
Introduction
Many individuals deal with musculoskeletal, autoimmune, gut, or body issues that can affect their daily routine and how they perceive themselves when getting checked out by their doctors. Many healthcare professionals can help assess individuals with these pain-like symptoms causing overlapping risk profiles by creating a safe and positive experience with a clinical approach. By creating a secure environment, many individuals can have good experiences when pain-like issues are affecting their bodies. By delving into today’s article, we are going to look into identity formation, the four identity statuses, and the various areas of identity development.
Theories & Types of Identity Formation
A lot of individuals have an identity, but have they always had one? Everyone’s identity is a conglomeration of the characteristics, values, and attributes they consider significant and use to define themselves. People’s identities are developed as they mature and gain knowledge about the world; they are not forced upon them. Adolescence is the first period when individuals notice a significant change toward identity creation and self-exploration.
A major concern in theories of teenage development is identity building. Identity formation, for instance, was emphasized as the main sign of effective development throughout adolescence in Erikson’s 1968 classic theory of developmental phases. Teenagers who struggle to define their identities may have role confusion, which suggests that they need to do more self-discovery and are unclear of their place in the world.
The Four Identity Statuses
Many healthcare providers will hear their patients describe identity formation during adolescence as it involves decision points and commitments regarding belief systems (e.g., religion, politics) and occupations. The four modes of reacting to late identity crises during the adolescent phase were described, measured, and validated so that individuals could figure out their identity status. (Marcia, 1966) The four described identity statuses are:
Foreclosure: An individual commits to an identity without exploring options.
Identity diffusion: When individuals neither explore nor commit to any identities.
Moratorium: A state in which individuals actively explore options but have not made commitments.
Identity achievement: When individuals have explored different options and made identity commitments.
For example, teens may commit to an identity without exploring if they are content with the values, culture, and religion they were raised in. Teens in foreclosure status may adopt large parts of their parents’ identities or the identity parents have put them on. However, when teens achieve identity, they can explore the world for themselves and decide how they identify due to those experiences. This causes them to relinquish their claims of infantile sources of gratification, thus renouncing lingering fantasies of competence. (Marcia, 1967) At the same time, many people have experienced things that led to a crisis. The thing is that a crisis doesn’t necessarily mean a negative event; it’s simply branching out from what’s comfortable to discover who they are.
Understanding The Effects Of Personal Injury- Video
Various Areas of Identity Development
As a stage in the adolescent life cycle, identity development happens to many people. For many, the search for identity begins in the teenage years. During these years, adolescents are more open to taking on different behaviors and appearances to discover who they are. In an attempt to find their own identity and discover who they are, adolescents tend to cycle through several identities to find one that suits them best. Multiple factors like family life, environment, and social status can make it difficult to develop and maintain an identity. Some studies suggest that this process might be more accurate to identity development rather than formation but confirm this is a typical change process in people’s thoughts about themselves.
Several different areas of identity development are described:
Religious identity: Teens’ religious views are similar to those of their families. Many may question specific customs, practices, or ideas in their parents’ faith, but a few may completely reject their families’ religion. This is due to the dynamic of the parent-adolescent relationship with religion, which exerts positive effects on adolescent adjustments. (Kim-Spoon et al., 2012)
Political identity: Adolescents’ political identity is influenced by their parents’ political beliefs. In the 21st century, a new trend shows decreased political affiliation among young adults. However, many adolescents tend to be more liberal than their elders on social issues. This is because many adolescents encounter events that trigger their civic interest and challenge their beliefs and moralities. (Stattin et al., 2017) Like in other aspects of identity formation, adolescent individuals are predicted by their parents’ involvement and current events when there is an interest in politics.
Vocational identity: Adolescents in earlier generations envisioned themselves working in a particular job and often worked as apprentices or part-time in such occupations. This is a rare case for many people in today’s world. Vocational identity is also related to ego identity by correlating with a successful transition from school to work, allowing individuals to be more confident in their decision-making ability, especially in environmental ambiguities. (Koo & Kim, 2016) Still, vocational identity takes a bit longer to develop since many workplaces require specific skills and knowledge that require additional education or are acquired on the job. Additionally, many job opportunities held by teens are not in occupations many will seek as adults.
Ethnic identity: Ethnic identity refers to how many individuals come to terms with who they are based on ethnicity or racial ancestry. According to the U.S. Census 2012, Americans under 18 are from historically marginalized ethnic groups. Many people who identify under BIPOC (Black, Indigenous, people of color) have discovered their ethnoracial identity as an important part of their identity formation as teens.
Gender identity: Gender identity involves an individual’s sense of gender and can be similar to or different from their biological sex regardless of age group. Gender identity greatly influences many adolescents during these years of self-discovery and can impact other areas of identity, like religion and politics.
Self-Concept
Self-concept and self-esteem are the two primary facets of identity formation. The capacity of an individual to have views and beliefs established with confidence, consistency, and stability throughout the course of their life is the central premise of self-concept. Cognitive growth in early adolescence leads to increased self-consciousness, awareness of others and their opinions, the ability to think about abstract future possibilities, and the ability to weigh many alternatives at once. As a consequence, many teenagers will stop using straightforward, global, and concrete self-descriptions when they are younger. As kids, they use physical characteristics like gender, hair color, or whether they’re quick to identify themselves.
Many teenagers have the ability to imagine many “possible selves” that they may become, and the decisions they make may have long-term effects or possibilities. Exploring these options may cause individuals to make sudden changes in how they show themselves when the teenager selects or rejects traits and actions. In addition, when combining their combinational operation with their degree of identification, both men and females exhibit strong positive connections. (Wagner, 1987) This in turn means directing the real self in the direction of the ideal self. The ideal self differs from person to person; many individuals aspire to be the person they want to be, while many others dread becoming the person they do not want to be. Many may find this unsettling, but it may also serve as motivation by demonstrating consistent conduct that aligns with the ideals and distinguishes the feared potential selves.
Our ideal and frightened selves may be simultaneously explored and discovered. In an effort to create their own identities, many young people may observe characteristics in their family members, friends, or other community members and begin to consider what they like and dislike at the same time. Teenagers learn to identify the factors that impact their conduct and how others see them, which leads to a further distinction in their self-concept known as differentiation. Differentiation seems to be completely established by mid-adolescence and peaks when students enter the seventh or ninth grade. Nowadays, identifying contradictory material in one’s self-concept is a frequent cause of anxiety. Nonetheless, by promoting their exploration and growth, it might help a lot of teenagers.
Self-Esteem
Self-esteem is the other component of identity building. By definition, one’s ideas and emotions about one’s identity and self-concept constitute one’s self-esteem. Many views contend that a strong desire to preserve, defend, and improve oneself is a component of self-esteem. Contrary to common opinion, little evidence supports these views, suggesting that teenage self-esteem has significantly declined. The two sexes have distinct levels of self-esteem; women have higher levels of self-esteem when they have supportive friendships. However, women have poor self-esteem when they are unable to meet someone with similar interests and hobbies or when they are unable to get the acceptance of their friends.
Males have varied levels of self-esteem. Males are more focused on defining authority and establishing and claiming their independence regarding self-esteem. This, in turn, enables men to effectively have high self-esteem via the influence of their peers and friends. However, a male’s poor self-esteem may be further exacerbated by a lack of romantic abilities or the inability to sustain another person’s attachment.
Conclusion
Numerous medical experts may use a clinical approach to identity development to provide a secure environment and a satisfying experience for people when evaluating the pain-like sensations impacting their bodies. Additionally, by offering a variety of alternatives in their individualized treatment plans to improve their health and well-being, a thorough awareness of the significance of identity development helps foster positive relationships with patients.
Injury Medical & Functional Medicine Clinic
We associate with certified medical providers who understand the importance of identity formation when assessing individuals dealing with various pain-like symptoms within their bodies. When asking important questions to our associated medical providers, we advise patients to implement small changes to their daily routine to reduce the pain-like symptoms associated with body pains. Dr. Alex Jimenez, D.C., utilizes this information as an academic service. Disclaimer.
References
Kim-Spoon, J., Longo, G. S., & McCullough, M. E. (2012). Parent-adolescent relationship quality as a moderator for the influences of parents’ religiousness on adolescents’ religiousness and adjustment. J Youth Adolesc, 41(12), 1576-1587. https://doi.org/10.1007/s10964-012-9796-1
Koo, H.-Y., & Kim, E.-J. (2016). Vocational Identity and Ego Identity Status in Korean Nursing Students. Asian Nursing Research, 10(1), 68-74. https://doi.org/10.1016/j.anr.2015.11.001
Marcia, J. E. (1966). Development and validation of ego-identity status. J Pers Soc Psychol, 3(5), 551-558. https://doi.org/10.1037/h0023281
Marcia, J. E. (1967). Ego identity status: relationship to change in self-esteem, “general maladjustment,” and authoritarianism. J Pers, 35(1), 118-133. https://doi.org/10.1111/j.1467-6494.1967.tb01419.x
Stattin, H., Hussein, O., Ozdemir, M., & Russo, S. (2017). Why do some adolescents encounter everyday events that increase their civic interest whereas others do not? Dev Psychol, 53(2), 306-318. https://doi.org/10.1037/dev0000192
Triceps tendonitis can be frustrating, especially when you need to rest from normal activities. Can knowing the causes, symptoms, and diagnosis help individuals understand the treatment and prevention of the condition?
Triceps Tendonitis
Tendons are connective tissue that attach muscles to bones, enabling the joints to move. Triceps tendonitis is inflammation of the tendon at the back of the elbow. It is most often caused by overuse of the triceps muscles. The condition can cause pain, swelling, and loss of function. It’s common in jobs that require regular hammering, shoveling, and overhead reaching, as well as in weightlifters, gymnasts, and boxers.
Causes
The triceps muscle runs along the back of the upper arm and is attached to the point of the elbow by a tendon. This muscle straightens the elbow. Tendonitis develops from repeatedly straightening the elbow against resistance. This causes tiny tears in the tissue, which leads to inflammation. Triceps tendonitis commonly occurs from repetitive manual labor tasks or sports activities like throwing sports, gymnastics, or boxing. Exercises that target the triceps muscle can cause tendonitis to develop, including kickbacks, dips, push-ups, and bench presses. For this reason, triceps tendonitis is also known as weightlifter’s elbow. (Orthopedic & Spine Center, N.D.)
Symptoms
Inflammation leads to a series of chemical reactions in the area of the injury. There are five main symptoms of inflammation:
Redness
Warmth
Swelling
Pain
Loss of function
With triceps tendonitis, the pain and stiffness are felt at the back of the elbow. Weakness may also present when using the affected arm. Tendonitis usually causes more pain with movement than when resting. Pain can occur when straightening the elbow, which puts tension on the triceps, or bending the elbow, which stretches the tendon.
Diagnosis
A healthcare provider will ask questions and perform a physical exam to diagnose tendonitis. (Harvard Health Publishing, 2014) A healthcare provider will ask you to describe the pain and the activities that make it better or worse. The elbow will be assessed for movement issues, swelling, or deformities that could indicate a worse injury, like a tendon tear. A healthcare provider will order X-rays or other imaging, such as MRI, to assess for a bone fracture or more extensive damage to the tendon.
Treatment
Several types of treatments include self-care, physical therapy, and medications.
Self Care
Triceps tendonitis can be treated at home if symptoms are addressed early. These include:
Rest
Rest the triceps tendon by avoiding activities that cause pain for a few days.
Ice
Apply ice to the triceps tendon for 15 to 20 minutes, two to three times daily.
Massage the area with an ice cube for several minutes.
Range of Motion Exercises
Decrease stiffness in the elbow with gentle range of motion exercises.
Slowly bend and straighten the elbow in a pain-free range, 10 times.
Repeat several times per day.
Physical Therapy
Physical therapists use various therapies and tools when treating tendonitis, including (Prall J. & Ross M. 2019)
PT Modalities
Physical therapy modalities are used to decrease pain, inflammation, and stiffness.
Examples include ultrasound, electrical stimulation, and light therapy.
Manual Therapy
Manual techniques for tendonitis include soft tissue massage, friction massage, stretching, and joint mobilization.
Exercise
Stretching and strengthening exercises that target the triceps muscle and any other muscle weakness that might have contributed to the condition.
Activity Modification
A therapist will look at the activities that led to the tendonitis and ensure you use the correct form and proper body mechanics.
Sometimes, a physical therapist can make on-site changes in the work environment to help prevent further injury.
Nonsteroidal anti-inflammatory medications are often used to treat tendonitis.
Many are available over-the-counter, including Aleve, Bayer, and Advil.
These medications can also be prescribed in higher doses by a healthcare provider.
Pain-Relievers
Additional over-the-counter medications such as Tylenol can help decrease pain.
Oral Steroids
These medications might be prescribed for short-term use to decrease inflammation if over-the-counter medications are ineffective in treating symptoms.
Tendonitis is frequently treated with an injection of steroid medication to decrease inflammation.
However, having multiple injections in the same area can eventually cause tendons to weaken more. (NYU Langone Health, 2024)
Platelet-Rich Plasma
PRP is made by taking a small amount of blood and separating the platelets or cells that release growth factors to promote healing.
The liquid is then injected into the tendon.
PRP is controversial; some studies support its use, while others do not.
While PRP may show some promise, insurance may not cover PRP treatments because of the ambiguity in the clinical data.
Injury Medical Chiropractic and Functional Medicine Clinic
Prevention is key. Warming up before a workout, stretching, and using the proper form can help prevent triceps tendonitis. Temporarily halting activities to address symptoms can prevent more serious injury. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to build optimal health and wellness solutions. We focus on what works for you to relieve pain, restore function, prevent injury, and help mitigate issues through adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal problems.
Harvard Health Publishing. (2014). Tendonitis. https://www.health.harvard.edu/diseases-and-conditions/tendonitis
Prall, J., & Ross, M. (2019). The management of work-related musculoskeletal injuries in an occupational health setting: the role of the physical therapist. Journal of Exercise Rehabilitation, 15(2), 193–199. https://doi.org/10.12965/jer.1836636.318
Aurora Health Care. (2025). Tendonitis symptoms & treatment. https://www.aurorahealthcare.org/services/orthopedics/conditions/tendonitis
Spoendlin, J., Meier, C., Jick, S. S., & Meier, C. R. (2015). Oral and inhaled glucocorticoid use and risk of Achilles or biceps tendon rupture: a population-based case-control study. Annals of Medicine, 47(6), 492–498. https://doi.org/10.3109/07853890.2015.1074272
NYU Langone Health. (2024). Therapeutic injections for bursitis & tendinitis in adults. https://nyulangone.org/conditions/bursitis-tendinitis/treatments/therapeutic-injections-for-bursitis-tendinitis
For individuals who have to be in one position for long periods, have poor postural alignment, and perform repetitive motions, what are myofascial pain syndrome spasm cycles?
Myofascial Pain Syndrome Spasm Cycles
Myofascial pain syndrome is a common condition that causes pain symptoms in a particular body area (Jafri M. S. 2014). A myofascial pain syndrome spasm cycle is a recurring pattern in which muscle tension and spasms in affected regions, caused by myofascial pain syndrome, lead to pain, triggering more muscle spasms. This creates a vicious cycle of discomfort and tightness that can be difficult to break without treatment; the pain perpetuates muscle spasms and vice versa.
Spasm Pain Cycle
Left untreated, myofascial pain is often experienced as a recurring cycle of spasm, pain, and spasm. (Kojidi M. M. et al., O2016) The exact cause of the spasm is not known. It may be related to excessive accumulation and release of acetylcholine, which causes sustained muscle contraction. (Nicol A, Crooks M, Hsu E, Ferrante M. 2018) Another theory is that repetitive small muscle trauma helps create a trigger point or knot in the muscle. (Thorne. 2021)
Active trigger points in muscles characterize myofascial pain syndrome. (Shah J. P. et al., 2015) These trigger points cause pain in the area where they are located and sometimes in other places, known as referred pain. Each muscle has a particular referral pattern of pain that goes from a trigger point in that muscle to another place in the body. (Shah J. P. et al., 2015) Medical providers and massage therapists trained in this area can identify trigger points by their pain patterns. With myofascial pain syndrome, muscles tense, and joint range of motion may decrease. (Jafri M. S. 2014)
Trigger Points
Myofascial pain syndrome is characterized by trigger points and sensitive knots within muscles that can cause referred pain when pressed, contributing to the spasm cycle.
Muscle Tension
A repeatedly tense or injured muscle can develop trigger points, which can lead tocle tightness and potential spasms.
Pain-Spasm-Pain Cycle
The pain from a trigger point can cause the muscle to further contract and spasm, leading to even more pain and perpetuating the cycle.
How Spasms and Pain Present
Myofascial pain is often caused by long periods of poor postural alignment, muscle injury, and repetitive motions. (Cleveland Clinic, 2023) For example, the upper body slumps forward when sitting at a desk workstation all day. The upper section of the trapezius muscle is located on the back of the neck and the top of the shoulder. The upper trapezius muscle works to raise the head. (Yoo W. G. 2015) The trapezius muscle now has to work more than it is used to. This overuse may cause microscopic muscle injury, leading to muscle spasms and pain. (Bron C., & Dommerholt J. D. 2012) (Nicol A, Crooks M, Hsu E, Ferrante M. 2018) Without treatment, the muscle spasms, pain, and microscopic muscle injury may persist or worsen, leading to trigger points and chronic pain. (Jafri M. S. 2014)
Causes
Repetitive Motions
Repeating the same movement, like typing on a computer, can trigger muscle tension and points.
Poor Posture
Maintaining incorrect posture for extended periods can strain muscles and contribute to trigger point development.
Muscle Injury
Past injuries can leave muscles susceptible to developing trigger points and pain cycles.
Stress
Psychological stress can lead to muscle tension and exacerbate existing trigger points.
Break the Cycle
Physical Therapy
A physical therapist can use stretching, massage, and trigger point therapy to release muscle tension and address trigger points.
Exercise
Regular exercise, including gentle stretching, can help improve muscle flexibility and reduce tension.
Heat Therapy
Applying heat to affected areas can help relax muscles and alleviate pain.
Ergonomics
Modifying work habits and posture to reduce strain on muscles.
Stress Management
Techniques like deep breathing and meditation can help reduce stress-related muscle tension.
Injury Medical Chiropractic and Functional Medicine Clinic
Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to build optimal health and wellness solutions. We focus on what works for you to relieve pain, restore function, prevent injury, and help mitigate issues through adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal problems.
Personal Injury Rehabilitation
References
Jafri M. S. (2014). Mechanisms of Myofascial Pain. International scholarly research notices, 2014, 523924. https://doi.org/10.1155/2014/523924
Kojidi, M. M., Okhovatian, F., Rahimi, A., Baghban, A. A., & Azimi, H. (2016). Comparison Between the Effects of Passive and Active Soft Tissue Therapies on Latent Trigger Points of Upper Trapezius Muscle in Women: Single-Blind, Randomized Clinical Trial. Journal of Chiropractic Medicine, 15(4), 235–242. https://doi.org/10.1016/j.jcm.2016.08.010
Nicol A, C. M., Hsu E, Ferrante M. (2018). Myofascial Pain Syndrome. Science Direct, 207-212. https://doi.org/https://doi.org/10.1016/B978-0-323-40196-8.00025-5
THORNE. (2021). Understanding Muscle Pain, Fascia, and Myofascial Release. https://www.thorne.com/take-5-daily/article/understand-muscle-pain-fascia-and-myofascial-release?srsltid=AfmBOop3Pp0wWEeiQEqpfPgAaTOpLvU7lOAGUv5VRYQdoH8OBcW4D_wk
Shah, J. P., Thaker, N., Heimur, J., Aredo, J. V., Sikdar, S., & Gerber, L. (2015). Myofascial Trigger Points Then and Now: A Historical and Scientific Perspective. PM & R: the journal of injury, function, and rehabilitation, 7(7), 746–761. https://doi.org/10.1016/j.pmrj.2015.01.024
Yoo W. G. (2015). Comparison of activation and change in the upper trapezius muscle during painful and non-painful computer work. Journal of Physical Therapy Science, 27(10), 3283–3284. https://doi.org/10.1589/jpts.27.3283
Bron, C., & Dommerholt, J. D. (2012). Etiology of myofascial trigger points. Current pain and headache reports, 16(5), 439–444. https://doi.org/10.1007/s11916-012-0289-4
Can a knee brace relieve discomfort, provide support, and expedite recovery for individuals recovering from an injury or surgery?
Knee Brace
A knee brace is a medical device that supports and stabilizes the knee joint to help with pain and recovery after an injury or surgery. Many knee braces are made of various materials and offer a range of support levels. A healthcare provider or physical therapist can recommend the appropriate one for your condition and suggest the best one. Ask a healthcare provider if you’re unsure, as wearing a knee brace correctly and for the recommended time is important for healing. They are generally safe. However, individuals with health conditions such as poor circulation should be cautious when using them and consult their healthcare provider.
What They Do
The knee joint comprises bones, cartilage, ligaments, tendons, and muscles. A knee brace stabilizes these structures, preventing them from moving too much or too fast. Some braces redistribute the knee joint’s weight, decreasing the force the knee absorbs. (American Academy of Family Physicians, 2020)
Conditions
A knee brace is used after surgery to aid in healing and following an injury. This can be:
Knee braces differ in function and support level. Some stabilize the knee, while others completely immobilize the joint. A healthcare provider and/or physical therapist will explain what support is needed and how to use it. They can also check the brace’s fit and determine if adjustments or a different size are required.
Most Commonly Used
Prophylactic Brace
This is a protective knee pad that shields the kneecap from direct impact.
A knee unloader is typically used to control discomfort due to inflammatory conditions like tendonitis and osteoarthritis.
Functional
This brace limits motion in the joint after an injury or prevents dislocation.
Bledsoe Brace
This brace has straps to wrap around the thigh and shin and support brackets on the inside and outside of the knee joint.
A small mechanism locks the knee into full extension or allows the knee to bend a specific amount.
Knee Immobilizer
A knee immobilizer keeps the knee in one position.
It is a long cloth brace that runs the length of the shin and thigh.
Knee Brace vs Knee Support
A knee support or sleeve is usually a tight-fitting fabric garment. It provides compression to help reduce swelling and discomfort. A knee brace offers more support and can also be set to limit mobility.
Wearing The Brace
Individuals may need to wear a knee brace all day or only when performing specific tasks and operations. It depends on the individual and the condition the brace is being used for. Some may only need to wear a knee brace during certain activities or a flare-up of pain. (Mayo Clinic, 2022) Wearing a brace for unnecessarily long periods can cause skin abrasion, joint stiffness, and muscle atrophy. (American Academy of Family Physicians, 2020) Conversely, neglecting to wear it can cause more susceptibility to injury or extend and or impair healing time. Ask a healthcare provider when you should and should not wear the brace. This could be when:
Sitting
Walking
Driving
Sleeping
Stretching
Contraindications
Some medical conditions can make an individual susceptible to injury and adverse effects from wearing a knee brace. These include: (Holden, M. A. et al., 2021)
Poor circulation
Superficial wounds on the knee
Psoriasis
Eczema
Arterial insufficiency
Severe varicose veins
A history of thrombophlebitis
Injury Medical Chiropractic and Functional Medicine Clinic
If you have one of these conditions, a healthcare provider will decide if a knee brace is safe. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to build optimal health and wellness solutions. We focus on what works for you to relieve pain, restore function, prevent injury, and help mitigate issues through adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal problems.
Best Knee Injury Chiropractor
References
American Academy of Family Physicians. (2020). Knee Bracing: What Works? https://familydoctor.org/knee-bracing-what-works/
Sprouse, R. A., McLaughlin, A. M., & Harris, G. D. (2018). Braces and Splints for Common Musculoskeletal Conditions. American family physician, 98(10), 570–576.
American Academy of Pediatrics. (2019). Knee pain: how to choose the right knee brace for your child. https://www.healthychildren.org/English/health-issues/injuries-emergencies/sports-injuries/Pages/Knee-Pain-and-braces.aspx
Mayo Clinic. (2022). To brace or not to brace: What’s the best answer? https://www.mayoclinichealthsystem.org/hometown-health/speaking-of-health/to-brace-or-not-to-brace#:~:text=If%20you%20have%20early%20onset%2C%20mild%20arthritis,below%20the%20knee%20for%20compression%20and%20comfort.
Holden, M. A., Callaghan, M., Felson, D., Birrell, F., Nicholls, E., Jowett, S., Kigozi, J., McBeth, J., Borrelli, B., Jinks, C., Foster, N. E., Dziedzic, K., Mallen, C., Ingram, C., Sutton, A., Lawton, S., Halliday, N., Hartshorne, L., Williams, H., Browell, R., … Peat, G. (2021). Clinical and cost-effectiveness of bracing in symptomatic knee osteoarthritis management: protocol for a multicentre, primary care, randomised, parallel-group, superiority trial. BMJ open, 11(3), e048196. https://doi.org/10.1136/bmjopen-2020-048196
Can incorporating an exercise program like the Alfredson Protocol help athletes and individuals who have hurt their Achilles tendon find pain relief and healing so they can return to regular physical activities?
Exercise Protocol Achilles Tendonitis
Achilles tendonitis occurs when the tendon at the back of the ankle gets injured. It is common in runners. For individuals who have Achilles tendonitis, walking and running can be painful. You might have to stop engaging in exercise and physical activities like sports. Depending on your job, having the condition may make working harder. Here are a few of the signs and symptoms of the condition:
Pain in the back of the lower leg, just above the heel.
Pain with running, jumping, or pointing the toes.
A small lump on the Achilles tendon just above the heel.
The first line of treatment is to rest and ice the tendon. Anti-inflammatory medications can help reduce pain. (American Academy of Orthopaedic Surgeons, 2022) Physical therapy can include strengthening exercises, ultrasound heat therapy, and deep massage. Exercises stretching the nearby muscles will help gradually increase the stress the tendon can handle, eventually reducing inflammation and swelling. Stretching and flexibility exercises will help an Achilles tendon heal. (University of Michigan, 2023)
The only way to determine if an individual has injured their Achilles tendon is to see a doctor. If the injury is Achilles tendonitis, a physical therapist may be recommended. A physical therapist can train individuals on the Alfredson protocol, an exercise protocol program for those with Achilles tendonitis (tendinopathy) that research has shown is helpful for those with the condition. The therapist will train on how to exercise to strengthen the tendon. The exercises stretch the Achilles tendon to help it handle forces and stress, known as eccentric loading. (Stevens M., & Tan C. W. 2014)
Inflammation
Tendonitis is inflammation of a tendon. However, studies have shown that the tendon might not be inflamed in those with the condition. When an area of the body is inflamed, inflammatory cells are present. Individuals usually feel pain in the inflamed area. For those with Achilles tendonitis, the tendon will present with pain, but not necessarily because the tendon is inflamed. Under a microscope, researchers examined tissue from the tendons of those with Achilles tendonitis. They did not find inflammatory cells in the tissue. (Stevens M., & Tan C. W. 2014) This means that although individuals felt pain, they were not inflamed. If there are no inflammatory cells in the tendon, this could explain why those with Achilles tendonitis often do not find relief from the anti-inflammatory treatment of non-steroidal anti-inflammatory drugs (NSAIDs). Studies have shown that gentle exercise protocols for the tendon are more helpful. However, researchers are not sure why these exercises are so beneficial. (O’Neill S., Watson P. J., & Barry S. 2015)
Eccentric Exercise
A chiropractic physical therapy team can help individuals heal the injury with eccentric loading exercises. Eccentric loading exercises work the muscles and tendons to help them get stronger. Once healing has begun, they can help strengthen the tendon. Individuals start slowly with easy exercises and then work up to harder ones. They will have the patient lengthen or stretch out the muscle. As the patient moves, the muscles and tendons contract or shorten. The Alfredson protocol consists of eccentric loading exercises for the Achilles and the muscles that support it.
Alfredson Protocol
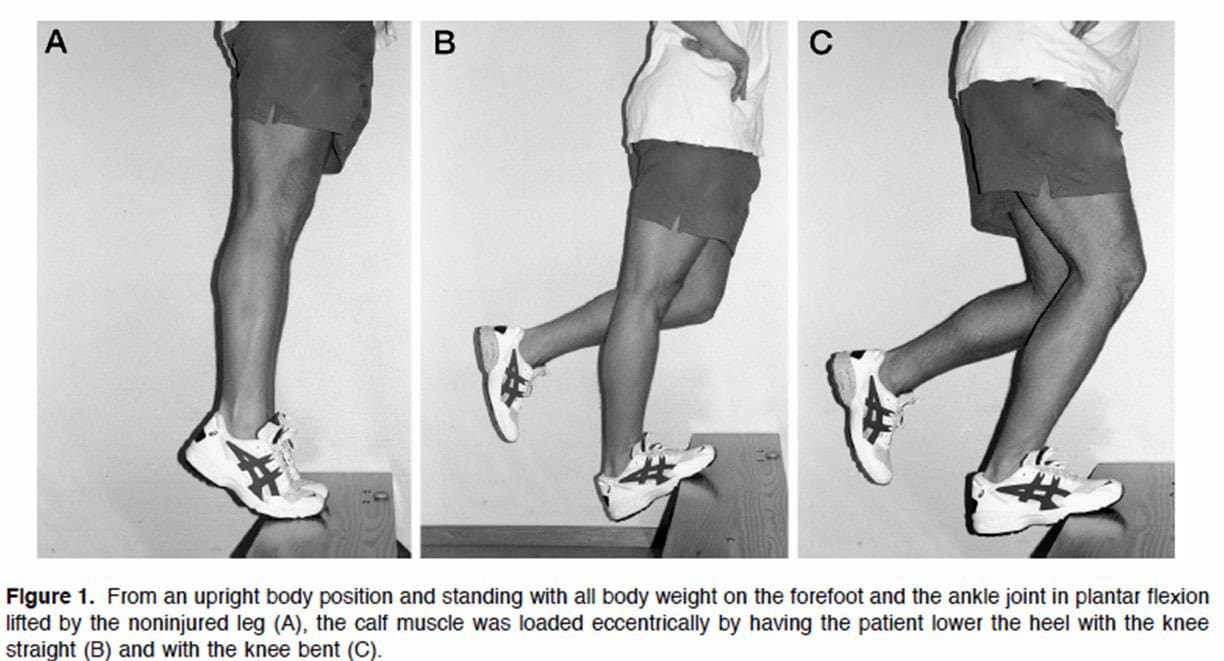
Before exercising, talk to a doctor or physical therapist to know if it’s safe. How to do the Alfredson protocol:
First, stand on a small step or curb.
Stand with the balls of your feet on the edge.
Your heels should hang over the edge.
Hold onto something for balance.
Keep the knees straight.
This will load a muscle part of the Achilles tendon called the gastrocnemius.
Using both feet, lift the heels and rise onto the balls of the feet.
Keep the foot with the painful Achilles tendon on the step.
Lift the non-injured foot off the step.
Slowly lower down using the injured ankle.
The heel should move towards the floor.
The ball of the foot should remain in contact with the edge of the step.
Return the non-injured foot to the step.
Repeat the exercise.
Do three sets of 15 reps with the knees straight. Then, do the Alfredson protocol again with the knees slightly bent. This will work a muscle called the soleus, which connects to the gastrocnemius. Perform three sets of 15 repetitions. Perform both exercises twice a day. This could be in the morning and the evening. The Alfredson protocol is most beneficial when done for about 12 weeks. (Stevens M., & Tan C. W. 2014)
Injury Medical Chiropractic and Functional Medicine Clinic
The Alfredson exercise protocol can be done at home with a step or raised platform to put the feet on safely. Individuals should consider working with a personal trainer to ensure safety and get the most out of the workouts. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to build optimal health and wellness solutions. We focus on what works for you to relieve pain, restore function, prevent injury, and help mitigate issues through adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal problems.
American Academy of Orthopaedic Surgeons. OrthoInfo. (2022). Achilles Tendinitis. https://orthoinfo.aaos.org/en/diseases–conditions/achilles-tendinitis/
University of Michigan. (2023). Achilles Tendon Injury: Physical Therapy and Rehab. https://www.uofmhealth.org/health-library/tr2261
Stevens, M., & Tan, C. W. (2014). Effectiveness of the Alfredson protocol compared with a lower repetition-volume protocol for midportion Achilles tendinopathy: a randomized controlled trial. The Journal of orthopaedic and sports physical therapy, 44(2), 59–67. https://doi.org/10.2519/jospt.2014.4720
O’Neill, S., Watson, P. J., & Barry, S. (2015). WHY ARE ECCENTRIC EXERCISES EFFECTIVE FOR ACHILLES TENDINOPATHY?. International journal of sports physical therapy, 10(4), 552–562.
The vastus lateralis is a muscle on the outside part of the thigh. Injuries to the muscle include strains, tendinitis, femoral nerve compression, and others. Can rehabilitation like heat and ice, massage, and strength and mobility exercises help individuals return to normal activities and function?
Vastus Lateralis Muscle
The vastus lateralis is the largest of the four quadriceps muscles on the thigh’s outer portion. The vastus lateralis helps extend the knee joint and maintain the knee position when walking or running. The vastus lateralis functions to work with the other quad muscles to help extend the knee joint.
Anatomy
Most muscles are attached to bone points of attachment, called the origin and insertion points. The vastus lateralis origin and insertion points are as follows (Vieira, EPL. 2017)
Origin
The origin is on the upper inter-trochanteric line of the femur or thigh bone.
It also arises from the base of the greater trochanter and the linea aspera, the supracondylar ridge, and the lateral intermuscular septum.
Insertion
From its origin, the muscle courses down the lateral thigh and inserts as part of the lateral quadriceps tendon on the tibial tubercle, an elevated portion of the upper shin.
The muscle is a large, flat structure with different attachments and a flat aponeurosis or sheath of connective tissue on the outer thigh.
The femoral nerve from lower back levels two, three, and four controls or innervates the muscle.
Blood supply to the muscle goes through the lateral circumflex femoral artery of the upper thigh.
Function
The muscle works with the other quadriceps muscles to extend or straighten the knee. The quads are responsible for functional activities like walking, running, climbing stairs, and getting up from a seated position. The vastus lateralis and the iliotibial band, which courses down the lateral thigh next to this muscle, form the lateral wall of the thigh. The vastus lateralis is on the opposite side of the vastus medialis muscle on the inner portion of the thigh. These muscles work together to maintain the appropriate position of the patella/kneecap in the femoral groove of the thigh bone. Malfunctioning these muscles properly can lead to knee pain from patellofemoral stress syndrome. (American Academy of Orthopaedic Surgeons, 2024)
Conditions
Many different injuries and conditions can affect the vastus lateralis and quad muscles, especially in athletes or active individuals. These injuries can cause vastus lateralis pain and other problems. (Timothy J. Von Fange, 2024) Some of the injuries and conditions include:
Patellofemoral Stress Syndrome – PFSS
This occurs when the kneecap tracks improperly in the femoral groove of the knee joint.
This leads to pain and difficulty when walking and running.
Vastus Lateralis Strain
A sudden force on the thigh can cause the quad muscle to be strained.
If the vastus lateralis suffers a pull injury, individuals may have pain, muscle swelling, thigh bruising, and walking difficulties.
Patellar Tendinitis
Irritation of the quad tendon that courses over the kneecap can cause patellar tendinitis.
Femoral Nerve Compression Weakness
The femoral nerve may become pinched or irritated from a herniated disc, lumbar stenosis, or arthritis.
Pain, numbness, tingling, or weakness in the thigh may result.
Iliotibial Band Friction Syndrome
Tight or weak muscles can irritate the IT band, and the vastus lateralis muscle can be affected.
Injury Rehabilitation
Injury to the vastus lateralis or quad muscles can cause pain, swelling of the thigh, or limited walking ability. Various treatments are available to help expedite recovery. A primary healthcare provider may recommend working with a physical therapy team. Self-care techniques can include:
Heat and Ice
Ice may be applied to the lateral thigh the first few days after injury to control pain and decrease swelling and inflammation.
Ice should be applied for 10 to 15 minutes.
Individuals may switch to heat two to three days after to promote circulation and improve tissue mobility.
Heat should be applied for 10 to 15 minutes.
Massage
Massage can help decrease pain and promote circulation.
Massage techniques can improve tissue mobility before stretching to help improve quadriceps motion.
Exercises and Stretching
A physical therapy team will prescribe certain exercises and stretches to help regain strength and range of motion. After an injury, quad stretching can improve the mobility and function of the muscle group.
Prone Towel Quad Stretch
Lie on your stomach and place a towel or strap around the ankle.
Bend the knee up, and gently pull on the towel to bend the knee fully.
A pulling sensation should be felt in the front of the thigh.
Hold the stretch for 30 seconds and release.
Repeat three times.
Half-kneeling Quad and Hip Flexor Stretch
Kneel on one knee.
Slowly move forward until a stretch is felt in the front of the hip and thigh.
Hold this position for 30 seconds.
Relax back to the starting position.
Repeat three times.
Back Exercises
If femoral nerve irritation coming from the lower back is causing thigh pain or weakness, exercises to release the nerve may be helpful and can include:
Prone press-ups
Supine lumbar flexion
Lumbar side glides
The exercises are designed to relieve pressure on the lumbar nerve, and postural correction exercises may be performed to maintain decompression.
Strengthening
Weakness to the vastus laterals and quads may be causing injury, and strengthening exercises may be prescribed during rehabilitation and can include:
Hip-strengthening exercises
Straight leg raises
Leg extension exercises
Lunges
Squats
Strengthening exercises should be done two to four times weekly with appropriate rest between sessions.
Balance exercises and sport-specific plyometric training may be recommended to ensure the quad functions normally.
Most quadriceps and vastus lateralis muscle injuries heal within six to eight weeks.
Recovery may be shorter or longer depending on the nature of the injury.
Injury Medical Chiropractic and Functional Medicine Clinic
By understanding the anatomy and function of the vastus lateralis muscle, a healthcare provider can help individuals understand their specific injury and develop a treatment program to rehabilitate the muscle properly. At Injury Medical Chiropractic and Functional Medicine Clinic, we focus on what works for you and strive to develop fitness and better the body through research methods and total wellness programs. These natural programs use the body’s ability to achieve improvement goals, and athletes can condition themselves to excel in their sport through proper fitness and nutrition. Our providers use an integrated approach to create personalized programs, often including Functional Medicine, Acupuncture, Electro-Acupuncture, and Sports Medicine principles.
Knee Injury Chiropractor
References
Vieira EPL. (2017). Anatomic study of the portions long and oblique of the vastus lateralis and vastus medialis muscles. J Morphol Sci., 28(4), 0-. http://www.jms.periodikos.com.br/article/587cb49f7f8c9d0d058b47a1/pdf/jms-28-4-587cb49f7f8c9d0d058b47a1.pdf
American Academy of Orthopaedic Surgeons. (2024). Patellofemoral pain syndrome. https://orthoinfo.aaos.org/en/diseases–conditions/patellofemoral-pain-syndrome/
Timothy J Von Fange. (2024). Quadriceps muscle and tendon injuries. UpToDate. https://www.uptodate.com/contents/quadriceps-muscle-and-tendon-injuries/print
Ramírez-delaCruz, M., Bravo-Sánchez, A., Esteban-García, P., Jiménez, F., & Abián-Vicén, J. (2022). Effects of Plyometric Training on Lower Body Muscle Architecture, Tendon Structure, Stiffness, and Physical Performance: A Systematic Review and Meta-analysis. Sports medicine – open, 8(1), 40. https://doi.org/10.1186/s40798-022-00431-0
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine