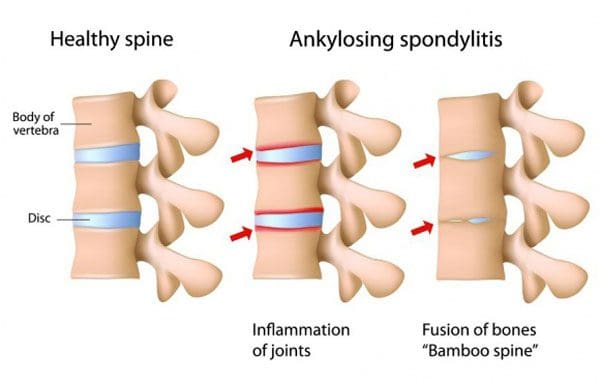
Individuals with ankylosing spondylitis have a new treatment option that was previously used for rheumatoid arthritis. It is a medication that belongs to a class known as JAK inhibitors. Ankylosing spondylitis combines joint pain with reduced mobility. Ankylosing spondylitis is different because in severe cases, the bones in the spine can fuse together, literally reducing mobility.
The disease typically begins with pain and stiffness in the back. This is usually after some time of inactivity. Symptoms start before the age of 45 and develop gradually. There is no cure for ankylosing spondylitis but there are treatments that can improve symptoms and put the condition into remission. Ankylosing spondylitis treatment is the most successful when addressed early before irreversible damage to the joints begins.
Janus Kinase Inhibitors
Janus kinase inhibitors have traditionally been used to treat:
Rheumatoid arthritis
Psoriatic arthritis
Ulcerative colitis
The medication works by decreasing the immune system�s activity. Janus kinase inhibitor drugs affect several cellular compounds that are important in the development and progression of ankylosing spondylitis. Currently, there are only three Janus kinase inhibitor medications available in the United States and FDA-approved to treat rheumatoid arthritis:
Xeljanz
Rinvoq
Olumiant
Each of the approved inhibitors targets specific enzymes
Current Ankylosing Spondylitis Treatments
Janus kinase inhibitors are not given to individuals right away. However, it could be an option if first and second-line treatments are not working. Treatments usually consist of:
First-Line Treatments
NSAIDs
Nonsteroidal anti-inflammatory medications are the most commonly used to treat ankylosing inflammation, pain, and stiffness.
Chiropractic
Chiropractic physical therapy is a major part of ankylosing spondylitis treatment keeping the spine flexible and as healthy as possible. A chiropractic/physical therapy team design and develop specific exercises to fit individual needs, which include:
Stretching and Range-of-motion exercises help maintain flexibility in the joints
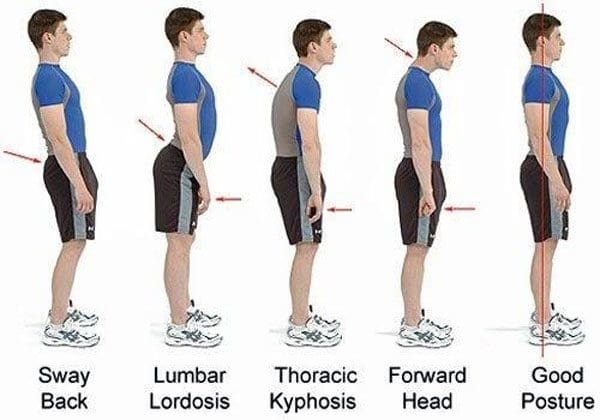
Sleeping and walking posture adjustment exercises
Abdominal and spinal exercises to maintain a healthy posture
If nonsteroidal anti-inflammatory medications do not relieve symptoms, then biological medications could be prescribed. This class of medications includes:
Tumor necrosis factor blockers work by targeting cell protein that is part of the immune system, known as tumor necrosis alpha. This protein causes inflammation in the body, and the blockers suppress it.
Interleukin 17 Inhibitors
Interleukin 17 in the body’s immune system defends against infection. It uses an inflammatory response to fight infections. The IL-17 inhibitors suppress the inflammatory response and help reduce symptoms.
Other Treatment Options
Lifestyle Adjustments
Following a medical treatment plan is often combined with diet and lifestyle adjustments that are recommended to help with the condition, these include:
Most individuals with ankylosing spondylitis do not require surgery. However, a doctor could recommend surgery if there is joint damage, the hip-joint needs to be replaced, or if the pain is severe.
Inhibitor Potential
Studies are ongoing in the treatment of ankylosing spondylitis. The drug is currently in Phase 3 trials for the treatment of adults. The trial results have shown patients with active ankylosing spondylitis showed improvement in:
Fatigue
Inflammation
Back pain
The study enrolled adults with active ankylosing spondylitis who took at least two NSAIDs that were ineffective at treating symptoms. Most of the participants were men, average age of 41, and no prior usage of biologic disease-modifying antirheumatic drugs.
Janus kinase could become a standard treatment
There is still not enough research to make a prediction, but the data is promising. The inhibitors seem to be a safe option when used in a properly screened, well-matched setting that includes regular monitoring. The inhibitors appear to be effective and have the advantages of being taken orally and working fast.
Body Composition
Osteoarthritis and weight loss
Being obese has shown to be a high-risk factor for the development of osteoarthritis. This is not only from the effects of extra weight on the body’s joints but also as a result of the inflammatory effects of adipose tissue. The lower back, hips, and knees, bear the majority of the body’s weight.
An excess amount of adipose tissue on the body’s midsection and legs has been shown to negatively impact the weight-bearing joints. Promoting Lean Body Mass and encouraging weight loss lowers the risk of osteoarthritis and improves an individual’s quality of life. Exercise is regarded safe for individuals with osteoarthritis and should be incorporated to improve body composition, reduce Body Fat Mass, improve Lean Body Mass and maintain a healthy weight.
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
References
Hammitzsch A, Lorenz G, Moog P. Impact of Janus Kinase Inhibition on the Treatment of Axial Spondyloarthropathies. Frontiers in Immunology 11:2488, Oct 2020; doi 10.3389/fimmu.2020.591176.�https://www.frontiersin.org/article/10.3389/fimmu.2020.591176, accessed Jan 21, 2021.
van der Heijde D, Baraliakos X, Gensler LS, et al. Efficacy and safety of filgotinib, a selective Janus kinase 1 inhibitor, in patients with active ankylosing spondylitis (TORTUGA): results from a randomized, placebo-controlled, phase 2 trial.�Lancet.�2018 Dec 1;392(10162):2378-2387. doi: 10.1016/S0140-6736(18)32463-2. Epub 2018 Oct 22. PMID: 30360970.�https://pubmed.ncbi.nlm.nih.gov/30360970/�accessed Jan 19, 2021.
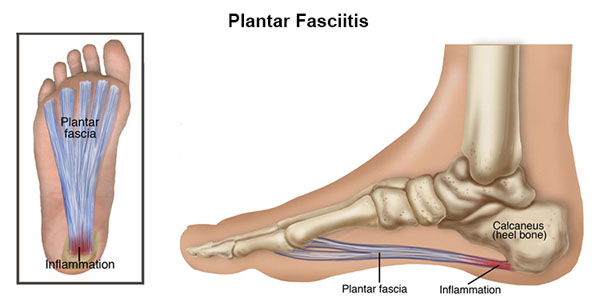
One of the most likely causes of foot/heel pain is inflamed plantar fascia, which causes plantar fasciitis. It can be a painful and common injury from overuse of the ligaments in the foot. When this pain presents, it can make an individual not want to walk or place any type of pressure on the feet, as the pain worsens with pressure or impact on the foot. �
�
Chiropractic care doesn�t just treat the spine but can help with various other musculoskeletal issues throughout the body. With chiropractic adjustments, rest, icing, and exercises, the ligaments, and tissues of the feet are worked out, massaged, and stretched back to their normal range. �
�
Plantar Fascia
There is a ligament called the plantar fascia. It runs along the bottom of the foot and connects the toes to the heel. The plantar fascia absorbs shock and helps support the feet when walking. However, ligament tension can begin to increase, specifically when standing for long periods. When the tension reaches its limit, small tears can begin to form along with inflammation causing pain.
The pain occurs when walking, standing, or immediately after waking up. The condition can happen to anyone but is more likely to become an issue for those who stand or walk as a regular part of their job, home activity, etc. Side effects from the foot pain often cause individuals to adjust their walking gait to avoid feeling discomfort, that stresses the rest of the body like the muscles, ligaments, joints that can lead to various types of injury/s. �
�
Chiropractic Treatment
Individuals with an inflamed plantar fascia often experience a shooting/stabbing pain that worsens in the morning or after standing or sitting for an extended time. Repetitive impact on the feet and poor arch support from shoes cause small tears to happen over time from the continued stress. If it has just started the pain can be treated with ice and rest, but they are not for solving the root cause. Chiropractic can help bring pain relief that lasts along with recurrence prevention. Here are some a few ways a chiropractor can help: �
Ankle Re-alignment
Ankle misalignment can contribute to plantar fasciitis at the plantar fascia has to work harder to move the foot without the ankle’s support. Manipulation and realignment of the ankle will improve foot function.
�
Massage
A chiropractor along with a physical therapy team can be utilized for soft tissue massage and trigger point therapy to release tension.
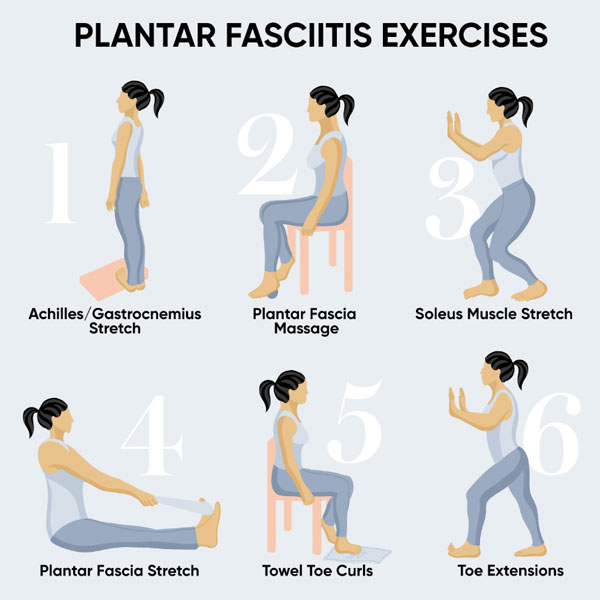
Exercises and Stretches
Various stretching and exercising techniques can be implemented to help speed up the healing process. A chiropractor will work the individual through exercises and stretches designed to relieve inflammation and stretch out the tissue. Specific exercises will also be taught to help strengthen the lower leg muscles to stabilize the heel and help prevent pain.
�
Posture
A chiropractor will correct any improper posture/s that has contributed to the foot pain or has become a way of being able to function as a result of the pain. This will return the individual to a normal gait when walking and running. Pressure on the feet and plantar fascia will be alleviated.
�
Spinal/Hip Re-alignment
Individuals learn to avoid pain by walking/moving in a different way than how the body is supposed to. This results in pain in the hips and back, as the body is being pulled in various ways. Manipulation and mobilization will be used to realign the body to its proper form.
�
Footwear/Orthotics
A chiropractor will make adjustments to the feet, ankles, and spine to reduce pain and relieve the pressure on the plantar fascia. Supportive footwear and orthotics could be recommended for extended/preventative care. Once diagnosed with a foot problem wearing proper shoes that support the feet is essential.
Orthotics can also help prevent injury to the back, joints, and muscles that were stretched or over-worked from an abnormal gait. When the pressure is relieved, the ligament starts to heal. This can take a few weeks. The result is a healthier heel/foot with proper function. Chiropractic can accelerate the healing process combined with home care. If pain is presenting in the heel, do not delay and focus on healing the foot.
Reduce Plantar Fasciitis
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
References
Goff, James D, and Robert Crawford. �Diagnosis and treatment of plantar fasciitis.��American family physician�vol. 84,6 (2011): 676-82.
Tight and sore hamstrings commonly occur during workout and exercise, but can just as easily result from a fall or other accident. Individuals usually experience pain located at the back of the thigh with associated weakness along with the feeling of the muscles becoming tighter and a consistent soreness. Consistent tightness in the back of the legs is not only uncomfortable but can also make movement difficult.
Many individuals stretch every day, do yoga, etc trying to relieve hamstring tension, with short-term relief only to have the tightness return. This is frustrating but more importantly, indicates that the problem might not have to do with the muscle�s length. There could be an underlying issue that needs to be identified and addressed. A chiropractic approach will diagnose and treat the root of the pain, not just the symptoms.
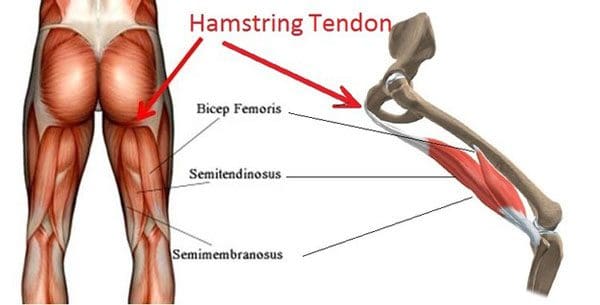
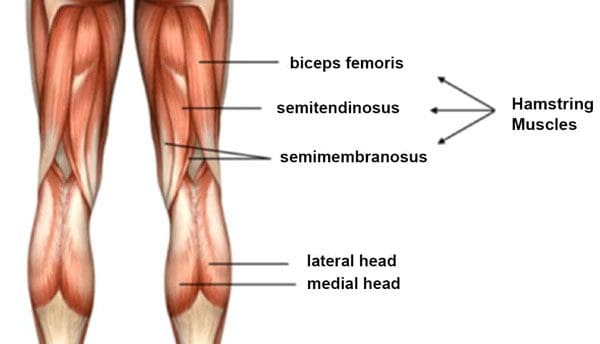
Hamstring/s Tightness
The hamstring is not a single string. It is a set of three muscles that run along the back of the thigh. The muscles allow for the bending of the leg at the knee. With a hamstring strain, one or more of these muscles can become overloaded and can start to tear. Strains often happen during activities that involve running, jumping, and/or sudden stopping and starting. This is where stretching doesn’t help, however, a chiropractic adjustment can help.
Weak Muscle Compensation
One possible cause for the tightness has to do with various related muscles and not the hamstrings themselves. Muscles that typically stabilize and facilitate movement could be too weak or are not functioning properly. What usually happens is that the muscles that are active have to work harder to compensate for the others that are not working/functioning properly.
The tension in the hamstrings can be alleviated through chiropractic exercises/stretches that activate the stabilizing muscles and get the circulation moving to promote strength and take the pressure off the hamstrings.
These muscle weaknesses can be caused by spinal misalignments that pull the body in an awkward fashion, throwing the body’s balance off. Each condition feeds the other as the hamstrings have to work harder, the body leans to the side that doesn’t cause pain, causing the spine to shift out of alignment and so begins the awkward body shifting to avoid the pain cycle. A chiropractic adjustment will restore balance and stability to the entire body.
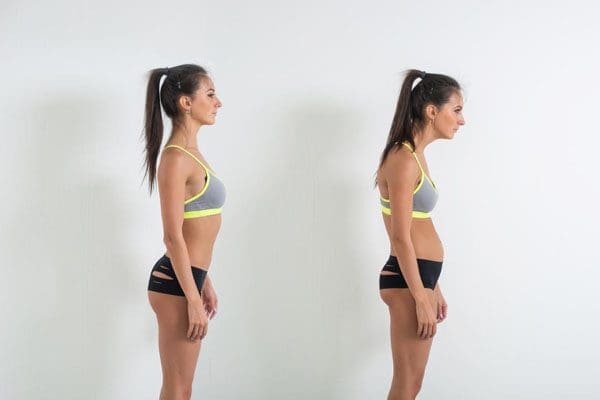
A Pelvic Tilt
Pelvic tilt could be a contributing factor for tightness and soreness. This comes from:
Poor posture
Lack of physical activity
Weight gain
These factors can cause the pelvis to shift forward ever so slightly. But just that slight tilting could be pulling on the hamstrings. In order to rectify the tilt, exercise is recommended, and chiropractic manipulation to realign any spinal shifting.
Sciatic Irritation
Another issue is sciatic nerve irritation that could mimic tightness in the muscles. The sciatic nerve runs down the back of the leg and the irritation could make the hamstring appear to be tight. This is where stretching the hamstrings can worsen the condition by irritating the sciatic nerve, causing inflammation.
The sciatic nerve could also be experiencing irritation from spinal misalignment. A vertebral disc could be bulging or herniated. This could inflame the nerve root. A bone spur or inflamed joint could be impinging/compressing on the nerve root exits.
A chiropractic treatment plan will relieve the tension being placed on the nerve and allow for proper blood circulation and transmission of signals without interruptions. Talk to a chiropractor about an examination to identify the exact root causing the discomfort.
Advanced Chiropractic Treatment
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
References
Hoskins, Wayne, and Henry Pollard. �Hamstring injury management–Part 2: Treatment.��Manual therapy�vol. 10,3 (2005): 180-90. doi:10.1016/j.math.2005.05.001
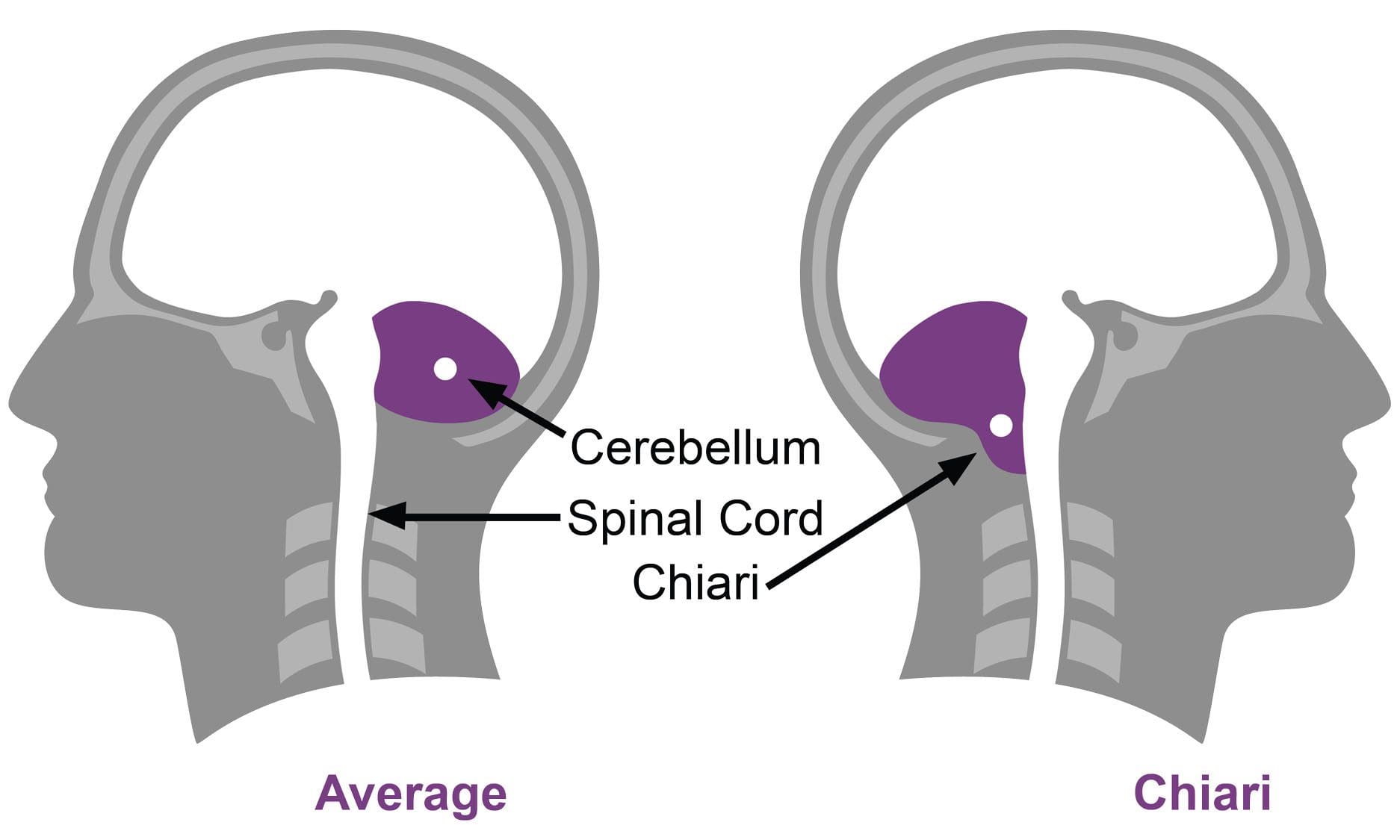
Chiari malformation is a condition that causes brain tissue to extend out and settle into the spinal canal. It protrudes out where the skull and neck meet. It occurs because part of the skull is too small or shaped in a unique way that allows part of the brain to settle into the foramen magnum. The foramen magnum is a large opening at the bottom of the skull. The brain’s nerves go through into the spinal canal and join the spinal cord. However, only the nerves should be present. The brain should not be able to push/press/leak through. When it does this is Chiari malformation.
Causes
Chiari malformation can be caused by structural problem/s with the:
Brain
Skull
Spinal canal
Structural conditions/issues can be present at birth, which are congenital defects. This is also called primary Chiari malformation and is not caused by any other condition. Secondary Chiari malformations are caused by something else, most often through surgery. This is extremely rare, but it is possible to develop after having surgery to remove a tumor in the skull or neck region. A surgeon could have removed too much bone while removing the tumor. This allowed the brain to settle into the open space.
Types
There are 4 types and are categorized by how much brain tissue protrudes into the spinal canal.
Type I
This is the adult version and is also the most common.
It is usually first noticed and discovered from an examination for something else. Most individuals don’t realize that they have Chiari malformation unless the symptoms are severe. With Type I a part of the brain, specifically the cerebellar tonsils settle into the foramen magnum.
Type II
Type II is also known as Arnold-Chiari malformation. This is the pediatric version. Symptoms are more severe with Type II because more brain tissue comes through. With this type, the cerebellar tonsils and some of the brainstem protrude. With Type II myelomeningocele, which is a form of spina bifida is a concern. What happens is the vertebrae and spinal canal do not close correctly before birth, so the spinal cord has no protection.
Type III
This type also affects children and is more severe than types 1 or 2. Here a significant portion of the brain, including the cerebellum and the brainstem protrude all the way through the foramen into the spinal canal.
The symptoms vary based on the type and severity. The most common symptom is a headache. Individuals with a Chiari malformation usually have headaches in the occipital region of the brain. This is the back of the head, right where the skull joins the cervical spine/neck. The headaches can be aggravated being in certain positions and actions, tilting the head back, and coughing. Typical symptoms include:
However, Chiari malformation can interrupt the flow of cerebrospinal fluid. Cerebrospinal fluid is necessary to protect the brain and spinal cord. If the normal flow is disrupted it becomes more difficult for the brain and spinal cord to send/receive nerve messages. The pressure built up can also cause nerve issues/problems. For some individuals, symptoms can come and go. This depends on how much cerebrospinal fluid has built up. Individuals with Type I sometimes don’t have any symptoms. It all depends on the severity.
Diagnosis
Diagnosis is done with a magnetic resonance imaging test or MRI. The MRI will show the various parts of the brain, skull, spinal cord, and spinal canal. They will be able to see abnormalities that could point to Chiari malformation.
Treatment
The recommended treatment depends on the severity. If pain is presenting a doctor could recommend pain medications to help manage the pain. Non-steroidal anti-inflammatory meds could also be recommended to reduce inflammation. Analgesics or pain killers can be recommended. Often both non-steroidal anti-inflammatories and analgesics are available in over-the-counter and prescription. The doctor will figure out the best medication treatment plan.
Surgery can be used to relieve symptoms and is the only way to relieve the pressure on the spinal cord and nerves. The goal is to stop the malformation from worsening. Surgeons use a posterior fossa decompression procedure. The surgeon removes part of the skull to make more room for the brain to sit in. This takes the pressure off the brain and spinal cord, and should reduce the neurological symptoms and problems. The surgeon may increase the size of the dura or the sac around the brain.
Laminectomies at C1 and C2, which are the first and second levels of the neck and are utilized to make more room for the brain. The surgeon will place a patch that is made from animal or synthetic tissue that will grow into the dura. The patch makes the dura bigger, which allows more room for the brain. Not all surgeries involve the dural patch.
Neck Pain Chiropractic Care
Dr. Alex Jimenez�s Blog Post Disclaimer
The scope of our information is limited to chiropractic, musculoskeletal, physical medicines, wellness, and sensitive health issues and/or functional medicine articles, topics, and discussions. We use functional health & wellness protocols to treat and support care for injuries or disorders of the musculoskeletal system. Our posts, topics, subjects, and insights cover clinical matters, issues, and topics that relate and support directly or indirectly our clinical scope of practice.*
Our office has made a reasonable attempt to provide supportive citations and has identified the relevant research study or studies supporting our posts. We also make copies of supporting research studies available to the board and or the public upon request. We understand that we cover matters that require an additional explanation as to how it may assist in a particular care plan or treatment protocol; therefore, to further discuss the subject matter above, please feel free to ask Dr. Alex Jimenez or contact us at 915-850-0900. The provider(s) Licensed in Texas& New Mexico*
PODCAST: Dr. Alex Jimenez, Kenna Vaughn, Lizette Ortiz, and Daniel “Danny” Alvarado discuss nutrition and fitness during these times. During quarantine, people have become more interested in improving their overall health and wellness by following a proper diet and participating in exercise. The panel of experts in the following podcast offers a variety of tips and tricks on how you can improve your well-being. Moreover, Lizette Ortiz and Danny Alvarado discuss how they’ve been helping their clients achieve their optimal well-being during these COVID times. From eating fruits, vegetables, lean meats, good fats, and complex carbohydrates to avoiding sugars and simple carbohydrates like white pasta and bread, following a proper diet and participating in exercise and physical activity is a great way to continue to promote your overall health and wellness. – Podcast Insight
If you have enjoyed this video and/or we have helped you in any way
please feel free to subscribe and share us.
Thank You & God Bless.
Dr. Alex Jimenez RN, DC, MSACP, CCST
PODCAST: Dr. Alex Jimenez and Dr. Marius Ruja discuss the importance of personalized medicine genetics and micronutrients for overall health and wellness. Following a proper diet and participating in exercise alone isn’t enough to make sure that the human body is functioning properly, especially in the case of athletes. Fortunately, there are a variety of tests available that can help people determine if they have any nutritional deficiencies that may be affecting their cells and tissues. Vitamin and mineral supplements can also ultimately help improve an individual’s overall health and wellness. While we may not be able to change certain aspects of our genes, Dr. Alex Jimenez and Dr. Marius Ruja discuss that following a proper diet and participating in exercise while taking the proper supplements, can benefit our genes and promote well-being. – Podcast Insight
If you have enjoyed this video and/or we have helped you in any way
please feel free to subscribe and share us.
Thank You & God Bless.
Dr. Alex Jimenez RN, DC, MSACP, CCST
IFM's Find A Practitioner tool is the largest referral network in Functional Medicine, created to help patients locate Functional Medicine practitioners anywhere in the world. IFM Certified Practitioners are listed first in the search results, given their extensive education in Functional Medicine