The sciatic nerve can be compressed, pinched, twisted, moved out of position by a variety of things, including injury/s and spinal conditions, diseases, and the most common a herniated disc. This could be time to try the chiropractic solution that can treat sciatica symptoms and bring relief quickly. If you are experiencing a shooting, electrical, tingling, numb pain down one of your legs could be a presenting of sciatica symptoms.
Sciatica
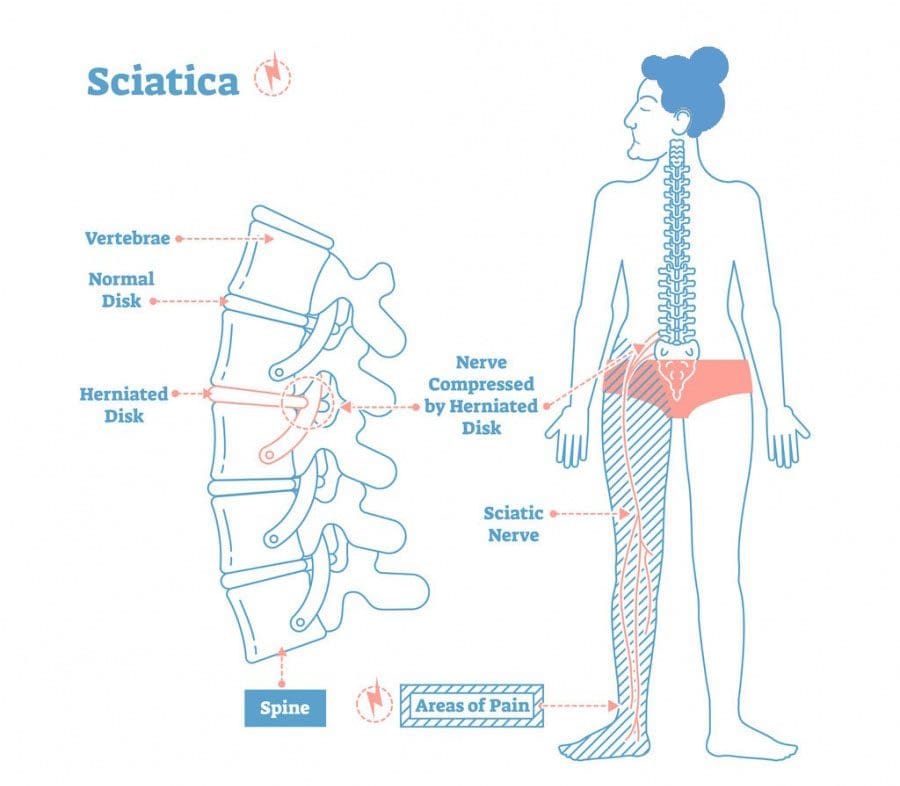
Sciatica is really a symptom itself caused by lumbar radiculopathy. Lumbar radiculopathy is a medical term referring to a low back condition/injury/disorder that is affecting the nerves in this area. The sciatic nerve travels from the lower back down both of the legs and into the feet. Added pressure placed on the nerve from a herniated disc can lead to common symptoms.
Shooting pain that goes down from the low back, through the leg, calf and sometimes into the foot
A feeling of electricity down one leg
Burning pain
Pain from moving
Numbness
Weakness
Causes
Causes of sciatica include:
Vertebrae Out of Alignment
Misaligned vertebrae, referred to as subluxations can put pressure on nerves in the spine � including the sciatic nerve.
Disc Herniation
The discs that cushion the vertebrae are made up of a tough outer layer and a softer inner layer. When the outer layer is damaged and the inner layer comes out into the spine, it is referred to as disc herniation.
A herniated disc means that the inner layer of the disc is putting pressure on nerves in the spine. A herniated disc impacts the sciatic nerve and can lead to sciatica.
Car Accidents
A car accident can easily damage the spine and soft tissues. An accident can cause a misalignment of the spine, a herniated disc, or other injuries that cause symptoms of sciatica.
Sports Injury/s
Even the fittest athletes are susceptible to back injuries, which in turn can cause sciatica. The spine and discs can be damaged due to a large impact, repetitive motion injuries, or even twisting the wrong way.
Work Injuries
Many sufferers of sciatica do not realize that their workplace activities � including repetitive motions and sitting or standing in one position for long periods of time � can lead to sciatica.
How Chiropractic Solution Helps
Prevention found that sixty percent of individuals with sciatica failed to find relief from other treatments found their symptoms improved after chiropractic treatment.
The chiropractic solution works because it gets to the source of the problem and relieves pressure on the sciatic nerve. Chiropractic treatments include:
Realignment
Spinal misalignments are often the cause of sciatica can be corrected through careful chiropractic adjustments. The chiropractor analyzes the misalignment, then applies pressure to the area to correct the misalignment. The pressure is removed from the sciatic nerve, and this is done on and off to get the correct position and massaging the inflamed tissues until symptoms improve.
Spine Decompression
For those whose sciatica is caused by a herniated disc, spinal decompression can bring real relief. Using a specially designed table, the chiropractor can gently stretch the spine � creating space for the disc to heal and pull back from the sciatic nerve.
Find Relief
Please contact our chiropractic team today to schedule an appointment if you are experiencing symptoms of sciatica. We are ready to help you feel better and get back on your feet again. We focus on improving your ability through flexibility, mobility and agility programs tailored for all age groups and disabilities.�We do this so that we may reach as many El Pasoans who need us, no matter the affordability issues.
Severe *Sciatica”* Pain Relief | El Paso, Tx (2020)
NCBI Resources
Patients with sciatica feel better with time, usually a few weeks. If pain continues, other treatment modalities can be discussed.�Muscle spasms can accompany sciatica symptoms and can be treated with heat or ice therapy. A doctor may advise�light exercise like short walks�and once recovery is established they may give you exercises to strengthen your back and core.
Sciatica is not only caused by a spinal injury, although this is the primary cause, sciatica can also surprisingly be caused by your clothes and shoes. Sciatica is defined as symptoms that include back, leg, and foot pain caused by the compression of the sciatic nerve. Other symptoms can include shootingelectrical rays of pain, weakness, and numbness from your low back all the way down your legs into your feet.
Because of the intensity, many assume it has to be something serious like a work/car accident, sports injury or severe trauma. All of this can lead to sciatica, but there are also everyday things that we do daily that can also cause it. Here are some lesser-known ways of developing sciatica.
Items in Your Back Pocket
Many of us put our phones or wallets into our back pockets. When we carry these items in our pocket and then sit down on them, this can become a gradual trigger to sciatica. When we sit with these items begin to irritate the piriformis muscle. The sciatic nerve is right underneath this muscle and can get compressed. This cause has not been defined by the medical community, but a few names floating around include (back-pocket sciatica and cell-phone sciatica).
Wearing High Heels
High heels push your weight forward and so your body wanting to remain upright responds by flexing the hips to keep you straight. The risk of sciatica happens when this flexing at the hips stretches the hamstrings that can irritate the sciatic nerve running alongside the hamstrings. And besides sciatica high heels can cause a bevy of other spinal problems.
Wearing Tight Jeans and Underwear
Overly tight-fitting pants and underwear might look and feel great, however, they can also contribute to sciatic nerve pain. Wearing tight clothing is not bad but realize that wearing this type of clothing every day will start to compress the muscles, ligaments, and nerves. Mix it up with clothing that allows you to move freely. If your clothing cuts off circulation absolutely do not wear it. And when it comes to tight pants, change postures and don’t stay in the same position for too long, especially sitting.
Excess Weight
Research has found an association between being overweight and having sciatica.�Excess body weight puts stress on your spine. This added pressure combined with sedentarism can cause spinal disorders that include sciatica. Being able to maintain a healthy weight will greatly reduce your risk of developing sciatica symptoms.
The Impact of Sciatica
Even if just gradual weakness develops down your leg or a sudden burst of pain comes and goes, do not ignore it and make an appointment with your doctor or chiropractor to understand the issue and underlying cause/s and set up a preventative treatment plan before it gets out of hand. There are many sciatica treatments/therapies to reduce or eliminate low back and leg pain. Your doctor/chiropractor will work with you to develop a custom sciatic preventive exercise treatment plan.
Severe *Sciatica”* Pain Relief | El Paso, Tx (2020)
NCBI Resources
A study cited by the health magazine�Prevention found that sixty percent of sciatica sufferers who failed to get relief from other treatments found their symptoms improved after chiropractic care. Please contact our chiropractic team today to schedule an appointment if you are experiencing symptoms of sciatica. We are ready to help you feel better and get back on your feet again.
Inversion tables and inversion treatment/therapy could help with low back/leg pain and sciatica. It�s non-surgical and an option your doctor, or chiropractor could recommend to you before looking into more invasive options. Individuals with low back pain, sciatica or both found inversion therapy with an inversion table provided relief from symptoms, and continued use has kept them and their spines healthy.
With an inversion table, you don�t have to use gravity boots or completely hanging upside down. There are inversion boots and hanging racks that also offer inversion therapy, this type is not for beginners. With experience, you can move on to this type but for now, leave it to individuals in top health and athletic condition. This type of inversion table therapy is an alternative that doesn’t require being completely upside down.
An Ancient Therapy Brought Back
Inversion therapy is nothing new. Hippocrates, the father of medicine, saw what inversion therapy could do and the benefits around 400 BC. The goal is to use gravity to release compression in the spine. The downward force pulls everything toward the earth’s center.
How It Works
Inversion therapy works in a way like spinal traction.
For example, when we stand and sit gravity pulls the spine downward and this is what compresses the discs, vertebral bodies, nerves, and other spinal structures. The physical dynamics along with gravity helps relieve spinal compression. As the spine is stretched out the pressure on your back is reduced.
The theory behind inversion therapy sounds like a fantastic non-surgical option to back pain. However, the research going into inversion therapy is a bit more mixed. One study found that almost 77% of patients that were candidates for surgery no longer needed the surgery after using inversion therapy. For patients that didn�t use inversion therapy, only 23% avoided surgery.
But like all back pain/sciatica treatment plans, it’s what works for you. Ask your doctor/chiropractor about the pros and cons of this type of treatment as it relates to your condition to make an informed decision.
Other Benefits
Many patients report that inversion therapy is a great way to:
Stretch the muscles and ligaments
Reduce muscle spasms
Improve circulation
Stretching stimulates the lymph glands which increases the flow of lymphatic fluids, that are part of the body’s waste disposal. Cellular health depends on healthy blood circulation to be delivered, to nourish and remove waste.
The therapy also helped to relieve motion sickness and stress. This is because the body is more aware of its spatial orientation along with balance as the inner ear gets stimulated while inverted. As stated earlier it is not necessary to be positioned completely upside down to benefit from this therapy. Inversion tables are adjustable and offer the flexibility to find the best angle.
Discuss Inversion Therapy with A Doctor
Before you start using an inversion table�talk to your doctor. Certain medications and health conditions could make using an inversion table unsafe.
It could be recommended against inversion table therapy if you have:
There could be other medical conditions that are not listed but could interfere with inversion therapy, so make sure your doctor knows all your medical history/conditions and current health state before beginning.
Starting Inversion Therapy
How to start an inversion therapy program? Take it very slow, easy, taking your time and have someone there to help and assist until you are comfortable doing it on your own.�The tables can be set at different angles and it is recommended you start at the first and work your way to the last. At the 15-degree angle, your body will feel a stretch along with the benefits of increased blood circulation.
Most people don’t have to go beyond 60-degrees, as the spine decompresses at this angle. But you might want to completely invert yourself as you work through the different degrees and go for the full inversion. But don’t overdo it and listen to what your body tells you.
The tables come in a variety of styles, so be sure to research the different brands. Some tables can include a sliding backrest and foot lock that lets you work in gentle stretching exercises during inversion. This could include head movements from side-to-side, stretching the arms overhead, and doing abdominal sit-ups or crunches.
But first, find out from your doctor how often you should invert and the kinds of movements that will help with your condition and enhance your inversion program. Inversion therapy is another option for a back, sciatic pain treatment plan. For the different forms of spine pain, a doctor will try several non-surgical treatment options before discussing surgery. Inversion therapy could be part of a conservative treatment plan and could help prevent the need for spine surgery.
*Effective Treatment* for Sciatic Nerve Pain| El Paso, Tx
NCBI Resources
The spine is the primary support for the body. When it breaks down, the body suffers. Regular chiropractic treatment ensures that the spinal column remains in proper alignment which, in turn, keeps the body in proper alignment. It helps with joint health as well as the health of the related muscles and ligaments.
Your chiropractor can also recommend stretching and strength-building exercises to help keep your spine healthy and supple. Chiropractic helps to keep the back flexible which aids in preventing injury. A healthy spine is also less likely to become misaligned or experience pain. It can significantly improve your quality of life as you are more flexible and mobile.
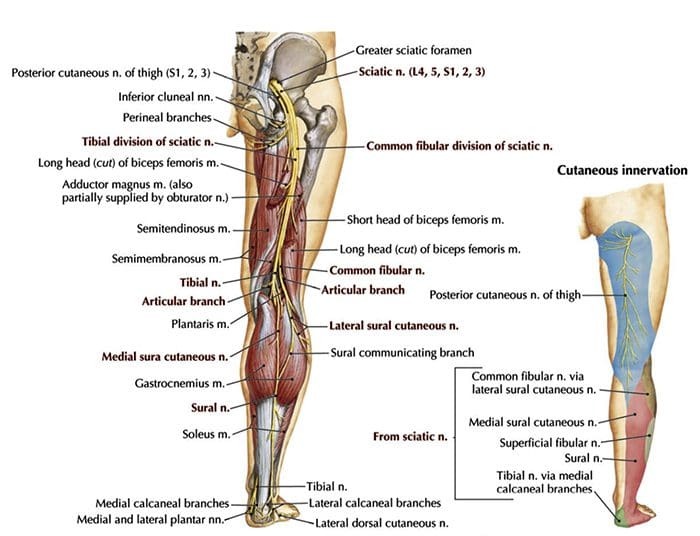
Sciatica is pain that can be accompanied by numbness, tingling and occasionally weakness along the course of the sciatic nerve. The sciatic nerve is the thickest in the body and is formed from nerve roots exiting the spine, and extend into the buttocks and down the back of the legs to the toes. Common causes of sciatica along with non-surgical treatment options are presented by a chiropractor and a physical therapist.
Causes of Sciatica and Non-Surgical Care
Compressed Lumbar Disc also called lumbar radiculopathy
Probably one of the most common causes of sciatica that I treat. About 90% of patients have a positive response to alternative/conservative treatment. I use x-rays as a guide to follow where the nerve is compressed and where the best manipulation areas are for me to adjust. Spinal manipulation is a very safe procedure and most cases will heal without surgery.
Dr. Alex Jimenez D.C. and a practicing physical therapist� �Combined with chiropractic treatment and massage, we may use a topical steroid combined with electric stimulation or ultrasound to adjust/release the area where the nerve is compressed.”
Lumbar traction is also used to reduce the size of the disc herniation and combine this with exercises, which are customized to the patient. Extending back and flexing exercises are also incorporated into the treatment plan and each is made specific to the patient. Patients may experience muscle spasms or joint stiffness, which is also relieved by massage therapy and joint mobilizations. Patients could also be trained on Kinesio tape application to relieve pressure and relax muscles.
Remember that strengthening the core is the key to reduce the risk of worsening the injury and getting new ones.
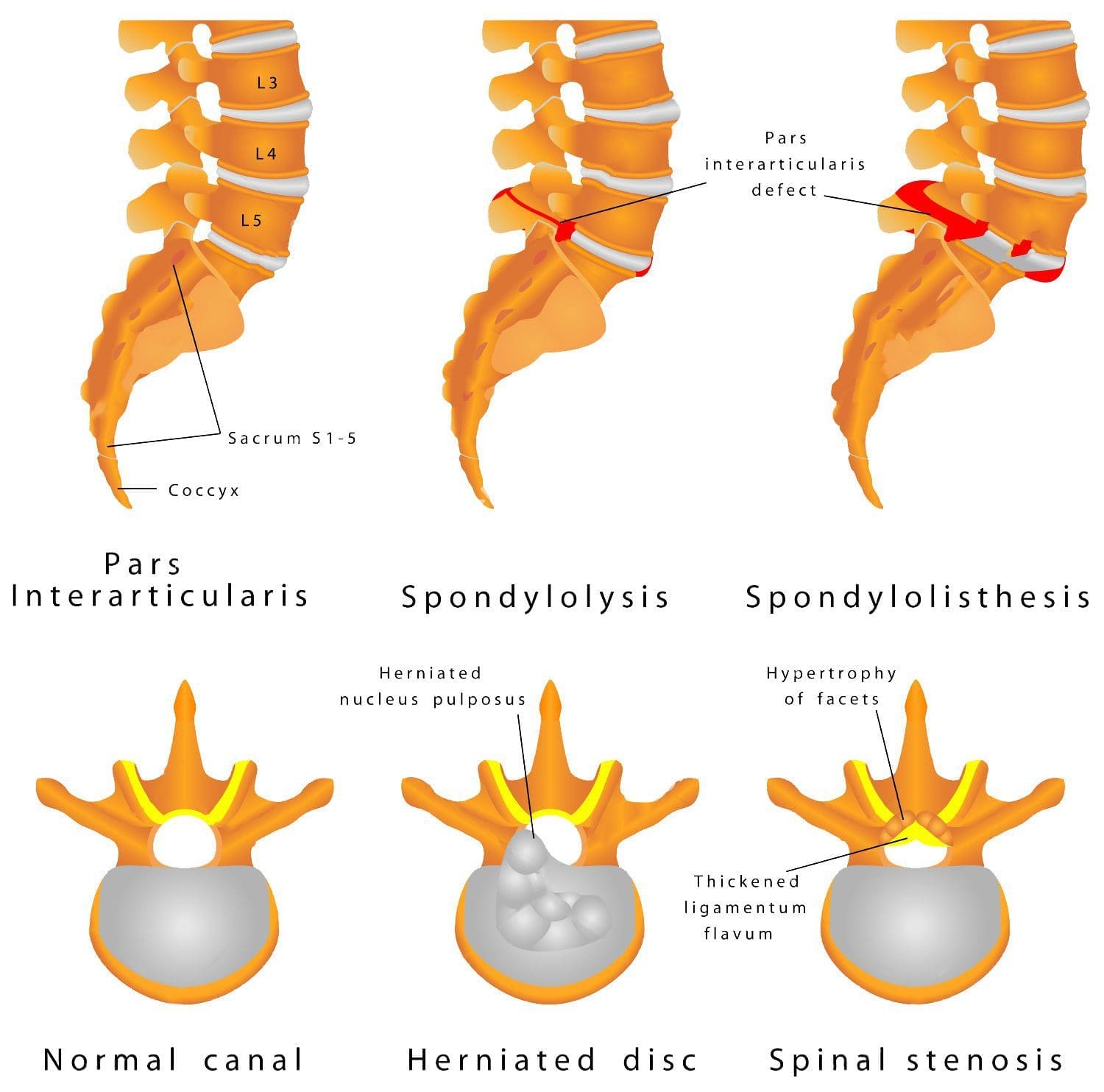
Lumbar Spinal Stenosis
This is a condition that can be difficult to treat because of the mechanical nature of the compression on the nerves. The cause is often a combination of osteoarthritis, disc bulging and spinal holes that have narrowed�called neuroforamen. Physical therapy consists of traction, stretching, exercises, and chiropractic to lessen pain and inflammation.
Spondylolisthesis
This condition can be caused by trauma or degeneration of the spine. Conservative care is highly beneficial.
Extending the spine can worsen symptoms, therefore flexion-based exercises are what we recommend. Therapeutic exercises are utilized for abdominal strengthening and core stabilization. We get the patient to increase hip extension to reduce stress on the lumbar spine.� Manual therapies can also be used to control inflammation and alleviate muscle tightness or spasms.
Piriformis Syndrome
Piriformis syndrome also responds positively to conservative treatment. We look for the main cause when we see piriformis syndrome. This type of injury happens when a patient has a job or play a sport where they shorten and overuse the muscle.
We create a custom treatment/exercise program based on what is found structurally. Most of the time the piriformis muscle gets over-used because the hips are weak, so strengthening the hips and the core is key. Sciatic nerve mobilization can also help increase�sciatic nerve mobility. This can be achieved with instrument-assisted soft tissue mobilization/Graston technique along with deep tissue massage will get optimal results.
Pregnancy
Sciatic symptoms often do present in pregnant women, which can make the pregnancy miserable. Our goal is to reduce symptoms and restore normal function with gentle exercise, massage, and hot/cold therapy.
The pelvic girdle is what we focus on, along with core stabilization, and Kinesio tape application to stabilize the girdle because of ligamentous laxity or loosening of the hips.
Trauma
Any kind of trauma that hits the gluteal area can become inflamed and spasm and bind around the sciatic nerve. We focus on relieving the pain and inflammation with manual therapies, and gentle exercises. These are based on what is found from the examination and how intense/extensive the trauma was.
Light spinal mobilization and massage have been proven to activate the body’s natural painkillers to alleviate and release the tight muscles. More rigorous exercises are brought in to the treatment plan as the patient gets stronger. These will strengthen their core and get them back to regular activities, job, and their sport.
*Effective Non-Surgical Treatment* for Sciatic Nerve Pain| El Paso, Tx
NCBI Resources
You may be suffering from�sciatica if you have ever experienced a shooting, nerve-like pain down one of your legs. The sciatic nerve can be impacted by a number of different things, including injury and degenerative diseases, that can lead to sciatica. Fortunately, chiropractic can be an effective non-surgical treatment for sciatica.
A car accident can easily damage the spine and soft tissues. An auto accident may cause a misalignment of the spine, a herniated disc, or other injuries that cause symptoms of sciatica.
Most of us know what sciatica means and that is low back pain that radiates/spreads into the buttock down into the leg and sometimes into the foot. The pain can be mild to excruciating, but fortunately, if it is mild�sciatica can usually be alleviated in 3 months.�These are a few non-invasive conservative treatment therapies that can be done at the house.
Here are a few at the house sciatica remedies for people who started experiencing sciatic nerve pain or whose pain is not severe. But you should get a doctor�s approval before trying any of these at the house therapies.
If sciatica has been present for a few weeks or the low back and leg pain has become debilitating you should see a doctor.
House Tip 1. Exercise is OK & Beneficial
It might seem strange to exercise when you�re in pain, but research has shown that too much rest can aggravate back and leg symptoms.
Remember this is not a hardcore burning massive calories exercise, but a gentle exercise routine that you can work into your day.
These Exercises should not be painful or strenuous.
A walk around the house is a great form of physical activity that keeps your spine strong without worsening the injury.
Make your spine stronger with core exercises, but make sure they will not exacerbate your sciatica symptoms. And remember that exercise triggers the release of endorphins to reduce the pain.
House Tip 2. Start Stretching
Start doing gentle stretches regularly. Stretching will improve your spinal flexibility and motion range and also builds core strength. Most stretches can be done while watching your favorite show/movie.
House Tip 3. Ice Packs and Heating Pads Help
Alternating heat and ice therapy can bring relief from nerve pain. Ice helps reduce inflammation, and heat generates blood flow to the areas of pain that speeds up healing. Both help reduce muscle spasms that usually come with sciatica.
Apply the ice pack for 15 minutes once every hour, and then bring the heat for 15 minutes every 2 or 3 hours. Remember to protect your skin when using these pads, and never sleep with the heat or ice pads.
House Tip 4. Change Your Posture
If you are working at your desk or just relaxing, don’t stay in the same position too long, as it can make the pain spike.
Therefore move around and change your posture every 20 minutes. Using the correct posture for various activities will help take the pressure off your spine and reduce symptoms.
House Tip 5. If You Need To Use Medication Properly
Over-the-counter non-steroidal anti-inflammatory medications can help ease symptoms when they present. These medications can relieve inflammation and pain, whereas acetaminophen (Tylenol) only reduces pain.
However, there are health risks, so make sure to discuss their safety with your doctor.
Examples include:
Ibuprofen (Advil, Motrin)
Aspirin (Ecotrin)
Naproxen (Aleve)
The Remedies Are Not Working
Recognize when at the house remedies are not reducing your symptoms. When the treatments aren’t helping, it could be time to see a doctor, chiropractor or spine specialist.
People including myself want to avoid the doctor. It could be knowing how to use your health insurance or if you don�t have any. Whatever the reason do not opt for the ignorance is bliss and hope it will all go away.
If you need help figuring out how to use your insurance here at Injury Medical our staff are trained to help guide you through the process. And if you don’t have insurance we can still help and work out different types of plans.
Now there are sciatica symptoms that warrant immediate medical attention. In these rare cases, holding off medical care could cause permanent nerve damage.
If any of the following occur, please see your doctor as soon as you can:
There is severe throbbing/stinging pain in your low back and legs
Nerve associated symptoms like:
Weakness
Numbness
Tingling
Electric shock-like pain
The pain is not improving after 2 weeks
The pain gets worse, even with house therapies
Loss of bowel or bladder control
At the end of the day reducing sciatica symptoms doesn�t always mean having to use an extreme treatment approach. Relieving sciatica symptoms at the house with light exercise, ice/heat therapy, correct posture, and medication can help speed up recovery. The most important thing you can do is to take it seriously and call your doctor or chiropractor if relief is not happening.
Please contact our chiropractic team today to schedule an appointment if you are experiencing symptoms of sciatica. We are ready to help you feel better and get back on your feet again!
*Effective Treatment* for Sciatic Nerve Pain| El Paso, Tx
NCBI Resources
A study cited by the health magazine�Prevention�found that sixty percent of sciatica sufferers who failed to get relief from other treatments found their symptoms improved after chiropractic care. In fact, they got the same level of relief as those who went through surgery � without any of the serious side effects that so often come with surgical procedures.
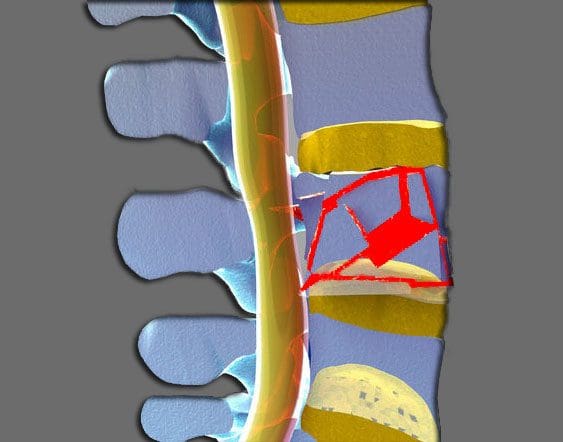
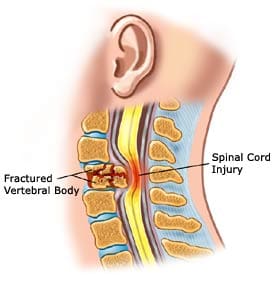
A burst fracture describes an injury to the spine where the vertebrae get compressed severely. These types of injuries occur from severe trauma, like an automobile accident or a serious fall, sports injury, work injury. These injuries entail a great deal of force into the spine, so much so that a vertebra can get crushed.
When crushed in the front of the spine, a wedge-shaped fracture occurs and is known as a compression fracture.
But if the vertebral body gets crushed in all directions this is known as a burst fracture.
The term burst means that the vertebral body spreads out in all directions.
Severe Injury
This is a much more severe injury than a compression fracture. With the bones crushed and possible rough jagged edges, if they spread out the spinal cord has a high probability of being injured. The fragments can bruise the spinal cord causing paralysis or partial neurologic injury. The spine becomes far less stable than from a compression fracture.
Nerve Injury
Neurologic injuries from a burst fracture can range from no injury to paralysis. This depends on the amount of force present at the time of the injury and how much the spinal canal is compromised.
A greater amount of force equals more bony fragments that can be forced into the spinal canal and cause higher loss of spinal cord function.
This can cause loss of:
Strength
Sensation
Reflexes below the injury
With an incomplete spinal cord injury, partial paralysis or partial reflex loss occurs.
With a mild burst fracture, only short-term symptoms could be present and no neurologic injury.
Intense Pain
Burst fractures can cause intense pain and the pain is right where the trauma took place.
But pain can also present in the legs and feet depending on how the spinal nerves were affected, shifted or pinched. Patients complain of an electric tingling or shooting type sensation in their legs with spinal cord compression. With a burst fracture, individuals are unable to walk right after the trauma. But the pain percentage present is severe enough that they know not to try and walk.
Diagnosis
If at the sight of the accident the patient says that they have severe back pain should not be in a seated flexed position. They need to be kept lying flat and transported in a flat position.
If they stand or sit with a burst fracture, it can increase the possibility of a neurologic injury.
Burst fractures require immediate medical attention from an orthopedic or neurosurgeon. The patient is taken to an emergency room and x-rays, CT scans are gathered.
The diagnosis of a burst fracture is typically made with x-rays and a CT scan.
Sometimes, an MRI will be ordered to assess the amount of:
Soft tissue trauma
Bleeding
Ligament injury
The CT scan and x-rays allow the doctor to determine the level of the fracture, and if it is a:
Compression fracture
Burst fracture
Fracture-dislocation
This will determine how much the spinal canal has been compromised and if its angulation or angle has taken an abnormal bend or curve. These factors all contribute to the development of an optimal treatment plan.
The physical exam will document:
Spinal deformity and Angulation of the spine
Tenderness of the spine where the fracture is located
Neurologic exam
Neurologic exam should include testing:
Muscle strength
Sensation
Reflexes of the lower extremities
Testing of bowel and bladder control
Treatment & Recovery
A stable burst fracture can be treated without surgery.
A stable burst fracture falls into these parameters:
There is no neurologic injury
The angulation is less than 20 degrees
The amount of spinal canal compromise is less than 50%
With this type of treatment, a brace along with physical therapy/chiropractic can have excellent results.
A turtle or clamshell brace TLSO�(Thoracic Lumbar Sacral Orthosis) is a body cast used in the treatment of a burst fracture.
The brace is worn for eight to twelve weeks for adequate and optimal healing.
There are times when a fracture thought stable and treated can start to angulate. This may require surgery. However, all burst fractures require some form of treatment.
Recovery
Nonsurgical treatment patients stay in the hospital for one or two days while their brace is fit.
X-rays are done in the standing position to make sure the spine stays stable.
Pain medications are prescribed for three to four weeks
Non-narcotic medications can begin after the final week
When the brace is removed, physical therapy and chiropractic are instituted to help return strength to the core and lower extremities.
Surgical patients will remain in the hospital for three to five days.
They will be fitted with a brace after the incisions present less pain and are recovered from the surgery.
They can walk within one or two days with the help of a physical therapist.
X-rays are taken to follow the position of the spine and see how the healing is progressing.
Chiropractic/Physical therapy is implemented to help with core strength and lower extremity strength.
Recovery time depends on the severity of the neurologic injury.
Patients that don’t have a neurologic injury can make a full recovery with return to most activities.
Patients with partial neurological injuries can also expect to fully recover.
Unfortunately, with permanent neurologic injury, recovery can be limited.
But treatment for burst fractures today is superior to what they were years ago, especially with spine specialists and specific spinal procedures.
Chiropractic Rehab
Chiropractic is not a treatment for fractures but is a treatment for subluxations and rehabilitation with these types of fractures. Once a fracture has stabilized and healed properly, a chiropractic evaluation can rule out any lingering subluxation, herniation, and joint restriction. The adjustments are safe and effective in establishing optimal function to a subluxated joint.
Chiropractic Treatment For Car Accident Injuries El Paso, Texas
We focus on what works for you. We also strive to create fitness and better the body through researched methods and total wellness programs. These programs are natural and use the body�s own ability to achieve goals of improvement.
NCBI Resources
Chiropractors can help alleviate some of the long-term and immediate concerns associated with bone fractures. A chiropractor can help with compression techniques which are beneficial in maintaining the bone in place for healing. A chiropractor may also advocate wellness techniques, such as a healthy diet that will optimize the body�s ability to restore its original health and wellness. Chiropractors may also educate a patient on a variety of exercises and stretches to reduce the likelihood of complications and which, if done properly and at fixed intervals, will promote quicker recovery.
Being pregnant is one of life’s many joys, however, with the added weight comes normal back pain that can lead to severe back pain that can lead to sciatica.
Expecting mothers have much to look forward to but when back pain and sciatica take hold, it can be exhausting, frustrating, and extremely painful. Women experiencing pregnancyback pain varies from woman to woman. To help prevent and alleviate back pain/sciatica, here are some answers as to how and why symptoms develop and what to do to make the pregnancy a joyful occasion.
Pregnancy Back Pain and Sciatica
Changes to the body throughout pregnancy affect more than its physical appearance.
The most common change is weight gain. Increased body weight, especially when bending puts pressure on the spinal discs. The most pressure is placed on the low back. Back, leg pain, and sciatica are common complaints.
Weight gain can cause piriformis syndrome and sciatica. The piriformis muscles help with thigh movement. Piriformis syndrome can develop if the muscle compresses the sciatic nerve, which causes a pinching or electrical shock feeling in the buttocks and back of the leg.
What some might not know is that as the uterus grows, the body’s center of gravity gets thrown off. What happens is the uterus expands inside the pelvis, and the spinal nerves in the low back that flow into the sciatic nerve gets compressed and irritated.
Hormones like relaxin, which is a hormone that relaxes the pelvic ligaments and helps prepare the mother’s body for birth. Relaxin loosens the ligaments in the other areas of the body, but primarily the joints in the pelvis, low back, and knees. When exercising or lifting objects it is easy to strain these relaxed areas. Therefore, move slowly, and avoid any sudden movements.
What Steps To Take
Work with a:
Doctor
Chiropractor
Midwife
Health care provider to keep body weight in check
Take note of posture:
Stand up straight
Shoulders back
Avoid leaning backward
Try a pillow:
A standard-sized pillow
Body pillow to help make sleeping comfortable
A pillow can be positioned between the knees and under the abdomen for support.
Prenatal yoga helps:
Stretch and tone muscles
Maintain flexibility
Improve balance and circulation
Relieves tension
Deep breathing plays a major role in yoga and is an added benefit as it can help expecting mothers relax during labor.
Simple cardiovascular exercises like walking or swimming can help keep weight under control and the body in shape. Ask a doctor or chiropractor if these types of exercises are right for you.
Prenatal massage is another option to help relieve pain and tension.
This type of massage eases:
Anxiety by stabilizing hormone levels
Back pain
Pelvic pain
Hip pain
Improves circulation and digestion
Helps reduce fatigue
A warm shower or bath can helps ease back pain.
Expectant mothers should avoid aromatic oils or aromatherapy candles like:
Basil
Juniper
Peppermint
Rosemary
Star anise
Some of these oils can cause contractions.
Acupuncture is another form of alternative therapy that can treat back pain and sciatica. Sterile, millimeter thin disposable needles are inserted into points on the body that are known as energy channels. The needles help to restore the balance of energy in the body. However, expectant mothers need to be past six months to receive this type of treatment as the energy flow can cause contractions.
Ergonomics At Work & Home
Expectant mothers should avoid:
Awkward postures
Over-exercising
Heavy lifting
Repetitive work
Especially during the third trimester.
The low back and leg muscles have to work harder to keep the body balanced. Just basic standing or walking can be a challenge. Swelling is common. Make sure to take constant breaks and full-body rest combined with elevating the feet can be very helpful.
Adding an ergonomic and adjustable chair with a lumbar support backrest and footrest is worth the investment. A chair like this can helps take the pressure off of the spine and working at a desk much more comfortable. It benefits to frequently stand and sit continually changing the body’s posture and working the various muscles, joints, and ligaments to keep the body loose. And it can be a form of exercise.
Light walking also helps to reduce any swelling through increased circulation.
Hopefully, you will not have to go through any kind of back pain or sciatica. But if pregnancy back pain and sciatica start to creep in, talk to your doctor, chiropractor, midwife, or health care professional first.
When your body is truly healthy, you will arrive at your optimal fitness level proper physiological fitness state. We want to help you live a new and improved lifestyle. Over the last two decades, while researching and testing methods with thousands of patients, we have learned what works effectively at decreasing pain while increasing human vitality.
We focus on what works for you. We also strive to create fitness and better the body through researched methods and total wellness programs. These programs are natural and use the body’s own ability to achieve goals of improvement.
Back Pain During Pregnancy Treatment El Paso, TX Chiropractor
NCBI Resources
Keeping the body, including the spine, in proper alignment is vital to mobility, flexibility, and overall wellness of the body even when it is not pregnant. However, pregnancy puts specific stress on the body, creating certain needs that chiropractic care can meet. It is safe, it is effective, it is fast, and it works.
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine