Dr. Alex Jimenez at El Paso Back Clinic®: Beating Back Pain from Long Desk Hours
Businesswoman experiences worsening back pain while sitting at her desk.
If your back pain gets worse the longer you sit at your desk, you are not alone. Many people in El Paso face this issue due to long hours spent in sedentary jobs. Sitting for extended periods can put pressure on the spine, tighten muscles, and reduce blood flow, leading to stiffness, aches, and, in some cases, chronic problems (Colorado Pain Care, n.d.). The positive news is that you can take simple steps to reduce the pain and prevent it from worsening. At El Paso Back Clinic® in El Paso, TX, the wellness chiropractic care team, led by Dr. Alex Jimenez, DC, APRN, FNP-BC, focuses on helping people just like you find natural, long-term relief through personalized plans.
Prolonged sitting stresses the lower back by increasing disc pressure by up to 90% compared to standing. It flattens the spine’s natural curve, strains muscles, and creates imbalances (Colorado Pain Care, n.d.). Slouching or leaning forward adds extra load to the neck and upper back. Over time, this can lead to tight hips, weak core muscles, and ongoing discomfort that affects daily life.
At El Paso Back Clinic®, our experts understand these issues caused by sedentary work. They use a holistic approach that combines chiropractic adjustments, functional medicine, and rehab to address root causes like poor posture and muscle imbalances from desk jobs (Jimenez, n.d.-a).
Here are practical changes to start today:
Move often: Get up every 30 minutes to stand, walk, or shift positions. Short 1-2 minute breaks improve circulation and ease tension (Huntsville Hospital Health System, n.d.; Sydney West Physio, n.d.).
Use regular breaks: Set a timer for quick walks to get water or to stretch. This habit prevents stiffness from building up throughout the day.
Add dynamic movement: While sitting, shift weight, uncross legs periodically, or use a footrest to change angles. These small actions keep the spine mobile (Colorado Pain Care, n.d.).
A proper ergonomic setup supports optimal posture and reduces strain.
Follow these key tips:
Set your chair so that your feet are flat on the floor, your knees are at 90 degrees, and your hips are level with or above your knees.
Add lumbar support (a small pillow or rolled towel works) to maintain the lower back’s curve.
Place your screen at eye level to avoid looking down or up too much.
Keep the keyboard and mouse close so elbows bend at 90 degrees and shoulders stay relaxed.
Avoid crossing legs for long, as it can tilt the pelvis (Senara Chiropractic & Med Spa, n.d.; Huntsville Hospital Health System, n.d.).
Consider alternating between sitting and standing with a standing desk. Even partial standing reduces spinal pressure.
Stretches help loosen tight spots from sitting, such as the hips, shoulders, and neck.
Try these simple ones:
Hip flexor stretch: Kneel on one knee, gently push hips forward, and hold 20-30 seconds per side.
Chest and shoulder opener: Clasp hands behind your back or use a wall to stretch forward.
Neck tilts: Slowly tilt the head side to side or forward/back; hold for 10-15 seconds.
Upper back extension: Hands behind head, gently arch upper back (Sydney West Physio, n.d.).
Do them hourly or during breaks for better flexibility.
Strengthening the core supports the spine and improves posture long-term.
Include these:
Planks: Hold forearm plank 20-30 seconds.
Cat-camel: On hands and knees, arch and round back slowly.
Bridges: Lie back, lift hips while squeezing glutes.
Walking or gentle yoga: Build overall strength (Huntsville Hospital Health System, n.d.; Sydney West Physio, n.d.).
Aim for 20-30 minutes of activity most days.
For lasting relief, professional care targets alignment, mobility, and personalized fixes. At El Paso Back Clinic®, Dr. Alex Jimenez leads a team offering integrated chiropractic care. This includes spinal adjustments to correct misalignments, non-surgical spinal decompression for disc relief, acupuncture, functional medicine for nutrition and stress, and rehab exercises tailored to desk-related issues.
Dr. Jimenez, with dual expertise as a chiropractor and nurse practitioner, emphasizes posture correction, mobility training, and the prevention of sedentary pain through evidence-based methods. The clinic helps restore function without drugs or surgery, focusing on root causes like imbalances from prolonged sitting (Jimenez, n.d.-a; Jimenez, n.d.-b).
Other options in El Paso exist, but El Paso Back Clinic® stands out for its comprehensive wellness approach, advanced diagnostics, and patient-centered plans that go beyond basic adjustments.
If pain includes numbness, tingling, or weakness in the legs, or persists despite changes, seek evaluation to rule out serious conditions (University of Maryland Medical System, n.d.).
Start small: improve movement, setup, and stretches. If needed, contact El Paso Back Clinic® for expert help. Many in El Paso regain comfort and stay active with this care.
How Telemedicine Can Assist in the Management of Sciatica (with Integrative Chiropractic Care)
A man at home consults a chiropractor via telemedicine for back pain and sciatica.
Sciatica can make even simple tasks—like getting out of bed, sitting at a desk, or driving—feel almost impossible. When pain shoots down your leg or feels like burning, stabbing, or tingling, the idea of driving across town to sit in a waiting room can be overwhelming.
Telemedicine offers a way to get expert help for sciatica without leaving home. Telemedicine can significantly improve the quality of life for many individuals experiencing limited mobility or frequent flare-ups of pain. Spine specialists and integrative chiropractic teams now use secure video visits to evaluate symptoms, design treatment plans, and follow patients through recovery. UT Southwestern Medical Center+1
Dr. Alexander Jimenez, DC, APRN, FNP-BC, is a dual-licensed chiropractor and nurse practitioner in El Paso, Texas. His integrative model combines medical decision-making (such as imaging and prescriptions) with chiropractic and functional medicine. This blended approach fits perfectly with telemedicine because it allows him to assess nerve pain, guide movement, and adjust treatment plans over time—even when the patient is at home. El Paso, TX Doctor Of Chiropractic
What Is Sciatica?
Sciatica is not a disease by itself. It is a pattern of symptoms caused by irritation or compression of the sciatic nerve. This nerve starts in the lower back, runs through the hips and buttocks, and travels down each leg.
Common symptoms include:
Sharp or burning pain in the lower back, buttocks, and legs
Numbness, tingling, or “pins and needles” in the leg or foot
Weakness when trying to stand, walk, or lift the leg
Pain that worsens with sitting, coughing, or bending
Sciatica is usually caused by:
Herniated or bulging discs pressing on a nerve root
Spinal stenosis (narrowing of the spinal canal)
Degenerative disc disease
Muscle or joint dysfunction in the pelvis and lower back
Less commonly, tumors, infections, or serious conditions
Because sciatica can have many causes, proper evaluation and treatment planning are very important—this is where telemedicine can help you start sooner and stay on track.
What Is Telemedicine and How Does It Work for Back and Nerve Pain?
Telemedicine (also called telehealth) is health care delivered via secure video or phone rather than an in-person visit. You use a smartphone, tablet, or computer to speak with your provider, similar to a video call with family or friends.
Clinics that treat spine and nerve problems have made telemedicine a core part of their care model. They use it for first visits, follow-ups, second opinions, and surgical planning, especially for conditions like back pain, neck pain, and sciatica. UT Southwestern Medical Center+1
During a typical telemedicine visit for sciatica, your provider can:
Ask detailed questions about your pain pattern
Watch how you move on camera
Guide simple movement and strength tests
Review MRI, X-ray, or CT results
Explain treatment options, including chiropractic, physical therapy, injections, or surgery if needed
Many clinics report that they can accurately diagnose spine issues through video visits and that most telemedicine-based surgical plans do not require major changes after in-person exams. UT Southwestern Medical Center
Why Telemedicine Is Especially Helpful for Sciatica
People with sciatica often have trouble sitting, driving, or walking long distances. Telemedicine meets them where they are—literally.
Key benefits for sciatica patients
Less travel and less pain getting to care
No long car rides or sitting in waiting rooms
Easier for patients who have mobility issues or rely on others for transportation Southeast Texas Spine+1
Faster access to evaluation and treatment
Many clinics can schedule telemedicine visits sooner than in-person visits
You can start treatment earlier instead of waiting weeks to be seen
Better continuity of care
Telemedicine makes it easier to attend follow-ups, especially during long recovery plans
Providers can adjust medications, exercises, and activity limits in real time Southeast Texas Spine+1
Home-based evaluation of your real environment
Your provider can see your work setup, couch, bed, or home office
Straight-leg raise or seated leg raise while on camera
Heel and toe walking to assess nerve strength
Balance and gait observation
Imaging and tests
Your nurse practitioner or physician can order MRI, X-rays, or CT scans when needed
They may also recommend nerve tests (EMG/NCS) through in-person referrals
Spine centers and orthopedic clinics report that telemedicine visits can help determine when conservative care is sufficient and when urgent in-person care or surgery is needed. UT Southwestern Medical Center+1
Integrative Chiropractic Telemedicine for Sciatica
Integrative chiropractic telemedicine combines:
Medical care—history, diagnosis, imaging orders, prescriptions, and referrals
Chiropractic care—movement analysis, spinal and pelvic mechanics, and guided home-based therapies
Dr. Jimenez’s dual-scope role as a chiropractor and nurse practitioner is a strong example of this model. In his practice, he uses telemedicine to:
Review MRI and other imaging results with patients
Coordinate conservative care (chiropractic, physical therapy, massage, acupuncture, and functional medicine)
Monitor nerve symptoms and red flags that require fast in-person intervention
Looks for patterns of dysfunction in the lower back, pelvis, and hips
Guides you through gentle tests and movements
Designs a home exercise and stretching plan
Educates you about ergonomics, sleep positions, and movement habits
Even without hands-on adjustments, chiropractic expertise is used to understand mechanics and guide safe self-care at home. Evolve Chiropractic+2HealthCentral+2
Telemedicine and Medication Management for Sciatica
Telemedicine is also useful for medication oversight and pain management. Virtual pain management services can:
Review current medications and supplements
Start or adjust anti-inflammatory drugs, muscle relaxers, or nerve pain medications when appropriate
Help taper short-term medications to avoid long-term dependence
Coordinate with other therapies like physical therapy and chiropractic care Everlywell+1
This is important because the goal is not just to reduce pain for a few days but to manage it safely while addressing the underlying cause.
Guided Home Exercises and Self-Care for Sciatica via Telemedicine
A large part of sciatica management involves what you do every day at home. Telemedicine allows your integrative provider to coach you in real time.
Types of exercises a provider may guide over video
Always follow your own provider’s instructions. The list below is for education, not a personal prescription.
An integrative chiropractor, such as Dr. Jimenez, will often blend chiropractic reasoning (how joints and muscles are moving) with physical therapy-style exercise progressions to build strength and reduce nerve irritation over time. Integrative Medical of DFW+1
Telemedicine and Physical Therapy for Sciatica
Physical therapy is a key part of long-term sciatica care. Telemedicine makes it easier for your team to coordinate and supervise this care.
An NP–chiropractor team can:
Refer you to in-person physical therapy when you need hands-on manual work
Work with therapists to align goals: pain reduction, nerve mobility, strength, and posture
Review PT progress notes with you by video
Add or modify home exercises between in-person therapy visits
Modern integrative clinics describe physical therapy as treatment focused on your goals, your function, and your time—whether you are recovering from an acute episode of sciatica or managing long-term spine issues. Integrative Medical of DFW+1
Telemedicine for Office Workers and Remote Workers with Sciatica
Many people with sciatica sit for long periods at desks or work remotely at kitchen tables, couches, or beds. Poor ergonomics can worsen nerve pain.
Telemedicine allows providers to see your real work setup and give specific advice.
They may help you:
Adjust chair height, screen level, and keyboard position
Chiropractic-based telemedicine visits for office workers often focus on spinal alignment, hip position, and load sharing between joints — even if the provider cannot physically adjust the spine during the visit, they can teach you how to move better and reduce pressure on the sciatic nerve. tigardchiropracticautoinjury.com+1
How to Prepare for a Telemedicine Visit for Sciatica
Preparing well can make your telemedicine visit smoother and more helpful.
Before your appointment
Check your technology
Test your camera, microphone, and internet connection
Charge your device and have a backup (like a phone) ready
Choose your space
Find a quiet, private room
Make sure you have enough room to stand, walk, and lie down if needed
Gather information
List your current medications and supplements
Have your medical history and imaging reports handy
Dr. Jimenez’s clinical experience shows that when patients feel seen and supported—through regular check-ins, education, and coordinated care—they are more likely to stay consistent with their home program and achieve better long-term outcomes. El Paso, TX Doctor Of Chiropractic+1
Practical Tips for Getting the Most from Telemedicine for Sciatica
Here are some simple strategies to make telemedicine work for you:
Treat the visit like an in-person appointment
Show up on time and minimize distractions
Have a notebook handy for instructions
Be specific about your goals
“I want to sit for 30 minutes without pain”
“I want to walk around the block again”
Clear goals help your provider design better plans
Use photos or videos
Take a short video of how you walk or how you get out of a chair during painful times
Share this with your provider if their platform allows
Stay consistent with home exercises
Put reminders in your phone
Tie exercises to habits (after brushing teeth, after lunch, etc.)
Ask for a written or emailed summary
Many clinics send a visit summary through the patient portal
This can include your diagnosis, exercise plan, and red-flag symptoms
The Future: Telemedicine, Sciatica, and Integrative Care
Telemedicine is no longer just an emergency backup plan—it is a core part of modern spine and pain care. Spine centers, pain clinics, and integrative practices across the country use telemedicine to: UT Southwestern Medical Center+2NJ Spine & Orthopedic+2
Speed up diagnosis and treatment
Improve convenience for patients in pain
Coordinate care between specialists, therapists, and primary providers
Support long-term recovery with flexible follow-ups
For people with sciatica, this means you can:
Get expert guidance without leaving your home
Partner with an integrative chiropractor and nurse practitioner who can see both the nerve problem and the whole person
Combine remote consultations, at-home exercises, and lifestyle changes into a comprehensive plan
Under the care of a dual-licensed provider like Dr. Alexander Jimenez, telemedicine becomes more than a video call. It becomes a bridge between medical science, chiropractic biomechanics, and day-to-day life—helping you move from intense nerve pain toward safer movement, better function, and long-term relief. El Paso, TX Doctor Of Chiropractic+2Evolve Chiropractic+2
Introduction: My Personal Commitment to the Medico-Legal World—Bridging the Gap Between Clinical Science and Courtroom Proof
By Dr. Alex Jimenez, DC, APRN, FNP-BC | Board-Certified Nurse Practitioner & Chiropractor
Injury Medical Clinic PA, El Paso, Texas
The answer to the crucial question of whether the injury can be conclusively proven, dated, and causally connected to the traumatic event frequently determines the outcome of the high-stakes world of personal injury litigation.
My life’s work at Injury Medical Clinic PA is dedicated to answering this question with an unassailable “Yes.” I have spent decades developing a diagnostic and documentation protocol that transcends the limitations of standard clinical practice. For me, a patient is not just a set of symptoms; they are a complex medico-legal case requiring forensic-level analysis. I recognized early on that El Paso attorneys needed more than a standard radiologist’s report or a simple chiropractor’s diagnosis—they needed a comprehensive, integrated expert who could seamlessly bridge advanced musculoskeletal biomechanics (my foundation as a Chiropractic Physician, DC) with the rigorous standards of comprehensive medical management and documentation (my expertise as a Board-Certified Nurse Practitioner, APRN, FNP-BC).
This unique duality is the engine of our practice. I am not just treating the patient; I am building the legal case. My goal for every personal injury client referred to me is to deliver definitive diagnostic proof that withstands the most rigorous cross-examination, establishes clear causality using objective biomechanical markers, and determines a scientifically validated timeline for the injury—what I call injury dating.
This lengthy post serves as my own, in-depth guide to legal counsel, shedding light on the extent of my involvement in the evaluation of injuries. I meticulously examine the procedures that I use to assess patient cases. These procedures are indispensable for determining the root cause of an illness and for shedding light on the actual degree of disability and impairment that has resulted from traumatic events. I take great pride in my role as a professional in that I am committed to the idea that when a clinical case is brought before a jury, the attorneys representing the plaintiff have complete confidence in the credibility and scientific basis of the expert testimony that I provide.
Dr. Alex Jimenez, DC, APRN, FNP-BC
I will deeply discuss, from my personal experience:
The Diagnostic Imperative: My sophisticated capability to personally stage and interpret complex Magnetic Resonance Imaging (MRI) findings, distinguishing acute trauma from pre-existing conditions using forensic principles.
Causality and Timing: My systematic, proprietary methodology for establishing causality and determining the precise timing (injury dating) of trauma using advanced biomechanical and physiological markers like Modic changes and Wolff’s Law.
The Dual-Licensed Advantage: The justification and profound benefit of treatment and testimony provided by me, a dual-licensed professional, within the El Paso legal community.
Expert Credibility: How attorneys frequently utilize my expert testimony as the credible, objective voice regarding injury dating, impairment, and functional loss, ensuring my documented assessments and evaluations meet the stringent Daubert Standard.
1.0 The Diagnostic Imperative: Personally Staging and Interpreting Complex MRI Findings—Going Beyond the Radiologist’s Report
In my experience, the Magnetic Resonance Imaging (MRI) scan is the single most crucial piece of objective evidence in spinal injury litigation. However, I’ve found that a standard radiologist report often focuses primarily on morphology—describing what is seen—but fails to provide the critical context of causality and chronicity necessary for a successful legal claim.
At Injury Medical Clinic PA, I do not simply accept the outside read; I forensically interpret the physiological, mechanical, and temporal signatures embedded within the MRI data myself. I personally review every single slice and sequence because my ultimate testimony depends on my deep understanding of the images.
1.1 Meeting the Daubert Standard: My Personal Protocols for Scientific Admissibility
In the medico-legal domain, any scientific evidence I present, especially complex imaging findings, must adhere to the Daubert Standard. This requires my expert testimony to be grounded in the methods and procedures of science and supported by appropriate validation (Spinal Diagnostics, n.d.). My entire documentation protocol is built around this necessity.
I personally ensure my findings are admissible by:
Employing Validated Methodology: I utilize diagnostic criteria and staging methods that are thoroughly established in peer-reviewed orthopedic and radiological literature, such as the classification of disc pathology and the chronology of vertebral changes (Wang et al., 2017).
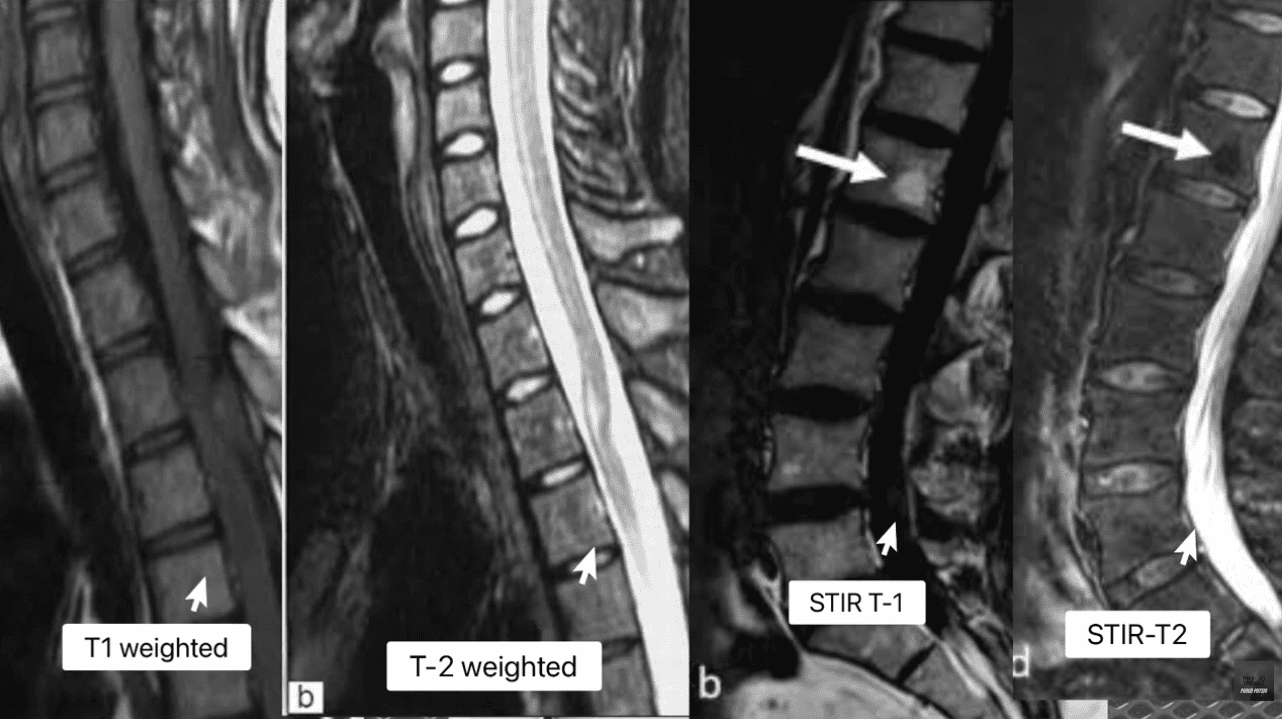
Focusing on Objectivity: My reports meticulously cite the specific MRI pulse sequences (T1, T2, STIR) and image numbers where the pathology is visualized, allowing opposing counsel and the court to verify the data. This objectivity mirrors the rigor seen in advanced quantitative neuroimaging tools like NeuroQuant®, which are successfully used to meet the Daubert standard in TBI cases (National Institutes of Health, 2022).
Simplifying Complex Science: When I testify, my goal is to translate complex terms into easily digestible concepts for the jury. I do not just state a Modic 1 change is present; I explain why it’s a marker of acute trauma, making the science reliable and understandable. This is a crucial skill that attorneys rely on me for.
1.2 Decoding the Spinal Pathologies: My Forensic Review of T1, T2, and STIR Sequences
My method for forensic MRI interpretation depends on a nuanced understanding of various pulse sequences and their physiological meaning (Advanced MRI Interpretation, n.d.). I meticulously review the T1-weighted, T2-weighted, and Short Tau Inversion Recovery (STIR) sequences because they tell different stories about the underlying tissue pathology.
MRI Staging Acute Vs Chronic Injuries
MRI Sequence
Primary Signal (Bright)
Primary Signal (Dark)
Pathological Significance
T1-Weighted
Fat (Marrow), Contrast (Gadolinium)
Water (Edema, CSF), Cortical Bone
Anatomy: Excellent for visualizing fatty infiltration (chronic muscle atrophy, Modic 2) and overall anatomical structure.
T2-Weighted
Water (Edema, CSF), Degenerated Disc
Fat (Marron), Cortical Bone
Pathology: Crucial for identifying water, making it the primary sequence for acute inflammation, disc herniation (fluid), and spinal cord changes.
STIR (Fat-Suppressed)
Water (Edema, CSF, Inflammation)
Fat (Marrow)
Acuity: The definitive sequence for acute trauma. By suppressing fat signal, any remaining bright signal is unequivocally edema, confirming acute inflammation in bone or soft tissue.
The presence of edema (abnormal fluid accumulation) in the bone marrow or soft tissues surrounding the spine is, in my professional opinion, the most powerful, objective indicator of acute trauma. This edema is the body’s immediate inflammatory response to injury and provides the temporal signature required for my precise injury dating.
1.3 Injury Dating: My Systematic Methodology for Establishing a Timeline of Trauma
The ability to accurately date an injury—to definitively state that a spinal pathology is new or acute, rather than chronic and pre-existing—is, without question, the cornerstone of a successful personal injury claim. My clinic utilizes physiological and biomechanical principles to establish this timeline with forensic precision.
1.3.1 Modic Changes: The Gold Standard for Vertebral Endplate Chronology
Modic changes are alterations in the vertebral body endplates and adjacent bone marrow, visible on MRI, that reflect different stages of pathological response. I rely on them heavily because they provide an objective and scientifically validated marker for estimating the age of an injury (Wang et al., 2017; Spinal Diagnostics, n.d.).
Determining Age of Injury Via MRI Staging
Modic Type 1 (MC1) – The Acute Signature: MC1 represents the acute inflammatory stage characterized by bone marrow edema. When I see this, I know I’m looking at an injury that is active and recent.
My Staging: I stage this based on the specific signal patterns: Dark on T1 and Bright on T2/STIR (Spinal Diagnostics, n.d.). The persistent bright signal on STIR is the definitive confirmation of active, acute inflammation.
My Testimony: I explain to attorneys that MC1 changes typically resolve or transition to the fatty Type 2 changes within approximately 6 to 8 weeks (Spinal Diagnostics, n.d.). Therefore, the presence of MC1 is a powerful, objective sign of recent trauma, often correlating directly with the patient’s reported high pain scores (Jensen et al., 2024). When a defense expert attempts to argue degeneration, my documentation of MC1 provides the irrefutable evidence of a specific, new acute event.
Modic Type 2 (MC2) – The Chronic Transition: MC2 represents the replacement of normal bone marrow with fatty tissue (Wang et al., 2017). This is a marker of a more subacute or chronic condition.
My Staging: I stage this based on the characteristic Bright on T1/T2 but crucially, Dark on STIR (fat-suppressed) sequence (Spinal Diagnostics, n.d.).
My Testimony: I use MC2 to show pre-existing degeneration, which ironically, strengthens my credibility. By acknowledging a chronic condition at one level (MC2) while simultaneously proving an acute injury at another (MC1), I demonstrate objectivity and isolate the liability to the new, acute trauma.
1.3.2 Wolff’s Law and My Chronological Interpretation of Bone Spurs
Further reinforcing my injury dating is my application of Wolff’s Law, a fundamental biomechanical principle that bone tissue adapts to the loads placed upon it (Spinal Diagnostics, n.d.). Chronic instability leads to the formation of osteophytes (bone spurs) as the body attempts to stabilize the segment through the piezoelectric effect (Spinal Diagnostics, n.d.).
The Biomechanical Timeline: I rely on scientific research confirming that it takes approximately six months for a bone spur to become radiographically visible or significant (Spinal Diagnostics, n.d.).
My Medico-Legal Implication: When I review a patient’s initial X-rays or CT scans following an MVA, and I find a complete absence of chronic osteophyte formation in the affected segment (e.g., C5-C6), yet the MRI shows an acute disc herniation, I have created an unassailable timeline. The absence of the six-month marker (the bone spur) provides strong supporting evidence that the soft-tissue injury is acute and causally related to the recent collision.
1.4 The Crucial Differential Diagnosis: My Approach to Acute Trauma vs. Chronic Degeneration
Distinguishing new trauma from old, asymptomatic degeneration is essential for proving the extent of damage. I use specific MRI markers to draw this clear line, transforming a murky diagnosis into legal certainty.
Many accident victims have some degree of pre-existing, asymptomatic degeneration. The defense always targets this reality. My expertise lies in identifying and quantifying the acute-on-chronic injury (Spinal Diagnostics, n.d.).
The tell-tale radiological sign I look for is the clear observation of newly extruded disc material extending beyond the border of a mature, pre-existing osteophyte (Spinal Diagnostics, n.d.). The osteophyte, being a chronic boney change, acts as an anatomical baseline for pre-injury status. Any disc material that has been forcefully extruded beyond this chronic bony landmark is, by definition, new trauma and directly quantifiable aggravation. I personally measure this new extrusion and document its displacement in my reports.
1.4.2 The Vacuum Disc Phenomenon: The Irrefutable Marker of Old Pathology
I use the Vacuum Disc Phenomenon as another definitive marker of a chronic, old condition. This finding—nitrogen gas (a distinct signal void, appearing black) within the center of the disc on all MRI sequences (T1, T2, and STIR)—is a reliable sign of old, irreversible degenerative changes and instability (Spinal Diagnostics, n.d.; Advanced MRI Interpretation, n.d.).
When I find a vacuum disc at one level, I include it in my report. This establishes my objectivity, allowing me to state confidently that while one level is chronic, the adjacent, non-vacuum level that displays Modic 1 changes is acute and causally related to the MVA. This approach prevents the defense from collapsing the entire spine into a single, pre-existing condition.
1.5 Analysis of Complex Non-Disc Spinal Pathologies: The Hidden Injuries
Beyond disc herniation, I specialize in the advanced interpretation of other complex spinal pathologies frequently misunderstood or missed by general practitioners, yet vital for proving injury.
1.5.1 The Spinal Epidural Venous Plexus (Batson’s Plexus): Dural Tenting
The Spinal Epidural Venous Plexus (Batson’s Plexus) is a valveless network highly susceptible to sudden pressure changes (Advanced MRI Interpretation, n.d.). In court, I must distinguish between normal physiological changes and pathological ones.
My Differential Diagnosis: Trauma can cause a physiological venous dilation because a disc extrusion can push on the thecal sac—a phenomenon known as dural tenting. This must be carefully distinguished from a pathological Epidural Varix (a symptomatic dilation that causes neural compression) (Advanced MRI Interpretation, n.d.). I rely on sequences like contrast-enhanced MRI (when medically necessary) and non-contrast flow-sensitive sequences to confirm the difference. Incorrectly diagnosing normal venous dilation as a compressive pathology can undermine an entire claim, and my careful distinction preserves my credibility.
1.5.2 Post-Traumatic Muscle Changes: Fatty Infiltration of the Multifidus
The deep lumbar muscles, particularly the multifidus, are essential stabilizers. I have seen time and again how pain-induced inhibition leads to rapid structural changes in this muscle.
My Injury Dating and Causality: This muscle transformation begins to appear on imaging as early as 2 to 12 weeks post-injury (Spinal Diagnostics, n.d.; Central Ohio Spine and Joint, n.d.). Fatty infiltration (visible as a bright signal on T1-weighted images) is highly associated with chronic pain and instability. The degree of infiltration is a crucial prognostic indicator, correlating negatively with functional improvement (Xu et al., 2024). The presence and severity of multifidus fatty infiltration provide powerful objective evidence of chronic functional impairment and instability directly resulting from the traumatic event. I use this finding to prove permanent injury to the core stabilizing system, which is critical for future medical damages.
2.0 Establishing Causality: My Biomechanical and Legal Framework
The defense is designed to argue that a plaintiff’s pain is due to aging or unrelated issues. My documentation provides the scientific and legal rebuttals necessary to establish clear causation—a process I personally manage from the moment the patient walks through my door.
2.1 The “Eggshell Plaintiff” Doctrine: My Documentation Strategy
A foundational principle in personal injury law is the “Eggshell Plaintiff” Rule: a defendant must take the victim as they find them (Cornell Law School, n.d.). This means the defendant is fully liable for the plaintiff’s injuries, even if those injuries are more severe than they would have been in an average person due to an existing, pre-disposed condition (Rafi Law Firm, n.d.).
My Personal Role: Successfully applying this doctrine in court requires meticulous documentation, which I provide by:
Defining the Baseline: Precisely evaluating the pre-accident state (using the Vacuum Disc, Modic 2/3, and chronic osteophyte timelines). I acknowledge the pre-existing state without minimizing the new trauma.
Quantifying the Acute Change: Using Modic Type 1 and Acute-on-Chronic findings to objectively demonstrate the new, causally related injury (Spinal Diagnostics, n.d.).
Proving Exacerbation: Establishing that the traumatic event (MVA) directly aggravated the pre-existing condition, resulting in new symptoms, functional loss, and permanent impairment. My reports meticulously connect the mechanism of injury to the exacerbation, ensuring the court grasps the full scope of liability.
2.2 The Biomechanical Signatures of Soft Tissue and Ligamentous Injury (Whiplash)
Soft tissue injuries, or whiplash-associated disorders (WAD), are commonly challenged as subjective. My examination protocol goes beyond standard range of motion checks to confirm structural injury.
Occult Ligamentous Injury: I utilize the MRI’s fluid-sensitive sequences (STIR) to search for occult tears and sprains. I look for the hyperintense (bright) signal in the interspinous and supraspinous ligaments (Spinal Diagnostics, n.d.), which represents edema and tearing. This finding transforms a subjective “sprain/strain” into an objective, structural instability.
Facet Capsular Edema: The facet joints are often injured during MVA hyperflexion/hyperextension. I meticulously look for capsular edema or effusion (bright signal around the joint) on T2/STIR images. This is a highly specific finding for acute trauma to the joint capsule, which often correlates to localized, severe pain.
The Biomechanical Correlation: I thoroughly document the mechanism of injury (e.g., rear-end collision, specific speed data if available) and link the vector of force to the specific pathology found (e.g., a rear-end vector causing anterior compression and posterior ligamentous tearing) (NCBI, 2023). This correlation is crucial in court to overcome defense arguments that the forces were insufficient to cause the documented injury.
3.0 The Dual-Licensed Advantage: My DC & APRN/FNP-BC Model in El Paso
The most compelling aspect of the Injury Medical Clinic PA model, and the primary reason for my success in the medico-legal field, is my unique qualification as a dual-licensed professional. The integration of the Doctor of Chiropractic (DC) and the Advanced Practice Registered Nurse/Family Nurse Practitioner (APRN/FNP-BC) licenses creates a holistic, comprehensive, and legally powerful care model that is unmatched in the El Paso area.
3.1 Comprehensive Care Models: My Integrated Approach
I bring together the best of both worlds, creating a single source of expertise that satisfies both the clinical and legal standards of care:
My Role as a Chiropractic Physician (DC): I provide unparalleled expertise in spinal biomechanics, functional assessment, manual therapy, and the non-surgical management of complex musculoskeletal injuries. The DC perspective is critical for evaluating the long-term functional impairment caused by disc, facet, and ligament pathology.
My Role as a Nurse Practitioner (APRN/FNP-BC): I provide the essential medical framework, including the ability to prescribe medication (e.g., muscle relaxants, neuropathic agents), order and manage advanced diagnostic testing (e.g., specific, medically-prescribed MRI protocols, nerve conduction studies), manage co-morbidities, and, most crucially, write comprehensive, authoritative medical-legal reports and provide expert testimony that carries the weight of a board-certified medical professional, satisfying the standard medical scrutiny of the court.
This integration ensures the patient receives optimal physical rehabilitation alongside rigorous medical documentation, all under one practice. My reports are medical documents authored by an APRN/FNP-BC, while the therapeutic details reflect the specialized biomechanical insight of a DC. This synergy is invaluable to attorneys.
3.2 Justification for Dual-Licensed Intervention: Case Archetypes in My Practice
I manage these three case archetypes every day, and they demonstrate why my dual-licensed approach is often medically and legally necessary:
Case Archetype
Clinical Presentation in My Clinic
My Dual-Licensed Treatment Rationale
Medico-Legal Value in My Reports
Type 1: Complex Cervical WAD with Radiculopathy.
Patient presents with neck pain, headaches, and confirmed numbness/tingling in the arm. MRI shows a C5-C6 disc bulge impinging on the nerve root.
My DC Expertise: Focus on specific spinal mobilization to reduce segmental dysfunction and restore cervical curve stability. My APRN Expertise: Prescribe gabapentin or NSAIDs for nerve pain, order Electromyography/Nerve Conduction Velocity (EMG/NCV) studies, and administer facet or trigger point injections if necessary (Mayo Clinic, 2024).
Causality: The combined finding of clinical radiculopathy (confirmed by NCV—a medical test I ordered) and the biomechanical trauma (my DC diagnosis) is documented under a single, authoritative medical record (my APRN report). I can objectively testify to the severity of the neurological deficit.
Type 2: Acute Lumbar Disc Extrusion with Failed Conservative Care.
Patient suffers acute L5-S1 disc extrusion causing severe, debilitating sciatica that is not responding to basic care.
My DC Expertise: Implement specialized non-surgical spinal decompression protocols and advanced core stabilization exercises. My APRN Expertise: Medically evaluate the patient’s pain using objective outcome measures (Oswestry Disability Index), rule out Red Flags (Cauda Equina), manage opioid/non-opioid medication, and critically, document the failure of conservative care, which justifies the trajectory toward advanced interventions or surgical consultation.
Damages & Prognosis: My comprehensive documentation of conservative care failure establishes the persistent, debilitating nature of the injury. This robust history is essential for the attorney to justify the valuation of both past and high-value future medical costs in front of a jury.
Type 3: Acute-on-Chronic Spinal Instability.
Patient has pre-existing, asymptomatic spinal stenosis (Modic Type 2 changes), but the MVA results in new symptoms and a new Modic Type 1 change at the adjacent level.
My DC Expertise: Focus on restoring segmental stability to the traumatized level while protecting the degenerated level. My APRN Expertise: Personally interpret the complex MRI (Modic 1 vs. Modic 2) to clearly delineate the acute injury (liability) from the pre-existing condition (eggshell) (Spinal Diagnostics, n.d.).
Defeating the Defense: My precise diagnostic report legally isolates the acute trauma (Modic 1) from the chronic degeneration (Modic 2/Vacuum Disc), providing the attorney with clear, objective evidence to apply the Eggshell Plaintiff doctrine and secure recovery for the aggravation and new injury.
4.0 My Credible Expert Witness Testimony: Illuminating Disability and Driving Monetary Recoveries
My ultimate function for the legal community is to serve as the credible, objective voice that clarifies the patient’s impairment for the jury. My testimony is built upon the synthesis of advanced clinical diagnostics and established medico-legal principles that I personally adhere to.
4.1 The Credibility Foundation: My Daubert-Compliant Testimony
Attorneys frequently utilize my expertise because my methodology is rooted in the scientific method, ensuring my opinions are admissible under the Daubert Standard. My expert testimony is not merely anecdotal; it is a direct presentation of verifiable scientific data:
Measurable Markers: When I testify, I don’t just state an opinion. I point to the imaging and explain that the Modic Type 1 change is not random, but an established scientific finding with a specific 6-8 week timeline, proving the freshness of the bone trauma (Wang et al., 2017). I use analogies, like comparing the Modic 1 change to a fresh bruise on the bone, which makes the complex science undeniable to a layperson jury.
Biomechanically Sound Conclusions: I personally explain how the physics of the impact (the vector, the forces) translates into the specific, demonstrable injury, such as the mechanism by which a sudden flexion-extension event causes an annular tear (Paredes et al., 2023). This link between physics and physiology is critical for proving causation.
The Power of the Dual Role: When I stand before the court, my opinion integrates the highest standard of musculoskeletal diagnosis (DC) with the authority of advanced medical management (APRN). I am uniquely positioned to counter both the defense’s biomechanics expert and their medical expert.
4.2 My Method for Translating Pathology into Permanent Impairment and Disability
The value of a personal injury case is directly linked to the demonstrability and permanency of the injury. My detailed reports translate abstract medical findings into tangible, compelling evidence of long-term disability for the jury.
4.2.1 Quantifying Functional Loss: From Imaging to Activities of Daily Living (ADLs)
I shift the focus from what the injury looks like on an MRI to how it permanently impairs the patient’s life:
Multifidus Fatty Infiltration: I explain to the jury that the increased bright signal on the patient’s T1 MRI is not simply “fat,” but the objective, measurable sign of a permanent loss of spinal stability (Central Ohio Spine and Joint, n.d.). I elaborate that the muscle is no longer functional, leading to chronic instability, increased risk of re-injury, and an inability to perform basic ADLs like prolonged sitting, standing, or lifting—directly correlating to a lower quality of life and permanent functional loss.
Irreversible Cord Damage (Myelomalacia): If I identify Myelomalacia (softening, necrosis, and scarring of the spinal cord tissue) on a T2 image (hyperintensity within the cord), I use this to establish a definitive, catastrophic, permanent neurological injury (Spinal Diagnostics, n.d.). This finding is irreversible and dictates a life of permanent neurological deficits, which is irrefutable evidence of severe disability that warrants significant monetary recovery.
4.2.2 Linking Causality to Prognosis and Future Medical Costs
My reports connect the initial traumatic event to the long-term cost of care. This is vital for the attorney’s calculation of future medical damages.
Permanent Impairment Rating (PIR): I use objective prognostic indicators—such as the severity of multifidus infiltration (Xu et al., 2024), the persistence of Modic 1 changes, or the presence of irreversible ligament instability—to generate a scientifically grounded Permanent Impairment Rating (PIR) using the AMA Guides to the Evaluation of Permanent Impairment.
Future Medical Requirements: The report then outlines the need for future care (e.g., ongoing chiropractic maintenance, periodic APRN follow-ups, medication management, or potential injections/surgical consultations) directly necessitated by the MVA. This robust justification of future needs is critical for maximizing the final settlement or jury award.
By establishing causation, chronicity, and prognosis through my rigorous, peer-reviewed methodology, I provide the unassailable evidence necessary to maximize the plaintiff’s recovery and to position legal counsel to confidently present even the most complex clinical cases before a jury. My role is to ensure that the injury is not only treated effectively but also documented exhaustively, establishing Injury Medical Clinic PA as the premier clinic for injuries resulting from accidents in the El Paso area.
National Institutes of Health (NIH). (2022). Updated Review of the Evidence Supporting the Medical and Legal Use of NeuroQuant® and NeuroGage® in Patients With Traumatic Brain Injury. PMC – PubMed Central. https://pmc.ncbi.nlm.nih.gov/articles/PMC9027332/
Understanding Nerve Conditions of the Spine: Causes, Symptoms, and Treatments
The spine is a critical part of the body, serving as a highway for nerves that transmit signals between the brain and the rest of the body. When something goes wrong with these nerves—whether they’re compressed, irritated, or damaged—it can lead to a range of uncomfortable symptoms like pain, numbness, tingling, or weakness. These issues, known as nerve-related spine conditions, can affect the back, arms, or legs and stem from various causes, including injuries, degenerative conditions, or infections. In this article, we’ll explore these conditions, their symptoms, causes, and how they’re diagnosed and treated, with a special focus on integrative approaches like those used by Dr. Alexander Jimenez, a chiropractor and nurse practitioner in El Paso, Texas. We’ll also look at how chiropractic care, targeted exercises, massage therapy, acupuncture, and integrative medicine can promote healing and prevent long-term problems.
What Are Nerve-Related Spine Conditions?
Nerve-related spine conditions happen when the spinal nerves or spinal cord are compressed, irritated, or damaged. The spine is made up of bones called vertebrae, which protect the spinal cord—a bundle of nerves that carries messages to and from the brain. Between the vertebrae are intervertebral discs, which act as cushions, and small openings called foramina, where nerve roots exit the spinal cord to connect to other parts of the body. When these nerves or the spinal cord itself are affected, it can disrupt the signals, leading to symptoms like pain, numbness, tingling, or weakness (Mayo Clinic Health System, n.d.).
Some of the most common nerve-related spine conditions include:
Radiculopathy: Often referred to as a “pinched nerve,” this condition occurs when a nerve root is compressed or irritated as it exits the spine. It can cause pain, numbness, or weakness that radiates along the nerve’s path. For example, lumbar radiculopathy can lead to sciatica, a condition characterized by pain that shoots from the lower back down the leg (Cleveland Clinic, n.d.).
Spinal stenosis refers to the narrowing of the spinal canal, which puts pressure on the spinal cord or nerve roots. It’s often caused by aging or degenerative changes and can lead to symptoms like back pain, numbness, or difficulty walking (HSS Education, n.d.).
Herniated or Bulging Discs: Discs can bulge or herniate (when the inner gel-like material pushes out), pressing on nearby nerves. This can cause pain, tingling, or weakness in the arms or legs, depending on where the disc is located (Penn Medicine, n.d.).
Degenerative Conditions: Conditions like arthritis or bone spurs can narrow the spaces where nerves travel, causing compression and symptoms like pain or stiffness (Health Central, n.d.).
Trauma or Injury: Accidents, such as car crashes or falls, can damage the spine and compress nerves, leading to immediate or delayed symptoms (Verywell Health, n.d.).
Infections or Structural Abnormalities: Infections, tumors, or abnormal spine alignment (like scoliosis) can also press on nerves, causing similar symptoms (MSD Manuals, n.d.).
These conditions can range from mild annoyances to serious issues requiring immediate medical attention, especially if they cause severe symptoms like loss of bladder or bowel control, which may indicate cauda equina syndrome, a medical emergency (Verywell Health, n.d.).
Symptoms of Nerve-Related Spine Conditions
The symptoms of nerve-related spine conditions depend on where the nerve compression or damage occurs and the severity of the condition. Common symptoms include:
Pain: This can be sharp, burning, or aching and may stay in one spot (like the neck or lower back) or radiate to other areas, such as the arms, buttocks, or legs. For example, sciatica often causes burning pain that travels from the lower back to the legs (Penn Medicine, n.d.).
Numbness or Tingling: These sensations, often described as “pins and needles,” can occur in the hands, arms, feet, or legs, depending on the affected nerve (Cleveland Clinic, n.d.).
Weakness: Muscle weakness in the arms, hands, or legs can make it hard to lift objects, walk, or maintain balance. In severe cases, it can cause issues like foot drop, where a person struggles to lift their foot while walking (Johns Hopkins Medicine, n.d.).
Loss of Coordination: Compression of the spinal cord (myelopathy) can affect fine motor skills, making tasks like buttoning a shirt or writing difficult (Verywell Health, n.d.).
Balance Issues: Spinal stenosis or myelopathy can cause trouble walking or maintaining balance, sometimes described as feeling like “walking through mud” (Spine-health, n.d.).
Loss of Bladder or Bowel Control: This is a rare but serious symptom that requires immediate medical attention, as it may signal cauda equina syndrome (HSS Education, n.d.).
Symptoms can develop suddenly, like after an injury, or gradually, as with degenerative conditions like arthritis. If you experience severe or worsening symptoms, especially loss of bladder or bowel control, seek medical care right away.
Causes of Nerve-Related Spine Conditions
Nerve-related spine conditions can have many causes, ranging from natural aging to sudden injuries. Here are some of the main culprits:
Degenerative Changes: As people age, the spine can undergo wear and tear. Osteoarthritis can cause bone spurs, and degenerative disc disease can lead to bulging or herniated discs, both of which can press on nerves (Mayo Clinic Health System, n.d.).
Herniated or Bulging Discs: When a disc’s inner material bulges or herniates, it can push against nearby nerves, causing pain or numbness. This is a common cause of radiculopathy, including sciatica (Penn Medicine, n.d.).
Spinal Stenosis: The spinal canal can narrow due to thickened ligaments, bone spurs, or other changes, putting pressure on the spinal cord or nerve roots (Cleveland Clinic, n.d.).
Trauma: Car accidents, sports injuries, or falls can fracture vertebrae, dislocate joints, or cause swelling that compresses nerves, leading to severe consequences. For example, a car crash can lead to whiplash, which may cause nerve damage in the neck (Solomon Law, n.d.).
Infections: Spinal infections, like abscesses, can press on the spinal cord or nerves, causing pain and neurological symptoms (MSD Manuals, n.d.).
Structural Abnormalities: Conditions like scoliosis (abnormal spine curvature) or tumors can compress nerves, leading to symptoms like pain or weakness (Johns Hopkins Medicine, n.d.).
Inflammatory or Autoimmune Conditions: Diseases like rheumatoid arthritis can cause inflammation that compresses nerves, contributing to symptoms (OrthoTOC, n.d.).
Each cause can lead to different symptoms and requires specific diagnostic and treatment approaches to address the root issue.
Diagnosing Nerve-Related Spine Conditions
Diagnosing nerve-related spine conditions starts with a doctor asking about your symptoms and medical history, followed by a physical exam to check for numbness, weakness, reflexes, and posture. Depending on the findings, additional tests may be needed to pinpoint the cause (Penn Medicine, n.d.). Common diagnostic tools include:
Imaging tests, such as X-rays, CT scans, or MRIs, can reveal the spine’s structure, including bones, discs, and nerves, to identify compression or damage (Spine Info, n.d.).
Nerve Conduction Studies (NCS) and Electromyography (EMG): These tests assess the function of nerves and muscles, and can help confirm nerve damage (Spine Info, n.d.).
Myelogram: A special X-ray or CT scan with contrast dye can highlight pressure on the spinal cord or nerves (Spine Info, n.d.).
Dr. Alexander Jimenez, a chiropractor and nurse practitioner in El Paso, Texas, uses a dual-scope approach to diagnosis, combining his expertise in chiropractic care and advanced nursing. His clinic utilizes advanced neuromusculoskeletal imaging techniques, such as MRIs and CT scans, to obtain a clear picture of the spine’s condition. Dr. Jimenez correlates patient injuries—whether from work, sports, car accidents, or personal incidents—with clinical findings to create a precise diagnosis. This approach ensures that the treatment plan targets the specific cause of the nerve issue, whether it’s a herniated disc, spinal stenosis, or trauma-related damage (Jimenez, n.d.).
Treatment Options for Nerve-Related Spine Conditions
Treatment for nerve-related spine conditions depends on the cause, severity, and symptoms. Most doctors start with conservative (non-surgical) treatments, moving to surgery only if needed. Here’s an overview of common treatments:
Non-Surgical Treatments
Medications: Over-the-counter pain relievers, such as ibuprofen, or prescription medications, like gabapentin, can help manage pain and inflammation (Spine Info, n.d.).
Physical Therapy: Targeted exercises can strengthen muscles, improve posture, and reduce pressure on nerves. Physical therapy is often effective for radiculopathy and spinal stenosis (Cleveland Clinic, n.d.).
Epidural Steroid Injections: These deliver anti-inflammatory medication directly to the affected nerve root, reducing pain and swelling (Penn Medicine, n.d.).
Chiropractic Care: Adjustments and manipulations can realign the spine, relieving pressure on nerves. Dr. Jimenez’s clinic utilizes chiropractic techniques to treat conditions such as sciatica and herniated discs, with a focus on restoring spinal alignment (Jimenez, n.d.).
Massage Therapy: This can relax tight muscles, improve blood flow, and reduce nerve irritation, especially for conditions caused by muscle tension or spasms (Inova, n.d.).
Acupuncture: By stimulating specific points, acupuncture can reduce pain and promote natural healing, often used alongside other treatments (Total Spine Ortho, n.d.).
Activity Modification: Avoiding activities that worsen symptoms, like heavy lifting, can help the spine heal (Penn Medicine, n.d.).
Surgical Treatments
If conservative treatments are not effective, surgery may be necessary. Common procedures include:
Laminectomy: Removes part of a vertebra to create more space for nerves, often used for spinal stenosis (Spine Info, n.d.).
Microdiscectomy: Removes part of a herniated disc that’s pressing on a nerve, commonly used for radiculopathy (Spine Info, n.d.).
Spinal Fusion: Fuses vertebrae together to stabilize the spine, used for severe degenerative conditions or trauma (Inova, n.d.).
Dr. Jimenez’s clinic takes an integrative approach, combining chiropractic care with targeted exercises, massage therapy, and acupuncture to treat nerve-related spine conditions. For example, a patient with sciatica resulting from a herniated disc may receive spinal adjustments to realign the spine, exercises to strengthen core muscles, and acupuncture to alleviate pain. This holistic approach addresses the root cause while promoting long-term healing and preventing future problems (Jimenez, n.d.).
Dr. Alexander Jimenez’s Integrative Approach in El Paso
Dr. Alexander Jimenez, a chiropractor and nurse practitioner in El Paso, Texas, has extensive experience treating nerve-related spine conditions caused by work, sports, personal, or motor vehicle accident injuries. His clinic uses a dual-scope approach, blending chiropractic expertise with advanced medical knowledge to provide comprehensive care. Here’s how his clinic handles these cases:
Treating Different Types of Injuries
Work Injuries: Repetitive motions or heavy lifting at work can lead to conditions like herniated discs or radiculopathy. Dr. Jimenez uses spinal adjustments, targeted exercises, and ergonomic advice to relieve nerve compression and prevent recurrence (Jimenez, n.d.).
Sports Injuries: Athletes may suffer nerve compression from trauma or overuse. The clinic employs chiropractic care, physical therapy, and massage to restore function and reduce pain, helping athletes return to their activities (Jimenez, n.d.).
Personal Injuries: Falls or other accidents can cause nerve damage. Dr. Jimenez’s team uses advanced imaging to assess the injury and creates personalized treatment plans, often including acupuncture and exercise (Jimenez, n.d.).
Motor Vehicle Accident (MVA) Injuries: Car crashes can cause whiplash or other trauma that compresses nerves. The clinic provides detailed diagnostic assessments, including MRIs, to identify nerve damage and offers treatments like spinal adjustments and massage to promote healing (Solomon Law, n.d.; Jimenez, n.d.).
Medical Care and Legal Documentation
Dr. Jimenez’s clinic is skilled in handling the medical and legal aspects of injury cases, especially for MVAs. They provide thorough documentation of injuries, diagnoses, and treatments, which is critical for insurance claims or legal cases. For example, if a patient has radiculopathy from a car accident, the clinic documents the injury’s impact on their daily life, the diagnostic findings (like MRI results), and the treatment plan. This detailed paperwork supports patients in legal proceedings while ensuring they receive proper medical care (Jimenez, n.d.).
Integrative Medicine for Healing and Prevention
Dr. Jimenez’s approach emphasizes integrative medicine, combining chiropractic care with other therapies to address the cause of nerve issues and enhance overall health. For instance:
Chiropractic Adjustments: Realign the spine to relieve nerve pressure, effective for conditions like sciatica or herniated discs.
Targeted Exercises: Strengthen muscles around the spine to improve stability and prevent future injuries.
Massage Therapy: Reduces muscle tension and improves circulation, aiding in nerve healing.
Acupuncture: Stimulates natural pain relief and promotes recovery, especially for chronic pain.
Lifestyle Changes: Advice on posture, ergonomics, and nutrition helps prevent long-term problems (Jimenez, n.d.).
This integrative approach not only treats the immediate symptoms but also focuses on long-term health, reducing the risk of chronic pain or recurring issues.
How Integrative Medicine Promotes Healing
Integrative medicine, as practiced by Dr. Jimenez, combines conventional medical treatments with complementary therapies to address the whole person, not just the symptoms. For nerve-related spine conditions, this approach offers several benefits:
Natural Healing: Chiropractic care and acupuncture stimulate the body’s natural healing processes, reducing reliance on medications (Total Spine Ortho, n.d.).
Pain Reduction: Therapies such as massage and acupuncture can help reduce pain levels, thereby improving quality of life (Inova, n.d.).
Improved Function: Exercises and adjustments restore mobility and strength, helping patients return to normal activities (Cleveland Clinic, n.d.).
Prevention: By addressing underlying causes, like poor posture or weak muscles, integrative medicine reduces the risk of future nerve problems (Jimenez, n.d.).
For example, a patient with spinal stenosis might receive adjustments to improve spinal alignment, exercises to strengthen their core, and massage to relax tight muscles. Over time, these treatments can reduce nerve compression, improve mobility, and prevent the condition from worsening.
Preventing Long-Term Problems
Preventing long-term nerve-related spine issues involves addressing the root causes and maintaining spinal health. Here are some strategies:
Maintain Good Posture: Proper posture reduces strain on the spine and nerves (Mayo Clinic Health System, n.d.).
Stay Active: Regular exercise, especially core-strengthening workouts, supports the spine and prevents injuries (Cleveland Clinic, n.d.).
Utilize ergonomics: Adjust workstations or lifting techniques to prevent repetitive strain (Jimenez, n.d.).
Manage Weight: Excess weight can put pressure on the spine, worsening nerve conditions (Health Central, n.d.).
Seek Early Treatment: Addressing symptoms early with chiropractic care or physical therapy can prevent conditions like radiculopathy from becoming chronic (Spine Info, n.d.).
Dr. Jimenez’s clinic emphasizes these preventive measures, educating patients on lifestyle changes to keep their spines healthy and reduce the risk of future nerve issues.
Conclusion
Nerve-related spine conditions, like radiculopathy, spinal stenosis, and herniated discs, can cause significant discomfort and disrupt daily life. These conditions stem from various causes, including degenerative changes, trauma, infections, or structural issues, and lead to symptoms like pain, numbness, tingling, and weakness. Through proper diagnosis using imaging and clinical assessments, doctors can pinpoint the cause and recommend treatments, ranging from medications and physical therapy to surgery in severe cases. Integrative approaches, like those used by Dr. Alexander Jimenez in El Paso, combine chiropractic care, targeted exercises, massage therapy, and acupuncture to treat injuries from work, sports, or accidents while promoting natural healing. By addressing the root cause and focusing on prevention, these methods can help patients recover and avoid long-term problems. If you’re experiencing symptoms of a nerve-related spine condition, consult a healthcare provider to explore your treatment options and start your journey to recovery.
Dr. Alex Jimenez: Pioneering Integrative Care as a Chiropractor and Nurse Practitioner
Dr. Alex Jimenez, a licensed chiropractor and board-certified nurse practitioner based in El Paso, Texas, brings over 25 years of expertise to his Injury Medical & Chiropractic Clinic practice. His dual licensure provides unique insights into the etiologies, pathogenesis, and treatment of complex clinical conditions, enabling him to deliver patient-centered, integrative care that bridges physical medicine, functional medicine, and advanced diagnostics. Combining chiropractic expertise with nurse practitioner-driven medical management, Dr. Jimenez offers comprehensive treatment protocols tailored to acute and chronic conditions, promoting metabolic resilience, longevity, and whole-person wellness.
Dual Expertise: Chiropractic and Nurse Practitioner Roles
Dr. Jimenez’s practice stands out due to his ability to integrate the biomechanical focus of chiropractic care with a nurse practitioner’s diagnostic and therapeutic scope. As a chiropractor, he specializes in restoring musculoskeletal function, particularly after trauma, neck, back, spine, and soft tissue injuries. His chiropractic interventions emphasize non-invasive techniques, such as spinal decompression, manual adjustments, and functional rehabilitation, to alleviate pain and enhance mobility.
As a board-certified nurse practitioner, Dr. Jimenez employs evidence-based medicine to address systemic and metabolic dysfunctions. His expertise extends to managing chronic degenerative disorders, hormonal imbalances, weight loss, sexual health, and pain syndromes. This dual perspective allows him to identify underlying disease causes, from biomechanical misalignments to physiological imbalances, and design treatment regimens that address symptoms and root causes.
The synergy of these roles enables Dr. Jimenez to offer a holistic approach that is particularly effective for complex conditions such as sciatica, fibromyalgia, disc herniation, spondylolisthesis, and chronic neck or back pain. His integrative protocols combine functional medicine assessments, lifestyle interventions, and advanced diagnostics to achieve homeostasis and physiological balance.
Treatment Protocols: Evidence-Based and Patient-Centered
Drawing from integrative protocols outlined on his website, www.chiromed.com, Dr. Jimenez employs a multidisciplinary approach to patient care. His treatment plans are grounded in evidence-based medicine, functional medicine, and lifestyle wellness strategies, tailored to each patient’s unique health profile, lifestyle, and medical history. Below are key components of his integrative care model:
1. Chiropractic Care and Functional Rehabilitation
Spinal Decompression: Non-surgical decompression therapy is used to relieve pressure on spinal discs, addressing conditions like disc herniation, sciatica, and spinal stenosis. This modality promotes healing by improving blood flow and nutrient delivery to affected areas.
Manual Adjustments: Targeted adjustments correct spinal misalignments, reduce nerve compression, and restore joint mobility. These are particularly effective for whiplash, scoliosis, and poor posture.
Functional Strength Training: Dr. Jimenez designs conditioning programs to enhance recovery and prevent re-injury. These programs are tailored for athletes and individuals seeking optimal performance and incorporate mobility, flexibility, and agility training.
2. Functional Medicine Assessments
Functional medicine tools evaluate metabolic, hormonal, and nutritional status. These assessments identify the root causes of conditions such as fatigue, weight gain, or chronic pain, enabling precise interventions.
Advanced diagnostic protocols, including blood panels and imaging, provide data-driven insights into etiologies and pathogenesis. This allows Dr. Jimenez to address underlying dysfunctions rather than merely masking symptoms.
3. Lifestyle and Nutritional Interventions
Weight Loss and Metabolic Resilience: Dr. Jimenez integrates nutritional counseling and metabolic optimization strategies to support sustainable weight loss and prevent chronic diseases like diabetes or cardiovascular disorders.
Hormone and Sexual Health: Personalized regimens address hormonal imbalances and sexual dysfunction, improving quality of life and overall wellness.
Pain Management: Nutritional and lifestyle modifications complement physical therapies to manage chronic pain syndromes, reducing reliance on pharmaceuticals.
4. Specialized Care for Complex Conditions
Sciatica and Disc Injuries: Dr. Jimenez employs targeted decompression and rehabilitation protocols to alleviate nerve compression and restore function.
Chronic Degenerative Disorders: Conditions like fibromyalgia, arthritis, and spondylolisthesis are managed through integrative plans that combine physical therapy, nutritional support, and metabolic optimization.
Sports and Auto Accident Injuries: Tailored rehabilitation programs address soft tissue damage, shoulder injuries, and whiplash, ensuring rapid recovery and long-term resilience.
5. Advanced Wellness Programs
Dr. Jimenez’s clinic offers comprehensive wellness programs on longevity, skin care, and hair loss. These programs integrate nutritional supplementation, lifestyle coaching, and cutting-edge therapies to promote vitality and aesthetic health.
High-level conditioning programs optimize performance for athletes, incorporating functional strength training and recovery-focused interventions.
Integrative Team and Clinic Highlights
Injury Medical & Chiropractic Clinic is El Paso’s largest mobility, flexibility, and agility center, integrating chiropractors, nurse practitioners, registered nurses, nutritionists, and physical performance trainers. The clinic’s multidisciplinary team collaborates to deliver personalized care, ensuring patients achieve measurable health outcomes. Key services include:
Acupuncture: A Complementary therapy to reduce pain and promote relaxation.
Advanced Nutritional Programs: Evidence-based dietary plans to support metabolic health and recovery.
Physical Performance Training: Programs to enhance fitness, prevent injuries, and optimize athletic performance.
The clinic accepts major insurances, including Aetna, Blue Cross Blue Shield, Cigna, and First Health, making care accessible to a broad patient base.
Insights from Dual Licensure
Dr. Jimenez’s licensure as both a chiropractor and nurse practitioner provides him with a comprehensive understanding of disease processes and treatment modalities. His chiropractic training equips him to address biomechanical dysfunctions, while his nurse practitioner expertise allows him to manage systemic conditions with a medical lens. This dual perspective enhances his ability to:
Clarify Etiologies: By combining musculoskeletal assessments with metabolic and hormonal evaluations, Dr. Jimenez identifies multifactorial causes of conditions, ensuring targeted interventions.
Understand Pathogenesis: His knowledge of disease progression informs proactive treatment plans that halt or reverse degenerative processes.
Design Appropriate Regimens: Integrating physical, nutritional, and medical therapies, Dr. Jimenez creates synergistic treatment plans that address both symptoms and underlying dysfunctions.
This integrative approach is particularly valuable for patients with chronic or multifactorial conditions, as it addresses the interplay between physical, metabolic, and lifestyle factors.
Patient-Centered Care: In-Person and Online
Dr. Jimenez’s practice emphasizes personalized attention, whether patients visit in person at 11860 Vista Del Sol, Suite 128, El Paso, TX 79936, or engage through telehealth. His functional medicine series, accessible via www.dralexjimenez.com, educates patients on holistic health principles, covering topics from spinal health to metabolic optimization. The website features:
Informative Content: Blog posts, articles, and videos provide insights into chiropractic care, functional medicine, and injury rehabilitation.
Patient Testimonials: Success stories highlight the transformative impact of Dr. Jimenez’s care, showcasing outcomes for conditions like sciatica, sports injuries, and chronic pain.
Appointment Booking: A user-friendly interface allows patients to schedule in-person or online consultations, with clear guidance on what to expect during their first visit.
Commitment to Education and Community Health
Dr. Jimenez is dedicated to empowering patients through education. His website is comprehensive, offering evidence-based information on health conditions, treatment options, and wellness strategies. By fostering health literacy, Dr. Jimenez enables patients to make informed decisions and take charge of their well-being.
His commitment extends to the El Paso community, where he aims to expand access to integrative care. Dr. Jimenez promotes proactive health management and preventive care through workshops, online content, and community outreach.
Conclusion
Dr. Alex Jimenez’s dual expertise as a chiropractor and nurse practitioner positions him as a leader in integrative medicine. His ability to bridge physical medicine with systemic health management allows him to address complex clinical issues with precision and compassion. Dr. Jimenez delivers personalized care that promotes healing, resilience, and longevity by leveraging evidence-based protocols, advanced diagnostics, and lifestyle interventions.
For more information or to schedule an appointment, visit www.dralexjimenez.com or contact the clinic at +1-915-412-6677.
Is applying ice the best option for individuals who experience an acute back strain injury?
Temperature Treatment
Ice temperature treatment, also known as cryotherapy or cold therapy, is a treatment that uses freezing temperatures to reduce pain and swelling. It can be applied in a variety of ways, including:
Ice packs:
Ice massage
Coolant sprays
Whirlpools
Ice baths
Ice is usually recommended for acute injuries and is a common and simple way to treat pain and swelling. Individuals can buy freezable gel packs or make their own with ice cubes in a plastic bag or towel. Heat therapy tends to be used more with chronic issues involving muscle spasms to increase blood circulation.
How Ice Relieves Pain and Reduces Inflammation
Ice temperature treatment works by:
Narrowing blood vessels slows blood circulation to the injured area and soft tissues and reduces swelling.
Reduced blood flow also helps control excessive swelling.
Ice has a short-term analgesic-numbing effect. The coldness numbs nerve endings, relieving pain symptoms.
Relieving the pain allows the muscles to relax.
Controlling blood circulation helps control pain by reducing the flow of irritating chemicals that can inundate the injury site. These chemicals are a natural and the correct response to inflammation, but the ice keeps them in check to help control pain.
After a Back Injury
For a back strain injury, ice and anti-inflammatory medication like NSAIDs are the first line of treatment during the inflammatory phase, which usually lasts 24 to 72 hours. Because heat can increase inflammation by increasing blood circulation, it is not recommended as an initial treatment. After the first few days, most doctors and pain specialists recommend using ice or heat, depending on the individual’s preference. While researchers continue to investigate the best ways to treat acute injuries, most doctors still recommend ice as the first line of defense for back injuries.
A review of studies evaluated 20 different treatment categories to learn about their safety and effectiveness. (McIntosh G. & Hall H. 2011) Treatments included over-the-counter pain medications, acupuncture, McKenzie exercises, other back exercises, and temperature treatments. Regarding temperature treatment, the review found moderate evidence that using a heat wrap 5 days after the injury could help relieve pain. However, there was not enough evidence to support the effectiveness of any of the temperature treatments, necessitating more research. (McIntosh G. & Hall H. 2011)
Physical Therapy and Activity
The review found that prolonged rest should be avoided, and gentle exercise and a progressive return to physical activity should be encouraged to achieve the best outcomes for pain relief and restoring function. Staying active significantly reduces time off from work and chronic disability for up to 1 year compared to traditional medical treatment. (McIntosh G. & Hall H. 2011) Research also found that introducing physical therapy early on could expedite recovery. Mobility work, targeted exercises, and strengthening exercises have been shown to relieve pain, reduce injury recurrence, and improve overall function. More research supports physical activity and exercise as effective treatment options for acute lower back strains. However, further research regarding temperature treatments is required. (French S. D. et al., 2006) (See Q. Y. et al., 2021)
Injury Medical Chiropractic and Functional Medicine Clinic
It is important to talk with a healthcare provider to determine the cause and extent of the injury to provide individualized patient education regarding treatment. This can include physical therapy, rest, health coaching, medication, and surgery, which may be recommended in certain cases. Overcoming these limitations is possible. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop an optimal health and wellness solution. We focus on what works for you to relieve pain, restore function, prevent injury, and help mitigate the pain through spinal adjustments that help the body realign itself. They can also work with other medical professionals to integrate a treatment plan to resolve musculoskeletal issues.
Beyond the Surface: Understanding the Effects of Personal Injury
References
McIntosh, G., & Hall, H. (2011). Low back pain (acute). BMJ clinical evidence, 2011, 1102.
French, S. D., Cameron, M., Walker, B. F., Reggars, J. W., & Esterman, A. J. (2006). A Cochrane review of superficial heat or cold for low back pain. Spine, 31(9), 998–1006. https://doi.org/10.1097/01.brs.0000214881.10814.64
See, Q. Y., Tan, J. B., & Kumar, D. S. (2021). Acute low back pain: diagnosis and management. Singapore Medical Journal, 62(6), 271–275. https://doi.org/10.11622/smedj.2021086
Back pain is one of the most common reasons for seeking health care. Individuals dealing with back pain but don’t know the cause may have some inflammatory joint disease or autoimmune condition. Can seeing a rheumatologist help?
Rheumatologist
Depending on what’s causing the back pain, individuals may need to see their primary doctor for a referral. Individuals are recommended to see a rheumatologist if they have back pain that doesn’t come from an injury that doesn’t go away after a few weeks, pain that comes back after treatment, or symptoms that suggest a rheumatic condition. Rheumatologists treat severe or persistent back pain and are experts in autoimmune diseases, including lupus, Sjogren’s syndrome, rheumatoid arthritis, ankylosing spondylitis, axial spondylitis, Psoriatic arthritis, and other forms of inflammatory or autoimmune arthritis.
What Do They Do?
A rheumatologist is an internist or pediatrician who has completed special training in treating conditions that are:
Inflammatory
Autoimmune
Related to painful joint disease
The doctors diagnose, treat, and manage these conditions long-term. Depending on diagnosis and care needs, they may also lead or be part of a team that includes other healthcare providers.
Symptoms
When muscles ache, pain presents, or joints hurt, and especially if there are signs of inflammation that don’t go away, seeing a healthcare provider is recommended. Symptoms of inflammation include:
Redness
Swelling
Pain
Stiffness
Loss of joint function
Usually, to see a rheumatologist, individuals need a referral from their primary care provider and may be referred when:
There is no evidence of a back injury.
At-home therapies like heat application, prescription medications, or physical therapy are unsuccessful.
There is uncertainty about what’s causing the back pain, but I suspect it’s rheumatological.
Blood tests for inflammatory markers or certain antibodies yield abnormal results.
There is a diagnosis of a rheumatic condition and recommend a specialist to manage it.
There is a family history of a rheumatic or autoimmune condition that may cause back pain.
Some types of arthritis can cause permanent, progressive joint damage.
Conditions
Conditions that can affect the spine and cause back pain and are treated by a rheumatologist include: (Johns Hopkins Medicine, 2024)
Rheumatoid arthritis (RA)
This often starts in smaller joints of the hands and feet and later moves to the neck and/or back.
It can also affect different body organs and have systemic symptoms.
Ankylosing Spondylitis (AS)
Primarily a disease of the spine, it may also impact the shoulders, hips, knees, and ankles.
Systemic symptoms, including fever and fatigue, can manifest.
Axial Spondylitis
This primarily affects the spine, chest, and pelvis.
It may also cause problems with the connective tissue, eyes, bowel, and skin.
Psoriatic Arthritis (PsA)
Pain in the lower back is common, especially in severe cases.
It can affect other joints and cause psoriasis.
Reactive Arthritis
This is a reaction to infection.
It is more common in the limbs, hands, and feet joints but can involve the spine.
Enteropathic Arthritis
This mainly affects the spine but can include other joints.
It is associated with inflammatory bowel disease.
Autoimmune diseases that don’t specifically target the spine but can also cause back pain include:
Lupus
Sjögren’s syndrome
Hashimoto’s thyroiditis
Finding a Doctor
Individuals may be fine with their primary healthcare provider’s choice regarding which rheumatologist to see. However, they may want to research other options to ensure the right rheumatologist is chosen. Things to look at include:
Search online medical directories.
Visit the websites of the doctors being considered to learn more about their training, approach, and specialties.
Check online reviews.
Check on health insurance coverage.
Ask members of the healthcare team, friends, and family for recommendations.
Contact rheumatologists’ offices to see if they are accepting new patients.
Once decided, pass along the information to the primary care doctor so they can make the referral.
Preparing For The Initial Visit
Before seeing a new rheumatologist, take a few minutes to prepare so you can make the most of the appointment. Individuals will want to have:
A list of back-related symptoms, including frequency and severity.
A list of what makes symptoms better or worse.
A copy of recent test results and records from other doctors.
Individuals can ask their provider/s to send their medical information to the rheumatologist’s office in advance.
A list of treatments that have been tried and how well they worked.
A list of all medications, over-the-counter and prescription, supplements, and herbal products taken.
A list of medication allergies.
Complete medical history and family history of potentially related diseases.
A list of any questions regarding conditions, treatment, etc.
If possible, fill out any paperwork for the new office beforehand to save time on the appointment day.
Injury Medical Chiropractic and Functional Medicine Clinic
Talking with a healthcare provider is important. Injury Medical Chiropractic and Functional Medicine Clinic works with primary healthcare providers and specialists to develop personalized treatment programs. Using an integrated approach to treating injuries and chronic pain syndromes to improve flexibility, mobility, and agility and help individuals return to normal activities. If other treatments are needed, Dr. Jimenez has teamed up with top surgeons, clinical specialists, medical researchers, and rehabilitation providers.
Quick Patient Initiation Process
References
Hospital for Special Surgery. (2023). What Is a Rheumatologist and What Conditions Do They Treat? https://www.hss.edu/conditions_what-is-a-rheumatologist.asp#when
Yale University School of Medicine. Dee, J. E. (2021). 5 reasons why a patient should see a rheumatologist. https://medicine.yale.edu/news-article/5-reasons-to-see-a-rheumatologist/
National Institute of Arthritis and Musculoskeletal and Skin Diseases. (2023). Autoimmune diseases. Retrieved from https://www.niams.nih.gov/health-topics/autoimmune-diseases
Johns Hopkins Medicine. (2024). Spinal arthritis (arthritis in the back or neck). https://www.hopkinsmedicine.org/health/conditions-and-diseases/spinal-arthritis
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine